
Nicotine effects on affective response in depression-prone smokers
11
ORIGINAL INVESTIGATION Nicotine effects on affective response in depression-prone smokers Bonnie Spring & Jessica Werth Cook & Bradley Appelhans & Anne Maloney & Malia Richmond & Jocelyn Vaughn & Joseph Vanderveen & Donald Hedeker Received: 7 June 2007 / Accepted: 3 October 2007 / Published online: 25 October 2007 # Springer-Verlag 2007 Abstract Rationale Comorbidity between cigarette smoking and depression is thought to arise because depression-prone smokers self-administer nicotine to improve mood. Yet little evidence supports this view, and nicotine’ s effect on positive affect deficiency in depression remains largely unstudied. Objectives We hypothesized that (1) nicotine would dispel negative affect and enhance positive affect and (2) effects would be stronger for smokers vulnerable to depression, particularly during a depressed state. Materials and methods Regular smokers (N =165) were recruited from the community: 63 with no history of major depressive disorder (MDD), 61 with recurrent past but no current MDD, and 41 with both current and past MDD. During four sessions, participants smoked either a nicoti- nized (NIC+) or denicotinized (NIC−) cigarette double blind after experiencing a negative mood induction or while undergoing a positive mood induction. Positive and negative affects were measured at baseline and at two time points after smoking. Results Previously depressed smokers showed a heightened positive mood response to positive mood induction when smoking a nicotinized cigarette. Nicotine also increased the degree to which positive mood induction dispelled negative mood in depression-vulnerable smokers. Finally, nicotine worsened the negative affect response to negative mood induction for all groups. Conclusion Self-administering nicotine appears to improve depression-prone smokers’ emotional response to a pleasant stimulus. Keywords Nicotine . Depression . Tobacco smoking . Affect . Tobacco use Cigarette smoking is associated with both trait and state aspects of vulnerability to major depressive disorder (MDD) (Breslau et al. 2004; Hitsman et al. 2003). Smokers are twice as likely as nonsmokers to have a lifetime history of major depression (Breslau et al. 1993; Quattrocki et al. 2000; Grant et al. 2004). Temporally, the occurrence of MDD predicts heightened risk of starting to smoke, and starting to smoke predicts increased risk of developing MDD (Kendler et al. 1993; Wu and Anthony 1999). Among adult smokers, greater nicotine dependence is associated with increased risk of mental disorders, includ- ing depression (John et al. 2004). The nature of the mechanism(s) linking smoking and depression remains unclear. Smoking may cause neuro- adaptations that predispose to depression (Balfour and Ridley 2000; Duncan and Rees 2005). Alternatively, depression may prompt experimentation to find behaviors, like smoking, that relieve (self-medicate) negative moods (Glassman et al. 1990; Khantzian 1997; Murphy et al. 2003). Finally, conjoint vulnerabilities to nicotine depen- dence and to depression may heighten an individual’ s sensitivity to mood-enhancing effects of nicotine. Stated differently, vulnerability to depression may moderate nico- tine’ s effect on mood. Psychopharmacology (2008) 196:461–471 DOI 10.1007/s00213-007-0977-7 B. Spring Hines Hospital, VA Medical Center, Hines, IL, USA B. Spring (*) : B. Appelhans : A. Maloney : J. Vaughn Northwestern University, 680 N. Lakeshore Drive, Suite 1220 Chicago, IL 60611, USA e-mail: [email protected] B. Spring : J. W. Cook : A. Maloney : M. Richmond : J. Vanderveen : D. Hedeker University of Illinois, Chicago, IL, USA
-
Upload
northwestern -
Category
Documents
-
view
1 -
download
0
Transcript of Nicotine effects on affective response in depression-prone smokers

ORIGINAL INVESTIGATION
Nicotine effects on affective responsein depression-prone smokers
Bonnie Spring & Jessica Werth Cook &
Bradley Appelhans & Anne Maloney & Malia Richmond &
Jocelyn Vaughn & Joseph Vanderveen & Donald Hedeker
Received: 7 June 2007 /Accepted: 3 October 2007 / Published online: 25 October 2007# Springer-Verlag 2007
AbstractRationale Comorbidity between cigarette smoking anddepression is thought to arise because depression-pronesmokers self-administer nicotine to improve mood. Yet littleevidence supports this view, and nicotine’s effect on positiveaffect deficiency in depression remains largely unstudied.Objectives We hypothesized that (1) nicotine would dispelnegative affect and enhance positive affect and (2) effectswould be stronger for smokers vulnerable to depression,particularly during a depressed state.Materials and methods Regular smokers (N=165) wererecruited from the community: 63 with no history of majordepressive disorder (MDD), 61 with recurrent past but nocurrent MDD, and 41 with both current and past MDD.During four sessions, participants smoked either a nicoti-nized (NIC+) or denicotinized (NIC−) cigarette doubleblind after experiencing a negative mood induction or whileundergoing a positive mood induction. Positive andnegative affects were measured at baseline and at two timepoints after smoking.Results Previously depressed smokers showed a heightenedpositive mood response to positive mood induction when
smoking a nicotinized cigarette. Nicotine also increased thedegree to which positive mood induction dispelled negativemood in depression-vulnerable smokers. Finally, nicotineworsened the negative affect response to negative moodinduction for all groups.Conclusion Self-administering nicotine appears to improvedepression-prone smokers’ emotional response to a pleasantstimulus.
Keywords Nicotine . Depression . Tobacco smoking .
Affect . Tobacco use
Cigarette smoking is associated with both trait and stateaspects of vulnerability to major depressive disorder(MDD) (Breslau et al. 2004; Hitsman et al. 2003). Smokersare twice as likely as nonsmokers to have a lifetime historyof major depression (Breslau et al. 1993; Quattrocki et al.2000; Grant et al. 2004). Temporally, the occurrence ofMDD predicts heightened risk of starting to smoke, andstarting to smoke predicts increased risk of developingMDD (Kendler et al. 1993; Wu and Anthony 1999).Among adult smokers, greater nicotine dependence isassociated with increased risk of mental disorders, includ-ing depression (John et al. 2004).
The nature of the mechanism(s) linking smoking anddepression remains unclear. Smoking may cause neuro-adaptations that predispose to depression (Balfour andRidley 2000; Duncan and Rees 2005). Alternatively,depression may prompt experimentation to find behaviors,like smoking, that relieve (self-medicate) negative moods(Glassman et al. 1990; Khantzian 1997; Murphy et al.2003). Finally, conjoint vulnerabilities to nicotine depen-dence and to depression may heighten an individual’ssensitivity to mood-enhancing effects of nicotine. Stateddifferently, vulnerability to depression may moderate nico-tine’s effect on mood.
Psychopharmacology (2008) 196:461–471DOI 10.1007/s00213-007-0977-7
B. SpringHines Hospital, VA Medical Center,Hines, IL, USA
B. Spring (*) : B. Appelhans :A. Maloney : J. VaughnNorthwestern University,680 N. Lakeshore Drive,Suite 1220 Chicago, IL 60611, USAe-mail: [email protected]
B. Spring : J. W. Cook :A. Maloney :M. Richmond :J. Vanderveen :D. HedekerUniversity of Illinois,Chicago, IL, USA

Hypotheses for the present study derived from thevulnerability model (Zubin and Spring 1977; Spring andZubin 1978), widely applied in psychopathology research(Hankin and Abela 2005; Glantz and Pickens (1992). Themodel predicts increasing expression of a behavioralphenotype as the combined loading of trait and statevulnerability increase from no diathesis, through thepresence of the diathesis, through the combined presenceof the diathesis, and the current psychopathologic state. Inthis study, a depressive diathesis was inferred from arecurrent history of episodes of major depressive disorder.Depressive state was evidenced by a current majordepressive episode. We predicted increasing expression ofthe behavioral phenotype (derivation of affective benefitfrom nicotine) as smokers manifested increasing depressivevulnerability as follows: never depressed; recurrentlypreviously but not currently depressed; both recurrentlypreviously and currently depressed.
Negative mood has been the focus of most research ondepression-prone smokers. Positive mood has not generallybeen examined, even though low positive affect appears to bemore selectively associated with depression (Clark andWatson 1991; Coyne et al. 1994). The paucity of researchon positive mood deficiency among depression-pronesmokers may reflect a view that high negative affect equatesto low positive affect. There is evidence, however, thatpositive and negative affect convey nonredundant informa-tion generally (Clark and Watson 1988) and among smokersspecifically (Werth Cook et al. 2004a, b). In this study, weexamined the premise that depression-prone smokers derivedisproportionate desirable effects on both positive andnegative mood from self-administering nicotine.
Evidence is mixed regarding whether nicotine has moodregulating effects in the non-nicotine deprived state. Re-exposing deprived smokers to nicotine has been shown toreduce negative affect (Gentry et al. 2000; Masson andGilbert 1999; Parrott and Garnham 1998) and increasepositive affect (Pomerleau and Pomerleau 1992; Perkinset al. 2006). However, such effects may be attributed toreversal of nicotine withdrawal symptoms. Some studies ofnon-deprived smokers show nicotine to reduce negativemood (Cutler and Barrios 1988; Warburton and Mancuso1998; Perkins et al. 1992; Gilbert et al. 1989). Othersstudies, however, show no nicotine effect on dysphoria(Conklin and Perkins 2005; Herbert et al. 2001; Hutchisonet al. 2000). Nicotine effects on positive mood have alsobeen observed inconsistently. Among non-deprived smok-ers, nicotine administration stimulated a mild increment inpleasurable emotions in two studies (Malpass and Higgs2007; Warburton and Mancuso 1998), but lacked impact onpositive mood in another (Parrott and Garnham 1998).
Discrepant prior findings regarding nicotine’s effects onmood likely reflect both individual differences in nicotine
responsivity (Lerman et al. 2006) and variability in theexperimental protocol used to assess affective change. AsPerkins (1995) noted, nicotine’s behavioral effects exhibitbaseline dependency: the magnitude of nicotine’s effectdepends upon the mood state that immediately precedessmoking. Baseline mood state is, in turn, influenced by theexperimental design. If baseline mood is uncontrolled,variation in daily life circumstances before testing introdu-ces affective variability that impedes the ability to detect aclear signal from nicotine. Not surprisingly, then, nicotinehas shown strongest ability to dispel negative affect whenadministered during or after experimentally induced dys-phoric mood (Lane et al. 1995; Levin et al. 1991; Perkins etal. 1992). Nicotine’s impact on experimentally inducedpositive affect has not, to our knowledge, previously beenexamined. Thus, the current research design used astandardized but personally salient experimental induction(happy or sad music plus autobiographical memories) toregulate baseline affective state.
In sum, the present study examined nicotine’s effects onexperimentally induced positive and negative affect, andtested whether those effects are moderated by depressivevulnerability. We hypothesized that (1) nicotine woulddispel experimentally induced negative affect and enhanceinduced positive affect and (2) effects would be stronger forsmokers vulnerable to depression, particularly if they werecurrently in a depressive episode.
Materials and method
Overview
The research design compared affective responses tosmoking a nicotinized vs a de-nicotinized cigarette in threegroups of smokers of increasing depressive vulnerability asfollows: never depressed; previously but not currentlydepressed; previously and currently depressed. We pre-dicted that nicotine would engender increasing affectivebenefit (both enhancing positive mood and dispellingnegative mood) as depressive vulnerability increased.Nicotine effects were examined in two affective contextsin which a depression-prone smoker might use nicotine toself-regulate mood. A positive mood induction protocolmodeled nicotine self-administration to try to get into apositive mood. A negative mood induction protocolmodeled nicotine self-administration to try to dispel anegative mood. The time line of events for the positive andnegative mood induction protocols are shown in Figs. 1 and2, respectively. The two protocols were analyzed asseparate substudies because they involved slightly differenttimelines. To minimize expectational effects, though, weadministered the four protocol conditions (positive induc-
462 Psychopharmacology (2008) 196:461–471

tion, nicotinized [NIC+]; positive induction de-nicotinized[NIC−]; negative induction NIC+; negative induction NIC−)in completely random order. Thus, the design for both thepositive and the negative mood induction substudies was amixed model with one between subjects factor (group) andtwo repeated measures factors (nicotine and time). Depen-dent variables were positive mood and negative mood.
Participants
Smokers were recruited from the community via flyers andlistserv announcements seeking individuals between ages18–65 who smoked at least 15 cigarettes per day for the past1 year. Eligibility criteria excluded candidates based on:current use of nicotine replacement, medically unstablecondition, difficulty reading the mood questionnaire, non-responsivity to negative mood induction, and Axis I disorderother than nicotine dependence or major depressive disorder.To reduce the influence of hormonal fluctuation on affectiveresponses, menopausal, peri-menopausal, and pregnantwomen were also excluded, as were those taking contra-ceptives that fully suppress menstruation.
Eligible smokers (n=165) were categorized as meetingDSM-IV criteria for either no history of major depressivedisorder (MDD) (n=63: 32 women), recurrent past but no
current MDD (n=61: 34 women), or both current and pastMDD (n=41: 25 women). Three participants (all currentlydepressed) were taking antidepressant medications.
Procedure
Screening sessions Interested study candidates werescreened by telephone. Those meeting initial entry criteriaattended in-person screening during which their eligibilitywas assessed further. Depression status was appraised by theStructured Clinical Interview for DSM-IV, non-patient ver-sion (SCID-NP) (Spitzer et al. 1992). Smoking status wasverified by an ecolyzer carbon monoxide (CO) value of ≥8parts per million (ppm). Questionnaires were administered toassess mood, positive and negative memories, nicotinedependence, and smoking history. To evaluate responsive-ness to negative mood induction, participants self-rated theirmood using the Profile of Mood States (POMS) (McNair etal. 1971), underwent a 10-min negative mood induction, andthen re-completed the POMS. To be eligible, participantsneeded to respond with ≥4 point increase on POMSDysphoria and no increase on POMS Vigor.
Event Cumulative Timeline
Smoke own cigarette
Rest
-17 min
Baseline mood
assessment
0 min 10
Negative mood induction
Smoke study cigarette
Post-induction mood
assessment 1
Rest
Post-induction mood
assessment 2
10 min
23 min
30 min
40 min
60 min
Fig. 2 Negative mood induction protocol timeline
Event Cumulative Timeline
Smoke own cigarette
Rest
-17 min
Baseline mood
assessment
0 min
Positive mood Induction
while smoking study
cigarette
10 min
Post-induction mood
assessment 1
Rest
Post-induction mood
assessment 2
17 min
27 min
37 min
Fig. 1 Positive mood induction protocol timeline
Psychopharmacology (2008) 196:461–471 463

Laboratory sessions The two positive mood inductionsessions and two negative mood induction sessions wereadministered randomly in counterbalanced order at least24 h apart. Participants were tested individually. Femalesubjects were tested between days 7 and 21 of their men-strual cycle to minimize influences of hormonal fluctuationon affective responses. To reduce the impact of diurnalvariation, all sessions were scheduled between 11 A.M. and6:00 P.M. Each session lasted approximately 2 h. To reducepossible effects of caffeine and nicotine withdrawal,participants were encouraged to drink their usual amountof caffeinated beverage and smoke their usual amountbefore each session.
CO was measured at the outset of each experimentalsession to confirm an ecolyzer value of at least 8 ppm.Those with CO less than 8 ppm upon arrival wererescheduled. Participants then smoked one of their owncigarettes to standardize nicotine exposure and minimizepossible nicotine withdrawal effects during testing. Nextthey completed a baseline mood questionnaire beforeundergoing positive or negative mood induction.
Positive mood induction After reporting baseline mood,participants sat quietly for 7 min, while smoking theprovided nicotinized or denicotinized cigarette (cf.,Fig. 1). During the same interval they listened to audio-taped “happy” music and imagined a positive autobio-graphical memory that the experimenter suggested fromthose gathered during screening. The audiotaped excerptsfrom Pachelbel’s Canon in D and Spring, Summer, and Fallof Vivaldi’s Four Seasons have been shown to inducepositive mood (McCabe et al. 2000; Roisman et al. 2006).After mood induction and smoking, participants re-ratedtheir mood at two additional time points.
Negative mood induction The negative mood inductionprotocol has been demonstrated to have good reliabilityover repeated administrations (Hernandez et al. 2003).After reporting baseline mood, participants sat quietly for10 min while listening to an audiotape of “sad” music andimagining the negative autobiographical memory suggestedby the experimenter (cf., Fig. 2). The sad musicalcompilation included excerpts from Prokofiev’s RussiaUnder the Mongolian Yoke and Barber’s Adagio PourCordes. Both have been shown to induce dysphoric moods(Clark and Teasdale 1982; Gerrards-Hesse et al. 1994;Martin 1990). Three minutes post-induction, participantssmoked a nicotinized or a denicotinized cigarette. Thenthey re-rated their mood at two more time points. Forsafety, a positive mood induction was performed at the endof each negative mood induction session. Participants werenot sent home unless their PANAS negative affect scorehad returned to baseline.
Nicotinized/denicotinized cigarettes The research designvaried the nicotine content of cigarettes while holdingconstant the sensory effects of smoking. Nicotinizedcigarettes had an FTC-method estimated nicotine deliveryof 1.0-mg nicotine. Denicotinized cigarettes had an esti-mated nicotine delivery of 0.1-mg nicotine. Both were bothproduced by Lifetech and were matched for tar and carbonmonoxide content. Nicotinized and denicotinized cigaretteswere presented in counterbalanced order.
Assessments—screening session
Negative memory questionnaires To obtain autobiographi-cal memories for the mood inductions, a negative memoryquestionnaire and a positive memory questionnaire wereadministered during screening. Four negative and fourpositive memories were collected. Participants rated eachnegative memory on a scale of 1 to 10 to indicate how sador upset the memory made them feel. They rated eachpositive memory from 1 to 10 to indicate how happy orcheerful the memory made them feel. They also rated allmemories from 1 to 10 on a scale of vividness. Thenegative memories chosen were rated 7 or above on upsetand were the two most similar with respect to theirnegativity and vividness ratings. Likewise, the chosenpositive memories were rated 7 or above on cheerfulnessand were the two rated most similar on pleasantness andvividness.
Axis I disorders The Structured Clinical Interview forDSM-IV, non-patient version (SCID-NP; Spitzer et al.1992) was administered to determine whether participantsmet criteria for current and past axis I disorders. The SCID(Spitzer et al. 1992) has moderate construct validity, asshown by its favorable comparison with other diagnosticassessment methods (Williams et al. 1992). Traineddiagnosticians, supervised by clinical psychologists, gavethe interview.
Current depressive symptoms The Hamilton DepressionRating Scale (HDRS) (Hamilton 1960, 1967) was givento assess the severity of current depressive symptoms. The21-item HDRS is a semi-structured clinician-administeredinterview that has been shown to have acceptable inter-raterreliability (Bech et al. 1975).
The conjoint findings of the HDRS and the SCID-NPdetermined participants’ group designation. Never de-pressed smokers failed to meet DSM-IV criteria for currentor past MDD and received a HDRS score of 0 or 1.Previously depressed smokers met criteria for at least twoprior MDD episodes, but did not meet MDD criteria in thepast 6 months, and had a HDRS score ≤10. Currently
464 Psychopharmacology (2008) 196:461–471
depressed smokers had at least one prior MDD episode,currently met MDD criteria and had a HDRS score ≥13.
Nicotine dependence Level of nicotine dependence wasmeasured by the Fagerström Test for Nicotine Dependence(FTND; Heatherton et al. 1991). The FTND has demon-strated adequate internal consistency and strong test-retestreliability (Pomerleau et al. 1994).
Assessments—screening and experimental sessions
Smoking status During screening, participants reportedtheir average daily amount smoked. Smoking status wasalso assessed via ecolyzer (EC-50, Vitalograph) measure-ment of expired CO. Candidates with CO less than 8 ppmat screening were excluded. To minimize withdrawaleffects, participants were reminded to smoke their usualamount before each experimental session. They were askedto report on their smoking that day and assessed for CO atthe beginning of each experimental session.
Cigarette characteristic rating scale A rating scale mea-suring cigarette likeability (Pickworth et al. 1999) was usedto assess the nicotinized and denicotinized cigarettes.Participants rated the harshness and taste of experimentalcigarettes smoked during each session on a scale from 1(“not at all”/“bad”) to 10 (“a lot”/“great”).
Assessments—outcome
Negative and positive affect The Positive Affect andNegative Affect Schedule (PANAS; Watson et al. 1988)was given to assess self-reported mood. The PANAS shows
good internal consistency, test–retest reliability, and validityevidence (Watson et al. 1988). The 10 negative and 10positive PANAS mood terms are rated on five-point Likert-type response scales from 1, very slightly or not at all, to 5,extremely. PANAS positive and negative scale scores eachrange between 10 and 50 (Watson et al. 1988).
Data analysis
Chi-square analyses for categorical variables and ANOVAsfor continuous variables were performed to compare thegroups on demographic characteristics, depressive symp-toms, cigarettes smoked, and nicotine dependence. Differ-ences were found for age, depressive symptoms, andnicotine dependence, as shown in Table 1.
We hypothesized that, relative to placebo, nicotinewould enhance experimentally induced positive mood anddispel experimentally induced negative mood, particularlyin smokers with recurrent prior depression, and especially ifthey were in a MDD episode. Four repeated measuresANOVAs, with Huynh-Feldt corrections for sphericityviolations, modeled the effect of nicotine and depressivevulnerability on change in PANAS positive and negativeaffect ratings in response to induced positive and negativemood. Because we were interested in comparisons betweenspecific depression groups, we followed the recommenda-tion of Rosenthal et al. (2000) for “focused” analyses.Accordingly, we tested our hypotheses through orthogonala priori contrasts capturing hypothesized differences be-tween prespecified groups.
For the between-subjects depression group factor, twoHelmert contrasts were tested in each analysis: (a) a“depression history” contrast comparing never depressedsmokers with ones whose history of recurrent episodes
Table 1 Participant demographic characteristics (N=165)
Never (n=63) History (n=61) Current (n=41)
Age (M, SD) 27.1 (10.7)a 31.5 (10.6)b 27.3 (11.2)Gender (% female) 50.8 55.7 61.0Education(% with ≥ some college) 87.3 78.7 82.9Ethnicity (%)African-American 17.5 27.9 12.2Asian/Pacific Islander 6.3 6.6 22.0Caucasian 71.4 57.4 61.0Hispanic 3.2 3.3 4.9Multiethnic 1.6 3.3 0Native American 0 1.6 0Hamilton (M, SD) 0.2 (0.4)a 2.6 (2.4)b 16.5 (2.9)c
Fagerstrom (M, SD) 4.2 (2.0)a 5.2 (2.0)b 5.0 (1.9)Number of cigarettes smoked per day (M, SD) 19.1 (5.5) 18.4 (4.6) 18.6 (5.1)
Values labeled with different superscripts differ significantly from each other at p<0.05.
Psychopharmacology (2008) 196:461–471 465

indicated that they were depression-prone (i.e., combiningpreviously and currently depressed participants), and (b) a“depression state” contrast comparing previously depressedsmokers with currently depressed ones. For the within-subjects condition factor, a simple contrast between NIC+vs NIC− was used. Finally, for the time factor, orthogonalpolynomial contrasts were tested to characterize thetemporal pattern of mood responses in terms of their linearand quadratic trend components. Three-way interactionswere predicted between the depression group contrasts(depression vulnerability and depression state) and thewithin-subjects factors of condition (NIC+ vs NIC−) andtime (one premood induction assessment and two post-mood induction assessments). Together, these contrastsallowed for planned comparisons of the depression groups’temporal pattern of affective responses to nicotine undereach affective induction.
Our analyses were aimed at detecting differences in thewithin-subjects pattern of mood responses to a moodinduction due to smoking a NIC+ vs a NIC− cigarette. Inother words, we sought to compare the impact of smokingthese two types of cigarettes on an individual’s pattern ofmood changes. Thus, analyzing data from several partic-ipants who did not smoke both a NIC+ and NIC− cigaretteafter either mood induction would not contribute subject-specific information relevant to the difference between NIC+vs NIC− cigarettes on mood responses. Therefore, weexcluded from analyses data from three never depressedparticipants, three previously depressed participants, and onecurrently depressed participant who did not smoke bothtypes of cigarettes during the negative mood induction. Wealso excluded data from one never depressed participant whodid not smoke both types of cigarettes during the positivemood induction.
Results
Preliminary analyses
Comparability of placebo and active cigarettes Separateone-way ANOVAs tested whether the NIC+ vs NIC−cigarettes differed in perceived harshness or taste in thepositive and negative mood inductions. NIC+ cigaretteswere rated as having slightly better taste than NIC−cigarettes in both the positive (means: 3.6 vs 2.6, F(1,329)=18.95, p<0.001) and negative (means: 3.4 vs 2.3, F(1,325)=24.99, p<0.001) mood inductions. The two kinds ofcigarettes did not differ in perceived harshness for eitherinduction.
Correlations between positive and negative affect Pearsoncorrelations demonstrated that positive and negative affect
ratings were consistently moderately inversely relatedacross condition (Table 2).
Covariates Given the presence of group differences in ageand nicotine dependence, and the differences in taste ratingsbetween the NIC+ and NIC− cigarettes, we performed ourprimary analyses with and without these variables includedas covariates. Inclusion of the covariates did not alter thestatistical significance of results. For simplicity, we reportthe final models without covariates.
Primary analyses
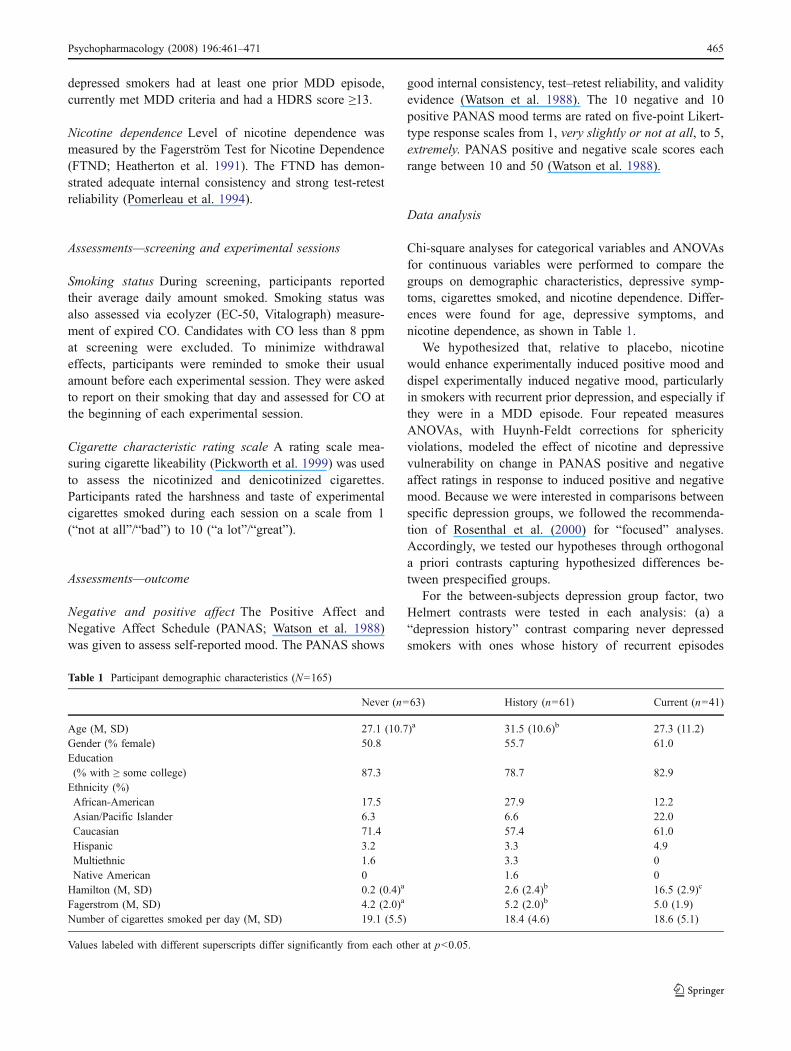
Responses to positive mood induction Positive affectiveresponses to positive mood induction showed a significantthree-way interaction of depression state by condition bytime (F(2,323)=3.54, p=0.03). Both the linear and quadratictrends for this effect approached significance (linear:F(1,161)=3.70, p=0.06; quadratic: F(1,161)=3.37, p=0.07).As shown in Fig. 3, previously depressed smokers showeda heightened positive affective response to positive moodinduction when smoking a NIC+ compared to a NIC−cigarette. This difference across time was not solely linear(e.g., the NIC+ to NIC− difference did not continue to growover time), nor solely quadratic (the NIC+ to NIC−difference did not start at a baseline level, enlarge, andthen return to its baseline level). Rather, it was thecombined pattern of linear and quadratic changes over time
Table 2 Zero-order Pearson correlations between PANAS positiveand negative affect ratings at each assessment (N=165)
Induction Values
Positive inductionNicotinizedBaseline −0.21**Post 1 −0.20*Post 2 −0.18*
De-nicotinizedBaseline −0.28***Post 1 −0.26**Post 2 −0.25**
Negative inductionNicotinizedBaseline −0.21**Post 1 −0.19*Post 2 −0.28***
De-nicotinizedBaseline −0.24**Post 1 −0.28***Post 2 −0.26**
*p<0.05**p<0.01***p<0.001.
466 Psychopharmacology (2008) 196:461–471
that significantly differentiated the groups’ response to theNIC+ vs NIC− cigarettes. Negative affective responsesto the positive mood induction showed a significantinteraction of depression vulnerability by condition by time(F(2,322)=3.91, p=0.02). Never depressed smokers differedfrom depression-prone smokers in nicotine’s effect on thelinear (F(1,161)=4.40, p=0.04) trend in their affectiveresponses. The effect for the quadratic trend alsoapproached significance (F(1,161)=3.24, p=0.07). As shownin Fig. 4, the positive mood induction’s propensity to dispelnegative mood was heightened when depression vulnerablesmokers smoked a nicotinized cigarette.
Responses to negative mood induction Affective responsesto the negative mood induction showed no significant three-way interactions of group by condition by time. No
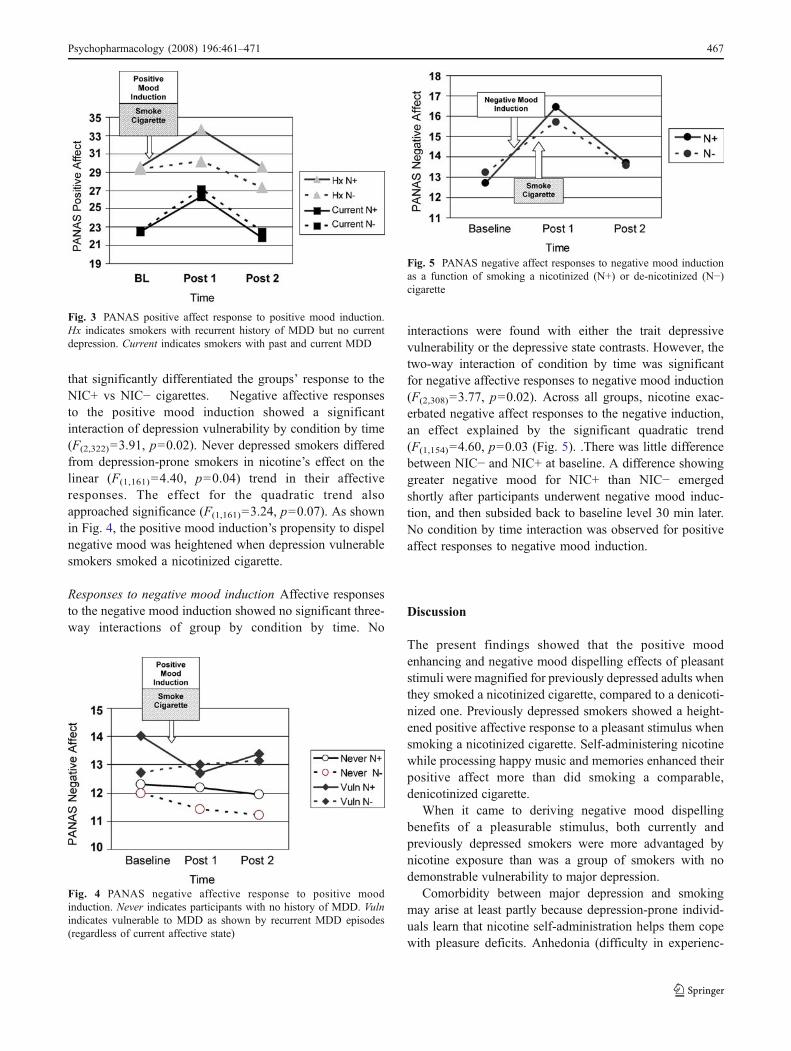
interactions were found with either the trait depressivevulnerability or the depressive state contrasts. However, thetwo-way interaction of condition by time was significantfor negative affective responses to negative mood induction(F(2,308)=3.77, p=0.02). Across all groups, nicotine exac-erbated negative affect responses to the negative induction,an effect explained by the significant quadratic trend(F(1,154)=4.60, p=0.03 (Fig. 5). .There was little differencebetween NIC− and NIC+ at baseline. A difference showinggreater negative mood for NIC+ than NIC− emergedshortly after participants underwent negative mood induc-tion, and then subsided back to baseline level 30 min later.No condition by time interaction was observed for positiveaffect responses to negative mood induction.
Discussion
The present findings showed that the positive moodenhancing and negative mood dispelling effects of pleasantstimuli were magnified for previously depressed adults whenthey smoked a nicotinized cigarette, compared to a denicoti-nized one. Previously depressed smokers showed a height-ened positive affective response to a pleasant stimulus whensmoking a nicotinized cigarette. Self-administering nicotinewhile processing happy music and memories enhanced theirpositive affect more than did smoking a comparable,denicotinized cigarette.
When it came to deriving negative mood dispellingbenefits of a pleasurable stimulus, both currently andpreviously depressed smokers were more advantaged bynicotine exposure than was a group of smokers with nodemonstrable vulnerability to major depression.
Comorbidity between major depression and smokingmay arise at least partly because depression-prone individ-uals learn that nicotine self-administration helps them copewith pleasure deficits. Anhedonia (difficulty in experienc-
Fig. 3 PANAS positive affect response to positive mood induction.Hx indicates smokers with recurrent history of MDD but no currentdepression. Current indicates smokers with past and current MDD
Fig. 4 PANAS negative affective response to positive moodinduction. Never indicates participants with no history of MDD. Vulnindicates vulnerable to MDD as shown by recurrent MDD episodes(regardless of current affective state)
Fig. 5 PANAS negative affect responses to negative mood inductionas a function of smoking a nicotinized (N+) or de-nicotinized (N−)cigarette
Psychopharmacology (2008) 196:461–471 467

ing positive affect or pleasure) has long been considered acore symptom of major depression and a vulnerabilityfactor for the disorder (Fawcett et al. 1983; Loas 1996;Meehl 1987). Anhedonia can be measured reliably andeven objectively (Leventhal et al. 2006; Pizzagalli et al.2005). Moreover, fMRI findings have shown anhedonia tobe associated with dysfunction in brain neural systemsunderlying responsivity to emotional stimuli (Keedwellet al. 2005). Yet, the focus of research on comorbid sub-stance use and depression has continued to be on how welldrugs dispel negative mood. Largely neglected has been thequestion of whether drug self-administration can helpovercome pleasure deficits and instantiate positive emo-tions. In prior work (Werth Cook et al. 2004b), we found thatanhedonic smokers in early nicotine withdrawal were proneto cigarette cravings that were mediated by decreasedpositive mood, rather than by increased negative mood.Likewise, the current findings suggest that self-administeringnicotine to enhance pleasure is at least as important an aspectof the depression-prone smoker’s attachment to cigarettes asis the use of cigarettes to dispel negative mood.
Preclinical data are consistent with our finding thatnicotine enhanced depression-prone smokers’ response to apleasurable stimulus. In particular, our results are compat-ible with animal research showing that reward threshold,measured by the amount of current rats self-administer tobrain reward centers (Kornetsky and Bain 1990), is lowered(i.e., made more rewarding) during nicotine administration(Huston-Lyons and Kornetsky 1992). In other words, non-drug stimuli became more rewarding when nicotine wassimultaneously administered. Conversely, intracranial self-stimulation requires more intense current during nicotinedeprivation (Epping-Jordan et al. 1988), signifying thatnon-drug stimuli become less rewarding in the absence ofnicotine. It has been suggested that nicotine’s ability tobolster responding to rewarding non-nicotine stimuli maybe an important component in maintaining smokingbehavior (Chaudhri et al. 2006). As such, nicotine mayenhance depression-prone smokers’ response to typicallyrewarding events, further entrenching smoking behavioramong this recalcitrant group of tobacco users.
It is difficult to explain why currently depressed smokersresembled previously depressed ones in deriving height-ened negative mood dispelling but not positive moodenhancing effects from pairing nicotine with a pleasurableemotional stimulus. For previously depressed smokers, thebenefit derived from self-administration nicotine during apositive experience was consistent across affective spheres.In other words, nicotine made the previously depressedsmoker feel both less bad (decreased negative affect) andmore good (increased positive affect). It was as thoughpairing nicotine with a pleasant event unlocked the “sweetspot” for depression-prone smokers, enabling them to feel
less displeasure and more pleasure. For currently depressedsmokers, in contrast, the benefit of pairing nicotine with apleasant stimulus was confined to helping the smoker feelless bad (less dysphoric). But that restriction was notbecause nicotine failed to unleash the depressed smoker’spleasure about a positive stimulus. Rather, it was becausesmoking a denicotinized cigarette while thinking about apositive stimulus also increased positive mood.
We considered three explanations for why smokingeither a nicotinized or a denicotinized cigarette improvedcurrently depressed smokers’ positive affect to a pleasantstimulus, whereas their currently euthymic depression-prone peers required nicotine to get an increment inpleasure. First, we wondered whether antidepressant usageby the currently depressed smokers might have normalizedthe group’s ability to respond positively to a pleasantstimulus, even without pairing it with nicotine. However,because only 3 of 41 currently depressed patients weretaking antidepressants and because there was no markeddeviation between their response pattern and that of theirunmedicated counterparts, we considered that explanationunlikely. Second, we considered whether previously de-pressed smokers in this study might have a strongerdepressive diathesis than currently depressed smokers,manifested by being able to decrease displeasure but notquite increase pleasure by pairing nicotine with positivestimuli. However, the lack of difference (t(96)=0.49, p=0.63) in the number of prior MDD episodes between ourcurrently [(mean=2.76; SD=1.94) and previously (mean=2.59; SD=1.42), depressed groups casts doubt upon thatexplanation. Finally, we considered whether being in adepressed state might heighten sensitivity to the smallamount of nicotine present in the denicotinized cigarette.Hypersensitivity to the rewarding subjective effects of adopamine (amphetamine) probe has previously beenreported in depressed adults, and is accompanied by alteredactivation in neuroanatomic reward substrates (Tremblayet al. 2002, 2005). Hence, we considered that theobservation warrants replication and that the hypersensitiv-ity explanation warrants exploration.
We expected that smoking a nicotinized cigarette woulddispel negative mood invoked by an upsetting memory andsad music, with such an effect heightened among depres-sion-prone smokers. In fact, we found the opposite: self-administering nicotine modestly but significantly worsenedmood among smokers who had just been exposed to anegative emotional stimulus. That effect occurred regard-less of depressive vulnerability. Nicotine may have causedmood deterioration by helping smokers ruminate on thenegative imaginal content to which they had been exposed.On the basis of correlational observations (Richmond et al.2001), we previously hypothesized such an effect amonghighly ruminative individuals. The present experimental
468 Psychopharmacology (2008) 196:461–471

findings suggest that, in at least some contexts, nicotinetransiently worsens negative emotional reactions among theaverage smoker—not just among high ruminators.
It can be noted that the failure of nicotine to reducenegative affect in the negative affect-induction procedure isconsistent with models that posit an effect of nicotine onattentional allocation (Gilbert 1995; Kassel and Unrod2000). Findings supporting these attentional models suggestthat nicotine does not reduce negative affect when stressorsare proximal and strong, as our personally salient memoryand musical mood induction appeared to be. That researchsuggests that nicotine may reduce negative affect primarilywhen it can bias attentional and associative processes awayfrom negative and towards positive or benign stimuli. Suchattentional biasing appears unable to override the kind ofsalient, proximal negative stimuli used in the presentnegative affect-induction procedure.
Our study had several limitations. First, the sample wasrelatively young (late 20s, early 30s). Thus, some controlgroup members might also be vulnerable to depression butnot yet passed through the full risk period for diathesis tobe expressed. Although possible and a pitfall that couldundermine internal validity, it should be noted thatinclusion of depression-prone smokers in the control groupwould bias the study conservatively against our hypotheses.Second although the effects we observed were statisticallysignificant, they were small in magnitude (Cohen 1992).Thus, their clinical significance, especially as applied to anindividual patient, cannot be assumed.
Another limitation is that we were not successful atequating the nicotinized and denicotinized cigarettes ontaste. The nicotinized cigarette tasted better than thedenicotinized one, although the two were similar onharshness. Even though we covaried out effects of cigarettetaste, there remains the possibility that effects ascribed tonicotine might be attributable instead to the nicotinizedcigarette’s better taste. That possibility of bias would beparticularly worrisome if the nicotinized cigarette hadproduced consistently advantageous effects. It did not,however. Although responses to nicotine in the positivemood induction condition were advantageous (increasedpleasure, decreased displeasure), they were disadvantageousin the negative mood induction condition (increased displea-sure). Thus, variation in the sensory characteristics of thestudy cigarettes, as distinct from pharmacological effects ofnicotine, is unlikely to explain the study outcomes.
Some would consider it a limitation that our positive andnegative mood induction protocol timelines differed slight-ly. Importantly, the temporal difference did not mar theinternal validity of the research design, which analyzedpositive affect induction and negative affect induction asseparate substudies. We designed the affect inductionprotocols thusly to give them ecological validity. We aimed
to model the two main emotional contexts in whichdepression-prone smokers have been thought to self-administer nicotine to induce pleasure, on the one hand,and dispel displeasure, on the other hand. Because chronicor recurrent negative emotionality characterizes individualsvulnerable to depression (Clark et al. 2003), we modelednicotine self-administration in an effort to dispel recurrentnegative mood. (That we learned that nicotine self-administration actually transiently worsens mood in thiscontext was clinically informative, but unknown to us whenwe designed the protocol). In contrast, because anhedonia isthought to be a feature of depressive vulnerability (Loas1996), positive affect may be habitually low or absent.Because it seemed unlikely that a depression-prone smokerwould expect nicotine self-administration alone to engenderpositive mood, we modeled the context in which such asmoker self-administers nicotine in tandem with a positivestimulus to “prime the pump” and activate a feeling ofpleasure.
The findings have potential implications for smokingcessation. Elevated negative mood after quitting smokinghas been a hypothesized pathway through which depres-sion-prone smokers relapse to smoking (Spring et al. 2003,2007a, b; Hall et al. 1996). Our results suggest analternative pathway: that depression-prone smokers mayrelapse because they experience a loss in pleasure that waspreviously buttressed by nicotine. A decline in positiveaffect after quitting smoking has been observed in non-psychiatric populations (Werth Cook et al. 2004a, b), andlinked with relapse to smoking (al’Absi et al. 2004). Ifdepression-prone smokers rely on nicotine for pleasureenhancement, they may have a particularly difficult timemaintaining abstinence. Research is needed to examinewhether positive mood management interventions improvequit rates among smokers vulnerable to depression.
Acknowledgements Supported by a VA Medical Research MeritReview grant to Dr. Spring and by NIH grants P30 CA060553 andR25 CA100600. Portions of this paper were presented at the AnnualMeeting of the Society for Research in Nicotine and Tobacco, Austin,Texas, February, 2007. We express appreciation to Dennis McChargueand Neal Doran for discussions during the conduct of the research andan anonymous reviewer for noting the relevance of attentionalallocation models to our findings.
References
al’ Absi M, Hatsukami D, Davis GL, Wittmers LE (2004) Prospectiveexamination of effects of smoking abstinence on cortisol andwithdrawal symptoms as predictors of early smoking relapse.Drug Alcohol Depend 73:267–278
Balfour DJ, Ridley DL (2000) The effects of nicotine on neuralpathways implicated in depression: a factor in nicotine addiction?Pharmacol Biochem Behav 66:79–85
Psychopharmacology (2008) 196:461–471 469
Bech P, Gram L, Dein F, Jacobsen O, Vitger J, Bolwig T (1975)Quantitative rating of depressive states. Acta Psychiatr Scand51:161–170
Breslau N, Kilbey MM, Andreski P (1993) Nicotine dependence andmajor depression: new evidence from a prospective investigation.Arch Gen Psychiatry 50:31–35
Breslau N, Novak SP, Kessler RC (2004) Daily smoking and thesubsequent onset of psychiatric disorders. Psychol Med 34:323–333
Chaudhri N, Caggiula AR, Donny EC, Palmatier MI, Liu X, Sved A(2006) Complex interactions between nicotine and nonpharma-cological stimuli reveal multiple roles for nicotine in reinforce-ment. Psychopharmacology 184:353–366
Clark DM, Teasdale JD (1982) Diurnal variation in clinical depressionand accessibility of memories of positive and negative experi-ences. J Abnorm Psychol 91:87–95
Clark LA, Watson D (1988) Mood and the mundane: relationsbetween daily life events and self-reported mood. J Pers SocPsychol 54:296–308
Clark LA, Watson D (1991) Tripartite model of anxiety anddepression: psychometric evidence and taxonomic implications.J Abnorm Psychol 100:316–336
Clark LA, Vittengl J, Kraft D, Jarrett RB (2003) Separate personalitytraits from states to predict depression. J Pers Disord 17:152–172
Cohen J (1992) A power primer. Psychol Bull 112:155–159Conklin CA, Perkins KA (2005) Subjective and reinforcing effects of
smoking during negative mood induction. J Abnorm Psychol114:153–164
Coyne JC, Fechner-Bates S, Schwenk TL (1994) Prevalence, nature,and comorbidity of depressive disorders in primary care. GenHosp Psych 16:267–276
Cutler GH, Barrios FX (1988) Effects of deprivation on smokers’mood during the operation of a complex computer simulation.Addict Behav 13:379–382
Duncan B, Rees DI (2005) Effect of smoking on depressivesymptomatology: a reexamination of data from the NationalLongitudinal Study of Adolescent Health. Am J Epidemiol162:461–470
Epping-Jordan MP, Watkins SS, Koob GF, Markou A (1988) Dramaticdecreases in brain reward function during nicotine withdrawal.Nature 393:76–79
Fawcett J, Clark DC, Scheftner WA, Gibbons RD (1983) Assessinganhedonia in psychiatric patients. Arch Gen Psychiatry 40:79–84
Gentry MV, Hammersley JJ, Hale CR, Nuwer PK, Meliska CJ (2000)Nicotine patches improve mood and response speed in a lexicaldecision task. Addict Behav 25:549–557
Gerrards-Hesse A, Spies K, Hesse FW (1994) Experimental induc-tions of emotional states and their effectiveness: a review. Br JPsychol 85:55–78
Gilbert DG (1995) Smoking: individual differences, psychopathology,and emotion. Taylor & Francis, Philadelphia, PA
Gilbert DG, Robinson JH, Chamberlin CL, Spielberger CD (1989)Effects of smoking/nicotine on anxiety, heart rate, and lateraliza-tion of EEG during a stressful movie. Psychophysiology 26:311–320
Glantz MD, Pickens RW (Eds) (1992) Vulnerability to drug abuse.American Psychological Association, Washington, DC
Glassman AH, Helzer JE, Covey LS, Cottler LB, Stetner F, Tipp JE,Johnson JE (1990) Smoking, smoking cessation, and majordepression. J Am Med Assoc 264:1546–1549
Grant BF, Hasin DS, Chou SP, Stinson FS, Dawson DA (2004)Nicotine dependence and psychiatric disorders in the UnitedStates: results from the national epidemiologic survey on alcoholand related conditions. Arch Gen Psychiatry 61:1107–1115
Hall SM, Muñoz RF, Reus VI, Sees K, Duncan C, Humfleet GL,Hartz DT (1996) Mood management and nicotine gum in
smoking treatment: a therapeutic contact and placebo-controlledstudy. J Consult Clin Psychol 64:1003–1009
Hamilton M (1960) A rating scale for depression. J Neurol NeurosurgPsychiatry 23:56–62
Hamilton M (1967) Development of a rating scale for primarydepressive illness. Br J Soc Clin Psychol 6:278–296
Hankin BL, Abela JRZ (Eds) (2005) Development of psychopathol-ogy: a vulnerability-stress perspective. Sage Publications, Thou-sand Oaks, CA
Heatherton TF, Kozlowski LT, Freckler RC, Fagerstrom K (1991) TheFagerstrom Test for Nicotine Dependence: a revision of theFagerstrom Tolerance Questionnaire. Addiction 86:1119–1127
Herbert M, Foulds J, Fife-Schaw C (2001) No effect of cigarettesmoking on attention or mood in non-deprived smokers.Addiction 96:1349–1356
Hernandez S, Vander Wal JS, Spring B (2003) A negative moodinduction procedure with efficacy across repeated administrationsin women. J Psychopathol Behav Assess 25:49–55
Hitsman B, Borrelli B, McChargue DE, Spring B, Niaura R (2003)History of depression and smoking cessation outcome: a meta-analysis. J Consult Clin Psychol 71:657–663
Huston-Lyons D, Kornetsky C (1992) Effects of nicotine on thethreshold for rewarding brain stimulation. Pharmacol BiochemBehav 41: 755–759
Hutchison KE, Niaura R, Swift R (2000) The effects of smoking highnicotine cigarettes on prepulse inhibition, startle latency, andsubjective responses. Psychopharmacology 150:244–252
John U, Meyer C, Rumpf HJ, Hapke U (2004) Smoking, nicotinedependence and psychiatric comorbidity: a population-basedstudy including smoking cessation after three years. DrugAlcohol Depend 76:287–295
Kassel JD, Unrod M (2000) Smoking, anxiety, and attention: Supportfor the role of nicotine in attentionally mediated anxiolysis. JAbnorm Psychol 109:161–166
Keedwell PA, Andrew C, Williams SCR, Brammer MJ, Phillips ML(2005) The neural correlates of anhedonia in major depressivedisorder. Biol Psychiatry 58:843–853
Kendler KS, Neale MC, MacLean CJ, Heath AC, Eaves LJ, Kessler LC(1993) Smoking and major depression: a causal analysis. ArchGen Psychiatry 50:36–43
Khantzian EJ (1997) The self-medication hypothesis of substance usedisorders: a reconsideration and recent applications. Harv RevPsychiatry 4:231–244
Kornetsky C, Bain G (1990) Brain-stimulation reward: a model fordrug induced euphoria. In: Adler M W, Cowan, A (eds) Modernmethods in pharmacology testing and evaluation of drugs ofabuse. Wiley-Liss, New York, p 211–231
Lane J, Rose J, Lefebre J, Keefe F (1995) Effects of cigarette smokingon perception of thermal pain. J Exp Clin Psychopharm 3:140–147
Lerman C, Jepson C, Wileyto EP, Epstein LH, Rukstalis M, Patterson F,Kaufmann V, Restine S, Hawk L, Niaura R, Berrettini W (2006)Role of functional genetic variation in the dopamine D2 receptor(DRD2) in response to bupropion and nicotine replacementtherapy for tobacco dependence: results of two randomizedclinical trials. Neuropsychopharmacology 31:231–242
Leventhal AM, Chasson GS, Tapia E, Miller EK, Pettit JW (2006)Measuring hedonic capacity in depression: a psychometricanalysis of three anhedonia scales. J Clin Psychol 62:1545–1558
Levin ED, Rose JE, Behm F, Caskey NH (1991) The effects ofsmoking-related sensory cues on psychological stress. PharmacolBiochem Behav 39:265–268
Loas G (1996) Vulnerability to depression: a model centered onanhedonia. J Affect Disord 41:39–53
Malpass D, Higgs S (2007) Acute psychomotor, subjective andphysiological responses to smoking in depressed outpatient
470 Psychopharmacology (2008) 196:461–471

smokers and matched controls. Psychopharmacology 190: 363–372
Martin M (1990) On the induction of mood. Clin Psychol Rev10:669–697
Masson CL, Gilbert DG (1999) Cardiovascular and mood responses toquantified doses of cigarette smoke in oral contraceptive usersand nonusers. J Behav Med 22:589–604
McCabe SB, Gotlib IH, Martin RA (2000) Cognitive vulnerability fordepression: deployment of attention as a function of history ofdepression and current mood state. Cogn Ther Res 24:427–444
McNair DM, Lorr M, Droppleman LF (1971) EITS manual for theprofile of mood states. Educational and Industrial Testing ServiceSan Diego
Meehl PE (1987) Hedonic capacity ten years later: some clarifications.In: Clark CC, Fawcett J (eds) Anhedonia and affect deficit states.PMA Publishing, New York
Murphy JM, Horton NJ, Monson BR, Laird NM, Sobol AM, LeightonAH (2003) Cigarette smoking in relation to depression: historicaltrends from the Stirling County Study. Am J Psychiatry 160:1663–1669
Parrott AC, Garnham NJ (1998) Comparative mood states andcognitive skills of cigarette smokers, deprived smokers andnonsmokers. Human Psychopharmacol Clin Exp 13:367–376
Perkins KA (1995) Individual variability in responses to nicotine.Behav Genet 25:119–132
Perkins KA, Grobe JE, Fonte C, Breus M (1992) “Paradoxical” effectsof smoking on subjective stress versus cardiovascular arousal inmales and females. Pharmacol Biochem Behav 42:301–11
Perkins KA, Doyle T, Ciccocioppo M, Conklin C, Sayette M (2006)Sex differences in the influence of nicotine dose instructions onthe reinforcing and self-reported rewarding effects of smoking.Psychopharmacology 184:600–607
Pickworth WB, Fant RV, Nelson RA, Rohrer MS, Henningfield JE(1999) Pharmacodynamic effects of new de-nicotinized ciga-rettes. Nicotine Tob Res 1:357–364
Pizzagalli DA, Jahn AL, O’Shea JP (2005) Toward an objectivecharacterization of an anhedonic phenotype: a signal-detectionapproach. Biol Psychiatry 57:319–327
Pomerleau CS, Pomerleau OF (1992) Euphoriant effects of nicotine insmokers. Psychopharmacology 108:460–465
Pomerleau CS, Carton SM, Lutzke ML, Flessland KA, Pomerleau OF(1994) Reliability of the Fagerstrom Tolerance Questionnaire andthe Fagerstrom Test for Nicotine Dependence. Addict Behav19:33–39
Quattrocki E, Baird A, Yurgelun-Todd D (2000) Biological aspects of thelink between smoking and depression. Harv Rev Psychiatry 8:99–110
Richmond M, Spring B, Sommerfeld BK, McChargue D (2001)Rumination and cigarette smoking: a bad combination fordepressive outcomes? J Consult Clin Psychol 69:836–840
Roisman GI, Fortuna K, Holland A (2006) An experimentalmanipulation of retrospectively defined earned and continuousattachment security. Child Dev 77:59–71
Rosenthal R, Rosnow RL, Rubin DB (2000) Contrasts and effect sizesin behavioral research: a correlational approach. CambridgeUniversity Press, Cambridge, UK
Spitzer RL, Williams JB, Gibbon M, First MB (1992) The structuredclinical interview for DSM-III-R (SCID). History, rationale, anddescription. Arch Gen Psychiatry 49:624–629
Spring B, Zubin J (1978) Attention and information processing asindicators of vulnerability to schizophrenic episodes. J PsychiatrRes 14:289–302
Spring B, Pingitore R, McChargue DE (2003) Reward value of cigarettesmoking for comparably heavy smoking schizophrenic, depressed,and nonpatient smokers. Am J Psychiatry 160:316–322
Spring B, Doran N, Pagoto S, McChargue D, Werth Cook J, Bailey K,Crayton J, Hedeker D (2007a) Fluoxetine, smoking, and historyof major depression: a randomized controlled trial. J Consult ClinPsychol 75:85–94
Spring B, Hitsman B, Pingitore R, McChargue DE, Gunnarsdottir D,Corsica J, Pergadia J, Doran N, Crayton JW, Baruah S, Hedeker D(2007b) Effect of tryptophan depletion on smokers and non-smokers with and without a history of major depression. BiolPsychiatry 61:70–77
Tremblay LK, Naranjo CA, Cardenas L, Hermann N, Busto UE(2002) Probing the brain reward system in major depressivedisorder: altered response to dextroamphetamine. Arch GenPsychiatry 59:409–416
Tremblay LK, Naranjo CA, Graham SJ, Herrmann N, Mayberg HS,Hevenor S, Busto US (2005) Functional neuroanatomicalsubstrates of altered reward processing in major depressivedisorder revealed by a dopaminergic probe. Arch Gen Psychiatry62:1228–1236
Warburton DM, Mancuso G (1998) Evaluation of the informationprocessing and mood effects of a transdermal nicotine patch.Psychopharmacology 135:305–310
Watson D, Clark LA, Tellegen A (1988) Development and validationof brief measures of positive and negative affect: the PANASscales. J Pers Soc Psychol 54:1063–1070
Werth Cook J, Spring B, McChargue DE, Hedeker D (2004a) Hedoniccapacity, cigarette craving and diminished positive mood.Nicotine Tob Res 6:37–45
Werth Cook J, Spring B, McChargue DE, Borrelli B, Hitsman B,Niaura R, Keuthen NJ, Kristeller J (2004b) Influence offluoxetine on positive and negative affect in a clinic-basedsmoking cessation trial. Psychopharmacology 173:153–159
Williams JBW, Gibbon M, First MB, Spitzer RL, Davies M, Borus J,Howes MJ, Kane J, Pope HG, Rounsaville B, Wittchen HU(1992) The structured clinical interview for DSM-III-R (SCID).Multisite test–retest reliability. Arch Gen Psychiatry 49:630–636
Wu LT, Anthony JC (1999) Tobacco smoking and depressed mood inlate childhood and early adolescence. Am J Public Health89:1837–1840
Zubin J, Spring B (1977) Vulnerability: a new view of schizophrenia. JAbnorm Psychol 86:103–126
Psychopharmacology (2008) 196:461–471 471




















