Cardiovascular Risk Behavior among Sedentary Female Smokers and Smoking Cessation Outcomes
20
TOBACCO INDUCED DISEASES Vol. 3, No. 1:7-26 (2005) © PTID Society Cardiovascular Risk Behavior among Sedentary Female Smokers and Smoking Cessation Outcomes Tellervo Korhonen 1 , Taru Kinnunen 1 , Zandra Quiles 2 , Robert F. Leeman. 3 , Donna Medaglia Terwal 1 , Arthur J.Garvey 1 1 Tobacco Dependence Treatment and Research, Harvard School of Dental Medicine, Boston, MA; 2 Lehman College—CUNY, New York, NY; 3 Department of Psychiatry, Yale University School of Medicine, New Haven, CT ABSTRACT: Background. We examined female sedentary smokers’ additional cardiovascular disease (CVD) risk behaviors and their associations to smoking cessation. Method. This study was part of a randomized controlled trial testing the effectiveness of exercise and nicotine gum in smoking cessation. Included in the analyses were 148 participants. Dietary habits and alcohol consumption were measured as additional CVD risk behaviors. High-fat diet and heavy alcohol use were considered those risk behaviors. Nicotine dependence, length of the longest quit attempt, depressive symptoms, self-efficacy, and education were examined as other baseline variables. Abstinence from tobacco was recorded through 12 months. Results. Diet was related to depressive symptoms at baseline. Alcohol use was related to nicotine dependence and education level. Heavy alcohol use alone and accumulation of two added risk behaviors predicted poorer smoking cessation outcome. Although diet alone was not associated with cessation outcome the high-fat diet interacted with depressive symptoms, such that the depressed women with high-fat diet were significantly more likely to relapse in their quit attempt compared to other subgroups. Conclusions. Non-moderate alcohol use alone and accumulation of multiple CVD risk behaviors seem to be associated with lower success in smoking cessation. KEYWORDS: smoking; health behaviors; smoking cessation; cardiovascular diseases; women’s health INTRODUCTION Smoking cessation results in many positive health consequences; most immediately and substantially cessation reduces the risk for coronary heart disease and other cardiovascular diseases (CVD) [ 1 ]. It has been suggested that treating tobacco dependence is more cost-effective than any other preventive cardiology measure [2]. However, many clinical trial studies report declining abstinence rates over time from the 1970s to 1990s [3, 4]. One explanation is that nowadays smokers tend to be highly dependent on nicotine [ 5 ]. Highly dependent smokers tend to have lower education, more depressive symptoms, consume unhealthy foods, and report more hazardous drinking and less physical activity than smokers with low dependence [6-9]. Studies in the U.S. have shown that smoking women are more likely to use alcohol, marijuana and cocaine, and have greater substance use severity than the non-smokers [10-13]. Further, smoking is predictive of many other negative health behaviors. Indeed, while unhealthy
-
Upload
independent -
Category
Documents
-
view
8 -
download
0
Transcript of Cardiovascular Risk Behavior among Sedentary Female Smokers and Smoking Cessation Outcomes

TOBACCO INDUCED DISEASES Vol. 3, No. 1:7-26 (2005) © PTID Society
Cardiovascular Risk Behavior amongSedentary Female Smokers and Smoking
Cessation Outcomes
Tellervo Korhonen1, Taru Kinnunen1, Zandra Quiles2, Robert F. Leeman.3,Donna Medaglia Terwal1, Arthur J.Garvey1
1Tobacco Dependence Treatment and Research, Harvard School of Dental Medicine, Boston,MA; 2Lehman College—CUNY, New York, NY; 3Department of Psychiatry, Yale University
School of Medicine, New Haven, CT
ABSTRACT: Background. We examined female sedentary smokers’ additionalcardiovascular disease (CVD) risk behaviors and their associations to smokingcessation. Method. This study was part of a randomized controlled trial testingthe effectiveness of exercise and nicotine gum in smoking cessation. Included inthe analyses were 148 participants. Dietary habits and alcohol consumption weremeasured as additional CVD risk behaviors. High-fat diet and heavy alcohol usewere considered those risk behaviors. Nicotine dependence, length of the longestquit attempt, depressive symptoms, self-efficacy, and education were examined asother baseline variables. Abstinence from tobacco was recorded through 12months. Results. Diet was related to depressive symptoms at baseline. Alcoholuse was related to nicotine dependence and education level. Heavy alcohol usealone and accumulation of two added risk behaviors predicted poorer smokingcessation outcome. Although diet alone was not associated with cessationoutcome the high-fat diet interacted with depressive symptoms, such that thedepressed women with high-fat diet were significantly more likely to relapse intheir quit attempt compared to other subgroups. Conclusions. Non-moderatealcohol use alone and accumulation of multiple CVD risk behaviors seem to beassociated with lower success in smoking cessation.
KEYWORDS: smoking; health behaviors; smoking cessation; cardiovasculardiseases; women’s health
INTRODUCTION
Smoking cessation results in manypositive health consequences; mostimmediately and substantially cessationreduces the risk for coronary heart diseaseand other cardiovascular diseases (CVD)[1]. It has been suggested that treatingtobacco dependence is more cost-effectivethan any other preventive cardiologymeasure [2]. However, many clinical trialstudies report declining abstinence ratesover time from the 1970s to 1990s [3, 4].One explanation is that nowadays smokers
tend to be highly dependent on nicotine[5]. Highly dependent smokers tend tohave lower education, more depressivesymptoms, consume unhealthy foods, andreport more hazardous drinking and lessphysical activity than smokers with lowdependence [6-9].
Studies in the U.S. have shown thatsmoking women are more likely to usealcohol, marijuana and cocaine, and havegreater substance use severity than thenon-smokers [10-13]. Further, smoking ispredictive of many other negative healthbehaviors. Indeed, while unhealthy

8 Korhonen MT, Kinnunen T, Quiles Z, Leeman RF, Terwal DM, Garvey AJ
behaviors have shown pair-wise andmultiple accumulation, smoking inparticular, has the strongest and mostconsistent associations with otherunhealthy behaviors [8, 14-16]. Thisclustering of smoking and other unhealthybehaviors, “risk behavior syndrome”, mayhave already emerged at a young age, suchas during elementary school [17, 18] .Readiness to quit smoking is also related toother health behaviors. Smokers who donot want to quit smoking (consonantsmokers) differ in their health behaviorfrom those willing to quit (dissonantsmokers). Smokers in the pre-contemplation stage, not planning to quitwithin the next six months, demonstratefewer positive health practices [19 ] .Particularly, female consonant smokerstend to be more sedentary and heavierdrinkers than female dissonant smokers[20].
The cardiovascular association of otherunfavorable health behaviors besidessmoking, such as alcohol use and diet, hasbeen documented [21-23]. Alcohol use hasa J-shape association to risk of CVDsuggesting that moderate alcoholconsumption would be protective whereasno alcohol drinking and heavy alcohol usewould be risk factors [23 ]. There is,however, a recent study suggesting thatthis J-shape association would not be trueamong current smokers [24]. In relation toCVD, the unhealthy dietary practicesinclude the high consumption of saturatedfats, salt and refined carbohydrates, as wellas low consumption of fruits andvegetables - and these tend to clustertogether [21, 22, 25]. Further, smoking incombination with other risk factors has aparticularly high impact on total CVD risk[26].
Although the presence of multiplehealth risk behaviors is related topredictors of continued smoking, such asnicotine dependence, the association ofthose unfavorable health behaviors withsmoking cessation outcomes is stillunclear. Particularly for female smokers,dietary intake plays an important role in
smoking cessation via post-cessationweight gain [1]. In addition, smokers areless likely to be ready to make positivechanges in their dietary fat and fiberintakes [27]. Based on these notions itwould be relevant to argue that a smokerwith an unhealthy diet would be morelikely to gain weight during quitting andthus, more likely to relapse because ofweight concerns. There is only one earlierstudy examining prospective relationshipbetween diet and smoking cessationoutcomes [28]. In this particular study theunhealthy diet was analyzed together withlow physical activity level. The studyfound a significant association betweenhigh dietary fat intake / low physicalactivity level and smoking dependencyamong men and women. However, theassociation to cessation outcome wassignificant only among men but not amongwomen. Shiffman et al. [2 9 ] havesuggested that drinking alcohol in generalis a significant precipitant of smokingrelapse after a quit attempt. However, noprevious study has examined whether theassociation of alcohol use with smokingcessation outcome would follow similar J-shape found in relation to CVD [23] –recently challenged by specific findingsamong smokers [24].
To understand the complex reasonsfor women’s difficulties in smokingcessation there is need for a morecomprehensive analyses of potential riskfactors of high relapse rate after a quitattempt. It is known that various healthbehaviors, in addition to smoking, carry asignificant risk for CVD. However, it isstill unclear, if and how those behaviorswould be risk factors for smokingcessation. Our main objective was toanalyze if female sedentary smokers’additional CVD health risk behaviors, dietand alcohol use, predict abstinence fromtobacco use. The secondary objective wasto examine these risk behaviors’association to other variables related tosmoking cessation. These include variableswhich reflect smoking-related (nicotinedependence, length of the longest past quit

Cardiovascular Risk Behavior among Sedentary Female Smokers & Smoking Cessation Outcomes 9
attempt), socio-economic (education), andpsycho-social (depressive symptoms, self-efficacy) components of the smokingcessation process.
METHODS
Study designSedentary female smokers from the
Greater Boston area were recruited for arandomized controlled trial testing theeffectiveness of aerobic exercise as anadjunct to nicotine gum therapy. Theinclusion criteria included an age of 18-55years[JS1], no major cardiac conditions(e.g. history of acute cardiac eventsincluding MI or current abnormal restingEKG), not pregnant or planning pregnancy,not suffering from any severe psychiatricconditions, bleeding ulcers or insulindependent diabetes.The participants were followed from 3weeks before cessation to 1 year post-cessation. We provided all participantswith nicotine gum treatment and briefcounseling (how to use gum, possiblewithdrawal symptoms and how to dealwith them). We randomly assigned theparticipants to one of three conditions: (1)Exercise intervention condition (‘exercisegroup’). This consisted of two 45-minuteexercise sessions per week from 3 weekspre-cessation through 2 weeks post-cessation. At that time, and continuingthrough 16 weeks post-cessation, exercisesessions were reduced to one per week. Inaddition, the participants were asked toexercise 2-3 times per week on their own.(2) Equal contact control condition(‘wellness group’). This included wellnesslectures and discussions for the same timeperiod and with the same frequency andduration as the exercise intervention.Compliance with both ‘exercise group’ and‘wellness group’ was monitored through16 weeks by recording attendance of thesessions in both groups plus by self-
reported frequency of home exercise in theexercise group. (3) Standard care controlcondition (‘control group’).[JS2] Thisincluded only the nicotine gum treatmentand brief counseling received by the othertwo groups as well. The present set ofanalyses is not investigating theintervention effect, and only thoseconditions that had equal contact times andsimilar abstinence rates (the main outcomemeasure of the trial), were included in thepresent report. The sample consisted of148 participants randomized into the‘exercise group’ (n=92) and ‘wellnessgroup’ (n=56). Cox Proportional Hazardmodel Survival analysis for 12-monthfollow up indicated no significantdifference in abstinence rates between theexercise and wellness group (p = 0.600).The standard care ‘control group’ wasexcluded as it differed in the main outcomeboth from the ‘wellness group’ and‘exercise group’ (p < .05) and did not haveequal contact.
Figure 1 shows the experimental designof the trial with numbers of participants ineach group. The research study wasapproved by the Harvard Medical SchoolOffice for Research Subject Protection andby the Brigham and Women’s Hospital’sHuman Research Committee. Allparticipants signed the Informed Consentform.
ParticipantsParticipant characteristics are shown in
Table 1. On average, participants were38.1 (SD = 9.6) years old and smoking18.2 (SD = 8.1) cigarettes per day.The majority were Caucasian/white(80.1%) and single, separated, divorced orwidowed (80.3%). All participants had atleast high school education.

10 Korhonen MT, Kinnunen T, Quiles Z, Leeman RF, Terwal DM, Garvey AJ
TABLE 1. Characteristics of Study Participants at Baseline
(%) n
Race/ethnicityWhiteAfrican AmericanHispanicOther
80.112.3 4.8 2.8
1171874
Marital statusSingleMarriedDivorced/separated/widowed
56.519.723.8
832935
EducationHigh school graduate or G.E.D.Some college/business/technical schoolCollege graduatePost-college degree
8.146.030.415.5
12684523
Mean (SD)
Age 38.1 (9.6)
Number of cigarettes/day 18.3 (8.1)
SampleSedentary
Womenages 18-55
Exercise Intervention Group(n=92)
3 wks + 16 wks TxNicotine gum 16 wks
Equal Contact Control Group(n=56)
3 wks + 16 wks TxNicotine gum 16 wks
Standard Care Control Group(n=35)
Brief AdviceNicotine gum 16 wks
Fig. 1. Experimental design of the trial.
Participants of this study (n=148)

TOBACCO INDUCED DISEASES Vol. 3, No. 1:7-20 (2005) © PTID Society
Assessments Risk behaviors. As mentioned earlier, allparticipants were daily smokers (>5cigarettes per day) with a sedentarylifestyle (exercising <3 times per week for30 minutes). Thus, every participant wasengaged at least in two compromisingbehaviors, which have been identified asCVD risk factors [30, 31]. As additionalCVD risk behaviors, we measured dietarybehavior and alcohol consumption [21-23].
Dietary behavior. In the baselinequestionnaire we asked the participantshow often they had eaten various foodsduring the past week, such as fruit, juice,green salad, cooked vegetables,hamburgers, hot dogs, sausages, frenchfries, potato chips, cookies, etc. Thefrequency for each type of food productwas scored as follows: 0= never, 1 = in 1-2days, 2= in 3-5 days, 3= in 6-7 days, 4=every day. We used this data and our ownmethod to categorize the participants intothree groups. The “high-fat” group wasdefined as a diet high in saturated fatsfound in animal products, such as meat,eggs and dairy. Thus, high frequency(scored as 3-4) of eating hamburgers, hotdogs, sweet pastries etc. and low frequency(scored as 0-1) of eating fruit, juice, greensalad, cooked vegetables etc. wascategorized as a “high-fat” diet.Respectively, high frequency of eatingfruit, juice, green salad etc. and lowfrequency of eating hamburgers, hot dogs,sausages, etc. were categorized as a “high-vegetable” diet. Those who did not fit intothese two categories were classified intothe “mixed diet” category. The proportionsof participants in each group were asfollows: high-fat (27%), high-vegetable(30%), and mixed diet (43%). The “high-fat” diet was regarded as a dietary riskbehavior, most of the foods in this groupbeing high in saturated fats, salt, andrefined carbohydrates, but low in fruits andvegetables [21, 22].
Alcohol use. Data on alcoholconsumption were based on questions ofhow many cans/bottles (12 oz) of beer,glasses of wine (6 oz) or mixed drinks (e.g.
scotch, brandy, gin, vodka) our participantsdrink per week on average. Based on sumscores, we created three alcoholconsumption groups as follows: no alcoholuse at all (29% of the participants), 1-7drinks per week (mean=3.5, SD=1.9) (49%of the participants), and more than sevendrinks per week (mean=14, SD=7.1) (22%of the participants). The definition ofspecific risk behavior group was difficultbecause of inconsistent evidence.According to the J-shaped relationship ofalcohol use and risk of CVD, non-use ofalcohol on one hand, and more than 7drinks per week on the other hand shouldbe regarded as alcohol-related riskbehavior for CVD [23], suggesting that thetwo first groups could be merged as onerisk group. However, this J-shapedassociation has been recently challengedamong smokers [24]. Thus, in relation tosmoking cessation, we analyzed alcoholconsumption in those three separatecategories.
Other baseline variables. Nicotinedependence, length of the longest past quitattempt, depressive symptoms, self-efficacy, and education were examined asother baseline variables. These variableswere selected to reflect smoking-related,psycho-social and socio-economiccomponents of the smoking cessationprocess. Earlier studies have suggestedtheir association with continuing smoking[32], smoking cessation [33-37], or otherhealth behaviors [6, 28]. Nicotinedependence was assessed with theFagerström test for Nicotine Dependence(FTND) [38], a 6-item revision of theFagerström Tolerance Questionnaire.Scores of the FTND range from 0 to 10.Length of the longest past quit attempt wasbased on the question “What is the longesttime you have ever been able to quitsmoking?” Participants were asked torecord time by year, month, week, and/ordays. For data analyses, we convertedthese reports into days of abstinence. Tomeasure participants’ depression status atbaseline we used the Center forEpidemiological Studies Depression Scale

12 Korhonen MT, Kinnunen T, Quiles Z, Leeman RF, Terwal DM, Garvey AJ
(CES-D) [3 9 ]. The CES-D is anestablished self-report measure of both thefrequency and severity of depressivesymptoms. It consists of 20 symptoms thatwere rated on how frequently a person hadexperienced a given symptom during thepast week. The appropriate items werereverse-scored and responses weresummed to create a depression score,which can range from 0 to 60. Inaccordance with the standard scoringprocedure for the CES-D, participants whoscored higher than 15 were classified asdepressed and those who scored 15 orbelow were classified as non-depressed[39]. Self-efficacy was measured with theitem “How confident are you that you willbe able to quit smoking for the next 3months?” rated on a 5-point scale rangingfrom 0, very slightly or not at all, to 4,extremely confident. Education wasmeasured as the highest level of formaleducation ranging from “Grade school” upto “Post-graduate degree”.Abstinence. Abstinence from cigaretteswas measured immediately after quitting.The definition of relapse implemented inthis study was taken from therecommendations of the National TaskForce of Relapse (7 consecutive days orepisodes of smoking)[40]. For this studyabstinence was recorded at 3, 7, 14, 30, 60,90 120, 180, 270 and 360 days postcessation. Self-reported abstinence wasverified by expired carbon monoxide atevery follow-up visit. Salivary cotininelevels were monitored after nicotine gumuse was discontinued. Abstinence wasdetermined on an intent-to-treat basis, inthat the participants who reported for thebaseline visit and pre-quit visit receivedthe NRT with behavioral counseling but atsome subsequent time became lost tofollow-up, were considered to haverelapsed. Both the CO and salivarycotinine were measured at the baselinevisit as well. Whether the intervention ledto any harm reduction is an important issueand will be evaluated in the relevantanalysis and further reported in a separatepaper. The current paper focuses on the
baseline risk behaviors as predictors ofquitting.
Statistical analysesUnivariable statistical methods
included chi-square analyses withcategorical variables, and analyses ofvariance plus Tukey’s HSD post hoc testsfor independent samples with continuousvariables. Nicotine dependence, depressivesymptoms, and self-efficacy were used ascontinuous sum scores in the analyses ofvariance. Length of the longest past quitattempt, although a continuous variable,was not normally distributed (skewness =4.10). Thus, it was classified into 2categories using a median split (120 daysor less / more than 120 days). Educationwas classified into 2 categories (less thancollege graduate / college graduate ormore).
As multivariable methods, survivalanalyses (proportional hazards models)were performed to examine therelationships among risk behaviors,smoking-related variables, and relapse.Reference cell coding was used in post hocanalyses to test pair-wise differences inabstinence rates among the subgroups [41].The statistical significance of the pair-wisedifferences in the survival curves weretested by Log Rank and Cox’s F tests. Inorder to analyze accumulation effect ofmultiple risk behaviors we used number ofthose behaviors as a three categoryvariable (0, 1, 2 added risk behaviors).The classification into a risk behavior wasbased on the survival analyses for dietarybehavior and alcohol consumption. Thegroup of each behavior (diet or drinking)showing the strongest association withrelapse was regarded as a risk behavior.For crude hazard ratios and for testing theinteractions, the other explanatoryvariables were dichotomized as follows:n i c o t i n e d e p e n d e n c e(high=FTND>5/low=FTND<5), longestquit attempt (short=<120 days/ long= >120days), depression (depressed=CES-D>15/non-depressed=CES-D<15), self-efficacy(low=confidence

Cardiovascular Risk Behavior among Sedentary Female Smokers & Smoking Cessation Outcomes 13
score<2.5/high=confidence score>2.5) andeducation (low=<college/high=>college).The cutoff points were selected becausethey provided mean splits, except the CES-D, where the cutoff point was based onearlier literature [42]. First, we computedthe unadjusted survival models for diet,alcohol use and accumulation of riskbehaviors (0, 1, 2), as well as for nicotinedependence, longest quit attempt,depressive symptoms, self-efficacy andeducation separately (crude hazard ratios).Second, we computed the adjusted modelsfor diet, alcohol and accumulatedbehaviors, adjusting for nicotinedependence, longest quit attempt,depressive symptoms, self-efficacy andeducation (adjusted hazard ratios). Finally,we tested all possible interactions betweeneach behavior (alcohol use, diet) and eachof the other baseline variables.
RESULTS
The random assignment resulted infairly equal number of both ‘exercise’ and“wellness’ group participants in theadditional risk behaviors groups (p=0.830,χ2 test). As shown in Table 2, dietarybehavior was related to depression status atbaseline (p =0.053, analysis of variance).Those engaged in a mixed diet had higherdepression scores than those with a highproportion of vegetables in their diet( p <0.05, Tukey’s test). Alcoholconsumption was related to nicotinedependence (p =0.026, analysis ofvariance). Those with moderate drinkinghad lower FTND score compared to thosewith no alcohol use at all (p<0.05, Tukey’stest). Alcohol use was also related toeducational level. The proportion ofwomen with less than college degree waslowest in the group with moderate drinking(p=0.013, χ2 test) (see Table 3).
TABLE 2. Socioeconomic, Smoking-related and Psycho-social Baseline Variables by DietaryBehavior
High-fat diet(n=40)
Mixed diet(n=64)
High-vegetable diet(n=44)
% n % n % n P value
Education% < college degree 57.5 23 51.6 33 54.6 24 0.903 a
Longest quit attempt% < 120 days 60.0 24 43.7 28 52.3 23 0.264a
Mean (SD) Mean (SD) Mean (SD) P value
FTND b - score 5.3 2.3 4.5 2.6 5.4 2.4 0.142c
CESDd - score 14.3e,f 9.9 16.1 f 9.8 11.4 e 9.6 0.053c
Self-efficacy - score 2.4 0.9 2.5 0.9 2.4 0.8 0.950c
a χ2 testb Fagerstrom Test for Nicotine Dependencec analysis of variance and Tukey’s Testd Center for Epidemiological Studies-Depressione,f mixed diet > vegetable diet; p<0.05

14 Korhonen MT, Kinnunen T, Quiles Z, Leeman RF, Terwal DM, Garvey AJ
TABLE 3. Socio-economic, Smoking-related and Psycho-social Baseline Variables byAlcohol Use
0 drinks/week (n=43)
1-7 drinks/week (n=72)
>7 drinks/week (n=32)
% n % n % n P value
Education% < college degree 75.0 41.7 53.1 0.013a
Longest quit attempt% < 120 days 43.2 19 51.4 37 59.4 13 0.373 a
Baseline variable Mean (SD) Mean (SD) Mean (SD) P value
FTNDb - score 5.8d 2.4 4.5e 2.2 4.9 d, e 2.8 0.026c
CESDf - score 12.5 9.7 14.7 8.8 15.7 12.5 0.344c
Self-efficacy - score 2.5 0.8 2.5 0.9 2.3 0.9 0.623c
a χ2 testb Fagerstrom Test for Nicotine Dependencec analysis of variance and Tukey’s Testd,e No alcohol > 1-7 drinks/week; p<0.05,f Center for Epidemiological Studies-Depression
Based on unadjusted survival analysis, thequality of diet alone did not predictabstinence (see Table 4). The Hazard ratiofor high-fat diet vs. high-vegetable dietwas 1.27 (CI95% 0.83-1.95), but theassociation was not significant. Thesurvival curve for diet is shown in Figure2. Alcohol use alone was a significantpredictor of cessation outcome. Those whoconsumed more than 7 drinks per weekwere more likely to relapse than those who
used alcohol moderately (Hazardratio=1.62, CI95% 1.06-2.48). Those withno alcohol use showed a marginally higherrisk for relapse (Hazard ratio=1.17, CI95%0.80-1.70). The survival curve for alcoholis shown in Figure 3, where the differencebetween the curve of moderate drinkersand the one of high consumers wassignificant (p=0.020 Log Rank test; p=0.01Cox F-test).

Cardiovascular Risk Behavior among Sedentary Female Smokers & Smoking Cessation Outcomes 15
TABLE 4. Survival Analyses of Likelihood of Relapse: Crude Hazard Ratios (n=146)
Hazard Ratio 95% CIa χ2 P value
DietHigh-vegetableMixedHigh-fat
1.001.081.27
0.73-1.580.83-1.96
0.141.20
0.7120.272
AlcoholNo alcohol
1-7 drinks/week>7 drinks/week
1.171.001.62
0.80 - 1.70
1.06 - 2.48
0.64
5.02
0.422
0.025
Accumulation of risk behaviorsNo risk behaviors>7 drinks/week or high-fat diet>7 drinks/week and high-fat diet
1.001.302.56
0.93 – 1.831.16 – 5.62
2.345.44
0.1260.020
Nicotine dependence Low (FTND<5) High (FTND>5)b
1.001.05 0.76 – 1.46 0.09 0.760
Longest quit attempt Long (<120 days)
Short (<120 days)1.001.25 0.91-1.73 1.86 0.172
Baseline depressionNon-depressed (CESD≤15)
Depressed (CESD>15)c
1.001.02 0.73-1.42 0.01 0.919
Self-efficacy High (confidence score>2.5) Low (confidence score<2.5)
1.001.07 0.77-1.47 0.14 0.706
EducationHigh (>college degree)Low (<college degree)
1.001.12 0.81-1.55 0.46 0.499
a CI = Confidence Intervalb FTND = Fagerstrom Test for Nicotine Dependencec CESD = Center for Epidemiological Studies-Depression

16 Korhonen MT, Kinnunen T, Quiles Z, Leeman RF, Terwal DM, Garvey AJ
Cumulative Proportion Surviving (Kaplan-Meier)
Dietary behavior
High-fat diet (n=40) Mixed diet (n=64) High-vegetable diet (n=44)
0 50 100 150 200 250 300 350 400 450
Days Post Cessation
-10%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Cum
ulat
ive
Pro
port
ion
Sur
vivi
ng
Fig. 2. Percent abstinent during 365 days post-cessation by diet.No significant differences were observed.
Cumulative Proportion Surviving (Kaplan-Meier)
Alcohol consumption
No alcohol (n=44) 1 - 7 drinks per week (n=72) > 7 drinks per week (n=32)
0 50 100 150 200 250 300 350 400 450
Days Post Cessation
-10%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Cum
ulat
ive
Pro
port
ion
Sur
vivi
ng
Fig. 3. Percent abstinent during 365 days post-cessation by alcohol consumption. Differencebetween the curve of moderate drinkers and the one of high consumers was significant (p=0.02Log Rank test; p=0.01 Cox F-test).
Cardiovascular Risk Behavior among Sedentary Female Smokers & Smoking Cessation Outcomes 17
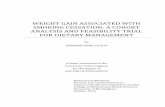
The accumulation of risk behaviors wasanalyzed in three groups as follows: no riskbehaviors (n=83), i.e. no heavy alcohol useand no high-fat diet, one risk behavior(n=58), i.e. heavy alcohol use withouthigh-fat diet (n=25) or high-fat dietwithout heavy alcohol use (n=33), and tworisk behaviors (n=7), i.e. heavy drinkingand high-fat diet. When analyzed by thisaccumulation of added risk behaviors,those who consumed >7 drinks per week
and had high-fat diet, showed asignificantly higher risk for relapse thanthose without those added risk behaviors(Hazard ratio =2.56, CI95% 1.16-5.62).The survival curves for accumulationeffect and numbers of participants in eachgroup are shown in Figure 4, where thedifference between the curve of 2 risks andthe one of no risks was significant(p=0.001 Cox F-test).
Cumulative Proportion Surviving (Kaplan-Meier)Number of Risk Behaviors
N o r i s k b e h a v i o r s ( n = 8 3 )
O n e r i s k b e h a v i o r ( n = 5 8 )
T w o r i s k b e h a v i o r s ( n = 7 )
0 50 100 150 200 250 300 350 400 450
Days Post Cessation
-10%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Cum
ulat
ive
Pro
porti
on S
urvi
ving
Fig. 4. Percent abstinent during 365 days post-cessation by accumulation of risk behaviors. The differencebetween the curve of two risks and the one of no risks was significant (p=0.001 Cox F-test).
No alcohol
1 – 7 drinks per week> 7 drinks per week

18 Korhonen MT, Kinnunen T, Quiles Z, Leeman RF, Terwal DM, Garvey AJ
Cumulative Proportion Surviving (Kaplan-Meier)
Diet in depressed participants
fat diet (n=17) mixed diet (n=30) vegetable diet (n=15)
0 50 100 150 200 250 300 350 400 450
Days Post Cessation
-10%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Cum
ulat
ive
Pro
port
ion
Sur
vivi
ng
Cumulative Proportion Surviving (Kaplan-Meier)
Diet in non-depressed participants
fat diet (n=22) mixed diet (n=34) vegetable diet (n=28)
0 50 100 150 200 250 300 350 400 450
Days Post Cessation
-10%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Cum
ula
tive P
roport
ion S
urv
ivin
g
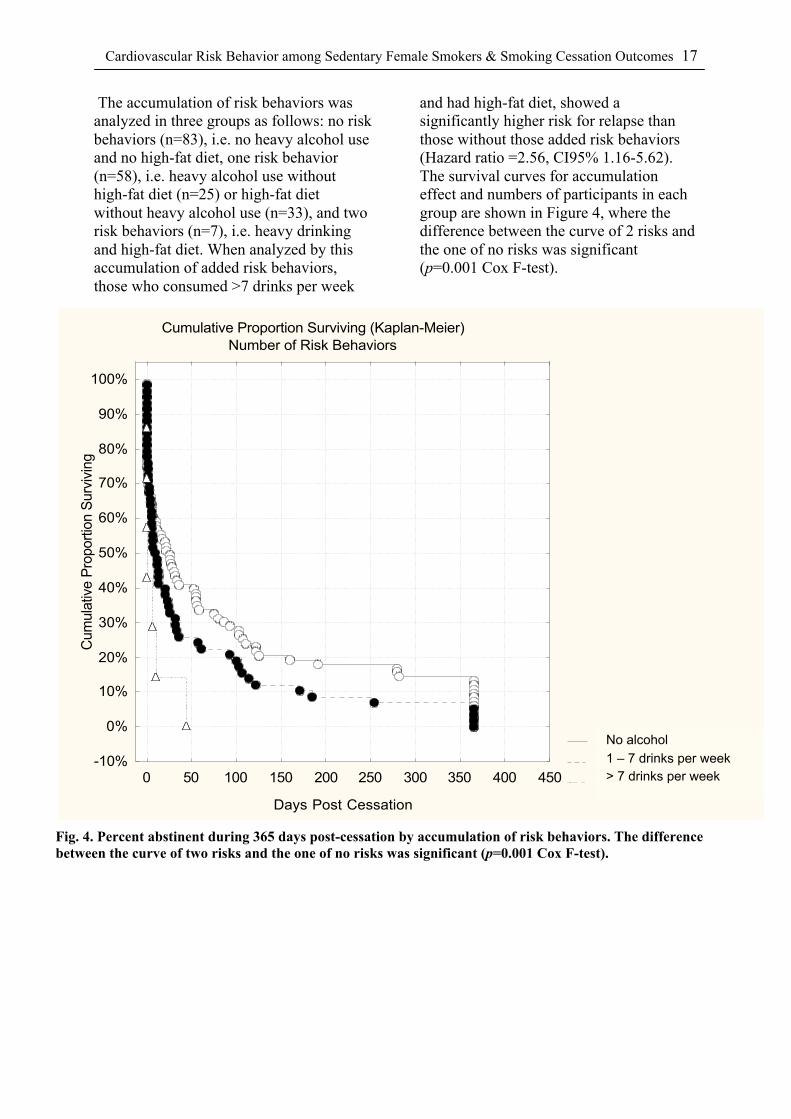
None of the other baseline variablesstudied had any significant main effect onabstinence. When adjusting for the othervariables (Table 5), the associations ofalcohol alone (1.62; 1.06-2.48) and alcoholaccumulated with high-fat (2.56; 1.16-5.62) remained significant. Finally, wetested the interactions of heavy alcohol useand high-fat diet with all other baselinevariables. Only one significant interactionwas found, i.e. between baselinedepressive symptoms and dietary behavior(p= 0.019). When adjusting for otherbaseline variables the quitters with highCESD scores were three times as likely torelapse (Hazard ratio = 3.02, CI95% 1.20-
7.57) in comparison to those with highvegetable diet and low depression score(Table 6). The pair-wise comparisonsbetween each subgroup based on referencecell coding are shown in Table 7. Thesurvival curves of subgroups by depressivesymptoms and diet group are shown inFigure 5a and 5b. Based on both pair-wisecomparison tests, the survival of those withhigh depression scores and high-fat dietwas significantly poorer than among thosedepressed with high-vegetable diet (p=0.02Log Rank test; p=0.01 Cox F test). Amongthe participants with low depression scoresthere was no significant difference bydietary behavior in abstinence.
Fig. 5a. Percent abstinent during 365 days post-cessation by diet group in depressed participants.Abstinence of those with high depression scores andhigh-fat diet was significantly poorer than among thosedepressed with high-vegetable diet (p=0.02 Log Ranktest; p=0.01 Cox F test).
Fig. 5b. Percent abstinent during 365 days post-cessation by diet group in non-depressedparticipants. Among the participants with lowdepression scores no significant differences bydietary behavior were observed.
Fig. 5a. Percent abstinentduring 365 days post-cessationby diet group in depressedparticipants. Abstinence ofthose with high depressionscores and high-fat diet wassignificantly poorer thanamong those depressed withhigh-vegetable diet (p=0.02 LogRank test; p=0.01 Cox F test).
Fig. 5b. Percent abstinentduring 365 days post-cessation by diet group innon-depressed participants.Among the participants withlow depression scores nosignificant differences bydietary behavior wereobserved.
Cardiovascular Risk Behavior among Sedentary Female Smokers & Smoking Cessation Outcomes 19
TABLE 5. Survival Analyses of Likelihood of Relapse: Adjusteda Hazard Ratios (n=146)
Hazard Ratio 95% CIb χ2 P value
DietHigh-vegetableMixedHigh-fat
1.001.161.27
0.76-1.750.81-1.99
0.471.11
0.4900.292
AlcoholNo alcohol1-7 drinks/week>7 drinks/week
1.101.001.62
0.71-1.69
1.05-2.50
0.18
4.66
0.669
0.031
Accumulation of risk behaviorsNo risk behaviors>7 drinks/week or high-fat diet>7 drinks/week and high-fat diet
1.001.302.57
0.92-1.841.08-6.09
2.224.59
0.1360.032
a Adjusted for nicotine dependence, longest quit attempt, baseline depression, self-efficacy,and educationb CI = Confidence Interval
TABLE 6. Survival Analyses of Likelihood of Relapse: Interaction Model with Adjusted a
Hazard Ratios (n=146)
Hazard Ratio 95% CIb χ2 P value
DietHigh-vegetableMixedHigh-fat
1.001.040.85
0.62-1.750.48-1.50
0.030.31
0.8730.579
Baseline depressionNon-depressed (CESD≤15)
Depressed (CESD>15)c
1.000.72 0.38-1.37 1.01 0.314
Interaction: Diet x DepressionHigh-veg. diet x Non-depressedMixed diet x DepressedHigh-fat diet x Depressed
1.001.373.02
0.61-3.071.20-7.57
0.585.52
0.4470.019
a adjusted for nicotine dependence, longest quit attempt, self-efficacy, educationb CI = Confidence Intervalc CESD=Center for Epidemiological Studies-Depression

20 Korhonen MT, Kinnunen T, Quiles Z, Leeman RF, Terwal DM, Garvey AJ
TABLE 7. Pair-wise Comparisons between Groups by Depression and Dieta
χ2 P valueb
Depressed+No High-fat Diet vs. Depressed+High-fat diet 6.48 0.011
Non-Depressed+No High-fat Diet vs. Non-Depressed+High-fat diet 0.31 0.579
Non-Depressed+No High-fat Diet vs. Depressed+High-fat diet 3.68 0.055
Non-Depressed+No High-fat Diet vs. Depressed+ No High-fat Diet 1.01 0.314
Non-Depressed+High-fat diet vs. Depressed+High-fat diet 0.91 0.339
Non-Depressed+High-fat diet vs. Depressed+No High-fat Diet 0.24 0.623
a adjusted for nicotine dependence, longest past quit attempt, self-efficacy, educationb based on reference cell coding
DISCUSSION
This study suggested that added CVDrisk behaviors such as high alcoholconsumption predict poorer cessationoutcome in a quit attempt. Theaccumulation of added risk behaviors -although reflecting a relatively smallnumber of participants - also predictedlower abstinence. Dietary behavior alonewas not related to cessation outcome.However, being engaged in high-fat dietseemed to interact with depression,suggesting that depressed women engagingin high-fat diet are more likely to relapse intheir quit attempt.
Sherwood et al. [28] found that thebaseline multiple health risk behaviorswere associated with higher FagerstromNicotine Dependence (FTND) scores andlower self-efficacy from refraining fromsmoking. Our results partly support theseresults as our data showed a marginallysignificant association between alcohol useand FTND. However, in the presentanalysis self-efficacy, measured as baselineconfidence to quit smoking, was notassociated with engaging in additional riskbehaviors. Studies among a populationsample and among hospitalized smokershave found that alcohol use had strongerassociations with smoking-relatedvariables, such as nicotine dependence,
than with variables related to smokingcessation motivation [43, 44].
Regarding smoking cessation outcome,we found that multiple compromisinghealth behaviors are significantly related topoor abstinence among women, whereasan earlier study [28] found a significantassociation among men only. Differentresults may be due to different healthbehaviors examined in these two studies;i.e. diet and alcohol use in the presentanalysis versus diet and physical activity inSherwood’s study [28]. Also, all ourparticipants already had two riskbehaviors; i.e. smoking and sedentarylifestyle.
Quality of the diet alone did not predictcessation outcome, but alcohol use alonewas a significant predictor. Those whoconsumed more than seven drinks perweek were significantly more likely torelapse than those with moderate drinking.The hazard ratio for those who did notconsume alcohol at all was elevated, too,but did not reach statistical significance.Alcohol use seems to be quite unstable as apredictor of smoking cessation. Forexample, a recent cross-sectional study didnot show significant associations betweenalcohol use and smoking cessation [45]. Afurther challenge is the definition ofalcohol consumption as CVD riskbehavior. According to the J-shaped

Cardiovascular Risk Behavior among Sedentary Female Smokers & Smoking Cessation Outcomes 21
relationship of alcohol use and risk ofCVD, non-use of alcohol on one hand, andmore than 7 drinks per week on the otherhand should be regarded as alcohol-relatedrisk behavior for CVD [23]. This J-shapedassociation has been recently challengedamong smokers [2 4 ]. In relation tosmoking cessation, we analyzed alcoholconsumption in three separate categories.Based on our results, the definition ofcessation related risk behavior includedhigh alcohol consumption only. Thus,similar J-shaped association as suggestedfor CVD risk could not be replicated inrelation to smoking cessation.
We used nicotine dependence, lengthof the longest past quit attempt, depressivesymptoms, self-efficacy, and education asbaseline predictors to be analyzed inaddition to health risk behaviors. One issueis whether there is evidence of thosefactors predicting abstinence. Recentstudies indicate that including nicotinedependence, length of the longest past quitattempt, depression and education wererelevant to analyses of cessation [46, 47].However, another recent study suggeststhat the effect of education disappearswhen adjusting for other variables, such asother health behaviors and socialenvironment [45]. Among female smokersin our trial, any of these variables as suchhad neither unadjusted nor adjusted effecton abstinence. However, after controllingfor all other baseline variables therelationship between accumulation of riskbehavior and cessation outcome wasslightly attenuated, yet remainingsignificant (p=0.032). Thus, it seems thatcontrolling for those variables wasrelevant.
Although dietary behavior alone wasnot related to smoking cessation outcomewe found a significant interaction betweendiet and depression. Women (n=17) whohad high depression scores and high-fatdiet had significantly highest risk forrelapse. One could ask whether theseparticipants’ weight or weight concerns hassomething to do with this result. Thebaseline average body mass index (BMI)
was only marginally higher among thehigh-fat group (mean=27.4 vs. 26.2 inmixed and 25.7 in vegetable diet;p=0.380). In subgroups by depression anddiet interaction there was no significantdifference. However, the weight concernswere highest in the high-fat diet group withhigh depression score (weight concernmean score=14.1, SD=5.7) in comparisonto other subgroups such as the high-fatgroup with low depression score (mean=11.0, SD=5.8), the depressed (mean=12.3, SD=5.3) and the non-depressed withmixed or vegetable diet (mean=10.3,SD=5.7). These differences were almostsignificant (p=0.070). We also carried outa further interaction model adjusted forweight concerns at baseline, but this didnot radically change the results shown intable 6. It looks like weight concerns maybe an issue to be analyzed in largersamples in relation to dietary behavior anddepression.
Interaction between a health riskbehavior and depressive symptoms inassociation with smoking cessation hasbeen reported earlier among smokers inoutpatient alcoholic treatment [48]. In thisparticular study, the interaction suggestedthat greater number of days since last drinkwas associated with greater readiness toquit, being significant only among patientswith low depression scores. In the presentstudy, alcohol use had a direct effect only,but no significant interaction withdepression.
Interestingly, the depressed womenwho did not use high-fat diet wererelatively successful in this study.According to the pair-wise comparisons,these women were not significantlydifferent from any of the non-depressedwomen. The only significantly lesssuccessful group was the depressed womenwith high-fat diet. Partly this may be asurprising result, as usually depressivesymptoms at baseline predict low successin smoking cessation. It is possible that therelatively low weight concerns of thesedepressed women - with a healthier diet -have contributed to this result. This notion,

22 Korhonen MT, Kinnunen T, Quiles Z, Leeman RF, Terwal DM, Garvey AJ
however, needs to be investigated in alarger sample. One explanation may be thatin our trial all subjects received NRT. In anearlier study NRT was particularlybeneficial for depressed quitters [42]. Itlooks like NRT could assist depressedsmokers to reduce the gap to the non-depressed ones measured at baseline. Thisresult could not be explained by highernicotine dependence because aftercontrolling for FTND the results remainedthe same.
Every woman in our study already hadat least 2 main CVD risk factors, i.e.smoking [49] and a sedentary lifestyle[50]. In addition, some 40% (n=65) had 1 -2 additional risk factors, i.e. unfavorablediet and/or alcohol use [22, 23]. Further,30% had at baseline high level ofdepressive symptoms, which is also a riskfactor for development of CVD [51] .Hence, our results raise a further questionwhether multiple risk behaviorinterventions should be combined toreduce the total burden of their CVD riskfactors. It has been suggested that changein one risk behavior may relate to changein another. For example, the cognitivemechanisms associated with changes insmoking behavior are related to thecognitive variables which have been shownto predict changes in other behaviors [52].The readiness to change multiple riskbehaviors was studied among nicotine andalcohol dependent outpatients [53 ] .Patients reported higher confidence toabstain from alcohol than from cigarettes.Those with high motivation for changingalcohol use and low motivation to quitsmoking remained longer in the program,whereas those with high motivation forchanging both behaviors dropped out early.It seems that, in spite of readiness tochange dual-dependency behaviors, actualquitting both simultaneously may provedifficult. Smoking cessation in dual-dependence programs may be lesssuccessful than in interventions targetingsmoking only. However, in terms of totalcardiovascular risk profile, some combinedinterventions may produce higher public
health impact. For example, smokingcessation together with exercise or dietaryintervention may have significantcombined effects, although the absolutequit rates would not be highest.
Regarding limitations of the study, oursample was relatively small and selected.Our participants represent smoking womenwho are willing to quit smoking and whohave sedentary lifestyle. Thus, our resultsare suggestive and further studies withlarger samples are needed to confirm thesignificance of multiple CVD riskbehaviors and their interactions with othersmoking related variables. Further,although the participants had a sedentarylifestyle at baseline, this may not be truefor all of them once they commenced thestudy. Specifically, the exerciseintervention, if optimally followed, wouldmake these participants more active duringtheir quit process. Of the three groups inthe study both exercise and wellness hadsimilar one year abstinence rates.However, the mechanisms by which thiswas achieved are not clear. In regard toadopting exercise into their sedentarylifestyles we analyzed the self-reportedfrequency of exercise behavior at thebaseline and at the end of treatment at 16weeks after quitting. Based on the dataavailable at 16 weeks, the three risk groupsdid not differ in changes from the baselinein exercise behavior (F=. 608 (2) p=0.549), and hence suggest that increasedexercise does not explain the observeddifferences. It has to be noted though thatdata on 16 week exercise status was onlyavailable for 4 participants in the riskgroup of 2 risk behaviors. Further, therelapse to smoking and subsequent dropout was rapid, and thus, there was aminimal time for major changes in healthbehaviors to occur. Finally, as anadditional limitation of the study, we haveto note that both added risk behaviors weremeasured by self-reports. It is possible thatthere has been some under-reporting ofalcohol use and recall bias associated withone-week retrospective dietary reportsversus food diaries. Thus, this possible bias
Cardiovascular Risk Behavior among Sedentary Female Smokers & Smoking Cessation Outcomes 23
may have caused slight dilution of thesebehaviors’ effects on the results.
Acknowledgments: This research wassupported by the Grant DA12503 from theNational Institute on Drug Abuse (NIDA).The work of the corresponding author hasbeen supported by the Grants from theAcademy of Finland (200075, 103650) andfrom the Finnish Foundation forCardiovascular Research. The authorswould like to thank Dr. L. Howard Hartley,M.D. from the Brigham and Women’sHospital, Boston, for his valuablecontribution in the testing procedures ofthe study participants.
REFERENCES
1. U.S. Department of Health andHuman Services. Women andsmoking: A report of the SurgeonGeneral. Washington (DC): U.S.Gov. Printing Office, 2001.
2. Benowitz NL. Cigarette smokingand cardiovascular disease:Pathophysiology and implicationsfor treatment. Prog Cardiovasc Dis2003; 46:91-111.
3. Irvin JE, Brandon TH. Theincreasing recalcitrance of smokersin clinical trials. Nicotine Tob Res2000;2:79-84.
4. Irvin JE, Hendricks PS, BrandonTH. The increasing recalcitrance ofsmokers in clinical trials II:Pharmacotherapy trials. NicotineTob Res 2003;5:27-35.
5. Fagerstrom KO, Kunze M,Schoberberger R et al. Nicotinedependence versus smokingprevalence: comparisons amongcountries and categories ofsmokers. Tob Control 1996;5:52-56.
6. Schumann A, Hapke U, Rumpf HJ,Meyer C, John U. The associationbetween degree of nicotinedependence and other healthbehaviours. Findings from a
German general population study.Eur J Public Health 2001;11:450-2.
7. Haukkala A, Uutela A, VartiainenE, McAlister A, Knekt P.Depression and smoking cessation:the role of motivation and self-efficacy. Addict Behav 2000;25:311-316.
8. Laaksonen M, Prättälä R, KaristoA. Patterns of unhealthy behaviourin Finland. Eur J Public Health2001;11:294-300.
9. Murphy JM, Horton NJ, MonsonRR, Laird NM, Sobol AM,Leighton AH. Cigarette smoking inrelation to depression: Historicaltrends from the Stirling CountyStudy. Am J Psychiatry2003:160:1663-1669.
10. Emmons KM, Wechsler H,Dowdall G, Abraham M. Predictorsof smoking among US collegestudents. Am J Public Health1998;88:104-107.
11. Schorling JB, Gutgesell M, Klas P,Smith D, Keller A. Tobacco,alcohol and other drug use amongcollege students. J Subst Abuse1994;6:105-115.
12. Chetwynd J, Some characteristicsof women smokers. N Z Med J1986;99:14-17.
13. Krejci J, Steinberg ML, ZiedonisD. Smoking status and substanceabuse severity in a residentialtreatment sample. Drug AlcoholDepend 2003;72:249-254.
14. Laaksonen M, Luoto R, HelakorpiS, Uutela A. Associations betweenhealth-related behaviors: A 7-yearfollow-up of adults. Prev Med2002;34:162-170.
15. Johnson NA, Boyle CA, Heller RF.Leisure-time physical activity andother health behaviours: Are theyrelated? Aust J Public Health1995;19:69-75.
16. Prättälä R., Karisto A, Berg MA.Consistency and variation inunhealthy behavior among Finnish

24 Korhonen MT, Kinnunen T, Quiles Z, Leeman RF, Terwal DM, Garvey AJ
men, 1982-1990. Soc Sci Med1994;39:115-122.
17. Escobedo LG, Reddy M, DuRantRH. Relationship between cigarettesmoking and health risk andproblem behaviors among USadolescents. Arch Pediatr AdolescMed 1997;151:66-71.
18. Coogan PF, Adams M, Geller ACet al. Factors associated withsmoking among children andadolescents in Connecticut. Am JPrev Med 1998;15:17-24.
19. Boyle RG, O’Connor P, Pronk N,Tan A. Health behaviors ofsmokers, ex-smokers, and neversmokers in an HMO. Prev Med2000;31:177-182.
20. Haukkala A, Laaksonen M, UutelaA. Smokers who do not want toquit--is consonant smoking relatedto lifestyle and socioeconomicfactors? Scand J Public Health2001;29:226-232.
21. WHO. Diet, nutrition and theprevention of chronic diseases.Report of a joint WHO/FAO expertconsultation. WHO TechnicalReport Series 916. Geneva: WorldHealth Organization, 2003.
22. Centers for Disease Control andPrevention. Behavioral Risk FactorSurveillance System. 2000 BRFSSSummary Prevalence Report.Washington (DC): CDC, 2001.
23. Stampfer MJ, Colditz GA, WillettWC, Speizer FE, Hennekens CH. Aprospective study of moderatealcohol consumption and the risk ofcoronary disease and stroke inwomen. N Engl J Med1988;319:267-273.
24. Ebbert JO, Janney CA, Sellers TA,Folsom AR, Cerhan JR. Theassociation of alcohol consumptionwith coronary heart diseasemortality and cancer incidencevaries by smoking history. J GenIntern Med 2005;20(1):14-20.
25. Pearson TA, Blair SN, Daniels SRet al. AHA guidelines for primary
prevention of cardiovasculardisease and stroke: 2002 update.Circulation 2002;106:388-391.
26. Houterman S, Verschuren WMM,Kromhout D, Smoking, bloodpressure and serum cholesterol-effects on 20-year mortality.Epidemiology 2003;14:24-29.
27. Emmons KM, Marcus BH, LinnanL, Rossi JS, Abrams DB.Mechanisms in multiple risk factorinterventions: Smoking, physicalactivity, and dietary fat intakeamong manufacturing workers.Prev Med 1994;23:481-489.
28. Sherwood, N.E., et al., Smokerswith multiple behavioral riskfactors: how are they different?Prev Med, 2000. 31(4):299-307.
29. Shiffman S, Shumaker SA, AbramsDB et al. Models of smokingrelapse. Health Psychol 1986;5:13-27.
30. Burns DM. Epidemiology ofsmoking-induced cardiovasculardisease. Prog Cardiovasc Dis2003;46:11-29.
31. U.S.Department of Health andHuman Services. The effects ofphysical activity on health anddisease. The Surgeon General'sreport on physical activity andhealth. Washington (DC): U.S.Gov.Printing Office, 1996.
32. Droomers M, Schrijvers CT,Mackenbach JP, Why do lowereducated people continue smoking?Explanations from the longitudinalGLOBE study. Health Psychol2002;21:263-272.
33. Fagerstrom KO, Schneider NG.Measuring nicotine dependence: Areview of the Fagerstrom ToleranceQuestionnaire. J Behav Med1989;12:159-182.
34. Borrelli B, Bock B, King T, PintoB, Marcus BH. The impact ofdepression on smoking cessation inwomen. Am J Prev Med1996;12:378-384.
Cardiovascular Risk Behavior among Sedentary Female Smokers & Smoking Cessation Outcomes 25
35. Farkas A.J, Pierce JP, Zhu SH et al.Addiction versus stages of changemodels in predicting smokingcessation. Addiction 1996;91:1271-1280.
36. Ockene J, Emmons K, MermelsteinRJ et al. Relapse and maintenanceissues for smoking cessation.Health Psychology 2000;19:17-31.
37. Niaura R., Shadel WG. Assessmentto inform smoking cessationtreatment. In: The TobaccoDependence Treatment Handbook:A Guide to Best Practices. AbramsDB et al., Editors. 2003, TheGuildford Press: New York, NY. p.27-72.
38. Heatherton TF, Kozlowski LT,Frecker RC, Fagerstrom KO. TheFagerström Test for NicotineDependence: A revision of theF a g e r s t r ö m T o l e r a n c eQuestionnaire. Br J Addict1991;86:1119-1127.
39. Radloff LS. The CES-D scale: Aself-report depression scale forresearch in the general population.A p p l i e d P s y c h o l o g i c a lMeasurement 1977;1:385-401.
40. Ossip-Klein D, Bigelow G, ParkerSR, Curry S, Hall S, Kirkland S.Classification and assessment ofsmoking behavior . HealthPsychology 1986;5:3-11.
41. Glantz AS, Slinker BK. Primer ofapplied regression and analysis ofvariance. 1990, New York:McGraw-Hill.
42. Kinnunen T, Doherty K, MilitelloFS, Garvey AJ. Depression andS m o k i n g C e s s a t i o n :Characteristics of DepressedSmokers and Effects of NicotineReplacement. J Consult ClinPsychol 1996; 64:791-798.
43. Cargill BR, Emmons KM, KahlerCW, Brown RA. Relationshipamong alcohol use, depression,smoking behavior, and motivationto quit smoking with hospitalized
smokers. Psychol Addict Behav2001;15:272-275.
44. John U, Meyer C, Rumpf HJ,Schumann A, Thyrian JR, HapkeU. Strength of the relationshipbetween tobacco smoking, nicotinedependence and the severity ofalcohol dependence syndromecriteria in a population-basedsample. A l c o h o l A l c o h o l2003;38:606-612.
45. Siahpush M, Borland R, Scollo M.Factors associated with smokingcessation in a national sample ofAustralians. Nicotine Tob Res2003;5:597-602.
46. Garvey AJ, Kinnunen T,Nordstrom BL et al. Effects ofnicotine gum dose by level ofnicotine dependence. Nicotine TobRes 2000;2:53-63.
47. Ferguson JA, Patten CA, SchroederDR, Offord KP, Eberman KM,Hurt RD. Predictors of 6-monthtobacco abstinence among 1224cigarette smokers treated fornicotine dependence. Addict Behav2003;28:1203-1218.
48. Hitsman B, Abrams DB, ShadelWG et al. Depressive symptomsand readiness to quit smokingamong cigarette smokers inoutpatient alcohol treatment.Psychol Addict Behav 2002;16:264-268.
49. Schmitz JM. Smoking cessation inwomen with cardiac risk. Am J MedSci 2003; 326:192-196.
50. Schnohr P, Jensen JS, Scharling H,Nordestgaard BG. Coronary heartdisease risk factors ranked byimportance for the individual andcommunity: A 21 year follow-up of12 000 men and women from TheCopenhagen City Heart Study. EurHeart J 2002;23:620-626.
51. Musselman DL, Evans DL,Nemeroff CB. The relationship ofdepression to cardiovasculardisease: epidemiology, biology, and

26 Korhonen MT, Kinnunen T, Quiles Z, Leeman RF, Terwal DM, Garvey AJ
treatment. Arch Gen Psychiatry1998;55:580-592.
52. King TK, Marcus BH, Pinto BM,Emmons KM, Abrams DB.Cognitive-behavioral mediators ofchanging multiple behaviors:Smoking and a sedentary lifestyle.Prev Med 1996;25:684-691.
53. Stotts AL, Schmitz JM, GrabowskiJ. Concurrent treatment for alcoholand tobacco dependence: Arepatients ready to quit both? DrugAlcohol Depend 2003; 69:1-7.





![[Contributions of auriculotherapy in smoking cessation: a pilot study]](https://static.fdokumen.com/doc/165x107/63334633b94d623842021dc0/contributions-of-auriculotherapy-in-smoking-cessation-a-pilot-study.jpg)