
Shape from sound: Evidence for a shape operator in the lateral occipital cortex
Upload
independentCategory
view
0download
0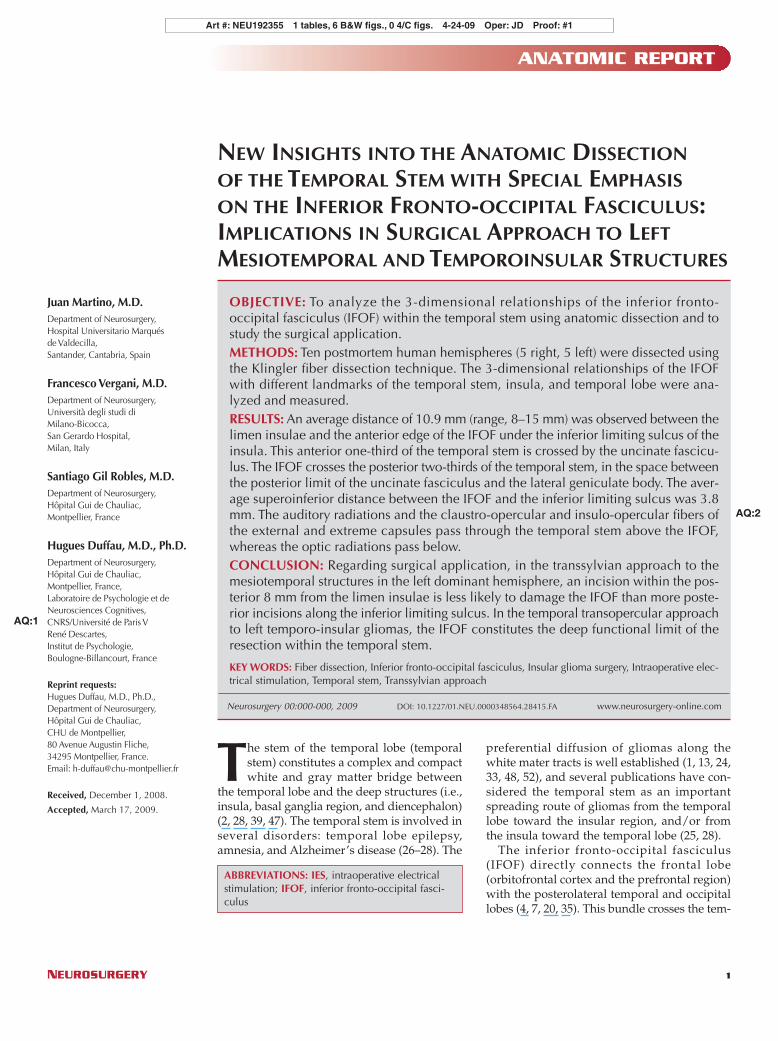
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 | 1
ANATOMIC REPORT
Juan Martino, M.D.Department of Neurosurgery,Hospital Universitario Marquésde Valdecilla,Santander, Cantabria, Spain
Francesco Vergani, M.D.Department of Neurosurgery,Università degli studi diMilano-Bicocca,San Gerardo Hospital,Milan, Italy
Santiago Gil Robles, M.D.Department of Neurosurgery,Hôpital Gui de Chauliac,Montpellier, France
Hugues Duffau, M.D., Ph.D.Department of Neurosurgery,Hôpital Gui de Chauliac,Montpellier, France,Laboratoire de Psychologie et deNeurosciences Cognitives,CNRS/Université de Paris VRené Descartes,Institut de Psychologie,Boulogne-Billancourt, France
Reprint requests:Hugues Duffau, M.D., Ph.D.,Department of Neurosurgery,Hôpital Gui de Chauliac,CHU de Montpellier,80 Avenue Augustin Fliche,34295 Montpellier, France.Email: [email protected]
Received, December 1, 2008.
Accepted, March 17, 2009.
The stem of the temporal lobe (temporalstem) constitutes a complex and compactwhite and gray matter bridge between
the temporal lobe and the deep structures (i.e.,insula, basal ganglia region, and diencephalon)(2, 28, 39, 47). The temporal stem is involved inseveral disorders: temporal lobe epilepsy,amnesia, and Alzheimer’s disease (26–28). The
preferential diffusion of gliomas along thewhite mater tracts is well established (1, 13, 24,33, 48, 52), and several publications have con-sidered the temporal stem as an importantspreading route of gliomas from the temporallobe toward the insular region, and/or fromthe insula toward the temporal lobe (25, 28).
The inferior fronto-occipital fasciculus(IFOF) directly connects the frontal lobe(orbitofrontal cortex and the prefrontal region)with the posterolateral temporal and occipitallobes (4, 7, 20, 35). This bundle crosses the tem-
Art #: NEU192355 1 tables, 6 B&W figs., 0 4/C figs. 4-24-09 Oper: JD Proof: #1
ABBREVIATIONS: IES, intraoperative electricalstimulation; IFOF, inferior fronto-occipital fasci-culus
NEW INSIGHTS INTO THE ANATOMIC DISSECTIONOF THE TEMPORAL STEM WITH SPECIAL EMPHASISON THE INFERIOR FRONTO-OCCIPITAL FASCICULUS:IMPLICATIONS IN SURGICAL APPROACH TO LEFTMESIOTEMPORAL AND TEMPOROINSULAR STRUCTURES
OBJECTIVE: To analyze the 3-dimensional relationships of the inferior fronto-occipital fasciculus (IFOF) within the temporal stem using anatomic dissection and tostudy the surgical application.METHODS: Ten postmortem human hemispheres (5 right, 5 left) were dissected usingthe Klingler fiber dissection technique. The 3-dimensional relationships of the IFOFwith different landmarks of the temporal stem, insula, and temporal lobe were ana-lyzed and measured.RESULTS: An average distance of 10.9 mm (range, 8–15 mm) was observed between thelimen insulae and the anterior edge of the IFOF under the inferior limiting sulcus of theinsula. This anterior one-third of the temporal stem is crossed by the uncinate fascicu-lus. The IFOF crosses the posterior two-thirds of the temporal stem, in the space betweenthe posterior limit of the uncinate fasciculus and the lateral geniculate body. The aver-age superoinferior distance between the IFOF and the inferior limiting sulcus was 3.8mm. The auditory radiations and the claustro-opercular and insulo-opercular fibers ofthe external and extreme capsules pass through the temporal stem above the IFOF,whereas the optic radiations pass below.CONCLUSION: Regarding surgical application, in the transsylvian approach to themesiotemporal structures in the left dominant hemisphere, an incision within the pos-terior 8 mm from the limen insulae is less likely to damage the IFOF than more poste-rior incisions along the inferior limiting sulcus. In the temporal transopercular approachto left temporo-insular gliomas, the IFOF constitutes the deep functional limit of theresection within the temporal stem.
KEY WORDS: Fiber dissection, Inferior fronto-occipital fasciculus, Insular glioma surgery, Intraoperative elec-trical stimulation, Temporal stem, Transsylvian approach
Neurosurgery 00:000-000, 2009 DOI: 10.1227/01.NEU.0000348564.28415.FA www.neurosurgery- online.com
AQ:2
AQ:1

2 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 www.neurosurgery-online.com
MARTINO ET AL.
Art #: NEU192355 1 tables, 6 B&W figs., 0 4/C figs. 4-24-09 Oper: JD Proof: #1
poral stem to pass from the ventral insular region to the tempo-ral lobe. Lesions to the temporal stem have been associatedwith amnesia, learning disorders, visual processing disorders,and aphasia, and it has recently been suggested that the IFOFmight be an unrecognized component of the temporal steminvolvement in some of these abnormalities (28). Our grouphad previously suggested that the IFOF is an important subcor-tical component of the semantic system, because intraoperativeelectrical stimulation (IES) of this fascicle has induced seman-tic paraphasias with high reproducibility (11, 12). Despite theimportant role of this fascicle in language function and the riskof inducing severe neurological disorders if damaged in thetemporal stem of the dominant hemisphere, the 3-dimensionalrelationships of this fascicle within the temporal stem remainpoorly described, and recent publications have yielded con-flicting results (28, 39, 47).
Fiber dissection technique, first described by Klingler (29),Klingler and Gloor (30), and Ludwing and Klingler (32), uti-lizes a frozen stage during brain fixation. This process spreadsthe white matter fibers, permitting the dissection of the tractsand isolation of the individual fiber bundles. This techniqueprovides a unique opportunity to study the IFOF anatomy atthe level of the temporal stem, because it enables complete dis-section and isolation of this fascicle from the remainder of thecomponents of the temporal stem. In this anatomic study, thetemporal stem of 10 human hemispheres was dissected usingthe Klingler technique with the main objective of analyzing the3-dimensional relationships between the IFOF and the remain-der of the components of the temporal stem. The surgical impli-cations of this anatomic analysis in 2 established neurosurgicalapproaches that cross the temporal stem in the dominant hemi-sphere (i.e., the transsylvian approach to the mesial temporalstructures, and the temporal transopercular approach to thetemporo-insular gliomas) are discussed.
MATERIALS AND METHODSTen human cerebral hemispheres (5 right side and 5 left side),
obtained from fresh autopsy specimens of adults, were fixed in 10%formalin solution for at least 40 days. The pia mater, arachnoid mem-brane, and vascular structures were carefully removed, and the hemi-spheres were frozen at �15�C for 15 days. The water crystallizationinduced by the freezing process disrupts the structure of the gray mat-ter (with high water content), which enables the cortex to be peeled offof the brain surface. The freezing process also spreads along the whitematter fibers, facilitating the dissection of the fiber tracts. The speci-mens were washed under running water for several hours before per-forming the dissection.
Before the dissection began, a detailed study of the superficialanatomy of the sulci and gyri was made. The specimens were dis-sected in a stepwise manner, from the lateral surface to the medial sur-face, according to the fiber dissection technique described by Klingler(29), Klingler and Gloor (30), Ludwing and Klingler (32), and Türeet al. (45). The dissections were performed under loop magnification(�3.2). Wooden spatulas were used in the initial steps of the dissectionto peel away the brain cortex and the U-shaped fibers (also known asintergyral or arcuate fibers), which are short association fibers thatinterconnect the adjacent gyri. Once the fibers of the IFOF were iden-
F1
F2
tified, the remaining dissection was performed using curving metallicdissectors with various tip sizes. At the level of the temporal stem, thedistances between the IFOF and different landmarks of the temporallobe, temporal stem, and insula were measured. Numerous digital pho-tographs were taken during the dissection.
RESULTS
Initial Dissection until the Identification of the IFOFBefore the dissection began, a detailed analysis of the surface
anatomy of each hemisphere was performed, and any variabil-ity in the gyral and sulcal pattern was registered. The cortex ofthe frontal operculum was removed using wooden spatulas,exposing the U-shaped fibers (Fig. 1, A and B). Once the cortexof the frontal operculum is removed, it can be easily lifted, per-mitting exposure of the insular cortex (Fig. 1C). The surfaceanatomy of the insula, which has a triangular shape, was stud-ied. The insular apex, the most prominent laterally projectingarea of the insular convexity, is directed anteriorly and inferi-orly toward the limen insulae. The central sulcus of the insulaseparates the anterior short gyri and posterior long gyri. Theanterior, superior, and inferior limiting sulci of the insula sep-arate the insular cortex from the fronto-orbital, frontoparietal,and temporal opercula, respectively. The anteroinferior portionof the insular cortex was removed, exposing the extreme cap-sule (Fig. 2A). At the anteroinferior portion of the extreme andexternal capsules, the uncinate fasciculus and the IFOF wereexposed (Fig. 2B). In this region, both fasciculi narrow in sec-tion and the IFOF is located dorsal and posterior to the unci-nate fasciculus (Fig. 2C). The anterior cortex of the limen insu-lae and the posterosuperior insular cortex were preserved, sothat the relationships between the IFOF and these structurescould be analyzed.
FIGURE 1. Photographs of cadav-eric specimens demonstrating step-wise fiber dissection of the lateralsurface of a left hemisphere. A, lat-eral surface of the hemisphere, afterthe pia mater and arachnoid mem-branes have been removed. B, thecortex of the frontal operculum hasbeen removed, exposing the U-shaped fibers, also known as intergyral or arcuate fibers, which are shortassociation fibers that interconnect the adjacent gyri. C, the frontoparietaland temporal operculum are lifted, exposing the insular cortex. A, ante-rior; P, posterior; S, superior; I, inferior.
A B
C

Dissection and Isolation of the IFOF at the Temporal StemDuring this second stage, the fibers of the IFOF were dis-
sected and isolated from the surrounding fiber tracts. Becausethe structure of the IFOF is very delicate, a thin and blunt metaldissector was used for this stage of the dissection. Care wastaken to avoid transecting axons, by teasing with the metallicdissector, rather than cutting, thus minimizing the risk of spu-rious tracts.
The removal of the U-shaped fibers of the extreme capsuleconnecting the insular cortex and claustrum with the frontaloperculum exposed the anterior termination of the IFOF anduncinate fasciculus at the frontal operculum. At the anteroinfe-rior portion of the extreme and external capsules, the IFOF andthe uncinate fasciculus run parallel with a posterior and inferiororientation. Then, both fascicles cross the temporal stem. At thislevel, both fascicles are flattened. The uncinate fasciculus crossesthe anterior one-third of the temporal stem, passing throughthe region of the limen insulae and a few millimeters of theinferior limiting sulcus of the insula (Figs. 2C and 6). The IFOFcrosses the posterior two-thirds of the temporal stem, in theregion between the posterior limit of the uncinate fasciculusand the lateral geniculate body (Figs. 2C, 4, and 5). At the lateralportion of the temporal stem, the fibers of the uncinate fascicu-
lus curve in an anterior direction to reach the anterior temporallobe, whereas the fibers of the IFOF turn in a posterior directioncoursing above the roof of the temporal horn, superior andmedial to the optic radiations (Figs. 2C, 4, and 5). On the basisof the different orientation of both fascicles within the temporalstem, they could be clearly differentiated and separated.
Once the superficial surface of the IFOF was completelyexposed, the deep surface of the bundle was carefully sepa-rated from the deeper structures. This deep dissection started atthe anteroinferior portion of the extreme and external capsules,because it is easier to separate the IFOF from the deeper struc-tures at this level. Further dissection in a posterior directionpermitted complete isolation of the fibers of the IFOF from theremainder of the components of the temporal stem (Figs. 3–5).It was evidenced that the auditory radiations, the claustro-opercular and insulo-opercular fibers of the external andextreme capsules pass through the temporal stem above theIFOF, whereas the optic radiations pass below (Figs. 3–5). Theuncinate fasciculus crosses the anterior portion of the temporalstem in the same plane as the IFOF. The anterior commissureand the inferior thalamic peduncle cross the temporal stembelow the uncinate fasciculus.
The dissection revealed that the most dorsal and posteriorfibers of the IFOF do not cross the temporal stem, but ratherrun below the insula, directly reaching the sagittal stratum atthe lateral surface of the atrium of the lateral ventricle (Fig. 5).
Distances Measured in the Temporal StemThe following distances were measured within the temporal
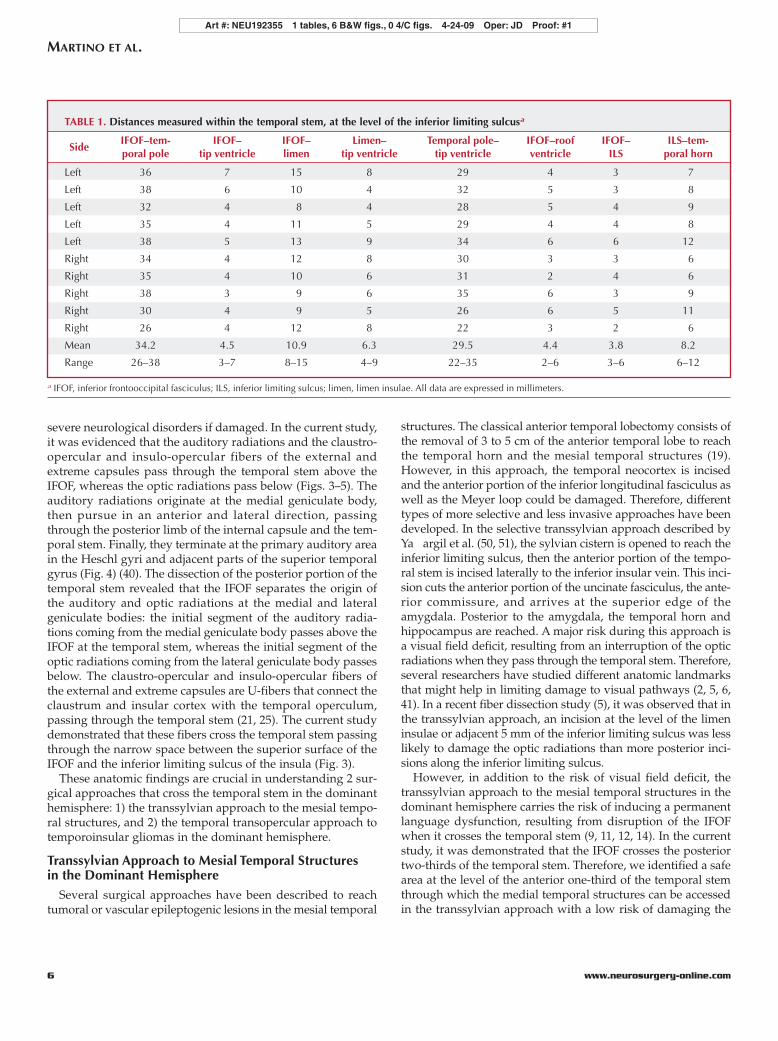
stem, at the level of the inferior limiting sulcus of the insula(Fig. 6; Table 1): the anteroposterior distance between the tem-poral pole and the anterior edge of the IFOF (average, 34.2mm; range, 26–38 mm), the anteroposterior distance betweenthe limen insulae and the anterior edge of the IFOF (average,10.9 mm; range, 8–15 mm), the anteroposterior distancebetween the anterior tip of the temporal horn and the anterioredge of the IFOF (average, 4.5 mm; range, 3–7 mm), the antero-posterior distance between the limen insulae and the anteriortip of the temporal horn (average, 6.3 mm; range, 4–9 mm), theanteroposterior distance between the temporal pole and theanterior tip of the temporal horn (average, 29.5; range, 22–35mm), the superoinferior distance between the inferior surfaceof the IFOF and the roof of the temporal horn (average, 4.4mm; range, 2–6 mm), the superoinferior distance between thesuperior surface of the IFOF and the inferior limiting sulcus(average, 3.8 mm; range, 3–6 mm), and the superoinferior dis-tance between the inferior limiting sulcus and the roof of thetemporal horn (average, 8.2 mm; range, 6–12 mm). This dis-tance approximates the thickness of the temporal stem.
DISCUSSION
Anatomic ConsiderationsThe temporal stem constitutes a white and gray matter bridge
between the temporal lobe and insula, basal ganglia region, and
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 | 3
INFERIOR FRONTO-OCCIPITAL FASCICULUS AND TEMPORAL STEM
Art #: NEU192355 1 tables, 6 B&W figs., 0 4/C figs. 4-24-09 Oper: JD Proof: #1
FIGURE 2. Photographs showingthe stepwise dissection of the insu-lar region and temporal stem of aleft hemisphere, exposing the infe-rior fronto-occipital fasciculus(IFOF) and uncinate fasciculus. A,the anteroinferior portion of theinsular cortex has been removed,exposing the anteroinferior portionof the extreme capsule. B, enlarged view. The uncinate fasciculus and theIFOF are exposed (arrow) at the anteroinferior portion of the extreme andexternal capsules. C, dissection of the IFOF (solid arrow) and uncinate fas-ciculus (dotted arrow) at the anteroinferior portion of the extreme andexternal capsules, and at the temporal stem. The posterosuperior portion ofthe insula, claustrum, and extreme and external capsules have been lifted,exposing the insular portion of the IFOF. Small pieces of blue paper wereplaced between the IFOF and the deeper structures to demonstrate that thefibers of the fascicle were completely dissected and isolated from the sur-rounding fiber tracts. At the anteroinferior portion of the extreme andexternal capsules, both fasciculi narrow in section, and the IFOF is locateddorsal and posterior to the uncinate fasciculus. At the temporal stem, bothfascicles are flattened, and the uncinate fasciculus passes through the ante-rior one-third and the IFOF through the posterior two-thirds of the tempo-ral stem. A, anterior; P, posterior; S, superior; I, inferior.
A B
C
F3-5
AQ:3
F6T1

diencephalon (2, 39, 47). The anterior limit of the temporal stemis the amygdala and the posterior limit is the lateral geniculate
body (15, 16, 28, 44). From a view at the inferior limiting sulcus,the following anatomic landmarks identify the anterior and pos-terior limits of the temporal stem: the anterior limit correspondsto the limen insulae, and the posterior limit is the most anteriorpoint where the Heschl gyri intersect the inferior limiting sulcus(this anatomic region corresponds to the lateral geniculate body)(Fig. 4) (47). The temporal stem is limited superiorly by the infe-rior limiting sulcus, and inferiorly by the roof of the temporalhorn of the lateral ventricle (2, 17, 28, 47). The following whitematter tracts compose the temporal stem: claustro-opercularand insulo-opercular fibers of the external and extreme cap-sules, auditory radiations, IFOF, uncinate fasciculus, optic radi-ations, anterior commissure, and inferior thalamic peduncle (17,28, 39, 44, 47). The amygdala is not currently considered as partof the temporal stem. However, several dissection studies haveevidenced that the upper portion of the amygdala blends intothe claustrum and globus pallidus without any clear demarca-tion (2, 40). Therefore, in our opinion, the amygdala can beviewed as a gray matter bridge that passes from the uncalregion to the basal ganglia region, and consequently may beconsidered as part of the temporal stem.
4 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 www.neurosurgery-online.com
MARTINO ET AL.
Art #: NEU192355 1 tables, 6 B&W figs., 0 4/C figs. 4-24-09 Oper: JD Proof: #1
FIGURE 3. IFOF dissection at the insula and temporalstem of a left hemisphere. A coronal cut of the temporallobe 8 mm posterior to the limen insulae has been per-formed; the temporal horn is opened (arrowhead). At theinsula and temporal stem, the IFOF (small straightarrow) has been completely dissected and separatedfrom the superficial and deeper structures. Small piecesof blue paper were placed between the IFOF and thedeeper structures to demonstrate that the fibers of thefascicle were completely dissected and isolated from thesurrounding fiber tracts. The temporal operculum, thedorsal portion of the insula, claustrum, and extremeand external capsules have been separated from theIFOF and lifted superiorly. The claustro-opercular andinsulo-opercular fibers of the extreme and external cap-sules (superior straight dotted arrow) are U-fibers thatconnect the claustrum and insular cortex with the tem-poral operculum. These fibers cross the temporal stempassing through the narrow space between the superiorsurface of the IFOF and the inferior limiting sulcus ofthe insula. In the temporal transopercular approach totemporo-insular gliomas in the dominant hemisphere,the IFOF constitutes the deep functional limit of theresection within the temporal stem. Consequently, thissurgical route to the insular region passes through thespace between the superior surface of the IFOF and theinfer ior l imit ing sulcus (b ig curved arrow).Preservation at the temporal stem of the deep functionalboundary of the IFOF will also avoid damaging theoptic radiations, because they cross the temporal stembelow the IFOF (inferior straight dotted arrow). L, lat-eral; M, medial; S, superior; I, inferior.
FIGURE 4. IFOF dissection at the insula, temporalstem, and temporal lobe of a left hemisphere. A coronalcut of the temporal lobe 8 mm posterior to the limeninsulae has been performed, and the uncinate fasciculushave been removed. The temporal operculum anterior toHeschl gyri has been removed. The Heschl gyri (largedotted arrow) pursue in a posterior and medial directionfrom the temporal operculum to the posterior insula; themost anterior point where the Heschl gyri intersect theinferior limiting sulcus corresponds to the posteriorlimit of the temporal stem (small dotted arrow). Thedorsal portion of the insula, claustrum, and extremeand external capsules (arrowhead) have been liftedsuperiorly, exposing the insular and temporal portionsof the IFOF (arrow). Small pieces of blue paper wereplaced between the IFOF and the deeper structures todemonstrate that the fibers of the fascicle were com-pletely dissected and isolated from the surrounding fibertracts. The IFOF crosses the posterior two-thirds of thetemporal stem, superficial and medial to the optic radi-ations. A, anterior; P, posterior; S, superior; I, inferior.
The IFOF is a long white matter bundle that directly connectsthe frontal lobe (orbitofrontal cortex and the prefrontal region)with the posterolateral temporal and occipital lobes (4, 7, 20,35). The functions of this fascicle are poorly understood: itseems to be implicated in reading, attention, visual process-ing, and language (3, 8, 11, 12, 18, 22, 42). We had previouslydemonstrated that IES of the IFOF induced semantic para-phasias (i.e., errors with regard to the meaning of the wordtarget), with a high reproducibility, whatever the portion of thebundle stimulated (frontal, insular, or occipitotemporal) (11,12). On the basis of these observations, we have recently sug-gested that the IFOF might have an important role in the sub-cortical network underlying the semantic system (9, 11, 12).IES mapping identifies cortical and subcortical structures thatare essential for brain function. Consequently, we have alsosuggested that during surgery in the dominant hemisphere,the IFOF should be identified and preserved, in order to avoida permanent postoperative language deficit (9, 11, 12, 14).
Despite the fact that the IFOF is a prominent component ofthe temporal stem and despite its important role in languagefunction, the number of publications analyzing the course ofthis fascicle in the temporal stem are scarce, and they haveyielded conflicting results. Regarding the anteroposterior loca-tion of the IFOF within the temporal stem, some authors haveconsidered that it passes through the anterior portion of thetemporal stem (39), others think it passes through the posteriorportion (28), and still others describe it as crossing the entire
length of the temporal stem (47). In the current study, it wasevidenced that the uncinate fasciculus crosses the anterior one-third of the temporal stem, passing through the region of thelimen insulae and adjacent few millimeters of the inferior lim-iting sulcus. However, the fibers of the IFOF are separated fromthe limen insulae when they cross the temporal stem. An aver-age distance of 10.9 mm was observed between the anterioredge of the IFOF and the limen insulae at the inferior limitingsulcus (Fig. 6). Interestingly, the fibers of the IFOF turn in a pos-terior direction at the lateral portion of the temporal stem.Therefore, they pass through the posterior two-thirds of thetemporal stem (Figs. 4–6).
Lesions of the optic radiations within the temporal stemproduce a disabling visual field deficit. Consequently, the 3-dimensional relationships of the optic radiations in the tempo-ral stem have been extensively studied. Recent publicationshave evidenced that they cover the superior and lateral surfaceof the temporal horn, that the Meyer loop arrives anteriorly tothe tip of the temporal horn, and that they are located inferiorand lateral to the IFOF (28, 38, 39, 41, 43). However, less atten-tion has been given to the spatial relationships of other impor-tant components of the temporal stem that may also induce
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 | 5
INFERIOR FRONTO-OCCIPITAL FASCICULUS AND TEMPORAL STEM
Art #: NEU192355 1 tables, 6 B&W figs., 0 4/C figs. 4-24-09 Oper: JD Proof: #1
FIGURE 5. IFOF dissection at the insula, temporalstem, and temporal lobe of a left hemisphere. A coronalcut of the temporal lobe 8 mm posterior to the limeninsulae has been performed, and the lateral surface of thetemporal horn has been opened (arrowhead). The tempo-ral operculum anterior to the Heschl gyri has beenremoved. The most dorsal and posterior fibers of theIFOF do not cross the temporal stem; they course belowthe insula, directly reaching the sagittal stratum at thelateral surface of the atrium of the lateral ventricle (dot-ted arrow). The ventral and anterior fibers of the IFOFcross the posterior two-thirds of the temporal stem,superficial and medial to the optic radiations (solidarrow). A, anterior; P, posterior; S, superior; I, inferior.
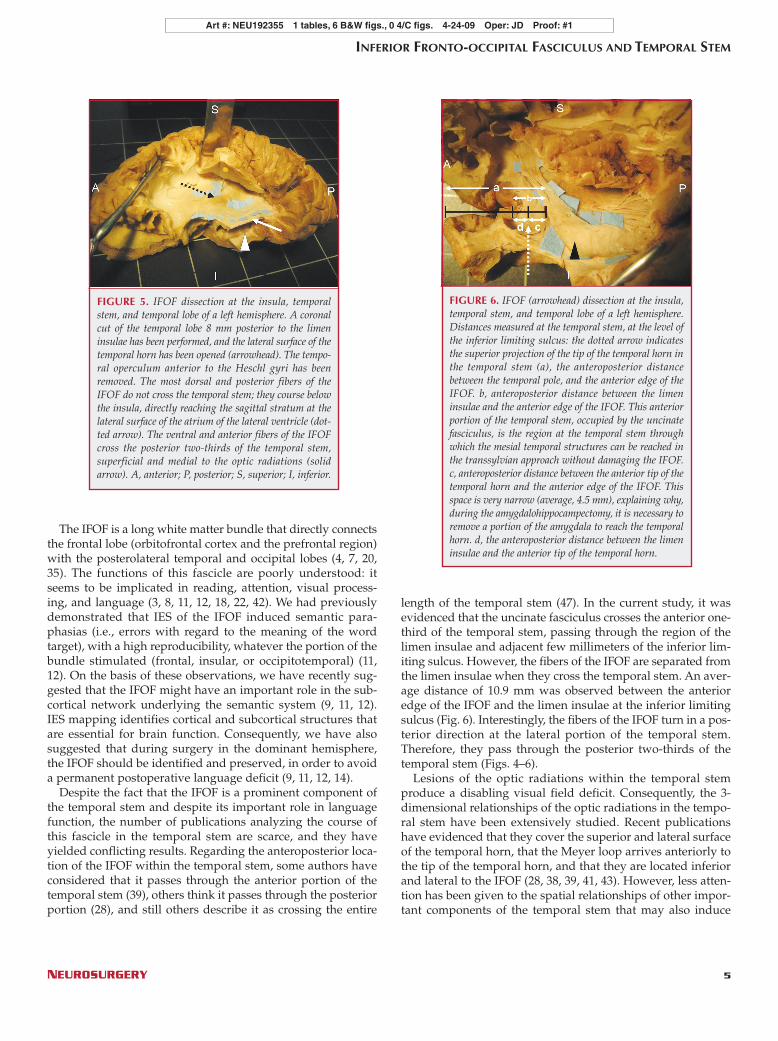
FIGURE 6. IFOF (arrowhead) dissection at the insula,temporal stem, and temporal lobe of a left hemisphere.Distances measured at the temporal stem, at the level ofthe inferior limiting sulcus: the dotted arrow indicatesthe superior projection of the tip of the temporal horn inthe temporal stem (a), the anteroposterior distancebetween the temporal pole, and the anterior edge of theIFOF. b, anteroposterior distance between the limeninsulae and the anterior edge of the IFOF. This anteriorportion of the temporal stem, occupied by the uncinatefasciculus, is the region at the temporal stem throughwhich the mesial temporal structures can be reached inthe transsylvian approach without damaging the IFOF.c, anteroposterior distance between the anterior tip of thetemporal horn and the anterior edge of the IFOF. Thisspace is very narrow (average, 4.5 mm), explaining why,during the amygdalohippocampectomy, it is necessary toremove a portion of the amygdala to reach the temporalhorn. d, the anteroposterior distance between the limeninsulae and the anterior tip of the temporal horn.
severe neurological disorders if damaged. In the current study,it was evidenced that the auditory radiations and the claustro-opercular and insulo-opercular fibers of the external andextreme capsules pass through the temporal stem above theIFOF, whereas the optic radiations pass below (Figs. 3–5). Theauditory radiations originate at the medial geniculate body,then pursue in an anterior and lateral direction, passingthrough the posterior limb of the internal capsule and the tem-poral stem. Finally, they terminate at the primary auditory areain the Heschl gyri and adjacent parts of the superior temporalgyrus (Fig. 4) (40). The dissection of the posterior portion of thetemporal stem revealed that the IFOF separates the origin ofthe auditory and optic radiations at the medial and lateralgeniculate bodies: the initial segment of the auditory radia-tions coming from the medial geniculate body passes above theIFOF at the temporal stem, whereas the initial segment of theoptic radiations coming from the lateral geniculate body passesbelow. The claustro-opercular and insulo-opercular fibers ofthe external and extreme capsules are U-fibers that connect theclaustrum and insular cortex with the temporal operculum,passing through the temporal stem (21, 25). The current studydemonstrated that these fibers cross the temporal stem passingthrough the narrow space between the superior surface of theIFOF and the inferior limiting sulcus of the insula (Fig. 3).
These anatomic findings are crucial in understanding 2 sur-gical approaches that cross the temporal stem in the dominanthemisphere: 1) the transsylvian approach to the mesial tempo-ral structures, and 2) the temporal transopercular approach totemporoinsular gliomas in the dominant hemisphere.
Transsylvian Approach to Mesial Temporal Structuresin the Dominant Hemisphere
Several surgical approaches have been described to reachtumoral or vascular epileptogenic lesions in the mesial temporal
structures. The classical anterior temporal lobectomy consists ofthe removal of 3 to 5 cm of the anterior temporal lobe to reachthe temporal horn and the mesial temporal structures (19).However, in this approach, the temporal neocortex is incisedand the anterior portion of the inferior longitudinal fasciculus aswell as the Meyer loop could be damaged. Therefore, differenttypes of more selective and less invasive approaches have beendeveloped. In the selective transsylvian approach described byYa argil et al. (50, 51), the sylvian cistern is opened to reach theinferior limiting sulcus, then the anterior portion of the tempo-ral stem is incised laterally to the inferior insular vein. This inci-sion cuts the anterior portion of the uncinate fasciculus, the ante-rior commissure, and arrives at the superior edge of theamygdala. Posterior to the amygdala, the temporal horn andhippocampus are reached. A major risk during this approach isa visual field deficit, resulting from an interruption of the opticradiations when they pass through the temporal stem. Therefore,several researchers have studied different anatomic landmarksthat might help in limiting damage to visual pathways (2, 5, 6,41). In a recent fiber dissection study (5), it was observed that inthe transsylvian approach, an incision at the level of the limeninsulae or adjacent 5 mm of the inferior limiting sulcus was lesslikely to damage the optic radiations than more posterior inci-sions along the inferior limiting sulcus.
However, in addition to the risk of visual field deficit, thetranssylvian approach to the mesial temporal structures in thedominant hemisphere carries the risk of inducing a permanentlanguage dysfunction, resulting from disruption of the IFOFwhen it crosses the temporal stem (9, 11, 12, 14). In the currentstudy, it was demonstrated that the IFOF crosses the posteriortwo-thirds of the temporal stem. Therefore, we identified a safearea at the level of the anterior one-third of the temporal stemthrough which the medial temporal structures can be accessedin the transsylvian approach with a low risk of damaging the
6 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 www.neurosurgery-online.com
MARTINO ET AL.
Art #: NEU192355 1 tables, 6 B&W figs., 0 4/C figs. 4-24-09 Oper: JD Proof: #1
TABLE 1. Distances measured within the temporal stem, at the level of the inferior limiting sulcusa
IFOF–tem- IFOF– IFOF– Limen– Temporal pole– IFOF–roof IFOF– ILS–tem-Side
poral pole tip ventricle limen tip ventricle tip ventricle ventricle ILS poral horn
Left 36 7 15 8 29 4 3 7
Left 38 6 10 4 32 5 3 8
Left 32 4 8 4 28 5 4 9
Left 35 4 11 5 29 4 4 8
Left 38 5 13 9 34 6 6 12
Right 34 4 12 8 30 3 3 6
Right 35 4 10 6 31 2 4 6
Right 38 3 9 6 35 6 3 9
Right 30 4 9 5 26 6 5 11
Right 26 4 12 8 22 3 2 6
Mean 34.2 4.5 10.9 6.3 29.5 4.4 3.8 8.2
Range 26–38 3–7 8–15 4–9 22–35 2–6 3–6 6–12
a IFOF, inferior frontooccipital fasciculus; ILS, inferior limiting sulcus; limen, limen insulae. All data are expressed in millimeters.

IFOF. Obvious interindividual differences were observed in thelength of this space between the limen insulae and the anterioredge of the IFOF, but in any of the cases studied, this distancewas inferior to 8 mm (Fig. 6). This anterior region of the tempo-ral stem is occupied by the uncinate fasciculus, which isinevitably transected in this approach. If a wider exposure isneeded, the incision could be extended laterally, because thefibers of the IFOF turn in a posterior direction at the lateral por-tion of the temporal stem. Consequently, a wider anteroposte-rior distance is created between the IFOF and the limen insulae(Figs. 3–6). However, this maneuver increases the risk of dam-aging the optic radiations because the medial limit of the Meyerloop is located in the lateral portion of the anterior temporalstem. Another interesting observation was that, in all the casesdissected, the tip of the temporal horn was located between thelimen insulae and the anterior edge of the IFOF (Fig. 6). As aconsequence, the space between the anterior edge of the IFOFand the tip of the ventricle is very narrow (average, 4.5 mm),explaining why it is necessary to remove a portion of the amyg-dala during the amygdalohippocampectomy to reach the tem-poral horn. Interestingly, a strictly transsylvian transuncalapproach to lesions restricted to the mesial temporal couldavoid damage of the uncinate, the IFOF, and the optic radiation.
Temporal Transopercular Approach to TemporoinsularGliomas in the Dominant Hemisphere
The surgical approach to insular gliomas represents a chal-lenging and controversial area in neurosurgery. Some authorsadvocate systematical use of the transsylvian approach, even ininsulo-opercular tumors (46, 49), whereas others use thisapproach only in purely insular tumors (31, 34, 53). Our grouphas recently reported a series of 51 consecutive patients whounderwent surgery for a low-grade glioma involving the insularlobe (10). In this series, the frontal and/or temporal transopercu-lar approach was systematically used for the insulo-operculartumors. In the first step of the transopercular approach, IES isapplied to the frontal and/or temporal operculum in order todistinguish between the regions essential for the function,which induce clinical disturbances during stimulation, andshould be surgically preserved, and not essential for the func-tion (without clinical disturbances during stimulation, andwhich can be removed without consequences). This enables anelective subpial resection of the operculum to be performed,even in the dominant side, in order to not only remove thetumor but to also give a better exposure of the insula. The insu-lar component of the tumor is subsequently approached pass-ing through the base of the periinsular sulci. Subpial dissectionis used to gently remove the tumoral tissue below the periinsu-lar sulci. This step is a critical aspect of the procedure, becauseit creates a surgical route from the operculum to the insularregion, providing access to the insular portion of the tumor. Inthe last stage of the procedure, the insular component of thetumor is removed subpially. During insular resection, subcor-tical stimulation is used to identify and preserve the pyramidalpathway and the language tracts in awake patients. Indeed,although diffusion tensor imaging integrated in modern navi-
gational systems would represent a valuable adjunct, especiallyduring a transtemporal stem approach, this technique is onlyable to provide anatomic data, and not functional data, to thecontrary of awake mapping. In particular, intraoperative stim-ulation enables differentiation of the fibers of the uncinate fas-ciculus and those of the IFOF, by inducing semantic parapha-sia during stimulation involving specifically the IFOF (12).
In the particular case of a temporoinsular glioma, the tempo-ral stem is infiltrated and expanded, because it is the anatomicroute crossed by the tumor to pass from the insular region to thetemporal lobe (28). The temporal transopercular approach totemporoinsular gliomas must cross the temporal stem to removethe part of the tumor passing from the insula to the temporalregion. In the dominant hemisphere, this approach encounters 2crucial functional structures within the temporal stem, i.e., theIFOF and the optic radiations. Thus, in this specific case, the fol-lowing question can be asked: once the temporal operculum hasbeen removed, which is the surgical route within the temporalstem that enables the resection of the deep component of a tem-poroinsular glioma without damaging these 2 important func-tional structures? The answer to this question requires a detailedknowledge of the 3-dimensional organization of the white mat-ter tracts that compound the temporal stem. In the present work,it was observed that the IFOF conforms an anatomic boundarywithin the temporal stem that separates the structures that passabove (the auditory radiations and the claustro-opercular andinsulo-opercular fibers of the external and extreme capsules)from the optic radiations that pass below (Figs. 3–5). The surgi-cal route from the temporal operculum to the insula through thetemporal stem must preserve this functional deep limit of theIFOF. Consequently, it should pass through the space betweenthe superior surface of the IFOF and inferior limiting sulcus. Thecurrent anatomic data are supported by previous IES mappingstudies in which the IFOF was identified as the deep limit of theresection within the temporal stem, in the transopercularapproach to the insular region in the dominant hemisphere (9,11, 12, 14). This space superficial to the IFOF is crossed by the U-fibers that connect the insular cortex and claustrum with thetemporal operculum. The anatomic dissection of this regionrevealed that this space is very narrow (average, 3.8 mm; range,3–6 mm) (Fig. 3). However, in a temporoinsular glioma, the tem-poral stem is enlarged (28), and the space between the IFOF andthe inferior limiting sulcus is widely expanded. Consequently,the resection of these insulo-opercular and claustro-opercularconnections opens a wide surgical route between the IFOF andthe inferior limiting sulcus, providing access to the insular com-ponent of the tumor. Interestingly, preservation at the level ofthe temporal stem of the deep functional boundary of the IFOFwill also help in avoiding damage to the optic radiations,because they are located below this limit (Fig. 3). Regarding theacoustic radiations, they terminate in the posterior portion ofthe superior temporal gyrus (i.e., in the Heschl gyri). Languagedisturbances are frequently elicited during electrostimulationof this area (23, 36, 37). Therefore, opercular resection is nor-mally anterior to this region, and the acoustic radiations are fre-quently spared in the resection.
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 | 7
INFERIOR FRONTO-OCCIPITAL FASCICULUS AND TEMPORAL STEM
Art #: NEU192355 1 tables, 6 B&W figs., 0 4/C figs. 4-24-09 Oper: JD Proof: #1
8 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 www.neurosurgery-online.com
MARTINO ET AL.
Art #: NEU192355 1 tables, 6 B&W figs., 0 4/C figs. 4-24-09 Oper: JD Proof: #1
CONCLUSIONS
The uncinate fasciculus crosses the anterior one-third of thetemporal stem, passing through the region of the limen insulaeand a few millimeters of the inferior limiting sulcus of the insula.The IFOF crosses the posterior two-thirds of the temporal stem,in the region between the posterior limit of the uncinate fascicu-lus and the lateral geniculate body. The auditory radiations andthe claustro-opercular and insulo-opercular fibers of the externaland extreme capsules pass through the temporal stem above theIFOF, whereas the optic radiations pass below.
The integration of these anatomic data into the surgical strat-egy of the following trajectories through the temporal stem inthe dominant hemisphere will decrease the risk of damagingthe IFOF. In the transsylvian approach to the mesial temporalstructures, an incision within the posterior 8 mm from thelimen insulae is less likely to damage the IFOF than more pos-terior incisions along the inferior limiting sulcus. In the tempo-ral transopercular approach to temporo-insular gliomas in thedominant hemisphere, the IFOF constitutes the deep functionallimit of the resection within the temporal stem. Consequently,this surgical route through the temporal stem to reach the insu-lar region should pass through the space between the superiorsurface of the IFOF and the inferior limiting sulcus. Preserva -tion at the temporal stem of the deep functional boundary ofthe IFOF will also avoid damaging the optic radiations becausethey are located below this limit.
DisclosureJuan Martino, M.D., receives specific funding from the Post-MIR Wenceslao
López-Albo’s grant of the Fundación “Marqués de Valdecilla,” IFIMAV, Santander,Cantabria, Spain. The other authors have no personal financial or institutionalinterest in any of the drugs, materials, or devices described in this article.
REFERENCES
1. Beliën AT, Paganetti PA, Schwab ME: Membrane-type 1 matrix metallopro-tease (MT1-MMP) enables invasive migration of glioma cells in central nerv-ous system white matter. J Cell Biol 144:373–384, 1999.
2. Campero A, Tróccoli G, Martins C, Fernandez-Miranda JC, Yasuda A, RhotonAL Jr: Microsurgical approaches to the medial temporal region: An anatom-ical study. Neurosurgery 59 [Suppl 2]:ONS279–ONS308, 2006.
3. Catani M, Mesulam M: What is a disconnection syndrome? Cortex44:911–913, 2008.
4. Catani M, Thiebaut de Schotten M: A diffusion tensor imaging tractographyatlas for virtual in vivo dissections. Cortex 44:1105–1132, 2008.
5. Choi C, Rubino PA, Fernandez-Miranda JC, Abe H, Rhoton AL Jr: Meyer’sloop and the optic radiations in the transsylvian approach to the mediobasaltemporal lobe. Neurosurgery 59 [Suppl 2]:ONS228–ONS236, 2006.
6. Coppens JR, Mahaney KB, Abdulrauf SI: An anteromedial approach to thetemporal horn to avoid injury to the optic radiation fibers and uncinate fas-ciculus: Anatomical and technical note. Neurosurg Focus 18:E3, 2005.
7. Crosby EC, Humphrey T, Lauer EW: Correlative Anatomy of the Nervous System.New York, Macmillan, 1962.
8. Doricchi F, Thiebaut de Schotten M, Tomaiuolo F, Bartolomeo P: White mat-ter (dis)connections and gray matter (dys)functions in visual neglect: Gaininginsights into the brain networks of spatial awareness. Cortex 44:983–995,2008.
9. Duffau H: The anatomo-functional connectivity of language revisited. Newinsights provided by electrostimulation and tractography. Neuropsychologia46:927–934, 2008.
AQ:4
AQ:5
AQ:6
10. Duffau H: A personal consecutive series of surgically treated 51 cases of insu-lar WHO grade II glioma: Advances and limitations. J Neurosurg (in press).
11. Duffau H, Peggy Gatignol ST, Mandonnet E, Capelle L, Taillandier L:Intraoperative subcortical stimulation mapping of language pathways in aconsecutive series of 115 patients with Grade II glioma in the left dominanthemisphere. J Neurosurg 109:461–471, 2008.
12. Duffau H, Gatignol P, Mandonnet E, Peruzzi P, Tzourio-Mazoyer N, CapelleL: New insights into the anatomo-functional connectivity of the semanticsystem: A study using cortico-subcortical electrostimulations. Brain128:797–810, 2005.
13. Duffau H, Khalil I, Gatignol P, Denvil D, Capelle L: Surgical removal of cor-pus callosum infiltrated by low-grade glioma: Functional outcome and onco-logical considerations. J Neurosurg 100:431–437, 2004.
14. Duffau H, Thiebaut de Schotten M, Mandonnet E: White matter functionalconnectivity as an additional landmark for dominant temporal lobectomy. JNeurol Neurosurg Psychiatry 79:492–495, 2008.
15. Duvernoy HM: The Human Brain Stem and Cerebellum: Surface, Structure,Vascularization, and Three-Dimensional Sectional Anatomy with MRI. Vienna,Springer-Verlag, 1995.
16. Duvernoy HM: The Human Brain: Surface, Three-Dimensional Sectional Anatomyand MRI, and Blood Supply. Vienna, Springer-Verlag, 1999.
17. Ebeling U, von Cramon D: Topography of the uncinate fascicle and adjacenttemporal fiber tracts. Acta Neurochir (Wien) 115:143–148, 1992.
18. Epelbaum S, Pinel P, Gaillard R, Delmaire C, Perrin M, Dupont S, Dehaene S,Cohen L: Pure alexia as a disconnection syndrome: New diffusion imagingevidence for an old concept. Cortex 44:962–974, 2008.
19. Falconer MA, Meyer A, Hill D, Mitchell W, Pond DA: Treatment of temporallobe epilepsy by temporal lobectomy; a survey of findings and results. Lancet268:827–835, 1955.
20. Fernández-Miranda JC, Rhoton AL Jr, Álvarez-Linera J, Kakizawa Y, Choi C,de Oliveira EP: Three-dimensional microsurgical and tractographic anatomyof the white matter of the human brain. Neurosurgery 62 [Suppl 3]:989–1028,2008.
21. Fernández-Miranda JC, Rhoton AL Jr, Kakizawa Y, Choi C, Alvarez-Linera J:The claustrum and its projection system in the human brain: A microsurgicaland tractographic anatomical study. J Neurosurg 108:764–774, 2008.
22. Fox CJ, Iaria G, Barton JJ: Disconnection in prosopagnosia and face process-ing. Cortex 44:996–1009, 2008.
23. Gatignol P, Capelle L, Le Bihan R, Duffau H: Double dissociation betweenpicture naming and comprehension: An electrostimulation study.Neuroreport 15:191–195, 2004.
24. Giese A, Bjerkvig R, Berens ME, Westphal M: Cost of migration: Invasion ofmalignant gliomas and implications for treatment. J Clin Oncol 21:1624–1636,2003.
25. Hentschel SJ, Lang FF: Surgical resection of intrinsic insular tumors.Neurosurgery 57:176–183, 2005.
26. Horel JA: The neuroanatomy of amnesia. A critique of the hippocampal mem-ory hypothesis. Brain 101:403–445, 1978.
27. Horel JA, Misantone LJ: The Klüver-Bucy syndrome produced by partial iso-lation of the temporal lobe. Exp Neurol 42:101–112, 1974.
28. Kier EL, Staib LH, Davis LM, Bronen RA: MR imaging of the temporal stem:Anatomic dissection tractography of the uncinate fasciculus, inferior occip-itofrontal fasciculus, and Meyer’s loop of the optic radiation. AJNR Am JNeuroradiol 25:677–691, 2004.
29. Klingler J: Erleichterung der makroskopischen Praeparation des Gehirnsdurch den Gefrierprozess [in German]. Schweiz Arch Neurol Psychiatr36:247–256, 1935.
30. Klingler J, Gloor P: The connections of the amygdala and of the anterior tem-poral cortex in the human brain. J Comp Neurol 115:333–369, 1960.
31. Lang FF, Olansen NE, DeMonte F, Gokaslan ZL, Holland EC, Kalhorn C,Sawaya R: Surgical resection of intrinsic insular tumors: Complication avoid-ance. J Neurosurg 95:638–650, 2001.
32. Ludwing E, Klingler J: Atlas Cerebri Humani: Der innere Bau des Gehirnsdargestellt auf Grund mackroskopischer Präparate [in German]. Boston, Little,Brown, 1956.
33. Mandonnet E, Capelle L, Duffau H: Extension of paralimbic low gradegliomas: Toward an anatomical classification based on white matter invasionpatterns. J Neurooncol 78:179–185, 2006.
AQ:7
34. Neuloh G, Pechstein U, Schramm J: Motor tract monitoring during insularglioma surgery. J Neurosurg 106:582–592, 2007.
35. Nieuwenhuys R, Voogd J, van Huijzen C: The Human Central Nervous System.Berlin, Springler-Verlag, 1988.
36. Ojemann GA: Individual variability in cortical localization of language. JNeurosurg 50:164–169, 1979.
37. Ojemann GA: Functional mapping of cortical language areas in adults.Intraoperative approaches. Adv Neurol 63:155–163, 1993.
38. Peltier J, Travers N, Destrieux C, Velut S: Optic radiations: A microsurgicalanatomical study. J Neurosurg 105:294–300, 2006.
39. Peuskens D, van Loon J, Van Calenbergh F, van den Bergh R, Goffin J, PletsC: Anatomy of the anterior temporal lobe and the frontotemporal regiondemonstrated by fiber dissection. Neurosurgery 55:1174–1184, 2004.
40. Rhoton AL Jr: The cerebrum. Neurosurgery 51:S1–S51, 2002.41. Rubino PA, Rhoton AL Jr, Tong X, Oliveira E: Three-dimensional relationships
of the optic radiation. Neurosurgery 57:219–227, 2005.42. Rudrauf D, Mehta S, Grabowski TJ: Disconnection’s renaissance takes shape:
Formal incorporation in group-level lesion studies. Cortex 44:1084–1096, 2008.43. Sincoff EH, Tan Y, Abdulrauf SI: White matter fiber dissection of the optic
radiations of the temporal lobe and implications for surgical approaches tothe temporal horn. J Neurosurg 101:739–746, 2004.
44. Taoka T, Iwasaki S, Sakamoto M, Nakagawa H, Fukusumi A, Myochin K,Hirohashi S, Hoshida T, Kichikawa K: Diffusion anisotropy and diffusivity ofwhite matter tracts within the temporal stem in Alzheimer disease: Eval -uation of the “tract of interest” by diffusion tensor tractography. AJNR Am JNeuroradiol 27:1040–1045, 2006.
45. Türe U, Ya argil MG, Friedman AH, Al-Mefty O: Fiber dissection technique:Lateral aspect of the brain. Neurosurgery 47:417–427, 2000.
46. Vanaclocha V, Sáiz-Sapena N, Garcia-Casasola C: Surgical treatment of insu-lar gliomas. Acta Neurochir (Wien) 139:1126–1135, 1997.
47. Wang F, Sun T, Li XG, Liu NJ: Diffusion tensor tractography of the temporalstem on the inferior limiting sulcus. J Neurosurg 108:775–781, 2008.
48. Yasargil MG: Microneurosurgery: CNS Tumors: Surgical Anatomy, Neuro -pathology, Neuroradiology, Neurophysiology, Clinical Considerations, Operability,Treatment Options. Stuttgart, Georg Thieme-Verlag, 1994.
49. Yasargil MG, Reeves JD: Tumours of the limbic and paralimbic system. ActaNeurochir (Wien) 116:147–149, 1992.
50. Yasargil MG, Teddy PJ, Roth P: Selective amygdalo-hippocampectomy.Operative anatomy and surgical technique. Adv Tech Stand Neurosurg12:93–123, 1985.
51. Yasargil MG, Wieser HG, Valavanis A, von Ammon K, Roth P: Surgery andresults of selective amygdala-hippocampectomy in one hundred patientswith nonlesional limbic epilepsy. Neurosurg Clin N Am 4:243–261, 1993.
52. Yoshida D, Watanabe K, Noha M, Takahashi H, Teramoto A, Sugisaki Y:Tracking cell invasion of human glioma cells and suppression by anti-matrixmetalloproteinase agent in rodent brain-slice model. Brain Tumor Pathol19:69–76, 2002.
53. Zentner J, Meyer B, Stangl A, Schramm J: Intrinsic tumors of the insula: Aprospective surgical study of 30 patients. J Neurosurg 85:263–271, 1996.
AcknowledgmentsWe thank the Montpellier University of Medicine Anatomy Laboratory staff
for help in the preparation of the specimens.
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 | 9
INFERIOR FRONTO-OCCIPITAL FASCICULUS AND TEMPORAL STEM
Art #: NEU192355 1 tables, 6 B&W figs., 0 4/C figs. 4-24-09 Oper: JD Proof: #1
Author Query
AQ 1: Please spell out CNRS.
AQ 2: Cannot find the spelling “claustro-opercular.” Is this the same as “claustrum opercular”?
AQ 3: Please specify what measurement(s) constitute “this distance” in the last sentence of this para-graph.
AQ 4: Please verify Disclosure statement and spell out all abbreviations as appropriate.
AQ 5: Please check book title as changed for reference 16.
AQ 6: Please provide German to English translation for Reference 29.
AQ 7: Please provide English translation of book title in reference 32.
Art #: NEU192355 1 tables, 6 B&W figs., 0 4/C figs. 4-24-09 Oper: JD Proof: #1
Copyright © 2022 FDOKUMEN




















