
A Safe and Effective Technique for Harvesting the Occipital Artery for Posterior Fossa Bypass...
45
Accepted Manuscript A Safe and Effective Technique for Harvesting the Occipital Artery for Posterior Fossa Bypass Surgery: A Cadaveric Study Hitoshi Fukuda, MD Alexander Evins, MD Justin Burrell, MS Philip E. Stieg, MD, PhD Antonio Bernardo, MD PII: S1878-8750(13)01114-5 DOI: 10.1016/j.wneu.2013.09.015 Reference: WNEU 2108 To appear in: World Neurosurgery Received Date: 8 May 2013 Revised Date: 13 August 2013 Accepted Date: 10 September 2013 Please cite this article as: Fukuda H, Evins A, Burrell J, Stieg PE, Bernardo A, A Safe and Effective Technique for Harvesting the Occipital Artery for Posterior Fossa Bypass Surgery: A Cadaveric Study, World Neurosurgery (2013), doi: 10.1016/j.wneu.2013.09.015. This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of A Safe and Effective Technique for Harvesting the Occipital Artery for Posterior Fossa Bypass...
Accepted Manuscript
A Safe and Effective Technique for Harvesting the Occipital Artery for Posterior FossaBypass Surgery: A Cadaveric Study
Hitoshi Fukuda, MD Alexander Evins, MD Justin Burrell, MS Philip E. Stieg, MD, PhDAntonio Bernardo, MD
PII: S1878-8750(13)01114-5
DOI: 10.1016/j.wneu.2013.09.015
Reference: WNEU 2108
To appear in: World Neurosurgery
Received Date: 8 May 2013
Revised Date: 13 August 2013
Accepted Date: 10 September 2013
Please cite this article as: Fukuda H, Evins A, Burrell J, Stieg PE, Bernardo A, A Safe and EffectiveTechnique for Harvesting the Occipital Artery for Posterior Fossa Bypass Surgery: A Cadaveric Study,World Neurosurgery (2013), doi: 10.1016/j.wneu.2013.09.015.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Title: A Safe and Effective Technique for Harvesting the Occipital Artery for Posterior Fossa Bypass Surgery: A Cadaveric Study Authors: Hitoshi Fukuda, MD1,2, Alexander Evins MD1, Justin Burrell MS1, Philip E. Stieg MD, PhD1, Antonio Bernardo MD1 Departmental and Institutional Affiliations: 1Department of Neurological Surgery Weill Cornell Medical College Cornell University New York, NY USA
2Department of Neurosurgery Kyoto University School of Medicine Kyoto, Kyoto Japan Disclosure of Funding: None. Financial Support, Industry Affiliations, Grants, and/or Financial Disclosures: None. No financial disclosures for any author. Corresponding Author Information: Name: Antonio Bernardo Address: Weill Cornell Medical College
1300 York Avenue, Baker F2212 New York, NY 10065 USA
Phone: (212) 746-1468 Fax: (212) 746-7007 Email: [email protected]
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 1
Abstract 1
2
Objective 3
The occipital artery (OA) is an important donor artery for posterior fossa revascularization. 4
Harvesting the OA is believed to be difficult and time-consuming due to its 3-dimensional course 5
through different suboccipital tissue layers. We propose a safe and effective means of dissecting 6
the OA. 7
8
Methods 9
The course of the OA was explored in five cadaveric heads (10 sides). The OA was divided into 10
three segments based on the vertical muscle layer it ran through; subcutaneous, transitional, and 11
intramuscular. Three different approaches were attempted and their respective advantages and 12
disadvantages were assessed. 13
14
Results 15
The subcutaneous segment of the OA was found to run above the galea without traversing any 16
vertical layers, and was thus easily dissected down to the superior nuchal line (SNL). The 17
segment between the SNL and the digastric groove, traditionally the suboccipital segment, was 18
divided into transitional and intramuscular segments. After detaching and retracting the 19
suboccipital muscles, the OA was found to run in a single vertical layer of connective tissue. 20
Dissection of the transitional segment was more involved as it ran between the SNL and the 21
superior edge of the splenius capitis muscle, and vertically through the galea aponeurotica and 22
the tendon of the sternocleidomastoid muscle (SCM). 23
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 2
24
Conclusion 25
This segmentation provided a safe and effective procedure for harvesting the OA, where 26
dissection of the transitional segment is a critical step. Although the course of the OA is complex, 27
precise anatomical knowledge of the suboccipital muscles and a stepwise dissection make 28
harvesting the OA relatively simple. 29
30
Keywords: occipital artery; posterior fossa bypass; microsurgical anatomy; cadaver31
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 3
32
Introduction 33
Posterior fossa extracranial-intracranial bypass is an important procedure for the 34
treatment of ischemic disease affecting posterior circulation, skull base tumors involving the 35
main arterial branches, and complex or giant posterior circulation aneurysms (3-4, 7, 15). The 36
occipital artery (OA) is an important donor artery for posterior fossa revascularization due to its 37
size, anatomical proximity to target recipient vessels, and flow rate. The OA has been reported to 38
provide a mean blood flow of 15-80 ml/min when used for posterior fossa bypass (11). 39
Harvesting the OA is believed to be difficult and time-consuming due to its 3-40
dimensional course through different suboccipital tissue layers. We propose three different 41
dissection methods for the safe and effective harvesting the OA. 42
43
Methods 44
Five adult cadaveric heads with 10 OA’s were injected with colored latex. The scalp and 45
subcutaneous tissues were removed and the OA, from the digastric groove to the vertex, was 46
divided into three segments – intramuscular, transitional, and subcutaneous – based on the 47
vertical anatomical layers traversed. The intramuscular segment was defined as the proximal part 48
of the OA extending from the digastric groove to the superior edge of the splenius capitis muscle 49
(SPC). The transitional segment was defined as the middle part of the OA extending from the 50
superior edge of the SPC to the superior nuchal line (SNL); and the subcutaneous segment was 51
defined as the most distal part of the OA above the SNL. 52
A conventional hockey-stick shaped scalp incision was made and the OA was harvested 53
as a donor vessel. The incision, at the spinous process of C4, was extended to the midline above 54
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 4
the external occipital protuberance and directed laterally 3 cm above the SNL. The incision was 55
then directed inferiorly along the mastoid process, ending 1 cm below the mastoid tip (Figure 56
1A). 57
A distal-type hockey-stick shaped incision and a proximal-type hockey-stick shaped 58
incision were performed according to the starting point of the incision. The distal-type hockey-59
stick incision first exposed the distal end of the OA and then proceeded proximally. The 60
proximal-type hockey-stick incision first exposed the proximal portion of the OA near the 61
mastoid process and then proceeded distally. A novel reverse-C incision was also assessed. The 62
inferior and superior ends of the C-incision were located on the spinous process of C2 and above 63
the external occipital protuberance, respectively. The apex of the C-incision was located on the 64
mastoid process (Figure 1B). 65
The OA was harvested in each of these incisions based on its anatomical course. The 66
subcutaneous segment was dissected from a reflected epigaleal layer, the transitional segment 67
was carefully dissected from multiple muscle layers, and the intramuscular segment was 68
harvested by uncovering the SPC from an underlying single connective tissue layer. In each 69
specimen, the feasibility of an OA-posterior inferior cerebellar artery (PICA) bypass was 70
assessed by grafting the end of the OA to the caudal loop of the PICA. 71
72
Results 73
Segmentation of the OA 74
The scalp and subcutaneous tissue in the occipital region were dissected to visualize the 75
course of the OA and the muscle layers it traversed. The OA originated from the posterior aspect 76
of the external carotid artery, proximal to the origin of the facial artery. The OA ran 77
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 5
posterosuperiorly along the medial surface of the posterior belly of the digastric muscle. Under 78
the mastoid groove, the OA turned posteromedially and ran through multiple suboccipital 79
muscles. Near the external occipital protuberance, the OA turned upwards and terminated in one 80
or two main terminal trunks. The OA provided arterial supply to most of the muscles of the upper 81
posterior and lateral portion of the neck, the occipital muscles, and the posterior half of the scalp. 82
Upon our initial dissection, the OA, distal to the posterior belly of the digastric muscle, 83
was divided into three segments, subcutaneous, transitional, and intramuscular, described above 84
(Figure 2A). The proximal section of the OA, covered by the posterior belly of the digastric 85
muscle, was not included in our investigation as harvesting this segment is rarely required for 86
posterior fossa bypass surgery. 87
The intramuscular segment of the OA, from the digastric groove to the superior edge of 88
SPC, ran in a single fatty connective tissue layer between the SPC and the semispinalis capitis 89
muscle (SSC) – a posterior extension of the connective tissue of the infratemporal fossa – we 90
termed the styloid diaphragm (Figures 2A and 2B) (5). The transitional segment of the OA, from 91
the superior edge of the SPC to the SNL, exited the styloid diaphragm and traveled superficially 92
through the tendon of the sternocleidomastoid (SCM) muscle and the galea aponeurotica until 93
(Figure 2B). This segment bent approximately 90° and ascended towards the vertex. The 94
subcutaneous segment was located above the SNL and superficial to the galea aponeurotica. 95
Overall, the intramuscular and the subcutaneous segments of the OA remained within the 96
single tissue layer referred to as the styloid diaphragm and the epigaleal layer, respectively. 97
Conversely, the transitional segment crossed multiple vertically superimposed tissue layers 98
including the tendon of the SCM and the galea aponeurotica. 99
On average, the length of the intramuscular and the transitional segments were measured 100
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 6
at 6 cm and 1 cm, respectively. The length of the subcutaneous segment ranged from 4 cm to 7 101
cm depending on the superior extension of the skin incision. An 11-14 cm graft was, in all cases, 102
long enough to suitably reach the caudal loop of the ipsilateral PICA. The graft was trimmed 103
down to 8-9 cm to prevent kinking when performing OA-PICA anastomosis. 104
In all cases, the OA was successfully harvested and no damage to the artery, indicated by 105
an intact adventitia and absent latex exposure, was observed during dissection. 106
107
Harvesting the OA Using a “Distal-type Hockey-Stick Approach” 108
A conventional hockey-stick shaped scalp incision, as described above, was used. Our 109
anatomical findings suggest the use of a stepwise incision with multiple sequential steps instead 110
of incising the whole site at once. 111
A skin incision was initiated at the upper half of the planned incision site above the 112
superior nuchal line. The distal end of the subcutaneous segment, found 4-5 cm from the midline 113
under the horizontal part of the incision, was ligated and cut (Figures 1A and 3A). The scalp flap 114
was then reflected inferiorly to the superior nuchal line. The occipital muscle was included in the 115
flap in order to protect the OA (Figure 3A). The OA was then dissected off of the surrounding 116
tissue (Figure 3A). 117
The lateral skin incision was extended to the tip of the mastoid process. The transitional 118
segment of the OA was surrounded by the superior nuchal line superiorly, the medial edge of the 119
tendon of the SCM laterally, and the SPC inferiorly (Figures 2B, 3B, and 3C). The transitional 120
segment was varied in its course, and in some cases ran so medially that it was covered by the 121
trapezius muscle (Figure 3D). As a result, the SCM and SPC were exposed first, and then the 122
transitional segment was localized in all three directions, SCM, SPC, and SNL (Figure 3B). The 123
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 7
point where the distal end of the transitional segment pierced the galea aponeurotica was found 124
and delicately dissected until it was covered by the superior edge of the SPC (Figures 3C and 125
3D). 126
The midline skin incision was extended to the C4 spinous process (Figure 1A). The 127
tendon of the SCM was detached from the occipital bone and retracted laterally to expose the 128
attachment of the SPC (Figure 3E). The tendon of the SPC could be easily confused with the 129
SCM because they are in close proximity. The SPC was detached and retracted infero-medially 130
to reveal the intramuscular segment of the OA as it traversed the styloid diaphragm (Figure 3F). 131
Here, the belly of the SPC was carefully dissected in order to preserve a significant amount of 132
protective fatty tissue. The intramuscular segment was followed proximally within the styloid 133
diaphragm to the inferior edge of the posterior belly of the digastric muscle. The styloid 134
diaphragm and the intramuscular segment of the OA were covered by the longissimus capitis 135
muscle in 8 of 10 specimens (Figure 3G); and in these cases, the longissimus capitis muscle was 136
also detached from the mastoid process and retracted infero-medially. At this point, the OA was 137
sufficiently dissected (11-14 cm). 138
Further dissection may be added depending on the purpose of the operation, even though 139
an adequate amount of the OA was isolated. When extensive exposure of the sigmoid sinus is 140
required, the attachment of the posterior belly of the digastric muscle could be partly detached to 141
allow for a larger craniotomy. When exposure of the suboccipital triangle is necessary, the 142
superior oblique capitis muscle can be dissected and reflected infero-laterally. Both procedures 143
require careful dissection in order to avoid injury to the proximal portion of the intramuscular 144
segment (Figure 3H). 145
146
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 8
Harvesting the OA Using a “Proximal-type Hockey-Stick Approach” 147
Harvesting of the OA through a proximal to distal incision began with the lateral skin 148
incision of the traditional hockey-stick shaped incision on the mastoid process. The incision was 149
extended to the horizontal part just before the point where it crosses the subcutaneous segment of 150
the OA (Figure 4A). The subcutaneous segment was outlined with a skin marker in order to 151
avoid disconnection of the distal end of the subcutaneous segment and to spare the blood flow of 152
the OA during dissection of the intramuscular segment. The bellies of the SCM and the SPC 153
were exposed and used as landmarks for localizing the transitional segment of the OA, as 154
described in the distal-type hockey-stick incision. The proximal part of the transitional segment 155
passed beneath the superior edge of the SPC and was exposed by following the SPC belly 156
superiorly because the subcutaneous segment of the OA was not yet dissected free (Figure 4B). 157
Detachment of the SCM prior to identifying the transitional segment was not done in order to 158
avoid injury to the OA at the point where it pierces the tendon of the SCM. 159
Once the proximal portion of the transitional OA was exposed, the SCM and the SPC 160
were detached and retracted laterally and infero-medially, respectively. The intramuscular 161
segment of the OA was harvested from the styloid diaphragm, as described previously (Figure 162
4C). The entire skin incision was completed and extended to the inferior end of the midline skin 163
incision. The suboccipital muscles were detached from the suboccipital bone subperiosteally, and 164
the skin-muscle flap was reflected inferiorly (Figure 4D). The muscles composing the 165
suboccipital triangle may be left attached to the bone if needed. The subcutaneous OA was 166
severed at the level of the horizontal skin incision. Once the skin-muscle layer was reflected 167
inferiorly, the rest of the transitional and subcutaneous segments were harvested through the 168
galea aponeurotica and the tendon of the SCM (Figure 4E). 169
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 9
170
Application of a Novel Reverse-C Incision 171
Both proximal and distal types of traditional hockey-stick shaped incisions were found to 172
be safe and effective, and relatively easy for the surgeon to rely on familiar anatomy seen during 173
common approaches to the posterior fossa. However, the pedicle of the scalp flap of the hockey-174
stick incisions was located inferiorly, and thus inferior exposure of the SPC was inadequate to 175
properly dissect the transitional segment of the OA. Additionally, since the scalp flap was 176
reflected inferiorly, the distal end of the subcutaneous segment of the OA had to be ligated and 177
cut during the procedure (Figures 3A and 4D). The dissection could pose some degree of 178
technical difficulty due to a lack of proper tension on the arterial wall and subsequent collapse of 179
the donor artery, or disconnection of the OA at the early stage that could cause graft occlusion. 180
To mitigate these potential pitfalls, a novel reverse-C incision, with the pedicle on the 181
midline, was initiated. A C-shaped scalp incision was made with both ends on the midline and 182
the apex on the mastoid process. The general concept of the dissection was the same as that of 183
the hockey-stick incisions, but the scalp flap was medially reflected. This enabled adequate 184
exposure of the SPC during dissection of the transitional segment and spared the blood flow of 185
the graft until the recipient artery was ready. 186
The superior half of the C-shaped scalp incision exposed the subcutaneous segment and 187
the tendon of the SCM (Figures 5A and 5B). The scalp incision was then extended inferiorly and 188
the scalp flap reflected medially. The continuity of the OA was spared at the end of the 189
subcutaneous segment because the superior half of the scalp incision and the point of scalp flap 190
reflection were nearly parallel to the subcutaneous segment (Figure 5C). This medially reflected 191
scalp incision allowed for a wide exposure of the SPC, and facilitated safe and adequate 192
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 10
exposure of the transitional segment equally from medially, inferiorly, and superiorly (Figure 193
5C). Dissection of the intramuscular segment was the same as the hockey-stick incision (Figure 194
5D). The full length of the dissected OA was retracted anteriorly from the scalp incision and the 195
integrity of the donor OA was kept intact until the recipient artery was completely prepared 196
(Figure 5E). This maneuver helped to avoid graft collapse or occlusion during dissection. 197
198
Discussion 199
The OA has been widely used as a donor artery for posterior fossa extracranial-200
intracranial bypass surgery, especially when the PICA is the recipient vessel (OA-PICA 201
anastomosis) (3-4, 15). Recent advances in endovascular techniques have improved the treatment 202
of posterior circulation ischemia with the use of angioplasty and/or stenting instead of bypass 203
surgery (12). However, OA-PICA anastomosis remains an important tool in the treatment of 204
complicated aneurysms or brain tumors involving the vertebral artery or the PICA when the 205
parent artery has to be sacrificed and failure of bypass could lead to catastrophic ischemia of the 206
cerebellum and brainstem (4, 15). OA-PICA anastomosis is considered to be more challenging 207
than superficial temporal artery-middle cerebral artery bypass due to the narrow and deep 208
surgical corridor needed to reach the recipient vessels (10). Further, the OA runs between 209
multiple muscle layers, and harvesting the OA is more difficult than harvesting the superficial 210
temporal artery that runs in a single epigaleal layer. Simplifying the OA dissection would help 211
surgeons concentrate on the intradural anastomosis and achieve shorter operative times. 212
Although the precise anatomy of the OA has been described in depth (1-2), effective 213
methods for dissecting the OA have yet to be addressed. Conventionally, the suboccipital 214
musculature has been reflected with the scalp as one layer, and the OA has been harvested from 215
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 11
the reflected side by digging and sectioning the belly of multiple suboccipital muscles (16). 216
Substantial damage of muscle fibers results and can cause significant postoperative occipital pain 217
or muscular atrophy. Therefore, we propose this less invasive technique that detaches each 218
muscle separately. 219
Previous articles have described that the OA runs between the SPC and the SSC, which is 220
helpful for harvesting the OA during a traumatic dissection of suboccipital muscles (1-2). 221
However, more detailed anatomical knowledge about the intramuscular segment of the OA needs 222
to be applied for safely and effectively harvesting the artery. 223
The intramuscular segment of the OA was found to run in the styloid diaphragm, which 224
links the posterior belly of digastric muscle with the styloid muscles and divides the 225
infratemporal fossa into the prestyloid region and the retrostyloid region (5). Because the 226
intramuscular segment of the OA then ran in the superficial part of the styloid diaphragm, 227
dissection of the OA from the SPC should be performed with care. Thick fatty tissue underneath 228
the OA prevents identification of the belly of the SSC, negating the SSC as a surgical landmark 229
during harvesting (Figures 3F and 4C). Notably, the most proximal part of the isolated OA 230
(intramuscular segment) could be injured during the dissection of the posterior belly of the 231
digastric muscle and the superior oblique capitis muscle. We believe this practical anatomy of the 232
suboccipital muscles will help surgeons dissect the intramuscular segment of the OA quickly, 233
efficiently, and safely (1-2). 234
Dissecting the transitional segment is a key step in harvesting the OA. Although the 235
transitional segment is distinct from the other segments in terms of the anatomical structures it 236
transverses, conventionally the transitional segment has been included in the suboccipital 237
segment from the digastric groove to the superior nuchal line and has never been discussed 238
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 12
independently (1-2). This segment is about 1 cm long and lies below the superior nuchal line, but 239
its course varies both horizontally and vertically. The transitional segment pierces two vertical 240
anatomical planes, the galea aponeurotica and then the tendon of the SCM, when observed 241
distally to proximally. However, 2 of the 10 OA’s in our study had a more medial course and 242
instead pierced the tendon of the trapezius muscle and ran under its belly before reaching the 243
styloid diaphragm. Additionally, the transitional segment of the OA bends between the horizontal 244
intramuscular segment and the ascending subcutaneous segment (1-2). The angle of this curve 245
varies between approximately 45° and 135°, making it difficult to speculate the course of the OA 246
during dissection of this segment. Given this anatomical complexity, we believe that the 247
transitional segment should be localized by first exposing the SCM and SPC, and isolating the 248
proximal end of the OA, and then detaching the muscles. 249
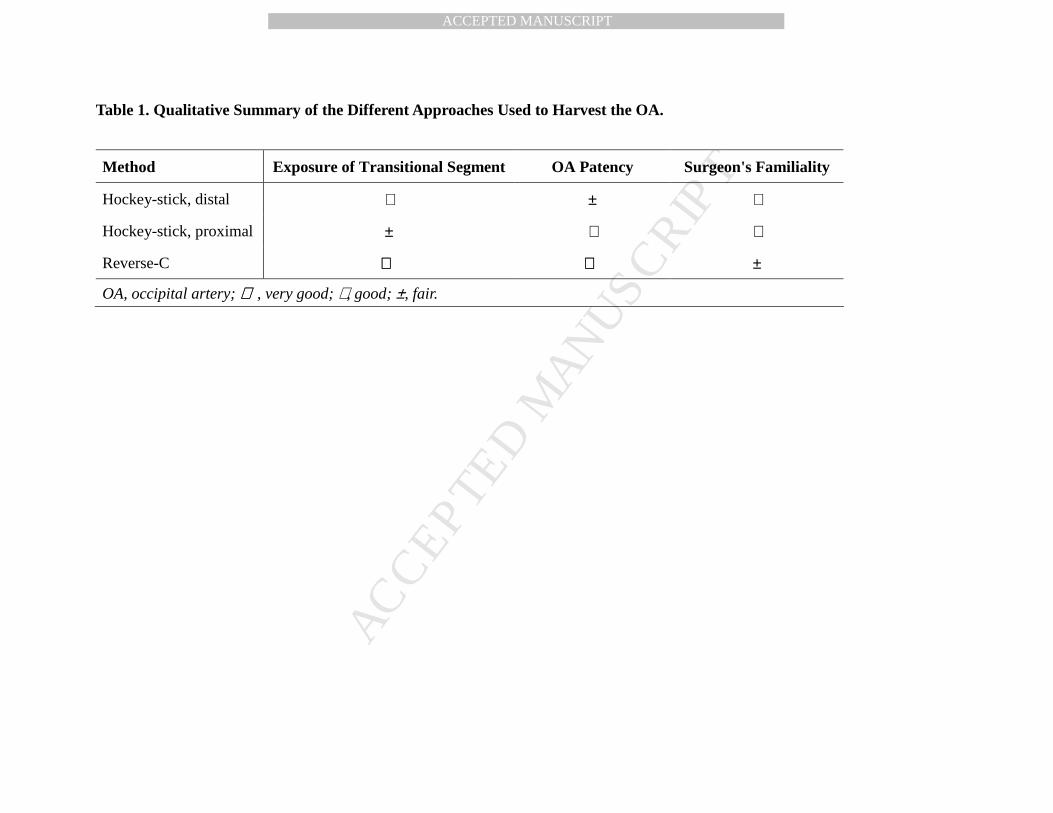
We attempted three different incisions for harvesting the OA, including one with a novel 250
course, and qualitatively analyzed each (Table 1). Each approach was designed to be less 251
traumatic to the occipital muscles than the traditional method of harvesting the OA (16). 252
Cosmetically, there is little concern when incising the occipital region, although a shorter 253
reverse-C skin incision is slightly more desirable. Surgeons should choose the dissection method 254
depending on their own preference and working knowledge of the associated anatomy. However, 255
dissecting the transitional segment of the OA is important for the harvesting process. We 256
recommend that less experienced surgeons use the distal-type hockey-stick or reverse-C incision, 257
as the transitional segment of the OA is localized from multiple directions (Table 1). The 258
proximal-type hockey-stick approach is suitable for experienced surgeons familiar with the 259
complicated anatomy of the suboccipital muscles since exposure of the transitional segment of 260
the OA is relatively technically difficult. Postauricular straight, lazy-S, and regular C-shaped skin 261

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 13
incisions, with the apex of the C placed medially and the opening placed laterally – preferred by 262
some surgeons for lateral suboccipital craniotomies – were also considered and attempted (6, 14). 263
However, in the regular C-shaped incision, lateral reflection of the skin flap exposed the 264
transitional segment of the OA before the SCM and SPC. Thus, blind dissection of the 265
transitional segment, without the SCM and the SPC as landmarks, greatly increased the potential 266
for vascular injury. 267
When applying this method clinically, several practical issues must be taken into 268
consideration. A patient with a short neck often has a thick scalp and substantial fatty tissue 269
between the occipital muscles, which makes exposure of the OA difficult. In such cases, 270
preoperative CT angiography superimposed onto the patient’s scalp anatomy and/or detection of 271
the course of the OA by Doppler ultrasonography can be especially helpful. Preoperative 272
imaging is also useful for detecting atherosclerotic changes to the OA in older patients. In both 273
distal and proximal type hockey-stick approaches, where the distal end of the OA is removed 274
early during the dissection, collapse of the graft is a potential issue. Reserving a branch of the 275
OA on the skin flap can help mitigate this by maintaining blood flow in the graft. 276
Despite thorough anatomical knowledge and careful dissection, the possibility of injury 277
to the OA still exists due to its notably tortuous course. Surgeons should be prepared to use 278
bipolar cautery to deal with bleeding from a small branch of OA, 10-0 nylon sutures to repair a 279
minor laceration of the wall of OA without narrowing of the vessel, or removal and 280
reconstruction, by end-to-end anastomosis, of a severely damaged portion of OA. 281
For surgeons who want to master extracranial and intracranial bypass surgery, laboratory 282
training of anastomosis techniques can be accomplished using silicone tubes, animal vessels, and 283
deep bypass setting equipment (8-9. 13). However, because laboratory training of donor vessel 284
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 14
dissection is unavailable and surgeons rarely have a chance to dissect the OA, cadaveric 285
dissection provides alternative opportunities for mastery before applying these skills to a live 286
patient. 287
288
Conclusions 289
As a result of our study, we found that dividing the OA into three practical segments, 290
based on findings obtained during the harvesting procedure, is essential for defining an optimal 291
dissection strategy. Three different dissection methods were proposed, where dissection of the 292
transitional segment of the OA played a critical role. We recommended that surgeons possess 293
thorough knowledge of the anatomy of the OA before attempting posterior fossa bypass surgery. 294
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 15
References 295
1. Alvernia JE, Fraser K, Lanzino G: The occipital artery: a microanatomical study. 296
Neurosurgery 58(1 Suppl):ONS114-22, 2006. 297
2. Ateş O, Ahmed AS, Niemann D, Baskaya MK: The occipital artery for posterior circulation 298
bypass: microsurgical anatomy. Neurosurg Focus 24(2):E9, 2008. 299
3. Ausman JI, Diaz FG, Vacca DF, Sadasavin B: Superficial temporal and occipital bypass 300
pedicles to superior, anterior inferior, and posterior inferior cerebellar arteries for 301
vertebrobasilar insufficiency. J Neurosurg 72(4):554-8, 1990. 302
4. Ausman JI, Lee MC, Klassen AC, Seljeskog EL, Chou SN: Stroke: what’s new? Cerebral 303
revascularization. Minn Med 59(4):223-7, 1976. 304
5. Bejjani GK, Sullivan B, Salas-Lopez E, Abello J, Wright DC, Jurjus A, Sekhar LN: Surgical 305
anatomy of the infratemporal fossa: the styloid diaphragm revisited. Neurosurgery 306
43(4):842-52, 1998. 307
6. Ciric I, Zhao JC, Rosenblatt S, Wiet R, O’Shaughnessy B: Suboccipital retrosigmoid 308
approach for removal of vestibular schwannomas: facial nerve and hearing preservation. 309
Neurosurgery 56(3):560-70, 2005. 310
7. Friedman JA, Piepgras DG: Current neurosurgical indications for saphenous vein graft 311
bypass. Neurosurg Focus 15;14(3):e1, 2003. 312
8. Hino A: Training in microvascular surgery using a chicken wing artery. Neurosurgery 313
52(6):1495-7, 2003. 314
9. Inoue T, Tsutsumi K, Saito K, Adachi S, Tanaka S, Kunii N: Training of A3-A3 side to side 315
anastomosis in a deep corridor using a box with 6.5cm depth: technical note. Surg Neurol 316
66(6):638-41, 2006. 317
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 16
10. Kawashima M, Rhoton Jr AL, Tanriover N, Ulm AJ, Yasuda A, Fujii K: Microsurgical 318
anatomy of cerebral revascularization. Part II: posterior circulation. J Neurosurg 102(1):132-319
47, 2005. 320
11. Khodadad G: Short- and long-term results of microvascular anastomosis in the 321
vertebrobasilar systems, a critical analysis. Neurol Res 3(1):33-65, 1981. 322
12. Lee CJ, Morasch MD: Endovascular management of vertebral artery disease. Expert Rev 323
Cardiovasc Ther 9(5):575-8, 2011. 324
13. Matsumura N, Hamada H, Yamatani K, Hayashi N, Hirashima Y, Endo S: Side to side 325
arterial anastomosis model in the rat internal and external carotid arteries. J Reconstr 326
Microsurg 17(4):263-6; 2001. 327
14. Ojemann RG: Retrosigmoid approach to acoustic neurinoma (vestibular schwannoma). 328
Neurosurgery 48(3):553-8, 2001. 329
15. Sekhar LN, Kalakovanda C: Cerebral revascularization for aneurysms and tumors. 330
Neurosurgery 50(2):321-31; 2002. 331
16. Sundt Jr TM, Piepgras DG: Occipital to posterior inferior cerebellar bypass surgery. J 332
Neurosurg 48(6):916-28, 1978. 333
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 17
Figure Legends 334
335
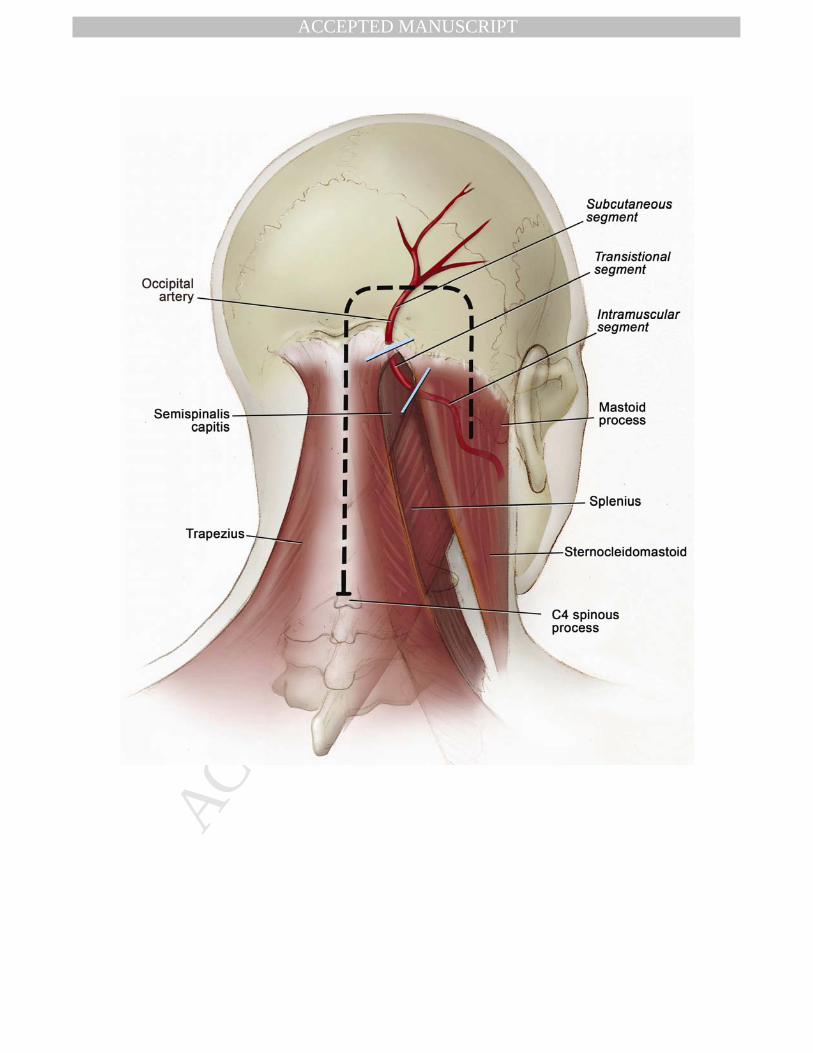
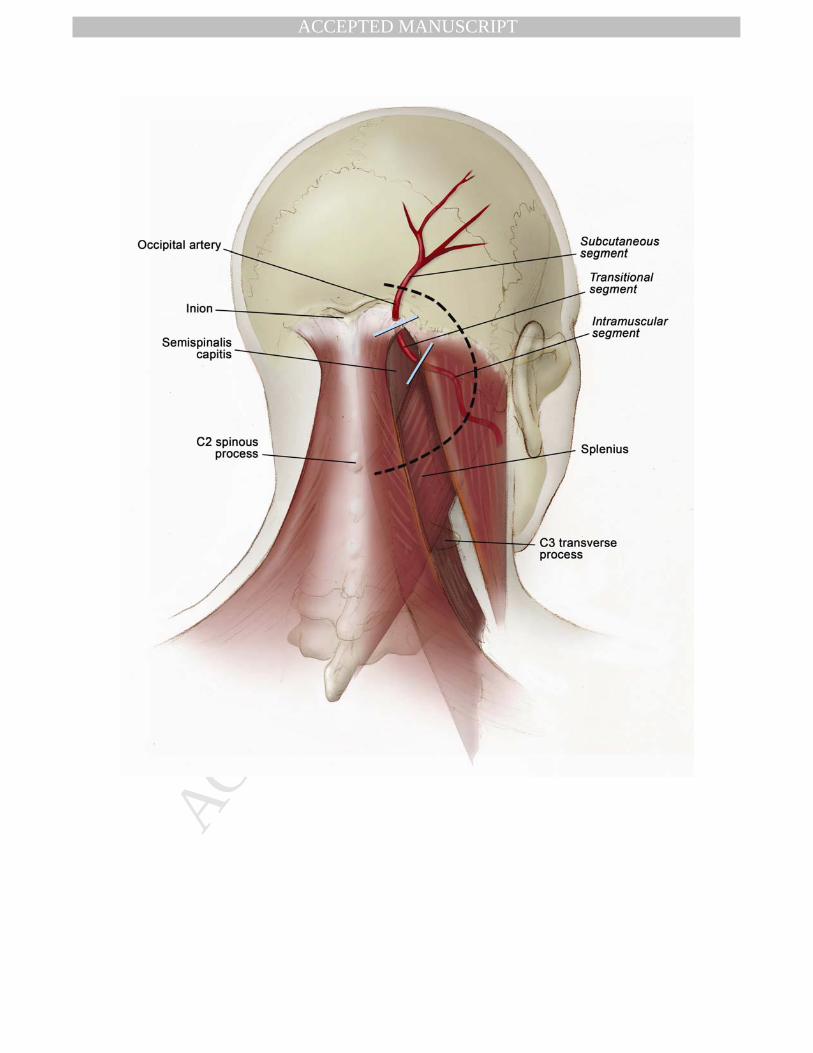
Figure 1. Skin incisions utilized to harvest the occipital artery. (A) A hockey-stick shaped skin 336
incision used for the distal and proximal hockey stick approaches. (B) A novel reverse-C skin 337
incision. 338
339
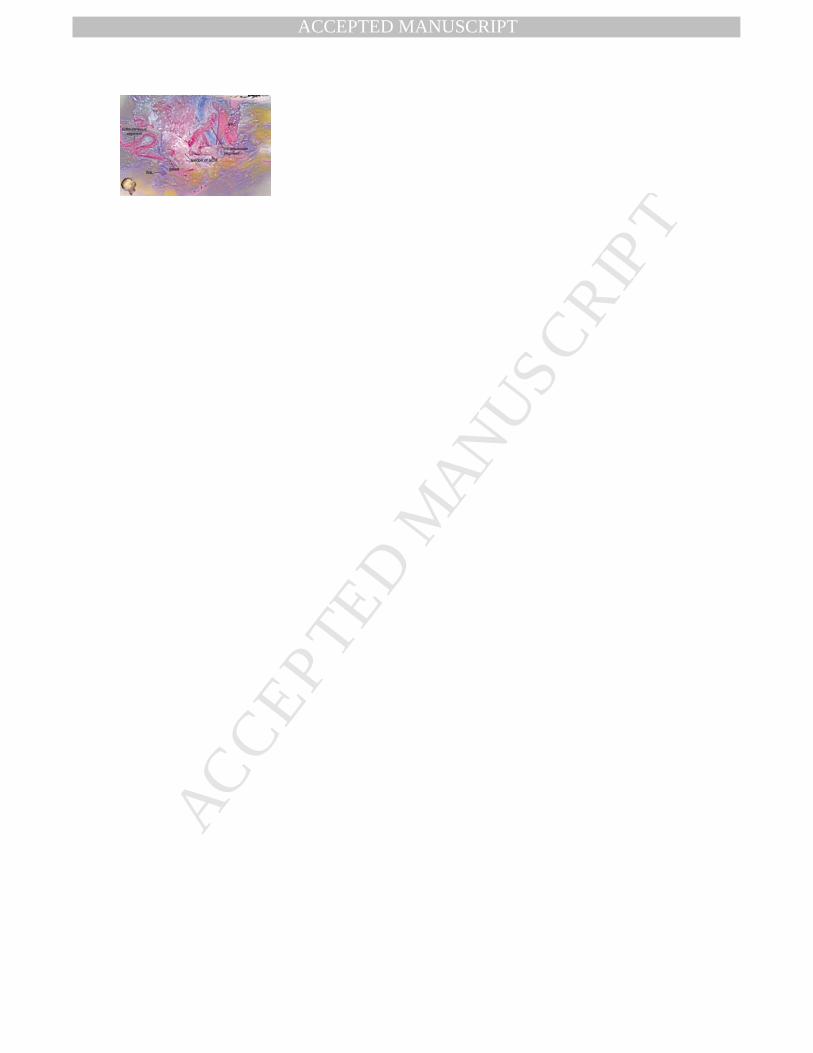
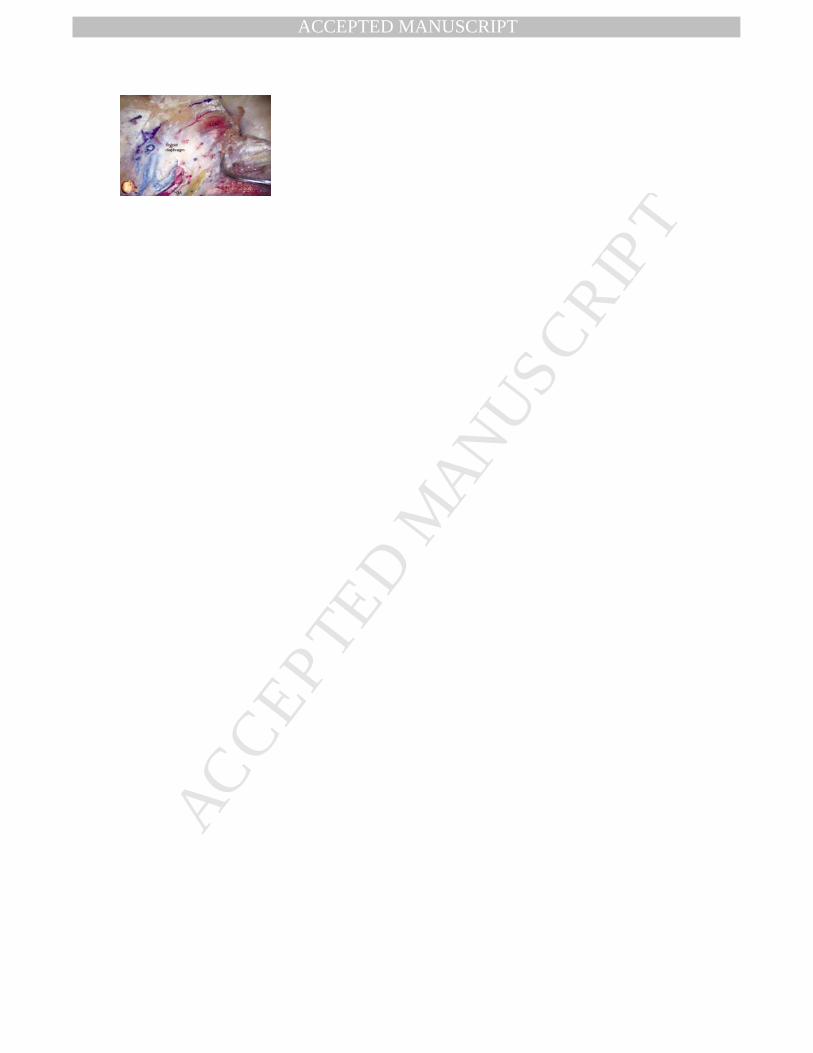
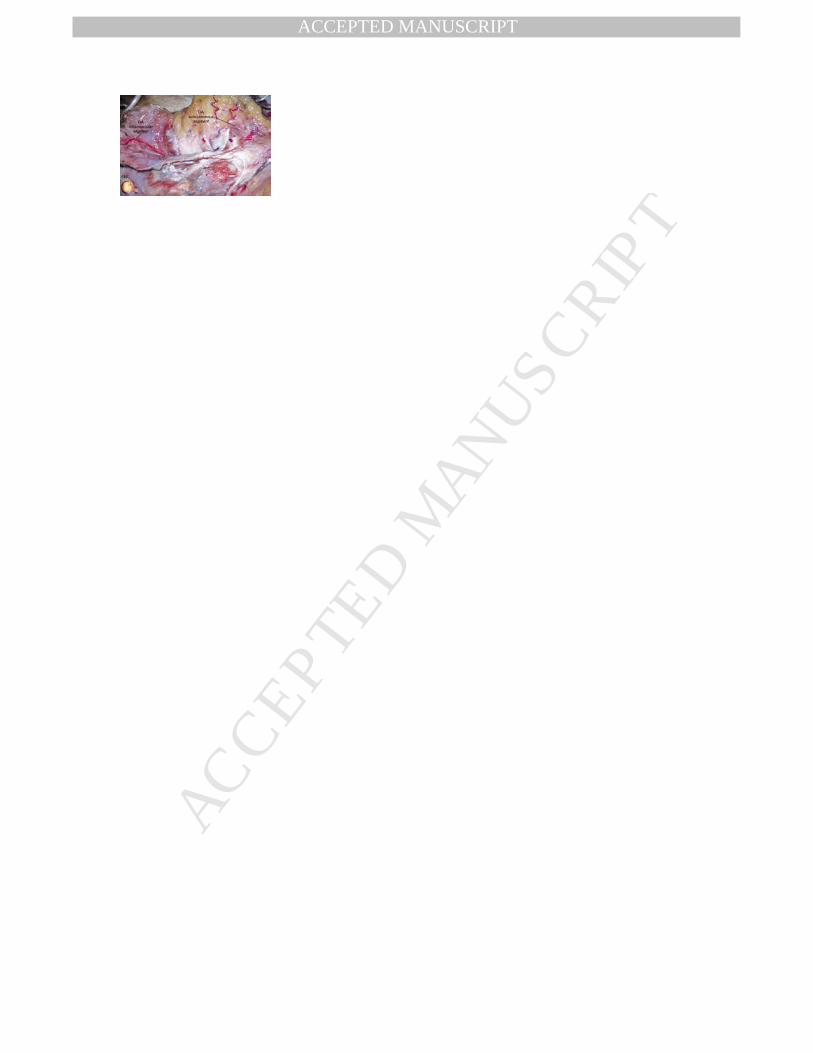
Figure 2. The scalp and the subcutaneous tissue were removed from the suboccipital region to 340
reveal the course of the OA harvested for the posterior fossa bypass. (A) The right OA is exposed 341
and divided into three practical segments; subcutaneous, transitional, and intramuscular. The 342
solid black lines indicate borders between each segment. The SNL is depicted with the purple 343
marking line. The SCM is removed and the SPC is incised in the middle to reveal the underlying 344
intramuscular segment of the OA. (B) The OA pierces the galea aponeurotica and the tendon of 345
the SCM in the transitional segment. The galea and the tendon of the SCM are partly left around 346
the OA. OA, occipital artery; SCM, sternocleidomastoid muscle; SNL, superior nuchal line; 347
SPC, splenius capitis muscle; SSC, semispinalis capitis muscle. 348
349
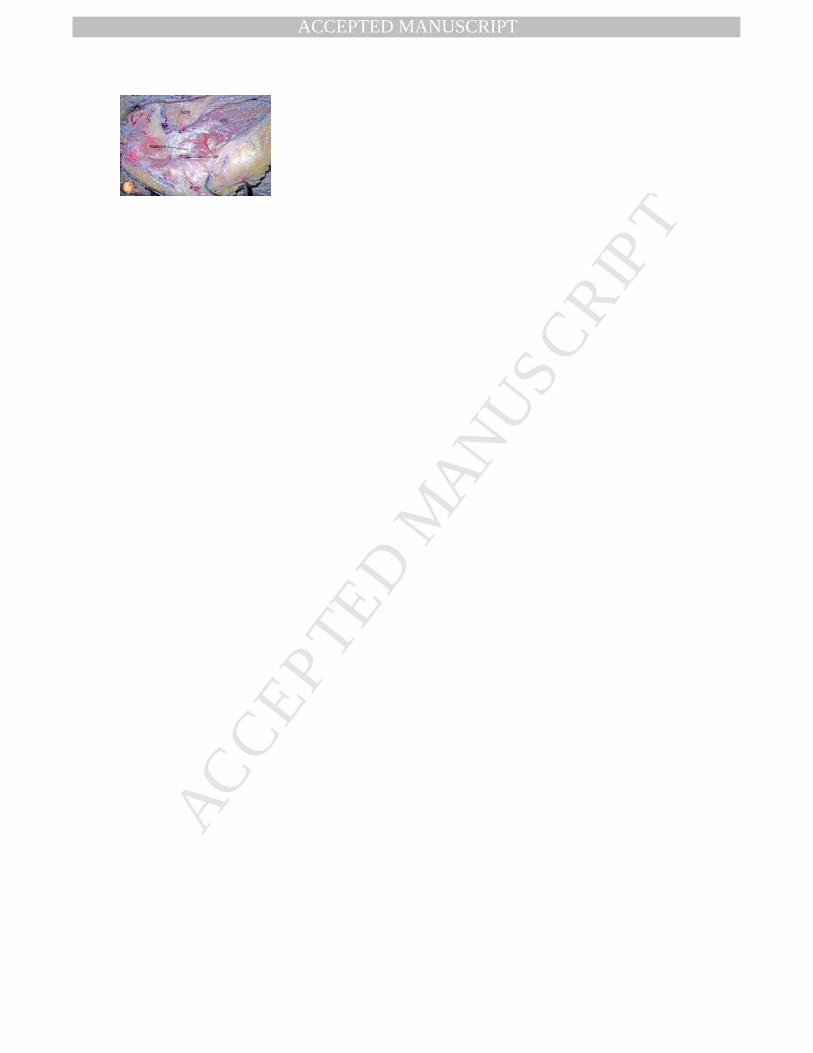
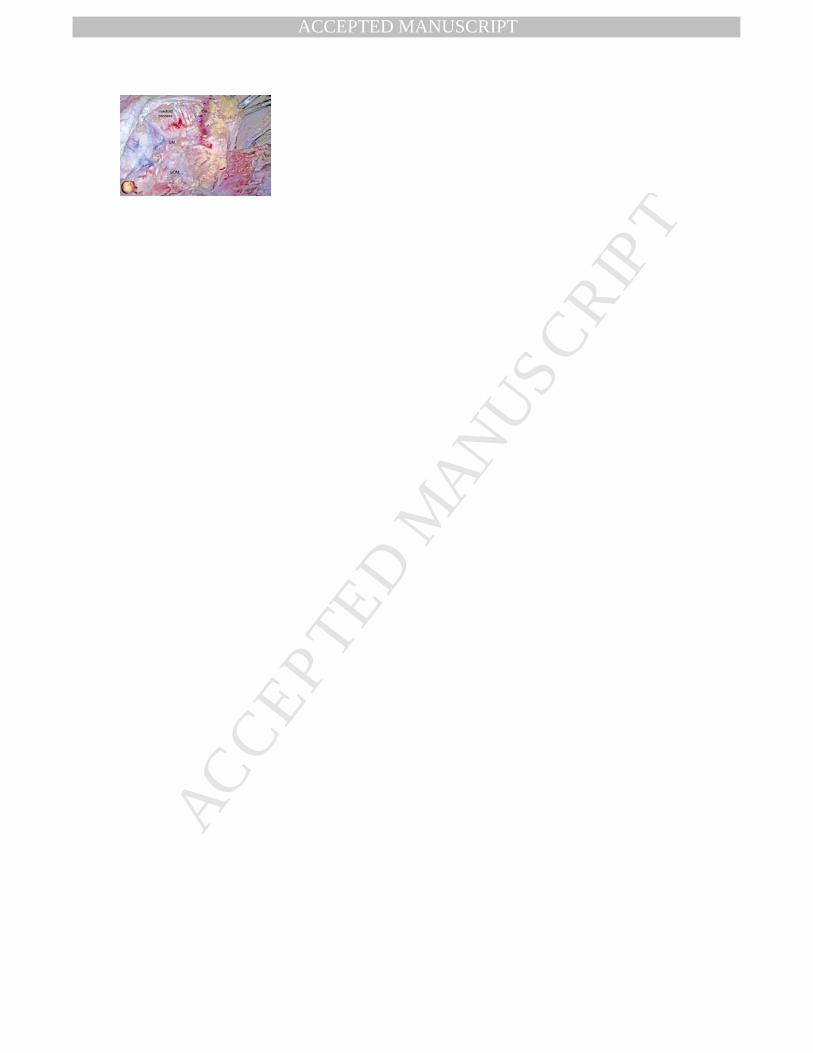
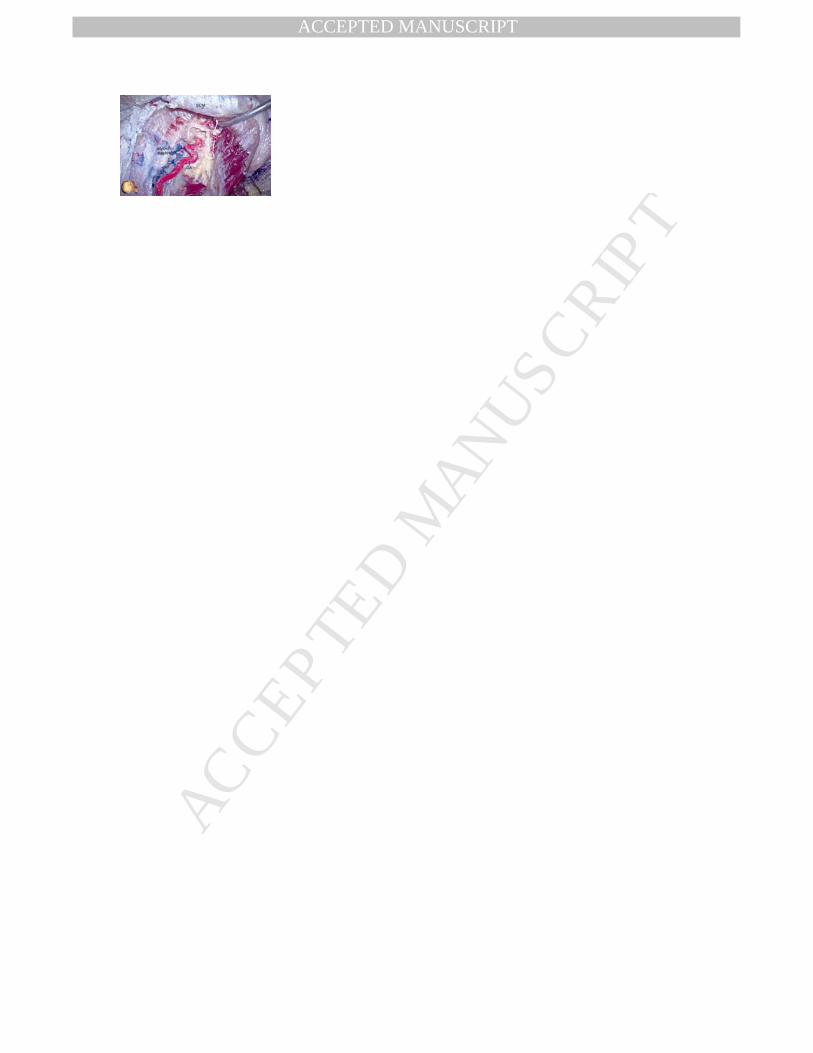
Figure 3. Stepwise harvesting of the OA using a distal hockey-stick approach. (A) A U-shaped 350
skin incision was made above the superior nuchal line. The distal end of the OA is ligated and 351
cut. The scalp flap is detached from the bone and reflected inferiorly, followed by dissection of 352
the occipital muscle and the galea aponeurotica to reveal the subcutaneous segment of the OA. 353
(B) The skin incision is extended along the mastoid process and the scalp flap is retracted 354
medially. The SNL, SCM, and SPC are exposed in that order. (C) The transitional segment of the 355
OA; surrounded by the tendon of the SCM (large black dashed line), the SPC (small dashed 356
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 18
line), and the SNL (blue dashed line); is carefully exposed. The arrow indicates the corner 357
between the lateral edge of the tendon of the SCM and the superior border of the SPC where the 358
transitional segment of the OA is located. (D) A specimen demonstrating a more medial course of 359
the OA is shown. Here, the OA is covered by the tendon of the trapezius muscle instead of that of 360
the SCM. (E) The SCM is detached from the suboccipital bone (bluish marking) and is reflected 361
anteriorly. The attachment of the SPC to the mastoid process is exposed (arrowheads). (F) The 362
SPC is detached from the mastoid process and reflected inferiorly. The OA is observed running 363
in a single fatty connective tissue layer, termed the styloid diaphragm. (G) The OA is partly 364
harvested from the styloid diaphragm. In this case, the proximal part of the OA together with the 365
styloid diaphragm is covered by the longissimus capitis muscle (LCM), which is subsequently 366
detached. (H) Dissection of the OA is completed. The anatomical proximity of the proximal end 367
of the harvested OA to the digastric muscle (DM) and the superior oblique capitis muscle (SOM) 368
is notable. OA, occipital artery; SCM, sternocleidomastoid muscle; SNL, superior nuchal line; 369
SPC, splenius capitis muscle; SSC, semispinalis capitis muscle; LCM, longissimus capitis 370
muscle; DM, digastric muscle; SOM, superior oblique capitis muscle. 371
372
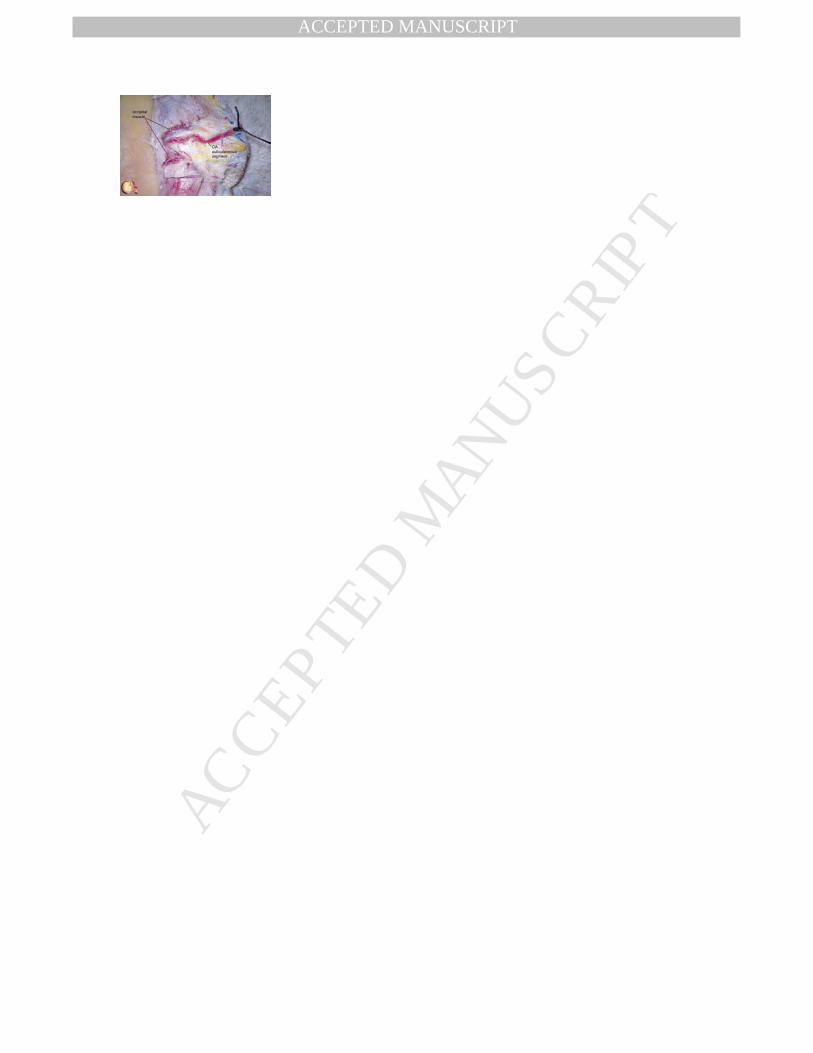
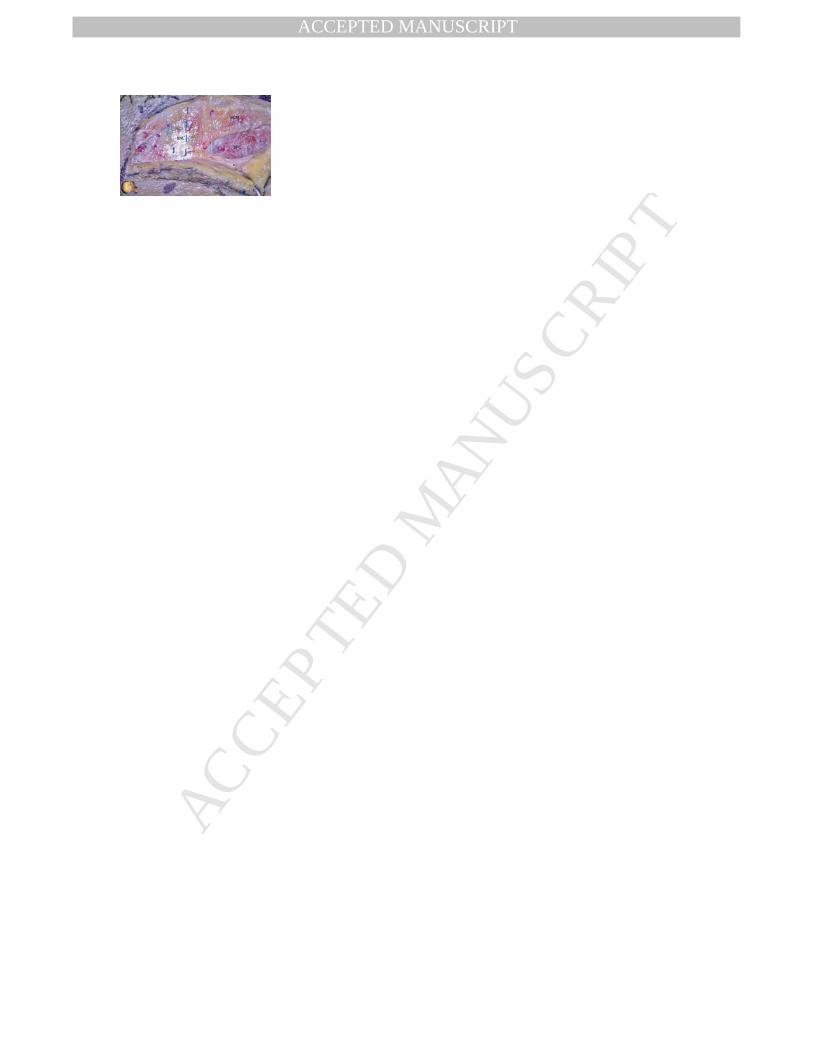
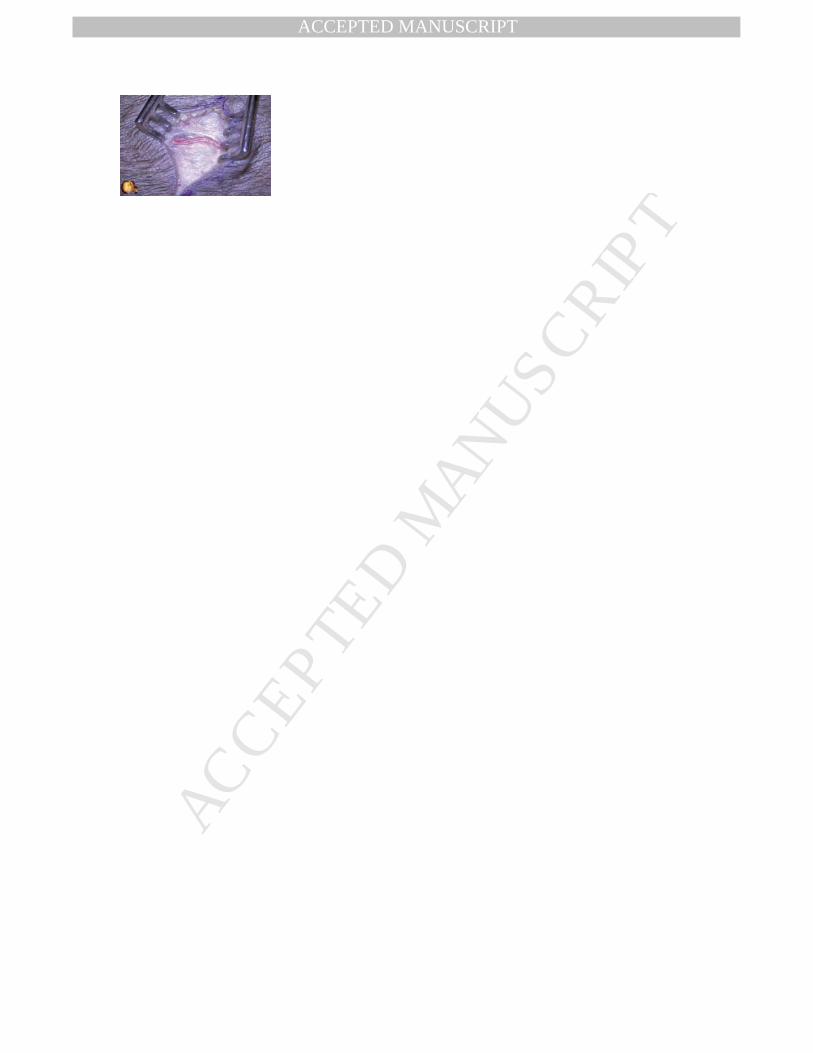
Figure 4. Stepwise harvesting of the OA using a proximal hockey-stick approach. (A) A straight 373
skin incision is made along the mastoid process. The SNL (blue dashed line), SCM, and SCM are 374
exposed in that order. The medial edge of the skin incision stops just before the distal end of the 375
OA in order to preserve blood flow during dissection of the intramuscular segment. (B) The scalp 376
flap is further retracted medially to expose the lateral edge of the tendon of the SCM (large black 377
dashed line), the superior border of the SPC (small black dashed line), and the transitional 378
segment of the OA. (C) The SCM and the SPC are detached from the occipital bone and 379
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFukuda, 19
retracted anteriorly and inferiorly, respectively. The intramuscular segment of the OA is 380
harvested from the styloid diaphragm. In this specimen, the OA and the styloid diaphragm are 381
located above the LCM. (D) After the intramuscular and transitional segments of the OA are 382
exposed, the distal end of the subcutaneous segment of the OA is severed. The scalp-muscle flap 383
is detached from the occipital bone and reflected inferiorly. The undissected subcutaneous 384
segment of the OA is partially visible through the galea aponeurotica (arrow). (E) The proximal 385
hockey-stick approach is completed by dissection of the subcutaneous segment of the OA from 386
the reverse side. OA, occipital artery; SCM, sternocleidomastoid muscle; SNL, superior nuchal 387
line; SPC, splenius capitis muscle; LCM, longissimus capitis muscle. 388
389
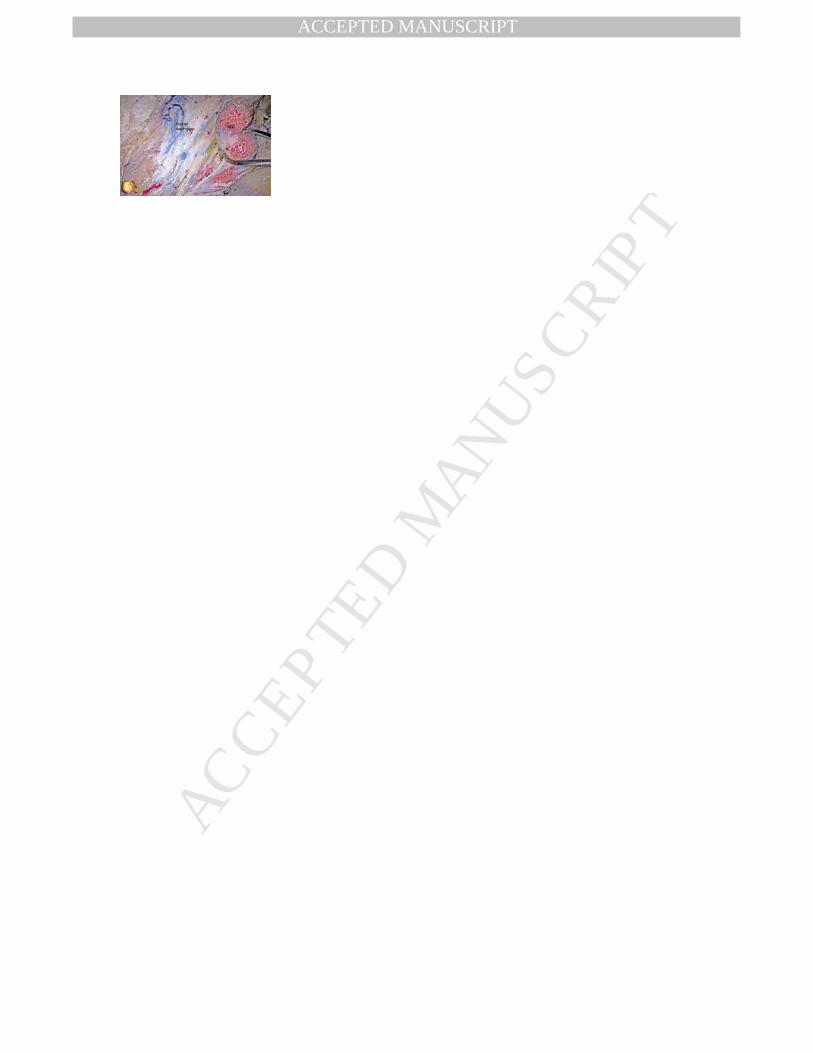
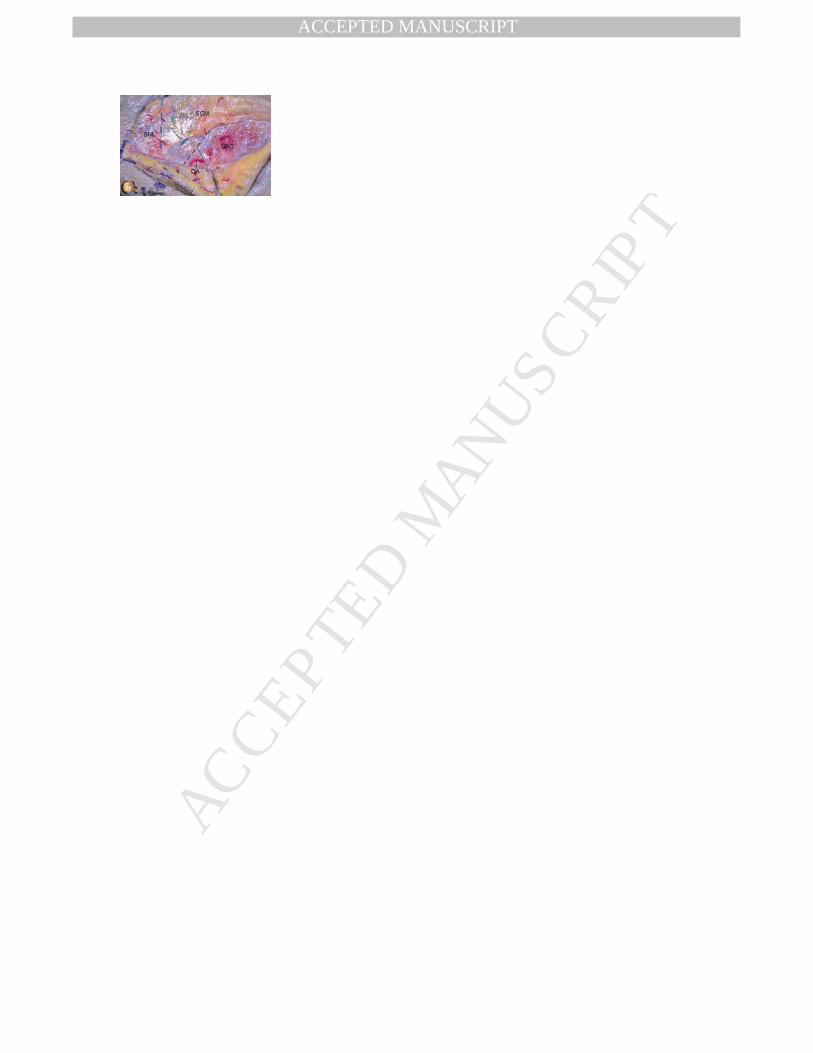
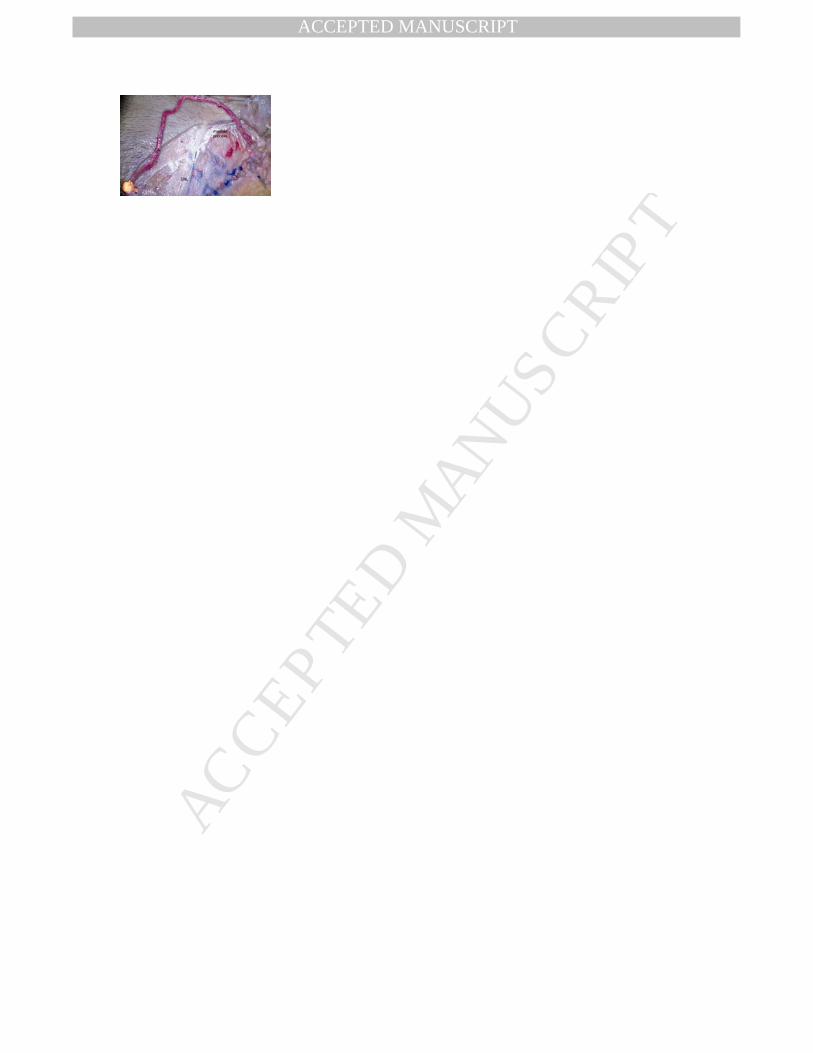
Figure 5. A right OA is harvested through a novel reverse-C skin incision. (A) The distal end of 390
the subcutaneous segment of the OA is exposed under a transverse skin incision. (B) The 391
superior half of the reverse-C skin incision is completed. The distal end of the subcutaneous 392
segment of the OA and the SCM are exposed. (C) The whole skin incision is completed and the 393
scalp flap is retracted medially. The transitional segment of the OA is identified by following the 394
OA, as well as the lateral edge of the SCM (large black dashed line) and the superior edge of the 395
SPC (small black dashed line). The SNL is indicated by the blue dashed line. (D) The 396
intramuscular segment of the OA is dissected off of the styloid diaphragm. (E) The full length of 397
the dissected OA is moved anteriorly out of the craniotomy site with continuity of the OA at the 398
distal end of the scalp spared, keeping blood flow intact until the recipient vessel is prepared. 399
OA, occipital artery; SCM, sternocleidomastoid muscle; SNL, superior nuchal line; SPC, 400
splenius capitis muscle. 401
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Abbreviations OA, occipital artery PICA, posterior inferior cerebellar artery SCM, sternocleidmastoid SNL, superior nuchal line SPC, splenius capitis muscle SSC, semispinalis capitis muscle
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 1. Qualitative Summary of the Different Approaches Used to Harvest the OA.
Method Exposure of Transitional Segment OA Patency Surgeon's Familiality
Hockey-stick, distal + ± +
Hockey-stick, proximal ± + +
Reverse-C ++ ++ ±
OA, occipital artery; ++, very good; +, good; ±, fair.




















