
Neonatal Skin Care: Clinical Outcomes of the AWHONN/NANN Evidence-Based Clinical Practice Guideline
11
J OGN N CLINICAL STUDIES Neonatal Skin Care: Clinical Outcomes of the AW0N"RT Evidence-Bused Clinical Practice Guideline Carolyn €3. Lund, RN, MS, FAAN, Jason Y% Osborne, PhD, Joanne Kuller, RN, MS, Alfred T. Lane, MD, FAAP, Judy Wright Lott, RNC, DNS, NNP, Deborah A. Raines, PhD, RNC = Objective: To test the effectiveness of an evi- dence-based clinical practice guideline for neona- tal skin care on selected clinical outcomes for new- borns in neonatal intensive-care units (NICU), special-care units (SCU), and well-baby nurseries. Design: Prospective evaluation of the collab- orative neonatal skin care research-basedpractice project of the Association of Women's Health, Obstetric and Neonatal Nurses and the National Association of Neonatal Nurses. Setting: NlCU and well-baby units in 51 hos- pitals located throughout the United States. Participants: Member site coordinators (N = 51) and the neonates (N= 2,820) observed during both the pre- and postimplementationphases of the project. Method: Site coordinators received special- ized education in neonatal skin care and implement- ed an evidence-based clinical practice guideline addressing 10 aspects of neonatal skin care. Base- line observations of skin condition, care practices, and environment of newly admitted neonates were collected by site coordinators. Postimplementation observations were then completed. Main Outcome Measures: Skin condition was assessed with the Neonatal Skin Condition Score (NSCS), which ranges from a score of three (best condition) to a score of nine (worst condition), based on dryness, erythema, and skin breakdown. Changes in frequency of selected skin care prac- tices were used to assess the effectiveness and fea- sibility of using the practice guideline in everyday clinical practice. Aspects of the care environment with potential effect on skin integrity were moni- tored to determine risk factors. Results: Fifty-one site coordinators made 1 1,468 systematic assessments of 2,464 NlCU and SCU newborns and 356 well newborns. Baseline skin scores were better in well newborns compared with premature newborns. After implementation of the guideline, skin condition was improved, as reflected by less visible dryness, redness, and skin breakdown in both the NICU/SCU and well new- borns. The guideline was integrated into care, as evidenced by increased use of emollients, particu- larly with premature infants, and decreased fre- quency of bathing. A relationship was shown between selected aspects of the environment and alterations in skin integrity. Conclusions: Use of the AWHONN/NANN Neonatal Skin Care Research-Based Clinical Prac- tice Guideline was successfully implemented at 51 sites, and effectiveness was demonstrated by changed care practices and improved skin condi- tion in premature and full-term newborns. The results of this project support a wider dissemination of the project's practice guideline for neonatal skin care. JOGNN, 30,41-51; 2001. Keywords: Neonatal skin care-Neonatal skin care evidence-based practice-Neonatal skin integrity Accepted: November 2000 January I February 2002 JOGNN 42
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Neonatal Skin Care: Clinical Outcomes of the AWHONN/NANN Evidence-Based Clinical Practice Guideline

J OGN N CLINICAL STUDIES
Neonatal Skin Care: Clinical Outcomes of the A W 0 N " R T Evidence-Bused Clinical Practice Guideline Carolyn €3. Lund, RN, MS, FAAN, Jason Y% Osborne, PhD, Joanne Kuller, RN, MS, Alfred T. Lane, M D , FAAP, Judy Wright Lott, RNC, DNS, NNP, Deborah A. Raines, PhD, RNC
= Objective: To test the effectiveness of an evi- dence-based clinical practice guideline for neona- tal skin care on selected clinical outcomes for new- borns in neonatal intensive-care units (NICU), special-care units (SCU), and well-baby nurseries.
Design: Prospective evaluation of the collab- orative neonatal skin care research-based practice project of the Association of Women's Health, Obstetric and Neonatal Nurses and the National Association of Neonatal Nurses.
Setting: NlCU and well-baby units in 51 hos- pitals located throughout the United States.
Participants: Member site coordinators (N = 51) and the neonates (N= 2,820) observed during both the pre- and postimplementation phases of the project.
Method: Site coordinators received special- ized education in neonatal skin care and implement- ed an evidence-based clinical practice guideline addressing 10 aspects of neonatal skin care. Base- line observations of skin condition, care practices, and environment of newly admitted neonates were collected by site coordinators. Postimplementation observations were then completed.
Main Outcome Measures: Skin condition was assessed with the Neonatal Skin Condition Score (NSCS), which ranges from a score of three (best condition) to a score of nine (worst condition), based on dryness, erythema, and skin breakdown. Changes in frequency of selected skin care prac- tices were used to assess the effectiveness and fea-
sibility of using the practice guideline in everyday clinical practice. Aspects of the care environment with potential effect on skin integrity were moni- tored to determine risk factors.
Results: Fifty-one site coordinators made 1 1,468 systematic assessments of 2,464 NlCU and SCU newborns and 356 well newborns. Baseline skin scores were better in well newborns compared with premature newborns. After implementation of the guideline, skin condition was improved, as reflected by less visible dryness, redness, and skin breakdown in both the NICU/SCU and well new- borns. The guideline was integrated into care, as evidenced by increased use of emollients, particu- larly with premature infants, and decreased fre- quency of bathing. A relationship was shown between selected aspects of the environment and alterations in skin integrity.
Conclusions: Use of the AWHONN/NANN Neonatal Skin Care Research-Based Clinical Prac- tice Guideline was successfully implemented at 51 sites, and effectiveness was demonstrated by changed care practices and improved skin condi- tion in premature and full-term newborns. The results of this project support a wider dissemination of the project's practice guideline for neonatal skin care. JOGNN, 30,41-51; 2001.
Keywords: Neonatal skin care-Neonatal skin care evidence-based practice-Neonatal skin integrity
Accepted: November 2000
January I February 2002 JOGNN 42

The skin, of vital importance to newborns, provides a barrier to microorganisms and toxins, assists in ther- moregulation, and facilitates communication through the tactile senses. Maintaining an intact skin barrier is necessary during the adaptation from intrauterine to extrauterine life for all newborns but is particularly challenging for premature and full-term newborns who require intensive or special care. The skin is subject to potential disruption and trauma during clinical prac- tices such as bathing (Gfatter, Hackl, & Braun, 1997; Morelli & Weston, 1987; Tupker, Pinnagoda, Coen- raads, & Nater, 1990), use of antimicrobial skin disin- fectants (Harpin & Rutter, 1982; Schick & Milstein, 1981), and adhesive application and removal (Harpin & Rutter, 1983; Lund et al., 1997).
_________ ____ __
T h e aim of this study was to test the impact of
the project guideline on patient outcomes,
specifically skin condition and changes in
selected skin care practices.
A significant body of research is available about neo- natal skin development and physiology, as well as care practices for both premature and full-term newborns (Lund, Kuller, Lane, Lott, & Raines, 1999). Recogniz- ing both the recent advances and heightened interest for evidence-based skin care practices, the Association for Women's Health, Obstetric and Neonatal Nurses (AWHONN) and the National Association of Neona- tal Nurses (NANN) collaborated to support the Neonatal Skin Care Research-Based Practice Project (RBP4).
The project included four phases. Phase 1, planning, involved developing an evidence-based clinical practice guideline and an evaluation plan including data collec- tion tool development and data management. Phase 2, implementation, entailed recruiting and training of site coordinators, implementing the guideline at the select- ed sites, and assessing pre- and postguideline skin con- dition and collecting data about care practices. Phase 3, evaluation, included analyzing data, disseminating project and individual site results to participating sites, interpreting positive implications of project results, and identifying potential barriers to implementing the guideline in clinical practice. Phase 4, dissemination, is constructed during Phase 3 and represents the ongoing organizational program to continue to advance neona- tal skin care evidence-based practice through educa- tional activities and products.
The aim of this study was to test the impact of the project guideline on patient outcomes, specifically skin condition and changes in selected skin care practices. This report is based on the systematic observations and assessments made by site coordinators before and after implementing the project guideline.
Hypotheses The project science team identified three research
questions: (a) Will nurses change clinical practices after receiving education and implementing an evidence- based clinical practice guideline? (b) Will patient out- comes be positively affected by the use of an evidence- based clinical practice guideline in the setting of the neonatal intensive-care unit (NICU), special-care unit (SCU), and well-baby nursery? and (c) How does the caregiving environment influence skin integrity?
The following hypotheses related to clinical practice changes:
1. The frequency of bathing as recorded in the nursing record or by direct observation will be decreased after implementing the guideline.
2. The use of emollients as recorded in the nursing record will be increased after implementing the guideline.
The following hypotheses related to patient outcomes: 1. Full-term newborns will have better skin condition,
assessed by the Neonatal Skin Condition Score (NSCS), compared to premature neonates and neonates in the NICU and SCU.
2. Skin condition, assessed by the NSCS, will improve after implementing the neonatal skin care evidence- based clinical practice guideline.
3 . Premature newborns' postguideline NSCS will show greater improvement over time compared to their pre- guideline assessment.
4. There will be no increase in positive blood cultures dur- ing the period of observation after implementing the guideline.
The following hypothesis related to the caregiving
Care and environmental factors with potential for skin injury will be positively correlated with skin breakdown, as reflected by a higher NSCS.
environment:
Method The project involved developing an evidenced-based
clinical practice guideline addressing 10 areas of neona- tal skin care:
1. assessment 2. bathing 3 . emollients 4. adhesives 5. disinfectants
42 JOG" Volume 30, Number 1

TABLE 1 Highlights of the Neonatal Skin Care Research- Based Clinical Practice Guideline
Bathing
Emollients
Disinfectants
Adhesives
TEWL
Cord care
Decrease frequency, neutral pH cleansers, water only for infants weighing less than 1,000 g
Aquaphor ointment twice daily for infants less than 32 weeks during first 2 4 weeks; use as needed for dryness in other patients
remove completely after procedure; isopropyl alcohol use discouraged because less effective, drying to skin
use gelled electrodes; avoid solvents and bonding agents
For infants younger than 30 weeks gestational age, select high humidi- ty (>70%), transparent dressings, or Aquaphor ointment to reduce evaporative water and heat loss; use incubators, supplemental con- ductive heat to avoid drying effects of radiant warmers; measure humi- dity routinely
Routine use of isopropyl alcohol not recommended
Povidone-iodine or chlorhexidine,
Minimize use as much as possible;
6. control of transepidermal water loss 7 . prevention and treatment of skin breakdown 8. diaper dermatitis 9. umbilical cord
10. circumcision care
Content highlights from the skin care guideline are list- ed in Table 1. Volunteer site coordinators, after special training, introduced and evaluated the guideline in 5 1 intensive care, special care, and well-baby nurseries.
Because the evidence-based skin care interventions were based on previously reviewed and published re- search, the guideline was considered a standard of care and not an experimental intervention. Institutional re- view board approval was not required in most settings, although a few of the participating sites did obtain approval and parental consent. Many sites considered this project under the purview of a quality improve- ment project and introduced their participation during unit-based quality improvement committee meetings. The data collection was then considered an audit of patient care following implementation of selected changes in practice.
Evaluation included collecting information about the skin condition, care environment, and other influ- ences on skin integrity such as medications, nutrition, and climate. Site coordinators were instructed to make
TABLE 2 The Neonatal Skin Condition Score (NSCS)
Dryness 1 = normal, no sign of dry skin 2 = dry skin, visible scaling 3 = very dry skin, cracking/fissures
1 = no evidence erythema 2 = visible erythema 40% body surface 3 = visible erythema >SO% body surface
1 = none evident 2 = small localized areas 3 = extensive
Erythema
Breakdowdexcoriation
Note. Perfect score = 3; worst score = 9.
twice-weekly observations of newly admitted patients to their units over an 8-week period before the site co- ordinators’ training session, using the following tools:
Patient demographic tool: to collect basic demo- graphic information about the patients being observed, including birth weight, gestational age, race, and diag- nosis for each of the patients that were observed.
Twice-weekly skin assessment tool: provided a “snapshot” of newborn skin condition and daily care practices. Skin condition was assessed using the NSCS, which uses a 9-point scale addressing skin dryness, ery- thema, and breakdown (see Table 2). The scoring sys- tem was adapted from a visual scoring system used in a previous study (Lane & Drost, 1993). The following were also recorded: microclimate, including use and type of heating devices, humidity, and temperature; details of care with potential impact on skin condition; and bathing and emollient use, as documented in nurs- ing progress record in the previous 24 hours to deter- mine adherence to the guideline. Nutrition delivered to NICU and SCU patients not receiving significant enter- a1 nutrition was documented, including parenteral pro- tein, fat, and trace minerals. Blood and skin cultures were reported, with the type of organisms identified.
A second period of observation of newly admitted patients occurred after the site coordinators imple- mented the skin care guideline in their individual units. Each site was to include at least 30 patients during both observation periods, before and after the implementa- tion of the guideline. Each infant was observed twice weekly for as long as he or she was hospitalized, end- ing when discharged or transferred to another hospital or at the end of the 8-week observation period. The
January I February 2001 JOG” 43

interval between observations was at the discretion of the site coordinator. Some infants had as many as 16 observations recorded, whereas others were observed once or twice. The well-baby population was usually observed twice, on 2 consecutive days, due to their lim- ited hospital stays.
A simplified Twice Weekly Skin Assessment Form was provided for the well-baby sample. The form was stream- lined to facilitate data collection, as fewer monitoring devices and other treatments are used by this popula- tion. The goal was to assess the skin condition of the well-baby sample at least twice during their brief hos- pitalizations; the observations were generally 24 hours apart. NICU or SCU infants also could be ob-served using this simplified form if their clinical condition was relatively uncomplicated, such as newborns with diag- noses that would “rule out” sepsis or hyperbilirubinemia.
Analysis Data analysis proceeded in several stages. First, as
each infant’s data were entered, they were checked for errors. Initial data cleaning such as checking for out-of- range values was performed. Second, preliminary descriptive statistics were generated, and the two sam- ples were checked for similarity on descriptive variables via analysis of variance (ANOVA) and chi-square tests. Third, tests of the intervention were performed, also using ANOVA tests. Finally, repeated measures ANOVA were performed to examine differences in the change in skin condition over time across the preinter- vention and postintervention assessments.
Results
collection before data were analyzed for this report). The number of assessments for each NICUlSCU
infant ranged from 1 to 16 (the maximum allowed), with a median of 4 and a mean of 4.8, Because two observations were allowed each week, the maximum number of weeks that an infant could be observed was 8 weeks. The initial assessment was conducted during the 1st week of hospitalization at the site coordinator’s discretion. The number of assessments for each well baby ranged from 1 to 8, with only 5% of the sample having more than 3 assessments. There were 11,468 observations in the NICU sample and 628 observations in the well-baby sample.
Sample Demographics In the sample as a whole, there were 1,467 male
infants and 1,315 female infants. The racial makeup of the sample was 60.2% white, 18.6% African Ameri- can, 13.8% Latino/a, 2.4% Asian, 0.1% Native Amer- ican, 0.4% Pacific Islander, 3.2% multiracial, and 1.4% other.
The birth weights of the entire sample ranged from 500 to 5,700 g (M = 2,110 g). The breakdown of NICU/SCU infants by weight is included in Table 4. Mean gestational age for the NICUlSCU sample was reported as 33 weeks (range 20-42 weeks) by either examination or dates.
Primary diagnoses included prematurity (67.6%), respiratory distress syndrome (46.1 YO), and sepsis (22.7%). Other diagnoses identified were meconium aspiration, congenital malformation, congenital heart defects, seizures, birth depression, apnea, necrotizing enterocolitis, and pneumonia,
To check for differences in the pre- and postguideline samples, a multivariate analysis of variance (MANOVA) tested for mean differences between the two groups. No significant differences were observed in age, birth weight, gestational age at birth, sex ratio, or race. Sig- nificant differences were found only in the maternal administration of antenatal steroids and number of diagnoses per infant, both of which were higher in the
Sample A total of 2,820 infants were included in the analy-
sis, including 2,464 in the NICU and SCU and 356 in the well-baby nursery (see Table 3). Included in this analysis were 56 sites in the preguideline set and 51 in the postguideline set ( 5 sites did not complete the data
TABLE 3
-
preintervention (or preguideline) group ( p < .05).
Number of Infants and Assessments Included in Project
All Infants NZCU Infunts NICU Assessments Well-Baby Participants Well-Baby Assessments Preguideline 1,371 1,234 5,222 137 258 Postguideline 1,449 1,230 6,246 219 370 Total sample 2,820 2,464 11,468 356 628
Note. NICU = neonatal intensive-care unit.
44 JOG” Volume 30, Number 1
TABLE 4 Breakdown of Neonatal Intensive-Care Unit Sample by Weight
Birth Weight (g)
, 5 1,000 1,001-1,500 1,50 1-2,000 2,001-2,500 2,501-3,000 3,001-3,500 > 3,500
Number of Infants
n (%)
394 (14.0) 529 (18.8) 539 (19.1) 354 (12.6) 292 (10.4) 297 (10.5) 345 (12.2)
Skin Condition Scores: NICU Sample Skin condition was assessed using the NSCS. A score
of 3 indicates excellent skin condition, and a score of 9 indicates the most disrupted skin condition. Initial NSCS scores for all infants did not differ between the pre- and postguideline groups (3.68 vs. 3.63 in the complete sample). Therefore, any change in skin condi- tion over the period of observation can be related to the intervention (use of the guideline) rather than differ- ences in baseline skin condition.
The effect of using the skin care guideline on NICU/ SCU infants’ skin condition was analyzed using a 2 (pre- vs. postintervention) x 4 (time) repeated measures ANOVA. Participants with a total initial NSCS higher than 3 and with 4 or more observations (4 is the medi- an) were included in these analyses because of the need for repeated observations reflecting change over time. These infants had a higher baseline NSCS than the sam- ple as a whole, probably because of greater severity of illness or younger gestational age reflected in longer hospital stays.
Results of the analysis revealed significant changes in the NSCS over time (F = 104.53, p < .0001) and an interaction of group and time ( F = 6.69, p < .0001) (see Table 5 ) . These results indicated that, after implemen- tation of the evidenced-based skin care guideline, infants with disrupted skin conditions improved more rapidly compared with infants with disrupted skin con- ditions before use of the guideline.
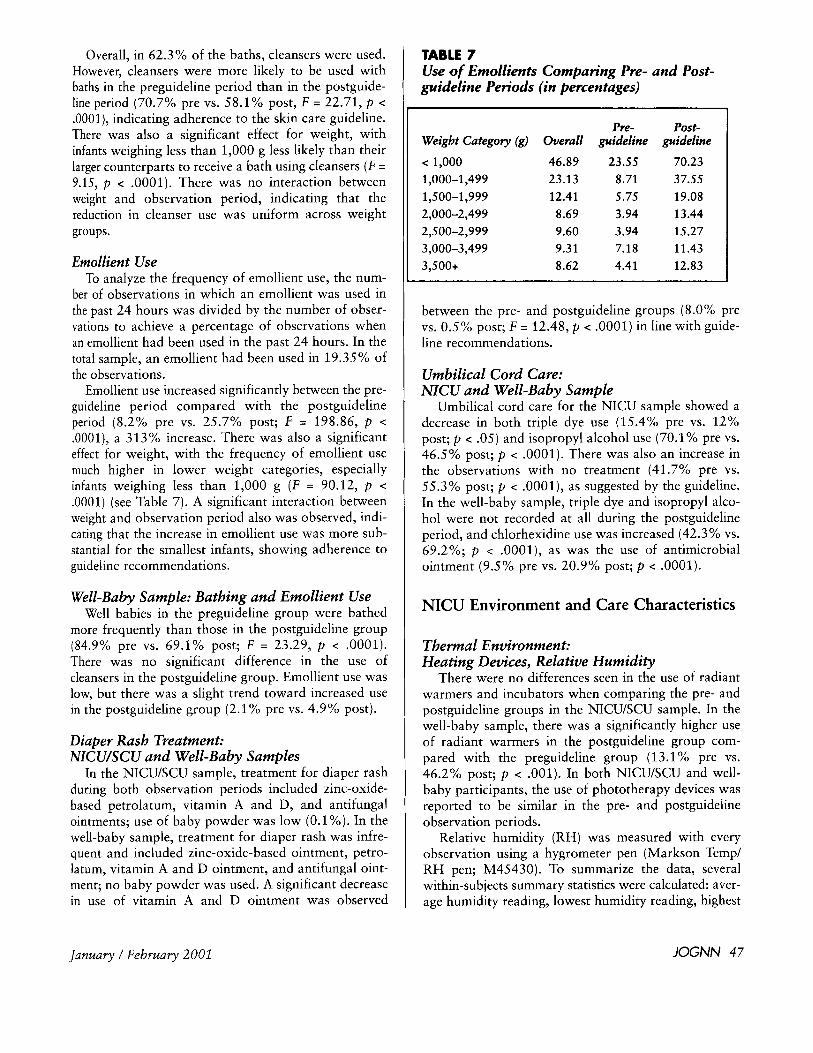
An analysis that extended to six time periods, or 3 weeks of twice-weekly observations, shows a similar pattern of improving skin condition as a result of using the guideline. In this sample, with more observation periods (but fewer participants), the postguideline group started with higher scores compared with the pre-guideline group (4.54 pre vs. 4.63 post) but had lower scores at the sixth observation period, by the 3rd
TABLE 5 Neonatal Skirr Condition Scores ( N S C S ) in Pre- a i d Postgtiicleliire Grotips With l-’our or More Obsewatioirs
Total
Preguideline 4.52 4.26 4.08 4.03 0.49 Postguideline 4.64 4.19 3.98 3.80 0.84
Note. 3 = best possible score; 9 = worst possible score.
Time 1 Time 2 Time 3 Time 4 Change
Change in Skin Condition Over First Three Weeks of Life
4.3
4.1
3.9
- Pre-guideline . I . Post-guideline
3 .7 - 3.5 ,
Observations I 2 3 4 5 6
FIGURE 1 Changes in Neonatal Skin Condition Scores over six obser- vations ( 3 weeks) in the NICU/SCU sample.
week of life (3.88 pre vs. 3.55 post; p < .001). Again, the skin care after the guideline was implemented resulted in improvement in skin condition, as reflected in lower NSCS (see Figure 1).
Furthermore, when an overall index of skin condi- tion is created by averaging NSCS scores across all observations, there is a trend toward average scores being better for infants in the postguideline group than those in the preguideline group (mean scores 3.82 pre vs. 3.74 post; F = 3.24, p < .07). There was also a trend for infants in the postguideline group to reach ideal skin condition (NSCS = 3) faster than those in the preguideline group (average of 3.30 observations vs. 3.61 observations; one-tailed significance level of p < .075).
The incidence of skin condition recidivism (skin scores worsened at some point during observation) also was analyzed. The ideal trend would be a continually decreasing NSCS toward 3.0, but some infants showed worsening scores at some point during the observation. There was a significant difference in recidivism rates between the pre- and postguideline groups, with infants in the postguideline group less likely to show worsen- ing of skin scores than infants in the preguideline group (50.0% pre vs. 41.1% post; F = 3.85, p < .05).
January I February 2001 JOGNN 45

Analyses of infants less than 1,000 g with scores greater than 3 (90 in the preguideline group and 11 1 in the postguideline group) revealed results similar to those for the complete sample, with significant changes in skin scores over time ( F = 14.79, p < .0001), no main effect of group membership in initial scores ( F < 1, not significant), and an interaction of changes in total skin scores over time and group membership ( F = 4.77, p c .03). Before implementation, the skin score dropped from 4.86 to 4.74 after two observations. However, after the guideline was implemented, the skin score dropped more significantly from 4.90 to 4.48.
T h e primary cause of skin breakdown
was listed as adhesives, followed by diaper
rash, friction, thermal burns, infection,
birth injury, and chemical burns due to
intravenous infiltrates.
Skin Condition: Location, Cause, and Treatment of Breakdown
The most common location for skin breakdown in the NICU/SCN sample was on the extremities for both the pre- and postguideline groups, followed by the front and back of the trunk and the face. The primary cause of breakdown was listed as adhesives in both groups, followed by diaper rash, friction, thermal burns, infection, birth injury, and chemical burns due to intravenous infiltrates. Other causes cited most often were attributed to heelsticks and other laboratory blood samples as well as intravenous-related injuries.
Treatment of skin breakdown most commonly was listed as ointment, followed by irrigation with normal saline and application of hydrophilic, hydrogel, and gauze dressings to a lesser extent. Other treatments included petrolatum-based ointment, antifungal oint- ment, and transparent adhesive dressings.
Skin Condition Scores: Well-Baby Sample A total of 356 well babies were included in the study.
Their mean NSCS was significantly lower in the post- guideline group compared with the preguideline group (3.68 pre vs. 3.5 post; p < .05). Seventy-three infants had skin assessment scores greater than 3, with 34 in the preguideline and 39 in the postguideline group com- pleting two observations. The infants in the postguide- line group showed greater improvement in skin scores
TABLE 4 Percentage of Observations With Documented Baths in Pre- Versus Postguideline Periods
Weight Categoty (g)
> 1,000 1,000-1,499 1,500-1,999 2,000-2,499
3,000-3,499 3,500+
2,500-2,999
Preguideline (%)
37.2 51.7 54.8 45.8 49.5 52.0 44.1
Postguideline (%I 28.6 37.4 46.5 45.1 44.6 44.5 40.2
during the two observation periods compared with infants in the preguideline group ( F = 4.77, p < .03). Infants in the preguideline group were more likely to have their skin condition worsen during their short hospital stays compared with those in the postguide- line group (30.6% pre vs.19.8% post; F = 5.30, p < .02).
The most common location for skin breakdown in the well-baby sample was on the extremities, followed by the back of the trunk, including the buttocks, and face. The most common cause of breakdown was dia- per rash, but the incidence was significantly reduced in the postguideline sample (18.2% pre vs. 8.8% post; p < .01). Other causes of breakdown included adhesives and friction.
Skin Care Routines
Bathing: NICU Sample The frequency of bathing was determined by the
number of times an infant was reported to have been bathed divided by the number of observations to deter- mine the percentage of observations in which the infant had been bathed in the past 24 hours. In the total sam- ple (pre- and postguideline groups), infants had been bathed within 24 hours of 45% of the observations.
There was a significant and substantial decrease in the frequency of bathing in the NICU sample between the preguideline period compared with the postguide- line period (48.4% pre vs. 40.7% post; F = 25.37, p c .0001). There was also a significant difference in fre- quency of bathing by weight group, with infants weigh- ing less than 1,000 g bathed substantially less frequent- ly than the infants in the other groups ( F = 9.18, p < .0001) (see Table 6). There was no interaction between weight group and observation period, indicating a decrease in frequency of bathing in all weight groups comparing the pre- and postguideline periods.
46 JOGNN Volume 30, Number 1
Overall, in 62.3% of the baths, cleansers were used. However, cleansers were more likely to be used with baths in the preguideline period than in the postguide- line period (70.7% pre vs. 58.1% post, F = 22.71, p < .0001), indicating adherence to the skin care guideline. There was also a significant effect for weight, with infants weighing less than 1,000 g less likely than their larger counterparts to receive a bath using cleansers ( F = 9.15, p < .0001). There was no interaction between weight and observation period, indicating that the reduction in cleanser use was uniform across weight groups.
Emollient Use To analyze the frequency of emollient use, the num-
ber of observations in which an emollient was used in the past 24 hours was divided by the number of obser- vations to achieve a percentage of observations when an emollient had been used in the past 24 hours. In the total sample, an emollient had been used in 19.35% of the observations.
Emollient use increased significantly between the pre- guideline period compared with the postguideline period (8.2% pre vs. 25.7% post; F = 198.86, p < .0001), a 313% increase. There was also a significant effect for weight, with the frequency of emollient use much higher in lower weight categories, especially infants weighing less than 1,000 g (F = 90.12, p < .0001) (see Table 7). A significant interaction between weight and observation period also was observed, indi- cating that the increase in emollient use was more sub- stantial for the smallest infants, showing adherence to guideline recommendations.
Well-Baby Sample: Bathing and Emollient Use Well babies in the preguideline group were bathed
more frequently than those in the postguideline group (84.9% pre vs. 69.1% post; F = 23.29, p < . O O O l ) . There was no significant difference in the use of cleansers in the postguideline group. Emollient use was low, but there was a slight trend toward increased use in the postguideline group (2.1% pre vs. 4.9% post).
Diaper Rash Treatment: NlCU/SCU and Well-Baby Samples
In the NICU/SCU sample, treatment for diaper rash during both observation periods included zinc-oxide- based petrolatum, vitamin A and D, and antifungal ointments; use of baby powder was low (0.1%). In the well-baby sample, treatment for diaper rash was infre- quent and included zinc-oxide-based ointment, petro- latum, vitamin A and D ointment, and antifungal oint- ment; no baby powder was used. A significant decrease in use of vitamin A and D ointment was observed
TABLE 7 Use of Emollients Comparing Pre- and Post- guideline Periods (in percentages)
Weight Cutegoy (g) Overall
< 1,000 46.89 1,000-1,499 23.13 1,500-1,999 12.41 2,000-2,499 8.69 2,500-2,999 9.60 3,000-3,499 9.31 3,500+ 8.62
Pre- guideline
23.55 8.71 5.75 3.94 3.94 7.18 4.41
Post- guideline
70.23 37.55 19.08 13.44 15.27 11.43 12.83
between the pre- and postguideline groups (8.0% pre vs. 0.5% post; F = 12.48, p < .0001) in line with guide- line recommendations.
Umbilical Cord Care: NICU and Well-Baby Sample
Umbilical cord care for the NICU sample showed a decrease in both triple dye use (15.4% pre vs. 12% post; p < .05) and isopropyl alcohol use (70.1% pre vs. 46.5% post; p < .0001). There was also an increase in the observations with no treatment (41.7% pre vs. 55.3% post; p < .0001), as suggested by the guideline. In the well-baby sample, triple dye and isopropyl alco- hol were not recorded at all during the postguideline period, and chlorhexidine use was increased (42.3% vs. 69.2%; p < .0001), as was the use of antimicrobial ointment (9.5% pre vs. 20.9% post; p < .0001).
NICU Environment and Care Characteristics
Thermal Environment: Heating Devices, Relative Humidity
There were no differences seen in the use of radiant warmers and incubators when comparing the pre- and postguideline groups in the NICU/SCU sample. In the well-baby sample, there was a significantly higher use of radiant warmers in the postguideline group com- pared with the preguideline group (13.1% pre vs. 46.2% post; p < .001). In both NICU/SCU and well- baby participants, the use of phototherapy devices was reported to be similar in the pre- and postguideline observation periods.
Relative humidity (RH) was measured with every observation using a hygrometer pen (Markson Temp/ RH pen; M45430). To summarize the data, several within-subjects summary statistics were calculated: aver- age humidity reading, lowest humidity reading, highest
January /February 2001 JOG" 47
humidity reading, and the variability in humidity read- ings, calculated as highest humidity reading minus the lowest humidity reading. Only infants with at least two humidity observations were included in this analysis.
In the NICUlSCU sample as a whole, mean RH de- creased between the pre- and postguideline groups (47.67% RH pre vs. 36.45% RH post; F = 525.32, p < .0001). This may have been related to seasonal varia- tions; the preguideline observations were collected dur- ing the spring and postguideline observations during the fall/winter seasons when hospital heating systems are used more consistently. In the well-baby sample, the mean RH decreased between the pre- and postguideline groups (39% pre vs. 29.55% post; F = 344.38, p < .0001), again probably reflecting seasonal variations.
Changes in humidity by weight group were observed, with significantly higher humidity readings in lower birth weight infants ( F = 27.07, p < .0001) (see Table 8). Because the guideline recommends using tents, hoods, or high-humidity incubators to control transepidermal water loss in the very low birth weight infants, this is the likely explanation for this difference. The use of high humidity (RH > 70%) in infants weigh- ing less than 1,000 g was reported as 16% in the pre- guideline period, increasing to 22% in the postguide- line period. However, the specific use of high humidity (RH > 70%) was not required in the guideline because alternative methods are available, such as the use of emollients or transparent adhesive dressings (Busta- mante & Steslow, 1989; Knauth, Gordin, McNelis, & Baumgart, 1989; Mancini, Sookdeo-Drost, Madison, Smoller, & Lane, 1994; Nopper et al., 1996; Vernon, Lane, Wischerath, Davis, & Menegus, 1990).
Therapeutic Intewen tions With Potential for Skin Inju y
A list of 15 interventions with potential for identifi- able skin injury was identified that included monitors, tubes, respiratory devices, intravascular devices, muscle paralysis, vasopressors, ostomies, and surgical wounds. In the NICU/SCU sample, infants had an average of 5 items recorded during both the pre- and postguideline observations. Table 9 shows the percentages of obser-
T h e positive outcomes from the large sample
of newborns assessed in this project support
the safety and efficacy of using the guideline
in daily skin care practices for neonates.
TABLE 8 Relative Humidity Readings in Neonatal lntensive-Care Unit/Special-Care Unit Sam- ple by Weight (in percentages)
Weight Category (g) < 1,000 1,000-1,499 1,500-1,999
2,500-2,999 3,000-3,499 3,500+
2,000-2,499
Overall 49.15 42.72 40.64 40.42 40.59 41.34 40.36
PW- guideline
52.89 48.34 46.27 46.80 47.26 47.91 47.07
Post- guideline
45.40 37.11 35.01 34.04 33.93 34.77 33.64
vations that included items on this list. The well-baby sample had fewer items reported, with the most com- mon items being electrocardiogram electrodes, pulse oximeters, and intravascular devices.
The number of devices was found to be significantly related to higher scores on the NSCS ( r = .14, p < .0001), increased recidivism (scores became higher at some point during the observation period ( r = .29, p < .0001), and increased number of locations for break- down and excoriation ( r = .30, p < .0001). These re- lationships remained after controlling for infant weight.
Infections: NICU/SCU Sample Sites reported blood cultures and skin cultures of all
participants in the pre- and postguideline observation periods. There were no significant differences between the pre- and postguideline groups in terms of positive blood cultures. Table 10 lists the organisms identified in blood cultures for the NICU sample. There were signif- icant differences in the number of positive blood cultures as a function of weight group (F = 44.87, p c .0001). Infants weighing less than 1,000 g had infection rates at least 10 times that of infants weighing more than 2,000 g, as might be expected for extremely premature infants.
There were more skin cultures reported in the post- guideline group compared with the preguideline group. Because the guideline recommended that skin cultures be obtained in infants with unexplained skin break- down or excoriations that appeared erythematous or with purulent exudate, the increase is viewed as a result of the application of guideline recommendations and does not indicate any increase in skin infections. Organisms reported in skin cultures included staphylo- coccus epidermidis, staphylococcus aureus, e. coli, klebsiella, pseudomonas, serratia, and candida albi- cam, reflecting the type of colonization seen in critical- ly ill neonates in the intensive-care environment.
48 lOGNN Volume 30, Number 1

TABLE 9 Therapeutic lnteruentions With Potential for Skin lnjury in Neonatal lntensive-Care Unit Sample
I
Inttvwution Total (%) Prcgrrideline (%) Postgnidcline (%) P EKG electrode-gel 93.9
Peripheral venoudarterial catheter 74.5 Pulse oximeter probe $7.8
Temperature probe 72.3 NasogastidOG tube 61.5 Umbilical catheter 40.4 E l T 36.2 Central venous catheter 22.2 Nasal cannula 21.1 Nasal CPAP 16.5 Vasopressor 10.2 EKG electrode: regular 9.7 Transcutaneous monitor 8.9 Surgical wound 6.6 Urine bag 3.0 Pancuronium or vecuronium use 2.0 Ileostorny 0.8 Castrostorny 0.4
Total 5.68 Tracheostorny 0.2
(median = 5)
Note. Total N for this analysis I 2,369. EKG = electrocardiogram.
*p < .w1.
91.8 87.1 73.6 71.6 60.5 40.8 37.1 19.2 22.2 15.6 10.4 10.5 8.9 6.4 2.5 2.2 0.5 0.5 0.3 5.62
94.7 88.6 75.5 72.9 62.6 40.0 35.3 25.2 20.0 17.4 10.0 8.9 8.9 6.8 3.6 1.8 1.1 0.3 0.1 5.74
8.32* 1.24 1.17
1.11 c 1
< 1 < 1 12.05' 1.79 1.47
1.7 < 1
c 1 < 1
< 1
< 1
2.44
1.66
1.88 1.32
Discussion These results demonstrate the effectiveness and fea-
sibility of implementing an evidenced-based, neonatal skin care practice guideline in a variety of acute-care settings for premature and full-term neonates. The par- ticipating sites reflect a diverse geographic distribution, as well as different types of acute-care hospitals, includ- ing academic, private, and children's hospitals as described in Lund et al. (2001). The positive outcomes we report from the large sample of newborns assessed in this project support the safety and efficacy of using the guideline in daily skin care practices for neonates.
Changes such as decreasing the frequency of bathing and use of cleansers with bathing are included in the research-based clinical practice guideline because of evi- dence that bathing can be drying and potentially irri- tating to the skin (Gfatter et al., 1997; Morelli & Weston, 1987; Tupker et al., 1990). There is also concern about the destabilizing effects of bathing on vital signs and temperature, particularly in premature or ill newborns (Penny-MacGillivray, 1996; Peters, 1996). Specific brands
TABLE 1 0 Blood Cultures: Rate and Organisms ldenti- fied in Neonatal intensive-Care Unit/Special- Care Unit Sample
Organism Staph epidermidis Staph aureus E. coli Klebsiella Candida albicans Pseudmonas Serratia Total
Preirrten/entin n % 36 (2.9) 10 (0.8) 12 (1.0) 3 (0.2) 9 (0.7) 2 (0.2) 2 (0.2) 74
POSti~i4WtWtiOtl
n % 37 (3.4) 8 (0.7) 5 (0.5) 7 (0.6) 7 (0.6) 1 (0.1) 1 (0.1) 66
of cleansers were not named in the guideline because no research currently exists for neonates comparing one brand with another. However, synthetic detergents with
January / Febrztary 2001 JOG" 49

a neutral pH and minimal dyes and perfumes are rec- ommended based on evidence in infants (Gfatter et al., 1997), as well as the concern over early exposure to unnecessary chemicals (Cetta, Lambert, & Ros, 1991).
Emollient use has been shown to be effective in reducing dryness of skin surfaces and improving the barrier function of the skin (Lane & Drost, 1993; Nop- per et al., 19961, particularly in very low birth weight infants. Our sample reflects an impressive increase in the use of emollients overall, particularly in infants less than 32 weeks gestation, as recommended in the guide- line. Aquaphor original formula ointment (Beiersdorf, CT) was specifically named because this emollient was studied in two randomized, controlled trials (Nopper et al., 1996; Pabst, Starr, Qaiyumi, Schwalbe, & Gewolb, 1999). It is petrolatum based, water miscible, and con- tains no preservatives, dyes, or perfumes.
Concerns about the use of topical petrolatum-based ointments and an increase in systemic fungal infections have been raised recently (Campbell, Zaccaria, & Baker, 2000), despite the previous research showing no increase in colonization patterns with microorganisms (Lane & Drost, 1993; Nopper et al., 1996; Pabst et al., 1999). Our observations are reassuring, as there was no increase in the numbers of positive blood cultures with fungal or bacterial organisms when comparing the 2- month periods before and after the guideline was implemented. Admittedly, our project was not designed to rigorously study the relationship between skin care practices and infection. However, the results of a large, randomized controlled trial of 1,191 infants with birth- weights of 501-1,000 g were recently presented by the Vermont-Oxford Network. Edwards (2000) reported no effect on the combined primary outcomes of sepsis plus mortality and no increase in fungal infections with the twice daily application of Aquaphor ointment for the first two weeks of life; the control group received Aquaphor on an as needed basis only. Of note, an increase in coagulase negative staphylococcus epider- midis blood infections was noted in infants 501-750 g, although the mechanism and relationship to emollient use are not clearly understood. These results will be integrated into the final clinical practice guideline.
The most promising aspect of the project lies in the improvement in the overall skin condition in infants observed after implementation of the guideline, as evi- denced by lower scores on the NSCS tool during the observation period. Although initial scores were similar in both the pre- and postguideline groups, NSCS scores improved more quickly after the guideline had been introduced in the NICU/SCU sample. There were also fewer times when the scores worsened during the obser- vations (“recidivism”) with the guideline in use.
The well-baby sample had better skin scores overall, as might be expected. Yet, 20% had scores higher than 3, indicating some degree of skin disruption. A recent study describes the potential susceptibility of newborn skin to irritants, finding significant anatomic variabili- ty in barrier function, pH, and hydration of the stratum corneum in full-term newborns in the first 2 days of life (Yosipovitch, Maayan-Metzger, Merlob, & Sirota, 2000). The process of adaptation to extrauterine life may well be the explanation for these findings. Our well-baby sample in the postguideline group experi- enced improvement in their skin scores when skin dis- ruption was noted, likely because of the interventions suggested in the guideline.
The causes of skin breakdown listed in the project clearly show the effect of the care environment on skin integrity. Adhesives top the list of causes of skin break- down in this project, and research supports this obser- vation (Harpin & Rutter, 1983; Lund et al., 1997). The problems with adhesives deserve increased attention in new product development, with systematic scientific evaluation to determine the least disruptive adhesives that adhere well enough to secure life-support systems, intravascular lines, respiratory therapy equipment, and monitors.
The list of 15 care items with potential for skin injury was positively correlated with skin scores, as evi- denced by worse skin scores when an increased number of items were marked. This reflects not only the amount of technology in use but also the level of illness in the infants who require these care items. It is useful, therefore, to inventory the level of care in neonates requiring intensive care in terms of their relative risk for developing skin injury.
Cord care practices reported during the skin obser- vation periods show a decline in the initial application of isopropyl alcohol and triple dye and an increase in both chlorhexidine and antimicrobial ointment, reflect- ing the guideline recommendation that alcohol is less effective compared to these agents. Routine application of alcohol until the cord “falls off” was also reported less frequently, as this can actually delay the time to cord separation (Dore et al., 1998).
In summary, this evidenced-based neonatal skin care clinical practice guideline has been successfully imple- mented in 51 nurseries, including intensive, special care, and well-baby settings. The results show an improvement in skin condition and changes in clinical practice in line with guideline recommendations. In addition, the skin scoring system and inventory of envi- ronmental and care items have been shown to be cor- related to skin condition and patient outcomes and can assist nurses in identifying risk factors for impaired skin integrity in the neonatal population.
50 JOG” Volume 30, Number 1

Acknowledgment The AWHONNmANN Neonatal Skin Care Project
was funded by a n educational grant from Johnson & Johnson Consumer Products Company, Division of Johnson & Johnson Consumer Companies, Inc.
REFERENCES
Bustamante, S., & Steslow, J. (1989). Use of a transparent adhesive dressing in very low birthweight infants. Jour- nal of Perinatology, 9, 165-169.
Campbell, J. R., Zaccaria, E., & Baker, C. J. (2000). Systemic candidiasis in extremely low birth weight infants receiving topical petrolatum ointment for skin care: A case-control study. Pediatrics, 105, 1041-1045.
Cetta, F., Lambert, G., & Ros, S. (1991). Newborn chemical exposure from over-the-counter skin care products. Clinical Pediatrics, 30, 286-289.
Dore, S., Buchan, D., Codas, S., Hamber, L., Stewart, M., Cowan, D., & Jamieson, L. (1998). Alcohol versus nat- ural drying for newborn cord care. Journal of Obstet- ric, Gynecologic and Neonatal Nursing, 27, 621-627.
Edwards, W., Conner, J., Gerdes, J., Hoath, S., Lewallen, P., Mujsce, D., Ohlinger, J., & Soll, R. (2000, December). The effect of Aquaphor emollient ointment on nosoco- mial sepsis rates and skin integrity in infants of birth- weights 501-1,000 grams. Paper presented at the Hot Topics Neonatology Conference, Washington, DC.
Gfatter, R., Hackl, P., & Braun, F. (1997). Effects of soap and detergents on skin surface pH, stratum corneum hydra- tion and fat content in infants. Dermatology, 195,258- 262.
Harpin, V., & Rutter, N. (1982). Percutaneous alcohol absorption and skin necrosis in a preterm infant. Archives of Disease in Childhood, 57, 477-479.
Harpin, V., & Rutter, N. (1983). Barrier properties of the new- born infant’s skin. Journal of Pediatrics, 202,419-425.
Knauth, A., Gordin, M., McNelis, W., & Baumgart, S. (1989). Semipermeable polyurethane membrane as an artificial skin for the premature neonate. Pediatrics, 83,
Lane, A. T., & Drost, S. S. (1993). Effects of repeated appli- cation of emollient cream to premature neonates’ skin. Pediatrics, 92, 415-419.
Lund, C., Kuller, J., Lane, A., Lott, J., & Raines, D. (1999). Neonatal skin care: The scientific basis for practice. Journal of Obstetric, Gynecologic, and Neonatal Nurs- ing, 28, 241-254.
Lund, C. H., Kuller, J., Lane, A. T., Lott, J. W., Raines, D. A., & Thomas, K. K. (2001). Neonatal skin care: Evalua- tion of the AWHONNNANN research-based practice project on nurses’ knowledge and skin care practices. Journal of Obstetric, Gynecologic, and Neonatal Nurs- ing, 30, 30-40.
Lund, C. H., Nonato, L. B., Kuller, J. M., Franck, L. S., Cul- lander, C., & Durand, D. J. (1997). Disruption of bar- rier function in neonatal skin associated with adhesive removal. Journal of Pediatrics, 13 1 , 367-372.
945-950.
Mancini, A., Sookdeo-Drost, S., Madison, K., Smoller, R., & Lane, A. (1994). Semipermeable dressings improve epi- dermal barrier function in premature infants. Pediatric Research, 36, 306-314.
Morelli, J. G., & Weston, W. L. (1987). Soaps and shampoos in pediatric practice. Pediatrics, 80, 634-637.
Nopper, A. J., Horii, K. A., Sookdeo-Drost, S., Wang, T. H., Mancini, A. J., & Lane, A. T. (1996). Topical ointment therapy benefits premature infants. Jottrnal of Pedi- atrics, 128, 660-669.
Pabst, R. C., Starr, K. P., Qaiyumi, S., Schwalbe, R. S., & Gewolb, I. H. (1999). The effect of repeated applica- tion of Aquaphor on skin condition, fluid require- ments, and bacterial colonization in very low birth weight infants. Journal of Perinatology, 19, 278-283.
Penny-MacGillivray, T. (1996). A newborn’s first bath. When? Journal of Obstetric, Gynecologic, and Neona- tal Nursing, 25, 481-487.
Peters, K. (1996). Selected physiologic and behavioral responses of the critically ill premature neonate to a routine nursing intervention (Abstract). Neonatal Net- work, 15, 74.
Schick, J. B., & Milstein, J. M. (1981). Burn hazard of iso- propyl alcohol in the neonate. Pediatrics, 68, 587-588.
Tupker, R. A., Pinnagoda, J., Coenraads, P. J., & Nater, J. P. (1990). Evaluation of detergent-induced irritant skin reactions by visual scoring and transepidermal water loss measurement. Dermatologic Clinics, 8, 33-35.
Vernon, H., Lane, A., Wischerath, L., Davis, J., & Menegus, M. (1990). Semipermeable dressing and transepidermal water loss in premature infants. Pediatrics, 86,357-362.
Yosipovitch, G., Maayan-Metzger, A., Merlob, P., & Sirota, L. (2000). Skin barrier properties in different body areas in neonates. Pediatrics, 106, 105-108.
Carolyn H. Lund is a neonatal clinical nurse specialist, Children’s Hospital Oakland, Oakland, CA.
Jason W Osborne is an assistant professor of instructional psychology and technology at the Department of Education- al Psychology, University of Oklahoma, Norman, OK.
Joanne Kuller is a nurse educator in Lafayette, CA.
Alfred T. Lane is chairman, Department of Dermatology, Stanford University Medical Center, Stanford, CA.
Judy Wright Lott is an associate professor of nursing at the College of Nursing and Health, University of Cincinnati, Cincinnati, OH.
Deborah A. Raines is an associate professor, College of Nurs- ing, Florida Atlantic University, Davie.
Address for correspondence: Carolyn H. Lund, RN, MS, FAAN, Intensive Care Nursery, Children’s Hospital Oak- land, 747 52nd Street, Oakland, CA 94609.
January I‘ February 2001 JOGNN 51




















