
Effect of solvents on radiation-induced grafting of styrene onto fluorinated polymer films
Upload
independentCategory
view
1download
0
Natural history of infrainguinal vein graft stenosis relative to bypass grafting technique Ashish K. Gupta , MD, Dennis F. Bandyk, MD, Daycha Cheanvechai, MD, and Brad L. Johnson , MD, Tampa, Fla.
Purpose- To determine whether the incidence of vein graft stenosis is related to bypass grafting technique and thus modification of postoperative surveillance protocols may be required. Methods: From 1991 to 1996, 338 infrainguinal vein bypasses constructed using in situ (n = 131), reversed (n = 120), nonreversed translocated (n = 48), or spliced/upper extremity vein (n = 39) 'grafting techniques were evaluated by intraoperative duplex scanning to optimize bypass construction and serially thereafter to detect developing vein graft stenoses. Bypass procedures were performed in 322 patients for critical limb ischemia (83%), clandication (13%), or popliteal aneurysm (4%). Using life-table analysis, graft patency and revision/failure rates were compared relative to grafting technique, need for operative revision, and intraoperative duplex scan results. Results: Three-year primary and secondary graft patency rates were higher (p < 0.001) for in situ bypass grafts (85%/97%) compared with reversed (57%/83%), nonreversed trans- located (62%/78%), or alternative (51%/76%) vein bypass grafts. During a mean fol- low-up interval of 19 months, the incidence of graft revision was higher for reversed saphenous (23%) and alternative (28%) vein bypass grafts compared with in situ (10%) or noureversed (16%) saphenous vein bypass grafts. Despite a normal intraoperative graft duplex scan, the revision/failure rate of reversed vein grafts was 2.5 times greater than in situ/noureversed translocated vein conduits (primary patency rate at 3 years, 60% vs 87%, p = 0.009). Bypass grafts modified at operation on the basis of duplex scanning were two times more likely to require postoperative revision than grafts with normal intraoperative s c a n s .
Conclusions: The incidence of postoperative graft stenosis and need for revision varies with bypass grafting technique. Reversed vein bypasses and grafts modified at operation may be more prone than in situ vein bypass grafts to develop stenosis and thus require intensive surveillance. Infrainguinal vein graft failure and the need for revision may be reduced by the adoption of bypass grafting techniques that include valve lysis and intraoperative duplex scan assessment. (J Vase Surg 1997;25:211-25.)
Veins used for infrainguinal lower extremity arte- rial revascularization are prone to develop strictures. The cause of this harbinger for graft thrombosis varies and may involve technical imperfection(s) in vein conduit preparation/tunneling or anastomosis construction, healing of traumatized vein walls, inti-
From the Division of Vascular Surgery, Department of Surgery, University of South Florida College of Medicine.
Presented at the Forty-fourth Scientific Meeting of the Interna- tional Society for Cardiovascular Surgery, North American Chapter, Chicago, Ill., June 9-10, 1996.
Reprint requests: Dennis Bandyk, MD, Division of Vascular Sur- gery, HMT #730, 4 Columbia Dr., Tampa, FL 33606.
Copyright © 1997 by The Society for Vascular Surgery and Inter- national Society for Cardiovascular Surgery, North American Chapter.
0741-5214/97/$5.00 + 0 24/6/77978
real hyperplasia, or atherosclerosis. Both in situ and reversed vein grafting techniques can result in resid- ual defects that serve as the origin for the majority of graft stenoses that develop and require repair within 1 year after implantation, l s To identify the "failing graft," frequent vascular laboratory evaluations using duplex scanning have been advocated after discharge from the hospital despite the fact that fewer than one quarter of grafts will develop a lesion that threatens patency. 4,s I f the natural history of graft stenosis was better understood, a more rationale surveillance pro- tocol could be instituted, especially if early postoper- ative duplex scan findings permitted categorization o f grafts into low-risk, medium-risk, or high-risk groups.
The use of duplex scanning at operation to mon-
211
JOURNAL OF VASCULAR SURGERY 212 Gupta et al. February 1997
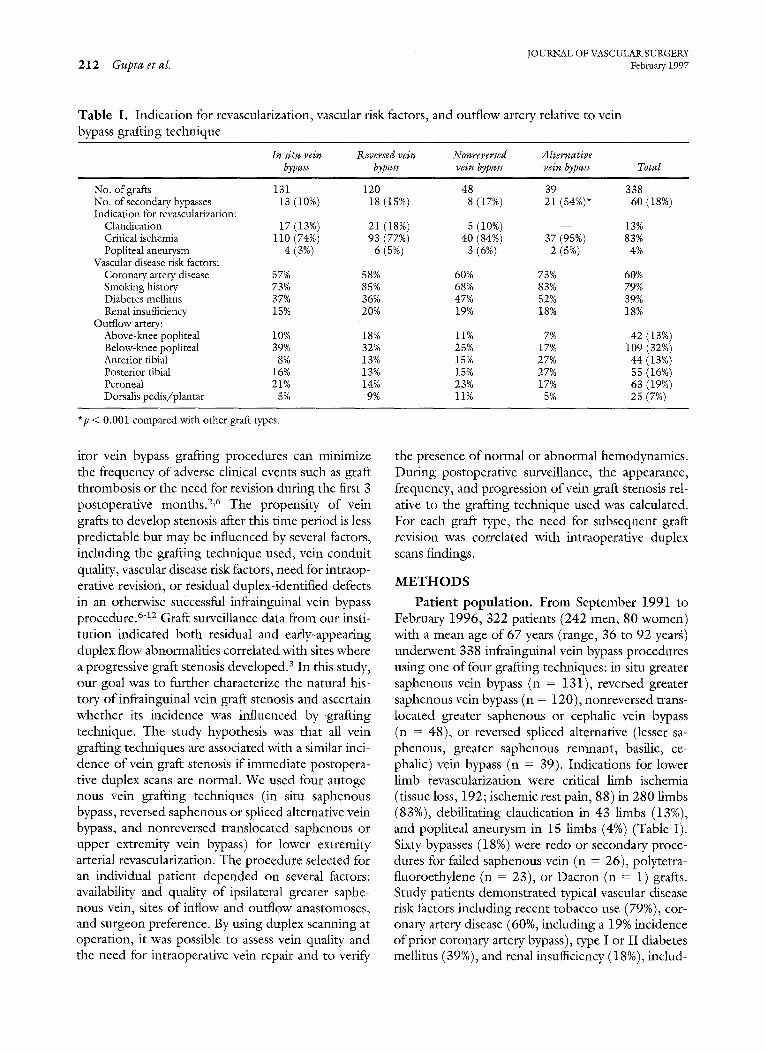
Table I. Indication for revascularization, vascular risk factors, and outflow artery relative to vein bypass grafting technique
In situ vein Reversed vein Nonrever sed Alternative bypass bypass vein bypass vein bypass Total
No. of grafts 131 No. of secondary bypasses 13 Indication for revascularization:
Claudicafion 17 Critical ischemia 110 Popliteal aneurysm 4
Vascular disease risk factors: Coronary artery disease 57% Smoking history 73% Diabetes mellitus 37% Renal insufficiency 15%
Outflow artery: Above-lmee popliteal 10% Below-knee popliteal 39% Anterior tibial 8% Posterior tibial 16% Peroneal 21% Dorsalis pedis/plantar 5%
120 48 39 338 (10%) 18(15%) 8 (17%) 21(54%)* 60(18%)
(13%) 21 (18%) 5(i0%) -- 13% (74%) 93(77%) 40(84%) 37(95%) 83% (3%) 6(5%) 3(6%) 2(5%) 4%
58% 60% 73% 60% 85% 68% 83% 79% 36% 47% 52% 39% 20% 19% 18% 18%
18% 11% 7% 42(13%) 32% 25% 17% 109(32%) 13% 15% 27% 44(13%) 13% 15% 27% 55(16%) 14% 23% 17% 63(19%) 9% ii% 5% 25(7%)
*p < 0.001 compared with other graft types.
itor vein bypass grafting procedures can minimize the frequency of adverse clinical events such as graft thrombosis or the need for revision during the first 3 postoperative months. 2,6 The propensity of vein grafts to develop stenosis after this time period is less predictable but may be influenced by several factors, including the grafting technique used, vein conduit quality, vascular disease risk factors, need for intraop- erative revision, or residual duplex-identified defects in an otherwise successful infrainguinal vein bypass procedure. 6-12 Graft surveillance data from our insti- tution indicated both residual and early-appearing duplex flow abnormalities correlated with sites where a progressive graft stenosis developed, a In this study, our goal was to further characterize the natural his- tory of infrainguinal vein graft stenosis and ascertain whether its incidence was influenced by grafting technique. The study hypothesis was that all vein grafting techniques are associated with a similar inci- dence of vein graft stenosis if immediate postopera- tive duplex scans are normal. We used four autoge- nous vein grafting techniques (in situ saphenous bypass, reversed saphenous or spliced alternative vein bypass, and nonreversed translocated saphenous or upper extremity vein bypass) for lower extremity arterial revascularization. The procedure selected for an individual patient depended on several factors: availability and quality of ipsilateral greater saphe- nous vein, sites of inflow and outflow anastomoses, and surgeon preference. By using duplex scanning at operation, it was possible to assess vein quality and the need for intraoperative vein repair and to verify
the presence of normal or abnormal hemodynamics. During postoperative surveillance, the appearance, frequency, and progression of vein graft stenosis rel- ative to the grafting technique used was calculated. For each graft type, the need for subsequent graft revision was correlated with intraoperative duplex scans findings.
METHODS
Patient population. From September 1991 to February 1996, 322 patients (242 men, 80 women) with a mean age of 67 years (range, 36 to 92 yearg) underwent 338 infrainguinal vein bypass procedures using one of four grafting techniques: in situ greater saphenous vein bypass (n = 131), reversed greater saphenous vein bypass (n = 120), nonreversed trans- located greater saphenous or cephalic vein bypass (n = 48), or reversed spliced alternative (lesser sa- phenous, greater saphenous remnant, basilic, ce- phalic) vein bypass (n = 39). Indications for lower limb revascularization were critical limb ischemia (tissue loss, 192; ischemic rest pain, 88) in 280 limbs (83%), debilitating elaudication in 43 limbs (13%), and popliteal aneurysm in 15 limbs (4%) (Table I). Sixty bypasses (18%) were redo or secondary proce- dures for failed saphenous vein (n = 26), polytetra- fluoroethylene (n = 23), or Dacron (n = 1) grafts. Study patients demonstrated typical vascular disease risk factors including recent tobacco use (79%), cor- onary artery disease (60%, including a 19% incidence of prior coronary artery bypass), type I or II diabetes mellitus (39%), and renal insufficiency (18 %), includ-

JOURNAL OF VASCULAR SURGERY Volume 25, Number 2 Gupta e t aL 213
ing 11 patients on hemodialysis or with a prior renal transplant). The number of secondary bypass proce- dures was increased (p < 0.001) in the alternative vein bypass group. Excluded from the study were vein grafts performed for trauma, and 12 infraingui- nal vein bypasses performed in patients in whom postoperative follow-up and thus detailed graft sur- veillance was not possible.
Vein grafting technique varied with surgeon's preference, ipsilateral saphenous vein availability/ quality, and sites selected for the proximal and distal anastomosis. All procedures were performed by two staff surgeons assisted by vascular fellows or chief residents in general surgery. Valve lysis during in situ saphenous and nonreversed translocated vein bypass procedures was performed using the Karmody scis- sors and a modified Mills valvulotome (American V. Mueller, Chicago, Ill.) via a "blind" retrograde tech- nique. Six in situ vein bypasses were performed using angioscopy-directed valvulotomy. The technique of reversed vein bypass grafting was patterned after re- ports from the Division of Vascular Surgery, Oregon Health Sciences University. 7,8 The location of the proximal anastomosis was similar for the various grafts types. Overall, the inflow artery was the com- mon femoral artery in 186 procedures (55%), super- ficial femoral artery in 95 (28%), profunda femoral artery in 27 (8%), and popliteal artery in 30 (9%). The sites of distal anastomosis relative to the graft types were similar (Table I). The outflow artery was the popliteal in 45% of limbs, tibial in 48% of limbs, and pedal in 5%.
Instrumentation and scanning technique. In- traoperative duplex scans were performed with one of three color duplex ultrasound systems (ATL HDI Ultramark 9, ATL HDI 3000, Advanced Technol- ogy Laboratories, Bothell, Wash.; Accuson 128 XP, Accuson Corp., Smyrna, Ga.). All studies were con- ducted using a linear array probe (7 to 10 MHz) with and without an acoustic standoff. A sterile plastic sleeve filled with acoustic gel was used to cover the transducer. Imaging of the vein graft, anastomoses, and adjacent native arteries was performed in multi- pie planes with a vascular laboratory technologist adjusting the ultrasound system for optimal color Doppler imaging and recording of centerstream Doppler angle-corrected (60 degrees or less relative to vessel axis) velocity spectra.
Vein bypass grafts were visually inspected and patency confirmed by pulse palpation or continuous- wave Doppler flow analysis before duplex scanning. Papaverine (30 to 60 rag) was injected directly into the graft to augment blood flow and thus enhance
the sensitivity of duplex scanning in detection and grading of residual stenosis. The entire bypass graft was imaged for anatomic and flow abnormalities. After in situ saphenous vein grafting, color Doppler imaging was used to locate remaining patent vein branches for ligation. In graft segments or anasto- motic regions with a color Doppler flow abnormality of a stenosis (lumen narrowing, increased velocity, color flow map aliasing, color-flow jet), velocity spec- tra were recorded proximal to and at the site of maximum flow disturbance with measurements of peak systolic velocity (PSV) and calculation of the velocity ratio (Vr), where Vr = PSV~t lesion//PSVproximal . Defects were classified into four stenosis categories, and a previously described algorithm for graft revision was used. 3 In general, when duplex scanning demon- strated both a defect/narrowing in the vessel lumen and velocity spectra (PSV > 180 cm/sec, Vr > 2.5) of a severe or high-grade stenosis, immediate revision of the site was performed. Abnormalities, such as stenosis, retained valve leaflets, low graft flow, or sites of platelet thrombus formation were repaired using one of several procedures (primary repair, valvu- lotome reintroduction, vein patch angioplasty, vein interposition grafting, or graft replacement with venovenostomy). Graft segments or anastomotic sites with moderate flow abnormalities/stenosis were further evaluated by transverse imaging to measure vessel diameter and assess for lumen for evidence of thrombus formation. Segments with borderline ste- noses were typically rescanned after additional papav- erine administration to assess hemodynamic response to flow augmentation. If PSV at the site increased to greater than 200 cm/sec in a normal diameter vein or anastomosis, exploration and revision was per- formed. Sites with residual or, unrepaired moderate duplex focal flow abnormalities were noted in the patient's record and the graft site evaluated during postoperative follow-up for persistence, progression, or regression of the lesion. Intraoperative arterio- grams were obtained in fewer than 15% of cases, typically when intraoperative duplex findings were equivocal regarding a hemodynamically significant lesion or for comparison to an abnormal duplex scan. No graft was revised at operation on the basis of arteriography alone.
After operation, duplex graft surveillance was re- peated before discharge from the hospital, 6 weeks later, and at 3- to 6-month intervals thereafter using the same ultrasound systems used for intraoperative studies. The need for subsequent graft revision was based on serial duplex findings, measurement of an- kle-brachial systolic pressure index (ABI), physical

JOURNAL OF VASCULAR SURGERY 2 1 4 Gupta et al. February 1997
Table II. Comparison life table cumulative patency rates relative to infrainguinal grafting technique and results of intraoperative duplex scanning
Primary patency Secondary patency
No. of grafts I-year 27ear 3-year I-year 2-year 3-year
All grafts: In situ saphenous ] 31 Reversed saphenous 120 Nonreversed saphenous 48 Alternative veins 39
Normal intraoperative duplex scan: In situ saphenous 111 Reversed saphenous 109 Nonreversed saphenous 37 Alternative veins 25
89% 85% 85%* 99% 97% 97% 75% 66% 57% 94% 89% 83% 76% 62% 62% 87% 78% 78% 71% 60% 51% 90% 90% 76%
91% 87% 87%* 99% 97% 97%~ 76% 71% 59% 95% 91% 85% 84% 67% 67% 96% 86% 86% 72% 72% 58% 94% 77% 77%
*p < 0.006 versus reversed vein bypasses, p < 0,05 versus nonreversed and alternative veins. I"P < 0.054 versus reversed vein bypasses.
examination, and in selected patients, arteriography. Stenosis involving inflow/outflow arteries or lesions selected for treatment by percutaneous transluminal angioplasty had arteriographic imaging to verify the abnormality and monitor its treatment. Patients with vein bypass grafts identified to have a high-grade stenosis (PSV > 300 cm/sec, Vr > 3.4) were recom- mended to undergo graft revision, particularly if as- sociated with a decrease in ABI greater than 0.2, or if arteriography confirmed a >70% diameter-reduction stenosis. All patent grafts were followed for a mini- mum of 1 month (range, 1 to 67 months) with a mean follow-up interval of 19 months.
Data analysis. The frequency of intraoperative graft revision and incidence of normal intraopera- tive/predischarge duplex scans were tabulated for each vein bypass type. Adverse patient outcomes in- cluding death, graft failure, and need for graft revi- sion were recorded relative to graft type and time after the primary grafting procedure. Primary and secondary cumulative graft patency rates were deter- mined according the SVS/ISCVS reporting stan- dards with estimates calculated by the Peto life-table method. Life table patency rates were reported when SEM was less than 10%, and comparisons between patency rates were made with the Mantel-Haenszel log-rank test of significance. Statistical comparisons between categorical parameters were performed with Pearson's ×2 analysis. Statistics were considered sig- nificant ifp value was less than 0.05.
RESULTS
Four patients (1.2%) died within 30 days of oper- ation, including two patients after a myocardial in- farction, one patient after a stroke, and one patient with respiratory failure after aspiration pneumonia.
The cumulative survival rate of patients with patent bypass grafts was 92% at i year, 86% at 2 years, 77% at 3 years, and 75% at 4 years. No vein grafts were lost because of infection or a wound healing complica- tion. The early (<30 day) graft thrombosis rate was 1.2% (4 of 334 bypasses), but all were successfully salvaged by thrombectomy and revision (secondary patcncy rate of 100%).
The primary and secondary cumulative patency rates relative to vein bypass grafting technique are listed in Table II and presented graphically to 4 years in Figs. 1 and 2 (Appendix A and B). Compared with reversed vein grafts, in situ vein bypass grafts had a higher 4-year primary (85% + 3.6% vs 57% + 7%; p < 0.001) and secondary (97% + 2% vs 83% + 5%; p < 0.009) patency rate. The 3-year primary and second- ary cumulative patency rates of nonreversed translo- cated (62%/78%) and spliced alternative/upper ex- tremity vein bypass grafts (51%/76%) were similar to reversed vein bypass grafts but less than in situ vein bypass grafts (p < 0.002). Both primary and second- ary cumulative patency rates of reversed vein bypass grafts demonstrated a steady decline with time, and the need for revision and failure of in situ saphenous vein bypass diminished with time. During the first postoperative year, reversed vein bypasses were re- vised two times more frequently than in situ bypasses for duplex-identified stenosis or unexpected throm- bosis. Beyond 1 year, 2% of in situ bypass grafts at risk underwent secondary procedures compared with greater than 5% of reversed veins per year (Figs. 3 and 4).
Intraoperative duplex scanning prompted the re- vision of 56 bypass grafts (16%), including 36% of spliced alternative vein bypasses, 23% ofnonreversed translocated vein bypasses, 15% of in situ vein by-

JOURNAL OF VASCULAR SURGERY Volume 25, Number 2 Gupta et al. 2 1 5
100
~ ~ i i i i . i -" i i i i i i _-85%
. . . . . . . 6 2 %
~ 5 7 %
>.. ¢0 t - (1)
Q_
(1) > . m
.-.¢
E ¢D
90
80
70
60
50
40
30
20
10
0
, ~ ~ _ ~ . . ~ , ~ ~ 5 1 %
In situ vs reversed/alternative: p < 0.001 (log rank)
In situ vs nonreversed: p < 0.006 (log rank)
~ I S V B
+ R S V B
+ N R V B
AVB
I r I I I I i i I I r J I i i I i r I t I J i I i
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Months
Fig. 1. Life table analysis of primary patency rates of in situ saphenous (ISVB), reversed vein (RSVB), nonreversed translocated (NRVB), and alternative autogenous (AVB) vein bypass grafts.
>., 0 e-
n
>
t~
E " !
o
100
90
80
70
60
50
40
30
20
10
0
[ ~ ~ '- : '- :97% o
" :/ ; ~ : : ~ ~ ' - ~ " ~ - ~ R V B - 78% AVR - 7R°/.
ISVB
In situ vs reversed: p = 0.009 (log rank) ÷ R S V B + N RVB
In gihJ v.~ n n n r ~ v e . m e d : n = (3 £)(35 ( Ion r a n k / . . . . ~-AVB
I I I I I I I I [ I I I I I I I ] I
O 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54 56
Months
Fig. 2. Life table analysis of secondary patency rates of in situ saphenous (ISVB), reversed vein (RSVB), nonreversed translocated (NRVB), and alternative autogenous (AVB) vein bypass grafts.
passes, and 9% of reversed vein bypasses (Table III). After revision, duplex scan of the site showed im- proved hemodynamics but focal disturbed flow (Vp = 125-75 cm/sec) persisted in 19 grafts (34%). Eleven reversed vein bypass grafts (n = 11) that required intraoperative revision had a 2-year second- ary patency rate of 61% + 12%, which was less (p =
0.05) than the 100% -+ 10% 2-year secondary pa- tency rate of 20 in situ vein bypasses modified during the primary procedure.
The results of intraoperative/predischarge du- plex scanning correlated with the need for subse- quent revision or graft failure (Table II, Appendix C and D). In situ saphenous vein bypass grafts with

JOURNAL OF VASCULAR SURGERY 2 1 6 Gupta et al. February 1997
18
16
14
12
10
8
6
4
2
0
115 Postoperative Months l[[
n 0 - 6 • 6 - 1 2 m 1 2 - 2 4 m > 2 4
4
2 2 I m 2
I I I I
I SVB RVB N RVB AVB
Bypass Grafting Technique Fig. 3. Number of graft revisions during postoperative follow-up relative to bypass grafting technique.
30% - 26% . . . . . . . . =- - -
25% "O
.in :> 20%
£E
15%
(5 "6 lo%
o~ 5%
0%
ISVB RVB NRVB AVB
17%
Bypass Graft Technique Fig. 4. Percent of grafts revised during each postoperative time interval relative to bypass grafting technique.
normal or accepted duplex scans exhibited a higher (p = 0.009) primary patency rate at 3 years (87% -+ 4%) compared with reversed vein grafts (59% + 8%). Despite duplex scans judged to have no significant anatomic or hemodynamic abnormality, 11 of 111 (i0%) in situ vein bypass grafts failed or required revision during follow-up compared to 31 of 109 (28%) reversed vein grafts (p < 0.001, X 2 = 12.0). Graft revision based on duplex surveillance was suc- cessful, the 3-year secondary patency rate of in situ
(97%) and reversed (85%) saphenous vein bypasses were not statistically different (p = 0.06). Nonre- versed-translocated saphenous and spliced alternative vein bypasses with normal early duplex scans subse- quently failed or required revision of a duplex-iden- tified abnormality at an incidence similar to that of reversed vein grafts (2-year primary graft patency rate of 67% + 12% and 72% + I0%, respectively). Fifteen of the 44 graft revisions performed on grafts with normal intraoperative duplex scans occurred within 3
JOURNAL OF VASCULAR SURGERY Volume 25, Number 2 Gupta et al. 217
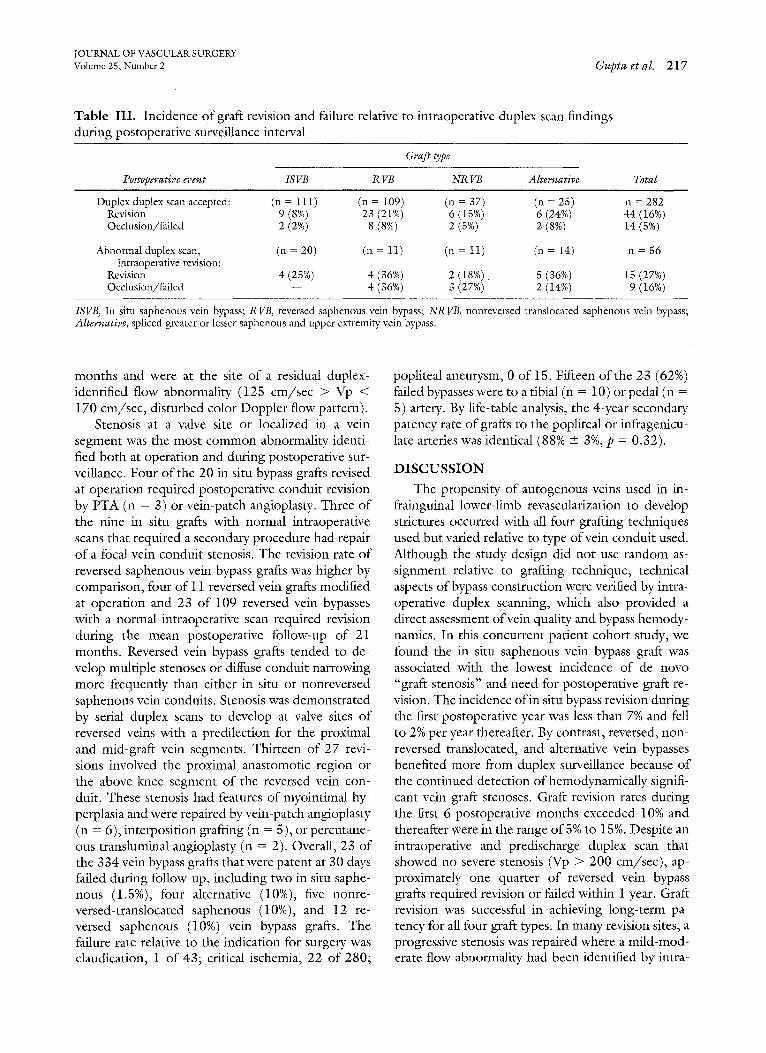
Table III . Incidence O f graft revision and failure relative to intraoperative duplex scan findings during postoperative surveillance interval
Graft type
Postoperative event ISVB R VB NR VB Alternative Total
Duplex duplex scan accepted: (n - 111) (n = 109) (n = 37) (n = 25) n = 282 Revision 9 (8%) 23 (21%) 6 (15%) 6 (24%) 44 (16%) Occlusion/failed 2 (2%) 8 (8%) 2 (5%) 2 (8%) 14 (5%)
Abnormal duplex scan, (n = 20) (n = 11) (n = 11) (n = 14) n = 56 intraoperative revision:
Revision 4 (25%) 4 (36%) 2 (18%) 5 (36%) 15 (27%) Occlusion/failed -- 4 (36%) 3 (27%) 2 (14%) 9 (16%)
ISVB, In situ saphenous vein bypass; RVB, reversed saphenous vein bypass; NRVB, nonreversed translocated saphenous vein bypass; Alternative, spliced greater or lesser saphenous and upper extremity vein bypass.
months and were at the site of a residual duplex- identified flow abnormality (125 cm/sec > Vp < 170 cm/sec, disturbed color Doppler flow pattern).
Stenosis at a valve site or localized in a vein segment was the most common abnormality identi- fied both at operation and during postoperative sur- veillance. Four of the 20 in situ bypass grafts revised at operation required postoperative conduit revision by PTA (n = 3) or vein-patch angioplasty. Three of the nine in situ grafts with normal intraoperative scans that required a secondary procedure had repair of a focal vein conduit stenosis. The revision rate of reversed saphenous vein bypass grafts was higher by comparison, four of 11 reversed vein grafts modified at operation and 23 of 109 reversed vein bypasses with a normal intraoperative scan required revision during the mean postoperative follow-up of 21 months. Reversed vein bypass grafts tended to de- velop multiple stenoses or diffuse conduit narrowing more frequently than either in situ or nonreversed saphenous vein conduits. Stenosis was demonstrated by serial duplex scans to develop at valve sites of reversed veins with a predilection for the proximal and mid-graft vein segments. Thirteen of 27 revi- sions involved the proximal anastomotic region or the above-knee segment of the reversed vein con- duit. These stenosis had features of myointimal hy- perplasia and were repaired by vein-patch angioplasty (n = 6), interposition grafting (n = 5), or percutane- ous transluminal angioplasty (n = 2). Overall, 23 of the 334 vein bypass grafts that were patent at 30 days failed during follow-up, including two in situ saphe- nous (1.5%), four alternative (10%), five nonre- versed-translocated saphenous (i0%), and 12 re- versed saphenous (10%) vein bypass grafts. The failure rate relative to the indication for surgery was claudication, 1 of 43; critical ischemia, 22 of 280;
popliteal aneurysm, 0 of 15. Fifteen of the 23 (62%) failed bypasses were to a tibial (n = 10) or pedal (n = 5) artery. By life-table analysis, the 4-year secondary patency rate of grafts to the popliteal or infragenicu- late arteries was identical (88% -+ 3%, p = 0.32).
DISCUSSION
The propensity of autogenous veins used in in- frainguinal lower-limb revascularization to develop strictures occurred with all four grafting techniques used but varied relative to type of vein conduit used. Although the study design did not use random as- signment relative to grafting technique, technical aspects of bypass construction were verified by intra- operative duplex scanning, which also provided a direct assessment of vein quality and bypass hemody- namics. In this concurrent patient cohort study, we found the in situ saphenous vein bypass graft was associated with the lowest incidencc of de novo "graft stenosis" and need for postoperative graft re- vision. The incidence of in situ bypass revision during the first postoperative year was less than 7% and fell to 2% per year thereafter. By contrast, reversed, non- reversed translocated, and alternative vein bypasses benefited more from duplex surveillance bccause of the continued detection of hemodynamically signifi- cant vein graft stenoses. Graft revision rates during the first 6 postoperative months exceeded 10% and thereafter were in the range of 5% to 15%. Despite an intraopcrativc and predischarge duplex scan that showed no severe stenosis (Vp > 200 cm/sec), ap- proximately one quarter of reversed vein bypass grafts required revision or failed within 1 year. Graft revision was successful in achieving long-term pa- tency for all four graft types. In many revision sites, a progressive stenosis was repaired where a mild-mod- erate flow abnormality had been identified by intra-

IOURNAL OF VASCULAR SURGERY 218 Gupta et aL February 1997
Table IV. Rank order listing of vein bypass graft type relative to the intensity (frequency) of postoperative duplex surveillance
Relative need for Type of vein bypas duplex surveillance
Modified reversed vein bypasses Alternative vein bypasses Reversed vein bypasses Nonreversed vein bypasses In situ saphenous vein bypass In situ vein bypasses with
normal intra-operative duplex scan
Intensive surveillance (every 1 to 3 months)
Infrequent surveillance (every 6 to 12
months)
operative duplex scanning. For vein bypass grafts with intraoperative duplex scans judged to be satis- factory, the 3-year secondary patency rates were not statistically different for in situ, reversed, and nonre- versed translocated vein bypasses.
Based on duplex graft surveillance and observa- tions made at the time of graft revision, the tendency of reversed vein bypass grafts to develop stenoses appeared to be related to stricture at the valve appa- ratus caused by myointimal hyperplasia. Duplex flow abnormalities were observed at reversed valve sites in some patients both immediately and later after graft implantation, and at some valves, a high-grade steno- sis developed. Stenosis within the vein conduit was less likely to occur when valve lysis was performed and its completeness verified by intraoperative du- plex scanning, that is, no disturbed flow at valve site. Although the role of the reversed valve in postopera- tive graft stenosis has been questioned, several inves- tigators have demonstrated flow abnormalities at valves, and in an atherosclerotic animal model, re- versed valves developed vein wall-thickening with t ime . 16-18
Our initial goal in performing postoperative graft surveillance was to enhance long-term patency. We added intraoperative duplex monitoring in an at- tempt to eliminate early graft thrombosis and hope- fully reduce the need for subsequent graft revision. Intraoperativc graft imaging has proved to be an excellent method to monitor vein conduit prepara- tion and quality, anastomoses patency, as well as other adjunctive procedures, such as endarterectomy and patch angioplasty, used to enhance graft inflow. 2 Bypass imaging can be performed in less than 15 minutes and is preferred by the authors over arteriog-
raphy. Surgical intervention is optimized because grafts with normal intraoperative demonstrate a low incidence of early graft failure and revision. 6 Only four grafts in this series thrombosed within 30 days and all were successfully restored to patency (100% secondary patency rate). Beyond the early postoper- ative period, the predilection for graft stenosis was influenced by several factors, the most significant being an abnormal intraoperative scan that prompted graft modification, replacement, or repair. Grafts re- vised at operation had higher incidence of postoper- ative revision (27%) and failure (16%) compared with grafts with scans judged satisfactory (16% and 5%, respectively). The need for operative revision can be viewed as a measure of vein conduit quality, particularly if abnormalities not associated with valve lysis are de- tected. Although randomized and nonrandomized clinical trials of in situ and reversed saphenous vein bypass grafts have not demonstrated differences in pa- tency, 14,1s these head-to-head comparisons were flawed by a lack of objective criteria for assessing technical adequacy. We have demonstrated that when duplex scanning is used to monitor the techni- cal aspects of the procedure, the need for postopera- tive graft revision, particularly after in situ bypass grafting, was decreased. The in situ bypass primary patency rate (85% at 4 years) was augmented com- pared with published reports that relied on other Doppler or imaging (angioscopy, arteriography) techniques (53% to 70% at 4: to 5 years) to assess technical adequacy.i°-12 Upgrading the quality of the autogenous vein based on angioseopy or duplex as- sessment is a valid concept because normal intraop- erative studies arc associated with a low incidence of early graft failure, and early primary patency is opti- mized. Unfortunately, achieving normal graft hemo- dynamics as assessed with color duplex ultrasonogra- phy is not always possible because vein segments of marginal quality or diameter must be used, and anas- tomosis to diseased artery segments are typically a required clement of the procedure. The results of intraoperative duplex monitoring have demonstrated a clear relationship between technical precision and the durability of arterial reconstruction. After both the carotid endarterectomy and infrainguinal vein bypass procedures, the incidence of adverse out- comes was increased when defects were not re- paired. 1,3,1a A prior prospective study of the origins of vein graft stenosis also emphasized the association of residual defects with the subsequent development of a graft stenosis.~4 The application ofintraoperative duplex scanning affords an opportunity to maximize early graft patency and can represent cost-effective

JOURNAL OF VASCULAR SURGERY Volume 25, Number 2 Gupta et al. 2 1 9
care if the number of subsequent graft revision pro- cedures are reduced.
The results achieved in this study are comparable with those of published reports of specific grafting techniques. The assisted-primary (secondary) pa- tency rates of in situ saphenous and reversed vein bypass grafts of 97% and 83% at 3 years exceed or mirror the results published from the Albany (in situ bypass, 84%), Milwaukee (in situ bypass, 86%), and Portland (ipsilateral greater saphenous vein, 84%; contralateral greater saphenous vein, 79%) vascular surgery services, a,7,1° The results of in situ versus the other types of grafting methods are not comparable, in part because of differences in the number of sec- ondary or redo procedures, and features of vein con- duit selection and preparation. The number of sec- ondary procedures was significantly higher (p < 0.001) in the alternative bypass group. When an in situ bypass procedure could be performed and the intraoperative duplex scan was normal (85% of cas- es), the higher primary and secondary patency rates translates into decreased patient-care cost and a re- duced need for surveillance. Only nine of 111 in situ bypass grafts with normal intraoperative/predis- charge scans required revision by 2 years (primary patency rate of 87%), and in three limbs the revision did not involve the venous conduit. Thus intensive (3-month) graft surveillance beyond the first 6 months was not cost-effective for this patient cohort. Duplex surveillance at 6-month intervals is probably sufficient to identify occlusive lesions developing within, proximal to, and distal to the in situ vein bypass graft (Table IV). Whether yearly surveillance is appropriate is not known, but in active patients with normal scans and minimal atherosclerosis of inflow and runoff arteries, the likelihood of rapid atherosclerofic disease progression is unlikely. By comparison, bypass grafts revised at operation and alternative vein bypasses require intensive surveil- lance, particularly during the first postoperative year. Stricture at valve sites and venovenostomies were detected by serial scans during follow-up. Duplex surveillance at 6 weeks after surgery and then at 3-month intervals is recommended for these graft types at high-risk for stenosis. Reversed and nonre- versed saphenons vein bypass grafts posed an inter- mediate risk for postoperative graft stenosis. Despite normal intraoperative and predischarge duplex scans, these grafts developed conduit stricture in an unpre- dictable mode, and thus surveillance at regular 3-month intervals for the first year is recommended. If a moderate duplex stenosis is identified (150 c m / sec < PSV < 300 cm/sec; Vr < 3.4), serial scans at
6-week intervals are recommended to detect stenosis progression. This algorithm has been effective in our patient population. Only five of the 23 graft occlu- sions that occurred during follow-up did so unex- pectedly involving a bypass with normal prior duplex surveillance. Beyond 1 year, it is our current practice to perform grafts scans at 6-month intervals for all bypass grafts with no previously identified abnormal- ity.
Surgeons should be competent in the various techniques ofinfrainguinal vein bypass grafting. Nei- ther in situ or reversed vein grafting is possible or preferable in all patients. This study is a primer for the expected natural history of infrainguinal bypass grafting when various techniques, vein conduits, and duplex surveillance are used. When possible, we pre- fer to use the in situ saphenous vein bypass grafting technique. Verification of normal in situ bypass he- modynamics at operation is important, and when achieved the likelihood of failure or need of revision is reduced compared with the other grafting tech- niques. Of note, the nonreversed translocated saphe- nous vein bypass, a technique which also involves valve lysis, did not achieve primary and secondary patency rates comparable with the in situ vein bypass. This grafting method was used in some instances when length or quality of the greater saphenous vein was found to be inadequate, but its tendency to develop stenosis appears to be real. This observation supports the concept of minimizing vein conduit mobilization and ischemia, as well as performing valve lysis to reduce the number of valve sites at risk for the development of a stenosis. Although the study design did not include randomization with respect to grafting technique, when intraoperative duplex scans were normal, it appears the intrinsic failure rate of the reversed vein conduit may exceed that of the in situ saphenous vein.
R E F E R E N C E S
1. Mills JL, Bandyk DF, Gahtan V, Esses GE. The origin of infrainguinal vein graft stenosis: a prospective study based on duplex surveillance. J Vase Surg 1995;21:16-25.
2. Bandyk DF, Mills JL, Gahtan V, Esses GE. Intraoperative duplex scanning of arterial reconstructions: fate of repaired and unrepaired defects. J Vase Surg 1994;20:426-33.
3. Bergamini TM, Towne JB, Bandyk DI:, Seabrook GR, Schmitt DD. Experience with in situ saphenous vein bypasses during 1981 to 1989: determinant factors of long-term pa- tency. J Vase Surg 1991;13:137-49.
4. Mills JL, Harris EJ, Taylor LM Jr, Beckett WC, Porter JM. The importance of routine surveillance of distal bypass grafts with duplex scanning: a study of 379 reversed vein grafts. J Vase Surg 1990;12:379-89.
5. Lundell A, Lindblad B, Bergqvist D, Hansen F. Femoropop- liteal-crural graft patency is improved by an intensive surveil-

JOURNAL OF VASCULAR SURGERY 220 Gupta et al. February 1997
lance program: a prospective randomized study. J Vasc Surg 1995;21:26-34.
6. Bandyk DF, Johnson BL, Gupta AK, Esses GE. Nature and management of duplex abnormalities encountered during in- frainguinal vein bypass grafting. J Vase Surg I996;24:430-8.
7. Taylor LM, Edwards JM, Phinney ES, Porter JM. Reversed vein bypass to infrapopliteal arteries. Ann Surg 1987;205: 90-7.
8. Gentile AT, Lee RW, Moneta GL, Taylor LM Jr, Edwards JM, Porter JM. Results of bypass to the popliteal and tibial arteries with alternative sources of autogenous vein. J Vasc Surg 1996;23:272-80.
9. Leather RP, Chang BB, Darling RC III, Shah DM. The in situ saphenous vein bypass: a if-year experience. In: Whitte- more AD, editor. Advances in vascular surgery. St. Louis: Mosby-Year Book, 1994:9-24.
10. Belkin M, Conte MS, Donaldson MC, Mannick JA, Whitte- more AD. Preferred strategies for secondary infrainguinal bypass: lessons learned from 300 consecutive reoperations. J Vase Surg 1995;21:282-95.
11. Chang BB, Darling RC III, Bock DEM, Shah DM, Leather RP. The use of spliced vein bypasses for infrainguinal arterial reconstruction. J Vase Surg 1995;21:403-12.
12. Miller A, Marcaccio EJ, Tannenbaum GA, Kwolek CJ, Stone- bridge PA, Lavin PT, et al. Comparison of angioscopy and angiography for monitoring infrainguinal bypass vein grafts:
results of a prospective randomized trial. J Vasc Surg 1993; 17:382-98.
13. Mills JL, Fujitani RM, Taylor SM. The contribution of rou- tine intraoperative completion arteriography to early graft patency. Am J Surg 1992;164:506-11.
14. Wengerter ICR, Veith FJ, Gupta SK, Goldsmith J, Farrell E, Harris PL, et al. Prospective randomized multicenter compar- ison of in situ and reversed vein infrapopliteal bypasses. J Vasc Surg 1991;13:189-99.
15. Sasajima T, Kubo Y, Kokubo M, et al. Comparison of re- versed and in situ saphenous vein grafts for infragenicular bypass~ Cardiovasc Surg 1993;1:38-43.
16. Moody AP, Edwards PR, Harris PL. The etiology of vein graft strictures: a prospective marker study. Eur J Vase Surg 1992;6:509-11.
17. Walsh DB, Downing S, Ahmed SW, Wallace RB. Valvular obstruction of blood flow through saphenous veins. J Surg Res 1987;42:39-42.
18. Chanz A, Ruan XM, Fishbein MC, Sandhu M, Matloff JM. Influence of vein valves in the development of arteriosclerosis in venoarterial grafts in the rabbit. I Thorac Cardiovasc Surg 1995;110:1381-90.
Submitted June 14, 1996; accepted Sep. 13, 1996.
D I S C U S S I O N Dr. Jonathan B. Towne (Milwaukee, Wis.). I would
like to congratulate Dr. Gupta on an excellent presentation and compliment his group on the performance of a well- carried-out clinical study.
We would agree that vein grafts that require intraoper- ative modification to correct strictures, technical errors, or require splicing of vein segments have a higher incidence of postoperative stenoses that require revision in the fol- low-up period. This series represents a unique opportunity to evaluate the long-term evolution of lower extremity bypasses performed with the in situ technique as compared with the reversed vein technique. What I found quite interesting was that the incidence of revisions were greater in the reversed veins than in the in situ veins. Also, the reversed veins tend to develop long segment strictures more commonly than seen with the in situ graft. This certainly suggests that ischemia that may occur during harvest, which was not severe enough to affect periopera- tive patency but did have a long-term effect by inciting the formation of fibrointimal hyperplasia, would tend to cause graft failure in the follow-up period. It would be interest- ing in trying to compare these two techniques if the au- thors could tell us the incidence of normal grafts (intraop- erative studies that were absolutely normal) that developed subsequent problems in the follow-up period.
This series represents what I would describe as inter-
mediate follow-up with a relatively few patients being ob- served greater than 3 years. Therefore, the lesions that are likely to be found in this series are those relating to fi- brointimal hyperplasia, which are commonly seen in the period between 1 month and 24 months after surgery. We would continue to urge that long-term, ongoing surveil- lance be performed. As we noted in our presentation last year, beyond 24 months the incidence of atherosclerotic lesions in the inflow and outflow vessels and beyond 3 to 4 years with the development of atherosclerosis in the con- duit itself can result in graft-threatening and potentially limb-threatening lesions. We noticed an annual incidence of 10% that occurred in postoperative years two through six.
Also, I would like to ask the authors whether they have any ideas why the reversed vein bypass grafts sometimes develop stenosis at the site of vein valve leaflets.
Dr. Dennis F. Bandyk. Thank you, Dr. Towne, for your comments and for introducing me to the in situ saphenous vein bypass grafting technique. It was while working with you in Milwaukee that my interest in infrain- guinal graft surveillance began, and this study represents an extension of that work.
It is difficult to answer your question dealing with outcome differences observed between in situ and reversed saphenous vein bypass grafts with absolutely normal intra-

JOURNAL OF VASCULAR SURGERY Volume 25, Number 2 Gupta et al. 221
operative scans. The criteria of a "normal" intraoperative scan is not well defined. Both in situ and reversed vein bypass groups had some grafts with uncorrected flow ab- normalities at vane and anastomotic sites, but overall the number of bypass grafts with no duplex abnormality was similar for the two graft types. This study focused primarily on the natural history of vein bypass grafts with normal or "accepted" intraoperative scans and those with abnormal scans that required revision. The need for intraoperative revision was an easily defined and important event because it indicated the occurrence of technical problems or a "poor quality" venous conduit. We found that revised grafts behaved differently and required more postoperative revisions for stenosis or occlusion than grafts with normal scan results or a minor residual flow abnormality. We also observed that both in situ and reversed vein bypass grafts that had normal scan results at 3 months subsequently had a low incidence of graft stenosis/failure. When grafts with normal intraoperative scan results were compared, the in- cidence of graft stenosis/failure was higher in reversed vein compared with in situ saphenous vein conduits.
An unanswered question is why do reversed and lysed in situ vein valve sites develop stenosis after implantation into the arterial circulation. At some of these sites, residual flow abnormalities were identified by duplex scanning dur- ing and after surgery, and a progressive myointimal lesion developed. But in some reversed vein bypass grafts, the postoperative scans were normal for months before the stenosis appeared. Some valves in reversed vein bypass grafts have been observed to be functional by duplex scan- ning, that is, the mobile leaflets open and close during the triphasic pulse cycle. The vascular group at the University of Washington have serially imaged functional valves in reversed vein bypass grafts and found that some of them developed stenosis, but the incidence and nature of the occlusive process has not been determined.
Dr. Joseph L. Mills (Tucson, Ariz.). The authors have attempted to analyze a difficult issue: the performance of reversed and in situ saphenous vein bypass procedures. I believe that the methods of the study are flawed and that the conclusions drawn may be unjustified. The authors have compared apples and oranges, and, being from Flor- ida, they have concluded that oranges are superior.
One needs to realize that this was a selected group of patients who underwent infrainguinal vein bypass grafting; only patients who had intraoperative scans were included. I t was the senior author's policy to perform in situ vein bypass procedures when an adequate, ipsilateral saphenous vein bypass conduit was available. Reversed vein grafting was used by this surgeon when in situ or nonrcversed vein bypass grafting was not believed to be an option. This is a clear selection bias.
The authors did indicate that factors such as graft inflow/outflow sites, the presence of diabetes, and other atherosclerotic risk factors were equally distributed be-. tween the various graft types. However, none of these factors have anything to do with long-term graft patency
rates. More important factors, such as thc quality of the vein, whether the conduit was modified, whether concom- itant procedures were performed to treat inflow disease, and prior leg bypass, were not included in the authors' analysis.
I went back and reviewed 81 of the 159 reversed saphenous and alternative vein bypass procedures that I performed during a 2-year period of this study. In this group, 24% were redo operations, 12% included inflow and outflow procedures, and 15 of 70 greater saphenous vein grafts required an extension segment to achieve sufficient length. Only 43 reversed vein bypass procedures were performed with ipsilateral greater saphenous vein and thus could also have been performed 'with the in situ grafting technique. This is the more appropriate control group to compare with the in situ vein bypass graft in the absence of randomization. Unless an appropriate control group is defined, one cannot conclude that one vein grafting tech- nique is superior to another.
Dr. Bandyk. Most vascular surgeons used a number of different techniques in performing infrainguinal bypass grafting procedures. As Dr. Mills emphasized, the patients included in the reversed and nonreversed or in situ groups are probably not homogeneous, especially with regard to the number of redo bypass procedures, which was the highest in the alternative/upper extremity vein bypass group.
This study does provide clinically useful information to surgeons who perform both in situ and reversed vein by- pass grafting procedures. The study data clearly show that if you perform an in situ saphenous vein bypass procedure and monitor its adequacy with duplex scanning, the early graft failure rate will be low (< 3%), and the reconstruction is likely to be more durable than if a reversed vein bypass procedure was performed. I believe that even reversed ipsilateral saphenous vein grafts will require more revisions than a comparable in situ vein bypass graft because of the retained functional valve sites and other factors, such as vein wall ischemia, that are involved in harvesting the saphenous vein and placing it in the reversed configura- tion.
Dr. Alun H. Davies (London, U.K.). I would like to bring a few things to your attention. In the European literature, there is quite a lot of evidence to suggest that vein graft stenosis is not related to valve cusp sites, and this has been well shown in two studies. Furthermore, the comment with respect to the reversed vein being ischemic, there is now good evidence that there are no changes in compliance with time between the reversed and nonre- versed, which is about one of the only noninvasive ways of assessing whether there is a difference in isehemia, and again there is no difference in outcome. The main criteria and the difference that I see from the data that you pre- sented are that there are different surgeons performing the operation. I would be interested in your comments.
Dr. Bandyk. With respect to the last point, only two surgeons participated in terms of performing these opera-

JOURNAL OF VASCULAR SURGERY 222 Gupta et al. February 1997
tions. These procedures were performed with the help o f
chief residents and vascular fellows.
Regarding vein valves and reversed conduits, many o f the valves are no t at the side branches. When you perform
in situ grafting with an open technique or you look at
reversed veins, some valves are in segments other than
where side branches are, and so it might be difficult to identify where all the valve sites are in reversed vein con- duit. But I realize that it is controversial with respect to the role of the reversed vein valve in terms of postoperative stenosis. I think that this is a topic that requires further study.
A p p e n d i x A. Life table cumulative primary graft patency analysis for 338 infrainguinal vein bypass grafts relative to grafting technique
No. grafts No. grafts No. grafts Interval Cumulative Standard Interval (too) " at risk revised/failed withdrawn patency rate patency rate error (%)
In situ saphenous vein: 0-1 131 4 0 0.97 1.00 1-6 127 5 23 0.96 0.97 2.1 6-12 99 4 15 0.96 0.92 2.4
12-18 80 1 22 0.99 0.89 3.0 18-24 57 1 13 0.98 0.87 3.2 24-30 43 0 9 1.0 0.85 3.6 30-36 34 0 11 1.0 0.85 3.6 36-42 23 0 6 1.0 0.85 3.6 42-48 17 0 8 1.0 0.85 3.6 48-54 9 1 7 0.82 0.85 3.6
Reversed saphenous vein: 0-1 120 2 2 0.98 1.00 1-6 116 17 13 0.85 0.98 2.3 6-12 86 8 9 0.90 0.83 3.5
12-18 69 3 16 0.95 0.75 4.2 18-24 50 3 12 0.93 0.71 4.5 24-30 35 2 16 0.93 0.66 4.9 30-36 17 1 8 0.92 0.62 5.7 36-42 8 0 3 1.0 0.57 6.9 42-48 5 0 2 1.0 0.57 6.9 48-54 3 0 3 1.0 0.57 6.9
Nonreversed translocated saphenous vein: 0-1 48 0 2 1.00 1.00 1-6 46 4 13 0.93 1.00 0.0 6-12 29 4 6 0.85 0.90 4.6
12-18 19 1 9 0.93 0.76 7.5 18-24 9 1 3 0.87 0.71 8.6 24-30 5 0 2 1.0 0.62 11 30-36 3 0 2 1.0 0.62 11 36-42 1 0 0 1.0 0.62 11 42 -48 1 1 0 0.0 0.62 11
Alternative reversed vein bypass: 0-1 39 2 0 0.95 1.0 1-6 37 7 9 0.74 0.95 5.7 6-12 21 1 3 0.95 0.74 7.4
12-18 17 2 5 0.86 0.70 8.0 18-24 10 0 2 1.0 0.60 9.3 24-30 8 1 3 0.85 0.60 9.3 30-36 4 0 2 1.0 0.51 11 36-42 2 0 1 1.0 0.51 ' 11 42-48 1 0 1 1.0 0.51 11

JOURNAL OF VASCULAR SURGERY Volume 25, Number 2 Gupta et al. 223
A p p e n d i x B. Life t ab le c u m u l a t i v e s e c o n d a r y graf t p a t e n c y analysis fo r 338 in f r a ingu ina l ve in bypass
graf ts re la t ive t o g r a f t i n g t e c h n i q u e
No, grafts No. grafts No. grafts Interval Cumulative Standard Interval (mo) at risk failed withdrawn patency rate patency rate error (%)
In situ saphenous vein: 0-1 131 0 0 1.0 1.0 1-6 131 0 24 1.0 1.0 0.0 6-12 107 1 20 0.99 1.0 0.0
12-18 86 0 24 1.0 0.99 1.0 18-24 62 1 16 0.98 0.99 1.0 24-30 45 0 9 1.0 0.97 2.0 30-36 36 0 12 1.0 0.97 2.0 36-42 24 0 7 1.0 0.97 2.0 42-48 17 0 8 1.0 0.97 2.0 48-54 9 0 8 1.0 0.97 2.0
Reversed saphenous vein: 0-1 120 0 2 1.0 1.0 1-6 118 5 13 0.95 1.0 1.4 6-12 100 2 11 0.98 0.96 1.9
12-18 87 1 19 0.97 0.94 2.3 18-24 67 2 15 0.98 0.92 2.6 24-30 50 1 21 0.98 0.89 3.3 30-36 28 1 12 0.96 0.87 3.9 36-42 15 0 7 1,0 0.83 5.3 42-48 8 0 3 1.0 0.83 5.3 48-54 5 0 4 1,0 0.83 5.3
Nonreversed translocated saphenous vein: 0-1 48 0 2 1,0 1.0 1-6 46 1 13 0,98 1.0 6-12 32 3 8 0,89 0.98 2.4
12-18 21 0 10 1.0 0.87 6.1 18-24 11 1 4 0.89 0.87 6.1 24-30 6 0 2 1,0 0.78 10 30-36 4 0 2 1,0 0.78 10 36-42 2 0 1 1,0 0.78 10 42-48 1 0 1 0.0 0.78 10
Alternative reversed vein bypass: 0-1 39 0 0 1,0 1.0 1-6 39 2 11 0,94 1.0 6-12 26 1 5 0.96 0.94 4.0
12-18 20 0 10 1,0 0.90 5.5 18-24 10 0 2 1.0 0.90 5.5 24-30 8 1 3 0,85 0.90 5.5 30-36 4 0 2 1.0 0.76 13 36-42 2 0 1 1,0 0.76 13 42-48 1 0 1 1,0 0.76 13

JOURNAL OF VASCULAR SURGERY 2 2 4 Gupta et al. February 1997
Appendix C. Life table cumulative primary graft patency analysis for 282 infrainguinal vein bypass grafts with accepted as normal intraoperative duplex scans relative to grafting technique
No. grafts No. grafts No. grafts Interval Cumulative Standard Interval (mo) at r i s k revised/failed withdrawn patency rate patency rate error (%)
In siva saphenous vein: 0-1 111 3 0 0.97 1.0 1-6 108 4 20 0.96 0.97 2.4 6-12 84 2 14 0.97 0.93 2.5
12-18 69 1 17 0.98 0.91 2.9 18-24 51 1 13 0.98 0.89 3.2 24-30 37 0 7 1.0 " 0.87 3.7 30-36 30 0 10 1.0 0.87 3.7 36-42 20 0 5 1.0 0.87 3.7 42-48 15 0 7 1.0 0.87 3.7 48-54 8 1 7 0.85 0.87 3.7
Reversed saphenous vein: 0-1 109 1 2 0.99 1.0 1-6 106 16 14 0.84 0.99 2.3 6-12 76 6 9 0.92 0.83 3.7
12-18 61 1 14 0.98 0.76 4.3 18-24 46 2 12 0.95 0.75 4.4 24-30 32 2 14 0.92 0.71 4.9 30-36 16 1 8 0.92 0.65 6.0 36-42 7 0 3 1.0 0.59 7.5 42-48 4 0 2 1.0 0.59 7.5 48-54 2 0 2 0.6 0.59 7.5
Nonreversed translocated saphenous vein: 0-1 37 0 2 1.00 1.00 1-6 35 1 10 0.97 1.00 0.0 6-12 24 3 4 0.87 0.97 3.1
12-18 17 1 7 0.93 0.84 7.5 18-24 9 1 3 0.87 0.77 9.2 24-30 5 0 2 1.0 0.67 12 30-36 3 0 2 1.0 0.67 12 36-42 1 0 0 1.0 0.67 12 42-48 1 1 0 0.0 0.67 12
Alternative reversed vein bypass: 0-1 25 0 0 1.0 1.0 1-6 25 5 6 0.77 1.0 5.7 6- i2 14 1 3 0.93 0.77 8.9
12-18 10 0 2 1.0 0.72 10 18-24 8 0 2 1.0 0.72 10 24-30 6 1 1 0.82 0.72 10 30-36 4 0 2 1.0 0.58 14 36-42 2 0 1 1.0 0.58 14 42-48 1 0 1 1.0 0.58 14

JOURNAL OF VASCULAR SURGERY Volume 25, Number 2 Gupta et al. 2 2 5
Appendix D. Life table cumulative secondary graft patency analysis for 282 infrainguinal vein bypass grafts with accepted as normal intraoperative duplex scans relative to grafting technique
No. grafts No. grafts No. grafts Interval Cumulative Standard Interval (mo) at risk failed withdrawn patency rate pateney rate error (%)
In situ saphenous vein: 0-1 111 0 0 1.0 1.0 1-6 111 0 21 1.0 1.0 0.0 6-12 90 1 15 0.99 1.0 0.0
12-18 74 0 19 1.00 0.99 1.2 18-24 55 1 14 0.98 0.99 1.2 24-30 40 0 7 1.0 0.97 2.3 30-36 33 0 11 1.0 0.97 2.3 36-42 22 0 7 1.0 0.97 2.3 42-48 15 0 7 1.0 0.97 2.3 48-54 8 0 8 0.85 0.97 2.3
Reversed saphenous vein: 0-1 109 0 2 1.0 1.0 1-6 107 3 14 0.97 1.0 0.9 6-12 90 2 10 0.98 0.97 1.6
12-18 78 0 16 1.0 0.95 2.2 18-24 62 2 14 0.96 0.95 2.2 24-30 46 0 21 1.0 0.91 3.2 30-36 25 1 11 0.93 0.91 3.2 36-42 13 0 6 1.0 0.85 5.5 42-48 7 0 4 1.0 0.85 5.5 48-54 3 0 2 1.6 0.85 5.5
Nonreversed translocated saphenous vein: 0-1 37 0 2 1.0 1.0 1-6 35 0 10 1.0 1.0 0.0 6-12 25 1 5 0.96 1.0 0.0
12-18 19 0 7 1.0 0.96 4.3 18-24 12 1 4 0.91 0.96 4.3 24-30 7 0 2 1.0 0.86 10.7 30-36 4 0 2 1.0 0.86 10.7 36-42 2 0 1 1.0 0.86 10.7 42-48 1 1 0 1.0 0.86 10.7
Alternative reversed vein bypass: 0-1 25 0 0 1.0 1.0 1-6 25 0 7 1.0 1.0 0.0 6-12 18 1 5 0.94 1.0 0.0
12-18 12 0 4 1.0 0.94 6.2 18-24 8 0 2 1.0 0.94 6.2 24-30 6 1 1 0.82 0.77 6.2 30-36 4 0 2 1.0 0.77 16 36-42 2 0 1 1.0 0.77 16 42-48 1 0 1 1.0 0.77 16
Copyright © 2022 FDOKUMEN




















