Motility and trafficking in B-cell non-Hodgkin's lymphoma (Review)

Multivariate Analysis of T-cell Functional Defects and Circulating Serum Factors in Ho dg kin 's Disease
RICHARD S. SCHULOF, MD, PHD, RICHARD S. BOCKMAN, MD, PHD, JOHN A. GAROFALO, MD, CONSTANCE CIRRINCIONE, MS, SUSANNA CUNNINGHAM-RUNDLES, PHD, GABRIEL FERNANDES, PHD, NOORBlBl K. DAY, PHD, CARL M. PINSKY, MD, GENEVIEVE S. INCEFY, PHD, HOWARD T. THALER, PHD,
ROBERT A. GOOD, PHD, MD, AND SUDHIR GUPTA, MB, BS
A comprehensive immunologic and serologic analysis was performed on 31 untreated patients with Hodgkin's disease. Immune evaluations stressed T-cell functional activity and included traditional parameters (PHA responsiveness and delayed hypersensitivity skin reactivity), as well as newer func- tional assays (T-cell colony formation, chemotaxis, spontaneous and antibody-dependent cytotoxicity , and concanavalin A-induced suppressor cell activity (CISA)). Serum factors included ferritin, prosta- glandins, zinc, copper, immune complexes, and thymic hormone activity. Every patient exhibited at least one T-cell or serum abnormality. The greatest percentage of patients exhibited T-cell defects in chemotaxis (85%), colony formation (81%), and PHA reactivity (64%). Immune defects were more common with advanced disease but were not related to absolute T-cell or monocyte count, skin test anergy, or abnormalities of TpIT y cell proportions. Linear relationships were identified among ab- normalities in the three assays employing mononuclear cells (PHA, colony formation, CISA) which may have reflected the inhibitory influence of monocytes present in the mononuclear cell preparations. Low serum zinc correlated with marked impairment of T-cell chemotaxis. Elevated prostaglandins were associated with high PHA reactivity and with depressed colony formation. Our results indicate that many complex factors, including intrinsic T-cell defects, contribute to the impaired immunity associ- ated with Hodgkin's disease.
Cancer 48:964-973, 1981.
ATIENTS with Hodgkin's disease (HD) frequently P exhibit impairments in a wide range of T-cell dependent immune functions.'-" Some of the ab- normalities, such as the depressed lymphoproliferative response to T-cell mitogens (e .g . , phytohemagglutinin, PHA), have been attributed to the presence of cir- culating non-T suppressor cells."H However, other reported defects reflect primary T-cell abnormalities. These include intrinsic functional defects such as im- paired T-cell locomotor activity,!'."' as well as a mal-
From the Memorial Sloan-Kettering Cancer Center, New York, New York.
Supported by NIH grants T32-CA-09207, CA-23766, CA-24476, CA-19267, CA-08748, CA-23500, AI-I 1843, and NS-I 1457.
Address for reprints: Richard S. Schulof, MD, PhD, Department of Medicine, Division of Hematology and Oncology, the George Washington University School of Medicine, 2150 Pennsylvania Avenue, N. W . , Washington. DC 20037.
The authors gratefully acknowledge the physicians on the Hematology-Lymphoma Service at Memorial Hospital for allowing us to study their patients: Ms. S. Sullivan for obtaining the blood specimens: Ms. T. Rosen, Mr. S. Ellis and Ms. J . Myers for per- forming the data compilation and computerization: and Dr. Maria de Sousa for help in preparing the manuscript.
Accepted for publication August 26, 1980.
distribution of different functional subsets of T-cells (Ty, Tp) between blood and spleen.!'-"
A number of serum abnormalities have also been de- scribed in association with HD.'"z3 Serum derange- ments include the presence of circulating immune
elevations in serum ferritini5 and prostaglandin (PGE) levels,"" and alterations of serum zinc and copper.20-22 It has also been shown that the presence of some inhibitory factors ( e . g . , ferritin, PGE) correlated with impairments of T-cell functions in vjrro, such as depressed E-rosette formation,"'-"' as well as depressed PHA-induced lymphoprolifera-
The present investigation used several recently de- veloped assays of T-cell functional activity in order to elucidate the extent of T-cell dysfunction in HD. Com- parisons were made between T-cell functional defects and abnormalities in more traditional immune param- eters, such as PHA reactivity and delayed hypersen- sitivity (DTHS) skin reactivity. In addition, i t was of interest to determine if any of the immune defects were related to abnormalities of well-defined circulating serum inhibitory substances. For this purpose, a com-
tion.f;,li
0008-543></81/08151964/$1.05 0 American Cancer Society
964

965 No. 4 T-CELL FUNCTION A N D SERUM FACTORS I N HODGKIN’S DISEASE . SChl4lqj’ct a / .
prehensive immunologic and serologic analysis was performed on 31 previously untreated adult patients with HD.
Materials and Methods
Putients
Thirty-one consecutive and previously untreated adult patients seen at Memorial Hospital from August 1978 to July 1979 were evaluated. The patients in- cluded 17 men and 14 women with a median age of 28 years (range 18-69) Tissue biopsy specimens were histologically subclassified by our pathology depart- ment according to the Rye system.24 Twenty-seven cases were classified as nodular sclerosing HD, and four as mixed cellularity. All patients subsequently underwent staging laparotomy (except those with clinically overt Stage IV disease) and were patho- logically staged according to the Ann Arbor system”’
IV-A, 3; IV-B, 3. Fifteen patients were considered to have localized (Stages 1 and 11) disease, and 16 (Stages 111 and 1V) as having widespread disease.
as follows: I-A, 4 ; 11-A, 8; 11-B, 3; 111-A, 5 : 111-B, 5 ;
Pnratn ct crs
Patients were evaluated in the two weeks immedi- ately preceding laparotomy procedures. All patients gave written informed consent prior to participating in the study. Blood specimens were obtained for ini- mune and serologic evaluations using two to three separate venipunctures. The following T-cell immune parameters were evaluated: (1) T-cell proportions and absolute numbers; (2) T-cell subset proportions (Tyl Tp); (3) PHA reactivity; (4) T-cell colony formation in soft agar; (5) Concanavalin A-induced suppressor cell activity (CISA); (6) T-cell mediated spontaneous (SLMC) and antibody dependent (ADCC) cytotoxicity; and (7) T-cell chemotaxis. Due to technical limitations resulting from the multi-laboratory nature of the study, it was not always possible to obtain complete immune tests on all patients. Twenty-five patients received delayed hypersensitivity skin testing (DTHS) using mumps, candida, streptokinase/streptodornase and PPD recall antigens and 15 patients had primary DNCB sensitization. Methods for skin testing have been pre- viously described.4 Lymphocyte and monocyte counts were determined using differentials obtained from Wright-stained blood smears.
The following serum factors were quantified: ( 1 ) serum copper and zinc: ( 2 ) serum immune complex levels; (3) ferritin; (4) serum prostaglandins (PGE); and (5) thymic hormone activity (factor thymique serique, FTS).
Pwpciriitioti oj‘ Ppripht.rii1 Blood Lymphocytes
Peripheral blood lymphocyte subpopulations were prepared as previously described.”’ Briefly, mono- nuclear cells (MC) were isolated from fresh heparinized blood by Ficoll-Hypaque (FH) density gradient centri- fugation. Aliquots of the MC were used in assays for PHA reactivity, T-cell colony formation, and CISA. MC were depleted of monocytes by allowing them to ingest carbonyl iron (Lymphocyte Separator reagent, Tarrytown, NY) followed by re-centrifugation on FH. Aliquots of monocyte-depleted lymphocytes (PBL) were used for analysis of E-rosette (E-RFC) per- centages. T-cells were isolated from PBL by E-rosette formation with neuraminidase-treated sheep red blood cells (nSRBC) followed by re-centrifugation on FH and lysis of nSRBC with tris-ammonium chloride. T-cells routinely included >95% E-RFC, < I % surface im- munoglobulin-bearing cells, and <0.3’1( peroxidase- staining’i (monocytes + granulocytes) cells. Purified T-cells were used for analysis of subset proportions and for evaluation of chemotaxis, SLMC, and ADCC.
T- Ccll ( I t i d T- Cell Sic hset An ci 1 y ~ i.)
T-cell (E-RFC) percentages were determined on PBL according to the method of Bentwich ct u1.2x Absolute levels were obtaining by multiplying E-RFC per- centages and the absolute lymphocyte count. T-cells with sutface Fc receptors for IgG (Ty cells) or IgM (Tp cells) were determined using purified T-cells (in- cubated overnight i n medium containing 20% fetal calf serum) and EA rosette formation employing IgG, or IgM-coated ox-RBC, respectively.”!’
Asstiys of 7-cell Firtiction
Detailed procedures for each assay have been pub- lished elsewhere. Briefly, (1) PHA responses were evaluated in microtiter plates using 96 hours of in- cubation. ’ Eight different concentrations of PHA-P (Difco Labs, Detroit, MI) (3 pg/ml -+ 286 pg/ml) were utilized to determine maximal “C-thymidine incorpora- tion. (2) T-cell colony assays were carried out using MC in medium supplemented with PHA and a double- layer semisolid agar technique.:”’ At the end of a seven- day incubation period, the number of colonies that contained >50 cells were scored with an inverted microscope. (3) CISA was assessed for the PHA- induced proliferative responses of both autologous and normal MC responder cells using two different sup- pressor/responder cell ratios (2: 1 and 1: I):” CISA was generated by incubating MC with 20 pg/ml Con A (Pharmacia Fine Chemicals, Piscataway, NJ) for 24 hours. An index of Con A-inducible suppressor cell
966 CANCER August 15 1981 Vol. 48
TABLE 1. Quantitative Abnormalities of Mononuclear Cell Subpopulations -
Percentages patients abnormal ~ ~~
All Stages Stages Parameters patients I and I1 111 and IV
Monocytosis
Lymphocy topenia
4 Percentage T-cells
J Absolute T-cells
J T p percentages
t Ty percentages
4 TpTy ratio ( ~ 3 . 3 ) 8S% (22126) 92% ( I 1/12) 79% ( I 1/14)
( > 450/mm:’)* 4’7% (14130)t 50% (7114) 44% (7116)
(<: 13201mm:’) 52% (16131) 40% (6115) 63% (10116)
(E-RFC) (<64%) 7% (2127) 8% (1113) 7% (1114)
(<10161mm’) 48% (13127) 46% (6113) 50% (7114)
( 4 1 5 % ) 4%; (l/26) 0% (0112) 7% (1114)
(> 20%) 5896 (15126) 58% (7112) 57% (8114)
* Values considered abnormal at our institution. : Numerator = total number of patients abnormal; denominator
= total number of patients studied.
activity (SISA) was calculated as previously de- scribed.:” (4) T-cell locomotion was evaluated in modified Boyden Chambers by the leading front method.!’ Casein (1 mg/ml (Merckes, Darmstadt, West Germany) and endotoxin activated serum (1%) were
used as chemoattractants. ( 5 ) T-cell SLMC and ADCC were assessed using ”‘Cr-labeled myeloid K562 cell lines, and IgG-coated “‘Cr-labeled chicken RBC, re- spectively as target cells, and target/effector ratios of 1:50.’’2 The calculation of cytotoxicity was pre- viou s I y described. : j r
Serum Factors
Serum PGE levels were determined by double anti- body radioimmunoassay.”3 Immune complexes were determined by the Raji cell technique of Theofilopoulos el al.34 Zn+ and CU++ levels were established by ap- propriate atomic absorption spectra analysis.” Cir- culating thymic hormone (FTS activity) was deter- mined on filtered plasma by the azathioprine rosette inhibition assay of Dardenne and Bach.:l5 Spleen cells from adult thymectomized C57B1/6 mice were utilized and the greatest dilution of tested sample that restored azathioprine sensitivity was considered the active concentration.
Control Subjects
Each assay of T-cell function was performed in a different laboratory at our institution. Each laboratory
TABLE 2. Comparison of Immune Parameters between Normal Subjects and Patients with Hodgkin’s Disease
Parameters
Hodgkin’s disease patients Normal subjects Stages I and I1 Stages I11 and IV
Percentages of TI* 48.2 r 4 . F 44.8 t 4.5 29.6 i- 2.7*[!
Percentages of Ty 10.6 t 1.3 23.3 t 3.3-1 21.3 t 2.61,
TdTY 5.1 t 0.6 2.9 f_ 0.91 1.8 f 0.3:
I’HA response (cpm) 20992.0 t 702.0 15745.9 t 1310.51 9196.7 t 1064.007
‘I-cell colonies 2274.0 i 360.0 785.5 i- 245.83 266.5 t 85.0s
CISA (summation index, SISA) 156.3 t 14.2 133.9 t 19.5 91.3 5 17.9t
SLMC (% cytolysis) 17.5 t 2.9 13.4 t 3.4 16.2 5 1.4
(15 ) (12) (14)
(15) (12) (14)
(15) (12) (14)
(27) (13) (9)
(13) (13) (13)
(20) (11) (11)
(27) (8) ( 10)
(28) (7) (9) ADCC (%; cytolysis) 45.2 t 5.1 54.7 ? 8.1 54.7 t 5.4
Chemotaxis (distance migrated in pM) Casein 99.8 t 3.1 53.8 5 12.0s 33.9 f 7.9s
EAS 84.5 t 4.4 48.3 2 10.29 36.9 t 10.09
(29) (6) (7)
(29) (6) (7)
Signifcant differences between normals and patient groups indi-
Significant differences between Stage 111-IV patients and Stage
1-11 patients indicated by: “ P < 0.05; 1 P < 0.0001.
in parentheses. cated by: * P << 0.05: t P < 0.02; i P < 0.001; S P < 0.0001. ** Numbers refer to mean t SEM; number of subjects indicated
No. 4 T-CELL FUNCTION A N D SERUM FACTORS I N HODGKIN'S DISEASE . SchUlof et a!. 967
has generated its own series of normal values using subjects reasonably matched in age (range 20-60 years) for the patients with Hodgkin's disease, and run concurrently with the patient samples.
Statisticul Methods"6
Laboratory measures were treated as both con- tinuous and categorical variables, the latter obtained by defining normal and abnormal ranges. Categorical data were examined using the chi-square procedure or the Fisher exact test for small samples. Correlations among continuous variables were determined using the Pearson product-moment correlation coefficient. Least squares linear regression was applied to those variables with significant correlations. Significant differences among normal subjects, patients with Stage 1-11 disease, and patients with Stage 111-IV disease were assessed by analysis of variance and the Tukey method for multiple comparisons. P values refer to two-sided tests. Because of the large number of tests performed, marginally significant results (P - 0.05) must be inter- preted with some caution.
For certain variables with skewed distributions, the base,,, logarithmic transformation was used to improve statistical efficiency. These measures were T-cell colonies, PHA, absolute T-cell counts, ferritin, TpITy and copperlzinc.
Results Cell Counts (Tubles 1 and 2)
Approximately half of the patients demonstrated absolute lymphocytopenia and monocytosis. More than 90% of the patients studied demonstrated normal percentages of T-cells (E-RFC); however, approxi- mately half of the patients exhibited absolute T-cell lymphopenia. There was a greater tendency for lymphocytopenia in Stage 111 -1V patients (63%) than in Stage 1-11 patients (40%). Tp-cell percentages were generally within the normal range. However, Ty-per- centages were elevated in more than 50% of patients, and abnormalities in the Tp/Ty ratio were detected in more than 80% of patients. In addition, both Stage 1-11 and Stage 111-IV patients exhibited statistically significant elevations in mean Ty cell proportions (P < 0.001) and depressions in the mean Tp/Ty ratio (P < 0.002) when compared with normal subjects. Stage 111-IV patients had significantly lower mean Tp-cell proportions (P = 0.004) compared with either the normal subjects or the Stage 1-11 patients.
Functional T-cell Defects (Tables 2 and 3)
The three immune functions that were most often abnormal were PHA responsiveness (64%), T-cell
TABLE 3. Abnormalities of Immune Functions
Percentages of patients abnormal
Parameters
J PHA response*
1 T-cell colonies*
4 USA* (SISA < 75) T-cell chemotaxist
(<15,000 cpm)'f
( < 860)
(<60 pM migration)
Casein EAS Either Casein or
EAS 1 T-cell SLMCt
(<lo%) 1 T-cell ADCCt
(< 30%) 1 In-vivn DTHS
Recall antigens" DNCB
All patients
64% (14122)s
81% (21126) 32% (7/22)
77% (10113) 62% (8113)
85% (11113)
22% (4/18)
13% (2116)
28% (7125) 20% (3115)
Stages I and I1
46% (6113)
69% (9113) 18% (2111)
50% (3/6) 50% (316)
67% (416)
38% (318)
14% (117)
25% (3112) 11% (119)
Stages 111 and I V
89% (8/9)
92% ( 121 13) 45% (511 1)
100% (7/7) 71% (517)
100% (717)
10% (1110)
1 I% (119)
31% (4113) 33% (216)
* Mononuclear cells used in assays. t Purified T-cells used in assays. 'f Values considered abnormal for individual assays shown in
5 Numerator = total number of patients abnormal; denominator
Considered abnormal when the patient was anergic to all four
parentheses.
= total number of patients studied.
recall antigens.
colony formation (81%), and T-cell chemotaxis (85% for defects resulting using either of the chemoat- tractants). There were highly significant ( P < 0.0001) impairments of each of these parameters in Hodgkin's disease patients with either widespread (Stage 111-IV) or localized (Stage 1-11) disease when compared with the normal subjects. CISA, SLMC, and DTHS re- sponses were abnormal in 20 to 35% of patients tested, whereas T-cell ADCC was abnormal in only 14% of patients. Mean CISA was significantly lower (P = 0.03) in Stage 111-IV patients compared with the normal controls. However, mean SLMC and ADCC were similar in the normal and Hodgkin's groups, regardless of stage. The functional T-cell defects were generally stage dependent and for each parameter studied (except SLMC and ADCC), a greater per- centage of Stage 111-IV patients were abnormal than Stage 1-11 patients. Nearly all of the evaluable Stage 111-IV patients exhibited abnormalities of PHA re- sponsiveness (89%), T-cell colony formation (92961, and T-cell chemotaxis (100%).
Serum Factors (Table 4 )
More than two thirds of evaluable patients exhibited detectable circulating immune complexes (76%) and elevated PGE levels (76%). The other serum factors
968 CANCER Augrrst 15 1981 Vol. 48
T 4 ~ i - t 4. Abnormalities of Circulating Serum Factors
Percentages of patients abnormal
All Stages Stages -
Parameters patients I and I1 111 and IV
1 Serum Z n t
f Serum Cui:
7‘ Cu/Zn ratio (>2.2) SS% (16129) 475% (7115) 64%. (9114) T Immune complexes
(Raji) (> I6 pg1ml) 76% (19125) 855% (11113) 67% (8112) 7 Ferritin
T Prostaglandins
1 Serum FTS
(<70 pg/dl)* 10%: (3129)t 0% (0.15) 21% (3114)
(>190 pgidl) 55% (16129) 40%) (6115) 715% (10114)
(>300 ng/ml) 28%. (5118) 20% (2110) 38% (318)
( > I . [ ng/ml) 76%. (13117) 75% (618) 78% (719)
activity: 54% (7113) 4395 (317) 67% (416)
x. Values considered abnormal at our institution. t Numerator == total number of patients abnormal; denominator
== total number of patients studied. $ The lower limits of normal vary according to age: <20 years,
21:32: 20- 30 years, 1?1:8; 3 0 4 40 years, >1:4; 40- 50 year.\, 2 I:2.
were less frequently abnormal. Serum zinc was only rarely (lo‘?; of patients) depressed, whereas elevations of serum copper were detected in approximately half of the patients. In general, Stage 111-IV patients ex- hibited a higher percentage of abnormalities (except for immune complexes) than the Stage 1-11 patients. The trend was most apparent with serum copper and FTS activity (studied in only 13 patients).
Corwlnriotis rrtnoiix Prirmierer.\ fig^. 1 -4)
Every patient studied exhibited at least one T-cell or serum abnormality. Each of the 28 patients who
I 3.000
c % I ,//
I . 1 3.oM) 3.m 4.m 4.m 5.000
LOG PHA
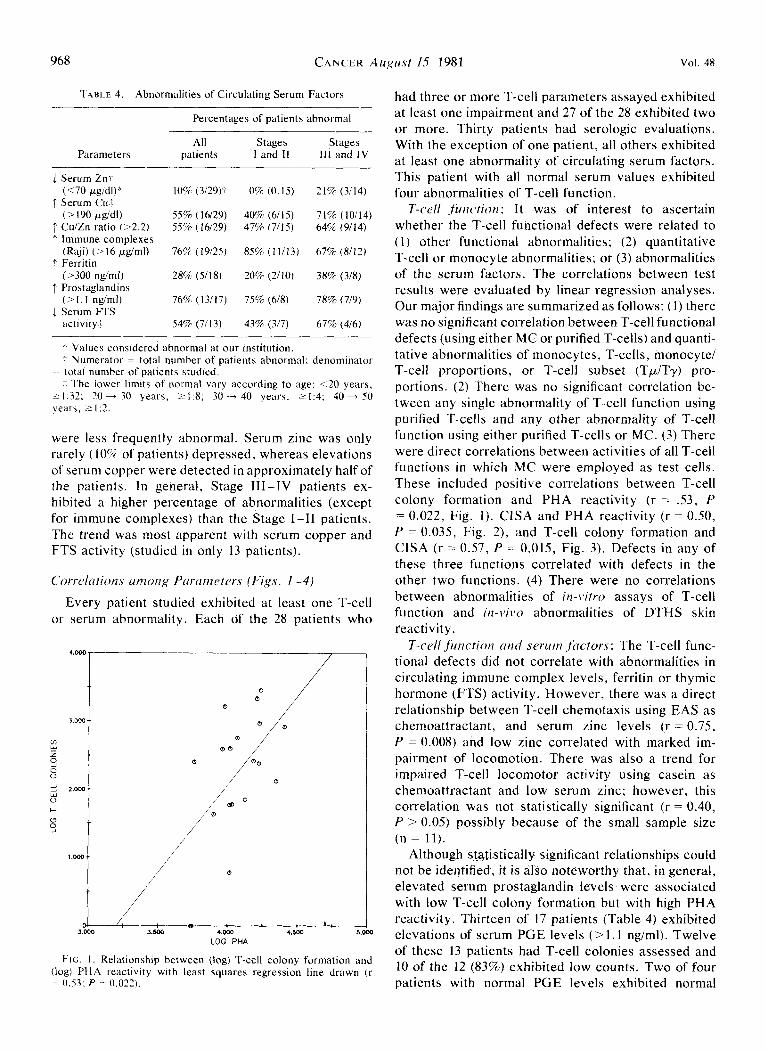
F I G . I . Relationship between (log) T-cell colony formation and (log) PHA reactivity with least squares regression line drawn ( r 7 0.53: P = 0.022).
had three or more T-cell parameters assayed exhibited at least one impairment and 27 of the 28 exhibited two or more. Thirty patients had serologic evaluations. With the exception of one patient, all others exhibited at least one abnormality of circulating serum factors. This patient with all normal serum values exhibited four abnormalities of T-cell function.
T-ccll Juriction: It was of interest to ascertain whether the T-cell functional defects were related to ( I ) other functional abnormalities; (2) quantitative T-cell or monocyte abnormalities; or (3) abnormalities of the serum factors. The correlations between test results were evaluated by linear regression analyses. Our major findings are summarized as follows: (1) there was n o significant correlation between T-cell functional defects (using either MC or purified T-cells) and quanti- tative abnormalities of monocytes, T-cells, monocyte/ T-cell proportions, or T-cell subset (TpITy) pro- portions. (2) There was no significant correlation be- tween any single abnormality of T-cell function using purified T-cells and any other abnormality of T-cell function using either purified T-cells or MC. (3) There were direct correlations between activities of all T-cell functions in which MC were employed as test cells. These included positive correlations between T-cell colony formation and PHA reactivity (r = .53, P = 0.022, Fig. I ) . CISA and PHA reactivity (r = 0.50, P = 0.035, Fig. 2), and T-cell colony formation and CISA (r = 0.57, P = 0.015, Fig. 3). Defects in any of these three functions correlated with defects in the other two functions. (4) There were no correlations between abnormalities of in-i . i fw assays of T-cell function and iti-vitso abnormalities of DTHS skin reactivity.
T-cell jirtiction and serum fnctors: The T-cell func- tional defects did not correlate with abnormalities in circulating immune complex levels, ferritin or thymic hormone (FTS) activity. However, there was a direct relationship between T-cell chemotaxis using EAS as chemoattractant, and serum zinc levels (r = 0.75, P = 0.008) and low zinc correlated with marked im- pairment of locomotion. There was also a trend for impaired T-cell locomotor activity using casein as chemoattractant and low serum zinc; however, this correlation was not statistically significant (r = 0.40, P > 0.05) possibly because of the small sample size (n = 11).
Although statistically significant relationships could not be identified, it is also noteworthy that, in general, elevated serum prostaglandin levels were associated with low T-cell colony formation but with high PHA reactivity. Thirteen of 17 patients (Table 4) exhibited elevations of serum PGE levels (>1.1 ngiml). Twelve of these 13 patients had T-cell colonies assessed and 10 of the 12 (83%) exhibited low counts. Two of four patients with normal PGE levels exhibited normal

No. 4 T-CELL FUNCTION A N D SERUM FACTORS I N HODGKIN'S DISEASE . S c h u b f e t a/ . 969
colony counts. In contrast, six of nine patients (67%) with elevated PGE levels exhibited PHA responses of > 13,000 cpm whereas all of the patients with normal PGE levels exhibited PHA responses below 13,000 cpm.
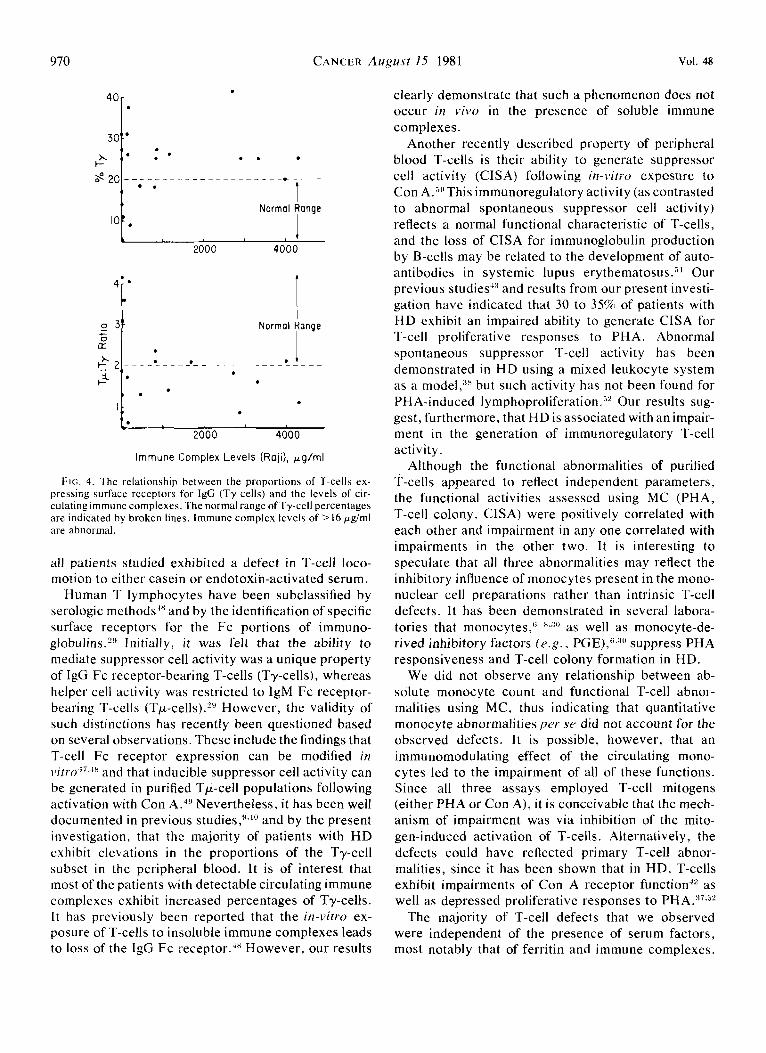
There were no significant correlations between altered T-cell subset proportions and abnormalities of circulating serum factors. Elevated Ty-proportions were almost always observed when immune complexes were detectable (Fig. 4). Ty-percentages were either normal or elevated in the absence of detectable immune complexes (< 16 pg/ml). There was a direct relation- ship (r = 0.50, P = 0.043) between absolute monocyte count and serum ferritin level. However, no correlation could be identified between monocyte count, lympho- cyte count, or T-cell count, and PGE.
Discussion
This investigation was undertaken to provide addi- tional insights into the mechanisms contributing to the impaired immunity in Hodgkin's disease. Previous
have indi- cated that the depressed immune responses are charac-
suppressor cell a b n ~ r m a l i t i e s ; ~ - ~ . ~ ~ , ~ " and (3) the presence of immunomodulating circulating serum factors. 17-19 The results of our multivariate analysis have demonstrated, as is generally accepted, that the vast majority of patients with HD exhibit abnormalities of T-cell immunity when a variety of assays are used. Indeed, every patient who had three or more T-cell functions assessed exhibited at least one abnormality. Even the patient with all normal serum values exhibited multiple defects of T-cell function.
It should be noted that most of the parameters ex- amined in our study have previously been shown to be abnormal in patients with Hodgkin's disease. Im- pairment of DTHS and of PBL proliferative responses have been well documented by US,^ and others.'-5 Although E-RFC percentages in H D have been shown to be abnormal in some report^,^*'"-'^^^^ other investi- gators,11,42 including ourselves,4,10.43 have found normal E-RFC percentages in the majority of untreated pa- tients. Nevertheless, it has been uniformly observed that absolute T-cell lymphopenia is common in Hodg- kin's disease patients. In the present investigation, more than half of the subjects exhibited such an ab- normality, which is consistent with other previous reports. 4 ~ 5 * 4 1
Several of the functional T-cell assays that we used have only recently been developed. These include the i n - v i m assessment of T-cell colony formation in semi- solid agar. One of us (RSB) has shown that this assay measures the clonal expansion of precursor T-cells under the stimulus of low concentrations of PHA."" It has also been shown that T-cell colony formation
studies by us9,10,37 and OtherS6-H.ll ,17--19,38-40
terized by (1) functional T-cell defect^,^-"*^^,^^ ( 2 )
M
F I G . 2 . Relationship between concanavalin A-induced suppressor cell activity (CISA) and (log) PHA reactivity with least squares regression line drawn (r = 0.50: P = 0.035).
is progressively depressed with advancing stage in HD.2" The magnitude of such a defect is illustrated by our observation that 81% of all patients studied in the present investigation exhibited an impairment of this parameter. Two of us (SG, GF) have also recently demonstrated that purified human T-cells exhibit directional movement (chemotaxis)"."' as well as SLMC and ADCC.32,44 We have recently shown that T-cells from patients with HD are frequently defective in these functions.9,10,45 In the present study, 85% of
ln
z 9 Q Q
0 V
w
j 2 . m W 0 l-
0 s
d ; : : : ! : : : : : : : : : 35 71 107 142 171) 214
CISA 9
FIG. 3. Relationship between (log) T-cell colony formation and concanavalin A-induced suppressor cell activity (CISA) with least squares regression line drawn (r = 0.57; P = 0.015).
970 CANCER AUgu.Yt I5 1981 Vol. 48
40r .
2 301 * . . , . . . t Normal Ronae
2000 4000 I.
'i' ;" O 31 K .
I Normol Ronge
11 . t- 2000 4000
Immune Complex Levels (Roji), pg/ml
F i c i . 4. The relationship between the proportions of T-cells ex- pressing surface receptors for IgG (Ty cells) and the levels of cir- culating immune complexes. The normal range of Ty-cell percentages are indicated by broken lines. Immune complex levels of 16 p g h l are abnormal.
all patients studied exhibited a defect in T-cell loco- motion to either casein or endotoxin-activated serum.
Human T lymphocytes have been subclassified by serologic methods'" and by the identification of specific surface receptors for the Fc portions of immuno- globulins.'" Initially, it was felt that the ability to mediate suppressor cell activity was a unique property of IgG Fc receptor-bearing T-cells (Ty-cells), whereas helper cell activity was restricted to IgM Fc receptor- bearing T-cells (Tp-cells).S!' However, the validity of such distinctions has recently been questioned based on several observations. These include the findings that T-cell Fc receptor expression can be modified in iiitro Ii.-'' and that inducible suppressor cell activity can be generated in purified Tp-cell populations following activation with Con A.49 Nevertheless, it has been well documented in previous studies,""' and by the present investigation, that the majority of patients with HD exhibit elevations in the proportions of the Ty-cell subset in the peripheral blood. I t is of interest that most of the patients with detectable circulating immune complexes exhibit increased percentages of Ty-cells. I t has previously been reported that the in-vitro ex- posure of T-cells to insoluble immune complexes leads to loss of the IgG Fc receptor.'H However, our results
clearly demonstrate that such a phenomenon does not occur in lvivo in the presence of soluble immune complexes.
Another recently described property of peripheral blood T-cells is their ability to generate suppressor cell activity (CISA) following in-\+tro exposure to Con A.""This immunoregulatory activity (as contrasted to abnormal spontaneous suppressor cell activity) reflects a normal functional characteristic of T-cells, and the loss of CISA for immunoglobulin production by B-cells may be related to the development of auto- antibodies in systemic lupus erythematosus.51 Our previous studies-'" and results from our present investi- gation have indicated that 30 to 35% of patients with HD exhibit an impaired ability to generate CISA for T-cell proliferative responses to PHA. Abnormal spontaneous suppressor T-cell activity has been demonstrated in HD using a mixed leukocyte system as a model,,'n but such activity has not been found for PHA-induced lymphoproliferation.j2 Our results sug- gest, furthermore, that HD is associated with an impair- ment in the generation of immunoregulatory T-cell activity .
Although the functional abnormalities of purified T-cells appeared to reflect independent parameters, the functional activities assessed using MC (PHA, T-cell colony, CISA) were positively correlated with each other and impairment in any one correlated with impairments in the other two. It is interesting to speculate that all three abnormalities may reflect the inhibitory influence of monocytes present in the mono- nuclear cell preparations rather than intrinsic T-cell defects. It has been demonstrated in several labora- tories that monocytes,"- '*du as well as monocyte-de- rived inhibitory factors ( ~ . g . , PGE),":{" suppress PHA responsiveness and T-cell colony formation in HD.
We did not observe any relationship between ab- solute monocyte count and functional T-cell abnor- malities using MC, thus indicating that quantitative monocyte abnormalities per se did not account for the observed defects. It is possible, however, that an immunomodulating effect of the circulating mono- cytes led to the impairment of all of these functions. Since all three assays employed T-cell mitogens (either PHA or Con A), i t is conceivable that the rnech- anism of impairment was via inhibition of the mito- gen-induced activation of T-cells. Alternatively, the defects could have reflected primary T-cell abnor- malities, since it has been shown that in HD, T-cells exhibit impairments of Con A receptor function42 as well as depressed proliferative responses to PHA."'."'
The majority of T-cell defects that we observed were independent of the presence of serum factors, most notably that of ferritin and immune complexes,

No. 4 T-CELL FUNCTION A N D SERUM FACTORS I N HODGKIN’S DISEASE . Schirluf ef al. 97 1
It must be stressed, however, that the assays were performed in medium that did not include autologous serum. Therefore, it would be expected that the in- fluence of circulating suppressive factors would be minimized unless they remained membrane bound ( e . g . , ferritin16 and immune complexes1x), were pre- viously internalized, or effected the normal physiologic activity of the lymphocytes prior to their isolation for immune testing ( e . g . , low serum zinc). It is interesting that a direct relationship existed between serum zinc levels and T-cell locomotor activity, but not between any of the other immune functions. Chronic zinc deficiency is associated with a number of defects of immune responsiveness.53,54 We would have antici- pated finding some relationship between low serum zinc and impairments of functional parameters since such an association has been well documented in animalss3 and mans4. However, the low serum zinc, found in only 10% of the patients studied (all with advanced disease), probably does not represent true nutritional zinc deficiency, but more likely redistribu- tion of serum zinc into various tissues such as the liver.55 The relationship between impaired T-cell chemotaxis and low serum zinc indicates that zinc is important for normal T-cell locomotor responses to chemotactic stimuli. Thus, our findings suggest that the impaired immunity associated with low serum zinc in cancer patients may be related to the defective mobilization of T-lymphocytes.
The quantitation in serum of any circulating sub- stance does not yield information regarding its site of origin. However, the positive relationship between absolute monocyte count and serum ferritin level sug- gests that circulating ferritin is, at least in part, mono- cyte-derived. Although ferritin is synthesized by reticuloendothelial cells in many different tissues, its synthesis by circulating monocytes has also been demonstrated.jG Our results suggest, furthermore, that the elevated serum ferritin levels observed in HD result from the monocytosis which frequently ac- companies the disease.
Although increased monocyte PGE synthesis has been demonstrated in HD,G*2“ we did not find any re- lationship between serum levels and absolute mono- cyte or lymphocyte counts. Thus, the serum values we obtained could have reflected either an ubiquitous origin of PGE in the body (including the tumor itself), or an increased production by monocytes (or a sub- population of monocytes) whose activity was not re- lated to the absolute monocyte count. We cannot explain why elevated serum PGE was associated with high PHA reactivity but with low T-cell colony forma- tion. It has been previously shown in carefully con- trolled i n - v i m studies that the addition of exogenous
PGE results in direct depression of both PHA re- activity”? and T-cell colony formation”) by PBL of normal subjects. It is possible that the serum PGE levels that we measured were not indicative of local PGE release by monocytes during the actual i n - v i m assay^.^^^^ However, it has also been demonstrated that PGE exerts different modulating effects on various subpopulations of T-cells, and whereas the PHA- induced proliferative responses of some high density T-cells are suppressed by PGE, responses of a low density T-cell subset are augmented by PGE.jX Thus, it is possible that the PHA-induced proliferative, and colony-forming assays that we used reflected the activi- ties of different subpopulations of T-cells.
In man, serum thymic hormone (FTS) levels become undetectable during the fourth and fifth decades of life.5g~6‘~ Patients with HD provide an ideal cancer patient group for evaluating defects of circulating FTS activity, since their median age is relatively young (in our study, 28 years). Thus, the age-matched control subjects would be expected to exhibit demonstrable FTS activity. Our results have confirmed previous observations that FTS levels are often depressed in HD.61 The low hormone activity could reflect either a primary abnormality of the endocrine thymus, or the effects of serum inhibitors which could interfere in the bioassay for FTS.6z Nevertheless, whatever the mechanism, we could not attribute low circulating FTS activity to any specific defect of T-cell function. However, the lack of correlation may be related to the small number of patients (13) that had FTS levels determined.
The present investigation was limited to an analysis of the immune and serum abnormalities associated with HD. The detailed clinical correlations to age, sex, histology, stage, B symptoms, tumor-cell bulk, and survival will be reported when we accrue a larger patient group and have a longer follow-up period. However, our results have several implications for further studies. The lack of concordance between skin test abnormalities and the i n - v i m functional assays of immunity illustrates the inadequacy of utilizing DTHS skin testing as a single method for assessing immune competence. In addition, it has recently been reported that a “lymphocyte score” based on abnor- malities of several different immune parameters proved to be a good prognostic indicator in HD.:j9 Therefore, a long-range goal of our program is to determine, using logistic regression methods, whether any combination of immune defects offers useful prognostic information for untreated patients. It would be of particular interest to see if a subgroup of patients with localized disease could be identified that might require more aggressive treatment regimens and vice versu. It is also apparent

972 CANCER Augusf 15 1981 Vol. 48
that future studies should employ autologous serum in the T-cell assays in order to elucidate more directly, the influence of well-defined serum factors on immune function.
REFERENCES
1. Schier WW. Cutaneous anergy in Hodgkin’s disease. N Engl .I Med 1954: 250:353-361.
2. Young RC, Corder MP, Haynes HA, DeVita VT. Delayed hypersensitivity in Hodgkin’s disease. A m J Med 1972: 52:63-72.
3 . Levy R, Kaplan HS. Impaired lymphocyte function inuntreated Hodgkin’s disease. N Engl J Med 1974: 298: 181 - 186.
4. Case DC, Hansen JA, Corrales E, e t ril. Comparison of multiple ir i i Y i w and irr i,itro parameters in untreated patients with Hodgkin’s disease. Cuncrr 1976: 38: 1807- 1815.
5. Holm G, Mellstedt H, Bjorkholm M, et t i / . Lymphocyte ab- normalities in untreated patients with Hodgkin’s disease. Cuncer 1976: 37:751-762.
6. Goodwin JS, Messner RP, Bankhurst AD, Peake GT, Saiki JK, Williams RC. Prostaglandin-producing suppressor cells in Hodgkin’s disease. N Engl .I Med 1977: 297:963-968.
7. Sibbit WL, Bankhurst AD, Williams RC. Studies of cell sub- populations mediating mitogen hyporesponsiveness in patients with Hodgkin’s disease. .I Clin / i i i . e . s t 1978: 61:55-63.
8. Schecter GP, Soehnlen F. Monocyte-mediated inhibition of lymphocyte blastogenesis in Hodgkin’s disease. Blood 1978: 52: 261-271.
9. Gupta S , Tan C. Subpopulations of human T lymphocytes. XVI. Abnormality of locomotion of T cells and of distribution of T cell subsets in peripheral blood and spleens from untreated chil- dren with Hodgkin‘s disease. Clin Immiinol ImmLmopUrhol 1980: 15:133-143.
10. Gupta S, Schulof R, Lee B, c’t ul. Imbalance of T-cell subsets and abnormal locomotion of T cells in untreated Hodgkin’s disease. In: Kaplan JG ed. The Molecular Basis of Immune Cell Function, New York: Elsevier, 1979:601-604.
I I . Romagnani S , Maggi E, Biagiotti R, Giudizi MG, Amadori A, Ricci M. Altered proportion of Tfi and Tysubpopulations in patients with Hodgkin’s disease. Scund J Immutzol 1978: 7:511-514.
12. de Sousa M, Yang M, Lopes-Corrales E, o r t i / . Ecostaxis: the principle and its application to the study of Hodgkin’s disease. Clin Exp Imrniinol 1977; 27:143-151.
13. Amlot PL, Pussell B, Slaney JM, Williams BD. Correlation between immune complexes and prognostic factors in Hodgkin’s disease. Clin E X ~ J / inmuno/ 1978: 3 1: 166- 175.
14. Brdndeis WE, Tan C , Wang Y, Good RA, Day NK. Cir- culating immune complexes, complement and complement com- ponent levels in childhood Hodgkin’s disease. Clin Exp Irnrnirriol 1980: 39:551-561.
15. Jones PA, Miller FM, Worwood M, Jacobs A. Ferritinaemia in leukemia and Hodgkin’s disease. Br J Cuncer 1973: 27:212-217.
16. Moroz Z, Lahat N, Binlaminor M, Ramot B. Ferritin on the surface of lymphocytes in Hodgkin’s disease patients. A possible blocking substance removed by levamisole. Clin Exp Imrizirnol 1977: 29:30-55.
17. Fuks Z, Strober S, Kaplan HS. Interaction between serum factors and T lymphocytes in Hodgkin’s disease. N EnRIJ Mrd 1976: 295: I273 - 1278.
18. Del Giacco GS, Tognella S, Leona Al, et (11. Interference of levamisole with inhibition of E-rosette formation by Hodgkin’s disease and systemic lupus erythematosus cytotoxic sera. Blood 1979: 53: 1002- 1006.
19. Ezdinli EZ, Simonson KL, Simonson LG, Wasser LP. T and B-RFC inhibiting factor in plasma from patients with active Hodgkin’s disease. Curiccv 1979: 44: 106- 115.
20. Gobbi PG, Scarpellini M, Minvia C, Pozzoli L, Perugini S. Plasma zinc levels in Hodgkin’s disease. Evaluation of 37 cases.
21. Thorling EB. Thorling K. The clinical usefulness of serum Ntrrrncilologic.tr 1978: 63: 144- 155.
copper determinations in Hodgkin’s disease. A retrospective study of 211 patients from 1963-1973. Cuncer 1976: 38:225-231.
22. Garofalo JA, Lacher MJ, Lee BJ, Lesser M, Schwdrtz MF, Good R. Serum zinc, serum copper and the Cu/Zn ratio in patients with untreated Hodgkin’s disease (in preparation).
2 3 . Bockman RS. Stage dependent reduction in T-colony forma- tion in Hodgkin’s disease: coincidence with monocyte synthesis of prostaglandins. J Clin Invest 1980; 66:523-531.
24. Lukes RJ, Craver LF, Hall TC, Rappaport H , Ruben P. Report of the nomenclature committee. Cancer Res 1966; 26:1311.
25. Carbone PP, Kaplan HS, Mushoff K, Smothers DW, Tubiana M. Report of the committee of Hodgkin’s disease staging classifica- tion. Cuncer Res 1971: 31:1860-1861.
26. Gupta S, Good RA. Subpopulations of human T lympho- cytes. 11. Effect of thymopoietin, corticosteroids and irradiation. Cell Itn~nrtnol 1977; 34: 10- 18.
27. Yam LT, Li CY, Crosby WH. Cytochemical identification of monocytes and granulocytes. A m J Clin Purhol 1971; 55:283-290.
28. Bentwich Z, Douglas SD, Siegal FP, Kunkel HG. Human lymphocyte sheep erythrocyte rosette formation: some charac- teristics of the interaction. Clin Ii~niiinol Immunoprithol 1973; 1:
29. Moretta LA, Ferrarini M, Mingari C, Moretta A, Webb SR. Subpopulations of human T cells identified by receptors for immuno- globulins and mitogen responsiveness. J Iwzrn~ifio/ 1976; 117: 2 17 1-2 174.
30. Bockman RS, Rothschild M. Prostaglandin E inhibition of T- lymphocyte colony formation. A possible mechanism of monocyte modulation of clonal expansion. J Clin Invest 1979: 64:812-819.
31. Schulof RS, Garofalo JA, Good RA, Gupta S. Concanavalin A-induced suppressor cell activity for T-cell proliferative responses: autologous and allogeneic suppression in aging humans. Cell Ini- azunol 1980; 56:80-88.
32. Gupta S, Fernandes G, Nair M, Good RA. Spontaneous and antibody dependent cell-mediated cytotoxicity by human T-cell subpopulations. Proc Nut/ Acrid Sci U S A 1978: 75:5137-5141.
33. Kurland J1, Bockman RS. prostaglandin E production by human blood monocytes and mouse peritoneal macrophages. J Exp Med 1978: 147:952-957.
34. Theofilopoulos A N , Wilson CB, Bokisch VA, Dixon FJ. Binding of soluble immune complexes to human lymphoblastoid cells. 11. Use of Raji cells to detect circulating immune complexes in animal and human sera. J E.xp Med 1974; 140:1230- 1244.
35. Dardenne M, Bach IF. The sheep cell rosette assay for the evaluation of thymic hormones. In: Van Bekum D, ed. The Biological Activity of Thymic Hormones, New York: Halsted Press, 1975:
36. Zar JH. Biostatical Analysis, Englewood Cliffs, Prentice Hall, Inc., 1974.
37. Schulof RS, Lacher MJ, Gupta S. Abnormal phytohemag- glutinin-induced T-cell proliferative responses in Hodgkin’s disease
38. Hillinger SM, Herzig GP. Impaired cell-mediated immunity in Hodgkin’s disease mediated by suppressor lymphocytes and mono- cytes. J Cliri I n i * c . . ~ f 1978: 50: 1620- 1626.
39. Bjorkholm M. Immunodeficiency in Hodgkin’s disease and its relation to prognosis. Scund J Haernutol 1978: Suppl 33.
40. Han T. Role of suppressor cells in depression of T lympho- cyte proliferative response in untreated and treated Hodgkin’s disease. Cuncrr 1980; 45:2 102 - 2 108.
41. Bobrove AM, Fuks Z, Strober S, Kaplan HS. Quantitation of T and B lymphocytes and cellular immune function in Hodgkin’s disease. Cancer 1975; 36: 169- 179.
42. Aisenberg AC, Weitzman S, Wilkes B. Lymphocyte receptors for concanavalin A in Hodgkin’s disease. Blood 1978: 51:439-443.
43. Schulof RS, Lee BJ, Lacher MJ, PI ul. Concanavalin A induced suppressor cell activity in Hodgkin’s disease. chi lrnrnitnol / i r i i~ iun~~pcirho/ 1980: 16:454-462.
44. Pross JF, Jondal M. Cytotoxic lymphocytes from normal donors. A functional marker of human non-T lymphocytes. Cliri E.rp I i i i ~ i r i i t i o l 1975: 21:226-235.
5 1 1-522.
145- 158.
Blood 1981: 57:607-613.

No. 4 T-CELL FUNCTION AND SERUM FACTORS IN HODGKIN'S DISEASE ' SChLllUfet a[. 973
45. Gupta S, Fernandes G, Schulof RS, Good RA. Spontaneous and antibody-dependent cellular cytotoxicity by T and non-T cells in Hodgkin's disease (manuscript in preparation).
46. Reinherz EL, Schlossman SF. The differentiation and function of human T lymphocytes. Cell 1980: 19:821-827.
47. Schulof RS, Fernandes G, Good RA, Gupta S. Neuraminidase treatment of human T lymphocytes: effect on Fc receptor phenotype and function. Clin Exp lmmunol 1980; 40:611-619.
48. Pichler WJ, Lum L, Broder S. Fc receptors on human T lymphocytes 1. Transition of Ty to T p cells. J lmmunol 1978: 12 1 : 1540- 1548.
49. Hayward AR, Lagward I , Lydyard PM, Morettd L, Dagg M, and Lawton AR. Fc-receptor heterogeneity of human suppressor T cells. J Imrnunol 1978; 121:l-5.
50. Shou L, Schwartz SA, Good RA. Suppressor cell activity after concanavalin A treatment of lymphocytes from normal donors. J Exp Med 1976; 143: 1100- 1 1 10.
51. Fauci AS, Steinberg AD, Haynes BF, Walen G. Immuno- regulatory aberrations in systemic lupus erythematosus. J Imrnunol 1978: 12 1 : 1473 - 1479.
52. Han T. Role of suppressor cells in depression of T lymphocyte proliferative response in untreated and treated Hodgkin's disease. Cuncer 1980: 45:2 102-2 108.
53. FernandesG, Nair M, One0 K , TanakaT, Floyd R, Good RA.
Impairment of cell-mediated immunity functions by dietary zinc deficiency in mice. Proc Nut/ Acud Sci USA 1979: 76:457-461.
54. Schloen LH, Fernandes G, Garofalo JA, Good RA. Nutrition, immunity and cancer-a review. 11. Zinc, lmmune function and cancer. Clin Bull 1979: 9:63-75.
55. Burch RE, Sullivan JF. Clinical and nutritional aspects of zinc deficiency and excess. Med Clin North A m 1916: 60:675-685.
56. Summers M, White G, Jacobs A. Ferritin synthesis in lympho- cytes, polymorphsand monocytes. BrJHaemarolt975: 30:425-434.
57. Goodwin JS, Webb DR. Regulation of the immune response by prostaglandins. Clin lrnmunol lmmunoputhol 1980; 15:106- 122.
58. Stobo JD, Kennedy MS, Goldyne ME. Prostaglandin E modulation of the mitogenic response of human T cells. J CIin Int'est
59. Bach JF, Bach MA, Blanot D, et ul. Thymic serum factor (FTS). Bull Insrit Pusteur 1978; 76:325-337.
60. lncefy GS, Dardenne M, Pahwa S, Grimes E, Pahwa RN, Smithwick E, er ul. Thymic activity in severe combined immuno- deficiency disease. Proc Natl Acud Sci USA 1977; 74:1250- 1253.
61. Goldstein AL, Hooper JA, Schulof RS, er ul. Thymosin and the immunopathology of aging. Fed Proc 1974; 33:2053-2056.
62. Twomey JJ, Lewis V M , Ford R. An inhibitor of thymic hormone activity in serum from patients with lymphoblastic leu- kemia. Am J Med 1980; 68:377-380.
1979: 64: 1188-1 195.
Copyright © 2022 FDOKUMEN