
Multisorbent Plasma Perfusion in Fulminant Hepatic Failure: Effects of Duration and Frequency of...
10
Multisorbent Plasma Perfusion in Fulminant Hepatic Failure: Effects of Duration and Frequency of Treatment in Rats with Grade III Hepatic Coma *Calvin J. Ryan, *Thapasimuthu Anilkumar, *Abdul J.A. Ben-Hamida, *Shirin E. Khorsandi, *Mohammed Aslam, ²Charles D. Pusey, ‡John D.S. Gaylor, and ‡James M. Courtney *Division of Surgery, Anaesthetics, and Intensive Care; ²Division of Medicine, Imperial College School of Medicine, Hammersmith Hospital Campus, London; and ‡Bioengineering Unit, University of Strathclyde, Glasgow, U.K. Abstract: Using the model of galactosamine-induced ful- minant hepatic failure in the rat, the effects of multisor- bent plasma perfusion over Asahi uncoated spherical char- coal, Plasorba (BR-350) resin, and an endotoxin removing adsorbent (polymyxin B-sepharose) were determined in Grade III hepatic coma animals by studying survival as influenced by timing, duration, and frequency of treat- ment. The effects of treatment on liver cell proliferation and endotoxin removal also were examined. The results demonstrate that duration and frequency of treatment are major contributing factors in the successful application of nonbiological membrane-based multisorbent liver support systems. Examination of the regenerative activity in the liver indicates an enhanced proliferative response follow- ing multisorbent plasma perfusion compared with un- treated fulminant hepatic failure (FHF) paired controls. Utilizing an endotoxin removal adsorbent alone, a marked reduction in systemic levels of endotoxin in FHF was dem- onstrated compared with nonperfused FHF paired con- trols. Despite current emphasis on bioartificial liver sup- port systems, plasma purification by multisorbent systems offers a simple method for the removal of circulating toxic metabolites in general together with specific toxin re- moval. Key Words: Liver failure—Support—Perfu- sion—Rat—Galactosamine—Endotoxin—Regeneration. Consideration of artificial liver support must rec- ognize the complexity of fulminant hepatic failure (FHF) syndrome, and the influence of the associated pathophysiological disorders on other organs and systems in the body (1). Overall, the consequences of the toxic effects of liver failure are the development of encephalopathy and cerebral edema, multiorgan failure, infection, and possible inhibition of liver re- generation. The accumulation in the circulation of high levels of toxic metabolites has led to the belief that one of the primary functions of an artificial liver support system is the removal of these potentially pathogenic molecules. However, the selection of a detoxification system in artificial liver support is complicated by the uncertainty regarding the nature and role of the toxic metabolites involved. There has been a long-standing interest in the po- tential role of sorbents as a nonbiological approach to the treatment of FHF. The application of these procedures has shifted with time, from the use of a single sorbent such as charcoal to that of multiple sorbents, and from the direct passage of blood over a sorbent in hemoperfusion to the purification of plasma in plasma perfusion (2–6). The aim of this study was to explore the potential clinical application of multisorbent plasma perfusion as an artificial liver support system in the treatment of FHF, utilizing the rat as an experimental model. Plasma perfusion over charcoal, anion exchange resin, and an endotoxin removal sorbent (multisor- bent regimen) was examined in Grade III hepatic coma animals. The effects of timing, duration, and frequency of treatment on survival were determined. Received May 2000; revised September 2000. Address correspondence and reprint requests to Dr. Calvin J. Ryan, Division of Surgery, Anaesthetics and Intensive Care, Im- perial College School of Medicine, Hammersmith Hospital Cam- pus, Du Cane Road, London W12 ONN, U.K. Artificial Organs 25(2):109–118, Blackwell Science, Inc. © 2001 International Society for Artificial Organs 109
-
Upload
imperialcollege -
Category
Documents
-
view
0 -
download
0
Transcript of Multisorbent Plasma Perfusion in Fulminant Hepatic Failure: Effects of Duration and Frequency of...

Multisorbent Plasma Perfusion in Fulminant HepaticFailure: Effects of Duration and Frequency of Treatment in
Rats with Grade III Hepatic Coma
*Calvin J. Ryan, *Thapasimuthu Anilkumar, *Abdul J.A. Ben-Hamida,*Shirin E. Khorsandi, *Mohammed Aslam, †Charles D. Pusey, ‡John D.S. Gaylor, and
‡James M. Courtney
*Division of Surgery, Anaesthetics, and Intensive Care; †Division of Medicine, Imperial College School of Medicine,Hammersmith Hospital Campus, London; and ‡Bioengineering Unit, University of Strathclyde, Glasgow, U.K.
Abstract: Using the model of galactosamine-induced ful-minant hepatic failure in the rat, the effects of multisor-bent plasma perfusion over Asahi uncoated spherical char-coal, Plasorba (BR-350) resin, and an endotoxin removingadsorbent (polymyxin B-sepharose) were determined inGrade III hepatic coma animals by studying survival asinfluenced by timing, duration, and frequency of treat-ment. The effects of treatment on liver cell proliferationand endotoxin removal also were examined. The resultsdemonstrate that duration and frequency of treatment aremajor contributing factors in the successful application ofnonbiological membrane-based multisorbent liver supportsystems. Examination of the regenerative activity in the
liver indicates an enhanced proliferative response follow-ing multisorbent plasma perfusion compared with un-treated fulminant hepatic failure (FHF) paired controls.Utilizing an endotoxin removal adsorbent alone, a markedreduction in systemic levels of endotoxin in FHF was dem-onstrated compared with nonperfused FHF paired con-trols. Despite current emphasis on bioartificial liver sup-port systems, plasma purification by multisorbent systemsoffers a simple method for the removal of circulating toxicmetabolites in general together with specific toxin re-moval. Key Words: Liver failure—Support—Perfu-sion—Rat—Galactosamine—Endotoxin—Regeneration.
Consideration of artificial liver support must rec-ognize the complexity of fulminant hepatic failure(FHF) syndrome, and the influence of the associatedpathophysiological disorders on other organs andsystems in the body (1). Overall, the consequences ofthe toxic effects of liver failure are the developmentof encephalopathy and cerebral edema, multiorganfailure, infection, and possible inhibition of liver re-generation. The accumulation in the circulation ofhigh levels of toxic metabolites has led to the beliefthat one of the primary functions of an artificial liversupport system is the removal of these potentiallypathogenic molecules. However, the selection of adetoxification system in artificial liver support is
complicated by the uncertainty regarding the natureand role of the toxic metabolites involved.
There has been a long-standing interest in the po-tential role of sorbents as a nonbiological approachto the treatment of FHF. The application of theseprocedures has shifted with time, from the use of asingle sorbent such as charcoal to that of multiplesorbents, and from the direct passage of blood overa sorbent in hemoperfusion to the purification ofplasma in plasma perfusion (2–6).
The aim of this study was to explore the potentialclinical application of multisorbent plasma perfusionas an artificial liver support system in the treatmentof FHF, utilizing the rat as an experimental model.Plasma perfusion over charcoal, anion exchangeresin, and an endotoxin removal sorbent (multisor-bent regimen) was examined in Grade III hepaticcoma animals. The effects of timing, duration, andfrequency of treatment on survival were determined.
Received May 2000; revised September 2000.Address correspondence and reprint requests to Dr. Calvin J.
Ryan, Division of Surgery, Anaesthetics and Intensive Care, Im-perial College School of Medicine, Hammersmith Hospital Cam-pus, Du Cane Road, London W12 ONN, U.K.
Artificial Organs25(2):109–118, Blackwell Science, Inc.© 2001 International Society for Artificial Organs
109
Examination of the relationship between degree ofhepatic coma, rate of liver regeneration, and treat-ment also was undertaken. Separate studies wereperformed to determine the potential of an endotox-in removal sorbent alone on survival.
MATERIALS AND METHODS
Animals and operative proceduresFemale Sprague-Dawley rats weighing between
265 to 325 g were used. All animals were caged in-dividually and allowed free access to food and water.All surgical procedures were performed under etheranesthesia and were clean but not sterile.
Induction of acute liver failureAcute FHF was induced by the intraperitoneal in-
jection of D(+) galactosamine hydrochloride (Gal-HCl) (Sigma Chemical Co. Ltd., Dorset, U.K.) at adose of 2.5 g/kg of body weight, using a modificationof techniques previously described (7–9). Prior toinjection, the Gal-HCl was dissolved in 0.9% salineand adjusted to physiological pH with 5N NaOH.Previously reported work established methods foridentifying animals in Grades I through IV hepaticcoma (8,9) following the system used for clinicalstaging (10). The characteristic features associatedwith the various stages of hepatic coma are Grade I(lethargy), Grade II (confusion and stupor butawake), Grade III (sleeping most of the time, butarousable, with occasional convulsions), and GradeIV (unarousable and unresponsive to pain, occa-sional convulsions). Blood glucose was maintainedby the inclusion of glucose in the drinking water inthe initial stages and thereafter by injection as andwhen required.
Blood accessThe technique for insertion of indwelling carotid
arterial (CA) and jugular venous (JV) cannulas, al-lowing perfusion in the unrestrained and consciousstate, was described in detail elsewhere (11,12). Thisminimizes any possible effects from stress and elimi-nates the necessity for anesthesia during the periodof perfusion.
Multisorbent plasma perfusionThe features and suitability of the membrane
plasma separation stage for performing multisorbentplasma perfusion in animals suffering from Gal-HCl-induced hepatic failure were previously described(8). With this system, we have demonstrated thatrepeated plasma separation can be performed at atransmembrane pressure <50 mm Hg and a filtrationrate of 0.21 to 0.22 ml/min (corresponding to thetreatment of 1 complete plasma volume) within 50 to
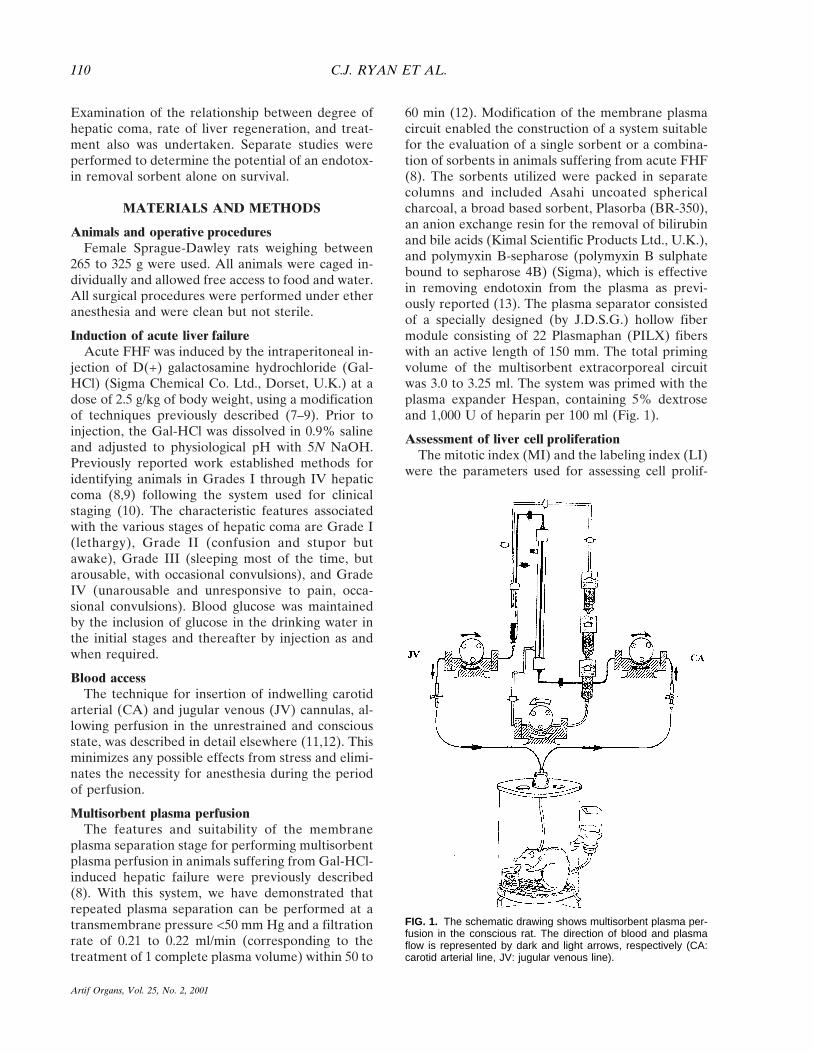
60 min (12). Modification of the membrane plasmacircuit enabled the construction of a system suitablefor the evaluation of a single sorbent or a combina-tion of sorbents in animals suffering from acute FHF(8). The sorbents utilized were packed in separatecolumns and included Asahi uncoated sphericalcharcoal, a broad based sorbent, Plasorba (BR-350),an anion exchange resin for the removal of bilirubinand bile acids (Kimal Scientific Products Ltd., U.K.),and polymyxin B-sepharose (polymyxin B sulphatebound to sepharose 4B) (Sigma), which is effectivein removing endotoxin from the plasma as previ-ously reported (13). The plasma separator consistedof a specially designed (by J.D.S.G.) hollow fibermodule consisting of 22 Plasmaphan (PILX) fiberswith an active length of 150 mm. The total primingvolume of the multisorbent extracorporeal circuitwas 3.0 to 3.25 ml. The system was primed with theplasma expander Hespan, containing 5% dextroseand 1,000 U of heparin per 100 ml (Fig. 1).
Assessment of liver cell proliferationThe mitotic index (MI) and the labeling index (LI)
were the parameters used for assessing cell prolif-
FIG. 1. The schematic drawing shows multisorbent plasma per-fusion in the conscious rat. The direction of blood and plasmaflow is represented by dark and light arrows, respectively (CA:carotid arterial line, JV: jugular venous line).
C.J. RYAN ET AL.110
Artif Organs, Vol. 25, No. 2, 2001

eration in the liver. Identification of S-phase cellswas carried out by the immunohistochemical detec-tion of the preinjected thymidine analog bromode-oxyuridine (BrdUrd) (Sigma) using a simple 2 stageindirect immunoperoxidase technique on routinelyprocessed, paraffin-wax-embedded tissue sections.BrdUrd was given at a dose of 50 mg/kg of bodyweight intraperitoneally, 45 to 60 min before sacri-ficing (9). To determine MI or LI, hepatocytes werescored continuously, and the number of mitotic cellsand labeled cells were counted. The values are ex-pressed as percentages (of the total cell count) ± SD.
Biochemical estimationsPlasma bilirubin, alkaline phosphatase, asparate
aminotransferase, alanine aminotransferase, andblood glucose were measured using microtechniquesbased on a routine biochemical autoanalyzer. Endo-toxin was measured by the chromogenic limulusamoebocyte lysate assay as previously reported (13).
Experimental designA total of 535 animals was used. Each animal was
subjected to cannulation of the carotid artery andjugular vein, and then allowed to recover. AcuteFHF was induced by the intraperitoneal injection of2.5 gm/kg of Gal-HCl 21 h later, and the course ofeach animal was followed. Approximately 40 hthereafter, the majority of animals were in Grades IIand III hepatic coma. Of these, only those exhibitingGrade III hepatic coma (sleeping most of the timebut arousable, with occasional convulsions) were se-lected for perfusion and control procedures (n 4219). Throughout the period of investigation, ani-mals in groups of 3 suffering from Grade III hepaticcoma (n 4 30) were selected and sacrificed at ran-dom for biochemical and histological examination toconfirm that the clinical signs of coma and severity ofdisease were the result of liver injury and not due toany other cause. The remaining animals (n 4 189)were pair matched and allocated to 3 separate ex-perimental studies.
Evaluation of multisorbent plasma perfusion onsurvival in FHF
Membrane plasma separation with online sorbenttreatment of plasma was used to assess the influenceof a multisorbent regimen on the course of galactos-amine (GalN)–induced acute FHF in rats sufferingfrom Grade III hepatic coma (n 4 120). On a ran-dom basis, animals were allocated to either multisor-bent plasma perfusion (n 4 60) or control proce-dures in which no perfusion was performed (n 4 60).The most effective treatment regimen (timing, dura-tion, and frequency) was determined. The multisor-
bent regimen consisted of Asahi uncoated sphericalcarbon, BR-350 resin, and polymyxin B-sepharose(PB-Seph). At all times, blood glucose levels weremonitored and corrected accordingly in both per-fused and nonperfused animals.
Seventy-five multisorbent plasma perfusions forvarying durations/frequencies were performed in 60FHF animals. Of these, 15 animals (Group 1) weresubjected to perfusion until 1 complete plasma vol-ume had been treated. Two further groups of 15 ani-mals (Groups 2 and 3) were subjected to perfusionuntil 2 and 4 plasma volumes were treated, respec-tively. In the remaining 15 animals (Group 4), 2 con-secutive multisorbent plasma perfusions were per-formed 4 h apart. In this group, 2 plasma volumeswere treated on each occasion. The remaining FHFanimals (n 4 60) were equally divided into 4 groupsas nonperfused paired controls. An attempt also wasmade in additional animals to perform 3 consecutivemultisorbent plasma perfusions each for the dura-tion of 2 plasma volumes. However, these animalswere unable to tolerate 3 consecutive treatmentsover such a short period of time (i.e., 4 h apart) dueto the effects of hemodilution and were excludedfrom the study.
Effects of multisorbent plasma perfusion on liverregeneration in FHF
Measurement of liver cell proliferation was madein a separate group of 39 FHF Grade III animalssubjected to multisorbent plasma perfusion or con-trol procedures. On a random basis, animals wereallocated to either multisorbent perfusion or controlprocedures. A total of 24 multisorbent plasma per-fusions were performed for varying times to coincidewith Groups 1, 2, and 3 previously mentioned. Ani-mals subjected to multisorbent plasma perfusion (n4 24) were divided equally into 3 groups of 8 ani-mals and subjected to 1 (Group P1), 2 (Group P2),and 4 (Group P4) plasma volume treatments. Allanimals were sacrificed 6 h after initiation of treat-ment. The remaining FHF animals were divided into2 groups of 7 and 8 animals, respectively, and servedas nonperfused controls. The first group (Group K)was sacrificed at the time of initiation of perfusion toascertain levels of proliferation at the start of treat-ment. The second group (Group C) was sacrificed 6h later to coincide with animals in Groups P1, P2,and P4.
Effects of endotoxin removal alone on survivalin FHF
Since endotoxemia is recognized to be an impor-tant factor in FHF, separate studies were performedin order to determine the adsorptive properties of
MULTISORBENT PLASMA PERFUSION IN EXPERIMENTAL LIVER FAILURE 111
Artif Organs, Vol. 25, No. 2, 2001

PB-Seph on the removal of endotoxin and the effectson survival in Grade III hepatic coma rats. On arandom basis, animals were allocated to either per-fusion or control procedures. In order to investigatethe potential of PB-Seph alone in the treatment ofGrade III hepatic coma, 2 columns were utilized foreach perfusion period (i.e., double the amount ofPB-Seph used in the multisorbent regimen). Eachperfusion period was for the duration of 2 plasmavolumes. Thirty procedures were performed in 30animals. Of these, 15 animals were subjected tomembrane plasma separation with online PB-Sephtreatment of plasma. The remaining animals servedas nonperfused paired controls. Serial blood sampleswere taken for measurement of plasma endotoxinlevels immediately before perfusion, and thereafterfollowing 1 and 2 plasma volume treatments, respec-tively. Serial blood samples were taken from non-perfused paired controls at selected times to coincidewith those subjected to perfusion.
Statistical analysisAll results are expressed as mean ±1 SD and ana-
lyzed by binomial distribution test and Student’s ttest where appropriate.
RESULTS
General observationsAll animals tolerated the surgical cannulation pro-
cedures well and regained consciousness within 10 to15 min of the operation. For animals subjected toplasma perfusion, blood flow remained constantthrough the extracorporeal circuit at 0.8 ml/min, andthere was no evidence of clots or fibrin strandswithin the various columns on examination. The fil-tration rate averaged 0.25 ml/min, thus allowing ap-proximately 1 plasma volume to be treated for each50 min of perfusion. Both arterial and venous in-dwelling cannulas remained patent throughout theperiod of investigation.
Confirmation of hepatic coma and liver damageThe deterioration of consciousness in rats follow-
ing GalN-induced FHF with time is shown in Fig. 2,and the results are expressed as mean ± SD. Theresults demonstrate that 36 to 40 h after injection,animals were either in Grades II or III hepatic coma;only those animals exhibiting Grade III hepaticcoma (sleeping most of the time but arousable, withoccasional convulsions) were selected for perfusionand control procedures in this study. The remaininganimals were either utilized for other experimentalwork not related to this investigation or allowed toprogress to Grade IV hepatic coma (unarousable,
and unresponsive to pain, occasional convulsions)and death. Detailed histological and biochemicaldata obtained from Grade III coma animals selectedat random throughout the period of investigationshowed severe hepatocellular injury in line withacute liver necrosis, including complete dissociationof liver cell plates and bleeding in central portal andmidzonal areas together with signs of mitotic activ-ity. The results confirmed a close relationship be-tween the severity of liver injury and the deteriora-tion of consciousness (i.e., development of hepaticcoma). Table 1 illustrates the main biochemicalchanges for animals selected and sacrificed at ran-dom in Grade III hepatic coma (n 4 30). The valuesobtained from 10 normal healthy animals also areshown. The results are expressed as mean ± 1 SD.
Survival following multisorbent plasma perfusionOne hundred thirty-five multisorbent plasma per-
fusions/control procedures were performed in 120animals suffering from Grade III hepatic coma. Atotal of 75 multisorbent plasma perfusions were per-formed in 60 FHF animals. The survival rates ofGrade III hepatic coma rats treated by different regi-
FIG. 2. The graph depicts the deterioration in consciousnesswith time for animals with FHF.
TABLE 1. Main biochemical changes for Grade IIIhepatic coma rats
Biochemical units Normal values Grade III hepatic coma
AST 98 ± 15 3,800 ± 180ALT 65 ± 8 2,105 ± 165AP 120 ± 16 450 ± 66BIL 3 ± 2 75 ± 9ET 0 ± 0 425 ± 65BG 9 ± 2 4 ± 2
AST: aspartate aminotransferase in U/L, ALT: alanine amino-transferase in U/L, AP: alkaline phosphatage in U/L, BIL: totalbilirubin mmol/L, ET: endotoxin in pg/ml, BG: blood glucose inmmol/L.
C.J. RYAN ET AL.112
Artif Organs, Vol. 25, No. 2, 2001
mens were determined separately, with untreatedpaired controls, in order to establish the therapeuticeffectiveness of each multisorbent treatment regi-men on survival. The effect on survival rate (percent-age) in perfused and nonperfused FHF rats is showngraphically in Fig. 3, which refers to data obtainedfrom 30 animals (15 perfused and 15 nonperfused) ineach group. Survival was classified as animals alive 3weeks following treatment or control procedures.
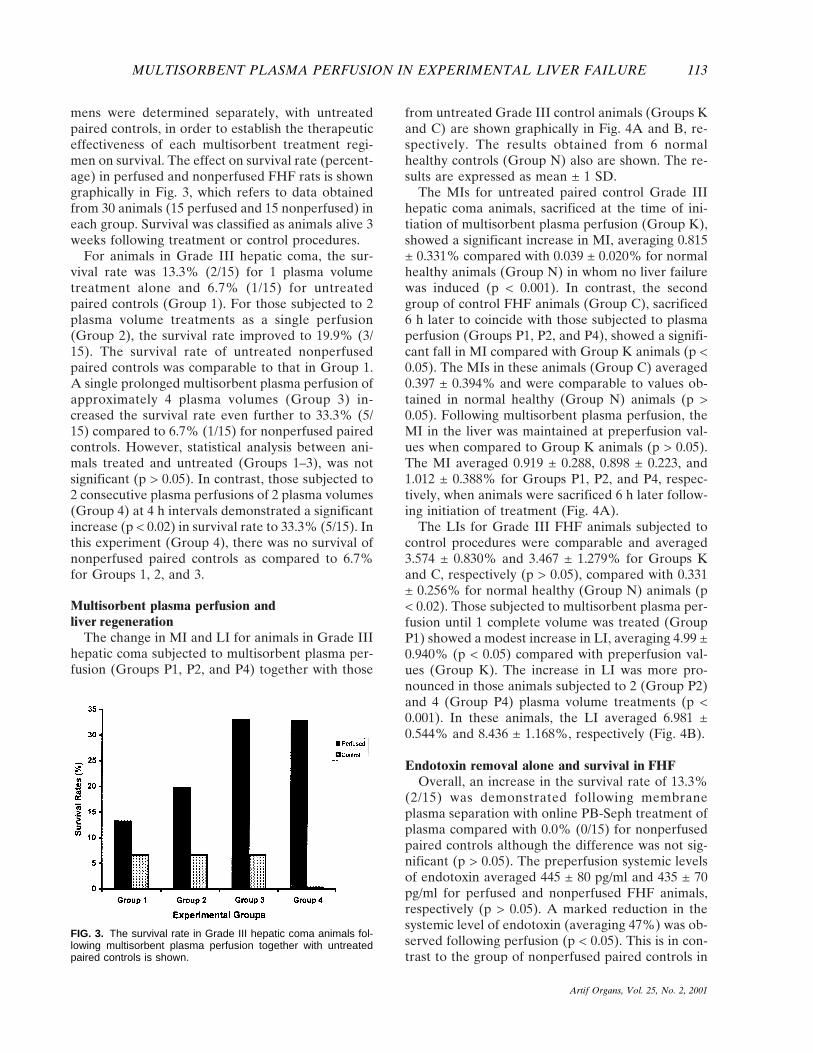
For animals in Grade III hepatic coma, the sur-vival rate was 13.3% (2/15) for 1 plasma volumetreatment alone and 6.7% (1/15) for untreatedpaired controls (Group 1). For those subjected to 2plasma volume treatments as a single perfusion(Group 2), the survival rate improved to 19.9% (3/15). The survival rate of untreated nonperfusedpaired controls was comparable to that in Group 1.A single prolonged multisorbent plasma perfusion ofapproximately 4 plasma volumes (Group 3) in-creased the survival rate even further to 33.3% (5/15) compared to 6.7% (1/15) for nonperfused pairedcontrols. However, statistical analysis between ani-mals treated and untreated (Groups 1–3), was notsignificant (p > 0.05). In contrast, those subjected to2 consecutive plasma perfusions of 2 plasma volumes(Group 4) at 4 h intervals demonstrated a significantincrease (p < 0.02) in survival rate to 33.3% (5/15). Inthis experiment (Group 4), there was no survival ofnonperfused paired controls as compared to 6.7%for Groups 1, 2, and 3.
Multisorbent plasma perfusion andliver regeneration
The change in MI and LI for animals in Grade IIIhepatic coma subjected to multisorbent plasma per-fusion (Groups P1, P2, and P4) together with those
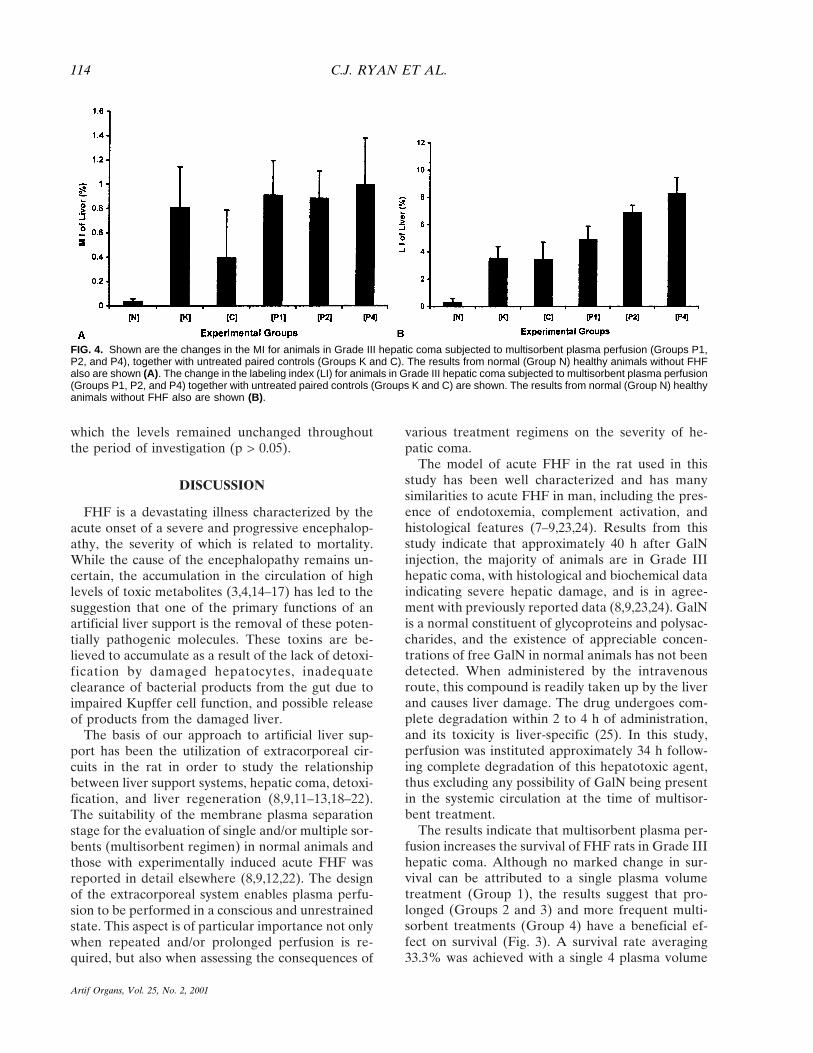
from untreated Grade III control animals (Groups Kand C) are shown graphically in Fig. 4A and B, re-spectively. The results obtained from 6 normalhealthy controls (Group N) also are shown. The re-sults are expressed as mean ± 1 SD.
The MIs for untreated paired control Grade IIIhepatic coma animals, sacrificed at the time of ini-tiation of multisorbent plasma perfusion (Group K),showed a significant increase in MI, averaging 0.815± 0.331% compared with 0.039 ± 0.020% for normalhealthy animals (Group N) in whom no liver failurewas induced (p < 0.001). In contrast, the secondgroup of control FHF animals (Group C), sacrificed6 h later to coincide with those subjected to plasmaperfusion (Groups P1, P2, and P4), showed a signifi-cant fall in MI compared with Group K animals (p <0.05). The MIs in these animals (Group C) averaged0.397 ± 0.394% and were comparable to values ob-tained in normal healthy (Group N) animals (p >0.05). Following multisorbent plasma perfusion, theMI in the liver was maintained at preperfusion val-ues when compared to Group K animals (p > 0.05).The MI averaged 0.919 ± 0.288, 0.898 ± 0.223, and1.012 ± 0.388% for Groups P1, P2, and P4, respec-tively, when animals were sacrificed 6 h later follow-ing initiation of treatment (Fig. 4A).
The LIs for Grade III FHF animals subjected tocontrol procedures were comparable and averaged3.574 ± 0.830% and 3.467 ± 1.279% for Groups Kand C, respectively (p > 0.05), compared with 0.331± 0.256% for normal healthy (Group N) animals (p< 0.02). Those subjected to multisorbent plasma per-fusion until 1 complete volume was treated (GroupP1) showed a modest increase in LI, averaging 4.99 ±0.940% (p < 0.05) compared with preperfusion val-ues (Group K). The increase in LI was more pro-nounced in those animals subjected to 2 (Group P2)and 4 (Group P4) plasma volume treatments (p <0.001). In these animals, the LI averaged 6.981 ±0.544% and 8.436 ± 1.168%, respectively (Fig. 4B).
Endotoxin removal alone and survival in FHFOverall, an increase in the survival rate of 13.3%
(2/15) was demonstrated following membraneplasma separation with online PB-Seph treatment ofplasma compared with 0.0% (0/15) for nonperfusedpaired controls although the difference was not sig-nificant (p > 0.05). The preperfusion systemic levelsof endotoxin averaged 445 ± 80 pg/ml and 435 ± 70pg/ml for perfused and nonperfused FHF animals,respectively (p > 0.05). A marked reduction in thesystemic level of endotoxin (averaging 47%) was ob-served following perfusion (p < 0.05). This is in con-trast to the group of nonperfused paired controls in
FIG. 3. The survival rate in Grade III hepatic coma animals fol-lowing multisorbent plasma perfusion together with untreatedpaired controls is shown.
MULTISORBENT PLASMA PERFUSION IN EXPERIMENTAL LIVER FAILURE 113
Artif Organs, Vol. 25, No. 2, 2001
which the levels remained unchanged throughoutthe period of investigation (p > 0.05).
DISCUSSION
FHF is a devastating illness characterized by theacute onset of a severe and progressive encephalop-athy, the severity of which is related to mortality.While the cause of the encephalopathy remains un-certain, the accumulation in the circulation of highlevels of toxic metabolites (3,4,14–17) has led to thesuggestion that one of the primary functions of anartificial liver support is the removal of these poten-tially pathogenic molecules. These toxins are be-lieved to accumulate as a result of the lack of detoxi-fication by damaged hepatocytes, inadequateclearance of bacterial products from the gut due toimpaired Kupffer cell function, and possible releaseof products from the damaged liver.
The basis of our approach to artificial liver sup-port has been the utilization of extracorporeal cir-cuits in the rat in order to study the relationshipbetween liver support systems, hepatic coma, detoxi-fication, and liver regeneration (8,9,11–13,18–22).The suitability of the membrane plasma separationstage for the evaluation of single and/or multiple sor-bents (multisorbent regimen) in normal animals andthose with experimentally induced acute FHF wasreported in detail elsewhere (8,9,12,22). The designof the extracorporeal system enables plasma perfu-sion to be performed in a conscious and unrestrainedstate. This aspect is of particular importance not onlywhen repeated and/or prolonged perfusion is re-quired, but also when assessing the consequences of
various treatment regimens on the severity of he-patic coma.
The model of acute FHF in the rat used in thisstudy has been well characterized and has manysimilarities to acute FHF in man, including the pres-ence of endotoxemia, complement activation, andhistological features (7–9,23,24). Results from thisstudy indicate that approximately 40 h after GalNinjection, the majority of animals are in Grade IIIhepatic coma, with histological and biochemical dataindicating severe hepatic damage, and is in agree-ment with previously reported data (8,9,23,24). GalNis a normal constituent of glycoproteins and polysac-charides, and the existence of appreciable concen-trations of free GalN in normal animals has not beendetected. When administered by the intravenousroute, this compound is readily taken up by the liverand causes liver damage. The drug undergoes com-plete degradation within 2 to 4 h of administration,and its toxicity is liver-specific (25). In this study,perfusion was instituted approximately 34 h follow-ing complete degradation of this hepatotoxic agent,thus excluding any possibility of GalN being presentin the systemic circulation at the time of multisor-bent treatment.
The results indicate that multisorbent plasma per-fusion increases the survival of FHF rats in Grade IIIhepatic coma. Although no marked change in sur-vival can be attributed to a single plasma volumetreatment (Group 1), the results suggest that pro-longed (Groups 2 and 3) and more frequent multi-sorbent treatments (Group 4) have a beneficial ef-fect on survival (Fig. 3). A survival rate averaging33.3% was achieved with a single 4 plasma volume
FIG. 4. Shown are the changes in the MI for animals in Grade III hepatic coma subjected to multisorbent plasma perfusion (Groups P1,P2, and P4), together with untreated paired controls (Groups K and C). The results from normal (Group N) healthy animals without FHFalso are shown (A). The change in the labeling index (LI) for animals in Grade III hepatic coma subjected to multisorbent plasma perfusion(Groups P1, P2, and P4) together with untreated paired controls (Groups K and C) are shown. The results from normal (Group N) healthyanimals without FHF also are shown (B).
C.J. RYAN ET AL.114
Artif Organs, Vol. 25, No. 2, 2001

treatment (Group 3) although this was not signifi-cantly different when compared to their respectivepaired control animals with a survival rate of 6.7%.However, animals subjected to 2 consecutive perfu-sions each consisting of 2 plasma volume treatments(Group 4) demonstrated a significant increase in sur-vival rate compared to 0% for their respective FHFuntreated paired control animals. The survival rateof 19.9% obtained following 2 plasma volume treat-ments (Group 2) utilizing the multisorbent regime inthe treatment of Grade III hepatic coma is in agree-ment with previous reported data from this labora-tory (8) and supports the current investigations. Theinvestigations of O’Grady and colleagues reportedthat the effectiveness of charcoal hemoperfusionover a single sorbent could not be confirmed in theircontrolled clinical trial (26). Similarly, previous workby the authors has demonstrated that plasma perfu-sion over a single charcoal sorbent was ineffective inthe treatment of late (Grade III) hepatic coma in therat (8). These studies further support the utilizationof a multisorbent system and the need for basic in-formation on the efficacy of such systems.
The potential for survival is ultimately dependentupon regeneration of an adequate functioning livermass although the development of severe complica-tions such as encephalopathy, cerebral edema, andinfection also have a major influence on outcome(1). The poor survival rate in patients with FHF hasbeen attributed to a lack of liver regeneration (27–30). Results to date suggest that in FHF there ap-pears to be an adequate supply of stimulatory sub-stances for liver regeneration (4,30), possiblysynthesized in response to a reduction in liver massthrough necrosis. However, unidentified circulatinginhibitory compounds are believed to counteracttheir effects by inhibiting and/or delaying the capa-bility of the injured liver to undergo a proliferativeresponse (8,9,27,31–35).
Examination of the regenerative activity in theliver indicates an enhanced regenerative responsefollowing multisorbent plasma perfusion comparedwith untreated paired controls. Membrane plasmaseparation with online multisorbent treatment ofplasma (Groups P1, P2, and P4) appears to maintainthe MI in the injured liver when compared withpreperfusion values obtained from FHF Grade IIIcontrol animals (Group K) sacrificed at the time ofinitiation of treatment (Fig. 4A). This is in contrastto the second group of control FHF animals in whichno perfusion was performed (Group C) in which theMI was shown to have fallen when animals weresacrificed to coincide with those subjected to perfu-sion (Groups P1, P2, and P4). It has been suggested
that continued hepatic injury may exceed the rate ofthe repair process of the injured liver (27) and maywell be a consequence of the fall in MI observed inanimals in Group C. The LI results obtained fromanimals subjected to 2 plasma volume treatments(Group P2) and 4 plasma volume treatments (GroupP4) suggest that perfusion may provide a more fa-vorable environment for the liver to continue to un-dergo a proliferative response (Fig. 4B) either by theremoval of toxic products in general or to the re-moval of inhibitory factors specific to liver regenera-tion.
Despite growing evidence for the presence of cir-culating inhibitory factors in the blood of patientswith FHF, there has been little evidence to substan-tiate the hypothesis that such putative toxic metabo-lites inhibit liver regeneration in FHF or whether thedegree of inhibition is related to the severity of thedisease. In previous studies from this laboratory (9),experiments were designed to address the possibilitythat blood contains inhibitory factors which directlyor indirectly suppress regeneration in the woundedliver and, by extension, could be responsible for thedefective liver regeneration associated with FHF inman. In those studies, the overall purpose was togauge the effect that plasma taken from rats in vari-ous stages of hepatic coma had on liver regenerationin a partially hepatectomized recipient animal(which has a well-defined pattern of DNA syntheticactivity) using reverse plasma exchange (RPE).Plasma exchange denotes an exchange of diseasedplasma with healthy plasma in order to effect a cure.We have used the term RPE to describe the transferof plasma taken from donor animals suffering fromFHF (pooled according to the grade of coma) tohealthy recipient rats previously subjected to a par-tial hepatectomy. The results established unequivo-cally that plasma taken from donor FHF animalscontains substances capable of inhibiting hepatocytereplication as demonstrated by markedly reducedrates of hepatocyte DNA synthesis. There also was adirect relationship between the degree of inhibitionand the severity of the disease (9), which confirmsthe present investigations. Furthermore, those trans-fused with Grade IV coma plasma completely sup-pressed any increase in liver weight at 24 h post-partial hepatectomy, essentially abolishing theregenerative response, as demonstrated by MIs andLIs. More recent studies from this laboratory follow-ing extracorporeal multisorbent pretreatment of do-nor FHF plasma, prior to transfusion into recipientanimals, confirm the removal of inhibitory factors toliver regeneration (Ryan et al., unpublished data)and supports the present findings.
MULTISORBENT PLASMA PERFUSION IN EXPERIMENTAL LIVER FAILURE 115
Artif Organs, Vol. 25, No. 2, 2001

Whether circulating toxins, including products ofhepatic necrosis, act directly on hepatocytes or an-tagonize the effects of substances, which stimulateregeneration, is not clear. The results with multisor-bent plasma perfusion suggest that such detoxifica-tion regimes do have a beneficial effect on regenera-tion in FHF and demonstrate the importance ofprolonged perfusion (Group P4) (Fig. 4B). Animalssubjected to 4 plasma volume treatments (Group 3)and those subjected to 2 consecutive perfusions(Group 4) had comparable survival rates, averaging33.3% for Grade III hepatic coma (Fig. 3). However,when compared to their respective paired controls(6.7% and 0%, respectively), only those in Group 4were statistically different. This, in conjunction withthe regenerative data, suggests that the “dose” oftreatment, including duration and frequency, is im-portant in liver cell proliferation in FHF.
Recent evidence suggests that inflammatory cellsand their products (particularly endotoxin and pro-inflammatory cytokines) play a significant role notonly in the amplification of the liver injury, but alsoby inhibiting liver regeneration. Endotoxemia is rec-ognized as an important factor in FHF, and maydamage hepatocytes and induce the release of a widerange of toxic substances from activated liver mac-rophages (14,15). The survival rate in this study uti-lizing 2 columns of PB-Seph in the treatment of 2plasma volumes was comparable to that obtainedwith the multisorbent regimen in the treatment of 1plasma volume (Group 1) (Fig. 3). In both instances,although not significant, a survival rate of 13.3% wasobserved following treatment compared to 6.7%(Fig. 3) and 0.0% for nonperfused paired controls,respectively. It is possible that PB-Seph has the po-tential to absorb toxic metabolites other than endo-toxin. Therefore, the comparable survival rates be-tween these 2 separate treatment regimes may be theresult of a direct relationship between the amount ofsorbent material present and the duration of treat-ment. The preperfusion systemic levels of endotoxinfor perfused and nonperfused FHF animals are com-parable to the main biochemical changes for GradeIII hepatic coma animals shown in Table 1.
Despite the marked reduction in the systemic lev-els of endotoxin (averaging 47%) with PB-Sephalone, it was not possible to ascertain whether thesurvival rate of 13.3% was solely a result of the re-moval of endotoxins or to toxic metabolites in gen-eral, including inhibitory factors specific to liver re-generation. However, a marked reduction in thesystemic levels of endotoxin in FHF following PB-Seph perfusion was demonstrated, which is particu-larly relevant owing to the high incidence of endo-
toxemia in liver disease (14,15,36). This was true forboth 1 and 2 plasma volume treatments.
With the recent development of a number of newstrategies, based on modern membrane technologyand small particle adsorbents, support for a nonbio-logical approach continues (37–44). Although bio-logical “hybrid” systems do have the potential ofmetabolic and/or synthetic function, they still appearto lack major excretory capabilities. However, someof these functions can be achieved readily with ad-sorbents, high performance hemodialysis, and blood/plasma exchange. Demetriou’s group has already in-cluded a charcoal column in their bioartificial systemin order to reduce the load of circulating toxic me-tabolites on the isolated hepatocytes held within thereactor (45), and future strategies will undoubtedlyinclude a combination of both “nonbiological” and“biological” approaches.
CONCLUSIONS
Despite current emphasis toward bioartificial liversupport systems (5,6,45–51), plasma purification byadsorbents offers the simplicity of the use of multiplesorbent regimens aimed at the removal of circulatingtoxic metabolites in general together with those de-signed for specific toxin removal (e.g., endotoxinsand associated cytokines). In this study, membraneplasma separation with online multisorbent treat-ment of plasma was demonstrated to have beneficialeffects in the treatment of Grade III hepatic coma,and the importance of duration and frequency oftreatment was demonstrated. With further under-standing of the regenerative process, the develop-ment of materials for specific removal of circulatingfactors which inhibit liver regeneration also is fea-sible and may, thereby, correct the balance betweenstimulatory and inhibitory factors.
Acknowledgment: This work was supported by a grantto C.J.R. from the Stanley Thomas Johnson Foundation.
REFERENCES
1. Williams R. Classification and clinical syndromes of acuteliver failure. In: Lee WM, Williams R, eds. Acute Liver Fail-ure. Cambridge, U.K.: Cambridge University Press, 1997:1–9.
2. Williams R, Murray-Lyon IM. Artificial Liver Support. Tun-bridge Wells, U.K.: Pitman Medical, 1974.
3. Williams R., ed. Fulminant hepatic failure. Semin Liver Dis1986;6(2):97–173.
4. Williams R, Hughes RD., eds. Acute Liver Failure: ImprovedUnderstanding and Better Therapy. BSG/SK&F InternationalWorkshop. London: Miter Press Ltd., 1991.
5. Hughes RD, Williams R. Use of bioartificial and artificialliver support devices. Semin Liver Dis 1996;16(4):435–44.
6. Atillasoy EO, Berk PD. Extracorporeal liver support: Histori-
C.J. RYAN ET AL.116
Artif Organs, Vol. 25, No. 2, 2001

cal background and critical analysis. In: Lee WM, Williams R,eds. Acute Liver Failure. Cambridge, U.K.: Cambridge Uni-versity Press, 1997:223–44.
7. Chirito E, Lister C, Chang TMS. Biochemical, haematologicaland morphological changes in a fulminant hepatic failure ratmodel for artificial liver assessment. Artif Organs 1979;3(1):42–6.
8. Ryan CJ, Aslam M, Courtney JM. Experimental proceduresfor the assessment of artificial liver support. In: Williams R,Hughes RD, eds. Acute Liver Failure: Improved Understand-ing and Better Therapy. BSG/SK&F International Workshop,London: Miter Press Ltd., 1991:60–6.
9. Anilkumar T, Ryan CJ, Aslam M, Poulson R, Alison M. Theanti-proliferative effect of plasma from rats with acute fulmi-nant hepatic failure. Scand J Gastroenterol 1997;32:1152–61.
10. Corall I, Williams R. Management of liver failure. Br J An-aesth 1986;58:234–45.
11. Ryan CJ, Courtney JM, Wood CB, Hood RG, Blumgart LH.Activated charcoal haemoperfusion via an extracorporeal cir-cuit in the unrestrained and unanaesthetised rat. Br J ExpPathol 1979;60:400–10.
12. Ryan CJ, Pusey CD, Aslam M., Gaylor JDS, Maini R, Court-ney JM. Repeated membrane plasma separation with on-linesorbent treatment of plasma in the conscious rat. Artif Organs1986;10(2):135–44.
13. Cohen J, Ryan CJ, Pusey CD, Aslam M. Protection fromendotoxaemia: A rat model of plasmapheresis and specificadsorption with polymyxin B sulphate. J Infect Dis1987;155(4):690–5.
14. Nolan JP. Intestinal endotoxin as mediators of hepatic injury:An idea whose time has come again. Hepatology 1989;10:887–91.
15. Triger DR. Endotoxin in liver disease: Time for re-appraisal.J Hepatol 1991;12:136–38.
16. Hoofnagle JH, Carithers RL, Shapiro C, Ascher N. Fulminanthepatic failure: Summary of a workshop. Hepatology 1995;21:240–52.
17. Lee WM, Williams R, eds. Acute Liver Failure. Cambridge,U.K.: Cambridge University Press, 1997.
18. Ryan CJ, Courtney JM, Blumgart LH. Haemoperfusion andDNA synthesis in the rat liver. Part II. Effect of haemoper-fusion on DNA synthesis in the rat liver undergoing compen-satory hyperplasia after partial hepatectomy. Artif Organs1982;6(2):182–9.
19. Ryan CJ, Courtney JM, Gibbons M, Aslam M, Batten J,Fleming JS, Wood CB, Paul J. Pre-DNA synthesis haemoper-fusion. In: Paul. JP, Gaylor JDS, Courtney JM, Gilchrist T,eds. Biomaterials in Artificial Organs. London: MacMillanPress, 1984:175–85.
20. Ryan CJ, Aslam M, Cohen J, Courtney JM. Artificial liversupport systems: design of preclinical evaluation programmes.In: Paul JP, McCruden J, Schuetz PW, eds. The Influence ofNew Technology on Medical Practice. London: MacMillanPress, 1988:59–66.
21. Ryan CJ, Aslam M, Courtney JM. Transference of hepaticcoma to normal rats from galactosamine treated donors byreverse plasma exchange. Bio Artif Cells Artif Organs1990;18(4):477–82.
22. Pusey CD, Aslam M, Cohen J, Ryan CJ. Experimental mod-els of plasma perfusion. J Clin Apheresis 1991;6:99–102.
23. Grun M, Liehr H, Rasenack U. Significance of endotoxaemiain experimental galactosamine hepatitis in rats. Acta Hepato-gastroenterol 1977;24:64–81.
24. Liehr H, Grun M, Seelig HP, Reutter W, Heine WD. On thepathogenesis of galactosamine hepatitis in rats. VirchowsArch B Cell Pathol 1978;26:331–44.
25. Keppler D, Decker K. Experimental hepatitis induced by D-galactosamine. Exp Mol Pathol 1968;9:279–90.
26. O’Grady JG, Gimson AES, O’Brian CJ, Pucknell A, HughesRD, Williams R. Controlled trials of charcoal haemoperfu-
sion and prognostic factors in fulminant hepatic failure. Gas-troenterology 1988;94:1186–92.
27. Grove CD, Hughes RD. Liver regeneration in relationship toacute liver failure. Gut 1991;32(Suppl):S92–6.
28. Chenard-Neu MP, Boudjema K, Bernuau J, Degott C, Bel-ghiti J, Cherqui D. Auxiliary liver transplantation: Regenera-tion of the native liver and outcome in 30 patients with ful-minant hepatic failure: A multicenter European study. Hep-atology 1996;23:1119–27.
29. Tomiya T, Fujiwara K. Liver regeneration in fulminant hepa-titis as evaluated by serum transforming growth factor alphalevels. Hepatology 1996;23:253–7.
30. Fausto N. Hepatocyte replication and liver regeneration. In:Lee WM, Williams R, eds. Acute Liver Failure. Cambridge,U.K.: Cambridge University Press, 1997:93–113.
31. Nakamura T, Arakaki R, Ichihara A. Interleukin-1B is a po-tent growth inhibitor of adult rat hepatocytes in primary cul-ture. Exp Cell Res 1988;179:488–97.
32. Zieve L, Dozeman R. Effect of hepatic failure toxins on re-generative enzymes in the liver after injury with galactos-amine in the rat. J Lab Clin Med 1989;113:463–8.
33. Hughes RD, Yamada H, Grove CD, Williams R. Inhibition ofhepatic DNA synthesis in fulminant hepatic failure. Dig DisSci 1991;36(6):816–9.
34. Yamada H, Toda G, Yoshiba M, Hashimoto N, Ikeda Y,Mitsui H, Kurokawa K, Sugata F, Hughes RD, Williams R.Humoral inhibitor of rat hepatocyte DNA synthesis from pa-tients with fulminant hepatic failure. Hepatology 1994;19(5):1133–40.
35. Williams R, ed. Fulminant Hepatic Failure. Semin Liver Dis1996:16(4).
36. Rolando N, Philpott-Howard J, Williams R. Management ofinfection in acute liver failure. In: Lee WM, Williams R, eds.Acute Liver Failure. Cambridge, U.K.: Cambridge UniversityPress, 1997:158–71.
37. Ash SR, Blake DE, Carr DJ, Carter C, Howard T, MakowkaL. Clinical effects of a sorbent suspension dialysis system inthe treatment of hepatic coma (the Biologic-DT). Int J ArtifOrgans 1992;15(3):151–61.
38. Stange J, Ramlow W, Mitzner SR, Schmidt R, Klinkman H.Dialysis against a recycled albumin solution enables the re-moval of albumin-bound toxins. Artif Organs 1993;17:809–13.
39. Hughes RD, Pucknell A, Routley D, Langley PG, WendonJA, Williams R. Evaluation of the BioLogic-DT sorbent-suspension dialyser in patients with fulminant hepatic failure.Int J Artif Organs 1994;17(12):657–62.
40. Weber C, Rajnoch C, Loth F, Schima H, Falkenhagen D. Themicrospheres based detoxification system (MDS). A new ex-tracorporeal blood purification procedure based on recircu-lated microspherical adsorbent particles. Int J Artif Organs1994;17:595–602.
41. von Appen K, Weber C, Losert U, Schima H, Gurland HJ,Falkenhagen D. Microspheres based detoxification system: Anew method in convective blood purification. Artif Organs1996;20(5):420–5.
42. Ash SR, Blake DE, Carr DJ, Harker KD. Push-pull sorbentbased pheresis for treatment of acute hepatic failure: TheBioLogic-detoxifier/plasma filter system. ASAIO J 1998;44(3):129–39.
43. Steczko J, Ash SR, Blake DE, Carr DJ, Bosley RH. Cytokinesand endotoxin removal by sorbents and its application inpush-pull sorbent-based pheresis: The BioLogic-DTPF sys-tem. Artif Organs 1999;23(4):310–8.
44. Strange J, Mitzner SR, Risler T, Erley CM, Lauchart W,Goehl H, Klammt S, Peszynski P, Freytag J, Hickstein H,Lohr M, Liebe S, Schareck W, Hopt UT, Schmidt R. Molecu-lar adsorbent recycling system (MARS): Clinical results of anew membrane-based blood purification system for bioartifi-cial liver. Artif Organs 1999;23(4):319–30.
45. Rozga J, Holzman MD, Ro M-S, Griffin DW, Neuzil DF,
MULTISORBENT PLASMA PERFUSION IN EXPERIMENTAL LIVER FAILURE 117
Artif Organs, Vol. 25, No. 2, 2001

Giorgio T, Moscioni AD, Demetriou AA. Development of ahybrid bioartificial liver. Ann Surg 1993;217:502–11.
46. Ellis AJ, Sussman NL, Kelly JH, Williams R. Clinical experi-ence with an extracorporeal liver assist device. In: Lee WM,Williams R, eds. Acute Liver Failure. Cambridge, U.K.: Cam-bridge University Press, 1997:255–65.
47. Gerlach JC. Hepatocyte culture and bioreactor design forliver support systems. In: Lee WM, Williams R, eds. AcuteLiver Failure. Cambridge, U.K.: Cambridge University Press,1997:245–54.
48. Naka S, Takeshita K, Yamamoto T, Tani T, Kodama M. Bio-artificial liver support system using porcine hepatocytes en-trapped in a three-dimensional hollow fiber module with col-
lagen gel: An evaluation in the swine acute liver failuremodel. Artif Organs 1999;23(9):822–8.
49. Pitkin Z, Mullon C. Evidence of absence of porcine endog-enous retrovirus (PERV) infection in patients treated with abioartificial liver support system. Artif Organs 1999;23(9):829–33.
50. Jauregui HO. Cellular component of bioartificial liver supportsystems. Artif Organs 1999;23(10):889–93.
51. Cuervas-Mons V, Colas A, Rivera JA, Pardos E. In vivo ef-ficacy of a bioartificial liver in improving recovery from ful-minant hepatic failure: A controlled study in pigs. Transplan-tation 2000;69(3):337–44.
C.J. RYAN ET AL.118
Artif Organs, Vol. 25, No. 2, 2001




















