Truly Connected in FVSD's Virtual Program ® - Ocean View ...

Research Paper
Multiple Sclerosis
0(00) 1–11
! The Author(s) 2009
Reprints and permissions:
sagepub.co.uk/journalsPermissions.nav
DOI: 10.1177/1352458509356010
msj.sagepub.com
Multiparametric MR investigation of themotor pyramidal system in patients with‘truly benign’ multiple sclerosis
Barbara Spano1,2, Mara Cercignani1, Barbara Basile1,Silvia Romano3, Rosalba Mannu3, Diego Centonze4,Carlo Caltagirone3,4, Placido Bramanti5,Ugo Nocentini3,4 and Marco Bozzali1
Abstract
One possible explanation for the mismatch between tissue damage and preservation of neurological functions in patients
with benign multiple sclerosis (BMS) is that the pathophysiology differs from that occurring in other multiple sclerosis
(MS) phenotypes. The objective of this study was to identify pathologically specific patterns of tissue integrity/damage
characteristics of patients with BMS, and markers of potential prognostic value. The pyramidal system was investigated in
10 BMS patients and 20 controls using voxel-based morphometry to assess grey matter (GM) atrophy, and diffusion
tractography and quantitative magnetization transfer to quantify the microstructural damage in the corticospinal tracts
(CSTs). Widespread reductions in GM volume were found in patients compared with controls, including the primary
motor cortex. A significant decrease was observed in the mean macromolecular pool ratio (F) of both CSTs, with no
fractional anisotropy (FA) change. GM volume of the primary motor areas was associated with clinical scores but not
with the CST parameters. The mismatch between F and FA suggests the presence of extensive demyelination in the CSTs
of patients with BMS, in the absence of axonal damage. The lack of correlation with GM volume indicates a complex
interaction between disruptive and reparative mechanisms in BMS.
Keywords
cortico-spinal tract, benign MS, diffusion tractography, magnetization transfer
Date received: 2nd September 2009; accepted: 28th October 2009
Introduction
The clinical presentation of multiple sclerosis (MS) in therelapsing–remitting (RR) form is characterized by deficitsreferable to focal demyelination of the central nervoussystem (CNS). In most cases, MS patients present withclinical and instrumental features that allow a definitediagnosis to be formulated in accordance with the mostrecently proposed diagnostic criteria.1,2 Conversely, thereare no clinical factors or instrumental parameters thatmay reliably contribute to define the prognosis of thedisease, whose clinical evolution remains substantiallyunpredictable.3 It is a matter of fact, however, that asignificant proportion of RRMS patients have only amoderate disease progression and no remarkable disabil-ity at longitudinal follow-ups, even many years after clin-ical onset.4,5 For this reason, the clinical definition ofbenign MS (BMS) was introduced4 to identify thoseRRMS patients who present with a favourable diseasecourse after a long-term follow-up.
Although some associations have been reportedbetween gender, sex, early clinical onset, certain clinicalpresentations, low frequencies of relapses during thefirst years, and the BMS course,5,6 the use of theseprognostic factors for clinical purposes at the singlecase level is hardly applicable. On the other hand,
1Neuroimaging Laboratory, Santa Lucia Foundation, IRCCS, Via Ardeatina
306, 00179 Rome, Italy.2Laboratorio Neurobioimmagini, IRCCS Centro Neurolesi ‘Bonino-Pulejo’,
S.S. 113, Via Provinciale Palermo, C Casazza, 98124 Messina, Italy.3Department of Clinical and Behavioural Neurology, Santa Lucia
Foundation, IRCCS, Via Ardeatina 306, 00179 Rome, Italy.4Department of Neuroscience, University of Rome ‘Tor Vergata’, Via
Montpellier 1, 00133 Rome, Italy.5Direzione Scientifica, IRCCS Centro Neurolesi ‘Bonino-Pulejo’, S.S. 113,
Via Palermo, Cntr. Casazza, 98124 Messina, Italy.
Corresponding author:
Dr Marco Bozzali, Neuroimaging Laboratory, Fondazione Santa Lucia, Via
Ardeatina 306, 00179 Rome, Italy. Email: [email protected]
Mult Scler OnlineFirst, published on December 9, 2009 as doi:10.1177/1352458509356010

some MRI studies, based on both conventional andquantitative techniques, failed to identify associationsbetween the severity of structural brain tissue damageand the preservation of neurological functions inpatients with BMS.7,8 There are several reasons thatmight account for this lack of association between mea-sures of brain tissue damage and clinical characteristicsof patients with BMS. First, the clinical definition ofBMS is to some extent arbitrary.3 It is traditionallybased on the Expanded Disability Status Scale(EDSS)9 score (�3.0) that RRMS patients reach aftera long disease duration (�10 years). Some authors havesuggested that MS should only be defined as benignafter at least 15 years from clinical onset.10 However,a recent 21-year follow-up study suggests that such adefinition is no more predictive of a long-term benignoutcome than using the traditional 10-year cut-off.11
Moreover, EDSS is a clinical measure which stronglydepends on motor disability, while it is much lessweighted towards other neurological deficits. Indeed,two recent large-scale studies12,13 have consistentlyreported that a relevant proportion (ranging from19% to 45%) of patients with BMS are in fact cogni-tively impaired. This explains, at least partially, theinconsistencies found in previous studies betweensevere brain tissue damage and a relative clinical pres-ervation (as assessed by the EDSS instrument) inpatients with BMS.6,7 Within such a background, itstill remains to be clarified whether the condition ofBMS is mainly due to a peculiar distribution of braintissue damage (which would preserve the motor func-tions), or it is characterized by different pathophysiolo-gical mechanisms resulting in a moderate clinical impact.
To contribute to addressing such an issue, weselected a group of patients fulfilling the classic criteriafor BMS (EDSS� 3.0; disease duration �10 years),3,5
after excluding, in each of them, the presence of con-comitant cognitive impairment (based on neuropsycho-logical evaluation).14 Under these strict conditions, theEDSS scores are presumably well associated with theclinical status of the patients. Then, we focused ourinvestigation on the pyramidal motor system, includingthe assessment of both, white (WM) and grey matter(GM). To investigate the GM we employed voxel-basedmorphometry, which is a spatially specific and unbiasedmethod of analysis of MR images reflecting the regio-nal GM volume at the voxel scale.15 For the investiga-tion of the pyramidal tract, we used diffusion tensorimaging (DTI) tractography16,17 for segmentation andquantification of fractional anisotropy (FA), a measureof WM integrity.18 DTI tractography is a MR tech-nique able to reconstruct in vivo WM fibre bundlesbased on the assumption that the principal directionof tissue water diffusion is parallel to the main fibredirection in every voxel. Moreover, in combination
with DTI, we used quantitative magnetization transfer(qMT), a recently developed technique,19 to perform aquantitative assessment of specific microstructuralcharacteristics from the segmented tracts.
MT is based on the exchange of magnetizationoccurring between spins in free water (liquid pool)and spins attached to macromolecules (macromole-cular spins). The latter protons, despite being MRIinvisible because of their short transverse relaxationtime (T2), are sensitive to off-resonance irradiation.This selective saturation is transferred to the liquidpool via cross relaxation and chemical exchange, andhence results in a reduction of MRI signal. Theamount of signal attenuation is proportional to thedensity of the macromolecular pool. It is believedthat molecules associated with myelin (cholesteroland sphyngomyelin) dominate the MT phenomenonin WM, which makes qMT particularly attractive forstudying MS. Indeed, evidence from post-mortem20
and animal studies21,22 suggests that one of the para-meters obtained from qMT, the relative size of themacromolecular pool, or F, is proportional to myelincontent in WM. Other quantitative parameters derivedfrom qMT include the forward exchange rate, RMB
0 ,and the transverse relaxation time of the macromole-cular pool,TB
2 . In humans, qMT has been used recentlyto investigate patients with MS,23–27 although clinicalapplications have been limited so far, mainly becauseof the long scan times required.
The principal aim of this study was to identify ana-tomically well localized and pathologically specific pat-terns of tissue integrity/damage that might account forthe subtle neurological deficits characteristic of patientswith ‘truly BMS’. A secondary aim was to identifymarkers of potential prognostic value to be employedin longitudinal studies on patients with RRMS.
Materials and methods
Subjects
We recruited 10 patients (male/female=2/8; mean (SD)age=44.5 (6.5) years) attending the MS outpatient clinicof Santa Lucia Foundation. Criteria for the diagnosis ofBMS were having a diagnosis of clinically definite MS28
with an EDSS score �3.0 after a disease duration of atleast 10 years,3,5,11 and no evidence of cognitive impair-ment.28 A full neurological examination and neuropsy-chological assessment were performed 24 hours beforeMRI acquisition. Patients’ disability and functionalimpairment were assessed using the EDSS. An extensiveneuropsychological battery included tests for:
1. information processing speed using the Symbol DigitModalities Test (SDMT);29
2 Multiple Sclerosis 0(00)

2. verbal memory using the California Verbal LearningTest—Second Edition (CVLT2);30
3. visuospatial memory using the Rey–OsterriethComplex Figure Test, immediate and delayedreproduction;31
4. visuospatial functions using the Benton Judgment ofLine Orientation Test;32
5. visuoconstructive functions using the Rey–OsterriethComplex Figure Test, copy;31
6. executive functions using the Modified Card SortingTest (MCST)33 and Stroop Color and Word Test;34
7. language using the Control Oral Words AssociationTest (COWAT) and Phrase Construction test.35
To be eligible patients had to score within the rangeof normality (<95% of the lower tolerance limit ofthe distribution from the Italian normative data) inall cognitive domains explored. Moreover, as additionalinclusion criterion, patients had to be steroid- andrelapse-free for at least 3 months before study entry.Twenty healthy controls (HC; male/female=8/12;mean (SD) age=40.5 (11.07) years) with no historyof neurological disorders and normal neurologicalexamination were also recruited.
The study was approved by the Local EthicsCommittee, and written informed consent was obtainedfrom all of the subjects before study entry.
MRI acquisitions
All MR imaging was obtained using a head-only 3.0-Tscanner (Siemens Magnetom Allegra, Siemens MedicalSolutions, Erlangen, Germany), equipped with a circu-larly polarized transmit–receive coil. The maximumgradient strength is 40mTm�1, with a maximum slewrate of 400mTm�1ms�1. The following sequences wereobtained for each subject during a single scanningsession:
1. dual-echo turbo spin echo (TSE) (TR=6190ms,TE1=12ms, TE2=109ms, echo train length(ETL)=5; matrix=256� 192; field of view(FOV)=230� 172.5mm2; 48 contiguous 3mmthick slices);
2. fluid attenuated inversion recovery (FLAIR)(TR=8170ms, TE=96ms, TI=2100ms; ETL=13; same FOV, matrix and number of slices as TSE);
3. morphological 3D T1-weighted magnetization pre-pared rapid acquisition gradient echo (MPRAGE)(TE=2.74ms, TR=2500ms, inversion time=900ms; flip angle=8�; matrix=256� 208� 176;FOV=256� 208� 176mm3);
4. diffusion weighted twice-refocused37 SE EPI(TR=170ms, TE=85ms, maximum b factor=1000 smm�2, isotropic resolution 2.3mm3;
matrix=96� 96; 60 slices), collecting seven imageswith no diffusion weighting (b0) and 61 images withdiffusion gradients applied in 61 non-collinear direc-tions [38];
5. a series of 12 MT-weighted 3D fast low-angle shot(FLASH) sequences (TR=35ms, TE=7.4,flip angle=7�; matrix=128� 96� 28; FOV=230� 172.5� 140mm3), with various combinationsof on-resonance equivalent flip angle and offset fre-quency (�f) of the Gaussian MT pulse (pulse dura-tion=15ms), optimised as described elsewhere;39 fora full list of sampling points, see Cercignani et al.;27
6. three 3D FLASH sequences with three different flipangles for mapping the observed T1 of the system(TR=15ms, TE=4.8ms, flip angle=5�, 7�, 15�,respectively; same matrix and FOV as theMT-weighted FLASH);
7. three 3D FLASH sequences with near-180� flipangles for B1 mapping40 (TR=28ms, TE=4.8ms,flip angles=155�, 180�, 205�, respectively;matrix=64� 64� 40, FOV=220� 220� 160mm3);this sequence was collected along the sagittal plane,while all the other sequences were collected in thenear-axial plane, with slices positioned to run parallelto a line that joins the most inferoanterior and infer-oposterior parts of the corpus callosum (AC–PC line).
The total scan time was approximately 50 minutes.
MR images post-processing and analysis
Lesion segmentation: T2-hyperintense lesions wereidentified by consensus by two observers on the shortecho images of the TSE, for every patient. Lesions wereoutlined on the same scan using a semi-automated localthresholding contouring software (Jim 4.0, XinapseSystem, Leicester, UK, http://www.xinapse.com/)FLAIR and long echo TSE scans were always used asa reference to increase confidence in lesion identifica-tion. The total lesion volume was calculated for everypatient.
Grey matter analysis: T1-weighted data were pro-cessed according to the VBM protocol, usingStatistical Parametric Mapping (SPM5, www.fil.ion.ucl.ac.uk/spm/), an iterative combination of segmenta-tions and normalisations to produce a GM probabilitymap41 in Montreal Neurological Institute (MNI) coor-dinates for each subject. GM maps were ‘modulated’ bymultiplying the intensity of each voxel in the finalimages by the local value derived from the deformationfield, or Jacobian determinant.42 All data were thensmoothed using a 12-mm full width at half maximum(FWHM) Gaussian kernel. To assess the presence ofbetween-group local differences in GM volume
Spano et al. 3

(BMS<HC and BMS>HC) we performed a categor-ical comparison between patients and controls, adjust-ing for total intra-cranial volume (estimated as the sumof GM, WM and CSF volume), age and gender.
Correction for multiple comparisons was applied atthe cluster level. After correction, a p-value of less than0.05 was accepted as significant (corresponding to acluster extent of approximately 400 voxels).
Post hoc, the average GM volume from relevantareas found to be atrophic (see results section) wasextracted for correlating with other variables.
Quantitative MT analysis: Quantitative MT data from2 out of 10 patients had to be discarded, because ofmotion artefacts.
For all of the remaining subjects, FLASH imagesfrom sequence 7 were reformatted to the axial plane.Next, in order to compensate for involuntary motion,all images obtained from sequences 5 (MT FLASH), 6(T1-mapping FLASH) and 7 (reformatted B1-mappingFLASH) were affine-registered using FLIRT43,44 tomatch the 15� FLASH of sequence 6. B1 maps werecomputed according to Dowell and Tofts,40 and T1maps were calculated by fitting the theoretical spoiledgradient echo signal equation45 as a function of the flipangle (after B1-correction) to the signal measured bysequence 5.46 A detailed description of the processingis given elsewhere.27
For MT modelling, we adopted here Ramani’s signalequation,39 a modification of Henkelman et al.’smodel19 for in vivo applications, where the continuouswave power equivalent (CWPE) approximation is used.As described in detail elsewhere,27,48 quantitative MTparameters were estimated on a voxel-by-voxel basis byfitting the model equation of the MT-weighted signal tothe data from sequence 5 using the Levenberg–Marquardt method, as implemented in NumericalRecipes.49 The CWPE value was adjusted accordingto the B1 maps at each voxel location. The absorptionlineshape of the macromolecular pool was modelledwith a super-Lorentzian.50
RB was set arbitrarily to 1 s�1 and kept fixed duringthe fitting, as in previous quantitative MT experi-ments.19,23,26 The fitting yielded maps of F, RMB
0 , andTB2 .
DTI and corticospinal tract reconstruction: DTI datawere processed using tools from the FMRIB softwarelibrary (FSL, www.fmrib.ox.ac.uk/fsl/) and fromCAMINO (www.camino.org.uk).
After correction for eddy current induced distortionsand involuntary motion (performed using eddy_correct,available with FSL), the diffusion tensor was estimatedvoxel-wise51 using CAMINO, and a map of FA wasobtained for every subject. In order to minimize thevariability in seed-point positioning, which is the
main source of variance in tractography studies,52 allDTI data were transformed into standard space, toobtain maps with comparable brain size and slice ori-entation for all subjects. This was achieved by comput-ing the affine transformation44 matching every subject’sFA to the FSL FA template, and then applying such atransformation to each component of the DT using thePPD (Preservation of Principal Direction) algorithm.53
The rotated DT was used to generate maps of FA, andof the eigenvalues and eigenvectors for every subject,from which colour-coded directionality maps in stan-dard space were computed.54
Seed and way points were manually drawn on eachsubject’s colour-coded map, based on published guide-lines.55 Seed-point regions were outlined to encompassthe cerebral peduncles on a single axial slice at the levelof the decussation on the cerebral peduncle. Next, themost ventral axial section where the central sulcus isvisible was selected, and two regions of interest(ROIs), one for either hemisphere, were outlined toinclude the WM just below the primary motor cortex.These regions were used as way-point ROIs.
The probabilistic index of connectivity (PICo) algo-rithm17, implemented in CAMINO, was used for prob-abilistic tractography. The probability of connection tothe seed point in every voxel is estimated bystreamline-based tracking iterations (5000 in this case)repeated in a Monte Carlo fashion, and the effect ofnoise is accounted for through a calibration step.Streamlines that did not reach the way-point ROIwere discarded. Only voxels with a probability of con-nection larger than 0.1 were retained as part of the cor-ticospinal tract (CST), to minimize the effects of noise.These voxels formed a binary mask identifying the CSTsin the same space as FA maps. The mean FA (averagedacross the whole tract) of both CSTs was then extractedand recorded as a summary measure for each subject,and it was used to compute the correlations with clinicalscores and other MRI-derived quantities.
For every subject, the spatial transformation match-ing the DTI scan to the MT-weighted scans (sequence 6)was then computed by affine followed by non-linearregistration (see FLIRT and FNIRT, http://www.fmrib.ox.ac.uk/fsl/fsl/list.html). The non-linear step was addedto compensate for EPI geometric distortions.56 Thetransformations were then applied to the maps definingthe CST which were used to compute the mean F, RMB
0
and TB2 values for each tract.
Statistical analysis
Statistical analyses were performed using SPSS 13.0 forWindows (SPSS Inc, USA). Age and gender were com-pared between groups using a t-test and a �2-test,respectively.
4 Multiple Sclerosis 0(00)

Between-group comparisons of mean CST para-meters (FA, F, RMB
0 and TB2 ) were performed using
two-sample t-tests.The presence of any association between GM
volume of the primary motor cortex, CST parametersand clinical variables was assessed using theSpearman’s non-parametric correlation analysis. Thesignificance level was set to p< 0.05.
Results
The mean (SD) disease duration of the recruitedpatients was 17.1 (4.5) years, and their median EDSSscore was 1.75 (range: 1–3). For 8 out of 10 patients theMS functional composite (MSFC) score was also avail-able [57]. Their mean MSFC was –0.3 (SD=0.66).
Following inclusion criteria, all patients scoredwithin the normal range at all administered neuropsy-chological tests.
The patients’ mean T2 lesion volume was 8.4 (SD=5.8) ml. Nine out of 10 patients (90%) had at least onelesion in the CST. There were no differences betweenpatients and controls with respect to gender (�2=3.33,df=1, p=0.07), or age (p=0.31). All patients wereunder disease-modifying treatments (either b–interferonsor glatiramer acetate) at the time of study entry.
GM atrophy
Patients with BMS showed widespread reductions inGM volume (p< 0.05, corrected at the cluster level).Atrophy was observed, bilaterally, in the precentralgyrus (primary motor areas), in the cingulate gyrus, in
the middle frontal gyrus and frontal pole, in the thala-mus, as well as in the left insula and in the right palli-dum. No areas of increased GM volume compared withcontrols were found. Table 1 and Figure 1 summarizethe results of the VBM analysis.
In order to investigate the relationship between CSTdamage and atrophy of the primary motor cortex, themean GM volume of the two clusters found in the leftand right primary motor cortices was extracted by aver-aging the mean intensity of all voxels included in theclusters in the modulated GM images of each patient.
DTI and qMT metrics of the CST
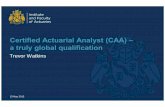
The CST was successfully reconstructed in all subjects inboth hemispheres. Examples from a patient and a HC areshown in Figure 2. The same figure also shows the CSTmasks after transformation into the same space as theMT data, overlaid onto one of the MT volumes.
When comparing patients and controls, a significantdecrease was observed in patients with respect to themean F and RMB
0 of both CSTs. Conversely, no differ-ence was found when comparing either TB
2 or FA.Detailed results of the comparisons are shown in Table 2.
In patients, the EDSS was correlated with the meanGM volume of the left primary motor cortex(R=�0.7, p=0.02, N=10); while the MSFC scorewas associated with the mean GM volume of theright motor cortex (R=0.9, p=0.002, N=8).
There was no significant association between theGM of the primary motor cortex and any of the CSTmean parameters. No correlation was found betweenFA and any of the MT parameters.
Table 1. Distribution of regional grey matter reduction in patients with benign multiple sclerosis
Cluster Structure MNI coordinates T value p-value
Thalamus (L) [�6,�32,�4] 7.55
1 Thalamus (R) [4,�28,6] 7.01 <0.001
Pallidum (R) [22,�2,�6] 5.95
2 Middle frontal gyrus (R) [46,24,40] 6.07 <0.001
Precentral gyrus (R) [58,�4,44] 5.57
Postcentral Gyrus (L) [�44,18,40] 5.85
3 Insular cortex (L) [�42,12,�10] 5.67 <0.001
Precentral Gyrus (L) [�48,�10,52] 5.22
4 Cingulate gyrus (L&C&R) [�4,�22,32] 5.69 <0.001
Superior frontal gyrus (L) [�24,30,44] 4.97
5 Frontal Pole (L) [�24,42,34] 4.81 0.011
Middle frontal gyrus (L) [�36,40,36] 4.49
L, left; R, right; C, central; MNI, Montreal Neurological Institute.
The table lists the clusters of significantly reduced grey matter (GM) volume in patients with benign multiple sclerosis as compared with healthy
controls. For each cluster, the main GM structures included are listed. The coordinates indicate the location of local maxima more than 8 mm apart
(which might occur within the same cluster). p-values are corrected for multiple comparisons at the cluster level.
Spano et al. 5

Discussion
This study, based on a multiparametric quantitativeMRI approach, has attempted for the first time adetailed investigation of the pyramidal system (CST
and GM from the primary motor areas) in patientswith the so-called ‘truly benign’ form of MS, with no,or only minor, clinical signs of motor dysfunction, andin the absence of any remarkable disability in any otherdomain. To this purpose, all of our patients were
Figure 1. Distribution of regional grey matter (GM) loss in patients with benign multiple sclerosis as compared with healthy
controls. The regions of statistically significant difference are rendered at a threshold of p-corrected = 0.05, at the cluster level, and
correspond to those summarized in Table 1. The areas of GM loss are overlaid onto a T1-weighted image in Montreal Neurological
Institute space. See the text for further details.
Table 2. Diffusion tensor imaging and quantitative magnetization transfer metrics from the corticospinal tract of benign multiple
sclerosis (BMS) patients and controls
Side BMS Controls p-valuea
FA L 0.39 (0.04) 0.39 (0.04) 0.941
R 0.39 (0.04) 0.40 (0.03) 0.277
F L 0.19 (0.01) 0.21 (0.02) 0.001
R 0.20 (0.02) 0.22 (0.01) 0.002
RMB0[s�1] L 1.83 (0.15) 2.04 (0.24) 0.034
R 1.83 (0.13) 2.08 (0.08) 0.006
TB2[ms] L 12.4 (0.9) 12.1 (0.8) 0.712
R 12.5 (1.6) 11.8 (0.8) 0.249
L, left; R, right; FA, fractional anisotropy; F, relative size of the macromolecular pool;RMB0 , pseudo-first-order forward exchange rate;TB
2 , transverse
relaxation rate of macromolecular pool.ap-values in bold are accepted as significant.
Mean (SD) values are obtained by averaging each parameter across all of the voxels included in the corticospinal tract reconstructed by tractography.
The p-values are obtained by independent two-sample t-test. The quantities for which units are not specified are dimensionless.
6 Multiple Sclerosis 0(00)

carefully investigated from a neuropsychological pointof view, to exclude the presence of higher-level functionimpairment, which would make the classification ofBMS uncertain.12–14 We first ran a whole-brain VBManalysis of regional GM volumes. The comparisonbetween BMS patients and HCs revealed a pattern ofGM atrophy involving the deep nuclei bilaterally, andseveral cortical regions with a preferential left side dis-tribution, consistently with a recent large-scale VBMstudy in patients with BMS.58 Although Mesaros
et al. did not report results from a direct contrastbetween BMS patients without cognitive impairmentand HCs (such as in our current study), the comparisonbetween this subgroup and an additional control groupwith secondary progressive MS (SPMS) revealed apreservation of the cerebellar GM in the former, withno other regional difference.
These findings indicate that, despite the clinical pres-ervation, patients with BMS, as well as those withSPMS, suffer from a diffuse GM volume loss of the
Figure 2. Examples of corticospinal tracts reconstructed with probabilistic diffusion tractography in a healthy subject (A, B) and in a
multiple sclerosis patient (C, D). Panels A and C show that the maps of the output of the tractography algorithm, by means of the
probability of connection to the left (blue) and right (orange) seed-points for the control and the patient, respectively, overlaid onto
the corresponding fractional anisotropy maps. The colour bar indicates the probability of connection, and the maps are thresholded to
exclude voxels with a probability of connection lower than 0.1. Panels B and D show the same maps, after co-registration with
quantitative magnetization transfer (MT) maps, overlaid onto the first MT volume.
Spano et al. 7

cerebral cortex. This is in contrast with the generalnotion that GM damage mostly contributes to stabledisability in patients with MS,59–61 and leaves the mis-match between brain tissue damage and a favourableclinical course in patients with BMS as an apparentparadox.8 It might be argued that tissue damage inthe spinal cord (which is present in the large majorityof patients with SPMS) together with that in the cere-bellum are important factors in determining locomotordisability in MS.58,62 However, the relative preservationof the cerebellum and the cord does not explain theabsence of cognitive impairment in our cohort ofBMS patients
A possible explanation for the mild disability and thediffuse cortical involvement found by us and byothers58 in BMS is that a reduced rate of brain atrophyover time, possibly reflecting a less predominant degen-erative component in the pathogenesis of BMS,63 mightaccount for a favourable clinical evolution of the dis-ease. Moreover, this is consistent with the hypothesisthat patients with BMS may benefit more than thosewith other MS phenotypes from compensation pro-cesses of brain plasticity.64 Unfortunately, thecross-sectional design of our study does not allow anyinference about rates of atrophy over time. An addi-tional limitation of this study lies in the lack of a com-parison with group of patients with SPMS andequivalent disease duration.
Nonetheless, the current study provides, for the firsttime, specific parameters of microstructural tissuestatus (i.e. demyelination; axonal loss; GM changes)in a neuronal pathway (the pyramidal system) whichis essential to account for the clinical state of patientswith ‘truly BMS’. In the CST, a bilateral reduction of Fvalues was found in patients compared with HCs, in theabsence of a concomitant FA reduction. MT is knownto be sensitive to myelin, and qMT provides a moredirect insight than MT ratio (MTR), by modelling theunderlying properties involved in the MT process. Thisovercomes the traditional limitations of the MTR,namely its dependency on sequence parameters, andthe fact that it represents the combination of severalquantities, and therefore has limited specificity.
Among qMT parameters, F in particular is believedto reflect myelination: a recent post-mortem studyshowed a strong association between f (the macromo-lecular fraction, equal to F/(1+F)) and histologicalmeasures of myelin in the brain of patients withMS.19 Consistently, experiments with animal modelsprovide evidence that F is a quantity strictly associatedwith myelin content in WM, while it does not reflectaxonal density.21,22 These experiments even suggest thatit is myelin alone that accounts for the contrast betweenGM and WM on F maps of wild-type mice brain.In contrast, FA, which reflects the spatial coherence/
directionality of neuronal fibres, has a differentsubstrate.65
The lack of correlation between F and FA wasrecently demonstrated in the WM of HCs byUnderhill et al. 66 The authors of this study concludedthat spatial coherence is the main factor driving regio-nal distinction of FA in normal WM, while MT para-meters are more informative on the underlying tissuecomposition. In MS, reductions in FA are likely toreflect a complex interaction between axonal damage,changes in fibre density and directionality, while reduc-tions in F simply reflect demyelination. Although otherbasic research investigations focused on clarifying cor-relations between FA and neuronal parameters havebeen less conclusive,65 FA in WM tissue is likely tobe dependent on the underlying neuronal density.Against this background, we can speculate that an iso-lated reduction of F in the CSTs of BMS patients withno associated FA reduction suggests that the occur-rence of degenerative pathophysiological processes inthe motor systems of these patients is limited. The inter-pretation of other qMT parameters, namely RMB
0 andTB2 , is more controversial. RMB
0 is moderately corre-lated with F,67 and thus is partially related to myelincontent. Consistently, we found a reduction in themean RMB
0 of both CSTs. On the other hand, TB2 is
uncorrelated with any other MT parameter, and itsusefulness as a marker of pathology is underdebate.21,25,28
In our cohort, the WM damage observed in CST ofpatients with truly BMS was unrelated to either mea-sures of GM density in the motor cortex or clinicalparameters. Conversely, GM density of the primarymotor areas was associated with EDSS and MSFCscores. A possible interpretation of these findings isthat BMS pathophysiology is principally characterizedby a subtle WM damage (mainly resulting in demyeli-nation with minimal axonal loss), which is followed byGM reorganization. GM density, in turn, correlateswith BMS patients’ clinical outcome, which is overallfavourable. Consistent with the idea that changesoccurring in the GM are the result of both WMabnormalities and GM plasticity, we did not find anysignificant correlation between GM density in themotor areas and any measure of WM integrity in theCST. The relationship between damage to the normalappearing WM and GM in MS has been largely inves-tigated in other phenotypes,68–70 without reaching aconclusive agreement. Some authors support thehypothesis that GM atrophy is secondary to WMdamage,71 others proposed that GM may be the pri-mary target of the disease process, resulting in second-ary axonal degeneration and demyelination in WM.72
According to our results, we might argue that ‘inflam-matory’ demyelination of axons is not amajor contributor
8 Multiple Sclerosis 0(00)

of progressive axonal damage and permanent disability inMS. Indeed, it is possible that the pathological processesoccurring in the NAWM and in the GM could to someextent develop independently from each other, as sug-gested by a recent post-mortem study.73 In BMS, therecurrent inflammatory episodes leading to concomitantprocesses of demyelination, remyelination, oedema andgliosis could also explain the lack of correlation betweenWM and GM alteration. Again, future studies includingnot only patients with BMS, but also patients with SPMS,might contribute to clarifying this issue.
Moreover, the majority of patients with BMS areunder disease-modifying treatments, making it difficultto make a clear distinction between BMS as a genuinedisease phenotype or a subgroup of RRMSpatients withan excellent response to therapies. Longitudinal studiesare needed to clarify the questions left unanswered.
In conclusion, this study contributes to clarifyingsome of the complex pathophysiological processesunderlying the favourable disease course in patientswith BMS. Future work will include the extension ofthis analysis to other neurological systems, such as thecorpus callosum, a comparison with patients with com-parable disease duration but less favourable clinicaloutcome, and longitudinal follow-ups.
References
1. Polman CH, Reingold SC, Edan G, et al. Diagnostic cri-
teria for multiple sclerosis: 2005 revisions to the
‘McDonald Criteria’. Ann Neurol 2005; 58: 840–846.2. Swanton JK, Fernando K, Dalton CM, et al. Modification
of MRI criteria for multiple sclerosis in patients with clin-
ically isolated syndromes. J Neurol Neurosurg Psychiatry
2006; 77: 830–833.3. Ramsaransing GS, De Keyser J. Benign course in multiple
sclerosis: a review. Acta Neurol Scand 2006; 113: 359–369.4. Mcalpine D. The benign form of multiple sclerosis. A
study based on 241 cases seen within three years of onset
and followed up until the tenth year or more of the disease.
Brain 1961; 84: 186–203.5. Hawkins SA, McDonnell GV. Benign multiple sclerosis?
Clinical course, long term follow up, and assessment of
prognostic factors. J Neurol Neurosurg Psychiatry 1999;
67: 148–152.6. Ramsaransing G, Maurits N, Zwanikken C, De Keyser J.
Early prediction of a benign course of multiple sclerosis on
clinical grounds: a systematic review. Mult Scler 2001; 7:
345–347.7. De Stefano N, Narayanan S, Francis SJ, et al. Diffuse
axonal and tissue injury in patients with multiple sclerosis
with low cerebral lesion load and no disability. Arch
Neurol 2002; 59: 1565–1571.8. Strasser-Fuchs S, Enzinger C, Ropele S, Wallner M,
Fazekas F. Clinically benign multiple sclerosis despite
large T2 lesion load: can we explain this paradox? Mult
Scler 2008; 14: 205–211.
9. Kurtzke JF. Rating neurologic impairment in multiplesclerosis: an Expanded Disability Status Scale (EDSS).Neurology 1983; 33: 1444–1452.
10. Lublin F, Reingold S. Defining the clinical course of mul-tiple sclerosis: Results of an international survey.Neurology 1996; 46: 907–911.
11. Costelloe L, Thompson A, Walsh C, Tubridy N,
Hutchinson M. Long-term clinical relevance of criteriafor designating multiple sclerosis as benign after 10years of disease. J Neurol Neurosurg Psychiatry 2008;
79: 1245–1248.12. Amato MP, Portaccio E, Stromillo ML, et al. Cognitive
assessment and quantitative magnetic resonance metrics
can help to identify benign multiple sclerosis. Neurology2008; 71: 632–638.
13. Rovaris M, Riccitelli G, Judica E, et al. Cognitive impair-
ment and structural brain damage in benign multiple scle-rosis. Neurology 2008; 71: 1521–1526.
14. Rovaris M, Barkhof F, Calabrese M, et al. MRIfeatures of benign multiple sclerosis: toward a new defi-
nition of this disease phenotype. Neurology 2009; 72:1693–1701.
15. Good CD, Johnsrude IS, Ashburner J, Henson RN,
Friston KJ, Frackowiak RS. A voxel-based morpho-metric study of ageing in 465 normal adult humanbrains. Neuroimage 2001; 14: 21–36.
16. Conturo TE, Lori NF, Cull TS, et al. Tracking neuronalfiber pathways in the living human brain. Proc Natl AcadSci U S A 1999; 96: 10422–10427.
17. Parker GJ, Haroon HA, Wheeler-Kingshott CA. A
framework for a streamline-based probabilistic index ofconnectivity (PICo) using a structural interpretation ofMRI diffusion measurements. J Magn Reson Imaging
2003; 18: 242–254.18. Pierpaoli C, Basser PJ. Toward a quantitative assessment
of diffusion anisotropy. Magn Reson Med 1996; 36:
893–906.19. Henkelman RM, Huang X, Xiang QS, Stanisz GJ,
Swanson SD, Bronskill MJ. Quantitative interpretation
of magnetization transfer. Magn Reson Med 1993; 29:759–766.
20. Schmierer K, Tozer DJ, Scaravilli F, et al. Quantitativemagnetization transfer imaging in postmortem multiple
sclerosis brain. J Magn Reson Imaging 2007; 26: 41–51.21. Ou X, Sun SW, Liang HF, Song SK, Gochberg DF. The
MT pool size ratio and the DTI radial diffusivity may
reflect the myelination in shiverer and control mice.NMR Biomed 2009; 22: 480–487.
22. Ou X, Sun SW, Liang HF, Song SK, Gochberg DF.
Quantitative magnetization transfer measured pool-sizeratio reflects optic nerve myelin content in ex vivo mice.Magn Reson Med 2009; 61: 364–371.
23. Tozer D, Ramani A, Barker GJ, Davies GR, Miller DH,
Tofts PS. Quantitative magnetization transfer mapping ofbound protons in multiple sclerosis. Magn Reson Med2003; 50: 83–91.
24. Davies GR, Tozer DJ, Cercignani M, et al. Estimationof the macromolecular proton fraction and boundpool T2 in multiple sclerosis. Mult Scler 2004; 10:
607–613.
Spano et al. 9

25. Levesque I, Sled JG, Narayanan S, et al. The role ofedema and demyelination in chronic T1 black holes: aquantitative magnetization transfer study. J Magn
Reson Imaging 2005; 21: 103–110.26. Narayanan S, Francis SJ, Sled JG, et al. Axonal injury in
the cerebral normal-appearing white matter of patientswith multiple sclerosis is related to concurrent demyelina-
tion in lesions but not to concurrent demyelination innormal-appearing white matter. Neuroimage 2006; 29:637–642.
27. Cercignani M, Basile B, Spano B, et al. Investigation ofquantitative magnetisation transfer parameters of lesionsand normal appearing white matter in multiple sclerosis.
NMR Biomed 2009; 22: 646–653.28. McDonald WI, Compston A, Edan G, et al.
Recommended diagnostic criteria for multiple sclerosis:
guidelines from the International Panel on the diagnosisof multiple sclerosis. Ann Neurol 2001; 50: 121–127.
29. Smith A. Symbol Digit Modalities test, manual. WebsterPsychological Services, 2000.
30. Delis DC, Kramer JH, Kaplan E, Ober BA. Californiaverbal learning test manual, 2nd ed. San Antonio, TX:Psychological Corporation, 2000 [Adult Version].
31. Carlesimo GA, Buccione I, Fadda L, et al.Standardizzazione di due test di memoria per uso clinico:Breve Racconto e Figura di Rey. Nuova Rivista di
Neurologia 2002; 12: 1–13.32. Benton AL, Varney NR, Hamsher KD. Visuospatial
judgment. A clinical test. Arch Neurol 1978; 35: 364–367.33. Nelson HE. A modified card sorting test sensitive to fron-
tal lobe defects. Cortex 1976; 12: 313–324.34. Gronwall DMA. Paced auditory serial-addition task: a
measure of recovery from concussion. Percept Motor
Skills 1977; 44: 367–373.35. Golden CJ. The stroop color and word test. Wood Dale,
IL: Stoelting Company, 1978.
36. Borkowsky JG, Benton AL, Spreen O. Word fluency andbrain damage. Neuropsychologia 1967; 5: 135–140.
37. Reese TG, Heid O, Weisskoff RM, Wedeen VJ.
Reduction of eddy-current-induced distortion in diffusionMRI using a twice-refocused spin echo.Magn Reson Med2003; 49: 177–182.
38. Jones DK, Horsfield MA, Simmons A. Optimal strategies
for measuring diffusion in anisotropic systems by mag-netic resonance imaging. Magn Reson Med 1999; 42:515–525.
39. Cercignani M, Alexander DC. Optimal acquisitionschemes for in vivo quantitative magnetization transferMRI. Magn Reson Med 2006; 56: 803–810.
40. Dowell NG, Tofts PS. Fast, accurate, and precise map-ping of the RF field in vivo using the 180 degrees signalnull. Magn Reson Med 2007; 58: 622–630.
41. Ashburner J, Friston KJ. Unified segmentation.
Neuroimage 2005; 26: 839–851.42. Ashburner J, Friston KJ. Why voxel-based morphometry
should be used. Neuroimage 2001; 14: 1238–1243.
43. Jenkinson M, Bannister P, Brady M, Smith S. Improvedoptimization for the robust and accurate linear registra-tion and motion correction of brain images. Neuroimage
2002; 17: 825–841.
44. Jenkinson M, Smith S. A global optimisation method for
robust affine registration of brain images. Med Image
Anal 2001; 5: 143–156.45. Ernst T, Anderson W. Application of Fourier transform
spectroscopy to magnetic resonance. Rev Sci Instrum
1966; 37: 93–102.46. Venkatesan R, Lin W, Haacke EM. Accurate determina-
tion of spin-density and T1 in the presence of RF-field
inhomogeneities and flip-angle miscalibration. Magn
Reson Med 1998; 40: 592–602.47. Ramani A, Dalton C, Miller DH, Tofts PS, Barker GJ.
Precise estimate of fundamental in-vivo MT parameters
in human brain in clinically feasible times. Magn Reson
Imaging 2002; 20: 721–731.48. Cercignani M, Symms MR, Schmierer K, et al.
Three-dimensional quantitative magnetisation transfer
imaging of the human brain. Neuroimage 2005; 27:
436–441.49. Press WH, Teukolsky SA, Vettering WT, Flannery BP.
Numerical recipes in C. Cambridge: Cambridge University
Press, 1992.50. Morrison C, Stanisz G, Henkelman RM. Modeling mag-
netization transfer for biological-like systems using a
semi-solid pool with a super-Lorentzian lineshape and
dipolar reservoir. J Magn Reson B 1995; 108: 103–113.51. Basser PJ, Mattiello J, LeBihan D. MR diffusion tensor
spectroscopy and imaging. Biophys J 1994; 66: 259–267.52. Heiervang E, Behrens TE, Mackay CE, Robson MD,
Johansen-Berg H. Between session reproducibility and
between subject variability of diffusion MR and tracto-
graphy measures. Neuroimage 2006; 33: 867–877.
53. Alexander DC, Pierpaoli C, Basser PJ, Gee JC. Spatial
transformations of diffusion tensor magnetic resonance
images. IEEE Trans Med Imaging 2001; 20: 1131–1139.54. Pajevic S, Pierpaoli C. Color schemes to represent the
orientation of anisotropic tissues from diffusion tensor
data: application to white matter fiber tract mapping in
the human brain. Magn Reson Med 1999; 42: 526–540.55. Wakana S, Caprihan A, Panzenboeck MM, et al.
Reproducibility of quantitative tractography methods
applied to cerebral white matter. Neuroimage 2007; 36:
630–644.56. Jezzard P, Balaban RS. Correction for geometric distor-
tion in echo planar images from B0 field variations.Magn
Reson Med 1995; 34: 65–73.57. Fischer JS, Rudick RA, Cutter GR Reingold SC. for the
National MS Society Clinical Outcomes Assessment Task
Force. (1999). The Multiple Sclerosis Functional
Composite measure (MSFC): an integrated approach to
MS clinical outcome assessment. Mult Scler 1999; 5:
244–250.58. Mesaros S, Rovaris M, Pagani E, et al. A magnetic res-
onance imaging voxel-based morphometry study of regio-
nal gray matter atrophy in patients with benign multiple
sclerosis. Arch Neurol 2008; 65: 1223–1230.59. Bozzali M, Cercignani M, Sormani MP, Comi G, Filippi
M. Quantification of brain gray matter damage in differ-
ent MS phenotypes using diffusion tensor MR imaging.
AJNR Am J Neuroradiol 2002; 23: 985–958.
10 Multiple Sclerosis 0(00)

60. Chen JT, Narayanan S, Collins DL, Smith SM,Matthews PM, Arnold DL. Relating neocortical pathol-ogy to disability progression in multiple sclerosis using
MRI. Neuroimage 2004; 23: 1168–1175.61. Charil A, Dagher A, Lerch J, Zijdenbos AP, Worsley KJ,
Evans AC. Focal cortical atrophy in multiple sclerosis:relation to lesion load and disability. Neuroimage 2007;
34: 509–517.62. Filippi M, Bozzali M, Horsfield MA, et al. A conven-
tional and magnetization transfer MRI study of the cer-
vical cord in patients with multiple sclerosis. Neurology2000; 54: 207–213.
63. Gauthier SA, Berger AM, Liptak Z, et al. Rate of brain
atrophy in benign vs early multiple sclerosis. Arch Neurol2009; 66: 234–237.
64. Rocca MA, Colombo B, Falini A, et al. Cortical adapta-
tion in patients with MS: a cross-sectional functionalMRI study of disease phenotypes. Lancet Neurol 2005;4: 618–626.
65. Beaulieu C. The basis of anisotropic water diffusion in
the nervous system—a technical review. NMR Biomed2002; 15: 435–455.
66. Underhill HR, Yuan C, Yarnykh VL. Direct quantitative
comparison between cross-relaxation imaging and diffu-sion tensor imaging of the human brain at 3.0 T.NeuroImage 2009; 47: 1568–1578.
67. Sled JG, Levesque I, Santos AC, et al. Regional varia-tions in normal brain shown by quantitative magnetiza-tion transfer imaging. Magn Reson Med 2004; 51:
299–303.68. Bodini B, Khaleeli Z, Cercignani M, Miller DH,
Thompson AJ, Ciccarelli O. Exploring the relationshipbetween white matter and gray matter damage in early
primary progressive multiple sclerosis: an in vivo studywith TBSS and VBM. Human Brain Mapping 2009; 30:2852–2861.
69. Geurts JJ, Barkhof F. Grey matter pathology in multiplesclerosis. Lancet Neurol 2008; 7: 841–851.
70. Henry RG, Shieh M, Amirbekian B, Chung S, Okuda
DT, Pelletier D. Connecting white matter injury and tha-lamic atrophy in clinically isolated syndromes. J NeurolSci 2009; 282: 61–66.
71. Trapp BD, Peterson J, Ransohoff RM, Rudick R, MorkS, Bo L. Axonal transection in the lesions of multiplesclerosis. N Engl J Med 1998; 338: 278–285.
72. Tsunoda I, Kuang LQ, Libbey JE, Fujinami RS. Axonal
injury heralds virus-induced demyelination. Am J Pathol2003; 162: 1259–1269.
73. Bo L, Geurts JJ, van der Valk P, Polman C, Barkhof F.
Lack of correlation between cortical demyelination andwhite matter pathologic changes in multiple sclerosis.Arch Neurol 2007; 64: 76–80.
Spano et al. 11
Copyright © 2022 FDOKUMEN