
Multiparametric magnetic resonance imaging vs. standard care in men being evaluated for prostate...
7
Urologic Oncology: Seminars and Original Investigations 33 (2015) 17.e1–17.e7 Original article Multiparametric magnetic resonance imaging vs. standard care in men being evaluated for prostate cancer: A randomized study Valeria Panebianco, M.D. a, * , Flavio Barchetti, M.D. a , Alessandro Sciarra, M.D. b , Antonio Ciardi, M.D. a , Elena Lucia Indino, M.D. a , Rocco Papalia, M.D. c , Michele Gallucci, M.D. c , Vincenzo Tombolini, Prof. a , Vincenzo Gentile, Prof b , Carlo Catalano, Prof. a a Department of Radiological Sciences, Oncology and Pathology, Sapienza University of Rome, Rome, Italy b Department of Urology, Sapienza University of Rome, Rome, Italy c Department of Urology, Regina Elena National Cancer Institute, Rome, Italy Received 22 July 2014; received in revised form 8 September 2014; accepted 15 September 2014 Abstract Objectives: To assess whether the proportion of men with clinically significant prostate cancer (PCa) is higher among men randomized to multiparametric magnetic resonance imaging (mp-MRI)/biopsy vs. those randomized to transrectal ultrasound (TRUS)-guided biopsy. Methods: In total, 1,140 patients with symptoms highly suggestive of PCa were enrolled and divided in 2 groups of 570 patients to follow 2 different diagnostic algorithms. Group A underwent a TRUS-guided random biopsy. Group B underwent an mp-MRI and a TRUS- guided targeted þ random biopsy. The accuracy of mp-MRI in the diagnosis of PCa was calculated using prostatectomy as the standard of reference. Results: In group A, PCa was detected in 215 patients. The remaining 355 patients underwent an mp-MRI: the findings were positive in 208 and unremarkable in 147 patients. After the second random þ targeted biopsy, PCa was detected in 186 of the 208 patients. In group B, 440 patients had positive findings on mp-MRI, and PCa was detected in 417 at first biopsy; 130 group B patients had unremarkable findings on both mp-MRI and biopsy. In the 130 group B patients with unremarkable findings on mp-MRI and biopsy, a PCa Gleason score of 6 or precancerous lesions were detected after saturation biopsy. mp-MRI showed an accuracy of 97% for the diagnosis of PCa. Conclusions: The proportion of men with clinically significant PCa is higher among those randomized to mp-MRI/biopsy vs. those randomized to TRUS-guided biopsy; moreover, mp-MRI is a very reliable tool to identify patients to schedule in active surveillance. r 2014 Elsevier Inc. All rights reserved. Keywords: Magnetic resonance imaging; Prostate cancer; Biopsy; Ultrasonography; Prostate-specific antigen 1. Introduction Prostate cancer (PCa) is the most commonly diagnosed cancer in men and the second cause of cancer-related death in men. The detection of PCa is traditionally based on digital rectal examination (DRE), serum prostate-specific antigen (PSA) level, and transrectal ultrasound (TRUS)–guided biopsies [1]. However, DRE fails to detect a substantial proportion of cancers and identifies predominantly large tumors and in a more advanced pathologic stage [2]. PSA level has a poor specificity (Spe) and a low positive predictive value (PPV), because benign conditions can cause an increase in serum PSA levels. TRUS is currently considered inad- equate for diagnosing PCa, as at least 40% of neoplastic foci are isoechoic when compared with the surrounding paren- chyma [3]. TRUS-guided biopsy, with 6- to 12-core sam- pling, 1 to 2 for each sextant, has been the diagnostic standard for PCa for many years. Because up to 30% of cancers are missed when performing sextant biopsies and 23% of those are high-risk PCas, the method has been extended to 45 cores for saturation biopsies [3-6]. Nevertheless, it does not solve http://dx.doi.org/10.1016/j.urolonc.2014.09.013 1078-1439/r 2014 Elsevier Inc. All rights reserved. * Corresponding author. Tel.: þ390-6-445-5602, þ39 335/8443792 (mobile); fax: þ390-6-445-6695. E-mail addresses: [email protected], valeria.panebianco@ uniroma1.it (V. Panebianco).
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Multiparametric magnetic resonance imaging vs. standard care in men being evaluated for prostate...
Urologic Oncology: Seminars and Original Investigations 33 (2015) 17.e1–17.e7
http://dx.doi.org/10.1016/j1078-1439/r 2014 Elsev
* Corresponding autho(mobile); fax: þ390-6-445E-mail addresses: valer
uniroma1.it (V. Panebianc
Original article
Multiparametric magnetic resonance imaging vs. standard care in menbeing evaluated for prostate cancer: A randomized study
Valeria Panebianco, M.D.a,*, Flavio Barchetti, M.D.a, Alessandro Sciarra, M.D.b,Antonio Ciardi, M.D.a, Elena Lucia Indino, M.D.a, Rocco Papalia, M.D.c, Michele Gallucci, M.D.c,
Vincenzo Tombolini, Prof.a, Vincenzo Gentile, Profb, Carlo Catalano, Prof.a
a Department of Radiological Sciences, Oncology and Pathology, Sapienza University of Rome, Rome, Italyb Department of Urology, Sapienza University of Rome, Rome, Italy
c Department of Urology, Regina Elena National Cancer Institute, Rome, Italy
Received 22 July 2014; received in revised form 8 September 2014; accepted 15 September 2014
Abstract
Objectives: To assess whether the proportion of men with clinically significant prostate cancer (PCa) is higher among men randomized tomultiparametric magnetic resonance imaging (mp-MRI)/biopsy vs. those randomized to transrectal ultrasound (TRUS)-guided biopsy.Methods: In total, 1,140 patients with symptoms highly suggestive of PCa were enrolled and divided in 2 groups of 570 patients to
follow 2 different diagnostic algorithms. Group A underwent a TRUS-guided random biopsy. Group B underwent an mp-MRI and a TRUS-guided targeted þ random biopsy. The accuracy of mp-MRI in the diagnosis of PCa was calculated using prostatectomy as the standard ofreference.Results: In group A, PCa was detected in 215 patients. The remaining 355 patients underwent an mp-MRI: the findings were positive in
208 and unremarkable in 147 patients. After the second random þ targeted biopsy, PCa was detected in 186 of the 208 patients. In group B,440 patients had positive findings on mp-MRI, and PCa was detected in 417 at first biopsy; 130 group B patients had unremarkable findingson both mp-MRI and biopsy. In the 130 group B patients with unremarkable findings on mp-MRI and biopsy, a PCa Gleason score of 6 orprecancerous lesions were detected after saturation biopsy. mp-MRI showed an accuracy of 97% for the diagnosis of PCa.Conclusions: The proportion of men with clinically significant PCa is higher among those randomized to mp-MRI/biopsy vs.
those randomized to TRUS-guided biopsy; moreover, mp-MRI is a very reliable tool to identify patients to schedule in active surveillance.r 2014 Elsevier Inc. All rights reserved.
Keywords: Magnetic resonance imaging; Prostate cancer; Biopsy; Ultrasonography; Prostate-specific antigen
1. Introduction
Prostate cancer (PCa) is the most commonly diagnosedcancer in men and the second cause of cancer-related death inmen. The detection of PCa is traditionally based on digitalrectal examination (DRE), serum prostate-specific antigen(PSA) level, and transrectal ultrasound (TRUS)–guidedbiopsies [1]. However, DRE fails to detect a substantial
.urolonc.2014.09.013ier Inc. All rights reserved.
r. Tel.: þ390-6-445-5602, þ39 335/[email protected], valeria.panebianco@o).
proportion of cancers and identifies predominantly largetumors and in a more advanced pathologic stage [2]. PSAlevel has a poor specificity (Spe) and a low positive predictivevalue (PPV), because benign conditions can cause an increasein serum PSA levels. TRUS is currently considered inad-equate for diagnosing PCa, as at least 40% of neoplastic fociare isoechoic when compared with the surrounding paren-chyma [3]. TRUS-guided biopsy, with 6- to 12-core sam-pling, 1 to 2 for each sextant, has been the diagnostic standardfor PCa for many years. Because up to 30% of cancers aremissed when performing sextant biopsies and 23% of thoseare high-risk PCas, the method has been extended to 45 coresfor saturation biopsies [3-6]. Nevertheless, it does not solve

V. Panebianco et al. / Urologic Oncology: Seminars and Original Investigations 33 (2015) 17.e1–17.e717.e2
the problem because of increased costs, complications, and asmall but significant risk of missing high-grade cancer [4].Patients with a suspected false-negative result on biopsy are adiagnostic challenge, because there is a progressively lowerdiagnostic yield from subsequent prostate biopsies. Second,third, and fourth rebiopsies are reported to detect cancer inonly 25% to 27%, 5% to 24%, and 4% to 21% of cases,respectively. Furthermore, as PCa is multifocal in 85% ofcases, TRUS biopsy may underestimate the extent and gradeof cancer, which can result in Gleason upgrading afterprostatectomy [7].
In summary, PSA levels, DRE, and TRUS-guidedbiopsy do not have the ability to correctly localize andstage PCa and to determine its volume and aggressiveness.
Currently, urologists use nomograms for decisionmaking in the management of PCa. PSA levels, DRE, andTRUS-guided biopsy are the input for PCa nomograms, butthese parameters are fairly imperfect [1,4]. There is a realneed for clinicians to base therapeutic decisions not only onnomograms but also on advanced imaging findings.
Recently, a great interest has been shown for multi-parametric magnetic resonance imaging (mp-MRI), whichis an advanced diagnostic technique able to identify focalareas suggestive of PCa that could be considered aspotential sites for targeted biopsies [3].
In this context, the aim of this study was to validate therole of mp-MRI as a first-line tool in the diagnosticexamination of patients with symptoms highly suggestiveof PCa to assess whether the proportion of men withclinically significant PCa is higher among those randomizedto mp-MRI/biopsy vs. those randomized to TRUS-guidedbiopsy.
2. Materials and methods
2.1. Patient population and study design
This prospective study was approved by the localEthics Committee, and all patients gave written informedconsent.
In total, 1,140 consecutive male patients with anyperformance status and without any age limitation (averageage of 64 y, age range: 51–82 y), with symptoms highlysuggestive of PCa, who were referred to our institution fromOctober 2011 to March 2014, were enrolled in the study.The following were the inclusion criteria:
(a)
Total PSA level 44 ng/ml (b) PSA density 40.15 (c) PSA velocity 40.75 ng/ml/y (d) Free/total PSA ratio o0.10 when total PSA level wasbetween 4 and 10 ng/ml.
The patients needed to meet all the 4 inclusion criteria tobe included in the study.
Patients who previously underwent a prostate biopsywere excluded from the study.
The patient population was divided randomly in 2 groupsto follow 2 different diagnostic algorithms. Group Aincluded 570 patients who underwent a TRUS-guidedbiopsy according to a standard random scheme. Group Bincluded 570 patients who first underwent an mp-MRIexamination and, subsequently, underwent a TRUS-guidedbiopsy: if a suspicious lesion was detected on mp-MRI, thepatient was referred to a targeted þ random biopsy, other-wise if the finding on mp-MRI was unremarkable, thepatient underwent a random standard biopsy. Group Apatients with unremarkable findings on the first biopsyunderwent an mp-MRI examination and subsequently asecond TRUS-guided biopsy: if a suspicious lesion wasdepicted on mp-MRI, a targeted þ random biopsy wasperformed, and if the finding on mp-MRI was unremark-able, the patient underwent a TRUS-guided biopsy with asaturation method. In group B, in patients with unremark-able findings for PCa at first biopsy, a TRUS-guided biopsywith a saturation technique was performed.
The patients who were successfully diagnosed for PCaunderwent therapy according to their personal preferencesand the European Association of Urology guidelines.
2.2. MR equipment and image acquisition protocol
MRI of the pelvis, focused on the prostate gland, wasperformed using a 3-T magnet (Discovery MR750, GEHealthcare, Milwaukee, and MAGNETOM Verio SiemensMedical Solutions) equipped with a phased-array coil andan endorectal coil. The MRI protocol included the follow-ing sequences:
T2-weighted (T2w) turbo spin-echo sequences (repeti-tion time [TR], 4,500 ms; echo time [TE] 110 ms; thick-ness, 3 mm; and matrix, 352 � 352) in axial, sagittal, andcoronal planes.
Diffusion-weighted imaging (DWI) sequences: slicethickness, 3 mm; TR, 3,100 ms; TE, 102 ms; and exponen-tial b values of 0, 500, 1,000, and 3,000 s/mm2.
Dynamic contrast-enhanced (DCE) MRI was obtainedusing a gradient-echo T1-weighted sequence in axial planes(TR, 3 ms; TE, 2 ms; thickness, 3 mm; time resolution, 12sections/3 s; and matrix, 320 � 192).
The diagnostic accuracy of each technique alone and incombination with the others was evaluated.
2.3. Analysis of MR images
The images were evaluated in consensus by 2 genito-urinary radiologists, with 13 and 4 years of experience,blinded to blood test results.
Each MRI technique (T2w, DWI, and DCE) wasassessed relying on the prostate imaging reporting and datasystem (PI-RADS) score [8].
V. Panebianco et al. / Urologic Oncology: Seminars and Original Investigations 33 (2015) 17.e1–17.e7 17.e3
In patients with 2 or more dubious foci of PCa withdifferent PI-RADS scores, the zone assumed to be the indexlesion to which to direct the biopsy was the one with thehigher PI-RADS score. In patients with 2 or more focisuggestive of PCa with the same PI-RADS score, the areareported to be the index lesion was the one with the lowerapparent diffusion coefficient (ADC) values.
2.4. TRUS-guided prostate biopsy
The random biopsy scheme consisted of 14 coresobtained from every sextant sector in the prostatic periph-eral zone (PZ), including the medial and the lateral aspectsof the base (4 cores), the medial and the lateral aspects ofthe midgland (6 cores), and the apex (4 cores).
The targeted þ random biopsy scheme included 12cores: 4 cores from each side of the base in the PZ, 4cores from each side of the medial and the lateral aspects ofthe midgland in the PZ, 2 cores from each side of the apexin the PZ, and 2 cores carefully targeted toward the part ofthe sextant containing the index lesion.
The saturation method consisted of 45 cores: 27 biopsy coreswere obtained from every sextant sector in the PZ of theprostate gland, including the medial and the lateral aspects of thebase (9 cores), the medial and the lateral aspects of the midgland(10 cores), and the apex (8 cores), and 18 cores were taken fromthe transitional zone (TZ) and the central zone, including 4 coresfrom each side of the ventral and the dorsal aspects of the TZand 14 cores from the medial and the lateral aspects at the basal,middle, and apical portion of the central zone.
All pathologic specimens were reviewed by a singlepathologist with 18 years of expertise in genitourinarypathology. Each specimen was classified as containing nocancer, a precancerous lesion (low-grade prostatic intra-epithelial neoplasia [LGPIN], high-grade prostatic intra-epithelial neoplasia [HGPIN], atypical small acinarproliferation [ASAP], and proliferative inflammatory atro-phy [PIA]), or PCa (grading based on the Gleason score).
2.5. Statistical analysis and clinical validation
Statistical data analysis was applied using the statisticalsoftware MedCalc for Windows. Sensitivity (Se), Spe, PPV,negative predictive value (NPV), and accuracy of T2w,combined T2w þ DCE, combined T2w þ DWI, combinedDCE þ DWI, and combined T2w þ DCE þ DWI in theidentification of PCa were calculated on a per-lesion basisanalyses. Receiver operating characteristic curves were devel-oped to summarize the data. Histologic step-section analysis ofprostatectomy specimens was used as the standard of reference.
3. Results
In group A, PZ PCa was detected in 215 patients afterthe first biopsy. In the remaining 355 patients with no
evidence of PCa at first biopsy, 208 had positive results onmp-MRI examination and the other 147 had unremarkablefindings on mp-MRI. After the second biopsy, PCa wasdetected in 186 of the 208 patients with positive findings onmp-MRI (Fig. 1), 47 of which were TZ tumors; in the 147patients with unremarkable findings on mp-MRI, PZ PCawith a Gleason score of 6 (3 þ 3) was detected in 43 cases,an LGPIN in 16 patients, an HGPIN in 18 cases, an ASAPin 11 patients, and a PIA in 12 patients.
In group B, 440 patients had positive findings on mp-MRI: in 417, PCa was detected after the first biopsy in thespecimens of the index lesion, 98 of which were TZ tumors(Fig. 2), whereas the remaining 23 (all with a PZ indexlesion with PI-RADS score Z 3) showed negative resultsfor PCa. In group B, 130 patients had unremarkablefindings both on mp-MRI and after the first biopsy. In 17of the 23 group B patients with positive findings on mp-MRI examination and unremarkable findings on the firstbiopsy, PZ PCa was detected after the second biopsy. In the130 group B patients with unremarkable findings both onmp-MRI and at the first biopsy, PZ PCa with a Gleasonscore of 6 (3 þ 3) was detected in 37 cases, an LGPIN in 9,an HGPIN in 11, an ASAP in 9, and a PIA in 3. Theaforementioned results are summarized in Fig. 3.
Among all the patients with a confirmed PCa diagnosis,425 underwent a radical prostatectomy, 327 underwentradiation therapy, 60 received focal therapies (37 menunderwent high-intensity focused ultrasound therapy, 16of which were MR guided, and 23 patients received acryoablation treatment), and 103 were enrolled in an activesurveillance program.
The results of mp-MRI in identification of neoplastic focicompared with radical prostatectomy findings are summar-ized in the Table and Fig. 4. The T2w sequence aloneshowed a Se of 67%, a Spe of 73%, a PPV of 89%, a NPVof 61%, and an accuracy of 76%; the area under the receiveroperating characteristic curve (AUC) was 0.798 (standarderror [SE] ¼ 0.0201, 95% CI: 0.757–0.803). The combinedT2w þ DCE protocol showed a Se of 71%, a Spe of 79%, aPPV of 91%, a NPV of 64%, and an accuracy of 87%. TheAUC was 0.841 (SE ¼ 0.0241, 95% CI: 0.823–0.878).
The combined T2w þ DWI protocol showed a Se of 79%,a Spe of 83%, a PPV of 95%, a NPV of 68%, and an accuracyof 91%. The AUC was 0.871 (SE ¼ 0.0436, 95% CI: 0.843–0.891). The combined DWI þ DCE protocol showed a Se of82%, a Spe of 89%, a PPV of 96%, a NPV of 72%, and anaccuracy of 95%. The AUC was 0.914 (SE ¼ 0.0519, 95%CI: 0.879–0.928). The combined T2w þ DCE þ DWI proto-col showed a Se of 86%, a Spe of 94%, a PPV of 99%, a NPVof 78%, and an accuracy of 97%. The AUC was 0.946 (SE ¼0.0345, 95% CI: 0.913–0.973).
Moreover, a correlation between ADC values and PCaaggressiveness was described: The ADC values for low-grade tumors were 1 � 0.23 mm2/s, intermediate-gradetumors were approximately 0.7 � 0.17 mm2/s, and high-grade tumors were approximately 0.5 � 0.13 mm2/s.
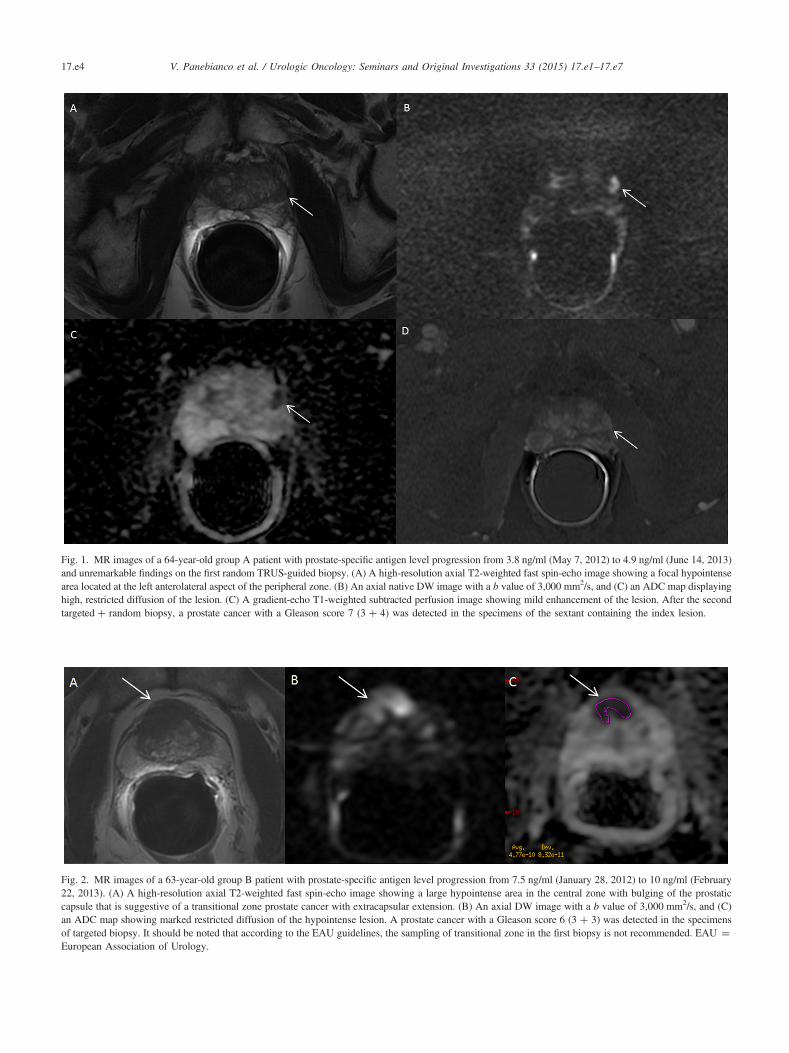
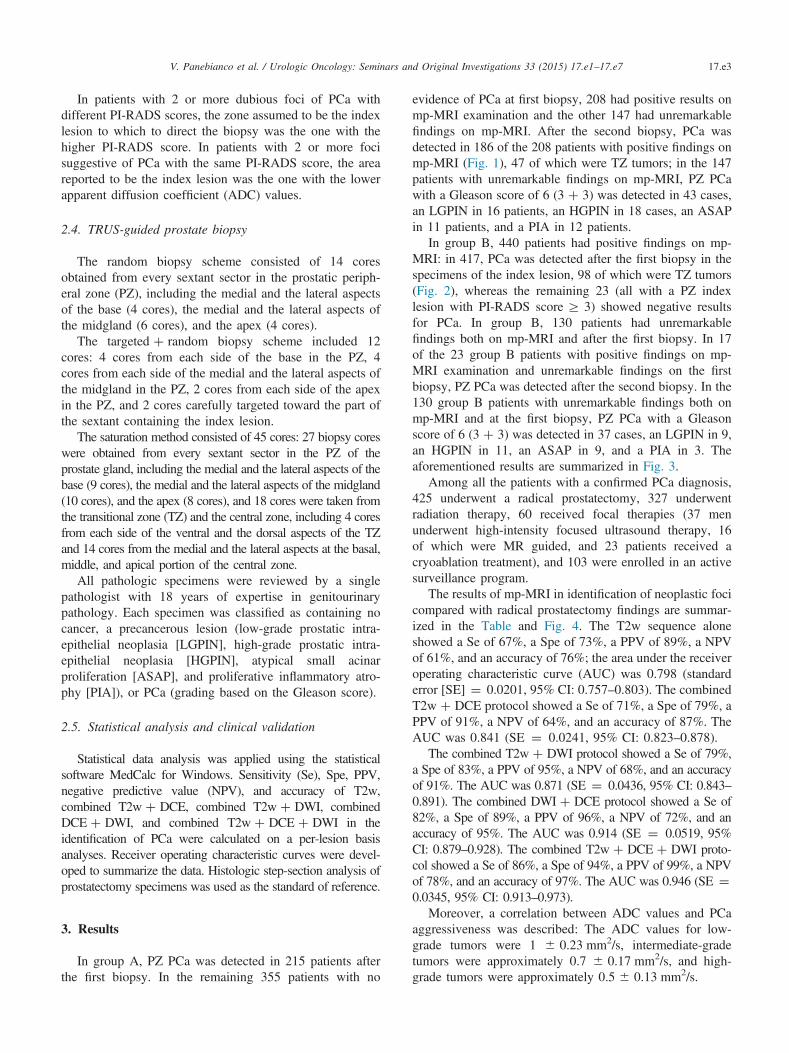
Fig. 1. MR images of a 64-year-old group A patient with prostate-specific antigen level progression from 3.8 ng/ml (May 7, 2012) to 4.9 ng/ml (June 14, 2013)and unremarkable findings on the first random TRUS-guided biopsy. (A) A high-resolution axial T2-weighted fast spin-echo image showing a focal hypointensearea located at the left anterolateral aspect of the peripheral zone. (B) An axial native DW image with a b value of 3,000 mm2/s, and (C) an ADC map displayinghigh, restricted diffusion of the lesion. (C) A gradient-echo T1-weighted subtracted perfusion image showing mild enhancement of the lesion. After the secondtargeted þ random biopsy, a prostate cancer with a Gleason score 7 (3 þ 4) was detected in the specimens of the sextant containing the index lesion.
Fig. 2. MR images of a 63-year-old group B patient with prostate-specific antigen level progression from 7.5 ng/ml (January 28, 2012) to 10 ng/ml (February22, 2013). (A) A high-resolution axial T2-weighted fast spin-echo image showing a large hypointense area in the central zone with bulging of the prostaticcapsule that is suggestive of a transitional zone prostate cancer with extracapsular extension. (B) An axial DW image with a b value of 3,000 mm2/s, and (C)an ADC map showing marked restricted diffusion of the hypointense lesion. A prostate cancer with a Gleason score 6 (3 þ 3) was detected in the specimensof targeted biopsy. It should be noted that according to the EAU guidelines, the sampling of transitional zone in the first biopsy is not recommended. EAU ¼European Association of Urology.
V. Panebianco et al. / Urologic Oncology: Seminars and Original Investigations 33 (2015) 17.e1–17.e717.e4
Fig. 3. A flow diagram depicting the results of the study design. AS ¼ active surveillance; FT ¼ focal therapy; RP ¼ radical prostatectomy; RT ¼radiation treatment.
Tablemp-MRI results in detecting PCa
MRI sequences Se(%)
Spe(%)
PPV(%)
NPV(%)
Accuracy(%)
AUC
T2w 67 73 89 61 76 0.798T2w þ DCE 71 79 91 64 87 0.841T2w þ DWI 79 83 95 68 91 0.871DWI þ DCE 82 89 96 72 95 0.914T2w þ DCE þ DWI 86 94 99 78 97 0.946
V. Panebianco et al. / Urologic Oncology: Seminars and Original Investigations 33 (2015) 17.e1–17.e7 17.e5
4. Discussion
Currently, urologists use nomograms for decisionmaking in the management of PCa. PSA levels, DRE, andTRUS-guided biopsy are the input for PCa nomograms, butthese parameters are fairly imperfect [1,4]. There is a realneed for clinicians to base therapeutic decisions on not onlynomograms but also advanced imaging findings.
Recently, great interest has been shown in mp-MRI,which combines high-resolution morphological T2w imag-ing and DWI for the evaluation of cell proliferation, DCEfor the evaluation of angiogenesis, and spectroscopicimaging for metabolic analysis [8,9]. The combinationof anatomical and functional information provided bymp-MRI, compared with morphological imaging based on
high-resolution T2w imaging only, makes it a promisingsuccessful imaging tool for improving the Se, Spe, andaccuracy in PCa detection, as validated by the results in ourstudy.
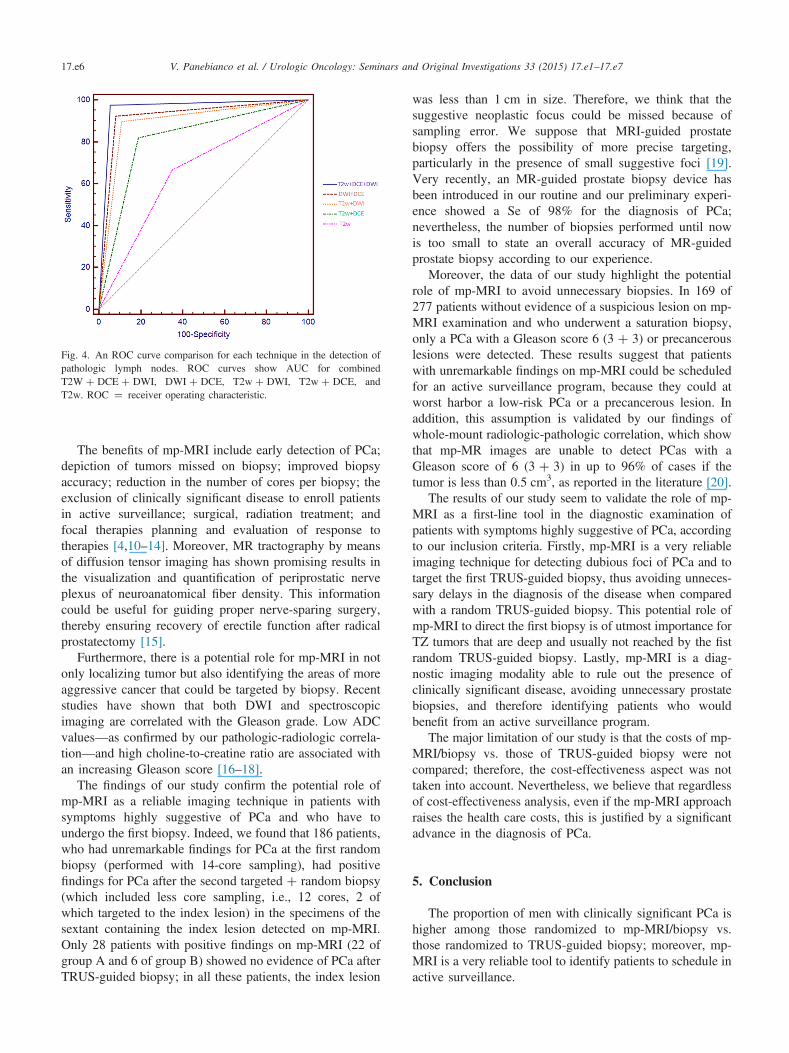
Fig. 4. An ROC curve comparison for each technique in the detection ofpathologic lymph nodes. ROC curves show AUC for combinedT2W þ DCE þ DWI, DWI þ DCE, T2w þ DWI, T2w þ DCE, andT2w. ROC ¼ receiver operating characteristic.
V. Panebianco et al. / Urologic Oncology: Seminars and Original Investigations 33 (2015) 17.e1–17.e717.e6
The benefits of mp-MRI include early detection of PCa;depiction of tumors missed on biopsy; improved biopsyaccuracy; reduction in the number of cores per biopsy; theexclusion of clinically significant disease to enroll patientsin active surveillance; surgical, radiation treatment; andfocal therapies planning and evaluation of response totherapies [4,10–14]. Moreover, MR tractography by meansof diffusion tensor imaging has shown promising results inthe visualization and quantification of periprostatic nerveplexus of neuroanatomical fiber density. This informationcould be useful for guiding proper nerve-sparing surgery,thereby ensuring recovery of erectile function after radicalprostatectomy [15].
Furthermore, there is a potential role for mp-MRI in notonly localizing tumor but also identifying the areas of moreaggressive cancer that could be targeted by biopsy. Recentstudies have shown that both DWI and spectroscopicimaging are correlated with the Gleason grade. Low ADCvalues—as confirmed by our pathologic-radiologic correla-tion—and high choline-to-creatine ratio are associated withan increasing Gleason score [16–18].
The findings of our study confirm the potential role ofmp-MRI as a reliable imaging technique in patients withsymptoms highly suggestive of PCa and who have toundergo the first biopsy. Indeed, we found that 186 patients,who had unremarkable findings for PCa at the first randombiopsy (performed with 14-core sampling), had positivefindings for PCa after the second targeted þ random biopsy(which included less core sampling, i.e., 12 cores, 2 ofwhich targeted to the index lesion) in the specimens of thesextant containing the index lesion detected on mp-MRI.Only 28 patients with positive findings on mp-MRI (22 ofgroup A and 6 of group B) showed no evidence of PCa afterTRUS-guided biopsy; in all these patients, the index lesion
was less than 1 cm in size. Therefore, we think that thesuggestive neoplastic focus could be missed because ofsampling error. We suppose that MRI-guided prostatebiopsy offers the possibility of more precise targeting,particularly in the presence of small suggestive foci [19].Very recently, an MR-guided prostate biopsy device hasbeen introduced in our routine and our preliminary experi-ence showed a Se of 98% for the diagnosis of PCa;nevertheless, the number of biopsies performed until nowis too small to state an overall accuracy of MR-guidedprostate biopsy according to our experience.
Moreover, the data of our study highlight the potentialrole of mp-MRI to avoid unnecessary biopsies. In 169 of277 patients without evidence of a suspicious lesion on mp-MRI examination and who underwent a saturation biopsy,only a PCa with a Gleason score 6 (3 þ 3) or precancerouslesions were detected. These results suggest that patientswith unremarkable findings on mp-MRI could be scheduledfor an active surveillance program, because they could atworst harbor a low-risk PCa or a precancerous lesion. Inaddition, this assumption is validated by our findings ofwhole-mount radiologic-pathologic correlation, which showthat mp-MR images are unable to detect PCas with aGleason score of 6 (3 þ 3) in up to 96% of cases if thetumor is less than 0.5 cm3, as reported in the literature [20].
The results of our study seem to validate the role of mp-MRI as a first-line tool in the diagnostic examination ofpatients with symptoms highly suggestive of PCa, accordingto our inclusion criteria. Firstly, mp-MRI is a very reliableimaging technique for detecting dubious foci of PCa and totarget the first TRUS-guided biopsy, thus avoiding unneces-sary delays in the diagnosis of the disease when comparedwith a random TRUS-guided biopsy. This potential role ofmp-MRI to direct the first biopsy is of utmost importance forTZ tumors that are deep and usually not reached by the fistrandom TRUS-guided biopsy. Lastly, mp-MRI is a diag-nostic imaging modality able to rule out the presence ofclinically significant disease, avoiding unnecessary prostatebiopsies, and therefore identifying patients who wouldbenefit from an active surveillance program.
The major limitation of our study is that the costs of mp-MRI/biopsy vs. those of TRUS-guided biopsy were notcompared; therefore, the cost-effectiveness aspect was nottaken into account. Nevertheless, we believe that regardlessof cost-effectiveness analysis, even if the mp-MRI approachraises the health care costs, this is justified by a significantadvance in the diagnosis of PCa.
5. Conclusion
The proportion of men with clinically significant PCa ishigher among those randomized to mp-MRI/biopsy vs.those randomized to TRUS-guided biopsy; moreover, mp-MRI is a very reliable tool to identify patients to schedule inactive surveillance.
V. Panebianco et al. / Urologic Oncology: Seminars and Original Investigations 33 (2015) 17.e1–17.e7 17.e7
References
[1] Chun FK, Steuber T, Erbersdobler A, Currlin E, Walz J, Schlomm T,et al. Development and internal validation of a nomogram predictingthe probability of prostate cancer Gleason sum upgrading betweenbiopsy and radical prostatectomy pathology. Eur Urol 2006;49:820–6.
[2] Smeenge M, Barentsz J, Cosgrove D, de la Rosette J, de Reijke T,Eggener S, et al. Role of transrectal ultrasonography (TRUS) in focaltherapy of prostate cancer: report from a consensus panel. BJU Int2012;110:942–8.
[3] Scattoni V, Raber M, Abdollah F, Roscigno M, Dehò F, Angiolilli D,et al. Biopsy schemes with the fewest cores for detecting 95% of theprostate cancers detected by a 24-core biopsy. Eur Urol 2010;57:1–8.
[4] Ukimura O, Coleman JA, de la Taille A, Emberton M, Epstein JI,Freedland SJ, et al. Contemporary role of systematic prostatebiopsies: indications, techniques, and implications for patient care.Eur Urol 2013;63:214–30.
[5] Barentsz JO, Richenberg J, Clements R, Choyke P, Verma S,Villeirs G, et al. ESUR prostate MRguidelines 2012. Eur Radiol2012;22:746–57.
[6] Heidenreich A, Bastian PJ, Bellmunt J, Bolla M, Joniau S,van der Kwast T, et al. EAU guidelines on prostate cancer. Part II:treatment of advanced, relapsing, and castration-resistant prostatecancer. Eur Urol 2014;65:467–79.
[7] Scattoni V, Zlotta A, Montironi R, Schulman C, Rigatti P, Montorsi F.Extended and saturation prostatic biopsy in the diagnosis and character-isation of prostate cancer: a critical analysis of the literature. Eur Urol2007;52:1309–22.
[8] Sciarra A, Barentsz J, Bjartell A, Eastham J, Hricak H, Panebianco V,et al. Advances in magnetic resonance imaging: how they are changingthe management of prostate cancer. Eur Urol 2011;59:962–77.
[9] Dickinson L, Ahmed HU, Allen C, Barentsz JO, Carey B, Futterer JJ,et al. Magnetic resonance imaging for the detection, localisation, andcharacterisation of prostate cancer: recommendations from a Euro-pean consensus meeting. Eur Urol 2011;59:477–94.
[10] Panebianco V, Barchetti F, Sciarra A, Musio D, Forte V, Gentile V,et al. Prostate cancer recurrence after radical prostatectomy: the roleof 3-T diffusion imaging in multi-parametric magnetic resonanceimaging. Eur Radiol 2013;23:1745–52.
[11] Panebianco V, Barchetti F, Musio D, Forte V, Pace A, De Felice F,et al. Metabolic atrophy and 3 T 1H—MR spectroscopy correlation
after radiation therapy for prostate cancer. BJU Int 2013, http://dx.doi.org/10.1111/bju.12553.
[12] Thompson J, Lawrentschuk N, Frydenberg M, Thompson L, Stricker P.The role of magnetic resonance imaging in the diagnosis and manage-ment of prostate cancer. BJU Int 2013;112(Suppl. 2):6–20, http://dx.doi.org/10.1111/bju.12381.
[13] Somford DM, Hoeks CM, Hulsbergen-van de Kaa CA, Hambrock T,Fütterer JJ, Witjes JA, et al. Evaluation of diffusion-weighted MRimaging at inclusion in an active surveillance protocol for low-riskprostate cancer. Invest Radiol 2013;48:152–7.
[14] Turkbey B, Mani H, Aras O, Ho J, Hoang A, Rastinehad AR, et al.Prostate cancer: can multiparametric MR imaging help identifypatients who are candidates for active surveillance? Radiology2013;268:144–52.
[15] Panebianco V, Barchetti F, Sciarra A, Marcantonio A, Zini C,Salciccia S, et al. In vivo 3D neuroanatomical evaluation ofperiprostatic nerve plexus with 3 T-MR diffusion tensor imaging.Eur J Radiol 2013;82:1677–82.
[16] Claus FG, Hricak H, Hattery RR. Pretreatment evaluation of prostatecancer: role of MR imaging and 1H MR spectroscopy. Radiographics2004;24(Suppl. 1):S167–80.
[17] Kobus T, Vos PC, Hambrock T, De Rooij M, Hulsbergen-Van de Kaa CA,Barentsz JO, et al. Prostate cancer aggressiveness: in vivo assessment ofMR spectroscopy and diffusion-weighted imaging at 3 T. Radiology2012;265:457–67.
[18] Hambrock T, Hoeks C, Hulsbergen-van de Kaa C, Scheenen T,Fütterer J, Bouwense S, et al. Prospective assessment ofprostate cancer aggressiveness using 3-T diffusion-weighted magneticresonance imaging-guided biopsies versus a systematic 10-coretransrectal ultrasound prostate biopsy cohort. Eur Urol 2012;61:177–84.
[19] Pokorny MR, de Rooij M, Duncan E, Schröder FH, Parkinson R,Barentsz JO, et al. Prospective study of diagnostic accuracy compar-ing prostate cancer detection by transrectal ultrasound-guided biopsyversus magnetic resonance (MR) imaging with subsequent MR-guided biopsy in men without previous prostate biopsies. Eur Urol2014, http://dx.doi.org/10.1016/j.eururo.2014.03.002.
[20] Shukla-Dave A, Hricak H, Akin O, Yu C, Zakian KL, Udo K, et al.Preoperative nomograms incorporating magnetic resonance imagingand spectroscopy for prediction of insignificant prostate cancer. BJUInt 2012;109:1315–22.




















