
Conventional imaging and multiparametric magnetic resonance (MRI, MRS, DWI, MRP) in the diagnosis of...
12
Vol. 56 - No. 4 THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGING 331 T he evaluation and management of prostate can- cer (PCa) are based mainly on parameters such as the serum prostate-specific antigen (PSA) level, clinical stage, and pathologic findings at biopsy or after surgery. 1, 2 The traditional radiology (RX-urog- raphy, RX-cystography) provides few information about the size of the prostate and an inconsistent supply about the pathological structural alterations, except for the repetitive injuries and suspected pros- tate cancer to bone. The three cross-sectional imaging modalities com- puted tomography (CT), ultrasonography, and mag- netic resonance imaging (MRI) have been proven in PCa patients, and they all have substantial limita- tions. 3 Great interest has been shown in multipara- metric MRI, which combines anatomic T2-weight- ed (T2W) imaging with MR spectroscopic imaging (MRSI), diffusion-weighted imaging (DWI), and/or dynamic contrast-enhanced MRI (DCE-MRI), espe- cially considering the possibility to routinely use high field intensity (1.5-3 Tesla magnet). The com- bination of anatomic, biologic, metabolic and func- tional dynamic information offered by multipara- metric MRI promises to make it a successful imaging tool for improving many aspects of PCa manage- ment. Nowadays there is the opportunity for clini- cians to make therapeutic decisions not only on pre- dictive methods nomograms which are PSA, digital 1 Department of Radiological Sciences Oncology and Pathology Sapienza University, Rome, Italy 2 Department of Urology, Sapienza University, Rome, Italy Q J NUCL MED MOL IMAGING 2012;56:331-42 V. PANEBIANCO 1 , A. SCIARRA 2 , A. MARCANTONIO 1 , V. FORTE 1 , T. BIONDI 1 , A. LAGHI 1 , C. CATALANO 1 Conventional imaging and Multiparametric Magnetic Resonance (MRI, MRS, DWI, MRP) in the diagnosis of prostate cancer The evaluation and management of prostate cancer (PCa) are based mainly on parameters such as the serum prostate-specific antigen level, clinical stage, and pathologic findings at biopsy or after surgery. The aim of this paper was to review the current roles of conventional imaging and multiparametric mag- netic resonance imaging (mpMRI) techniques in the diagnosis of PCa. A non systematic literature search using the Medline and Cochrane Library databases was performed up to January 2012. Bibliographies of retrieved articles and review articles were also ex- amined. Only those articles reporting complete data with clinical relevance for the present review (i.e., di- agnosis, staging) were selected. The advent of a high performance (1.5T) and higher fields strength (3T), and thus, higher spatial resolution, increased the potentiality and the diffusion of MR examinations. Intense research has focused on the use of comple- mentary techniques to improve the detection, char- acterization, and staging of PCa by MRI. This review article is divided into two major parts: the first one considers the technical aspects of mpMRI; the sec- ond part is intended to provide the impact of this technique on patients with PCa. Published data indi- cate an emerging role for MRI (particularly mpMRI combining T2 weighted imaging, diffusion weighted imaging, contrast enhanced MR, and spectroscopy) as the most sensitive and specific tool available for imaging PCa. MpMRI can provide metabolic infor- mation, characterize tissue and tumor vascularity, as well as tissue cellularity and correlate with tumor ag- gressiveness. KEY WORDS: Magnetic resonance imaging - Diffusion ma- gnetic resonance imaging - Magnetic resonance spectro- scopy - Prostatic neoplasms. Corresponding author: V. Panebianco, Department of Radiological Sciences, Oncology and Anatomical Pathology; La Sapienza, viale Regi- na Elena 324, 00161 Rome, Italy. E-mail: [email protected] MINERVA MEDICA COPYRIGHT® This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies (either sporadically or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other means which may allow access to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is not permitted. It is not permitted to remove, cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo, or other proprietary information of the Publisher.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Conventional imaging and multiparametric magnetic resonance (MRI, MRS, DWI, MRP) in the diagnosis of...

Vol. 56 - No. 4 THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGING 331
The evaluation and management of prostate can-cer (PCa) are based mainly on parameters such
as the serum prostate-specific antigen (PSA) level, clinical stage, and pathologic findings at biopsy or after surgery.1, 2 The traditional radiology (RX-urog-raphy, RX-cystography) provides few information about the size of the prostate and an inconsistent supply about the pathological structural alterations, except for the repetitive injuries and suspected pros-tate cancer to bone.
The three cross-sectional imaging modalities com-puted tomography (CT), ultrasonography, and mag-netic resonance imaging (MRI) have been proven in PCa patients, and they all have substantial limita-tions.3 Great interest has been shown in multipara-metric MRI, which combines anatomic T2-weight-ed (T2W) imaging with MR spectroscopic imaging (MRSI), diffusion-weighted imaging (DWI), and/or dynamic contrast-enhanced MRI (DCE-MRI), espe-cially considering the possibility to routinely use high field intensity (1.5-3 Tesla magnet). The com-bination of anatomic, biologic, metabolic and func-tional dynamic information offered by multipara-metric MRI promises to make it a successful imaging tool for improving many aspects of PCa manage-ment. Nowadays there is the opportunity for clini-cians to make therapeutic decisions not only on pre-dictive methods nomograms which are PSA, digital
1Department of Radiological SciencesOncology and Pathology
Sapienza University, Rome, Italy2Department of Urology, Sapienza University, Rome, Italy
Q J NUCL MED MOL IMAGING 2012;56:331-42
V. PANEBIANCO 1, A. SCIARRA 2, A. MARCANTONIO 1, V. FORTE 1, T. BIONDI 1, A. LAGHI 1, C. CATALANO 1
Conventional imaging and Multiparametric Magnetic Resonance (MRI, MRS, DWI, MRP) in the diagnosis of prostate cancer
The evaluation and management of prostate cancer (PCa) are based mainly on parameters such as the serum prostate-specific antigen level, clinical stage, and pathologic findings at biopsy or after surgery. The aim of this paper was to review the current roles of conventional imaging and multiparametric mag-netic resonance imaging (mpMRI) techniques in the diagnosis of PCa. A non systematic literature search using the Medline and Cochrane Library databases was performed up to January 2012. Bibliographies of retrieved articles and review articles were also ex-amined. Only those articles reporting complete data with clinical relevance for the present review (i.e., di-agnosis, staging) were selected. The advent of a high performance (1.5T) and higher fields strength (3T), and thus, higher spatial resolution, increased the potentiality and the diffusion of MR examinations. Intense research has focused on the use of comple-mentary techniques to improve the detection, char-acterization, and staging of PCa by MRI. This review article is divided into two major parts: the first one considers the technical aspects of mpMRI; the sec-ond part is intended to provide the impact of this technique on patients with PCa. Published data indi-cate an emerging role for MRI (particularly mpMRI combining T2 weighted imaging, diffusion weighted imaging, contrast enhanced MR, and spectroscopy) as the most sensitive and specific tool available for imaging PCa. MpMRI can provide metabolic infor-mation, characterize tissue and tumor vascularity, as well as tissue cellularity and correlate with tumor ag-gressiveness.Key words: Magnetic resonance imaging - Diffusion ma-gnetic resonance imaging - Magnetic resonance spectro-scopy - Prostatic neoplasms.
Corresponding author: V. Panebianco, Department of Radiological Sciences, Oncology and Anatomical Pathology; La Sapienza, viale Regi-na Elena 324, 00161 Rome, Italy. E-mail: [email protected]
Anno: 2012Mese: AugustVolume: 56No: 4Rivista: THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGINGCod Rivista: Q J NUCL MED MOL IMAGING
Lavoro: 2508-JNUtitolo breve: Conventional imaging and multiparametric MR in the diagnosis of prostate cancerprimo autore: PANEBIANCOpagine: 331-42
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

PANEBIANCO CONVENTIONAL IMAGING AND MULTIPARAMETRIC MR IN THE DIAGNOSIS OF PROSTATE CANCER
332 THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGING August 2012
parenchyma, in about two-thirds of cases;4-8 while in the other cases the lesions are isoechoic.
Locally advanced carcinoma can determine a pro-static capsule bulging and/or can infiltrate the cap-sule and the surrounding structures. The differential diagnosis between prostatic inflammation and can-cer is very hard because they show similar sono-graphic patterns.
Ultrasonography represents the first level exam in order to diagnose and to stage the prostate cancer although its sensitivity and specificity are very low (50%).9-12
In addition, the color-Doppler ultrasound allows detecting neoplastic foci as vascularized areas, but it does not improve the sensitivity of the exam.13,
14 The contrast enhanced ultrasound (CEUS) tech-nique increases both the sensitivity and specificity (70% and 65%, respectively) in the detection of tu-mor foci, nevertheless showing a wide variability of results, depending on PSA value, in the litera-ture.15 Elastosonography is a novel promising tech-nique aimed to quantify the tissue elasticity, which evaluates the strain ratio of healthy and pathological structures.16
Computed tomography and bone sCintigraphy
The three cross-sectional imaging modalities — computed tomography (CT) have been tested in PCa patients, and they all have substantial limitations. CT scan is not able to give significant additional infor-mation in the evaluation of prostate, mainly because the density of the neoplastic tissue does not suf-ficiently differ form the density of the healthy pros-tatic gland, even after contrast media administration. CT reports a low sensitivity (less than 50%) in the identification of localized neoplastic lesions. Moreo-ver, the sensitivity of CT in nodal staging is about 30%, as only based on an exclusive dimensional cri-teria (lymph nodes greater than 1 cm). CT scan is not often used even in the evaluation of patients who underwent radical prostatectomy, as lesions <2 cm are often unrecognized.
Bone scintigraphy (with or without dedicated rel-evant plain radiographs) has been the main meth-od for looking for metastatic bone disease, prior to intended curative treatment. Recommendations for instigating a radionuclide bone scan are well estab-lished. Patients with PSA ≤20 ng/mL and Gleason Score <8 have a 1% to 13% rate of positive bone scans.1
rectal examination (DRE) findings, and conventional imaging (suprapubic and transrectal ultrasound) and MR standard examination, but also on advanced multiparametric imaging and then on definitive his-topathological findings.
Evidence acquisition
The aim of this paper was to review the current roles of conventional imaging and multiparametric MRI techniques in the diagnosis of prostate cancer.
We searched the Medline and Cochrane Library databases (primary fields: prostatic neoplasm, mag-netic resonance; secondary fields: humans, spectros-copy, MRSI, 1-H NMR of prostate, dynamic contrast, quantitative perfusion, diffusion, early diagnosis, prostate biopsy, radical prostatectomy [RP], external radiation therapy [RT], focal therapies, recurrence). The search was performed without language restric-tion up to January 2012.
Conventional imaging: what is new and what is changed (past and present)
suprapubiC and transreCtal ultrasonography
Ultrasound (US) exam played an important role in the evaluation of prostate gland; in fact, US allowed a detailed structural assessment of the parenchyma, in its physiological and pathological conditions, as well as a more accurate measure of the organ di-mension.
The ultrasound exam of prostate-vesicular region consists of two different approaches: the suprapubic and the endocavitary one.
The suprapubic is a non-invasive approach, which provides a good visualization of the prostate-vesicu-lar complex; moreover it could be useful to quantify the residual volume of urine.
The endocavitary approach allows a detailed study of the peripheral region due to the anatomical region.
There are three different endocavitary probes: monoplanar, biplanar (commonly used in clinical practice) and multiplanar.
The latest multifrequency probes allow a deeper penetration-visualization of the ultrasound beam. Most prostate cancers origin in the posterior region of the gland (70-75%); they are displayed as hyp-oechoic areas, well defined from the surrounding
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

CONVENTIONAL IMAGING AND MULTIPARAMETRIC MR IN THE DIAGNOSIS OF PROSTATE CANCER PANEBIANCO
Vol. 56 - No. 4 THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGING 333
centrations of certain metabolites within voxels, in detail citrate, creatine, and choline. In PCa, ci-trate levels are reduced; creatine and choline lev-els are increased, thus PCa can be distinguished from healthy peripheral zone tissue by the choline plus creatine-to-citrate ratio with a cut-off value of 0.5.25 Unfortunately, some benign conditions, such as prostatitis and post-biopsy changes, may also re-sult in an increase of the ratio.3, 25 MRSI is an ac-curate technique to localize and characterize PCa, and to monitor changes indicating progression or treatment response.26 MRSI requires a longer acqui-sition time and more expertise than other functional MRI techniques, moreover the visualization of short echo time (TE) metabolites in prostate MRSI is dif-ficult due to lipid contamination and pulse timing constraints. Recently a new study reported that high quality prostate spectra are obtained by reducing the TE to 40 ms to detect short T2 metabolites, main-taining positive signal intensity of the spin-coupled citrate multiplet and managing lipid suppression.27
diffusion-weighted imaging
In diffusion-weighted imaging (DWI), proton dif-fusion properties within water are used to obtain image contrast. In clinical routine, 2 to 3 different b-values (ranging from 0 to 1000 sec/mm2) are gener-ally applied in a DW-MRI sequence for prostate, so that 2 to 3 images of the same volume with different signal intensity of tissues are obtained. If the signal intensity for each b-value is plotted, a curve with 2 to 3 points is obtained, which is generally displayed in a logarithmic scale. From this curve, by applying a specific formula, it is possible to calculate the appar-ent diffusion coefficient (ADC) of water molecules (expressed in mm2/s), which is the quantitative pa-rameter of this technique. ADC is often displayed on pixel-by-pixel maps (ADC maps), which are auto-matically generated from the workstation of the MRI scanners and commonly displayed in a grey scale: tissues with higher ADC values (increased diffusion) appear bright and tissues with lower ADC values (impeded diffusion) appear dark.28
The extracellular and intraductal water molecules move in all directions freely; therefore, in healthy prostate tissue within the peripheral zone, the so-called apparent diffusion coefficient (ADC) values are high. PCa tissue, destroying the normal glandular structure of the prostate, has a higher cellular den-sity than healthy prostate tissue. As a result the ex-
magnetiC resonanCe (mr)
MRI for prostate cancer (PCa) can be performed with a 1.5-Tesla (1.5 T) scanner and endorectal coil. The conventional sequences used to routinely visu-alize the prostate gland are the high definition TSE-T2 ones, able to discriminate between the peripheral and the central transitional zone because of their different water composition. The morphological ex-amination is performed along the three main spatial planes: axial, coronal and sagittal ones. The evalu-ation of the inferior abdomen must be performed using GRE T1 and TSE T2 axial sequences, in order to detect lymph nodes and to obtain an anatomical overview.
Tumor vascularization can be assessed by the dy-namic examination with GRE T1 sequences using different type of paramagnetic gadolinium based contrast media. All the acquired images are analyzed qualitatively and pathological foci are depicted as hyperintense areas marked by contrast media accu-mulation in the early arterial phase.17
Advanced imaging: multiparametric MR (MRI, MRS, DWI, MRP) when MR meet histopathology
The advent of a high performance (1.5 T) and higher fields strength (3T), and thus, higher spatial resolution, increased the potentiality and the diffu-sion of MR examinations.18, 19 Intense research has focused on the use of complementary techniques to improve the detection, characterization, and staging of PCa by MRI. In syntesis proton MRSI provides metabolic information, DWI shows the Brownian motion of extracellular water molecules, and DCE-MRI visualizes tissue vascularity, in detail the neoan-giogenesis.20-23
magnetiC resonanCe speCtrosCopiC imaging (1h-mrs)
With MRSI, three-dimensional (3D) data are ac-quired from the prostate, with volume elements (voxels) ranging from 0.24 cm3 to 0.34 cm3.24 Spec-troscopy is a technique that exploits the magnetic properties of certain atomic nuclei to determine physical and chemical properties of atoms or the molecules in which they are contained. It relies on the phenomenon of nuclear MR and can provide detailed information about the structure, dynamics, reaction state, and chemical environment of mol-ecules. Furthermore MRSI shows the relative con-
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

PANEBIANCO CONVENTIONAL IMAGING AND MULTIPARAMETRIC MR IN THE DIAGNOSIS OF PROSTATE CANCER
334 THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGING August 2012
of diagnosis and treatment. It is demonstrated that the ADC value at DWI (AUC=0.69) was the best per-forming single parameter for PCa detection when compared with T2-weighted imaging and DCE-MRI parameters.31 The clinical significance of PCa is re-lated to Gleason grades, Villeirs et al.37 investigated in 356 subjects (mean serum PSA = 11.5 ng/mL) the ability of MRSI (1.5T MRI) to predict the presence or absence of high-grade (Gleason score 4 + 3) PCa in men with elevated PSA. They found MRSI had signif-icantly higher sensitivity for high grade PCa (92.7%) than for lower grade tumours (67.6%) and a 7.4% false-positive rate. Moreover a recent study carried out by Hambrock T et al. demonstrated that there is a moderate correlation between ADC values and Gleason score.38 Multiparametric MRI techniques may also concur to the detection of transition-zone PCa. In a retrospective study of 23 patients, the ad-dition of DWI and DCE-MRI to T2-weighted MRI in-creased accuracy in the detection of transition-zone cancer from 64% to 79%.39 Also Delongchamps et al. have investigated about multiparametric MR in the detection of transitional zone tumor demonstrating that only T2W+DWI sequences resulted better than T2W alone (P=0.02).40 Recently Viswanath et al. have demonstrated that central gland (CG) and peripheral zone (PZ) prostate cancers have significantly differ-ing textural quantitative imaging signatures on T2w endorectal in vivo MRI.41 Moreover Vargas et al. de-scribed the anatomic features of the central zone of the prostate on T2-weighted and diffusion-weighted (DW) magnetic resonance (MR) images; they evalu-ated the diagnostic performance of MR imaging in detection of central zone involvement by prostate cancer demonstrating a sensitivity and specificity of 35% and 96% respectively.42
Biopsy strategies
Random TRUS-guided sextant biopsies have been reported to miss up to 30% of cancers, and when compared with RP for tumour localization, biopsy results had a positive predictive value (PPV) and a negative predictive value (NPV) of 83% and 36%, respectively.43 Although MRSI is not used at this time as a first approach to diagnose PCa, it can be use-ful in targeted biopsies, especially for patients with PSA levels suggestive of cancer and negative previ-ous biopsies.44 Biopsy strategies with an increased number of cores have also been proposed to reduce
tracellular space is reduced and, therefore, the water molecule movement is restricted so that PCa shows lower ADC values than surrounding, healthy, pe-ripheral-zone prostate tissue.20, 24 DWI examination can be obtained rapidly without the use of contrast medium, on the contrary DWI consists of echopla-nar imaging (EPI) sequences, which are susceptible to motion and magnetic field homogeneities.
Furthermore, the recent use of ultra high b val-ues (b=1000-2000) at 3 Tesla combined with the en-dorectal coil increases sensibility and sensitivity of this technique.29
dynamiC Contrast-enhanCed magnetiC resonanCe im-aging
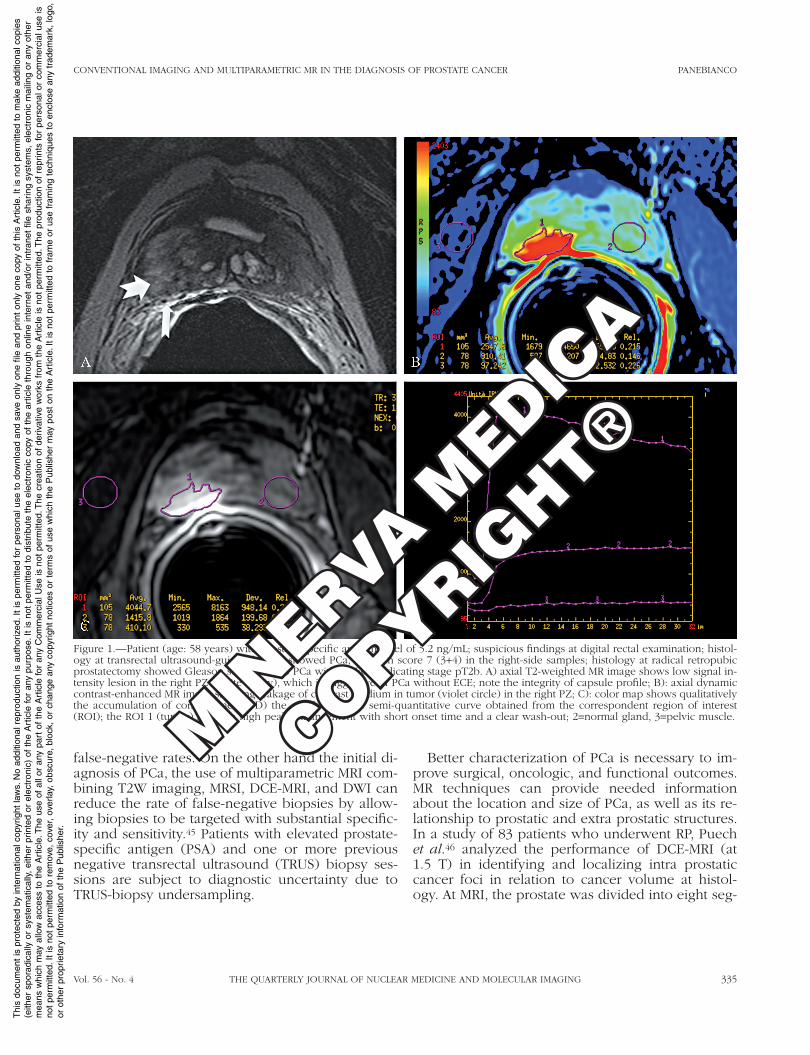
DCE-MRI consists of the acquisition of sequen-tial images using T1-weighted sequences during the passage of a contrast agent (gadopentetate dimeg-lumine) within prostatic tissue. The pharmacokinet-ics of gadolinium-based contrast agents in the pros-tate produce different enhancement patterns in PCa and benign tissues. The technique is based on the assessment of neoangiogenesis, which is an integral feature of tumors. DCE-MRI parameters can often be estimated qualitatively, semi-quantitatively and quan-titatively; color-map displays the contrast media accu-mulation (during perfusion time) using a qualitative colored scale; the semi-quantitative analysis consider signal enhancement onset time, time to peak, peak enhancement, and washout (Figure 1). The quantita-tive analysis in based on concentration to time ratio and regard the paramagnetic contrast media tran-sit time (k-trans) 30 DCE-MRI is limited by a lack of standardized acquisition protocols and analytic mod-els. DCE-MRI has high sensitivity, which can be use-ful for initial evaluation of potential tumor locations.
Initial diagnosis
As defined by the 2011 European Association of Urology guidelines,1 the primary methods for diag-nosing PCa include DRE, testing for serum concen-tration of PSA, and TRUS-guided prostate biopsy. The functional MRI techniques (MRSI, DWI, and DCE-MRI) have shown the opportunity of increasing the accuracy of conventional anatomic MRI in PCa detection (Figure 2).31-36 Since of their high specifi-city in comparison with PSA, their use could prevent unnecessary, systematic, random biopsies and delay
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.
CONVENTIONAL IMAGING AND MULTIPARAMETRIC MR IN THE DIAGNOSIS OF PROSTATE CANCER PANEBIANCO
Vol. 56 - No. 4 THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGING 335
Better characterization of PCa is necessary to im-prove surgical, oncologic, and functional outcomes. MR techniques can provide needed information about the location and size of PCa, as well as its re-lationship to prostatic and extra prostatic structures. In a study of 83 patients who underwent RP, Puech et al.46 analyzed the performance of DCE-MRI (at 1.5 T) in identifying and localizing intra prostatic cancer foci in relation to cancer volume at histol-ogy. At MRI, the prostate was divided into eight seg-
false-negative rates. On the other hand the initial di-agnosis of PCa, the use of multiparametric MRI com-bining T2W imaging, MRSI, DCE-MRI, and DWI can reduce the rate of false-negative biopsies by allow-ing biopsies to be targeted with substantial specific-ity and sensitivity.45 Patients with elevated prostate-specific antigen (PSA) and one or more previous negative transrectal ultrasound (TRUS) biopsy ses-sions are subject to diagnostic uncertainty due to TRUS-biopsy undersampling.
Figure 1.—Patient (age: 58 years) with prostate-specific antigen level of 5.2 ng/mL; suspicious findings at digital rectal examination; histol-ogy at transrectal ultrasound-guided biopsy showed PCa, Gleason score 7 (3+4) in the right-side samples; histology at radical retropubic prostatectomy showed Gleason score 7 (4+3) PCa without ECE indicating stage pT2b. A) axial T2-weighted MR image shows low signal in-tensity lesion in the right PZ (white arrow), which is suggestive of PCa without ECE; note the integrity of capsule profile; B): axial dynamic contrast-enhanced MR image showing leakage of contrast medium in tumor (violet circle) in the right PZ; C): color map shows qualitatively the accumulation of contrast media; D) the graph dysplays semi-quantitative curve obtained from the correspondent region of interest (ROI); the ROI 1 (tumor) shows a high peak enhancement with short onset time and a clear wash-out; 2=normal gland, 3=pelvic muscle.
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

PANEBIANCO CONVENTIONAL IMAGING AND MULTIPARAMETRIC MR IN THE DIAGNOSIS OF PROSTATE CANCER
336 THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGING August 2012
dard. The results of combined MRI/MRSI were rel-evant, but their accuracy did not differ significantly among the different areas of the prostate (AUC=0.71 for the base, 0.61 for the midgland, and 0.69 for the apex). Weinreb et al.48 published the results of a prospective multicentre study conducted by the American College of Radiology Imaging Network to assess the incremental value of MRSI to MRI in the sextant localization of peripheral-zone PCa. Authors analyzed imaging results for 134 patients with PCa
ments and results scored on a five-point scale. The sensitivity and specificity of DCE-MRI for identifica-tion of PCa foci of any volume were 32% and 95%, respectively. For identification of cancer foci >0.5 cc, the sensitivity and specificity were 86% and 94%, respectively, and the AUC was 0.874. In their study of 158 patients with clinical stage T1c PCa, Zhang et al.47 assessed the accuracy of MRI/MRSI in predict-ing PCa in 12 prostate regions, using whole-mount, step-section pathologic maps as the reference stan-
Figure 2.—Patient (age: 46 years) with prostate-specific antigen (PSA) progression, from 3.8 ng/mL (2010) to 4.8 ng/mL (2011). A) T2-weighted MRI shows little (<5-mm) hypointense signal intensity nodule (red circle) at middle third prostate level, in a right postero-lateral region; B) axial dynamic contrast-enhanced MR image showing leakage of contrast medium in tumour (red circle) in the right PZ; the yellow circle represents the normal tissue while the blu one is plotted over the pelvic muscle; C) DCE-MRI intensity/time curve displays a hypervascular lesion (red curve) with high peak enhancement with short onset time and a clear wash-out; 2(green)=central adenoma; 3(yellow)=normal gland; 4(blu)=pelvic muscle; D) MR spectroscopic imaging qulaitative analysis with reference images on the nodule shows three consecutive voxels with an increased ratio (Cho+Cr/Ci>1); E) diffusion weighted imaging (DWI) shows (green circle) high signal intensity in the right PZ, which may be suggestive of an area of water molecules restriction.
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

CONVENTIONAL IMAGING AND MULTIPARAMETRIC MR IN THE DIAGNOSIS OF PROSTATE CANCER PANEBIANCO
Vol. 56 - No. 4 THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGING 337
tecting cancer recurrence and monitoring therapy response.52 However, the findings still need to be validated in larger studies. Seitz et al. in their col-laborative review article 24 underlined that sensitiv-ity, specificity, and accuracy in tumour staging were higher with DCE-MRI than with MRSI. In a limited population of 64 cases, Kim et al.53 analyzed the role of a combined DWI and DCE-MRI technique (at 1.5T) in predicting the local stage, using pathologic results obtained at RP as the reference standard. In detecting extra prostatic extension, the combination of DWI and DCE-MRI displayed 82.4% sensitivity, 87.2% specificity, 70% PPV, and 93.2% NPV.
Higher values (92.3%, 93.1%, 85.7%, and 96.7%, respectively) were found when only cases with clin-ically high-risk disease features (cT3, PSA “20 ng/ml, or Gleason score: 8) were analyzed. The overall accuracy of PCa staging by MRI/MRSI was 80%; stag-ing accuracy was highest for the smallest tumour volumes (91% for tumour volumes <0.5 cm3 vs. 75% for tumor volumes >2 cm3). In the detection of extra capsular disease, MRI/MRSI had an AUC of 0.74. In a limited population of 27 patients considered for RP, Augustin et al.54 compared the accuracy of 3T MRI with the Partin tables in predicting pathologic stage. In the detection of extra capsular extension, MRI had an accuracy of 85.2%, sensitivity of 66.7%, and specificity of 100%. The Spearman r for correlation with extra capsular extension was higher for MRI findings (0.780) than for the Partin tables (0.363). Overall, 3T MRI was significantly more accurate than the Partin tables in predicting the final pathologic stage.
The possibility of improving the planning of a nerve-sparing RP, combining an oncologic and func-tional evaluation, is also clinically suggestive. The decision to preserve or resect the neurovascular bundles (NVBs) at RP is often difficult and based on preoperative clinical characteristics and intraopera-tive findings. MRI techniques can help predict the absence of tumor in the areas of the NVBs.
In a study of 75 patients with PCa scheduled for RP, Labanaris et al.55 analyzed the value of conven-tional and functional 1.5T MRI in predicting the risk of extra capsular extension in relation to NVBs. Cases were considered appropriate for nerve spar-ing surgery if the tumor did not extend outside the capsule in the postero-lateral region of the prostate as assessed by imaging. Based on MRI findings, the operative strategy was changed in 44% of cases. Among these, the findings favoured NVB preserva-
who underwent combined MRI/MRSI at 1.5T. Eight readers independently rated the likelihood of the presence of PCa in each prostate sextant by using a five-point scale then histopathologic results at RP were used as the reference standard. The accuracy of combined MRI/MRSI (AUC=0.58) was equivalent to that of MRI alone (AUC=0.60). This negative result for MRSI may have been partly related to the fol-lowing reason: the study population consisted pre-dominantly of patients with low-risk, small-volume disease: Most of the cases were clinical stage T1c, the mean PSA was 5.9 ng/mL, and the mean tumor volume was 2.75 cm3.
Katahira et al.49 studied 201 patients with PCa who underwent DWI before RP. Each prostate was divided into eight segments; on the basis of 1.5T MRI results, the probability of the presence of PCa in each segment was estimated using a five-point rating scale. Results were compared with those of whole-mount, step-section, histopathologic exami-nation. The sensitivity, specificity, and AUC of DWI for the localization of PCa were 73%, 89%, and 0.842, respectively.
While TRUS guided biopsy cannot offer an high sensitivity in biopsy strategies even if performed with image fusion approach, more recently an emerging technique such as Magnetic resonance guided biopsy (MRGB) has shown high prostate cancer (PCa) detection rates in studies with limited patient numbers. Hoeks CM et al. in a recent study demonstrated an increased sensitivity in cancer de-tection (47-56%). Complications occurred in only in 0.2% of patients (5 of 265).50
Recently some studies 51 have revealed the high diagnostic accuracy of combined proton 1H-mag-netic resonance spectroscopic imaging (1H-MRSI) and dynamic contrast-enhanced imaging magnetic resonance (DCEMR) in the management of prostate cancer.
Preoperative local staging and therapeutic planning
The literature shows a wide range (50-92%) in the accuracy of local staging by MRI. Magnetic reso-nance spectroscopic imaging can be used to pre-dict the presence or absence of cancer. It also pro-vides information about lesion aggressiveness, but does not give staging information owing to its poor spatial resolution. Thus, MRSI is a valid tool for de-
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

PANEBIANCO CONVENTIONAL IMAGING AND MULTIPARAMETRIC MR IN THE DIAGNOSIS OF PROSTATE CANCER
338 THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGING August 2012
Regarding the lymph node metastasis, 70% of the their are so small (<8 mm) to be evaluated using MRI, so conventional size criteria may underestimate the extent of nodal disease. A meta-analysis sug-gests that CT and MRI perform equally poorly in the detection of lymph node metastases from prostate cancer with a sensitivity of around 30%.60
Superiority of MRI over scintigraphy in detect-ing bone lesions has been suggested for a decade or more (MRI sensitivity 100% and specificity 80%; scintigraphy and conventional plain films sensitiv-ity 63%, specificity 64%).61, 62 However, its utility has been limited because of technical problems in whole skeletal acquisition.
Prostate recurrence
The level of evidence to support the use of mul-tiparametric MRI in this field starts to be significant, particularly for preoperative localization and map-ping of the tumor and an early diagnosis of local recurrence. Patients with a positive margin and a PSA that does not become undetectable should be referred for an oncology opinion before the PSA reaches 0.5 ng/mL, if clinically relevant. Multipara-metric MRI can be considered a valid tool to evalu-ate the prostatic fossa in patients with low PSA value (ranged between 0.2 ng/mL and 2 ng/mL) where, according to the EAU, other techniques (PET, TRUS biopsy) are not recommended. Where appropriate treatment (salvage radiotherapy) is considered, dy-namic contrast enhanced MRI and/or DWI could be performed.63
Different prospective studies on a significant pop-ulation have been presented. A 3T MRI evaluation can be sufficient, but the combination of at least two (DCE-MRI and MRSI) multiparametric techniques can improve results, particularly for an early diagno-sis of local recurrence 64 (Figure 3). In addition, MRSI and DWI can distinguish the presence of recurrence from healthy residual prostate tissue demonstrating how the diagnostic accuracy of combined 1HMRSI-DCEMR was higher than PET/CT to identify local prostate cancer recurrence, mostly in patients with low biochemical progression after RRP (0.2-2 ng/mL).65 Limitations are mainly related to possible ar-tifacts due to structure modification after the biopsy or the surgical procedure that can influence a cor-rect analysis of the prostate or of a possible recur-rence.
tion in 67% of cases with high clinical probability of extra capsular extension and opposed NVB preser-vation in 33% of cases with low clinical probability of extra capsular extension. Based on the final his-topathologic findings, the sensitivity, specificity, and accuracy of MRI in predicting seminal-vesicle inva-sion, extra capsular extension, or NVB involvement, and thereby obtaining a correct preoperative deci-sion, were 92%, 100%, and 100%, respectively. In a population of 62 patients who underwent RP, Brown et al.56 evaluated the impact of preoperative staging with 1.5T MRI on NVB-sparing aggressiveness and surgical margin positivity. They concluded that un-enhanced MRI is of limited usefulness in detecting extra capsular extension and therefore carries the risk of leading to inappropriate nerve-sparing sur-gery and possible positive surgical margins. MRSI, DWI, and DCE-MRI were not performed in the study.
The probability of recovering erectile function after RP is associated inversely with patient age and comorbidity, and directly with the extent and number of NVBs preserved. In patients reported to have undergone nerve preservation, poor recovery of erectile function after surgery raises several ques-tions. In a study of 53 patients with PCa who under-went bilateral nerve-sparing RP, Panebianco et al.57 analyzed the capability of a dedicated 3D, isotropic, MRI T2-weighted sequence to depict postsurgical changes in the NVBs. Postoperative MRI examina-tions were compared with the International Index of Erection Function five-item (IIEF-5) questionnaire, which served as the reference standard. The authors developed a relative five-point system for classify-ing MRI findings on the basis of anatomic course delineation for each or both NVBs. In all cases the correlation and regression analysis between MRI and IIEF-5 findings resulted in high coefficient val-ues (r=0.45; P=0.001). The imaging protocol and the NVB-change classification system proposed in this study can be applied successfully as early as 40 d after RP. Together, they could provide an additional diagnostic tool in the postoperative evaluation and treatment of erectile dysfunction. Recently McClure et al.58 investigated how multiparametric MRI can influence the decision to preserve neurovascular bundles in robotic-assisted laparoscopic prostatec-tomy (RALP). Also Naiki T et al.59 analyzed the neu-rovascular bundle involvement of localized prostate cancer and a comparison between T2+DWI+ADC and T2WI alone, was carried out demonstrating a significant higher sensitivity of multiparametric MR.
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

CONVENTIONAL IMAGING AND MULTIPARAMETRIC MR IN THE DIAGNOSIS OF PROSTATE CANCER PANEBIANCO
Vol. 56 - No. 4 THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGING 339
pears to be the most accurate imaging method for localizing primary PCa and staging primary or recur-rent PCa. The available literature suggests that mul-tiparametric MRI is helpful and clinically relevant for the following tasks at minimum: 1) detection of PCa in patients with previous negative prostate biopsies and persistently elevated serum markers, in whom it reduces the need for additional and more extensive biopsies and identifies suspicious areas for targeted sampling; 2) tumor aggressiveness of PCa to facili-tate appropriate treatment selection; 3) local stag-ing and 4) early identification of local recurrence in patients with biochemical recurrence after primary therapy.
Conclusions
The standard tests and predictive models that cli-nicians use to choose diagnostic and therapeutic strategies for PCa have considerable limitations, and a valid imaging tool is needed to improve all stag-es of PCa management. Published data indicate an emerging role for MRI (particularly multiparametric MRI combining T2W imaging, DWI, DCE, and MRSI) as the most sensitive and specific tool available for imaging PCa. Multiparametric MRI can provide met-abolic information, characterize tissue and tumour vascularity, as well as tissue cellularity and integ-rity and correlate with tumor aggressiveness.66 It ap-
Figure 3.—Patient (age: 58 years) with prostate-specific antigen (PSA) progression, from 0.1 to 0.8 ng/mL, 7 months after radical retropubic prostatectomy (RRP). At RRP, prostatic adenocarcinoma of Gleason 7 score (4+3) and stage pT2c was found. Locally recurrent prostate cancer was confirmed on the basis of a PSA decrease (PSA=0.1 ng/mL); A) T2-weighted MRI shows 5-mm intermediate signal intensity nodule (white arrow) in a right perianastomotic location; B) MR spectroscopic imaging qualitative analysis with reference images on the nodule shows three consecutive voxels with an increased ratio (Cho+Cr/Ci>1); C) the spectroscopic quantitative analysis confirms the re-duced citrate (Ci) signal and increased choline (Cho) one; D) dynamic contrast-enhanced (DCE) MRI shows a hypervascular lesion (white arrows); E, F) show DCE-MRI intensity/time curve and concentration/time curve of the same area demonstrating a hypervascular lesion.
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

PANEBIANCO CONVENTIONAL IMAGING AND MULTIPARAMETRIC MR IN THE DIAGNOSIS OF PROSTATE CANCER
340 THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGING August 2012
ultrasound in imaging and detection of prostate cancer: phase II multicenter clinical trial. World J Urol 2012 [Epub ahead of print].
16. Kapoor A, Kapoor A, Mahajan G, Sidhu BS. Real-time elastog-raphy in the detection of prostate cancer in patients with raised PSA level. Ultrasound Med Biol 2011;37:1374-81.
17. Cardone G, Messina A, Borrone M. RM della prostata: aspetti tecnici e protocolli In: Passariello R, Di Silverio F, Panebianco V, Sciarra A, editors. Imaging RM (risonanza magnetica) della prostata. Milano: Springer-Verlag Italia; 2009. p. 25-34.
18. Jacobs MA, Ouwerkerk R, Petrowski K, Macura KJ. Diffusion-weighted imaging with apparent diffusion coefficient mapping and spectroscopy in prostate cancer. Top Magn Reson Imaging 2008;19:261-72.
19. Mazaheri Y, Shukla-Dave A, Muellner A, Hricak H. MR imaging of the prostate in clinical practice. MAGMA 2008;21:379-92.
20. Somford DM, Futterer JJ, Hambrock T, Barentsz JO. Diffusion and perfusion MR imaging of the prostate. Magn Reson Imaging Clin N Am 2008;16:685-95, ix.
21. Futterer JJ, Barentsz J, Heijmijnk ST. Imaging modalities for pros-tate cancer. Expert Rev Anticancer Ther 2009;9:923-37.
22. Yakar D, Debats OA, Bomers JG, Schouten MG, Vos PC, van Lin E et al. Predictive value of MRI in the localization, staging, volume estimation, assessment of aggressiveness, and guidance of radiotherapy and biopsies in prostate cancer. J Magn Reson Imaging 2012;35:20-31.
23. Cornud F, Delongchamps NB, Mozer P, Beuvon F, Schull A, Mu-radyan N et al. Value of multiparametric MRI in the work-up of prostate cancer. Curr Urol Rep 2012;13:82-92.
24. Seitz M, Shukla-Dave A, Bjartell A, Touijer K, Sciarra A, Bastian PJ et al. Functional magnetic resonance imaging in prostate cancer. Eur Urol 2009;55:801-14.
25. Pucar D, Shukla-Dave A, Hricak H, Moskowitz CS, Kuroiwa K, Olgac S. Prostate cancer: correlation of MR imaging and MR spectroscopy with pathologic findings after radiation therapy-initial experience. Radiology 2005;236:545-53.
26. Sciarra A, Panebianco V, Salciccia S, Lisi D, Alfarone A, Gen-tilucci A et al. Determination of the time for maximal response to neoadjuvant hormone therapy for prostate cancer using mag-netic resonance with spectroscopy (MRSI) and dynamic contrast enhancement (DCEMR). Urol Oncol 2011 [Epub ahead of print].
27. Venugopal N, McCurdy B, Al Mehairi S, Alamri A, Sandhu GS, Sivalingam S et al. Short echo time in vivo prostate ¹H-MRSI. Magn Reson Imaging 2012;30:195-204
28. Petralia G, Giannarini G, Thoeny HC. Potential and limitations of diffusion-weighted magnetic resonance imaging in kidney, pros-tate and bladder cancer: a critical analysis of the literature. Eur Urol 2012;61:326-40.
29. Metens T, Miranda D, Absil J, Matos C. What is the optimal b value in diffusion-weighted MR imaging to depict prostate can-cer at 3T? Eur Radiol 2012;22:703-9.
30. Franiel T, Hamm B, Hricak H. Dynamic contrast-enhanced mag-netic resonance imaging and pharmacokinetic models in pros-tate cancer. Eur Radiol 2011;21:616-26.
31. Langer DL, van der Kwast TH, Evans AJ, Trachtenberg J, Wilson BC, Haider MA. Prostate cancer detection with multi-parametric MRI: logistic regression analysis of quantitative T2, diffusion-weighted imaging, and dynamic contrast-enhanced MRI. J Magn Reson Imaging 2009;30:327-34.
32. Riches SF, Payne GS, Morgan VA, Sandhu S, Fisher C, Germuska M et al. MRI in the detection of prostate cancer: combined ap-parent diffusion coefficient, metabolite ratio, and vascular pa-rameters. AJR Am J Roentgenol 2009;193:1583-91.
33. Kozlowski P, Chang SD, Meng R, Mädler B, Bell R, Jones EC et al. Combined prostate diffusion tensor imaging and dynamic con-trast enhanced MRI at 3T--quantitative correlation with biopsy. Magn Reson Imaging 2010;28:621-8.
34. Kitajima K, Kaji Y, Fukabori Y, Yoshida K, Suganuma N, Sug-imura K. Prostate cancer detection with 3 T MRI: comparison of diffusion-weighted imaging and dynamic contrast-enhanced MRI
At least multiparametric-MRI data need to be pre-sented to clinical colleagues in a simple but mean-ingful way, preferably using a structured reporting scheme. It consists of PI-RADS score which relays the probability of cancer risk and its aggression, plotted on a scheme.
Location, probability of extra-prostatic disease and pertinent incidental findings should be also in-cluded in the well structured report.52
References
1. Heidenreich A, Bellmunt J, Bolla M, Joniau S, Mason M, Matveev V et al. EAU guidelines on prostate cancer. Part 1: screening, diagnosis, and treatment of clinically localised disease. European Association of Urology. Eur Urol 2011;59:61-71.
2. Walz J, Burnett AL, Costello AJ, Eastham JA, Graefen M, Guil-lonneau B et al. A critical analysis of the current knowledge of surgical anatomy related to optimization of cancer control and preservation of continence and erection in candidates for radical prostatectomy. Eur Urol 2010;57:179-92.
3. Sciarra A, Panebianco V, Salciccia S, Cattarino S, Lisi D, Genti-lucci A et al. Modern role of magnetic resonance and spectros-copy in the imaging of prostate cancer. Urol Oncol 2011;1:12– 20.
4. Ciccariello M, Teodonio S. Background strumentale nell’imaging della prostata. In: Passariello R, Di Silverio F, Panebianco V, Sci-arra A, editors. Imaging RM (risonanza magnetica) della prostata. Milano: Springer-Verlag Italia; 2009. p. 17-24.
5. Lee F Jr, Bronson JP, Lee F, Torp-Pedersen ST, Siders DB, Thorn-bury JR et al. Non-palpable cancer of the prostate: assessment with transrectal ultrasound. Radiology 1991;178:197-9.
6. Lee F, Torp-Pedersen ST, Siders DB. Use of transrectal ultrasound in diagnosis, guided biopsy, staging, and screening of prostate cancer. Urology 1989;33(Suppl):7-12.
7. Lee F, Torp-Pedersen ST, Siders DB Littrup PJ, McLeary RD. Tran-srectal ultrasound in the diagnosis and staging of prostatic carci-noma. Radiology 1989;170(3 pt 1):609-15.
8. Cooner WH, Mosley BR, Rutherford CL Jr, Beard JH, Pond HS, Bass RB Jr et al. Clinical application of transrectal ultrasonog-raphy and prostate specific antigen in the search for prostate cancer. J Urol 1988;139:758-61.
9. Ellis WJ, Chetner MP, Preston SD, Brawer MK. Diagnosis of pros-tatic carcinoma: the yield of serum prostate specific antigen, digital rectal examination and transrectal ultrasonography. J Urol 1994;152(5 Pt 1):1520-5.
10. Gustafsson O, Norming U, Almgård LE, Fredriksson A, Gustavs-son G, Harvig B et al. Diagnostic methods in the detection of prostate cancer: a study of a randomly selected population of 2,400 men. J Urol 1992;148:1827-31.
11. Mettlin C, Murphy GP, Babaian RJ, Chesley A, Kane RA, Littrup PJ et al. The results of a five-year early prostate cancer detection intervention. Investigators of the American Cancer Society Na-tional Prostate Cancer Detection Project. Cancer 1996;77:150-9.
12. Jones WT, Resnick MI. Prostate ultrasound in screening, diagno-sis and staging of prostate cancer. Probl Urol 1999;04:343-57.
13. Rifkin MD, Sudakoff GS, Alexander AA. Prostate: techniques, re-sults and potential applications of color Doppler scanning. Radi-ology 1993;186:509-13.
14. Kelly IM, Lees WR, Rickards D. Prostate cancer and the role of color Doppler ultrasound. Radiology 1933;189:153-6.
15. Uemura H, Sano F, Nomiya A, Yamamoto T, Nakamura M, Miyo-shi Y et al. Usefulness of perflubutane microbubble-enhanced
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.

CONVENTIONAL IMAGING AND MULTIPARAMETRIC MR IN THE DIAGNOSIS OF PROSTATE CANCER PANEBIANCO
Vol. 56 - No. 4 THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGING 341
50. Hoeks CM, Schouten MG, Bomers JG, Hoogendoorn SP, Huls-bergen-van de Kaa CA, Hambrock T et al. Three-Tesla magnetic resonance-guided prostate biopsy in men with increased pros-tate-specific antigen and repeated, negative, random, systematic, transrectal ultrasound biopsies: detection of clinically significant prostate cancers. Eur Urol 2012 [Epub ahead of print].
51. Panebianco V, Sciarra A, De Berardinis E, Busetto G, Lisi D, Buonocore V et al. PCA3 Urinary Test Versus 1H-MRS and DCEMR in the Detection of Prostate Cancer Foci in Patients with Biochemical Alterations. Anticancer Res 2011;31:1399-405.
52. Barentsz JO, Richenberg J, Clements R, Choyke P, Verma S, Vil-leirs G et al. ESUR prostate MR guidelines 2012. Eur Radiol 2012 [Epub ahead of print].
53. Kim B, Breau RH, Papadatos D, Fergusson D, Doucette S, Cagi-annos I et al. Diagnostic accuracy of surface coil magnetic reso-nance imaging at 1.5 T for local staging of elevated risk prostate cancer. Can Urol Assoc J 2010;4:257-62.
54. Augustin H, Fritz GA, Ehammer T, Auprich M, Pummer K. Ac-curacy of 3-Tesla magnetic resonance imaging for the staging of prostate cancer in comparison to the Partin tables. Acta Radiol 2009;50:562-9.
55. Labanaris AP, Zugor V, Takriti S, Smiszek R, Engelhard K, Nutzel R et al. The role of conventional and functional endorectal mag-netic resonance imaging in the decision of whether to preserve or resect the neurovascular bundles during radical retropubic prostatectomy. Scand J Urol Nephrol 2009;43:25-31.
56. Brown JA, Rodin DM, Harisinghani M, Dahl DM. Impact of pre-operative endorectal MRI stage classification on neurovascular bundle sparing aggressiveness and the radical prostatectomy positive margin rate. Urol Oncol 2009;27:174-9.
57. Panebianco V, Sciarra A, Osimani M, Lisi D, Ciccariello M, Sal-ciccia S et al. 2D and 3D T2-weighted MR sequences for the assessment of neurovascular bundle changes after nerve-sparing radical retropubic prostatectomy with erectile function correla-tion. Eur Radiol 2009;19:220-9.
58. McClure TD, Margolis DJ, Reiter RE, Sayre JW, Thomas MA, Na-garajan R et al. Use of MR Imaging to Determine Preservation of the Neurovascular Bundles at Robotic-assisted Laparoscopic Prostatectomy. Radiology 2012;262:874-83.
59. Naiki T, Okamura T, Nagata D, Mori Y, Kawai N, Ogawa K et al. Preoperative prediction of neurovascular bundle involvement of localized prostate cancer by combined T2 and diffusion-weight-ed imaging of magnetic resonance imaging, number of posi-tive biopsy cores, and Gleason score. Asian Pac J Cancer Prev 2011;12:909-13.
60. Hövels AM, Heesakkers RA, Adang EM, Jager GJ, Strum S, Hoo-geveen YL et al. The diagnostic accuracy of CT and MRI in the staging of pelvic lymph nodes in patients with prostate cancer: a meta-analysis. Clin Radiol 2008;63:387-95.
61. Ketelsen D, Röthke M, Aschoff P, Merseburger AS, Lichy MP, Re-imold M et al. [Detection of bone metastasis of prostate cancer - comparison of whole-body MRI and bone scintigraphy]. Rofo 2008;180:746-52.
62. Gutzeit A, Doert A, Froehlich JM, Eckhardt BP, Meili A, Scherr P et al. Comparison of diffusion-weighted whole body MRI and skeletal scintigraphy for the detection of bone metastases in patients with prostate or breast carcinoma. Skeletal Radiol 2010;39:333-43.
63. Cirillo S, Petracchini M, Scotti L, Gallo T, Macera A, Bona MC et al. Endorectal magnetic resonance imaging at 1.5 Tesla to assess local recurrence following radical prostatectomy us-ing T2-weighted and contrast-enhanced imaging. Eur Radiol 2009;19:761-9.
64. Sciarra A, Panebianco V, Salciccia S, Osimani M, Lisi D, Ciccari-ello M et al. Role of dynamic contrast-enhanced magnetic reso-nance (MR) imaging and proton MR spectroscopic imaging in the detection of local recurrence after radical prostatectomy for prostate cancer. Eur Urol 2008;54:589-600.
65. Panebianco V, Sciarra A, Lisi D, Galati F, Buonocore V, Catalano
in combination with T2-weighted imaging. J Magn Reson Imag-ing 2010;31:625-31.
35. Cirillo S, Petracchini M, Della Monica P, Gallo T, Tartaglia V, Vestita E et al. Value of endorectal MRI and MRS in patients with elevated prostate-specific antigen levels and previous nega-tive biopsies to localize peripheral zone tumours. Clin Radiol 2008;63:871-9.
36. Moradi M, Salcudean SE, Chang SD, Jones EC, Buchan N, Casey RG et al. Multiparametric MRI maps for detection and grading of dominant prostate tumors. J Magn Reson Imaging 2012;35:1403-13.
37. Villeirs GM, De Meerleer GO, De Visschere PJ, Fonteyne VH, Verbaeys AC, Oosterlinck W. Combined magnetic resonance im-aging and spectroscopy in the assessment of high grade prostate carcinoma in patients with elevated PSA: a single-institution ex-perience of 356 patients. Eur J Radiol 2011;77:340-5.
38. Hambrock T, Somford DM, Huisman HJ, van Oort IM, Witjes JA, Hulsbergen-van de Kaa CA et al. Relationship between apparent diffusion coefficients at 3.0-T MR imaging and Gleason grade in peripheral zone prostate cancer. Radiology 2011; 259:453-61.
39. Yoshizako T, Wada A, Hayashi T, Uchida K, Sumura M, Uchida N et al. Usefulness of diffusion-weighted imaging and dynamic contrast-enhanced magnetic resonance imaging in the diagnosis of prostate transition-zone cancer. Acta Radiol 2008;49:1207-13.
40. Delongchamps NB, Beuvon F, Eiss D, Flam T, Muradyan N, Zer-bib M et al. Multiparametric MRI is helpful to predict tumor fo-cality, stage, and size in patients diagnosed with unilateral low-risk prostate cancer. Prostate Cancer Prostatic Dis 2011;14:232-7.
41. Viswanath SE, Bloch NB, Chappelow JC, Toth R, Rofsky NM, Genega EM et al. Central gland and peripheral zone prostate tu-mors have significantly different quantitative imaging signatures on 3 tesla endorectal, in vivo T2-weighted MR imagery. J Magn Reson Imaging 2012 [Epub ahead of print].
42. Vargas HA, Akin O, Franiel T, Goldman DA, Udo K, Touijer KA et al. Normal Central Zone of the Prostate and Central Zone In-volvement by Prostate Cancer: Clinical and MR Imaging Implica-tions. Radiology 2012;262:894-902.
43. De la Rosette JJ, Wink MH, Mamoulakis C, Wondergem N, ten Kate FJ, Zwinderman K et al. Optimizing prostate cancer detec-tion: 8 versus 12-core biopsy protocol. J Urol 2009;182:1329-36.
44. Sciarra A, Panebianco V, Ciccariello M, Salciccia S, Cattarino S, Lisi D et al. Value of magnetic resonance spectroscopy imaging and dynamic contrast-enhanced imaging for detecting prostate cancer foci in men with prior negative biopsy. Clin Cancer Res 2010;16:1875-83.
45. Aydn H, Kzlgöz V, Tatar IG, Damar C, Ugan AR, Paker I et al. Detection of prostate cancer with magnetic resonance imaging: optimization of T1-weighted, T2-weighted, dynamic-enhanced T1-weighted, diffusion-weighted imaging apparent diffusion co-efficient mapping sequences and MR spectroscopy, correlated with biopsy and histopathological findings. J Comput Assist To-mogr 2012;36:30-45.
46. Puech P, Potiron E, Lemaitre L, Leroy X, Haber GP, Crouzet S et al. Dynamic contrast-enhanced-magnetic resonance imaging evaluation of intraprostatic prostate cancer: correlation with rad-ical prostatectomy specimens. Urology 2009;74:1094-9.
47. Zhang J, Hricak H, Shukla-Dave A, Akin O, Ishill NM, Carlino LJ et al. Clinical stage T1c prostate cancer: evaluation with en-dorectal MR imaging and MR spectroscopic imaging. Radiology 2009;253:425-34.
48. Weinreb JC, Blume JD, Coakley FV, Wheeler TM, Cormack JB, Sotto CK et al. Prostate cancer: sextant localization at MR imag-ing and MR spectroscopic imaging before prostatectomy results of ACRIN prospective multi-institutional clinicopathologic study. Radiology 2009;251:122-33.
49. Katahira K, Takahara T, Kwee TC, Oda S, Suzuki Y, Morishita S et al. Ultra-high-b-value diffusion-weighted MR imaging for the detection of prostate cancer: evaluation in 201 cases with histo-pathological correlation. Eur Radiol 2011;21:188-96.
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.
PANEBIANCO CONVENTIONAL IMAGING AND MULTIPARAMETRIC MR IN THE DIAGNOSIS OF PROSTATE CANCER
342 THE QUARTERLY JOURNAL OF NUCLEAR MEDICINE AND MOLECULAR IMAGING August 2012
son Grade in Peripheral Zone Prostate Cancer. Radiology 2011;259:453-61.
Funding.—No fund was received for this work from any of the fol-lowing organizations: National Institutes of Health (NIH); Wellcome Trust; Howard Hughes Medical Institute (HHMI); and other(s).
Conflicts of interest.—None.
C et al. Prostate cancer: 1HMRS-DCEMR at 3T versus [(18)F]choline PET/CT in the detection of local prostate cancer recur-rence in men with biochemical progression after radical retro-pubic prostatectomy (RRP). Eur J Radiol 2011 [Epub ahead of print].
66. Hambrock T, Somford DM, Huisman HJ, van Oort IM, Witjes JA, Hulsbergen-van de Kaa CA et al. Relationship between Ap-parent Diffusion Coefficients at 3.0-T MR Imaging and Glea-
MIN
ERVA M
EDICA
COPYRIGHT®
Thi
s do
cum
ent
is p
rote
cted
by
inte
rnat
iona
l cop
yrig
ht la
ws.
No
addi
tiona
l rep
rodu
ctio
n is
aut
horiz
ed.I
t is
per
mitt
ed fo
r pe
rson
al u
se t
o do
wnl
oad
and
save
onl
y on
e fil
e an
d pr
int
only
one
cop
y of
thi
s A
rtic
le.I
t is
not
per
mitt
ed t
o m
ake
addi
tiona
l cop
ies
(eith
er s
pora
dica
lly o
r sy
stem
atic
ally
, ei
ther
prin
ted
or e
lect
roni
c) o
f th
e A
rtic
le fo
r an
y pu
rpos
e.It
is n
ot p
erm
itted
to
dist
ribut
e th
e el
ectr
onic
cop
y of
the
art
icle
thr
ough
onl
ine
inte
rnet
and
/or
intr
anet
file
sha
ring
syst
ems,
ele
ctro
nic
mai
ling
or a
ny o
ther
mea
ns w
hich
may
allo
w a
cces
s to
the
Art
icle
.The
use
of
all o
r an
y pa
rt o
f th
e A
rtic
le fo
r an
y C
omm
erci
al U
se is
not
per
mitt
ed.T
he c
reat
ion
of d
eriv
ativ
e w
orks
fro
m t
he A
rtic
le is
not
per
mitt
ed.T
he p
rodu
ctio
n of
rep
rints
for
pers
onal
or
com
mer
cial
use
isno
t pe
rmitt
ed.I
t is
not
per
mitt
ed t
o re
mov
e, c
over
, ov
erla
y, o
bscu
re,
bloc
k, o
r ch
ange
any
cop
yrig
ht n
otic
es o
r te
rms
of u
se w
hich
the
Pub
lishe
r m
ay p
ost
on t
he A
rtic
le.I
t is
not
per
mitt
ed t
o fr
ame
or u
se f
ram
ing
tech
niqu
es t
o en
clos
e an
y tr
adem
ark,
logo
,or
oth
er p
ropr
ieta
ry in
form
atio
n of
the
Pub
lishe
r.




















