Multimodal sensory testing of the rectum and rectosigmoid: development and reproducibility of a new...
12
PDFlib PLOP: PDF Linearization, Optimization, Protection Page inserted by evaluation version www.pdflib.com – [email protected]
Transcript of Multimodal sensory testing of the rectum and rectosigmoid: development and reproducibility of a new...

PDFlib PLOP: PDF Linearization, Optimization, Protection
Page inserted by evaluation versionwww.pdflib.com – [email protected]

Multimodal sensory testing of the rectum and
rectosigmoid: development and reproducibility
of a new method
C. BROCK,* T. D. NISSEN,� F. H. GRAVESEN,* J. B. FRØKJÆR,� H. OMAR,§ J. GALE,– H. GREGERSEN,*,**
O. SVENDSEN� & A. M. DREWES*,**
*Center for Visceral Biomechanics and Pain, Department of Gastroenterology, Aalborg Hospital, Aalborg, Denmark
�Faculty of Life Sciences, University of Copenhagen, Copenhagen, Denmark
�Department of Radiology, Aalborg Hospital, Aalborg, Denmark
§Department of Surgical Gastroenterology, Aalborg Hospital, Aalborg, Denmark
–Pfizer, Global Research & Development, Sandwich, Kent, UK
**Center for Sensory-Motor Interaction, Department of Health Science and Technology, Aalborg University, Aalborg, Denmark
Abstract Evaluation of rectal and rectosigmoid sen-
sation is important in basic, clinical and pharmaco-
logical studies. New methods to evoke and assess
multimodal (electrical, thermal and mechanical)
experimental pain of the upper gut activate distinct
pathways and mimics clinical pain. The aims of the
current study were to characterize the sensory re-
sponse and reproducibility to multimodal stimulation
of rectum and the rectosigmoid. A multimodal rectal
probe was developed. Mucosal electrostimulation was
delivered at the recto-sigmoid junction. In Rectum,
impedance planimetry was used for measurement of
cross-sectional area (CSA) during distension. Circu-
lation of water within the bag at either 4 or 60 �C was
applied for thermal stimulation. The method was
tested in 12 healthy volunteers (six men mean age
32 years) on two subsequent days. Mechanical and
sensory responses and referred pain areas were
assessed. Stimulation with electrical, thermal and
mechanical modalities resulted in different sensory
perceptions. The relationship between stimulus
intensity and sensory response was linear for all
modalities. Sensory response to different modalities
did not differ between investigation days (all P-val-
ues > 0.1). Approximately 75% of subjects felt referred
pain in distinct skin locations. Between-days repro-
ducibility was good for all modalities [intra-class
correlation (ICC) ‡0.6]. At sensory threshold, CSA
showed best reproducibility (ICC ‡ 0.9). At pain
detection threshold stretch ratio, CSA and electrosti-
mulation showed best reproducibility (ICC = 1.0; 0.9;
0.9). The present model was easily implemented,
robust and showed good reproducibility. It can be
used to study pathophysiology or pharmacological
interventions in healthy controls and in patients with
diseases involving the distal hindgut.
Keywords impedance planimetry, multimodal,
rectosigmoid, rectum, reproducibility, sensation,
visceral pain.
INTRODUCTION
Abdominal pain is among common symptoms respon-
sible for patients seeking gastroenterological consulta-
tions.1 Pathophysiology and mechanisms behind pain
conditions are poorly understood. This lack of know-
ledge makes treatment of abdominal pain difficult and
suboptimal. One way to improve the treatment of
abdominal pain disorders is to increase our under-
standing behind these symptoms, achieved through
standardized experimental human pain models. The
primary advantages of such models are controlled
stimuli, repeatedly and modulated delivery and assess-
ing the response with psychophysical and/or neuro-
physiological methods. Hence, confounding factors
Address for correspondence
Professor Asbjørn Mohr Drewes MD, DMSc, PhD,Center for Visceral Biomechanics and Pain,Department of Gastroenterology, Aalborg Hospital,DK-9100 Aalborg, Denmark.Tel: +45 9932 1111; fax: +45 9932 6507;e-mail: [email protected]: 29 October 2007Accepted for publication: 27 February 2008
Neurogastroenterol Motil (2008) 20, 908–918 doi: 10.1111/j.1365-2982.2008.01126.x
� 2008 The AuthorsJournal compilation � 2008 Blackwell Publishing Ltd908

such as those underlying clinical pain can to a large
extent be controlled and/or avoided.2
As pain is a multidimensional perception, it is
obvious that reaction to one stimulus only represents
a limited fraction of the entire pain experience. Com-
bining different stimulation methods and sensory
assessment will mimic clinical situations and provide
comprehensive and differentiated information of the
visceral nociceptive system.3,4 The great advantage of a
multimodal pain model is activation of various recep-
tor types involving different nerves, pathways and pain
mechanisms due to stimulus modalities such as elec-
trical, mechanical and thermal stimuli.2 Somatic
multimodal experimental pain models have shown
their value in drug testing.5 However, due to limited
accessibility of the gastrointestinal (GI) tract, experi-
mental visceral pain testing is more challenging.
Recently, we developed a multimodal oesophageal
probe that has proven its value in basic science,
clinical and pharmacological experiments.6 Altered
rectal compliance and/or anorectal sensations found
in functional disorders such as irritable bowel syn-
drome (IBS)7,8 reflects enhanced rectal sensitivity. On
the contrary, rectal sensation may be reduced in
constipation.9 As rectum is easily accessible and
relevant to study to explore diseases of the large
intestine, a multimodal approach to this organ is
highly warranted.
The aims were: (i) developing a multimodal rectal
probe combining mechanical, electrical and thermal
stimulation and (ii) testing reproducibility of sensory
assessment.
MATERIALS AND METHODS
Subjects
Twelve healthy volunteers (six males mean age
32 ± 10 years) were recruited from hospital and uni-
versity staff. None of them received medications or
suffered from any GI symptoms, diabetes or other pain-
related diseases. All subjects gave informed consent
prior to the experiments, carried out at the Center of
Visceral Biomechanics and Pain at Aalborg Hospital,
Denmark. Obtained Ethical Approval (VN 2003/
120mch) conforms to the Declaration of Helsinki.
Sensory assessment
Prior to the study, subjects were instructed to use the
0–10 electronic modified visual analogue scale (VAS),
where 0 = no perception; 1 = vague perception of mild
sensation (ST); 2 = definite perception of mild sensa-
tion; 3 = vague perception of moderate sensation;
4 = definite perception of moderate perception. For
painful sensations, the subjects used the scale from 5
to 10 anchored at 5 = pain detection threshold (PDT);
6 = slight pain; 7 = moderate pain; 8 = medium pain
intensity; 9 = intense pain and 10 = unbearable pain.
The scale has been described in details previously,2
proving to be robust and discriminating rectal sensa-
tions with high accuracy in basic and clinical stud-
ies.4,10–12 Pain detection threshold was chosen as the
endpoint during stimulation. Referred somatic pain
area corresponding to maximal sensory intensity was
drawn on transparent paper and digitized for measure-
ments (Trust, 1200 wireless tablet; Trust International
BV, Dordrecht, the Netherlands).
Stimulation device
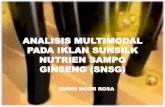
A 40-cm long, eight lumen custom-designed multi-
modal probe (Fig. 1) (GMC ApS, Hornslet, Denmark),
6.2 mm in outer diameter including a non-conducting,
non-compliant 30-lm thick polyestherurethane bag for
mechanical and thermal stimulation was build. The
70-mm long bag was maximally inflated [240 mL and
cross-sectional area (CSA) of 4478 mm2] to a diameter
of 76 mm and a circumference of 237 mm. This bag
size was chosen based on knowledge from pilot studies.
Electrical stimulation Two stainless steel electrodes
mounted at the tip with an inter-electrode distance of
2 mm were connected to a computer-controlled con-
stant-current stimulator (IES 230; JNI Biomedical ApS,
Klarup, Denmark). Electrical stimuli were applied
either as �single stimulus� consisting of five 1-ms
square-pulses applied at 200 Hz or as �repeated stimuli�consisting of a train of five �single stimulus� applied at
2 Hz (Fig. 1).
Thermal stimulation Recirculation of 0.009% saline at
60 or 4 �C through the bag served as thermal stimula-
tion. Water baths (Julabo VWR 5; Julabo, Labortechnik
GMBH, Seelbach, Germany) controlled temperature in
the closed circuit. A peristaltic pump (Type 111; Ole
Dich Instrumentmakers, Hvidovre, Denmark) circu-
lated with a flow rate of 150 mL min)1. The distal end
of the withdrawal lumen contained a temperature
sensor (Buhl & Bønsøe AS, Virum, Denmark). Thermal
stimulus was computed as the area under the time–
temperature curve (AUC), corrected for the baseline
temperature.13
Mechanical stimulation A pressure lumen was
continuously perfused with 0.1 mL min)1 0.009%
Volume 20, Number 8, August 2008 Multimodal rectal and rectosigmoid sensations
� 2008 The AuthorsJournal compilation � 2008 Blackwell Publishing Ltd 909
saline by a low-compliance perfusion system attached
to an external pressure transducer (Baxter, Deerfield,
IL, USA). Rectal mechanical stimulation based
exclusively on volume–pressure measurements14 can
result in inaccurate radius calculation during
distension. Hence, impedance planimetry (IP) was
included.10 A six-electrode impedance measuring
system was used for two luminal CSA inside the bag.
This IP system consists of two outer stainless steel
electrodes for excitation placed with an inter-
electrode distance of 46 mm connected to a constant
current generator in the IP box (GMC Aps). Two
pairs of detection electrodes, each consisting of two
electrodes with an inter-electrode distance of 2 mm,
were placed midway between the excitation elec-
trodes and connected to an impedance detection unit
(Fig. 1). Thus, CSA was recorded as the electrical
impedance of 37 �C 0.009% saline inside the bag.15
Due to the complex geometry,16 two CSA measure-
ments were used (Fig. 2) and based on these an
average was calculated. Assuming circularity the
stretch ratio was calculated at different sensory
scores relative to the radius r at the sensory thres-
hold = VAS1 and VASx (0, 1, 2, 3, 4, 5).
Figure 1 Schematic illustration of the multimodal rectal probe designed for electrical, thermal (heat and cold) and mechanicalstimulation (A and B). The protocol (C) illustrates the stimulation order that was performed until pain detection threshold (PDT).Electrical stimuli (single and repeated) were increased in steps of 0.5 mA. Thermal stimulation, either heat or cold was performedby circulating warm or cold water in the bag. After three preconditioning mechanical stimulation, two distensions (without andwith administration of 20 mg butylscopolamine intravenously) were given until the pain threshold [corresponding to 5 on thevisual analog scale (VAS)] was reached.
C. Brock et al. Neurogastroenterology and Motility
� 2008 The AuthorsJournal compilation � 2008 Blackwell Publishing Ltd910

Stretch ratio ¼ rVASx
rVAS1¼
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi
CSAVASx
pffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi
CSAVAS1
p :
Bag temperature, pressure and CSA were amplified,
analogue-to-digital converted and analysed (National
Instruments; Labview 6.1, Austin, TX, USA). Due to
earlier experiments,16 rectum was considered thin
walled (wall thickness to radius ratio <0.1) and thus
circumferential tension T was calculated based on
Laplace�s law:
T ¼ Dpri;
where Dp denotes the bag pressure corrected from the
baseline pressure, assumed equal to the transmural
pressure, and ri is the inner radius.
Study protocol
Each volunteer was studied 2 days separated by a
minimum of 1 week (mean 19 ± 10 days). Thirty
minutes prior to investigation a docosat and sorbitol
enema (Klyx�; Ferring, Copenhagen, Denmark) was
administered. Subjects lie on their right side while a
lubricated anoscope (Cat. No. E-03. 19. 925; Heine
Optotechnik, Herrsching, Germany) was placed in
the anal canal, through which the rectal probe was
advanced until resistance was felt at the recto-
sigmoid junction.
Stimulation order was electrical, thermal and
mechanical. As the anal canal is sensitive to thermal
stimulation, the insulating anoscope was manually
held during thermal stimulation.
Electrical stimulations The probe was positioned at
the recto-sigmoid junction at 17.7 ± 1.4 cm from the
anal verge. Impedance across electrodes below 3 kW(mean 1.5 ± 0.6 kX) ensured good mucosal contact.
During single electrostimulation intensity was blin-
ded, but gradually increased in steps of 0.5 mA, con-
taining intermittent sham stimuli with same or lower
intensity as the previous. Intensity was increased until
PDT was reached. First trial served to familiarize the
subject with the feeling and sensory evaluation, and
1 min later a second trial was performed.2 During
repeated electrostimulation, subjects were instructed
to evaluate the last of the stimuli, due to central
integration of repeated stimulations (reflecting the
initial phase of wind-up seen in animal experiments).17
At PDT, referred pain areas were drawn.
Thermal stimulation Prior to thermal and mechanical
stimulation withdrawal of the probe to a 13-cm fix-
point at the anal verge ensured bag position in the
rectum. Hence, the distance from lower bag limit to
outer sphincter was 5 cm. To ensure sufficient muco-
sal contact 60 mL of 37 �C 0.009% saline was initially
0
1
2
3
4
5
VA
S [–
]
0
1
2
3
4
5
VA
S [–
]
0
1
2
3
4
5
VA
S [–
]
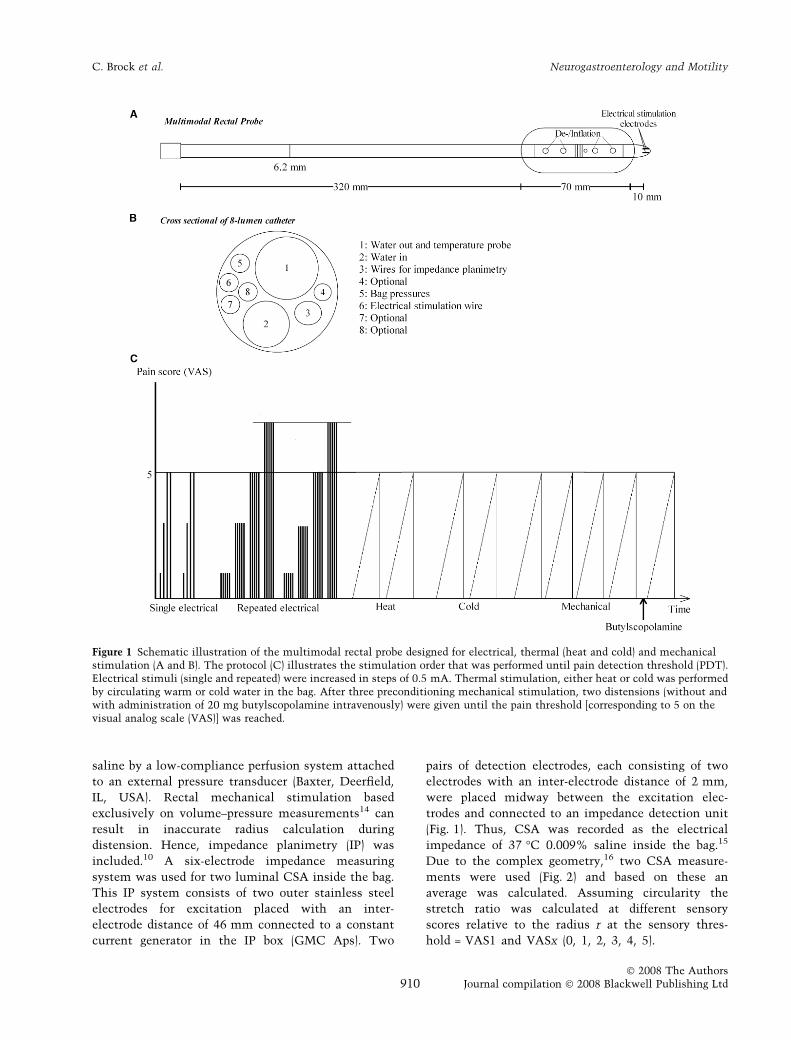
Figure 2 The top: On-line data acquisition including two-channel impedance planimetry measurement in the rectum. Disten-sion was performed until pain detection threshold that was reached after 120 s, corresponding to 240 mL. At this point, thedeflation of the bag starts with same perfusion rate as the inflation. The CSA curves show a non-linear pattern, which is simi-lar to the sensory score on the visual analog scale (VAS). The sensory score remains on a plateau while CSA does not increasedue to the filling of the bag, whereas the pressure curve increases. Bag distension induces relaxation distally as a result of aninhibitory reflex, hence distributing the volume distally. When the bag is filled in a more radial direction, the CSA and thesensory score is increased. The bottom: On-line data acquisition demonstrating the thermal stimulation with heat and cold.
Volume 20, Number 8, August 2008 Multimodal rectal and rectosigmoid sensations
� 2008 The AuthorsJournal compilation � 2008 Blackwell Publishing Ltd 911

filled in the bag. None reported more than a vague
perception (VAS = 1) to this mechanical filling. Then
re-circulation of 60 �C (heat) or 4 �C (cold) saline in the
bag was initiated, until PDT was reached or for a
maximum of 120 s. The bag was emptied and the
procedure was repeated after 1 min. Subjects drew re-
ferred pain areas. Details in temperature rise and de-
cline is shown in Fig. 4.
Mechanical stimulation Three distensions till PDT
was performed with 1-min interval to precondition the
tissue and to train subject in sensory assessment.18,19
After this, a single distension was performed, and the
subjects were asked to draw the referred pain area.
Distension stopped either at PDT or at the maximum
capacity of the bag and then the bag was emptied at
same rate as the inflation. Five minutes after these
distensions, a single distension was performed during
administration of 20 mg butylscopolamine (Busco-
pan�; Boehringer Ingelheim, Ingelheim, Germany)
intravenously.4 This antimuscarinic drug blocks the
cholinerge-mediated contractions. Subjects drew the
referred pain areas.
Statistics Data are given as mean ± SEM, using the
software package SigmaStat ver. 3.0 (SPSS Inc.,
Chicago, IL, USA). Reproducibility was evaluated as
follows:
1 Two-way analysis of variance for repeated mea-
surements (RM-ANOVA) was applied for assessment of
variation in sensory score over time in the total data
material. P-values < 0.05 indicate significant changes
over time.
2 Intra-class correlation (ICC) was calculated for
measurement of intra-individual variance. Intra-class
correlation evaluates each subject�s ability to reproduce
a response between days of study and illustrates the
difference between a subject�s score at repeated exper-
imental sessions. The ICC was calculated as:
ICC ¼ 1� rwithin
rtotal;
where rwithin is the variance within individuals and
rtotal is the sum of variance within individuals and
between the repetitions of the pain test.6 The param-
eter ranges from zero to one, with values closest to one
indicating the highest reproducibility. Previously
acceptable levels of ICC has been set to ‡0.6.6,20,21
3 Spearman�s rank-order coefficient was applied for
the assessment of the relationship between the stim-
ulus intensity at PDT and the referred pain area.
RESULTS
All subjects completed without adverse events. Gender
specific analyses were not performed. Study duration
was 72 (range 51–88) min. Technical problems
excluded electrostimulation in one subject and a bag
leaked in another subject. As experiments were
conducted it became apparent, that not all subjects
reached PDT to cold and mechanical stimulations.
Consequently, calculations at the higher pain scores
were based on fewer observations. The overall repro-
ducibility of the method is illustrated in Tables 1 and
2. The modality-specific findings were as follows.
Electrical stimulation "Repeated stimuli"
0
1
2
3
4
5
6
0 5 10 15 20 Electrical current (mA)
Pai
n s
core
(V
AS
)
1st day 2nd day
Electrical stimulation "Single stimulus"
0
1
2
3
4
5
6
0 5 10 15 20 Electrical current (mA)
Pai
n s
core
(V
AS
)
1st day 2nd day
Figure 3 Between study days reproducibility of single(A) and repeated (B) rectal electrical stimulations. Error barsrepresent the standard error of mean (SEM).
C. Brock et al. Neurogastroenterology and Motility
� 2008 The AuthorsJournal compilation � 2008 Blackwell Publishing Ltd912

Electrical stimuli
Single stimulation Sensory detection threshold was
reached at 8.1 ± 1.6 and 7.7 ± 2.0 mA first and second
day, respectively, and PDT was reached at 15.0 ± 2.4
and 15.3 ± 2.5 mA first and second day. There were no
differences between days (F = 0.1, P = 0.8). All subjects
reported a pricking pain. While 71% experienced
referred pain with a precise location, 29% had diffi-
culties in that (Table 3). Intra-class correlation indi-
cated highly reproducibility and consistent individual
pain score between days (see Table 1). Fig. 3 shows
average current corresponding to the different sensory
levels.
Repeated electrical Sensory detection threshold was
reached at 6.9 ± 1.6 and 6.1 ± 1.6 mA on first and second
day. Pain detection threshold was reached at 12.4 ± 2.1
and 12.0 ± 2.6 mA on first and second day. There were
no differences between days (F = 0.01, P = 0.8). Pain was
reported as pricking. Referred pain with a precise loca-
tion was felt by 70% of subjects (Table3). Intra-class
correlation values indicated highly and consistent indi-
vidual pain score between days (see Table 1).
Thermal stimuli
All subjects felt warmth around the bag during heat
stimulation. Stimulation temperatures at ST were
A B
Figure 4 Between study days reproducibility of cold (A) and heat (B) rectal thermal stimulation. The intensity of the thermalstimulation is calculated as the area under the time–temperature curve corrected for the baseline temperature. Error bars representthe standard error of mean (SEM). Temperature rise was approximately 4 s per 1 �C, and can be regarded as a linear increase whiletemperature decline was approximately 2 s per 1 �C initially, and then approximately 7 s per 1 �C from 15 �C downward.
Table 1 Between study days reproducibility of multimodal rectal stimulations
Modality
Two-way RM ANOVA
ST ICC PDT ICCF P-value
Single electrical stimulation 0.1 0.8 0.7 0.9Repeated electrical stimulation 0.01 0.8 0.8 0.9Heat 0.2 0.7 0.6 0.7Cold 0.3 0.6 0.5 0.9Pressure 0.08 0.8 0.9 0.8Pressure with butylscopolamine 0.8 0.4 0.5 0.6Volume <0.001 0.98 0.7 0.6Volume with butylscopolamine 0.3 0.6 0.9 0.8Tension 0.01 0.9 0.6 0.8Tension with butylscopolamine 1.2 0.3 0.6 0.5Cross sectional area 0.7 0.4 0.9 0.9Cross sectional area with butylscopolamine 1.8 0.2 0.9 0.8Stretch ratio 0.6 0.4 na* 1.0Stretch ratio with butylscopolamine 1.4 0.2 na* 1.0
Intra-class correlation coefficient (ICC) values are calculated at both sensory detection threshold (ST) and pain detection threshold(PDT) for the different modalities. ICC > 0.6 indicates acceptable reproducibility. RM ANOVA, repeated measures analysis ofvariance. *Stretch ratio cannot be calculated at ST, due to its definition.16
Volume 20, Number 8, August 2008 Multimodal rectal and rectosigmoid sensations
� 2008 The AuthorsJournal compilation � 2008 Blackwell Publishing Ltd 913

40.9 ± 0.8 and 43.1 ± 0.8 �C on first and second day.
Pain detection threshold was reached at 47.1 ± 1.4 and
48.9 ± 1.4 �C on first and second day. Heat stimulus,
expressed as area under curve (AUC) did not differ
significantly between study days (59 ± 21 and
74 ± 21 �C s at ST and 311 ± 91 and 351 ± 78 �C s at
PDT (F = 0.2, P = 0.7). Seventy-one per cent of the
subjects felt referred pain at a precise somatic location
(Table 3). Intra-class correlation values indicated a
consistent individual pain score between days, see
Table 1.
Bag temperatures during cold stimulation were
21.2 ± 1.4 and 16.4 ± 1.2 �C at ST on first and second
day. At PDT, they were 12.0 ± 3.2 and 11.0 ± 2.2 �C on
the 2 days. Cold stimulus expressed as AUC did not
differ between study days (ST: )227 ± 52 and
)239 ± 43 �C s; and PDT: )1051 ± 229 and
)1103 ± 263 �C s (F = 0.3, P = 0.6). Referred pain area
was felt in a precise somatic location in 75% of the
subjects (Table 3). Intra-class correlation values indi-
cated a good consistent individual pain score between
days (see Table 1). Fig. 4 shows the average AUC
corresponding to the different sensory levels.
Mechanical stimuli
During mechanical stimulation, no differences
between days were observed. Bag pressure was 2.2 ±
0.7 and 1.6 ± 0.3 kPa at ST on first and second day. At
PDT, bag pressure was 5.5 ± 4.0 and 4.9 ± 3.1 kPa
(F = 0.1, P = 0.8). Volume was 60 ± 13 and 67 ±
12 mL at ST on first and second day compared to
173 ± 56 and 174 ± 45 mL at PDT (F < 0.001, P = 0.98).
Tension was 42 ± 17 and 38 ± 12 Pa m at ST compared
to 157 ± 119 and 142 ± 82 Pa m at PDT (F = 0.01,
P = 0.9). One leaking bag and technical problems in
two subjects� left CSA calculation based upon nine
subjects. Intra-class correlation values indicated
stretch ratio at PDT and CSA at both ST and PDT as
excellent reproducible parameters between days (see
Table 1). Referred pain was felt in a precise location in
56% of the subjects (Table 3).
During mechanical stimulation followed by butyl-
scopolamine treatment, only 7 (78%) and 3 (33%)
subjects reached pain threshold the first and second
study day. Thus, ICC for CSA and stretch ratio
following butylscopolamine administration was calcu-
lated at a sensory score of 4. Administration of
butylscopolamine did not affect the between-day
response (CSA: F = 1.8, P = 0.2; stretch ratio: F = 1.4,
P = 0.2). Intra-class correlation values showed CSA and
volume at ST and stretch at PDT as the most repro-
ducible parameters between days (see Table 1).
Referred pain was felt in a precise location in 56% of
the subjects (Table 3). Fig. 5 shows the relationship
between sensory scores, CSA and stretch ratio. Fifty-
Table 2 Reproducibility expressed as ICC values, of the mean referred pain area (expressed in cm2) to each of the stimulusmodalities
Modality Mean ± SE – 1st day Mean ± SE – 2nd day P-value ICC
Electrical – single 8.6 ± 5.0 2.8 ± 1.3 0.4 0.5Electrical – repeated 8.3 ± 5.0 3.5 ± 1.3 1.0 0.5Heat 54.3 ± 26.8 17.7 ± 8.7 0.1 0.6Cold 20.2 ± 7.8 16.0 ± 6.1 0.8 0.7Mechanical 22.5 ± 7.4 18.4 ± 9.4 0.1 0.6Mechanical with butylscopolamine 20.8 ± 7.3 9.3 ± 5.1 0.1 0.5
P-values are calculated using repeated one-way ANOVA on ranks. Intra-class correlation (ICC) >0.6 indicates good reproducibility.
Table 3 Referred pain areas pointed to three different locations, and a proportion felt no referred pain
ModalityNo referredpain (%)
Referred painto the ventralabdominal wall (%)
Referred pain to theanal region incl.perineum (%)
Referred painto the glutealregion (%)
Electrical – single 29 13 25 33Electrical – repeated 30 17 13 40Heat 29 30 22 19Cold 25 25 42 8Mechanical 44 22 26 8Mechanical with butylscopolamine 48 14 29 9
C. Brock et al. Neurogastroenterology and Motility
� 2008 The AuthorsJournal compilation � 2008 Blackwell Publishing Ltd914

two per cent of subjects felt referred pain with a precise
location.
Referred pain areas
For all modalities, referred pain area did not differ
significantly between study days (all P-values > 0.1,
see Table 2). Considering the challenge in drawing
referred pain area to rectal stimulations, the ICC
between days was acceptable (see Table 1). Stimulation
intensity at PDT and referred pain area showed no
significant correlations (qelectrical = )0.084, P = 0.70;
qheat = 0.019, P = 0.60; qcold = 0.318, P = 0.23;
qmechanical = 0.016, P = 0.95).
Referred pain area did not project to a specific
dermatome, but projected to three different loca-
tions involving different dermatomes as listed in
Table 3.
DISCUSSION
A novel multimodal rectal and rectosigmoid sensory
approach was developed and tested in 12 healthy
subjects. Reproducibility was tested on two different
days at ST and PDT. We found no differences in
sensory response between study days for any of the
applied modalities: Electrical, thermal (heat and cold),
mechanical and corresponding referred pain areas.
With respect to the intra-individual variability, the
most reproducible stimuli were electrical stimulation
and mechanical stimulation in terms of stretch ratio.
Sensory assessment
Under normal circumstances, rectal stimulation evokes
numerous sensations. These includes filling and non-
painful urge to defecate at low distensions. As defor-
A
B
Figure 5 Reproducibility of mechani-cal stimulation of the rectumillustrated as sensory response vscross-sectional area (CSA) (A) andcircumferential stretch ratio (B). Theerror bars represent the standard errorof mean (SEM).
Volume 20, Number 8, August 2008 Multimodal rectal and rectosigmoid sensations
� 2008 The AuthorsJournal compilation � 2008 Blackwell Publishing Ltd 915

mation increases involving wall tension, stress and
strain, the result is an unpleasant and painful urge to
defecate. Previously, we have used a more detailed
qualitative sensory assessment.10 However, to simplify
the sensory rating in this comprehensive study, we only
used an intensity measure. This measurement has
previously been valid and reproducible in studies of
rectum and sigmoid colon in health and dis-
ease.3,5,10,13,22 The PDT showed the most robust and
reliable measure, however, sensory thresholds were also
acceptable. A quantitative description of the sensations
using for instance the sensations to air, urge to defecate
and pain23 or the McGill Pain Questionnaire24 was not
used, but should probably be included in future designs.
Positioning the probe
Previous experiments using a rectoscope have shown
that when a probe made in the current material is
advanced up along the rectal wall it meets resistance at
the recto-sigmoid junction where the sigmoid typically
bends.25 Therefore, we defined the recto-sigmoid junc-
tion as the place where the probe met resistance when
advanced smoothly through most of the rectum,
reaching the rectosigmoid or the proximal parts of
the rectum. Functionally, this does not matter as the
procedure was chosen to avoid electrical stimulation of
the lower rectum with its complex nerve innervations
and functions, and nearby organs.
Electrical stimulation
Different probe designs include easily mucosal electro-
stimulation.2 The main disadvantage is the non-phys-
iological stimulus and the lack of specificity of nerve
fibre stimulation, bypassing receptors and depolarizing
free nerve-endings directly.17,26 However, the direct
effect may also be advantageous as central pain path-
ways can be studied directly.26 As electrostimulation is
not restricted to the gut wall, somatic nerves and tissue
in close vicinity may also be activated.27,28
The ICC value at PDT of 0.9 shows highly repro-
ducibility, in accordance with other studies, where
reproducibility of electrical responses was tested in
oesophagus6 and rectum.20
Thermal stimulation
Thermo-sensitive receptors in the GI tract have been
demonstrated in animals29,30 and in all segments of the
human GI tract.6,11,22,26,27 However, the distribution of
receptors throughout the GI tract is variable. Thermal
stimulation in the rectum should – unlike the oesoph-
agus that may be in regular contact with hot or cold
foodstuff – be regarded as non-physiological. The dense
innervations of the anal canal respond to very small
temperature changes, compared to rectum where
thermo-sensitive afferents are sparse.31,32 Mucosal
thermoreceptors are easily stimulated by re-circulating
heated or cooled water through a rectal bag,2,2 and
similar designs have been used in several studies of the
oesophagus.3,6 All subjects reached PDT during heat
stimulation. The current temperature rise can be
regarded as linear, but both heat and cold stimulus
has been calculated as AUC. We are developing an
improved method for thermal stimulation, where the
investigator will be able to control the rate of temper-
ature change in the bag (A. E. Olesen, F. H. Gravesen,
C. Staahl, P. Kunwald, A. M. Drewes, H. Gregersen,
unpublished data). Recently, a rectal thermal probe
was designed33 based on a Peltier device heater. It
allows control of the temperature and location and
avoids heat stimulation of the anal canal, but a
disadvantage is the small area stimulated, especially
if the density of thermosensitive mucosal afferents is
not equally distributed.
During cold stimulation, nine of 12 reached pain
threshold. An explanation to this finding could be
differences in receptor types responding to heat and
cold. Stimulation temperatures above 43 �C and
below 15 �C result in a feeling of pain,34 which
corresponds with our findings. The temperature fall
during stimulation is non-linear, but even though
temperature drop below 15 �C takes approximately
7 s per 1 �C, a stimulation period of 120 s should
ensure stimulation in the painful range. The specific
heat-responsive TRPV1 receptors exhibiting thermal
activation threshold for temperatures above 43 �Chave been shown in primary sensory rectal neu-
rons.35 On contrary, information regarding specific
cold receptors such as the TRPA1 in the rectum is
sparse. Nine (75%) subjects reached pain threshold
during cold stimulation, suggesting activation of cold
receptors,30 the other three subjects tolerated cold
stimulation in 120 s, with temperatures as low as
9 �C. These findings may suggest that cold stimula-
tion is not as consistent as for instance heat stim-
ulation, but future studies should investigate this
thoroughly.
Mechanical stimulation
Traditionally, mechanical rectal sensitivity has mainly
been addressed using devices such as the �Barostat�.Advantages are its relatively low cost, reliability and
easiness to use.2,12 However, it has some obvious
C. Brock et al. Neurogastroenterology and Motility
� 2008 The AuthorsJournal compilation � 2008 Blackwell Publishing Ltd916

limitations. We have previously shown that rectum
has a complex geometry during distension leading to
an invalid estimation of the rectal radius and hence
erroneous computation of wall tension, stress and
strain.16 Any inflated bag tends to elongate in the
longitudinal direction.15 As rectum is not a cylindrical
or spherical organ, but more likely should be consid-
ered as an irregular cylinder, pressure–volume mea-
surements cannot be used to determine biomechanical
properties such as tension and strain. Based on pilots
prior to this study, we chose a bag with a maximum
capacity of 240 mL and a circumference of 237 mm.
This bag size was pain evoking in these subjects, but in
the full scale study it became apparent that not all
healthy subjects reached PDT. Preferably, future probe
designs should use larger bags, especially in studies of,
for example, constipation as a proportion of these have
elevated sensory thresholds secondary to large capa-
city/excessively compliant rectums.9,36
Methods based on IP allow direct measurements of
the rectal luminal CSA and calculations of the rectal
radius, wall tension and strain, assuming acceptable
circularity of the investigated gut segment.15 Imped-
ance planimetry was applied during rectal distension.
Due to the complex anatomy and the asymmetrical
filling of the rectum, several CSA measurements give a
more reliable profile of the distension-evoked changes
in shape. However, tone of the rectal wall and trans-
versal folds influences these. Consequently, we
decided to use two pairs of electrodes, using the
average value for further analysis. Pain detection
threshold to distension did not differ significantly
between the two study days. The ICC indicates a
variance within the subjects, but when the mechanical
distension was expressed as the stretch ratio at PDT,
ICC = 1.0 proofed excellent reproducibility both with-
out and with butylscopolamine. These findings are
consistent with Fig. 2 and previous data from our group
showing that tensile strain is the most direct stimuli to
mechano-sensitive afferents.10
Assessment of referred pain
Somatic referred pain area to rectal stimulation is
vulnerable to bias. It can be difficult to quantify and
differentiate between referred pain and the feeling of
the rectal probe positioned through the anal canal,
especially when the location is in the perineum.11 We
found no correlation between stimulus intensity and
referred pain area, thus convergence in the dorsal horn
was not more likely to appear at higher stimulus
intensities. In our experiment, the referred pain area
did not project to a single specific dermatome which is
in consistency with visceral sensory afferents project-
ing to the spine with a segmental overlap.
Gender differences
Women were not tested on specific days of their cycle
and future studies may aim at designing a stronger
model taking menstrual cycle variations into consid-
erations.
The multimodal concept in GI research
Sensory responses to a single stimulus of a given
modality only represent a limited part of the total pain
experience. Hence, to mimic clinical pain in experi-
mental models, a multimodal approach has many
advantages. The possibility of stimulating differenti-
ated receptors in different gut layers is advantageous
and has previously been used to evaluate the effect of
various analgesics.2 Multimodal oesophageal testing
has been successful for years.4 Multimodal pain mod-
els in the stomach, duodenum, jejunum and rectum
have also been developed.11 Some of these models can
be modified with chemical substances inducing exper-
imental sensitization and hyperalgesia, which then can
be assessed and modulated by drugs.2 In the large
intestine, chemical stimulation with glycerol and
hypertonic saline has been used37 and such stimula-
tions as well as capsaicin38 could be built into the
current model.
CONCLUSION
A novel multimodal rectal and rectosigmoid sensory
testing approach has been developed and evaluated. It
proved to be user-friendly, and the obtained data were
reproducible between study days and between individ-
uals. This indicates that the multimodal rectal probe is
suitable for studying functional pathophysiology or
pharmacological interventions in patients with pain
and hyper/hypo sensitivity in the large intestine.
ACKNOWLEDGMENTS
Pfizer Ltd, The Danish Research Council (SSVF), the
�Obelske Family Foundation� and �Spar Nord� Founda-
tion are acknowledged.
REFERENCES
1 Russo MW, Wei JT, Thiny MT et al. Digestive and liverdiseases statistics, 2004. Gastroenterology 2004; 126:1448–53.
Volume 20, Number 8, August 2008 Multimodal rectal and rectosigmoid sensations
� 2008 The AuthorsJournal compilation � 2008 Blackwell Publishing Ltd 917

2 Drewes AM, Gregersen H, Arendt-Nielsen L. Experimentalpain in gastroenterology: a reappraisal of human studies.Scand J Gastroenterol 2003; 38: 1115–30.
3 Drewes AM, Gregersen H. Multimodal pain stimulation ofthe gastrointestinal tract. World J Gastroenterol 2006; 16:2477–86.
4 Drewes AM, Frokjaer JB, Larsen E et al. Pain and mechan-ical properties of the rectum in patients with active ulcer-ative colitis. Inflamm Bowel Dis 2006; 12: 294–303.
5 Enggaard TP, Poulsen L, Arendt-Nielsen L et al. Theanalgesic effect of codeine as compared to imipramine indifferent human experimental pain models. Pain 2001; 92:277–82.
6 Staahl C, Reddy H, Andersen SD et al. Multi-modal andtissue-differentiated experimental pain assessment:reproducibility of a new concept for assessment of anal-gesics. Basic Clin Pharmacol Toxicol 2006; 98: 201–11.
7 Mertz H, Naliboff B, Munakata J et al. Altered rectal per-ception is a biological marker of patients with irritablebowel syndrome. Gastroenterolgy 1995; 109: 40–52.
8 Van der Veek PP, Van Rood YR, Masclee AA. Symptomseverity but not psychopathology predicts visceral hyper-sensitivity in irritable bowel syndrome. Clin Gastro-enterol Hepatol 2008; 6: 321–8.
9 Gladman MA, Dvorkin LS, Lunniss PJ, Williams NS, ScottSM. Rectal hyposensitivity: a disorder of the rectal wall orthe afferent pathway? An assessment using the barostat.Am J Gastroenterol 2005; 100: 106–14.
10 Petersen P, Gao C, Arendt-Nielsen L et al. Pain intensityand biomechanical responses during ramp-controlleddistension of the human rectum. Dig Dis Sci 2003; 48:1310–6.
11 Frokjaer JB, Andersen SD, Gale J et al. An experimentalstudy of viscero-visceral hyperalgesia using an ultrasound-based multimodal sensory testing approach. Pain 2005; 3:191–200.
12 Cremonini F, Houghton LA, Camilleri M et al. Barostattesting of rectal sensation and compliance in humans:comparison of results across two centres and overallreproducibility. Neurogastroenterol Motil 2005; 17: 810–20.
13 Pedersen J, Reddy H, Funch-Jensen P et al. Cold and heatpain assessment of the human oesophagus after experi-mental sensitisation with acid. Pain 2004; 2: 393–9.
14 Whitehead WE, Delvaux M. Standardization of Barostatprocedures for testing smooth muscle tone and sensorythreshold in the gastrointestinal tract. Dig Dis Sci 1997;42: 223–41.
15 Gregersen H. Biomechanics of the Gastrointestinal Tract:
New Perspectives on Motility Research and Diagnostics,1st edn. London: Springer, 2003.
16 Frokjaer JB, Liao D, Bergmann A et al. Three-dimensionalbiomechanical properties of the human rectum evaluatedwith magnetic resonance imaging. NeurogastroenterolMotil 2005; 17: 531–40.
17 Arendt-Nielsen L, Drewes AM, Hansen JB et al. Gut painreactions in man: an experimental investigation usingshort and long duration transmucosal electrical stimula-tion. Pain 1997; 69: 255–62.
18 Hammer HF, Phillips SF, Camilleri M et al. Rectal tone,distensibility, and perception: reproducibility and reponseto different distensions. Am J Physiol Gastrointest Liver
Physiol 1998; 274: G584–90.
19 Yang JP, Yao M, Jiang XH et al. Establishment of modelof visceral pain due to colorectal distension and itsbehavioral assessment in rats. World J Gastroenterol 2006;17: 2781–4.
20 Lagier E, Delvaux M, Vellas B et al. Influence of age onrectal tone and sensitivity to distension in healthy sub-jects. Neurogastroenterol Motil 1999; 11: 101–7.
21 Bruton A, Conway JH. Reliability: what is it, and how is itmeasured? Physiotherapy 2000; 86: 94–9.
22 Drewes AM, Petersen P, Qvist P, Nielsen J, Arendt-NielsenL. An experimental pain model based on electric stimula-tions of the colon mucosa. Scand J Gastroenterol 1999; 34:765–71.
23 Ford MJ, Camilleri M, Zinsmeister AR et al. Psychosen-sory modulation of colonic sensation in the humantransverse and sigmoid colon. Gastroenterology 1995; 109:1772–80.
24 Drewes AM, Helweg-Larsen S, Petersen P et al. McGillPain Questionnaire translated into Danish: experimentaland clinical findings. Clin J Pain 1993; 9: 80–7.
25 Brinkert W, Dimcevski G, Arendt-Nielsen L et al. Dysm-enorrhoea is associated with hypersensitivity in the sig-moid colon and rectum. Pain 2007; 132(Suppl. 1): S46–51.
26 Hobson AR, Aziz Q. Assessment of gastrointestinal sen-sation – a review. Dig Dis 2006; 4: 267–77.
27 Rossel P, Pedersen P, Niddam D et al. Cerebral response toelectric stimulation of the colon and abdominal skin inhealthy subjects and patients with irritable bowel syn-drome. Scand J Gastroenterol 2001; 36: 1259–66.
28 Loening-Baucke V, Read NW, Yamada T. Cerebral evokedpotentials after rectal stimulation. Electroencephalogr
Clin Neurophysiol 1991; 80: 490–5.29 Su X, Gebhart GF. Mechanosensitive pelvic nerve afferent
fibers innervating the colon of the rat are polymodal incharacter. J Neurophysiol 1998; 80: 2632–44.
30 Sengupta JN, Gebhart GF. Chapter 11. In: Johnson L, ed.Physiology of the gastrointestinal tract, 3rd edn. NewYork: Raven Press, 1994: 483–519.
31 Villanova N, Azpiroz F, Malagelada JR. Perception and gutreflexes induced by stimulation of gastrointestinal ther-moreceptors in humans. J Physiol 1997; 1: 215–22.
32 Miller R, Bartolo DC, Cervero F et al. Anorectal temper-ature sensation: a comparison of normal and incontinentpatients. Br J Surg 1987; 74: 511–5.
33 Chan CL, Scott SM, Birch MJ et al. Rectal heat thresholds:a novel test of the sensory afferent pathway. Dis Colon
Rectum 2003; 46: 590–5.34 Tominaga M, Caterina MJ. Thermosensation and pain.
J Neurobiol 2004; 61: 3–12.35 Chan CL, Facer P, Davis JB et al. Sensory fibres expressing
capsaicin receptor TRPV1 in patients with rectal hyper-sensitivity and faecal urgency. Lancet 2003; 361: 385–91.
36 Salvioli B, Bharucha AE, Rath-Harvey D et al. Rectalcompliance, capacity, and rectoanal sensation in fecalincontinence. Am J Gastroenterol 2001; 96: 2158–68.
37 Drewes AM, Babenko L, Birket-Smith L et al. Induction ofnon-painful and painful intestinal sensations by hyper-tonic saline: a new human experimental model. Eur J Pain
2003; 7: 81–91.38 Drewes AM, Schipper KP, Dimcevski G et al. Gut pain
and hyperalgesia induced by capsaicin: a human experi-mental model. Pain 2003; 2: 333–41.
C. Brock et al. Neurogastroenterology and Motility
� 2008 The AuthorsJournal compilation � 2008 Blackwell Publishing Ltd918