

























Audit of implantable cardioverter-defibrillators in a single UK centre

1941-3084American Heart Association. All rights reserved. Print ISSN: 1941-3149. Online ISSN: 2011 Copyright ©
Avenue, Dallas, TX 72514Circulation: Arrhythmia and Electrophysiology is published by the American Heart Association. 7272 Greenville
DOI: 10.1161/CIRCEP.110.958744 published online January 26, 2011;Circ Arrhythm Electrophysiol
Matthew Peters, Anastasios Saliaris, Magdi Saba, Stephen Shorofsky and Jean JeudyTimm Dickfeld, Jing Tian, Ghada Ahmad, Alejandro Jimenez, Aharon Turgeman, Richard Kuk,
Enhanced 3D Scar in Patients with ICDMRI-Guided Ventricular Tachycardia Ablation: Integration of Late Gadolinium
World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circep.ahajournals.org/content/suppl/2011/01/26/CIRCEP.110.958744.DC1.html Data Supplement (unedited) at:
initial publication. Advance online articles must include the digital object identifier (DOIs) and date ofpublication priority; they are indexed by PubMed from initial publication. Citations to available prior to final publication). Advance online articles are citable and establishnot yet appeared in the paper journal (edited, typeset versions may be posted when Advance online articles have been peer reviewed and accepted for publication but have
http://www.lww.com/reprintsReprints: Information about reprints can be found online at
[email protected] West Camden Street, Baltimore, MD 21201-2436. Phone: 410-528-4050. Fax: 410-528-8550. E-mail:Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters Kluwer Health,
http://circep.ahajournals.org/site/subscriptions/Subscriptions: Information about subscribing to Circulation: Arrhythmia and Electrophysiology is online at
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

1
MRI-Guided Ventricular Tachycardia Ablation: Integration of Late
Gadolinium Enhanced 3D Scar in Patients with ICD
Running title: Dickfeld et al.; MRI-Guided VT Ablation in ICD Patients
Timm Dickfeld, MD, PhD*, Jing Tian, MD, PhD*, Ghada Ahmad, MD*,
Alejandro Jimenez, MD*, Aharon Turgeman, M.Sc. M.B.A^, Richard Kuk, MD*,
Matthew Peters, MS*, Anastasios Saliaris, MD*, Magdi Saba, MD*,
Stephen Shorofsky, MD, PhD*, Jean Jeudy, MD#
Division of Cardiology* and Radiology#, University of Maryland, Baltimore Biosense Webster Inc., Tirat Carmel, Israel^
Corresponding Author:
Timm Dickfeld, MD, PhD
Division of Cardiology
University of Maryland
22 S. Greene Str., Room N3W77
Baltimore, MD 21201
Fax: 410-328-2062
Phone: 410-328-6056
E-mail: [email protected]
Journal Subject Codes: [22] Ablation/ICD/surgery, [30] CT and MRI, [106] Electrophysiology
MMMMMMMagagagagagagagdididididididi S S S S S S Sabababababababa,a,a,a,a,a,a, M M M M M M MDDDDDDD
dy, MMMMMMMD#D#D#D#D#D#D#
of Cardiology* and Radiology#, University of Maryland, Balof Cardiology* and Radiology#, University of Maryland, BalBiosense Webster Inc., Tirat Carmel, Israel^
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

2
Abstract:
Background - Substrate-guided ablation of ventricular tachycardia (VT) in patients with
implanted defibrillators (ICD) relies on voltage mapping to define the scar/border zone.
An integrated three-dimensional (3D) scar reconstruction from late gadolinium-enhanced
(LGE) MRI could facilitate VT ablations.
Methods and Results - Twenty-two patients with ICD underwent contrast-enhanced
cardiac MRI (CE-CMR) with a specific absorption rate <2.0W/kg prior to VT ablation.
Device interrogation demonstrated unchanged ICD parameters immediately before, after
or at 68±21 days follow-up (p>0.05). ICD imaging artifacts were most prominent in the
anterior wall and allowed full and partial assessment of LGE in 9±4 and 12±3 of 17
segments, respectively.
In fourteen patients with LGE a 3D scar model was reconstructed and successfully
registered with the clinical mapping system (accuracy: 3.9±1.8mm). Using ROC-curves
bipolar and unipolar voltages of 1.49mV and 4.46mV correlated best with endocardial
MRI scar.
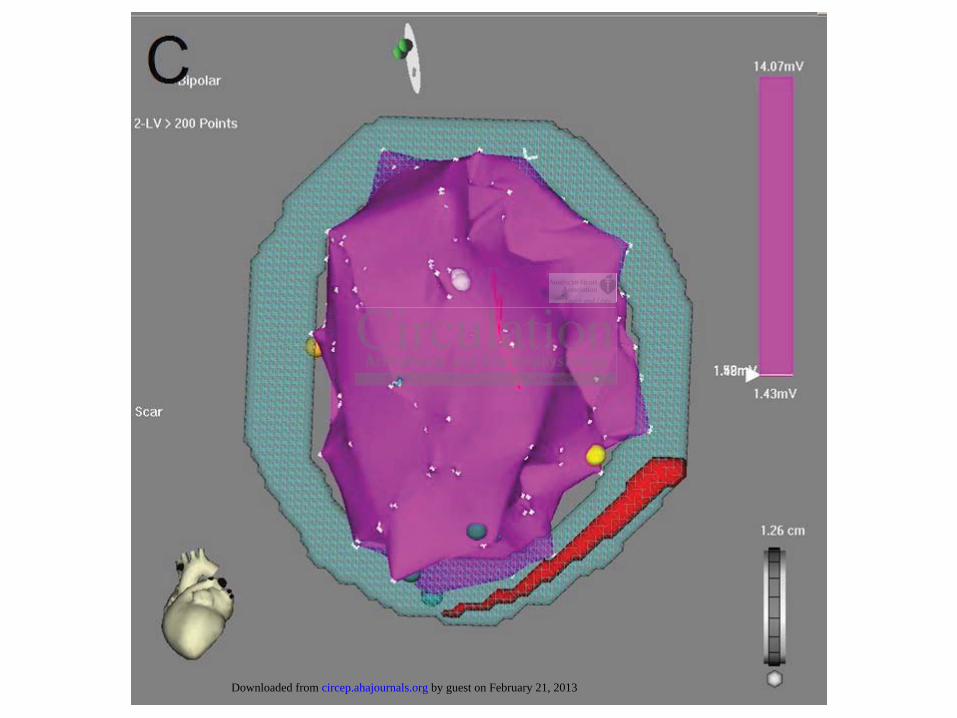
Scar visualization allowed the elimination of falsely-low voltage recordings (suboptimal
catheter contact) in 4.1±1.9% of <1.5mV mapping points.
Display of scar border zone allowed identification of excellent pacemapping sites with
only limited voltage mapping in 64% of patients. Viable endocardium of >2mm resulted
in >1.5mV voltage recordings despite up to 63% transmural midmyocardial scar
successfully ablated with MRI guidance. All successful ablation sites demonstrated LGE
(transmurality: 68±26%) and were located within 10mm of transition zones to 0-25% scar
in 71%.
Conclusions - CE-CMR can be safely performed in selected ICD patients and allows the
integration of detailed 3D scar maps into clinical mapping systems. This provides
supplementary anatomic guidance to facilitate substrate-guided VT ablations.
Key words: MRI/ICD/Ablation/Ventricular Tachycardia
uctededededddd aaaa aa andndndndndndnd sss s sssucucucucucucuccececececececesssss
he clinical mapping s stem (accurac : 3.9±1.8mm). Using R
o n
(
in 4 1±1 9% of <1 5mV mapping points
he clinical mapping system (accuracy: 3.9±1.8mm). Using Rm
olar voltages of 1.49mV and 4.46mV correlated best with en
n allowed the elimination of falsely-low voltage recordings (f
in 4 1±1 9% of <1 5mV mapping points
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

3
INTRODUCTION
With expanding ICD indications an increasing amount of patients present with
appropriate ICD shocks for ventricular arrhythmias.1, 2 The side effects and lack of long-
term efficacy of antiarrhythmics have made VT ablation an increasingly attractive
treatment option.3, 4
In ~70-90% of patients a substrate-guided VT ablation must be pursued due to
hemodynamic instability or multiple VT morphologies.4, 5 During the ablation tangential
or radial lesions are placed along and transsecting the scar border in an attempt to
eliminate conducting channels and VT exit sites.
In these procedures, voltage mapping is the “gold standard” for defining
myocardial scar/border zone or surviving myocardial channels. However, voltage
mapping has multiple limitations: a single endo- (or epi-)cardial voltage measurement
representing a poor surrogate for a complex intramural three-dimensional (3D) scar
anatomy; limited spatial resolution of the electroanatomic maps; prolonged mapping
times; and falsely-low voltage measurements due to imperfect catheter contact.6
MRI has the ability to accurately delineate myocardial scar,7 but ICDs are present
in the majority of VT patients and are still considered a contraindication or impact
imaging quality.8 This study evaluated the safety/diagnostic yield of cardiac MRI in the
largest reported ICD patient cohort to-date and is the first to assess the feasibility of
registered 3D MRI scar reconstructions to facilitate VT ablations in ICD patients.
METHODS
Patient Population
ndarrd”d”ddddd f f f f fffororororororor d d d ddddefefefefefefefiiiiinini
/b o
l a
o D
border zone or surviving myocardial channels. However, vo
ltiple limitations: a single endo- (or epi-)cardial voltage mea
oor surrogate for a complex intramural three-dimensional (3D
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

4
Consecutive patients with an ischemic/non-ischemic cardiomyopathy and ICD
scheduled for VT ablation for frequent ICD therapies were enrolled. Exclusion criteria
consisted of device implantation <6 weeks, epicardial lead/coil system,
abandoned/capped endovascular leads, ICDs manufactured before 2002, and creatinine
clearance <30ml/min. Written consent was obtained in all patients after institutional
approval of the research protocol.
Pre- and Post MRI ICD Interrogation
ICD interrogation was performed immediately before/after the MRI as well as
during follow-up visits. During the MRI tachyarrhythmia detection and/or therapy was
disabled. In pacemaker-dependent patients, bradycardia parameters were programmed to
VOO/DOO mode (60 beats per minute). In not pacemaker-dependent patients rate-
responsiveness feature was temporarily disabled and VVI or DDD programming was left
unchanged.
ECG, blood pressure and pulse oxymetry was continuously monitored during the
MRI and clinical symptoms were recorded. Post-MRI programming was restored to its
original parameters.
MR Imaging
MRI was performed supine using a 1.5T scanner (Siemens Avanto, Princeton, NJ,
USA). Imaging sequences resulted in a specific absorption rate (SAR) <2.0W/kg. Cine
turboFlash sequences to assess anatomic and dynamic characteristics were performed to
assess wall thinning and contractility (FOV=320-400mm/TR=75-80ms/TE=3-4ms/flip
/after the MRIRIIIIII a a
ectioioooooon nn n n n n ananananananand/d/d/d/d/d/d/ororororororor t t t t tt thh
e o
d t
fe m
emaker-dependent patients, bradycardia parameters were pro
de (60 beats per minute). In not pacemaker-dependent patientt
feature was temporarily disabled and VVI or DDD programm
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

5
angle=15°/slice thickness=8mm/10mm spacing). First-pass perfusion using dynamic
gradient echo sequences to assess regional hypoperfusion characteristics were performed
(FOV=320-400mm/TR=160-165ms/TE=1-1.5ms/flip angle=15°/slice
thickness=8mm/10mm spacing).
Inversion recovery images were obtained ECG-gated during diastole 10-15min
after iv. injection of 0.1mg/kg gadobenate dimeglumine (Multihance, Bracco, Princeton,
NJ). Short and long axis 2D (slice thickness=8mm/no gap/TI=250-350ms/TR=725-
950ms/TE=1-4ms/flip angle=25°) and 3D (slice thickness=4-6mm/no gap/TR=700-
750ms/TE=1-1.5ms/flip angle=10°) inversion recovery sequences (Figure 1) were
obtained after optimal nulling of the inversion time to assess late gadolinium
enhancement (LGE).
Delineation of MRI-Derived 3D Myocardium and LV Scar
2D and 3D MRI scans were exported in DICOM format to an external imaging
workstation. Left and right ventricular (LV, RV) endo- and epicardial surfaces as well as
intramyocardial boundaries of myocardial LGE were determined by a radiologist expert
reader with >10 years of experience and hand-planimetered on contiguous, reformatted
2/3D slices using modified Siemens VPT (Siemens, Princeton, NJ, USA) and Amira
software (Amira, Berlin, Germany). In areas of ICD artifact an approximated
reconstruction of the LV endo- and epicardium (without scar) was performed to facilitate
image registration. Scar was only reconstructed from LGE images and if no significant
ICD artifact was present. Reconstructed 3D models of the RV/LV anatomy with
embedded myocardial scar were exported as 3D Carto readable Mesh-files and allowed
ences (Figure 1111111))
latee g g gggggadadadadadadadolololololololinininininininiuiuiuiuiuiuiumm
G
M
GE).
MRI-Derived 3D Myocardium and LV Scar
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

6
the identification of mapping point positions on the corresponding 2D MRI images.
Quantitative and regional scar assessment was performed with Segment v1.x software.9
Using the IPE research software module (Biosense-Webster, Diamond Barr, CA) MRI
surfaces were uploaded into the clinical CartoMERGE system.
Registration of Voltage Map and MRI-Derived LV Anatomy and Scar
If the CartoSOUND module was used an anatomic 3D reconstruction of the RV
and LV was created from sequential 2D intracardiac ultrasound slices (SoundStar,
Biosense Webster) acquired from a RV position.
Using a 3.5mm open-irrigation tip catheter (Thermocool, Biosense Webster) LV
voltage maps were created via retrograde or transseptal approach using a filling threshold
of 15mm and voltage settings of 0.5mV-1.5mV. Uni- and bipolar signals were filtered at
10-400Hz and were acquired during sinus rhythm or ventricular pacing in case of
resynchronization therapy/pacemaker dependency. Signals were defined as normal,
fractionated (FP) or diastolic potentials (DP).10
Applying an “early registration” strategy visual alignment of the 3D MRI
reconstruction was performed with the CartoMERGE software using >10 RV/>50 LV
mapping points. Alternatively, using a “CartoSOUND registration” approach the MRI
LV/scar reconstructions were registered to the anatomic 3D RV and LV ultrasound
shells. This allowed the display of the extracted LV scar during an early stage of the LV
mapping (“early registration”) or even prior to entering the arterial circulation
(“CartoSOUND registration”). “Final registration” of the 3D MRI scar map was
performed after completing RV/LV mapping.
ool, BiBiBiBiBiBiBiosososososososenenenenenenensesesesesesese W W W W W W W
e i
l r
w a
ere created via retrograde or transseptal approach using a filli
ltage settings of 0.5mV-1.5mV. Uni- and bipolar signals wer
were acquired during sinus rhythm or ventricular pacing in ca
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

7
For visually alignment superior mitral valve (MV) points (12 o’clock) were used
as determined by electrical signals, fluoroscopy±ultrasound. Rotational errors were
minimized by aligning the superior and inferior RV septal insertion sites of the MRI-
derived shell with the RV/LV voltage map (Figure 1). For landmark point registration LV
apex, MV and RV septal insertions were selected.
Registration accuracy was determined using the internal CARTO summation
statistics, averaging the distance of the individual mapping points to the closest surface
point of the registered MRI shell.11
VT Ablation
After registration additional MRI-guided mapping was performed at sites <1.5mV
remote from matching MRI scar to determine falsely-low voltage recordings due to
suboptimal catheter contact as well as in areas of complex MRI border zone geometry.
VT was induced by programmed electrical stimulation (PES) with up to triple
extrastimuli from two RV and up to two LV sites (drive cycle length: 350/400/600ms;
minimum coupling interval 200ms). If VT was non-sustained or not tolerated
pacemapping sites were chosen based on MRI-defined border zone (after
“early/CartoSound registration”) and the 12-lead VT morphology. Matches 11/12 were
used to determine the approximate exit sites. In case of hemodynamically tolerated VT
standard entrainment criteria were used within areas of MRI scar.12 Successful ablation
lesions (50W; 60s) were defined as terminating VT or occurring at site of pacemap
matches.
s
t
e
istration additional MRI-guided mapping was performed at s
tching MRI scar to determine falsely-low voltage recordings
eter contact as well as in areas of complex MRI border zone
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

8
Additional tangential/radial ablation lines were created based on scar anatomy
defined by voltage and MRI data. LV mapping was completed (unless noted otherwise)
to assess “final registration” and location of FPs/DPs/voltage-defined border zone. PES
was repeated at the end of the VT ablation. Criteria defining ablation success were the
inability to induce the clinical/presumed clinical VT or sustained monomorphic VT with
longer cycle length.3
Statistical Analysis
SPSS for Windows 16.0 was used to perform the statistical analysis. Continuous
variables are expressed as mean ±1 SD unless otherwise noted.
Comparisons between pre- and post- MRI measures were conducted using the
Wilcoxon signed rank test. The Spearman Rank Correlation Test was obtained to assess
possible correlations. Differences were considered significant at a level of P<0.05.
Receiver operating characteristic (ROC) curves were created for unipolar/bipolar voltage
recordings to identify the best cut off voltage values to predict endocardial MRI scar.
Areas under the curve (AUCs) for each voltage recordings were reported and compared.
RESULTS
Patient Population
Four of the 26 screened patients were excluded due to an epicardial ICD system
(n=1), abandoned endocardial leads (n=2) or creatinine clearance of <30ml/min (n=1).
Twenty-two patients were enrolled in the study. Baseline characteristics are shown in
Table 1.
istical analysisssssss. ... ... C
d.
s u
d e
i <
sons between pre- and post- MRI measures were conducted u
d rank test. The Spearman Rank Correlation Test was obtaine
ions. Differences were considered significant at a level of P<
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

9
Safety of Cardiac MRI in Selected ICD Patients
CE-CMRI was performed in twenty-two patients with single (n=9), dual (n=10)
and bi-ventricular (n=3) ICDs (Data Supplement 1). ICDs were interrogated before/after
MRI and at 68±21 days follow-up (Table 2). Five devices were equipped with wireless
telemetry. Two patients were pacemaker-dependent with ventricular escape rates
<30bpm. No significant changes in battery voltage/impedance, atrial or ventricular
thresholds, intrinsic amplitudes or impedances were seen between pre-MRI, post MRI
and follow-up (Table 2).
No complication occurred during the MRI scanning. No inappropriate/inhibited
pacing or tachytherapy were observed.
Image Quality of Cardiac MRI in ICD Patients
Anatomic-dynamic and first-pass perfusion MR sequences demonstrated limited
artifacts and allowed detailed assessment of the septal, inferior, lateral and anterior wall
regarding anatomic-dynamic (100%/100%/100%/82%) and perfusion
(100%/100%/100%/91%) characteristics.
In LGE sequences for scar visualization ICD artifacts were more pronounced and
appeared as a central signal void (ICD generator) with a surrounding rim of increased
signal intensity (Figure 1A). LGE MRI allowed the partial/full evaluation of the septal
(50%/36%), inferior (100%/91%), lateral (100%/18%) and anterior (27%/0%) wall,
respectively. Only limited <1cm circumferential artifacts were caused by the ICD leads in
No iinananananananapppppppppppppprororororororoprprprprprprpriaiaiaiaiaiaiatet
h
f
herapy were observed.
f Cardiac MRI in ICD Patients
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

10
any of the imaging sequences (Figure 1A). Using the 17-segment AHA classification
LGE could be fully assessed in 9±4 segments and partially assessed in 12±3 segments.13
In ischemic patients 82±7% of scar had endocardial components with mid-
myocardial or epicardial components being predominantly seen as <1cm scar extensions
in the border zone. Of the seven patients with non-ischemic cardiomyopathy two (29%)
had exclusively epicardial or midmyocardial scar. Two non-ischemic patients (29%) had
no identifiable scar.
Extraction and Registration of 3D MRI Scar Map
CE-CMR-based scar integration into a mapping system prior to ablation was
performed in all fourteen patients with LGE that proceeded to a VT ablation (ischemic
cardiomyopathy: eleven). Of the other eight patients, three underwent placement of a left
ventricular assist device or heart transplantation for worsening heart failure, two
requested to have the MRI stopped due to claustrophobia, two had no visible scar and one
patient opted for pharmacological therapy.
Endocardial/epicardial RV/LV borders were successfully hand-planimetered on
contiguous 2D short axis slices in all patients with approximated LV wall contours in
areas of artifact. Detailed 3D scar anatomywas displayed embedded into the myocardium
(Figure 1). LV reconstruction from areas of artifact were separately reconstructed
(without scar) with different color annotation to simplify visualization if artifact and scar
were adjacent (Figure 2).
“Early registration” was performed in the first nine patients using 13±3 RV points
and 54±4 LV points with a registration accuracy of 5.7±3.9mm. In the last five patients
m ppririririririr ororororororor t t t t t to o o o o o o ababababababablalalalalalalatit
: eleven). Of the other eight patients, three underwent plac m
t t
fourteen patients with LGE that proceeded to a VT ablation
: eleven). Of the other eight patients, three underwent placem
t device or heart transplantation for worsening heart failure, tr
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

11
MRI-derived LV/scar maps were registered to CartoSOUND-reconstructed RV/LV shells
with a registration error of 4.6±3.1mm.
“Final registration” accuracy of the completed voltage map (58±39 RV and
190±32 LV points) was 3.9±1.8mm using visual alignment and 4.1±2.0mm with
landmark point/surface registration (Figure 1B). A full LV map was created in all nine
patients with “early registration” and two out of five patients with “CartoSOUND
registration”.
Intraprocedural MRI Guidance During VT Ablation
There was a good correlation between myocardial scar defined by CMR and
voltage.Endocardial voltage points of <0.1mV, <0.5mV and <1.5mV demonstrated MRI-
defined scar in 100%, 87% and 75%, respectively. Increasing transmurality of MRI-
derived scar correlated with decreasing endocardial bipolar voltage (r=-0.83;p<0.01;
Figure 3). ROC curves demonstrated the best cut off values for bipolar/unipolar voltage
recordings to optimally differentiate endocardial scar from non-scar defined by MRI are
1.49mV (AUC:0.86±0.01) and 4.46mV (AUC:0.78±0.02), respectively.
Procedure time for “early registration”, “CartoSOUND registration” and “final
registration” was 4±3min, 5±4min and 5±3min. The “early registration” or
“CartoSOUND registration” allowed the visualization of MRI-derived scar size, location
and transmural extent during 71% and 100% of the total LV mapping point acquisition,
respectively.
Display of the MRI scar guided the further mapping/ablation in several ways:
Detection of Suboptimal Catheter Contact
ar deeeeeefififififififinenenenenenened d d d d dd bybybybybybyby C C C CCCCMM
d
o
r
dial voltage points of <0.1mV, <0.5mV and <1.5mV demon
00%, 87% and 75%, respectively. Increasing transmurality o
related with decreasing endocardial bipolar voltage (r=-0.83;
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

12
Immediate identification of low voltage recordings (<1.5mV) in areas without
MRI-derived scar suggested imperfect catheter contact. Repeat mapping using
echocardiographic contact confirmation demonstrated that 78±12% of those points
(average voltage: 0.83±0.52mV) were shown to have voltages >1.5mV. This represented
4.1±1.9% of the total original <1.5mV mapping points. Locations of mislabeled points
were mid-anterior (37%), septal (29%), infero-basal (25%) and lateral (9%).
Targeted Mapping of Voltage/DP/FP
The integration of 3D MRI-defined scar provided an anatomic characterization of
the 3D scar/border zone geometry displaying varying transmurality and epi-, mid- and
endocardial scar components (Figure 4). Visualization of complex transition zones of scar
transmurality within scar or border zones allowed anatomically targeted mapping for
FPs/DPs or preserved voltages. FPs and DPs were found more frequently within 10mm of
the MRI scar border than in the scar center (69±18% vs. 31±17%, p<0.01). Additionally,
FPs and DPs were found more frequently in areas of >50% vs. <50% MRI-defined scar
transmurality (68±19% vs. 31±18%, p<0.01 and 74±28% vs. 26±28%, p<0.01,
respectively).
Targeted Pacemapping/Entrainment/Ablation
Empiric pacemap sites were selected along the displayed MRI border zone guided
by the 12-lead VT morphology prior to completing LV voltage mapping. This identified
presumptive VT exit sites with 11/12 pacemap match in 64% of patients (Figure 5A;5B).
Pacemap matches 11/12 were found within 10mm of the MRI scar border zone in 77%
of VTs. Mapping density was generally 5-10mm in these targeted locations.
urality and epipipipipipipi ,
mpleex xx x x x x trtrtrtrtrtrtranananananannsisisisisisisitititititititiononooooo
t p
e t
r A
thin scar or border zones allowed anatomically targeted map
erved voltages. FPs and DPs were found more frequently wit
rder than in the scar center (69±18% vs. 31±17%, p<0.01). A
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

13
MRI detected surviving papillary muscle within a large area of infarcted
myocardium in 7% of patients. Early integration of 3D-reconstructed viable myocardium
allowed identification of 11/12 pacemap match at scar/myocardial interface prior to
complete LV mapping (Figure 6).
Despite preserved endocardial voltage (>1.5mV) the display of MRI
midmyocardial scar with a transmurality of 11-63% identified a 11/12 pacemap match
(7% of patients) at the transition zone of enhanced/non-enhanced myocardium (Figure 7).
The identification of midmyocardial scar as VT substrate adjacent to alive endocardium
at the excellent pacemap location suggested a possible endocardial scar exit site,
explained the >1.5mV amplitude, and provided the rationale for ablation in “voltage-
defined” normal myocardium that successfully eliminated the clinical VT. During
bipolar, endocardial mapping a >2mm rim of viable endocardium was observed in 14%
of patients and resulted in >1.5mV voltage recordings during bipolar, endocardial
mapping. This was observed predominantly in non-ischemic patients with septal/infero-
lateral scar location, in which the mid-myocardial scar accounted for 27% and 100% of
total scar, respectively (Data Supplement 2). The preserved voltage would have
prevented the detection of adjacent intramyocardial scar based on voltage criteria alone.
Hemodynamically tolerated VT was induced in 14% of patients. Registration of
MRI-defined scar to the CartoSOUND shell enabled entrainment mapping within the scar
without prior voltage mapping and facilitated the identification of the successful ablation
site (Figure 8). In three of the five patients using the CartoSOUND registration strategy
real-time visualization of RF lesions within the MRI-defined abnormal substrate could be
confirmed by increasing local ultrasound signal intensity (Figure 8).
ardial scar exxititititititit s
for ababababababablalalalalalalatititititiitiononononononon i i i i i iin n n nnnn ““
d v
e a
myocardium that successfully eliminated the clinical VT. D
dial mapping a >2mm rim of viable endocardium was observ
esulted in >1.5mV voltage recordings during bipolar, endoca
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

14
Ablation Results
At PES 2.4±1.2 VTs/patient were inducible, with at least one VT matching the
presumed clinical VT by 12-lead surface ECG and/or ICD-based intracardiac
morphology/rate.3 Cycle length was 389±99ms with 5 left bundle branch, 24 right bundle
branch and 4 indeterminate morphologies (Data Supplement 2).
Twenty-two VTs were targeted for ablation. Acute procedural success was
assessed with PES including double (n=6) and triple extrastimuli (n=8). Clinical VT
remained inducible (n=1) or monomorphic VT, which was faster than the clinical VT, but
had not been previously clinically observed, was inducible and was not ablated (n=6).
All successful ablation sites demonstrated MRI scar (Figure 5C-F;7E-F). Average
scar transmurality was 68±26% [30-100%]. Eighty-one percent of ablation sites had
50% transmural scar components and were located within 10mm of transition zones to
0-25% transmural scar in 71%. Successful ablation sites were more commonly located in
the scar periphery (76%). Additional linear ablations were created a) along voltage/MRI
defined scar borders (n=12 patients); b) connecting areas of dense scar (<0.1mV/>85%
scar transmurality by MRI; n=3 patients); and c) connecting dense scar (<0.1mV/>85%
transmurality) to electrically non-conducting structures such as mitral valve ring (n=6
patients). More than one linear ablation strategy was applied in some patients.
No procedure-related complications were observed. After 15±12months follow-up
54% of patients had non-sustained or sustained VT documented by ICD interrogation
(time-to-first-occurrence 5±4 months post-ablation). Appropriate ICD shocks were seen
in 4 of the 14 patients. ICD shocks occurred in two patients during a heart failure
aster than the clclclclclclclini
nd wawawawawawaw s ss s s s s nononononononot t t t ttt ababababababablalalalalalalatt
e E
ty was 68±26% [30-100%]. Eighty-one percent of ablation i
o
essful ablation sites demonstrated MRI scar (Figure 5C-F;7Ed
ty was 68±26% [30-100%]. Eighty-one percent of ablation si
l scar components and were located within 10mm of transitio
by guest on February 21, 2013circep.ahajournals.orgDownloaded from
15
exacerbation, which resulted ultimately in the patients’ deaths 1 week and 20 months
after ablation. One patient underwent a second ablation and one patient was treated
medically.
DISCUSSION
The findings of this study are a) cardiac contrast-enhanced MRI can be safely
performed in selected patients with ICD; b) ICD artifact decreases imaging quality but
allows the detection of myocardial MRI scar in the majority of patients; c) 3D LV
anatomy and reconstructed MRI-derived scar can be accurately registered with clinical
mapping systems; d) MRI-derived scar provides anatomic guidance during mapping and
VT ablation and e) in combination with 3D ICE allows real-time assessment of ablation
lesions within the MRI substrate in some patients.
Safety and Diagnostic Yield of Cardiac MRI in ICD Patients
While most patients requiring VT ablations have ICDs, defibrillators are still
considered a contraindication for MRI as reflected by a recent FDA summary statement.8
While early reports demonstrated potential soft- and hardware failure with clinical
complications more recent phantom, animal and patient series have suggested that MRI
might be able to be performed safely with appropriate ICD and patient selection.8, 14-16
However, only a minority of MRI in these studies were performed for dedicated cardiac
imaging.
To our knowledge this is the largest study of cardiac MRI (n=22) performed in
ICD patients. No complications were seen with limited SAR of <2.0W/kg.
ely registered wwwwwwwi
uidancncncncncncnce e e e ee e dudududududuuririririririringngngngngngng m m
e) in combination with 3D ICE allows real-time assessment
e MRI substrate in some patients.
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

16
Gimbel et al. reported a “power-on-reset” in one of 7 ICD patients undergoing
non-thoracic MRI (SAR not specified). Nazarian et al. found no complications in 13
patients with cardiac MRI out of 24 ICD patients with thoracic/extra-thoracic MRI
(SAR<2W/kg). Naehle et al. reported recently on MRI in 18 ICD patients (4 patients with
cardiac MRI; SAR 2W/kg), which resulted in an acute decrease of battery voltage that
recovered at follow-up.
LGE MRI has been shown to accurately determine areas of myocardial necrosis7,
but imaging quality is impacted by ICD-induced geometric distortion, warping and
susceptibility-induced artifacts.17
In this study ICD artifacts significantly limited the detection of myocardial scar in
the anterior wall and depending on imaging plane/low implant location parts of the septal,
lateral and rarely inferior wall. However, LGE representing MRI scar could be visualized
in all patients.
The anatomic-dynamic and perfusion imaging sequences were less susceptible to
ICD artifacts and may allow the further characterization of the anterior wall scar substrate
based on anatomic (e.g. wall thinning), dynamic (e.g. hypocontractility), and first-pass
perfusion (hypoenhancement) characteristics, but was not performed in this study.
Feasibility of Image Integration of 3D MRI Derived Scar
Reconstruction of representative 3D scar models from 2D/3D image sequences
was possible in all cases. Integration and registration of the 3D reconstructed MRI scar
into the clinical mapping system was successfully performed in all patients. The final
registration accuracy was 3.9±1.8mm, which is similar to previously reported image
tectitiiiiiiononononononn o oo o o oof f f f f f f mymymymymymymyocoooooo
y b
and depending on imaging plane/low implant location parts
y inferior wall. However, LGE representing MRI scar could b
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

17
integration studies.18-20 Codreanu et al.21 and Desjardin et al.19 retrospectively
reconstructed and registered post-infarct MRI scar with previously acquired voltage
maps. Bogun et al. registered MRI-scar in fourteen non-ischemic patients in preparation
for VT or PVC ablation.18 All these studies used non-ICD patients and found a good
correlation between abnormal voltage and (especially endocardial) LGE.
Supplementary MRI Substrate Characterization During VT Ablation
To our knowledge this is the first time that early registration approaches have
been used to display intramural scar location and transmurality to guide the majority of
LV mapping and ablation.
An important finding of this approach is that ~4% of mapping points with initial
voltages of <1.5mV were found to be due to suboptimal catheter contact and that
simultaneous MRI scar display allowed for instantaneous correction resulting ultimately
in a more accurate substrate characterization. This is consistent with the findings of
Codreanu et al., who reported in 3 of 12 patients (25%) a >20% larger scar by voltage
criteria (<1.5mV) than by MRI, which they attributed to likely difficult catheter contact.21
Another important result of this study is that in over 60% of our patients the early
display of the MRI border zone combined with the 12-lead VT morphology allowed the
identification of 11/12 pacemap sites prior to detailed voltage mapping (normally
required to determine the border zone and pacemap sites). This is consistent with other
studies that found that successful ablation sites in ischemic VT were located in 68% at
the scar border zone.22 Additionally, not only the display of the lateral border zone, but
also the 3D integration of alive myocardium within a larger area of scar (such as
ty to guide the e e e e e e mm
r
m d
R g
rtant finding of this approach is that ~4% of mapping points
mV were found to be due to suboptimal catheter contact and
RI scar display allowed for instantaneous correction resulting
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

18
surviving papillary muscle) was able to visually guide successfully pacemapping prior to
complete voltage mapping. This may enable a faster, anatomically guided ablation
approach.
Furthermore, 3D MRI scar integration provided visualization of the
midmyocardial scar, functioning as the VT reentrant substrate that was not detected by
conventional voltage criteria. The midmyocardial scar display anatomically guided
pacemapping and provided the rationale to ablate in an endocardial site with normal
voltage and signal characteristics that successfully eliminated the clinical tachycardia. In
our study a >2mm rim of surviving endocardium was able to prevent the detection of up
to ~60% transmural midmyocardial scar using conventional voltage criteria.
Correspondingly, bipolar amplitudes of midmyocardial/epicardial scar were found in
ischemic patients to be 1.52±1.41mV.21
Differences between MRI scar and voltage defined scar have also been reported in
other studies. Twenty percent larger MRI scar than voltage scar was found by Codreanu
et al. in the infero-basal LV wall.21 Desjardins et al. reported normal EGM characteristics
in areas with 5±18% transmural scar.19 Similarly, we found that endocardial MRI scar of
<25% transmurality might not be detected by voltage mapping.23 This limitation of
voltage mapping to detect thin layers of scar may also help explain successful VT
ablations in myocardium with normal voltage amplitudes in 4% of patients.22
In this study, successful ablation sites displayed a scar transmurality of 68±26%
and were frequently adjacent to areas of <25% scar transmurality. This is consistent with
previous studies in ischemic patients that found a scar transmurality of 60±38% at
successful ablation sites19 and a preferential location in the border zone area.22 Similarly,
prevent the dedeeeeeetetttttt
volttagagagagagagage e e e e e e crcrcrcrcrcrritititititititerererererereriaiaiaiaiaiaia.
y
s
ces between MRI scar and voltage defined scar have also bee
y, bipolar amplitudes of midmyocardial/epicardial scar were
s to be 1.52±1.41mV.21
ces between MRI scar and voltage defined scar have also bee
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

19
LGE was seen at all ablation sites of LGE-positive patients with non-ischemic
cardiomyopathy.18
In this study the final decision about the ablation site relied on the conventional
parameters like pacemapping or concealed entrainment, which likely explains the similar
results to non-image-guided VT ablation studies.4 With improving protocols predictive
MRI characteristics of successful ablation sites could potentially be developed. In a
canine-model Ashikaga et al. demonstrated that high-resolution MRI was able to
delineate areas of surviving myocardial areas within scar that correlated with VT
channels during epicardial mapping.24 Several mathematical models exist which may be
able to predict VT channels and successful ablation sites based on the infarct border zone
geometry.25
Limitations
While in this small sample of ICD patients MRI did not result in adverse events,
this needs to be confirmed in larger patient cohorts and various imaging protocols.
ICD artifacts prevented the detection of LGE in the anterior wall and possibly
other parts of the LV. Complimentary anatomic/dynamic or perfusion imaging, which is
less susceptible to those artifacts could be used to provide additional information about
those areas. Alternatively, fusion imaging (e.g. PET/MRI) could help define the presence
of anterior scar.
While careful image registration was performed, misregistrations cannot be
excluded. However, the used registration algorithms have been validated in previous
models exist wwwwwwwhh
ed on n n n n n n thththththththe e e e e e inininininininfafafafafafafarcrcrrrrr t
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

20
studies and the overall registration accuracy was comparable to other reports suggesting
no significant additional error.18-20
The study population included patients with predominantly ischemic, but also
non-ischemic cardiomyopathy. However, this heterogeneity would be unlikely to affect
the MRI safety profile of ICDs. While scar distribution is frequently different in both
entities, only patients with LGE scar were used for 3D MRI scar registration and LGE
was found to be a critical component of all successful ablation sites.
CONCLUSIONS
3D MRI scar maps of ICD patients can be successfully extracted/registered and
provide an improved appreciation of the complex scar anatomy than can be provided by
voltage mapping alone. The early MRI scar display can assist in more accurate scar
delineation/mapping and provide anatomic guidance for identification of critical scar
substrate in many patients. Its impact on clinical parameters such as procedure times and
long-term success will need to be assessed in future randomized-controlled trials.
Acknowledgments: We thank Dr. Tom O’Donnell, PhD (Siemens Corporate Research,
New York) for his excellent technical support and software expertise.
This study was supported by a AHA Scientist Development Grant (0635304N).
Conflict of Interest Disclosures: Timm Dickfeld – Research Collaboration/Research
Grant (Minor):Biosense Webster; Aharon Turgeman - Employer Biosense-Webster
ly exxxxxxxtrtrtrtrtrtrracacacacacaca teteteteteteted/d/d/d/d/d/d/rererererereregggigg
o p
g a
p t
oved appreciation of the complex scar anatomy than can be p
g alone. The early MRI scar display can assist in more accura
ping and provide anatomic guidance for identification of crit
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

21
References:
1. Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M,
Troutman C, Anderson J, Johnson G, McNulty SE, Clapp-Channing N, vidson-Ray
LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH. Amiodarone or an implantable
cardioverter-defibrillator for congestive heart failure. N.Engl.J.Med. 2005;352:225-
37.
2. Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, Daubert JP,
Higgins SL, Brown MW, Andrews ML. Prophylactic implantation of a defibrillator
in patients with myocardial infarction and reduced ejection fraction. N.Engl.J.Med.
2002;346:877-83.
3. Aliot EM, Stevenson WG, mendral-Garrote JM, Bogun F, Calkins CH, Delacretaz
E, Della BP, Hindricks G, Jais P, Josephson ME, Kautzner J, Kay GN, Kuck KH,
Lerman BB, Marchlinski F, Reddy V, Schalij MJ, Schilling R, Soejima K, Wilber
D. EHRA/HRS Expert Consensus on Catheter Ablation of Ventricular Arrhythmias:
developed in a partnership with the European Heart Rhythm Association (EHRA), a
Registered Branch of the European Society of Cardiology (ESC), and the Heart
Rhythm Society (HRS); in collaboration with the American College of Cardiology
(ACC) and the American Heart Association (AHA). Heart Rhythm. 2009;6:886-
933.
4. Stevenson WG, Wilber DJ, Natale A, Jackman WM, Marchlinski FE, Talbert T,
Gonzalez MD, Worley SJ, Daoud EG, Hwang C, Schuger C, Bump TE, Jazayeri M,
Tomassoni GF, Kopelman HA, Soejima K, Nakagawa H. Irrigated radiofrequency
mplantation off aaaa ff
tionn ff f f f fraractctioioioioioioion.n.n.n.n.n.n. NNNNN N N.
8
S ,
P, Hindricks G, Jais P, Josep son ME, Kautzner J, Kay GN,
877-83.
Stevenson WG, mendral-Garrote JM, Bogun F, Calkins CH,
P, Hindricks G, Jais P, Josephson ME, Kautzner J, Kay GN,
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

22
catheter ablation guided by electroanatomic mapping for recurrent ventricular
tachycardia after myocardial infarction: the multicenter thermocool ventricular
tachycardia ablation trial. Circulation 2008;118:2773-82.
5. Marchlinski FE, Callans DJ, Gottlieb CD, Zado E. Linear ablation lesions for
control of unmappable ventricular tachycardia in patients with ischemic and
nonischemic cardiomyopathy. Circulation 2000;101:1288-96.
6. Dickfeld T, Kato R, Zviman M, Lai S, Meininger G, Lardo AC, Roguin A, Blumke
D, Berger R, Calkins H, Halperin H. Characterization of radiofrequency ablation
lesions with gadolinium-enhanced cardiovascular magnetic resonance imaging. J
Am Coll Cardiol 2006;47:370-8.
7. Kim RJ, Fieno DS, Parrish TB, Harris K, Chen EL, Simonetti O, Bundy J, Finn JP,
Klocke FJ, Judd RM. Relationship of MRI delayed contrast enhancement to
irreversible injury, infarct age, and contractile function. Circulation 1999;100:1992-
2002.
8. Faris OP, Shein M. Food and Drug Administration perspective: Magnetic resonance
imaging of pacemaker and implantable cardioverter-defibrillator patients.
Circulation 2006;114:1232-3.
9. Heiberg E, Ugander M, Engblom H, Gotberg M, Olivecrona GK, Erlinge D,
Arheden H. Automated quantification of myocardial infarction from MR images by
accounting for partial volume effects: animal, phantom, and human study.
Radiology 2008;246:581-8.
q y
neticc r resesononanancecececececece ii
ieno DS, Parrish T Harris Chen EL Simonetti O, Bun y
Judd RM. Relationship of MRI delayed contrast enhance e
ardiol 2006;47:370-8.
eno DS, Parrish TB, Harris K, Chen EL, Simonetti O, Bundy
Judd RM. Relationship of MRI delayed contrast enhanceme
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

23
10. Josephson, M. E. Clinical Cardiac Electrophysiology. 3rd ed. 2002. Philadelphia,
Lippincott Williams & Wilkins.
11. Bertaglia E, Brandolino G, Zoppo F, Zerbo F, Pascotto P. Integration of three-
dimensional left atrial magnetic resonance images into a real-time electroanatomic
mapping system: validation of a registration method. Pacing Clin.Electrophysiol.
2008;31:273-82.
12. Stevenson WG, Khan H, Sager P, Saxon LA, Middlekauff HR, Natterson PD,
Wiener I. Identification of reentry circuit sites during catheter mapping and
radiofrequency ablation of ventricular tachycardia late after myocardial infarction.
Circulation 1993;88:1647-70.
13. Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK,
Pennell DJ, Rumberger JA, Ryan T, Verani MS. Standardized myocardial
segmentation and nomenclature for tomographic imaging of the heart: a statement
for healthcare professionals from the Cardiac Imaging Committee of the Council on
Clinical Cardiology of the American Heart Association. Circulation 2002;105:539-
42.
14. Gimbel JR, Kanal E, Schwartz KM, Wilkoff BL. Outcome of magnetic resonance
imaging (MRI) in selected patients with implantable cardioverter defibrillators
(ICDs). Pacing Clin.Electrophysiol. 2005;28:270-3.
pp ggggggg
afteer r mymymyyyococarardididididididiaaaalalaa
n
M y
, Rumberger JA, Ryan T, Verani MS. Standardized myocard
n 1993;88:1647-70.
MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey
, Rumberger JA, Ryan T, Verani MS. Standardized myocard
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

24
15. Naehle CP, Strach K, Thomas D, Meyer C, Linhart M, Bitaraf S, Litt H, Schwab
JO, Schild H, Sommer T. Magnetic resonance imaging at 1.5-T in patients with
implantable cardioverter-defibrillators. J.Am.Coll.Cardiol. 2009;54:549-55.
16. Nazarian S, Roguin A, Zviman MM, Lardo AC, Dickfeld TL, Calkins H, Weiss
RG, Berger RD, Bluemke DA, Halperin HR. Clinical utility and safety of a protocol
for noncardiac and cardiac magnetic resonance imaging of patients with permanent
pacemakers and implantable-cardioverter defibrillators at 1.5 tesla. Circulation
2006;114:1277-84.
17. Schueler BA, Parrish TB, Lin JC, Hammer BE, Pangrle BJ, Ritenour ER,
Kucharczyk J, Truwit CL. MRI compatibility and visibility assessment of
implantable medical devices. J.Magn Reson.Imaging 1999;9:596-603.
18. Bogun FM, Desjardins B, Good E, Gupta S, Crawford T, Oral H, Ebinger M, Pelosi
F, Chugh A, Jongnarangsin K, Morady F. Delayed-enhanced magnetic resonance
imaging in nonischemic cardiomyopathy: utility for identifying the ventricular
arrhythmia substrate. J.Am.Coll.Cardiol. 2009;53:1138-45.
19. Desjardins B, Crawford T, Good E, Oral H, Chugh A, Pelosi F, Morady F, Bogun
F. Infarct architecture and characteristics on delayed enhanced magnetic resonance
imaging and electroanatomic mapping in patients with postinfarction ventricular
arrhythmia. Heart Rhythm. 2009;6:644-51.
20. Dickfeld, T., Lei, P, Dilsizian, V, Jeudy, J, Dong, J., Voudouris, A, Peters, R, Saba,
M, Shekhar, R, and Shorofsky, S. Integration of Three-Dimensional Scar Maps for
e BJJJJJJJ, , ,, RiRiRiRiRiRiRitetettttt nonoururrrrurr EEEEEEE
k t
e
g
k J, Truwit CL. MRI compatibility and visibility assessment
e medical devices. J.Magn Reson.Imaging 1999;9:596-603.
, Desjardins B, Good E, Gupta S, Crawford T, Oral H, Ebing
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

25
Ventricular Tachycardia Ablation With Positron Emission Tomography-Computed
Tomography. J Am Coll Cardiol Img 1, 73-82. 2008.
21. Codreanu A, Odille F, Aliot E, Marie PY, Magnin-Poull I, Andronache M, Mandry
D, Djaballah W, Regent D, Felblinger J, de CC. Electroanatomic characterization of
post-infarct scars comparison with 3-dimensional myocardial scar reconstruction
based on magnetic resonance imaging. J.Am.Coll.Cardiol. 2008;52:839-42.
22. Verma A, Marrouche NF, Schweikert RA, Saliba W, Wazni O, Cummings J,
Abdul-Karim A, Bhargava M, Burkhardt JD, Kilicaslan F, Martin DO, Natale A.
Relationship between successful ablation sites and the scar border zone defined by
substrate mapping for ventricular tachycardia post-myocardial infarction.
J.Cardiovasc.Electrophysiol. 2005;16:465-71.
23. Tian J, Smith MF, Jeudy J, Dickfeld T. Multimodality fusion imaging using
delayed-enhanced cardiac magnetic resonance imaging, computed tomography,
positron emission tomography, and real-time intracardiac echocardiography to
guide ventricular tachycardia ablation in implantable cardioverter-defibrillator
patients. Heart Rhythm. 2009;6:825-8.
24. Ashikaga H, Sasano T, Dong J, Zviman MM, Evers R, Hopenfeld B, Castro V,
Helm RH, Dickfeld T, Nazarian S, Donahue JK, Berger RD, Calkins H, Abraham
MR, Marban E, Lardo AC, McVeigh ER, Halperin HR. Magnetic resonance-based
anatomical analysis of scar-related ventricular tachycardia: implications for catheter
ablation. Circ.Res. 2007;101:939-47.
, ,,
scarr bbbb bbborordeddddedd r r zozoooooonnnnnnene
mapping for ventricular tachycardia post-myocardial infarctio
s
ith MF, Jeudy J, Dickfeld T. Multimodality fusion imaging u
mapping for ventricular tachycardia post-myocardial infarctio
sc.Electrophysiol. 2005;16:465-71.
ith MF, Jeudy J, Dickfeld T. Multimodality fusion imaging u
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

26
25. Ciaccio EJ, Ashikaga H, Kaba RA, Cervantes D, Hopenfeld B, Wit AL, Peters NS,
McVeigh ER, Garan H, Coromilas J. Model of reentrant ventricular tachycardia
based on infarct border zone geometry predicts reentrant circuit features as
determined by activation mapping. Heart Rhythm. 2007;4:1034-45.
Table 1. Baseline Characteristics of Patient Population Undergoing MR Imaging
Patient Characteristics Results
Age (years) 58±15
Sex (M/F) 21/1
Weight (Kg) 95.1± 26.8
Height (cm) 177± 9
Body surface area (m2) 2.1± 0.3
VT episodes/previous 30 days 17±12
Ischemic cardiomyopathy (%) 68
Non-ischemic cardiomyopathy (%) 32
Ejection fraction (%) 34±14
Hypertension (%) 50
Diabetes (%) 23
Hyperlipidemia (%) 59
Antiarrhythmic therapy (%) 100
Amiodarone (%) 68
Sotalol 28
Quinidine (%) 4
e
v
95.1± 26.8
177± 9
ea (m2) 2.1± 0.3
vious 30 days 17±12
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

27
Table 2. ICD parameters. ICD parameters measured before and after MRI as well as after
68±21 days of follow-up summarizing ventricular leads (n=22) and atrial leads (n=13)
measurements. To account for devices allowing only pulse width decrements thresholds
are also displayed as (V*ms). Significance evaluated with Wilcoxon Signed Ranks Test.
Parameters Pre-MRI Post-MRI Follow-Up p-value
(pre/post)
P-wave amplitude [mV] 3.3±2.1 3.0±1.4 3.1±1.6 p=0.35
R-wave amplitude [mV] 9.9±5.2 10.2±5.4 10.1±5.9 p=0.09
Atrial lead impedance [ ] 475±78 476±69 462±83 p=0.51
Ventricular lead impedance [ ] 461±97 451±89 450±95 p=0.82
Shock impedance [ ] 45±8 45±8 44±7 p=0.34
Atrial capture [V]
[V]*[ms]
1.5±0.9
0.41±0.23
1.4±0.9
0.41±0.22
1.5±1.0
0.41±0.28
p=0.32
p=0.66
Ventricular capture [V]
[V]*[ms]
1.6±0.7
0.43±0.18
1.6±0.7
0.44±0.16
1.5±0.7
0.44±0.15
p=0.32
p=0.79
Battery [V] 2.97±0.21 2.97±0.21 2.95±0.22 p=0.08
Figure Legends:
Figure 1. MRI and Extraction of Anatomy in ICD Patients. A) Inverse recovery serial
short-axis MR images (apical-to-base: 1-6). ICD results in high intensity artifact affecting
the anterior wall. ICD lead seen as low intensity signal in inferior right ventricle (RV).
Transmural late gadolinium enhancement (LGE) seen in inferior wall of left ventricle
(LV). B) Registration of Extracted 3D MRI. LV voltage map is aligned with MRI-
extracted endocardial shell (Endo; turquoise). Rotational errors are corrected by aligning
462±83 pppp=p=p=p=p=p=p=00
450±±±±±±±95959595959595 pppppp=p=p=p=p=p=p=0000000
0
00 44±0 150 44±0 160 43±0 18[V]*[ ]
n 0
0
0
ture [V]
[V]*[ ]
1.6±0.7
0 43±0 18
1.6±0.7
0 44±0 16
1.5±0.7
0 44±0 15
pp=0
0
nce [ ] 45±8 45±8 44±7 pp=0
[V]
[V]*[ms]
1.5±0.9
0.41±0.23
1.4±0.9
0.41±0.22
1.5±1.0
0.41±0.28
pp=0
pp=0
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

28
RV voltage map with reconstructed MRI RV slice (red). After integration of MRI-
extracted epicardial shell (Epi; blue mesh) embedded MRI-derived transmural scar
(brown) is well visible within myocardial wall.
Figure 2. Visualization of Anterior Scar, Artifact and Viable Myocardium A) MRI
demonstrates anterior artifact (grey arrows) concealing possible anterior scar, but allows
visualization of adjacent septal and lateral scar (brown arrows) and preserved inferior
viable myocardium (purple arrows). B) Corresponding 3D reconstruction demonstrates
approximated LV wall reconstruction from area of artifact (grey solid), septal and lateral
scar (brown mesh) and viable inferior myocardium (purple solid), which correlate with
<0.5mV and >1.5mV voltage recordings in registered voltage map.
Figure 3. Correlation of MRI Scar Transmurality and Bipolar Voltage. Increasing scar
transmurality demonstrates a good correlation with decreasing bipolar voltage (Spearman
Rank Correlation Analysis).
Figure 4. Complex 3D Scar Border Geometry. Clipping plane allows visualization of
endo-/epicardium (turquoise shell, black arrows). Note embedded basal transmural scar
(blue shell, white arrows) with decreasing epicardial extension towards the apex (yellow
arrows). Endocardial voltage map normalizes (red-to-purple color; red arrow) with
increasing alive endocardial component and does not detect mid-epicardial scar. Areas of
fractionated signals (pink tags) seen close to transition zone.
rey solid), sepepppppptatattttt
olid)d)))))), , , , ,,, whwhwhwhwhwhw icicicicicicich h h h h h h cococococococorrr
5
ation of MRI Scar Transmurality and Bipolar Voltage. Inc e
5mV voltage recordings in registered voltage map.
ation of MRI Scar Transmurality and Bipolar Voltage. Incre
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

29
Figure 5. MRI-Guided Identification of Ablation Site at Scar Border. “Early registration”
strategy guided pacemapping (orange-brown tags) along the border of the registered scar
mesh and allowed rapid identification of a fractionated, low-voltage site (yellow tag; A)
with 11/12 match (B). Note excellent correlation between scar mesh and abnormal
voltage area after “final registration” with complete LV map (blue/pink tags:
fractionated/diastolic potentials; A). Ablation at that site eliminated the clinical VT.
Endo/epicardium, intramyocardial scar and projected RF lesion of corresponding MRI
slice were extracted (C) and used for 80-sector analysis (D). Resulting diagram (E)
displays color-coded in analogous short-axis views the scar transmurality and identifies
RF location (arrow). Local scar characteristics at ablation sector (arrow) can be identified
in subselected regions-of-interest of LV wall (F).
Figure 6. MRI-Guided Pacemapping/Ablation. Despite significant metal artifact viable,
non-enhanced postero-medial papillary muscle (PM) with alive endo-, mid and epicardial
components embedded in inferior scar seen in MRI (A; black arrows; apical-to-basal scan
plane:1-4). Pacemapping (orange-brown tags) visually guided around 3D-
reconstructed/registered papillary muscle (turquoise) identifies fractionated, low-voltage
site at lateral PM insertion site (B; yellow tag; shown with “final registration”).
Pacemapping achieved 11/12 match (C) and ablation resulted in non-inducibility of VT.
Imaging planes (1-4) corresponding to Figure A.
Figure 7: MRI-Guided Detection and Ablation of Midmyocardial Scar. Normal
endocardial voltage map with lowest bipolar voltage in infero-lateral wall. MR imaging
ransmurality aaaaaaanndnnnnn
ctor (((((((arararararararrorororororor w)w)w)w)w)w)w) c c cccccanananaanaa
G i
gions-of-interest of LV wall (F).
Guided Pacemapping/Ablation. Despite significant metal arti
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

30
plane (white line, panel A) demonstrates corresponding infero-lateral midmyocardial scar
(B), which was 3D reconstructed displaying the accurate intramyocardial location (C).
Pacemapping at this location resulted in 11/12 pacemap match and ablation eliminated
VT. Eighty-sector analysis demonstrates maximum scar transmurality of 63% with
ablation sites located at scar border zone (E;F).
Figure 8. Ultrasound-guided Scar Registration and Ablation Confirmation.
Reconstructed inferior 3D scar (white arrows) is registered to CartoSOUND-constructed
RV/LV shell acquired from RV (“CartoSOUND registration”). After VT induction
entrainment mapping is limited to area of MRI reconstructed scar and identifies critical
channel basal inferior wall ((B; orange arrow) where ablation terminated the clinical VT.
Creation of successful ablation site could be confirmed by increased focal echodensity
(yellow arrow).
). After VT innnnnnnddddddd
scarrrrrrr a a aaaaandndndndndndnd i i i i ii idededededededentntntntntntntifi
f
e c
ferior wall ((B; orange arrow) where ablation terminated the
essful ablation site could be confirmed by increased focal ec
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

Supplemental Material
by guest on February 21, 2013circep.ahajournals.orgDownloaded from

P. # Etiology
Voltage Scar Location MRI Scar Location
MRI scar area endocardial [cm2]
Voltage area <0.5mV [cm2]
Voltage area <1.5mV [cm2] Pre-RFA VT
CL [ms]
Clinical VT
Post-RFA Induction
1 ischemic inferior, septal inferior, septal 70.2 19.4 69.8 RBBB 312 yes* Non-clinical VT Indeterminate 308 no
2 ischemic inferior, infero-septal, infero-lateral
inferior, infero-septal, infero-lateral 65.4 24.9 57.7 RBBB 320 yes* Non-clinical VT
RBBB 230 no 3 ischemic inferior, infero-septal inferior, infero-septal 38 13.2 39.4 RBBB 365 yes* No VT
LBBB 299 no
4 non-ischemic inferior, lateral inferior, lateral 28.9 22.5 37.1 RBBB 448 yes* No VT
5 ischemic inferior, infero-apical inferior, infero-apical 38.2 15.4 34.1 RBBB 441 yes* No VT 6 ischemic inferior inferior 24.3 11.9 23.8 RBBB 521 yes* Non-clinical VT
RBBB 345 no Indeterminate 440 no LBBB 362 no
7 ischemic anterior, septal anterior (A), septal 31.6 12.4 33.2 RBBB 532 yes* No inducible VT
8 non-ischemic
none lateral (mid/epicardial only) 6.2 (mid) 0 0 RBBB 520 yes* Non-clinical VT
RBBB 242 yes*
9 non-ischemic
inferior, infero-septal inferior, septal (mostly mid) 54.6 18.7 48.4 RBBB 280 yes*
No VT
(+20.2 mid) LBBB 278 yes* 10 ischemic inferior, infero-septal inferior, infero-septal 35.5 16.6 36.7 RBBB 422 yes* Clinical VT
RBBB 450 yes* LBBB 324 no RBBB 367 no
11 ischemic inferior, infero-lateral inferior, infero-lateral 17 7.5 24.6 RBBB 530 yes* Non-clinical VT RBBB 525 no Indeterminate 521 no
12 ischemic inferior inferior 34.4 4.2 33.1 RBBB 430 yes* No VT RBBB 595 no*
13 ischemic inferior inferior 42.7 21.4 45.5 RBBB 444 yes* No VT RBBB 412 yes*
14 ischemic anterior, septal, lateral
anterior (A), septal, lateral 60.1 51.9 63.6 RBBB 342 yes* Non-clinical VT
RBBB 360 yes* RBBB 304 yes* Indeterminate 347 no* LBBB 237 no
Data Supplement 2: Image-Guided Ventricular Tachycardia Ablation. Dickfeld et al.
by guest on February 21, 2013circep.ahajournals.org
Dow
nloaded from

Supplement 2: Individual Procedural and Imaging Patient Data. To allow valid comparison between MRI scar and voltage scar, area of ICD artifact was excluded for scar area analysis. Relevant Abbreviations: P# - patient number; mid – midmyocardial; (A) – predominant artifact; CL – cycle length of ventricular tachycardia; * - Ventricular tachycardia targeted during ablation (RFA)
by guest on February 21, 2013circep.ahajournals.org
Dow
nloaded from

Data Supplement 1: Image-Guided Ventricular Tachycardia Ablation. Dickfeld et al.
Lead Data # Generator Ventricular Lead Atrial Lead
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
Medtronic Maximo VR 7232 Medtronic Maximo VR 7232 Guidant Livian H227 RF Guidant Ventak Prism II 1861 St Jude Current VR RF 1207-36 Medtronic Virtuoso VR D154VWC Medtronic Maximo VR 7232 Medtronic EnTrust D154VRC Medtronic Maximo VR 7232 Medtronic EnTrust D154ATG Medtronic Insync Maximo 7303 Medtronic Concerto C154DWK Guidant Vitality A155 Medtronic Intrinsic 7288 St Jude Atlas II VR V168 Medtronic EnTrust D154ATG Medtronic Secura DR D224DRG St Jude Current RV RF 1207-36 Medtronic EnTrust D154VRC Guidant Vitality A155 Medtronic Marquis DR7274 Medtronic Secura DR D224DRG
Medtronic 6949 Sprint Fidelis Medtronic 6947 Sprint Quattro Medtronic 6945 Sprint Guidant 0148 Reliance St Jude 7001 Riata ST Medtronic 6949 Sprint Fidelis Medtronic 6947 Sprint Quattro Medtronic 6949 Sprint Fidelis Medtronic 6947 Sprint Quattro Medtronic 6947 Sprint Quattro Medtronic 6943 Sprint Medtronic 4193 Attain OTW (LV) Medtronic 6947 Sprint Quattro Medtronic 4194 AttainOTW (LV) Medtronic 6945 Spring Medtronic 6947 Sprint Quattro St Jude 7000 Riata ST Medtronic 6943 Sprint Medtronic 6947 Sprint Quattro St Jude 7120 Durata Medtronic 6949 Sprint Fidelis Guidant 0184 Reliance Medtronic 6947 Sprint Secure Medtronic 6945 Sprint
___ ___ Medtronic 5076 CapsureFix Novus Guidant 4087 Flextend ____ ____ ____ ____ Medtronic 5592 CapSure SP Medtronic 5076 CapSure Fix Novus St Jude 1688T Tendril SDX Medtronic 5076 CapsureFix Novus St Jude 1388T Tendril DX ____ Medtronic 5076 CapsureFix Novus Medtronic 5076 CapsureFix Novus ____ ____ Guidant 4087 Flextend Medtronic 4568 CapsureFix Medtronic 5076 Capsure Fix Novus
Supplement 1. ICD system specifications for individual patients. Ventricular lead denotes right ventricular ICD leads. Coronary sinus leads identified with (LV).
by guest on February 21, 2013circep.ahajournals.org
Dow
nloaded from
Copyright © 2022 FDOKUMEN




















