
Motivational determinants of interpersonal distress: How interpersonal goals are related to...
14
This article was downloaded by: [Thuringer University & Landesbibliothek] On: 25 May 2012, At: 02:18 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Psychotherapy Research Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/tpsr20 Motivational determinants of interpersonal distress: How interpersonal goals are related to interpersonal problems Andrea Thomas a , Helmut Kirchmann a , Holger Suess b , Sonja Bräutigam a & Bernhard Michael Strauss a a University Hospital Jena, Institute of Psychosocial Medicine and Psychotherapy, Jena, Germany b Burg-Klinik, Stadtlengsfeld, Germany Available online: 08 May 2012 To cite this article: Andrea Thomas, Helmut Kirchmann, Holger Suess, Sonja Bräutigam & Bernhard Michael Strauss (2012): Motivational determinants of interpersonal distress: How interpersonal goals are related to interpersonal problems, Psychotherapy Research, DOI:10.1080/10503307.2012.676531 To link to this article: http://dx.doi.org/10.1080/10503307.2012.676531 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Motivational determinants of interpersonal distress: How interpersonal goals are related to...
This article was downloaded by: [Thuringer University & Landesbibliothek]On: 25 May 2012, At: 02:18Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Psychotherapy ResearchPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/tpsr20
Motivational determinants of interpersonal distress:How interpersonal goals are related to interpersonalproblemsAndrea Thomas a , Helmut Kirchmann a , Holger Suess b , Sonja Bräutigam a & BernhardMichael Strauss aa University Hospital Jena, Institute of Psychosocial Medicine and Psychotherapy, Jena,Germanyb Burg-Klinik, Stadtlengsfeld, Germany
Available online: 08 May 2012
To cite this article: Andrea Thomas, Helmut Kirchmann, Holger Suess, Sonja Bräutigam & Bernhard Michael Strauss (2012):Motivational determinants of interpersonal distress: How interpersonal goals are related to interpersonal problems,Psychotherapy Research, DOI:10.1080/10503307.2012.676531
To link to this article: http://dx.doi.org/10.1080/10503307.2012.676531
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form toanyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses shouldbe independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims,proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly inconnection with or arising out of the use of this material.

Motivational determinants of interpersonal distress: How interpersonalgoals are related to interpersonal problems
ANDREA THOMAS1*, HELMUT KIRCHMANN1, HOLGER SUESS2,
SONJA BRAUTIGAM1, & BERNHARD MICHAEL STRAUSS1
1University Hospital Jena, Institute of Psychosocial Medicine and Psychotherapy, Jena, Germany & 2Burg-Klinik,
Stadtlengsfeld, Germany
(Received 14 April 2011; revised 27 February 2012; accepted 13 March 2012)
AbstractThis study aimed to link interpersonal goals with interpersonal problems and psychological distress and to investigatechanges in these variables during an inpatient psychotherapeutic treatment. Two hundred and fifty-eight patients treated ina psychosomatic hospital completed the German versions of the Circumplex Scales of Interpersonal Values, the Inventory ofInterpersonal Problems, and the Outcome Questionnaire before and at the end of their treatment. Patients initially reporteda strong need for bonding in the CSIV. Especially interpersonal goals related to avoidant, submissive, and altruistic behaviorwere associated with a wide range of different interpersonal problems, and were associated with more psychological distress.At the end of treatment, patients showed no substantial changes in their predominant communal goals, but significantlyreduced submissive goals. Additionally, changes of these goals were associated with changes of various interpersonalproblems and psychological distress. Focusing the value patients place on submissive experiences could help to improveinterpersonal problems.
Keywords: outcome research; interpersonal goals and problems; circumplex model
Interpersonal problems provide a common source of
distress and are therefore focused in psychotherapy
(Horowitz, 2004). In addition, interpersonal pro-
blems affect the nature of the therapeutic alliance
since patients’ interpersonal styles interact with
personal and role characteristics of the therapist,
setting ‘‘complementary’’ forces in motion that
either promote or inhibit therapeutic change
(Gurtman, 2004). Accordingly, current concepts of
almost all psychotherapy traditions more or less refer
to the patient’s interpersonal distress and highlight
the patient’s adaptive and maladaptive relationships
inclusively the therapeutic relationship, e.g. object
relations theory (e.g. Fairbairn, 1952), Relational
Psychoanalysis (Mitchell, 2003), Interpersonal
Reconstructive Therapy (Benjamin, 2003), Schema
Therapy (Young, Klosko, & Weishaar, 2003), or
Integrative Cognitive Therapy for Depression (ICT;
Castonguay, 1996).
In psychotherapy research the Inventory of Inter-
personal Problems (IIP; Horowitz, Alden, Wiggins,
& Pincus, 2000) is a common measure of inter-
personal distress. Findings based upon the IIP relate
to the interpersonal content of a large proportion of
patients’ presenting problems and treatment goals
(e.g. Cain, Pincus, & Grosse Holtforth, 2010; Salzer
et al., 2010). Interpersonal problems have also
shown to predict psychotherapy process and out-
come (e.g. Borkovec, Newman, Pincus, & Lyte,
2002; Ruiz et al., 2004). Changes of interpersonal
problems during psychotherapy are commonly seen
as an indicator of psychotherapy effectiveness
(e.g. Huber, Henrich, & Klug, 2007; Luyten, Low-
yck, & Vermote, 2010; Salzer et al., 2010). Given the
central importance of interpersonal distress in
psychotherapy, it seems reasonable to focus on
factors which might cause interpersonal problems.
In the interpersonal circumplex tradition, a recent
reformulation of the interpersonal circumplex model
(Horowitz et al., 2006) emphasizes interpersonal
motives, which are seen as relevant intraper-
sonal determinants directing an individual’s inter-
personal behavior in order to establish, maintain or
modify interactions with an impact on wellbeing of
the interactants. In this framework, interpersonal
problems are assumed to reflect enduring frustrations
Correspondence concerning this article should be addressed to Andrea Thomas, University Hospital Jena, Institute of Psychosocial
Medicine and Psychotherapy, Jena, Germany. Email: [email protected]
Psychotherapy Research,
2012, 1�13, iFirst article
ISSN 1050-3307 print/ISSN 1468-4381 online # 2012 Society for Psychotherapy Research
http://dx.doi.org/10.1080/10503307.2012.676531
Dow
nloa
ded
by [
Thu
ring
er U
nive
rsity
& L
ande
sbib
lioth
ek]
at 0
2:18
25
May
201
2

of interpersonal goals which are associated with
negative affect, e.g. anger, sadness, anxiety or lone-
liness (Shechtman & Horowitz, 2006). In their over-
view of interpersonal motives in psychotherapy,
Grosse Holtforth, Thomas and Caspar (2010) as-
sumed that insufficient satisfaction of important
interpersonal goals might be an essential origin of
the development and maintenance of psychological
disorders. Accordingly, they consider interpersonal
goals of relevance for the practicing psychotherapist.
A therapist understanding a patient’s problem from a
motivational perspective can help the patient modify
interpersonal goals which consequently may contri-
bute to change the patient’s problematic interpersonal
behavior. On the other hand, a therapist can also
encourage behavior that helps a patient satisfy im-
portant goals that have previously been frustrated.
Furthermore, attuning the therapist’s behavior to the
patient’s goals may foster a maximally beneficial
therapeutic relationship (Grosse Holtforth et al., 2010).
Interpersonal motives refer to motivation that is
directed towards other people. According to current
motivational concepts (e.g. Austin & Vancouver,
1996), interpersonal motives are considered to vary
hierarchically in their level of abstraction. The term
‘‘motive’’ generally describes a higher level of ab-
straction, whereas the term ‘‘goal’’ depicts a more
specific category or narrow level of abstraction
(Horowitz, 2004). Interpersonal motives are con-
ceptualized related to the two broad abstract cate-
gories, agency and communion, at the top of the
hierarchy (Bakan, 1966). An agentic motive empha-
sizes the self as a distinct unit, striving for influence
and control over other people. In contrast, a com-
munal motive is directed towards connection and
solidarity with other people. In this article we will use
the term interpersonal ‘‘goals’’, even if goal con-
structs at a higher level of abstraction are referred.
As an interpersonal measure, the Circumplex
Scales of interpersonal Values (CSIV; Locke, 2000)
was developed to assess interpersonal goals. Follow-
ing the typical structure of common interpersonal
circumplex measures, Locke constructed the CSIV
focusing on the hierarchical organization of goals: 64
items refer to different interpersonal goals and are
organized into eight subscales (or octants) which
assess higher-order categories of interpersonal moti-
vation. The octants are described along the two
dimensions Agency and Communion. Respondents
have to indicate the importance of the particular
interpersonal goal using a 5-point Likert scale from
0 ‘‘not important’’ to 4 ‘‘extremely important’’. Figure
1 shows the circumplex model of interpersonal values
including subscale denominations and item examples.
As reflected in Figure 1, the octants of the
interpersonal circumplex are commonly described
using rotated alphabetical abbreviations (counter-
clockwise), where P/A marks the beginning (A) and
the end (P) of the circle.
There is some evidence that motivational goals
relate to psychopathology and interpersonal pro-
blems. Recent research has distinguished between
approach and avoidance motivation (Elliot & Cov-
ington, 2001). Approach goals are assumed to target
need satisfaction, and avoidance goals the prevention
of need frustration. The Inventory of Approach and
Avoidance Motivation (IAAM; Grosse Holtforth &
Grawe, 2000) is a standardized self-report measure
to assess the intensity of approach and avoidance
goals with some of the subscales also referring to
interpersonal goals. Seven of 14 approach goals (e.g.
Intimacy, Affiliation, Status) and six of nine avoid-
ance goals (e.g. Separation, Deprecation, Humilia-
tion) are considered to be interpersonal in nature.
Using the IAAM, Grosse Holtforth and colleagues
(Grosse Holtforth, Bents, Mauler, & Grawe, 2006;
Grosse Holtforth, Pincus, Grawe, Mauler, & Cas-
tonguay, 2007) determined the associations between
approach and avoidance goals and interpersonal
problems. Results indicated that both strong
approach and strong avoidance goals were related
to interpersonal problems: strong approach goals
(e.g. wishing for greater intimacy, striving for status)
Figure 1. The German version of the Circumplex Scales of
Interpersonal Values. Octants, scales and item examples related
to an octant schema according to Gurtman and Balakrishnan,
1998.
2 A. Thomas et al.
Dow
nloa
ded
by [
Thu
ring
er U
nive
rsity
& L
ande
sbib
lioth
ek]
at 0
2:18
25
May
201
2

were related to interpersonal problems ranging from
being overly nurturant (LM) to being overly dom-
ineering (PA). In contrast, strong avoidance goals
(e.g. avoiding feelings of vulnerability or humiliation)
were related to friendly submissive/submissive
problems ranging from being overly socially avoidant
(FG) to being overly exploitable (JK). However, the
authors only found significant associations with
subscales predominantly describing interpersonal
motivation, and higher associations with interperso-
nal avoidance goals than with approach goals.
Correlation coefficients varied between r�.38 and
r�.35, indicating that there are at least moderate
connections between interpersonal goals and inter-
personal problems.
Berking, Grosse Holtforth, and Jacobi (2003)
examined psychotherapy effects with regard to
changes of motivational goals. To test the
assumptions, 64 inpatients undergoing cognitive
behavioral therapy were assessed using the IAAM
pre�post therapy and diverse outcome measures.
The authors showed that approach and avoidance
goals of predominantly interpersonal content nor-
malized after therapy. Effect sizes ranged from
d�.19 to d�.64. Furthermore, only changes of
avoidance goals were associated with better therapy
outcome indicated by correlations ranging from
r�.18 to r�.42. These findings indicate that
psychotherapy has an impact on changes of motiva-
tional goals, and that changes of specific goals are
relevant for therapy outcome since, at least in part,
outcome depends on changes of specific intentions.
In this study those approach and avoidance goals
predominantly interpersonal in nature turned out to
be the significant ones.
However, the IAAM does not claim to cover the
full range of interpersonal motivation. Converging
the German versions of the IAAM and the CSIV, as
described by Thomas, Locke and Strauss (in press),
each of four interpersonal approach and avoidance
goals referred to CSIV segments. Of the approach
goals, two converged with octant LM, one with
octant PA, and one with octant JK. Of the avoidance
goals, two goals converged with octant LM, one with
octant JK, and one with octant DE. The IAAM
especially did not cover the left segments of the
CSIV circumplex (e.g. ‘‘agentic and separate’’
(octant BC), ‘‘separate’’ (DE), ‘‘submissive and
separate’’ (FG), and ‘‘submissive’’ (HI)). Therefore,
focusing the full range of interpersonal goals could
help to discover specific association patterns between
interpersonal goals and problems.
Based upon the recent interpersonal model
describing interpersonal interactions with a focus
on interpersonal motives (Horowitz, 2004; Horowitz
et al., 2006), the aim of the present study was to
address salient interpersonal goals of psychotherapy
patients, and to examine whether interpersonal goals
determine interpersonal and non-interpersonal
distress as well as changes of interpersonal goals
during psychotherapy.
Specifically, the study intended to replicate and
extend the findings of Grosse Holtforth et al. (2006,
2007) and Berking et al. (2003) addressing the
following research questions: (1) What are the pre-
dominant interpersonal goals of psychotherapy pa-
tients? We assumed patients were indicating
predominant goals of the lower and the right-hand
segments of the circumplex, e.g. valuing the subscales
‘‘submissive and separate’’ (FG), ‘‘submissive’’ (HI),
‘‘submissive and communal’’ (JK), ‘‘communal’’
(LM), and ‘‘agentic and communal’’ (NO). (2)
How are interpersonal goals related to psychological
and interpersonal distress? We expected relationships
between the patients’ predominant interpersonal
goals and general psychological distress; these goals
should also predict psychological distress. Further-
more, there should be differential associations be-
tween interpersonal goals and interpersonal problems
congruent to the appropriate counterpart circumplex
structure: the respective subsets of interpersonal
goals should be positively associated with the appro-
priate counterparts of interpersonal problems. In
addition, we expected that the respective goals would
also predict the appropriate interpersonal problems.
(3) Do interpersonal goals change during psychother-
apy? We assumed that the patients’ predominant
goals should be reduced at post treatment (e.g.
‘‘submissive and separate’’ (FG), ‘‘submissive’’
(HI), ‘‘submissive and communal’’ (JK), ‘‘commu-
nal’’ (LM), and ‘‘agentic and communal’’ (NO)).
Compared to the means of a reference sample, the
patient sample should at least show a tendency to
‘‘normalize’’during psychotherapy. (4) Do changes of
interpersonal goals associate with changes of psycho-
logical and interpersonal distress? We assumed rela-
tionships between pre�post changes of the
patients’ predominant goals and pre�post changes
of interpersonal problems and psychological distress.
Method
Design and Procedure
The study was designed as a naturalistic pre�post
survey within a psychosomatic rehabilitation hospital
(Burg-Klinik Stadtlengsfeld) providing inpatient
psychotherapy. Usually, psychosomatic patients
spend a 6-week treatment in the unit. Based on
informed consent and after the study was approved
by the Ethics Commission of the University of Jena,
the patients filled out an assessment battery
Interpersonal goals and interpersonal problems 3
Dow
nloa
ded
by [
Thu
ring
er U
nive
rsity
& L
ande
sbib
lioth
ek]
at 0
2:18
25
May
201
2
including the German Circumplex Scales of Inter-
personal Values (CSIV), the short version (32 items)
of the German Inventory of Interpersonal Problems
(IIP-32), and the German version of the Outcome
Questionnaire (OQ-45) at the beginning and at the
end of their treatment.
Samples
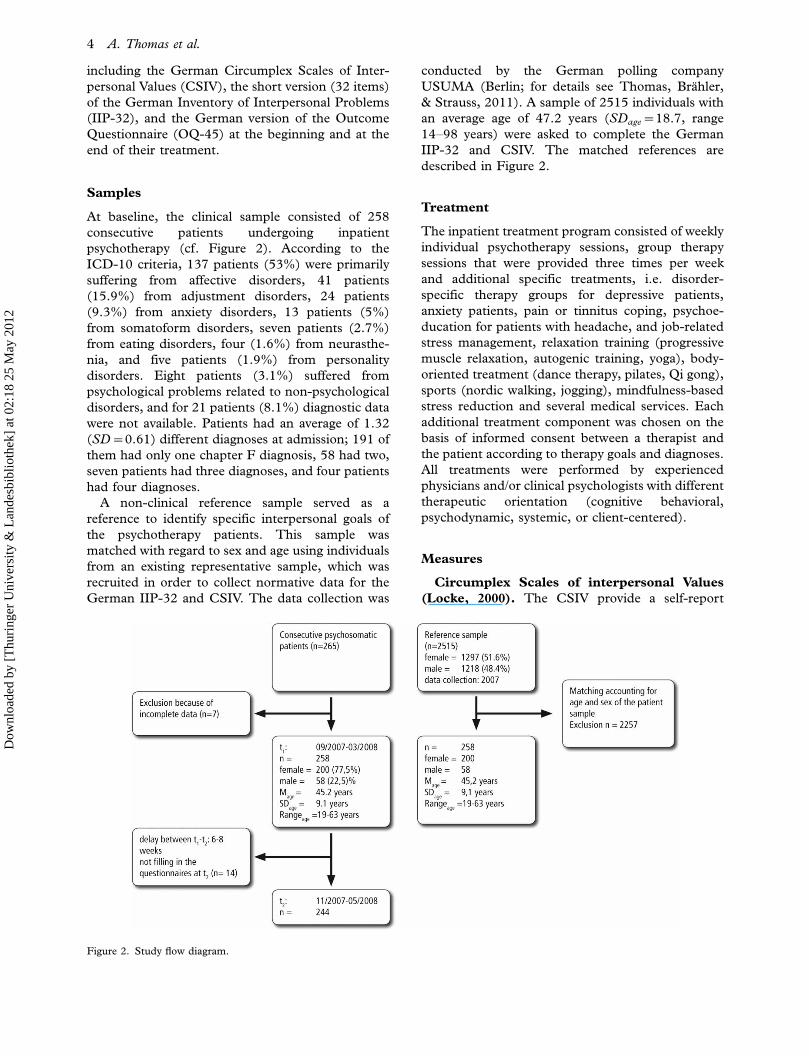
At baseline, the clinical sample consisted of 258
consecutive patients undergoing inpatient
psychotherapy (cf. Figure 2). According to the
ICD-10 criteria, 137 patients (53%) were primarily
suffering from affective disorders, 41 patients
(15.9%) from adjustment disorders, 24 patients
(9.3%) from anxiety disorders, 13 patients (5%)
from somatoform disorders, seven patients (2.7%)
from eating disorders, four (1.6%) from neurasthe-
nia, and five patients (1.9%) from personality
disorders. Eight patients (3.1%) suffered from
psychological problems related to non-psychological
disorders, and for 21 patients (8.1%) diagnostic data
were not available. Patients had an average of 1.32
(SD�0.61) different diagnoses at admission; 191 of
them had only one chapter F diagnosis, 58 had two,
seven patients had three diagnoses, and four patients
had four diagnoses.
A non-clinical reference sample served as a
reference to identify specific interpersonal goals of
the psychotherapy patients. This sample was
matched with regard to sex and age using individuals
from an existing representative sample, which was
recruited in order to collect normative data for the
German IIP-32 and CSIV. The data collection was
conducted by the German polling company
USUMA (Berlin; for details see Thomas, Brahler,
& Strauss, 2011). A sample of 2515 individuals with
an average age of 47.2 years (SDage�18.7, range
14�98 years) were asked to complete the German
IIP-32 and CSIV. The matched references are
described in Figure 2.
Treatment
The inpatient treatment program consisted of weekly
individual psychotherapy sessions, group therapy
sessions that were provided three times per week
and additional specific treatments, i.e. disorder-
specific therapy groups for depressive patients,
anxiety patients, pain or tinnitus coping, psychoe-
ducation for patients with headache, and job-related
stress management, relaxation training (progressive
muscle relaxation, autogenic training, yoga), body-
oriented treatment (dance therapy, pilates, Qi gong),
sports (nordic walking, jogging), mindfulness-based
stress reduction and several medical services. Each
additional treatment component was chosen on the
basis of informed consent between a therapist and
the patient according to therapy goals and diagnoses.
All treatments were performed by experienced
physicians and/or clinical psychologists with different
therapeutic orientation (cognitive behavioral,
psychodynamic, systemic, or client-centered).
Measures
Circumplex Scales of interpersonal Values
(Locke, 2000). The CSIV provide a self-report
Figure 2. Study flow diagram.
4 A. Thomas et al.
Dow
nloa
ded
by [
Thu
ring
er U
nive
rsity
& L
ande
sbib
lioth
ek]
at 0
2:18
25
May
201
2

measure of interpersonal motivation assessing the
full range of agentic and communal values as
described above. The eight 8-item subscales of the
measure were shown to have good internal consis-
tency (range .76�.86) and test�retest reliability
(range .76�.88). The CSIV showed circumplex
structure as well as convergent and discriminant
validity. Thomas et al. (in press) were able to
demonstrate that the subscales of the German
version (Inventar zur Erfassung interpersonaler Mo-
tive, IIM) also show good internal consistency (range
.71�.86) and test�retest reliability (range .82�.87), a
circumplex structure, and convergent and divergent
validity with measures of interpersonal traits (Inter-
personal Adjective List, IAL; Jacobs & Scholl, 2005),
interpersonal problems (32-item version of the In-
ventory of Interpersonal Problems Circumplex, IIP-
32; Thomas et al., 2011), and interpersonal goals
(Inventory of Approach and Avoidance Motivation,
IAAM; Grosse Holtforth & Grawe, 2000). The
measure also revealed discriminative validity with
IIM profiles differentiating social phobic patients
and healthy controls.
Inventory of Interpersonal Problems
(Horowitz et al., 2000). The 32-item version of
the IIP (IIP-32; Thomas et al., 2011) is the German
short version of the IIP-C and assesses maladaptive
behavioral styles associated with each octant of
the interpersonal circumplex as described above.
The measure consists of eight 4-item subscales.
The items are divided into two sections: issues one
‘‘finds hard to do with other people’’ and issues that
one ‘‘does too much’’. The authors showed that the
subscales have good internal consistency (range .60�.85), a circumplex structure, and convergent and
divergent validity with German measures of symp-
tom distress (Symptom Checklist, SCL-27; Hardt,
Egle, Kappis, Hessel, & Brahler, 2004; Outcome
Questionnaire, OQ-45.2; Lambert, Hannover, Nissl-
muller, Richard, & Kordy, 2002).
Outcome Questionnaire (German version:
Ergebnisfragebogen; Lambert et al., 2002).
The Outcome Questionnaire (OQ-45.2) was origin-
ally developed by Lambert et al. (1996) as a
standardized measure for assessing psychotherapy
outcome. The measure includes items relevant to
three domains central to mental health: subjective
discomfort, interpersonal relations, and social role
performance. The OQ-Total score is computed by
addition of the three subscale scores and appears
promising as a measure of general psychological
distress (Umphress, Lambert, Smart, Barlow, &
Clouse, 1997). The OQ-45.2 appears to have high
reliability (internal consistency between .71 and .93),
evidence to suggest good concurrent and construct
validity of the total score and sensitivity to change
(Haug, Puschner, Lambert, & Kordy, 2004).
Power Analysis
Because patients were treated by different therapists,
the design of the study implicated a possible nested
therapists’ effect. Checking for this effect, the
intraclass correlation coefficients (ICC, see Hedges
and Hedberg, 2007) were calculated for all subscales
of the measures. The ICC varied between ICC�.00
and ICC�.08 (MICC�.02, SDICC�.03), with most
of the subscales containing an ICCB.05, and two
subscales containing ICCs between .07 and .08.
MICC was used to adjust the real sample size to
take account of the possible therapists’ effect in
power analysis. Following Kish (1965), the design
effect (DEFF) is computed by: DEFF�1�ICC *
(average cluster size 1). We used DEFF to correct
our sample size as follows: Nadjusted�N/DEFF. With
an average cluster size of n�13 patients per thera-
pist, Nadjusted�211 patients resulted. Accordingly,
assuming an alpha error of 5% (significance
level�.05; two-tailed) pre�post differences with
small effects of d�0.2 by Cohen (1988) were
detected with a power of 89% using G-Power 2.0
(Erdfelder et al., 1996).
Statistical Analysis
Differences in interpersonal goals between the two
samples were calculated using t-tests to account for
failures of variance homogeneity. The alpha level was
adjusted according to Bonferroni. Effect sizes (Co-
hen’s d) were calculated using the means and the
pooled standard deviation of the two samples.
Pearson correlations and stepwise regressions were
calculated to analyze the associations of interperso-
nal goals with interpersonal problems, and psycho-
logical distress. Changes of interpersonal goals were
tested using General Linear Modeling (GLM) with
the within-subject variables ‘‘time’’ and ‘‘subscale’’,
as well as post hoc analyses. Because the ICC did not
exceed the threshold of ICC�.10 (Raudenbush &
Bryk, 2002), we did not apply hierarchical analyses,
but accounted for the possible design effect in the
power analysis and the computation of t-values
following the GLM analysis (see Table II). In order
to test the hypothesis that improvement of inter-
personal problems and psychological distress are
related to changes in interpersonal goals, we
computed Pearson correlations and stepwise regres-
sions with reliable change indices of all the CSIV and
IIP subscale scores and the reliable change index of
the OQ total score. Reliable change indices were
Interpersonal goals and interpersonal problems 5
Dow
nloa
ded
by [
Thu
ring
er U
nive
rsity
& L
ande
sbib
lioth
ek]
at 0
2:18
25
May
201
2

calculated according to the Gulliksen-Lord-Nowick
(GLN) method described by Hsu (1989). The GLN
method takes regression to the mean into account,
implying that more extreme scores will tend to
become less extreme over repeated measures,
because of imperfect reliability. The GLN method
attempts to control for this potential confound by
including a reference mean toward which scores
would tend to regress. In the present study, the
means and standard deviations of the reference
sample were used as hypothesized population scores
towards which the patients’ scores would be regres-
sing. The alpha level was adjusted according to
Bonferroni. All statistical calculations were
performed using the SPSS program (version 16.0).
Results
Identification of Specific Interpersonal Goals
Relevant for Psychotherapy Patients
Table II summarizes the average CSIV subscale
scores of the patients and the reference sample.
In Figure 3 the CSIV scores of both groups are
mapped within the circumplex structure. Regarding
interpersonal goals, the patients’ profile is slightly
shifted into the communal part of the circumplex
(cf. Figure 3). The clinical and reference samples
differed in some of the average scale scores of the
CSIV (cf. Table II). Patients reported significantly
stronger intensities of ‘‘communal’’ (LM, t�3.48,
df�510, p�.001, d�.31) and ‘‘agentic and com-
munal’’ goals (octant NO, t�5.99, df�509,
pB.001, d�.52) than references as well as on the
dimensional score of communion (COM, t�7.03,
df�509, pB.001, d�.62), indicating the patients’
predominant need for bonding. Accordingly, they
reported a significantly weaker subjective impor-
tance of ‘‘agentic and separate’’ (octant BC,
t�7.39, df�516, pB.001, d�.65) and ‘‘separate’’
goals (octant DE, t�5.40, df�516, pB.001,
d�.47). However, goals related to the subscales of
‘‘submissive and separate’’ (octant FG), ‘‘submis-
sive’’ (octant HI), and ‘‘submissive and communal’’
(octant JK) were valued as important as valued by
the reference sample.
Associations of Interpersonal Goals with
Interpersonal Problems and Psychological
Distress
Table I summarizes the correlations of interpersonal
goals, interpersonal problems, and overall psychological
Figure 3. Profiles of patients (pre/post) and references concerning interpersonal goals. Profiles reflect unipsatized stanine scores.
6 A. Thomas et al.
Dow
nloa
ded
by [
Thu
ring
er U
nive
rsity
& L
ande
sbib
lioth
ek]
at 0
2:18
25
May
201
2
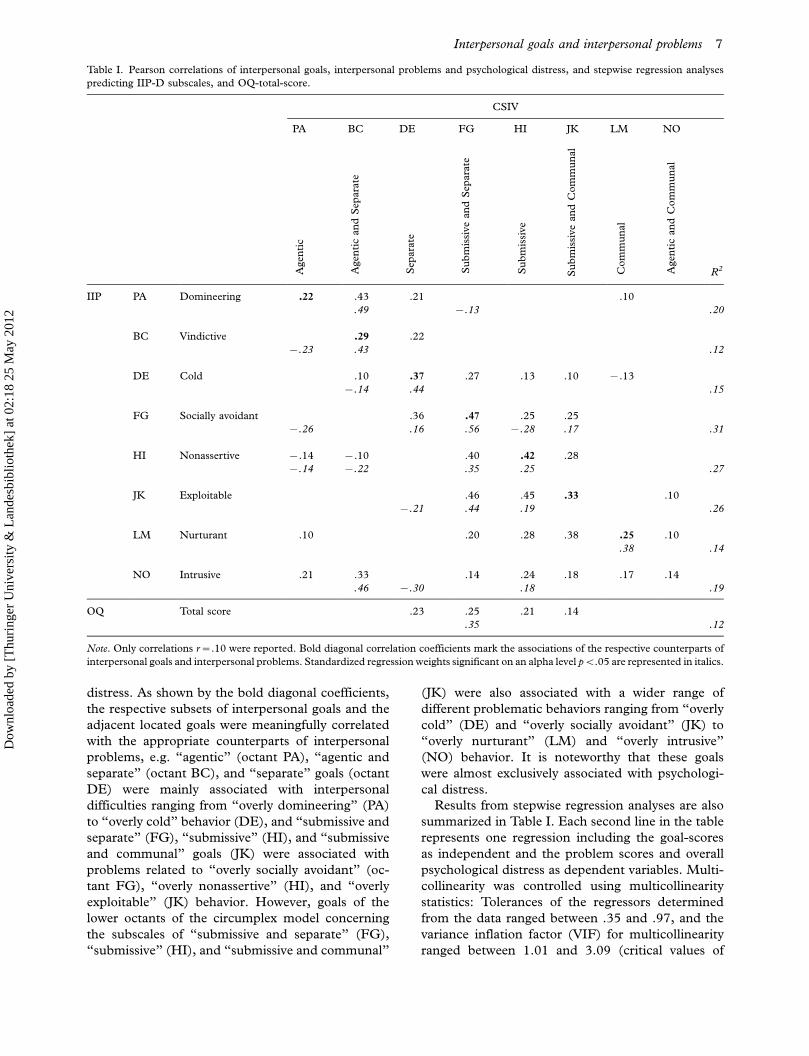
distress. As shown by the bold diagonal coefficients,
the respective subsets of interpersonal goals and the
adjacent located goals were meaningfully correlated
with the appropriate counterparts of interpersonal
problems, e.g. ‘‘agentic’’ (octant PA), ‘‘agentic and
separate’’ (octant BC), and ‘‘separate’’ goals (octant
DE) were mainly associated with interpersonal
difficulties ranging from ‘‘overly domineering’’ (PA)
to ‘‘overly cold’’ behavior (DE), and ‘‘submissive and
separate’’ (FG), ‘‘submissive’’ (HI), and ‘‘submissive
and communal’’ goals (JK) were associated with
problems related to ‘‘overly socially avoidant’’ (oc-
tant FG), ‘‘overly nonassertive’’ (HI), and ‘‘overly
exploitable’’ (JK) behavior. However, goals of the
lower octants of the circumplex model concerning
the subscales of ‘‘submissive and separate’’ (FG),
‘‘submissive’’ (HI), and ‘‘submissive and communal’’
(JK) were also associated with a wider range of
different problematic behaviors ranging from ‘‘overly
cold’’ (DE) and ‘‘overly socially avoidant’’ (JK) to
‘‘overly nurturant’’ (LM) and ‘‘overly intrusive’’
(NO) behavior. It is noteworthy that these goals
were almost exclusively associated with psychologi-
cal distress.
Results from stepwise regression analyses are also
summarized in Table I. Each second line in the table
represents one regression including the goal-scores
as independent and the problem scores and overall
psychological distress as dependent variables. Multi-
collinearity was controlled using multicollinearity
statistics: Tolerances of the regressors determined
from the data ranged between .35 and .97, and the
variance inflation factor (VIF) for multicollinearity
ranged between 1.01 and 3.09 (critical values of
Table I. Pearson correlations of interpersonal goals, interpersonal problems and psychological distress, and stepwise regression analyses
predicting IIP-D subscales, and OQ-total-score.
CSIV
PA BC DE FG HI JK LM NO
Agen
tic
Agen
tic
an
dS
epara
te
Sep
ara
te
Su
bm
issi
ve
an
dS
epara
te
Su
bm
issi
ve
Su
bm
issi
ve
an
dC
om
mu
nal
Com
mu
nal
Agen
tic
an
dC
om
mu
nal
R2
IIP PA Domineering .22 .43 .21 .10
.49 �.13 .20
BC Vindictive .29 .22
�.23 .43 .12
DE Cold .10 .37 .27 .13 .10 �.13
�.14 .44 .15
FG Socially avoidant .36 .47 .25 .25
�.26 .16 .56 �.28 .17 .31
HI Nonassertive �.14 �.10 .40 .42 .28
�.14 �.22 .35 .25 .27
JK Exploitable .46 .45 .33 .10
�.21 .44 .19 .26
LM Nurturant .10 .20 .28 .38 .25 .10
.38 .14
NO Intrusive .21 .33 .14 .24 .18 .17 .14
.46 �.30 .18 .19
OQ Total score .23 .25 .21 .14
.35 .12
Note. Only correlations r�.10 were reported. Bold diagonal correlation coefficients mark the associations of the respective counterparts of
interpersonal goals and interpersonal problems. Standardized regression weights significant on an alpha level pB.05 are represented in italics.
Interpersonal goals and interpersonal problems 7
Dow
nloa
ded
by [
Thu
ring
er U
nive
rsity
& L
ande
sbib
lioth
ek]
at 0
2:18
25
May
201
2

multicollinearity are defined as follows:
toleranceB.20; VIF�5; O’Brien, 2007). Related
to interpersonal problems, interpersonal goals
explained 12�31% of the variance in each subscale
of the IIP, with the highest explained variance for the
lower octant IIP-D subscales (e.g. ‘‘overly socially
avoidant’’, octant FG), and the lowest for the
subscale ‘‘overly vindictive’’ (BC). All types of
interpersonal problems could be predicted signifi-
cantly by interpersonal goals; each of the 12 best-
fitting regression equations reflected a different
subset of interpersonal goals as predictors. Con-
forming to our hypothesis, especially interpersonal
goals located on the left side of the circumplex (e.g.
octants BC ‘‘agentic and separate’’, and DE ‘‘sepa-
rate’’) predicted interpersonal problems of the left
side (e.g. BC ‘‘overly vindictive’’, DE ‘‘overly cold’’);
interpersonal goals of the lower octants (e.g. FG
‘‘submissive and separate’’, and HI ‘‘submissive’’)
predicted the appropriate interpersonal problems
(e.g. FG ‘‘overly socially avoidant’’, HI ‘‘overly
nonassertive’’, and JK ‘‘overly exploitable’’), and
‘‘communal’’ goals (octant LM) predicted the ap-
propriate interpersonal problems of ‘‘overly nurtur-
ant’’(octant LM). In contrast, ‘‘submissive and
communal’’ (JK) and especially ‘‘agentic and com-
munal’’ goals (NO) did not explain a remarkable
amount of variance of any problematic interpersonal
behavior. Regarding psychopathology, psychological
distress was exclusively predicted by ‘‘submissive and
separate’’ goals (FG).
Changes of Interpersonal Goals, Problems and
Psychological Distress During Treatment
To assess changes of interpersonal goals during
treatment, General Linear Modeling (GLM) with
repeated measures was conducted. GLM revealed
significant main effects for the within-subject vari-
ables ‘‘time’’ (Hotelings trace: F(1,239)�13.85,
pB.001, h2�.06) and ‘‘subscale’’ (Hotelings trace:
F(7,233)�53.51; pB.001, h2�.62) as well as a
significant interaction effect (‘‘time�subscale’’,
F(7,233)�6.60, pB.001, h2�.17).
Figure 3 and Table II illustrate the average
changes of the interpersonal goals. Post hoc paired
t-tests showed that the clinical sample decreased
slightly but significantly with respect to ‘‘submissive
and separate’’ (FG), ‘‘submissive’’ (HI), and ‘‘sub-
missive and communal’’ goals (JK), with patients
even changing to lower scores than the references.
However, there were only slight changes of the
Table II. Interpersonal goals of the patients (pre/post) and the reference sample.
Octant CSIV subscale MPre (SD) MPost (SD) MR (SD) t-value (tcorrected) dPre/Post
PA Agentic 2.43 2.49 2.46 �1.90 .12
(.59) (.54) (.50) (�1.35)
BC Agentic and Separate 1.37 1.37 1.82 �.16 .02
(.67) (.62) (.68) (�.16)
DE Separate 1.29 1.27 1.62 .49 .03
(.68) (.69) (.72) (.47)
FG Submissive and Separate 2.16 1.98 2.14 4.46* .24
(.78) (.75) (.70) (4.21*)
HI Submissive 2.26 2.06 2.23 4.91* .26
(.80) (.73) (.60) (4.91*)
JK Submissive and Communal 2.60 2.40 2.52 5.70* .31
(.67) (.62) (.52) (5.39*)
LM Communal 2.92 2.85 2.74 2.50 .12
(.62) (.57) (.55) (2.36)
NO Agentic and Communal 3.13 3.07 2.84 1.93 .11
(.57) (.52) (.55) (1.73)
Dimension
A Agency �.08 .12 �.01 �5.96* .30
(.69) (.63) (.44) (�5.35*)
C Communion .50 .45 .09 1.89 .08
(.64) (.59) (.69) (1.70)
Mean Total score �.06 �.20 �.05 3.72* .20
(.71) (.67) (.65) (3.34*)
Note. Mpre (SD) �patients’ mean and standard deviation before treatment; Mpost (SD)�patients’ mean and standard deviation post
treatment; MR (SD)�mean and standard deviation of the reference sample; t�t-value of paired t-test, p�p-value; tcorrected accounted for
the design effect following the formula tcorrected�M/SE*�DEFF with DEFF �1� ICCsubscale * (average cluster size �1); dPre/Post �effect
size Cohen’s d of the differences between the means of the patients pre/post. * indicates significant group differences with Bonferroni
corrected pB.006.
8 A. Thomas et al.
Dow
nloa
ded
by [
Thu
ring
er U
nive
rsity
& L
ande
sbib
lioth
ek]
at 0
2:18
25
May
201
2
predominant ‘‘communal’’ (LM) and ‘‘agentic and
communal’’ (NO) goals.
Associations Between Changes of Interpersonal
Goals and Interpersonal Problems
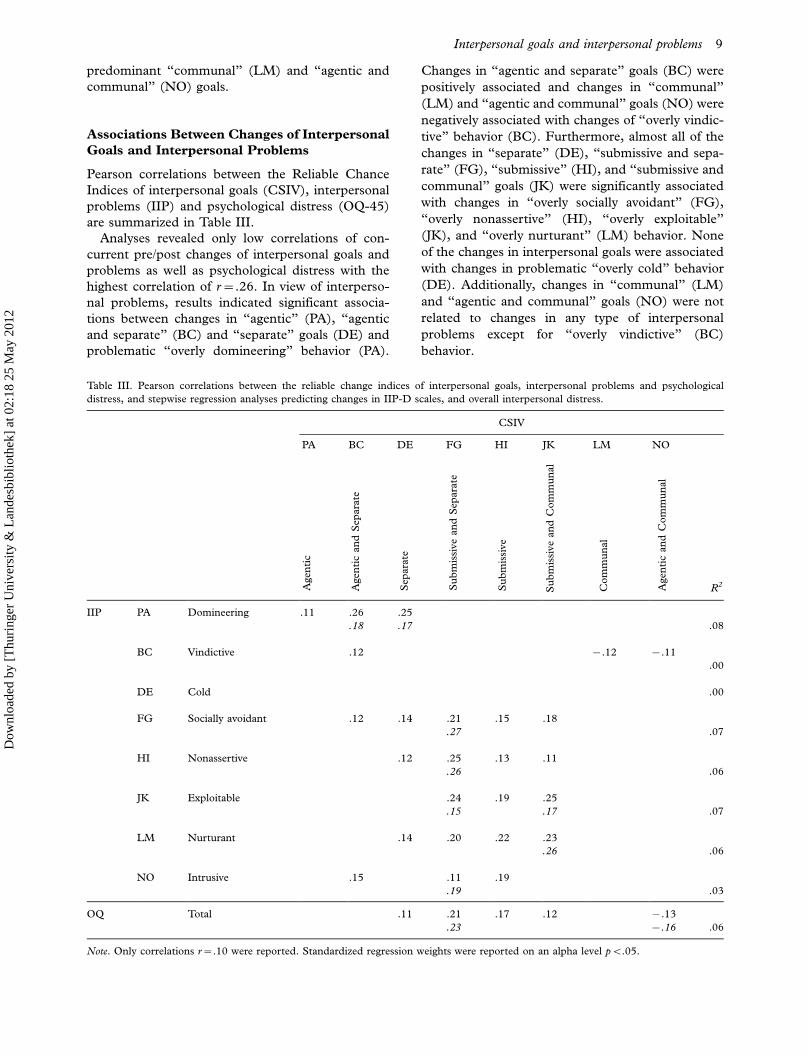
Pearson correlations between the Reliable Chance
Indices of interpersonal goals (CSIV), interpersonal
problems (IIP) and psychological distress (OQ-45)
are summarized in Table III.
Analyses revealed only low correlations of con-
current pre/post changes of interpersonal goals and
problems as well as psychological distress with the
highest correlation of r�.26. In view of interperso-
nal problems, results indicated significant associa-
tions between changes in ‘‘agentic’’ (PA), ‘‘agentic
and separate’’ (BC) and ‘‘separate’’ goals (DE) and
problematic ‘‘overly domineering’’ behavior (PA).
Changes in ‘‘agentic and separate’’ goals (BC) were
positively associated and changes in ‘‘communal’’
(LM) and ‘‘agentic and communal’’ goals (NO) were
negatively associated with changes of ‘‘overly vindic-
tive’’ behavior (BC). Furthermore, almost all of the
changes in ‘‘separate’’ (DE), ‘‘submissive and sepa-
rate’’ (FG), ‘‘submissive’’ (HI), and ‘‘submissive and
communal’’ goals (JK) were significantly associated
with changes in ‘‘overly socially avoidant’’ (FG),
‘‘overly nonassertive’’ (HI), ‘‘overly exploitable’’
(JK), and ‘‘overly nurturant’’ (LM) behavior. None
of the changes in interpersonal goals were associated
with changes in problematic ‘‘overly cold’’ behavior
(DE). Additionally, changes in ‘‘communal’’ (LM)
and ‘‘agentic and communal’’ goals (NO) were not
related to changes in any type of interpersonal
problems except for ‘‘overly vindictive’’ (BC)
behavior.
Table III. Pearson correlations between the reliable change indices of interpersonal goals, interpersonal problems and psychological
distress, and stepwise regression analyses predicting changes in IIP-D scales, and overall interpersonal distress.
CSIV
PA BC DE FG HI JK LM NO
Agen
tic
Agen
tic
an
dS
epara
te
Sep
ara
te
Su
bm
issi
ve
an
dS
epara
te
Su
bm
issi
ve
Su
bm
issi
ve
an
dC
om
mu
nal
Com
mu
nal
Agen
tic
an
dC
om
mu
nal
R2
IIP PA Domineering .11 .26 .25
.18 .17 .08
BC Vindictive .12 �.12 �.11
.00
DE Cold .00
FG Socially avoidant .12 .14 .21 .15 .18
.27 .07
HI Nonassertive .12 .25 .13 .11
.26 .06
JK Exploitable .24 .19 .25
.15 .17 .07
LM Nurturant .14 .20 .22 .23
.26 .06
NO Intrusive .15 .11 .19
.19 .03
OQ Total .11 .21 .17 .12 �.13
.23 �.16 .06
Note. Only correlations r�.10 were reported. Standardized regression weights were reported on an alpha level pB.05.
Interpersonal goals and interpersonal problems 9
Dow
nloa
ded
by [
Thu
ring
er U
nive
rsity
& L
ande
sbib
lioth
ek]
at 0
2:18
25
May
201
2

With regard to changes in psychological distress,
there were significant positive correlations with
changes of ‘‘separate’’ (DE), ‘‘submissive and sepa-
rate’’ (FG), ‘‘submissive’’ (HI), and ‘‘submissive and
communal’’ goals (JK) and a negative association
with changes of ‘‘agentic and communal’’ goals
(NO).
Results from stepwise regression analyses are also
summarized in Table III, again with each line
representing one regression with interpersonal goals
as independent variables and interpersonal problems
and psychological distress as dependent variables.
Related to changes in interpersonal problems and
psychological distress, changes in interpersonal goals
explained a maximum of 8% of the variance, with
the highest explained variance accounted for by
changes of the IIP-D scale ‘‘overly domineering’’
(PA), and the lowest for changes of the subscales
‘‘overly vindictive’’ (BC) and ‘‘overly cold’’ (DE).
Corresponding to the low correlations, in general, bweights were only small in magnitude. According to
our hypothesis, changes in ‘‘agentic and separate’’
(BC) and ‘‘separate’’ goals (DE) were meaningful
predictors of changes in interpersonal problems of
‘‘overly domineering’’ (PA) behavior. Furthermore,
changes in ‘‘submissive and separate’’ goals (FG)
mostly predicted changes in different types of inter-
personal problems, e.g. changes in ‘‘overly socially
avoidant’’ (FG), ‘‘overly nonassertive’’ (HI), ‘‘overly
exploitable’’ (JK), and ‘‘overly intrusive’’ (NO)
behavior. Regarding ‘‘overly vindictive’’ (BC) and
‘‘overly cold’’ (DE) behavior, none of the changes in
interpersonal goals were shown as meaningful pre-
dictors. Furthermore, changes in ‘‘communal’’
(LM), ‘‘agentic and communal’’ (NO) and ‘‘sub-
missive’’ goals (HI) did not predict changes in any
type of interpersonal problems.
With regard to changes in psychological distress,
the best-fitting regression equation also identified
changes in goals of the octant ‘‘submissive and
separate’’ (FG) as the most relevant predictor.
Discussion
Interpersonal impairment has been shown to be of
therapeutic relevance in psychotherapy from theore-
tical and clinical perspectives (e.g. Benjamin, 2003;
Horowitz & Strack, 2010; Kiesler, 1996; McLemore
& Benjamin, 1979). Different theorists, such as
Leary (1957), Horowitz (2004) and or Benjamin
(2003), have emphasized adult psychopathology as
being primarily expressed through developmentally
induced dysfunctional interpersonal relationship
patterns. Recent empirical studies provide ample
evidence for the association between interpersonal
problems, psychopathological symptoms, psy-
chotherapy process, and outcome (e.g. Borkovec
et al., 2002; Hardy, Tracey, Glidden-Tracey, Hess,
& Rohlfing, 2011; Huber et al., 2007; Salzer et al.,
2010). Accordingly, many therapeutic interventions,
especially psychodynamic and interpersonal ones,
target the patient’s maladaptive interpersonal pat-
terns using specific techniques (such as interpersonal
feedback, cf. Kiesler & Van Denburg, 1993) in order
to understand the patients’ perceptions, needs, and
feelings (Benjamin, 2003; Strupp & Binder, 1984).
The major task of the therapist is to disrupt the
maladaptive interpersonal pattern of the patient by
responding in unexpected and surprising ways,
allowing for new interpersonal experiences, and
changing fundamental perceptions, needs and feel-
ings that shape the patient’s reactions in interperso-
nal situations.
A recent theoretical concept concerning interper-
sonal motivation assumes insufficient satisfaction of
important interpersonal goals as an essential origin
of the development and maintenance of psychologi-
cal disorders (Horowitz, 2004). According to this
concept, interpersonal problems can be seen as
frustrated salient interpersonal motives reflecting a
perceived discrepancy between individual goals and
the consequences of interpersonal interactions with
an impact on affective reactions to an interpersonal
encounter and psychological distress as well
(Horowitz et al., 2006). Accordingly, Grosse
Holtforth et al. (2010) consider interpersonal goals
of relevance for the practicing psychotherapist:
Focusing the motivational issues of a patient’s
problem could help to modify the patient’s inter-
personal goals and may contribute to change the
problematic interpersonal behavior. Additionally, the
therapist should encourage behavior that helps a
patient to satisfy important goals that have
previously been frustrated. Beyond these strategies,
attuning the therapist’s behavior to the patient’s
goals may foster a maximally beneficial therapeutic
relationship (Grosse Holtforth et al., 2010).
Related to this model, our study focused on the
relevance of interpersonal goals in psychotherapy
patients and the associations between changes of
interpersonal goals, problematic interpersonal
behavior, and symptomatology.
We were able to show that psychosomatic patients
undergoing inpatient psychotherapy in a psychoso-
matic rehabilitation hospital valued communal goals
significantly more strongly than individuals of a non-
clinical reference sample at onset. The patients
revealed a special need for bonding described by
strong intentions to receive harmony, support and
approval from other people. In view of the relation-
ship between interpersonal goals and interpersonal
distress, the results point to a substantial importance
10 A. Thomas et al.
Dow
nloa
ded
by [
Thu
ring
er U
nive
rsity
& L
ande
sbib
lioth
ek]
at 0
2:18
25
May
201
2

of specific goals for specific types of interpersonal
problems. However, especially separate and submis-
sive goals were also related to different types of
problematic interpersonal behavior. Moreover, they
were also associated with more psychological
distress, and predicted distress. In contrast, the
predominant communal goals reflecting the patients’
strong need for bonding did not predict any proble-
matic behavior except for overly nurturant behavior.
Consistent with the findings of Grosse Holtforth
et al. (2007), associations varied between r��.48
and r�.48 and explained low percentages of var-
iance (between 12% and 31%), both also indicating
other potential sources of interpersonal problems
and psychopathology, and the fact that specific
interpersonal problems might affect different goals in
different people. Furthermore, insufficient learning,
aversive circumstances, etc. may also cause inter-
personal problems and psychological distress.
Regarding changes in interpersonal goals during
inpatient treatment, we found only slight but
significant changes in submissive goal types.
In contrast, there were only slight changes of the
predominant interpersonal characteristics of the
patients, i.e. higher scores of ‘‘communal’’ (LM)
and ‘‘agentic and communal’’ goals (NO) before
treatment. Additionally, changes in specific inter-
personal goals were associated with changes in
specific types of interpersonal problems and psycho-
logical distress. Moreover, especially changes in
‘‘submissive and separate’’ goals (FG) almost exclu-
sively predicted changes in a wide range of different
types of interpersonal problems and changes in
psychological distress. Again, the associations and
explained variances were only small in magnitude,
suggesting other mechanisms to be more relevant in
reducing interpersonal problems and psychological
distress.
However, our results are consistent with the
empirical findings by Grosse Holtforth and collea-
gues (2006, 2007) and Berking and colleagues
(2003). They showed that strong approach goals
(referring to need satisfaction) and especially strong
avoidance goals (preventing need frustration) were
associated with different types of interpersonal
problems, e.g. approach goals related to friendly
and friendly-dominant problems, and avoidance
goals were related to friendly-submissive and sub-
missive interpersonal problems. Berking et al. de-
scribed changes of interpersonal avoidance goals as
being associated with changes of outcome measures
and Grosse Holtforth et al. (2007) assumed a
‘‘suppressive’’ influence of strong avoidance goals
especially on need satisfaction of approach goals.
Although not differentiating between approach
and avoidance goals, ‘‘agentic’’ (PA), ‘‘agentic and
communal’’ (NO), and ‘‘communal’’ goals (LM)
mostly seem to represent approach goals, whereas
‘‘separate’’ (DE), ‘‘submissive and separate’’ (octant
FG), and ‘‘submissive’’ goals (octant HI) may mostly
represent avoidance goals, because they directly
address the prevention of depreciation and abandon-
ment. Since we cannot draw causal conclusions, it
might be that a given interpersonal problem could
have acted as a trigger for the development of
specific interpersonal goals. On the other hand, it
could be hypothesized that a given problematic
interpersonal behavior might be a consequence of
the strengths of specific interpersonal goals, or
specific mechanisms that could explain the
relationship between goals and problems. Although
psychosomatic patients showed an even higher need
for bonding than healthy references, however, the
related ‘‘communal’’ (LM) and ‘‘agentic and com-
munal’’ (NO) approach goals did not turn out to be
meaningful determinants of problematic interperso-
nal behavior and did not substantially change during
treatment. Accordingly, the results indicate that
strong intensities of goals themselves might not cause
problematic interpersonal behavior but rather a
combination of intense goals with specific mechan-
isms, i.e. potential suppression mechanisms of goal
types, such as suppressing behaviors that directly
target the need for bonding. In this respect, ‘‘sub-
missive and separate’’ (FG) and ‘‘submissive’’ goals
(HI) seem to be important aspects of the patients’
interpersonal and overall psychological distress.
Although patients reported these goals with a similar
intensity as references, it could be hypothesized that
these goals might still affect the patients’ distress
because of interference. Given the patients’ need for
bonding, patients might show ambiguous amiable
behavior (e.g. overly withdrawn, submissive and
altruistic behavior) because of their fears of depre-
ciation, conflict and abandonment, underpinning the
potential impact of these fears as a source for
developing psychological distress, e.g. suppressing
behaviors that directly target the need for bonding.
As a consequence, they may invite others to respond
not with affiliating but rather with domineering
behavior. Therefore, in psychotherapy treatment
therapists should question the value patients place
on submissive experiences helping to improve inter-
personal problems.
Our results in summary suggest some extensions
of the interpersonal model to incorporate approach
and avoidance motivation as distinct classes within
the system of interpersonal motivation. The distinc-
tion and localization of interpersonal approach goals
and interpersonal avoidance goals may contribute to
a more detailed understanding of the mechanisms by
Interpersonal goals and interpersonal problems 11
Dow
nloa
ded
by [
Thu
ring
er U
nive
rsity
& L
ande
sbib
lioth
ek]
at 0
2:18
25
May
201
2

which interpersonal motivation influences proble-
matic interpersonal behaviors.
Limitations and Perspectives
The present study has several limitations. The
generalizability of the results is potentially limited,
because our sample exclusively consisted of an
unselected group of inpatients from one hospital in
one country. Additionally, all constructs were only
operationalized by self-report measures. Future stu-
dies are needed to replicate our findings in similar
samples and across diverse samples (e.g. different
diagnostic subgroups). Larger sample sizes should be
used to further examine whether interpersonal goal
subtypes can be found among psychotherapy
patients, and whether they differ in the modification
of interpersonal goals and problems. Since other
studies (e.g. Haase et al., 2008) showed that
extensive changes on an interpersonal level could
not be observed immediately after treatment, but at
follow-up it can be assumed that modifications of
interpersonal goals and problems might occur with
some delay and that the relationship between the
variables might become evident when variations of
changes increase. Accordingly, future studies should
include longitudinal designs with control groups that
consider the delay of interpersonal changes and will
allow causal interpretations of the relationship be-
tween therapy outcome and changes of interpersonal
goals.
Another limitation might be related to the setting,
i.e. a rehabilitation hospital. The patients in our
sample were treated multimodally by different thera-
pists with a variety of therapeutic orientations. It
might be expected that psychotherapists and treat-
ment approaches using more interpersonal techni-
ques could be more effective in changing
interpersonal goals/problems than others which could
not be tested systematically within this study. Future
research should address changes of interpersonal
goals in different psychotherapeutic settings and
orientations. They would also allow for investigations
concerning the relations between specific psychother-
apeutic interventions as well as process variables and
changes of dysfunctional interpersonal issues.
Testing hypotheses related to interpersonal goals
and differentiated changes may help to provide a
clearer understanding of the causal and temporal
relationships between interpersonal goals and inter-
personal/psychological problems. If interpersonal
motivation turns out to have a significant influence
on therapeutic outcome, as Horowitz (2004) and
Grosse Holtforth et al. (2010) propose, effective
interventions should be identified to affect specific
interpersonal goals.
References
Austin, J.T., & Vancouver, J.B. (1996). Goal constructs in
psychology: Structure, process, and content. Psychological
Bulletin, 120(3), 338�375.
Bakan, D. (1966). The duality of human existence. An essay on
psychology and religion. Chicago: Rand McNally.
Benjamin, L.M. (2003). Interpersonal reconstructive therapy:
Promoting change in nonresponders. New York: Guilford Press.
Berking, M., Grosse Holtforth, M., & Jacobi, C. (2003).
Veranderung klinisch relevanter Ziele und Therapieerfolg: Eine
Studie an Patienten wahrend einer stationaren Verhaltensther-
apie [Changes in clinically relevant goals and therapy outcome:
A study with inpatients undergoing cognitive behavioral
therapy]. Psychotherapie, Psychosomatik und Medizinische
Psychologie, 53, 171�177.
Borkovec, T.D., Newman, M.G., Pincus, A.L., & Lyte, R. (2002).
A component analysis of cognitive-behavioral therapy for
generalized anxiety disorder and the role of interpersonal
problems. Journal of Consulting and Clinical Psychology, 70(2),
288�298.
Cain, N., Pincus, A.L., & Grosse Holtforth, M. (2010). Inter-
personal pathoplasticity in social phobia: A clinical replication.
Journal of Personality Assessment, 92(6), 514�527.
Castonguay, L.G. (1996). Integrative cognitive therapy for depression
treatment manual. Unpublished manuscript, The Pennsylvania
State University.
Elliot, A.J., & Covington, M.V. (2001). Approach and avoidance
motivation. Educational Psychology Review, 13(2), 73�92.
Erdfelder, E., Faul, F., & Buchner, A. (1996). GPOWER: A
general power analysis program. Behavior Research Methods,
Instruments, and Computers, 28, 1�11.
Fairbairn, W.R.D. (1952). Psychoanalytic studies of the personality.
London: Tavistock Publications.
Grosse Holtforth, M., Bents, H., Mauler, B., & Grawe, K.
(2006). Interpersonal distress as a mediator between avoidance
goals and goal satisfaction in psychotherapy inpatients. Clinical
Psychology and Psychotherapy, 13, 172�182.
Grosse Holtforth, M., & Grawe, K. (2000). Fragebogen zur
Analyse Motivationaler Schemata (FAMOS). Zeitschrift fur
Klinische Psychologie, 29, 170�179.
Grosse Holtforth, M., Pincus, A., Grawe, K., Mauler, B., &
Castonguay, L.G. (2007). When what you want is not what you
get: Goal importance, goal satisfaction, and interpersonal
problems. Journal of Social and Clinical Psychology, 26(10),
1095�1119.
Grosse Holtforth, M., Thomas, A., & Caspar, F. (2010).
Interpersonal motives. In L.M. Horowitz & S. Strack (Eds.),
Handbook of interpersonal psychology: Theory, research, assessment,
and therapeutic interventions (pp. 107�122). New York: Wiley.
Gurtman, M.B. (2004). Relational measures in psychotherapy on
process and outcome: A commentary on the studies. Journal of
Personality Assessment, 83(3), 248�255.
Gurtman, M.B., & Balakrishnan, J.D. (1998). Circular measure-
ment redux: The analysis and interpretation of interpersonal
circle profiles. Clinical Psychology: Science and Pracice, 5, 344�360.
Haase, M., Frommer, J., Franke, G., Hoffmann, T., Schulze-
Mutzel, J., Jager, S., Grabe, H., Spitzer, C., & Schmitz, N.
(2008). From symptom relief to interpersonal change: Treat-
ment outcome and effectiveness in inpatient psychotherapy.
Psychotherapy Research, 18, 615�624.
Haug, S., Puschner, B., Lambert, M.J., & Kordy, H. (2004).
Veranderungsmessung in der Psychotherapie mit dem Ergeb-
nisfragebogen (EB-45) [Assessment of change in psychother-
apy with the German version of the Outcome Questionnaire
12 A. Thomas et al.
Dow
nloa
ded
by [
Thu
ring
er U
nive
rsity
& L
ande
sbib
lioth
ek]
at 0
2:18
25
May
201
2

(OQ-45)]. Zeitschrift fur Differentielle und Diagnostische
Psychologie, 25(3), 141�151.
Hardt, J., Egle, U.T., Kappis, B., Hessel, A., & Brahler, E. (2004).
Die Symptom Checkliste SCL-27. Psychotherapie.
Psychosomatik und Medizinische Psychologie, 54, 1�10.
Hardy, A.O., Tracey, T.J.G., Glidden-Tracey, C., Hess, T.R., &
Rohlfing, J.E. (2011). Interpersonal contribution to outcome:
the relation of interpersonal distress and symptomatic improve-
ment as a result of psychotherapy. Clinical Psychology &
Psychotherapy, 18, 225�233.
Hedges, L.V., & Hedberg, E. (2007). Interclass correlation values
for planning group-randomized trials in education. Educational
Evaluation and Policy Analysis, 29(1), 60�87.
Horowitz, L.M. (2004). Interpersonal foundations of
psychopathology. Washington DC: American Psychological As-
sociation.
Horowitz, L.M., Alden, L.E., Wiggins, J.S., & Pincus, A.L.
(2000). Inventory of Interpersonal Problems manual. Odessa,
FL: The Psychological Corporation.
Horowitz, L.M., Wilson, K.R., Turan, B., Zolotsev, P., Con-
stantino, M.J., & Henderson, L. (2006). How interpersonal
motives clarify the meaning of interpersonal behavior: A revised
circumplex model. Personality and Social Psychology Review,
10(1), 67�86.
Horowitz, L.M., & Strack, S. (Eds.). (2010). ‘‘Handbook of
interpersonal psychology: Theory, research, assessment and thera-
peutic interventions.’’ New York: Wiley.
Hsu, L.M. (1989). Reliable changes in psychotherapy: Taking
into account regression toward the mean. Behavioral
Assessment, 11, 459�467.
Huber, D., Henrich, G., & Klug, G. (2007). The Inventory of
Interpersonal Problems (IIP): Sensitivity to change.
Psychotherapy Research, 17(4), 474�481.
Jacobs, I., & Scholl, W. (2005). Interpersonale Adjektivliste
(IAL) Die empirische Umsetzung theoretischer Circumplex-
Eigenschaften fur die Messung interpersonaler Stile.
Diagnostica, 51, 145�155.
Kiesler, D.J. (1996). Contemporary interpersonal theory and research:
Personality, psychopathology and psychotherapy. New York: Wiley.
Kiesler, D.J., & Van Denburg, T.F. (1993). Therapeutic impact
disclosure: A last taboo in psychoanalytic theory and practice.
Clinical Psychology & Psychotherapy, 1, 3�13.
Kish, L. (1965). Survey sampling. New York: Wiley & Sons.
Lambert, M.J., Hannover, W., Nisslmuller, K., Richard, M., &
Kordy, H. (2002). Fragebogen zum Ergebnis von Psychother-
apie. Zeitschrift fur Klinische Psychologie und Psychotherapie, 31,
40�47.
Lambert, M.J., Burlingame, G.M., Umphress, V., Hansen, N.B.,
Vermeersch, D.A., Clouse, G.C., & Yanchar, S.C. (1996). The
reliability and validity of the Outcome Questionnaire. Clinical
Psychology and Psychotherapy, 3(4), 249�258.
Leary, T.F. (1957). Interpersonal diagnosis of personality: A func-
tional theory and methodology for personality evaluation. New
York: Ronald.
Locke, K.D. (2000). Circumplex scales of interpersonal values:
reliability, validity, and applicability to interpersonal problems
and personality disorders. Journal of Personality Assessment,
75(2), 249�267.
Luyten, P., Lowyck, B., & Vermote, R. (2010). The relationship
between interpersonal problems and outcome in psychody-
namic hospitalization-based treatment for personality disorders:
A 12-month follow-up study. Psychoanalytic Psychotherapy,
24(4), 417�436.
McLemore, C.W., & Benjamin, L.S. (1979). Whatever happened
to interpersonal diagnosis? A psychosocial alternative to DSM-
III. American Psychologist, 34, 17�34.
Mitchell, S.A. (2003). Bindung und Beziehung. Auf dem Weg zu
einer relationalen Psychoanalyse. Gießen: Psychosozial Verlag.
O’Brien, Robert M. (2007). A caution regarding rules of thumb
for Variance Inflation Factors. Quality and Quantity, 41(5),
673�690.
Raudenbush, S.W., & Bryk, A.S. (2002). Hierarchical linear models
(2nd ed). Newbury Park, CA: Sage.
Ruiz, M., Pincus, A.L., Borkovec, T.D., Echemendia, R.J.,
Castonguay, L.G., & Raguesa, S.A. (2004). Validity of the
Inventory of Interpersonal Problems for predicting outcome:
An investigation with the Pennsylvania Practice Research
Network. Journal of Personality Assessment, 83(3), 213�222.
Salzer, S., Streeck, U., Jaeger, U., Masuhr, O., Warwas, J.,
Leichsenring, F., & Leibing, E. (2010). Der Zusammenhang
von interpersonalen Subtypen und der Veranderung interper-
sonaler Probleme am Beispiel stationarer Psychotherapiepa-
tienten [The relationship between interpersonal subtypes and
the modification of interpersonal problems in psychotherapy
inpatients]. Zeitschrift fur Psychosomatische Medizin und
Psychotherapie, 56, 191�206.
Shechtman, N., & Horowitz, L.M. (2006). Interpersonal and
noninterpersonal interactions, interpersonal motives, and the
effect of frustrated motives. Personality and Social Psychology
Bulletin, 32(8), 1126�1139.
Strupp, H.H., & Binder, J.L. (1984). Psychotherapy in a new key: A
guide to time-limited dynamic psychotherapy. New York: Basic.
Thomas, A., Locke, K., & Strauss, B. (in press). Das Inventar zur
Erfassung interpersonaler Motive: Entwicklung und Validier-
ung einer deutschsprachigen Version der Circumplex Scales of
interpersonal Values. [IIM: Development and validation of a
German form of the Circumplex Scales of interpersonal
values]. Diagnostica.
Thomas, A., Brahler, E., & Strauss, B. (2011). IIP-32: Entwick-
lung, Validierung und Normierung einer Kurzform des In-
ventars zur Erfassung interpersonaler Probleme [IIP-32:
Development, validation and standardization of a short form
of the Inventory of Interpersonal Problems]. Diagnostica, 57,
68�83.
Umphress, V., Lambert, M.J., Smart, D.W., Barlow, S.H., &
Clouse, G.C. (1997). Concurrent and construct validity of the
Outcome Questionnaire. Journal of Psychoeducational
Assessment, 15, 40�55.
Young, J.E., Klosko, J.S., & Weishaar, M.E. (2003). Schema
therapy: A practitioner’s guide. New York: Guilford Press.
Interpersonal goals and interpersonal problems 13
Dow
nloa
ded
by [
Thu
ring
er U
nive
rsity
& L
ande
sbib
lioth
ek]
at 0
2:18
25
May
201
2




















