Brief Interventions and Motivational Interviewing
21
Brief Interventions and Motivational Interviewing Page 1 of 21 PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All Rights Reserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in Oxford Handbooks Online for personal use (for details see Privacy Policy ). Subscriber: University of New Mexico; date: 16 October 2014 Subject: Psychology, Clinical Psychology Online Publication Date: Oct 2014 DOI: 10.1093/oxfordhb/9780199381708.013.007 Brief Interventions and Motivational Interviewing Jennifer Hettema, Christopher C. Wagner, Karen S. Ingersoll, and Jennifer M. Russo The Oxford Handbook of Substance Use Disorders, Volume 2 (Forthcoming) Edited by Kenneth J. Sher Oxford Handbooks Online Abstract and Keywords This chapter focuses on the use of brief interventions for the treatment of alcohol and other substance use disorders and risky use. The authors provide definitions of brief interventions and a rationale for their use. They review the evidence base for brief interventions across primary care, emergency medical, college, and correctional settings, and include analysis of the impact of brief intervention on drinking and drug use and the relative costs of such services. They also describe several widely used frameworks or organizing structures for brief interventions including FRAMES (provide feedback, emphasize responsibility, give advice, menu of options, express empathy, support self-efficacy), SBIRT (screening, brief intervention, and referral to treatment), and the five As (ask, assess, advise, assist, arrange). Finally, the authors discuss the therapeutic approach of motivational interviewing as an interaction style that can be used within the context of many brief intervention structures. Keywords: brief intervention, brief treatment, motivational interviewing Introduction Brief interventions provide a viable means to prevent the development and progression of substance use problems, treat a range of severities of use, and facilitate referral-making for those for whom more intensive treatment may be appropriate. Alcohol use disorders occur among more than 76 million people internationally (WHO, 2004) and rates of illicit substance use reach similar numbers (UNODC, 2009), indicating that the need for effective, efficient treatment is profound. Alcohol and substance use increase the risk for physical, mental health, and social problems (Rehm, 2003) and brief interventions within opportunistic settings promote significant, long- term reductions in use, associated problems, and cost (Fleming, 2002). Motivational interviewing (MI) is an evidence-based practice that is highly applicable to brief interventions and compatible with many recommended brief intervention approaches. This chapter provides an overview of the rationale, definition, and evidence base of brief interventions within different settings, and describes the MI model and its applicability to brief intervention approaches. Overview of Brief Interventions Definition Many terms are used to describe brief interventions, including “simple advice,” “minimal interventions,” “brief counseling,” or “short-term counseling” (Barry, 1999). The definition of “brief” varies widely across settings and even within the context of empirical research. On the continuum of substance abuse care, brief interventions can fill the gap between primary prevention and intensive or specialized treatment and can be implemented with a variety of settings and populations by specialists and nonspecialists. Although brief interventions are often
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Brief Interventions and Motivational Interviewing

Brief Interventions and Motivational Interviewing
Page 1 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
Subject: Psychology,ClinicalPsychologyOnlinePublicationDate: Oct2014
DOI: 10.1093/oxfordhb/9780199381708.013.007
BriefInterventionsandMotivationalInterviewingJenniferHettema,ChristopherC.Wagner,KarenS.Ingersoll,andJenniferM.RussoTheOxfordHandbookofSubstanceUseDisorders,Volume2(Forthcoming)EditedbyKennethJ.Sher
OxfordHandbooksOnline
AbstractandKeywords
Thischapterfocusesontheuseofbriefinterventionsforthetreatmentofalcoholandothersubstanceusedisordersandriskyuse.Theauthorsprovidedefinitionsofbriefinterventionsandarationalefortheiruse.Theyreviewtheevidencebaseforbriefinterventionsacrossprimarycare,emergencymedical,college,andcorrectionalsettings,andincludeanalysisoftheimpactofbriefinterventionondrinkinganddruguseandtherelativecostsofsuchservices.TheyalsodescribeseveralwidelyusedframeworksororganizingstructuresforbriefinterventionsincludingFRAMES(providefeedback,emphasizeresponsibility,giveadvice,menuofoptions,expressempathy,supportself-efficacy),SBIRT(screening,briefintervention,andreferraltotreatment),andthefiveAs(ask,assess,advise,assist,arrange).Finally,theauthorsdiscussthetherapeuticapproachofmotivationalinterviewingasaninteractionstylethatcanbeusedwithinthecontextofmanybriefinterventionstructures.Keywords:briefintervention,brieftreatment,motivationalinterviewing
IntroductionBriefinterventionsprovideaviablemeanstopreventthedevelopmentandprogressionofsubstanceuseproblems,treatarangeofseveritiesofuse,andfacilitatereferral-makingforthoseforwhommoreintensivetreatmentmaybeappropriate.Alcoholusedisordersoccuramongmorethan76millionpeopleinternationally(WHO,2004)andratesofillicitsubstanceusereachsimilarnumbers(UNODC,2009),indicatingthattheneedforeffective,efficienttreatmentisprofound.Alcoholandsubstanceuseincreasetheriskforphysical,mentalhealth,andsocialproblems(Rehm,2003)andbriefinterventionswithinopportunisticsettingspromotesignificant,long-termreductionsinuse,associatedproblems,andcost(Fleming,2002).Motivationalinterviewing(MI)isanevidence-basedpracticethatishighlyapplicabletobriefinterventionsandcompatiblewithmanyrecommendedbriefinterventionapproaches.Thischapterprovidesanoverviewoftherationale,definition,andevidencebaseofbriefinterventionswithindifferentsettings,anddescribestheMImodelanditsapplicabilitytobriefinterventionapproaches.
OverviewofBriefInterventions
DefinitionManytermsareusedtodescribebriefinterventions,including“simpleadvice,”“minimalinterventions,”“briefcounseling,”or“short-termcounseling”(Barry,1999).Thedefinitionof“brief”varieswidelyacrosssettingsandevenwithinthecontextofempiricalresearch.Onthecontinuumofsubstanceabusecare,briefinterventionscanfillthegapbetweenprimarypreventionandintensiveorspecializedtreatmentandcanbeimplementedwithavarietyofsettingsandpopulationsbyspecialistsandnonspecialists.Althoughbriefinterventionsareoften

Brief Interventions and Motivational Interviewing
Page 2 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
associatedwithopportunisticsettingslikeprimarycare,theycanalsobeimplementedinspecialtytreatmentsettingsforalcoholandsubstanceusedisorders.Furthermore,briefinterventionscanbeappliedtothefullrangeofseveritiesofuse,fromriskytodependent,thoughevidenceseemstosuggestthattheymaybemosteffectivewithlessseverepopulations.Targetedbehavioraloutcomesofbriefinterventionsvaryfromtreatmentengagementtodirectreductionofuse.Somehavedifferentiatedbriefinterventionsfrombrieftherapies.Fromthisperspective,briefinterventionsareapproachestohelpclientschangeoneparticularbehaviororaction,suchastreatmentattendance,whilebrieftherapiesaddresslargergoals,suchasmaintainingabstinenceorlonger-termtreatmentadherence(Barry,1999).Briefinterventionsmayalsovaryconsiderablyinthecommunicationstyleandunderlyingmodalityortheorybeingusedtoencouragechange.Inmanyways,briefinterventionscanbeseenasshellsthatcanholdavarietyoftreatmentmodalities.Althoughbriefinterventiontypesvary,manyhaveanemphasisontargetingandincreasingmotivationandrelyontheprinciplesandtechniquesofMI(Libby,2008).Whileformaldefinitionsvarywidely,mostagreethatbriefinterventionsareabodyofpracticesthatsharethecommonelementsofbeingtime-limited,structured,andgoal-oriented.Inaddition,briefinterventionsoftensharecertaincharacteristics,including(a)afocusonreduceddrinkingorharmreductionversusabstinence,(b)deliverybysomeonewhoisnotanaddictionsspecialist,(c)beingdirectedatriskyornondependentversusdependentsubstanceusers,and(d)attentiontotheconstructofmotivation(Moyeretal.,2002).Whilethediversityofbriefinterventionformatsincreasesavailabilityandaccessibility,variabilityindefinitionscreatesamethodologicalchallengetosummarizingtheliterature.
RationaleSeveralfactorsprovidearationaleforcontinuingtodevelop,investigateandimplementbriefinterventionsintheareaofsubstanceuse(Saitz,2005).Forone,whileratesofalcoholandothersubstancemisuseanddiagnosesarehigh,mostindividualsdonotreceivespecialtytreatment.TheNIAAA(2005)estimatesthat16%(40million)ofadultsintheUnitedStatesaredrinkingatriskylevelsand7.5%(19million)meetcriteriaforalcoholabuseordependence.TheseresultsaresimilartothosereportedintheNationalSurveyonDrugUseandHealth(SAMHSA,2010),whichestimatesthatover23millionAmericansmeetcriteriaforasubstanceusedisorder.Despitethesehighrates,theNSDUHreportsthatonly2.3millionAmericanswithanalcoholordrugusediagnosishavereceivedspecialtytreatmentfortheirsubstanceusedisorderinthelastyear.Thislowrateofparticipationinspecialtytreatmentrelatestomanyfactors.Mostimportant,perhaps,isthefactthatmanyindividualsarenotinterestedinreceivingsuchservices.Ofthenearly21millionpeoplewithadiagnosablesubstanceusedisorderwhodidnotreceivespecialtytreatmentin2008,fewerthan5%indicatedaperceivedneedfortreatment(SAMHSA,2010).Individualsreportdisinterestinspecialtytreatmentbecauseofmanyfactors,includingnotbeingreadytostopusing,nothavinghealthcoverageorabilitytopay,possiblenegativeeffectsonworkoremployment,andlackofinformationaboutwheretogofortreatment(SAMHSA,2010).Stigmaalsocontributestodisinterestinspecialtytreatment.Individualsareconcernedthatreceivingsuchtreatmentmightcausetheirneighborsorcommunitytohaveanegativeopinionofthem(Copeland,1997).Muchofthisfearofstigmatizationiswellgrounded,assomeformsoftreatmentsuchasmethadonemaintenancehavebeenlinkedtodiscrimination(Hettemaetal.,2009).Briefinterventionsinnon-specialtysettingsmayprovideaviablealternativeforindividualswhoarenotinterestedinparticipatinginspecialtytreatment.Suchtreatmentsarealsomoreacceptabletoindividuals,particularlythosewithlesssevereuselevelsorconsequences(Moyeretal.,2002).Inadditiontoindividualbarriersthatreduceparticipationinspecialtytreatment,systemicfactorsalsoplayarole.Forone,specialtysubstanceabusetreatmentprogramshavelimitedcapacityandareonlyabletoaccommodateafractionofthoseindividualswithsubstanceusedisorderdiagnoses.Whilethecapacityofoutpatienttreatmentprogramsishardtoestimate,residentialandinpatientsubstanceabuseprogramshavealimitedcapacityofbarely100,000bedsandexceeda90%utilizationrate,leavinglittleroomforadditionalpatients(SAMHSA,2006).Infact,longwaitinglistsarecommonlycitedasabarriertotreatmententryforsubstanceusedisorders(MacMasteretal.,2005).Limitedcapacityalsoappearstoaffectsomegroupsmorethanothers.Forexample,accesstospecialtytreatmentmaybeespeciallyproblematicforthoseindividualslivinginruralareas(Fortney&Booth2001).Professionalsinhealthcareencounteralargenumberofindividualswhoareusingsubstancesinariskymanneror

Brief Interventions and Motivational Interviewing
Page 3 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
whomeetcriteriaforsubstanceusedisorders.Withratesofriskyuseapproaching16%ofthegeneralpopulation(NIAAA,2005),aprimarycarephysicianwithapatientpanelsizeof2000encounters320patientswithpotentiallyharmfulalcoholuseannually.Theserateswouldbeevenhigherwhenincludingindividualswithriskydruguse.Whileopportunistictreatmentwithinmedicalsettingsmaybeaviablealternativetospecialtytreatment,lessthan16%reporteverydiscussingalcoholusewithahealthprofessional(McKnight-Eilyetal.,2014)and,unfortunately,problematicuseoftengoesundetectedinthesesettings.Forexample,primarycarephysiciansmayinterveneinonlyoneof10casesofalcoholdependence(McGlynnetal.,2003)andmaybeevenlesslikelytointervenewithriskyusers.Despitehighratesofalcoholandsubstancemisuseinternationally,andevidencetosupporttheeffectivenessofbriefinterventions,mostprovidersdonotusebriefinterventions.Alcoholandsubstanceusecontributetomanyotherproblemsthatarecommonlyencounteredwithinsettingsinwhichbriefinterventionscanbeadministered,increasingthebenefitsthatcanberealizedbyaddressingthisimportantneed.Forexample,inmedicalsettings,healthproblemssuchaslivercirrhosis,coronaryarterydisease,cancer,injury,suicide,andpsychiatricproblemscanbenegativelyaffectedbyorevencausedbyalcoholandsubstancemisuse.Providinginterventionsindifferenttimelimitedprofessionalsettingstoindividualswhowouldnototherwiseparticipateinspecializedtreatmentcouldhavesignificantpublichealthbenefits.
EvidenceBaseAlthoughtheconceptofbriefinterventionsisincreasinginpopularity,thisapproachisnotanewideainthetreatmentofalcoholandsubstanceusedisorders.Bienetal.(1993)citeanearlysalientexampleofthepromiseofbriefinterventioninastudyfromEdwardsetal.(1983),inwhichasinglesessionof“sympatheticandconstructive”advicewasfoundtobecomparabletoanextensivetreatmentpackageconsistingofAlcoholicsAnonymousfacilitation,medications,andextensivetreatmentthatcouldincludeinpatienttreatmentfornon-responders.Sincethattime,briefinterventionshavebeenthefocusofconsiderableresearchefforts,particularlyintheareaofalcoholuseinhealthcaresettings.Overall,researchsupportstheeffectivenessofbriefinterventions,whichgenerallyoutperformcomparisonconditionsandperformequallyaswellasextendedtreatment.
EvidencefromPrimaryCareSettingsTheWorldHealthOrganizationconductedalargeinternationaltrialintotheeffectivenessofbriefinterventionsinprimarycaresettings(Babor&Grant,1992).Investigatorsrandomlyassignedat-riskdrinkerstoacontrolcondition,a5-minuteadvicecondition,oraconditionthatincludedadviceplus15minutesofcounselingandaself-helpmanual.Bothinterventionconditionsledtosignificantreductionsinalcoholusecomparedwiththecontrolcondition.Severalrecentmeta-analyseshavefoundsimilarresultsregardingbriefinterventionswithinprimarycaresettings.Inameta-analysisof56studies,briefinterventions(fourorfewersessions)producedsignificanteffectsizesforalcoholconsumptionandotherdrinking-relatedoutcomevariablesamongnon–treatment-seekingpopulationsforupto1year(Moyeretal.,2002).Whitlocketal.(2004)foundthatbriefinterventionsinprimarycarereducedalcoholconsumptionanywherefromthreetoninedrinksperweek,oranoverallreductioninconsumptionof13%to34%.Inameta-analysisof22randomizedcontrolledtrialswithmorestringentacceptancecriteria,Kanerandcolleagues(2009)foundareductioninconsumptionbytwotofourdrinksat1-yearfollow-up,withgreatereffectsonmenthanwomen.Alsousingfairlynarrowselectioncriteria,Jonasetal.(2012)foundthatamongbriefinterventionsconductedwithnondependentalcoholmisusers,consumptiondecreasedby2.4to4.8drinksperweek.Briefinterventionsoftenhavebenefitsthatexceedreductioninconsumption.Onerecentmeta-analysisofbriefinterventionsforproblemdrinkingfoundadecreaseintherelativeriskofmortalitybyabouthalfcomparedwithcontrolconditions(Cuijpersetal.,2004).Maciosek(2006)foundthatthepracticeofalcoholscreeningandbriefinterventionwasaseffectiveaswidelyacceptedpreventionpracticessuchascervicalandcolorectalscreeningandinfluenzaimmunizationinreducingclinicallypreventableburden(CPB).CPBestimateshowmuchdisease,injury,anddeathwouldbepreventedifservicesweredeliveredtoalltargetedindividuals.Inanotherreview,Solbergetal.(2008)foundthatscreeningandbriefinterventionforalcoholdisorderswereamongthehighestrankedpreventiveservicesincost-effectiveness,returnoninvestment,andhowmanydollarswouldbesavedfor

Brief Interventions and Motivational Interviewing
Page 4 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
eachdollarspent.Infact,briefinterventionsforalcoholdisordersweremorecost-effectivethancervicalandcolorectalscreening,influenzaimmunization,andevenhypertensionscreeningandtreatment.Overall,briefinterventionsforriskydrinkinginprimarycaremaysave$4incostforevery$1invested(Fleming,2002).Whiletheevidenceinfavorofbriefinterventionsforalcoholuseisstrong,briefinterventionsforsubstanceusewithinprimarycaresettingshaveasmaller,butgrowing,evidencebase.Forexample,Bernsteinetal.(2005)foundthataone-sessionpeer-ledinterventionforcocaineandheroinusersidentifiedbyscreeningduringroutinemedicalcareproducedincreasedabstinenceforbothsubstancesat6-monthfollow-uppoint.Similarresultshavebeenfoundwithregularmarijuanausers(Copelandetal.,2001;Stephensetal.,2000).Anothergeneralfindingisthat,whenitcomestosubstanceabusetreatment,moreisnotnecessarilybetter,andeffectsdiminishovertime.IntheMoyerreview(2002),differencesbetweenbriefinterventionsandmoreextendedtreatmentsintreatmentseekingwerenegligible.Wutzkeetal.(2002)andKaneretal.(2009)similarlyfoundthattheintensityoftheinterventionwasnotrelatedtooutcome.Intheirreview,Bienetal.(1993)alsoconcludedthatextensivetreatmentsdonottendtooutperformbriefinterventions.WhiletheabovestudiessupporttheeffectivenessofBIcomparedwithmoreextensivetreatments,someevidencesuggeststhatlongertreatmentdurationisbeneficialinsomecases,particularlywheninvestigatedusingcommunityornoncontrolledtrials(Hubbardetal.,2003;McKay,2005).Asisthecasewithmanysubstanceuseinterventions,effectsofbriefinterventionstendtodiminishovertime.Anotherbriefinterventionstudyfoundthatparticipantswhoshowedsignificantreductionsinalcoholconsumptionatearlyfollow-uppointsnolongerdifferedfromcomparisonparticipantsonalcoholconsumption,mortality,oralcohol-relateddiagnosesafter10years(Wutzkeetal.,2002).
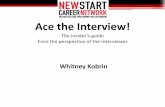
ClicktoviewlargerFigure1 .Thespectrumofalcoholuse.
Whenthinkingaboutbriefinterventions,itishelpfultohighlightthatthereisaspectrumofseveritywhenitcomestoalcoholandsubstancemisuse.Whilethealcoholorsubstancedependentindividualisperhapsthefirsttocometomind,thisgroupactuallyconstitutesasmallminorityofthepopulationofsubstanceusers.Thereisamuchlargerproportionofindividualswhoaredrinkingatriskylevels(seeFigure1).Briefinterventionwiththeseriskydrinkerscouldperhapsproducesomeofthelargestpayoffsbyreducingpersonalandsocietalcostsofsubstancemisuse.Evidencefrommeta-analysisalsosuggeststhattheeffectsofbriefinterventionmaybestrongerforthosewithriskyuseorlessseverealcoholproblems(Moyer,2002).
EvidencefromEmergencySettingsOfthe115millionvisitstoU.S.emergencydepartments(EDs)andtraumacentersannually(USDHHS,2007),anestimated29%arealcoholrelated(McDonald,2004)andasmanyas50%ofpresentingpatientsaredrinkingatriskylevels(Desy,2010).ThesesettingscreategreatpromiseforSBIRTimplementationbecauseofthehighbaserateofriskydrinkers,thepresenceofapotential“teachablemoment”thatmayresultfromalcohol-relatedinjuriesormedicalcomplications,andthepresenceofhighlyskilledmedicalprofessionalsaspotentialinterventionists.Somestudiessuggestthatbriefinterventionsconductedinemergencysettingshavebeneficialeffects;theyreducereinjuryratesbyasmuchas50%(Gentilelloetal.,1999),preventoneDWIarrestforeveryninebrief

Brief Interventions and Motivational Interviewing
Page 5 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
interventionsadministered(Schermeretal.,2006),andsavefourtimestheircostinsubsequenthealthcareexpenses(Gentilelloetal.,2005).Inresponsetotheseimpressivestatisticsandthecontrastingevidencethatemergencyphysiciansdonotroutinelyofferbriefinterventionstopatientspresentingwithalcohol-relatedinjuries(Lowensteinetal.,1990),in2005theAmericanCollegeofSurgeons(theprimaryorganizationresponsiblefordevelopingtraumacenterrequirements)enactedalandmarkresolutionthatmandatesLevelItraumacentersscreeninjuredpatientsforanalcoholusedisorderandprovidebriefinterventionstothosewhoscreenpositive.Morerecently,theAmericanCollegeofEmergencyPhysicians(ACEP)hasendorsedtheuseofSBIRTinEDsettings(ACEP,2011).Despitetheenthusiasm,someworrythatardencyoverEDSBIRThasoutpacedtheevidence(Saitz,2009).WhilethereisstrongevidencethatSBIRTtargetingriskyalcoholuseiseffectiveinprimarycaresettings(Moyer,2002;Whitlock,2004)evidencespecificallyfromEDsettingsismoremixed(Saitz,2009).Meta-analysesrevealthattherehavebeenseveralnegativetrialsofSBIRTinEDsettings(Nilsen,2008)resultinginquestionableevidenceoftheimpactofSBIRTonconsumption(Havard,2008).Criticspointout(Saitz,2009)thatthemostmethodologicallysoundofavailablecontrolledtrialsdonotfindsignificantbetween-groupdifferencesfavoringSBIRTovercontrol(Daeppenetal.,2007;D’Onofrio,2008).OfthepositivetrialsofSBIRTinEDsettings,manyhavemethodologicallimitationsincludinghighratesoffollow-upattrition(Gentilello,1999),debatableanalytictechniques(Schermeretal.,2006),orlackofacontrolgroup(Vaca,2011).Severalofthesesinglearmstudieshavefoundsignificantdrinkingimprovements,includingasix-sitenationalsinglearmstudythatfound50%reductionsinconsumption(Madras,2009),butitisdifficulttomakecausalinferenceswithoutacontrolgroup.A14-sitenationwideassessmentofreal-worldEDSBIRTimplementationconsidering3-,6-,and12-montheffectsshowedshort-termreductionsofat-riskdrinkingbutinsignificantdifferencesbetweensubjectsandcontrolpatientsat6and12months(Bernstein&Bernstein,2010).AdditionalmethodologicallysoundcontrolledtrialsofSBIRTwithEDpopulationsaredesperatelyneeded.
EvidencefromCollegeSettingsRatesofriskydrinkingandnegativeconsequencesarehighincollegepopulations(Larimeretal.,2004).Collegecampuseshaveseveralopportunisticsettingsinwhichbriefinterventionsforsubstanceabusecanoccur,includingstudenthealthclinics,studentorganizations,andjudicialsystemsthatdealwithalcoholanddrug-relatedpolicyviolations.Overall,effortstoscreenandprovidebriefinterventionwithcollegesampleshaveproducedpositiveresults(Larimeretal.,2004).Forexample,Schaus(2009)foundthatuptoonequarterofcollegestudentsseeninaprimarycareclinicatapublicuniversityweredrinkingatriskylevelsandthatatwosessioninterventionbasedonmotivationalinterviewingsignificantlyreduceddrinkingwithinthispopulation.Althoughtheevidenceisfairlystrongformanycollegebriefinterventions,thereismixedevidenceformandatedcollegesamples.Forexample,Ciminietal.(2009),foundnosignificantpre-postdifferencesindrinkingvariablesamongpublicuniversitystudentsmandatedtoparticipateintreatmentbecauseofaschoolalcoholpolicyviolation.Resultswerepoorforallthreeinterventionstyles,includingsmallmotivationalinterviewingclasses,interactive-educationalgroups,andpeer-facilitatedbriefinterventions.Similarly,Amaroetal.(2009)foundthatcollegestudentsmandatedtoparticipateinabriefinterventionbasedonemployeeassistanceprogrammodelsshowedfewimprovementsinprimarydrinkingoutcomesrelativetocontrolparticipants.However,anotherseriesofstudiesfoundimprovementsindrinkingamongcollegestudentsadjudicatedfordrinkingoffenseswhentheyunderwentbriefmotivationalinterventionsinsmall,interactivegroups(LaBrie,Lamb,Pedersen,&Quinlan,2006;Labrie,Thompson,Huchting,Lac,&Buckley,2007).Anotherfactorimpactingtheeffectivenessofbriefinterventionsamongcollegestudentsisinterventionstyle.Allbriefinterventionstylesdonotappeartohaveequivalenteffects.Forexample,educationalstrategieshavegenerallybeenfoundtobeineffectiveatreducingriskyalcoholuseamongcollegesamples;incontrast,briefmotivationalinterventionstendtohavefavorableresults(Larimer&Cronce;2002).Specifically,motivationalenhancementtherapysessions,combiningassessmentfeedbackandMI,haveshownpromiseamongcollegeindividuals(Baeretal.,2001;Marlattetal.,1998;Murphyetal.,2001)andgroups(LaBrieetal.,2008;LaBrie,Pedersen,Lamb,&Quinlan,2007).Assessmentandfeedbackresultsmayalsobeaparticularlyeffectivecomponentofotherbriefinterventionsfor

Brief Interventions and Motivational Interviewing
Page 6 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
collegestudentsamples,andseveralstudiesindicatethatnormativefeedbackalone,evenwhengivenbymail,maybeaneffectiveinterventionamongthispopulation(Murphyetal.,2004).Butler&Correia(2009)foundthatsuchfeedbackmaybeequallyeffectivewhenadministeredelectronicallyversusfacetoface.Infact,evenassessmentwithoutnormativefeedbackhasbeenfoundtosignificantlyaffectsomeaspectsofriskydrinking(Waltersetal.,2009).
EvidencefromCorrectionalSettingsAlcoholandsubstanceuseareassociatedwithcriminalbehavior,andasignificantproportionofthecriminaljusticepopulationhavehistoriesofalcoholordrugabuse(Lapham,2004).Thisfact,incombinationwiththeregularityandfrequencywithwhichcorrectionsstaffandofficerstypicallyinteractwithindividualsinvolvedinthecorrectionalsystem,hasledthesubstanceabusefieldtofocusonthefeasibilityofconductingbriefinterventionswithinsuchsettings.Whilemoststatesrequirescreeningofindividualsconvictedfordrivingwhileintoxicated,screeningofindividualswhocommittedothercrimesismuchmorevariable,despitegenerallyhighratesofuseamongthispopulation(Lapham,2004).However,criminaljusticesettingsoftenreferoffenderstospecializedtreatmentprograms.Infact,alargeproportionofpublicsystemreferralsforsubstanceabusetreatmentcomefromcriminaljusticesettings.Whilebriefinterventionswithincorrectionalsettingsseempromising,evidenceoftheeffectivenessofbriefinterventionswiththispopulationissparse.Davisetal.(2003)foundthatbriefMIincreasedthetreatmentengagementrateofsubstanceabusingveteransfollowingincarceration.However,Wells-ParkerandWilliams(2002)foundlessfavorableresultswhentestingtheimpactofagroupdiscussioninterventiononrecidivismforDWI.
FrameworksandOrganizingStructuresforDeliveringBriefInterventionsSeveralframeworksandorganizingstructuresareavailableforthedeliveryofbriefinterventions.Mostoftheseframeworksrecommendspecificstepsthatcanbeseenasshellsfilledwithdifferentinteractiontechniquesorstyles.Thissectionwillprovideanoverviewoftherationale,procedures,andevidencebaseforavarietyofbriefinterventionframeworks,includingscreening,briefintervention,andreferraltotreatment(SBIRT),FRAMES,the5As,andtheStagesofChange.
Screening,BriefIntervention,andReferraltoTreatmentSBIRTisapublichealthinitiativedesignedtoscreenindividualsforriskysubstanceuseorsubstanceusedisorders,conductbriefinterventionsthattargetindividualswithriskyalcoholusewhodonotneedspecializedtreatment,andreferthosewithmoresevereusetospecializedtreatment(http://sbirt.samhsa.gov/about.htm).SBIRTtypicallytakesplaceincommunityormedicalsettingswhereprofessionalshaveopportunitiestoscreenindividualsforsubstanceusedisordersanddeterminetheappropriatelevelofintervention.ThefirststepinSBIRTinvolvesscreeningindividualsforriskyorproblematicuse.Positivescreensmaythenbefollowedwithmoreintensiveassessmenttodeterminethepresenceofsubstanceusedisordersorotherrelevantsubstance-relatedconsequences.AscanbeseeninFigure1,substanceuseandrelatedconsequencesamongindividualsoccuronacontinuum,rangingfromabstinencetodependence.Epidemiologicresearchsuggeststhatmenwhoregularlydrinkmorethanfourstandarddrinksinaday(ormorethan14perweek)andwomenwhoregularlydrinkmorethanthreeinaday(ormorethansevenperweek)areatincreasedriskforalcohol-relatedproblems(Dawsonetal.,2005).Becauseofthis,theNIAAArecommendsasinglescreeningquestionqueryingthepresenceofusethatexceedstheselevelstoidentifyindividualswhoareatriskforalcohol-relatedproblems(NIAAA,2005).Otherscreeninginstrumentsforalcoholanddrugusearealsoavailableandeachhasitsownindividualbenefitsanddrawbacksintermsofsensitivity,specificity,andeaseofadministration.Forexample,theCAGEquestionnaire(Ewingetal.,1984)isafour-questionscreeningtoolthatiseasytouseandrememberbecauseofitsacronym:Haveyoueverfeltyoushouldcutdownonyourdrinking?Havepeopleannoyedyoubycriticizingyourdrinking?Haveyoueverfeltbadorguiltyaboutyourdrinking?Haveyoueverhadadrinkfirstthinginthemorningtosteadyyournervesortogetridofahangover(eye–opener)?Theinstrumentgenerallyhasgoodpsychometriccharacteristics(Fiellin,2000)includinginternalconsistencyreliability(Mischke&Venneri,1987).Endorsementof

Brief Interventions and Motivational Interviewing
Page 7 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
threeormoreitemshasbeenfoundtobestronglypredictiveofanalcoholusedisorder,withgoodlevelsofsensitivityandspecificity,butthecut-offscoreof1foridentificationofriskydrinkershasbeencriticizedforpoorsensitivityorhighratesoffalsepositives(MacKenzieetal.,1996).TheAlcoholUseDisordersIdentificationTest(AUDIT;Saundersetal.,1993)screensforthequantityandfrequencyofalcoholuse,bingedrinking,symptomsofdependence,andalcohol-relatedconsequences.Theinstrumentcanbeself-administeredandmaybeparticularlyappropriateforbriefinterventionstudiesbecauseofitsabilitytoidentifypeoplewhohaveproblemswithalcoholbutwhomaynotbedependent(Feillin,2000).TheMichiganAlcoholismScreeningTest(MAST;Selzer,1971)includesquestionsaboutdrinkingandalcohol-relatedproblems.Thisinstrumentcanbeparticularlyhelpfulinidentifyingalcoholdependence(Reidetal.,1999).TheDrugAbuseScreeningTest(DAST;Gavin,Ross,&Skinner,1989)isasimilarinstrumentthatisavailablefordetectingdrugusedisorders.Additionally,theWorldHealthOrganization(WHO)developedtheAlcohol,SmokingandSubstanceInvolvementScreeningTest(ASSIST)toscreenforproblematicorriskyuse(WHO,2008:http://www.who.int/substance_abuse/activities/assist_technicalreport_phase3_final.pdf).Theinstrumentyieldsariskcategoryfornicotine,alcohol,andarangeofdrugsthatcanbeusedtoinformtheappropriatelevelofbriefintervention.WhileNIAAArecommendsuniversalscreeningofallpatientsseeninprimarycaresettings,theapproachmaybeparticularlyapplicableorimportantduringphysicalexaminations,whenprescribingamedicationthatinteractswithalcohol,withwomenwhoarepregnantortryingtoconceive,withpatientswhoarelikelytodrinkheavily(suchassmokers,adolescents,andyoungadultsandthosewhohavehealthproblemsthatmightbealcoholrelated),orpatientswhohavechronicillnessesthatarenotrespondingtotreatmentasexpected(NIAAA,2005).WithintheSBIRTmodel,followingscreening,providersdeterminethelevelofinterventionthatmaybeappropriateforaparticularindividual.Severaltoolsandprocessescanbeusedtomakethisdetermination.ForproviderswhousetheASSIST,theinstrumentyieldsariskcategoryof“low,”“moderate,”or“high”thatcorrespondstorecommendedinterventiontypes,includingnointervention,briefintervention,orbriefinterventionplusreferral(WHO,2008).Forindividualswithnouseorlowriskuse,reinforcementofhealthybehaviorsistypicallyrecommended,butinterventionisnot.Forthosewhoscreenpositiveforat-riskuse,additionalassessmenttodeterminethepresenceofdependence,degreeofnegativeconsequences,orpresenceoffamilyhistorymaybeappropriate.Basedontheseresponses,individualswithriskydrinkingalonemaybeappropriateforbriefintervention,whilethosewithsignsofdependenceorapositivefamilyhistoryofdependencemaybemostappropriateforbrieftreatment(treatmentorintervention?)withreferraltospecialtytreatment.Providerscontinueworkingandinterveningwithpeoplewhoarenotinitiallyinterestedinreferraltotreatment.OneexampleofanSBIRTprotocolwasdevelopedbytheNIAAA(2005)asaguideforhealthcarepractitionerstoscreenandintervenewithpatientsatriskforalcoholproblems.Theguideincludesfoursteps.Thefirststepinvolvesaskingaboutalcoholuse,includingthepresenceorabsenceofuseand,inthepresenceofuse,thepresenceofheavydrinking(fiveormoredrinksformen;fourormoredrinksforwomen)oranelevatedAUDITscore(8orhigherformen;4orhigherforwomen).Forthosewhoareatrisk,steptwoinvolvesamorethoroughassessmentofalcoholuse,includingthediagnosisofalcoholabuseordependence.Stepthreeinvolvesgivingadviceandassistancebasedonthedrinkinglevelsofthepatient.Thisadvicemayincludeabstinenceandspecialtytreatmentforthosewithalcoholusedisordersandcuttingdownforthosewithriskyuse.NIAAArecommendsthatthenatureofassistanceorbriefinterventionshouldbedependentonthereadinesslevelofthepatient.Forthosewithlowreadinesstochange,providersareencouragedtohelppatientsexploreambivalencetochange,whilethosewhoarehighinreadinessmaybenefitfromsettingagoal,developingachangeplan,andreceivingeducationalresources.Atstepfour,providersareencouragedtoacknowledgethatchangeisdifficultandsupportanypositivechangesinthosewhowereunabletoreducedrinking,aswellasreinforceprogressinthosewhowereabletoeliminateriskyuse.Rescreeningatleastannuallyisencouraged.TheSBIRTmodelhasastrongevidencebaseforreducingratesofalcoholandsubstanceusewithinmedicalsettings.Forexample,theSubstanceAbuseandMentalHealthAdministration(SAMHSA)implementedandevaluatedanSBIRTinitiativeacrossavarietyofinpatient,outpatient,andemergencymedicalsettings(Madrasetal.,2009).ThesixsitesinthestudyhadsomeflexibilityregardingthespecificcomponentsoftheirSBIRTprotocol,butgenerallyscreenedpatientsusingtheDAST,AUDIT,quantity/frequencymeasuresofconsumptionorsomecombinationoftheabove.Nearly460,000individualswerescreenedwithinthetrial.Riskyuse,definedasdrinkingmorethanfivedrinksinonesittingorusingillicitsubstancesinthepast30days,wasidentifiedin23%ofpatients

Brief Interventions and Motivational Interviewing
Page 8 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
andtheseindividualswereprovidedwithbriefinterventionsthatincludedsite-customizedadaptationsoffeedback,FRAMES(seedescriptionlater),andMI.Inaddition,3%ofindividualswithhigherlevelsofusereceivedmoreintensivebrieftreatmentrangingfromonetoeightsessionsacrosssitesand4%ofindividualswhoindicatedsymptomsofsubstancedependencewerereferredforspecialtytreatment.Overall,thestudyrevealedverypositiveresultsfortheeffectsofSBIRT;thosewhoreceivedbriefinterventionreducedtheirdruguseby67.7%andtheiralcoholuseby38.6%.
FRAMESInareviewofbrieftreatmentforalcoholinterventions,MillerandSanchez(1993)identifiedseveralkeycharacteristicsofeffectivebriefinterventions(Bienetal.,1993).ThesecomponentscorrespondedtotheacronymFRAMES,whichreferstofeedbackofpersonalrisks,emphasizingthatresponsibilityforchangelieswiththeindividual,advice-giving,providingamenuofchangeoptions,anempathicinteractionstyle,andtheenhancementofself-efficacy.Whilemanyofthesecomponents,suchastheemphasisonempathyandenhancementofself-efficacy,areconsistentwithMI(Miller&Rollnick,2002),others,suchasadvicegiving,arenot.Feedbackofpersonalrisksinvolvesprovidingindividualswithobjectivefeedbackabouttheiralcoholorsubstanceuse.Thiscouldtaketheformofnormativefeedbackonstandardizedassessmentresults,asisdoneinmotivationalenhancementtherapy,orsimplyprovidinginformationaboutthepresenceorabsenceofriskyordependentuseortheimpactofuseonothermedicalorpsychosocialissues.Cliniciansemphasizetheimportanceofpersonalresponsibilitytoencouragetheindividual’ssenseofdegreeofpersonalcontrolandinterestininitiatingbehavioralchange.Advicetochangeinvolvesrecommendingthatindividualsstoporreduceuse,withclearguidanceabouthowtogetstarted,andwithanofferofsupport.Providingamenuofoptionsgivesindividualschoicesondrinkingorsubstanceusegoalsorspecifictreatmentoptions.Forexample,thepersonmaybepresentedwiththechoiceofwhethertocutdownoreliminatetheiruse,orofferedvarioustreatmentoptionssuchasself-change,communitysupportgroups,orformaltreatment.Usinganempathicandreflectiveinteractionstylehasbeenempiricallydemonstratedtobemoreeffectivethanconfrontationalapproaches(Miller&Rollnick,2002)andishighlyconsistentwiththeMIstyle.Finally,thevalueofenhancingself-efficacyisbasedondecadesofresearchonsocialcognitivetheory(Bandura,1986)thatindividuals’beliefsthattheycaneffectivelychangeincreasestheprobabilitythattheywillattempttoandsucceedatchange.Fortunately,self-efficacycanbedramaticallyinfluencedbyclinicians’actions,andclinicians’beliefintheirclients’abilitytochangehasbeenfoundtobepredictiveoftreatmentengagementandultimateoutcome(Leake&King,1977).
FiveAsThe5Asisaninterventionstrategy,drawnoriginallyfromthesmokingcessationliterature,thatprovidesrecommendedsequentialstepsforinterventionistsworkingwithbehavioralhealthissuessuchassubstanceuse(Fioreetal.,2000).Withinthemodel,providersareencouragedto:askaboutuse,assessseverityandreadinesstochange,advisecuttingdownorabstinence,assistingoalsettingandfurthertreatmentifnecessary,arrangetomonitorprogress,and,inarecentadditionofasixthA,assurecross-culturalefficacyofpractices(NIAAA,2005).Otherversionsofthemodelvaryslightly.Forexample,Whitlocketal.(2002)usetheformat:assess,advise,agree,assist,arrange.Assessinvolvescompletingvalidatedscreeningorassessmentinstrumentsandquestionstodeterminethepresenceorabsenceofaproblem.Assesscanalsoinvolvedetermininganindividual’sknowledgeaboutsubstanceusebehaviorandrelatedconsequences,motivationstochange,andperceivedbarriers.Withinthismodel,assessmentresultsareusedtoinforminterventionsandareoftenrelayedbacktotheindividualintheformoffeedback.Adviseinvolvesprovidingtheindividualwithpersonallyrelevantandspecificinformationaboutrecommendationsforchange.Theinterpersonalstylewithwhichadviceisgivencanvarydramaticallyacrossinterventionists.Agreereferstotheuseofcollaborativediscussionanddecision-makingtohelptheindividualdevelopagoal.Here,too,interventionistsareoftenencouragedtoprovideamenuofoptionsforindividuals,involvesignificantothers,anddevelopagoalthatisspecificandmeasurable.Assistinvolveshelpingtheindividualtodevelopaspecificchangeplanorstrategiestoachievetheirgoal.Suchstrategiesmayincludereferraltospecializedtreatment.Last,arrangeinvolvesfollow-uptoreinforcechange,assurecross-culturalappropriateness,revisegoals,oraddressbarriers.The5Ashaveastrongevidencebaseacrossavarietyofhealthbehaviors,includingsubstanceuse,andare

Brief Interventions and Motivational Interviewing
Page 9 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
consistentwithinterventionelementsfoundtobeassociatedwithimprovedoutcomesinreviewandmeta-analyses(Goldsteinetal.,2004).Inaddition,providersreportsatisfactionwiththe5Asapproach,whichtheyperceiveasrequiringlittletraining,havingastrongevidencebase,andbeingsimpleandflexible(Grandesetal.,2008).
TheTranstheoreticalModelThetranstheoreticalmodel(TTM;DiClementeetal.,1985;Prochaska&DiClemente,2005)isamodelofbehavioralchangethatfocusesonhowpeoplemakedeliberate,purposefulchanges.Themodellargelyfocusesonbehavioralchangesthatinvolveeliminatingproblembehaviorsandbeginningnew,healthierbehaviors.Themostwell-knownaspectoftheTTMisthe“stagesofchange”(SOC)model,whichviewsbehaviorchangeasaprocessthatprogressesfromlowproblemawarenessandreadinesstochangethroughhighawarenessandactiveeffortstoinitiateormaintainchange.Themodelhasfivestages:precontemplation(individualsmaynotrecognizetheirbehaviorasproblematicandarenotplanningtochange),contemplation(individualsareconsideringchangebutremainambivalentaboutwhetherthebenefitsofbehaviorchangeoutweighthecosts),preparation(individualshavedecidedtomakeachangeandaremakingplanstochange),action(individualsareactivelytakingstepstochange),andmaintenance(individualsareintegratingbehaviorchangeintotheirongoinglifestyle).Whileprogressionthroughthestagesofchangeissometimeslinear,thedevelopersemphasizethatindividualscanmovefromanystagetoanotherandcyclethroughthestagesmultipletimesbeforeachievingsustainedchange.Inadditiontothestagesofchange,theTTMmodelfocusesonchangeprocesses.Differentexperiencesandactivitiesarehypothesizedtofacilitateprogressionthroughthevariousstagesofchange,withsomeevidencesupportingthesehypotheses(DiClemente,2003;Perz,DiClemente,&Carbonari,1996).Experientialprocessesmaybemostrelevanttoprogressingthroughtheprecontemplationandcontemplationstages.Consciousnessraisingabouttheproblembehaviorandsolutions,becomingmoreattunedtoemotionalaspectsofchange,consideringhowtheproblemaffectsothers,andclarificationofvaluesinrelationtothebehaviorareallthoughttocontributetoprogressthroughtheearlystages.Behavioralprocessesarebelievedtofacilitateprogressthroughactionandmaintenancestages.Theseincludemakingachoiceandcommitmenttochange,controllingtemptationsandtriggers,avoidingrisks,substitutingandreinforcingalternativebehaviors,andusingavailablesupportstohelpachieveandmaintainchange.TheTTMrecognizesthataperson’sbeliefsaboutthebenefitsanddrawbacksofchange,self-efficacyintheabilitytochange,environmentaltemptations,andindividualbiopsychosocialcharacteristicscaninfluenceprogressiontowardchange(Prochaska&DiClemente,2005).Themodelhasbeenusedtohelpmatchindividualstoappropriatelevelsandstylesoftreatmentandsuchapplicationshavebeenfoundtolowerrelapseratesandimprovetreatmentengagementamongindividuals(Dempsey,2008).ItshouldbenotedthattheSOCmodelhasreceivedsomecriticismasaninappropriateassessmentofreadiness(West,2005)andashavinglimitedapplicationtoaddictioningeneral(Sutton,2001).However,itisaninfluentialmodelofthestagesandprocessesofchange.
BriefInterventionsandInteractionStyleAsBienetal.(1993)describeintheirreviewofbriefinterventionsforalcoholproblems,theclinician’sinteractionstylecanhaveasignificantimpactonoutcome.TheseauthorsciteearlystudiesbyChafetz(1961,1962,1968),whichdemonstratetheimportanceofinteractionstylewhenmakingreferralstospecialtytreatment.Inthesestudies,standardreferralproceduresusedtoencouragespecialtytreatmentforpatientspresentingtoemergencydepartmentswithalcohol-relatedproblemswerecomparedwithastandardizedbriefinterventionthatusedanempathiccommunicationstyle.Theempathicapproachimprovedattendanceratesatasubsequentappointmentforspecialtytreatmentbyupto72%.Incontrast,aninterventionfocusedonadvicegiving,persuasiveness,andtheauthorityofthephysician,designedtoincreaseengagementinspecialtytreatmentforactivelydrinkingpatientswithgastrointestinaldisease,didnotincreaseratesoffollow-upcarebeyondthoseofthecontrolcondition(Kuchipudietal.,1990).Severaltherapeuticstylesorinterventiontechniquescanbeusedtoformthebasisofbriefinterventions.However,wewillfocusontheuseofmotivationalinterviewingasaninteractionstylethatcanbeusedinisolationortofillthestepsintheframeworksdescribedabove.

Brief Interventions and Motivational Interviewing
Page 10 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
MotivationalInterviewing
OverviewoftheApproachMIisatherapeuticapproachusedtoexploreandresolveambivalenceaboutbehaviorchange.MIhasastrongevidencebaseforreducingsubstanceuseandrelatedproblemsandhasbeenappliedextensivelyinbriefinteractionswithinmedicalandotheropportunisticsettings(Hettemaetal.,2009).Theapproachhasbeendefinedas“aperson-centeredcounselingstyleforaddressingthecommonproblemofambivalenceaboutchange”(Miller&Rollnick,2013,p.21),as“aclient-centered,directivemethodforenhancingintrinsicmotivationtochangebyexploringandresolvingambivalence”(Miller&Rollnick,2002)or,similarly,asa“collaborative,person-centeredformofguidingtoelicitandstrengthenmotivationforchange”(Rollnicketal.,2008).Theperson-centeredaspectoftheapproachreferstotheassumptionthattheperceptionsandgoalsoftheindividualversusthoseoftheinterventionistsshouldbeattheforefrontoftheinteraction.Person-centeredapproachesalsotendtofocusontheexpressionofempathyandacceptancethroughtechniquessuchasreflectivelistening.However,inadditiontotheperson-centeredaspectsofMI,cliniciansusedirectiveorguidingstrategiestointentionallypursuetheresolutionofambivalence,elicitandstrengthenmotivationtochange,andreducesubstanceuseorrelatedconsequences.Thus,whilefocusingonandelicitingtheclient’sperceptions,theMIinterventioniststrategicallyseekstohelptheclientdevelopanawarenessofanydiscrepancybetweensubstanceuseandpersonalgoalsandvalues.MIwasfirstdescribedasanapproachtohelppeoplewithdrinkingproblems(Miller,1983)andhasbeenmostcommonlyusedwithsubstanceusingpopulations,includingtobacco,alcohol,andotherillicitsubstancessuchascocaine,marijuana,andopiates(Hettemaetal.,2009).Ambivalenceiscommonamongpeoplewithsubstanceuseproblemsanddisorders,astheyoftenhavemixedfeelingsabouttheiruse.Forexample,whileanindividualmayperceivesomenegativeconsequencesoftheiruse,suchashangovers,work,orrelationshipproblems,heorshemayalsoenjoysomeofthepositiveoutcomesofusesuchasintoxication,reductionofnegativeemotions,orassociatedsocialization.Apersoninthisambivalentstateislikelytoremainconflictedandrefrainfromchangeunlessthebalanceoftheprosandconsofcontinueduseshifts.MIpractitionersviewthespiritoftheunderlyingapproachasnecessaryforthesuccessfulimplementationofspecificskills.MIpractitionersassumethatindividualshavewithinthemprosocialandhealthyvaluesandthattheyshouldbetreatedaspartnersinthechangeexplorationprocessversusrecipientsofexpertadvice(Miller&Rollnick,2005).TheMIspiritencouragescollaboration,wheretheindividualisseenasanexpertonhisorherowncircumstancesandtheinterventionististheexpertonskillsforeffectivelymanagingaconstructiveconversationaboutchange.Therelationalstanceofcollaborationassumesthatindividualsarecapableofmakingsounddecisionsandoftenhavetheresourcesandinformationnecessarytoimplementthem.Infact,manyindividualsusingsubstanceuseatriskylevelsareoftenawareofthepotentialrisksoftheirbehavior,effectivestrategiestoreduceuse,andresourcestoassistthem,andmerelistingofthesefactsisunlikelytopromotechange.Rather,MIinterventionistsavoidprovidingunneededorunwantedinformation,andelicitmoreinformationthantheyprovide.FromtheMIperspective,itismoreimportantthattheinterventionistdevelopasupportiverelationshipwiththeindividualanddrawouttheperson’sownmotivationsthangiveinformation,educate,orpersuade,allofwhichmayleadtoresistanceandpotentiallydecreasetheperson’swillingnesstochange.ThespiritofMIisalsobasedonanimplicitandexplicitrespectoftheclient’sautonomy.Itencouragestheacknowledgementandsupportoftheindividual’sabilityandresponsibilitytoconsideroptions,makedecisions,andtakeaction.However,whilethespiritofMIisevocative,italsoallowsandevenencouragesinterventioniststoprovideopportunitiesforindividualstogainnewperspectivesontheirsubstanceusebehaviorsbythinkingaboutanddiscussingissuesrelatedtotheirbehaviorinanorganizedandsupportiveenvironment.
CoreSkillsMIpracticebuildsonitsspiritusingasetofkeyskillsthatcanbesummarizedusingtheacronymOARS:open-endedquestionsthatelicitthatindividual’sperspectiveorconsiderationofatopic,affirmationswhichcanhelptodeveloprapportandreinforcestrengthsorpositivechanges,reflectionsthatindicateinterest,acceptance,andunderstandingoftheclient,andsummariesthatcanbeusedtocapturethemeswithininteractionsandtransitionbetweentopics.Thesetechniquesareusedtobuildrapportandtherapeuticalliance,encourageconsiderationandexplorationofchange,andincreasecommitmenttochange.

Brief Interventions and Motivational Interviewing
Page 11 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
TherapeuticProcessesInadditiontotheemphasisonusingOARSasabasiccommunicationstyle,theMItherapistusesbroadertherapeuticprocesses:engaging,focusing,evokingandplanning(Miller&Rollnick,2013).Thefirstkeyprocessisengaging.EngagementinMIinvolvesdevelopingadeeptrustbetweenpractitionerandclientthatallowsforthedevelopmentofclient-centeredgoals.Whenclientsarenotdeeplyengaged,theytendtobemorepassive.WhileMIpractitionersmayhaveaclinicalinvestmentinaparticulardirectionforclientchange(suchasreducinguseorharm),MIdevelopsacollaborativerelationshipbetweenclientandpractitioner,asitisnotfocusedonknowledgeorskilldevelopment.Thesecondkeyprocessisfocusing.Onceclientsaresufficientlyengagedintherapeuticconversation,MIpractitionersbegintonarrowthefocustotheissueofclientchange.Whatdoestheclientnotlikeabouthisorherlife?Whatmightbedifferent,better?Whatmighttheclientliketokeepwhilemovingforward,andwhatcanbeleftbehind?ThethirdcentralMIprocessisevokingclientperspectivesandideasaboutchangeratherthanprovidingideasandperspectives.Atitscore,MIisbasedontheideathatpeoplemotivatethemselvestochange,andthataneffectivewaytoelicitclientchangeistostructureconversationssothatclientsidentifyanddiscussthereasons,desiresandneedstheyhavetomakechanges.Thisisdistinctfromamorepersuasiveapproach,inwhichtheinterventionistpersuadesortellstheindividualhowandwhyheorsheshouldchange.InMI,discrepanciesthoughttomotivatebehavioralchangearedevelopedbydrawingouttheindividual’sownideasandfeelingsaboutsubstanceuseandperceptionsabouthowthebehaviorfitsinwithpersonalgoalsandvalues.Giventhatambivalentpeoplehavebothsidesoftheargumentaboutmakingchangesvs.holdingtothecurrentcoursealreadyinternalized,MIpractitionersevokeclients’ownthoughtsaboutchangeandarecarefultoavoidextollingthevirtuesofchangeduetotheriskofmotivatingclientstomake“yes,but”argumentsdefendingthestatusquo.Thefourththerapeuticprocessisplanning.Atsomepoint,clients’focusofattentionshiftsfromwhetherandwhytochangetohow.Theshiftmaybesudden,withaclientwhohasbeenponderingpossibilitieswhodeclares“I’vegottochange”or“Ican’tgoonlikethisanymore.”Othertimes,theshiftmaybegradual,almostunnoticeable,astheclientgoesbackandforthbetweenchangingonewayoranother,orstayingthesame,consideringhypotheticalpossibilities,thentalkingabouthoweachpossibilitymightworkandwhathecoulddotowardthatend.Buthowevertheconversationoccurs,whenclientstilttowardfavoringchange,MIpractitionersshifttohelpingclientsdevelopchangeplansandputthemintoaction.
StrategiesofMIThecoreskillsandprinciplesofMIformthebasisformanyspecificstrategiesorinterventiontechniquesthatcanbeusedtoimplementmotivationalinterviewinginpractice.Whereasthecoreskillsaremicro-levelinteractionaltechniques,andtheprinciplesaremacro-levelguides,MIstrategiesareintermediatemethodstostructureconversationstomaximizetheemergenceofmotivationforchange.SeveralofthesestrategiesthatareparticularlyapplicabletobriefapplicationsofMIandexamplesofhowtousethemfollow.
1.Agendasettinginvolvesprioritizingtasksandtopicsforaninteraction.Examplesinclude:Howwouldyouliketospendourtimetogethertoday?Or,Whichoftheseissueswouldyouliketodiscussfirst?Or,I’dliketofigureoutwhat’sgoingonwithyoursorethroatandthenspendafewminutesfollowingupondiscussionofalcoholusefromlasttime.2.Importanceandconfidencescalingcanbeusedtoassessmotivationandalsoasatooltoelicittalkaboutchange.I’dliketounderstandmoreabouthowyouviewyourdrinking.Onascaleof0to10,with0beingnotatallimportant,and10beingextremelyimportant,howimportantisitforyoutochangeyourdrinkingnow?Thisquestion(andthesimilarquestionaboutconfidence)canbefollowedbyaskingtheindividualwhytheirscorewasnotsomethinglowerthanwhattheyindicatedandwhatitwouldtaketomovetoahighernumber,bothofwhichstrategicallyelicittalkaboutchange.3.ProvidinginformationinanMIconsistentwaycaninvolveaskingpermissionorprovidingamenuofoptions.Ihavesomeinformationaboutstrategiesforreducingdrinking.WoulditbeallrightifIsharedthemwithyou?Or,Youtalkedaboutwantingtogetsomemoreinformationaboutmanagingyourdrinking.Weofferseveraloptionshereincludingmeetingwithatherapisttodoakindof“checkup”aboutdrinking,enrollinginourdrinkers’supportgroup,ordiscussingyourhealthfurtherwiththenurseorwithme.ThereareadditionalresourcesIcanpointyouto,includingwrittenmaterialsandinteractiveprogramsontheinternet.Which,ifanyofthese,areofinteresttoyou?4.Elicit-Provide-Elicitinvolvesincreasingthecollaborativenatureofinformationprovisionbyelicitingwhatan

Brief Interventions and Motivational Interviewing
Page 12 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
individualalreadyknowsaboutatopic,providingadditionalorcorrectiveinformationinatailoredway,andthenelicitingaresponsetotheinformation.Whatdoyouknowaboutlevelsofsafedrinking?…Ithasbeenfoundthatwomenwhodrinkmorethan3drinksadayor7drinksinaweekareatanincreasedriskforavarietyofhealthandotherproblems.Whatdoyoumakeofthat?5.Exploringstrengthscanbeusedtohelpidentifyresourcesanddevelopplansaswellasincreaseself-efficacy.Whataresomepersonalqualitiesthatyouareproudof?Or,Whichstrengthsdidyouusetoovercomethatchallenge?6.Exploringvaluescanbeusedtohelpindividualsdevelopadiscrepancybetweenharmfulsubstanceuseandwhatismostimportanttothem.Whatthingsaremostimportanttoyouinyourliferightnow?Or,Takealookatthislistofvalues.Takeaminutetopickyourtopthreeandtellmewhattheymeantoyou.Or,You’vementionedhowimportantyourchildrenaretoyou.Whatimpact,ifany,doesyourmarijuanausehaveonyourchildren?7.Lookingbackwardgivesindividualsanopportunitytothinkaboutatimeintheirliveswhensubstanceusewasnotanissueandidentifybenefitsofthiswayofbeingandalsoeffectivestrategiesformaintainingthisbehavior.Let’stalkaboutatimebeforeyoustartedusing.Whatwereyoudoingthen?Howdidyoufeel?8.Lookingforwardinvolvesaskingindividualstothinkabouttheirlifedowntheroadconsideringiftheywereorweren’tabletomakechanges.Avariationistoaskindividualstoenvisionafuturethattheydesire.Wheredoyouthinkyou’regoingwithyourdrinkingifyoulookaheadafewyears?Whataresomeoftheworstthingsthatwilllikelyhappenifyoumaintainyourcurrenthabits?Whataresomeofthebestthingsthatmighthappenifyoumadesomechanges?9.Consideringhypotheticalchangeshelpsindividualstoidentifyimportantstepstowardschangeandgivesthemanopportunitytoforeseeadifferentfuturewithoutbeingforcedtomakeacommitment.Ifyouweretomakeachangeinyourdrinking,howmightyougoaboutitinordertosucceed?Whatwouldbechallenging?Whatwouldberewarding?
InadditiontodefiningwhatstrategiesMIincludes,itisalsousefultodefinewhatitdoesnotinclude.Forexample,unsolicitedadviceisnotofferedwithoutfirstobtainingpermissionfromtheindividual.Similarly,practitionersavoidconfrontingorwarningclientswiththeirownconcernsaboutdrinkingordrugusechoices.MIstrategiesortechniquesarenotsimplyaddedintointeractionsthatarehierarchicalinnature;rather,theMIstyleprescribesthatthetherapeuticrelationshipisinherentlynonhierarchicalandcollaborative.
EvidenceBaseSomeofthefirstempiricalevidenceinsupportoftheMImodelcamefromanearlystudyofMIinaDrinker’sCheck-upthatinvolvedassessingindividualsfordrinkingbehaviorandrelatedconsequencesandprovidingthemwithfeedbackinanMIconsistentmanner(Milleretal.,1988).Thisstudyshowedearlypositivefindingsthatbriefinterventionscouldsignificantlyreducedrinkingforupto1yearandafollow-upstudyfurtherdemonstratedthatMI-consistentinteractionstylepredictedthedegreeofclientsuccess(Milleretal.,1993).Followingthesestudies,afour-sessionadaptationofMIthatincludedpersonalizedfeedbackcalledMotivationalEnhancementTherapy(MET)wastestedwithinProjectMATCH,alargemulti-siterandomizedclinicaltrial,andwasfoundtoperformequallywellatreducingdrinkingasmoreextensivecognitivebehavioraltherapyand12-Stepfacilitationapproaches(ProjectMATCHResearchGroup,1997).Sincetheseearlystudies,therehasbeenanexplosionofinterestinandstudiesofMI,withmorethan200clinicaltrialsconductedtodate,andthesubsequentdevelopmentofanascentmodelofsomeofthemechanismsofMI(Miller&Rose,2009).MIanditsmostcommonadaptation,MET,havebeenlistedasevidence-basedpracticesontheNationalRegistryofEvidence-basedProgramsandPractices,whichisanorganizationthatfacilitatesthereviewandratingofsubstanceabusetreatmentmodalities.Severalmeta-analysesofMIhavebeenconductedtodate.Inoneearlyreview,30randomizedcontrolledtrialsofadaptationsofmotivationalinterviewing(AMIs)wereincluded(Burkeetal.,2003).ThemajorityofincludedstudiesinvestigatedtheimpactofMIonalcoholordruguse.Themeandoseoftheinterventionisgenerallyconsideredtobebriefinnature,rangingfrom15to240minutes,andaveraging99minutes.Theauthorsfoundsmalltomediumbetweengroupeffectsizesfordrinkingandmediumeffectsizesfordruguse.Intheseareas,AMIsdoubledabstinenceratesfrom1:5to2:5.OveralltheauthorsconcludedthatAMIsareeffectiveandefficient,astheycan

Brief Interventions and Motivational Interviewing
Page 13 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
producesimilarresultsintwosessionstothoseachievedbyotherinterventionsstylesin8sessions.Amorerecent,largermeta-analysisofMIincluded72studiescoveringarangeofproblembehaviors.Again,themajorityofstudiesfocusedonalcoholordruguseorengagementinsubstanceusetreatment.Hettemaandcolleagues(2005)foundsmalltomediumeffectsizesforalcoholanddruguseandmuchlargereffectsforengagementinsubstanceabusetreatment.Thismeta-analysisalsofoundthat,similartootherbehavioraltreatments,effectsofMIappearearlyandtendtodiminishsomewhatovertime,exceptinstudiesinwhichMIisaddedtosomeotherformoftreatment.TheyfoundthattheaverageeffectsizeofMIwasd=0.77atpost-treatment,d=0.31at4to6months,andd=0.30at6to12months.Anothermeta-analysiscomparedtheeffectivenessofMItobriefadviceonavarietyofhealthbehaviors(Rubak,2005).Seventy-twotrialswereincludedandthoseaddressingalcoholusefoundthatMIoutperformedbriefadvice-basedinterventiononobjectiveoutcomevariablessuchasbloodalcoholconcentrationandstandardethanolcontent.MIdemonstratedaneffectin74%oftheRCTsassessedandlikelihoodofaneffectincreasedwithincreasesinthenumberofminutespersessionandthenumberofencountersperpatient.TheauthorsconcludedthatMIismorebeneficialthanbriefadviceforabroadrangeoftargetbehaviors,includingsubstanceuse.Mostrecently,Lundahletal(2009)conductedameta-analysisof119experimentalandquasi-experimentalstudiesacrosssubstanceuse,healthbehaviors,andtreatmentengagementdomains.LundahlestimatedaneffectsizeforMIofg=0.28againstweakcomparisongroupsandanonsignificanteffectofg=0.09againstcompetingactivetreatments.WhiletheyquestiontheresultsoftheHettemaandMiller(2005)meta-analysisduetoinclusionofastronglypositiveoutliersample,theiranalysismaybeundulyinfluencedbyseveralnegativestudiesofMIforsmoking.Incontrast,theyreportthatapproximately75%ofallparticipantsinMIstudiesexperiencepositivegains,withapproximately25%experiencingmoderatetolargegains.Lundahlandcolleaguesofferanswerstoseveralcomponentquestionsinsecondaryanalyses,including:—DoesMIwork?(Yes)
-ShouldI,ormyagency,considerlearningoradoptingMI?(Yes)IsMIonlyindicatedforsubstanceuseproblems?(No)IsMIsuccessfulinmotivatingclientstochange?(Yes)
-IsMIsuccessfulonlywithclientswhohaveminorproblems?(No)-IsMIassuccessfulasotherinterventions?(Yes,exceptwithtobaccouseandsomemiscellaneousdrugproblems,andoftenMIisassuccessfulinlesserdoses)
AreMIeffectsdurable?(Yes,atleastupto1to2years)
-Shouldpractitionerslearn“basicMI”or“MET”?(LearnMItointegratewithotherapproaches;learnMETtotargetspecificbehaviorchanges)
Ismanual-guidedMIsuperiortothealternative?(No)
-DoestheformatofMIinfluenceoutcomes?(No)-DoesprofessionalbackgroundinfluencesuccessofMI?(No)-DoesMIdosagematter?(Yes—indiscretedeliveryforms,moreMIisrelatedtobettereffects)-DoesMIworkformostclients?(Uncertain)-DoesMIworkingroupformats?(Uncertain).WenotethatthemostrecentreviewoftheevidenceforMIingroupformatsindicatesthattheyshowconsiderablepromise(Wagner&Ingersoll,2013).
Intheareaofsubstanceabuse,abroadrangeofpopulationshavebeentreatedwithMIinclinicalandresearchsettings.Treatedpopulationsrangefromyouthexperimentingwithdrinkingthroughadultswithseverealcoholanddrugdependenceproblems,includingthosewhoseaddictionproblemshaveresultedincriminaljusticesysteminvolvement.StudieshaveshowntheefficacyofMItoreducedrinking,increaseabstinencefromdrinking,reduceheavydrinkingdays,facilitateparticipationinharmreductionstrategiessuchasusingneedleexchangeprograms,

Brief Interventions and Motivational Interviewing
Page 14 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
andreducedruguse.Inaddition,MIhasbeenusedtohelppatientswithanumberofmedicaldiagnosesandrelatedhealthconditions,someofwhichhavelessobviousrelationshipswithsubstanceabuse.Inthedomainofmentalhealth,thereismuchgrowthinapplicationsofMI(Arkowitzetal.,2008).Relatingtosubstanceuseproblems,MIhasbeenusedclinicallyandtestedinresearchasadualdisorderintervention,targetingbothsubstanceuseandmentalillness.TheU.S.DepartmentofJusticehasadoptedMIasapreferredpracticeforthosewhoareimprisonedorinvolvedincommunitycorrectionssettingsrelatedtosubstanceabuseissues.ApplicationsinchildprotectiveservicesanddomesticviolencepreventionandtreatmentservicesprovidefurtheropportunitytouseMIwiththoseinvolvedinthelegalsystem.Additionally,MIisbeingincreasinglyappliedtosimultaneousbehaviorchangeinitiatives.Forexample,promisingprojectsshowbenefitsofMIreducingtheriskofalcohol-exposedpregnancybytargetingbothdrinkingandcontraception(Floydetal.,2007).TherearemanypossiblebehavioraltargetsofMIandavarietyofsettingsinwhichtheinterventioncanbedelivered.ThoughMIbeganasanoutpatientinterventionforalcoholproblems,involvingmeetingwithatherapistforuptoanhour,applicationsinbriefermedicalconsultationsarebecomingincreasinglycommon.
Summary&ConclusionsOverall,briefinterventionsshowagreatdealofpromiseforaddressingalcoholandsubstanceabuseissues.Theycanbeeffectivelyappliedwithinavarietyofsettingsthroughseveralframeworksdevelopedtoguidetheirapplications.WhilemanyoftheseframeworksrecommendMI-consistentstrategies,avarietyoftherapeuticinteractiontechniquescouldbeusedtopopulatethem.Forexample,theadvisestrategythatispresentinbothFRAMESandthe5Aswouldpresentdifferentlydependingontheinterventionists’interactionstyle.AspectsofMIthatinvolveattemptingtoelicittheindividual’sperspectiveonanadvisablecourseofaction,suchasaskingpermissionbeforegivingadviceandemphasizingpersonalchoice,mayormaynotbeusedtoenhancethisstepwithintheseframeworks,makingthemmoreorlessconsistentwiththeMImodel.Similarly,whiledistinct,theSOCmodelandMI“grewuptogether”andcomplementoneanother(DiClemente&Velasquez,2002).DevelopersoftheSOCmodelciteMIasavaluableapproachtousewhenpeopleareintheearlierstagesofchange,tobuildinterestinandmotivationforchange.However,withinMItheconceptofstagesisseenmoreasaheuristicthanasareflectionofreality.MIemphasizesthatreadinesstochangeisabyproductofinterpersonalinteractionsandcanfluctuatefrommomenttomoment.Whenconsideringinteractiontechniquesthatmaybeusedwithinbriefinterventionframeworks,MIseemstobealogicalfirstchoiceand,withintheliterature,MIskillsandprinciplesarecommonlyoverlaidonframeworkssuchasSBIRTandthe5As.MIisanefficaciousmethodtofacilitatebehaviorchangewithstrongevidenceforitspositiveimpactonaddictivebehavior.Itoftenachievesgoodoutcomeswithfewersessionsandinlesstimethanothersubstanceabusetreatmentmethods.Ithasbecomeapopularapproachandisusedaroundtheworldforthetreatmentofsubstanceabuseaswellasotherbehavioralchangechallenges.Whiletheclinicalmethodshavebeendetailedthoroughly,usingMIinvariousbriefinterventionframeworkshasnotbeenthoroughlyresearched.Rollnickandcolleagues(2008)advisethatMIshouldonlybeappliedwhenthereisaprimaryfocusonincreasingreadinessforchangeandtheprinciplesandspiritdescribedabovehavebeenintentionallyimplemented.However,theynotethatitisstillunresolvedwhetherthespiritofmotivationalinterviewingcan,infact,becapturedinbriefinteractionsofaslittleas5to10minutes.AsMIexpandsintonewareasofapplicationbeyonditsindividualsubstanceabusecounselingroots,suchasbriefinterventioninprimarycare,thereisaneedtodevelopinnovativemethodsofdelivery,measureoutcomes,andprovideeffectivetrainingforpractitioners,agencies,andtrainers.
PrioritiesforFutureResearchWhileresearchhasshownpromisingresultsthroughapplicationofSBIRT,furtherresearchisneededinanumberofareas.Tostart,briefinterventionsshouldbestudiedinadditionalcaresettingsandwithotherpatientgroups.Asnoted,theenthusiasmforSBIRTthatpromptedtheAmericanCollegeofSurgeonstomandateLevelItraumacenterstoscreeninjuredpatientsforanalcoholusedisorders,andprovidebriefinterventionstothosewhoscreenpositive,wasbasedlargelyonthestrengthofevidencecollectedinprimarycaresettings.FurtherstudyoftheefficacyofSBIRTspecificallyinemergencydepartmentsettingsisneeded(Saitz,2009).Additionally,thebulkofevidencesupportingtheuseofSBIRTsurroundsthescreeningandtreatmentofalcohol-relatedproblems;studiesaddressinghowbriefinterventionsmighteffectivelyimpactothersubstanceabusewouldbehelpful.

Brief Interventions and Motivational Interviewing
Page 15 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
ItshouldalsobenotedthattheBriefInterventioncomponentofSBIRTreferstoarangeofdifferenttherapies.Inotherstudies,differentapproachestotherapyyieldedverydifferentresults.TheefficacyofMotivationalInterviewinghasbeendemonstratedwithbothdrinkingandsubstance-usingpatients(Hettemaetal.,2005).AstudydistinguishingbetweenMIandotherbriefinterventions,suchassimpleadvice,couldofferguidanceonwhichapproach(es)wouldbemostusefulandeffective.TrainingineffectiveapplicationofSBIRTisanotherdirectionforfutureresearch.Whilebriefinterventionscanimprovepatients’reductioninalcoholandsubstanceuse,thereisaninvestmentinstafftrainingrequired.AstudyofhowthelengthofanSBIRTtrainingprogramimpactsimplementationcouldguideorganizationsonwhatamountoftimeandtrainingresourceswouldberequiredtoeffectachangeinpatientoutcomes.Forprimarycarephysicians,anassessmentoftheircurrentuseofscreeningtodetectalcoholorsubstanceuseinpatientscouldprovideaspringboardtocomparesuchpracticeswiththepotentialimprovementsindetectionandtreatmentthroughSBIRT.ItwouldalsobeinterestingtoapplyMIwithprimarycarephysicianstoassesswhatissuestheyfacewiththeimplementationofSBIRTandMIwiththeirpatients.AllowingthemtoexplorethechallengesandpotentialbenefitsofimplementingSBIRTinasupportivecounselingsessionmightilluminatetheobstaclesfacedbyotherpractitionersinavarietyofsettings.
ReferencesAmaro,H.,Ahl,M.,Matsumoto,A.,Prado,G.,Mulé,C.,Kemmemer,A.,…&Mantella,P.(2009).Trialoftheuniversityassistanceprogramforalcoholuseamongmandatedstudents.JournalofStudiesonAlcoholDrugs,Suppl.,45–56.AmericanCollegeofEmergencyPhysicians(ACEP).[AccessedJuly14th,2014).Clinicalpracticeandmanagementpolicystatement:Alcoholscreeninginemergencydepartment.Availableat:http://www.acep.org/Clinical—-Practice-Management/Alcohol-Screening-in-the-Emergency-Department/.Arkowitz,H.,Westra,H.A.,Miller,W.R.,&Rollnick,S.(2008).Motivationalinterviewinginthetreatmentofpsychologicalproblems.NewYork:GuilfordPress.Babor,T.F.,&Grant,M.(Eds.).(1992).Projectonidentificationandmanagementofalcohol-relatedproblems.ReportonphaseII:Arandomizedclinicaltrialofbriefinterventionsinprimaryhealthcare.Geneva,Switzerland:WorldHealthOrganization.Baer,J.S.,Kivlahan,D.R.,&Blume,A.W.(2001).Briefinterventionforheavy-drinkingcollegestudents:4-yearfollow-upandnaturalhistory.AmericanJournalofPublicHealth91,1310–1316.Bandura,A.(1986).Socialfoundationsofthoughtandaction:Asocialcognitivetheory.EnglewoodCliffs,NJ:PrenticeHall.Barry,K.L.(Ed.)(1999).TIP34:Briefinterventionsandbrieftherapiesforsubstanceabuse.DHHSPublicationNo.(SMA)99-3353.DrugandAlcoholDependence,200577,49–59.Bernstein,J.,Bernstein,E.,Tassiopoulos,K.,Heeren,T.,Levenson,S.,&Hingson,R.(2005).Briefmotivationalinterventionataclinicvisitreducescocaineandheroinuse.DrugandAlcoholDependence,77,49–59.Bernstein,E.,Bernstein,J.,etal.(2010)Theimpactofscreening,briefinterventionandreferralfortreatmentinemergencydepartmentpatients’alcoholuse:A3-,6-and12-monthfollow-up.Alcohol&Alcoholism,45,514–519.Epub2010Sep27.Bien,T.H.,Miller,W.R.,&Tonigan,J.S.(1993).Briefinterventionsforalcoholproblems:Areview.Addiction,88,315–335.Burke,B.L.,Arkowitz,H.,&Menchola,M.(2003).Theefficacyofmotivationalinterviewing:Ameta-analysisofcontrolledclinicaltrials.JournalofConsultingandClinicalPsychology,71(5),843–861.Butler,L.H.,&Correia,C.J.(2009).Briefalcoholinterventionwithcollegestudentdrinkers:Face-to-faceversuscomputerizedfeedback.PsychologyofAddictiveBehaviors,23,163–167.

Brief Interventions and Motivational Interviewing
Page 16 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
Chafetz,M.E.(1961)Aprocedureforestablishingtherapeuticcontactwiththealcoholic.QuarterlyJournalofStudiesonAlcohol,22,325–328.Chaftez,M.E.,Blane,H.T.,Abram,H.S.,Golner,J.,Lacy,E.,McCourt,W.F.,…&Meyers,W.(1962).Establishingtreatmentrelationswithalcoholics.JournalofNervousandMentalDiseases,134,395–409.Chafetz,M.E.(1968)Researchinthealcoholclinic:Anaround-the-clockpsychiatricserviceoftheMassachusettsGeneralHospital.AmericanJournalofPsychiatry,124,1674–1679.Cimini,M.D.,Martens,M.P.,Larimer,M.E.,Kilmer,J.R.,Neighbors,C.,&Monserrat,J.M.(2009).Assessingtheeffectivenessofpeer-facilitatedinterventionsaddressinghigh-riskdrinkingamongjudiciallymandatedcollegestudents.JournalofStudiesonAlcoholandDrugs,16,57–66.Copeland,J.(1997).Barrierstoformaltreatmentamongwomenwhoself-managedchangeinaddictivebehaviors.JournalofSubstanceAbuseTreatment,14,183–190.Copeland,J.,Swift,W.,Roffman,R.,&Stephens,R.(2001).Arandomizedcontrolledtrialofbriefcognitive-behavioralinterventionsforcannabisusedisorder.JournalofSubstanceAbuseTreatment,21,55–64.Cuijpers,P.,Riper,H.,&Lemmers,L.(2004).Theeffectsonmortalityofbriefinterventionsforproblemdrinking:Ameta-analysis.Addiction,99,839–845.Daeppen,J.B.,Gaume,J.,Bady,P.,etal.(2007).Briefalcoholinterventionandalcoholassessmentdonotinfluencealcoholuseininjuredpatientstreatedintheemergencydepartment:Arandomizedcontrolledclinicaltrial.Addiction,102,1224–1233.Dawson,D.A.,Grant,B.F.,&Li,T.K.(2005).Quantifyingtherisksassociatedwithexceedingrecommendeddrinkinglimits.Alcoholism:ClinicalandExperimentalResearch,29,902–908.Dempsey,C.L.(2008).Stagesofchangemodel.Encyclopediaofsubstanceabuseprevention,treatment,andrecovery.SAGE.Desy,P.M.,Howard,P.K.,Perhats,C.,&Li,S.(2010).Alcoholscreening,briefintervention,andreferraltotreatmentconductedbyemergencynurses:Animpactevaluation.JournalofEmergencyNursing,36,538–545.DiClemente,C.C.(2003).Addictionandchange:howaddictionsdevelopandaddictedpeoplerecover.NewYork:GuilfordPress.DiClemente,C.C.,&Prochaska,J.O.(1985).Processesandstagesofself-change:Copingandcompetenceinsmokingbehaviorchange.InS.Shiffman&T.A.Wills(Eds.),Copingandsubstanceuse.NewYork:AcademicPress.DiClemente,C.C.,&Velasquez,M.(2002)Motivationalinterviewingandthestagesofchange.InW.R.Miller&S.Rollnick(Eds.),Motivationalinterviewing,secondedition:Preparingpeopleforchange.NewYork:Guilford.D’Onofrio,G.,Pantalon,M.V.,Degutis,L.C.,etal.(2008).Briefinterventionforhazardousandharmfuldrinkersintheemergencydepartment.AnnalsofEmergencyMedicine,51,742–750.Edwards,G.,Duckitt,A.,Oppenheimer,E.,Sheehan,M.,&Taylor,C.(1983).Whathappenstoalcoholics?Lancet,2,269–271.Ewing,J.A.(1984).Detectingalcoholism:TheCAGEquestionnaire.JournaloftheAmericanMedicalAssociation,252,1905–1907.Fiellin,D.A.,Reid,M.C.,&O’Connor,P.G.(2000).Screeningforalcoholproblemsinprimarycare:Asystematicreview.ArchivesofInternalMedicine,160,1977–1989.Fiore,M.C.,Bailey,W.C.,Cohen,S.J.,etal.(October2000).Treatingtobaccouseanddependence.Quickreferenceguideforclinicians.Rockville,MD:USDepartmentofHealthandHumanServices,PublicHealthService.

Brief Interventions and Motivational Interviewing
Page 17 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
Fleming,M.F.,Mundt,M.P.,French,M.T.,Manwell,L.B.,Staauffacher,E.A.,&Barry,K.L.(2002).Briefphysicianadviceforproblemdrinkers:Long-termefficacyandcost-benefitanalysis.AlcoholismClinicalandExperimentalResearch,26,36–43.Floyd,R.L.,Sobell,M.,Velasquez,M.M.,Ingersill,K.,Nettleman,M.,Sobell,L.,…Nagaraja,J.(2007).Preventingalcohol-exposedpregnancies:Arandomizedcontrolledtrial.AmericanJournalofPreventiveMedicine,32,1–10.Fortney,J.,&Booth,B.M.(2001).Accesstosubstanceabuseservicesinruralareas.RecentDevelopmentsinAlcoholism,15,177–197.Gavin,D.R.,Ross,H.E.,&Skinner,H.A.(1989).DiagnosticvalidityoftheDrugAbuseScreeningTestintheassessmentofDSM-IIIdrugdisorders.BritishJournalofAddiction,84,301–307.Gentilello,L.M.,Rivara,F.P.,&Donovan,D.M.(1999).Alcoholinterventionsinatraumacenterasameansofreducingtheriskofinjuryrecurrence.AnnalsofSurgery,230,473–483.Gentilello,L.M.,Ebel,B.E.,Wickizer,T.M.,Salkever,D.S.,&Rivara,F.P.(2005).Alcoholinterventionsfortraumapatientstreatedinemergencydepartmentsandhospitals:acostbenefitanalysis.AnnalsofSurgery,241,541–550.Goldstein,M.G.,Whitlock,E.P,&DePue,J.(2004).Multiplebehavioralriskfactorinterventionsinprimarycare:Summaryofresearchevidence.AmericanJournalofPreventiveMedicine,27(2S):61–70.Grandes,G.,Sanchez,A.,Cortada,J.M.,Balague,L.,Calderon,C.,Arrazola,A.,…Millan,E.(2008).Isintegrationofhealthylifestylepromotionintoprimarycarefeasible?Discussionandconsensussessionsbetweencliniciansandresearchers.BMCHealthServicesResearch,8,213–225.Havard,A.,Shakeshaft,A.,&Sanson-Fisher,R.(2008).Systematicreviewandmeta-analysesofstrategiestargetingalcoholproblemsinemergencydepartments:Interventionsreducealcohol-relatedinjuries.Addiction,103,368–376.Hettema,J.,Steele,J.,&Miller,W.R.(2005).Motivationalinterviewing.AnnualReviewofClinicalPsychology,1,91–111.Hettema,J.E.,&Sorensen,J.S.(2009).AccesstocareformethadonemaintenancepatientsintheUnitedStates.InternationalJournalofMentalHealthandAddictions,6,407–420.Hubbard,R.L.,Craddock,S.G.,&Anderson,J.(2003).Overviewof5-yearfollow-upoutcomesintheDrugAbuseTreatmentOutcomeStudies(DATOS).JournalofSubstanceAbuseTreatment,25,125–134.Jonas,D.E.,Garbutt,J.C.,Amick,H.R.,Brown,J.M.,Brownles,K.A.,Council,C.L.,…Harris,R.P.(2012).Behavioralcounselingaftercareeningforalcoholmisuseinprimarycare:Asystematicreviewandmeta-analysisfortheU.S.PreventiveServicesTaskForce.AnnalsofInternalMedicine.http://annals.org/on10/09-2012Kaner,E.F.,Dickinson,H.O.,Beyer,F.,Plenaar,E.,Schelesinger,C.,Campbell,F.,…Heather,N.(2009).Theeffectivenessofbriefalcoholinterventionsinprimarycarepopulations:Asystematicreview.DrugandAlcoholReview,28(3),301–323.Kristenson,H.,Ohlin,H.,Hulten-Nosslin,M.B.,Trell,E.,&Hood,B.(1983).Identificationandinterventionofheavydrinkinginmiddle-agedmen:Resultsandfollow-upof24-60monthsoflong-termstudywithrandomizedcontrols.Alcoholism:ClinicalandExperimentalResearch,7,203–209.Kuchipudi,V.,Hobein,K.,Fleckinger,A.,&Iber,F.L.(1990).Failureofa2-hourmotivationalinterventiontoalterrecurrentdrinkingbehaviorinalcoholicswithgastrointestinaldisease.JournalofStudiesonAlcohol,51,356–360.LaBrie,J.W.,Huchting,K.,Tawalbeh,S.,Pedersen,E.R.,Thompson,A.D.,Shelesky,K.,etal.(2008).Arandomizedmotivationalenhancementpreventiongroupreducesdrinkingandalcoholconsequencesinfirst-yearcollegewomen.PsychologyofAddictiveBehaviors:JournaloftheSocietyofPsychologistsinAddictiveBehaviors,22,149–155.LaBrie,J.W.,Lamb,T.F.,Pedersen,E.R.,&Quinlan,T.(2006).Agroupmotivationalinterviewingintervention

Brief Interventions and Motivational Interviewing
Page 18 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
reducesdrinkingandalcohol-relatedconsequencesinadjudicatedcollegestudents.JournalofCollegeStudentDevelopment,47,267–280.LaBrie,J.W.,Pedersen,E.R.,Lamb,T.F.,&Quinlan,T.(2007).Acampus-basedmotivationalenhancementgroupinterventionreducesproblematicdrinkinginfreshmenmalecollegestudents.AddictiveBehaviors,32,889–901.Labrie,J.W.,Thompson,A.D.,Huchting,K.,Lac,A.,&Buckley,K.(2007).Agroupmotivationalinterviewinginterventionreducesdrinkingandalcohol-relatednegativeconsequencesinadjudicatedcollegewomen.AddictiveBehaviors,32,2549–2562.Larimer,M.E.,Cronce,J.M.,Lee,C.M.,&Kilmer,J.R.(2004–2005).Briefinterventionincollegesettings.AlcoholResHealth,28,94–104.Larimer,M.E.,&Cronce,J.M.(2002).Identification,prevention,andtreatment:Areviewofindividual-focusedstrategiestoreduceproblematicalcoholconsumptionbycollegestudents.JournalofStudiesonAlcohol,Suppl.14,148–163.Leake,G.J.,&King,A.S.(1977).Effectofcounselorexpectationsonalcoholicrecovery.AlcoholHealth&ResearchWorld,11,16–22.Libby,T.A.(2008).BriefInterventions.InG.Fisher&N.Roget(Eds.),Encyclopediaofsubstanceabuseprevention,treatment,andrecovery.SAGE.Lowenstein,S.R.,Weissberg,M.,&Terry,D.(1990).Alcoholintoxication,injuriesanddangerousbehaviors—andtherevolvingemergencydepartmentdoor.JournalofTrauma,30,1252–1257.Lundahl,B.W.,Tollefson,E.,Kunz,C.,Brownell,C.,&Burke,B.L.(2009).Ameta-analysisofmotivationalinterviewing:Twentyfiveyearsofempiricalstudies.ResearchonSocialWorkPractice,65,1232–1245.MacMaster,S.(2005).Experienceswith,andperceptionsof,barrierstosubstanceabuseandHIVservicesamongAfrican-Americanwomenwhousecrackcocaine.JournalofEthnicityinSubstanceAbuse,4,53–75.Maciosek,M.V.,Coffield,A.B.,Edwards,N.M.,Flottemesch,T.J.,Goodman,M.J.,&Solberg,L.I.(2006).Prioritiesamongeffectiveclinicalpreventiveservices:Resultsofasystematicreviewandanalysis.AmericanJournalofPreventiveMedicine,31,52–61.MacKenzie,D.M.,Langa,A.,&Brown,T.M.(1996).Identifyinghazardousorharmfulalcoholuseinmedicaladmissions:AcomparisonofAUDIT,CAGEandbriefMAST.AlcoholandAlcoholism,31(6),591–599.Madras,B.K.,Compton,W.M.,Avula,D.,Stegbauer,T.,Stein,J.B.,&Clark,H.W.(2009).Screening,briefinterventions,referraltotreatment(SBIRT)forillicitdrugandalcoholuseatmultiplehealthcaresites:Comparisonatintakeand6monthslater.DrugandAlcoholDependence,99,280–295.Marlatt,G.A.,Baer,J.S.,&Kivlahan,D.R.(1998).Screeningandbriefinterventionforhigh-riskcollegestudentdrinkers:Resultsfroma2-yearfollow-upassessment.JournalofConsultingandClinicalPsychology,66,604–615.McDonald,A.J.,Wang,N.,&Camargo,C.A.(2004).USemergencydepartmentvisitsforalcohol-relateddiseasesandinjuriesbetween1992and2000.ArchivesofInternalMedicine,164,531–537.McGlynn,E.A.,Asch,S.M.,&Adams,J.(2003).ThequalityofhealthcaredeliveredtoadultsintheUnitedStates.NewEnglandJournalofMedicine,348,2635–2645.McKay,J.R.(2005).Isthereevidenceforextendedinterventionsforalcoholanddrugusedisorders?Addiction,11,1594–1610.McKnight-Eily,L.R.,Liu,Y.,Brewer,R.D.,Kanny,D.,Lu,H.,Denny,C.H.,Balluz,L.,Collins,J.(2014)Vitalsigns:Communicationbetweenhealthprofessionalsandtheirpatientsaboutalcoholuse—44statesandDistrictofColumbia,2011.MorbidityandMortalityWeekly,63,16–23.Miller,W.R.(1983).Motivationalinterviewingwithproblemdrinkers.BehaviouralPsychotherapy11,147–172.

Brief Interventions and Motivational Interviewing
Page 19 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
Miller,W.R.,Sovereign,R.G.,&Krege,B.(1988).Motivationalinterviewingwithproblemdrinkers:II.TheDrinker’sCheck-upasapreventiveintervention.BehaviouralPsychotherapy,16,251–268.Miller,W.R.,Benefield,R.G.,&Tonigan,J.S.(1993).Enhancingmotivationforchangeinproblemdrinking:Acontrolledcomparisonoftwotherapiststyles.JournalofConsultingandClinicalPsychology,61,455–461.Miller,W.R.,&Sanchez,V.C.(1993).Motivatingyoungadultsfortreatmentandlifestylechange.InG.Howard(Ed.),Issuesinalcoholuseandmisuseinyoungadults.NotreDame,IN:UniversityofNotreDamePress.Miller,W.R.,&Rollnick,S.(2013).Motivationalinterviewing:Helpingpeoplechange.NewYork:Guilford.Miller,W.R.,&Rose,G.S.(2009).Towardatheoryofmotivationalinterviewing.AmericanPsychologist,64,527–537.Mischke,H.D.,&Venneri,R.L.(1987).ReliabilityandvalidityoftheMAST,MortimerFilkinsquestionnaireandCAGEinDWIassessment.JournalofStudiesonAlcohol,48,492–501.Moyer,A.,Finney,J.W.,Swearingen,C.E.,&Vergun,P(2002).Briefinterventionsforalcoholproblems:Ameta-analyticreviewofcontrolledinvestigationsintreatmentseekingandnon-treatmentseekingpopulations.Addiction,97,279–292.Murphy,J.G.,Duchnick,J.J.,&Vuchinich,R.E.(2001).Relativeefficacyofabriefmotivationalinterventionforcollegestudentdrinkers.PsychologyofAddictiveBehaviors,15,373–379.Murphy,J.G.,Benson,T.A.,&Vuchinich,R.E.(2004).Acomparisonofpersonalizedfeedbackforcollegestudentdrinkersdeliveredwithandwithoutamotivationalinterview.JournalofStudiesonAlcohol,65,200–203.NationalInstituteonAlcoholAbuseandAlcoholism.(2005).Helpingpatientswhodrinktoomuch:Aclinician’sguide.NIHPublicationNo.05–3769.Bethesda,MD:NIH.Nilsen,P.,Baird,J.,Mello,M.J.,etal.(2008).Asystematicreviewofemergencycarebriefalcoholinterventionsforinjurypatients.JournalofSubstanceAbuseTreatment,35(2),184–201.Epub2008Feb20.Perz,C.A.,DiClemente,C.C.,&Carbonari,J.P.(1996).Doingtherightthingattherighttime:Theintersectionofstagesandprocessesofchangeinsuccessfulsmokingcessation.HealthPsychology,15,462–468.Prochaska,J.O.,&DiClemente,C.C.(2005).Thetranstheoreticalapproach.InJ.C.Norcross&M.R.Goldfried(Eds.),Handbookofpsychotherapyintegration(2nded.,pp.147–171).NewYork:OxfordUniversityPress.ProjectMATCHResearchGroup.(1997).Matchingalcoholismtreatmentstoclientheterogeneity:ProjectMATCHpost-treatmentdrinkingoutcomes.JournalofStudiesonAlcohol,58,7–29.Rehm,J.,Room,R.,Graham,K.,Monteiro,M.,Gmel,G.,&Sempos,C.T.(2003).Therelationshipofaveragevolumeofalcoholconsumptionandpatternsofdrinkingtoburdenofdisease:Anoverview.Addiction,98,1209–1228.Rollnick,S.,&Miller,W.R.(1995).Whatismotivationalinterviewing?BehaviouralandCognitivePsychotherapy,23,325–334.Rollnick,S.,Miller,W.R.,&Butler,C.C.(2008).Motivationalinterviewinginhealthcare.NewYork:GuilfordPress.Rubak,S.,Sandbaek,A.,Lauritzen,T.,&Christensen,B.(2005).Motivationalinterviewing:Asystematicreviewandmeta-analysis.TheBritishJournalofGeneralPractice,55(513),305–312.Saitz,R.(2005).Unhealtyalcoholuse.NewEnglandJournalofMedicine,352,596–607.Saitz,R.SBIRT:Hastheenthusiasmoutpacedtheevidence?Yes!(2009).InE.Bernstein,J.A.Bernstein,J.B.Stein,&R.Saitz(Eds.),SBIRTinemergencycaresettings:Arewereadytotakeittoscale?AcademicEmergencyMedicine,16(11),1072–1077.SAMHSA.(2006).NationalSurveyofSubstanceAbuseTreatmentServices(N-SSATS).http://wwwdasis.samhsa.gov/webt/state_data/US06.pdf

Brief Interventions and Motivational Interviewing
Page 20 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
Saunders,J.B.,Aasland,O.G.,Babor,T.F.,delaFuente,J.R.,&Grant,M.(1993).DevelopmentoftheAlcoholUseDisordersIdentificationTest(AUDIT):WHOcollaborativeprojectonearlydetectionofpersonswithharmfulalcoholconsumption.II.Addiction,88,791–804.Schaus,J.F.,Sole,M.L.,McCoy,T.P.,Mullett,N.,&O’Brien,M.C.(2009).Alcoholscreeningandbriefinterventioninacollegestudenthealthcenter:Arandomizedcontrolledtrial.JournalofStudiesonAlcoholandDrugs,Suppl.,131–141.Schermer,C.R.,Moyers,T.B.,Miller,W.R.,&Bloomfield,L.A.(2006).Traumacenterbriefinterventionsforalcoholdisordersdecreasesubsequentdrivingundertheinfluencearrests.JournalofTrauma,60,29–34.Selzer,M.L.(1971).TheMichiganAlcoholismScreeningTest:Thequestforanewdiagnosticinstrument.AmericanJournalofPsychiatry,127,1653–1658.Solberg,L.I.,Maciosek,M.V.,&Edwards,N.M.(2008).Primarycareinterventiontoreducealcoholmisuserankingitshealthimpactandcosteffectiveness.AmericanJournalofPreventiveMedicine,34,143–152.Stephens,R.S.,Roffman,R.A.,&CurtinL.(2000).Comparisonofextendedversusbrieftreatmentsformarijuanause.JournalofConsultingandClinicalPsychology,68,898–908.SubstanceAbuseandMentalHealthServicesAdministration.(2009).Resultsfromthe2008NationalSurveyonDrugUseandHealth:Nationalfindings.Rockville,MD:OfficeofAppliedStudies,NSDUHSeriesH-36,HHSPublicationNo.SMA09-4434.SubstanceAbuseandMentalHealthServicesAdministration.(2010).Resultsfromthe2009NationalSurveyonDrugUseandHealth:VolumeI.SummaryofNationalFindingsRockville,MD:OfficeofAppliedStudies,NSDUHSeriesH-38A,HHSPublicationNo.SMA10-4856.Sutton,S.(2001).Backtothedrawingboard?Areviewofapplicationsofthetranstheoreticalmodeltosubstanceuse.Addiction,96,175–186.UnitedNationsOfficeonDrugsandCrime.(UNODC).(2009).WorldDrugReport.http://www.unodc.org/documents/wdr/WDR_2009/WDR2009_eng_web.pdfU.S.DepartmentofHealthandHumanServices,CentersforDiseaseControlandPrevention.(2007).NationalHospitalAmbulatoryMedicalCareSurvey:2005emergencydepartmentsummary.Washington,DC:NationalCenterforHealthStatistics,386.Vaca,F.,Winn,D.,Anderson,C.,Kim,D.,&Arclia,M.(2011).Six-monthfollow-upofcomputerizedalcoholscreening,briefintervention,andreferraltotreatmentintheemergencydepartment.SubstanceAbuse,32(11),144–152.Walters,S.T.,Vader,A.M.,Harris,T.R.,&Jouriles,E.N.(2009).Reactivitytoalcoholassessmentmeasures:Anexperimentaltest.Addiction,104,1305–1310.Wagner,C.C.,&Ingersoll,K.S.(2013).TheevidenceforMIgroups.InC.C.Wagner&K.S.Ingersoll(Eds.),Motivationalinterviewingingroups(pp.70–86).NewYork:GuilfordPress.Wells-Parker,E.,&Williams,M.(2002).Enhancingtheeffectivenessoftraditionalinterventionwithdrinkingdriversbyaddingbriefindividualinterventioncomponents.SocialScienceResearch,63,655–664.West,R.(2005).Timeforachange:Puttingthetranstheoretical(stagesofchange)modeltorest.Addiction,100,1036–1039.Whitlock,E.P.,Orleans,C.T.,Pender,N.,&Allan,J.(2002).Evaluatingprimarycarebehavioralcounselinginterventions:Anevidence-basedapproach.AmericanJournalofPreventiveMedicine,22,267–284.Whitlock,E.P.,Polen,M.R.,Green,C.A.,Orleans,T.,&Klein,J.(2004).Behavioralcounselinginterventionsinprimarycaretoreducerisky/harmfulalcoholusebyadults:AsummaryoftheevidencefortheU.S.PreventiveServicesTaskForce.AnnalsofInternalMedicine,140,557–568.

Brief Interventions and Motivational Interviewing
Page 21 of 21PRINTED FROM OXFORD HANDBOOKS ONLINE (www.oxfordhandbooks.com). (c) Oxford University Press, 2014. All RightsReserved. Under the terms of the licence agreement, an individual user may print out a PDF of a single chapter of a title in OxfordHandbooks Online for personal use (for details see Privacy Policy).Subscriber: University of New Mexico; date: 16 October 2014
WorldHealthOrganization.(2004).Globalstatusreportonalcohol.Geneva:WorldHealthOrganization.Wutzke,S.E.,Conigrave,K.M.,Saunders,J.B.,&Hall,W.D.(2002).Thelong-termeffectivenessofbriefinterventionsforunsafealcoholconsumption:A10yearfollow-up.Addiction,97,665–675.
JenniferHettemaJenniferHettemaisPsychologyFellowatUniversityofCalifornia,SanFrancisco.ChristopherC.WagnerChristopherC.Wagner,VirginiaCommonwealthUniversityKarenS.IngersollKarenS.Ingersoll,UniversityofVirginiaJenniferM.RussoJenniferM.Russo,UniversityofVirginia