Mood and physiological effects of subcutaneous nicotine in smokers and never-smokers
11
ELSEVIER Drug and Alcohol Dependence 44 (I 997) 10% 115 Mood and physiological effects of subcutaneous nicotine in smokers and never-smokers Jonathan Foulds*, John A. Stapleton, Nicholas Bell, John Swettenham, Martin J. Jarvis, Michael A.H. Russell Heulth Behmiouv Unit, Institute of Psychicmy, 4 Windsor Walk, London SE5 8AF, UK Received 7 August 1996; revised 28 November 1996; accepted 28 November 1996 -- Abstract This study compared the effect of subcutaneous nicotine injections (2 x 0.3 mg and 2 x 0.6 mg) with saline on subjective and physiological measures in 18 never-smokers and 18 smokers (24-h nicotine deprived), under conditions of rest and cognitive testing. Prior to the injections the mood of the smokers had deteriorated to a level significantly below that of the never-smokers as a result of tobacco withdrawal. Cognitive tests caused reductions in calmness and increased alertness but there was no evidence of nicotine improving mood in either group under either condition. The 0.6 mg dose worsened mood in never-smokers and caused unpleasant symptoms (e.g. dizziness and arm pain) in both groups. Compared with smokers, never-smokers experienced stronger symptoms of nicotine toxicity and a greater reduction in alertness in response to the 0.6 mg dose, suggesting chronic tolerance to some nicotine effects in smokers. Nicotine produced similar increases in heart rate and decreases in finger pulse volume in both groups. Our results imply that if nicotine has a mood enhancing effect it occurs only after tolerance has been acquired to its primary adverse effects, and that its ability to reverse the mood deterioration caused by tobacco withdrawal is susceptible to situational factors such as our experimental conditions. 0 1997 Elseveier Science Ireland Ltd. Ke~~\+‘ords: Nicotine; Smokers; Non-smokers; Mood; Subjective effects; Heart-rate; Tolerance 1. Introduction Smokers frequently claim that cigarettes help reduce their subjective stress and anxiety and increase feelings of calmness and relaxation. For example, in one study 73% of smokers claimed to smoke more when worried (Russell et al.. 1974). and in a study of adolescent smokers, ‘feeling calmer’ was the most frequently (64”/0) reported subjective effect of smoking cigarettes (Mc- Neil1 et al., 1987). It has been assumed that the sub- stance in tobacco responsible for these subjective effects is nicotine (US Surgeon General, 1988). However, it remains unclear how nicotine can have sedative sub- * Corresponding author. Present address: Department of Addictive Behaviour, St George’s Hospital Medical School, Cranmer Terrace, London SWI7 ORE. Tel.: +44 181 7252783;fax: +44 181 7252914. jective effects when there is considerable evidence that the primary physiological effects are stimulant in na- ture. For example, a cigarette-sized dose of nicotine produces an increase in heart-rate, plasma adrenaline and noradrenaline (Cryer et al., 1976), and generally produces EEG changes indicative of increased arousal and alertness such as a reduction in theta-power and an increase in dominant alpha-frequency (Church, 1989; Foulds et al., 1994). This contrast between the reported subjective effects of nicotine and the measured physiological effects has been called the ‘nicotine paradox’ (Nesbitt, 1973). Added to this is the fact that smokers also (less fre- quently) report stimulant subjective effects, such as an increase in alertness from smoking in certain situations (Russell et al, 1974). Various explanations for these observations have been offered. It has been suggested 0376~8716:97/$17.00 G 1997 Elseveier Science Ireland Ltd. All rights reserved PII SO.376.87 16(96)01327-O
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Mood and physiological effects of subcutaneous nicotine in smokers and never-smokers

ELSEVIER Drug and Alcohol Dependence 44 (I 997) 10% 115
Mood and physiological effects of subcutaneous nicotine in smokers and never-smokers
Jonathan Foulds*, John A. Stapleton, Nicholas Bell, John Swettenham, Martin J. Jarvis, Michael A.H. Russell
Heulth Behmiouv Unit, Institute of Psychicmy, 4 Windsor Walk, London SE5 8AF, UK
Received 7 August 1996; revised 28 November 1996; accepted 28 November 1996
--
Abstract
This study compared the effect of subcutaneous nicotine injections (2 x 0.3 mg and 2 x 0.6 mg) with saline on subjective and physiological measures in 18 never-smokers and 18 smokers (24-h nicotine deprived), under conditions of rest and cognitive testing. Prior to the injections the mood of the smokers had deteriorated to a level significantly below that of the never-smokers as a result of tobacco withdrawal. Cognitive tests caused reductions in calmness and increased alertness but there was no evidence of nicotine improving mood in either group under either condition. The 0.6 mg dose worsened mood in never-smokers and caused unpleasant symptoms (e.g. dizziness and arm pain) in both groups. Compared with smokers, never-smokers experienced stronger symptoms of nicotine toxicity and a greater reduction in alertness in response to the 0.6 mg dose, suggesting chronic tolerance to some nicotine effects in smokers. Nicotine produced similar increases in heart rate and decreases in finger pulse volume in both groups. Our results imply that if nicotine has a mood enhancing effect it occurs only after tolerance has been acquired to its primary adverse effects, and that its ability to reverse the mood deterioration caused by tobacco withdrawal is susceptible to situational factors such as our experimental conditions. 0 1997 Elseveier Science Ireland Ltd.
Ke~~\+‘ords: Nicotine; Smokers; Non-smokers; Mood; Subjective effects; Heart-rate; Tolerance
1. Introduction
Smokers frequently claim that cigarettes help reduce their subjective stress and anxiety and increase feelings of calmness and relaxation. For example, in one study 73% of smokers claimed to smoke more when worried (Russell et al.. 1974). and in a study of adolescent smokers, ‘feeling calmer’ was the most frequently (64”/0) reported subjective effect of smoking cigarettes (Mc- Neil1 et al., 1987). It has been assumed that the sub- stance in tobacco responsible for these subjective effects is nicotine (US Surgeon General, 1988). However, it remains unclear how nicotine can have sedative sub-
* Corresponding author. Present address: Department of Addictive Behaviour, St George’s Hospital Medical School, Cranmer Terrace, London SWI7 ORE. Tel.: +44 181 7252783; fax: +44 181 7252914.
jective effects when there is considerable evidence that the primary physiological effects are stimulant in na- ture. For example, a cigarette-sized dose of nicotine produces an increase in heart-rate, plasma adrenaline and noradrenaline (Cryer et al., 1976), and generally produces EEG changes indicative of increased arousal and alertness such as a reduction in theta-power and an increase in dominant alpha-frequency (Church, 1989; Foulds et al., 1994).
This contrast between the reported subjective effects of nicotine and the measured physiological effects has been called the ‘nicotine paradox’ (Nesbitt, 1973). Added to this is the fact that smokers also (less fre- quently) report stimulant subjective effects, such as an increase in alertness from smoking in certain situations (Russell et al, 1974). Various explanations for these observations have been offered. It has been suggested
0376~8716:97/$17.00 G 1997 Elseveier Science Ireland Ltd. All rights reserved PII SO.376.87 16(96)01327-O

that nicotine has stimulant properties at low doses and sedative qualities at high doses (Ashton et al., 1980) and that nicotine has stimulant qualities when the individual is in a relaxed, unstimulated state, but seda- tive qualities when stressed or overstimulated (Golding and Mangan, 1982). It has also been suggested that perceived sedative enhancements may not be primary improvements, but rather a reversal of a mood deficit (e.g. Hughes, 1991) resulting from tobacco abstinence. A series of studies by Parrott and colleagues supports the ‘withdrawal-relief theory and also found that smoking can reduce stress and increase arousal simulta- neously (Parrott, 1995). Each of these theories has some supporting data, but even within th’e supportive studies there are often inconsistencies and contradictions. For example, one of the main studies quoted as showing a biphasic dose response relationship to intravenous nicotine (Ashton et al., 1980) estimated a maximal stimulant effect at a total dose of 0.05 mg (equivalent to less than one twentieth of a cigarette) and a maximal scdativc effect at a dose of 0.3 mg. Thus the dose producing a sedative effect was less than half of the typical nicotine intake from a single cigarette, and was therefore a relatively low dose compared with that of smoking. Even those studies which have found an effect of baseline subjective state on subsequent nicotine effect have generally failed to find a sedative effect of nicotine under any conditions (e.g. Perkins et al., 1992a).
Most studies which have examined the subjective effects of nicotine have administered it in tobacco and so have been unable to accurately control the dose or provide an adequate placebo. Very few have studied the effects of nicotine in non-smokers, in whom any mood changes are clearly not attributable to withdrawal-re- lief. However, the evidence in nonsmokers, though limited, suggests that nicotine either has no significant effect on mood or increases arousal and worsens mood, e.g. making subjects more ‘jittery’ and less relaxed (Perkins et al., 1993. 1994a) or increasing tension and depression (Newhouse et al., 1990). One study (Heish- man et al., 1993) found that 4 mg nicotine gum in- creased ratings on the MBG scale of the addiction research centre inventory in non-smokers (this scale is intended as a measure of stimulant/euphoriant drug effects). However, these non-smokers simultaneously reported a significant decrease in their desire for an- other dose. and so a straightforward mood improve- ment seems unlikely.
One aim of the present study was to assess whether nicotine. administered by subcutaneous injection in a placebo-controlled manner, has any beneficial effect on mood in never-smokers. If an enhancement were found it could only be interpreted as a primary effect. since tobacco withdrawal is not an issue for these subjects. This study also attempted to examine whether any such enhancement is sedative or stimulant in nature and
whether this is affected by relaxing or stressing situa- tions. A second aim was to assess how far any mood deterioration in abstaining smokers can be reversed by acute nicotine administration and whether the degree of enhancement is greater than any primary effect in never-smokers.
Another issue of interest is whether smokers develop chronic tolerance to nicotine’s effects.
It is clear that both smokers and non-smokers rapidly develop acute tolerance to some of nicotine’s cardiovascular and subjective effects (Porchet et al., 1988; Russell et al., 1990). Until recently, evidence of chronic tolerance has been limited to the observation that adolescent smokers frequently experience unpleas- ant symptoms from the first few cigarettes but once they have become regular smokers these disappear (US Surgeon General, 1988). Four recent studies have pro- vided some evidence that non-smokers obtain a greater subjective effect than smokers from a given dose of nicotine. However, in one of these studies the smokers were not abstinent and so there was a confounding of acute and chronic tolerance (Pomerleau et al., 1993). Similarly, in the studies by Perkins et al. (1993. 1994a) the smokers were only required to be abstinent overnight and so there was a chance that some had significant blood nicotine concentrations (e.g., 2 - 10 rig/ml) at baseline (Benowitz et al., 1982). A compari- son between nicotine sensitivity in smokers and non- smokers can only be made from a baseline in which both groups have the same blood-nicotine concentra- tions (i.e., zero) requiring the smokers to abstain from nicotine for at least 24 h (typically 12 half-lives, or six in a slow metabolizer, Benowitz, 1988). The other study (Srivastava et al., 1991) found greater subjective effects in non-smokers than smokers from similar plasma nicotine concentrations achieved via a transdermal patch. A final aim of the present study was to assess whether 24-h nicotine-deprived smokers obtain smaller physiological and subjective responses to a measured dose of nicotine than never-smokers, which would sug- gest the presence of chronic tolerance.
This study formed part of a larger study which also examined the effect of nicotine on cognitive perfor- mance (Foulds et al., 1996).
2. Materials and methods
2.1. Subjects
Eighteen smokers (mean daily consumption is 21 cigarettes) and 18 never-smokers (mean lifetime con- sumption is two cigarettes, range O-12, no tobacco in previous year) completed the study. Smokers were re- quired to have smoked at least 15 cigarettes per day for 2 years, while never-smokers were those with a life-time

consumption of fewer than 20 cigarettes (or other to- bacco equivalent), and no tobacco use in the previous year. The mean height and weight of the two groups were similar and both comprised nine men and nine women. Smokers tended to be a little older (30.9 versus 25.4 years) and to have had 2 fewer years of education on average. All subjects provided written informed consent and the study was approved by the Institute of Psychiatry Ethical Committee.
This was a double-blind, placebo-controlled cross- over study with three conditions (2 x saline, 2 x 0.3 mg nicotine base and 2 x 0.6 mg nicotine base) tested at weekly intervals after an initial practice session. Order of conditions was counterbalanced, such that three smokers and three never-smokers were randomly allo- cated to each dose order. The doses were given in the form of two injections in order to minimize any toxic symptoms and to maintain moderate nicotine levels for a sufficient time period. The injections were given sub- cutaneously, 40 min apart, into the upper left arm using a fine needle (gauge 25). The average dose per injection was 4.4 /lg!kg (0.3 mg dose) and 8.8 jig/kg (0.6 mg dose). Each 0.6 mg injection produced approximately half the blood nicotine concentration typically obtained by smoking a cigarette (Foulds et al., 1994).
2.3. Produres
Each subject attended the laboratory on four occa- sions with the first visit serving as a familiarization session, and to check for any unusual sensitivity to nicotine (all subjects received two 0.3 mg nicotine injec- tions, single blind). Smokers smoked normally on the day of their first visit but were required to abstain from all forms of nicotine use for 24 h prior to visits 2-4 to ensure blood nicotine concentrations close to zero. Abstinence was confirmed by an expired carbon- monoxide concentration of less than 10 ppm in all subjects. Subjects were also required to abstain from alcohol (24 h) and caffeine (2 h) prior to each visit. All visits for each subject began at the same time of day on the same day of the week.
Each session comprised three periods of data record- ing, separated by the two injections. In the period prior to the first injection subjects completed a tobacco with- drawal symptom questionnaire followed by a 35-min battery of computerised cognitive performance tests, the details of which are described elsewhere (Foulds et al., 1996). They were then seated in a comfortable reclining chair and connected to a polygraph in order to record resting physiological measures. Electrodes were attached and subjects were instructed to sit com- fortably for 10 min, while the baseline physiological
responses were recorded. They then completed the base- line mood and symptom questionnaires. After receiving the first injection subjects sat still for 15 min while the physiological measures were recorded again. The mood and symptom questionnaires were then completed for a second time followed by a 20 min rest which preceded the second subcutaneous injection. In the final period subjects completed. the cognitive test battery again prior to the third completion of the mood and symptom ratings. The cognitive performance tasks were expected to serve as a stressor and their effect. as measured by the final mood ratings, might be modified by the differ- ent nicotine doses.
The 24 h tobacco withdrawal symptoms question- naire, completed once at the beginning of each session. asked subjects to rate how much they had experienced six symptoms over the previous 24 h on a five-point scale (0, not at all; and 4, extremely). The symptoms were: irritability, restlessness, difficulty concentrating. feeling tense, increased appetite. and feeling miserable. A total score for each subject at each visit was obtained by summing the six ratings. This type of questionnaire has previously been shown to be sensitive to tobacco withdrawal and has been used in numerous smoking cessation studies (West and Russell, 1988).
The main measure of mood state was a slightly modified version of the Bond-Lader mood scale (Bond and Lader. 1974). The only alteration from the original version was that subjects were instructed to rate their feelings ‘in the last 5 min’ rather than at ‘a moment in time’. This scale consists of sixteen 100 mm bipolar visual-analogue-scales (VAS) measuring three general mood factors: 1. Akrtness (alert/drowsy, atten- tive/dreamy, lethargic/energetic, muzzy/clear-headed, well-coordinated:‘clumsy, mentally-slow:quick-witted, strong/feeble, interested/bored, incompetent/proficient); 2. Contentednnrss (happy;sad, antagonistic/amicable. troubled/tranquil, contented/discontented, withdrawn, gregarious); and 3. Cdmness (calm/excited, tenseire- laxed). Subjects placed a mark on each line to indicate how they were feeling, and their score was measured by the number of millimetres along the line (or 100 minus the distance for negative scales). A single score for each factor was computed as the mean response on the items comprising the factor. This scale has been found to be sensitive to drug-induced mood changes in numerous previous studies.
In addition to the Bond-Lader mood scale, subjects also completed a questionnaire designed to measure the strength of a number of other symptoms thought to be affected by nicotine. This consisted of 13 100 mm VASs with one end indicating absence of the symptom and the other that the symptom was severe. Subjects rated

the strength of these symptoms as experienced in the previous 5 min. A mean score was computed for items covering five main areas: (1) adverse nicotine symptoms covered affects associated with nicotine toxicity (sweat- ing, nausea, dizziness, coldness of hands, palpitations, headache and upset stomach); (2) three DSM-IV (American Psychiatric Association, 1994) nicotine with- drawal symptoms (anxiety, irritability, restlessness) pro- vided a dysphoria score; (3) hunger, which is recognised nicotine withdrawal symptom; (4) pain in the arm, which may be caused by the injections; and (5) craving for a cigarette.
2.5 Ph ~~siologicui meusures
Heart rate (HR), finger pulse volume (FPV), and skin conductance (SC) were recorded on-line using Psylab software (Contact Precision Instruments, London). For each measure the last 3 min of the pre-injection rest period provided the baseline. Responses occurring dur- ing the first 3 min after the injections were not recorded as it was expected that these would be largely influ- enced by the injection procedures rather than the drug, but responses were recorded continuously while the subject sat still during min 4- 15 post-injection.
The cardiovascular measures (HR and FPV) were recorded from a finger plethysmograph attached to the first finger of the non-dominant hand. HR was derived from the interval (ms) between the peaks on the finger pulse trace. and FPV was derived from the amplitude of the finger pulse trace (arbitrary units). Skin conduc- tance was recorded from silver-silver chloride electrodes attached to the middle phalanges of the second and third fingers of the non-dominant hand, with KY Jelly (Johnson and Johnson) as the electrolyte. The mean skin conductance level (SCL) and number of skin con- ductance fluctuations per minute (SCFs) were recorded.
2.6. Stutisticul unai!.si.s
The response to each condition was measured by pre- to post-injection changes. As no apriori assumptions could be made about the form of response across saline, 0.3 and 0.6 mg nicotine (particularly for never- smokers), the effect of each nicotine dose was assessed separately by comparison with saline. Smokers and never-smokers were analysed separately prior to a com- parison between them. No attempt was made to adjust for drug-sequence effects given the adequacy of the wash-out period and the inadequacy of adjustment procedures (Freeman. 1989; Senn, 1992). Nicotine ver- sus saline comparisons were by t-test, based on within- sub.ject variance, adjusting for time-period effects. Analysis of covariance was used to compare the nicotine effect between smokers and never-smokers. Nicotine minus saline differences were computed for
each subject and modelled by smoker status and demo- graphic characteristics. No attempt was made to assess the overall probability of one or more type 1 errors among the many tests conducted and some caution is therefore required when interpreting results which do not follow a general pattern.
3. Results
3.1. Ejfect of’ tobucco ubstinence
Pre-injection mood and physiological responses were compared between smokers and never-smokers, after controlling for background demographics (age, gender, weight, height, years of education). At visit 1, when the smokers were smoking normally, there was no evidence of a difference between the groups on Contentedness, Calmness, 24 h withdrawal score or dysphoria (all P > 0.2), although there was some suggestion that the smokers felt less alert than the never-smokers (P = 0.057). Nor was there any evidence of a difference in heart rate at Visit 1 (mean difference = 0.2 bpm, P = 0.94) or in any of the other physiological measures.
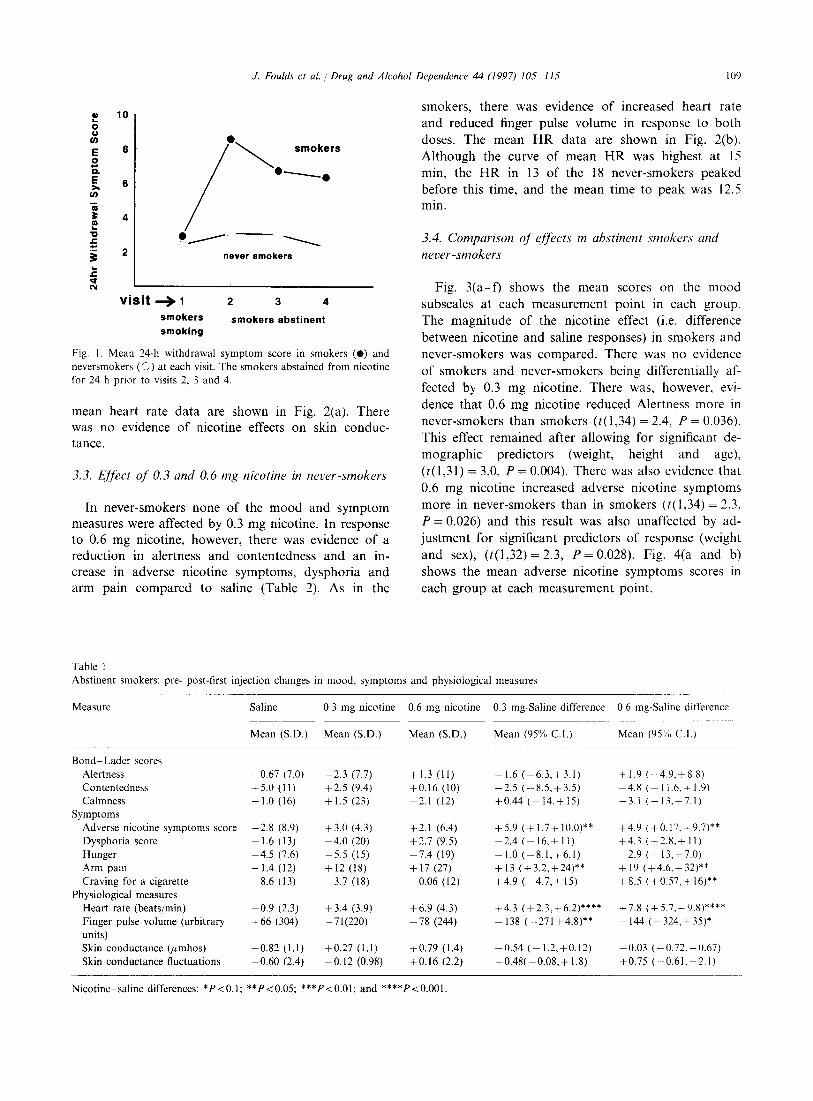
The groups were also compared on the difference between the score for visit 1 and the mean of the scores for visits 2-4 (when the smokers had been abstinent for 24 h). There was good evidence of mood deterioration on visits 2-4 compared with visit 1 in smokers relative to never-smokers on contentedness (P = O.Ol), calmness (P= 0.046), 24 h withdrawal score (PC 0.001) and dysphoria score (P = 0.048) but no evidence of deterio- ration on alertness (P = 0.31). There was also evidence of a drop in heart rate in the smokers relative to the never-smokers (mean difference in reduction 6.0 bpm, 95% CI 1.5-10.5, P = 0.011). The smokers, who had been similar in mood state and heart rate to the never- smokers when smoking normally, therefore started the experimental sessions from a lower baseline than the never-smokers. The typical pattern of pre-injection mood ratings is illustrated by the 24 h tobacco with- drawal symptom questionnaire, shown in Fig. 1.
3.2. Ejfect of 0.3 and 0.6 mg nicotine in abstinent-smokers
The change scores in smokers from pre- to post-first injection on each of the measures are shown in Table 1. There was no evidence of an effect of either nicotine dose on any of the mood scores. Both doses produced significant increases in adverse nicotine symptoms and arm pain. Craving for a cigarette was significantly higher on 0.6 mg nicotine than saline, although under both conditions the absolute responses were lower post- injection. Heart rate increased and FPV decreased in response to both nicotine doses compared to saline. The
J. Fould~ et ul. i Drug and Alcohol Dependence 44 (1997) 105-l 15 109
visit + i 2 3 4
smokers smokers abstinent smoking
Mean 24-h withdrawal symptom score in smokers (0) and neversmokers (0) at each visit. The smokers abstained from nicotine for 24 h prior to visits 2, 3 and 4.
mean heart rate data are shown in Fig. 2(a). There was no evidence of nicotine effects on skin conduc- tance.
3.3. Ej’kct of 0.3 and 0.6 mg nicotine in never-smokers
In never-smokers none of the mood and symptom measures were affected by 0.3 mg nicotine. In response to 0.6 mg nicotine, however, there was evidence of a reduction in alertness and contentedness and an in- crease in adverse nicotine symptoms, dysphoria and arm pain compared to saline (Table 2). As in the
smokers, there was evidence of increased heart rate and reduced finger pulse volume in response to both doses. The mean HR data are shown in Fig. 2(b). Although the curve of mean HR was highest at 15 min, the HR in 13 of the 18 never-smokers peaked before this time, and the mean time to peak was 12.5 min.
3.4. Comparison oj’ejj&ts in abstinent smokers and never -smokers
Fig. 3(a--f) shows the mean subscales at each measurement The magnitude of the nicotine
scores on the mood point in each group. effect (i.e. difference
between nicotine and saline responses) in smokers and never-smokers was compared. There was no evidence of smokers and never-smokers being differentially af- fected by 0.3 mg nicotine. There was, however, evi- dence that 0.6 mg nicotine reduced Alertness more in never-smokers than smokers (t(1,34) = 2.4, P = 0.036). This effect remained after allowing for significant de- mographic predictors (weight, height and age), (t(1,31) = 3.0, P = 0.004). There was also evidence that 0.6 mg nicotine increased adverse nicotine symptoms more in never-smokers than in smokers (t(1,34) = 2.3, P = 0.026) and this result was also unaffected by ad- justment for significant predictors of response (weight and sex), (t(1,32) = 2.3, P = 0.028). Fig. 4(a and b) shows the mean adverse nicotine symptoms scores in each group at each measurement point.
Table 1 Abstinent smokers: pre- post-first injection changes in mood, symptoms and physiological measures
Measure Saline 0.3 mg nicotine 0.6 mg nicotine 0.3 mg-Saline difference 0.6 mg-Saline difference
Mean (S.D.) Mean (CD.) Mean (SD.) Mean (95% C.I.) Mean (95’K C.I.)
BonddLader scores Alertness Contentedness Calmnesb
Symptoms Adverse nicotine symptoms score Dysphoria score Hunger Arm pain Craving for a cigarette
Physiological measures Heart rate (beatsjmin) Finger pulse volume (arbitrary units) Skin conductance bmhos) Skin conductance fluctuations
-0.67 (7.0) +5.0 (11) f1.0 (16)
-2.8 (8.9) -1.6 (13) -4.5 (7.6) -1.4 (12) -8.6 (13)
-0.9 (2.3) +66 (304)
+0.82 (1.1) -0.60 (2.4)
-2.3 (7.7) +2.5 (9.4) + 1.5 (23)
+3.0 (4.3) -4.0 (20) -5.5 (15) + I2 (18) -3.7 (18)
f3.4 (3.9) -71(220)
+0.27 (1.1) -0.12 (0.98)
+1.3 (II) +0.16 (IO) -2.1 (12)
+2.1 (6.4) +2.7 (9.5) -7.4 (19) + I7 (27) -0.06 (12)
+6.9 (4.3) -78 (244)
+0.79 (1.4) +0.16 (2.2)
-1.6 (-6.3,+3.1) -2.5 (-8.5,+3.5) +0.44 (-14.+15)
f5.9 (+1.7+10.0)** +4.9 (+0.17.+9.7)** -2.4 (-16,+11) f4.3 (-2.8,+11) -1.0 (-8.1,f6.1) -2.9 (-13,+7.0) +I3 (+3.2,+24)** + 19 (+4.6,+32)** f4.9 (-4.7,+ 15) +X.5 (+0.57.+ l6)**
+4.3 (+2.3,+6.2)**** -138 (-271+4.8)**
+7.8 (+5.7,+9x)**** -144 (-324,+35)*
-0.54 (-1.2,+0.12) +0.48( -0.08,+ 1.8)
+1.9 (-4.9,+8.8) -4.8 (-11.6,+1.9) -3.1 (-13.t7.1)
-0.03 (-0.72,+0.67) +0.75 (-0.61,+2.1)
Nicotine--saline differences: *P<O.l; **P<O.O5; ***P<O.Ol; and ****P<O.OOl.

(a) Smokers (b) Never Smokers
-3 0 3 6 9 12 15
t Time (minutes)
Injection
75
70
65
60
55 -3 0 3 6 9 12 15
t Time (minutes)
Injection
Fig. 1. Mean heart rate in (a) smokers and (b) never-smokers, before and after injections of placebo ( : Z), 0.3 mg (A) and 0.6 mg ( n ) nicotine.
Between the post-first injection measures and the post-second injection measures, subjects undertook a number of performance tests. As shown by the change in scores in both groups whilst receiving saline during this period (Fig. 3). the effect of the tests was to increase alertness (t( 1,315) = 4.57, P < 0.001) and to reduce both contentedness (t( 1,35) = 2.02, P = 0.026) and calmness (t( 1,35) = 2.97, P = 0.005) in comparison with the change over the period of the first injection, when no performance tests were undertaken. There were no differences between smokers and never-smok- ers when comparing these periods.
The combined effect of the two nicotine injections, giving 0.6 and 1.2 mg nicotine in total, was measured by the change in mood and symptom scores from pre-first injection baseline to post-second injection com- pared to saline. These comparisons also examine the effect of nicotine when subjects were under stress due to the performance tests. As shown in Fig. 3(aaf) and Fig. 4(a and b) the pattern of nicotine-saline differences over the whole period was similar to that observed over the period of the first injection. The only exceptions to the pattern of results shown in Tables 1 and 2 was a lack of effect on adverse nicotine symptoms and craving in smokers.
Two male never-smokers had to discontinue testing
for a brief period after the second 0.6 mg injection due to excessive dizziness and nausea (one vomited). None of the smokers had such a severe reaction.
4. Discussion
This study replicated the well established finding that when smokers abstain from smoking they experience a withdrawal syndrome characterised by a general wors- ening of mood (American Psychiatric Association, 1994). Whilst smoking, the mood of smokers was simi- lar to that of the never-smokers, both before and after adjustment for demographic characteristics. Although it is possible that the lack of an initial difference in mood was attributable to additional, uncontrolled inherent differences between the groups. the deficit observed in the smokers after a day without cigarettes cannot easily be explained by anything other than tobacco absti- nence. Hence, at the beginning of each test session, when the smokers had been abstinent for 24 h, the mood of the smokers was substantially worse than that of the never-smokers. This study also found that nicotine injections had no effect in reversing this mood deficit in smokers and that 0.6 mg nicotine produced a worsening of mood in never-smokers. Both smokers and never-smokers experienced a similar, dose related. increase in heart rate on receiving nicotine. Both groups also experienced symptoms associated with nicotine toxicity and these were significantly greater in never- smokers than smokers after 0.6 mg nicotine.

111
80 80
70
f E = 80 .?! a
60
50
40
(a)
Smokers
Pcmt- Post-
Never Smokers
WI
40 REST TESTS
I PW- Post- Port-
Inlectlon 1 lnlcctlon 1 Inlecllon : lnfectlon 1 InJ.ctlon 1 ln~ectlon 2
(b)
801
50
40 REST TESTS REST TESTS I I
I , Pt*- post- PO& PW- POW Pod-
InjectIon 1 lnjsction 1 Inpctlon 2 ln~ectlon 1 ln,.etlon 1 InJBctlon 2
80 80
70
60
40 REST TESTS
PW- Pest- POSb
50
40
80
70
60
W
(4 (f)
REST TESTS
PW- Paat- PC..,- ln].ctlon 1 Inl9alon 1 In,.euon 2
Inl.ctlon 1 lnlactlon 1 Inj~ctlon 2
Measurement Point Measurement Point
Fig. 3. (a f) Mean mood ratings (Bond-Lader mood scores) in smokers (a-c) and never-smokers (d -f) before and after an injection (placebo (:I), 0.3 mg (A) or 0.6 mg (m) nicotine) and then again after another similar injection and completion of performance tests.
The worsened mood in response to 0.6 mg injections effect, if it does exist, occurs only after adaptation has in never-smokers was probably related to the symptoms taken place. These results are consistent with those of of nicotine toxicity experienced at that dose. However, Perkins et al. (1993, 1994a) who found that nicotine the fact that they did not experience any mood en- administered to non-smokers via a nasal spray pro- hancement at the lower dose (which did not cause duced dose-dependant increases in ratings of feeling nicotine toxicity) implies that any mood enhancing ‘jittery’, ‘confusion’ and ‘fatigue’. Newhouse et al.

3. Foulds et al. ))) Drug and Alcohol Dependence 44 (1997) 105-l 15
(a) Smokers (b) Never Smokers
I I I
Pie- Post- Post- inJec;lon 1 InJection 1 injectlon 2
Measurement Point
20
15
10
5
0
/
\
& 5 e-t I I I
Pre- Post- Post- InJection 1 injection 1 injection 2
Measurement Point
Fig. 4. Mean ratings of adverse nicotine symptoms in (a) smokers and (b) never-smokers, before and after an injection (placebo (0 ), 0.3 mg (A) or 0.6 mg (m) nicotine) and then again after another similar injection and completion of performance tests.
(1990) found that intravenous nicotine increased anxi- ety over placebo in non-smoking Alzheimer patients and that a moderate dose increased ratings of tension, depression and confusion over a lower dose (no placebo given) in healthy non-smoking volunteers.
In smokers, our failure to demonstrate even a partial reversal of the withdrawal-induced mood deficit was surprising and has several possible explanations. Given that the mood of our abstinent smokers would pre- sumably have improved to its original level had they been allowed to smoke freely, it is possible that the mood deterioration observed on abstinence was not caused by a loss of nicotine and hence could not be expected to have been reversed by nicotine administra- tion. Although appealing in its simplicity, this explana- tion runs counter to evidence from numerous placebo-controlled smoking cessation studies demon- strating the effectiveness of non-tobacco nicotine deliv- ery systems (gum, patch, spray) in relieving dysphoric smoking withdrawal symptoms (e.g. Stapleton et al., 1995). These studies clearly implicate nicotine depriva- tion as being at least partly responsible for the tobacco withdrawal syndrome.
Another possible explanation is that there are mood- enhancing effects of nicotine when given in this way, at these doses. but that they are too small to be detected in a study of this size. If this were the case, the evidence from our results suggests that the effects are so small as to be of little consequence. On the four main measures of mood (alertness. contentedness, calmness, dysphoria) there were an equal number of non-significant positive and negative effects, indicating no overall tendency
towards enhancement. Additionally, this study was of sufficient size and the measures of sufficient sensitivity to detect clear negative effects in never-smokers in response to nicotine and to detect effects in response to the stressful performance tasks in both groups. The methodology was also able to detect enhancements in cognitive performance (Foulds et al., 1996).
More arm pain was experienced after the nicotine injections than after saline and it is possible that this masked any deficit-reversal effect of nicotine on mood in smokers. To investigate this we re-analyzed the dose- mood relationships after partialling out the effect of arm pain, ie by attributing as much of each dose-mood relationship as the data suggest to changes in arm pain, we adjusted them to the levels they would have been had there been no increase in arm pain. Although there was a significant change in arm pain between saline and both nicotine doses, this was only related to a corre- sponding change in mood in the case of Calmness after 0.3 mg nicotine (V = - 0.54, P < 0.02). The result of adjustment was to increase the estimate of change in Calmness to + 10.6, but this remained non-significant. In all other mood-dose comparisons the association between arm pain and mood was small and adjustment consequently negligible. As there was also evidence of an increase in arm pain in the never-smokers at the 0.6 mg dose compared with saline, we adopted the same procedure in re-analyzing their mood responses. Alert- ness was the only mood score in which the effect of 0. 6 mg nicotine correlated with arm pain (Y = + 0.56) ie if arm pain was affecting alertness it was having the effect of increasing alertness. Adjustment therefore had

Table 2 Never-smokers: pre- post-first injection changes in mood. symptoms and physiological measures
Measure Saline 0.3 mg nicotine 0.6 mg nicotine 0.3 mg saline difference 0.6 mg saline difference
Mean (S.D.) Mean (S.D.) Mean (SD.) Mean (95% C.I.) Mean (95% C.1.)
Bond- Lader scores Alertness Contentedness Calmness
Symptoms Adverse nicotine symptoms score Dysphoria score Hunger Arm pain Craving for a cigarette
Physiological measures Heart rate (beatsimin) Finger pulse volume (arbitrary units) Skin conductance (pmhos) Skin conductance fluctuations
-0.60 (II) -0.88 (12) + 1.2 (4.6) -0.08 (6.4) -0.71 (I I) +I.6 (13)
- 0.30 (4.6) -0.98 (3.1) + 1.7 (8.4) +2.7 (6.8) -0.33 (1.5)
-2.4 (3.4) +22 (192)
+0.80 (2.0) +0.72 (1.4)
+0.92 (3.4) -0.67 (4.6) -0.71(5.5) +5.7 (9.0) - 1.3 (3.4)
+ 0.41 (2.6) - 136 (165)
+ 1.2 (1.2) io.02 (1.3)
-9.4 (12) -7.2 (14) -1 I (20)
+14 (II) +10.3 (17) +3.9 (15) + 18 (20) +0.27 (1.8)
f4.9 (5.2) -108 (256)
f1.8 (1.6) f0.74 (1.7)
-0.28 (-6X).+5.4) -1.3 (G5.0,+2.4) +2.3 (-5.6,+ IO)
f1.2 (-1.4,+X8) -0.31 (-1.7,+2.4) -2.5 C-7.7.+2.8) f3.0 (-3.6,+9.6) -1.0 (-3.4.+1.4)
+2.8 (+1.0.+4.6)*** - 158 (-280, -36)**
+0.43 (-0.45,+ I .3) -0.70 ( - I .8. + 0.35)
Nicotine- saline differences: *P<O.l; **P<O.O5: ***P<O.Ol: and ****P<O.OOl.
-8.8 (- 17. - l.o)** -8.4 (-16. -1.3)** -10 (-21,+1.1)*
+ 14 (+7.2,+21)*** + I I (+2.1,+20)** +2.2 (-5.1.+9.5) +15 (+4.5,+26,*** f0.60 (-0.42.+ 1.6)
+7.3 (+4.1.+10)**** -130 (-252, -7.7)**
+I.0 (-0.28,+2.2) +0.02 (-1.3,+1.3)
the effect of increasing the estimated negative effect of 0.6 mg nicotine on Alertness (from - 8.8 to - 15).
More plausible explanations for the lack of acute effect in smokers centre around the size of the doses and the manner and setting in which they were adminis- tered. It could be that only inhaled nicotine, delivering more concentrated arterial boli of nicotine to the brain (Henningfield et al., 1993) self-administered in a natu- ral setting, produces positive effects on mood. We gave a quantity of nicotine equivalent only to that inhaled from a single cigarette, and this was divided into two doses administered 40 min apart. This may have been insufficient in quantity and speed of delivery to initiate reversal of the withdrawal deficit.
However, this would run counter to the other results of this study which showed clear effects on adverse nicotine symptoms, heart rate and finger pulse volume. Another explanation for our lack of effect is that the experimental setting, which prevented self-administra- tion and removed natural stimuli, somehow stifled the normal response. If this was the case then any mood- enhancing effects of nicotine are subtle and situation- specific.
Given that this study found no evidence of acute mood enhancement due to subcutaneous nicotine, even in withdrawn smokers, what is the evidence that smok- ers obtain mood enhancement when smoking? While some laboratory studies have reported mood-enhancing effects of smoking cigarettes, the effects have frequently been very transient, situation-specific, and limited to
one of the many mood measures taken. Perkins et al. (1992b) found that smoking reduced subjective stress compared with sham-smoking during a high- but not low- challenge task. However the effect occurred only immediately after smoking and dissipated shortly after- wards. Meliska and Gilbert (1991) found that smoking two nicotine cigarettes reduced drowsiness in overnight- deprived smokers, compared with smoking nicotine free cigarettes. However, there were no additional effects of smoking another three cigarettes and there were no nicotine effects on a range of other mood items mea- sured (including tension, happiness, worry, energy, alertness, relaxation, and sadness). Pomerleau and Pomerleau (1992) found that smokers reported more ‘euphoriant’ effects while smoking nicotine versus ultra low nicotine cigarettes, but acknowledged that these effects (described as a pleasurable ‘high, buzz, and rush’) may not have been clearly distinguished from dizziness and were experienced for only 10% of the smoking time. In a subsequent paper in which smokers reported their sensations using foot pedals while smok- ing a cigarette, Pomerleau and Pomerleau (1994) re- ported that clear euphoric effects are reported by the majority of subjects while smoking. These effects were very transient, consisting of an average of 3.6 episodes per cigarette, lasting a total of 127 s. This suggests the possibility that some positive mood sensations may be missed in studies like the present one which administer mood questionnaires at fixed time points and do not enquire about transient effects.

A number of other laboratory studies have failed to find any positive effects of smoking nicotine cigarettes on mood, e.g. Pomerleau and Pomerleau (1990) found that a psychological stressor (mental arithmetic) did not increase subsequent nicotine intake, and that smoking a nicotine cigarette did not reduce the induced anxiety compared with sham smoking. Gilbert et al. (1992) found that smoking a high nicotine cigarette produced more unpleasant feelings than a nicotine-free cigarette, and failed to find any increase in pleasant feelings following either the smokers’ usual brand or a high nicotine cigarette. A recent study by Perkins et al. (1994b) comparing the effects of cigarettes and nasal nicotine spray reported a virtually identical pattern of effects. with both producing effects like increased dizzi- ness. but neither producing improved mood (e.g., relax- ation). The failure to find mood enhancement following nicotine in the present study is therefore consistent with numerous other laboratory studies, and contrasts with smokers’ self-rated motives for smoking (Russell et al., 1974) and Foulds et al., 1996 results from uncontrolled studies of smokers smoking cigarettes ad-libitum in their own environment (e.g. Parrott, 1995).
Another finding from the present study was that smokers are less sensitive to 0.6 mg nicotine than never-smokers on some measures (alertness, adverse nicotine symptoms). These effects remained after ad- justing for other factors (e.g. weight) and provide evi- dencc of chronic tolerance to the unpleasant effects of nicotine in smokers. This is consistent with previous results based on comparisons with smokers who had abstained for a shorter time period (and so may have had some residual acute tolerance). Interestingly, how- ever. there was no evidence of chronic tolerance to nicotine’s effects on heart rate or finger pulse volume. These results are consistent with those of Perkins et al. ( 1994a). who found generally smaller subjective effects at a given plasma nicotine level in smokers (overnight deprived) compared with non-smokers, but no differ- ence in cardiovascular reactivity. The between-group differences in heart rate were more in the direction of increased sensitivity to nicotine in abstinent smokers than never-smokers; a possibility suggested by Pomer- leau (1995).
The relative increase in craving following the first 0.6 mg injection in smokers could be interpreted as a ‘priming’ effect. An increase in desire for a drug follow- ing administration of a small dose has been found in some human studies (e.g. de Wit and Chutuape, 1993). However. the absence of any consistent pattern of craving cffccts (e.g. on the 0.3 mg dose or after the second injections) suggests that this may have been a chance result.
The results of this study confirm that abstinence from tobacco worsens mood in smokers, and indicates that when a moderate acute dose of nicotine is administered
subcutaneously under double-blind conditions it pro- duces no improvements in mood in abstinent smokers and worsens mood in never-smokers. Acute mood en- hancements from nicotine have been hard to detect in laboratory studies, particularly in controlled studies using tobacco-free delivery systems. They might occur only through self-administration by smoking in re- sponse to situation-specific mood fluctuations.
Acknowledgements
The authors gratefully acknowledge the help of Mary Hayward, who administered the injections, Dr Alyson Bond for advice on the mood measures and Dr Robert West (St. George’s Hospital Medical School) for help- ful advice. The study was supported by the Medical Research Council and the Imperial Cancer Research Fund.
References
American Psychiatric Association (1994) Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). American Psychiatric Association. Washington, DC.
Ashton. H.. Marsh, V.R., Millman, J.E.. Rawlins, M.D.. Telford, R. and Thompson, J.W. (1980) Bi-phasic dose-related response of the CNV to IC nicotine in man. Br. J. Clin. Pharmacol. 10, 579-589.
Benowitz. N.L.. Kuyt, F. and Jacob, P. (1982) Circadian blood nicotine concentrations during cigarette smoking. Clin. Pharma- col. Ther. 32. 758-764.
Benowitz, N.L. (1988) Pharmacologic aspects of cigarette smoking and nicotine addiction. New. Eng. J. Med. 319, 1318 -1330.
Bond. A. and Lader, M. (1974) The use of analogue scales in rating subjective feelings. Br. J. Med. Psychol. 47, 21 I-218.
Church. R.E. (1989) Smoking and Human EEG. In: Smoking and Human Behaviour (Ney, T. and Gale, A., eds), pp. 239-256. Wiley. London.
Crycr, P.E., Haymond, M.W., Santiago, J.C. and Shah, SD. (1976) Norepinephrine and epinephrine relase and adrenergic mediation of smoking-associated hemodynamic and metabolic events. New. Eng. J. Med. 9. 573-577.
Foulds. J.. McSorley. K., Sneddon, J.. Feyerabend, C., Jarvis. M.J. and Russell, M.A.H. (1994) Effect of subcutaneous nicotine injec- tions on EEG J frequency in non-smokers: A placebo-controlled pilot study. Psychopharmacology 1 I5 (i-2). 163-166.
Foulds. J.. Stapleton, J., Swettenham. J.. Bell, N., McSorley, K. and Russel, M.A.H. (1996) Cognitive performance effects of subcuta- neous nicotine in smokers and never-smokers. Psychopharmacol- ogy 127, 31 38.
Freeman. P.R. (1989) The performance of the two-stage analysis of two-treatment, two-period crossover trials. Stats. Med. 8, 1421- 1432.
de Wit, H. and Chutuape, M.A. (1993) Increased ethanol choice in social drinkers following ethanol preload. Behav. Pharmacol. 4. 29 36.
Gilbert. D.G., Meliska, C.J., Williams. C.L. and Jensen, R.A. ( 1992) Subjective correlates of cigarette-smoking-induced elevation of peripheral beta-endorphin and cortisol. Psychopharmacology 106, 275 281.

J. Foulds et al. : Drug and Alcohol Dependence 44 (1997) 105. 115 115
Golding. J. and Mangan, G.L. (1982) Arousing and de-arousing effects of cigarette smoking under conditions of stress and mild sensory isolation. Psychophysiology 19, 449-456.
Heishman, S.J., Snyder, F.R. and Henningfield, J.E. (1993) Perfor- mance, subjective. and physiological-effects of nicotine in non- smokers. Drug. Alcohol. Depend. 34 (1) 1 I 18.
Henningfield, J.E., Stapleton, J.M., Benowitz, N.L., Gratson, R.F. and London, E.D. (I 993) Higher levels of nicotine in arterial than in venous blood after cigarette smoking. Drug. Alcohol. Depend. 33 (1). 23m 29.
Hughes, J.R. (1991) Distinguishing withdrawal relief and direct ef- fects of smoking. Psychopharmacology 104, 4099410.
McNeill. A.D., Jarvis, M. and West, R. (1987) Subjective effects of cigarette smoking in adolescents. Psychopharmacology 92, I 15- 117.
Meliska, C.J. and Gilbert. D.G. (1991) Hormonal and subjective effects of smoking the first five cigarettes of the day: a comparison in males and females. Pharmacol. Biochem. Behav. 40, 229-235.
Nesbitt, P.D. (1973) Smoking, physiological arousal and emotional response. J. Pers. Sot. Psychol. 25, 1377144.
Newhouse, P.A., Sunderland, T., Narang, P.K., Mellow, A.M., Fer- tig, J.B.. Lawlor, B.A. and Murphy, D.L. (1990) Neuroendocrine, physiologic, and behavioral responses following intravenous nicotine in nonsmoking healthy volunteers and in patients with Alzheimer’s disease. Psychoneuroendocrinology 15 (5 -6), 471~ 484.
Parrott. A.C. (1995) Stress modulation over the day in cigarette smokers. Addiction 90, 233-244.
Perkins, K.A., Grobe, J.E., Epstein, L.H., Caggiula, A.R. and Stiller, R.L. (1992a) Effects of nicotine on subjective arousal may be dependent on baseline subjective state. J. Subst. Abuse. 4, 131- 141.
Perkins, K.A., Grobe, J.E., Fonte, C. and Breus, M. (1992) ‘Paradox- ical’ effect of smoking on subjective stress versus cardiovascular arousal in males and females. Pharmacol. Biochem. Behav. 42 (2). 301-311.
Perkins, K.A., Grobe, J.E., Epstein, L.H., Caggiula, A., Stiller, R.L. and Jacob, R.G. (1993) Chronic and acute tolerance to subjective effects of nicotine. Pharmacol. Biochem. Behav. 45 (2), 375-381.
Perkins, K.A., Grobe, J.E., Fonte, C., Goettler, J., Caggiula, A.R., Reynolds, W.A., Stiller, R.L., Scierka, A. and Jacob, R.G. (1994) Chronic and acute tolerance to subjective, behavioral and cardio- vascular effects of nicotine in humans. J. Pharmacol. Exp. Ther. 270 (2). 628.-638.
Perkins, K.A., Sexton. J.E., Reynolds, W.A., Grobe, J.E., Fonte, C. and Stiller, R.L. (1994) Comparison of acute subjective and heart rate effects of nicotine intake via tobacco smoking versus nasal spray. Pharmacol. Biochem. Behav. 47 (2) 2955299.
Pomerleau, O.F. (1995) Individual differences in sensitivity to nicotine: Implications for genetic research on nicotine depen- dence. Behav. Genet. 25, 161-177.
Pomerleau, O.F., Hariharan, M., Pomerleau, C.S., Oliver, G. and Gutherie, S.K. (1993) Differences between smokers and never- smokers in sensitivity to nicotine: A preliminary report. Addiction 88 (l), 1133118.
Pomerleau, C.S. and Pomerleau, O.F. (1992) Euphoriant effects of nicotine in smokers, Psychopharmacology 108, 460-465.
Pomerleau, O.F. and Pomerleau, C.S. (1990) Cortisol response to a psychological stressor and/or nicotine. Pharmacol. Biochem. Be- hav. 36, 211-213.
Pomerleau, O.F. and Pomerleau, C.S. (1994) Euphoriant effects of nicotine. Tobacco Control 3, 374.
Porchet, H.C., Benowitz, N.L. and Sheiner, L.B. (1988) Phatmacody- namic model of tolerance: Application to nicotine. 3. Pharmdcol. Exp. Ther. 244 (l), 231-236.
Russell, M.A.H., Jarvis, M.J., Jones, G. and Feyerabend, C. (1990) Non-smokers show acute tolerance to subcutaneous nicotine. Psychopharmacology 102 (I), 56658.
Russell, M.A.H., Peto, J. and Pate], U.A. (1974) The classification of smoking by factorial structure of motives. J. R. Stat. Sot. 137. 313-333.
Senn, S.J. (1992) Is the ‘simple carry-over’ model useful? Stat. Med. 11, 7155726.
Srivastava, E.D., Russell, M.A.H., Feyerabend, C., Masterson, J.G. and Rhodes, J. (1991) Sensitivity and tolerance to nicotine in smokers and non-smokers. Psychopharmacology 105 (1). 63 68.
Stapleton, J.A., Russell, M.A.H., Feyerabend, C., Wiseman, SM., Gustavsson, G. and SPwe, U. (1995) Dose effects and predictors of outcome in a randomized trial of transdermal nicotine patches in general practice. Addiction 90 (l), 31-42.
US Surgeon General (1988) The Health Consequences of Smoking: Nicotine Addiction, US Government Printing Office, Washington, DC.
West, R.J. and Russell, M.A.H. (1988) Loss of acute tolerance and severity of cigarette withdrawal. Psychopharmacology 94, 5633 565.