Epithelial StructureRevealed by Chemical Dissection and Unembedded ElectronMicroscopy
Upload
khangminh22Category
view
0download
0
Am J Clin Pathol 2007;128:1023-1034 10231023 DOI: 10.1309/YU37DVCUFUHP8VPY 1023
© American Society for Clinical Pathology
Anatomic Pathology / MONOMORPHIC EPITHELIAL PROLIFERATIONS
Monomorphic Epithelial Proliferations
Characterization and Evidence Suggesting They Are the Pool of Partially Transformed Lesions From Which Some InvasiveCarcinomas Arise
Neal S. Goldstein, MD,1 Larry J. Kestin, MD,2 and Frank A. Vicini, MD2
Key Words: Breast; Molecular diagnostics; Precursors; Ductal carcinoma in situ; Hyperplasia; Monomorphic epithelial proliferations;Neoplastic cell transformation
DOI: 10.1309/YU37DVCUFUHP8VPY
A b s t r a c t
We studied whether precursor lesions(monomorphic epithelial proliferations [MEPs])contributed to ipsilateral breast failures (IBFs; localrecurrences). Margin status and MEPs near (within 4.2mm) of the initial excision margin in 70 carcinomapatients with IBFs and allelic imbalance clonality datawere recorded. Of the IBFs, 46 (66%) were clonal and24 (34%) were second primary carcinomas. Controlcases were 2 matching non-IBF cases for each studycase. MEP lesions were predominantly single-celllayered, slightly overcrowded, monomorphic, clonal-like luminal cell proliferations that unfolded terminalduct lobular units (TDLUs) in an overgrowth extensionpattern. MEPs often extended into TDLUs involved byhyperplasia of usual type. Clonal IBF cases had a meanof 6.24 MEPs near the initial excision margincompared with 3.85 MEPs in matched non-IBF controlsamples (P < .001). In the negative-margin subset,clonal IBF cases had mean of 7.82 MEPs near themargin, which was significantly greater than 4.26 in thedistinct IBF group (P = .012) and 2.85 in the non-IBFmatched control group (P < .001). MEPs seem to be thepool of partially transformed precursor lesions for mostinvasive carcinomas. Radiation therapy may reduce theIBF rate by eradicating these precursor lesions andpreventing new carcinomas from emerging rather thaneradicating microscopic residual disease.
Radiation after breast-conserving surgery significantlyreduces local recurrences, or ipsilateral breast failures (IBFs),in patients with invasive breast carcinoma treated with breastconserving surgery.1 The reduction in IBF rate from radiationis proportionally similar across all patient groups. Despite theefforts of many, the subset of patients unlikely to benefit fromradiation therapy has not been identified.1,2 Inconsistent mar-gin assessment, inadequate resection, and carcinoma multicen-tricity are generally accepted to be the key responsible factors.3
Although plausible when first considered, this explanation hasinconsistencies if taken to its conclusion. Given the strengthand breadth of the radiation–IBF risk reduction association,invoking this explanation would mean the overwhelmingmajority of patients following breast-conserving surgery havea sufficiently large volume of residual carcinoma in the adja-cent breast parenchyma. Because “negative” margin status hasbeen the standard of practice, it raises the question of what isradiation eradicating in the unexcised parenchyma to producesuch a significant statistical reduction in IBF rate?
The allelic imbalance (AI) assay is a well-establishedmethod for determining the clonality of 2 carcinomas, includinginitial and IBF breast carcinomas. Approximately 70% of IBFsare clonally related to the initial carcinoma, and 30% are clon-ally distinct, second primary carcinomas.4,5 The factors relatedto the development of IBFs are poorly understood. Similar toradiation’s association with reduction of IBF risk, residual car-cinoma, owing to inadequate resection or incomplete eradica-tion by radiation, is generally held responsible. Althoughresidual carcinoma is clearly behind some IBFs, the majorityof patients in whom clonal IBFs develop have negative finalmargins on the initial excision specimen,6 which leads to thequestion: What results in the IBF in the latter cases?
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/128/6/1023/1765209 by guest on 29 M
arch 2022

1024 Am J Clin Pathol 2007;128:1023-10341024 DOI: 10.1309/YU37DVCUFUHP8VPY
© American Society for Clinical Pathology
Goldstein et al / MONOMORPHIC EPITHELIAL PROLIFERATIONS
These 2 questions focused our investigation toward pos-sible alternative factors, specifically, whether a precursorlesion less than atypical ductal hyperplasia (ADH) or ductalcarcinoma in situ (DCIS) was a contributing factor in IBFs insome cases.
Most invasive breast carcinomas are high-grade molecu-lar group neoplasms.7 Hyperplasia of the usual type (HUT)was previously thought to be the precursor lesion for thesecarcinomas. It is currently considered a marker of increasedcarcinoma risk.8 A precursor lesion less than ADH has notbeen identified for these neoplasms. This is not the case forinvasive tubular carcinomas. The precursor, termed columnarcell lesion (CCL), has a variety of cytologic and architecturalalterations, each of which is associated with distinct and pro-gressively greater molecular alterations. Studies have elegant-ly shown they form a biologic continuum that merges intoADH/low-grade DCIS.9-12
The key features that draw CCLs together into a singleentity are monomorphism, slight hypercellularity, and anovergrowth replacement growth pattern, in our opinion. WithCCLs as the prototype, we wondered if there were similar pre-cursor lesions with these 3 key morphologic features for mostinvasive carcinomas. We termed these lesions, regardless ofthe cytologic features, monomorphic epithelial proliferations(MEPs) to divest ourselves of any presumed risk associationsand sidestep the terminology morass associated with CCLs,flat epithelial atypia, and flat and clinging DCIS.
The goals of this study were to characterize MEPs fromthe perspective of the potential precursor lesion to most inva-sive carcinomas and evaluate whether there was a relationshipbetween MEPs and initial or IBF carcinomas. To facilitate ourstudy of MEPs, we used the rim of tissue near the margin ofinitial excision specimens in patients in whom IBF developed,concentrating on the subset of patients with negative margins.
Materials and Methods
The study was reviewed and approved by the WilliamBeaumont Human Investigations Subject Committee asHICE2004103 (William Beaumont Hospital, Royal Oak, MI).Study IBF cases consisted of 70 patients with invasive breastcarcinoma treated with breast-conserving surgery and radia-tion therapy at William Beaumont Hospital from January 1982through December 2006 in whom IBF developed and forwhom adequate carcinoma in paraffin blocks was available fora clonality assay. Two matched control, non-IBF cases wereselected from the William Beaumont Hospital RadiationOncology database for each study IBF case. The 2 non-IBFcases were matched against the study IBF case for the identi-cal type and grade of invasive carcinoma, identical estrogenreceptor (ER) and progesterone receptor status, identical final
margin amount on the initial excision specimen, age at initialdiagnosis that was ± 5 years, and a follow-up period that wasnot less than 2.5 years shorter than that for the study case.
The following factors were recorded for each patient:birth date, date of initial and IBF carcinoma diagnoses, mor-phologic type and grade of the initial and IBF carcino-mas,13,14 ER and progesterone receptor status, and final mar-gin status of the initial carcinoma resection specimen. Finalmargin status was classified by distance and amount of carci-noma near the final inked margin as follows: negative, allinvasive carcinoma and DCIS more than half of a low-powerfield (4.2 mm) from the final margin; near, carcinoma withinhalf of a low-power field of the margin but not at the margin;or positive, final inked margin transected by invasive carcino-ma or DCIS. Cases with near final margins were subdividedinto 3 groups based on increasing amounts of carcinoma inthe rind of tissue adjacent to the final margin as follows: near,least amount, less than a 3-mm width of invasive carcinomaand fewer than 13 DCIS ducts; near, intermediate amount, awidth of invasive carcinoma of 3 mm or more and fewer than13 DCIS ducts); and near, greatest amount, more than 13DCIS ducts.6 Statistical tests, including the t test, Fisher exacttest, χ2 test, analysis of variance, and regression analysis,were performed with Systat v11.0 program (Systat Software,Point Richmond, CA).
A detailed description, including the polymerase chainreaction (PCR) parameters of our clonality assay, was previ-ously published.4,5 Briefly, initial and IBF carcinoma slideswere used as template guides to microdissect carcinoma out ofcorresponding paraffin blocks. A normal tissue block of non-radiated tissue was used as the patient control sample.Microsatellite markers from genes known to be frequentlydeleted or amplified in breast carcinoma and a high informa-tive rate were amplified by PCR ❚Table 1❚. The mean andmedian numbers of informative microsatellite markers percase were 19.6 and 20, respectively (range, 15-26 markers).Results were analyzed by using capillary electrophoresis (ABI310, Applied Biosystems, Foster City, CA). AI was consideredpresent in a microsatellite marker if the carcinoma allelic ratiowas ±50% of the normal tissue allelic ratio. Clonality wasdetermined on the pattern of microsatellite marker AIs in ini-tial and IBF carcinomas. A likelihood ratio (LR) of clonalitywas calculated.15 A high LR indicated a high probability thatthe 2 carcinomas were clonal. A small LR indicated a highprobability that the 2 carcinomas were clonally distinct, sepa-rate primary neoplasms.
Initial Carcinoma Resection Specimens
Of the 70 study IBF initial carcinomas 55 (79%) werereexcised as were 96 (68.6%) of the 140 control non-IBF car-cinomas (P = .17). All specimens were inked, serially sec-tioned perpendicular to the longest axis, and totally embedded.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/128/6/1023/1765209 by guest on 29 M
arch 2022
Am J Clin Pathol 2007;128:1023-1034 10251025 DOI: 10.1309/YU37DVCUFUHP8VPY 1025
© American Society for Clinical Pathology
All margins were evaluated in a perpendicular relationship tothe inked surface. None of the specimens were assessed using“orange-peel” section orientation. The mean number of tissueblocks submitted per study IBF case was 38.8 compared witha mean of 37.8 blocks per non-IBF control case (P = .075).The mean maximum dimensions of study IBF and non-IBFcontrol initial excision specimens were 6.1 and 5.8 cm,respectively (P = .28). The final margin status of study IBFcases was as follows: negative, 42 cases (60%); near, leastamount, 10 (14%); near, intermediate amount, 10 (14%); near,greatest amount in 4 (6%); and positive, 4 (6%).
Results
The mean and median ages at initial diagnosis of IBFstudy cases were 56.7 and 58.3 years, respectively (range,31.8-83.7 years; SD, 12.1 years). The mean and medianintervals between initial and IBF carcinomas were 7.0 and6.1 years, respectively (range, 8.1 months–19.5 years; SD,4.8 years). Of 70 IBFs, 46 (66%) were clonal with mean andmedian LR ratios of 7.631E+06 and 7.893E+04, respective-ly (range, 1.209E+03 to 3.181E+08). Of the IBFs, 24 (34%)were clonally distinct, second primary carcinomas (distinctIBFs) with mean and median LR ratios of 3.291E–07 and1.800E–08, respectively (range, 3.617E–06 to 2.307E–14).The mean IBF interval was significantly shorter in clonalIBF cases compared with distinct IBF cases (5.2 vs 10.5years; P < .001). The mean patient age, carcinoma grade,and distribution of final margin status on the initial excisionspecimen was similar between clonal and distinct IBF cases(data not shown).
Monomorphic Epithelial Proliferations
An MEP was defined as a slightly overcrowded, predom-inantly single layer of monomorphic, luminal epithelial cellsthat involved terminal duct lobular units (TDLUs) in an over-growth extension pattern that tended to retain the architectureof the TDLU or expand the acini in an unfolded lobule-likepattern. The cells comprising MEPs varied between patientsand ranged from innocuous to slightly atypical. By definition,MEPs were not frankly malignant, which distinguished themfrom cancerization of lobules by intermediate- or high-gradeDCIS. Also, MEPs did not have stratified or multilayeredcomplex architectural structures, which distinguished themfrom epithelial hyperplasia, ADH, and low-grade intraductalcarcinoma.
Included as an MEP was any lesion that was monomor-phic, slightly hypercellular, and involved TDLUs in an over-growth extension pattern, regardless of the cytologic features.The entity of MEP included but was not restricted to lesionstermed by others as CCLs and flat epithelial atypia.
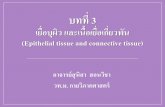
A characteristic low-magnification feature of MEPs wasthe appearance of an expanding, clonal-like proliferationreplacing preexisting luminal epithelial cells ❚Image 1A❚ and❚Image 1B❚. Architecturally, MEPs predominantly retained theTDLU outline, often with expanded acini that simulated bluntduct adenosis at low magnification. Acini of involved TDLUswere often slightly dilated, resulting in small, ectatic duct-likeprofiles clustered around a small intralobular duct (partiallycystic lobules).16-18 These TDLUs retained a circumscribed,ovoid, lobular shape that was 2 to 3 times larger than adjacent,uninvolved TDLUs. The mean number of acini in MEPsTDLUs was 7.4 compared with a mean of 8.7 in uninvolved,non-MEP TDLUs (P = .467). The mean number of adjacentTDLUs involved by an MEP lesion was 2.7 (range, 1-5).
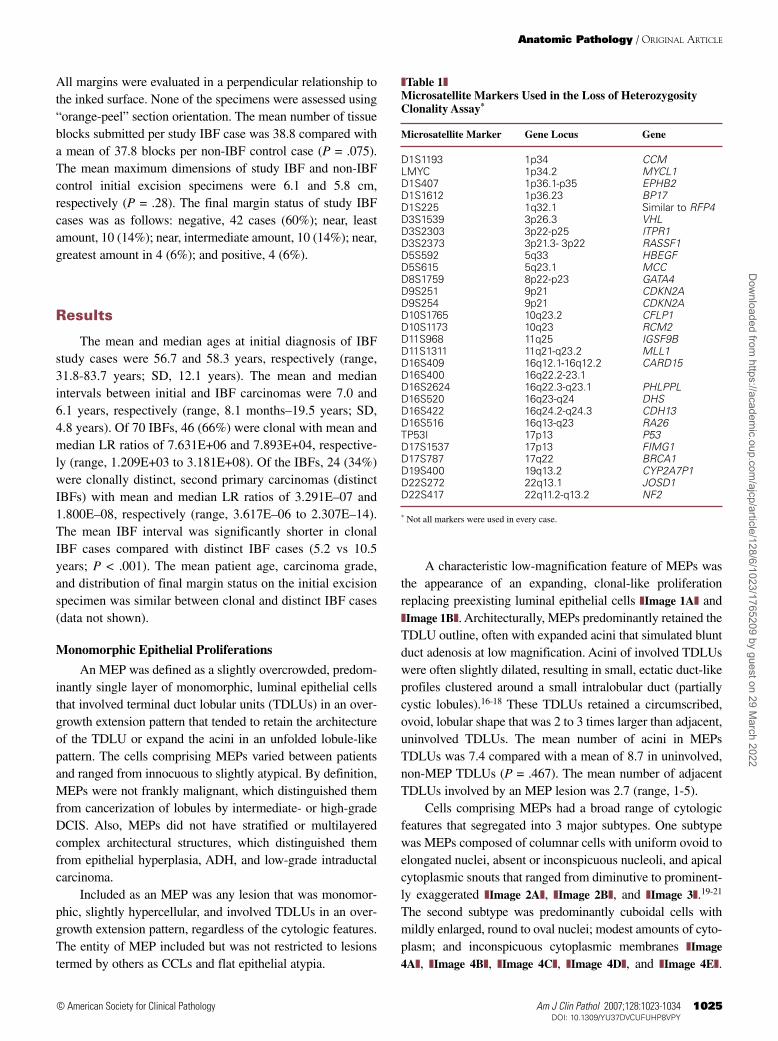
Cells comprising MEPs had a broad range of cytologicfeatures that segregated into 3 major subtypes. One subtypewas MEPs composed of columnar cells with uniform ovoid toelongated nuclei, absent or inconspicuous nucleoli, and apicalcytoplasmic snouts that ranged from diminutive to prominent-ly exaggerated ❚Image 2A❚, ❚Image 2B❚, and ❚Image 3❚.19-21
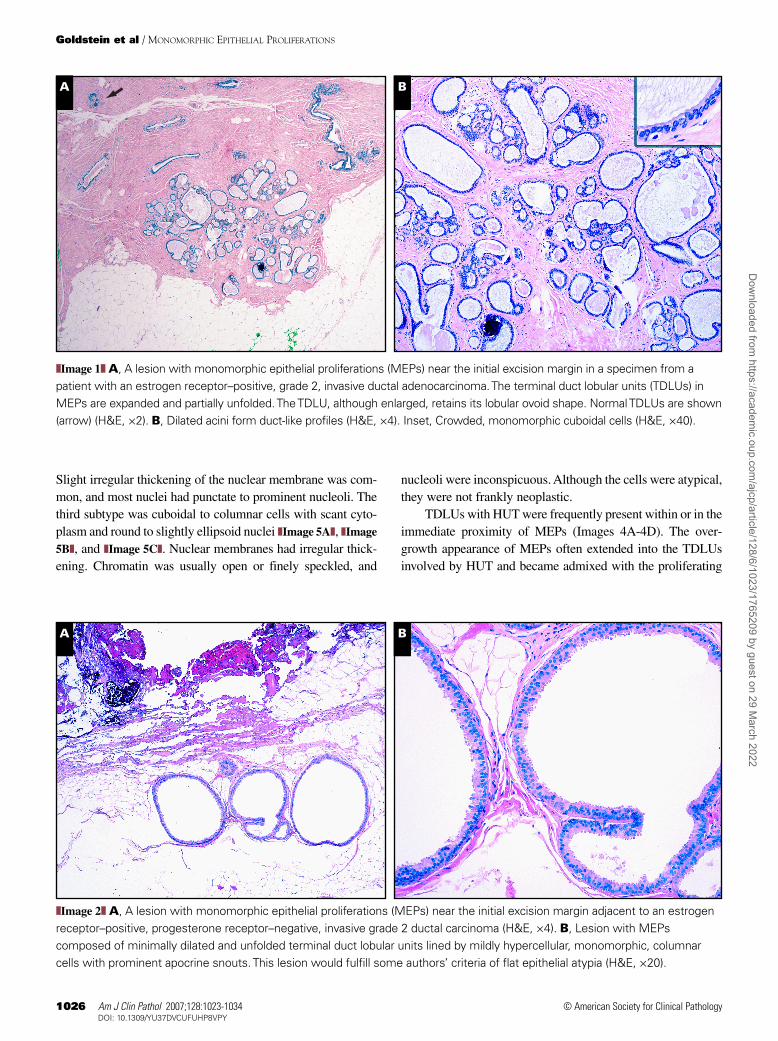
The second subtype was predominantly cuboidal cells withmildly enlarged, round to oval nuclei; modest amounts of cyto-plasm; and inconspicuous cytoplasmic membranes ❚Image
4A❚, ❚Image 4B❚, ❚Image 4C❚, ❚Image 4D❚, and ❚Image 4E❚.
Anatomic Pathology / ORIGINAL ARTICLE
❚Table 1❚Microsatellite Markers Used in the Loss of HeterozygosityClonality Assay*
Microsatellite Marker Gene Locus Gene
D1S1193 1p34 CCMLMYC 1p34.2 MYCL1D1S407 1p36.1-p35 EPHB2D1S1612 1p36.23 BP17D1S225 1q32.1 Similar to RFP4D3S1539 3p26.3 VHLD3S2303 3p22-p25 ITPR1D3S2373 3p21.3- 3p22 RASSF1D5S592 5q33 HBEGFD5S615 5q23.1 MCCD8S1759 8p22-p23 GATA4D9S251 9p21 CDKN2AD9S254 9p21 CDKN2AD10S1765 10q23.2 CFLP1D10S1173 10q23 RCM2D11S968 11q25 IGSF9BD11S1311 11q21-q23.2 MLL1D16S409 16q12.1-16q12.2 CARD15D16S400 16q22.2-23.1D16S2624 16q22.3-q23.1 PHLPPLD16S520 16q23-q24 DHSD16S422 16q24.2-q24.3 CDH13D16S516 16q13-q23 RA26TP53I 17p13 P53D17S1537 17p13 FIMG1D17S787 17q22 BRCA1D19S400 19q13.2 CYP2A7P1D22S272 22q13.1 JOSD1D22S417 22q11.2-q13.2 NF2
* Not all markers were used in every case.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/128/6/1023/1765209 by guest on 29 M
arch 2022
1026 Am J Clin Pathol 2007;128:1023-10341026 DOI: 10.1309/YU37DVCUFUHP8VPY
© American Society for Clinical Pathology
Goldstein et al / MONOMORPHIC EPITHELIAL PROLIFERATIONS
Slight irregular thickening of the nuclear membrane was com-mon, and most nuclei had punctate to prominent nucleoli. Thethird subtype was cuboidal to columnar cells with scant cyto-plasm and round to slightly ellipsoid nuclei ❚Image 5A❚, ❚Image
5B❚, and ❚Image 5C❚. Nuclear membranes had irregular thick-ening. Chromatin was usually open or finely speckled, and
nucleoli were inconspicuous. Although the cells were atypical,they were not frankly neoplastic.
TDLUs with HUT were frequently present within or in theimmediate proximity of MEPs (Images 4A-4D). The over-growth appearance of MEPs often extended into the TDLUsinvolved by HUT and became admixed with the proliferating
A B
❚❚Image 1❚❚ A, A lesion with monomorphic epithelial proliferations (MEPs) near the initial excision margin in a specimen from apatient with an estrogen receptor–positive, grade 2, invasive ductal adenocarcinoma. The terminal duct lobular units (TDLUs) inMEPs are expanded and partially unfolded. The TDLU, although enlarged, retains its lobular ovoid shape. Normal TDLUs are shown(arrow) (H&E, ×2). B, Dilated acini form duct-like profiles (H&E, ×4). Inset, Crowded, monomorphic cuboidal cells (H&E, ×40).
A B
❚❚Image 2❚❚ A, A lesion with monomorphic epithelial proliferations (MEPs) near the initial excision margin adjacent to an estrogenreceptor–positive, progesterone receptor–negative, invasive grade 2 ductal carcinoma (H&E, ×4). B, Lesion with MEPscomposed of minimally dilated and unfolded terminal duct lobular units lined by mildly hypercellular, monomorphic, columnarcells with prominent apocrine snouts. This lesion would fulfill some authors’ criteria of flat epithelial atypia (H&E, ×20).
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/128/6/1023/1765209 by guest on 29 M
arch 2022

Am J Clin Pathol 2007;128:1023-1034 10271027 DOI: 10.1309/YU37DVCUFUHP8VPY 1027
© American Society for Clinical Pathology
myoepithelial cells. The luminal cell component of HUTs werecytologically identical to the cells of the surrounding MEPs.
MEPs Near Initial Excision Specimen Final Margins
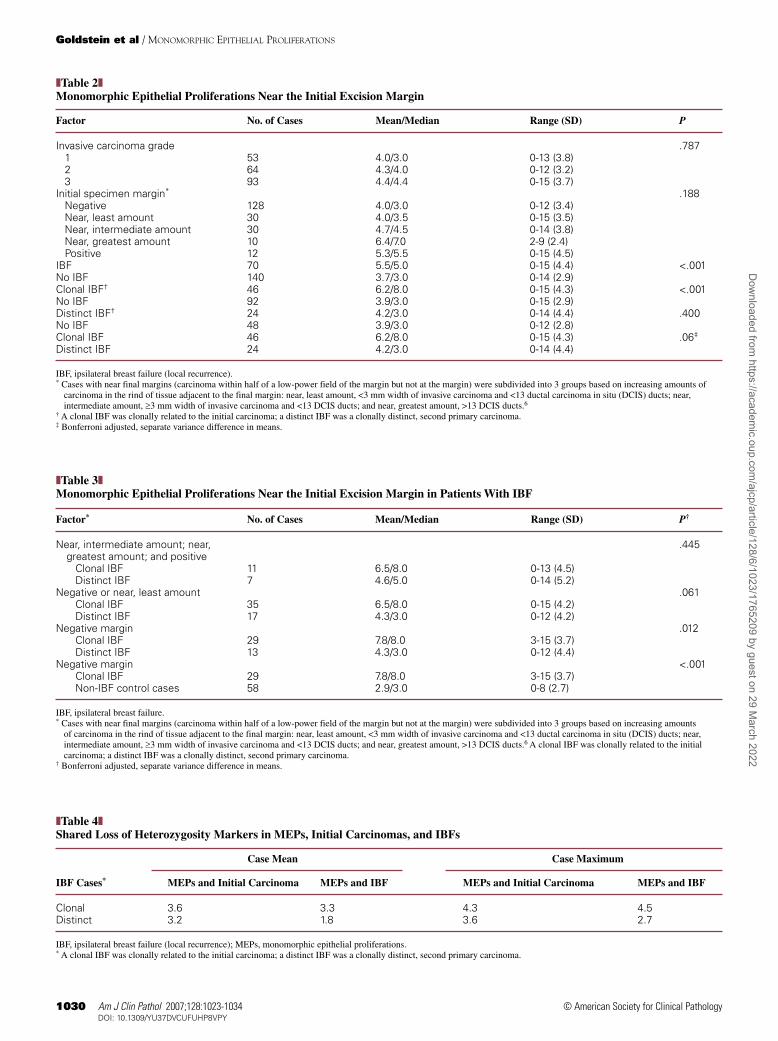
The mean and median numbers of MEPs near the finalmargin on the initial excision specimen in the 210 (study andmatched control) cases were 4.3 and 4.0, respectively (range,0-15; SD, 3.5). The mean number of MEPs near the initialexcision specimen margin was not related to the grade of inva-sive carcinoma or margin status ❚Table 2❚. The mean number ofMEPs was significantly higher in IBF cases compared withnon-IBF cases. This association was driven by the strength ofthe relationship between clonally related IBF cases, which hada mean of 6.2 MEPs near the initial excision specimen margincompared with a mean of 3.9 MEPs in matched non-IBF con-trol cases (P < .001). Distinct IBF cases had a number of MEPsnear the margin similar to that of non-IBF control cases.
The mean number of MEPs was not significantly differ-ent between clonal and distinct IBF groups when initial spec-imen margins that were negative or near, least amount wereanalyzed together ❚Table 3❚. When the analysis was restrictedto only cases with negative margins (no DCIS or invasive car-cinoma within 4.2 mm of the inked margin), clonal IBF caseshad a mean of 7.8 MEPs near the initial excision specimenmargin that was significantly greater than the mean of 4.3MEPs in the distinct IBF group (P = .012) and the mean of 2.9in the non-IBF matched control group (P < .001).
MEPs near the final margin on the initial excision speci-mens in the 42 IBF cases with negative initial excision margins
were carefully microdissected out of the paraffin blocks formolecular analysis using the glass slide as a template. Twenty-five cases (17 clonal IBF cases and 8 distinct IBF cases) hadDNA PCR amplification products of sufficient quality andquantity for meaningful interpretation. The mean number ofMEPs near the initial excision specimen margin analyzed percase was 4.4 in clonal IBF cases and 3.8 in distinct IBF cases.Only microsatellite markers with AIs in the respective initialand/or IBF carcinoma were evaluated to conserve MEP DNA.In clonal IBF cases, the mean number of microsatellite mark-ers with AIs shared between MEPs and initial carcinomas was3.6, which was similar to the mean of 3.3 shared betweenMEPs and IBFs ❚Table 4❚. The mean number of microsatellitemarker AIs shared between MEPs and initial carcinomas indistinct IBF cases was 3.2, which was substantially greaterthan the mean of 1.8 shared between MEPs and IBFs.
Discussion
Intraductal epithelial proliferations of the breast were tra-ditionally thought to progress through a stepwise linearsequence of mild and florid HUT, ADH, and intraductal carci-noma (DCIS) that eventuated in invasive carcinoma.22 HUTwas viewed for many years as the direct-lineage precursorlesion that was less than ADH. Accumulated morphologic andgenetic evidence suggests that HUT does not progress orrarely directly progresses to invasive carcinoma.8,23-27
Currently, it is considered to be a nonobligate marker ofincreased carcinoma risk.
There are 2 major molecular pathways leading to DCISand invasive breast carcinoma.7,28,29 Precursor lesions, lessthan ADH, for carcinomas with low- and high-grade molecularpathways have been the focus of recent interest. As a group,CCLs are the precursor lesions for some tubular and lobularcarcinomas with a low-grade molecular pathway. CCLs have avariety of cytologic and architectural alterations, each of whichis associated with distinct and progressively greater molecularalterations.30 Studies have elegantly shown that they form abiologic continuum that merges into low-grade DCIS.9-12 Aprecursor lesion less than ADH has not been identified for neo-plasms with a high-grade molecular pathway.7
The key morphologic features of CCLs are theirmonomorphism, slight hypercellularity, and TDLU over-growth extension pattern, in our opinion. Monomorphism sug-gests a clonal process. Slight hypercellularity indicates slightloss of control over architectural arrangement, possibly due toaberrant intercellular signaling. The TDLU overgrowth patternsuggests a slippage of cell cycle control or an aberrant prolif-eration response that is slightly greater than the backgroundnascent epithelium.31 By using CCLs and their relationship totubular carcinoma as the prototype, we expanded our search of
Anatomic Pathology / ORIGINAL ARTICLE
❚❚Image 3❚❚ A lesion with monomorphic epithelial proliferationshas dilated and unfolded the terminal duct lobular unit (H&E,×10). Inset, Monomorphic, slightly overcrowded columnarcells; although not frankly malignant, these cells are slightlymore atypical than the cells in Image 2 (H&E, ×60).
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/128/6/1023/1765209 by guest on 29 M
arch 2022
1028 Am J Clin Pathol 2007;128:1023-10341028 DOI: 10.1309/YU37DVCUFUHP8VPY
© American Society for Clinical Pathology
Goldstein et al / MONOMORPHIC EPITHELIAL PROLIFERATIONS
A B
C D
E❚❚Image 4❚❚ A, A lesion with monomorphic epithelial proliferations(MEPs) composed of a cluster of terminal duct lobular units(TDLUs) centered around a small interlobular duct. InvolvedTDLUs are at different stages of unfolding and dilation. Theterminal end of the interlobular duct has hyperplasia of the usualtype (HUT), which focally extends into the terminal duct of themiddle-level TDLU (H&E, ×1.5). B, The monomorphic epithelialcells of the lesion with MEPs seem to extend into and partiallyinvolve the HUT focus in the distal interlobular duct (H&E, ×10).C, Slightly hypercellular monomorphic epithelial cells replace the nascent TDLU epithelium. The MEP cell nuclei are slightlytoo large relative to the amount of cytoplasm. The nuclei ofoccasional cells have lost their basilar cytoplasmic position. Themitotic rate is increased (H&E, ×20). D, HUT focus in the distalinterlobular duct. The heterogeneous cell types comprising theHUT lesion are easily discerned. The MEP cells appear to haveovergrown into the HUT and become intimately admixed withthe other cells comprising the HUT (H&E, ×40). E, The HUTluminal cells are cytologically identical to the MEP cells thatextend out and unfold the surrounding TDLUs (H&E, ×40).
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/128/6/1023/1765209 by guest on 29 M
arch 2022

Am J Clin Pathol 2007;128:1023-1034 10291029 DOI: 10.1309/YU37DVCUFUHP8VPY 1029
© American Society for Clinical Pathology
precursor lesions for neoplasms with low- and high-grademolecular pathways to include all lesions with these 3 features,regardless of the cytologic features of the component cells. Wetermed these lesions MEPs. Under the MEP rubric were low-grade CCLs, including flat epithelial atypia,11,13,17-21,32,33
lesions termed hyperplastic enlarged lobular units by Lee etal,34 and lesions composed of cuboidal or slightly basaloidcells, termed nonstandard flat epithelial atypia by Boeckeret al.35,36
We found that MEP lesions were significantly more fre-quent in the rim of tissue near the initial excision margin inpatients in whom clonally related IBFs developed than inpatients in whom clonally distinct IBFs developed andpatients in whom no IBFs developed. In the subset of patientswith negative margins in initial excision specimen, patientswith clonal IBFs had significantly more MEPs near the mar-gin than patients with distinct IBFs and patients without IBFs.Although our analysis was limited, some MEPs in clonal and
distinct IBF cases shared AI microsatellite markers with theirrespective initial carcinoma. However, when shared AI mark-ers were compared between MEPs and IBF carcinomas, someMEPs had shared AI markers with their respective clonalIBFs, whereas there were almost no shared AI markersbetween MEPs in the initial excision specimens and distinctIBF carcinomas.
We suggest that MEPs, similar to CCLs, form the pool ofpartially transformed precursor lesions less than ADH orDCIS in many invasive carcinomas. MEPs also provide theconceptual framework that allows the integration of otherauthors’ findings into a single model.
Initiating molecular alterations in stem, progenitor, ortransit-amplifying cells early in life are thought to result inaberrant differentiation and increased susceptibility to furthermutations during a person’s lifetime.37-41 Breast epithelialstructures initially develop at puberty. TDLUs undergo pro-gressive differentiation during each menstrual cycle. With
Anatomic Pathology / ORIGINAL ARTICLE
A B
C❚❚Image 5❚❚ A, A lesion with a monomorphic epithelial proliferation(MEP) near the initial excision margin (not shown) from a patientwith a grade 3, estrogen receptor–positive, invasive ductalcarcinoma. The MEP expands and partially unfolds the involvedterminal duct lobular unit (TDLU). A normal, uninvolved TDLU isshown (arrow) (H&E, ×4). B, A predominantly single layer ofslightly hypercellular, monomorphic, epithelial cells involves theTDLU in an overgrowth extension pattern (H&E, ×20). C, Themonomorphic epithelial cells are atypical, but not franklymalignant. This is not cancerization of lobules by high-gradeductal carcinoma in situ cells. Conversely, there are insufficientarchitectural and cytologic features to diagnose atypical ductalhyperplasia (H&E, ×40).
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/128/6/1023/1765209 by guest on 29 M
arch 2022
1030 Am J Clin Pathol 2007;128:1023-10341030 DOI: 10.1309/YU37DVCUFUHP8VPY
© American Society for Clinical Pathology
Goldstein et al / MONOMORPHIC EPITHELIAL PROLIFERATIONS
❚Table 2❚Monomorphic Epithelial Proliferations Near the Initial Excision Margin
Factor No. of Cases Mean/Median Range (SD) P
Invasive carcinoma grade .7871 53 4.0/3.0 0-13 (3.8)2 64 4.3/4.0 0-12 (3.2)3 93 4.4/4.4 0-15 (3.7)
Initial specimen margin* .188Negative 128 4.0/3.0 0-12 (3.4)Near, least amount 30 4.0/3.5 0-15 (3.5)Near, intermediate amount 30 4.7/4.5 0-14 (3.8)Near, greatest amount 10 6.4/7.0 2-9 (2.4)Positive 12 5.3/5.5 0-15 (4.5)
IBF 70 5.5/5.0 0-15 (4.4) <.001No IBF 140 3.7/3.0 0-14 (2.9)Clonal IBF† 46 6.2/8.0 0-15 (4.3) <.001No IBF 92 3.9/3.0 0-15 (2.9)Distinct IBF† 24 4.2/3.0 0-14 (4.4) .400No IBF 48 3.9/3.0 0-12 (2.8)Clonal IBF 46 6.2/8.0 0-15 (4.3) .06‡
Distinct IBF 24 4.2/3.0 0-14 (4.4)
IBF, ipsilateral breast failure (local recurrence).* Cases with near final margins (carcinoma within half of a low-power field of the margin but not at the margin) were subdivided into 3 groups based on increasing amounts of
carcinoma in the rind of tissue adjacent to the final margin: near, least amount, <3 mm width of invasive carcinoma and <13 ductal carcinoma in situ (DCIS) ducts; near,intermediate amount, ≥3 mm width of invasive carcinoma and <13 DCIS ducts; and near, greatest amount, >13 DCIS ducts.6
† A clonal IBF was clonally related to the initial carcinoma; a distinct IBF was a clonally distinct, second primary carcinoma.‡ Bonferroni adjusted, separate variance difference in means.
❚Table 4❚Shared Loss of Heterozygosity Markers in MEPs, Initial Carcinomas, and IBFs
Case Mean Case Maximum
IBF Cases* MEPs and Initial Carcinoma MEPs and IBF MEPs and Initial Carcinoma MEPs and IBF
Clonal 3.6 3.3 4.3 4.5Distinct 3.2 1.8 3.6 2.7
IBF, ipsilateral breast failure (local recurrence); MEPs, monomorphic epithelial proliferations.* A clonal IBF was clonally related to the initial carcinoma; a distinct IBF was a clonally distinct, second primary carcinoma.
❚Table 3❚Monomorphic Epithelial Proliferations Near the Initial Excision Margin in Patients With IBF
Factor* No. of Cases Mean/Median Range (SD) P†
Near, intermediate amount; near, .445greatest amount; and positive
Clonal IBF 11 6.5/8.0 0-13 (4.5)Distinct IBF 7 4.6/5.0 0-14 (5.2)
Negative or near, least amount .061Clonal IBF 35 6.5/8.0 0-15 (4.2)Distinct IBF 17 4.3/3.0 0-12 (4.2)
Negative margin .012Clonal IBF 29 7.8/8.0 3-15 (3.7)Distinct IBF 13 4.3/3.0 0-12 (4.4)
Negative margin <.001Clonal IBF 29 7.8/8.0 3-15 (3.7)Non-IBF control cases 58 2.9/3.0 0-8 (2.7)
IBF, ipsilateral breast failure.* Cases with near final margins (carcinoma within half of a low-power field of the margin but not at the margin) were subdivided into 3 groups based on increasing amounts
of carcinoma in the rind of tissue adjacent to the final margin: near, least amount, <3 mm width of invasive carcinoma and <13 ductal carcinoma in situ (DCIS) ducts; near,intermediate amount, ≥3 mm width of invasive carcinoma and <13 DCIS ducts; and near, greatest amount, >13 DCIS ducts.6 A clonal IBF was clonally related to the initialcarcinoma; a distinct IBF was a clonally distinct, second primary carcinoma.
† Bonferroni adjusted, separate variance difference in means.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/128/6/1023/1765209 by guest on 29 M
arch 2022

Am J Clin Pathol 2007;128:1023-1034 10311031 DOI: 10.1309/YU37DVCUFUHP8VPY 1031
© American Society for Clinical Pathology
pregnancy, there is rapid proliferation and terminal secretorydifferentiation of TDLUs. Puberty and pregnancy are associ-ated with high-level proliferation of stem and progenitor cellsthat is the source material for lobular expansion. Geneticalterations incurred by stem and progenitor cells are thoughtto be dispersed throughout the lobe, its secondary lobules,and component TDLUs at the onset of puberty and with eachpregnancy.42,43
Each lobe is composed of discrete patches of monoclo-nal TDLUs derived from a single stem or progenitor cell.44,45
The proliferation rate, hormone receptor levels of luminalcells, and regression rate in TDLUs at menarche, in nulli-parous adults, and after pregnancy vary.46-49 Promotion stim-uli and the resultant proliferative response during the lifetimeof the person are applied at the individual monoclonal TDLUlevel.50 Over time, individual molecular events accrue in indi-vidual TDLUs that allow multiple, discrete clonal lesions,each with a unique set of genetic alterations, to emerge. Tot42
coined the term sick lobe syndrome to describe and explainthe lobar nature of these alterations in adults.
Several studies provide additional support for this model.One study found that the genetic heterogeneity found in HUT,ADH, and associated carcinomas supports the existence of afield cancerization defect.51 One study found that allelic loss-es in several key genes were sufficient to impair regulation ofproliferation arrest during normal menstrual cycle growth anddifferentiation in otherwise morphologically normalTDLUs.52 A subset of patients with HUT with a substantiallygreater percentage of cells dual-expressing ER-α and Ki-67had a significantly greater risk of subsequent invasive carcino-ma than patients with a smaller percentage of dual-expressingcells within HUT lesions.53 Meeker et al54 and Meeker andArgani55 found the extent of telomere shortening, a measure ofthe number of luminal cell replications, varied among benignTDLUs, potentially reflecting differences in sensitivity orreplication responsiveness between individual TDLUs. Webelieve that the multiple MEPs identified in most cases, oftenwith a range of cytologic appearances, are the morphologicmanifestation of the unique clonal proliferations derived fromgenetic alterations within individual TDLUs of a sick lobe.
We noted that MEPs frequently involved foci of HUT.The HUT involved by MEPs were often composed of cellsthat were cytologically identical to the MEP cells that extend-ed out and replaced the nascent cells of the surroundingTDLU. Although we did not formally investigate this relation-ship, its frequency suggested a more than happenstance rela-tionship. This observation could be viewed as running count-er to the opinions of contemporary authors. Boecker et al,based on a large personal experience and an erudite dissectionof the literature, lay out the argument that HUT is a dead-endlesion that is not a direct precursor of in situ or invasive breastcarcinoma.8,23,36,56,57
We suggest an alternative view to that of Boecker et alregarding the role of HUT in breast carcinogenesis. Somaticcell replication is finite owing to telomere shortening.58,59
Some HUTs and morphologically normal TDLUs adjacent toinvasive carcinomas have substantial telomere shortening,indicative of a large number of replication cycles that are notevident by morphologic examination alone.54,55 p16 isrequired to maintain cells in senescence once telomeresbecome critically short. Inactivation of p16 via hypermethyla-tion, with continued replication, leads to further telomere ero-sion, resulting in loss of the capping function and initiation ofthe breakage-fusion-bridge cycle. This causes high levels ofchromosomal instability and massive cell death, termedtelomere crisis.58,60-66
Levels of gene hypermethylation in normal breast epithe-lium are epidemiologically linked to carcinoma risk, support-ing the role of hypermethylation in the neoplastic transforma-tion process.67 In one study, hypermethylated field changes innormal parenchyma extended up to 4 cm beyond the invasivecarcinoma.68 Normal TDLUs from a substantial proportion ofhealthy, disease-free women contain p16-deficient luminalcells, which, under the appropriate conditions, can acquirechromosomal instability changes similar to those seen in pre-malignant lesions. These alterations occur during a preclonalphase that precedes morphologic premalignant lesions (ADHand DCIS).59,62,69-71
At the morphologic level, telomere crisis, chromosomalinstability, and cell immortalization begin in HUT lesions andare completed before the emergence of DCIS.72 Approximately10% of TDLUs with HUTs not associated with carcinomahave decreased apoptosis secondary to hypermethylation of14-3-3σ, evidence of biochemical transformation in morpho-logically normal (transformed) TDLUs.73 In other organs, suchas the cervix, active proliferation of the transition zone isrequired for neoplastic transformation to occur. It is possiblethat some HUTs, where cell proliferation is greatest, are themolecular engines from which MEPs are derived, with eachHUT focus giving rise to a clonally unique MEP. Cell immor-talization in the breast occurs temporally before neoplastictransformation.52 HUT, although not a direct precursor lesion,may be the nidus where partially transformed luminal cellswith slightly greater proliferation and lower apoptotic ratesarise. Morphologically, MEPs result from continued prolifera-tion and overgrowth expansion of these partially transformedclones. In the prototypic CCL lesion, initial bcl-2 immunoreac-tivity developed in 2 patterns: foci of columnar cells withapocrine snout morphologic features and a polyhedric patternwithin HUT.74 It is possible that the former pattern is theearliest stage of an MEP lesion arising out of HUT.
Most patients had multiple MEPs (mean, 4.3 MEPs nearthe margin per patient). We emphasize this point, in contrastwith the longstanding approach of viewing HUT as a singular
Anatomic Pathology / ORIGINAL ARTICLE
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/128/6/1023/1765209 by guest on 29 M
arch 2022

1032 Am J Clin Pathol 2007;128:1023-10341032 DOI: 10.1309/YU37DVCUFUHP8VPY
© American Society for Clinical Pathology
Goldstein et al / MONOMORPHIC EPITHELIAL PROLIFERATIONS
entity. Boecker et al36 pointed out that a small percentage ofHUTs have low-frequency genetic changes that are usuallyrandom and dissimilar from the alterations found in associat-ed carcinomas. These authors used this finding to support theiropinion that HUT was not a direct precursor lesion to carcino-ma. We suggest an alternative set of factors may be behind thisfinding that, in aggregate, support our MEP model. First, mul-tiple MEPs in a patient vary in number and cytologic featuresand, most likely, types of genetic alterations. Second, it is like-ly that a single or limited number of MEP lesions go throughtelomere crisis.53 Third, DCIS seems to arise from a single orlimited number of cells that survive crisis by telomerase reac-tivation.72 It is possible that the lack of repetitive and similargenetic alterations in HUT and associated carcinoma are dueto the low likelihood that the specific MEP that progressedinto and emerged through telomere crisis and subsequentlybecame invasive carcinoma was sampled for molecular analy-sis, especially because these events transpire throughout aperiod of time. It is interesting that Boecker et al and othersfound that a small proportion of HUTs are clonal neoplasticproliferations with low-level molecular alterations shared withinvasive carcinomas.8,75,76 This would be the expected resultgiven the aforementioned selection pressures on HUT.
This study is limited to describing MEPs and proposing amechanistic model of precursor lesions less than ADH or DCIS.In regard to radiation therapy after breast-conserving surgery,MEPs may explain some of the IBFs in patients with otherwisewidely negative margins. It is possible that the significant reduc-tion in IBF rate associated with radiation is via the eradicationof some or all MEPs, which prevents IBFs by reducing or elim-inating the pool of partially transformed clones from which sub-sequent IBFs emerge. Possibly, the low proliferative rate andnear-normal genetic profile allow some MEPs to be relativelyimmune to radiation. We identified an association betweenMEPs and IBFs; however, whether there is a direct cause-and-effect relationship between them is unknown.
Many aspects surrounding MEPs need to be studiedbefore they acquire clinical relevance, including a detailedcomparison of MEPs with previously described precursorlesions, such as ADH, CCL, and flat epithelial atypia. Thisstudy did not address the reproducibility of the MEP diagno-sis or correlate outcomes related to MEPs in a blinded man-ner. We recommend that MEPs should not be used as a diag-nostic entity until the clinical significance has been deter-mined. These subjects are being actively investigated and arethe focus of future studies.
From the Departments of 1Anatomic Pathology and 2RadiationOncology, William Beaumont Hospital, Royal Oak, MI.
Address reprint requests to Dr Goldstein: Dept of AnatomicPathology, William Beaumont Hospital, 3601 W 13 Mile Rd, RoyalOak, MI 48073.
References1. Early Breast Trialists’ Collaborative Group. Effects of
radiotherapy and of differences in the extent of surgery forearly breast cancer on local recurrence and 15-year survival: anoverview of the randomized trials. Lancet. 2005;366:2087-2106.
2. Lim M, Bellon JR, Gelman R, et al. A prospective study ofconservative surgery without radiation therapy in selectpatients with stage I breast cancer. Int J Radiat Oncol Biol Phys.2006;65:1149-1154.
3. Park CC, Mitsumori M, Nixon A, et al. Outcome at 8 yearsafter breast-conserving surgery and radiation therapy forinvasive breast cancer: influence of margin status and systemictherapy on local recurrence. J Clin Oncol. 2000;18:1668-1675.
4. Goldstein NS, Vicini FA, Hunter S, et al. Molecular clonalitydetermination of ipsilateral recurrence of invasive breastcarcinomas after breast-conserving therapy: comparison withclinical and biologic factors. Am J Clin Pathol. 2005;123:679-689.
5. Goldstein NS, Vicini FA, Hunter S, et al. Molecular clonalityrelationships in initial carcinomas, ipsilateral breast failures,and distant metastases in patients treated with breast-conserving therapy: evidence suggesting that some distantmetastases are derived from ipsilateral breast failures and thatmetastases can metastasize. Am J Clin Pathol. 2005;124:49-57.
6. Goldstein NS, Kestin L, Vicini F. Factors associated withipsilateral breast failure and distant metastases in patients withinvasive breast carcinoma treated with breast-conservingtherapy: a clinicopathologic study of 607 neoplasms from 583patients. Am J Clin Pathol. 2003;120:500-527.
7. Simpson PT, Reis-Filho JS, Gale T, et al. Molecular evolutionof breast cancer. J Pathol. 2005;205:248-254.
8. Boecker W, Moll R, Dervan P, et al. Usual ductal hyperplasiaof the breast is a committed stem (progenitor) cell lesiondistinct from atypical ductal hyperplasia and ductal carcinomain situ. J Pathol. 2002;198:458-467.
9. Abdel-Fatah TM, Powe DG, Hodi Z, et al. High frequency of coexistence of columnar cell lesions, lobular neoplasia, and low grade ductal carcinoma in situ with invasive tubularcarcinoma and invasive lobular carcinoma. Am J Surg Pathol.2007;31:417-426.
10. Dabbs DJ, Carter G, Fudge M, et al. Molecular alterations incolumnar cell lesions of the breast. Mod Pathol. 2006;19:344-349.
11. Fraser JL, Raza S, Chorny K, et al. Columnar alteration withprominent apical snouts and secretions: a spectrum of changesfrequently present in breast biopsies performed formicrocalcifications. Am J Surg Pathol. 1998;22:1521-1527.
12. Simpson PT, Gale T, Reis-Filho JS, et al. Columnar cell lesionsof the breast: the missing link in breast cancer progression? amorphological and molecular analysis. Am J Surg Pathol.2005;29:734-746.
13. Ellis IO, Schnitt SJ, Sastre-Garau X, et al. Tumours of thebreast. In: Tavassoli FA, Devilee P, eds. World HealthOrganization Classification of Tumours: Pathology and Genetics ofTumours of the Breast and Female Genital Organs. Lyon, France:IARC Press; 2003:9-112.
14. Elston CW, Ellis IO. Pathological prognostic factors in breastcancer, I: the value of histological grade in breast cancer:experience from a large study with long-term follow-up.Histopathology. 1991;19:403-410.
15. Sieben NL, Kolkman-Uljee SM, Flanagan AM, et al.Molecular genetic evidence for monoclonal origin of bilateralovarian serous borderline tumors. Am J Pathol. 2003;162:1095-1101.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/128/6/1023/1765209 by guest on 29 M
arch 2022

Am J Clin Pathol 2007;128:1023-1034 10331033 DOI: 10.1309/YU37DVCUFUHP8VPY 1033
© American Society for Clinical Pathology
16. Kusama R, Fujimori M, Matsuyama I, et al.Clinicopathological characteristics of atypical cystic duct(ACD) of the breast: assessment of ACD as a precancerouslesion. Pathol Int. 2000;50:793-800.
17. Oyama T, Maluf H, Koerner F. Atypical cystic lobules: an earlystage in the formation of low-grade ductal carcinoma in situ.Virchows Arch. 1999;435:413-421.
18. Oyama T, Iijima K, Takei H, et al. Atypical cystic lobule of thebreast: an early stage of low-grade ductal carcinoma in-situ.Breast Cancer. 2000;7:326-331.
19. Schnitt SJ. The diagnosis and management of pre-invasivebreast disease: flat epithelial atypia: classification, pathologicfeatures and clinical significance. Breast Cancer Res.2003;5:263-268.
20. Schnitt SJ, Vincent-Salomon A. Columnar cell lesions of the breast. Adv Anat Pathol. 2003;10:113-124.
21. Schnitt SJ. Flat epithelial atypia. In: Boecker W, ed.Preneoplasia of the Breast: A New Conceptual Approach toProliferative Breast Disease. Munich, Germany: Saunders;2006:369-378.
22. Lakhani SR, Chaggar R, Davies S, et al. Genetic alterations in “normal” luminal and myoepithelial cells of the breast. J Pathol. 1999;189:496-503.
23. Boecker W, Buerger H, Schmitz K, et al. Ductal epithelialproliferations of the breast: a biological continuum?comparative genomic hybridization and high-molecular-weightcytokeratin expression patterns. J Pathol. 2001;195:415-421.
24. Walker RA. Are all ductal proliferations of the breastpremalignant? J Pathol. 2001;195:401-403.
25. Ellis IO, Pinder SE, Lee AH, et al. A critical appraisal ofexisting classification systems of epithelial hyperplasia and insitu neoplasia of the breast with proposals for future methodsof categorization: where are we going? Semin Diagn Pathol.1999;16:202-208.
26. Buerger H, Mommers EC, Littmann R, et al. Correlation ofmorphologic and cytogenetic parameters of genetic instabilitywith chromosomal alterations in in situ carcinomas of thebreast. Am J Clin Pathol. 2000;114:854-859.
27. Shoker BS, Jarvis C, Sibson DR, et al. Oestrogen receptorexpression in the normal and pre-cancerous breast. J Pathol.1999;188:237-244.
28. Buerger H, Otterbach F, Simon R, et al. Comparative genomichybridization of ductal carcinoma in situ of the breast:evidence of multiple genetic pathways. J Pathol. 1999;187:396-402.
29. Buerger H, Simon R, Schäfer KL, et al. Genetic relation of lobular carcinoma in situ, ductal carcinoma in situ, andassociated invasive carcinoma of the breast. Mol Pathol.2000;53:118-121.
30. Pinder SE, Reis-Filho JS. Non operative breast pathology:columnar cell lesions. J Clin Pathol. 2006. doi:10.1136/jcp.2006.040634.
31. Noel JC, Fayt I, Fernandez-Aguilar S, et al. Proliferatingactivity in columnar cell lesions of the breast. Virchows Arch.2006;449:617-621.
32. Azzopardi JG. Underdiagnosis of malignancy. In: Problems inBreast Pathology. Philadelphia, PA: Saunders; 1979:192-213.
33. Rosen PP. Columnar cell hyperplasia is associated with lobularcarcinoma in situ and tubular carcinoma [letter]. Am J SurgPathol. 1999;23:1561.
34. Lee S, Mohsin SK, Mao S, et al. Hormones, receptors, andgrowth in hyperplastic enlarged lobular units: early potentialprecursors of breast cancer. Breast Cancer Res. 2006;8:R6.
35. Boecker W, Buerger H, Herbst H, et al. Basic principles of precursor lesions of breast cancer. In: Boecker W, ed.Preneoplasia of the Breast: A New Conceptual Approach toProliferative Breast Disease. Munich, Germany: Saunders;2006:337-368.
36. Boecker W, Buerger H, Herbst H, et al. Basic principles of benignproliferative breast disease. In: Boecker W, ed. Preneoplasia of theBreast: A New Conceptual Approach to Proliferative Breast Disease.Munich, Germany: Saunders; 2006:129-144.
37. Russo J, Balogh GA, Chen J, et al. The concept of stem cell in the mammary gland and its implication in morphogenesis,cancer and prevention. Front Biosci. 2006;11:151-172.
38. Savarese TM, Low HP, Baik I, et al. Normal breast stem cells,malignant breast stem cells, and the perinatal origin of breastcancer. Stem Cell Rev. 2006;2:103-110.
39. Dontu G, Al-Hajj M, Abdallah WM, et al. Stem cells innormal breast development and breast cancer. Cell Prolif.2003;36(suppl 1):59-72.
40. Liu BY, McDermott SP, Khwaja SS, et al. The transformingactivity of Wnt effectors correlates with their ability to inducethe accumulation of mammary progenitor cells. Proc Natl AcadSci U S A. 2004;101:4158-4163.
41. Kalirai H, Clarke RB. Human breast epithelial stem cells andtheir regulation. J Pathol. 2006;208:7-16.
42. Tot T. DCIS, cytokeratins, and the theory of the sick lobe.Virchows Arch. 2005;447:1-8.
43. Fridriksdottir AJ, Villadsen R, Gudjonsson T, et al.Maintenance of cell type diversification in the human breast. J Mammary Gland Biol Neoplasia. 2005;10:61-74.
44. Diallo R, Schaefer KL, Poremba C, et al. Monoclonality innormal epithelium and in hyperplastic and neoplastic lesionsof the breast. J Pathol. 2001;193:27-32.
45. Tsai YC, Lu Y, Nichols PW, et al. Contiguous patches ofnormal human mammary epithelium derived from a singlestem cell: implications for breast carcinogenesis. Cancer Res.1996;56:402-404.
46. Russo J, Lynch H, Russo IH. Mammary gland architecture as adetermining factor in the susceptibility of the human breast tocancer. Breast J. 2001;7:278-291.
47. Russo J, Tahin Q, Lareef MH, et al. Neoplastic transformationof human breast epithelial cells by estrogens and chemicalcarcinogens. Environ Mol Mutagen. 2002;39:254-263.
48. Milanese TR, Hartmann LC, Sellers TA, et al. Age-relatedlobular involution and risk of breast cancer. J Natl Cancer Inst.2006;98:1600-1607.
49. Walker RA, Martin CV. The aged breast. J Pathol.2007;211:232-240.
50. Avivar A, Garcia-Macias MC, Ascaso E, et al. Moderateoverexpression of AIB1 triggers pre-neoplastic changes inmammary epithelium. FEBS Lett. 2006;580:5222-5226.
51. Larson PS, de Las MA, Cerda SR, et al. Quantitative analysisof allele imbalance supports atypical ductal hyperplasia lesionsas direct breast cancer precursors. J Pathol. 2006;209:307-316.
52. Li Z, Meng ZH, Sayeed A, et al. Genome-wide allelotyping ofa new in vitro model system reveals early events in breastcancer progression. Cancer Res. 2002;62:5980-5987.
53. Shaaban AM, Sloane JP, West CR, et al. Breast cancer risk inusual ductal hyperplasia is defined by estrogen receptor-alphaand Ki-67 expression. Am J Pathol. 2002;160:597-604.
54. Meeker AK, Hicks JL, Gabrielson E, et al. Telomereshortening occurs in subsets of normal breast epithelium aswell as in situ and invasive carcinoma. Am J Pathol.2004;164:925-935.
Anatomic Pathology / ORIGINAL ARTICLE
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/128/6/1023/1765209 by guest on 29 M
arch 2022

1034 Am J Clin Pathol 2007;128:1023-10341034 DOI: 10.1309/YU37DVCUFUHP8VPY
© American Society for Clinical Pathology
Goldstein et al / MONOMORPHIC EPITHELIAL PROLIFERATIONS
55. Meeker AK, Argani P. Telomere shortening occurs earlyduring breast tumorigenesis: a cause of chromosomedestabilization underlying malignant transformation? JMammary Gland Biol Neoplasia. 2004;9:285-296.
56. Böcker W, Moll R, Poremba C, et al. Common adult stem cellsin the human breast give rise to glandular and myoepithelialcell lineages: a new cell biological concept. Lab Invest.2002;82:737-746.
57. Bankfalvi A, Ludwig A, De-Hesselle B, et al. Differentproliferative activity of the glandular and myoepitheliallineages in benign proliferative and early malignant breastdiseases. Mod Pathol. 2004;17:1051-1061.
58. Greenberg RA. Telomeres, crisis and cancer. Curr Mol Med.2005;5:213-218.
59. Romanov SR, Kozakiewicz BK, Holst CR, et al. Normalhuman mammary epithelial cells spontaneously escapesenescence and acquire genomic changes. Nature.2001;409:633-637.
60. Esteller M. Aberrant DNA methylation as a cancer-inducingmechanism. Annu Rev Pharmacol Toxicol. 2005;45:629-656.
61. Venkitaraman AR. Chromosomal instability and breast cancerpathogenesis. J Mammary Gland Biol Neoplasia. 2004;9:217-220.
62. McDermott KM, Zhang J, Holst CR, et al. p16(INK4a)prevents centrosome dysfunction and genomic instability inprimary cells. PLoS Biol. 2006;4:e51. doi:10.1371/journal.pbio.0040051.
63. Soler D, Genesca A, Arnedo G, et al. Telomere dysfunctiondrives chromosomal instability in human mammary epithelialcells. Genes Chromosomes Cancer. 2005;44:339-350.
64. Bailey SM, Murnane JP. Telomeres, chromosome instabilityand cancer. Nucleic Acids Res. 2006;34:2408-2417.
65. Yaswen P, Stampfer MR. Molecular changes accompanyingsenescence and immortalization of cultured human mammaryepithelial cells. Int J Biochem Cell Biol. 2002;34:1382-1394.
66. Li Y, Pan J, Li JL, et al. Transcriptional changes associatedwith breast cancer occur as normal human mammaryepithelial cells overcome senescence barriers and becomeimmortalized. Mol Cancer. 2007;6:7.
67. Lewis CM, Cler LR, Bu DW, et al. Promoter hypermethylationin benign breast epithelium in relation to predicted breastcancer risk. Clin Cancer Res. 2005;11:166-172.
68. Yan PS, Venkataramu C, Ibrahim A, et al. Mappinggeographic zones of cancer risk with epigenetic biomarkers innormal breast tissue. Clin Cancer Res. 2006;12:6626-6636.
69. Crawford YG, Gauthier ML, Joubel A, et al. Histologicallynormal human mammary epithelia with silenced p16(INK4a)over express COX-2, promoting a premalignant program.Cancer Cell. 2004;5:263-273.
70. Tlsty TD, Crawford YG, Holst CR, et al. Genetic andepigenetic changes in mammary epithelial cells may mimicearly events in carcinogenesis. J Mammary Gland BiolNeoplasia. 2004;9:263-274.
71. Berman H, Zhang J, Crawford YG, et al. Genetic andepigenetic changes in mammary epithelial cells identify asubpopulation of cells involved in early carcinogenesis. ColdSpring Harb Symp Quant Biol. 2005;70:317-327.
72. Chin K, de Solorzano CO, Knowles D, et al. In situ analyses ofgenome instability in breast cancer. Nat Genet. 2004;36:984-988.
73. Slater M, Danieletto S, Pooley M, et al. Differentiationbetween cancerous and normal hyperplastic lobules in breastlesions. Breast Cancer Res Treat. 2004;83:1-10.
74. Luna-More S, Weil B, Bautista D, et al. Bcl-2 protein innormal, hyperplastic and neoplastic breast tissues: a metaboliteof the putative stem-cell subpopulation of the mammary gland.Histol Histopathol. 2004;19:457-463.
75. Lakhani SR, Slack DN, Hamoudi RA, et al. Detection ofallelic imbalance indicates that a proportion of mammaryhyperplasia of usual type are clonal, neoplastic proliferations.Lab Invest. 1996;74:129-135.
76. Jones C, Merrett S, Thomas VA, et al. Comparative genomichybridization analysis of bilateral hyperplasia of usual type ofthe breast. J Pathol. 2003;199:152-156.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/128/6/1023/1765209 by guest on 29 M
arch 2022
Copyright © 2022 FDOKUMEN