
Molecular Targeting and Treatment of an Epidermal Growth Factor Receptor-Positive Glioma Using...
10
Molecular Targeting and Treatment of an Epidermal Growth Factor Receptor ^ Positive Glioma Using Boronated Cetuximab Gong Wu, 1 Weilian Yang, 1 Rolf F. Barth, 1 Shinji Kawabata, 1 Michele Swindall, 1 Achintya K. Bandyopadhyaya, 4 Werner Tjarks, 4 Behrooz Khorsandi, 5 Thomas E. Blue, 5 Amy K. Ferketich, 6 Ming Yang, 3 Gregory A. Christoforidis, 3 Thomas J. Sferra, 2,7 Peter J. Binns, 8 Kent J. Riley, 8 Michael J. Ciesielski, 9 and Robert A. Fenstermaker 9 Abstract Purpose: The purpose of the present study was to evaluate the anti ^ epidermal growth factor monoclonal antibody (mAb) cetuximab (IMC-C225) as a delivery agent for boron neutron capture therapy (BNCT) of a human epidermal growth factor receptor (EGFR) gene-transfected rat glioma, designated as F98 EGFR . Experimental Design: A heavily boronated polyamidoamine dendrimer was chemically linked to cetuximab by means of the heterobifunctional reagents N-succinimidyl 3-(2-pyridyldithio)- propionate and N-(k-maleimido undecanoic acid)-hydrazide. The bioconjugate, designated as BD-C225, was specifically taken up by F98 EGFR glioma cells in vitro compared with receptor- negative F98 wild-type cells (41.8 versus 9.1 Ag/g). For in vivo biodistribution studies, F98 EGFR cells were implanted stereotactically into the brains of Fischer rats, and 14 days later, BD-C225 was given intracerebrally by either convection enhanced delivery (CED) or direct intratumoral (i.t.) injection. Results: The amount of boron retained by F98 EGFR gliomas 24 h following CED or i.t. injection was 77.2 and 50.8 Ag/g, respectively, with normal brain and blood boron values <0.05 Ag/g. Boron neutron capture therapy was carried out at the Massachusetts Institute of Technology Research Reactor 24 h after CED of BD-C225, either alone or in combination with i.v. boronophe- nylalanine (BPA). The corresponding mean survival times (MST) were 54.5 and 70.9 days ( P = 0.017), respectively, with one long-term survivor (more than180 days). In contrast, the MSTs of irradiated and untreated controls, respectively, were 30.3 and 26.3 days. In a second study, the combination of BD-C225 and BPA plus sodium borocaptate, given by either i.v. or intracarotid injection, was evaluated and the MSTs were equivalent to that obtained with BD-C225 plus i.v. BPA. Conclusions: The survival data obtained with BD-C225 are comparable with those recently reported by us using boronated mAb L8A4 as the delivery agent. This mAb recognizes the mutant receptor, EGFRvIII. Taken together, these data convincingly show the therapeutic efficacy of molecular targeting of EGFR using a boronated mAb either alone or in combination with BPA and provide a platform for the future development of combinations of high and low molecular weight delivery agents for BNCTof brain tumors. Boron neutron capture therapy (BNCT) is based on the nuclear capture and fission reactions that occur when nonradioactive boron-10 is irradiated with low energy (e V 0.025 eV) thermal neutrons to produce 11 B in an unstable form, which undergoes instantaneous nuclear fission to produce a-particles and recoiling lithium-7 nuclei. These high linear energy transfer particles have a range of 5 to 9 Am, thereby restricting their destructive effects to only those cells containing 10 B. To be Authors’ Affiliations: Departments of 1 Pathology, 2 Pediatrics, and 3 Radiology, 4 College of Pharmacy, 5 Nuclear Engineering Program, and 6 School of Public Health, The Ohio State University; 7 Children’s Research Institute, Columbus, Ohio; 8 Nuclear Reactor Laboratory, Massachusetts Institute of Technology, Cambridge, Massachusetts; and 9 Department of Neurosurgery, Roswell Park Cancer Institute, Buffalo, NewYork Received 9/29/06; accepted 11/10/06. Grant support: NIH grants 1R01CA098945 (R.F. Barth) and 1R01NS39071 (T.J. Sferra); the Roswell Park Alliance Foundation (R.A. Fenstermaker); and U.S. Department of Energy through the program of Innovations in Nuclear Infrastructure and Education, Office of Nuclear Energy, Science and Technology (contract nos. DE- FG07-02ID14420 and DE-FG07-02 [K14420]) and the Office of Environmental and Biological Research (contract no. DE-FG02-02ER63358). The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. Note: Current address for T.J. Sferra: Department of Pediatrics, University of Oklahoma Health Sciences Center, Oklahoma City, OK; current address for S. Kawabata: Department of Neurosurgery, Osaka Medical College, Takatsuki City, Osaka, Japan. Presented in part at the 12th International Symposium on Neutron CaptureTherapy, Takamatsu, Japan, October 9-12, 2006. Requests for reprints: Rolf F. Barth, Department of Pathology, The Ohio State University, 165 Hamilton Hall, 1645 Neil Avenue, Columbus, OH 43210. Phone: 614-292-2177; Fax: 614-292-7072; E-mail: rolf.barth@osumc.edu. F 2007 American Association for Cancer Research. doi:10.1158/1078-0432.CCR-06-2399 Cancer Therapy: Preclinical www.aacrjournals.org Clin Cancer Res 2007;13(4) February 15, 2007 1260 Cancer Research. on February 8, 2016. © 2007 American Association for clincancerres.aacrjournals.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Molecular Targeting and Treatment of an Epidermal Growth Factor Receptor-Positive Glioma Using...

Molecular Targeting andTreatment of an Epidermal Growth FactorReceptor^Positive Glioma Using Boronated CetuximabGong Wu,1Weilian Yang,1Rolf F. Barth,1Shinji Kawabata,1Michele Swindall,1Achintya K. Bandyopadhyaya,4
Werner Tjarks,4 Behrooz Khorsandi,5 Thomas E. Blue,5 Amy K. Ferketich,6 Ming Yang,3
Gregory A. Christoforidis,3 Thomas J. Sferra,2,7 Peter J. Binns,8 Kent J. Riley,8
MichaelJ. Ciesielski,9 and Robert A. Fenstermaker9
Abstract Purpose: The purpose of the present study was to evaluate the anti ^ epidermal growth factormonoclonal antibody (mAb) cetuximab (IMC-C225) as a delivery agent for boron neutroncapture therapy (BNCT) of a human epidermal growth factor receptor (EGFR) gene-transfectedrat glioma, designated as F98EGFR.Experimental Design: A heavily boronated polyamidoamine dendrimer was chemically linkedto cetuximab by means of the heterobifunctional reagents N-succinimidyl 3-(2-pyridyldithio)-propionate and N-(k-maleimido undecanoic acid)-hydrazide. The bioconjugate, designated asBD-C225, was specifically taken up by F98EGFR glioma cells in vitro compared with receptor-negative F98 wild-type cells (41.8 versus 9.1 Ag/g). For in vivo biodistribution studies, F98EGFRcells were implanted stereotactically into the brains of Fischer rats, and 14 days later, BD-C225was given intracerebrally by either convection enhanced delivery (CED) or direct intratumoral(i.t.) injection.Results:The amount of boron retained by F98EGFR gliomas 24 h following CED or i.t. injectionwas 77.2 and 50.8 Ag/g, respectively, with normal brain and blood boron values <0.05 Ag/g.Boron neutron capture therapy was carried out at the Massachusetts Institute of TechnologyResearch Reactor 24 h after CEDof BD-C225, either alone or in combinationwith i.v. boronophe-nylalanine (BPA). The corresponding mean survival times (MST) were 54.5 and 70.9 days(P = 0.017), respectively, with one long-term survivor (more than180 days). In contrast, theMSTsof irradiated anduntreated controls, respectively, were 30.3 and 26.3 days. In a second study, thecombination of BD-C225 and BPA plus sodium borocaptate, given by either i.v. or intracarotidinjection, was evaluated and the MSTs were equivalent to that obtained with BD-C225 plus i.v.BPA.Conclusions: The survival data obtained with BD-C225 are comparable with those recentlyreportedbyus usingboronatedmAbL8A4 as the delivery agent.ThismAb recognizes themutantreceptor, EGFRvIII. Taken together, these data convincingly show the therapeutic efficacy ofmolecular targeting of EGFR using a boronated mAb either alone or in combination with BPAand provide a platform for the future development of combinations of high and low molecularweight delivery agents for BNCTof brain tumors.
Boron neutron capture therapy (BNCT) is based on the nuclearcapture and fission reactions that occur when nonradioactiveboron-10 is irradiated with low energy (e V 0.025 eV) thermalneutrons to produce 11B in an unstable form, which undergoes
instantaneous nuclear fission to produce a-particles andrecoiling lithium-7 nuclei. These high linear energy transferparticles have a range of 5 to 9 Am, thereby restricting theirdestructive effects to only those cells containing 10B. To be
Authors’Affiliations: Departments of 1Pathology, 2Pediatrics, and 3Radiology,4College of Pharmacy, 5Nuclear Engineering Program, and 6School of PublicHealth,The Ohio State University; 7Children’s Research Institute, Columbus, Ohio;8Nuclear Reactor Laboratory, Massachusetts Institute of Technology, Cambridge,Massachusetts; and 9Department of Neurosurgery, Roswell Park Cancer Institute,Buffalo, NewYorkReceived 9/29/06; accepted11/10/06.Grant support: NIH grants1R01CA098945 (R.F. Barth) and1R01NS39071 (T.J.Sferra); the Roswell Park Alliance Foundation (R.A. Fenstermaker); and U.S.Department of Energy through the program of Innovations in Nuclear Infrastructureand Education, Office ofNuclear Energy, Science andTechnology (contract nos.DE-FG07-02ID14420 andDE-FG07-02 [K14420]) and theOffice of Environmental andBiological Research (contract no. DE-FG02-02ER63358).
The costs of publication of this article were defrayed in part by the payment of pagecharges.This article must therefore be hereby marked advertisement in accordancewith18 U.S.C. Section1734 solely to indicate this fact.Note:Currentaddressfor T.J.Sferra:DepartmentofPediatrics,UniversityofOklahomaHealthSciencesCenter,OklahomaCity,OK;currentaddress forS.Kawabata:DepartmentofNeurosurgery,OsakaMedicalCollege,TakatsukiCity,Osaka, Japan.Presented in part at the12th International Symposium on Neutron CaptureTherapy,Takamatsu, Japan,October 9-12, 2006.Requests for reprints: Rolf F. Barth, Department of Pathology,The Ohio StateUniversity, 165 Hamilton Hall, 1645 Neil Avenue, Columbus, OH 43210. Phone:614-292-2177; Fax: 614-292-7072; E-mail: [email protected].
F2007 American Association for Cancer Research.doi:10.1158/1078-0432.CCR-06-2399
Cancer Therapy: Preclinical
www.aacrjournals.orgClin Cancer Res 2007;13(4) February15, 2007 1260
Cancer Research. on February 8, 2016. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from

effective, BNCT requires a sufficient amount (20-30 Ag/g) of10B, homogeneously distributed in the tumor, with concomi-tantly low 10B concentrations in surrounding normal tissues.These requirements, as well as clinical applications, have beendiscussed in detail in several recent reviews and monographs(1–5). BNCT primarily has been used to treat high-gradegliomas and either cutaneous primaries or cerebral metastasesof melanoma (1). More recently, it has also been used to treatpatients with recurrent tumors of the head and neck andcolorectal cancer metastatic to the liver (1).Both the epidermal growth factor (EGF) receptor (EGFR) and
its mutant isoform EGFRvIII frequently are overexpressed inhuman glioblastomas (6–9), which make them attractivetargets for the treatment of brain tumors (10). We haveinvestigated molecular targeting of EGFR or EGFRvIII usingEGF (11–13), or the monoclonal antibodies (mAb) cetuximab(14, 15) and L8A4 (16, 17), which have been linked to aheavily boronated polyamidoamine dendrimer. Cetuximab(Erbitux), known previously as IMC-C225, is a chimericmouse-human mAb that originally was produced in thelaboratory of Dr. John Mendelsohn (University of TexasM. D. Anderson Cancer Center, Houston, TX; ref. 18). It hasgreater affinity for EGFR than either EGF or transforminggrowth factor-a, and following binding, the receptor-antibodycomplex is rapidly internalized, thereby eliminating furtheractivation of the receptor (19, 20). Down-regulation of cellsurface receptor binding sites and competition of cetuximab forthe remaining binding sites can reduce or prevent furtheractivation by ligand. Several mechanisms have been proposedto explain the antitumor activity of cetuximab (21–23). Theseinclude cell cycle arrest (24), apoptosis (25), decrease inangiogenesis and cellular adhesion (26, 27), and inhibitionof matrix metalloproteinase expression and activity (28).Enhancement of the cytotoxic effects of chemotherapeuticagents (29) and the response to ionizing radiation have alsobeen reported (30). Cetuximab is reactive with both wild-typeEGFR and EGFRvIII (14), and recently, it has been approved bythe U.S. Food and Drug Administration for use in patients withEGFR-positive colorectal cancer metastatic to the liver andrecurrent head and neck cancers (31). Because of its pleiotropiceffects, cetuximab is particularly attractive as a boron deliveryagent for NCT of gliomas. In the present report, we describestudies to evaluate boronated cetuximab as a delivery agent forBNCT of the F98 rat glioma, which has been transfected with thegene encoding human EGFR (F98EGFR). Our data convincinglyshow its efficacy for BNCT of this tumor, used either alone or incombination with boronophenylalanine (BPA), a drug that hasbeen used clinically for BNCT of brain tumors (1).
Materials andMethods
Preparation of the bioconjugate BD-C225. Cetuximab was gener-ously provided to us by Dr. Daniel Hicklin (ImClone Systems, Inc.,New York, NY). Site-specific attachment of a heavily boronatedpolyamidoamine dendrimer was carried out, as described by us indetail elsewhere (14). Briefly, a fifth generation polyamidoaminedendrimer (Sigma-Aldrich, St. Louis, MO), containing 128 terminalamino groups, was reacted with an isocyanato polyhedral boraneanion, Na(CH3)3NB10H8NCO. This yielded a heavily boronatedmacromolecule, which contained f1,100 boron atoms per moleculeof dendrimer. Cetuximab was linked to the boronated dendrimer (BD)by two heterobifunctional linkers, N-succinimidyl 3-(2-pyridyldithio)-
propionate and N-(k-maleimido undecanoic acid)-hydrazide (14).Protein content of the bioconjugate was determined spectrophotomet-rically by means of the Coomassie blue assay reagent (Pierce, Rockford,IL) and boron was quantified by means of direct current plasma-atomicemission spectroscopy (DCP-AES; 32).
In vitro cellular uptake of BD-C225. For in vitro boron uptakestudies, F98 glioma cells, expressing 106 human EGFRs per cell(F98fEGFR), were used. These were produced by Dr. Frank Furnari(Ludwig Institute for Cancer Research, La Jolla, CA), who generouslyprovided them to us. Five million F98 wild-type (F98WT), F98fEGFR, orF98npEGFRvIII (17) glioma cells were seeded into T-150 flasks withDMEM containing 10% fetal bovine serum (Life Technologies, Inc.,Rockville, MD) supplemented with 100 units/mL penicillin and 100Ag/mL streptomycin. After incubation for 24 h at 37jC, the mediumwas replaced with DMEM containing 1.68 mg BD-C225 (90 Ag boron),and the cells were incubated for an additional 2 h at 37jC. Followingthis, the medium was decanted and the cells were washed thrice withPBS (pH 7.4), disaggregated by exposure to 0.5 mmol/L EDTA for5 min, counted, and sedimented. Cells were digested with concentratedsulfuric acid and 50% hydrogen peroxide, and boron uptake wasdetermined by DCP-AES (32).
In vitro neutron irradiation studies. For in vitro neutron irradiationstudies, F98fEGFR glioma cells, expressing 106 receptor sites per cell,were cultured until confluent. Cells were harvested by exposure to 0.5mmol/L EDTA and washed thrice with PBS, and aliquots containing 106
cells were dispensed into 2-mL plastic vials. Except for unirradiatedcontrol cells, either cetuximab or BD-C225 was added to all other vialsand incubated at 4jC for 90 min following which they were washedthrice with medium. Triplicate samples were irradiated with thermalneutrons at The Ohio State University Research Reactor for 1, 2, 5, or10 min at a thermal neutron flux of 109 cm�2 sec�1. After irradiation,aliquots of 10,000 cells were taken from each vial and seeded into 96-well microplates (Corning, Corning NY). Cell survival was determined72 h later by means of the sulforhodamine B assay (33). A clonogenicassay also was carried out following irradiation to assess cell survival(34). Briefly, varying numbers of F98fEGFR cells were seeded into 100-mm Petri dishes and incubated for 7 days at 37jC in an atmospherecontaining 95% air and 5% CO2. Following this, the medium wasdecanted and the cells were fixed by adding 2 to 3 mL of 37%formaldehyde, and then the plates were stained with 3 to 5 mL ofsaturated crystal violet. The number of colonies containing at least 50cells was enumerated visually by counting under a dissectingmicroscope. The surviving fraction was calculated from the number ofcolonies enumerated / number of cells plated � plating efficiency / 100.Tumor implantation and biodistribution of BD-C225. F98EGFR
glioma cells expressing 105 receptor sites per cell, described previouslyby us in detail (12), were used for in vivo studies. This cell line, whichhas been stable for over 5 years, was produced by transfecting F98 wild-type (F98WT) cells with the human gene encoding wild-type EGFR (11).These cells were used to obviate an immune response directed againsthuman EGFR, which we found occurred when cells expressing 106
receptor sites were implanted i.c. into immunocompetent Fischer rats.10
After i.c. implantation into syngeneic Fischer rats, the F98EGFR gliomaforms a progressively growing, infiltrative tumor that invariably resultsin the death of the host with an inoculum as few as 1,000 cells (35).Cells were maintained and propagated in vitro in supplemented DMEMcontaining 600 Ag/mL geneticin (G418; Sigma-Aldrich). F98WT cellswere cultured in the same medium, but without G418. Animal studieswere done in accordance with the Guide for the Care and Use ofLaboratory Animals (National Academy Press, Washington, DC, 1996)and the protocol was approved by the Institutional Laboratory AnimalCare and Use Committee of The Ohio State University (Columbus,OH). CD-Fischer rats (Charles River Laboratories, Wilmington, MA),weighing 200 to 220 g, were anesthetized with a 1.2:1 mixture of
10 R.F. Barth and W.Yang, unpublished data.
Molecular Targeting of EGFR-Positive Gliomas
www.aacrjournals.org Clin Cancer Res 2007;13(4) February15, 20071261
Cancer Research. on February 8, 2016. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from
ketamine/xylazine at a dose of 120 mg of ketamine/20 mg of xylazine/kg body weight. Following this, tumor cells were implanted stereo-tactically, as originally described by us (36). A small plastic screw(Arrow Machine Manufacturing, Inc., Richmond, VA) with an entryport, which allowed insertion of a 27-gauge needle, was embedded intothe calvarium before tumor cell implantation. BD-C225 was given i.c.by means of convection enhanced delivery (CED), using a syringepump at a rate of 0.33 AL/min for 30 min to deliver a volume of 10 AL(Harvard Apparatus Co., Cambridge, MA) as described previously (12).This technique, completely bypasses the blood-brain barrier, maximizesdelivery to the tumor and minimizes uptake by extracranial organs andblood (37, 38). For CED, a plastic cannula was inserted into the entryport and then advanced 5 mm below the dura into the tumor ofF98EGFR glioma-bearing rats. Biodistribution studies were carried out intumor-bearing rats 12 to 14 days following tumor cell implantation.Animals were divided into four experimental groups of four to five ratseach. Animals in groups 1 and 2 had F98EGFR gliomas and received750 Ag BD-C225 (40 Ag B) by CED at a rate of 0.33 AL/min or intra-tumoral (i.t.) injection. Rats in groups 3 and 4 received an i.v. injectionof BPA (500 mg/kg body weight, equivalent to 27 mg 10B/kg bodyweight) or BD-C225 by CED with i.v. BPA (Katchem Ltd., Prague, CzechRepublic). The biodistribution of BD-C225 was determined at 24 h afterCED by measuring concentrations of boron in various tissue samples byDCP-AES (32). Animals were euthanized by an overdose of halothanefollowing which tumors and normal tissues consisting of brain, blood,liver, kidney, and muscle were removed and weighed.
Therapy experiments and dosimetry. Neutron irradiations for these
experiments were identical to those reported previously by us using the
boronated mAb L8A4 (17). BNCT was done 14 days following stereo-
tactic implantation of 103 F98EGFR glioma cells. Rats were transportedapproximately 5 to 7 days before irradiation to Massachusetts Institute
of Technology (Cambridge, MA) where they were housed in an
accredited animal care facility supervised by the Division of Compar-
ative Medicine. Before irradiation at the Nuclear Reactor Laboratory,
they were randomized based on weight into experimental groups of 7 to11 animals each as follows: group 1, untreated controls; group 2,
irradiated controls; group 3, i.v. BPA, followed by BNCT; group 4, i.t. of
BD-C225 followed by BNCT; group 5, CED of BD-C225 followed
by BNCT; and group 6, CED of BD-C225 plus i.v. BPA, followed byBNCT. BNCT was initiated 24 h after CED of 10 AL of 750 Ag BD-C225(40 Ag 10B) and 2.5 h after i.v. administration of BPA (500 mg/kg body
weight). In a second study, using a different lot number of F98EGFR cells,
rats received BD-C225 in combination with either i.v. or intracarotid
administration of sodium borocaptate (BSH), another drug that hasbeen used in both experimental (39, 40) and clinical studies (1) of
BNCT. All irradiated rats were anesthetized with a mixture of ketamine
and xylazine. Irradiations were carried out at the MITR-II nuclear reactor
in the M011 irradiation facility (41). This produces a thermal neutron
beam of high purity and intensity with no measurable fast neutroncomponent (42). Rats were positioned two at a time in a lithiated (95%6Li enriched) polyethylene box that provided whole-body shielding
from the thermal neutrons during irradiation. The head of each animal
was aligned in the middle of a 13� 2 cm2 aperture, machined in the boxlid, which served as the beam delimiter. The output generated by four
fission counters, located at the periphery of the 15 cm circular field,
automatically controlled beam delivery and provided real-time data on
the relative neutron fluence during an irradiation and was used to
automatically control beam delivery that was reproducible to within 1%.The beammonitors were calibrated against dosimetric measurements,
which were carried out on both euthanized rats and phantoms madefrom type 6 nylon, using bare gold foils and a graphite-walled ionizationchamber (V = 0.1 cm3) flushed with reagent grade CO2 (43). Themeasured dose rates in brain (2.2% nitrogen by weight), normalized tothe reactor operating at a power of 5 MW, were 18.5 cGy/min forphotons, 7.7 cGy/min for thermal neutrons from the nitrogen capturereaction, and 3.4 cGy/min per Ag 10B in tissues. The estimateduncertainties on all these dose rates were 5%. Boron concentrations
were determined in tumor, normal brain, liver, and blood in a separategroup of animals 24 h after CED of BD-C225 and 2.5 h after i.v.injection of BPA to estimate absorbed doses in these tissues. Animalirradiations were done with the reactor operating at a power between 4.0and 4.8 MW. These took between 6.9 and 8.6 min to deliver a thermalneutron fluence of 2.64 � 1012 n cm�2 that matches previous doseprescriptions (13, 15). After completion of BNCT, the animals werereturned to The Ohio State University for clinical monitoring.Monitoring of clinical status and neuropathologic evaluation. All
animals were weighed thrice weekly and their clinical status wasevaluated at the same time. Once the animals had progressively growingtumors, as evidenced by the combination of sustained weight loss,ataxia, and periorbital hemorrhage, they were euthanized to minimizediscomfort. Survival times were determined by adding 1 day to the timebetween tumor implantation and euthanization. The brains of allanimals in the therapy studies were removed after death, fixed in 10%buffered formalin, and then cut coronally at the level of the opticalchiasm and 2 mm anterior and posterior to it. Coronal slices wereembedded in paraffin, cut at 4 Am, stained with H&E, and thenexamined microscopically to assess the histopathologic changes. Thetumor size index was determined from H&E-stained coronal sections ofbrain using a semiquantitative grading scale ranging from 0 to 4. Eachsection was scored as follows: 0, no tumor; 1, very small (i.e.,microscopic, <1 mm); 2, small (approximately 1-3 mm); 3, large(approximately 4-7 mm); and 4, massive (>8 mm); the mean score wascalculated for each group.Magnetic resonance imaging. Magnetic resonance (MR) images of
brain tumor–bearing rats were generated on a Bruker Avance scanner(Bruker, Billerica, MA) interfaced with Techron gradient amplifiers(Crown International, Elkhart, IN) and Magnex gradients (MagnexScientific, Abingdon, England) using a custom-built radio frequencyfront end. A custom-made, 4 cm in diameter birdcage coil was tuned tothe head of the rat at 340 MHz while the rat was in the prone position.Ultrasmall particles of iron oxide (SHU555C, Supravist; Schering AG,Berlin, Germany) were used as a contrast agent. These were given i.v.(2.0 mg Fe/kg) via a right femoral vein catheter after anesthetizing theanimals with isoflurane. Each animal was scanned before and afterinjection of ultrasmall particles of iron oxide using a high resolutionT2*-weighted gradient recalled echo sequence with an in-planeresolution of 78 Am. The images were generated with the followingpulse-sequence variables: time of repetition, 500 msec; time of echo,14.6 msec; flip angle, 22.5j; field of view, 4 cm; matrix, 512 � 512; slicethickness/gap, 1/0.1 mm; and acquisition time, 10 min and 14 s.
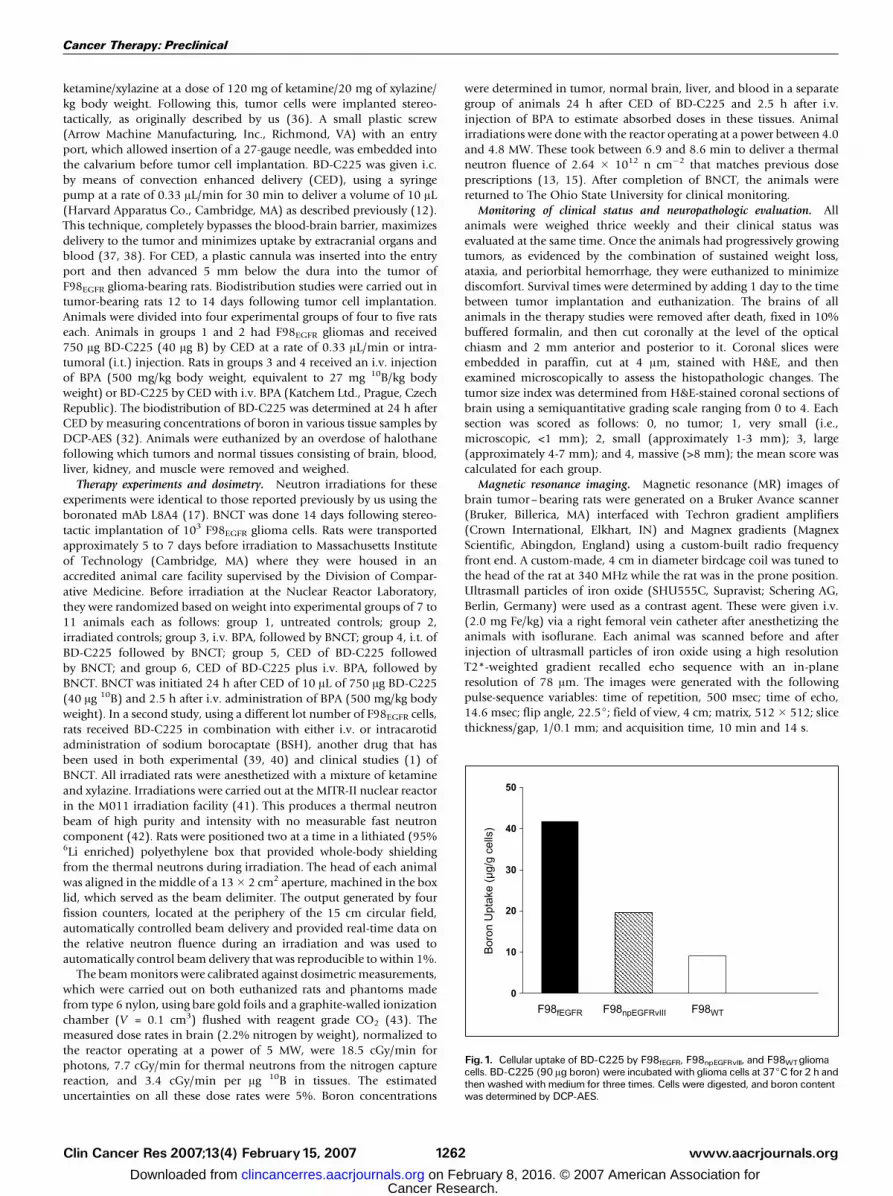
Fig. 1. Cellular uptake of BD-C225 by F98fEGFR, F98npEGFRvIII, and F98WTgliomacells. BD-C225 (90 Ag boron) were incubated with glioma cells at 37jC for 2 h andthen washed with medium for three times. Cells were digested, and boron contentwas determined by DCP-AES.
Cancer Therapy: Preclinical
www.aacrjournals.orgClin Cancer Res 2007;13(4) February15, 2007 1262
Cancer Research. on February 8, 2016. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from
Statistical evaluation of survival data. The mean survival time(MST), SE, and median survival time were calculated for each groupusing the Kaplan-Meier method that enabled Kaplan-Meier Survival andCox proportional hazard survival curves to be plotted (44). Thehypotheses involved comparing each BD-C225–treated animal to eachirradiated control. A log-rank test was used for these comparisons, witha Bonferroni method of adjustment for the multiple comparisons (45).Because five comparisons were tested for statistical significance withinthe BD-C225 tests, an a = 0.0125 was used.
Results
In vitro uptake and irradiation studies. To show that thebioconjugate was selectively taken up by EGFR-positive gliomacells, F98WT, F98fEGFR, and F98npEGFRvIII cells were incubatedwith 1.68 mg BD-C225 (90 Ag B) for 2 h at 37jC. Asdetermined by DCP-AES, 41.8 Ag B were taken up by 109
F98fEGFR cells, 19.6 Ag by F98npEGFRvIII cells, and 9.1 Ag byF98WT cells (Fig. 1), which was a 4.6- to 2.2-fold difference
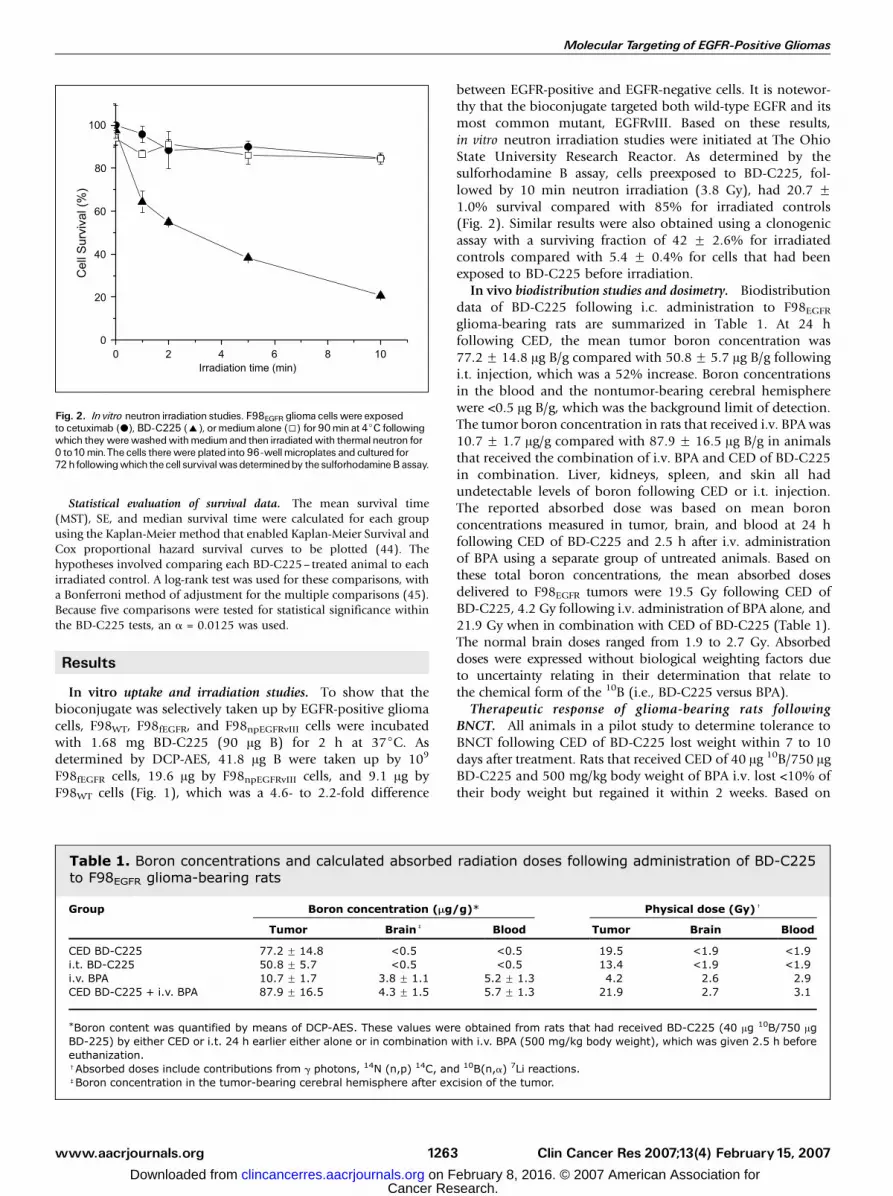
between EGFR-positive and EGFR-negative cells. It is notewor-thy that the bioconjugate targeted both wild-type EGFR and itsmost common mutant, EGFRvIII. Based on these results,in vitro neutron irradiation studies were initiated at The OhioState University Research Reactor. As determined by thesulforhodamine B assay, cells preexposed to BD-C225, fol-lowed by 10 min neutron irradiation (3.8 Gy), had 20.7 F1.0% survival compared with 85% for irradiated controls(Fig. 2). Similar results were also obtained using a clonogenicassay with a surviving fraction of 42 F 2.6% for irradiatedcontrols compared with 5.4 F 0.4% for cells that had beenexposed to BD-C225 before irradiation.
In vivo biodistribution studies and dosimetry. Biodistributiondata of BD-C225 following i.c. administration to F98EGFRglioma-bearing rats are summarized in Table 1. At 24 hfollowing CED, the mean tumor boron concentration was77.2 F 14.8 Ag B/g compared with 50.8 F 5.7 Ag B/g followingi.t. injection, which was a 52% increase. Boron concentrationsin the blood and the nontumor-bearing cerebral hemispherewere <0.5 Ag B/g, which was the background limit of detection.The tumor boron concentration in rats that received i.v. BPA was10.7 F 1.7 Ag/g compared with 87.9 F 16.5 Ag B/g in animalsthat received the combination of i.v. BPA and CED of BD-C225in combination. Liver, kidneys, spleen, and skin all hadundetectable levels of boron following CED or i.t. injection.The reported absorbed dose was based on mean boronconcentrations measured in tumor, brain, and blood at 24 hfollowing CED of BD-C225 and 2.5 h after i.v. administrationof BPA using a separate group of untreated animals. Based onthese total boron concentrations, the mean absorbed dosesdelivered to F98EGFR tumors were 19.5 Gy following CED ofBD-C225, 4.2 Gy following i.v. administration of BPA alone, and21.9 Gy when in combination with CED of BD-C225 (Table 1).The normal brain doses ranged from 1.9 to 2.7 Gy. Absorbeddoses were expressed without biological weighting factors dueto uncertainty relating in their determination that relate tothe chemical form of the 10B (i.e., BD-C225 versus BPA).Therapeutic response of glioma-bearing rats following
BNCT. All animals in a pilot study to determine tolerance toBNCT following CED of BD-C225 lost weight within 7 to 10days after treatment. Rats that received CED of 40 Ag 10B/750 AgBD-C225 and 500 mg/kg body weight of BPA i.v. lost <10% oftheir body weight but regained it within 2 weeks. Based on
Fig. 2. In vitro neutron irradiation studies. F98EGFR glioma cells were exposedto cetuximab (.), BD-C225 (E), ormedium alone (5) for 90min at 4jC followingwhich they werewashedwithmediumand then irradiatedwith thermalneutron for0 to10min.The cells therewere plated into 96-wellmicroplates and cultured for72hfollowingwhich thecell survivalwas determinedby the sulforhodamineBassay.
Table 1. Boron concentrations and calculated absorbed radiation doses following administration of BD-C225to F98EGFR glioma-bearing rats
Group Boron concentration (Mg/g)* Physical dose (Gy)c
Tumor Brainb Blood Tumor Brain Blood
CED BD-C225 77.2 F 14.8 <0.5 <0.5 19.5 <1.9 <1.9i.t. BD-C225 50.8 F 5.7 <0.5 <0.5 13.4 <1.9 <1.9i.v. BPA 10.7 F 1.7 3.8 F 1.1 5.2 F 1.3 4.2 2.6 2.9CED BD-C225 + i.v. BPA 87.9 F 16.5 4.3 F 1.5 5.7 F 1.3 21.9 2.7 3.1
*Boron content was quantified by means of DCP-AES. These values were obtained from rats that had received BD-C225 (40 Ag 10B/750 AgBD-225) by either CED or i.t. 24 h earlier either alone or in combination with i.v. BPA (500 mg/kg body weight), which was given 2.5 h beforeeuthanization.cAbsorbed doses include contributions from g photons, 14N (n,p) 14C, and 10B(n,a) 7Li reactions.bBoron concentration in the tumor-bearing cerebral hemisphere after excision of the tumor.
Molecular Targeting of EGFR-Positive Gliomas
www.aacrjournals.org Clin Cancer Res 2007;13(4) February15, 20071263
Cancer Research. on February 8, 2016. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from
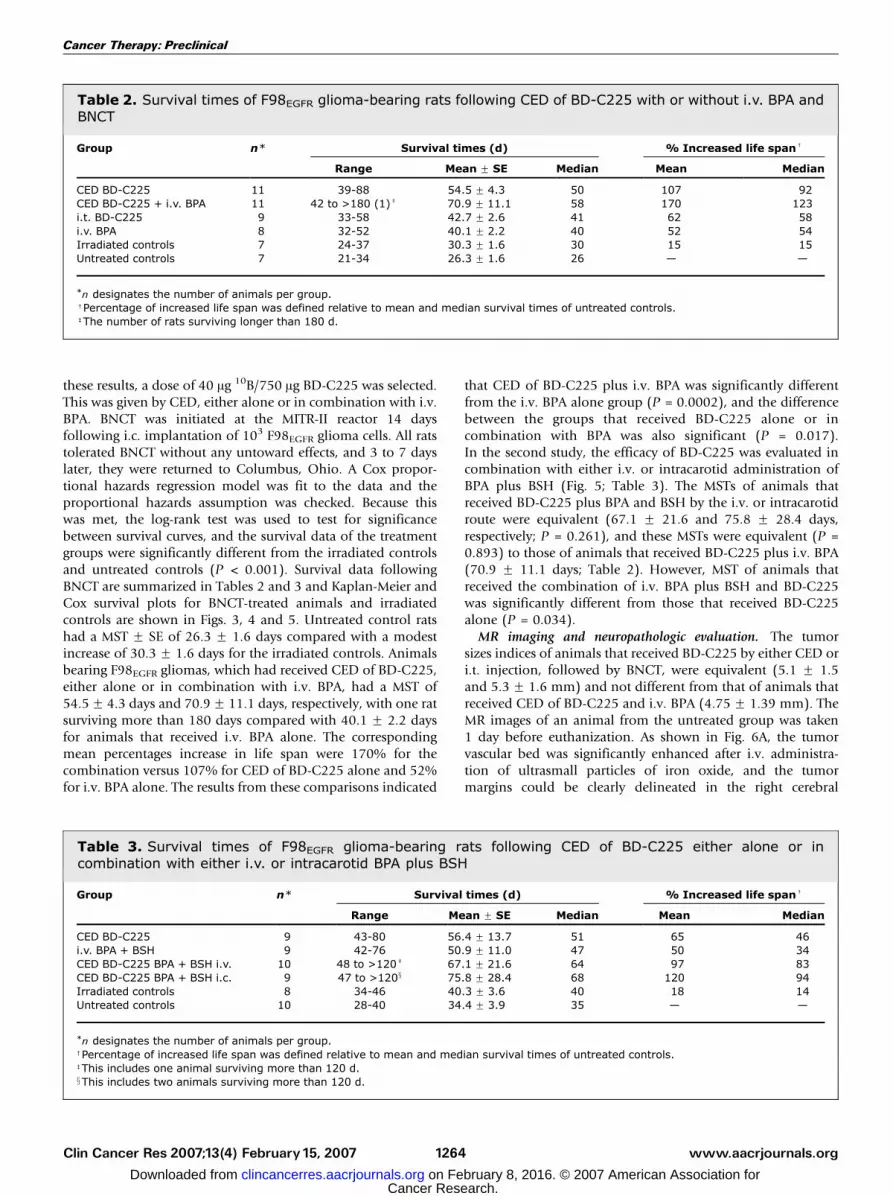
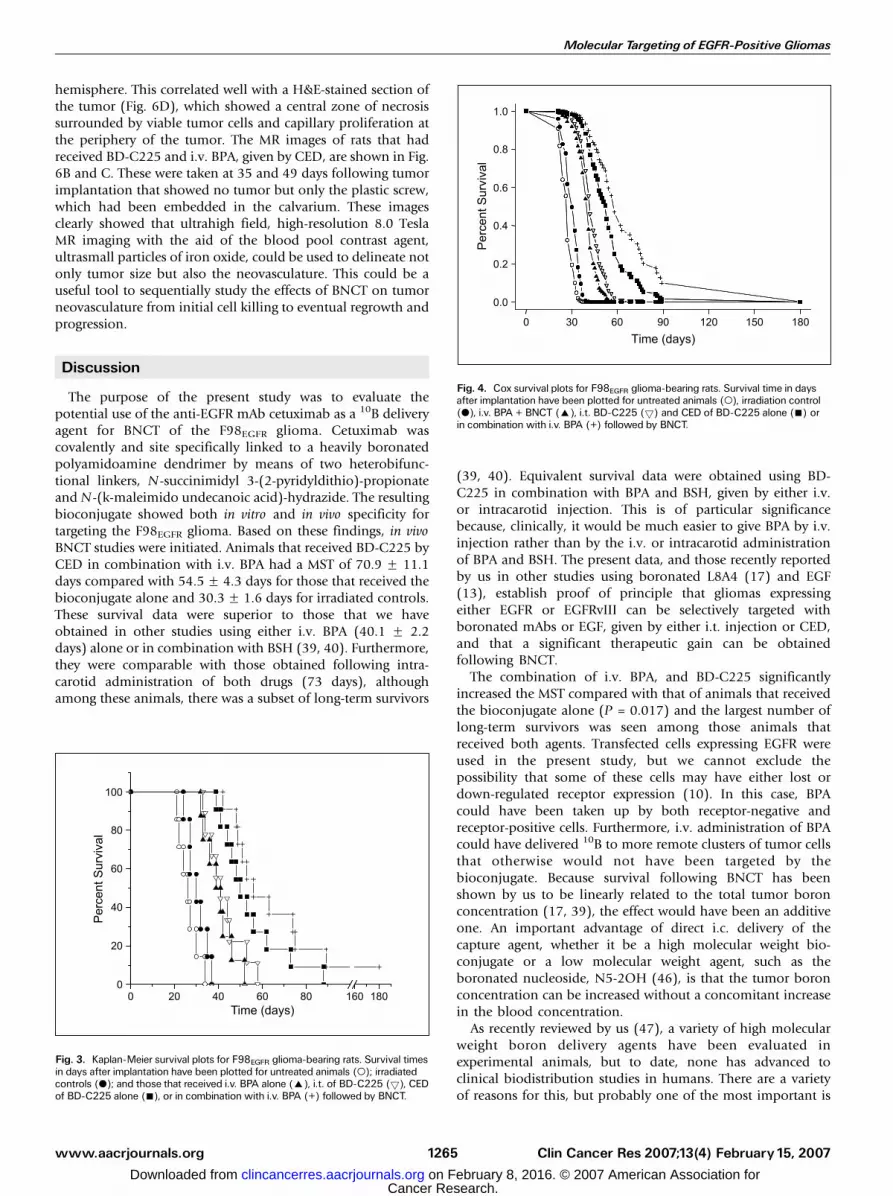
these results, a dose of 40 Ag 10B/750 Ag BD-C225 was selected.This was given by CED, either alone or in combination with i.v.BPA. BNCT was initiated at the MITR-II reactor 14 daysfollowing i.c. implantation of 103 F98EGFR glioma cells. All ratstolerated BNCT without any untoward effects, and 3 to 7 dayslater, they were returned to Columbus, Ohio. A Cox propor-tional hazards regression model was fit to the data and theproportional hazards assumption was checked. Because thiswas met, the log-rank test was used to test for significancebetween survival curves, and the survival data of the treatmentgroups were significantly different from the irradiated controlsand untreated controls (P < 0.001). Survival data followingBNCT are summarized in Tables 2 and 3 and Kaplan-Meier andCox survival plots for BNCT-treated animals and irradiatedcontrols are shown in Figs. 3, 4 and 5. Untreated control ratshad a MST F SE of 26.3 F 1.6 days compared with a modestincrease of 30.3 F 1.6 days for the irradiated controls. Animalsbearing F98EGFR gliomas, which had received CED of BD-C225,either alone or in combination with i.v. BPA, had a MST of54.5F 4.3 days and 70.9F 11.1 days, respectively, with one ratsurviving more than 180 days compared with 40.1 F 2.2 daysfor animals that received i.v. BPA alone. The correspondingmean percentages increase in life span were 170% for thecombination versus 107% for CED of BD-C225 alone and 52%for i.v. BPA alone. The results from these comparisons indicated
that CED of BD-C225 plus i.v. BPA was significantly differentfrom the i.v. BPA alone group (P = 0.0002), and the differencebetween the groups that received BD-C225 alone or incombination with BPA was also significant (P = 0.017).In the second study, the efficacy of BD-C225 was evaluated incombination with either i.v. or intracarotid administration ofBPA plus BSH (Fig. 5; Table 3). The MSTs of animals thatreceived BD-C225 plus BPA and BSH by the i.v. or intracarotidroute were equivalent (67.1 F 21.6 and 75.8 F 28.4 days,respectively; P = 0.261), and these MSTs were equivalent (P =0.893) to those of animals that received BD-C225 plus i.v. BPA(70.9 F 11.1 days; Table 2). However, MST of animals thatreceived the combination of i.v. BPA plus BSH and BD-C225was significantly different from those that received BD-C225alone (P = 0.034).MR imaging and neuropathologic evaluation. The tumor
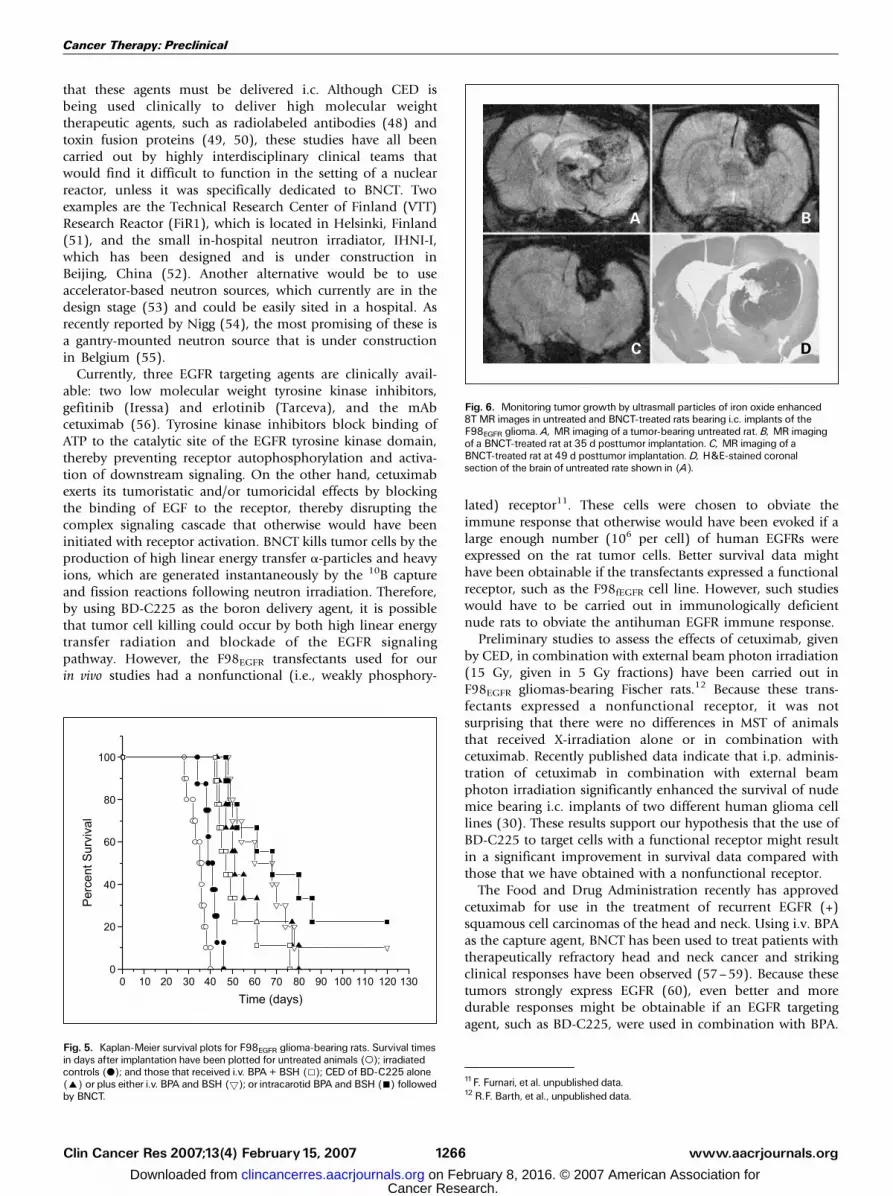
sizes indices of animals that received BD-C225 by either CED ori.t. injection, followed by BNCT, were equivalent (5.1 F 1.5and 5.3 F 1.6 mm) and not different from that of animals thatreceived CED of BD-C225 and i.v. BPA (4.75 F 1.39 mm). TheMR images of an animal from the untreated group was taken1 day before euthanization. As shown in Fig. 6A, the tumorvascular bed was significantly enhanced after i.v. administra-tion of ultrasmall particles of iron oxide, and the tumormargins could be clearly delineated in the right cerebral
Table 2. Survival times of F98EGFR glioma-bearing rats following CED of BD-C225 with or without i.v. BPA andBNCT
Group n* Survival times (d) % Increased life spanc
Range Mean F SE Median Mean Median
CED BD-C225 11 39-88 54.5 F 4.3 50 107 92CED BD-C225 + i.v. BPA 11 42 to >180 (1)b 70.9 F 11.1 58 170 123i.t. BD-C225 9 33-58 42.7 F 2.6 41 62 58i.v. BPA 8 32-52 40.1 F 2.2 40 52 54Irradiated controls 7 24-37 30.3 F 1.6 30 15 15Untreated controls 7 21-34 26.3 F 1.6 26 — —
*n designates the number of animals per group.cPercentage of increased life span was defined relative to mean and median survival times of untreated controls.bThe number of rats surviving longer than 180 d.
Table 3. Survival times of F98EGFR glioma-bearing rats following CED of BD-C225 either alone or incombination with either i.v. or intracarotid BPA plus BSH
Group n* Survival times (d) % Increased life spanc
Range Mean F SE Median Mean Median
CED BD-C225 9 43-80 56.4 F 13.7 51 65 46i.v. BPA + BSH 9 42-76 50.9 F 11.0 47 50 34CED BD-C225 BPA + BSH i.v. 10 48 to >120b 67.1 F 21.6 64 97 83CED BD-C225 BPA + BSH i.c. 9 47 to >120x 75.8 F 28.4 68 120 94Irradiated controls 8 34-46 40.3 F 3.6 40 18 14Untreated controls 10 28-40 34.4 F 3.9 35 — —
*n designates the number of animals per group.cPercentage of increased life span was defined relative to mean and median survival times of untreated controls.bThis includes one animal surviving more than 120 d.xThis includes two animals surviving more than 120 d.
Cancer Therapy: Preclinical
www.aacrjournals.orgClin Cancer Res 2007;13(4) February15, 2007 1264
Cancer Research. on February 8, 2016. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from
hemisphere. This correlated well with a H&E-stained section ofthe tumor (Fig. 6D), which showed a central zone of necrosissurrounded by viable tumor cells and capillary proliferation atthe periphery of the tumor. The MR images of rats that hadreceived BD-C225 and i.v. BPA, given by CED, are shown in Fig.6B and C. These were taken at 35 and 49 days following tumorimplantation that showed no tumor but only the plastic screw,which had been embedded in the calvarium. These imagesclearly showed that ultrahigh field, high-resolution 8.0 TeslaMR imaging with the aid of the blood pool contrast agent,ultrasmall particles of iron oxide, could be used to delineate notonly tumor size but also the neovasculature. This could be auseful tool to sequentially study the effects of BNCT on tumorneovasculature from initial cell killing to eventual regrowth andprogression.
Discussion
The purpose of the present study was to evaluate thepotential use of the anti-EGFR mAb cetuximab as a 10B deliveryagent for BNCT of the F98EGFR glioma. Cetuximab wascovalently and site specifically linked to a heavily boronatedpolyamidoamine dendrimer by means of two heterobifunc-tional linkers, N-succinimidyl 3-(2-pyridyldithio)-propionateand N-(k-maleimido undecanoic acid)-hydrazide. The resultingbioconjugate showed both in vitro and in vivo specificity fortargeting the F98EGFR glioma. Based on these findings, in vivoBNCT studies were initiated. Animals that received BD-C225 byCED in combination with i.v. BPA had a MST of 70.9 F 11.1days compared with 54.5 F 4.3 days for those that received thebioconjugate alone and 30.3 F 1.6 days for irradiated controls.These survival data were superior to those that we haveobtained in other studies using either i.v. BPA (40.1 F 2.2days) alone or in combination with BSH (39, 40). Furthermore,they were comparable with those obtained following intra-carotid administration of both drugs (73 days), althoughamong these animals, there was a subset of long-term survivors
(39, 40). Equivalent survival data were obtained using BD-C225 in combination with BPA and BSH, given by either i.v.or intracarotid injection. This is of particular significancebecause, clinically, it would be much easier to give BPA by i.v.injection rather than by the i.v. or intracarotid administrationof BPA and BSH. The present data, and those recently reportedby us in other studies using boronated L8A4 (17) and EGF(13), establish proof of principle that gliomas expressingeither EGFR or EGFRvIII can be selectively targeted withboronated mAbs or EGF, given by either i.t. injection or CED,and that a significant therapeutic gain can be obtainedfollowing BNCT.The combination of i.v. BPA, and BD-C225 significantly
increased the MST compared with that of animals that receivedthe bioconjugate alone (P = 0.017) and the largest number oflong-term survivors was seen among those animals thatreceived both agents. Transfected cells expressing EGFR wereused in the present study, but we cannot exclude thepossibility that some of these cells may have either lost ordown-regulated receptor expression (10). In this case, BPAcould have been taken up by both receptor-negative andreceptor-positive cells. Furthermore, i.v. administration of BPAcould have delivered 10B to more remote clusters of tumor cellsthat otherwise would not have been targeted by thebioconjugate. Because survival following BNCT has beenshown by us to be linearly related to the total tumor boronconcentration (17, 39), the effect would have been an additiveone. An important advantage of direct i.c. delivery of thecapture agent, whether it be a high molecular weight bio-conjugate or a low molecular weight agent, such as theboronated nucleoside, N5-2OH (46), is that the tumor boronconcentration can be increased without a concomitant increasein the blood concentration.As recently reviewed by us (47), a variety of high molecular
weight boron delivery agents have been evaluated inexperimental animals, but to date, none has advanced toclinical biodistribution studies in humans. There are a varietyof reasons for this, but probably one of the most important is
Fig. 3. Kaplan-Meier survival plots for F98EGFR glioma-bearing rats. Survival timesin days after implantation have been plotted for untreated animals (o); irradiatedcontrols (.); and those that received i.v. BPA alone (E), i.t. of BD-C225 (5), CEDof BD-C225 alone (n), or in combination with i.v. BPA (+) followed by BNCT.
Fig. 4. Cox survival plots for F98EGFR glioma-bearing rats. Survival time in daysafter implantation have been plotted for untreated animals (o), irradiation control(.), i.v. BPA + BNCT (E), i.t. BD-C225 (5) and CED of BD-C225 alone (n) orin combination with i.v. BPA (+) followed by BNCT.
Molecular Targeting of EGFR-Positive Gliomas
www.aacrjournals.org Clin Cancer Res 2007;13(4) February15, 20071265
Cancer Research. on February 8, 2016. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from
that these agents must be delivered i.c. Although CED isbeing used clinically to deliver high molecular weighttherapeutic agents, such as radiolabeled antibodies (48) andtoxin fusion proteins (49, 50), these studies have all beencarried out by highly interdisciplinary clinical teams thatwould find it difficult to function in the setting of a nuclearreactor, unless it was specifically dedicated to BNCT. Twoexamples are the Technical Research Center of Finland (VTT)Research Reactor (FiR1), which is located in Helsinki, Finland(51), and the small in-hospital neutron irradiator, IHNI-I,which has been designed and is under construction inBeijing, China (52). Another alternative would be to useaccelerator-based neutron sources, which currently are in thedesign stage (53) and could be easily sited in a hospital. Asrecently reported by Nigg (54), the most promising of these isa gantry-mounted neutron source that is under constructionin Belgium (55).Currently, three EGFR targeting agents are clinically avail-
able: two low molecular weight tyrosine kinase inhibitors,gefitinib (Iressa) and erlotinib (Tarceva), and the mAbcetuximab (56). Tyrosine kinase inhibitors block binding ofATP to the catalytic site of the EGFR tyrosine kinase domain,thereby preventing receptor autophosphorylation and activa-tion of downstream signaling. On the other hand, cetuximabexerts its tumoristatic and/or tumoricidal effects by blockingthe binding of EGF to the receptor, thereby disrupting thecomplex signaling cascade that otherwise would have beeninitiated with receptor activation. BNCT kills tumor cells by theproduction of high linear energy transfer a-particles and heavyions, which are generated instantaneously by the 10B captureand fission reactions following neutron irradiation. Therefore,by using BD-C225 as the boron delivery agent, it is possiblethat tumor cell killing could occur by both high linear energytransfer radiation and blockade of the EGFR signalingpathway. However, the F98EGFR transfectants used for ourin vivo studies had a nonfunctional (i.e., weakly phosphory-
lated) receptor11. These cells were chosen to obviate theimmune response that otherwise would have been evoked if alarge enough number (106 per cell) of human EGFRs wereexpressed on the rat tumor cells. Better survival data mighthave been obtainable if the transfectants expressed a functionalreceptor, such as the F98fEGFR cell line. However, such studieswould have to be carried out in immunologically deficientnude rats to obviate the antihuman EGFR immune response.Preliminary studies to assess the effects of cetuximab, given
by CED, in combination with external beam photon irradiation(15 Gy, given in 5 Gy fractions) have been carried out inF98EGFR gliomas-bearing Fischer rats.12 Because these trans-fectants expressed a nonfunctional receptor, it was notsurprising that there were no differences in MST of animalsthat received X-irradiation alone or in combination withcetuximab. Recently published data indicate that i.p. adminis-tration of cetuximab in combination with external beamphoton irradiation significantly enhanced the survival of nudemice bearing i.c. implants of two different human glioma celllines (30). These results support our hypothesis that the use ofBD-C225 to target cells with a functional receptor might resultin a significant improvement in survival data compared withthose that we have obtained with a nonfunctional receptor.The Food and Drug Administration recently has approved
cetuximab for use in the treatment of recurrent EGFR (+)squamous cell carcinomas of the head and neck. Using i.v. BPAas the capture agent, BNCT has been used to treat patients withtherapeutically refractory head and neck cancer and strikingclinical responses have been observed (57–59). Because thesetumors strongly express EGFR (60), even better and moredurable responses might be obtainable if an EGFR targetingagent, such as BD-C225, were used in combination with BPA.
11F. Furnari, et al. unpublished data.12 R.F. Barth, et al., unpublished data.
Fig. 6. Monitoring tumor growth by ultrasmall particles of iron oxide enhanced8TMR images in untreated and BNCT-treated rats bearing i.c. implants of theF98EGFR glioma. A, MR imaging of a tumor-bearing untreated rat. B, MR imagingof a BNCT-treated rat at 35 d posttumor implantation. C, MR imaging of aBNCT-treated rat at 49 d posttumor implantation. D, H&E-stained coronalsection of the brain of untreated rate shown in (A).
Fig. 5. Kaplan-Meier survival plots for F98EGFR glioma-bearing rats. Survival timesin days after implantation have been plotted for untreated animals (o); irradiatedcontrols (.); and those that received i.v. BPA + BSH (5); CED of BD-C225 alone(E) or plus either i.v. BPA and BSH (5); or intracarotid BPA and BSH (n) followedby BNCT.
Cancer Therapy: Preclinical
www.aacrjournals.orgClin Cancer Res 2007;13(4) February15, 2007 1266
Cancer Research. on February 8, 2016. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from

Based on all of our published data, which have shownequivalent efficacy for boronated EGF, L8A4, and cetuximab,however, we have concluded that the latter would be the bestchoice for boron delivery because it is the only agent that has
been approved for clinical use (61). Conceivably, BD-C225could be moved into clinical biodistribution studies within ashort period time, if those clinicians who are treating patientswith EGFR-positive tumors with BNCT were so inclined.
References1. Barth RF, Coderre JA, Vicente MG, Blue TE. Boronneutron capture therapy of cancer: current statusand future prospects. Clin Cancer Res 2005;11:3987^4002.
2. Zamenhof RG, Coderre JA, Rivard MJ, Patel H.Topics in neutron capture therapy. Proceedings of theEleventhWorld Congress on Neutron Capture Thera-py. Appl Radiat Isot 2004;61:731^1130.
3. Barth RF, editor. A critical assessment of boron neu-tron capture therapy. JNeurooncol 2003;62:1^210.
4.Vicente MGH, editor. Boron in medicinal chemistry.Anti-CancerAgents Med Chem 2006;6:73^181.
5. NakagawaY, KobayashiT, Fukuda H, editors. Advan-ces in Neutron Capture Therapy. Proceedings 12th In-ternational Congress on Neutron Capture Therapy,Takamatsu, Japan. October 9^12. 2006.
6. Bigner SH, Humphrey PA,Wong AJ, et al. Character-ization of the epidermal growth factor receptor in hu-man glioma cell lines and xenografts. Cancer Res1990;50:8017^22.
7. SauterG,Maeda T, WaldmanFM,DavisRL,FeuersteinBG. Patterns of epidermal growth factor receptor am-plification inmalignant gliomas.AmJPathol1996;148:1047^53.
8. Schwechheimer K, Huang S, Cavenee WK. EGFRgene amplification-rearrangement in human glioblas-tomas. Int JCancer 1995;62:145^8.
9. Frederick L,Wang XY, Eley G, James CD. Diversityand frequency of epidermal growth factor receptormutations in human glioblastomas. Cancer Res 2000;60:1383^7.
10. Mendelsohn J, Baselga J. Epidermal growth factorreceptor targeting in cancer. Semin Oncol 2006;33:369^85.
11. Barth RF,YangW, Adams DM, et al. Molecular tar-geting of the epidermal growth factor receptor forneutron capture therapy of gliomas. Cancer Res2002;62:3159^66.
12. YangW, Barth RF, Adams DM, et al. Convection-enhanced delivery of boronated epidermal growthfactor for molecular targeting of EGF receptor-positivegliomas. Cancer Res 2002;62:6552^8.
13.YangW, Barth RF,Wu G, et al. Boronated epidermalgrowth factor as a delivery agent for neutron capturetherapy of EGF receptor positive gliomas. Appl RadiatIsot 2004;61:981^5.
14.Wu G, Barth RF, Yang W, et al. Site-specific conju-gation of boron-containing dendrimers to anti-EGFreceptor monoclonal antibody cetuximab (IMC-C225) and its evaluation as a potential delivery agentfor neutron capture therapy. Bioconjug Chem 2004;15:185^94.
15. Barth RF,Wu G,YangW, et al. Neutron capture ther-apy of epidermal growth factor (+) gliomas usingboronated cetuximab (IMC-C225) as a deliveryagent. Appl Radiat Isot 2004;61:899^903.
16. Yang W, Barth RF, Wu G, et al. Development of asyngeneic rat brain tumor model expressing EGFRvIIIand its use for molecular targeting studies withmonoclonal antibody L8A4. Clin Cancer Res 2005;11:341^50.
17. YangW, Barth RF,Wu G, et al. Molecular targetingand treatment of EGFRvIII-positive gliomas usingboronated monoclonal antibody L8A4. Clin CancerRes 2006;12:3792^802.
18. Goldstein NI, Prewett M, Zuklys K, Rockwell P,Mendelsohn J. Biological efficacy of a chimeric anti-body to the epidermal growth factor receptor in a hu-man tumor xenograft model. Clin Cancer Res 1995;1:1311^8.
19. Sato JD, Kawamoto T, Le AD, et al. Biologicaleffects in vitro of monoclonal antibodies to human
epidermal growth factor receptors. Mol Biol Med1983;1:511^29.
20.Gill GN, KawamotoT, Cochet C, et al. Monoclonalanti-epidermal growth factor receptor antibodieswhich are inhibitors of epidermal growth factorbinding and antagonists of epidermal growth factorstimulated tyrosine protein kinase activity. J BiolChem 1984;259:7755^60.
21. Mendelsohn J, Baselga J. Status of epidermalgrowth factor receptor antagonists in the biology andtreatment of cancer. JClin Oncol 2003;21:2787^99.
22. Castillo L, Etienne-Grimaldi MC, Fischel JL, et al.Pharmacological background of EGFR targeting. AnnOncol 2004;15:1007^12.
23. Sartor CI. Mechanisms of disease: radiosensitiza-tion by epidermal growth factor receptor inhibitors.Nat Clin Pract Oncol 2004;1:80^7.
24. Kiyota A, Shintani S,MiharaM, et al. Anti-epidermalgrowth factor receptor monoclonal antibody 225upregulates p27(KIP1) and p15(INK4B) and inducesG1arrest in oral squamous carcinoma cell lines.Oncol-ogy 2002;63:92^8.
25.Wu X, Fan Z, Masui H, Rosen N,MendelsohnJ. Ap-optosis induced by an anti-epidermal growth factorreceptor monoclonal antibody in a human colorectalcarcinoma cell line and its delay by insulin. JClin Invest1995;95:1897^905.
26. Huang SM, Harari PM. Modulation of radiation re-sponse after epidermal growth factor receptor block-ade in squamous cell carcinomas : inhibition ofdamage repair, cell cycle kinetics, and tumor angio-genesis. Clin Cancer Res 2000;6:2166^74.
27. Perrotte P, MatsumotoT, Inoue K, et al. Anti-epider-mal growth factor receptor antibody C225 inhibits an-giogenesis in human transitional cell carcinomagrowing orthotopically in nude mice. Clin Cancer Res1999;5:257^65.
28. Huang SM, Li J, Harari PM. Molecular inhibition ofangiogenesis and metastatic potential in humansquamous cell carcinomas after epidermal growthfactor receptor blockade. Mol Cancer Ther 2002;1:507^14.
29. Sung FL, PoonTC, Hui EP, et al. Antitumor effectand enhancement of cytotoxic drug activity by cetux-imab innasopharyngeal carcinoma cells. InVivo 2005;19:237^45.
30. Eller JL, Longo SL, Kyle MM, et al. Anti-epidermalgrowth factor receptor monoclonal antibody cetuxi-mab augments radiation effects in glioblastoma mul-tiforme in vitro and in vivo. Neurosurgery 2005;56:155^62.
31. Harding J, Burtness B. Cetuximab: an epidermalgrowth factor receptor chemeric human-murinemonoclonal antibody. DrugsToday (Barc) 2005;41:107^27.
32. Barth RF, Adams DM, SolowayAH, et al. Determi-nation of boron in tissues and cells using direct-current plasma atomic emission spectroscopy. AnalChem1991;63:890^3.
33. Papazisis KT, Geromichalos GD, Dimitriadis KA,KortsarisAH.Optimizationof thesulforhodamineBcol-orimetric assay. JImmunolMethods1997;208:151^8.
34. Pauwels B, Korst AE, de Pooter CM, et al. Compar-ison of the sulforhodamine B assay and the clono-genic assay for in vitro chemoradiation studies.Cancer Chemother Pharmacol 2003;51:221^6.
35. Barth RF. Rat brain tumor models in experimentalneuro-oncology: the 9L, C6, T9, F98, RG2 (D74),RT-2, and CNS-1 gliomas. J Neurooncol 1998;36:91^102.
36. YangW, Barth RF, Carpenter DE, MoeschbergerML, Goodman JH. Enhanced delivery of boronophe-
nylalanine for neutron capture therapy by means ofintracarotid injection and blood-brain barrier disrup-tion. Neurosurgery1996;38:985^92.
37. Morrison PF, Laske DW, Bobo H, Oldfield EH,Dedrick RL. High-flow microinfusion: tissue penetra-tion and pharmacodynamics. AmJPhysiol 1994;266:R292^305.
38. Laske DW, Morrison PF, Lieberman DM, et al.Chronic interstitial infusion of protein to primate brain:determination of drug distribution and clearance withsingle-photon emission computerized tomographyimaging. JNeurosurg1997;87:586^94.
39.BarthRF,YangW,RotaruJH,etal.Boronneutroncap-ture therapyof brain tumors: enhanced survival follow-ing intracarotid injection of either sodium borocaptateor boronophenylalanine with or without blood-brainbarrierdisruption.CancerRes1997;57:1129^36.
40. Barth RF,YangW, Rotaru JH, et al. Boron neutroncapture therapy of brain tumors: enhanced survivaland cure following blood-brain barrier disruption andintracarotid injectionof sodiumborocaptate andboro-nophenylalanine. Int J Radiat Oncol Biol Phys 2000;47:209^18.
41. Harling OK, Riley KJ, Binns PJ, Patel H, Coderre JA.The MITuser center for neutron capture therapy re-search. Radiat Res 2005;164:221^9.
42. Harling OK, Riley KJ. Fission reactor neutron sour-ces for neutron capture therapy-a critical review.JNeurooncol 2003;62:7^17.
43. Rogus RD, Harling OK,Yanch JC. Mixed field do-simetry of epithermal neutron beams for boron neu-tron capture therapy at the MITR-II research reactor.Med Phys1994;21:1611^25.
44. KleinJP,MoeschbergerML. Survival analysis: tech-niques for censored and truncated data. 2nd ed. NewYork (NY): Springer; 2003.
45. Madsen RW, Moeschberger ML. Statistical con-cepts. Englewood Cliffs (NJ): Prentice-Hall; 1986.
46. Barth RF,YangW, Al-Madhoun AS, et al. Boron-containing nucleosides as potential delivery agentsfor neutron capture therapy of brain tumors. CancerRes 2004;64:6287^95.
47.Wu G, Barth RF, Yang W, et al. Boron containingmacromolecules and nanovehicles as delivery agentsfor neutron capture therapy. Anti-CancerAgents MedChem 2006;6:167^84.
48. Reardon DA, Akabani G, Coleman RE, et al. Salvageradioimmunotherapy with murine iodine-131-labeledantitenascinmonoclonalantibody81C6 forpatientswithrecurrentprimaryandmetastaticmalignantbraintumors:phase IIstudy results. JClinOncol2006;24:115^22.
49. Laske DW,Youle RJ, Oldfield EH. Tumor regressionwith regional distribution of the targeted toxin TF-CRM107 in patients with malignant brain tumors. NatMed1997;3:1362^8.
50. Parney IF, Kunwar S, McDermott M, et al. Neurora-diographic changes following convection-enhanceddelivery of the recombinant cytotoxin interleukin 13-PE38QQR for recurrent malignant glioma. J Neuro-surg 2005;102:267^75.
51. Joensuu H, Kankaanranta L, Seppa« la« T, et al. Boronneutron capture therapy of brain tumors: clinical trialsat the Finnish facility using boronophenylalanine.JNeurooncol 2003;62:123^34.
52. Zhou Y, Gao Z, Li Y, Guo C, Liu X. Design andconstruction of the in-hospital neutron irradiator-1<IHNI-I>. In: Nakagawa Y, Kobayashi T, Fukuda H,editors. Advances in Neutron CaptureTherapy 2006.Proceedings 12th International Congress on NeutronCapture Therapy; 2006 October 9 ^ 12; Takamatsu,Japan. pp. 557^560.
53. Blue TE, Yanch JC. Accelerator-based epithermal
Molecular Targeting of EGFR-Positive Gliomas
www.aacrjournals.org Clin Cancer Res 2007;13(4) February15, 20071267
Cancer Research. on February 8, 2016. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from

neutron sources for boron neutron capture therapy ofbrain tumors. JNeurooncol 2003;62:19^31.
54. NiggD.Neutron sources andapplications in radiothe-rapyQabriefhistory, andcurrent trends. In:NakagawaY,Kobayashi T, Fukuda H, editors. Advances In NeutronCaptureTherapy 2006. Proceedings 12th InternationalCongress on Neutron CaptureTherapy; 2006 October9^12;Takamatsu, Japan.
55. Stichelbaut F, Forton E, JongenY. Design of a beamshaping assembly for an accelerator-based BNCT sys-tem. In: NakagawaY, Kobayashi T, Fukuda H, editors.Advances In Neutron Capture Therapy 2006. Pro-
ceedings 12th International Congress on NeutronCapture Therapy; 2006 October 9 ^12; Takamatsu,Japan. pp. 308^311.
56. Ciardiello F. Epidermal growth factor receptor inhibi-tors incancer treatment. FutureOncol 2005;1:221^34.
57.Obayashi S, Kato I, Ono K, et al. Delivery of10boronto oral squamous cell carcinoma using boronopheny-lalanine and borocaptate sodium for boron neutroncapture therapy. Oral Oncol 2004;40:474^82.
58. Kato I, Ono K, Sakurai Y, et al. Effectiveness ofBNCT for recurrent head and neck malignancies. ApplRadiat Isot 2004;61:1069^73.
59. Kato I, Ono K, Sakurai F. Boron neutron capturetherapy for recurrent head and neck malignancies. In:Nakagawa,Y, Kobayashi T, Fukuda H, editors. Advan-ces in Neutron CaptureTherapy 2006. 12th Interna-tional Congress on Neutron CaptureTherapy; 2006October 9^12,Takamatsu, Japan. pp.1^4.
60. Ford AC, Grandis JR. Targeting epidermal growthfactor receptor in head and neck cancer. Head Neck2003;25:67^73.
61. Frieze DA, McCuneJS. Current status of cetuximabfor the treatment of patients with solid tumors. AnnPharmacother 2006;40:241^50.
Cancer Therapy: Preclinical
www.aacrjournals.orgClin Cancer Res 2007;13(4) February15, 2007 1268
Cancer Research. on February 8, 2016. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from
2007;13:1260-1268. Clin Cancer Res Gong Wu, Weilian Yang, Rolf F. Barth, et al. Cetuximab
Positive Glioma Using Boronated−Factor Receptor Molecular Targeting and Treatment of an Epidermal Growth
Updated version
http://clincancerres.aacrjournals.org/content/13/4/1260
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/13/4/1260.full.html#ref-list-1
This article cites 51 articles, 18 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/13/4/1260.full.html#related-urls
This article has been cited by 4 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
To request permission to re-use all or part of this article, contact the AACR Publications
Cancer Research. on February 8, 2016. © 2007 American Association forclincancerres.aacrjournals.org Downloaded from




















