
Gentamicin-eluting bioresorbable composite fibers for wound healing applications
Upload
independentCategory
view
2download
0
142
TCM Vol. 13, No. 4, 2003
Molecular Mechanisms of In-Stent Restenosis and Approach to Therapy with Eluting Stents
Ciro Indolfi,* Annalisa Mongiardo, Antonio Curcio, and Daniele Torella
Restenosis is the principal drawback of percutaneous coronary proce-dures. Until now, the only widely accepted way to reduce restenosis ratehas been the stent. However, clinical restenosis still represents themajor limitation of this technology. This article summarizes recentlaboratory and clinical investigations concerning the mechanismsresponsible for the transmission of mitogenic signals from plasmamembrane to the nucleus in vascular smooth muscle cells that deter-mine neointima formation after stent deployment. Recent experimentaldata on the impact of diabetes and physical exercise on restenosis alsois reviewed. Finally, the new concept of local drugs that elute directly tothe site of vascular injury from coated stents and the available clinicalresults obtained with rapamycin or paclitaxel-eluting stents are discussed.
(Trends Cardiovasc Med 2003;13:142–148)
© 2003, Elsevier Inc.
restenosis still represents the major lim-itation for the widespread use of this de-vice, especially when the stent is em-ployed in complex stenoses. Therefore,the problem of in-stent restenosis (ISR)is becoming at least as important as res-tenosis after percutaneous transluminalcoronary angioplasty (PTCA).
The goal of this review is to summa-rize recent laboratory investigations onthe molecular mechanisms responsiblefor the transmission of mitogenic signalsfrom plasma membrane to the nucleusin vascular smooth muscle cells (VSMCs)that determine neointima formation afterstent deployment. The approaches to in-hibit VSMC proliferation in vivo are dis-cussed, and particular emphasis is placedon the eluting stents—the new break-through device for ISR prevention.
• Mechanisms of Restenosis after Balloon Angioplasty and Stenting
Restenosis is considered a local vascularmanifestation of the general biologic re-sponse to injury (Indolfi et al. 1999). Post-balloon angioplasty (PTCA) restenosis is
thought to involve primarily negative re-modeling and, partially, neointima hyper-plasia (Indolfi et al. 2002b). Histologi-cally, however, ISR is quite distinct fromrestenosis after PTCA (Figure 1). In fact,intravascular ultrasound (IVUS) studiessuggest that coronary stents provide me-chanical scaffolding that virtually elimi-nates long-term negative remodeling andthat ISR is largely a result of VSMC pro-liferation, which is exaggerated after stentdeployment due to the high-pressuretechnique of stent deployment (Farb et al.1999, Indolfi et al. 1995b and 2000c).
A commonly accepted model of theresponse to arterial injury suggests thatgrowth factors are released after injury,thereby changing the composition ofthe extracellular matrix and triggering aproliferation and migration program.VSMCs undergo a phenotypic modula-tion from a contractile to a syntheticphenotype (dedifferentiation), prolifer-ate into the media, migrate from themedia into the intima, and subsequentlyform the neointima. Moreover, it has beenshown that bone marrow cells give riseto the part of the VSMCs that contributeto arterial remodeling after vascular in-jury (Sata et al. 2002). These data, how-ever, have been challenged by the recentfindings of Hu et al. (2002) who werenot able to confirm the invasion of bonemarrow-derived cells into the intima ofatherosclerotic vein grafts. Nevertheless,wherever they originate, VSMCs that formthe neointima tissue remain the maintarget if restenosis is to be challenged.
• VSMC Intracellular Signaling After Vascular Injury
In the past few years, many investigatorshave focused their attention on the rela-tive importance of single receptors inthe complex mechanism of VSMC growthcontrol after vascular injury (Indolfi et al.1999). However, it is unlikely that the in-hibition of only a single receptor wouldbe clinically relevant to the preventionof ISR. Therefore, in the last few years,we have studied mainly the commonpathways that multiple receptors em-ploy to transmit mitogenic signals fromthe membrane to the nucleus in VSMCsafter arterial injury; in particular, the roleof the
ras
-
raf
-mitogen-activated proteinkinases (MAPK) pathway and the cyclicadenosine monophosphate (cAMP)-dependent signaling in activated VSMCs(Figure 2) (Indolfi et al. 1996 and 1999).
Ciro Indolfi, Annalisa Mongiardo, and AntonioCurcio are at the Division of Cardiology,Magna Græcia University, Catanzaro, Italy.Daniele Torella is at the Division of Cardiol-ogy, Federico II University, Naples, Italy.
* Address correspondence to: Ciro Indolfi,MD, FACC, FESC, Head, Division of Cardiol-ogy, Magna Graecia University, Via TommasoCampanella, 115, Catanzaro 88100, Italy. Tel.:(
�
011) 39-0961-712310; fax: (
�
011) 39-0961-712310; e-mail: [email protected].
© 2003, Elsevier Inc. All rights reserved.1050-1738/03/$-see front matter
Restenosis, which is defined as “the arte-rial healing response after injury incurredduring transluminal coronary revascu-larization,” has been the principal draw-back of percutaneous coronary interven-tions (PCI) since their introduction nearly25 years ago (Al Suwaidi et al. 2000).The only widely accepted way to reducerestenosis rate has been the use of coro-nary stents, and the last years have seena prompt and widespread adoption ofcoronary stents that have revolutionizedthe field of interventional cardiology (AlSuwaidi et al. 2000). However, clinical
TCM Vol. 13, No. 4, 2003
143
The
ras-raf
-MAPKs Signaling of Smooth Muscle Cells After Vascular Injury
Ras
proteins are key transducers of mi-togenic signals from plasma membraneto the nucleus in many cell types. Sev-eral mutants of
ras
(such as N17 H-
ras
and L61,S186 H-
ras
) act in a dominantnegative manner to block normal
ras
ac-tivation (Indolfi et al. 1999). N17 H-
ras
has reduced affinity for guanosine triphos-phate (GTP) and is defective in the finalstep of the exchange process, displace-ment of guanine-exchange factor (GEF)by GTP, and sequestering of GEFs intodead-end complexes (Indolfi et al. 1999).This mutant has been used to removeGEF activity from cells so that activa-tion of endogenous
ras
proteins cannotoccur. We (Indolfi et al. 1995a) investi-gated the role of
ras
proteins in the vas-cular response to arterial injury in vivoby inactivating cellular
ras
function inrats in which the common carotid arterywas subjected to balloon injury. In ani-mals treated with Nl7 H-
ras
, a signifi-cant reduction of neointima formation(
�
55%) was observed 14 days afterballoon injury compared with animals
treated with RSV-IacZ (Indolfi 1995a). Asimilar effect on neointima formationafter vascular injury was observed withthe inhibition of MAPKK by a domi-nant inhibitor mutant gene (Indolfi etal. 1997b).
Activation of cAMP–Protein Kinase A Signaling Inhibits Neointima Formation After Balloon Injury
cAMP is involved in the regulation of avariety of cellular functions, such as cellproliferation and differentiation. Hor-
mone-activated receptors increase theintracellular cAMP by inactivating the
�
subunit of the trimeric G-protein com-plex (G
�
s), which stimulates adenylatecyclase (Figure 2). To evaluate the ef-fects of cAMP on VSMC proliferation,we (Indolfi et al. 1997a) treated culturesof these cells in vitro with different con-centrations of 8-Br-cAMP and analyzedcell growth at different treatment peri-ods. cAMP markedly inhibited VSMCproliferation. We next sought to deter-mine whether cAMP was able to inhibitVSMC proliferation in vivo by balloon-
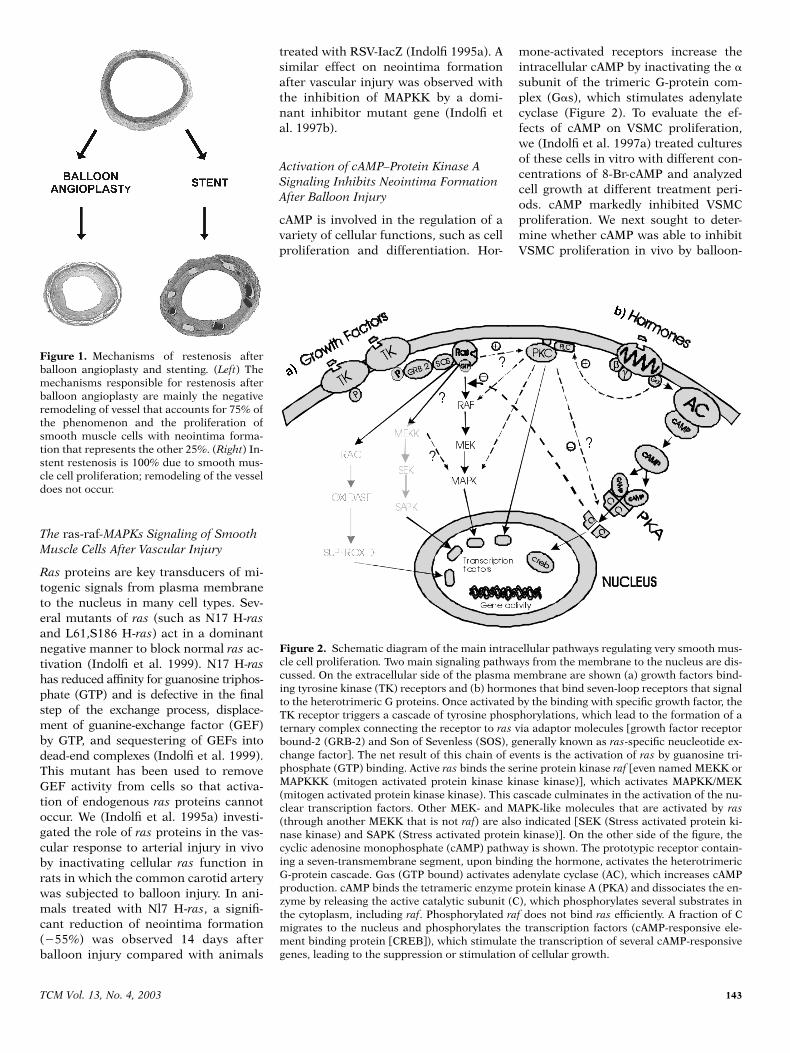
Figure 1. Mechanisms of restenosis afterballoon angioplasty and stenting. (Left) Themechanisms responsible for restenosis afterballoon angioplasty are mainly the negativeremodeling of vessel that accounts for 75% ofthe phenomenon and the proliferation ofsmooth muscle cells with neointima forma-tion that represents the other 25%. (Right) In-stent restenosis is 100% due to smooth mus-cle cell proliferation; remodeling of the vesseldoes not occur.
Figure 2. Schematic diagram of the main intracellular pathways regulating very smooth mus-cle cell proliferation. Two main signaling pathways from the membrane to the nucleus are dis-cussed. On the extracellular side of the plasma membrane are shown (a) growth factors bind-ing tyrosine kinase (TK) receptors and (b) hormones that bind seven-loop receptors that signalto the heterotrimeric G proteins. Once activated by the binding with specific growth factor, theTK receptor triggers a cascade of tyrosine phosphorylations, which lead to the formation of aternary complex connecting the receptor to ras via adaptor molecules [growth factor receptorbound-2 (GRB-2) and Son of Sevenless (SOS), generally known as ras-specific neucleotide ex-change factor]. The net result of this chain of events is the activation of ras by guanosine tri-phosphate (GTP) binding. Active ras binds the serine protein kinase raf [even named MEKK orMAPKKK (mitogen activated protein kinase kinase kinase)], which activates MAPKK/MEK(mitogen activated protein kinase kinase). This cascade culminates in the activation of the nu-clear transcription factors. Other MEK- and MAPK-like molecules that are activated by ras(through another MEKK that is not raf) are also indicated [SEK (Stress activated protein ki-nase kinase) and SAPK (Stress activated protein kinase)]. On the other side of the figure, thecyclic adenosine monophosphate (cAMP) pathway is shown. The prototypic receptor contain-ing a seven-transmembrane segment, upon binding the hormone, activates the heterotrimericG-protein cascade. G�s (GTP bound) activates adenylate cyclase (AC), which increases cAMPproduction. cAMP binds the tetrameric enzyme protein kinase A (PKA) and dissociates the en-zyme by releasing the active catalytic subunit (C), which phosphorylates several substrates inthe cytoplasm, including raf. Phosphorylated raf does not bind ras efficiently. A fraction of Cmigrates to the nucleus and phosphorylates the transcription factors (cAMP-responsive ele-ment binding protein [CREB]), which stimulate the transcription of several cAMP-responsivegenes, leading to the suppression or stimulation of cellular growth.

144
TCM Vol. 13, No. 4, 2003
injuring rat carotid arteries. At the timeof balloon injury, we locally delivered 8-Br-cAMP. In the 8-Br-cAMP group, a sig-nificant reduction of neointima (
�
54%)was observed 14 days after vascular in-jury compared with the control group(Indolfi et al. 1997a). An inhibition ofneointimal formation after vascular in-jury also was observed in other experi-ments (Indolfi et al. 2000b), in whichsystemic administration of 8-Cl-cAMPreduced protein kinase A (PKA) RI
�
-subunit expression and upregulated PKARII
�
-subunit expression.
Cyclin-Dependent Kinase Complexes
The cell cycle is a key regulator of thedescribed intracellular signals and hasdirect effects on multiple cell processes,including VSMC proliferation and cellmigration (Boehm and Nabel 2001).VSMCs within the media of adult arter-ies normally are quiescent, proliferate atlow rates, and exist in the G0 phase ofthe cell cycle. Upon stimulation bygrowth factors or after arterial injury,VSMCs exit the quiescent stage G0 andprogress through the G1 and G1/S tran-sition of the cell cycle. G1 progression isregulated by the assembly and phos-phorylation of G1 cyclin–cyclin-depen-dent kinase (CDK) complexes, predomi-nantly cyclin D–CDK and cyclin E–CDK-2 in VSMCs (Nabel 2002). Endogenousinhibitors of the cyclin–CDK complexesare termed the CDK inhibitors (CKIs).Two groups of CKIs are dominant incardiovascular biology: the CDK inhibi-tor protein (CIP/KIP) family, which in-cludes p21
Cip1
and p27
Kip1
; and the INK4family, which includes p16
Ink4a
(Nabel2002, Tanner et al. 1998).
Cells in the late S or G2/M phase donot migrate. There is a window of op-portunity in the G1 to G1/S transitionduring which VSMCs are able to mi-grate in response to mitogenic stimuli.Therefore, proteins such as the CKIsthat regulate G1 cell cycle progressionare likely candidates to regulate the ini-tiation of migration as well. p27
Kip1
isone important candidate, given that itis tightly regulated by mitogens. Theprotein p27
Kip1
is an important regula-tor of the mammalian cell cycle (Nabel2002). An increase in p27
Kip1
causesproliferating cells to exit from the cellcycle, whereas a decrease in p27
Kip1
isrequired for quiescent cells to resume
cell division (Boehm et al. 2002). Lowlevels of p27
Kip1
are associated with ex-cessive cell proliferation in pathologicconditions such as inflammation andrestenosis (Ophascharoensuk et al. 1998,Tanner et al. 1998). High levels ofp27
Kip1
are observed in conditions of di-minished cell proliferation, such as inthe late stages of arterial wound repair inatherosclerosis and restenosis (Tanneret al. 1998, 2000). Notably, we (Indolfi etal. 2001a) demonstrated that A-kinaseanchor protein (AKAP), downstreammolecules of the cAMP–PKA cascade, in-hibiting VSMC proliferation in vivo
byincreasing p27
Kip1
protein levels.
• Inflammation and Restenosis
An increasing body of evidence suggeststhat inflammation plays a pivotal role inlinking early vascular injury to the detri-mental consequence of neointimal growthand lumen shrinkage (Welt and Rogers2002). In this regard, the widespread useof coronary stents has altered fundamen-tally the vascular response to injury bycausing a more intense and prolonged in-flammatory state (Welt and Rogers 2002).Indeed, the initial events immediatelyafter stent placement result in endothe-lium damage and the deposition of alayer of platelets and fibrin at the in-jured site (Indolfi et al. 2000c). Activatedplatelets express adhesion molecules,which attach to circulating leukocytesvia platelet receptors and begin a pro-cess of rolling along the injured surface(Welt and Rogers 2002). The migrationof leukocytes across the platelet-fibrinlayer and into the tissue is driven bychemical gradients of cytokines releasedfrom VSMCs and resident leukocytes.Growth factors are released from platelets,leukocytes, and VSMCs, which influencethe proliferation and migration of VSMCsfrom the media into the neointima. Thus,the resultant neointima consists ofVSMCs, extracellular matrix, and macro-phages recruited over several weeks.
• Restenosis and Diabetes
Diabetes is one of the main problems ofpercutaneous coronary revascularization,representing the actual dark side of ISR.We (Indolfi et al. 2001b) studied the ef-fect of balloon injury on neointimal hy-perplasia in streptozotocin-induced dia-betic rats with or without adjunct insulin
therapy. In addition, to study the effectof balloon injury in nondiabetic ratswith hyperinsulinemia, pancreatic isletswere transplanted under the kidney cap-sule in normal rats. First, we demon-strated that glucose did not increaseVSMC proliferation and migration invitro. In contrast, insulin induced a sig-nificant increase in VSMC proliferationand migration in cell cultures (Indolfi etal. 2001b). Furthermore, in VSMC cul-ture, insulin increased MAPK activation.Surprisingly, a reduction in neointimalhyperplasia was documented consistentlyafter vascular injury in hyperglycemicstreptozotocin-induced diabetic rats invivo, whereas insulin therapy significantlyincreased neointimal hyperplasia inthese rats (Indolfi et al. 2001b). Interest-ingly, after experimental balloon angio-plasty in hyperinsulinemic nondiabeticislet-transplanted rats, a significant in-crease in neointimal hyperplasia alsowas observed (Indolfi et al. 2001b).
Therefore, hyperinsulinemia throughactivation of the
ras
–MAPK
pathway,rather than hyperglycemia per se, appearsto be crucial in determining the exagger-ated neointimal hyperplasia after bal-loon angioplasty in diabetic animals.
• The Prevention of ISR With Eluting Stents
Because the stent is the only device ableto reduce restenosis, a major effort hasbeen made currently to improve this de-vice’s technology so as to further reducerestenosis after PCI. More recently, therehas been great enthusiasm about thepossibility that stents may be coatedwith slowly eluting antirestenotic agents.Indeed, the new concept of local drugdelivery directly to the site of vascularinjury via polymeric- or nonpolymeric-coated stents is by now the most reason-able and effective approach to achieve ad-equate localized antiproliferative effects.
A proposed explanation for the re-peated failure of clinical drug studieshas been that agents given systemicallyat nontoxic doses cannot reach sufficientlevels in injured arteries to impact sig-nificantly on the restenotic process. Localadministration of drugs offers distinctadvantages: the active drug is applied tothe vessel at the precise site and at thetime of vessel injury, local drug deliverymay be able to achieve higher tissueconcentrations of the drug, and systemic

TCM Vol. 13, No. 4, 2003
145
release is minimal and may reduce therisk of remote or systemic toxicity.
Synthetic polymers have been thesubject of study for vascular applications(van Beusekom et al. 1998). Several ma-terials have been tested for coating ofstents. Although conflicting results be-tween some of these studies (vanBeusekom et al. 1998) exist, they may berelated, in part, to characteristics sec-ondary to the synthetic polymer itself:surface characteristics (roughness, po-rosity, and contaminants), bulk, andfragmentation and degradation rate inthe case of bioabsorbable polymers (vanBeusekom et al. 1998). More recently,hydrogel coating has been proposed todelivery specific drugs and a new classof peptide-based hydrogels with the po-tential for applications in biotechnologyand, more crucially, in-stent coating hasbeen proposed (Nowack et al. 2002).
• Candidate Agents to Use in Eluting Stents
The candidate drug to use in elutingstents should be able to inhibit the com-plex molecular mechanisms of restenosiswithout local toxic effects. Uncontrolledneointima tissue accumulations showsome parallels to benign tumor growths;thus, the use of antineoplastic agentsseems to be a logical choice. Numerouspharmacologic agents with antiprolifera-tive properties have been tested for theirpotential to inhibit restenosis, mostlywith disappointing results (Indolfi et al.1999). Potential candidates for local drugdelivery are numerous and are listed inTable 1. We include a summary of rapa-mycin and paclitaxel, which are the mostpromising of the agents that are under-going clinical trials (Table 1).
Rapamycin (Sirolimus)
Rapamycin is a naturally occurringmacrocyclic lactone, which is highly ef-fective in preventing the onset and se-verity of disease in several animal modelsof autoimmune disease. Rapamycin in-hibits VSMC proliferation in vitro andin vivo by blocking the cell cycle at theG1/S transition (Gallo et al. 1999) andinhibits VSMC migration in vitro (Poonet al. 1996). Rapamycin is an antibioticthat prevents growth factor-dependentdownregulation of p27
Kip1
(Nourse et al.
1994). Sun et al. (2001) demonstrated thatrapamycin inhibits the migration ofmouse VSMCs containing p27Kip1(p27
Kip
�
/
�
and p27
Kip1
�
/
�
),
but not mouseVSMCs lacking p27
Kip1
(p27
Kip1–/–
). It alsopossesses important anti-inflammatoryproperties, as evidenced by its initialdevelopment as an antifungal agentand its current use as an immunomod-ulatory agent in the treatment of renaltransplant rejection.
Sirolimus (rapamycin) has been testedin several experimental and clinicalstudies to reduce the rate of restenosisafter stenting. Sousa et al. (2001) pro-vided a first glimpse at the 1-year dataafter the implantation of Sirolimus-eluting stents in humans after a previousreport on the safety of this novel ap-proach. This report describes a verysmall study, but with striking results.After 12 months of follow-up, the au-thors demonstrated a uniquely stable re-sult: not a single patient had sustainedclinical or angiographic restenosis (Sousaet al. 2001). These results are amplifiedby the recently reported, 238-patient,double-blind, randomized RAVEL trialin Europe and Latin America, with theSirolimus-eluding BX velocity balloon-expandable stent in the treatment ofpatients with de novo native coronarylesions, which found that restenosis at 6months was reduced from 26% in pa-tients receiving placebo to 0 in those re-
ceiving Sirolimus-eluting stents (Figure 3)(Morice et al. 2002). However, the strik-ing results obtained in the RAVEL studywere probably due to patient selection.In fact, an analysis of patients enrolledin the SIRIUS trial (Jenkins et al. 2002),who had longer lesions and were athigher risk for restenosis, showed a 9.2%rate of restenosis in patients treated withSirolimus-eluting stent compared with a32.3% rate of restenosis in the controlgroup. In addition, in the SIRIUS trial(Jenkins et al. 2002), the target lesionrevascularization (the so-called “clinicalrestenosis”) was 6.8% in the Sirolimusgroup compared with 16.6% in the con-trol group (
P
�
.01) (Figure 3).The results obtained with Sirolimus-
eluting stents were striking and werenot observed with other therapeutic ap-proaches; however, there are some con-cerns related to a “late malapposition”of the stents that was observed in 8.9%of the patients in the SIRIUS trial (Jen-kins et al. 2002). Although in the clinicaltrials an increased acute, subacute, orchronic thrombosis was not documented,an antiplatelet therapy after deploymentof an eluting stent was continued for alonger period (2 to 6 months) in order toprevent negative clinical events relatedto a delayed endothelialization or a latestent malapposition. Definitely, a longerfollow-up is needed.
Paclitaxel
Paclitaxel is an antineoplastic agent thatis used currently to treat several types ofcancer (Rowinsky and Donehower 1995).It is a diterpenoid with a characteristictaxane skeleton of 20 carbon atoms,
Table 1. Agents used in coated stents to prevent restenosis and ongoing trials
Agent Trials
Rapamycin and analogues
Rapamycin RAVEL/SIRIUSTacrolimus Everolimus Micophenolic acid
TaxolTaxane SCOREPaclitaxel TAXUS II/IVPaclitaxel ELUTES/ASPECT/
DELIVER
OtherBatimistat BRILLIANTDexamethosone STRIDEActinomycin D ACTIONResten NG ABT-578
Figure 3. Percentage of target lesion revas-cularization (TLR) in the ongoing trials usingeluting stents to prevent restenosis after stentdeployment.

146
TCM Vol. 13, No. 4, 2003
which exerts its pharmacologic effectsthrough formation of numerous decen-tralized and unorganized microtubules(Rowinsky and Donehower 1995). Pacli-taxel enhances the assembly of extraordi-narily stable microtubules, interruptingproliferation, migration, and signal trans-duction. Paclitaxel inhibits proliferationand migration of cultured VSMCs in adose-dependent manner (Axel et al. 1997).In vivo
studies have shown that pacli-taxel may prevent or attenuate resteno-sis (Kolodgie et al. 2002).
There are several ongoing clinical trialsof paclitaxel-coated stents. In the TAXUS Itrial (Grube et al. 2002), 61 patients wererandomized to receive a paclitaxel-coatedor a bare stent. At 6-month follow-up,no restenosis was seen in the paclitaxel-coated stent group, whereas the resteno-sis rate in the bare stent group was 10%(Figure 3) (Grube et al. 2002). However,the later European Evaluation of Pacli-taxel Eluting Stent (ELUTES) trial re-ported a target lesion revascularizationrate of 5% at 12 months compared witha rate of 16% in the standard stent group(Figure 3) (Jenkins et al. 2002).
In other clinical trials, the taxol de-rivative QP2 was used (Honda et al.2001). The first clinical experience witha paclitaxel derivative-eluting stentcovered by polyacrylate sleeves for ISRrevealed that the antiproliferative effectwas not confirmed at the 12-monthfollow-up, resulting in an increase ofrestenosis rate in treated patients (Liis-tro et al. 2002). Restenotic lesions fromthese eluting stents at 12 monthsshowed persistent fibrin deposition withvarying degrees of inflammation, andthe pathologic changes represented adelayed healing. The authors (Virmaniet al. 2002) concluded that the nonbio-degradable polymer alone might haveinduced chronic inflammation.
Recently available (although not yetpublished) data showed a beneficial ef-fect of paclitaxel-eluting stents in theTAXUS II trial (Jenkins et al. 2002).TAXUS II is a triple-blind randomizedtrial aimed at evaluating the safety andefficacy of paclitaxel “moderate release”(MR) and “slow release” (SR) elutingstents. The target vessel revascularization(TVR) rate in the TAXUS MR group was6.2% in the treated group comparedwith 17.7% in the control group (
P
�
.01), and was 7.7% vs. 14.3% (
P
�
.001)in the TAXUS SR group (Figure 3).
Limitations of the Eluting Stents
Although the principle of stent implan-tation is well established and most of theapplied drugs and polymers have beenused in clinical practice for many years,there is little experimental and only pre-liminary clinical knowledge of the acuteand long-term effects of drug eluting incoronary arteries. Thus, a number of con-cerns and open questions should be in-vestigated in the future. Some of theseissues are as follows:
Safety issues of eluting stents• Thrombosis• Late malapposition• Aneurysm• Edge effects• Overlapped segments• Polymer-induced inflammation
Issues impacting use of eluting stents• Efficacy• Safety• Regulatory (off-label use)• Cost and reimbursement
A serious concern is the possibility ofdelayed wound healing and re-endothe-lialization. All the tools used to preventrestenosis—including stent-based drugdelivery—may delay maturation andnormal endothelial function, and thusincrease the potential for a late throm-botic event. The delay of re-endothelial-ization is an important issue that canlimit the beneficial effect of elutingstents. Consequently, achieving completere-endothelialization of injured vesselafter stenting, with a regenerated endo-thelium showing normal morphologiccharacteristics and functions, may hinderrestenosis. In this regard, it is notewor-thy that statins prevent restenosis by in-hibiting VSMC proliferation (Indolfi etal. 2000c) and accelerating re-endothe-lialization through mobilization and in-corporation of bone marrow-derivedendothelial progenitor cells into the in-jury site (Walter et al. 2002). Moreover,the use of an agent that induces theheme oxigenase-1 pathway, which inhib-its VSMC proliferation (Duckers et al.2001) and increases endothelial prolifer-ation (Li Volti et al. 2002), could repre-sent a new potential drug for the elutingstent.
The major concern with regard to theuse of eluting stents is late malapposi-tion. Late malapposition has been de-scribed in both the RAVEL (Morice et al.
2002) and multicentre randomized dou-ble blind study of the Sirolimus coatedBX velocity stent (SIRIUS) (Jenkins etal. 2002) trials in a small cohort ofpatients that were enrolled for IVUSanalysis. In the SIRIUS trial, the latemalapposition was described in ap-proximately 10% of the patients treatedwith Sirolimus-coated stents, althoughit was not correlated with a significantadverse clinical outcome.
• Nonpharmacological Prevention of ISR: The Role of Physical Exercise
Several population-based studies (Indolfiet al. 2002a) have demonstrated that in-cremental levels of regular physical ac-tivity are inversely proportional to long-term cardiovascular mortality, but theeffects of dynamic exercise on neointi-mal hyperplasia and arterial remodelingafter vascular injury have not yet beenstudied.
Therefore, in our laboratory, the con-sequences of balloon dilation-inducedinjury and stenting on vascular remodel-ing were assessed in sedentary andtrained rats (Indolfi et al. 2002a). A sig-nificant reduction of both neointimalhyperplasia and negative remodelingwas observed 14 days after balloon in-jury in trained rats compared with sed-entary rats. Notably, decreases in neoin-timal hyperplasia and platelet aggregationalso were observed after stent deploy-ment in trained rats compared withsedentary rats (Indolfi et al. 2002a).Compared with the sedentary group, thearteries isolated from trained rats showedhigher levels of endothelial nitric oxidesynthase (eNOS) protein expression andactivity 7 days after arterial injury (In-dolfi et al. 2002a). Moreover, we demon-strated that exercise training producedaccelerated re-endothelialization of theinjured arterial segments of exercisedrats compared with the segments of sed-entary rats (Indolfi et al. 2002a). Thepivotal role played by nitric oxide in theexercise-related effects on restenosis wasdemonstrated by l-n-mono-methyl-argi-nine (L-NMMA) administration, whicheliminated the benefits of physical train-ing on the vessel wall after vascular in-jury (Indolfi et al. 2002b).
In summary, physical exercise, whichincreases eNOS expression and activity,could favorably affect restenosis afterballoon angioplasty and stenting; how-

TCM Vol. 13, No. 4, 2003
147
ever, further clinical studies should beperformed to evaluate the effective im-pact of physical training on restenosisafter angioplasty or stenting in humans.
• Conclusions and Future Perspectives
In the last few years, laboratory andanimal investigations have clarified themechanisms responsible for the prolif-eration of VSMCs after vascular injuryand proposed several therapeutic options(Indolfi et al. 1996, 1999). The informa-tion thus obtained has been translatedrapidly to the clinical scenario with theintroduction of “eluting stents” coatedwith rapamycin or paclitaxel that, in sev-eral studies, demonstrated efficacy andsafety in preventing ISR.
Drug-eluting stents represent one ofthe greatest breakthroughs in interven-tional cardiology. However, many unan-swered questions still need to be resolvedbefore the potential of these techniquesis determined. We hope that many ofthese issues will be addressed after thecompletion of planned and ongoing tri-als with longer follow-up. In addition,these new technologies should be testedin high-risk patients to prove effective-ness in the daily routine of treatingpatients who have not, until now, beenincluded in the published trials.
References
Al Suwaidi J, Berger PB, Holmes DR: 2000.Coronary artery stents. JAMA 284:1828–1836.
Axel DI, Kunert W, Goggelmann C, et al.:1997. Paclitaxel inhibits arterial smoothmuscle cell proliferation and migration
invitro
and
in vivo
using local drug delivery.Circulation 96:636–645.
Boehm M, Nabel EG: 2001. Cell cycle and cellmigration: new pieces to the puzzle. Circu-lation 103:2879–2881.
Boehm M, Yoshimoto T, Crook MF, et al.:2002. A growth factor-dependent nuclearkinase phosphorylates p27(Kip1) and regu-lates cell cycle progression. EMBO J 21:3390–3401.
Duckers HJ, Boehm M, True AL, et al.: 2001.Heme oxygenase-1 protects against vascu-lar constriction and proliferation. Nat Med7:693–698.
Farb A, Sangiorgi G, Carter AJ, et al.: 1999.Pathology of acute and chronic coronarystenting in humans. Circulation 99:44–52.
Gallo R, Padurean A, Jayaraman T, et al.:1999. Inhibition of intimal thickening afterballoon angioplasty in porcine coronaryarteries by targeting regulators of the cellcycle. Circulation 99:2164–2170.
Grube E, Silber S, Hauptmann KE, et al.:2002. TAXUS I: six- and twelve-month re-sults from a randomized, double-blind trialon a slow-release paclitaxel-eluting stentfor de novo coronary lesions. Circulation106:r76–r80.
Honda Y, Grube E, de la Fuente LM, et al.:2001. Novel drug-delivery stent: intravas-cular ultrasound observations from thefirst human experience with the QP2-elut-ing polymer stent system. Circulation104:380–383.
Hu Y, Mayr M, Metzler B, et al.: 2002. Bothdonor and recipient origins of smoothmuscle cells in vein graft atheroscleroticlesions. Circ Res 91:e13–e20.
Indolfi C, Avvedimento EV, Di Lorenzo E, etal.: 1997a. Activation of cAMP–PKA signal-ing
in vivo
inhibits smooth muscle cell pro-liferation induced by vascular injury. NatMed 3:775–779.
Indolfi C, Avvedimento EV, Rapacciuolo A, etal.: 1995a. Inhibition of cellular RAS pre-vents smooth muscle cell proliferationafter vascular injury
in vivo.
Nat Med6:541–545.
Indolfi C, Avvedimento EV, Rapacciuolo A, etal.: 1997b. In vivo gene transfer: preven-tion of neointima formation by inhibitionof mitogen-activated protein kinase kinase.Basic Res Cardiol 92:378–384.
Indolfi C, Chiariello M, Avvedimento EV:1996. Selective gene therapy of prolifera-tive disorders: sense and antisense. NatMed 6:634–635.
Indolfi C, Cioppa A, Stabile E, et al.: 2000a.Effects of hydroxymethylglutaryl coenzymeA reductase inhibitor simvastatin onsmooth muscle cell proliferation
in vitro
and neointimal formation
in vivo
after vas-cular injury. J Am Coll Cardiol 35:214–221.
Indolfi C, Coppola C, Torella D, et al.: 1999.Gene therapy for restenosis after balloonangioplasty and stenting. Cardiol Rev7:324–331.
Indolfi C, Di Lorenzo E, Rapacciuolo A, et al.:2000b. 8-Chloro-cAMP inhibits smoothmuscle cell proliferation
in vitro
andneointimal formation induced by ballooninjury in vivo. J Am Coll Cardiol 36:288–293.
Indolfi C, Esposito G, Di Lorenzo E, et al.:1995b. Smooth muscle cell proliferation isproportional to the degree of balloon in-jury in a rat model of restenosis. Circula-tion 92:1230–1235.
Indolfi C, Esposito G, Stabile E, et al.: 2000c.A new rat model of small vessel stenting.Basic Res Cardiol 95:179–185.
Indolfi C, Stabile E, Coppola C, et al.: 2001a.Membrane-bound protein kinase A inhib-its smooth muscle cell proliferation
in vitro
and
in vivo
by amplifying c-AMP–PKA sig-nals. Circ Res 88:319–324.
Indolfi C, Torella D, Cavuto L, et al.: 2001b.Effects of balloon injury on neointimal hy-perplasia in streptozotocin-induced diabe-tes and in hyperinsulinemic non-diabeticpancreatic islet-transplanted rats. Circula-tion 103:2980–2986.
Indolfi C, Torella D, Coppola C, et al.: 2002a.Physical training increases eNOS vascularexpression and activity and reduces res-tenosis after balloon angioplasty or arterialstenting in rats. Circ Res 91:1190–1197.
Indolfi C, Torella D, Coppola C, et al.: 2002b.Rat carotid artery dilation by PTCA bal-loon catheter induces neointima formationin presence of IEL rupture. Am J Physiol283:H760–H767.
Jenkins NP, Prendergast BD, Thomas M:2002. Drug eluting coronary stents. BMJ325:1315–1316.
Kolodgie FD, John M, Khurana C, et al.:2002. Sustained reduction of in-stentneointimal growth with the use of a novelsystemic nanoparticle paclitaxel. Circula-tion 106:1195–1198.
Liistro F, Stankovic G, Di Mario C, et al.:2002. First clinical experience with a pacli-taxel derivate-eluting polymer stent systemimplantation for in-stent restenosis: imme-diate and long-term clinical and angio-graphic outcome. Circulation 105: 1883–1886.
Li Volti G, Wang J, Traganos F, et al.: 2002.Differential effect of heme oxygenase-1 inendothelial and smooth muscle cell cycleprogression. Biochem Biophys Res Com-mun 296:1077–1082.
Morice MC, Serruys PW, Sousa JE, et al.:2002. A randomized comparison of aSirolimus-eluting stent with a standardstent for coronary revascularization. NEngl J Med 346:1773–1780.
Nabel EG: 2002. CDKs and CKIs: moleculartargets for tissue remodelling. Nat RevDrug Discov 1:587–598.
Nourse J, Firpo E, Flanagan WM, et al.: 1994.Interleukin-2-mediated elimination of thep27Kip1 cyclin-dependent kinase inhibitorprevented by rapamycin. Nature 372:570–573.
Nowak AP, Breedveld V, Pakstis L: 2002. Rap-idly recovering hydrogel scaffolds fromself-assembling diblock copolypeptide am-phiphiles. Nature 417:424–428.
Ophascharoensuk A, Fero ML, Hughes J, etal.: 1998. The cyclin-dependent kinase in-hibitor p27Kip1 safeguards against inflam-matory injury. Nat Med 4:575–580.

148
TCM Vol. 13, No. 4, 2003
Poon M, Marx SO, Gallo R, et al.: 1996. Rapa-mycin inhibits vascular smooth muscle cellmigration. J Clin Invest 98:2277–2283.
Rowinsky EK, Donehower RC: 1995. Pacli-taxel (taxol). N Engl J Med 332:1004–1014.
Sata M, Saiura A, Kunisato A, et al.: 2002.Hematopoietic stem cells differentiate intovascular cells that participate in the patho-genesis of atherosclerosis. Nat Med 8:403–409.
Sousa JEMR, Costa MA, Abizaid A, et al.:2001. Sustained suppression of neointimalproliferation by Sirolimus-eluting stents:one-year angiographic and intravascularultrasound follow-up. Circulation 104: 2007–2011.
Sun J, Marx SO, Chen HJ, et al.: 2001. Rolefor p27 (Kip1) in vascular smooth musclecell migration. Circulation 103:2967–2972.
Tanner FC, Boehm M, Akyurek LM, et al.: 2000.Differential effects of the cyclin-dependentkinase inhibitors p27(Kip1), p21(Cip1), andp16(Ink4) on vascular smooth muscle cellproliferation. Circulation 101: 2022–2025.
Tanner FC, Yang ZY, Duckers E, et al.: 1998.Expression of cyclin-dependent kinase in-hibitors in vascular disease. Circ Res82:396–403
van Beusekom HM, Schwartz RS, van derGiessen WJ: 1998. Synthetic polymers.Semin Interv Cardiol 3:145–148
Virmani R, Liistro F, Stankovic G, et al.: 2002.Mechanism of late in-stent restenosis afterimplantation of a paclitaxel derivate-elutingpolymer stent system in humans. Circula-tion 106:2649–2651.
Walter DH, Rittig K, Bahlmann FH, et al.:2002. Statin therapy accelerates reendo-thelialization: a novel effect involving mo-bilization and incorporation of bone mar-row-derived endothelial progenitor cells.Circulation 105:3017–3024.
Welt FG, Rogers C: 2002. Inflammation andrestenosis in the stent era. ArteriosclerThromb Vasc Biol 22:1769–1776.
PII S1050-1738(03)00038-0 TCM
(mean age
�
9.9
�
4 years) with no or-ganic heart disease and normal baselineelectrocardiogram (ECG) (except for si-nus bradycardia), who suffered from ep-isodes of syncope and seizures usuallyrelated to physiologic or emotional stress.The mean age at which the first syncopeoccurred was 7.8
�
4 years. These chil-dren had no structural heart disease anda normal QT interval. Interestingly, theVT could be reproduced in these pa-tients by a treadmill exercise test or byinfusing small amounts of isoproterenolat a rate sufficient to accelerate the car-diac rate to 150 to 160 beats per minute(bpm). Upon receiving treatment with
�
-blockers, the patients’ symptoms un-derwent almost complete resolution,and no episodes of VT could be foundon 24-hour Holter monitoring.
Swan et al. (1999) described two un-related families suffering from autosomal-dominant CPVT. However, compared withLeenhardt et al.’s patients (1995), symp-toms in these two families began at alater age (21
�
10 years). Among af-fected family members, the cumulativecardiac mortality by the age of 30 yearswas 31%. Ventricular arrhythmias hada distinctive pattern of bidirectionalVT, somewhat different from that de-scribed by Leenhardt et al. (1995),which was more chaotic in appearance.Affected members in these familieswere treated successfully with
�
-blockers.With the use of linkage analysis, Swanet al. (1999) mapped the disease-causinggene to the long arm of chromosome 1at 1q42–1q43. Priori et al. (2001) andLaitinen et al. (2001) identified, for thefirst time, several missense mutationsin the ryanodine receptor 2 gene(
RYR2
) in four patients and three
fami-lies harboring the disease. Recently,Priori et al. (2002) reported on the clin-ical and molecular characterization of30 probands with CPVT and their 118family members.
RYR2
mutations wereidentified in only 14 of the 30 probands.The ryanodine receptor is a sarcoplas-mic reticulum (SR) channel, responsi-ble for the release of Ca
2
�
ions from theSR in response to Ca
2
�
ingress to thecytoplasm through the sarcolemmalCa
2
�
channels (“calcium-induced cal-cium release”) (Stokes and Wagen-knecht 2000). Recently, the spectrum of
RYR2
-related diseases was expandedwhen Tiso et al. (2001) described mu-tations in patients suffering from ar-
A Missense Mutation in the
CASQ2
Gene Is Associated with Autosomal-Recessive Catecholamine-Induced Polymorphic Ventricular Tachycardia
Michael Eldar,* Elon Pras, and Hadas Lahat
Catecholamine-induced polymorphic ventricular tachycardia (CPVT),a rare disease that occurs in subjects without obvious organic heartdisease, is characterized by episodes of syncope, seizures, or suddendeath in response to physiologic or emotional stress. This reportreviews evidence that a missense mutation in the
CASQ2
gene is asso-ciated with autosomal-recessive CPVT. (Trends Cardiovasc Med 2003;13:148–151) © 2003, Elsevier Inc.
Michael Eldar and Hadas Lahat are at theHeart Institute, Sheba Medical Center, TelHashomer, Israel. Elon Pras is at the DanekGartner Institute of Human Genetics, ShebaMedical Center, Tel Hashomer, Israel.
* Address correspondence to: MichaelEldar, MD, Heart Institute, Sheba MedicalCenter, Tel Hashomer 52621, Israel. Tel.:(�03) 635-2303; fax: (�03) 534-3888; e-mail:[email protected].
© 2003, Elsevier Inc. All rights reserved.1050-1738/03/$-see front matter
Catecholamine-induced polymorphic ven-tricular tachycardia (CPVT), a rare dis-ease that occurs in subjects without obvi-ous organic heart disease, is characterizedby episodes of syncope, seizures, or sud-den death in response to physiologic oremotional stress (Viskin and Belhassen1998). The disease, first described as acase report (Reid et al. 1975), was de-fined as a clinical entity by Leenhardtet al. (1995), who described 21 children
Copyright © 2022 FDOKUMEN




















