Molecular mechanisms of endocrine resistance and their implication in the therapy of breast cancer
20
Review Molecular mechanisms of endocrine resistance and their implication in the therapy of breast cancer Marinella Zilli, Antonino Grassadonia, Nicola Tinari, Alessia Di Giacobbe, Simona Gildetti, Jamara Giampietro, Clara Natoli, Stefano Iacobelli ⁎ on behalf of Consorzio Interuniversitario Nazionale per la Bio-Oncologia (CINBO) Department of Oncology and Neurosciences, University “G. D'Annunzio” Medical School, Via dei Vestini, 66100 Chieti, Italy abstract article info Article history: Received 17 May 2008 Received in revised form 11 August 2008 Accepted 14 August 2008 Available online 29 August 2008 Keywords: Endocrine resistance Breast cancer Estrogen receptor Hormonal therapy The use of endocrine agents is a safe and effective treatment in the management of hormone-sensitive breast cancer. Unfortunately, sooner or later, tumor cells develop resistance to endocrine manipulation making useless this approach. During the last decade, new molecules and intracellular signaling pathways involved in endocrine resistance have been identified. Several studies have documented that estrogen receptor signaling may maintain a pivotal role in the tumor growth despite the failure of a previous hormonal treatment. In this review we will discuss the general principles for optimizing the choice of endocrine therapy based on an understanding of the molecular mechanisms responsible for resistance to the different anti-hormonal agents. © 2008 Elsevier B.V. All rights reserved. Contents 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63 2. ER: structure and function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63 2.1. ERα and ERβ subtypes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63 2.2. Genomic (nuclear) ER signaling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64 2.3. Non-genomic (membrane) ER signaling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65 3. Different therapeutic approaches to block estrogen action . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66 3.1. Selective ER modulators (SERMs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66 3.2. Aromatase inhibitors (AIs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66 3.3. Selective ER down-regulators (SERDs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67 4. Mechanisms of endocrine resistance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67 4.1. Estrogen receptor status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67 4.1.1. Loss of expression of ERα. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67 4.1.2. Mutations of ERα . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68 4.1.3. Altered expression of ERβ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68 4.2. Intracellular milieu. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68 4.2.1. Altered expression of coregulators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68 4.2.2. Increased growth factor signaling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68 4.2.3. Estrogen hypersensitivity and supersensitivity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70 4.3. Altered metabolism of endocrine agents. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70 4.3.1. Pharmacogenomics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71 4.3.2. Drug interactions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71 5. Optimization of endocrine therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71 5.1. Sequential or concomitant use of endocrine therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71 5.2. Predictive factors of endocrine response. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72 5.2.1. HER2 status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72 Biochimica et Biophysica Acta 1795 (2009) 62–81 ⁎ Corresponding author. Tel.: +39 0871 3556732; fax: +39 0871 3556707. E-mail address: [email protected] (S. Iacobelli). 0304-419X/$ – see front matter © 2008 Elsevier B.V. All rights reserved. doi:10.1016/j.bbcan.2008.08.003 Contents lists available at ScienceDirect Biochimica et Biophysica Acta journal homepage: www.elsevier.com/locate/bbacan
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Molecular mechanisms of endocrine resistance and their implication in the therapy of breast cancer

Biochimica et Biophysica Acta 1795 (2009) 62–81
Contents lists available at ScienceDirect
Biochimica et Biophysica Acta
j ourna l homepage: www.e lsev ie r.com/ locate /bbacan
Review
Molecular mechanisms of endocrine resistance and their implication in the therapyof breast cancer
Marinella Zilli, Antonino Grassadonia, Nicola Tinari, Alessia Di Giacobbe, Simona Gildetti, Jamara Giampietro,Clara Natoli, Stefano Iacobelli ⁎on behalf of Consorzio Interuniversitario Nazionale per la Bio-Oncologia (CINBO)Department of Oncology and Neurosciences, University “G. D'Annunzio” Medical School, Via dei Vestini, 66100 Chieti, Italy
⁎ Corresponding author. Tel.: +39 0871 3556732; fax:E-mail address: [email protected] (S. Iacobelli).
0304-419X/$ – see front matter © 2008 Elsevier B.V. Aldoi:10.1016/j.bbcan.2008.08.003
a b s t r a c t
a r t i c l e i n f oArticle history:
The use of endocrine agents Received 17 May 2008Received in revised form 11 August 2008Accepted 14 August 2008Available online 29 August 2008Keywords:Endocrine resistanceBreast cancerEstrogen receptorHormonal therapy
is a safe and effective treatment in the management of hormone-sensitive breastcancer. Unfortunately, sooner or later, tumor cells develop resistance to endocrine manipulation makinguseless this approach. During the last decade, newmolecules and intracellular signaling pathways involved inendocrine resistance have been identified. Several studies have documented that estrogen receptor signalingmay maintain a pivotal role in the tumor growth despite the failure of a previous hormonal treatment.In this reviewwewill discuss the general principles for optimizing the choice of endocrine therapy based on anunderstanding of the molecular mechanisms responsible for resistance to the different anti-hormonal agents.
© 2008 Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 632. ER: structure and function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
2.1. ERα and ERβ subtypes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 632.2. Genomic (nuclear) ER signaling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 642.3. Non-genomic (membrane) ER signaling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
3. Different therapeutic approaches to block estrogen action . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 663.1. Selective ER modulators (SERMs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 663.2. Aromatase inhibitors (AIs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 663.3. Selective ER down-regulators (SERDs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
4. Mechanisms of endocrine resistance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 674.1. Estrogen receptor status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
4.1.1. Loss of expression of ERα. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 674.1.2. Mutations of ERα . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 684.1.3. Altered expression of ERβ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
4.2. Intracellular milieu. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 684.2.1. Altered expression of coregulators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 684.2.2. Increased growth factor signaling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 684.2.3. Estrogen hypersensitivity and supersensitivity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
4.3. Altered metabolism of endocrine agents. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 704.3.1. Pharmacogenomics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 714.3.2. Drug interactions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
5. Optimization of endocrine therapy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 715.1. Sequential or concomitant use of endocrine therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 715.2. Predictive factors of endocrine response. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
5.2.1. HER2 status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
+39 0871 3556707.
l rights reserved.

63M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
5.2.2. PR status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 725.2.3. New potential predictive markers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
6. Overcoming endocrine resistance by signal transduction inhibitors (STIs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 747. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
1. Introduction
It has long been established that estrogen is involved in thepathogenesis of breast cancer and sustains the growth of estrogenreceptor (ER) expressing breast cancer cells. Consequently, therapieshave been developed to reduce estrogen levels or block signalingthrough ER in breast cancer cells. Although introduced more than100 years ago, endocrine therapy is still an integral component in thesystemic treatment of ER-positive breast cancer at any stage.Endocrine therapy is based on different approaches, including: (i)block of ER by the use of selective ER modulators (SERMs), such astamoxifen; (ii) reduction of estrogen levels through aromataseinhibitors (AIs); (iii) induction of ER degradation by selective estrogenreceptor down-regulators (SERDs), such as fulvestrant.
For over thirty years tamoxifen has been the cornerstone for thetreatment of breast cancer [1]. Five years of adjuvant tamoxifenreduce the annual risk of recurrence and death for breast cancer by47% and 26%, respectively [2]. Moreover, tamoxifen inducesobjective response or disease stabilization in more than 50% ofpreviously untreated metastatic breast cancer patients with ER-positive tumors [3]. The main problem limiting the use of tamoxifenis de novo and acquired resistance to the drug. In fact, only abouthalf of ER-positive tumors are responsive to tamoxifen, and eveninitially responding tumors eventually develop resistance to thedrug during the course of the treatment [4]. Several clinical trialssuggest that AIs possess an enhanced anti-tumor effect as comparedwith tamoxifen, and might be effective in patients resistant totamoxifen [5–7]. Recently fulvestrant has been reported to be asactive as AIs in tamoxifen-resistant metastatic breast cancer patients[8] and also shows a certain efficacy in patients progressing to AIs[9]. However despite the integration of more powerful endocrineagents, resistance to all forms of endocrine therapy remains a majorproblem.
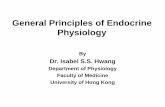
Fig. 1. Schematic representation of the structure of human ERα and ERβ nuclear receptorsdomain at the N-terminus contains the ligand-independent transcriptional activation funcnuclear localization signal (NLS), the D domain corresponds to the hinge region, the E domainfunction 2 (AF2) and the F domain at the C-terminus. Numbers outside each box refer to am
Much evidence has established that ER-transcriptional activity is acomplex event of which estrogen binding is only a small part. Thebiological activity of ER is critically influenced by the cellular context,i.e. growth factor signaling pathways and availability of coregulatoryproteins, along with the correct sequence of the response elements inthe promoter of target genes. These factors significantly affect theefficacy of endocrine agents and are related to de novo or acquiredresistance to endocrine manipulation. During hormonal treatmentmodifications of the cellular molecular environment can determine aswitch of gene transcription from an estrogen-dependent to anestrogen-independent modality, and eventually induce transcriptionof estrogen-sensitive genes in the absence of ER.
A better understanding of the molecular mechanisms responsiblefor the loss of estrogen dependency might enable novel strategies fortherapeutic intervention. This article reviews some of the known andemerging complexities of ER signaling in breast cancer and discussesthe therapeutic implications of these findings.
2. ER: structure and function
2.1. ERα and ERβ subtypes
ER belongs to a superfamily of nuclear receptors, including those ofother steroid hormones, thyroid hormones, vitamin D, and retinoicacid [10]. Two molecular forms of ER have been described: ERα andERβ. These are produced by two distinct genes located on chromo-some 6 and 14, respectively [11,12]. ERα and ERβ display a highrelative tissue-specific expression, with overlapping distribution insome tissues. ERβ is more expressed in prostate, bone, ovaries(granulosa cells), lungs, and in various parts of the central andperipheral nervous system, while ERα is predominantly expressed inthe pituitary gland, ovaries (thecal and interstitial cells), uterus, liver,kidneys, adrenals, and the mammary glands [13–15].
. Both ERα and ERβ are characterized by a well-defined domain organization: the A/Btion 1 (AF1), the C domain represents the DNA-binding domain (DBD) and contains aharbors the ligand-binding domain and the ligand-dependent transcriptional activationino-acid number. Percentage of amino-acid homology for each domain is also shown.

64 M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
Normally, when bound to their ligand, the ERs function astranscriptional factors of specific target genes [16,17]. Like othersteroid hormone receptors both the ER subtypes contain a well-defined domain organization, designated A/B through F [18–20](Fig. 1). The A/B domain, which is located at the N-terminus, containsthe activation function 1 (AF1) [21], a region responsible for theconstitutive and ligand-independent transcriptional activity of ER.The C domain, referred to as DNA-binding domain (DBD), is respon-sible for specific DNA binding and receptor dimerization [22]. The Ddomain is a flexible hinge between the C and E domains and con-tains a nuclear localization signal [23]. The E domain, referred to asligand-binding domain (LBD), is a twelve-helix region involved inligand binding and receptor dimerization. It harbors a secondnuclear localization signal and the activation function 2 (AF2), res-ponsible for the ligand-dependent activation of ER [21]. The Fdomain, located at the extreme carboxy-terminus of the ERs, is asmall region that although unnecessary for transcriptional activationexerts a complex modulatory role on both AF1 and AF2 activities ofthe receptor [24–26].
ERα and ERβ share a high degree of homology in their DBD (96%)and LBD (55%) [12]. On the other hand the N-terminal A/B domain andthe C-terminal F domain are the most variable regions. They have lessthan 20% amino-acid identity which indicates that these domains maycontribute to ER-subtype-specific actions on target genes [27].Compared to ERα, ERβ exhibits a weak AF1 activity [28,29] andshows a different response to agonist/antagonist ligands [25,30].These differences suggest that ERα and ERβ could have distinctfunctions in terms of gene regulation and biologic response and maycontribute to the selective actions of estrogen in different targettissues [31].
Both ERα and ERβ are present in normal breast tissue, but onlyERα is essential for ductal growth. In fact, ERα-knockout mice showvery little growth of mammary ducts [32], while ERβ-knockout micedevelop a normal mammary gland with regular ductal branching [33].It is likely that ERβ exerts pro-differentiative and anti-proliferative
Fig. 2. Nuclear-initiated steroid signaling (NISS) and membrane-initiated steroid signaling (Mdiffuse passively through the cytoplasmic and the nuclear membrane and to bind its nuclear rspecific DNA sequence defined as estrogen-responsive element (ERE) located in the promoteAlternatively, the activated ER binds to other transcription factors such as Fos (F) and Jun (Jresponsive genes (non-classical pathway), such as cyclin D1 and insulin-like growth factordimer, with growth factor receptors (GFR) and activates the signal transduction pathways o
functions [33]. Several studies have reported an increase in ERα/ERβratio in breast cancer as compared with benign tumors and normaltissues [34–36], suggesting that ERα is most closely associated withcarcinogenesis, while ERβ can protect against the mitogenic activity ofestrogens in mammary premalignant lesions. There is evidence thatthe estrogen-induced proliferation of ERα-positive breast cancer cellscan be inhibited by ERβ overexpression [37–39]. Indeed, ERβ has beenshown to repress c-myc, cyclin D1 and cyclin A and to increase theexpression of p21 and p27 causing cell-cycle arrest in G2 phase [38]and to decrease the contents of positive proliferation regulators suchas cyclin E, Cdc25A, p45skp2 [37]. All these observations suggest thatthe loss of ERβ expression may be involved in tumor progression [40]and this leads to the consideration that ERβ functions as a putativetumor suppressor gene [41]. Consistent with its anti-tumor activitythe ERβ expression has been reported to be associated with a betterprognosis in breast cancer patients [42].
Routinely the evaluation of the ER expression in breast cancer, asdetermined by immunohistochemistry refers to ERα; consequently,the available information on the prognostic and predictive value of ERare related to this receptor form. If not otherwise specified, “ER” willrefer to ERα throughout this review.
ER acts through two different mechanisms: genomic and non-genomic (Fig. 2).
2.2. Genomic (nuclear) ER signaling
In the absence of estrogen, ERs lie in the cell nucleus as inactive,monomeric molecules bound to heat-shock proteins [43]. Estrogenbinds to the LBD of the receptor and causes a series of ERmodifications, including conformational changes, phosphorylations,dissociation from the chaperon proteins and homo-, or hetero-dimerization [16]. The ER dimer binds to the consensus sequenceGGTCAnnnTGACC, known as estrogen-response element (ERE),located in the promoter region of estrogen-regulated genes [44,45],and determines up-regulation of genes involved in cell proliferation
ISS) pathways of estrogen receptor (ER). Due to its steroidal nature, estrogen is able toeceptor. The activated ER binds, as a dimer and in the presence of coactivators (CoA), to ar of some estrogen-regulated genes (classical pathway), such as complement 3 and pS-2.), that in turn bind to different DNA sequences (e.g. AP-1) and activate other estrogen-receptor 1 (IGFR1). Estrogen can also bind to a membrane receptor that cooperates, asf AKT and MAPK, leading to gene activation.

65M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
and survival and down-regulation of genes with anti-proliferative orpro-apoptotic activity and the final effect is of growth stimulation[46,47].
The perfectly palindromic ERE sequence derives from severalhighly estrogen-responsive genes from Xenopus laevis [48,49].Whereas in human genome most estrogen-target genes have animperfect palindromic sequences in their promoter, differing from theconsensus sequence in one or more nucleotides. Different EREs inducedifferent conformational change of the ER and therefore couldconstitute a mechanism for modulation of estrogen-mediated genetranscription [50].
The above described mechanism of ER action is referred to as“classical pathway” and is directly related to the ability of ER toregulate the expression of genes containing ERE sequence in theirpromoter, such as complement 3 and pS-2 [51].
ER can influence the transcription of genes lacking ERE sequenceand regulated by other transcription factors that bind to alternativeregulatory DNA sequences. This mechanism does not require a directbinding of ER to DNA given that it can be activated by ERα lacking DBD[52,53]. The promoter elements involved in this response include AP-1sites, cyclic AMP-response elements (CREs) and Sp1 sites, whichdirectly bind Jun/Fos [54], c-Jun/ATF-2 [55] and Sp-1 [56], respectively.ER interacts with these transcription factors, it stabilizes their directbinding to DNA and thus enhances transcription. This mechanismdefined as “non-classical pathway” underlies the estrogen-inducedtranscription of genes such as cyclin D1 [57] and IGFR1 [58].
In some estrogen-target genes the regulation of transcription ismore complex, because more than one ERE-like sequence and/or EREhalf-sites are seen in the promoter [44,59]. Some genes have in theirregulatory region both ERE and non-classical sites. An example is thevascular endothelial growth factor (VEGF), whose transcription can beinduced by estrogen through a variant ERE or through SP1 sites,according to the cellular context [60–63]. Interestingly some ERE half-sites can act in synergy with other regulatory elements within a genepromoter region. For example, the promoter of the PR gene containsthe combination of a half ERE upstream of two Sp1 binding sites. ERcould influence PR expression directly by binding to the half-site andindirectly by interacting with proteins bound to the Sp1 sites [64].
The classical and non-classical pathways are known as “genomic”or “nuclear-initiated steroid signaling (NISS)” pathways. The recruit-ment of estrogen-bound ER in the promoter region of sensitive genesdirectly via ERE or indirectly via non-classical sites is able to inducegene transcription only if AF1 and/or AF2 are activated. Depending onthe cellular milieu and the specific promoter type either AF1 or AF2can be dominant [21,65,66], but generally a synergism involving boththese activation functions occurs [16,67]. It is important to note that ifeither AF1 or AF2 is dominant estrogen behaves as an agonist on genetranscription.
AF2 activation is totally dependent on ligand. The binding ofestrogen to ER induces a rearrangement of the LBD helices 3, 5, and 12with the creation of a hydrophobic cleft, where specifically orientatedhelix 12 seals inside the hormone and uncovers the AF2 region. Thisregion serves as a binding surface for proteins containing α-helicalleucine-rich peptide motifs, known as LXXLL motifs or NR boxes,which act as coactivators or corepressors of ER (collectively named ascoregulatory proteins) [68–70]. The most studied coactivators aremembers of the p160 family of nuclear-receptor coactivators, includ-ing: nuclear-receptor coactivator 1 (NCoA1), also known as steroidreceptor coactivator 1 (SRC-1); NCoA2, also known as SRC-2 ortranslation initiation factor 2 (TIF2); and NCoA3, also known asamplified in breast cancer 1 (AIB1) or SRC-3 [70,71]. Binding of thesemolecules to AF2 enhances transcriptional activity of ER by forminglarge complexes that recruit histone-acetyltransferase (HAT), anenzyme causing the chromatin decondensation required for genetranscription. In contrast, corepressor proteins such as nuclear-receptor corepressor 1 (NCoR1) and NCoR2 reduce ER-driven
transcription by recruitment of histone-deacetylase complexes(HDAC) at the promoter site. This leads to chromatin condensationand decreased rate of transcriptional initiation [72].
The type of coregulatory proteins recruited by ER depends on theconformational structure of the receptor which is affected not only bythe nature of ligand (estrogen versus tamoxifen, see ahead) but also bythe specific ERE sequence [59,73].
Diversely from AF2 activity, AF1 activity is ligand independent andwas originally identified by its ability to stimulate transcription in anERα deletion mutant that contained only the N-terminus fused to aheterologous DBD [74]. In the absence of estrogen, AF1 is activated byphosphorylation at specific serine residues (Ser104, Ser106, Ser118,Ser167) following the activation of p42/p44 mitogen-activated proteinkinase (MAPK), phosphatidylinositol 3 kinase (PI3K)/protein kinase B(AKT), and p38 MAPK pathways [75–78]. These different kinasepathways are triggered by growth factor receptors (GFRs), such asepidermal growth factor receptor (EGFR) or insulin-like growth factorreceptor 1 (IGFR1) [79]. AF1 phosphorylation stimulates ER-transcrip-tional activity by recruitment of coactivators which may be unique forAF1 or identical to those that bindAF2 [80]. Themechanismunderlyingthe ability of estrogen to increaseAF1 activity is not understoodwell. Inresponse to estrogen binding ER phosphorylation is enhanced, mainlyon Ser118, and to a lesser extent on Ser104/Ser106 [81], the same residuesinvolved in AF1 constitutive activity [82]. Moreover, in response toestrogen AF1 synergizes with the ligand-dependent AF2 through therecruitment of coactivators that simultaneously interact with both AFs[83–85]. Both AF1 phosphorylations and AF1–AF2 interaction con-tribute to the estrogen-induced ER-transcriptional activity.
The phosphorylation of ER by GFR-dependent kinases is anessential component of the ordinary regulation and function of ER.However, in the absence of estrogen ER exhibits a minimal phosphor-ylation status responsible for its AF1 constitutive activity. It is likelythat the conformational change of ER induced by estrogen bindingenhances the ability of the kinases to phosphorylate the receptor [81].
It is important to note that in particular cellular milieu, growthfactor signaling pathways can directly activate ER and the transcrip-tion of ER-regulated genes in the absence of estrogen [86]. Thismechanism might result in the lack of efficacy of various endocrinetherapies, to be discussed in detail below.
ERα and ERβ exhibit similar patterns of gene activation at classicalERE-containing target genes even if ERβ requires higher estrogenconcentrations than ERα [87]. However, ERα and ERβ have completelydifferent effects at non-classical AP-1 sites after estrogen binding: ERαactivates, while ERβ inhibits transcription [88–90]. For example, geneexpression of cyclin D1 regulated by estrogen via AP-1 sites isstimulated by ERα, but it is inhibited by ERβ [91]. Therefore therelative cellular expression of ERα and ERβ will determine the finaleffect of estrogen on cyclin D1 expression. This suggests that ERβmayindeed modulate the proliferative effects of ERα by blocking its actionon the cyclin D1 gene or other key pro-proliferative target genescontaining CRE or AP-1 sites [91]. Interestingly enough, in response toestrogen ERα activation of AP-1-dependent genes requires thepresence of the N-terminal domain, as demonstrated by the absenceof activation in the N-terminal deletionmutant [24]. However, the ERβchimera containing the N-terminal domain of ERα shows no activa-tion. This suggests that there is a fundamental difference between ERαand ERβ ligand activation at AP-1 sites which involves protein–proteininteractions other than or in addition to the N-terminal domain [24].
2.3. Non-genomic (membrane) ER signaling
In addition to the above nuclear effects there are ER functions thatcan occur very quickly in the cell (minutes from the addition ofestrogen) and are initially independent of gene transcription. Thisrapid non-genomic mechanism of action is mediated by themembrane-associated ER and is also called membrane-initiated

66 M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
steroid signaling (MISS) pathway [92]. ER localization to themembrane requires receptor palmitoylation and binding to caveolin1 [93]. At the membrane ER is associates with caveolin rafts and uponestrogen binding interacts as dimers, directly with adaptor proteins(Shc), Src, p85 subunit of PI3K, and G-proteins [93,94], resulting in theactivation of: GFRs, e.g. EGFR, IGFR1, HER2; cytoplasmatic kinases, e.g.MAPKs, PI3K, AKT and the mammalian target of rapamycin (mTOR);signaling enzymes, e.g. adenyl cyclases [95–97]. In turn, cytoplasmatickinases can phosphorylate ER and its coregulators, resulting in theactivation of nuclear ER-driven transcription [98]. All together theseobservations suggest that the non-genomic and genomic activities ofER are complementary and even synergistic. In addition, manyproteins encoded by ER target genes, such as TGFα and amphiregulin(AR), are key components of GFRs signaling. Therefore the ER and GFRpathways establish a bidirectional functional activation leading to anamplification of the growth signal.
Non-genomic activity is highly dependent on and regulated bycoregulatory proteins, and it is influenced by the overall signaltransduction pathways operating in a specific cell or tumor milieu.The most studied membrane ER coregulators are: proline-glutamicacid, leucine-rich protein 1 (PELP1), also called modulator of non-genomic activity of ER (MNAR), and the metastasis-associated (MTA)proteins. MNAR/PELP1 is overexpressed in breast cancer and enhancesboth genomic ER activity on gene transcription and non-genomic ERactivity on the c-Src/p42/44 MAPK phosphorylation cascade [96,99].On the other hand, members of the MTA coregulators inhibit genomicactivity but they enhance non-genomic action of ER. The nuclearMTA1factor and its variant MTA1s, for example, inhibit nuclear ER activity,the former by traditional recruitment of corepressors to the ER-transcriptional complexes, the latter by sequestering ER in thecytoplasm [100,101]. In this way, MTA1s concurrently increases non-genomic ER activity [100].
Defined motifs in E domain of ER are critical for membranelocalization and function of the receptor [102]. Mutations in thesemotifs prevent ER dimerization, association with caveolin-1, and non-genomic ER signaling activation of p42/44 MAPK, PI3K, and cAMP[103]. However, ER interaction with the signaling molecule MNARinvolves both the amino (N)-terminus and portions of the E domain ofER [104].
In some tissues, such as bone and endothelial cells, estrogensignaling is predominantly non-genomic [105]. It is important to notethat, for its activation, the non-genomic ER pathway is highlydependent on ligand [106].
3. Different therapeutic approaches to block estrogen action
3.1. Selective ER modulators (SERMs)
SERMs such as tamoxifen, toremifene and raloxifene, are a class ofcompounds endowed with estrogen agonistic and antagonisticactivity in different tissues [107]. SERMs competitively inhibit bindingof estrogen to ER and profoundly affect both the genomic and non-genomic activity of ER. Tamoxifen, the prototype of SERMs, binds tonuclear ER and, just like estrogen, induces its dimerization. However,unlike estrogen, the binding of tamoxifen to ER leads to a reposition-ing of helix 12 which causes a partial occlusion of the coactivator-binding groove [68,69], thus hampering AF2-dependent interactionswith coactivators, and promotes the recruitment of corepressors[108,109]. Therefore, tamoxifen inhibits AF2 activation and blocks thetranscription of genes that depend essentially on AF2 function fortheir expression.
The agonistic properties of SERMs depend largely on AF1[74,107,110] and consequently SERMs act as agonists in contextswhere the AF1 activity is strong [66,111]. For this reason the agonistic/antagonistic effect of tamoxifen in different tissues is largely due tothe relative expression of AF1- or AF2-dependent genes. The nature of
AF1 activation by tamoxifen is unclear but it may involve phosphor-ylations of ER and recruitment of coactivators similar to estrogen [78].
The tissue-dependent effect of tamoxifen is also related to thedifferent cellular availability of coactivators and corepressors[112,113]. For example, tamoxifen exhibits marked agonistic activityin several endometrial cell lines where the coactivator SRC-1 isexpressed at high levels. However it behaves as antagonist inmammary cells with a similar coregulator expression profile, exceptfor low levels of SRC-1 [114]. Remarkably, mammary cells transfectedwith SRC-1 are stimulated by tamoxifen whereas endometrial cellssilenced for SRC-1 expression loose the tamoxifen-agonistic activity[114], indicating that SRC-1 is required for tamoxifen agonism. It hasbeen observed that SRC-1-mediated agonistic effect of tamoxifeninvolves genes whose promoters do not contain a classical ERE [114]and depends largely on a direct interaction of SRC-1 with AF1 [84,110].Recently it has been reported that the AF1 agonistic activity oftamoxifen can be promoted also by a direct binding of coactivators tothe AF2 region [115]. In particular, tamoxifen induces a physical andfunctional interaction of the coactivator PGC-1βwith AF2. PGC-1β canalso bind SRC-1 and the simultaneous interaction of SRC-1 with AF1creates a molecular bridge between AF1 and AF2 responsible for AF1activation [115]. In this way specific AF2 coactivators, such as PGC-1β,may recognize and bind the ER/tamoxifen complex thereby con-tributing to the agonistic properties of tamoxifen.
The agonistic/antagonistic activity of tamoxifen has been studiedextensively, by transient transfection of cells with plasmids containingthe estrogen-sensitive promoter region fused with a reporter gene(chloramphenicol acetyltransferase assay, luciferase assay) and mea-surement of the resulting enzyme activity. These experiments haveshown that on ERE regulated genes, in which estrogen is agonist withboth ER subtypes [116], tamoxifen has agonistic or antagonistic effect,depending on the cellular context [117]. Intriguingly, on AP-1regulated genes in which estrogen is agonist through ER-α, butantagonist through ER-β, tamoxifen behaves largely as an agonist andindependently of ER subtypes [54,88,118]. Similar observations havebeen made for the non-classical SP-1 pathway [56,119]. Therefore, it isnot surprising that endometrial cells exhibiting very active non-classical pathway are stimulated by tamoxifen, whereas in ER-positivebreast cancer cells which show a minimal active non-classicalpathway tamoxifen functions as a pure antagonist [120].
In addition to the genomic effects tamoxifen also influences thenon-genomic ER pathway acting as agonist [97,98]. This effect is notrelevant in breast cancer cells that possess low levels of membrane ERand inwhich receptor tyrosine kinases (RTKs), such as EGFR or humanepidermal growth factor-2 (HER2) are poorly expressed [98]. On thecontrary, in tumor cells expressing abundant EGFR, HER2, orcoregulatory proteins able to sequester ER outside the nucleus suchasMTA1s and PELP1, theMISS pathway contributesmore substantiallyto cell growth. In this milieu, the agonistic effect of tamoxifen becomesrelevant and can explain the observed cellular resistance to thiscompound [96,98,101]. For this reason, estrogen-deprivation therapywith AIs, shutting off both the NISS and MISS activities of ER, might bemore effective than tamoxifen in HER2 amplified tumors.
In summary, tamoxifen is an anti-estrogen for those cells in whichthe prevalent estrogen-driven gene transcription is mediated by ERAF2 activity, whereas it behaves as partial agonist when estrogeneffect depend on AF1, non-classical pathway or MISS pathway.
3.2. Aromatase inhibitors (AIs)
Estrogen is produced, besides in the ovaries, also in extra-ovariantissues, especially peripheral adipose tissue [121] by cytochrome p-450 aromatase (CYP19). This enzyme converts androstenedione andtestosterone produced by the adrenal gland to estrone and estradiol,respectively. AIs block the aromatase enzyme and thus decreaseestrogen levels. This effect is more relevant in post-menopausal

67M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
women inwhom estrogen production occurs essentially by peripheralaromatization of androgens.
Two classes of AIs are currently in clinical use: steroidal, e.g.exemestane, that binds the enzyme irreversibly, and non-steroidal,e.g. anastrozole and letrozole, which block the enzyme reversibly[122]. These third-generation AIs have greater potency, specificity andreduced side effects compared with first and second-generationcompounds, such as aminoglutethimide and formestane and thereforeare increasingly used in the hormonal treatment of post-menopausalwomen with ER-positive breast cancer.
3.3. Selective ER down-regulators (SERDs)
Fulvestrant, the prototype of SERDs, is a 7-alkylsulphinyl analogueof 17β-estradiol and structurally distinct from SERMs [123]. Theunique C7 side chain of fulvestrant is crucial for its mode of action andis responsible for its pure antagonistic activity [124]. Like estrogen andtamoxifen, fulvestrant binds the ER LBD though because of the longbulky side chains at the 7α position it induces a distinct conforma-tional change of the pocket [125], specifically in the position of helix12, hampering receptor dimerization and binding to DNA [126]. Thereis evidence that in the presence of fulvestrant, ER nuclear localizationis disrupted with increased ER degradation [127]. This processinvolves the ubiquitin–proteasome pathway [127]. It has beenreported that fulvestrant induces helix 12 of ER to interact withcytokeratins CK8/CK18, members of the nuclear matrix intermediatefilament, drawing the receptor into close proximity to nuclear matrix-associated proteasomes for subsequent degradation [128]. Interest-ingly enough, point mutations into helix 12 and decreased levels ofCK8/CK18 disrupt fulvestrant-mediated ER degradation [128] that isessential for the anti-proliferative activity of this anti-estrogen [129].Moreover, no interaction between ERβ and either CK8 or CK18 wasobserved after fulvestrant treatment [128], and this may play a role inthe inability of fulvestrant to degrade this ER isoform [130].
The ER down-regulation, observed in the presence of SERDs,completely inhibits ER-mediated gene transcription, inactivating bothAF1 and AF2 [131].
4. Mechanisms of endocrine resistance
The mechanisms responsible for resistance to endocrine therapymay be common to all three classes of drugs (SERMs, AIs, SERDs) ormay be specific for a particular agent (Table 1). These mechanisms canbe encompassed into three main categories: (i) modifications ofestrogen receptor status; (ii) alterations of the intracellular molecularmilieu; (iii) anomalies in the metabolism of endocrine agents.
4.1. Estrogen receptor status
4.1.1. Loss of expression of ERαObviously, any anti-estrogen therapy can be effective only in
cancer cells that are dependent on ER activation to maintain their
Table 1Molecular mechanisms of resistance to different endocrine treatments in breast cancer
Mechanisms of resistance SERMs AIs SERDs
Loss of ERα X X XMutated ERα XERβ expression XLack of PR XDrug metabolism XCoA/CoR expression XIncreased GF signaling X X XIncreased ER sensitivity X
Abbreviations: SERMs, selective estrogen receptor modulators; AIs, aromatase inhi-bitors; SERDs, selective estrogen receptor down-regulators; ER, estrogen receptor; PR,progesterone receptor; CoR, corepressor; GF, growth factor.
growth and proliferation. Therefore, the expression of ER is the mainpredictor of response to endocrine therapy and the lack of ER is themain mechanism of de novo resistance to endocrine therapy.
In a significant fraction of breast cancers, the absence of ER-geneexpression has been associated with aberrant methylation of CpGislands, located in the 5′ regulatory regions of the ERα gene [132,133].However, up to 35% of ER/PR-positive tumors also exhibit substantialER-gene methylation, suggesting that methylation alone does notdetermine ER expression [134]. An alternative explanation for the lossof ER expression is represented by an increased deacetylation ofhistones, that results in a more compact nucleosome structure thatlimits transcription [133,135]. The inhibition of HDAC, the enzymeresponsible for histone deacetylation, is able to restore ER expressionin ER-negative human breast cancer lines without a concomitantdemethylation of the CpG island in the promoter [136]. It is importantthat an increase in ER expression by a combination of a HDAC inhibitorand a DNA methyltransferase-1 (DNMT1) inhibitor is able to restoretamoxifen sensitivity in ER-negative breast cancer cells MDA-MB-435,both in vitro and in vivo [137]. Therefore, HDAC and DNMT1 may bepotential targets for therapeutic intervention in the treatment of asubset of ER-negative breast cancers.
Generally, ER-negative breast cancers have higher expression ofEGFR and HER2 compared with ER-positive tumors [138]. Evidencesuggests that activation of growth factor signaling might reduce ERexpression and/or function [139]. For example, in MCF-7 cells, an ER-positive human breast cancer cell line, treatment with EGF reduces ERexpression by increasing signaling through EGFR, PI3K/AKT and PKC[140]. Therefore, growth factor signaling might contribute to thetranscriptional repression of ER gene, resulting in endocrine resis-tance. However, in tumor cells expressing ER, activation of growthfactor pathways can potentiate ER signaling (see below).
It has been hypothesized that loss of ER expression might beresponsible for acquired resistance to tamoxifen. However, only 17–28% of tumors with acquired resistance to tamoxifen do not express ER[141,142], and approximately 20% of tamoxifen-resistant tumors willeventually respond to second-line treatment with AIs or fulvestrant[8,143]. These observations imply that patients with acquiredresistance to tamoxifen might have tumors still expressing ER andtherefore, a benefit from other endocrine agents. As will be describedlater, tamoxifen resistance mostly relies on a complex network ofintracellular kinase signaling that augments its agonistic activity.
On the other hand, the loss of ER expression is the mainmechanism of acquired resistance to fulvestrant. For example, MCF-7 cells becoming resistant to this drug irreversibly loss ER [144],although in an early phase the loss is reversible upon removal of thedrug [145]. In the absence of ER the growth of fulvestrant-resistantcells is promoted primarily via increased EGFR/MAPK signaling[144,145]. Similarly, in tamoxifen-resistant HER2 transfected MCF-7cells (MCF-7/HER2/neu-18), resistance to estrogen deprivation andfulvestrant is accompanied by a loss of ER and an increase of HER2 andMAPK activation [146]. In contrast, wild-type MCF-7 cells, whichexpress low levels of HER2, become resistant to estrogen deprivationthrough a mechanism of receptor hypersensitivity (see below) withincreased ER expression and MAPK activation [147]. These observa-tions could be clinically relevant in breast cancer progressing on AIs:HER2-positive tumors are likely resistant to any other endocrinemanipulation, including fulvestrant, because of ER loss; whereas,HER2-negative tumors might be sensitive to fulvestrant since ERpathway is still active.
Thus, ER expression in the tumor should be reassessed during thecourse of the disease in order to select themost appropriate therapy ateach time.
Whether ER loss is due to a selection of ER-negative tumor cellclones from a heterogeneous population of cells, or to a reduced ERexpression/increased ER degradation in initially ER-positive cells, iscurrently unknown [132,146,148,149].

Fig. 3. Autocrine signaling loop limiting the anti-proliferative effect of endocrinetherapy. Since estrogen-activated ER down-regulates the transcription of EGFR andHER2 genes, anti-estrogen agents determine an increase of EGFR/HER2 expression.These receptor tyrosine kinases activate the downstream MAPK/AKT cascade which, inturn, phosphorylates and activates nuclear ER, counteracting the inhibitory effect of theanti-hormonal therapy. As a consequence, the persistent ER activation leads to thetranscription of ER-sensitive genes, including amphiregulin, a growth factor able to bindand activate EGFR. In this way, an autocrine proliferative loop is established.
68 M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
4.1.2. Mutations of ERαMutation of ER might affect the response to anti-estrogens. For
example, in tamoxifen-resistant MCF-7 xenografts, a point mutationthat causes a tyrosine for aspartate substitution at amino-acid 351(D351Y) in the ligand-binding domain of ER has been described [150].Similarly, co-expression of wild-type ER along with an ER variantlacking exon 5 within the LBD and unable to bind estrogen, confersresistance to tamoxifen [151].
It should be considered that mutations of ER occur in less than 1%of human breast cancers [152], and therefore they are not likely tocontribute significantly to the resistance to tamoxifen and more ingeneral to SERMs. A single amino-acid substitution, changing lysine303 to arginine, has been detected in 20 of 59 hyperplastic breastlesions [153]. This mutation produces an enhanced ER-mediated cellgrowth by increasing ER sensitivity to estrogen and altering the cross-talk between ER and various cellular pathways that normally down-regulate ER signaling [153]. Theoretically, such loss of regulation couldcontribute to the development of endocrine resistance, but no clinicalevidence has been reported thus far.
4.1.3. Altered expression of ERβERβ has a negative influence on ERα-promoted transcription
[87] and its expression has been reported to be associated with abetter prognosis in breast cancer patients [42]. In addition, ERβexpression and/or activity might be implicated in the resistance toSERMs. For example, high levels of ERβ have been observed intamoxifen-resistant breast cancer cells [154] probably due to anincrease of AP-1-dependent gene transcription triggered by ERβ inthe presence of tamoxifen [88]. However, other studies reported lowlevels of ERβ to be predictive of tamoxifen resistance [155,156]. Asseen in ERα, the loss of ERβ expression in breast cancer is fre-quently related to hypermethylation of CpG islands in the genepromoter [157].
Given the incongruent results, no conclusion on the role of ERβ inthemechanism of resistance to endocrine therapy can be drawn at thistime. The methodology to assess ERβ and its splicing variants, patientselection criteria and the small number of patients analyzed, couldexplain these controversial results. Therefore, in order to verify therole of ERβ expression on endocrine responsiveness in breast cancerwill likely require large-scale clinical trials.
4.2. Intracellular milieu
4.2.1. Altered expression of coregulatorsIt is known that coregulatory proteins can significantly influence
ER-mediated transcription [70]. Moreover, sincemany of thesemay bepresent at rate-limiting levels in the nucleus, changes in their level ofexpression and/or activity can lead to alterations of ER signaling. Inparticular, overexpression of coactivators and/or down-regulation ofcorepressors can abrogate the effects of endocrine therapy, especiallyin the case of SERMs [110]. To this regard, a retrospective study hasshown that patients with tumors overexpressing AIB1 along withHER2 and receiving adjuvant tamoxifen displayed a shorter 5-yeardisease free survival, as compared to patients with tumors over-expressing only one or none of these two molecules [158]. Amongpatients with elevated HER2 expression, those with low AIB1 had amore favorable prognosis. Recent results extend above data byshowing that AIB1 expression is a highly significant marker of relapseand death of tamoxifen-treated patients with HER3-overexpressingtumors [159]. This provides clinical evidence to suggest a cross-talkbetween ERα and growth factor receptor pathways through changes inexpression and activity of specific coactivator proteins, such as AIB1. Infact, signaling through the HER receptor pathways activates AIB1 byphosphorylation at six different phosphorylation sites [160] andtherefore, tumors with high levels of both AIB1 and HER receptors(HER2 or HER3) are less responsive to tamoxifen therapy probably
because of increased estrogen agonistic activity of tamoxifen-boundER.
Similarly, resistance is seen when cells express low levels of ERcorepressors. In vitro studies have established that the corepressorNCOR1 binds ER and inhibits the partial agonistic activity of tamoxifen[161]. Importantly, low expression of NCOR1 is associated withsignificantly shorter relapse-free survival in tamoxifen-treatedpatients [162]. Therefore, evaluation of NCOR1 expression mayrepresent an important new tool in predicting tamoxifen resistance.
4.2.2. Increased growth factor signalingEstrogen is a positive regulator of cell-cycle and physiologically
determines a negative feed-back to control cell growth by down-regulating genes involved in proliferation, such as EGFR/HER2 (Fig. 3)[163]. For this reason, anti-hormonal agents, which impede estrogeneffect, unleash EGFR/HER2 expression. These RTKs are responsible fora persistent ER nuclear activity, through the activation of MAPK andAKT signaling that phosphorylates ER at Ser118 and Ser167 [164]. Theconsequent increased expression of ER-sensitive genes, in particularthe EGFR ligand amphiregulin, creates a short circuit that maintainscell growth and proliferation during endocrine therapies [165]. In thisway the expression of estrogen-repressed survival/proliferation genes(EGFR/HER2) becomes a factor limiting the efficacy of hormonaltherapy (Fig. 3) [164]. Notably, ER activity is to be considered within acomplex system of interlocking intracellular signal transductionpathways. In fact, membrane ER can activate HER2 signaling and inturn the kinase cascade downstream of HER2 can phosphorylate andactivate ER and its coregulatory proteins [98], determining anamplification of the proliferative signaling. Tamoxifen stimulatesthis cross-talk through an agonistic effect on membrane ER thatresults in further activation of EGFR/HER2 pathway [97,98]. Intamoxifen-resistant breast cancer cells an increased non-genomicfunction of ER via cooperation with EGFR pathway has been reported[166]. This event seems to be related to a redistribution of the ER fromthe nucleus to the cytoplasm and plasma membrane resulting in anenhancement of its interaction with EGFR [166].
The acquired resistance to tamoxifen has been also associated withan increased transcription of estrogen-sensitive genes via AP-1 sites,presumably due to tamoxifen-liganded ER agonistic activity [167]. Thep38 MAPK is a major upstream modulator of AP-1 transcriptionalactivity and may potentiate the agonistic effects of tamoxifen at AP-1[118].

Fig. 4. Ability of breast tumor cells overexpressing growth factor receptors (GFR) to overcome tamoxifen growth inhibition. The overexpression of GFR and the cross-talk betweenmembrane ER and GFR are responsible for an overwhelming MISS activity of ER in the presence of tamoxifen. The subsequent increase of MAPK/AKT signaling cascade determinesphosphorylation of coregulatory proteins which are responsible for the estrogen-like effect of tamoxifen in the nucleus. In this milieu, ER recruits coactivators (CoA) rather thancorepressor (CoR) to the DNA-binding complex. In this phase, tumor cells are still sensitive to aromatase inhibitors (AIs) or fulvestrant (F) that are able to inhibit the established ER/GFR cross-talk by blocking both MISS and NISS activities.
69M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
An involvement of HER2 in the de novo resistance of breast cancercells to tamoxifen has long been hypothesized [168]. In BT474 HER2-overexpressing breast cancer cells, HER2 signaling has been shown toinduce resistance to tamoxifen by inhibiting its pro-apoptotic effect[169]. The growth stimulatory effect of tamoxifen has also beenobserved in HER2-overexpressing MCF-7/HER2-18 cells, a valid in vitromodel of de novo tamoxifen resistance [98]. In these HER2-positivebreast cancer cell lines, both estrogen and tamoxifen activate themembrane ER, which in turn triggers EGFR/HER2 signaling. The EGFR/HER2 downstream kinases, p42/44 MAPK and AKT, phosphorylate and
Fig. 5.Overexpression of growth factor receptors (GFRs) causes endocrine resistance throughestrogen inhibition is to continue utilizing the ERmachinery for gene transcription, initially, iactivation of coactivators (CoA), in which tamoxifen (T) acts as agonist (A), and, later, in a ligathe absence of ligand (estrogen or tamoxifen) (B). Sustained growth factor signaling promot(TFs), including NFkB and myc, able to maintain gene transcription for cell proliferation (C)
functionally activate both nuclear ER and its coactivator AIB1 [98]. Inthis molecular milieu, the nuclear tamoxifen–ER complex is able torecruit coactivators rather than corepressors, resulting in enhancedexpression of estrogen-regulated genes (Figs. 4 and 5A). This ability iscompletely reversed by the addition of gefitinib, an EGFR tyrosinekinase inhibitor which can block signaling from EGFR/HER2 hetero-dimers, suggesting that this pathway is directly involved in the growth-promoting activity of tamoxifen in HER2-overexpressing cells [98].
Differently from tamoxifen, estrogen deprivation strikingly inhi-bits the growth of HER2-overexpressing MCF-7 cells (MCF-7/HER2-
differentmechanisms. The energetically more convenient way the cell uses to overcomen a ligand-dependent manner, creating amolecular milieu, e.g. phosphorylations (P) andnd-independent manner, making critical phosphorylations (P) that enable ER to work ines ER loss and ER-independent growth, with activation of different transcription factors.

70 M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
18). This latter evidence suggests that in patients with ER-positive,HER2 overexpressing tumors, AIs might represent a more effectivetherapeutic option than tamoxifen. This hypothesis is supported byresults of clinical trials [170,171].
The increased EGFR/HER2 signaling is also involved in acquiredresistance to tamoxifen [142,172]. In wild-type MCF-7 cells, thedevelopment of resistance to this agent is associated with increasedexpression of EGFR and HER2, activation of EGFR/HER2 heterodimersand phosphorylation of MAPK, AKTand nuclear ER on Ser118 and Ser167
[165,172,173]. In these cells tamoxifen enhances the ER-driventranscription of TGFα and amphiregulin, which in turn activateEGFR, thus sustaining an autocrine loop responsible for cell growth[172]. Recent evidence suggests a role for IGF-IR signaling in tamoxifenresistance. Thus, in tamoxifen-resistant breast cancer cells, the IGF-IIplays a crucial role in regulating basal EGFR/MAPK signaling and cellproliferation [174].
In conclusion, in ER-positive cells with de novo or acquiredresistance to tamoxifen, overexpression or hyperactivation of RTKsturns the normal molecular cross-talk between ER and GFRs into avicious circle responsible for cell proliferation and involving genomicand non-genomic ER activities. For these reasons, AIs and fulvestrant,endocrine agents able to inhibit both ER activities, are still effective inpatients with ER-positive, HER2-overexpressing tumors [170] (Fig. 4).Unfortunately tumors also become eventually resistant to estrogenwithdrawal, since tumor cells develop the ability to use differentgrowth factor signaling pathways which initially activate ER in theabsence of estrogen (estrogen-independent, but ER-dependent cells)[144,175,176] (Fig. 5B) and finally induce estrogen-sensitive genes inan ER-independent manner (estrogen- and ER-independent cells)[140,177] (Fig. 5C). At this phase when tumors are composedpredominantly, if not entirely, by ER-negative GFR-overexpressingcells, they are resistant even to SERDs. In these cells the estrogen-induced pathways become completely useless: GFRs, via MAPK andPI3-kinase signaling are able to activate different transcription factors(e.g. NFkB) [178] that induce, in an ER-independent manner, theexpression of the same genes critical for cell proliferation (e.g. cyclinD1 and c-myc) [179] (Fig. 5C).
Recently it has been found that exemestane-resistant breast cancercells express a high level of amphiregulin that is responsible for cellproliferation through the EGFR/MAPK pathway [176]. Interestingly,exposure of cells to exemestane induces amphiregulin expression inan ER-dependent manner [176].
Therefore, GFRs play central roles in resistance to various endo-crine therapies, such as AIs and fulvestrant, in addition to tamoxifen[144–146].
4.2.3. Estrogen hypersensitivity and supersensitivityA major mechanism by which breast cancer cells become resistant
to endocrine therapy is the acquisition of an increased sensitivity toestrogen (hypersensitivity), i.e. the ability to growth in the presence oflow levels of estrogen. The adaptation to estrogen withdrawal in vitromimics the resistance to AIs in vivo [180]. To study the molecularchanges associated with estrogen deprivation, a model has beendeveloped by culturing estrogen-dependent, ER-positive MCF-7 cellsin estrogen-freemedium (LTED, long-term estrogen-deprivation cells)[181]. These cells grow in estrogen concentrations four-log lower thanthat needed by wild-type MCF-7 cells (10−13 versus 10−9 M) [182] andexpress 4 to 10-fold increased ER levels as compared to wild-typeMCF-7 cells.
The ability of LTED cells to grow in the presence of very lowestrogen concentrations has been attributed to an increased utiliza-tion of MISS, rather than NISS, ER pathway [182], able to rapidlytrigger GFR signaling [181]. It has been reported that an up-regulationof the cross-talk between IGFR1 and ER induces the activation ofMAPK and PI3K/AKT, responsible for the estrogen hypersensitivitystatus of LTED cells [182]. Estradiol was shown to stimulate the
adaptor protein Shc, a key modulator of several RTKs, and to increaseMAPK phosphorylation in a time- and dose-dependent manner [182].Interestingly these events were blocked by fulvestrant, indicating thatER is a key upstream component of MAPK activation in LTED cells[181]. However, MAPK does not appear to be the only intracellularsignaling pathway involved in the growth of LTED cells, since MAPKinhibitors are unable to fully block the estrogen hypersensitivity status[183]. On the contrary, dual-inhibition of MAPK and PI3K, with U0126and LY294002 respectively, is able to completely reverse estrogenhypersensitivity [183].
In another LTEDmodel, MCF-7 cells, maintained in culturemediumdeprived of estrogen for over 80 weeks, switched from a hypersensi-tive phase (cell growth stimulated by very low estrogen concentra-tions) to an apparent estrogen-independent phase (LTED-I) in whichestrogen no longer affected their growth [184]. The exclusion ofinsulin from the culture medium surprisingly decreased cell growthbut restored estrogen sensitiveness, suggesting that LTED-I cells werenot estrogen-independent but super-sensitized to trace amounts ofresidual estrogen [185]. In LTED-I cells, ER-ERE transcriptional activitywas 7 to 10 times higher than that of wild-type MCF-7. Although p42/p44 MAPK and PI3K in LTED-I cells were functionally active (in partdue to HER2 overexpression) their specific inhibition by U0126 andLY294002 had no effect on the basal phosphorylation status of Ser118
and reduced, only in part, cell proliferation and ER-transcriptionalactivity. In contrast, treatment of LTED-I cells with fulvestrantmarkedly inhibited cell growth and ER-ERE transcription, indicatingthat these cells were super-sensitized to residual estrogen in themedium, and that cell growth was mediated by the ER-ERE pathway[185].
It is likely that in LTED-I cells the increased ER-transcriptionalactivity is due not only to the phosphorylation of Ser118, but also to thephosphorylation of other sites, such as Ser167 and Thr311 [77]. Animportant role might be played by the activity of coactivators such asAIB1 [186]. In fact, increased p42/p44 MAPK phosphorylationdetermines the recruitment of AIB1 into the ER-transcriptionalcomplex responsible for enhanced ER-sensitive gene transcription[186,187].
Interestingly, fulvestrant is able to inhibit the proliferation of LTED-I cells but not that of wild-type MCF-7 cells [185,188]. This evidence,translated into clinic, suggests that fulvestrantmight bemore effectivein breast cancer become resistant to AIs than in hormone-responsivedisease [185]. Moreover, since tamoxifen has no inhibitory effect onLTED cells [184], fulvestrant can be considered a more appropriatetreatment following AIs resistance.
In summary, AI resistance appears to be the result of the acquiredability of the cells to become super-sensitized to very low concentra-tions of estrogen. This super-sensitized status is caused by an adaptiveincrease of ER expression and function. Moreover, the increasedexpression of HER2 and IGFR1 promotes activation of MAPK, ERphosphorylation and ERE transcription, suggesting the presence of across-talk between ER and GFRs [189].
4.3. Altered metabolism of endocrine agents
Most of the studies correlating metabolism of endocrine agentswith response to treatment regard tamoxifen.
Tamoxifen undergoes extensive metabolism resulting in two activemetabolites: 4-hydroxytamoxifen (4-OH tamoxifen) and 4-hydroxy-N-desmethyl tamoxifen (endoxifen). The former has been consideredto play an important role in tamoxifen's anticancer effect [190] givenits 100-fold greater affinity for the ER and its 30- to 100-fold greaterpotency in suppressing estrogen-dependent cell proliferation whencompared with the parent drug [191]. However, endoxifen is moreimportant than 4-OH tamoxifen in terms of the relative contributionto the overall anticancer activity of tamoxifen. Endoxifen has identicalproperties and potency compared with 4-OH tamoxifen in terms of its

Table 2Choice of endocrine therapy after failure of a previous anti-hormonal agent based onpre-clinical and clinical evidence
SERMsfailure
AIs (steroid)failure
AIs (non-steroid)failure
SERDsfailure
SERMs NA − − −AIs (steroid) ++ NA + +AIs (non-steroid) ++ + NA +SERDs ++ ++ ++ NA
NA: not applicable; −: not appropriate; +: good; ++: optional.
71M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
binding affinity to ERs [192], suppression of estradiol-stimulated cellproliferation [193] and gene expression [192]. Furthermore, steady-state plasma endoxifen concentrations are 5- to 10-fold higher than 4-OH tamoxifen [193–195]. Even if themetabolism of tamoxifen to 4-OHtamoxifen is catalyzed by multiple enzymes, endoxifen is formedpredominantly by the CYP2D6 via 4-hydroxylation of N-desmethyltamoxifen, the most abundant tamoxifen metabolite [196]. For thisreason CYP2D6 activity might be responsible for interindividualvariability in response to tamoxifen.
4.3.1. PharmacogenomicsRecent clinical studies have demonstrated that women carrying
genetic variants associated with low or absent CYP2D6 activityhave significantly lower levels of endoxifen during treatment withtamoxifen [194].
By far the most frequent null allele in Caucasians is 2D6⁎4, whichoccurs with a frequency of about 20 to 25% and is responsible for 70 to90% of all “poor metabolizer” [197]. The key mutation is a G to Atransition which causes a shift of the consensus acceptor splice site ofthe third intron by one base, thereby resulting in a spliced mRNAwithone additional base that has an altered reading frame and a prematurestop codon [197]. In Oriental populations, the frequency of the ⁎4allele is only around 1% or less [198].
As a consequence, patients treated with tamoxifen and carrying ahomozygotic CYP2D6 ⁎4/⁎4 genotype, tend to have a higher risk ofdisease recurrence [199]. Similar results have been observed with theCYP2D6 alleles ⁎5, ⁎10, ⁎41, all variants associated with impairedenzyme function [200].
At present however, no prospective trial has been conducted to testthe hypothesis that CYP2D6 genotype can predict outcome. Identify-ing the germline polymorphisms that predict tamoxifen response is apromising field of research but, up to date, the available results are notapplicable into clinical practice.
Contrary to tamoxifen, there is little data correlating alterations inaromatase (CYP19) function and sensitivity to AIs treatment. In aretrospective study including 1975 healthy post-menopausal women,two single-nucleotide polymorphisms (SNPs) of the aromatase gene(rs10046 and [TCT]+/−) were associated with differences in estradiollevels, but no correlations were observed with breast cancer risk[201].
It has been reported that two specific SNPs of aromatase gene,Thr364 and double mutant Arg39Cys264, can affect the activity of theenzyme [202]. Moreover, the double mutant Arg39Cys264 displays asignificant reduced response to exemestane and letrozole comparedwith the wild-type enzyme [202]. However, there is no clinicalevidence to date that genetic variations in CYP19 lead to resistance toaromatase inhibition.
4.3.2. Drug interactionsSome selective serotonin reuptake inhibitors, such as paroxetine
and fluoxetine, commonly prescribed to treat hot flashes in womenreceiving tamoxifen, are known to inhibit CYP2D6 [203]. Therefore,patients receiving paroxetine have a decreased plasma concentra-tion of endoxifen [193] and might have no benefit from tamoxifentreatment.
In fact, a recent study reported that coprescription of CYP2D6inhibitors, in addition to CYP2D6 genetic variation, was an indepen-dent predictor of breast cancer outcome in post-menopausal womenreceiving tamoxifen [204].
5. Optimization of endocrine therapy
Deciphering the molecular mechanisms that underlie endocrineresistance is essential for establishing the most appropriate hormoneagent according to tumor characteristics and for defining the optimalsequence of endocrine therapies (Table 2). Moreover, this knowledge
is critical for development of new therapeutic approaches able todelay or reverse the hormonal resistance in breast cancer patients.
5.1. Sequential or concomitant use of endocrine therapy
Many breast cancer patients fail to respond to any form ofendocrine therapy since the outset of treatment. As the major causeof this phenomenon is the absence of ER expression patients with ER-negative tumors should not be offered endocrine therapy [2]. On theother hand, resistance to SERMs, AIs or SERDs is likely to be mediatedby distinct molecular pathways which explain the lack of cross-resistance between different classes of compounds [205,206]. Oftenpatients whose tumor is resistant to one form of endocrine therapymay still be responsive to other types of endocrine treatment [207].This is of primary importance for the sequential use of endocrineagents.
A common mechanism of resistance to SERMs is the activation ofnon-genomic ER signaling. Thus, in patients whose tumor becomesresistant to tamoxifen, second-line treatment with AIs, shutting offboth the genomic and non-genomic ER activities, represents aneffective therapy as evidenced by several clinical studies both inmetastatic [208,209] and adjuvant setting [210–213].
Clinical experience suggests that while AIs are valid second-lineagents after tamoxifen, the opposite is not true. Second-line treatmentwith fulvestrant (which inhibits both genomic and non-genomiceffects of ER) in tamoxifen-resistant patients is at least as effective asanastrozole [8,143]. It is not yet established which treatment, AIs orfulvestrant, is more appropriate after tamoxifen failure.
The use of AIs after fulvestrant failure and the reverse sequence(fulvestrant after AIs failure) have also been investigated. Data hasbeen presented to show that AIs still retain some activity afterprogression on second-line fulvestrant [214]. This observation is incontrast with pre-clinical findings which indicate that resistance tofulvestrant is associated with ER loss and estrogen independence[144,145]. It is likely that different mechanisms, rather than ER loss,may be responsible for fulvestrant resistance, although no directevidence has been provided as yet. It has been shown that an intactNEDD8 pathway, leading to ER ubiquitination and degradation, isessential for the anti-proliferative activity of fulvestrant and that thedisruption of NEDD8 pathway impairs fulvestrant's ability to degradeER [129]. In this way, tumor cells might be resistant to fulvestrant butmaintain ER expression/activity, thus being sensitive to AIs. On theother hand, the inverse sequence, i.e. the use of fulvestrant after AIfailure, is strongly supported by results from both pre-clinical andclinical studies. A clinical benefit rate of about 30% has been reportedusing fulvestrant in patients with AI-resistant breast cancer [9]. This isconsistent with the hypothesis that LTED cells, an in vitro model of AIresistance, are hyper- or super-sensitized to very low estrogenconcentrations, and that adaptation to estrogen withdrawal isdependent on ER signaling [181,185]. In these cells ligand-indepen-dent activation of ER by growth factor signaling is, at least in part,responsible for resistance to estrogen deprivation.
As above discussed, amplification of growth factor signalingpathways is also involved in the resistance to SERMs, suggestingthat fulvestrant is a more appropriate alternative to tamoxifen

72 M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
following the onset of AI resistance [184]. In patients with metastaticbreast cancer who had progressed after treatment with non-steroidalAIs, the steroidal AI exemestane showed some anti-tumor activity,thus suggesting a lack of cross-resistance between exemestane andnon-steroidal AIs [215]. A recent published randomized clinical trialconcluded that exemestane and fulvestrant are equally active afterfailure of non-steroidal AIs [216].
Classical anticancer drugs are often used in combination in order toincrease cell kill by targeting different mechanisms simultaneously.However, the experience of combining hormonal agents, i.e. tamox-ifen with anastrozole, has been discouraging [217]. Although notcompletely understood yet, the explanation of these negative resultsmay rely on the estrogen agonistic properties of tamoxifen, whichbecome dominant at low estrogen concentrations, preventing the fullestrogen-deprivation effect of AIs. Moreover, concomitant adminis-tration of anastrozole or letrozole with tamoxifen was found todecrease the plasma levels of these AIs by 30–40% and by 20–30%respectively, whereas tamoxifen plasma levels were unaffected[218,219]. Therefore, the currently available clinical [217], experi-mental [220] and pharmacokinetic [218,219] data do not support thegeneral use of concomitant tamoxifen and AIs.
Pre-clinical data has shown that fulvestrant is an effective inhibitorof LTED cell growth and that estradiol at concentration N10−10 Mantagonizes this inhibitory effect [185]. Therefore, fulvestrant may bemore effective in patients who have plasma and/or intratumoral levelsof estrogen below physiological concentrations. On this basis severalclinical trials are currently investigating the use of fulvestrant incombination with AIs in breast cancer therapy either following priornon-steroidal AI treatment or as first-line therapy. In particular, thestudy of Faslodex versus Exemestane with/without Arimidex (SoFEAtrial) randomizes women with ER-positive, locally advanced/meta-static breast cancer failing non-steroidal AIs to receive fulvestrantalone, exemestane alone or the combination of fulvestrant withanastrozole. Another study, the SWOG 226, compares the efficacy of acombination of fulvestrant plus anastrozole with anastrozole alone inthe first-line setting.
An intratumoral aromatase model in rodents, constituted by MCF-7 cells engineered to express aromatase and inoculated intoovariectomized athymicmice, has been developed in order to evaluatethe activity of the association of fulvestrant and AI [221]. It has beenshown that the acquired resistance to anastrozole or fulvestrant wasreversed by combining the two agents rather than switching thetreatments [221]. In this model, the administration of anastrozole plusfulvestrant from the beginning or in sequence was associated with adown-regulation of signaling proteins involved in hormonal resis-tance (IGFRIβ, MAPK, AKT, mTOR, and ERα) compared with tumorstreated with a single agent [221]. These results suggest the possibilityto reverse or delay the development of resistance to AIs by blockingsimultaneously ER and aromatase enzyme in breast cancer patients.
5.2. Predictive factors of endocrine response
Since the introduction of SERMs, the hormonal therapy of breastcancer has been progressing rapidly with the advent of drugs such asAIs and SERDs. The prediction of individual response to thesehormonal agents is critical for an appropriatemanagement of patients.Although the presence of ER in breast cancer tissues is the strongestpredictor of response to all forms of endocrine therapy many patientswith ER-positive tumors do not respond to this type of treatment. Forthis group of patients, HER2, PR and other less known molecules havebeen proposed as predictive factors of endocrine sensitivity.
5.2.1. HER2 statusPre-clinical data supports the hypothesis that SERMs may be less
effective when growth factor signaling pathways are active [98]. Infact, the activation of the PI3K/AKT/mTOR signaling cascade via the
HER family of receptors, activates other cell survival pathways thatprotect breast cancer cells from tamoxifen-induced apoptosis [77].Moreover, HER2 overexpression results in increasedMISS ER activity, apathway in which tamoxifen acts as agonist [169,222]. Bothphenomena are completely reversed by specific EGFR/HER2 inhibi-tors, indicating the presence of an active cross-talk between ER andthe growth factor signaling pathways [98]. These evidences areconsistent with several clinical studies showing that patients withtumors overexpressing HER2 may derive less benefit from adjuvanttamoxifen than those with HER2-negative tumors [223,224]. How-ever, other trials have come to different conclusions [225,226]. Thereason of these incongruent results is probably related to a diversepercentage of patients receiving adjuvant chemotherapy in thedifferent studies. It is likely that the use of chemotherapy may obscurethe interaction between HER2 and tamoxifen.
HER2 overexpression has been also investigated as predictivefactor of AI sensitivity. Experimental studies have shown that humanbreast cancer xenografts overexpressing HER2, which exhibits a denovo resistance to tamoxifen are completely inhibited by estrogenwithdrawal [98]. Consistent with this finding is the observation that,in the neoadjuvant setting tumors overexpressing HER2 show higherresponse rates to AIs as compared to that obtained with tamoxifen[170,227]. The major benefit from AIs over tamoxifen in short-termtreatment (neoadjuvant setting) may not necessarily translate into along-term better outcome (adjuvant setting). In fact, in two recentadjuvant studies HER2 status failed to identify patients withdifferential relative benefit from AI over tamoxifen [228,229].Interestingly, the proliferation marker Ki67, determined before andafter neoadjuvant treatment with either AI or tamoxifen, is notsignificantly reduced by these endocrine therapies in HER2-positivetumors compared with those HER2-negative. This data suggests thatHER2 overexpressing tumor cells, despite an initial better response toneoadjuvant AI, are able to use survival pathways alternative to ER andcan quickly develop an estrogen-independent proliferation, i.e.hormonal resistance to both AI and tamoxifen [230].
In the metastatic setting, a meta-analysis of 12 different studiesinvolving more than 2000 patients concluded that, as compared toHER2-negative, HER2-positive tumors are less responsive to any typeof endocrine treatment. However, the study was not designed to verifyif AIs are better than tamoxifen in patients with HER2-positive tumors[231].
The overall message coming out from pre-clinical and clinicalstudies is that patients with HER2-positive tumors may showresistance to tamoxifen and may be more sensitive to AIs, at least inan initial phase.
Finally, HER2 status has been also evaluated as predictive factor ofresponse to fulvestrant. In a recent prospective analysis it has beenshown that the efficacy of fulvestrant in metastatic breast cancerpatients does not depend on HER2 status [232]. This might be causedby the unique mechanism of action of this agent, able to block nuclearand membrane-bound ER and consequently the above-mentionedcross-talk between ER pathway and growth factor pathways,responsible for the escape from anti-hormone control [232].
5.2.2. PR statusIn patients with metastatic breast cancer, PR expression may
predict response to tamoxifen [233,234]. Increased benefit fromtamoxifen has also been observed in the adjuvant setting, in patientswith PR-positive breast cancer [235]. Moreover, in a large retro-spective meta-analysis including women with early breast cancertreated with tamoxifen patients with ER-positive/PR-positive tumorsshowed a significantly lower relative risk of recurrence and death ascompared with those with ER-positive/PR-negative tumors [236]. Inthis study ER and PR levels in tumor samples were measured in twodifferent central laboratories using identical standardized qualitycontrolled methodology in order to guarantee the accuracy of

73M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
hormonal receptor determination. The Oxford overview does notshow a relationship between PR levels and tamoxifen benefit [2].However, the latter study also failed to show the predictive value of ERin earlier analyses raising questions about the quality of receptorassay.
Interestingly, pre-clinical and clinical evidences suggest that theabsence of PR in ER-positive breast cancer may reflect growth factorsignaling activation [237,238] rather than a non-functional ERsignaling pathway. In breast cancer cells it has been shown thatshort-term treatment (hours) with IGF-1, EGF and heregulin reducesPR expression at transcriptional level, as a result of PI3K/AKT pathwayactivation [238–240]. Growth factor signaling stimulates ligand-independent activation of ER and shifts ER activity from the classicalNISS to a predominantly MISS or non-classical NISS, resulting in theloss of tamoxifen antagonistic effect [171]. In PR-negative tumors theblock of growth factor signaling with targeted agents recovers SERMsensitivity [98,241], indicating that PR-negative phenotype reflectsactivation of growth factor pathways. Tumors with high MISS ERactivity are still highly dependent on estrogen and therefore may besensitive to estrogenwithdrawal therapy [171]. Consistently, the ATACtrial showed that AIs could be superior to tamoxifen in tumorsexpressing ER but not PR [7], supporting the results of other reports[171,233]. However, this observation has not been confirmed by otherstudies [242]. Moreover, when ER/PR status of tumor samples fromthe ATAC trial was centrally reviewed, a greater benefit of anastozolefor ER-positive/PR-negative patients was not evidenced [229]. Finally,in the extended adjuvant MA.17 trial the major benefit from letrozolewas observed in patients with ER-positive/PR-positive tumorscompared to those with ER-positive/PR-negative tumors [243,244].However, the authors recommended caution for clinical decision-making based on these results because the data referred to is a subsetanalysis and hormonal receptors were not measured centrally [243].
Importantly, PR status has been also evaluated as predictive factorof response to fulvestrant. In a recent prospective analysis, PRnegativity does not significantly influence response rate and time todisease progression in metastatic breast cancer patients treated withfulvestrant [232].
Whether loss of expression of PR can predict a poor clinicaloutcome of endocrine therapy remains controversial and needs to befurther investigated. Recently, it has been suggested that PR expres-sion measured by RT-PCR might be a useful prognostic factor in breastcancer [245].
5.2.3. New potential predictive markersIn addition to HER2 and PR, there are other molecules studied as
predictive factors of endocrine response in breast cancer. Theseinclude: VEGF, VEGF receptor (VEGFR), p53, tissue inhibitor metallo-proteinase-3 (TIMP3), cyclin D1, p-21-activated kinase 1 (PAK1),urokinase-type plasminogen activator (uPA) and plasminogen acti-vator inhibitors (PAI-I) [246–252]. Unfortunately, controversial resultshave been obtained and thus far none of the newly proposedpredictive factors can be transferred to the clinical practice.
Results from non-randomized trials of adjuvant tamoxifenrevealed that decreased VEGF expression is predictive of betteroutcome [248,253,254]. On the contrary, VEGF expression showed nopredictive value in patients randomized to two-year adjuvanttamoxifen versus no treatment, while expression of VEGFR2 corre-lated with poor response to tamoxifen [249].
In a retrospective study involving 73 patients with metastaticbreast cancer treated with endocrine therapy at the first relapse, p53cell accumulation predicted resistance to endocrine therapy [250].However, other studies failed to show any predictive role of p53 statusin either metastatic or adjuvant setting [225,226,255].
Another interesting molecule is TIMP-3. This is a unique memberof the metalloproteinase system that is able to inhibit metallopro-teases [256] and to induce cell apoptosis [257]. In breast cancer
patients high tumor levels of TIMP-3 have been reported to correlatewith the success of adjuvant tamoxifen [247]. This is probably due tothe ability of tamoxifen to reduce bcl-2 thus increasing TIMP-3-induced apoptosis [247].
Cyclin D1 is a critical regulator of the cell-cycle promoting G1-Sphase transition after binding to cyclin-dependent kinases (cdk) 4 andcdk6 [258]. In addition to its original role cyclin D1 also affects theactivity of various transcription factors in a cdk-independent manner,including ER [259]. In this respect cyclin D1 interacts with ER andallows recruitment of coactivators to the receptor in the absence ofestrogen [259]. Cyclin D1 overexpression has been associated withimproved breast cancer survival [260]. This beneficial effect has beencorrelated with cyclin D1's ability to repress the anti-apoptotictranscription factor, STAT3. However, two clinical studies have founda strong link between cyclin D1 overexpression and resistance totamoxifen [261,262]. Recent data suggests that in the presence oftamoxifen cyclin D1 binds preferentially to ER rather than to STAT3,increasing cell survival and proliferation [252].
Interestingly, the same chromosomal region of the cyclin D1 gene(11q13) contains PAK1, a gene coding for a protein involved in severalcellular processes, including cytoskeleton reorganization and promo-tion of cell survival. Its amplification, reported in about 15% of breastcancer, has been associated with decreased benefit from adjuvanttamoxifen [251].
The components of the urokinase system, uPA and PAI-1, are wellestablished prognostic factors in breast cancer [263] and have alsobeen studied as predictors of tamoxifen efficacy [246]. In patients withrecurrent breast cancer increased levels of uPA and PAI-1 have beenshown to correlate with a higher probability of tamoxifen failure[246].
Overall, data on new potential predictive factors of endocrineresponse is controversial and does not allow a definitive conclusion.Several methodological problems could explain these conflictingresults, including heterogeneity of the tumor cell population, differentsampling (primary tumor versus metastatic, biopsy versus surgicalspecimen, primary tumor versus post-treatment biopsy), differentdetection methods (amplification versus expression, biochemicalversus immunohistochemical assay) and different cut-off values.
In the last few years the use of microarrays for gene profiling hasprovided a refined molecular classification of human breast cancer[264]. Gene expression studies have consistently confirmed theheterogeneity of breast cancer, providing new insights into themechanisms of resistance to endocrine therapy. A microarrayapproach was used to identify DNA methylation markers in apopulation of 278 ER-positive, node-negative breast cancer patientstreated with tamoxifen. The combination of tumor grade, tumor size,ER expression levels and DNA methylation identified a subgroup ofpatients with excellent outcome after tamoxifen treatment (DFS 95%at 10 years versus 62% in the poor prognosis group) [265].
Current research efforts are directed at the discovery of specificgene profiles, referred to as “molecular signatures” that could, identifypatients likely to respond to endocrine therapy.
Using paraffin-embedded tumor samples from node-negative ER-positive breast cancer patients a recurrence-score (Oncotype DX™)has been identified and validated by the evaluation of 21 genesthrough RT-PCR [266]. Oncotype DX™ seems to accurately identify agroup of patients with excellent prognosis when treated withadjuvant tamoxifen. Additionally, a simple two-gene expressionratio between the Homeobox B13 gene (HOXB13) and the Interleukin17B receptor (IL17BR) has been evaluated in patients with ER-positivebreast cancer at risk for tumor recurrence after adjuvant tamoxifen. Inparticular a high HOXB13/IL17BR expression ratio was found to bepredictive of disease recurrence in a multivariate analysis [267].Another gene expression profile has been developed to predictresponse to tamoxifen in patients with metastatic disease [268].This signature, based on the differential expression of 81 genes in the

74 M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
primary tumor, was able to discriminate between tamoxifen-respon-sive and -resistant tumors [268].
The use of in vitro cell-based large-scale genetic screens aimed atevaluating gain- or loss-of-function of specific genes, has also yieldedinsights into the mechanisms of tamoxifen resistance. This approach,which allows the establishment of functional relationships betweengenotype and occurrence of endocrine resistance, provides anindication on the relevant genes to be clinically validated. Forexample, a gain-of-function approach utilizing retroviral cDNAlibraries, has demonstrated that fibroblast growth factor (FGF) 17overexpression causes tamoxifen resistance in vitro [269]. Thisprompted to investigate the FGF pathway (FGF17 and the receptorsFGFR1–4) for the response to tamoxifen in patients with recurrentbreast cancer [270]. In these patients, high mRNA FGFR4 expressionwas predictive of poor response to tamoxifen and shorter progression-free survival [270]. Similarly, using a loss-of-function approach (iRNAscreen), CDK10 has been identified as a modifier of tamoxifensensitivity [271]. In fact, CDK10 silencing increased ETS2-driventranscription of c-RAF, resulting in MAPK pathway activation andloss of tumor cell reliance upon estrogen signaling. Patients withtumors expressing low levels of CDK10 relapse early on tamoxifen[271].
The high-throughput techniques have raised great hope for abetter understanding of tumor biology and the mechanisms under-lying resistance to endocrine therapy but, at the moment, the lack ofreproducibility in different centers is a large limitation to their clinicalapplication. However, it is likely in the near future that thestandardization of the procedures will allow to identify key moleculesinvolved in endocrine resistance of breast cancer and to predictresponse to a specific anti-hormonal agent. This knowledge will helpin the choice of individualized treatment and will be the bases for thedevelopment of new molecularly targeted agents.
6. Overcoming endocrine resistance by signal transductioninhibitors (STIs)
As discussed above, during endocrine therapy the up-regulation ofgrowth factor signaling is the most important adaptative molecularchange that occurs in breast cancer cells and which eventuallydetermines endocrine resistance [165,241,272,273]. For this reason,the combination of anti-hormonal agents with different growth factorsignaling inhibitors (e.g. anti-HER2, anti-EGFR or anti-Ras signaling)may be effective in preventing endocrine resistance and restoringresponsiveness [273–275].
Several studies have used STIs to prevent the onset of resistanceduring hormonal treatment. In ER-positive human breast cancer cells,tamoxifen or AIs synergize with farnesyl transferase inhibitors (FTIs)in inhibiting cell growth and enhancing cell death [276]. In an in vitrostudy gefitinib in combinationwith tamoxifen or fulvestrant promotesan anti-proliferative and pro-apoptotic effect higher than thatachieved with either drug alone [164]. In particular, the two-agentcombinationwas able to prevent the activation of EGFR/p42/44 MAPKsignaling and significantly delayed the development of tamoxifenresistance [164].
STIs might also have a role in the treatment of hormone-resistantbreast cancer. In HER2-overexpressing MCF-7 cells (MCF-7/HER2-18),treatment with gefitinib eliminates tamoxifen-agonistic activity andrestores its anti-tumor effect, both in vitro and in vivo [98]. Likewise,the enhanced ER-mediated gene transcription observed in LTED cellscan be abrogated by agents able to interrupt upstream signaling,including gefitinib and the MAPK-inhibitor UO126 [185]. Anotherimportant pathway involved in hormone-resistant breast cancer isPI3K/AKT pathway [277]. In response to different growth factors (EGF,VEGF, IGF-1, heregulin) PI3K activates AKT, which promotes cellsurvival through phosphorylation of substrates involved in theapoptotic machinery, such as Bad and caspase 9 [277]. The PI3K/AKT
signaling pathway also regulates the G1/S transition of cell-cycle byactivating mTOR, that regulates p70S6 kinase and 4E-binding protein-1 [278,279]. This cell survival pathway can be abrogated by the specificPI3K inhibitor LY294002, and by mTOR inhibitors, such as temsir-olimus (CCI-779) or everolimus (RAD-001) [278]. The relevance of aPI3K/AKT pathway in the hormone-resistant phenotype is empha-sized by the evidence that MCF-7 cells, transfected to produce aconstitutively active AKT, proliferate under reduced estrogen concen-trations and are resistant to the growth inhibitory effects of tamoxifen[278]. Treatment of these cells with temsirolimus restores sensitivityto tamoxifen, that suggests that AKT-induced tamoxifen resistancemay bemediated by signaling throughmTOR pathway [278]. Recently,the dual EGFR/HER2 inhibitor lapatinib has been shown to cooperatewith tamoxifen in determining a more rapid and profound cell-cyclearrest than that observed when either agent alone in hormone-resistant cells is used [280]. When used in combination the two drugscaused a greater reduction of cyclin D1, an increase of p27 kinaseinhibitor and a greater inhibition of cyclin E-cdk2 [280], all of whichare molecular changes associated with cell growth inhibition.
Finally, data from two different HER2-overexpressing ER-positivebreast cancer xenograft models (MCF-7/HER2-18 and BT474 cells)indicates that tamoxifen or estrogen deprivation is more active in thepresence of a complete blockade of all HER dimer pairs, achieved bycombining pertuzumab, trastuzumab, and gefitinib, rather than in thepresence of a single HER inhibitor [281]. This suggests that tumor cellscan escape the block of a single HER dimer pathway using analternative HER signaling and therefore, the best anti-tumor effect ofendocrine therapy might be reached if it is used in combinationwith aHER-inhibitor “cocktail” [281].
The above pre-clinical findings provided a strong rationale for thedevelopment of clinical trials in which endocrine therapy is combinedwith STIs in patients with ER-positive breast cancer. These trials, mostof which are ongoing, use combinations of inhibitors of HER2, EGFR,farnesyl transferase, mTOR, with either tamoxifen, AIs or fulvestrant[275]. Even if metabolic drug–drug interaction might be a concern inthese studies, thus far no clinically relevant pharmacokinetic altera-tion has been reported. For example, co-administration of lapatiniband letrozole might potentially alter the metabolism of either drug,since lapatinib inhibits CYP3A4 and letrozole is a substrate of thisenzyme. However, a recent phase I study on lapatinib plus letrozoleindicates that the combination of these two drugs is safe, does notresult in a pharmacokinetic interaction, and has clinical activity [282].
A careful selection of patients, along with sequential tumorbiopsies during therapy will help to identify the most relevantmolecular target associated with endocrine sensitivity and resistance.
7. Conclusions
In ER-positive breast cancer cell growth and proliferation is largelymaintained by active transcription of estrogen-sensitive genes.Therefore, therapies blocking ER signaling are widely used to inhibitthe transcription of these genes and to disrupt breast cancer growth.
The idea that estrogen binding to ER, by itself, can entirely mediateestrogen-target gene transcription is an oversimplification. In fact,recent progress in understanding ER biology and function hasrevealed a complex signaling interaction between ER and other signaltransduction pathways, mainly triggered by EGFR, HER2 and IGFR. Inaddition, ER function is critically influenced by the expression andactivity of coregulatory proteins.
The resistance to all forms of endocrine therapy remains a majorproblem in the management of hormone-sensitive breast tumors.Distinct molecular mechanisms seem to be involved in the therapeuticfailure of SERMs, AIs or SERDs, consistent with the reported lack ofcross-resistance among different anti-hormones [205,206,214,215].The main cause of primary endocrine resistance is the absence of ERexpression and therefore, patients with ER-negative tumors should

75M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
not be offered any form of endocrine therapy. Other molecularmechanisms bywhich breast cancer cells can escape hormonal controlinclude: mutations of ER, altered expression of ERβ, alterations in theexpression/activity of coactivators/corepressors, hyperactivity of GFsignaling pathways, modifications in the metabolism of endocrineagents, and, finally, loss of ER expression.
Up-regulation of GFRs is responsible for resistance to variousendocrine approaches [144–146] in different ways, depending on theagent, the time of exposure, and the constitutive molecular char-acteristics of tumor cells. In the presence of GFR hyperactivity there isa time-dependent molecular adaptation of cells to the long-lastingimpaired estrogen signaling. Initially, GFR signaling increases ERactivity and through its bidirectional cross-talk with ER creates amolecular milieu (phosphorylations of ER and its coactivators) inwhich tamoxifen acts as an agonist. Later, sustained growth factorsignaling activity leads to critical phosphorylations on ER that inducetranscription of estrogen-sensitive genes in a ligand-independentmanner. Finally, GFR signaling is able to activate estrogen-sensitivegenes in ER-independent manner and this is associated with ER loss.At this final phase tumors become resistant even to SERDs (Fig. 5).
The knowledge of the specific molecular mechanisms of resistanceto each endocrine agent is crucial for defining the optimal timing andsequence of their administration. Literature data described hereinsuggests that a reasonable modality of using the available endocrineagents could be to start with tamoxifen, particularly if the tumor doesnot express molecules reflecting an hyperactivation of growth factorsignaling, i.e. absence of HER2 and presence of PR. On the contrary,patientswith tumors overexpressingHER2 or lacking PRmight achievemore benefit fromAI treatment. After tamoxifen failure, we propose touse AI and reserve fulvestrant as the last endocrine treatment.
Importantly, the molecular characterization of the complex signal-ing networks operating in endocrine resistant cells, e.g. EGFR, HER2,MAPK, AKT, mTOR, will enable the development of pharmaceuticalcompounds targeted at the various components of these pathways inorder to overcomeordelay the onset of resistance to endocrine therapyin breast cancer [273–275]. Based onpre-clinical data, clinical trials areongoing to evaluate the activity of endocrine agents in associationwithSTIs. The hope is that novel targeted therapies might maximize thebenefit of hormonal treatment and delay the use of chemotherapy inpatients with metastatic breast cancer.
Unfortunately, current knowledge is insufficient to identify groupsof patients who will derive benefit from the different endocrineagents, and there is a pressing need for new molecular and clinicaldata to improve understanding in this area. In the future, molecularprofiling of individual tumors will help to predict the most appro-priate endocrine therapy for each patient.
References
[1] V.C. Jordan, A.M. Brodie, Development and evolution of therapies targeted to theestrogen receptor for the treatment and prevention of breast cancer, Steroids 72(2007) 7–25.
[2] Early Breast Cancer Trialists' Collaborative Group (EBCTCG), Effects of che-motherapy and hormonal therapy for early breast cancer on recurrence and15-year survival: an overview of the randomised trials, Lancet 365 (2005)1687–1717.
[3] I.A. Jaiyesimi, A.U. Buzdar, D.A. Decker, G.N. Hortobagyi, Use of tamoxifen forbreast cancer: twenty-eight years later, J. Clin. Oncol. 13 (1995) 513–529.
[4] C.K. Osborne, Tamoxifen in the treatment of breast cancer, N. Engl. J. Med. 339(1998) 1609–1618.
[5] W.J. Gradishar, Tamoxifen—what next? Oncologist 9 (2004) 378–384.[6] K. Strasser-Weippl, P.E. Goss, Advances in adjuvant hormonal therapy for
postmenopausal women, J. Clin. Oncol. 23 (2005) 1751–1759.[7] Arimidex, Tamoxifen, Alone or in Combination (ATAC) Trialists' Group, J.F. Forbes,
J. Cuzick, A. Buzdar, A. Howell, J.S. Tobias, M. Baum, Effect of anastrozole andtamoxifen as adjuvant treatment for early-stage breast cancer: 100-monthanalysis of the ATAC trial, Lancet Oncol. 9 (2008) 45–53.
[8] A. Howell, J. Pippen, R.M. Elledge, L. Mauriac, I. Vergote, S.E. Jones, S.E. Come, C.K.Osborne, J.F. Robertson, Fulvestrant versus anastrozole for the treatment ofadvanced breast carcinoma: a prospectively planned combined survival analysisof two multicenter trials, Cancer 104 (2005) 236–239.
[9] L. Perey, R. Paridaens, H. Hawle, K. Zaman, F. Nolé, H. Wildiers, M. Fiche, D.Dietrich, P. Clément, D. Köberle, A. Goldhirsch, B. Thürlimann, Clinical benefit offulvestrant in postmenopausal womenwith advanced breast cancer and primaryor acquired resistance to aromatase inhibitors: final results of phase II SwissGroup for Clinical Cancer Research Trial (SAKK 21/00), Ann. Oncol. 18 (2007)64–69.
[10] R.V. Weatherman, R.J. Fletterick, T.S. Scanlan, Nuclear-receptor ligands andligand-binding domains, Annu. Rev. Biochem. 68 (1999) 559–581.
[11] S. Green, P. Walter, G. Greene, A. Krust, C. Goffin, E. Jensen, G. Scrace, M.Waterfield, P. Chambon, Cloning of the human estrogen receptor cDNA, J. SteroidBiochem. 24 (1986) 77–83.
[12] G.G. Kuiper, E. Enmark, M. Pelto-Huikko, S. Nilsson, J.A. Gustafsson, Cloning of anovel receptor expressed in rat prostate and ovary, Proc. Natl. Acad. Sci. U.S.A. 93(1996) 5925–5930.
[13] G.G. Kuiper, B. Carlsson, K. Grandien, E. Enmark, J. Häggblad, S. Nilsson, J.A.Gustafsson, Comparison of the ligand binding specificity and transcript tissuedistribution of estrogen receptors alpha and beta, Endocrinology 138 (1997)863–870.
[14] J.M. Emmen, J.F. Couse, S.A. Elmore, M.M. Yates, G.E. Kissling, K.S. Korach, In vitrogrowth and ovulation of follicles from ovaries of estrogen receptor (ER){alpha}and ER{beta} null mice indicate a role for ER{beta} in follicular maturation,Endocrinology 146 (2005) 2817–2826.
[15] H.A. Harris, Estrogen receptor-beta: recent lessons from in vivo studies, Mol.Endocrinol. 21 (2007) 1–13.
[16] C.K. Osborne, R. Schiff, S.A. Fuqua, J. Shou, Estrogen receptor: current under-standing of its activation and modulation, Clin. Cancer Res. 7 (Suppl 12) (2001)S4338–S4342.
[17] C.K. Osborne, R. Schiff, Estrogen-receptor biology: continuing progress andtherapeutic implications, J. Clin. Oncol. 23 (2005) 1616–1622.
[18] V. Kumar, S. Green, G. Stack, M. Berry, J.R. Jin, P. Chambon, Functional domains ofthe human estrogen receptor, Cell 51 (1987) 941–951.
[19] R.M. Evans, The steroid and thyroid hormone receptor superfamily, Science 13(240) (1988) 889–895.
[20] S. Nilsson, J.A. Gustafsson, Estrogen receptor transcription and transactivation:basic aspects of estrogen action, Breast Cancer Res. 2 (2000) 360–366.
[21] L. Tora, J. White, C. Brou, D. Tasset, N. Webster, E. Scheer, P. Chambon, The humanestrogen receptor has two independent nonacidic transcriptional activationfunctions, Cell 59 (1989) 477–487.
[22] S. Mader, P. Chambon, J.H. White, Defining a minimal estrogen receptor DNAbinding domain, Nucleic Acids Res. 21 (1993) 1125–1132.
[23] D. Picard, V. Kumar, P. Chambon, K.R. Yamamoto, Signal transduction by steroidhormones: nuclear localization is differentially regulated in estrogen andglucocorticoid receptors, Cell Regul. 1 (1990) 291–299.
[24] R.V. Weatherman, T.S. Scanlan, Unique protein determinants of the subtype-selective ligand responses of the estrogen receptors (ERalpha and ERbeta) atAP-1 sites, J. Biol. Chem. 276 (2001) 3827–3832.
[25] A. Koide, C. Zhao, M. Naganuma, J. Abrams, S. Deighton-Collins, D.F. Skafar, S.Koide, Identification of regions within the F domain of the human estrogenreceptor alpha that are important for modulating transactivation and protein–protein interactions, Mol. Endocrinol. 21 (2007) 829–842.
[26] D.F. Skafar, C. Zhao, The multifunctional estrogen receptor- alpha F domain,Endocrine 33 (2008) 1–8.
[27] E.M. McInerney, K.E. Weis, J. Sun, S. Mosselman, B.S. Katzenellenbogen,Transcription activation by the human estrogen subtype β (ERβ) studied withERβ and ERα receptor chimeras, Endocrinology 139 (1998) 4513–4522.
[28] J.M. Hall, D.P. McDonnell, The estrogen receptor beta-isoform (ERbeta) of thehuman estrogen receptor modulates ERalpha transcriptional activity and is a keyregulator of the cellular response to estrogens and antiestrogens, Endocrinology140 (1999) 5566–5578.
[29] S.T. Pearce, V.C. Jordan, The biological role of estrogen receptors alpha and beta incancer, Crit. Rev. Oncol. Hematol. 50 (2004) 3–22.
[30] J.A. Schwartz, L. Zhong, S. Deighton-Collins, C. Zhao, D.F. Skafar, Mutationstargeted to a predicted helix in the extreme carboxyl-terminal region of thehuman estrogen receptor-alpha alter its response to estradiol and 4-hydro-xytamoxifen, J. Biol. Chem. 277 (2002) 13202–13209.
[31] J.A. Gustafsson, M. Warner, Estrogen receptor beta in the breast: role in estrogenresponsiveness and development of breast cancer, J. Steroid Biochem. Mol. Biol.74 (2000) 245–248.
[32] D.B. Lubahn, J.S. Moyer, T.S. Golding, J.F. Couse, K.S. Korach, O. Smithies,Alteration of reproductive function but not prenatal sexual development afterinsertional disruption of the mouse estrogen receptor gene, Proc. Natl. Acad. Sci.U.S.A. 90 (1993) 11162–11166.
[33] C. Förster, S. Mäkela, A. Wärri, S. Kietz, D. Becker, K. Hultenby, M. Warner,J.A. Gustafsson, Involvement of estrogen receptor beta in terminal differen-tiation of mammary gland epithelium, Proc. Natl. Acad. Sci. U.S.A. 99 (2002)15578–15583.
[34] P. Roger, M.E. Sahla, S. Mäkelä, J.A. Gustafsson, P. Baldet, H. Rochefort, Decreasedexpression of estrogen receptor beta protein in proliferative preinvasivemammary tumors, Cancer Res. 61 (2001) 2537–2541.
[35] J.A. Shaw, K. Udokang, J.M. Mosquera, H. Chauhan, J.L. Jones, R.A. Walker,Oestrogen receptors alpha and beta differ in normal human breast and breastcarcinomas, J. Pathol. 198 (2002) 450–457.
[36] B.W. Park, K.S. Kim, M.K. Heo, S.S. Ko, S.W. Hong,W.I. Yang, J.H. Kim, G.E. Kim, K.S.Lee, Expression of estrogen receptor-beta in normal mammary and tumortissues: is it protective in breast carcinogenesis? Breast Cancer Res. Treat. 80(2003) 79–85.

76 M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
[37] A. Ström, J. Hartman, J.S. Foster, S. Kietz, J. Wimalasena, J.A. Gustafsson, Estrogenreceptor beta inhibits 17beta-estradiol-stimulated proliferation of the breastcancer cell line T47D, Proc. Natl. Acad. Sci. U.S.A. 101 (2004) 1566–1571.
[38] S. Paruthiyil, H. Parmar, V. Kerekatte, G.R. Cunha, G.L. Firestone, D.C. Leitman,Estrogen receptor beta inhibits human breast cancer cell proliferation and tumorformation by causing a G2 cell cycle arrest, Cancer Res. 64 (2004) 423–428.
[39] C. Williams, K. Edvardsson, S.A. Lewandowski, A. Ström, J.A. Gustafsson, Agenome-wide study of the repressive effects of estrogen receptor beta onestrogen receptor alpha signaling in breast cancer cells, Oncogene 27 (2008)1019–1032.
[40] A. Bardin, N. Boulle, G. Lazennec, F. Vignon, P. Pujol, Loss of ERbeta expression as acommon step in estrogen-dependent tumor progression, Endocr. Relat. Cancer11 (2004) 537–551.
[41] G. Lazennec, Estrogen receptor beta, a possible tumor suppressor involved inovarian carcinogenesis, Cancer Lett. 231 (2006) 151–157.
[42] H. Sugiura, T. Toyama, Y. Hara, Z. Zhang, S. Kobayashi, Y. Fujii, H. Iwase, H.Yamashita, Expression of estrogen receptor beta wild-type and its variantERbetacx/beta2 is correlated with better prognosis in breast cancer, Japanese J.Clin. Oncol. 37 (2007) 820–828.
[43] J. Cheung, D.F. Smith, Molecular chaperone interactions with steroid receptors:an update, Mol. Endocrinol. 14 (2000) 939–946.
[44] R. O'Lone, M.C. Frith, E.K. Karlsson, U. Hansen, Genomic targets of nuclearestrogen receptors, Mol. Endocrinol. 18 (2004) 1859–1875.
[45] J.S. Carroll, M. Brown, Estrogen receptor target gene: an evolving concept, Mol.Endocrinol. 20 (2006) 1707–1714.
[46] K.M. Dobrzycka, S.M. Townson, S. Jiang, S. Oesterreich, Estrogen receptorcorepressors — a role in human breast cancer? Endocr. Relat. Cancer 10 (2003)517–536.
[47] J. Frasor, J.M. Danes, B. Komm, K.C. Chang, C.R. Lyttle, B.S. Katzenellenbogen,Profiling of estrogen up- and down-regulated gene expression in human breastcancer cells: insights into gene networks and pathways underlying estrogeniccontrol of proliferation and cell phenotype, Endocrinology 144 (2003)4562–4574.
[48] L. Klein-Hitpass, G.U. Ryffel, E. Heitlinger, A.C. Cato, A 13 bp palindrome is afunctional estrogen responsive element and interacts specifically with estrogenreceptor, Nucleic Acids Res. 16 (1988) 647–663.
[49] F.V. Peale, L.B. Ludwig, S. Zain, R. Hilf, R.A. Bambara, Properties of a high-affinityDNA binding site for estrogen receptor, Proc. Natl. Acad. Sci. U.S.A. 85 (1988)1038–1042.
[50] J.R. Wood, V.S. Likhite, M.A. Loven, A.M. Nardulli, Allosteric modulation ofestrogen receptor conformation by different estrogen response elements, Mol.Endocrinol. 15 (2001) 1114–1126.
[51] M. Berry, A.M. Nunez, P. Chambon, Estrogen responsive element of the humanpS2 gene is an imperfectly palindromic sequence, Proc. Natl. Acad. Sci. U.S.A. 86(1989) 1218–1222.
[52] R. Duan, W. Porter, S. Safe, Estrogen-induced c-fos protooncogene expression inMCF-7 human breast cancer cells: role of estrogen receptor Sp1 complexformation, Endocrinology 139 (1998) 1981–1990.
[53] I. Samudio, C. Vyhlidal, F. Wang, M. Stoner, I. Chen, M. Kladde, R. Barhoumi, R.Burghardt, S. Safe, Transcriptional activation of DNA polymerase α geneexpression in MCF-7 cells by 17β-estradiol, Endocrinology 142 (2001)1000–1008.
[54] P.J. Kushner, D.A. Agard, G.L. Greene, T.S. Scanlan, A.K. Shiau, R.M. Uht, P. Webb,Estrogen receptor pathways to AP-1, J. Steroid Biochem. Mol. Biol. 74 (2000)311–317.
[55] M. Sabbah, D. Courilleau, J. Mester, G. Redeuilh, Estrogen induction of the cyclinD1 promoter: involvement of a cAMP response-like element, Proc. Natl. Acad. Sci.U.S.A. 96 (1999) 11217–11222.
[56] B. Saville, M.Wormke, F.Wang, T. Nguyen, E. Enmark, G. Kuiper, J.A. Gustafsson, S.Safe, Ligand-, cell-, and estrogen receptor subtype (α/β)-dependent activation atGC-rich (Sp1) promoter elements, J. Biol. Chem. 275 (2000) 5379–5387.
[57] J. Eeckhoute, J.S. Carroll, T.R. Geistlinger, M.I. Torres-Arzayus, M. Brown, A cell-type-specific transcriptional network required for estrogen regulation of cyclinD1 and cell cycle progression in breast cancer, Genes Dev. 20 (2006) 2513–2526.
[58] S. Maor, D. Mayer, R.I. Yarden, A.V. Lee, R. Sarfstein, H. Werner, M.Z. Papa,Estrogen receptor regulates insulin-like growth factor-I receptor gene expressionin breast tumor cells: involvement of transcription factor Sp1, J. Endocrinol. 191(2006) 605–612.
[59] C.J. Gruber, D.M. Gruber, I.M. Gruber, F. Wieser, J.C. Huber, Anatomy of theestrogen response element, Trends Endocrinol. Metab. 15 (2004) 73–78.
[60] M.D. Mueller, J.L. Vigne, A. Minchenko, D.I. Lebovic, D.C. Leitman, R.N. Taylor,Regulation of vascular endothelial growth factor (VEGF) gene transcription byestrogen receptors alpha and beta, Proc. Natl. Acad. Sci. U.S.A. 97 (2000)10972–10977.
[61] H. Buteau-Lozano, M. Ancelin, B. Lardeux, J. Milanini, M. Perrot-Applanat,Transcriptional regulation of vascular endothelial growth factor by estradiol andtamoxifen in breast cancer cells: a complex interplay between estrogenreceptors alpha and beta, Cancer Res. 62 (2002) 4977–4984.
[62] M. Stoner, M. Wormke, B. Saville, I. Samudio, C. Qin, M. Abdelrahim, S. Safe,Estrogen regulation of vascular endothelial growth factor gene expression inZR-75 breast cancer cells through interaction of estrogen receptor alpha and SPproteins, Oncogene 23 (2004) 1052–1063.
[63] H. Buteau-Lozano, G. Velasco, M. Cristofari, P. Balaguer, M. Perrot-Applanat,Xenoestrogens modulate vascular endothelial growth factor secretion in breastcancer cells through an estrogen receptor-dependent mechanism, J. Endocrinol.196 (2008) 399–412.
[64] L.N. Petz, A.M. Nardulli, Sp1 binding sites and an estrogen response element half-site are involved in regulation of the human progesterone receptor A promoter,Mol. Endocrinol. 14 (2000) 972–985.
[65] T.A. Pham, Y.P. Hwung, D. Santiso-Mere, D.P. McDonnell, B.W. O'Malley,Ligand-dependent and -independent function of the transactivation regionsof the human estrogen receptor in yeast, Mol. Endocrinol. 6 (1992)1043–1050.
[66] M.T. Tzukerman, A. Esty, D. Santiso-Mere, P. Danielian, M.G. Parker, R.B. Stein, J.W.Pike, D.P. McDonnell, Human estrogen receptor transactivational capacity isdetermined by both cellular and promoter context and mediated by twofunctionally distinct intramolecular regions, Mol. Endocrinol. 8 (1994) 21–30.
[67] R. Métivier, G. Penot, G. Flouriot, F. Pakdel, Synergism between ERalphatransactivation function 1 (AF-1) and AF-2 mediated by steroid receptorcoactivator protein-1: requirement for the AF-1 alpha-helical core and for adirect interaction between the N- and C-terminal domains, Mol. Endocrinol. 15(2001) 1953–1970.
[68] A.M. Brzozowski, A.C. Pike, Z. Dauter, R.E. Hubbard, T. Bonn, O. Engström, L.Ohman, G.L. Greene, J.A. Gustafsson, M. Carlquist, Molecular basis of agonism andantagonism in the oestrogen receptor, Nature 389 (1997) 753–758.
[69] A.K. Shiau, D. Barstad, P.M. Loria, L. Chen, P.J. Kushner, D.A. Agard, G.L. Green, Thestructural basis of estrogen receptor/coactivator recognition and the antagonismof this interaction by tamoxifen, Cell 95 (1998) 927–937.
[70] N.J. McKenna, R.B. Lanz, B.W. O'Malley, Nuclear receptor coregulators: cellularand molecular biology, Endocr. Rev. 20 (1999) 321–344.
[71] C. Leo, J.D. Chen, The SRC family of nuclear receptor coactivators, Gene 245(2000) 1–11.
[72] J.D. Chen, R.M. Evans, A transcriptional corepressor that interacts with nuclearhormone receptors, Nature 377 (1995) 454–457.
[73] P. Yi, M.D. Driscoll, J. Huang, S. Bhagat, R. Hilf, R.A. Bambara, M. Muyan, Theeffects of estrogen-responsive element- and ligand-induced structural changeson the recruitment of cofactors and transcriptional responses by ER alpha and ERbeta, Mol Endocrinol. 16 (2002) 674–693.
[74] J.A. Lees, S.E. Fawell, M.G. Parker, Identification of two transactivation domains inthe mouse oestrogen receptor, Nucleic Acids Res. 17 (1989) 5477–5488.
[75] S. Kato, H. Endoh, Y. Masuiro, T. Kitamoto, S. Uchiyama, H. Sasaki, S. Masushige, Y.Gotoh, E. Nishida, H. Kawashima, D. Metzger, P. Chambon, Activation of theestrogen receptor through phosphorylation bymitogen-activated protein kinase,Science 270 (1995) 1491–1494.
[76] G. Bunone, P.A. Briand, R.J. Miksicek, D. Picard, Activation of the unligandedestrogen receptor by EGF involves the MAP kinase pathway and directphosphorylation, EMBO J. 15 (1996) 2174–2183.
[77] R.A. Campbell, P. Bhat-Naksatri, N.M. Patel, D. Constantinidou, S. Ali, H. Nakshatri,Phosphatidylinositol 3-kinase/AKT-mediated activation of estrogen receptoralpha: a new model for anti-estrogen resistance, J. Biol. Chem. 276 (2001)9817–9824.
[78] R.S. Thomas, N. Sarwar, F. Phoenix, R.C. Coombes, S. Ali, Phosphorylation atserines 104 and 106 by Erk1/2 MAPK is important for estrogen receptor-alphaactivity, J. Mol. Endocrinol. 40 (2008) 173–184.
[79] R. Schiff, S. Massarweh, J. Shou, C.K. Osborne, Breast cancer endocrine resistance:how growth factor signaling and estrogen receptor coregulators modulateresponse, Clin. Cancer Res. 9 (2003) 447S–454S.
[80] J.M. Hall, J.F. Couse, K.S. Korach, The multifaceted mechanisms of estradiol andestrogen receptor signalling, J. Biol. Chem. 276 (2001) 36869–36872.
[81] D.A. Lannigan, Estrogen receptor phosphorylation, Steroids 68 (2003) 1–9.[82] D. Metzger, R. Losson, J.M. Bornert, Y. Lemoine, P. Chambon, Promoter specificity
of the two transcriptional activation functions of the human oestrogen receptorin yeast, Nucleic Acids Res. 20 (1992) 2813–2817.
[83] E.M. McInerney, M.J. Tsai, B.W. O'Malley, B.S. Katzenellenbogen, X Analysis ofestrogen receptor transcriptional enhancement by a nuclear hormone receptorcoactivator, Proc. Natl. Acad. Sci. U.S.A. 93 (1996) 10069–10073.
[84] P. Webb, P. Nguyen, J. Shinsako, C. Anderson, W. Feng, M.P. Nguyen, D. Chen, S.M.Huang, S. Subramanian, E. McKinerney, B.S. Katzenellenbogen, M.R. Stallcup, P.J.Kushner, Estrogen receptor activation function 1 works by binding p160coactivator proteins, Mol. Endocrinol. 12 (1998) 1605–1618.
[85] Y. Kobayashi, T. Kitamoto, Y. Masuhiro, M. Watanabe, T. Kase, D. Metzger, J.Yanagisawa, S. Kato, p300 mediates functional synergism between AF-1 and AF-2 of estrogen receptor alpha and beta by interacting directly with the N-terminalA/B domains, J. Biol. Chem. 275 (2000) 15645–15651.
[86] N.L. Weigel, Y. Zhang, Ligand-independent activation of steroid hormonereceptors, J. Mol. Med. 76 (1998) 469–479.
[87] K. Pettersson, F. Delaunay, J.A. Gustafsson, Estrogen receptor β acts as a dominantregulator of estrogen signaling, Oncogene 19 (2000) 4970–4978.
[88] K. Paech, P. Webb, G.G. Kuiper, S. Nilsson, J. Gustafsson, P.J. Kushner, T.S. Scanlan,Differential ligand activation of estrogen receptors ERalpha and ERbeta at AP-1sites, Science 277 (1997) 1508–1510.
[89] P. Webb, P. Nguyen, C. Valentine, G.N. Lopez, G.R. Kwok, E. McInerney, B.S.Katzenellenbogen, E. Enmark, J.A. Gustafsson, S. Nilsson, P.J. Kushner, Theestrogen receptor enhances AP-1 activity by two distinct mechanisms withdifferent requirements for receptor transactivation functions, Mol. Endocrinol. 13(1999) 1672–1685.
[90] P. Webb, C. Valentine, P. Nguyen, R.H. Price, A. Marimuthu, B.L. West, J.D. Baxter,P.J. Kushner, ERbeta binds N-CoR in the presence of estrogens via an LXXLL-likemotif in the N-CoR C-terminus, Nucl. Recept. 1 (2003) 4.
[91] M.M. Liu, C. Albanese, C.M. Anderson, K. Hilty, P. Webb, R.M. Uht, R.H. Price, R.G.Pestell, P.J. Kushner, Opposing action of estrogen receptors alpha and beta oncyclin D1 gene expression, J. Biol. Chem. 277 (2002) 24353–24360.

77M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
[92] M. Razandi, A. Pedram, S.T. Park, E.R. Levin, Proximal events in signaling byplasma membrane estrogen receptors, J. Biol. Chem. 278 (2003) 2701–2712.
[93] M. Marino, P. Ascenzi, Membrane association of estrose receptor a and binfluences 17b-estradiol-mediated cancer cell proliferation, Steroids 73 (2008)853–858.
[94] A.J. Evinger, E.R. Levin, Requirements for estrogen receptor a membranelocalization and function, Steroids 70 (2005) 361–363.
[95] S. Kahlert, S. Nuedling, M. van Eickels, H. Vetter, R. Meyer, C. Grohe, Estrogenreceptor alpha rapidly activates the IGF-1 receptor pathway, J. Biol. Chem. 275(2000) 18447–18453.
[96] C.W. Wong, C. McNally, E. Nickbarg, B.S. Komm, B.J. Cheskis, Estrogen receptor-interacting protein that modulates its nongenomic activity-crosstalk with Src/Erk phosphorylation cascade, Proc. Natl. Acad. Sci. U.S.A. 99 (2002) 14783–14788.
[97] R. Schiff, S. Massarweh, J. Shou, L. Bharwani, S.K. Mohsin, C.K. Osborne, Cross-talkbetween estrogen receptor and growth factor pathways as a molecular target forovercoming endocrine resistance, Clin. Cancer Res. 10 (2004) 331S–336S.
[98] J. Shou, S. Massarweh, C.K. Osborne, A.E. Wakeling, S. Ali, H. Weiss, R. Schiff,Mechanisms of tamoxifen resistance: increased estrogen receptor-HER2/neucross-talk in ER/HER2-positive breast cancer, J. Natl. Cancer Inst. 96 (2004)926–935.
[99] R.K. Vadlamudi, R.A. Wang, A. Mazumdar, Y. Kim, J. Shin, A. Sahin, R. Kumar,Molecular cloning and characterization of PELP1, a novel human coregulator ofestrogen receptor alpha, J. Biol. Chem. 276 (2001) 38272–38279.
[100] R. Kumar, R.A. Wang, A. Mazumdar, A.H. Talukder, M. Mandal, Z. Yang, R. Bagheri-Yarmand, A. Sahin, G. Hortobagyi, L. Adam, C.J. Barnes, R.K. Vadlamudi, Anaturally occurring MTA1 variant sequesters oestrogen receptor-alpha in thecytoplasm, Nature 418 (2002) 654–657.
[101] R. Kumar, R.A. Wang, R. Bagheri-Yarmand, Emerging roles of MTA familymembers in human cancers, Semin. Oncol. 30 (2003) 30–37.
[102] A. Pedram, M. Razandi, R.C. Sainson, J.K. Kim, C.C. Hughes, E.R. Levin, A conservedmechanism for steroid receptor translocation to the plasma membrane, J. Biol.Chem. 282 (2007) 22278–22288.
[103] E.R. Levin, Bidirectional signaling between the estrogen receptor and theepidermal growth factor receptor, Mol. Endocrinol. 17 (2003) 309–317.
[104] F. Barletta, C.W. Wong, C. McNally, B.S. Komm, B. Katzenellenbogen, B.J. Cheskis,Characterization of the interactions of estrogen receptor and MNAR in theactivation of cSrc, Mol. Endocrinol. 18 (2004) 1096–1108.
[105] S. Kousteni, J.R. Chen, T. Bellido, L. Han, A.A. Ali, C.A. O'Brien, L. Plotkin, Q. Fu, A.T.Mancino, Y. Wen, Reversal of bone loss in mice by nongenotropic signaling of sexsteroids, Science 298 (2002) 843–846.
[106] G. Castoria, A. Migliaccio, A. Bilancio, M. Di Domenico, A. de Falco, M. Lombardi, R.Fiorentino, L. Varricchio, M.V. Barone, F. Auricchio, PI3-kinase in concert with Srcpromotes the S-phase entry of oestradiol-stimulated MCF-7 cells, EMBO J. 20(2001) 6050–6059.
[107] D. McDonnell, Themolecular pharmacology of SERMs, Trends Endocrinol. Metab.10 (1999) 301–311.
[108] M.L. Privalsky, The role of corepressors in transcriptional regulation by nuclearhormone receptors, Annu. Rev. Physiol. 66 (2004) 315–360.
[109] K.W. Nettles, G.L. Greene, Ligand control of coregulator recruitment to nuclearreceptors, Annu. Rev. Physiol. 67 (2005) 309–333.
[110] C.L. Smith, Z. Nawaz, B.W. O'Malley, Coactivator and corepressor regulation ofthe agonist: antagonist activity of the mixed antiestrogen, 4-hydroxytamoxifen,Mol. Endocrinol. 11 (1997) 657–666.
[111] M. Berry, D. Metzger, P. Chambon, Role of the two activating domains of theoestrogen receptor in the cell-type and promoter-context dependent agonisticactivity of the anti-oestrogen 4-hydroxytamoxifen, EMBO J. 9 (1990) 2811–2818.
[112] C.L. Smith, B.W. O'Malley, Coregulator function: a key to understanding tissuespecificity of selective receptor modulators, Endocr. Rev. 25 (2004) 45–71.
[113] V.C. Jordan, B.W. O'Malley, Selective estrogen-receptor modulators and anti-hormonal resistance in breast cancer, J. Clin. Oncol. 25 (2007) 5815–5824.
[114] Y. Shang, M. Brown, Molecular determinants for the tissue specificity of SERMs,Science 295 (2002) 2465–2468.
[115] D. Kressler, M.B. Hock, A. Kralli, Coactivators PGC-1beta and SRC-1 interactfunctionally to promote the agonist activity of the selective estrogen receptormodulator tamoxifen, J. Biol. Chem. 282 (2007) 26897–26907.
[116] K. Pettersson, J.A. Gustafsson, Role of estrogen receptor beta in estrogen action,Annu. Rev. Physiol. 63 (2001) 165–192.
[117] J.D. Fan, B.L. Wagner, P.D. McDonnell, Identification of the sequences within thehuman complement 3 promoter required for estrogen responsiveness providesinsight into the mechanism of tamoxifenmixed agonist activity, Mol. Endocrinol.10 (1996) 1605–1616.
[118] P. Webb, G.N. Lopez, R.M. Uht, P.J. Kushner, Tamoxifen activation of the estrogenreceptor/AP-1 pathway: potential origin for the cell-specific estrogen-like effectsof antiestrogens, Mol. Endocrinol. 9 (1995) 443–456.
[119] A. Zou, K.B. Marschke, K.E. Arnold, E.M. Berger, P. Fitzgerald, D.E. Mais, E.A.Allegretto, Estrogen receptor beta activates the human retinoic acid receptoralpha-1 promoter in response to tamoxifen and other estrogen receptorantagonists, but not in response to estrogen, Mol. Endocrinol. 13 (1999) 418–430.
[120] D.P. McDonnell, J.D. Norris, Analysis of the molecular pharmacology of estrogenreceptor agonists and antagonists provides insights into themechanism of actionof estrogen in bone, Osteoporos. Int. 7 (1997) 29S–34S.
[121] C. Longcope, J.H. Pratt, S.H. Schneider, S.E. Fineberg, Aromatization of androgensby muscle and adipose tissue in vivo, J. Clin. Endocrinol. Metab. 46 (1978)146–152.
[122] I.E. Smith, M. Dowsett, Aromatase inhibitors in breast cancer, N. Engl. J. Med. 348(2003) 2431–2442.
[123] A.E. Wakeling, M. Dukes, J. Bowler, A potent specific pure antiestrogen withclinical potential, Cancer Res. 51 (1991) 3867–3873.
[124] J. Bowler, T.J. Lilley, J.D. Pittam, A.E. Wakeling, Novel steroidal pure antiestrogens,Steroids 54 (1989) 71–99.
[125] A.C. Pike, A.M. Brzozowski, J. Walton, R.E. Hubbard, A.G. Thorsell, Y.L. Li, J.A.Gustafsson, M. Carlquist, Structural insights into the mode of action of a pureantiestrogen, Structure 9 (2001) 145–153.
[126] S.E. Fawell, R. White, S. Hoare, M. Sydenham, M. Page, M.G. Parker, Inhibition ofestrogen receptor-DNA binding by the “pure” antiestrogen ICI 164,384 appears tobe mediated by impaired receptor dimerization, Proc. Natl. Acad. Sci. U.S.A. 87(1990) 6883–6887.
[127] R.W. Carlson, The history and mechanism of action of fulvestrant, Clin. BreastCancer 6 (2005) S5–S8.
[128] X. Long, K.P. Nephew, Fulvestrant (ICI 182,780)-dependent interacting proteinsmediate immobilization and degradation of estrogen receptor-alpha, J. Biol.Chem. 281 (2006) 9607–9615.
[129] M. Fan, R.M. Bigsby, K.P. Nephew, The NEDD8 pathway is required forproteosome-mediated degradation of human estrogen receptor (ER)-alpha andessential for the antiproliferative activity of ICI 182,780 in ERalpha-positivebreast cancer cells, Mol. Endocrinol. 17 (2003) 356–365.
[130] N.T. Peekhaus, T. Chang, E.C. Hayes, H.A. Wilkinson, S.W. Mitra, J.M. Schaeffer, S.P.Rohrer, Distinct effects of the antiestrogen Faslodex on the stability of estrogenreceptors-alpha and -beta in the breast cancer cell line MCF-7, J. Mol. Endocrinol.32 (2004) 987–995.
[131] A.L. Wijayaratne, S.C. Nagel, L.A. Paige, D.J. Christensen, J.D. Norris, D.M. Fowlkes,D.P. McDonnell, Comparative analyses of mechanistic differences amongantioestrogens, Endocrinology 140 (1999) 5828–5840.
[132] Y.L. Ottaviano, J.P. Issa, F.F. Parl, H.S. Smith, S.B. Baylin, N.E. Davidson, Methylationof the estrogen receptor gene CpG island marks loss of estrogen receptorexpression in human breast cancer cells, Cancer Res. 54 (1994) 2552–2555.
[133] X. Yang, D.L. Phillips, A.T. Ferguson, W.G. Nelson, J.G. Herman, N.E. Davidson,Synergistic activation of functional estrogen receptor (ER)-alpha by DNAmethyltransferase and histone deacetylase inhibition in human ER-alpha-negative breast cancer cells, Cancer Res. 61 (2001) 7025–7029.
[134] R.G. Lapidus, A.T. Ferguson, Y.L. Ottaviano, F.F. Parl, H.S. Smith, S.A.Weitzman, S.B.Baylin, J.P. Issa, N.E. Davidson, Methylation of estrogen and progesteronereceptor gene 5′ CpG islands correlates with lack of estrogen and progesteronereceptor gene expression in breast tumors, Clin. Cancer Res. 2 (1996) 805–810.
[135] F.F. Parl, Multiple mechanisms of estrogen receptor gene repression contribute toER-negative breast cancer, Pharmacogenomics J. 3 (2003) 251–253.
[136] X. Yang, A.T. Ferguson, S.J. Nass, D.L. Phillips, K.A. Butash, S.M.Wang, J.G. Herman,N.E. Davidson, Transcriptional activation of estrogen receptor alpha in humanbreast cancer cells by histone deacetylase inhibition, Cancer Res. 60 (2000)6890–6894.
[137] J. Fan, W.J. Yin, J.S. Lu, L. Wang, J. Wu, F.Y. Wu, G.H. Di, Z.Z. Shen, Z.M. Shao,ERalpha negative breast cancer cells restore response to endocrine therapy bycombination treatment with both HDAC inhibitor and DNMT inhibitor, J. CancerRes. Clin. Oncol. 134 (2008) 883–890.
[138] N. Normanno, F. Ciardiello, R. Brandt, D.S. Salomon, Epidermal growth factor-related peptides in the pathogenesis of human breast cancer, Breast Cancer Res.Treat. 29 (1994) 11–27.
[139] C.J. Creighton, A.M. Hilger, S. Murthy, J.M. Rae, A.M. Chinnaiyan, D. El-Ashry,Activation of mitogen-activated protein kinase in estrogen receptor alpha-positive breast cancer cells in vitro induces an in vivo molecular phenotype ofestrogen receptor alpha-negative human breast tumors, Cancer Res. 66 (2006)3903–3911.
[140] A. Stoica, M. Saceda, V.L. Doraiswamy, C. Coleman, M.B. Martin, Regulation ofestrogen receptor-alpha gene expression by epidermal growth factor, J.Endocrinol. 165 (2000) 371–378.
[141] S.R. Johnston, G. Saccani-Jotti, I.E. Smith, J. Salter, J. Newby, M. Coppen, S.R. Ebbs,M. Dowsett, Changes in estrogen receptor, progesterone receptor, and pS2expression in tamoxifen-resistant human breast cancer, Cancer Res. 55 (1995)3331–3338.
[142] M.C. Gutierrez, S. Detre, S. Johnston, S.K. Mohsin, J. Shou, D.C. Allred, R. Schiff, C.K.Osborne, M. Dowsett, Molecular changes in tamoxifen-resistant breast cancer:relationship between estrogen receptor, HER-2, and p38 mitogen-activatedprotein kinase, J. Clin. Oncol. 23 (2005) 2469–2476.
[143] C.K. Osborne, J. Pippen, S.E. Jones, L.M. Parker, M. Ellis, S. Come, S.Z. Gertler, J.T.May, G. Burton, I. Dimery, A. Webster, C. Morris, R. Elledge, A. Buzdar, Double-blind, randomized trial comparing the efficacy and tolerability of fulvestrantversus anastrozole in postmenopausal women with advanced breast cancerprogressing on prior endocrine therapy: results of a North American trial, J. Clin.Oncol. 20 (2002) 3386–3395.
[144] R.I. Nicholson, C. Staka, F. Boyns, I.R. Hutcheson, J.M. Gee, Growth factor-driven mechanisms associated with resistance to estrogen deprivation inbreast cancer: new opportunities for therapy, Endocr. Relat. Cancer 11 (2004)623–641.
[145] R.A. McClelland, D. Barrow, T.A. Madden, C.M. Dutkowski, J. Pamment, J.M.Knowlden, J.M. Gee, R.I. Nicholson, Enhanced epidermal growth factor receptorsignaling in MCF-7 breast cancer cells after long-term culture in the presence ofthe pure antiestrogen ICI 182,780 (Faslodex), Endocrinology 142 (2001)2776–2788.
[146] S. Massarweh, C.K. Osborne, S. Jiang, A.E. Wakeling, M. Rimawi, S.K. Mohsin, S.Hilsenbeck, R. Schiff, Mechanisms of tumor regression and resistance to estrogendeprivation and fulvestrant in a model of estrogen receptor-positive, HER-2/neu-positive breast cancer, Cancer Res. 66 (2006) 8266–8273.

78 M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
[147] W.S. Shim, M. Conaway, S. Masamura, W. Yue, J.P. Wang, R. Kmar, R.J. Santen,Estradiol hypersensitivity and mitogen-activated protein kinase expression inlong-term estrogen deprived human breast cancer cells in vivo, Endocrinology141 (2000) 396–405.
[148] H. Sonoo, J. Kurebayashi, Y. Iino, H. Inaji, T. Watanabe, M. Toi, S. Kobayashi, B. Sato,M. Yoshimoto, Current status and controversial issues concerning endocrinetherapy for patients with recurrent breast cancer in Japan, Breast Cancer 6 (1999)344–350.
[149] M. Stoner, B. Saville, M. Wormke, D. Dean, R. Burghardt, S. Safe, Hypoxia inducesproteasome-dependent degradation of estrogen receptor alpha in ZR-75 breastcancer cells, Mol. Endocrinol. 16 (2002) 2231–2242.
[150] D.M.Wolf, V.C. Jordan, The estrogen receptor from a tamoxifen stimulatedMCF-7tumor variant contains a point mutation in the ligand binding domain, BreastCancer Res. Treat. 31 (1994) 129–138.
[151] S.A. Fuqua, D.C. Allred, R.J. Auchus, Expression of estrogen receptor variants, J.Cell. Biochem. 53 (2004) 194–197.
[152] M.H. Herynk, S.A. Fuqua, Estrogen receptor mutations in human disease, Endocr.Rev. 25 (2004) 869–898.
[153] S.A. Fuqua, C. Wiltschke, Q.X. Zhang, A. Borg, C.G. Castles, W.E. Friedrichs, T.Hopp, S. Hilsenbeck, S. Mohsin, P. O'Connell, D.C. Allred, A hypersensitiveestrogen receptor-alpha mutation in premalignant breast lesions, Cancer Res. 60(2000) 4026–4029.
[154] V. Speirs, C. Malone, D.S. Walton, M.J. Kerin, S.L. Atkin, Increased expression ofestrogen receptor beta mRNA in tamoxifen-resistant breast cancer patients,Cancer Res. 59 (1999) 5421–5424.
[155] T.A. Hopp, H.L. Weiss, I.S. Parra, Y. Cui, C.K. Osborne, S.A. Fuqua, Low levels ofestrogen receptor beta protein predict resistance to tamoxifen therapy in breastcancer, Clin. Cancer Res. 10 (2004) 7490–7499.
[156] S. Borgquist, C. Holm, M. Stendahl, L. Anagnostaki, G. Landberg, K. Jirström,Oestrogen receptors alpha and beta show different associations to clinicopatho-logical parameters and their co-expression might predict a better response toendocrine treatment in breast cancer, J. Clin. Pathol. 61 (2008) 197–203.
[157] A. Rody, U. Holtrich, C. Solbach, K. Kourtis, G. von Minckwitz, K. Engels, S. Kissler,R. Gätje, T. Karn, M. Kaufmann, Methylation of estrogen receptor beta promotercorrelates with loss of ER-beta expression in mammary carcinoma and is an earlyindication marker in premalignant lesions, Endocr. Relat. Cancer 12 (2005)903–916.
[158] C.K. Osborne, V. Bardou, T.A. Hopp, G.C. Chamness, S.G. Hilsenbeck, S.A. Fuqua, J.Wong, D.C. Allred, G.M. Clark, R. Schiff, Role of the estrogen receptor coactivatorAIB1 (SRC-3) and HER-2/neu in tamoxifen resistance in breast cancer, J. Natl.Cancer Inst. 95 (2003) 353–361.
[159] T. Kirkegaard, L.M. McGlynn, F.M. Campbell, S. Müller, S.M. Tovey, B. Dunne, K.V.Nielsen, T.G. Cooke, J.M. Bartlett, Amplified in breast cancer 1 in humanepidermal growth factor receptor— positive tumors of tamoxifen-treated breastcancer patients, Clin. Cancer Res. 13 (2007) 1405–1411.
[160] F.F. Zheng, R.C. Wu, C.L. Smith, B.W. O'Malley, Rapid estrogen-inducedphosphorylation of the SRC-3 coactivator occurs in an extranuclear complexcontaining estrogen receptor, Mol. Cell. Biol. 25 (2005) 8273–8284.
[161] E. Cottone, F. Orso, N. Biglia, P. Sismondi, M. De Bortoli, Role of coactivators andcorepressors in steroid and nuclear receptor signaling: potential markers oftumor growth and drug sensitivity, Int. J. Biol. Markers 16 (2001) 151–166.
[162] I. Girault, F. Lerebours, S. Amarir, S. Tozlu, M. Tubiana-Hulin, R. Lidereau, I. Bièche,Expression analysis of estrogen receptor alpha coregulators in breast carcinoma:evidence that NCOR1 expression is predictive of the response to tamoxifen, Clin.Cancer Res. 9 (2003) 1259–1266.
[163] R.I. Yarden, M.A. Wilson, S.A. Chrysogelos, Estrogen suppression of EGFRexpression in breast cancer cells: a possible mechanism to modulate growth,J. Cell. Biochem. 81 (2001) 232–246.
[164] J.M. Gee, M.E. Harper, I.R. Hutcheson, T.A. Madden, D. Barrow, J.M. Knowlden, R.A.McClelland, N. Jordan, A.E. Wakeling, R.I. Nicholson, The antiepidermal growthfactor receptor agent gefitinib (ZD1839/Iressa) improves antihormone responseand prevents development of resistance in breast cancer in vitro, Endocrinology144 (2003) 5105–5117.
[165] J.M. Knowlden, I.R. Hutcheson, H.E. Jones, T. Madden, J.M. Gee, M.E. Harper, D.Barrow, A.E. Wakeling, R.I. Nicholson, Elevated levels of epidermal growth factorreceptor/c-erbB2 heterodimers mediate an autocrine growth regulatory path-way in tamoxifen resistant MCF-7 cells, Endocrinology 144 (2003) 1032–1044.
[166] P. Fan, J. Wang, R.J. Santen, W. Yue, Long-term treatment with tamoxifenfacilitates translocation of estrogen receptor alpha out of the nucleus andenhances its interaction with EGFR in MCF-7 breast cancer cells, Cancer Res. 67(2007) 1352–1360.
[167] S.R. Johnston, B. Lu, G.K. Scott, P.J. Kushner, I.E. Smith, M. Dowsett, C.C. Benz,Increased activator protein-1 DNA binding and c-Jun NH2-terminal kinaseactivity in human breast tumors with acquired tamoxifen resistance, Clin. CancerRes. 5 (1999) 251–256.
[168] C.C. Benz, G.K. Scott, J.C. Sarup, R.M. Johnson, D. Tripathy, E. Coronado, H.M.Shepard, C.K. Osborne, Estrogen-dependent, tamoxifen-resistant tumorigenicgrowth of MCF-7 cells transfected with HER2/neu, Breast Cancer Res. Treat. 24(1992) 85–95.
[169] Y.L. Chung, M.L. Sheu, S.C. Yang, C.H. Lin, S.H. Yen, Resistance to tamoxifen-induced apoptosis is associated with direct interaction between Her2/neu andcell membrane estrogen receptor in breast cancer, Int. J. Cancer 97 (2002)306–312.
[170] M.J. Ellis, A. Coop, B. Singh, L. Mauriac, A. Llombert-Cussac, F. Jänicke, W.R. Miller,D.B. Evans, M. Dugan, C. Brady, E. Quebe-Fehling, M. Borgs, Letrozole is moreeffective neoadjuvant endocrine therapy than tamoxifen for ErbB-1- and/or
ErbB-2-positive, estrogen receptor-positive primary breast cancer: evidencefrom a phase III randomized trial, J. Clin. Oncol. 19 (2001) 3808–3816.
[171] M. Dowsett, J. Cuzick, C. Wale, T. Howell, J. Houghton, M. Baum, Retrospectiveanalysis of time to recurrence in the ATAC trial according to hormone receptorstatus: an hypothesis-generating study, J. Clin. Oncol. 23 (2005) 7512–7517.
[172] I.R. Hutcheson, J.M. Knowlden, T.A. Madden, D. Barrow, J.M. Gee, A.E.Wakeling, R.I. Nicholson, Oestrogen receptor-mediated modulation of the EGFR/MAPKpathway in tamoxifen-resistant MCF-7 cells, Breast Cancer Res. Treat. 81 (2003)81–93.
[173] N.J. Jordan, J.M. Gee, D. Barrow, A.E. Wakeling, R.I. Nicholson, Increasedconstitutive activity of PKB/Akt in tamoxifen resistant breast cancer MCF-7cells, Breast Cancer Res. Treat. 87 (2004) 167–180.
[174] J.M. Knowlden, I.R. Hutcheson, D. Barrow, J.M. Gee, R.I. Nicholson, Insulin-likegrowth factor-I receptor signaling in tamoxifen-resistant breast cancer: asupporting role to the epidermal growth factor receptor, Endocrinology 146(2005) 4609–4618.
[175] A. Brodie, G. Sabnis, L. Macedo, Xenograft models for aromatase inhibitor studies,J. Steroid Biochem. Mol. Biol. 106 (2007) 119–124.
[176] X. Wang, S. Masri, S. Phung, S. Chen, The role of amphiregulin in exemestane-resistant breast cancer cells: evidence of an autocrine loop, Cancer Res. 68 (2008)2259–2265.
[177] J.N. Holloway, S. Murthy, D. El-Ashry, A cytoplasmic substrate of mitogen-activated protein kinase is responsible for estrogen-alpha down-regulation inbreast cancer cells: the role of nuclear factor-kappa B, Mol. Endocrinol. 18 (2004)1396–1410.
[178] Y. Zhou, S. Eppenberger-Castori, U. Eppenberger, C.C. Benz, The NFkB pathwayand endocrine-resistant breast cancer, Endocr. Relat. Cancer 12 (2005)S37–S46.
[179] A. Mawson, A. Lai, J.S. Carroll, C.M. Sergio, C.J. Mitchell, B. Sarcevic, Estrogen andinsulin/IGF-I cooperatively stimulate cell cycle progression in MCF-7 breastcancer cells through differential regulation of c-Myc and cyclin D1, Mol. Cell.Endocrinol. 229 (2005) 161–173.
[180] S. Chen, S. Masri, X. Wang, S. Phung, Y.C. Yuan, X. Wu, What do we know aboutthe mechanisms of aromatase inhibitor resistance? J. Steroid Biochem. Mol. Biol.102 (2006) 232–240.
[181] R.J. Santen, R.X. Song, Z. Zhang, R. Kumar, M.H. Jeng, S. Masamura, W. Yue, L.Berstein, Adaptive hypersensitivity to estrogen: mechanism for superiority ofaromatase inhibitors over selective estrogen receptor modulators for breastcancer treatment and prevention, Endocr. Relat. Cancer 10 (2003) 111–130.
[182] R.J. Santen, R.X. Song, Z. Zhang, R. Kumar, M.H. Jeng, A. Masamura, J. Lawrence, L.Berstein, W. Yue, Long-term estradiol deprivation in breast cancer cells up-regulates growth factor signaling and enhances estrogen sensitivity, Endocr.Relat. Cancer 12 (suppl 1) (2005) S61–S73.
[183] R.J. Santen, R.X. Song, Z. Zhang, W. Yue, R. Kumar, Adaptive hypersensitivity toestrogen: mechanism for sequential responses to hormonal therapy in breastcancer, Clin. Cancer Res. 10 (2004) 337S–345S.
[184] C.M. Chan, L.A. Martin, S.R. Johnston, S. Ali, M. Dowsett, Molecular changesassociated with the acquisition of estrogen hypersensitivity in MCF-7 breastcancer cells on long-term estrogen deprivation, J. Steroid Biochem, Mol. Biol. 81(2002) 333–341.
[185] L.A. Martin, I. Farmer, S.R. Johnston, S. Ali, C. Marshall, M. Dowsett, Enhancedestrogen receptor (ER) alpha, ERBB2, and MAPK signal transduction pathwaysoperate during the adaptation ofMCF-7 cells to long term estrogen deprivation, J.Biol. Chem. 278 (2003) 30458–30468.
[186] J. Font de Mora, M. Brown, AIB1 is a conduit for kinase-mediated growth factorsignaling to the estrogen receptor, Mol. Cell. Biol. 20 (2000) 5041–5047.
[187] H.J. List, R. Reiter, B. Singh, A. Wellstein, A.T. Riegel, Expression of the nuclearcoactivator AIB1 in normal and malignant breast tissue, Breast Cancer Res. Treat.68 (2001) 21–28.
[188] M. Dowsett, L.A. Martin, I. Smith, S. Johnston, Mechanisms of resistance toaromatase inhibitors, J. Steroid Biochem, Mol. Biol. 95 (2005) 167–172.
[189] S.R. Johnston, L.A. Martin, M. Dowsett, Life following aromatase inhibitors-werenow for endocrine sequencing? Breast Cancer Res. Treat. 93 (2005) S19–S25.
[190] V.V. Jordan, M.M. Collins, L. Rowsby, G. Prestwich, A monohydroxylatedmetabolite of tamoxifen with potent antioestrogenic activity, J. Endocrinol. 75(1977) 305–316.
[191] V.C. Jordan, Metabolites of tamoxifen in animals and man: identification,pharmacology, and significance, Breast Cancer Res. Treat. 2 (1982) 123–138.
[192] M.D. Johnson, H. Zuo, K.H. Lee, J.P. Trebley, J.M. Rae, R.V. Weatherman, Z. Desta, D.A. Flockhart, T.C. Skaar, Pharmacological characterization of 4-hydroxy-Ndes-methyl tamoxifen, a novel active metabolite of tamoxifen, Breast Cancer Res.Treat. 85 (2004) 151–159.
[193] V. Stearns, M.D. Johnson, J.M. Rae, A. Morocho, A. Novielli, P. Bhargava, D.F. Hayes,Z. Desta, D.A. Flockhart, Active tamoxifen metabolite plasma concentrations aftercoadministration of tamoxifen and the selective serotonin reuptake inhibitorparoxetine, J. Natl. Cancer Inst. 95 (2003) 1758–1764.
[194] Y. Jin, Z. Desta, V. Stearns, B. Ward, H. Ho, K.H. Lee, T. Skaar, A.M. Storniolo, L. Li, A.Araba, R. Blanchard, A. Nguyen, L. Ullmer, J. Hayden, S. Lemler, R.M.Weinshilboum, J.M. Rae, D.F. Hayes, D.A. Flockhart, CYP2D6 genotype, anti-depressant use, and tamoxifen metabolism during adjuvant breast cancertreatment, J. Natl. Cancer Inst. 97 (2005) 30–39.
[195] S. Borges, Z. Desta, L. Li, T.C. Skaar, B.A. Ward, A. Nguyen, Y. Jin, A.M. Storniolo, D.M. Nikoloff, L. Wu, G. Hillman, D.F. Hayes, V. Stearns, D.A. Flockhart, Quantitativeeffect of CYP2D6 genotype and inhibitors on tamoxifen metabolism: implicationfor optimization of breast cancer treatment, Clin. Pharmacol. Ther. 80 (2006)61–74.

79M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
[196] Z. Desta, B.A. Ward, N.V. Soukhova, D.A. Flockhart, Comprehensive evaluation oftamoxifen sequential biotransformation by the human cytochrome P450 systemin vitro: prominent roles for CYP3A and CYP2D6, J. Pharmacol. Exp. Ther. 310(2004) 1062–1075.
[197] U.M. Zanger, S. Raimundo, M. Eichelbaum, Cytochrome P450 2D6: overview andupdate on pharmacology, genetics, biochemistry, Naunyn Schmiedebergs Arch.Pharmacol. 369 (2004) 23–37.
[198] S.L. Wang, J.D. Huang, M.D. Lai, B.H. Liu, M.L. Lai, Molecular basis of geneticvariation in debrisoquin hydroxylation in Chinese subjects: polymorphism inRFLP and DNA sequence of CYP2D6, Clin. Pharmacol. Ther. 53 (1993)410–418.
[199] M.P. Goetz, J.M. Rae, V.J. Suman, S.L. Safgren, M.M. Ames, D.W. Visscher, C.Reynolds, F.J. Couch, W.L. Lingle, D.A. Flockhart, Z. Desta, E.A. Perez, J.N. Ingle,Pharmacogenetics of tamoxifen biotransformation is associated with clinicaloutcomes of efficacy and hot flashes, J. Clin. Oncol. 23 (2005) 9312–9318.
[200] W. Schroth, L. Antoniadou, P. Fritz, M. Schwab, T. Muerdter, U.M. Zanger, W.Simon, M. Eichelbaum, H. Brauch, Breast cancer treatment outcome withadjuvant tamoxifen relative to patient CYP2D6 and CYP2C19 genotypes, J. Clin.Oncol. 25 (2007) 5187–5193.
[201] A.M. Dunning, H. Dowsett, C.S. Healey, L. Tee, R.N. Luben, E. Folkerd, K.L. Novik, L.Kelemen, S. Ogata, P.D. Pharoah, D.F. Easton, N.E. Day, B.A. Ponder, Polymorph-isms associated with circulating sex hormone levels in postmenopausal women,J. Natl. Cancer Inst. 96 (2004) 936–945.
[202] C.X. Ma, A.A. Adjei, O.E. Salavaggione, J. Coronel, L. Pelleymounter, L. Wang, B.W.Eckloff, D. Schaid, E.D. Wieben, A.A. Adjei, R.M. Weinshilboum, Humanaromatase: gene resequencing and functional genomics, Cancer Res. 65 (2005)11071–11082.
[203] S.V. Otton, S.E. Ball, S.W. Cheung, T. Inaba, R.L. Rudolph, E.M. Sellers, Venlafaxineoxidation in vitro is catalysed by CYP2D6, Br. J. Clin. Pharmacol. 41 (1996)149–156.
[204] M.P. Goetz, S.K. Knox, V.J. Suman, J.M. Rae, S.L. Safgren, M.M. Ames, D.W. Visscher,C. Reynolds, F.J. Couch, W.L. Lingle, R.M. Weinshilboum, E.G. Fritcher, A.M. Nibbe,Z. Desta, A. Nguyen, D.A. Flockhart, E.A. Perez, J.N. Ingle, The impact ofcytochrome P450 2D6 metabolism in women receiving adjuvant tamoxifen,Breast Cancer Res. Treat. 101 (2007) 113–121.
[205] S. Ali, R.C. Coombes, Endocrine-responsive breast cancer and strategies forcombating resistance, Nat. Rev. Cancer 2 (2002) 101–112.
[206] A. Ring, M. Dowsett, Mechanisms of tamoxifen resistance, Endocr. Relat. Cancer11 (2004) 643–658.
[207] R.W. Carlson, Sequencing of endocrine therapies in breast cancer-integration ofrecent data, Breast Cancer Res. Treat. 75 (Suppl 1) (2002) S27–S32.
[208] P. Dombernowsky, I. Smith, G. Falkson, R. Leonard, L. Panasci, J. Bellmunt, W.Bezwoda, G. Gardin, A. Gudgeon, M. Morgan, A. Fornasiero, W. Hoffmann, J.Michel, T. Hatschek, T. Tjabbes, H.A. Chaudri, U. Hornberger, P.F. Trunet, Letrozole,a new oral aromatase inhibitor for advanced breast cancer: double-blindrandomized trial showing a dose effect and improved efficacy and tolerabilitycompared with megestrol acetate, J. Clin. Oncol. 16 (1998) 453–461.
[209] A.U. Buzdar, W. Jonat, A. Howell, S.E. Jones, C.P. Blomqvist, C.L. Vogel, W.Eiermann, J.M. Wolter, M. Steinberg, A. Webster, D. Lee, Anastrozole versusmegestrol acetate in the treatment of post-menopausal women with advancedbreast carcinoma: results of a survival update based on a combined analysis ofdata from two mature phase III trials. Arimidex Study Group, Cancer 83 (1998)1142–1152.
[210] R.C. Coombes, L.S. Kilburn, C.F. Snowdon, R. Paridaens, R.E. Coleman, S.E. Jones, J.Jassem, C.J. Van de Velde, T. Delozier, I. Alvarez, L. Del Mastro, O. Ortmann, K.Diedrich, A.S. Coates, E. Bajetta, S.B. Holmberg, D. Dodwell, E. Mickiewicz, J.Andersen, P.E. Lønning, G. Cocconi, J. Forbes, M. Castiglione, N. Stuart, A. Stewart,L.J. Fallowfield, G. Bertelli, E. Hall, R.G. Bogle, M. Carpentieri, E. Colajori, M. Subar,E. Ireland, J.M. Bliss, Survival and safety of exemestane versus tamoxifen after 2–3 years' tamoxifen treatment (Intergroup Exemestane Study): a randomisedcontrolled trial, Lancet 369 (2007) 559–570.
[211] M. Kaufmann, W. Jonat, J. Hilfrich, H. Eidtmann, G. Gademann, I. Zuna, G. vonMinckwitz, Improved overall survival in postmenopausal women with earlybreast cancer after anastrozole initiated after treatment with tamoxifencompared with continued tamoxifen: the ARNO 95 study, J. Clin. Oncol. 25(2007) 2664–2670.
[212] F. Boccardo, A. Rubagotti, M. Puntoni, P. Guglielmini, D. Amoroso, A. Fini, G.Paladini, M. Mesiti, D. Romeo, M. Rinaldini, S. Scali, M. Porpiglia, C. Benedetto, N.Restuccia, F. Buzzi, R. Franchi, B. Massidda, V. Distante, D. Amadori, P. Sismondi,Switching to anastrozole versus continued tamoxifen treatment of early breastcancer: preliminary results of the Italian tamoxifen anastrozole trial, J. Clin.Oncol. 23 (2005) 5138–5147.
[213] R. Jakesz, W. Jonat, M. Gnant, M. Mittlboeck, R. Greil, C. Tausch, J. Hilfrich, W.Kwasny, C. Menzel, H. Samonigg, M. Seifert, G. Gademann, M. Kaufmann, J.Wolfgang, Switching of postmenopausal women with endocrine-responsiveearly breast cancer to anastrozole after 2 years' adjuvant tamoxifen: combinedresults of ABCSG trial 8 and ARNO 95 trial, Lancet 366 (2005) 455–462.
[214] I. Vergote, J.F. Robertson, U. Kleeberg, G. Burton, C.K. Osborne, L. Mauriac,Postmenopausal women who progress on fulvestrant (‘Faslodex’) remainsensitive to further endocrine therapy, Breast Cancer Res. Treat. 79 (2003)207–211.
[215] P.E. Lønning, E. Bajetta, R. Murray, M. Tubiana-Hulin, P.D. Eisenberg, E.Mickiewicz, L. Celio, P. Pitt, M. Mita, N.K. Aaronson, C. Fowst, A. Arkhipov, E. DiSalle, A. Polli, G. Massimini, Activity of exemestane in metastatic breast cancerafter failure of nonsteroidal aromatase inhibitors: a phase II trial, J. Clin. Oncol. 18(2000) 2234–2244.
[216] S. Chia, W. Gradishar, L. Mauriac, J. Bines, F. Amant, M. Federico, L. Fein, G.Romieu, A. Buzdar, J.F. Robertson, A. Brufsky, K. Possinger, P. Rennie, F. Sapunar, E.Lowe, M. Piccart, Double-blind randomized placebo controlled trial of fulvestrantcompared with exemestane after prior nonsteroidal aromatase inhibitor therapyin postmenopausal women with hormone receptor-positive, advanced breastcancer: results from EFECT, J. Clin. Oncol. 26 (2008) 1664–1670.
[217] M. Baum, A.U. Buzdar, J. Cuzick, J. Forbes, J.H. Houghton, J.G. Klijn, T. Sahmoud,Anastrozole alone or in combination with tamoxifen versus tamoxifen alone foradjuvant treatment of postmenopausal women with early breast cancer: firstresults of the ATAC randomized trial, Lancet 359 (2002) 2131–2139.
[218] J.N. Ingle, V.J. Suman, P.A. Johnson, J.E. Krook, J.A. Mailliard, R.H. Wheeler, C.L.Loprinzi, E.A. Perez, V.C. Jordan, M. Dowsett, Evaluation of tamoxifen plusletrozole with assessment of pharmacokinetic interaction in postmenopausalwomen with metastatic breast cancer, Clin. Cancer Res. 5 (1999) 1642–1649.
[219] M. Dowsett, J. Cuzick, A. Howell, I. Jackson, Pharmacokinetics of anastrozole andtamoxifen alone, and in combination, during adjuvant endocrine therapy forearly breast cancer in postmenopausal women: a sub-protocol of the ‘Arimidexand tamoxifen alone or in combination’ (ATAC) trial, Br. J. Cancer 85 (2001)317–324.
[220] Q. Lu, Y. Liu, B.J. Long, D. Grigoryev, M. Gimbel, A. Brodie, The effect of combiningaromatase inhibitors with antiestrogens on tumor growth in a nude mousemodel for breast cancer, Breast Cancer Res. Treat. 57 (1999) 183–192.
[221] L.F. Macedo, G.J. Sabnis, O.G. Goloubeva, A. Brodie, Combination of anastrozolewith fulvestrant in the intratumoral aromatase xenograft model, Cancer Res. 68(2008) 3516–3522.
[222] J.S. Ross, J.A. Fletcher, K.J. Bloom, G.P. Linette, J. Stec, W.F. Symmans, L. Pusztai, G.N. Hortobagyi, Targeted therapy in breast cancer: the HER-2/neu gene andprotein, Mol. Cell Proteomics 3 (2004) 370–398.
[223] J.C. Hu, K. Mokbel, Does c-erbB2/HER2 overexpression predict adjuvanttamoxifen failure in patients with early breast cancer? Eur J Surg Oncol 27(2001) 335–337.
[224] M. Dowsett, S. Johnston, L.A. Martin, J. Salter, M. Hills, S. Detre, M.C. Gutierrez, S.K. Mohsin, J. Shou, D.C. Allred, R. Schiff, C.K. Osborne, I. Smith, Growth factorsignalling and response to endocrine therapy: the Royal Marsden experience,Endocr. Relat. Cancer 12 (2005) 113S–117S.
[225] D.A. Berry, H.B. Muss, A.D. Thor, L. Dressler, E.T. Liu, G. Broadwater, D.R. Budman,I.C. Henderson, M. Barcos, D. Hayes, L. Norton, HER-2/neu and p53 expressionversus tamoxifen resistance in estrogen receptor-positive, node-positive breastcancer, J. Clin. Oncol. 18 (2000) 3471–3479.
[226] A.S. Knoop, S.M. Bentzen, N.M. Nielsen, B.B. Rasmussen, C. Rose, Value ofepidermal growth factor receptor, HER2, p53, and steroid receptors in predictingthe efficacy of tamoxifen in high-risk postmenopausal breast cancer patients, J.Clin. Oncol. 19 (2001) 3376–3384.
[227] L. Zhu, L.W. Chow, W.T. Loo, X.Y. Guan, M. Toi, Her2/neu expression predicts theresponse to antiaromatase neoadjuvant therapy in primary breast cancer:subgroup analysis from celecoxib antiaromatase neoadjuvant trial, Clin. CancerRes. 10 (2004) 4639–4644.
[228] B.B. Rasmussen, M.M. Regan, A.E. Lykkesfeldt, P. Dell'Orto, B. Del Curto, K.L.Henriksen, M.G. Mastropasqua, K.N. Price, E. Méry, M. Lacroix-Triki, S. Braye, H.J.Altermatt, R.D. Gelber, M. Castiglione-Gertsch, A. Goldhirsch, B.A. Gusterson, B.Thürlimann, A.S. Coates, G. Viale, BIG 1-98 Collaborative and International BreastCancer Study Groups, Adjuvant letrozole versus tamoxifen according tocentrally-assessed ERBB2 status for postmenopausal women with endocrine-responsive early breast cancer: supplementary results from the BIG 1-98randomised trial, Lancet Oncol. 9 (2008) 23–28.
[229] M. Dowsett, C. Allred, J. Knox, E. Quinn, J. Salter, C. Wale, J. Cuzick, J. Houghton, N.Williams, E. Mallon, H. Bishop, I. Ellis, D. Larsimont, H. Sasano, P. Carder, A.L.Cussac, F. Knox, V. Speirs, J. Forbes, A. Buzdar, Relationship between quantitativeestrogen and progesterone receptor expression and human epidermal growthfactor receptor 2 (HER-2) status with recurrence in the arimidex, tamoxifen,alone or in combination trial, J. Clin. Oncol. 26 (2008) 1059–1065.
[230] M.J. Ellis, Y. Tao, O. Young, S.White, A.D. Proia, J. Murray, L. Renshaw, D. Faratian, J.Thomas, M. Dowsett, A. Krause, D.B. Evans, W.R. Miller, J.M. Dixon, Estrogen-independent proliferation is present in estrogen-receptor HER2-positiveprimary breast cancer after neoadjuvant letrozole, J. Clin. Oncol. 24 (2006)3019–3025.
[231] M. De Laurentiis, G. Arpino, E. Massarelli, A. Ruggiero, C. Carlomagno, F.Ciardiello, G. Tortora, D. D'Agostino, F. Caputo, G. Cancello, A meta-analysis onthe interaction between HER-2 expression and response to endocrine treatmentin advanced breast cancer, Clin. Cancer Res. 11 (2005) 4741–4748.
[232] R. Bartsch, C.Wenzel, G. Altorjai, U. Pluschnig, R.M. Mader, M. Gnant, R. Jakesz, M.Rudas, C.C. Zielinski, G.G. Steger, Her2 and progesterone receptor status are notpredictive of response to fulvestrant treatment, Clin. Cancer Res. 13 (2007)4435–4439.
[233] P.M. Ravdin, S. Green, T.M. Dorr, W.L. McGuire, C. Fabian, R.P. Pugh, R.D. Carter, S.E. Rivkin, J.R. Borst, R.J. Belt, Prognostic significance of progesterone receptorlevels in estrogen receptor-positive patients with metastatic breast cancertreated with tamoxifen: results of a prospective Southwest Oncology Groupstudy, J. Clin. Oncol. 10 (1992) 1284–1291.
[234] R.M. Elledge, S. Green, R. Pugh, D.C. Allred, G.M. Clark, J. Hill, P. Ravdin, S. Martino,C.K. Osborne, Estrogen receptor (ER) and progesterone receptor (PgR), by ligand-binding assay compared with ER, PgR and pS2, by immuno-histochemistry inpredicting response to tamoxifen in metastatic breast cancer: a SouthwestOncology Group study, Int. J. Cancer 89 (2000) 111–117.
[235] M. Fernö, O. Stål, B. Baldetorp, T. Hatschek, A.C. Källström, P. Malmström, B.Nordenskjöld, S. Rydën, Results of two or five years of adjuvant tamoxifen

80 M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
correlated to steroid receptor and S-phase levels: South Sweden Breast CancerGroup, and South-East Sweden Breast Cancer Group, Breast Cancer Res. Treat. 59(2000) 69–76.
[236] V.J. Bardou, G. Arpino, R.M. Elledge, C.K. Osborne, G.M. Clark, Progesteronereceptor status significantly improves outcome prediction over estrogenreceptor status alone for adjuvant endocrine therapy in two large databases, J.Clin. Oncol. 21 (2003) 1973–1979.
[237] C.K. Osborne, J. Shou, S. Massarweh, R. Schiff, Crosstalk between estrogenreceptor and growth factor receptor pathways as a cause for endocrine therapyresistance in breast cancer, Clin. Cancer Res. 11 (2005) 865s–870s.
[238] X. Cui, R. Schiff, G. Arpino, C.K. Osborne, A.V. Lee, Biology of progesteronereceptor loss in breast cancer and its implications for endocrine therapy, J. Clin.Oncol. 23 (2005) 7721–7735.
[239] X. Cui, P. Zhang, W. Deng, S. Oesterreich, Y. Lu, G.B. Mills, A.V. Lee, Insulin-likegrowth factor-I inhibits progesterone receptor expression in breast cancer cellsvia the phosphatidylinositol 3-kinase/AKT/mammalian target of rapamycinpathway: progesterone receptor as a potential indicator of growth factor activityin breast cancer, Mol. Endocrinol. 17 (2003) 575–588.
[240] H.J. Kim, X. Cui, S.G. Hilsenbeck, A.V. Lee, Progesterone receptor loss correlateswith human epidermal growth factor receptor 2 overexpression in estrogenreceptor-positive breast cancer, Clin. Cancer Res. 12 (2006) 1013S–1018S.
[241] H. Kurokawa, A.E. Lenferink, J.F. Simpson, P.I. Pisacane, M.X. Sliwkowski, J.T.Forbes, C.L. Arteaga, Inhibition of HER2/neu (erbB-2) and mitogen-activatedprotein kinases enhances tamoxifen action against HER2-overexpressing,tamoxifen-resistant breast cancer cells, Cancer Res. 60 (2000) 5887–5894.
[242] G. Viale, M.M. Regan, E. Maiorano, M.G. Mastropasqua, P. Dell'Orto, B.B.Rasmussen, J. Raffoul, P. Neven, Z. Orosz, S. Braye, C. Ohlschlegel, B. Thürlimann,R.D. Gelber, M. Castiglione-Gertsch, K.N. Price, A. Goldhirsch, B.A. Gusterson, A.S.Coates, Prognostic and predictive value of centrally reviewed expression ofestrogen and progesterone receptors in a randomized trial comparing letrozoleand tamoxifen adjuvant therapy for postmenopausal early breast cancer: BIG 1-98, J. Clin. Oncol. 25 (2007) 3846–3852.
[243] P.E. Goss, J.N. Ingle, S. Martino, N.J. Robert, H.B. Muss, M.J. Piccart, M. Castiglione,D. Tu, L.E. Shepherd, K.I. Pritchard, R.B. Livingston, N.E. Davidson, L. Norton, E.A.Perez, J.S. Abrams, D.A. Cameron, M.J. Palmer, J.L. Pater, Efficacy of letrozoleextended adjuvant therapy according to estrogen receptor and progesteronereceptor status of the primary tumor: National Cancer Institute of CanadaClinical Trials Group MA.17, J. Clin. Oncol. 25 (2007) 2006–2011.
[244] V.C. Jordan, R.D. Gelber, Problems with the progesterone receptor in practice? J.Clin. Oncol. 25 (2007) 1957–1959.
[245] F.L. Baehner, Quantitative RT-PCR analysis of ER and PR by oncotype DX indicatesdistinct and different associations with prognosis and prediction of tamoxifenbenefit, 29th Annual San Antonio Breast Cancer Symposium (Abs 45), BreastCancer Res. Treat. 100 (2006) S20.
[246] M.E. Meijer-van Gelder, M.P. Look, H.A. Peters, M. Schmitt, N. Brünner, N.Harbeck, J.G. Klijn, J.A. Foekens, Urokinase-type plasminogen activator system inbreast cancer: association with tamoxifen therapy in recurrent disease, CancerRes. 64 (2004) 4563–4568.
[247] P.N. Span, R.L. Lindberg, P. Manders, V.C. Tjan-Heijnen, J.J. Heuvel, L.V. Beex, C.G.Sweep, Tissue inhibitors of metalloproteinase expression in human breastcancer: TIMP-3 is associated with adjuvant endocrine therapy success, J. Pathol.202 (2004) 395–402.
[248] L. Rydén, M. Stendahl, H. Jonsson, S. Emdin, N.O. Bengtsson, G. Landberg, Tumor-specific VEGF-A and VEGFR2 in postmenopausal breast cancer patients withlong-term follow-up. Implication of a link between VEGF pathway and tamoxifenresponse, Breast Cancer Res. Treat. 89 (2005) 135–143.
[249] L. Rydén, K. Jirström, P.O. Bendahl, M. Fernö, B. Nordenskjöld, O. Stål, S.Thorstenson, P.E. Jönsson, G. Landberg, Tumor-specific expression of vascularendothelial growth factor receptor 2 but not vascular endothelial growth factoror human epidermal growth factor receptor 2 is associated with impairedresponse to adjuvant tamoxifen in premenopausal breast cancer, J. Clin. Oncol. 23(2005) 4695–4704.
[250] H. Yamashita, T. Toyama, M. Nishio, Y. Ando, M. Hamaguchi, Z. Zhang, S.Kobayashi, Y. Fujii, H. Iwase, p53 protein accumulation predicts resistance toendocrine therapy and decreased post-relapse survival in metastatic breastcancer, Breast Cancer Res. 8 (2006) R48.
[251] J. Bostner, M. Ahnström Waltersson, T. Fornander, L. Skoog, B. Nordenskjöld, O.Stål, Amplification of CCND1 and PAK1 as predictors of recurrence and tamoxifenresistance in postmenopausal breast cancer, Oncogene 26 (2007) 6997–7005.
[252] Y. Ishii, S. Waxman, D. Germain, Tamoxifen stimulates the growth of cyclin D1-overexpressing breast cancer cells by promoting the activation of signaltransducer and activator of transcription 3, Cancer Res. 68 (2008) 852–860.
[253] B. Linderholm, K. Grankvist, N. Wilking, M. Johansson, B. Tavelin, R. Henriksson,Correlation of vascular endothelial growth factor content with recurrences,survival, and first relapse site in primary node-positive breast carcinoma afteradjuvant treatment, J. Clin. Oncol. 18 (2000) 1423–1431.
[254] D. Coradini, E. Biganzoli, C. Pellizzaro, S. Veneroni, S. Oriana, F. Ambrogi, R. Erdas,P. Boracchi, M.G. Daidone, E. Marubini, Vascular endothelial growth factor innode-positive breast cancer patients treated with adjuvant tamoxifen, Br. J.Cancer 89 (2003) 268–270.
[255] R.M. Elledge, S. Green, L. Howes, G.M. Clark, M. Berardo, D.C. Allred, R. Pugh, D.Ciocca, P. Ravdin, J. O'Sullivan, S. Rivkin, S. Martino, C.K. Osborne, bcl-2, p53, andresponse to tamoxifen in estrogen receptor-positive metastatic breast cancer: aSouthwest Oncology Group study, J. Clin. Oncol. 15 (1997) 1916–1922.
[256] A.F. Chambers, L.M. Matrisian, Changing views of the role of matrix metallopro-teinases in metastasis, J. Natl. Cancer Inst. 89 (1997) 1260–1270.
[257] A.H. Baker, S.J. George, A.B. Zaltsman, G. Murphy, A.C. Newby, Inhibition ofinvasion and induction of apoptotic cell death of cancer cell lines by over-expression of TIMP-3, Br. J. Cancer 79 (1999) 1347–1355.
[258] K. Helin, Regulation of cell proliferation by the E2F transcription factors, Curr.Opin. Genet. Dev. 8 (1998) 28–35.
[259] R.M. Zwijsen, E. Wientjens, R. Klompmaker, J. van der Sman, R. Bernards, R.J.Michalides, CDK-independent activation of estrogen receptor by cyclin D1, Cell88 (1997) 405–415.
[260] C. Gillett, P. Smith, W. Gregory, M. Richards, R. Millis, G. Peters, D. Barnes, CyclinD1 and prognosis in human breast cancer, Int. J. Cancer 69 (1996) 92–99.
[261] M. Stendahl, A. Kronblad, L. Rydén, S. Emdin, N.O. Bengtsson, G. Landberg,Cyclin D1 overexpression is a negative predictive factor for tamoxifenresponse in postmenopausal breast cancer patients, Br. J. Cancer 90 (2004)1942–1948.
[262] K. Jirström, M. Stendahl, L. Rydén, A. Kronblad, P.O. Bendahl, O. Stål, G. Landberg,Adverse effect of adjuvant tamoxifen in premenopausal breast cancer with cyclinD1 gene amplification, Cancer Res. 65 (2005) 8009–8016.
[263] M.J. Duffy, T.M. Maguire, E.W. McDermott, N. O'Higgins, Urokinase plasminogenactivator: a prognostic marker in multiple types of cancer, J. Surg. Oncol. 71(1999) 130–135.
[264] F. Cardoso, Microarray technology and its effect on breast cancer (re)classification and prediction of outcome, Breast Cancer Res. 5 (2003) 303–304.
[265] S. Maier, I. Nimmrich, T. Koenig, S. Eppenberger-Castori, I. Bohlmann, A. Paradiso,F. Spyratos, C. Thomssen, V. Mueller, J. Nährig, F. Schittulli, R. Kates, R. Lesche, I.Schwope, A. Kluth, A. Marx, J.W. Martens, J.A. Foekens, M. Schmitt, N. Harbeck,European Organisation for Research and Treatment of Cancer (EORTC)PathoBiology group, DNA-methylation of the homeodomain transcription factorPITX2 reliably predicts risk of distant disease recurrence in tamoxifen-treated,node-negative breast cancer patients—technical and clinical validation in amulti-centre setting in collaboration with the European Organisation forResearch and Treatment of Cancer (EORTC) PathoBiology group, Eur. J. Cancer43 (2007) 1679–1686.
[266] S. Paik, S. Shak, G. Tang, C. Kim, J. Baker, M. Cronin, F.L. Baehner, M.G. Walker, D.Watson, T. Park, W. Hiller, E.R. Fisher, D.L. Wickerham, J. Bryant, N. Wolmark, Amultigene assay to predict recurrence of tamoxifen-treated, node-negativebreast cancer, N. Engl. J. Med. 351 (2004) 2817–2826.
[267] X.J. Ma, Z. Wang, P.D. Ryan, S.J. Isakoff, A. Barmettler, A. Fuller, B. Muir, G.Mohapatra, R. Salunga, J.T. Tuggle, Y. Tran, D. Tran, A. Tassin, P. Amon, W. Wang,W. Wang, E. Enright, K. Stecker, E. Estepa-Sabal, B. Smith, J. Younger, U. Balis, J.Michaelson, A. Bhan, K. Habin, T.M. Baer, J. Brugge, D.A. Haber, M.G. Erlander, D.C.Sgroi, A two-gene expression ratio predicts clinical outcome in breast cancerpatients treated with tamoxifen, Cancer Cell 5 (2004) 607–616.
[268] M.P. Jansen, J.A. Foekens, I.L. van Staveren, M.M. Dirkzwager-Kiel, K. Ritstier, M.P.Look, M.E. Meijer-van Gelder, A.M. Sieuwerts, H. Portengen, L.C. Dorssers, J.G.Klijn, E.M. Berns, Molecular classification of tamoxifen-resistant breast carcino-mas by gene expression profiling, J Clin Oncol 23 (2005) 732–740.
[269] D. Meijer, T. van Agthoven, P.T. Bosma, K. Nooter, L.C. Dorssers, Functional screenfor genes responsible for tamoxifen resistance in human breast cancer cells, MolCancer Res 4 (2006) 379–386.
[270] D. Meijer, A.M. Sieuwerts, M.P. Look, T. van Agthoven, J.A. Foekens, L.C.Dorssers, Fibroblast growth factor receptor 4 predicts failure on tamoxifentherapy in patients with recurrent breast cancer, Endocr Relat Cancer 15(2008) 101–111.
[271] E. Iorns, N.C. Turner, R. Elliott, N. Syed, O. Garrone, M. Gasco, A.N. Tutt, T. Crook,C.J. Lord, A. Ashworth, Identification of CDK10 as an important determinant ofresistance to endocrine therapy for breast cancer, Cancer Cell 13 (2008)91–104.
[272] L. Witters, L. Engle, A. Lipton, Restoration of estrogen responsiveness by blockingthe HER-2/neu pathway, Oncol. Rep. 9 (2002) 1163–1166.
[273] R.I. Nicholson, I.R. Hutcheson, J.M. Knowlden, H.E. Jones, M.E. Harper, N. Jordan, S.E. Hiscox, D. Barrow, J.M. Gee, Nonendocrine pathways and endocrine resistance:observations with antiestrogens and signal transduction inhibitors in combina-tion, Clin. Cancer Res. 10 (2004) 346S–354S.
[274] S.R. Johnston, J. Head, S. Pancholi, S. Detre, L.A. Martin, I.E. Smith, M. Dowsett,Integration of signal transduction inhibitors with endocrine therapy: anapproach to overcoming hormone resistance in breast cancer, Clin. Cancer Res.9 (2003) 524S–532S.
[275] S.R. Johnston, Clinical trials of intracellular signal transductions inhibitors forbreast cancer—a strategy to overcome endocrine resistance, Endocr. Relat.Cancer 12 (2005) S145–S157.
[276] C.A. Ellis, M.D. Vos, M. Wickline, C. Riley, T. Vallecorsa, W.G. Telford, J. Zujewskil,G.J. Clark, Tamoxifen and the farnesyl transferase inhibitor FTI-227 synergize toinhibit growth in estrogen receptor-positive breast tumor cell lines, BreastCancer Res. Treat. 78 (2003) 59–67.
[277] S. Pancholi, A. Lykkesfeldt, M. Dowsett, S. Johnston, L.A. Martin, Elevated levelsof AKT and p90rsk provide tamoxifen-resistant MCF-7 cells with a survivaladvantage involving Bad and Bcl-2, Proc. Am. Assoc. Cancer Res. 45 (2004)A5168.
[278] L.A. deGraffenried, W.E. Friedrichs, D.H. Russell, E.J. Donzis, A.K. Middleton, J.M.Silva, R.A. Roth, M. Hidalgo, Inhibition of mTOR activity restores tamoxifenresponse in breast cancer cells with aberrant AKT activity, Clin. Cancer Res. 10(2004) 8059–8067.
[279] S.R. Johnston, L.A. Martin, J. Head, I. Smith, M. Dowsett, Aromatase inhibitors:combinations with fulvestrant or signal transduction inhibitors as a strategyto overcome endocrine resistance, J. Steroid Biochem. Mol. Biol. 95 (2005)173–181.

81M. Zilli et al. / Biochimica et Biophysica Acta 1795 (2009) 62–81
[280] I. Chu, K. Blackwell, S. Chen, J. Slingerland, The dual ErbB1/ErbB2 inhibitorlapatinib (GW572016) cooperates with tamoxifen to inhibit both cell prolifera-tion and estrogen-dependent gene expression in antiestrogen resistant breastcancer, Cancer Res. 65 (2005) 18–25.
[281] G. Arpino, C. Gutierrez, H. Weiss, M. Rimawi, S. Massarweh, L. Bharwani, S. DePlacido, C.K. Osborne, R. Schiff R, Treatment of human epidermal growth factor
receptor 2-overexpressing breast cancer xenografts with multiagent HER-targeted therapy, J. Natl. Cancer Inst. 99 (2007) 694–705.
[282] Q.S. Chu, M.E. Cianfrocca, L.J. Goldstein, M. Gale, N. Murray, J. Loftiss, N. Arya, K.M.Koch, L. Pandite, R.A. Fleming, E. Paul, E.K. Rowinsky, A phase I andpharmacokinetic study of lapatinib in combination with letrozole in patientswith advanced cancer, Clin. Cancer Res. 14 (2008) 4484–4490.