Mind wandering away from pain dynamically engages antinociceptive and default mode brain networks
6
Mind wandering away from pain dynamically engages antinociceptive and default mode brain networks Aaron Kucyi a,b , Tim V. Salomons a,c,d , and Karen D. Davis a,b,e,f,1 a Division of Brain, Imaging and Behaviour–Systems Neuroscience, Toronto Western Research Institute, University Health Network, Toronto, ON, Canada M5T 2S8; b Institute of Medical Science, University of Toronto, Toronto, ON, Canada M5S 1A8; c Department of Psychiatry, University of Toronto, Toronto, ON, Canada M5S 1A8; d School of Psychology and Clinical Language Sciences, University of Reading, Reading RG6 6AL, United Kingdom; e Division of Neurosurgery, Toronto Western Hospital, Toronto, ON, Canada M5T 2S8; and f Department of Surgery, University Health Network, Toronto, ON, Canada M5T 2S8 Edited by Marcus E. Raichle, Washington University in St. Louis, St. Louis, MO, and approved October 4, 2013 (received for review July 8, 2013) Human minds often wander away from their immediate sensory environment. It remains unknown whether such mind wandering is unsystematic or whether it lawfully relates to an individual’s tendency to attend to salient stimuli such as pain and their asso- ciated brain structure/function. Studies of pain–cognition interac- tions typically examine explicit manipulation of attention rather than spontaneous mind wandering. Here we sought to better rep- resent natural fluctuations in pain in daily life, so we assessed behavioral and neural aspects of spontaneous disengagement of attention from pain. We found that an individual’s tendency to attend to pain related to the disruptive effect of pain on his or her cognitive task performance. Next, we linked behavioral find- ings to neural networks with strikingly convergent evidence from functional magnetic resonance imaging during pain coupled with thought probes of mind wandering, dynamic resting state activity fluctuations, and diffusion MRI. We found that (i ) pain-induced default mode network (DMN) deactivations were attenuated dur- ing mind wandering away from pain; (ii ) functional connectivity fluctuations between the DMN and periaqueductal gray (PAG) dy- namically tracked spontaneous attention away from pain; and (iii ) across individuals, stronger PAG–DMN structural connectivity and more dynamic resting state PAG–DMN functional connectivity were associated with the tendency to mind wander away from pain. These data demonstrate that individual tendencies to mind wander away from pain, in the absence of explicit manipulation, are subserved by functional and structural connectivity within and between default mode and antinociceptive descending modu- lation networks. pain modulation | salience network | stimulus-independent thought | ventral attention network | experience sampling H umans spend nearly half their time on thoughts unrelated to their present sensory environment (1), a phenomenon referred to as “mind wandering.” These thoughts can persist even when engaged in salient and challenging everyday activities (1, 2), such as driving a car through traffic. In such situations, mind wandering can be deleterious. However, in some situations, mind wandering may be beneficial, such as when an individual needs to cope with pain. Cognitive manipulations, such as alterations of attention/dis- traction (3–5), placebo effects (6–9), changing expectations, and other strategies (10), have shown some efficacy in altering per- ceptions and neural responses elicited by painful stimuli. It is generally assumed that these effects involve enhanced endoge- nous analgesic activity within the descending pain modulatory system [e.g., prefrontal cortex, perigenual cingulate cortex, per- iaqueductal gray (PAG), and rostroventral medulla] and de- creased activity in regions that support the salience of pain [e.g., insula and midcingulate cortex (MCC)] (10). A crucial assumption in previous studies of explicit pain ma- nipulation is that there is a static, invariant neurocognitive state during incoming nociceptive activity. However, the experience of pain can vary significantly, depending on trial-to-trial fluctuations in the prestimulus brain state (11–14). This may be due to intrinsic activity that fluctuates on multiple time scales, a hallmark of brain function related to ongoing cognitive, behavioral, and perceptual dynamics (15, 16). Pain modulation may therefore be considered as an ongoing, intrinsically dynamic process, rather than a binary (on/off) phenomenon triggered by explicit manipulation. The study of mind wandering during pain is thus well suited to examine the dynamic nature of pain modulation. The brain’s default mode network (DMN) has been implicated in mind wandering and self-oriented attention (17–20), but its in- teractions with pain-related brain networks in the disengagement of attention from pain are poorly understood. Furthermore, it remains unknown whether spontaneous disengagement of at- tention from pain and associated network activity is stable within individuals and predictive of behavior. Thus, we developed an experience sampling approach (17, 19, 21) to examine the frequency and cognitive aspects of sponta- neous attentional fluctuations during painful stimulation in 51 healthy volunteers. We established test–retest reproducibility of an individual’s tendency to attend away from pain, which we term “intrinsic attention to pain” (IAP), and tested whether IAP relates to behavioral performance on a cognitive task. Using functional magnetic resonance imaging (fMRI), we tested the hy- pothesis that the interplay between the DMN, salience-/attention- related regions, and the descending pain modulatory system reflects interactions between mind wandering and ongoing pain. We then used diffusion-weighted MRI (DWI) and resting state fMRI to determine whether intrinsic structural/functional connections between key regions that interact during attentional fluctuations away from pain are related to interindividual differences in IAP. Significance The mind easily wanders away from mundane tasks, but pain is presumed to automatically capture attention. We demonstrate that individuals differ in how often their minds spontaneously wander away from pain and that these differences are asso- ciated with the disruptive effect of pain on cognitive perfor- mance. Brain–behavior relationships underscore these individual differences. When people’s minds wander away from pain, there are increased activations of the default mode network (DMN) and strong interactions between the DMN and periaqueductal gray (PAG), an opiate-rich region mediating pain suppression. Individuals with greater tendencies to mind wander from pain have stronger anatomical links and dynamic functional com- munication between PAG and DMN. These findings provide clinically important clues about why some individuals cannot disengage from pain. Author contributions: A.K., T.V.S., and K.D.D. designed research; A.K. performed research; A.K. and T.V.S. analyzed data; and A.K., T.V.S., and K.D.D. wrote the paper. The authors declare no conflict of interest. This article is a PNAS Direct Submission. 1 To whom correspondence should be addressed. E-mail: [email protected]. This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10. 1073/pnas.1312902110/-/DCSupplemental. www.pnas.org/cgi/doi/10.1073/pnas.1312902110 PNAS Early Edition | 1 of 6 NEUROSCIENCE
Transcript of Mind wandering away from pain dynamically engages antinociceptive and default mode brain networks

Mind wandering away from pain dynamically engagesantinociceptive and default mode brain networksAaron Kucyia,b, Tim V. Salomonsa,c,d, and Karen D. Davisa,b,e,f,1
aDivision of Brain, Imaging and Behaviour–Systems Neuroscience, Toronto Western Research Institute, University Health Network, Toronto, ON, Canada M5T2S8; bInstitute of Medical Science, University of Toronto, Toronto, ON, Canada M5S 1A8; cDepartment of Psychiatry, University of Toronto, Toronto, ON,Canada M5S 1A8; dSchool of Psychology and Clinical Language Sciences, University of Reading, Reading RG6 6AL, United Kingdom; eDivision of Neurosurgery,Toronto Western Hospital, Toronto, ON, Canada M5T 2S8; and fDepartment of Surgery, University Health Network, Toronto, ON, Canada M5T 2S8
Edited by Marcus E. Raichle, Washington University in St. Louis, St. Louis, MO, and approved October 4, 2013 (received for review July 8, 2013)
Human minds often wander away from their immediate sensoryenvironment. It remains unknown whether such mind wanderingis unsystematic or whether it lawfully relates to an individual’stendency to attend to salient stimuli such as pain and their asso-ciated brain structure/function. Studies of pain–cognition interac-tions typically examine explicit manipulation of attention ratherthan spontaneous mind wandering. Here we sought to better rep-resent natural fluctuations in pain in daily life, so we assessedbehavioral and neural aspects of spontaneous disengagement ofattention from pain. We found that an individual’s tendency toattend to pain related to the disruptive effect of pain on his orher cognitive task performance. Next, we linked behavioral find-ings to neural networks with strikingly convergent evidence fromfunctional magnetic resonance imaging during pain coupled withthought probes of mind wandering, dynamic resting state activityfluctuations, and diffusion MRI. We found that (i) pain-induceddefault mode network (DMN) deactivations were attenuated dur-ing mind wandering away from pain; (ii) functional connectivityfluctuations between the DMN and periaqueductal gray (PAG) dy-namically tracked spontaneous attention away from pain; and (iii)across individuals, stronger PAG–DMN structural connectivity andmore dynamic resting state PAG–DMN functional connectivitywere associated with the tendency to mind wander away frompain. These data demonstrate that individual tendencies to mindwander away from pain, in the absence of explicit manipulation,are subserved by functional and structural connectivity withinand between default mode and antinociceptive descending modu-lation networks.
pain modulation | salience network | stimulus-independent thought |ventral attention network | experience sampling
Humans spend nearly half their time on thoughts unrelated totheir present sensory environment (1), a phenomenon referred
to as “mind wandering.” These thoughts can persist even whenengaged in salient and challenging everyday activities (1, 2), such asdriving a car through traffic. In such situations, mind wandering canbe deleterious. However, in some situations, mind wandering maybe beneficial, such as when an individual needs to cope with pain.Cognitive manipulations, such as alterations of attention/dis-
traction (3–5), placebo effects (6–9), changing expectations, andother strategies (10), have shown some efficacy in altering per-ceptions and neural responses elicited by painful stimuli. It isgenerally assumed that these effects involve enhanced endoge-nous analgesic activity within the descending pain modulatorysystem [e.g., prefrontal cortex, perigenual cingulate cortex, per-iaqueductal gray (PAG), and rostroventral medulla] and de-creased activity in regions that support the salience of pain [e.g.,insula and midcingulate cortex (MCC)] (10).A crucial assumption in previous studies of explicit pain ma-
nipulation is that there is a static, invariant neurocognitive stateduring incoming nociceptive activity. However, the experience ofpain can vary significantly, depending on trial-to-trial fluctuationsin the prestimulus brain state (11–14). This may be due to intrinsicactivity that fluctuates on multiple time scales, a hallmark of brain
function related to ongoing cognitive, behavioral, and perceptualdynamics (15, 16). Pain modulation may therefore be consideredas an ongoing, intrinsically dynamic process, rather than a binary(on/off) phenomenon triggered by explicit manipulation. Thestudy of mind wandering during pain is thus well suited toexamine the dynamic nature of pain modulation. The brain’sdefault mode network (DMN) has been implicated in mindwandering and self-oriented attention (17–20), but its in-teractions with pain-related brain networks in the disengagementof attention from pain are poorly understood. Furthermore, itremains unknown whether spontaneous disengagement of at-tention from pain and associated network activity is stable withinindividuals and predictive of behavior.Thus, we developed an experience sampling approach (17, 19,
21) to examine the frequency and cognitive aspects of sponta-neous attentional fluctuations during painful stimulation in 51healthy volunteers. We established test–retest reproducibility ofan individual’s tendency to attend away from pain, which weterm “intrinsic attention to pain” (IAP), and tested whether IAPrelates to behavioral performance on a cognitive task. Usingfunctional magnetic resonance imaging (fMRI), we tested the hy-pothesis that the interplay between the DMN, salience-/attention-related regions, and the descending painmodulatory system reflectsinteractions between mind wandering and ongoing pain. We thenused diffusion-weighted MRI (DWI) and resting state fMRI todetermine whether intrinsic structural/functional connectionsbetween key regions that interact during attentional fluctuationsaway from pain are related to interindividual differences in IAP.
Significance
The mind easily wanders away frommundane tasks, but pain ispresumed to automatically capture attention. We demonstratethat individuals differ in how often their minds spontaneouslywander away from pain and that these differences are asso-ciated with the disruptive effect of pain on cognitive perfor-mance. Brain–behavior relationships underscore these individualdifferences. When people’s minds wander away from pain, thereare increased activations of the default mode network (DMN)and strong interactions between the DMN and periaqueductalgray (PAG), an opiate-rich region mediating pain suppression.Individuals with greater tendencies to mind wander from painhave stronger anatomical links and dynamic functional com-munication between PAG and DMN. These findings provideclinically important clues about why some individuals cannotdisengage from pain.
Author contributions: A.K., T.V.S., and K.D.D. designed research; A.K. performed research;A.K. and T.V.S. analyzed data; and A.K., T.V.S., and K.D.D. wrote the paper.
The authors declare no conflict of interest.
This article is a PNAS Direct Submission.1To whom correspondence should be addressed. E-mail: [email protected].
This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.1073/pnas.1312902110/-/DCSupplemental.
www.pnas.org/cgi/doi/10.1073/pnas.1312902110 PNAS Early Edition | 1 of 6
NEU
ROSC
IENCE

ResultsUnique Protocol to Evaluate Mind Wandering Away from Pain. Sub-ject testing was carried out in two sessions. In session 1, subjectscompleted experience sampling and cognitive interference tasksincluding epochs of painful transcutaneous electrical nerve stim-ulation (TENS) of the left median nerve (Methods). In session 2,subjects completed experience sampling during fMRI, DWI, andresting state fMRI scans.For the experience sampling task, the TENS level was main-
tained to consistently elicit pain intensity rated as 4–5 out of 10.Participants were instructed to avoid actively attending eithertoward or away from pain (SI Methods). On each trial, partic-ipants viewed a fixation cross while receiving painful TENSwhich was interrupted after 20 s with a thought probe in whichsubjects indicated whether their attention had just been “only onpain,” “mostly on pain,” “mostly on something else,” or “only onsomething else” (Fig. 1A). An IAP score was calculated for eachsubject based on the proportions of trials in the task with reportsof attention to pain vs. attention to something else and couldrange from +2 (always attending to pain) to −2 (always attendingto something else) (Methods). At the end of trials, participantswere asked to rate the degree to which their reports of “somethingelse” belonged to the categories of external sensory distractions(EDs) (e.g., auditory/visual events), task-related interferences(TRIs) (e.g., considering response to upcoming probe), or mindwandering (MW) (i.e., thoughts completely unrelated to presentenvironment) (19).The cognitive interference task was one we used previously
(22) to characterize the degree to which individuals prioritizecognitive task performance versus pain (Fig. 2A). The differencebetween mean reaction time (RT) across pain vs. no-pain trialswas used to quantify the effect of pain on performance as donepreviously (22). Subjects were classified as P type if their RTswere slower during concomitant pain compared with “no pain”trials (i.e., pain dominates) or A type if they had faster RTsduring concomitant pain (i.e., attention dominates).
Behavioral Results. The IAP scores for sessions 1 and 2 rangedfrom, respectively, −1.1 to +1.9 (mean ± SD = 0.17 ± 0.67) and−1.3 to +1.6 (mean ± SD = 0.01 ± 6.8). Individual subjectsshowed marked fluctuations in their attention to pain from trialto trial (e.g., Fig. 1A) but did so with remarkably consistentfrequency between the two sessions (see below). The group dataindicate an almost equal split of trials in which subjects were ex-periencing “only or mostly pain” vs. trials in which the experience
was “only or mostly something else” (Fig. 1B): trials were rated as“only pain” (session 1: 13.8%; session 2: 11.0%), “mostly pain”(session 1: 41.4%; session 2: 39.3%), “mostly something else”(session 1: 38.1%; session 2: 39.4%), or “only something else”(session 1: 6.7%; session 2: 10.3%) (Fig. 1B). There was astrong, significant intraclass correlation (ICC) between IAP scoresduring session 1 vs. session 2 (ICC = 0.83; P = 4.7 × 10−10) (Fig.1D), suggesting that IAP is a trait-like quality.Participants reported that they were confident in their abilities
to accurately indicate attentional state during the task (averageconfidence rating ± SD out of 7 = 5.7 ± 0.82; 1 indicates notconfident at all, and 7 indicates very confident). Participantsrated the degree to which their reports of Something Elsebelonged to the categories of EDs, TRIs, and MW (Likert scale: 1indicates never, 7 indicates always) as follows: EDs (session 1:2.6 ± 1.63; session 2: 3.8 ± 1.61), TRIs (session 1: 3.9 ± 1.60;session 2: 3.5 ± 1.15), and MW (session 1: 4.8 ± 1.58; session 2:4.1 ± 1.52) (Fig. 1C).Correlations between session 1 and session 2 of the frequen-
cies of categories that prompted Something Else reports alsorevealed significant positive correspondence (EDs: Spearman’sρ = 0.44, P = 0.002; TRIs: ρ = 0.39, P = 0.005; MW: ρ = 0.61, P =2 × 10−6) (Table S1). This suggests that the sensory/cognitivecontents of attentional fluctuations away from pain were alsostable within individuals. The correspondences between ratingcategories were as follows: EDs vs. TRIs (session 1: ρ = 0.28, P =0.051; session 2: ρ = 0.33, P = 0.018), EDs vs. MW (session 1: ρ =−0.29, P = 0.037; session 2: ρ = −0.41, P = 0.003), and TRIs vs.MW (session 1: ρ = −0.65, P = 2.7 × 10−7; session 2: ρ = −0.22,P = 0.13). Therefore, participants who were high in MW gen-erally tended to be low in TRIs and EDs.We next tested whether individual factors impact IAP and
found a modest trend toward a positive correlation between IAPand pain catastrophizing scale (PCS) scores (r = 0.30; P = 0.03;not significant after Bonferroni correction) (Fig. 1E). There wasno correlation between IAP and daydreaming frequency scale(DDF) scores (r = −0.085; P = 0.55), indicating that the tendencyto attend away from pain is unrelated to the tendency to day-dream in general.Finally, we tested our hypothesis that individuals who fre-
quently reported that they attended to pain during experiencesampling would be more likely to show P-type behavior (i.e.,slower RTs during pain), whereas those who frequently attendedaway from pain would be more likely to show A-type behavior(i.e., faster RTs during pain). We found a significant positivecorrelation (r = 0.42, P = 0.003) between mean RT across pain
Fig. 1. Experience sampling during painful stimu-lation reveals frequency and sensory/cognitiveaspects of attentional fluctuations away from pain.(A) Task trial design (Upper) and example of fluc-tuations in attentional state during the psycho-physics session (Lower). (B) Distribution of theincidence of trials in session 1 (n = 51) (Upper) andsession 2 (n = 50) (Lower) in which subjects experi-enced pain and/or something else. (C) Group aver-ages (±SD) for ratings of something else being MW,TRIs, and EDs for session 1 and session 2. (D) Con-sistency of responses between session 1 and session2 in IAP scores (ICC = 0.83; P = 4.7 × 10−10). (E) IAPscores from session 1 positively correlated with paincatastrophizing scale scores (r = 0.30; P = 0.03). ISI,interstimulus interval.
2 of 6 | www.pnas.org/cgi/doi/10.1073/pnas.1312902110 Kucyi et al.

vs. no-pain trials and IAP that supported this hypothesis andprovides behavioral validation for the experience sampling task(Fig. 2B). There was no correlation between mean RT acrosspain vs. no-pain trials and PCS (r = 0.086; P = 0.55).
Neural Correlates of Ongoing Fluctuations in Attention to Pain. Wenext analyzed trial-to-trial brain activity fluctuations occurringduring experience sampling with fMRI. When subjects reportedattention to pain, activations occurred in regions previouslyreported as being pain- and salience-related [e.g., insula, MCC,thalamus, contralateral primary somatosensory cortex and sec-ondary somatosensory cortex, and temporoparietal junction(TPJ)] (23–25), and deactivations occurred in nodes of the DMN[medial prefrontal cortex (mPFC), posterior cingulate cortex(PCC)/precuneus, and temporooccicipital junction (TOJ)] (Fig.S1; full list in Table S2). In contrast, there were no significantdeactivations in Something Else trials wherein subjects reportedthat their thoughts/feelings were on something other than pain.However, the regions activated in “Pain” trials were also acti-vated in “Something Else” trials (Fig. S1; full list in Table S3).Crucially, Pain compared with Something Else trials were asso-ciated with greater activation of a predominantly right-lateral-ized network (e.g., right TPJ/S2, right IFG, right dorsolateralprefrontal cortex, and bilateral insula), including regions that areconsistent with previous definitions of the “ventral attention”and “salience” networks (26–28) (Fig. 3A; full list in Table S4).Something Else compared with Pain trials were associated withgreater activation of the DMN (e.g., mPFC, PCC/precuneus,lateral parietal areas, and medial temporal lobe) and regionsimplicated in executive control (superior parietal lobule, supe-rior/middle frontal gyrus, and supplementary motor area) (Fig.3B; full list in Table S5).Given the purported role of the DMN in MW and our ob-
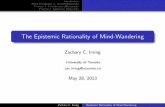
served anticorrelations of MW with EDs and TRIs, we nexttested how individual differences in the change of activationwithin the DMN core (mPFC and PCC/precuneus) (18) betweenSomething Else compared with Pain trials [Δ DMN activation(Else > Pain)] related to MW or other distractions from pain.For EDs, TRIs, and MW, respectively, there was a significantnegative correlation (ρ = −0.61, P = 0.0002), no significantcorrelation (ρ = −0.24, P = 0.19), and a significant positivecorrelation (ρ = 0.45, p = 0.011) with Δ DMN activation (Else >Pain) (Fig. 4). Therefore, individuals distracted because of EDswere unlikely to engage the DMN, whereas high-MW individualswere likely to engage the DMN when their attention fluctuatedaway from pain.
Functional Coupling Between PAG and DMN.We next tested whetheractivity in the descending pain modulatory system interacts withattention networks, potentially to suppress ascending nociceptiveinput during attentional fluctuations away from pain. To do this,
we used psychophysiological interaction analysis (PPI) (29) todetermine whether functional connectivity of the descending painmodulatory system related to attention toward vs. away frompain. We focused on the PAG because it has a high concentrationof opiate-containing neurons with descending projections (30) andhas functional interactions with the cingulate/prefrontal corteximplicated in cognitive modulation of pain (5, 7).During Something Else compared with Pain trials, we found
enhanced functional coupling of the PAG with DMN regions(mPFC, PCC/precuneus/retrosplenial cortex, and medial tem-poral lobe) and left middle frontal gyrus (Fig. 5A; full list inTable S6). No regions had significantly greater PAG functionalconnectivity for periods associated with attention to vs. awayfrom pain. However, PPI analysis for a PCC seed revealed sev-eral regions (angular gyrus, inferior/middle temporal gyrus, lin-gual gyrus, and cerebellar regions) with greater functionalconnectivity for attention toward compared with away from pain(Fig. S2).
Structural Connectivity Between PAG and mPFC. White matter con-nections have been identified between the mPFC and PAG inhumans (31, 32). Thus, our finding of increased PAG–DMNfunctional coupling within individuals during attentional fluctu-ations away from pain raises the possibility that individuals withstronger PAG–DMN anatomical connections more easily dis-engage attention from pain. We therefore tested the hypothesisthat there is stronger structural connectivity in the mPFC–PAGpathway in individuals who tend to attend away from pain than inindividuals who have greater IAP.To evaluate structural connectivity, we first used probabilistic
tractography (33) to define the pathway between the PAG andthe mPFC region that was identified in our PPI analysis (Fig. 5).We then applied tract-based spatial statistics (34) to calculatemean fractional anisotropy (FA) in the mPFC–PAG white matter“skeleton” pathway. We found a significant negative correlationbetween mPFC–PAG tract FA and IAP score (r = −0.36, P =0.009), supporting the hypothesis that individuals who fre-quently attend away from pain have stronger descending structural
Fig. 2. Tendency to attend to pain relates to the disruptive effect of pain oncognitive task performance. (A) The task required subjects to choose the boxwith the greatest number of digits (highest count). Green-outlined boxesshow the correct response in this example. Subjects performed the task withpain (P) and without pain (NP). Subjects with mean reaction time (RT) for Pfaster than for NP trials were classified as A type (attention dominates).Subjects with slower RTs for P compared with NP trials were P-type (paindominates) (3, 22). (B) Positive correlation between ΔRT [P − NP] in thecognitive interference task and IAP from experience sampling (n = 48) (r =0.42; P = 0.003). Quadrants show classification of subjects of A/P type andlow/high IAP.
Fig. 3. Salience network and DMN activations relate to fluctuations in at-tention to pain (n = 32). (A) Regions with greater activation during periodspreceding reports of attention to pain compared with attention to some-thing else. Bar graphs show mean % signal change (±SD), extracted from 3-mm-radius spheres at peak coordinates. (B) Regions with greater activationduring periods preceding reports of attention to something else comparedwith attention to pain. Bar graphs show mean % signal change (±SD),extracted from 3-mm-radius spheres at peak coordinates. Statistical imagesare thresholded at FWE-corrected Z > 2.3; cluster P < 0.05.
Kucyi et al. PNAS Early Edition | 3 of 6
NEU
ROSC
IENCE
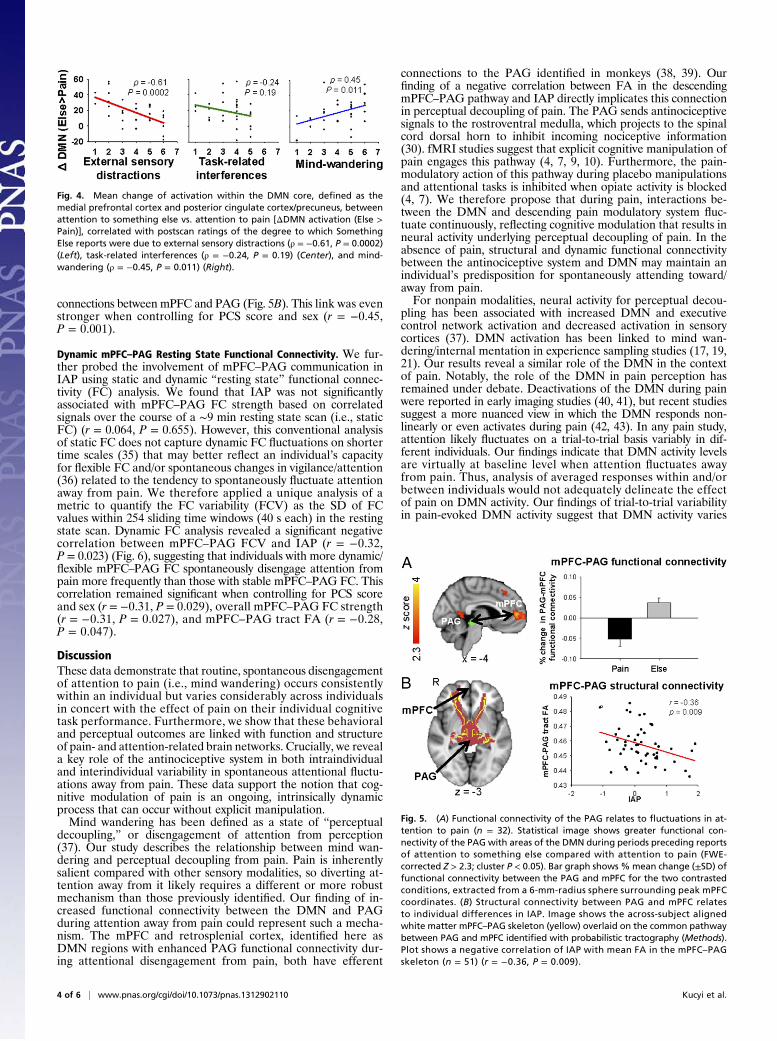
connections between mPFC and PAG (Fig. 5B). This link was evenstronger when controlling for PCS score and sex (r = −0.45,P = 0.001).
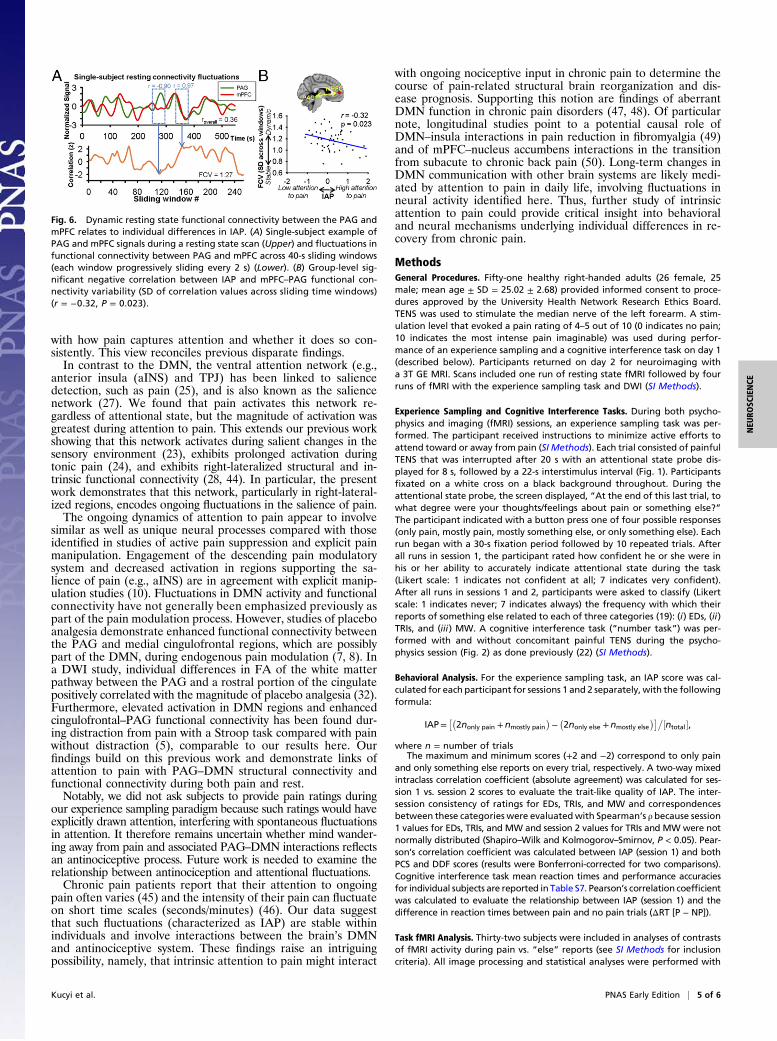
Dynamic mPFC–PAG Resting State Functional Connectivity. We fur-ther probed the involvement of mPFC–PAG communication inIAP using static and dynamic “resting state” functional connec-tivity (FC) analysis. We found that IAP was not significantlyassociated with mPFC–PAG FC strength based on correlatedsignals over the course of a ∼9 min resting state scan (i.e., staticFC) (r = 0.064, P = 0.655). However, this conventional analysisof static FC does not capture dynamic FC fluctuations on shortertime scales (35) that may better reflect an individual’s capacityfor flexible FC and/or spontaneous changes in vigilance/attention(36) related to the tendency to spontaneously fluctuate attentionaway from pain. We therefore applied a unique analysis of ametric to quantify the FC variability (FCV) as the SD of FCvalues within 254 sliding time windows (40 s each) in the restingstate scan. Dynamic FC analysis revealed a significant negativecorrelation between mPFC–PAG FCV and IAP (r = −0.32,P = 0.023) (Fig. 6), suggesting that individuals with more dynamic/flexible mPFC–PAG FC spontaneously disengage attention frompain more frequently than those with stable mPFC–PAG FC. Thiscorrelation remained significant when controlling for PCS scoreand sex (r = −0.31, P = 0.029), overall mPFC–PAG FC strength(r = −0.31, P = 0.027), and mPFC–PAG tract FA (r = −0.28,P = 0.047).
DiscussionThese data demonstrate that routine, spontaneous disengagementof attention to pain (i.e., mind wandering) occurs consistentlywithin an individual but varies considerably across individualsin concert with the effect of pain on their individual cognitivetask performance. Furthermore, we show that these behavioraland perceptual outcomes are linked with function and structureof pain- and attention-related brain networks. Crucially, we reveala key role of the antinociceptive system in both intraindividualand interindividual variability in spontaneous attentional fluctu-ations away from pain. These data support the notion that cog-nitive modulation of pain is an ongoing, intrinsically dynamicprocess that can occur without explicit manipulation.Mind wandering has been defined as a state of “perceptual
decoupling,” or disengagement of attention from perception(37). Our study describes the relationship between mind wan-dering and perceptual decoupling from pain. Pain is inherentlysalient compared with other sensory modalities, so diverting at-tention away from it likely requires a different or more robustmechanism than those previously identified. Our finding of in-creased functional connectivity between the DMN and PAGduring attention away from pain could represent such a mecha-nism. The mPFC and retrosplenial cortex, identified here asDMN regions with enhanced PAG functional connectivity dur-ing attentional disengagement from pain, both have efferent
connections to the PAG identified in monkeys (38, 39). Ourfinding of a negative correlation between FA in the descendingmPFC–PAG pathway and IAP directly implicates this connectionin perceptual decoupling of pain. The PAG sends antinociceptivesignals to the rostroventral medulla, which projects to the spinalcord dorsal horn to inhibit incoming nociceptive information(30). fMRI studies suggest that explicit cognitive manipulation ofpain engages this pathway (4, 7, 9, 10). Furthermore, the pain-modulatory action of this pathway during placebo manipulationsand attentional tasks is inhibited when opiate activity is blocked(4, 7). We therefore propose that during pain, interactions be-tween the DMN and descending pain modulatory system fluc-tuate continuously, reflecting cognitive modulation that results inneural activity underlying perceptual decoupling of pain. In theabsence of pain, structural and dynamic functional connectivitybetween the antinociceptive system and DMN may maintain anindividual’s predisposition for spontaneously attending toward/away from pain.For nonpain modalities, neural activity for perceptual decou-
pling has been associated with increased DMN and executivecontrol network activation and decreased activation in sensorycortices (37). DMN activation has been linked to mind wan-dering/internal mentation in experience sampling studies (17, 19,21). Our results reveal a similar role of the DMN in the contextof pain. Notably, the role of the DMN in pain perception hasremained under debate. Deactivations of the DMN during painwere reported in early imaging studies (40, 41), but recent studiessuggest a more nuanced view in which the DMN responds non-linearly or even activates during pain (42, 43). In any pain study,attention likely fluctuates on a trial-to-trial basis variably in dif-ferent individuals. Our findings indicate that DMN activity levelsare virtually at baseline level when attention fluctuates awayfrom pain. Thus, analysis of averaged responses within and/orbetween individuals would not adequately delineate the effectof pain on DMN activity. Our findings of trial-to-trial variabilityin pain-evoked DMN activity suggest that DMN activity varies
Fig. 4. Mean change of activation within the DMN core, defined as themedial prefrontal cortex and posterior cingulate cortex/precuneus, betweenattention to something else vs. attention to pain [ΔDMN activation (Else >Pain)], correlated with postscan ratings of the degree to which SomethingElse reports were due to external sensory distractions (ρ = −0.61, P = 0.0002)(Left), task-related interferences (ρ = −0.24, P = 0.19) (Center), and mind-wandering (ρ = −0.45, P = 0.011) (Right).
Fig. 5. (A) Functional connectivity of the PAG relates to fluctuations in at-tention to pain (n = 32). Statistical image shows greater functional con-nectivity of the PAG with areas of the DMN during periods preceding reportsof attention to something else compared with attention to pain (FWE-corrected Z > 2.3; cluster P < 0.05). Bar graph shows %mean change (±SD) offunctional connectivity between the PAG and mPFC for the two contrastedconditions, extracted from a 6-mm-radius sphere surrounding peak mPFCcoordinates. (B) Structural connectivity between PAG and mPFC relatesto individual differences in IAP. Image shows the across-subject alignedwhite matter mPFC–PAG skeleton (yellow) overlaid on the common pathwaybetween PAG and mPFC identified with probabilistic tractography (Methods).Plot shows a negative correlation of IAP with mean FA in the mPFC–PAGskeleton (n = 51) (r = −0.36, P = 0.009).
4 of 6 | www.pnas.org/cgi/doi/10.1073/pnas.1312902110 Kucyi et al.
with how pain captures attention and whether it does so con-sistently. This view reconciles previous disparate findings.In contrast to the DMN, the ventral attention network (e.g.,
anterior insula (aINS) and TPJ) has been linked to saliencedetection, such as pain (25), and is also known as the saliencenetwork (27). We found that pain activates this network re-gardless of attentional state, but the magnitude of activation wasgreatest during attention to pain. This extends our previous workshowing that this network activates during salient changes in thesensory environment (23), exhibits prolonged activation duringtonic pain (24), and exhibits right-lateralized structural and in-trinsic functional connectivity (28, 44). In particular, the presentwork demonstrates that this network, particularly in right-lateral-ized regions, encodes ongoing fluctuations in the salience of pain.The ongoing dynamics of attention to pain appear to involve
similar as well as unique neural processes compared with thoseidentified in studies of active pain suppression and explicit painmanipulation. Engagement of the descending pain modulatorysystem and decreased activation in regions supporting the sa-lience of pain (e.g., aINS) are in agreement with explicit manip-ulation studies (10). Fluctuations in DMN activity and functionalconnectivity have not generally been emphasized previously aspart of the pain modulation process. However, studies of placeboanalgesia demonstrate enhanced functional connectivity betweenthe PAG and medial cingulofrontal regions, which are possiblypart of the DMN, during endogenous pain modulation (7, 8). Ina DWI study, individual differences in FA of the white matterpathway between the PAG and a rostral portion of the cingulatepositively correlated with the magnitude of placebo analgesia (32).Furthermore, elevated activation in DMN regions and enhancedcingulofrontal–PAG functional connectivity has been found dur-ing distraction from pain with a Stroop task compared with painwithout distraction (5), comparable to our results here. Ourfindings build on this previous work and demonstrate links ofattention to pain with PAG–DMN structural connectivity andfunctional connectivity during both pain and rest.Notably, we did not ask subjects to provide pain ratings during
our experience sampling paradigm because such ratings would haveexplicitly drawn attention, interfering with spontaneous fluctuationsin attention. It therefore remains uncertain whether mind wander-ing away from pain and associated PAG–DMN interactions reflectsan antinociceptive process. Future work is needed to examine therelationship between antinociception and attentional fluctuations.Chronic pain patients report that their attention to ongoing
pain often varies (45) and the intensity of their pain can fluctuateon short time scales (seconds/minutes) (46). Our data suggestthat such fluctuations (characterized as IAP) are stable withinindividuals and involve interactions between the brain’s DMNand antinociceptive system. These findings raise an intriguingpossibility, namely, that intrinsic attention to pain might interact
with ongoing nociceptive input in chronic pain to determine thecourse of pain-related structural brain reorganization and dis-ease prognosis. Supporting this notion are findings of aberrantDMN function in chronic pain disorders (47, 48). Of particularnote, longitudinal studies point to a potential causal role ofDMN–insula interactions in pain reduction in fibromyalgia (49)and of mPFC–nucleus accumbens interactions in the transitionfrom subacute to chronic back pain (50). Long-term changes inDMN communication with other brain systems are likely medi-ated by attention to pain in daily life, involving fluctuations inneural activity identified here. Thus, further study of intrinsicattention to pain could provide critical insight into behavioraland neural mechanisms underlying individual differences in re-covery from chronic pain.
MethodsGeneral Procedures. Fifty-one healthy right-handed adults (26 female, 25male; mean age ± SD = 25.02 ± 2.68) provided informed consent to proce-dures approved by the University Health Network Research Ethics Board.TENS was used to stimulate the median nerve of the left forearm. A stim-ulation level that evoked a pain rating of 4–5 out of 10 (0 indicates no pain;10 indicates the most intense pain imaginable) was used during perfor-mance of an experience sampling and a cognitive interference task on day 1(described below). Participants returned on day 2 for neuroimaging witha 3T GE MRI. Scans included one run of resting state fMRI followed by fourruns of fMRI with the experience sampling task and DWI (SI Methods).
Experience Sampling and Cognitive Interference Tasks. During both psycho-physics and imaging (fMRI) sessions, an experience sampling task was per-formed. The participant received instructions to minimize active efforts toattend toward or away from pain (SI Methods). Each trial consisted of painfulTENS that was interrupted after 20 s with an attentional state probe dis-played for 8 s, followed by a 22-s interstimulus interval (Fig. 1). Participantsfixated on a white cross on a black background throughout. During theattentional state probe, the screen displayed, “At the end of this last trial, towhat degree were your thoughts/feelings about pain or something else?”The participant indicated with a button press one of four possible responses(only pain, mostly pain, mostly something else, or only something else). Eachrun began with a 30-s fixation period followed by 10 repeated trials. Afterall runs in session 1, the participant rated how confident he or she were inhis or her ability to accurately indicate attentional state during the task(Likert scale: 1 indicates not confident at all; 7 indicates very confident).After all runs in sessions 1 and 2, participants were asked to classify (Likertscale: 1 indicates never; 7 indicates always) the frequency with which theirreports of something else related to each of three categories (19): (i) EDs, (ii)TRIs, and (iii) MW. A cognitive interference task (“number task”) was per-formed with and without concomitant painful TENS during the psycho-physics session (Fig. 2) as done previously (22) (SI Methods).
Behavioral Analysis. For the experience sampling task, an IAP score was cal-culated for each participant for sessions 1 and 2 separately, with the followingformula:
IAP=��2nonly pain +nmostly pain
�−�2nonly else +nmostly else
���½ntotal�,
where n = number of trialsThe maximum and minimum scores (+2 and −2) correspond to only pain
and only something else reports on every trial, respectively. A two-way mixedintraclass correlation coefficient (absolute agreement) was calculated for ses-sion 1 vs. session 2 scores to evaluate the trait-like quality of IAP. The inter-session consistency of ratings for EDs, TRIs, and MW and correspondencesbetween these categories were evaluatedwith Spearman’s ρ because session1 values for EDs, TRIs, and MW and session 2 values for TRIs and MWwere notnormally distributed (Shapiro–Wilk and Kolmogorov–Smirnov, P < 0.05). Pear-son’s correlation coefficient was calculated between IAP (session 1) and bothPCS and DDF scores (results were Bonferroni-corrected for two comparisons).Cognitive interference task mean reaction times and performance accuraciesfor individual subjects are reported in Table S7. Pearson’s correlation coefficientwas calculated to evaluate the relationship between IAP (session 1) and thedifference in reaction times between pain and no pain trials (ΔRT [P − NP]).
Task fMRI Analysis. Thirty-two subjects were included in analyses of contrastsof fMRI activity during pain vs. “else” reports (see SI Methods for inclusioncriteria). All image processing and statistical analyses were performed with
Fig. 6. Dynamic resting state functional connectivity between the PAG andmPFC relates to individual differences in IAP. (A) Single-subject example ofPAG and mPFC signals during a resting state scan (Upper) and fluctuations infunctional connectivity between PAG and mPFC across 40-s sliding windows(each window progressively sliding every 2 s) (Lower). (B) Group-level sig-nificant negative correlation between IAP and mPFC–PAG functional con-nectivity variability (SD of correlation values across sliding time windows)(r = −0.32, P = 0.023).
Kucyi et al. PNAS Early Edition | 5 of 6
NEU
ROSC
IENCE

FMRIB Software Library (FSL) v5.0, MATLAB v7.12.0, fMRISTAT (51), andstatistical package for the social sciences (SPSS) v21.0 (IBM Corp.). Contrastswere performed to identify activation/deactivation during stimulation be-fore pain and else reports as well as pain > else and else > pain differences(SI Methods). Group-level analysis was performed with FMRIB’s local analysisof mixed effects (FLAME) 1 + 2 (whole-brain family-wise error (FWE)-cor-rected Z > 2.3; cluster P < 0.05).
We performed a PPI analysis (29) with a seed region defined in the PAG aswas done previously (7) (SI Methods). Contrasts were performed betweentwo interaction regressors (PAG time course × stimulation before painreports and PAG time course × stimulation before else reports) to identifyregions with pain > else and else > pain PAG functional connectivity (FLAME1 + 2 thresholding: whole-brain FWE-corrected Z > 2.3; cluster P < 0.05).
Diffusion MRI Analysis. Probabilistic tractrography was used to define themPFC–PAG pathway for analysis with tract-based spatial statistics (TBSS) inall 51 participants (SI Methods). A white matter skeleton obtained from TBSSwas masked with the PAG–mPFC pathway derived from probabilistic trac-tography. Pearson’s correlation coefficient was then calculated betweenmean PAG–mPFC pathway FA values and IAP (session 1) scores.
Resting State fMRI Analysis. Mean time series across voxels were calculatedfrom preprocessed data (SI Methods) within PAG and within mPFC. OverallFC strength was calculated as the Fisher-transformed correlation betweenPAG and mPFC mean time series. For dynamic FC analysis, both time serieswere split into 40-s sliding time windows, with each window shifted 2 sforward from the previous window (i.e., 1 volume [i.e., 1 TR (repetitiontime)]). Fisher-transformed correlations between PAG and mPFC within eachof the 254 obtained windows were then computed, and FCV was calculatedas the SD of these correlation values. Pearson’s correlation coefficient wasthen calculated for PAG–mPFC FC and FCV vs. IAP (session 1) scores (datawere normally distributed). To test the effect of sliding window duration onthe correlation between FCV and IAP, we redid the FCV analysis using 30-,50-, and 60-s windows and demonstrated converging results (Table S8).
ACKNOWLEDGMENTS. We thank Adrian Crawley, Geoff Pope, NathalieErpelding, Gang Wang, Eugen Hlasny, and Keith Ta for technical assistance.We also thank Adrian Crawley, Eve De Rosa, Lucia Gagliese, MojganHodaie, and Mary Pat McAndrews for critical review of the study design.This work was performed at Toronto Western Research Institute, UniversityHealth Network and funded by the Canadian Institutes of Health Research.
1. Killingsworth MA, Gilbert DT (2010) A wandering mind is an unhappy mind. Science330(6006):932.
2. Kane MJ, et al. (2007) For whom the mind wanders, and when: An experience-sam-pling study of working memory and executive control in daily life. Psychol Sci 18(7):614–621.
3. Seminowicz DA, Mikulis DJ, Davis KD (2004) Cognitive modulation of pain-relatedbrain responses depends on behavioral strategy. Pain 112(1–2):48–58.
4. Sprenger C, et al. (2012) Attention modulates spinal cord responses to pain. Curr Biol22(11):1019–1022.
5. Valet M, et al. (2004) Distraction modulates connectivity of the cingulo-frontal cortexand the midbrain during pain—An fMRI analysis. Pain 109(3):399–408.
6. Wager TD, et al. (2004) Placebo-induced changes in FMRI in the anticipation andexperience of pain. Science 303(5661):1162–1167.
7. Eippert F, et al. (2009) Activation of the opioidergic descending pain control systemunderlies placebo analgesia. Neuron 63(4):533–543.
8. Wager TD, Scott DJ, Zubieta JK (2007) Placebo effects on human mu-opioid activityduring pain. Proc Natl Acad Sci USA 104(26):11056–11061.
9. Eippert F, Finsterbusch J, Bingel U, Büchel C (2009) Direct evidence for spinal cordinvolvement in placebo analgesia. Science 326(5951):404.
10. Wiech K, Ploner M, Tracey I (2008) Neurocognitive aspects of pain perception. TrendsCogn Sci 12(8):306–313.
11. Boly M, et al. (2007) Baseline brain activity fluctuations predict somatosensory per-ception in humans. Proc Natl Acad Sci USA 104(29):12187–12192.
12. Ohara S, Crone NE, Weiss N, Kim JH, Lenz FA (2008) Analysis of synchrony demon-strates that the presence of “pain networks” prior to a noxious stimulus can enablethe perception of pain in response to that stimulus. Exp Brain Res 185(2):353–358.
13. Ploner M, Lee MC, Wiech K, Bingel U, Tracey I (2010) Prestimulus functional connectivitydetermines pain perception in humans. Proc Natl Acad Sci USA 107(1):355–360.
14. Mayhew SD, Hylands-White N, Porcaro C, Derbyshire SW, Bagshaw AP (2013) Intrinsicvariability in the human response to pain is assembled from multiple, dynamic brainprocesses. Neuroimage 75:68–78.
15. Deco G, Jirsa VK, McIntosh AR (2011) Emerging concepts for the dynamical organi-zation of resting-state activity in the brain. Nat Rev Neurosci 12(1):43–56.
16. Palva JM, Palva S (2011) Roles of multiscale brain activity fluctuations in shaping thevariability and dynamics of psychophysical performance. Prog Brain Res 193:335–350.
17. Christoff K, Gordon AM, Smallwood J, Smith R, Schooler JW (2009) Experience sam-pling during fMRI reveals default network and executive system contributions tomind wandering. Proc Natl Acad Sci USA 106(21):8719–8724.
18. Andrews-Hanna JR, Reidler JS, Sepulcre J, Poulin R, Buckner RL (2010) Functional-anatomic fractionation of the brain’s default network. Neuron 65(4):550–562.
19. Stawarczyk D, Majerus S, Maquet P, D’Argembeau A (2011) Neural correlates ofongoing conscious experience: Both task-unrelatedness and stimulus-independenceare related to default network activity. PLoS ONE 6(2):e16997.
20. Mason MF, et al. (2007) Wandering minds: The default network and stimulus-independent thought. Science 315(5810):393–395.
21. Vanhaudenhuyse A, et al. (2011) Two distinct neuronal networks mediate theawareness of environment and of self. J Cogn Neurosci 23(3):570–578.
22. Erpelding N, Davis KD (2013) Neural underpinnings of behavioural strategies thatprioritize either cognitive task performance or pain. Pain 154(10):2060–2071.
23. Downar J, Crawley AP, Mikulis DJ, Davis KD (2000) A multimodal cortical network forthe detection of changes in the sensory environment. Nat Neurosci 3(3):277–283.
24. Downar J, Mikulis DJ, Davis KD (2003) Neural correlates of the prolonged salience ofpainful stimulation. Neuroimage 20(3):1540–1551.
25. Mouraux A, Diukova A, Lee MC, Wise RG, Iannetti GD (2011) A multisensory in-vestigation of the functional significance of the “pain matrix” Neuroimage 54(3):2237–2249.
26. Corbetta M, Patel G, Shulman GL (2008) The reorienting system of the human brain:From environment to theory of mind. Neuron 58(3):306–324.
27. Seeley WW, et al. (2007) Dissociable intrinsic connectivity networks for salience pro-cessing and executive control. J Neurosci 27(9):2349–2356.
28. Kucyi A, Hodaie M, Davis KD (2012) Lateralization in intrinsic functional connectivityof the temporoparietal junction with salience- and attention-related brain networks.J Neurophysiol 108(12):3382–3392.
29. Friston KJ, et al. (1997) Psychophysiological and modulatory interactions in neuro-imaging. Neuroimage 6(3):218–229.
30. Millan MJ (2002) Descending control of pain. Prog Neurobiol 66(6):355–474.31. Hadjipavlou G, Dunckley P, Behrens TE, Tracey I (2006) Determining anatomical
connectivities between cortical and brainstem pain processing regions in humans: Adiffusion tensor imaging study in healthy controls. Pain 123(1–2):169–178.
32. Stein N, Sprenger C, Scholz J, Wiech K, Bingel U (2012) White matter integrity of thedescending pain modulatory system is associated with interindividual differences inplacebo analgesia. Pain 153(11):2210–2217.
33. Behrens TE, Berg HJ, Jbabdi S, Rushworth MF, Woolrich MW (2007) Probabilisticdiffusion tractography with multiple fibre orientations: What can we gain? Neuro-image 34(1):144–155.
34. Smith SM, et al. (2006) Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. Neuroimage 31(4):1487–1505.
35. Chang C, Glover GH (2010) Time-frequency dynamics of resting-state brain connec-tivity measured with fMRI. Neuroimage 50(1):81–98.
36. Hutchison RM, et al. (2013) Dynamic functional connectivity: Promise, issues, and in-terpretations. Neuroimage 80:360–378.
37. Schooler JW, et al. (2011) Meta-awareness, perceptual decoupling and the wanderingmind. Trends Cogn Sci 15(7):319–326.
38. An X, Bandler R, Ongür D, Price JL (1998) Prefrontal cortical projections to longitu-dinal columns in the midbrain periaqueductal gray in macaque monkeys. J CompNeurol 401(4):455–479.
39. Parvizi J, Van Hoesen GW, Buckwalter J, Damasio A (2006) Neural connections of theposteromedial cortex in the macaque. Proc Natl Acad Sci USA 103(5):1563–1568.
40. Coghill RC, et al. (1994) Distributed processing of pain and vibration by the humanbrain. J Neurosci 14(7):4095–4108.
41. Porro CA, Cettolo V, Francescato MP, Baraldi P (1998) Temporal and intensity codingof pain in human cortex. J Neurophysiol 80(6):3312–3320.
42. Ter Minassian A, et al. (2013) Dissociating anticipation from perception: Acute painactivates default mode network. Hum Brain Mapp 34(9):2228–2243.
43. Loggia ML, et al. (2012) Disentangling linear and nonlinear brain responses to evokeddeep tissue pain. Pain 153(10):2140–2151.
44. Kucyi A, Moayedi M, Weissman-Fogel I, Hodaie M, Davis KD (2012) Hemisphericasymmetry in white matter connectivity of the temporoparietal junction with theinsula and prefrontal cortex. PLoS ONE 7(4):e35589.
45. Viane I, Crombez G, Eccleston C, Devulder J, De Corte W (2004) Acceptance of theunpleasant reality of chronic pain: Effects upon attention to pain and engagementwith daily activities. Pain 112(3):282–288.
46. Foss JM, Apkarian AV, Chialvo DR (2006) Dynamics of pain: Fractal dimension oftemporal variability of spontaneous pain differentiates between pain States. J Neurophysiol95(2):730–736.
47. Baliki MN, Geha PY, Apkarian AV, Chialvo DR (2008) Beyond feeling: Chronic painhurts the brain, disrupting the default-mode network dynamics. J Neurosci 28(6):1398–1403.
48. Weissman-Fogel I, et al. (2011) Abnormal cortical activity in patients with temporo-mandibular disorder evoked by cognitive and emotional tasks. Pain 152(2):384–396.
49. Napadow V, Kim J, Clauw DJ, Harris RE (2012) Decreased intrinsic brain connectivity isassociated with reduced clinical pain in fibromyalgia. Arthritis Rheum 64(7):2398–2403.
50. Baliki MN, et al. (2012) Corticostriatal functional connectivity predicts transition tochronic back pain. Nat Neurosci 15(8):1117–1119.
51. Worsley KJ, et al. (2002) A general statistical analysis for fMRI data. Neuroimage15(1):1–15.
6 of 6 | www.pnas.org/cgi/doi/10.1073/pnas.1312902110 Kucyi et al.