Evidence about extending the duration of oral contraceptive use to suppress menstruation
Upload
independentCategory
view
0download
0
PDFlib PLOP: PDF Linearization, Optimization, Protection
Page inserted by evaluation versionwww.pdflib.com – [email protected]

PART II. CONTRACEPTION AND STERILIZATION
Mechanism of Action of Progesterone as Contraceptive for
Lactating Womena S. DfAZ, P. MIRANDA, A. BRANDEIS,
H. CARDENAS, AND H. B. CROXATTO Instituto Chileno de Medicina Reproductiva
Consultorio de Planijcacibn Familiar J. K Lastarria 29, Depto. I01
Santiago, Chile
INTRODUCTION
Although lactational amenorrhea is associated with a strong inhibition of fertility, breastfeeding women in whom menstrual cycles are reinitiated or who introduce supple- ments to their infant’s diet, thereby diminishing the amount of breastfeeding, are exposed to a rapidly increasing risk of pregnancy.’.* Therefore contraceptive methods are required during breastfeeding and should be selected from among those that do not interfere with milk production, the infant’s growth, and maternal and infant health.3
Progesterone (P) administration has proven an effective and innocuous contracep- tive method for lactating women when administered via subdermal implants4 or vaginal rings.5 Plasma levels that cause this contraceptive effect are within the lower half of the normal luteal phase valuess Such levels are able to prolong the length of lactational amenorrhea, and 70% of treated women remain in such condition by the end of the eighth postpartum month, while only 33% of the control subjects are amenorrheic at that time.3 Furthermore, the occurrence of regular bleeding, which may reflect recovery of ovarian cyclicity, is a rare event in progesterone-treated women.5
The present study was designed to establish the mechanism by which progesterone prolongs lactational amenorrhea and infertility. Previous work showed that prolonged lactational amenorrhea in untreated women is associated with higher prolactin (PRL) levels, a greater PRL increase in response to suckling,6 and lower estradiol (EJ levels’ than those found in lactating women whose menstrual cycles resume early after de- livery.
These differences were detected since the first postpartum month and when all women were fully nursing and cannot be attributed to differences in the breastfeeding pattern between groups. They suggest that a different sensitivity to suckling of the breast-hypothalamus-pituitary system may explain different lengths of lactational amenorrhea.
‘This work was undertaken as part of the contraceptive development program sponsored and coordinated by the International Committee for Contraception Research of The Population Council, Inc., New York. The financial support provided by the U.S. Agency for International Development, the United Nations Population Fund, the Andrew W. Mellon Foundation, the Rockefeller Foundation, and the George J. Hecht Fund is gratefully acknowledged. The content of this report does not necessarily reflect the policy of any of the funding sources.
11

12 ANNALS NEW YORK ACADEMY OF SCIENCES
The following is a preliminary report of the endocrine profile associated with the use of progestrone in lactating women. We hypothesized that progesterone would bring all women into the pattern observed in spontaneously occurring prolonged amenorrhea. To explore this hypothesis, basal and postsuckling PRL levels, E, levels, and follicular growth were examined in lactating women treated with progesterone vaginal rings or a Copper-T 380-A device as contraceptives.
MATERIALS AND METHODS
Population
Participants were urban postpartum women who wanted to breastfeed their child for as long as possible and were selected according to the following criteria: age 18-38, parity 1-3, normal pregnancy, vaginal delivery at term of a healthy child of normal birthweight, and no chronic disease or condition requiring continuous drug therapy. Only healthy women with an adequate nutritional status and Hb levels higher than 100 P/L were included.
Follow-up Study
Women were given an appointment at days 7, 20, and 30 post partum for clinical evaluation, reinforcement of instructions for breastfeeding on demand, and information on the choices available to avoid a new pregnancy. A monthly calendar was provided to record the number of nursing episodes each day and night and all days on which bleeding or spotting occurred. Contraceptive methods were initiated at day 60 f 5 post partum according to the woman’s choice. Thereafter, follow-up visits were scheduled monthly up to the end of the first year and at 3-month intervals during the second postpartum year.
The women were instructed not to give their babies any liquid or solid food or water and to use the breast as the only source of water and nutrients, during the first 6 months post partum except for the administration of vitamin drops. Milk supplements were indicated only when inadequate infant growth was diagnosed. The Boston percen- tile weight curve for male infantss was used as the reference standard. Nondairy meals were introduced after the sixth postpartum month.
Treatments
Progesterone vaginal rings (PVR) were manufactured by The Population Council, New York. Rings that were used to assess the contraceptive efficacy of progesterone, initially released daily doses that ranged from 5 to 15 mg per day. The 15-mg ring was used in the study of the mechanism of action, and showed a release rate in vitro that ranged from 15 mg per day at the beginning of incubation to 10 mg per day at 90 days.

D I M ef al.: PROGESTERONE AS CONTRACEPTIVE 13
When incubated in vitro after being used by women for 3 months, they released 9 f 0.5 mg per day, which allows us to assume that in vitro and in vivo release rates are comparable. Progesterone plasma levels ranged from 20 nmol/r. during the first ten days to 11 nmol/L at day 90.9 Rings were self-administered at day 60 f 5 post partum and were replaced at 90 f 5-day intervals.
A contemporary control group was formed by women treated with a Copper-T device (T-Cu), also inserted at day 60 k 5 post partum. Data collected in untreated women who were willing to rely on lactational infertility2 were used to compare pregnancy rates.
Blood-Sampling Protocols
The objective of the first study (Study A) was to assess ovarian function in lactating women treated with a PVR or a T-Cu device. For this purpose, blood samples for measurement of P and E, levels were obtained once weekly after treatment. On the same day pelvic ultrasonography was performed to assess the presence and size of ovarian follicles. After detection of follicular activity, blood samples and ultrasonogra- phy were performed twice a week to detect ovulation.
The objective of the second study (Study B) was to assess PRL basal levels, PRL response to suckling, and PRL levels after suckling in women treated with a PVR or a T-Cu. For this purpose blood samples were obtained at fortnightly intervals. Each time, the first sample was drawn around 1600 hr, at least 1 y2 hours after the preceding nursing episode. The baby was nursed afterwards and the next sample was obtained 30 minutes after the initiation of suckling. The hour of the day and the interval after suckling in which samples are drawn have been selected because the PRL response to suckling shows a significant difference at this time between women with a short and with a long period of amenorrhea.6 The sampling was initiated at admission and continued until the eighth postpartum month or the second menses.
The samples were collected in tubes containing heparin and the plasma was stored at - 20" C until assayed. Women were free to withdraw from the study at any time without jeopardizing their medical care.
Hormone Assays
Prolactin, estradiol, and progesterone were measured using the reagents and meth- odology of the WHO Programme for the Provision of Matched Assay Reagents for the RIA of Hormones in Reproductive Physiology.'O All samples from an individual woman were analyzed in duplicate in the same assay.
Definitions
The following definitions were used: Ovulation: In Study A the occurrence of ovulation was assessed by ultrasound
examination done twice a week. In the control group, it was confirmed when progester- one plasma levels above 9.5 nmolh were detected after follicular rupture.
14 ANNALS NEW YORK ACADEMY OF SCIENCES
First postpartum bleeding: In both studies first postpartum bleeding was defined as any bleeding separated from the puerperal bleeding by 10 or more days and which consisted of at least one day of normal bleeding or three consecutive days of spotting. Bleeding induced by the insertion of the PVR or the IUD was not considered in the analysis.
Pregnancy: Pregnancy was diagnosed by clinical examination and confirmed by the presence of hCG in urine. The day of conception was calculated by adding 14 days to the first day of the last menses and, where required, adjusted subsequently according to the gestational age of the newborn when this was available.
Data Analysis
The Pearl Index was used to calculate pregnancy rates. Monthly mean values for each hormone in each subject were calculated to account for irregularities in the number of samples per subject per month. Mean values per group were calculated for each postpartum month using the mean monthly level per subject allocated to the group. The comparison of PRL and E2 levels was done by ANCOVA. Hormonal levels and time post partum were considered continuous variables and treatment was regarded as a discontinuous variable. The duration of the nursing episode that originated the PRL response was also compared by ANOVA.
Prolactin levels were log-transformed before the analysis because of the larger variance observed in the higher concentration in comparison to the lower values. The exception was A PRL, because in a few samples the level decreased after suckling.
Fisher’s exact probability test was used to assess differences in distribution between groups. The SAS Statistics Software (SAS Institute, Inc., Box 8000, Cary, NC) was used for data analysis. Values of p < 0.05 were considered significant.
RESULTS
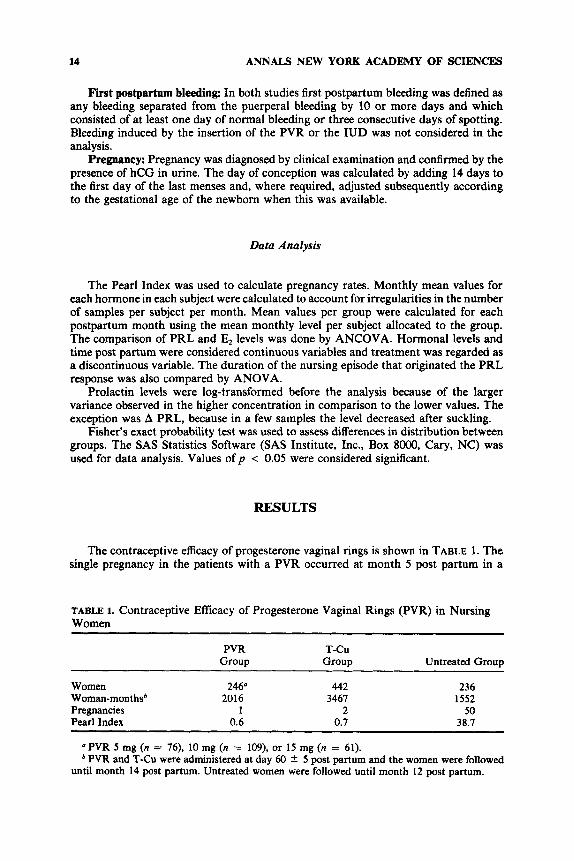
The contraceptive efficacy of progesterone vaginal rings is shown in TABLE 1. The single pregnancy in the patients with a PVR occurred at month 5 post partum in a
TABLE 1. Contraceptive Efficacy of Progesterone Vaginal Rings (PVR) in Nursing Women
PVR T-CU Group Group Untreated Group
Women 246“ 442 236 Woman-monthsb 2016 3461 1552 Pregnancies 1 2 50 Pearl Index 0.6 0.1 38.7
“PVR 5 mg (n = 76), 10 mg (n = 109), or 15 mg (n = 61). * PVR and T-Cu were administered at day 60 2 5 post partum and the women were followed
until month 14 post partum. Untreated women were followed until month 12 post partum.

DIAZ et al.: PROGESTERONE AS CONTRACEPTIVE 15
TABLE 2. Characteristics of Women Enrolled in the Studies of the Endocrine Profile
Study Group
PVR (n = 36)
T-CU (n = 28)
Age (yr) Parity (no.) Weight (kg) Height (cm) Percent amenorrheic
at day 60 at day 180 at day 240
at month 3 at month 6
Female Male
Birth Month 6
Percent fully nursing
Sex of the infant (%)
Infant’s weight (9)
24.5 f 3.4 2.0 -t 0.8
58.4 f 7.1 154.9 f 4.2
100 83 18
100 68
61.1 39.9
3253 f 215 7110 f 969
25.5 f 4.3 2.1 f 0.1
58.3 f 6.3 154.7 If: 4.0
100 39 29
100 74
53.6 46.4
3324 5 319 1924 f 192
NOTE: Values are mean f SD unless sbecified. No significant differences were found between groups except for the length of amenorrhea (p
< 0.oOol).
fully nursing cycling woman who removed the ring for more than 36 hours during the twelfth day of a menstrual cycle. Nursing women treated with a PVR or a T-Cu showed similar pregnancy rates, whereas untreated women showed a significantly higher risk of pregnancy during the first postpartum year.
The endocrine studies were performed in 36 users of a PVR and 28 users of a T-CU who had similar characteristics at admission and a similar breastfeeding performance (TABLE 2). All women were amenorrheic at admission. Seventy-eight percent of PVR users and 29% of T-Cu users remained in amenorrhea at the end of the eighth month post partum. The PVR group experienced a significantly lower risk of bleeding (p < 0.O001) than did the control group.
Study A
Sixteen women were enrolled in each group. Progesterone levels are shown in FIGURE 1. Ring users show progesterone levels that fluctuate between 16 nmoVL and 9 nmolh according to the length of use of each ring. Mean progesterone levels in Copper-T users were below 6 nmolh and increased with time according to the occur- rence of ovulation.
The results of ultrasound examinations are summarized in TABLE 3. Although ovarian images were atypical when compared to those of normally cycling women, there was evidence of follicular growth in both groups of nursing women since the

16 ANNALS NEW YORK ACADEMY OF SCIENCES
0’, I 1 0 3 6
Treatment month FIGURE 1. Progesterone plasma levels (X 2 SE) in nursing women treated with a progesterone vaginal ring (0, n = 8) or a Copper-T device ( 0 , n = 16); p = 0.0001.
beginning of the observation. Six vaginal ring users showed follicles that reached 10 mm in diameter throughout months 3 to 8 post partum. Follicles bigger than 15 mm were observed only three times (4% of woman-months examined), but preovulatory follicles or evidences of ovulation were not detected. Eleven T-CU users showed follicles that reached 10 mm in diameter. Follicles larger than 15 mm were observed 14 times (23% of woman-months examined), and in seven subjects ovulation was diagnosed by ultrasound and progesterone plasma levels above 9.5 nmolh . The proportion of subjects who ovulated was significantly higher (p = 0.016) in the control group as was the proportion of woman-months where large follicles were detected (p < 0.001).
TABLE 3. Distribution of Lactating Women Treated with Progesterone Rings or a Copper-T Device according to the Largest Follicle Observed in Each Postpartum Month ~~~~ ~
Largest Follicular Diameter (mm)
PVR Group T-Cu Group Postpartum
Month N <10 10-15 >15 N <10 10-15 >15
3 4 5 6 7 8
Total %
16 13 14 10 14 12 14 12 13 11 9 8
80 66 100 82
3 3 1 1 2 1
11 14
0 16 10 4 2 1 14 8 4 2 1 14 6 3 5 1 11 6 2 3 0 4 1 1 2 0 2 2 0 0 3 61 33 14 14b 4 100 54 23 23
NOTE: Both treatments were administered at day 60 2 5 postpartum. Subjects were examined once a week until the finding of one follicle 10 mm in diameter and
A significantly higher proportion of women in the T-Cu group showed follicles > 15 mm than twice a week thereafter. Study was discontinued after two ovulations.
did those in the PVR group (p = 0.0006, Fisher’s exact test).

D1AZ ef al.: PROGESTERONE AS CONTRACEPTIVE 17
0 D .- g 100 u) W - * O 0 I
* . . . . . . , .*. .. . . . . 4. . . . . . . ,
- 1
0 I
3 1
6
Treatment month FIGURE 2. EstradioI plasma levels (X ? SE) in nursing women treated with a progesterone vaginal ring (0, n = 16) or a Copper-T device ( 0 , n = 14); p = O.ooO1.
Pretreatment E, levels (X 2 SD) were 156 61 pmol/L and 172 2 89 pmol/L in the PVR and T-Cu groups, respectively. Post-treatment mean values (FIG. 2) were lower in the PVR than in the T-Cu group throughout the period examined (p = 0.OOOl). The highest E, observed each month was also significantly lower in the PVR group (TABLE 4).
Study B
Thirty-two healthy, fully breastfeeding women were enrolled (PVR n = 20, T-Cu n = 12). The basal plasma PRL levels, A PRL, and plasma PRL levels at 30 minutes after the initiation of suckling are shown in FIGURES 3-5. Basal PRL levels were similar
TABLE 4. Mean of the Highest E, Level in Lactating Women Treated with a Progesterone Vaginal Ring or a Copper-T Device
Treatment Month
Highest Estradiol (pmol/L)
Group Group PVR T-CU
1 214 2 99 342 2 184 2 175 2 53 327 2 181 3 196 ? 71 399 2 196 4 156 2 60 549 2 384 5 189 t 59 324 2 111 6 233 2 70 314 t 159
NOTE: Both treatments were administered at day 60 C 5 post partum. Samples were drawn once a week until finding a 10-mm follicle and twice a week thereafter. p < 0.05 except in month 6.

18 ANNALS NEW YORK ACADEMY OF SCIENCES
3w01 A I
E CI
C
V
.- L
9 1000 a
1 1
3 6 0
0 Treatment month
FIGURE 3. Basal prolactin plasma levels (X +- SE) in nursing women treated with a progesterone vaginal ring (0, n s 20) or a Copper-T device ( 0 , n = 12); no significant difference was found between groups.
in both groups. h PRL and the postsuckling PRL level were significantly higher (p = 0.0007 andp = 0.009, respectively) in women treated with the PVR than in those with the T-Cu. No significant difference between groups was found for the duration of the nursing episodes that elicited the different PRL response (p = 0.07).
DISCUSSION
These preliminary results show that the administration of progesterone to nursing women was associated with a longer period of amenorrhea, lower estradiol levels,
Treatment month
FIGURE 4. Prolactin increase (APRL) in response to suckling in nursing women treated with a progesterone vaginal ring (0, n = 20) or a Copper-T device ( 0 , n = 12); p 0.0007.

DfAZ et nl.: PROGESTERONE AS CONTRACEPTIVE 19
4000-
3000-
2000-
1000-
earlier arrest of follicular growth, and higher PRL increase in response to suckling in comparison with those values in control women. The plasma progesterone levels re- quired to obtain these effects are within the lower half of the normal luteal phase values. The high efficacy of such low levels poses interesting questions about the mode of action of steroids in the physiologic condition associated with lactation.
Lactations1 amenorrhea is dependent on the inhibitory effect of the suckling stimu- lus upon the hypothalamic-pituitary-ovarian axis. 1 1 ~ 1 2 However, some women are less sensitive to suckling. Ovulation and pregnancy can occur in fully nursing women in spite of a high suckling frequency., Lower PRL levels, a diminished PRL response to suckling, and higher E, levels since the first postpartum month are associated with early recovery of menstrual cycles in fully nursing
The endocrine pattern found in PVR-treated women was similar to the one observed in control nursing women who experience a long period of lactational amenorrhea and differs from the pattern found in nursing women who start cycling early after delivery.
- 1 I 1
0 3 6 Treatment month
FIGURE 5. Prolactin levels after suckling in nursing women treated with a PVR (0. n = 20) or a Copper-T device ( 0 , n = 12); p = 0.009.
These findings suggest that progesterone may increase the sensitivity of the breast- hypothalamus-pituitary-ovarian axis to the influence of suckling either directly or by decreasing the effect of estrogens. On the other hand, progesterone may affect the GnRH-releasing process independently of suckling.
An increased sensitivity to suckling is supported by the occurrence of a higher PRL response in progesterone-treated women. Such increased sensitivity may affect both prolactin and gonadotropin secretion, by the same or different pathways, resulting in a longer period of inhibition of gonadotropic secretion induced by suckling itself and of ovarian suppression, as shown by the E, levels and the pattern of follicular growth.
The source and role of the higher E, levels found in untreated lactating women who experience a short period of amenorrhea have not been established. However, if E, exerts a positive feedback on gonadotropic secretion during breastfeeding, progester- one may counteract such an effect and prolong the period of inhibition of gonadotropic secretion by this mechanism.
It has been established that progesterone affects the release of LH by decreasing the frequency and increasing the amplitude of LH pulses either during the luteal phase
20 ANNALS NEW YORK ACADEMY OF SCIENCES
of the menstrual cycle” or when administered to normal women in the midfollicular phase.I4 The influence of progesterone in nursing women may then be explained by a direct inhibitory effect upon the GnRH-releasing neurons. In such cases, the lower I$ levels found in progesterone-treated women would be just an indicator of the altered hypothalamic function. However, vaginal rings delivering similar doses of progesterone in nonnursing women were unable to inhibit ovulation in all subject^.'^ Therefore, the strong inhibitory effect of progesterone upon ovarian function requires the association with the inhibitory effect of suckling.
We conclude that progesterone administration to lactating women seems to enhance the influence of suckling upon the hypothalamic-pituitary-ovarian axis and to sustain the physiologic mechanisms of lactational amenorrhea, which are yet to be disclosed.
SUMMARY
Progesterone vaginal rings releasing 5- 15 mg/day were tested as a contraceptive for lactating women. Progesterone plasma levels achieved ranged from 10 to 20 nmol/ L. Pregnancy rates at the end of the year were < 1% and 39% in treated (n = 210) and untreated (n = 236) nursing women, respectively. Around 70% of treated and 30% of untreated women were amenorrheic at 8 months post partum. The endocrine profile during the first 8 months post partum was assessed in 36 treated and 28 untreated nursing women. Pre- and postsuckling prolactin (PRL) levels were measured at 1600 hr at fortnightly intervals and E, determinations and ovarian ultrasound were per- formed twice a week. Prolactin increases in response to suckling and postsuckling PRL levels were higher, E, levels were lower, and follicular growth was arrested at earlier stages in progesterone-treated than in untreated women. The pattern observed in progesterone-treated women was similar to that in prolonged lactational amenorrhea. This suggests that progesterone increases the sensitivity of the breast-hypothalamic- pituitary system to suckling and reinforces the mechanism of lactational infertility.
REFERENCES
1. KENNEDY, K. I., R. RIVERA & A. S. MCNEILLY. 1989. Consensus statement on the use of breastfeeding as a family planning method. Contraception 39 477-49 1.
2. D~Az, S., G. RODR~GUEZ, 0. PERALTA, P. MIRANDA, M. E. CASADO, A. M. SALVATIERRA, C. HERREROS, A. BRANDEIS & H. B. CROXATTO. 1988. Lactational amenorrhea and the recovery of ovulation and fertility in fully nursing Chilean women. Contraception 2 8 53-67.
CROXATTO, H. B. & S. D~Az. 1987. Postpartum contraception. In Fertility Regulation Today and Tomorrow. E. Diczfalusy & M. Bygdeman, Eds.: 181 - 195. Raven Press. New York.
4. D~Az, S., 0. PERALTA, G. JUEZ, C. HERREROS, M. E. CASAW, A. M. SALVATIERRA, P. MIRANDA & H. B. CROXATTO. 1984. Fertility regulation in nursing women. VI. Contraceptive effectiveness of a subdermal progesterone implant. Contraception 30
5 . D~Az, S., T. M. JACKANICZ, C. HERREROS, G. JUEZ, 0. PERALTA, P. MIRANDA, M. E. CASADO, V. SCHIAPPACASSE, A. M. SALVATIERRA, A. BRANDEIS & H. B. CROXATTO. 1985. Fertility regulation in nursing women. VIII. Progesterone plasma levels and contra- ceptive efficacy of a progesterone-releasing vaginal ring. Contraception 32 603-622.
3.
31 1-326.

D1AZ ef 41.: PROGESTERONE AS CONTRACEPTIVE 21
6.
7.
8. 9.
10.
11.
12.
13.
14.
D~Az, S., M. SERON-FERRE, H. CARDENAS, V. SCHIAPPACASSE, A. BRANDEIS & H. B. CROXATTO. 1989. Circadian variation of basal plasma prolactin, prolactin response to suckling and the length of amenorrhea in nursing women. J. Clin. Endocrinol. Metab. 68: 946-955.
DiAZ, S., H. CARDENAS, A. BRANDEIS, P. MIRANDA, V. SCHIAPPACASSE, A. M. SALVATIE- RRA, C. HERREROS, M. SERON-FERRE & H. B. CROXATTO. Endocrine profile in the first months postpartum and the length of the lactational amenorrhea. J. Clin. Endocrinol. Metab. In press.
NELSON, W. E., Ed. 1964. Textbook of Pediatrics, 8th ed. Saunders. Philadelphia, PA. JACKANICZ, T., H. B. CROXAITO & S. D~Az. 1988. Personal communication. WHO SPECIAL PROGRAMME OF RESEARCH DEVELOPMENT AND RESEARCH TRAINING IN
HUMAN REPRODUCTION. 1987. Programme for the Provision of Matched Assay Reagents for the RIA of Hormones in Reproductive Physiology. Method Manual, 1 lth ed. WHO. Geneva.
HOWIE, P. W., A. S. MCNEILLY, M. J. HOUSTON, A. COOK & H. BOYLE. 1981. Effect of supplementary food on suckling patterns and ovarian activity during lactation. Br. Med. J. 283 757.
MCNEILLY, A. S., A. GLASIER & P. W. HOWIE. 1985. Endocrine control of lactational infertility. I. I n Maternal Nutrition and Lactational Infertility. J. Dobbing, Ed.: 1-24. Nest16 Nutrition, Vevey. Raven Press. New York.
FILICORI, M., N. SANTORO, G. R. MERRIAM & W. F. CROWLEY, JR. 1986. Characterization of the physiological pattern of episodic gonadotropin secretion throughout the human menstrual cycle. J. Clin. Endocrinol. Metab. 62: 1136- 1144.
STEELE, P. A. & S. J. JUDD. 1986. Role of endogenous opioids in reducing the frequency of pulsatile luteinizing hormone secretion induced by progesterone in normal women. Clin. Endocrinol. 25: 669-674.
Copyright © 2022 FDOKUMEN