
Mater Mothers Hospital Alignment 2
399
Mater Mothers Hospital Alignment 2 May 14, 2016
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Mater Mothers Hospital Alignment 2

Mater Mothers Hospital
Alignment 2
May 14, 2016

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Housekeeping
• Toilets
• Fire exits
• Phones on silent

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Good morning and welcome
Time Task Who
9 am Welcome, housekeeping, learning
objectives
Dr Wendy Burton
9:10 Models of Care, Private Practice
Midwives
Anne Williamson, GPLM
Dr Wendy Burton
9:25 Preconception planning Dr Amie Hanlon
10:20 Fertility Dr Amie Hanlon
11:10 Diabetes in Pregnancy Dr Amie Hanlon
11:30 Lunch
Tour of the hospital (optional)
All

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Break for lunch
Time Task Who
12:25 pm Preterm labour, Premature Rupture of
Membranes
Dr Wendy Burton
Claire Maguire
12:40 Post Partum care case work All
12:50 Case Presentations and group
discussion Dr Rob Butler
1:25 Infectious diseases in pregnancy Dr Rob Butler
2:15 Ectopic pregnancy Dr Rob Butler
2:45 Afternoon Tea All

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Welcome back—last session
Time Task Who
3:15 Updates Dr Wendy Burton
3.35 pm Breastfeeding Kathleen Goldsmith, LC
4:05 Neonatal cases All
4:15 Neonatal examination Dr David Cartwright
Dr Andrea McGlade
4:40 Common neonatal presentations Dr Andrea McGlade
4:55-5.00pm Conclusion All

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Learning Objectives
The Advanced Alignment content has been
sourced from feedback provided by the more
than 1 000 GPs who have completed an
alignment since Nov 2008.
The topics that came up repeatedly were
preconception, fertility, postpartum and neonatal
care, breastfeeding and complications in
pregnancy.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Learning Objectives
By the end of these sessions, you should have a
better understanding of the issues, concerns
and available services for women or their
children with
• preconception, fertility or breastfeeding issues
• complications in pregnancy
• common and/or important post partum and
neonatal presentations

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Our thanks go to...
• The Alignment Team
• The Mater Mothers Hospital
• BSPHN for supporting the GP role and for
sponsoring today
• Our presenters, past and present
• Those GPs who provided verbal or written
feedback about our program

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
This presentation is available online
www.materonline.org.au/whats-on/professional-development/gp-
education/resources
It will be updated as required, so may vary in appearance from the
power point you viewed when you attended the alignment program
From www.materonline.org.au go to Shared Care Alignment, find
program resources and look for the most recent Alignment 2 (note
we run three programs, Alignment 1, 2 and, starting this year,
Alignment 3!)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Online resources
www.materonline.org.au/services/maternity/health-professional-information/guidelines-and-policies
brochures.mater.org.au
www.health.gov.au/antenatal
www.ranzcog.edu.au
www.health.qld.gov.au/qcg
www.nhmrc.gov.au/your-health/egenetics/health-practitioners/genetics-family-medicine-australian-handbook-general-prac
www.beyondblue.org.au
www.asid.net.au
www.gplearning.racgp.org.au/
www.adips.org
www.bsphn.org.au
www.brisbanenorthphn.org.au/page/news-and-events/metro-north-maternity-gp-alignment-program-resources/

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.materonline.org.au
This is a 36 page summary of the essential principles underlying GP maternity shared care.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.health.gov.au/antenatal
This is a 306 page comprehensive, evidence based document focusing primarily on first trimester care. The 8 page summary is particularly helpful and there are specific chapters on care for ATSI and rural and remote women.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.health.gov.au/antenatal
Module 2 addresses care in the second and third trimesters of pregnancy and provides guidance on core practices, lifestyle considerations, clinical assessments, common conditions and maternal health tests for healthy pregnant women.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.health.qld.gov.au/qcg/
QHealth has a number of evidence based guidelines and education resources available online

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.materonline.org.au

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Click through to www.bsphn.org.au
This hyperlink takes you to the Maternity Share Care page

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
http://www.bsphn.org.au/education
-events/maternal-shared-care/

Mater Models of care
Anne Williamson, RM, GPLM
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Mater Models of Care
MMH has a number of specialised models of care.
Identification of indigenous status, refugee
background, social risk, drug and alcohol use or
previous pregnancy loss will assist with triage to
the appropriate clinic
Women may choose to have GP share care but
their booking appointments and assessment will
occur in the specialist clinic

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Antenatal Clinics, Models of Care

www.matermothers.org.au/hospitals/mater-mothers-hospital/choosing-your-maternity-care

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
http://brochures.mater.org.au/Home/Brochures/Mater-Mothers-Hospital/Mater-Midwives-Partnership-Program.aspx#top

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Midwifery Group Practice
• This is a midwifery led model of care (MOC) that
works in close collaboration with an obstetrician.
They accept women with various levels of risk,
including suitable women wishing to have a vaginal
birth after caesar (VBAC)
• The RBWH has the birth centre with a similar MOC
and a public water birth option BUT it is a ballot
system and if women live outside the RBWH
catchment, they are not accepted at RBWH

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Midwifery Group Practice
• MGP is for Medicare eligible women who live in the Mater Mothers catchment
• It is not suitable for women who require an interpreter
• MGP is for women planning a vaginal birth
• MGP accept women with various levels of risk, including suitable women wanting vaginal birth after caesarean section
• Women have an allocated midwife they can contact by mobile
• The booking appointment is at the woman‘s home
• Antenatal appointments and education are conducted in a group setting

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Midwifery Group Practice • The allocated midwife or one of her colleagues will care
for the woman during the birth and postnatally
• Women are usually discharged home on the day they give birth
• Young Mothers Group Practice (YMGP) is for women <21 especially those with complex social needs
• All women including MGP have an obstetric booking appointment
• MGP midwives work in consultation with an obstetrician
This is a high-demand model of care so get the referrals in EARLY! (as soon as the due date is
established)
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.mater.org.au/Home/Hospitals/
Mater-Mothers-Hospital/Choosing-your-maternity-care
• Information is available online for women
regarding their options for antenatal care
• Please inform women of their different options
and indicate on the referral form which model of
care they have chosen

Preconception Care
Dr Amie Hanlon MBBS FRANZCOG
Staff Specialist, Mater Mothers Hospital

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Preconception Counseling is about having a mindful approach to preparing for and starting a family. By intentionally preparing your
physical body and opening yourself, heart and soul, you “give birth” to yourself as a mother.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Does it work?
• There is a lack of research and evidence except
for some specific areas

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What are we trying to do?
• Identify risks and act to minimise them
• Optimise health
• Educate

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Do women and health professionals
value preconception care?
YES!!!

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Does it work?
Infertile couples identified & treated sooner
Earlier access to STI screening and genetic counselling
Smoking cessation & ↑ infant birthweight
↓congenital abnormalities

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Who should we offer it to?
• Likely benefits for both high and low risk women
• Highly valued by patients
• Consider as part of your regular health check-
ups
• ?at PAP smear time

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Aspects of Pre-pregnancy Care
• Review of medical and family histories
• Detecting, treating and preventing infections
• Addressing lifestyle factors, nutrition and environmental
exposures

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Review of medical and family histories
• Diabetes
• Hypertension
• Epilepsy
• Thyroid
• Thrombophilias
• Mental illness
• Cardiac disease
• Autoimmune disorders
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Review of medical and family histories
• Medication review
• Ethnic origin
• Family history • NTDs
• CF
• Fragile X
• Tay-Sachs
• Thalassaemia
• Sickle cell
• PKU • Consanguinity

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Personal Obstetric History
• What happened in her previous pregnancy and
what can we do to prepare?
– GDM
– Hypertension
– IUGR
– Labour and Delivery story

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Detecting, treating and preventing infections
• Chlamydia
• Toxoplasmosis
• Varicella Zoster
• Rubella
• CMV
• HSV
• HBV, HCV
• HIV
• Syphilis
• Influenza
• Bordetella Pertussis

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Detecting, treating and preventing infections
• Avoid feeding raw/undercooked meats to pets, avoid cat faeces/litter, wear gloves when gardening
• Hygiene
• Care with urine, saliva, nappies of young children
• Screen STIs
• Vaccinations
• VZV
• Pertussis
• Rubella
• Flu-Vax

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Addressing lifestyle factors, nutrition
and environmental exposures
• Avoid alcohol
• Quit smoking, avoid passive smoking
• Avoid cannabis
• Limit caffeine intake
• Review exposures to toxins in household, workplace or at
recreational activity

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Folic Acid • 0.5mg daily for at least one month before
conception and continuing at least until 12
weeks of gestation
• 5mg if at increased risk
– Anticonvulsant use
– Pre-pregnancy DM
– Previous child or family Hx of NTD
– ? Obese women

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Iodine
• Australia is classified by WHO as a mildly iodine
deficient nation
• NHMRC recommends dietary supplementation
of 150mcg of iodine prior to or as soon as
possible after finding out they are pregnant and
continuing through pregnancy and lactation

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
B12
• Vegetarians and Vegans should be
supplemented during pregnancy and lactation
• RDI – 6mcg/day

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Vitamin D
• Test and/or supplement high risk women
• High rates of deficiency in Australia
• Esp. veiled women, dark skinned women, obese
women and those who use sunscreen regularly
or who get little sunlight exposure
• Changes to Medicare rules mean that a rebate
only applies if risk/eligibility criteria are met,
which are likely to be women who have a lack of
sun exposure or deeply pigmented women.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Other Vitamins
• No evidence to support routine supplementation
• Vit A – harmful
• Vit C and E – of no benefit

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Iron
• Increased demands during pregnancy
• Discontinuing iron-containing multivitamins for the
period that women have symptoms of nausea and
vomiting may improve symptoms
• Routine supplementation not recommended but
have a low threshold for suspecting and
supplementing
– Vegetarians
– Multiple pregnancy

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Calcium
• Cochrane suggests benefit of calcium
supplementation in reducing incidence of
hypertensive disorders and preterm labour
• Benefit greater in those with low baseline
calcium intake
• Intake should be 1300mcg/day
• If starting supplement – 1000mcg daily

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Other minerals • No evidence to support routine supplementation
with Mg, Fl, Zn or rare minerals
• No evidence to support use of other nutritional
supplements – (eg. Omega 3 fatty acids etc.)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Exercise and Weight
• Moderate intensity aerobic exercise (swimming, running,
aerobics, cycling) has no negative effect of mother or
baby in a normal health pregnancy
• No association with miscarriage, congenital
malformations, ectopic, PPROM, placental insufficiency,
IUGR or IUFD (multiple studies!!)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Exercise and Weight
• One study has actually shown that physically fit
women who ran or did aerobics during their
pregnancy had fewer medical interventions
during labour
• Fewer studies on weight training but no adverse
findings with light to moderate weight training
(free weights or machines) and some suggestion
of benefit at reducing low back discomfort (due
to increased core strength)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Addressing lifestyle factors, nutrition
and environmental exposures • Avoid
• soft cheeses
• Un-pasteurised milk
• Pate
• raw eggs
• hot dogs
• deli meats
• undercooked meats
• reheated left-overs
• Aim for normal BMI through regular exercise and balanced nutritious diet
• Avoid predatory fish • Wash fruit and vegetables

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Introducing Jane • Jane is a 24yo receptionist who presents for a
discussion about contraception.
• She has never been pregnant and has been a patient of your practice on and off for a number of years although her last visit was 3 years ago when she presented with a sinus infection.
• She tells you that she has recently moved in with her boyfriend of 18 months. She thinks that she and her partner might consider starting trying for a baby in the next year or so but are not ready just yet to have a baby.
• While they have been using condoms for contraception, they have occasionally had unprotected sex.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What would you consider?
• General issues?
• What to discuss?
• Anything to arrange?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Preconception Care and Fertility
Small Group Work • 6 groups
– 10 mins
• Consider the cues
– Hypothesise re the specific issues that may unfold
– How might you address these?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Lisa
• Lisa is a 30yo accountant who presents for her routine Pap smear
• She is a longstanding patient of your practice and comes to see you regularly for her smears
• She is overweight, with a BMI of 37 which you have discussed previously. She has never been pregnant and is currently single, but has recently met what she hopes to be the man of her dreams
• During your consultation she brings up that she is very interested in having children and is worried about ―time running out‖

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Maddie
• Maddie is 19yo Type I diabetic who has been under your care since childhood
• She works part time in the local child care centre
• It has been a struggle to work with Maddie to control her diabetes during her teen years
• You last saw her 8 months ago and she presents needing prescriptions
• She is sexually active in a new relationship and when you ask if she is planning on having a baby, she shrugs and says, ―whatever. . . .‖

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Melissa
• Melissa is a 42yo G3P2M1. Her children are 10 and
12 and both pregnancies were complicated by GDM
• Her father has recently been hospitalised with a
myocardial infarct at the age of 64 and she decided to
come in for a check-up
• Her BP has always been good and her BMI is normal
• She stopped her OCP 2 year ago after reading in a
blog that she was at risk of clots
• She remains sexually active but considers that at her
age she is unlikely to fall pregnant and she isn‘t really
worried if she did

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Wai Lin
• Wai Lin is a 38yo CEO of a large international
hotel chain and is new to your practice
• She presents requesting a prescription for the
OCP to allow her to skip her period for her
upcoming wedding in a couple of months
• She is using condoms for contraception at
present. She is a longstanding smoker, and
travels regularly for work
• She is planning children, but not right now

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.alcohol.gov.au/internet/alcohol/publishing.nsf/Content/wwtk

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Jessica • Jessica is a 29 year old who is well known to your
practice. She presents for some preconception advice, having stopped her OCP 3 months ago. She has been tracking her periods (there‘s an App for that!) and has looked into websites such as Fertility Friend and is wondering if she should purchase an ovulation kit.
• Her history is unremarkable apart from a distressing episode of depression for which she was briefly hospitalised in her late teens. She was medicated for several years but was able to successfully wean off medication four years ago and no longer sees her psychiatrist.
• There is a family history of diabetes, coeliac disease and bipolar disorder

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Amina
• Amina is a 22yo veiled woman from Somalia who
speaks very little English
• She presents accompanied by her husband, Ahmed,
who translates for her. He is a FIFO worker
• They were married 2 months ago and are keen to fall
pregnant
• They present requesting advice but appear quite shy
• Amina‘s last bloods on file show a Hb of 95 with a
low MCV and follow-up testing confirmed a
thalassaemia trait.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Mater Preconception Care Clinic
• Midwives administer tool
• Consult regarding
additional issues

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Study
• Compare outcomes of pregnancies • women who have had a pre-conception consultation VS
• women who did not
• 8 GOALS OF PERICONCEPTION HEALTH
1. FOLIC ACID 5. OPTIMIZE MEDICAL
CONDITION
2. WEIGHT MANAGEMENT
6. GENETIC SCREEING AND
COUNSELING
3. VACCINATION (RUB, VZV,HBV,
FLU) 7. REPRODUCTIVE RISK
ASSESSMENT
4. CEASE SMOKING, ALCOHOL,
DRUGS 8. PSYCHOSOCIAL
INTERVENTION

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Preconception care at Mater Australian and New Zealand Journal of Obstetrics and Gynaecology 2014; 54: 510–514
Background: To date, there is a lack of evidence to suggest that a systematic and coordinated
approach to prepregnancy care might make a difference.
Aims: To evaluate whether women who receive preconception care through a structured approach will
be more likely to be healthy around the time of conception compared with women who plan their
pregnancy but have not been exposed to preconception care.
Methods: A case control study was undertaken of women who attended the preconception care
service and subsequently conceived, received maternity care and gave birth at Mater Health Services
Brisbane between January 2010 and January 2013. Pregnancy information and birth outcomes for
each woman who attended the service were matched with those of three women who reported that
they had planned their pregnancy but did not attend the service. Records were matched for
prepregnancy BMI, age, parity, prepregnancy smoking status and number of health conditions.
Results: Pregnant women who attended preconception care were more likely to have received
adequate peri-conceptual folate, to report being vaccinated against influenza and hepatitis B, to have
consulted with a specialist with the specific aim of optimising a pre-existing health condition and to
report less weight gain up until booking. Preterm birth and hypertensive disorders of pregnancy were
less common amongst women who had attended preconception care, and there were trends towards a
decreased incidence of gestational diabetes, LGA and fetal anomalies.
Conclusion: These preliminary data provide some optimism that a comprehensive preconception care
service may positively influence maternal and neonatal outcomes.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
But Aime, I only have 15 minutes...!
Covering the basics:
• Pap Smear, breast examination (if not within 18/12)
• Cardiac auscultation
• Antenatal screen
– FBC, Blood group/Ab, Rubella/Syphilis/Hep B/Hep
C/HIV +/- VZV
• Further bloods and imaging as determined by history
Review appointment to discuss results and provide
• Nutrition advice
• Alcohol and smoking cessation advice

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Folate
• Folate, Folate, Folate, Folate, Folate,
• Folate, Folate, Folate, Folate, Folate,
• Folate, Folate, Folate, Folate, Folate,
• Folate, Folate, Folate, Folate, Folate,
• Folate, Folate, Folate, Folate, Folate,
• Folate, Folate, Folate, Folate, Folate,
• 0.5 mg Vs 5 mg Folate, Folate, Folate
• Iodine, Calcium and Vit D

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Infertility—the GP workup
• 15% of couples are affected by subfertility or infertility
• For women who are 25-35 years old, there is a 20% per cycle pregnancy rate; 85-90% are pregnant within 12 months
• Medical evaluation goals for the subfertile/infertile couple are to
– Find a cause
– Provide a realistic prognosis
– Provide options for treatment
• GP role involves
– Educating in normal reproductive physiology
– Initial assessment and work-up
– Referral if/when appropriate

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Infertility/Subfertility
Female factors
• Age
• PCOS
• Obesity (>25, 3 x risk)
• PID
• Endocrine/Auto-immune
• Endometriosis
• Medications/smoking
• Ovarian failure
• Structural defect/fibroids
Male factors
• Smoking (incl pot)
• Drugs (e.g.
anabolic steroids)
• Varicocoele
• Heat
• Insecticides, CHC
• Y chrs deletions
• Structural defects

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Female History
• Primary/Secondary (GPMET*), duration, contraception
• Cycle – menarche, LNMP, regularity, dysmenorrhoea, menorrhagia, intermenstrual bleeding, midcycle – pain/mucus, premenstrual syndrome
• Sexual – activity, dyspareunia, post coital bleeding
• Gynae History – Pap, STD, Breast Examination (opportunistic health screening)
• Infectious Hx – Rubella, VZV, Hep B,C,HIV, PID, Syphilis
• PMHx, PSHx, Treatments, Other, Allergies
• Preconception care issues as per previous slides
*Gravida, Parity, Miscarriages, Ectopics, Terminations

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Female Examination
• Ht, Wt, BMI, BP, HR, Waist circumference (ideal<80 cm)
• Weight change
• Endocrine – thyroid, PCOS (acne, hirsutism), galactorrhoea
• Cardiorespiratory
• Abdominal (surgical scars)
• Speculum – Cervix/Pap, +/- VE

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Female Investigations • Mid-luteal Progesterone (Day 21)
• AN Screen – FBC, blood group/Ab, Serology – Rubella, VZV
• Baseline (Day 3) –
– LH/FSH (during/after menstruation) or AMH (not cycle dependant, thought not to be affected by the OCP)
– Thyroid
– Pituitary, Drugs – Prolactin
– PCOS - SHBG, Androgen profile, ?OGTT/Lipids
• Tubal patency (Day 5-10) – HSG (Hysterosalpingogram, X-ray + dye ~ $346 cost, rebate ~$100), sonohysterogram (USS + saline ~$1220, rebate ~ $600, Pelvic USS included)
• Pelvic USS (Day 5-10)– ovaries, structural lesions, ? fibroids

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
AMH
• The new kid on the block
• Thought to be a measure of ovarian reserve
• May be elevated in women with PCOS
• Needs to be interpreted with care – the levels fall
progressively with age and the use of an AMH
nomogram will assist with understanding the
value of a reading in an individual woman

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
AMH Nomogram www.sciencedirect.com/science/article/pii/S0015028210024106

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Male History
• Primary/Secondary, duration
• Sexual – activity, dysfunction
• Male Hx – STD, testicular injury, epididymo-orchitis
• Infectious Hx – Hep B,C,HIV
• PMHx, PSHx, Treatments, Other, Allergies
• Diet, Lifestyle, Smoking, Supplements

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Male Examination
• Ht, Wt, BMI, BP, HR, Waist circumference (ideal<90 cm)
• Cardiorespiratory
• Stature, shave
• Surgical scars – abdominal/inguinal/testicular
• Size – testes, epididymis, spermatic cord, hernia, penis

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Male Investigations
• Semen analysis (>2ml, >20M/ml, motility, morphology)
• If needed
– FSH, LH, Testosterone
– Consider Karyotype

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Summary
• Infertility – sterility/subfertility, primary/secondary
• One year regular unprotected intercourse, unless clinical indications of underlying pathology, e.g. menstrual irregularity, significant pelvic symptoms, scrotal injury/surgery, advanced maternal age > 38.
• Couples should initially have 3 sets of tests: semen analysis, bloods and imaging of the pelvis to assess ovaries, uterus and tubal patency (Pelvic USS + SHG or USS + HSG)
• Treatment
– cause-based (diagnosis/treatment)
– symptomatic (IVF secures the pregnancy)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Case work
• You have 10 min

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Lisa
Lisa is a 30yo accountant who presents for her routine Pap smear. She is a
longstanding patient of your practice and comes to see you regularly for Pap
smears. She is overweight, with a BMI of 37 and you have had discussions with
her about this previously. She has never been pregnant and is currently single
but has recently met what she hopes to be the man of her dreams. During your
consultation she brings up that she is very interested in having children and is
worried about ―time running out‖.
Lisa comes back 2 years later for her next smear. Her
relationship didn‘t last and she is now very worried about
whether she will ever have children.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Maddie
Maddie is 19yo Type I diabetic that has been under your care since
childhood. She works part time in the local child care centre. It has been a
struggle to work with Maddie to control her diabetes during her teen years.
You last saw her 8 months ago and she presents needing prescriptions.
She is sexually active in a new relationship and when you ask if she is
planning on having a baby, she shrugs and says, ―whatever. . . .‖
Maddie is now 24 and has her life in order. Her
diabetes is well controlled and she got married 6
months ago. She fell pregnant on her honeymoon but
sadly had an ectopic. She has not been on
contraception since then, she continues to try to fall
pregnant and notes her cycles have been irregular.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Melissa Melissa is a 42yo G3P2M1. Her children are 10 and 12 and both pregnancies
were complicated by GDM. Her father has recently been hospitalised with a
myocardial infarct at the age of 64 and she decided to come in for a check-up.
Her BP has always been good and her BMI is normal. She tells you that she
stopped her OCP 2 year ago after hearing that she could be at risk of clots. She
remains sexually active but considers that at her age she is unlikely to fall
pregnant and she isn‘t really worried if she did.
Melissa presents a month later. Her father died and
she is devastated. She has decided that she would
really like another child.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Wai Lin
Wai Lin is a 38yo CEO of a large international hotel chain and new to your practice. She presents requesting a prescription for the OCP to allow her to skip her period for her upcoming wedding in a couple of months. She is using condoms for contraception at present. She is a longstanding smoker, and travels regularly for work. She is planning children but not right now.
Wai Lin presents 12 months later. She stopped using contraception 5 months ago and is worried about not being pregnant. She read on the internet that she needs an early referral for IVF. She has cut down on her smoking, but still drinks fairly regularly. Her cycles are regular.
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Jessica Jessica is a 29 year old who is well known to your practice. She presents for some preconception advice, having stopped her OCP 3 months ago. She has been tracking her periods (there‘s an App for that!) and has looked into websites such as Fertility Friend and is wondering if she should purchase an ovulation kit. Her history is unremarkable apart from a distressing episode of depression for which she was briefly hospitalised in her late teens. She was medicated for several years but was able to successfully wean off medication 4 years ago and no longer sees her psychiatrist. There is a family history of diabetes, coeliac disease and bipolar disorder.
Jessica presents 14 months later, having failed to conceive. She did not follow your advice about seeing her psychiatrist, in part because she considers that time to be behind her and also because it is not something she has shared with her partner. She would like a referral to a fertility specialist, but has heard that they use hormones and she is concerned that this may affect her mood.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
http://cope.org.au

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Management of mental illness
in the perinatal period
If public specialist assessment is required:
Metro South Acute Care Services (1300 MH
CALL = 1300 64 22 55) offer initial triage and
assessment for severe or complex
presentations. They can also provide expert
advice on management and advice around
medications

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Management of mental illness
in the perinatal period
Options continued..
• Mental health assessment and plan if required and manage/refer as appropriate e.g. medication, psychology review privately, via ATAPS (no/low gap) through your PHN for women with a health care card (or experiencing financial hardship) or under Medicare (gap payments usual) or psychiatrist referral.
• A number of psychiatrists offer a one-off assessment with ongoing care returning to the GP.
• Belmont Private Hospital offers the GP Liaison Assessment Service, Ph 1800 700 274, which is a prompt referral option.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Take home message
• Perinatal mental illness is a significant cause of morbidity and mortality, affecting maternal and neonatal outcomes, the health of families and of the community.
• A woman will have an EPDS completed at her booking in appointment. As per the PHR (Pregnancy Health Record) please administer again by 34 weeks, at 6 weeks post partum and prn
• Identification and appropriate treatment is essential to promote optimal outcomes
• Suicide is the leading cause of maternal death in the developed world
• In Qld in 2011, suicide was the number one cause of maternal mortality within a year of the end of pregnancy*
• *Source: Qld Maternal and Perinatal Quality Council

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Amina
Amina is a 22yo veiled woman from Somalia who speaks very little English. She presents accompanied by her husband, Ahmed, who translates for her. He is a FIFO worker. They were married 2 months ago and are keen to fall pregnant. They present requesting advice but appear quite shy. Amina‘s last bloods on file show a Hb of 95 with a low MCV and follow-up testing confirmed a thalassaemia trait.
It is now 13 months later and Amina and Ahmed see you following their third miscarriage. Amina avoids eye contact and says nothing during the consultation.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.health.qld.gov.au/multicultural/default.asp

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
http://www.materonline.org.au/services/refugee-services/
mater-refugee-complex-care-clinic
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Management • Organise a 2nd appointment
– without partner if possible
• Resources
– Domestic Violence Hotline
1800 811 811 http://www.dvconnect.org/
• Facilitate early referral to hospital
– Flag concerns/suspicions
– Enable social worker support

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Diabetes in Pregnancy
• Why do all my GTT reports now talk about ―old‖
and ―new‖ criteria?
• What is the current ―best practice‖?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Old Criteria/Traditional Approach
• GCT on everyone at 26-28 weeks
– 75g glucose load, non-fasting
– If 1hr BSL >7.9, then proceed to . . .
• GTT
– Fast for test, 75g glucose load
– If fasting >5.4 or 2hr >7.9 . . . .
• THEY HAVE DIABETES

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
This works!!!
• ACHOIS study showed
– Reduced incidence of serious perinatal
complications
– At the expense of more IOL and more
admissions to neonatal nursery
– No difference in LSCS rate

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Are the diagnostic levels right?
• In effect since 1991
• Extrapolated from adult medicine
• Are we setting the arbitrary line in the wrong
place?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
HAPO study
• Data on pregnancy outcomes from 25000
women plotted against GTT results
• Demonstrated
– Linear relationship between risk and glucose
intolerance
– Likely that our diagnostic cut-offs were
missing a substantial number of affected
pregnancies

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Linear relationship • How and where do we set the bar?
Yep, the IADPDSG – very helpful as a pnemonic!!!

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Recommendations from expert group
• Early testing
– Low risk – random BSL or fasting BSL
– High risk – GTT
• (obese, previous GDM, PCOS, previous
macrosomia, high risk ethnic group)
• Screen everyone at 26-28wks with GTT
• Change to the new criteria (based on the HAPO
data)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What the Mater is doing
• We tried the early screening thing for low risk
women (random or fasting BSL) for a while but had
absolutely no positives so have decided to ditch it.
• Latest is to also offer HbA1C at booking for those in
a high risk group as an alternative to GTT (GTT still
first choice but HbA1C also OK)
• Still recommend all get screened with GTT at 26-28
weeks (unless early screening already positive)
• New diagnostic criteria adopted

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Currently -
• Not everyone in favour of the international
recommendations
• RANZCOG and ADIPS agreed to implement the
new criteria from Jan 2015
• GP college is dragging it‘s feet!

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Welcome back from lunch
Time Task Who
12:25 pm Preterm labour, Premature Rupture of
Membranes
Dr Wendy Burton
Claire Maguire
12:40 Post Partum care case work All
12:50 Case Presentations and group
discussion Dr Rob Butler
1:25 Infectious diseases in pregnancy Dr Rob Butler
2:15 Ectopic pregnancy Dr Rob Butler
2:45 Afternoon Tea All

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
• Preterm labour (PTL)
• Premature Rupture of Membranes (PROM)
• Preterm Premature Rupture of Membranes (PPROM)
PTL, PROM, PPROM:
What referral to make or test to do
when?
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Pregnancy complications
• Sandra, age 30 years, is a healthy G1P0 who presents
for her scheduled appointment at 28 weeks. She
mentions that over the past 12 hours she has noticed
small amounts of clear fluid leaking onto her underwear.
The following issues need to be considered:
• Does she have PROM?
• Is the fetus viable?
• Is there infection?
Sandra should have a comprehensive assessment, such
as would be done at the PAOU

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Diagnosis PPROM
• Temperature – chorioamnionitis (chorio)
• Maternal and fetal pulse rate – chorio
• Uterine tenderness – chorio/abruption
• Fetal Heart Rate – confirm fetal viability
• Speculum exam – confirm rupture of membranes, colour
of liquor, dilatation of cervix.
• DO NOT PERFORM a digital examination unless the
woman is about to deliver
• Swabs/urine—Chlamydia, Neisseria, lower vaginal swab,
Group B Strep (GBS), E.coli

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Management PPROM
• Best practice care of PPROM involves transfer to tertiary unit if safe
• Consider
– Steroids if less than 36-38 weeks (depending upon mode of delivery)
– MgSO4 if less than 30 weeks and labouring
• If labouring
– IV antibiotics (penicillin) or known GBS +ve
– Tocolysis – nifedipine orally
• If not in labour
– Erythromycin PO

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
PPROM outcomes
• Most deliver within the first 7 days
• If undelivered, they may be managed as an outpatient
• Positive GBS status – induction of labour (IOL) offered at 34 weeks
• Negative GBS status – IOL offered at 37 weeks
• Breech presentation carries a risk of cord prolapse and head entrapment – Caesarean Section offered with rescue steroids prior to surgery
• If the baby is delivered remotely, arrange transfer* to a tertiary unit along with the placenta
• *via Qld Retrieval Service if in a rural or remote area

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Pregnancy complications
• Melanie—healthy 26 year old G1P0
• Uncomplicated pregnancy to date
• 38 weeks pregnant
• Presentation = small amounts of clear fluid
leaking onto her underwear for the past couple
of days
• No abdominal pain or tightening
• What are the issues that need to be considered?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Pregnancy concerns
• Katie—healthy 32 year old G2P1
• Previous pregnancy and delivery were normal
• This pregnancy has been uncomplicated
• 35 week presentation with frequent, intermittent abdominal pain which feels like labour
• Reviewed by PAOU yesterday, diagnosed as having Braxton Hicks contractions and sent her home without a PVE
• Katie does not think she is having Braxton Hicks and would like you to assess her cervix
• What do you do?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Pregnancy complications
• Krystal—healthy 28 year old G1P0
• 33 weeks presentation
• Uncomplicated pregnancy
• Presents with painful abdominal tightenings for
the past couple of days.
• At first these were erratic and uncomfortable
• Now painful, more frequent, lasting longer
• What are the issues that need to be considered?
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Summary of routine tests
Abdominal pain Is she in PTL?
Digital examination can be done if clinically indicated however be aware it may interfere with tests for PTL
Speculum examination – cervix dilated? ROM? – Swabs – Specific testing e.g. Actim partus – Cervical length on USS
If PTL likely arrange transfer* for management • Tocolysis • Steroids • If in labour IV antibiotics (penicillin) • If not in labour, antibiotics not indicated *via Qld Retrieval Service if in a rural or remote area www.health.qld.gov.au/qcg/html/publications.asp

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Qld Maternity and Neonatal
Clinical Guidelines

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Post partum care
Time Task Who
12:25 pm Preterm labour, Premature Rupture of
Membranes
Dr Wendy Burton
Claire Maguire
12:40 Post Partum care case work All
12:50 Case Presentations and group
discussion Dr Rob Butler
1:25 Infectious diseases in pregnancy Dr Rob Butler
2:15 Ectopic pregnancy Dr Rob Butler
2:45 Afternoon Tea All

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Post Partum Care
• You have 10 min for case work
• Each table will need a scribe and a presenter
• Your time starts now

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Blue Group Post partum care
• Julia is a G1P1 who had uncomplicated
pregnancy, a straightforward delivery and post
partum course. She is now 6 days post partum
and presents for her routine visit, along with
baby Jack. They have booked two
appointments, 15 min for Julia and 30 min for
Jack.
• What do you complete for Julia’s checkup?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Systems based approach to Post Partum Care
Post Partum check at 5-10/7
History:
• Adacel/Boostrix
• Breasts
• Complications, calves, contraception
• Delivery
• EPDS prn
• Feeding

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Systems based approach to Post Partum Care
Examination:
• Abdominal examination to monitor uterine
involution; wound check if LSCS
• Breasts +/- BP
• Careful inspection of perineum if vaginal delivery

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Contraception options at 5-10/7 pp
– Abstinence
– Condoms
– Minipill
– Depo/Implanon
– NOT COCP, even if not planning to breastfeed
– NOT IUCD

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Red group, post partum care
• Megan is a G1P1 who had well controlled GDM,
a vaginal birth and third degree perineal tear
• Now 6 weeks post partum, she presents for her
routine visit
• Baby Jasmine has the following appointment for
6 week review and immunisations
• What do you complete for Megan’s checkup?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Systems based approach to Post Partum Care
Post Partum check at 6/52
History:
• Adacel/Boostrix
• Bladder, bowels, breasts
• Calves, contraception
• Delivery debrief prn
• EPDS
• Feeding
• Gestational Diabetes follow up prn
• Hypertension follow up prn

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Systems based approach to Post Partum Care
Examination:
• Abdomen
• Breasts, BP
• Consider Pap smear, inspect perineum if
tear/episiotomy

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Perineal care
• After 6 weeks postpartum for women with anal sphincter injury and those reporting symptoms of anal sphincter dysfunction: – Refer to gynaecologist or uro-gynaecologist or
colorectal surgeon – Care considerations may include:
– Endoanal ultrasound
– Anorectal manometry – Consideration of secondary sphincter repair
– Refer to physiotherapist for assessment and individualised PFMT to help manage pelvic floor dysfunction
Source: Queensland Maternity and Neonatal Clinical Guidelines Program http://www.health.qld.gov.au/qcg/

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Perineal Care Queensland
Maternity and Neonatal Clinical
Guidelines Program www.health.qld.gov.
au/qcg/

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Green Group Post partum care
• Anna is a G1P1 who had uncomplicated pregnancy, a straightforward delivery and post partum course. She is now 5 days post partum and presents for her routine visit, along with baby Trinity. As you commence your routine post partum check, you enquire about feeding and Anna reports that Trinity is unsettled and not feeding well, so this morning she has given Trinity a formula top up.
• How do you manage Anna’s checkup?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Mater breastfeeding advice
• Go to www.brochures.mater.org.au from there you
access the Mater Mothers Hospital link and you will
find a number of topics, including the following:
• Antenatal breastfeeding advice
• Breastfeeding your new baby
• Breastfeeding support centre
• Breastfeeding, blocked ducts and mastitis
• Breastfeeding, expressing and taking your preterm
baby home

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Online breastfeeding options • www.breastfeedinginc.ca/content.php?pagename=videos

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Additional services for
families
www.childrens.health.qld.gov.
au/community-health/child-
health-service/early-feeding-
support-drop-clinics/

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Private face to face or telephone services
• ABA 1800 686 268 www.breastfeeding.asn.au
• Lactation consultants:
• www.lcanz.org/find-a-consultant-qld.htm
• Mater Breastfeeding Support Centre Ph 3163 8200
• Possums Clinic

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Yellow group, Post partum care
• Nicole is a G1P1 who had a normal pregnancy
and uncomplicated vaginal delivery. She
presents at 5 weeks requesting a checkup,
looking pale and tired, reporting that she is still
bleeding very heavily, with pain, blood clots and
regular flooding.
• What do you check?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Orange group, Post partum care
• Carol, a G2P2 whose GTT was positive at 28 weeks
and who you have not seen since you referred her
back to ANC, had a LSCS, delivering a bonny babe
weighing an impressive 4 900 g (10 lb 12 oz). She
is 8 days post partum and presents looking flushed
and moving slowly. Her mother is looking after the
baby and her husband has brought her into your
rooms. Your preliminary observations reveal a temp
of 39.2, BP 105/68 and PR of 112 bpm.
• What is your approach?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Pink group, Post partum care
• Jessie, age 32 years, is a G3P2M1 who had a
natural birth with a private Obstetrician 6 weeks ago.
Jessie has presented for Joshua‘s immunisations
and well baby check. Her husband Pete is with
them and when you complete her EPDS (it wasn‘t
done by her obstetrician…) he shakes his head and
looks concerned as Jessie gives you her answers.
Her score is 11 and she answered ―Never‖ to Q10.
• What do you do?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Infections in pregnancy
Time Task Who
12:25 pm Preterm labour, Premature Rupture of
Membranes
Dr Wendy Burton
Claire Maguire
12:40 Post Partum care case work All
12:50 Case Presentations and group
discussion Dr Rob Butler
1:25 Infectious diseases in pregnancy Dr Rob Butler
2:15 Ectopic pregnancy Dr Rob Butler
2:45 Afternoon Tea All

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Infections in pregnancy
Dr Rob Butler MBBS FRANZCOG
VMO, Mater Private Hospital
Senior Lecturer & Examiner, University of Queensland
Eve Health
Shop 5, 199 Grey Street
South Bank QLD 4101
Telephone 1300 383 432 Facsimile 07 3332 1990
Email [email protected]
Website www.evehealth.com.au

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Rationale and approach
• Focus on common pathogens likely to be
encountered in primary care
• What do patients want to know?
– ―Do I really have this infection?‖
– ―What will it do to me?‖
– ―What will it do to my baby?‖
– ―Can it be treated?‖
– ―What are the long-term consequences?‖

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Outline
• Systemic infections
– Pyelonephritis/Listeria/Influenza
• Local infections/colonisation
– GBS/Bacterial vaginosis
• The congenital infections
– ‗TORCH‘/Varicella/Parvovirus
• Vertical transmission
– HIV/Hepatitis B&C/HSV

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Outline
• Systemic infections
– Pyelonephritis/Listeria/Influenza
• Local infections/colonisation
– GBS/Bacterial vaginosis
• The congenital infections
– ‗TORCH‘/Varicella/Parvovirus
• Vertical transmission
– HSV
– Extra slides after talk: Syphilis/Rubella/HepB/HepC/HIV

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Screening – to check or not?
Recommend Not recommended
MSU m/c/s CMV
Hep B Toxoplasma
Hep C Parvovirus
HIV Herpes Simplex
Syphilis +/- GBS
Rubella
Varicella (if no +ve history)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
UTI/Pyelonephritis
• Increased susceptibility to UTI in pregnancy
– Impaired bladder emptying
– Increased residual volume
– Increased vesicourethral reflux
– Ureteric stasis & hydronephrosis
– Increased urine glucose & alkalinity
• Classification
– Asymptomatic bacteriuria
– Cystitis
– Pyelonephritis

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Asymptomatic bacteriuria
• Uncontaminated, culture +ve MSU
• No clinical infection
• Incidence ~15%, of these:
– 30% progress to pyelonephritis
– Screening/treatment is recommended

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Pyelonephritis
• Incidence 3-4%
• Clinical
– UTI symptoms + loin pain/back pain
– Fever/dehydration
– Electrolyte/creatinine disturbances
– Haematuria with ketones/leuks/nitrites
– Raised WCC not reliable – CRP more useful
• USS KUB/Blood cultures
• Consequences
– Preterm birth (PTB)
– Renal injury/sepsis/DIC

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Listeriosis
• Listeria monocytogenes – Gram +ve, facultative anaerobe
• Source
– Uncooked foods – seafood/dairy/coleslaw
– Re-heated meats
• Clinical:
– Fevers/‘flu-like illness
– Blood cultures/genital swabs confirm Listeria
– Trans-placental spread

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Listeriosis
• Consequences
– Not teratogenic
– 1st trimester, miscarriage rate 50%
– 2nd/3rd trimester, pregnancy loss 40-50%
• Treatment
– Amoxyl/ampicillin and gentamicin
– Delivery depending on gestation

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Influenza
• Pregnant women are at high risk of sequelae from ‗flu – Exacerbated by smoking/asthma – Vaccine not contra-indicated in pregnancy, at any
gestation • NNT = 5 • Passive IgG protects baby in first 6 months
• Birds and swines: – Particularly severe infections – Relenza/Tamiflu (neuraminidase inhibitors) – Admission, support and treatment of bacterial
superinfection – Screening relaxed/vaccine available since 7/2009
• But guideline includes ‗pregnant women‘ in the early treatment group during CONTAIN/PROTECT phases

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Group B Strep
• Common commensal of the GIT
• Prevalence of genital tract colonisation = 20%
• Consequences of infection
– Mother
• Chorioamnionitis
• Endometritis
– Baby
• Sepsis/meningitis/CP/neonatal death

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Group B Strep
• If carriage… 50% colonisation of neonate
• However, rate of infection is still only 3/1000
without prophylaxis

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Group B Strep
• So, who to treat?
– Screen all (USA/NSW) – anorectal/LVS at 37/40 (currently developing bedside assay)
Vs
– Risk factor based prophylaxis • Previous perinatal infection
• Any +ve swab or urine culture in this pregnancy
• Gestation <37 weeks
• ROM > 18hrs, when in labour
• Intrapartum pyrexia

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Group B Strep
• How and when to treat:
– Intrapartum only (unless PPROM with +ve swabs) • Benzylpenicillin
• Clindamycin
– Ideally at least 2 hours before delivery
– If inadequate prophylaxis, baby requires bloods and observation
• Remember, severe anaphylaxis in 1:100 000
• NNT for screening 1:400 vs risk factor approach 1:300

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Bacterial Vaginosis
• Polymicrobial overgrowth, causing vaginitis
– Gardnerella vaginalis is most commonly implicated
• Prevalence is ~20% in pregnant population
• Symptoms; discharge/odour, especially after intercourse/irritation
• Diagnosis
– Amsel Criteria • pH>4.5
• Clue cells
• Amine ‗whiff‘ test
• Characteristic thin, grey discharge adherent to vaginal walls
– Nugent score on microscopy

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Bacterial Vaginosis
• Consequences
– Not teratogenic
– Associated with preterm labour/PPROM/endometritis
• Studies (major conclusions);
– Asymptomatic, incidental detection in pregnancy does not require treatment
– If detected AND there is a history of preterm birth, treatment reduces risk of subsequent PTB (from PPROM)
• Treatment; metronidazole/tinidizole

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Congenital Infections ‘TORCH’
• Toxoplasmosis
• Syphilis
• Rubella
• CMV
• Varicella
• Parvovirus
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
General principles
• Most cause a non-specific viral-like syndrome +/-
rash
• Most avoided by food hygiene/hand hygiene advice
• Serology is mainstay of diagnosis
– If IgG +/IgM -, there is evidence of past exposure
– If IgG +/IgM +, there MAY be acute infection
• Retest with different IgM assay
• IgG level over time
• IgG avidity index

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Risk of impact on fetus by trimester

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
General ultrasound features
• IUGR, especially with normal symmetry and
polyhydramnios (although could also be oligo)
• Intra-cranial calcifications (especially toxo)
• Hydrocephalus
• Microcephaly
• Echogenic bowel
• Hydrops

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
General neonatal syndrome
• Death
• Cerebral palsy
• Delayed developmental milestones
• Chorioretinitis
• Sensory neural deafness
• Haematological consequences
– Anaemia/thrombocytopenia/hepatosplenomegally
• Skin scarring/rash

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Points on individual pathogens…
• Toxoplasmosis
• Varicella
• CMV
• Parvovirus

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Toxoplasma gondii
• Parasitic protozoa
• Cats are not
the enemy!

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Lifecycle

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Toxoplasmosis
• Sources
– Raw, undercooked meat/unwashed vegetables
– Garden dirt
• Chance of infection is:
– Low in 1st T (but sequelae are high if infected)
– Moderate in 2nd T (sequelae moderate risk)
– High in 3rd T (but sequelae are low if infected)
• Investigate further with USS/amniocentesis
• Treat with spiramycin or pyramethamine/sulphadoxine (with folinic acid)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Varicella – antenatal exposure
• Herpes virus
• ‗Exposure‘ = sharing home/face to face >5mins
• Check serology if no reliable history of chicken pox
• If –ve IgG, and…
– Exposure < 96hrs, give Zoster Immunoglobulin (ZIG)
– Exposure >96hrs, no ZIG but Acyclovir if risk factors
for maternal complications (>20/40, smoker, asthma)
– Vaccination not recommended during pregnancy;
recommend vaccination post partum in an IgG
negative woman

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Varicella – antenatal exposure
• 10 day incubation; infectious from 2 days prior, to last scab
• If well and…
– < 24hrs, give acyclovir
– > 24hrs, observe (admit if high risk)
• If unwell, admit to ICU for IV acyclovir – pneumonitis is a severe complication (mortality 40% untreated)
• Try to delay delivery for 7 days (passive Ig)
• Risk of transmission to the fetus (fetal varicella syndrome)
– < 12/40: 0.5%
– 12-20/40: 2%
– > 20/40: Negligible

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Varicella – antenatal exposure

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
CMV
• Herpesvirus (largest virus in this group)
• Most common cause of congenital infection (0.5-2%)
• High risk groups (annual seroconversion rate):
– 2-3%, general population (healthcare workers included)
– 10%, childcare workers
– 20-30%, parents of children in childcare
• If infected…
– 1st trimester: 10% infection rate, 90% of these symptomatic
– 2nd half of pregnancy: 90% infection rate, 10% of these
symptomatic

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
CMV – no good news…
• The bad news:
– Sensitivity of amniocentesis PCR is 45% <20 weeks
• Improves 6 weeks after infection (which takes us to viability)
• Even worse news:
– The test result does not predict the degree of impairment
• The worst news…
– CMV may persist, or reactivate
• Risk of infection > 10% for 2 years
• Return to baseline at 4 years
• Screening is not recommended

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Parvovirus B19
• 60% of women are immune but untested, which leaves an overall risk of congenital infection of…
– 20% if exposed at home
– <10% if community exposure
• Consequences
– 10% extra pregnancy loss < 20/40
– 3% develop hydrops (anaemia), of which…
• 1/3 IUFD; 1/3 resolve with intrauterine transfusion (IUT); 1/3 resolve spontaneously
• USS 1-2 weekly up to 12 weeks,
cordocentesis/IUT

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Vertical transmission
• HSV
• Hep B
• Hep C
• HIV
• Unlike the congenital infections, these are:
– Less associated with congenital syndromes
– a significant cause of maternal morbidity

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
HSV
• 20% of population are sero-positive for HSV II
• Primary infection >30 weeks gestation:
– Vertical transmission is 30% following SVD
– Very small risk of trans-placental infection (<5%)
• Secondary infection and active lesions at birth:
– Vertical transmission is 0.5% following SVD
– If no lesions, risk is negligible (?danger of shedding)
– Why not screen for shedding??

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
HSV - management
• Treat primary lesion with therapeutic acyclovir
• Prophylaxis should be offered if recurrent (>3) outbreaks
• Caesarean recommended for recent primary/active HSV
• Most cases of neonatal infection, no history of lesions
– Only 10-25% of sero-positive women report a history of herpes
– Localised (eyes/mouth)
– CNS or disseminated; mortality 20-30%, severe morbidity

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Take-home messages
• Never rely on the result of a single test
– Repeat weeks apart/another assay/IgG avidity
• Don‘t screen for infections if the result doesn‘t help clinical management
• Public health implications
– Isolate, contact-tracing
• Breastfeeding is only contra-indicated
in HIV, and encouraged for passive
Ig in others
• Wash your hands!!

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Thank you
• Subsequent slides contain notes on:
• * Syphilis
• * Rubella
• * Hep B/C
• * HIV

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Syphilis
• Gram –ve spirochete
• Complicated to diagnose
– Specific tests (TPPA/FTA-ABs/syphilis EIA)
– Non-specific tests (VDRL/RPR titre)
– Generally if 1st+ve, confirm with 2nd
Primary Secondary Latent Tertiary
Low Moderate Low Negligible
– IM procaine penicillin (desensitise if allergy)
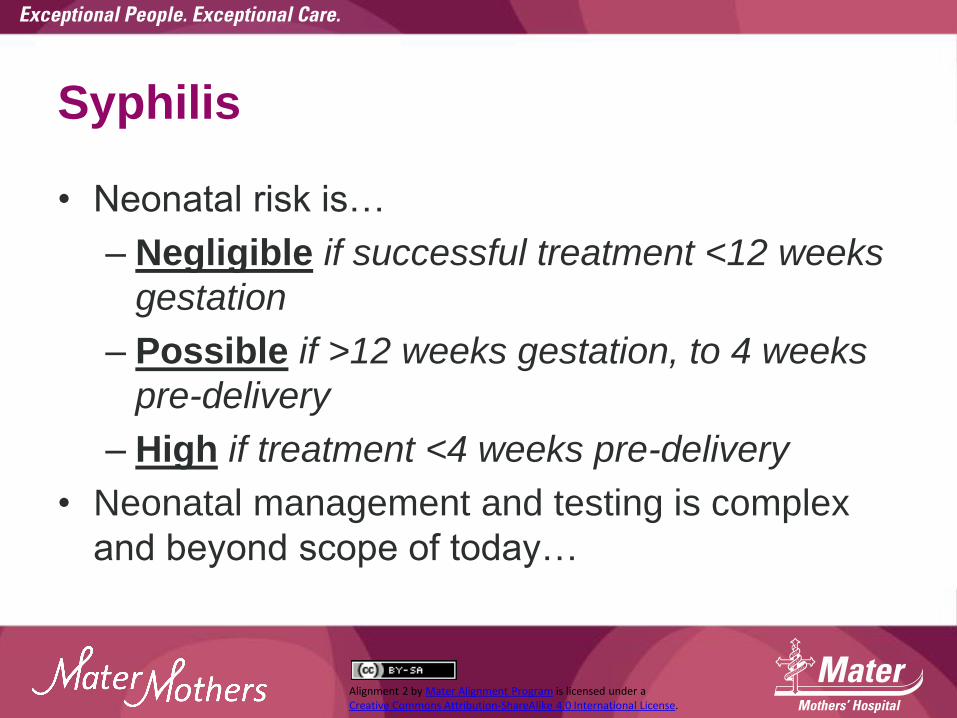
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Syphilis
• Neonatal risk is…
– Negligible if successful treatment <12 weeks
gestation
– Possible if >12 weeks gestation, to 4 weeks
pre-delivery
– High if treatment <4 weeks pre-delivery
• Neonatal management and testing is complex
and beyond scope of today…

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Rubella
• RNA togavirus
• Usually vaccinated, but common to have low-immunity
– <30 = low titre in pregnancy (booster post-partum)
• If maternal infection, fetal risk depends on trimester:
– <8 weeks = 90-100%
– 8-12 weeks = 50%
– 12-20 weeks = 20%
– >20 weeks = <1%
• Supportive treatment, consider termination in 1st T
• Amnio/CVS may be used, but studies not conclusive

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Hep B
• Screening with HBsAg
– If +ve, confirm with HBeAg (high risk carrier) or anti-HBeAb
– DNA if still unsure
– LFTs
• Referral to liver clinic (most treatment can wait)
• Without prophylaxis, vertical transmission > 90% if eAg +ve
– Give neonate HBV vacc and Ig + neonatal/paeds followup
– Caesarean is not protective
• Infection in pregnancy/low titre: Give HBIg and vacc x 3

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Hep C
• Screening with Hep C Abs
– If +ve, some guidelines suggest HepC RNA (??usefulness)
• Referral to liver clinic (most treatment can wait)
• Vertical transmission
– <1% if RNA –ve
– 5% if RNA +ve
– But…
• management/followup is the same
• Caesarean is not protective
• Avoid fetal blood sampling/electrodes/
ventouse

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
HIV
• Multi-disciplinary principles of management • Antenatal
– New diagnosis (screen +ELISA) – confirm with Western Blot
– Regular assessment of CD4/RNA viral load/LFT – Test for TORCH/other STIs – Antenatal HAART (ZDV usually maintained)
• Delivery/post-natal – Intrapartum IV ZDV prophylaxis (avoid PROM) – C/S traditional - there is the option of SVD if well
controlled/-ve load in light of increasing evidence of safety
– Breastfeeding contraindicated

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Zika virus
• The Center for Disease Control in the US has
concluded ―that a causal relationship exists
between prenatal Zika virus infection and
microcephaly and other serious brain
anomalies.‖ http://www.nejm.org/doi/full/10.1056/NEJMsr1604338

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Zika Virus: Symptoms
• Incubation: 3-12 days
• 20% Symptomatic
– Mild lasting ~ 1 week
• Low-grade fever
• Arthralgia (small joints: hands/ feet), myalgia
• conjunctivitis
• Headaches
• Rash – maculopapular
– Exclude other viral illnesses based on travel history

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Zika Virus: Diagnosis
• Index of Suspicion:
– Symptomatology
– Travel History
• Diagnostic testing
– Exclude other viruses: Serology • poor specificity for Flaviviruses
– Reverse-transcriptase (RT)-PCR • Blood: 1 week
• Urine: 2 weeks

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Zika Virus: Testing
• Diagnostic testing
– No commercially available testing kits
• Who?
– Mothers: • Symptomatology + Travel History within 2 weeks
– Neonates: • Children with microcephaly or intracranial calcifications born to mothers
with travel history
• Children born to mothers suspected to have had Zika virus
• Testing Recommendations
– Exclude dengue and chikungunya
– Reverse-transcriptase (RT)-PCR thru QldHealth • Blood: 1 week
• Urine: 2 weeks

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Zika Virus: Pregnancy
• Limited understanding of Outcomes
• No evidence that pregnancy alters susceptibility
– Flaviviruses
• Typically not teratogenic/pathogenic
• Few case reports of congenital anomalies arising
out of Flavivirus infection
– Zika
• ? Frequency of vertical transmission
• ? Rate of abnormality after infection

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Zika virus: Pregnancy outcomes
• Abnormalities reported
– Brain: Microcephaly and intracranial abnormality • Brain atrophy; calcification
– Placenta: calcification • Fetal growth restriction
• ? Few reported cases until now
– Underreporting
– Endemic disease with early age at exposure for immunity before pregnancy
– Rare disease
– More virulent strain

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Managing the risk
• Prevention
– Public Health • Prevent vector becoming endemic in our mosquito
population
• Control mosquito populations
– Patient • Avoid travel to endemic areas
• Reduce mosquito bites (Aedes aegypti– daytime) – Insect repellants containing DEET, picaridin and IR3535
are safe to use in pregnancy

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Interim recommendations for reducing the risk of sexual transmission of Zika virus CDC: Date published: 18 February 2016

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
MFM Referral
• Who?
– All suspected maternal Zika virus cases • Test all symptomatic pregnant women with travel history within 2
weeks – RT-PCR notification
• Request?
– Tertiary level Growth scan q4 weekly • MFM role: Triage when not symptomatic; baseline biometry then
serial growth monitoring; requires 20 week fetal anomaly scan if not done
– Detail all relevant information on referral
• Antenatal Care
– Continue locally unless congenital abnormality suspected
– Neonatal testing

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.health.gov.au
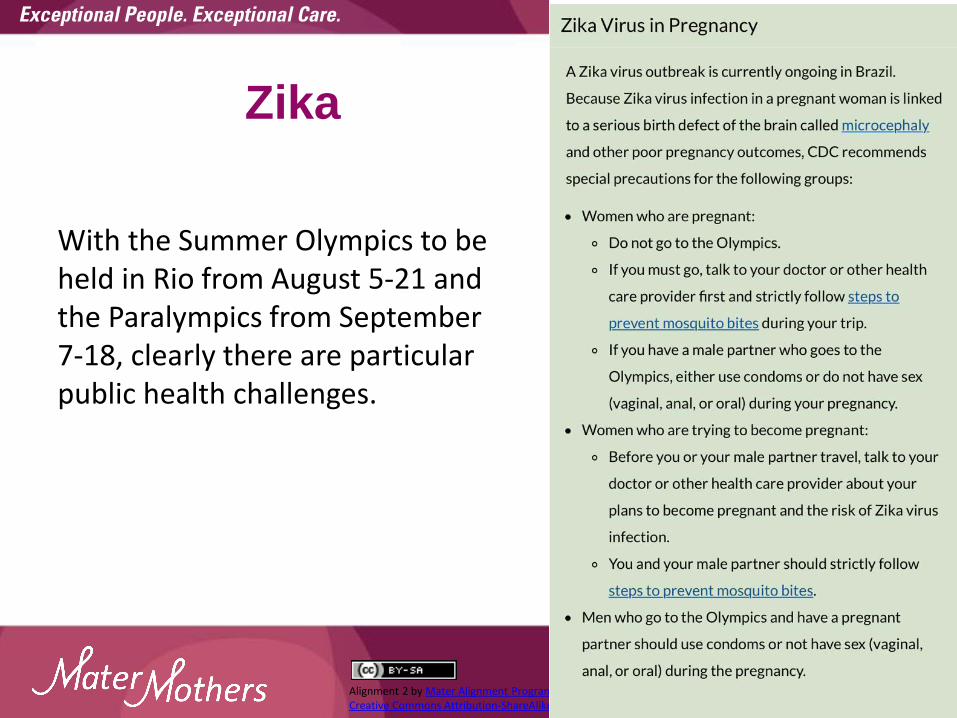
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Zika
With the Summer Olympics to be held in Rio from August 5-21 and the Paralympics from September 7-18, clearly there are particular public health challenges.
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Ectopic pregnancy
Time Task Who
12:25 pm Preterm labour, Premature Rupture of
Membranes
Dr Wendy Burton
Claire Maguire
12:40 Post Partum care case work All
12:50 Case Presentations and group
discussion Dr Rob Butler
1:25 Infectious diseases in pregnancy Dr Rob Butler
2:15 Ectopic pregnancy Dr Rob Butler
2:45 Afternoon Tea All

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Ectopic pregnancy a few pointers
Outline
• Early pregnancy assessment
• Management options for ectopic pregnancy
• Follow-up and management of next pregnancy
• Unusual cases

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
A classic presentation…
• Jodie, 24yo G1P0, LNMP 6 weeks ago
• +ve urine HCG
• Considerations
– Clinical picture (pregnancy symptoms/pain/bleeding)
– Planned pregnancy? Folate? Antenatal screening?
– Serum B-HCG 800
– USS:
• Left ovary 2cm vascular structure, c/w corpus luteum
• Endometrium 18mm, no gestational sac seen

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What now?
• LNMP dates correlation with HCG?
• Clinical assessment – abdominal pain?
• Repeat HCG – timing?
• Repeat imaging – timing?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Another scenario
• Ms A.A, 22yo G1P0T1
• Referred to consultation rooms with 5 weeks
continuous bleeding
– Elective TOP 3 months earlier (was told ‗very
early pregnancy‘ at time of D&C)
– Depot provera at the time of procedure, no
repeat dose, using condoms as well
– Mild abdo pain

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Another scenario
• USS:
– 5 x 5cm left adnexal heterogeneous mass with limited vascularity, adjacent to ovary
– Thin and uniform endometrium and normal right adnexa
– Small amount of free fluid in the POD
• Possibilities?
– B-HCG +ve, quantitative = 1030

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Classic symptoms and risk factors
• Triad of:
– Amenorrhoea, 6-8 weeks post LNMP
– Abdominal pain (and especially shoulder/rectal)
– Bleeding
• Most significant risk factors:
– Previous ectopic pregnancy
– Pregnancy associated with emergency
contraception/POP/IUDs
– Tubal surgery/infection/PID

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Ultrasound: Correlation with B-HCG
• IUP can usually be seen with B-HCG levels
above 800
• A threshold of 1500 will detect 98% of IUPs
– Pitfall; multiple pregnancy
• Higher thresholds will result in more missed
ectopics
• An IUP almost always excludes ectopic
(heterotopic awareness when risk factors)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Appropriate rise in HCG
• B-HCG usually doubles every 48hrs between 5-
8 weeks gestation in a viable IUP
– If the B-HCG is slowly rising by < 50%, it is
usually a non-viable IUP, or ectopic (99%
accuracy)
– Consider multiple or molar pregnancy in
rapidly rising levels
– Single isolated level is less useful for
uncertain clinical scenarios

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What about progesterone?
• High levels (> 65nmol/L) help exclude ectopic
(only 2.5% are ectopic above this level)
• Low levels (< 15nmol/L) predict non-viable IUP
(<1% will be ongoing viable IUP)
• Progesterone differentiates viable from non-
viable pregnancy, but not ectopic from
miscarriage
• Clinical/B-HCG criteria are usually sufficient

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Rare sites
• Around 5% of ectopic pregnancies will be:
– Cornual
– Ovarian
– Caesarean scar
– Abdominal
– Cervical
• The major issues with these are:
– High and appropriately rising B-HCG/progesterone
– Large size and catastrophic rupture if undiagnosed

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Management options
• Expectant
– If falling B-HCG and stable patient, especially PUL
• Medical (methotrexate) criteria
– Stable patient, proven ectopic
– B-HCG < 5000 associated with success >90%
– No C/I to use and reliable follow-up
– Useful for ‗rare site‘ locations (infusion protocol)
• Surgical
– 95% ‗cure‘ rate

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Importance of follow-up
• Especially if PUL or medical management
• Follow B-HCG weekly until –ve (one
measurement is adequate if not GTD)
• Anti-D, vaccinations
• Opportunity for contraception/pre-conception
discussion

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What about next time - prognosis?
• Fertility outcomes
– Pregnancy rates 65-85% per year
– Referral for fertility assessment if > 12/12, and
will likely require IVF
• Recurrence is ~15%
– Salpingectomy ~ 10%
– Salpingotomy ~15-20%
– Methotrexate ~15-20%

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What about next time - Mx?
• Early diagnosis of pregnancy, symptom
awareness
• Serum quantitative B-HCG level
– If <1500 and asymptomatic, repeat 2-3 days
– If rising appropriately, TV USS when B-HCG >
1500
– If rise <50%, consider miscarriage or ectopic
and refer early (allows for all options of
management)
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Interesting Case – Ms LT
• 28yo G2 P0 E1 (previous PUL – MTX)
• PV bleeding, abdominal pain
• Observations stable
• B-HCG
– 31/05: 16 800
– 05/06: 36 000
• USS – 25 x 25 x 30mm right cornual ectopic
pregnancy

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Options for treatment
• Expectant?
• Medical?
– IM MTX – OR 5.5 for failed therapy if B-HCG > 5000
– IV MTX
– Direct injection
• Surgical?
– Wedge resection • Open
• Lap
– Hysteroscopic

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Medical management
• MTX by IV infusion
• F/U clinically stable
• B-HCG
– 12/06: 50 000
– 13/06: 45 000
– 15/06: 50 000
• Impression – failed medical management
• Multi-disciplinary decision for surgical management

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Follow-up
• B-HCG
– 22/06: 1630
– 29/06: 284
– 06/07: 65
– 13/07: 17
– 27/07: <5

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Management issues next time…
• Early diagnosis
• Recurrence
• Placentation
• Delivery
– Timing
– Mode

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Summary
• B-HCG and clinical correlation
• Traditional B-HCG patterns can be unreliable
• Keep in mind the rare cases
• Anti-D
• Refer early for ultrasound next pregnancy, but
not too early!
• Recurrence of ectopic pregnancy, 10-15%

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Welcome back—last session
Time Task Who
3:15 Updates Dr Wendy Burton
3.35 pm Breastfeeding Kathleen Goldsmith, LC
4:05 Neonatal cases All
4:15 Neonatal examination Dr David Cartwright
Dr Andrea McGlade
4:40 Common neonatal presentations Dr Andrea McGlade
4:55-5.00pm Conclusion All

Alignment updates A quick summary of changes and issues that have arisen since the program commenced in 2008

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Testing for Diabetes in Pregnancy
• Early OGTT (HbA1c if not tolerated e.g. due to
nausea/vomiting) for high risk women
• No glucose challenge testing and no random BSL
• Routine OGTT (24 – 28 weeks) for all women not
previously noted as abnormal
• OGTT diagnostic criteria have changed as of January 1
2015
• Prompts are built into the referral template (please
ensure you have the most current version)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
GDM Flowchart
(page 36)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Gestational Diabetes Mellitus
Tight sugar control is recommended;
• fasting BSLs of < 5.0
• 1 hour post prandial of < 8.0
• 2 hour post prandial of < 7.0
The figures vary, but women with GDM have
~ 60% risk of developing Type 2 DM in the
next 10 years, hence the following
recommendations

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Postnatal care of women with GDM
Recommendations:
• Oral glucose tolerance testing (OGTT) six–twelve weeks postpartum to exclude diabetes (cc MMH please)
• Follow up HbA1c testing at least every three years, annually if planning a pregnancy (this now attracts an annual Medicare rebate for high risk patients)
• Repeat HbA1c or OGTT prior to or OGTT early in next pregnancy
• Follow up of impaired fasting glucose by twice yearly checks for frank diabetes in addition to assessment of other risk factors of macrovascular disease

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Education Resources
• Booklets /Pamphlets • Demonstrations (e.g. food models, blood glucose meter) • Useful websites
• You2: www.you2.org.au • Diabetes Australia www.diabetesaustralia.com.au • Australian Diabetes Educators Association
www.adea.com.au • Australasian Diabetes in Pregnancy Society
www.adips.org • Queensland Clinical Guidelines
www.health.qld.gov.au/qcg/html/education.asp#videoconference

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
The catchment area • Mater Mothers Hospital is a private hospital contracted by Queensland
Health to conduct an agreed number of public births per year. Mater
Mothers is both a tertiary referral centre and a local hospital for women
within its catchment. Due to high demand Mater Mothers is unable to
accept routine low risk referrals from outside the catchment area.
Consideration is made for indigenous women and women requiring a
specialist drug and alcohol service
• Women who may require tertiary care should be referred by the GP to
their local health service, where their care may commence, if within the
capacity of the local hospital, or appropriate referrals organised if not.
Please communicate with the MMH GP Liaison if you are at all
uncertain, or if time is critical
• Catchment restrictions do not apply to insured women choosing to birth
at Mater Mothers Private. The GP refers to a private obstetrician and the
woman contacts the Private Booking Office on 3163 8847. A list of
private obstetricians is available at www.materonline.org.au

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.materonline.org.au/
Women living within the
catchment area will be
accepted, however proof of
address is required.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.materonline.org.au/services/
maternity/health-
professional-information/
guidelines-and-policies

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Please consider signing up
• Mater Health Services have created a web site
for where, among other things, women can look
at the models of care available at MMH. Women
who do not have a GP can use this tool to locate
an aligned GP. If you consent being on this list,
a patient could search for and find you on the
mater.org.au site.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.mater.org.au/Home/Hospitals/Mater-Mothers-Hospital/
Choosing-your-maternity-care/Shared-care-GPs

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Please remember to include the woman’s BMI in your referral—that helps the hospital with triage and the researchers with their project

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Please watch out for AOTC
We will keep you updated e.g. about changes to the GDM
pathway, guideline alterations, education events. AOTC,
including past editions, is available online http://www.materonline.org.au/whats-on/professional-development/gp-
education/resources

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Thyroid disease Known thyroid
disease?
Routine testing not
recommended (test > 30 years old, family Hx thyroid
disease, coeliac disease)
Repeat TSH, add T3 | T4 +
antibodies
No further testing
50μg thyroxine
No
TSH > 2.5
Normal
TSH > 2.5 +/- antibodies
Repeat TSH in 4/52
↓ to 25 μg/d
TSH > 2.5 TSH < 0.4
Hyper or hypo?
Endocrine RIVCheck TFT 6-8/
52ly
TSH should be < 2.5↑ thyroxine by 30% once pregnant
↓ thyroxine post partum
Yes
Hyper
Hypo
TSH < 2.5 antibody +ve
TSH usually drops 1st trimester
TSH < normal range
Referral not needed
Physician review +/- referral
Free T3 | T4 elevated
Free T3 | T4 normal
Repeat TSH @ 18, 26 + 34/52 and adjust
dose prn
TSH low
50 μg thyroxine
↑ to 75 μg/d
Watch this space –we’re working on a flow chart to make life simpler!

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
READ AOTC!!!

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.materonline.org.au

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.materonline.org.au/


Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
MAH referral information

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Waitlist information
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
QHealth referral template
This is a helpful document, with decision support built in. An electronic version is available for MD3 on www.gmsbml.org.au and is a supplied template on BP (QHealth Maternity). You can download a paper copy at www.health.qld.gov.au/caru/pathways/docs/mater_refer.pdf

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Online education resources
QHealth has a range of power points, video
conferences, knowledge assessments and
flowcharts available online which flow from
their Maternity and Neonatal Guideline work.
GP relevant topics include Obesity, Early
Pregnancy Loss, Vaginal Birth after caesarean
section (VBAC), Breastfeeding initiation, Neonatal Examination and Neonatal Jaundice
http://www.health.qld.gov.au/qcg/html/implementation.asp#Education

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.health.qld.gov.au/qcg/html/education.asp#videoconference

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Who is responsible for abnormal results?
The clinician who orders the test is responsible for the follow up and prompt referrals when appropriate
• Although a copy of the result is sent to MMH, it is entered into their system without being seen and is only reviewed when the woman comes for an appointment or contacts the hospital for advice
• There are guidelines for consultation and referral and managing abnormal results available in sections 6 and 12 of the MMH GP Maternity Shared Care Guideline www.materonline.org.au/services/maternity/health-professional-information/guidelines-and-policies

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Referral process
• Women with medical conditions should be referred to an
obstetrician on the antenatal referral template. The obstetrician
will consult and refer to the obstetric medicine specialist
• If an already booked woman develops a medical condition
during her pregnancy, please fax a letter to ANC (not another
antenatal referral form) including the relevant clinical details, so
that the appropriate referrals can be organised
• If you are uncertain, or if the woman requires urgent review,
phone the consultant, registrar via switch (3163 8111) or the GP
Liaison Midwife on telephone 07 3163 1861 (you can leave a
message) email [email protected] or mobile 0466 205 710.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
The referral pathway
• All women, regardless of their medical or obstetric risk, should to be referred to their local obstetric hospital. A comprehensive referral will allow the hospital staff to triage appropriately and where necessary, the local obstetricians will liaise with or refer women onto MMH
• Should a woman booked with another hospital develop a complication, contact her local obstetric service so that they can make the appropriate arrangements

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Pertussis immunisation
• From April 2015, Qld Health are funding Adacel for
women in the third trimester of each pregnancy
• The evidence supports a move from a cocooning
strategy to a passive immunity strategy
• Due to the rapid decline in antibody titres,
vaccination is recommended with each pregnancy to
provide maximal protection to every infant; this
includes pregnancies which are closely spaced (e.g.
< 2 years)
• 10 Australian babies died from pertussis from 2006-
2012 and another died in 2015 in WA

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/Handbook10-home
• By immunising women during pregnancy, the infant
benefits from in utero transfer of antibodies
• Pertussis antibodies peak a couple of weeks after
immunisation and then fall rapidly, while transplacental
antibody transfer is most efficient from 30 weeks
onwards
• Immunising women from 28-32 weeks gestation is
recommended, however immunising any time in the third
trimester is beneficial
• Vaccination of mothers at least 7 days before delivery
reduced pertussis disease by 91% in infants <3 months
of age

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Pertussis issues for baby
What about blunting?
• Studies have shown lower levels of anti-pertussis antibodies
at 7 months of age in children born to women vaccinated with
dTpa during pregnancy, compared to children of mothers who
were not vaccinated. However, when children were given a
booster dose of DTPa-containing vaccine at 12–18 months of
age, levels of anti-pertussis antibodies 1 month later were
similar irrespective of whether the child‘s mother was
vaccinated during pregnancy or not.
• From March 2016, an extra DTPa booster dose has been
funded by the Queensland Immunisation Program for children
aged 18 months

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Pertussis immunisation
• Qld Health is no longer funding Pertussis vaccination for fathers or extended family members/household contacts of newborns
• The Australian Technical Advisory Group on Immunisation recommends vaccination every 10 years for the following groups:
– fathers
– extended family members
– household contacts
– medical staff

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Serological testing for varicella immunity
from infection and/or vaccination
• Screening for varicella immunity (from natural infection) or a past history of vaccination should be undertaken as part of pre-pregnancy planning and varicella vaccine given to non-immune women prior to conception.
• Testing to check for seroconversion after varicella vaccination is not recommended. Commercially available laboratory tests are not usually sufficiently sensitive to detect antibody levels following vaccination, which may be up to 10-fold lower than levels induced by natural infection.
• Protection (commensurate with the number of vaccine doses received, see 4.22.4 Vaccines above) should be assumed if a child or adult has documented evidence of receipt of age-appropriate dose(s) of a varicella-containing vaccine.
www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/handbook10-4-22

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Mater Shared Electronic Health
Record
• MHS have an electronic alternative to the Pregnancy
Health Record (PHR)
• There are 3 component parts: Hospital, Mater Doctor
Portal and Mater Patient Portal

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Mater Doctor Portal
Mater Doctor Portal for GPs and private obstetricians (external clinicians)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Your next steps…
For further information about these projects contact:
1800 228 470
Or indicate your interest on the feedback form for
this session

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.materonline.org.au/getattachment/Services/Maternity/Health-Professional-Information/Guidelines-and-
Policies/MMH_AntenatalAppointmentSchedule.pdf
18-20 week visit
• Review morphology scan and follow up/referrals prn
• Organise follow up of placental position prn
• Confirm EDC, if not already done
24 weeks
• Routine AN assessment ? Additional care required
• Fundal height and health promotion/parent education
28 weeks
• As above + FBC, Blood group antibodies, GTT +/- antiD
• Discuss infant feeding, Vit K and Hep B
• Discuss and commence birth plan
• Consider discharge planning
• EPDS routinely administered between 28-34 weeks or prn

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Don’t forget… 31 weeks
• As above, review results and follow up prn
• Confirm consent for Vit K, Hep B
34 weeks
• AntiD prn
• Repeat USS if low lying placenta on morphology scan
• Routine assessment, reassess schedule
• Discuss birth plan
38 & 40 weeks
• Routine assessment
• Confirm understanding of the signs of labour and indications for admission to hospital

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Please don’t forget to enquire or inform
women about….
• Breastfeeding intentions and availability of
support e.g. ABA, Mater Breastfeeding Support
Centre, brochures.mater.org.au
• Vit K and Hep B
• Birthing plans
• When to come to hospital/ring labour ward
• Post natal checks

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
http://brochures.mater.org.au/Home/Brochures/Mater-Mothers-
Hospital/Information-for-parents-about-labour-and-birth

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Are you aware...? c) Special Conditions – Shared Care and Ante-natal Care
• GPs who treat obstetric cases (including the provision of Ante-
natal Care) but who are not insured for obstetrics (under the GP
Obstetrics or GP Rural Obstetrics Categories) must adhere to the
following minimum guidelines to ensure their entitlement to
indemnity is maintained under the Policy:
Shared Care Guidelines (summarised)
• Women are to have their full antenatal screening tests
• Women are to be referred to an obstetrician, GP obstetrician or
obstetric hospital clinic by 20 weeks
• Women must have a review by an obstetrician/GP
obstetrician/obstetric hospital clinic at 36 weeks and again at term

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Categories of Insurance Guide
www.miga.com.au • Should any problems occur before 36 weeks, the
obstetrician/GP obstetrician/hospital clinic must be advised and consulted
• The delivery of the baby must rest with the consultant/obstetric hospital
• If you are required to adhere to more restrictive Shared Care Guidelines which apply in your State, region, hospital or clinic, then those guidelines must also be complied with to maintain your entitlement to indemnity
• GPs are covered in an emergency situation but must have obstetric cover if they wish to be involved in inductions, management of labour or deliveries
• If you are a GP Obstetrician and you wish to deviate from the relevant Shared Care Guidelines which apply, you must hold GP obstetric insurance, regardless of whether the delivery is in the public or private system.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Moving on….
Time Task Who
3:15 Updates Dr Wendy Burton
3.35 pm Breastfeeding Kathleen Goldsmith, LC
4:05 Neonatal cases All
4:15 Neonatal examination Dr David Cartwright
Dr Andrea McGlade
4:40 Common neonatal presentations Dr Andrea McGlade
4:55-5.00pm Conclusion All

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Mater on line breastfeeding advice
• Go to www.brochures.mater.org.au from there you access the Mater Mothers Hospital link and you will find the following topics:
• Antenatal breastfeeding advice
• A guide to breastfeeding
• Breastfeeding support centre
• Breastfeeding support centre – equipment
• Breastfeeding, expressing and taking your preterm baby home

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Breastfeeding
Mater Mothers’ Breastfeeding Support Centre

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
• Milk is formed in alveoli and carried by ducts to the nipple.
• The lobes are not neatly arranged around the
nipple but intertwined like roots of a tree.
• Clusters of secretory alveoli form a lobule that drains into the ductule. Ductules from 20-40 lobules join to form the lactiferous duct.
• Between 4 and 18 milk ducts exit the nipple
The lactating Breast

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Lactating breast…..
• As well as glandular tissue the breast also has
connective and fat tissue around the lobes.
• Each lobe is separated by adipose tissue, blood
vessels, nerves and lymphatics.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Basics of Milk Production
• Milk supply doesn‘t start out as a demand and
supply process.
• During pregnancy and the first few days
postpartum milk supply is hormonally driven.
(Endocrine control system).

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Endocrine Control
• Lactogenesis 1 – breasts start producing colostrum from around 16 weeks. Progesterone inhibits milk secretion.
• Lactogenesis 2 – milk will increase in volume around 30-40 hours after birth and the delivery of the placenta.
• These stages occur whether a mother breastfeeds her baby or not.
• The impact of expressing and breastfeeding in the first 4 days has a major impact on ongoing supply issues long term.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Autocrine Control of Milk Synthesis
• After Lactogenesis 2 there is a switch to ‗local
control‘.
• This maintenance stage is called Lactogenesis
3.
• Milk removal is the primary control mechanism
for supply.
• Prolactin receptors are only laid down in the first
6 weeks. Frequent breast stimulation during this
time is essential for ongoing adequate supply.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What does current research
tell us about milk production?
• Milk contains a small whey protein called Feedback Inhibitor of Lactation (FIL).
• When the breast is full and more FIL is present, productions slows.
• When the breast is emptier, and less FIL is present, production speeds up.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Storage Capacity
• Mother‘s with large or small storage capacities
can still produce plenty of milk for their baby.
• However – a mother with a large storage
capacity may be able to go longer between
feeds without impacting on her supply or her
baby‘s growth.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Positioning and Attachment

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Recognising nutritive sucking
Really good drinking Nibbling
www.breastfeedinginc.ca

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Common breastfeeding problems
Low milk supply •Is it really low supply or issues with milk transfer?
•Does the baby appear to ‗drink‘ at the breast?
•Wet and dirty nappies? / lactose Overload ?
•Age of baby? / reflux ?
•Mother‘s medical history.
•Encourage parents to identify nutritive drinking-
ABA links and videos available

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Using Medication to Increase Supply
• Domperidone is known to increase pituitary prolactin secretion and human milk production. This is not a long term solution, medication should be associated with effective breast drainage and an effective feeding plan.
• Fenugreek is a common herbal preparation that has been shown to increase milk supply.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Blocked Ducts and Mastitis
• Reddened area or segment of breast which becomes tender, hard and painful.
• If a fever is also present - the Mother has mastitis and may require antibiotics.
If untreated/poor drainage. An abscess may develop that can be Diagnosed via Ultrasound.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Management of Blocked Ducts and Mastitis

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Painful or damaged nipples
• Most likely cause is
poor latch.
• ? Thrush
• ? Infection
• ?Tongue-tie
• ?vasospasm
secondary to nipple
compression.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
How To Get Help • Mothers requiring further assistance with
are able to book an appointment at the Mater Mothers’ Hospital Breastfeeding Support Centre. This no cost appointment is available for all mothers with children up to six months of age.
• Australian Breastfeeding Association 1800 686 2 686 (1800 mum 2 mum)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Breastfeeding Support Centre
Level 7, Mater Mothers Hospital
Raymond Terrace, Brisbane
PH- 3163 8847

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Recognising nutritive sucking
Really good drinking Nibbling
www.breastfeedinginc.ca

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Neonatal examinations and presentations
Time Task Who
3:15 Updates Dr Wendy Burton
3.35 pm Breastfeeding Kathleen Goldsmith, LC
4:05 Neonatal cases All
4:15 Neonatal examination Dr David Cartwright
Dr Andrea McGlade
4:40 Common neonatal presentations Dr Andrea McGlade
4:55-5.00pm Conclusion All

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Blue Group Neonatal care
• Julia is a G1P1 who had uncomplicated pregnancy, a straightforward delivery and post partum course. She is now 6 days post partum and presents for her routine visit, along with baby Jack. They have booked two appointments, 15 min for Julia and 30 min for Jack.
• What do you complete for Jack’s checkup?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Red group, post partum care
• Megan is a G1P1 who had well controlled GDM,
a vaginal birth and third degree perineal tear
• Now 6 weeks post partum, she presents for her
routine visit
• Baby Jasmine has the following appointment for
6 week review and immunisations
• What do you complete for Jasmine’s checkup?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Neonatal Examination –
Systematic Approach
• Top to toes (as per Red Book checklist)
• Growth parameters: weight, length, HC
• Hips, Heart, Hernias, Eyes are the key elements
Thanks to Dr Julie Beak, paediatrician, for providing most of the following slides

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.health.qld.gov.au/qcg/documents/g-newexam.pdf

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
The tricky bits....
• Examination of red reflex in an infant who won‘t open their
eyes
• Auscultation of the heart in a crying infant (or for that
matter, a crying child)
• Uneven thigh creases
• Clicky Vs Clunky hips
• CDH Vs DDH – why the change?
• How much jaundice is too much jaundice?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Green group Neonatal care
• Rebecca is a G1P1 who had uncomplicated pregnancy, a straightforward delivery and post partum course. She is now 6 weeks post partum and presents for her routine visit, along with baby Olivia. Rebecca is worried something is wrong with Olivia’s hip as the nurse at the chemist has commented that Olivia has a “clicky” hip. As you undress Olivia ready for her examination, you notice a small inguinal lump.
• How do you conduct your examination?
• What do you advise?
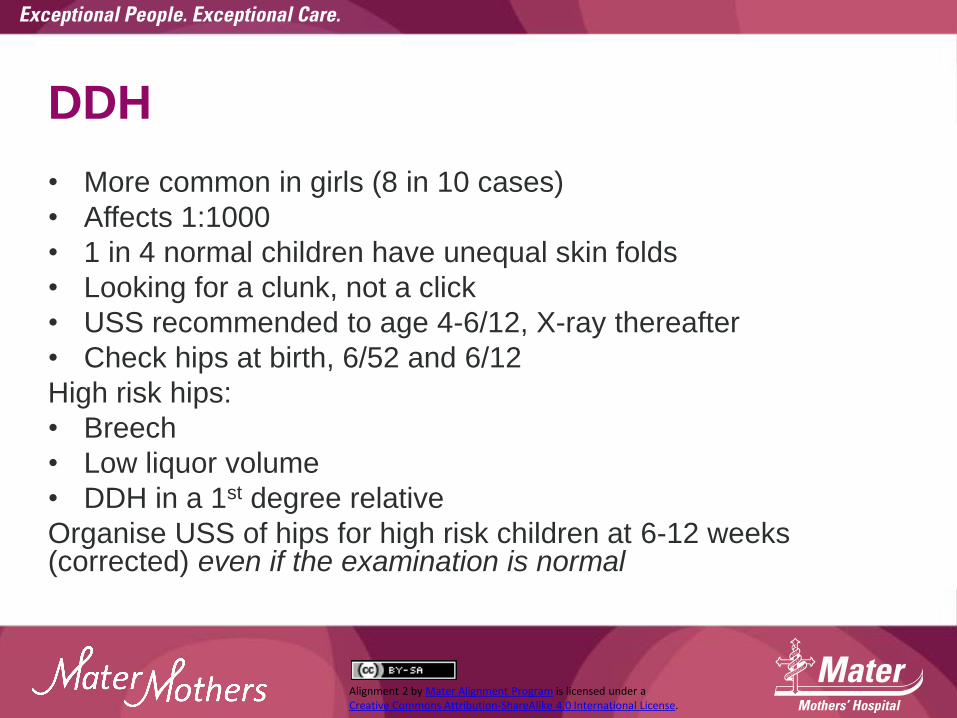
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
DDH
• More common in girls (8 in 10 cases)
• Affects 1:1000
• 1 in 4 normal children have unequal skin folds
• Looking for a clunk, not a click
• USS recommended to age 4-6/12, X-ray thereafter
• Check hips at birth, 6/52 and 6/12
High risk hips:
• Breech
• Low liquor volume
• DDH in a 1st degree relative
Organise USS of hips for high risk children at 6-12 weeks (corrected) even if the examination is normal
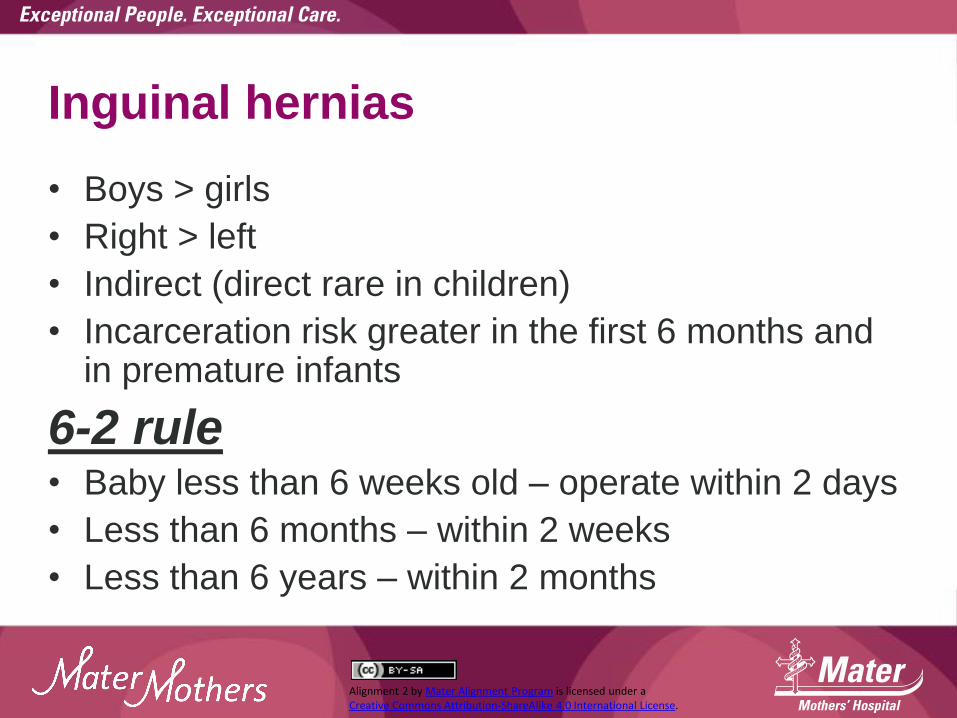
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Inguinal hernias
• Boys > girls
• Right > left
• Indirect (direct rare in children)
• Incarceration risk greater in the first 6 months and in premature infants
6-2 rule • Baby less than 6 weeks old – operate within 2 days
• Less than 6 months – within 2 weeks
• Less than 6 years – within 2 months

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Umbilical hernias
• More pronounced with crying
• Easily reducible
• Usually close in the first 3 years
• Consider surgery if still present as school
commences

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Yellow group Neonatal care
• Caden presents for his 6 week check up and he is going well and growing well. His physical examination is unremarkable except for retractile testes. The RHS milks down well, but the LHS is more difficult to locate.
• What do you advise?
• What is the current management of undescended testes?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
The scrotum...
• Undescended testes – present in 3% of neonates, ¾
will resolve spontaneously by 3-6 months. If still
present at > 6 months, surgery will be required.
Optimal age for surgery ~ 12 months
• Retractile testes usually do not require an operation—
follow up until the position of the testis is certain
• Hydroceles transilluminate, don‘t empty, you can feel
the spermatic cord above and they usually resolve on
their own. If not resolved by 15-18 months, they are
unlikely to do so and surgery may be required

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
So do paediatric surgeons...
Request/require ultrasound scans for
• Hernias?
Maybe, but don‘t delay a referral in a neonate
• Undescended testes?
No! An experienced paediatric surgeon has a
much better pick up rate than USS.
• Hydroceles?
No!

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Orange group Neonatal care
• Rosie presents for her 5-10 day check on day 9. She is a settled child, which is a welcome relief for her parents who had a fussy first child, Adam, who is now 5 years old. Her birth length was 53 cm, weight 3810 and HC 35 cm. Your examination reveals a drowsy, jaundiced, otherwise normal full term infant whose length is 51.4 cm (despite repeated efforts to replicate the birth length!), wt 3650, HC 36.2.
• What do you advise?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Neonatal Jaundice
Statewide guideline
www.health.qld.gov.au/qcg/documents/g_jaundice.pdf
If in any doubt, order a serum BR and investigate further prn. Cut off level for action >200-250

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Jaundice

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Pink group Neonatal care
• Oliver is the first child of Michelle (age 38) and Bob (age 40) and was delivered 3 weeks ago at term by LSCS for failure to progress and fetal distress. His Apgars were 7 and 9 and they were discharged on day 4. Oliver, Bob and Michelle have booked in to see you as he is a fussy child, who cries a lot.
• Where do you start and if the examination is normal, what do you advise?

The unsettled baby in the first 16 weeks:
what to do
With thanks and acknowledgement to Dr Pamela Douglas MBBS FRACGP PhD IBCLC The Possums Clinic www.possumsonline.com Associate Professor (Adjunct), Centre for Health Practice Innovation, Griffith University Senior Lecturer, Discipline of General Practice, The University of Queensland
306

Overview
307
1. Why is infant crying a problem? 2. Baby’s health 3. Mother’s health 4. Feeds
5. Sensation
6. Sleep

1Wolke D, Samara M, Alvarez Wolke M. Meta-analysis of fuss/cry durations and colic prevalence across countries. 2011: Presented at the 11th International Infant Cry Research Workshop, 18-10 June 2011, Netherlands
308
1

Why is crying a problem?
309
1Wake M, Morton-Allen E, Poulakis Z, Hiscock H, Gallagher S. Prevalence, stability, and outcomes of cry-fuss and sleep problems in the first 2 years of life: prospective community-based study. Pediatrics. 2006;117:836-842. 2Odom E, Scanlon K, Perrine C, Grummer-Strawn L. Reasons for earlier than desired cessation of breastfeeding. Pediatics. 2013;131:e726-732.
‘Normal’ and self-limiting but 1 in 5 families report excessive crying1
Many more start formula due to unsettled behaviour2

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Why is crying a problem?
310
↑risk of: Behavioural problems in later childhood1,2
Premature weaning3
Child abuse4
Postnatal depression5
1Schmid G, Wolke D. Preschool regulatory problems and attention-deficit/hyperactivity and cognitive deficits at school age in children born at risk: different phenotypes of dysregulation? Early Human Development. 2014;90:399-405. 2Winsper C, Wolke D. Infant and toddler crying, sleeping and feeding problems and trajectories of dysregulated behavior across childhood. Journal of Abnormal Child Psychology. 2013;2013:DOI 10.1007/s10802-10013-19813-10801.
3Howard C, Lanphear N, Lanphear B, Eberly S, Lawrence R. Parental responses to infant crying and colic: the effect on breastfeeding duration. Breastfeed Med. 2006;1(3):146-155.
4Reijneveld SA, van der Wal M, Brugman E, Hira Sing R, Verloove-Vanhorick S. Infant crying and abuse. Lancet. 2004;364:1340-1342. 5Vik T, Grote V, Escribano J, Socha J, Verduci E, Fritsch M, et al. Infantile colic, prolonged crying and maternal postnatal depression. Acta Paediatr. 2009;8:1344-1348.
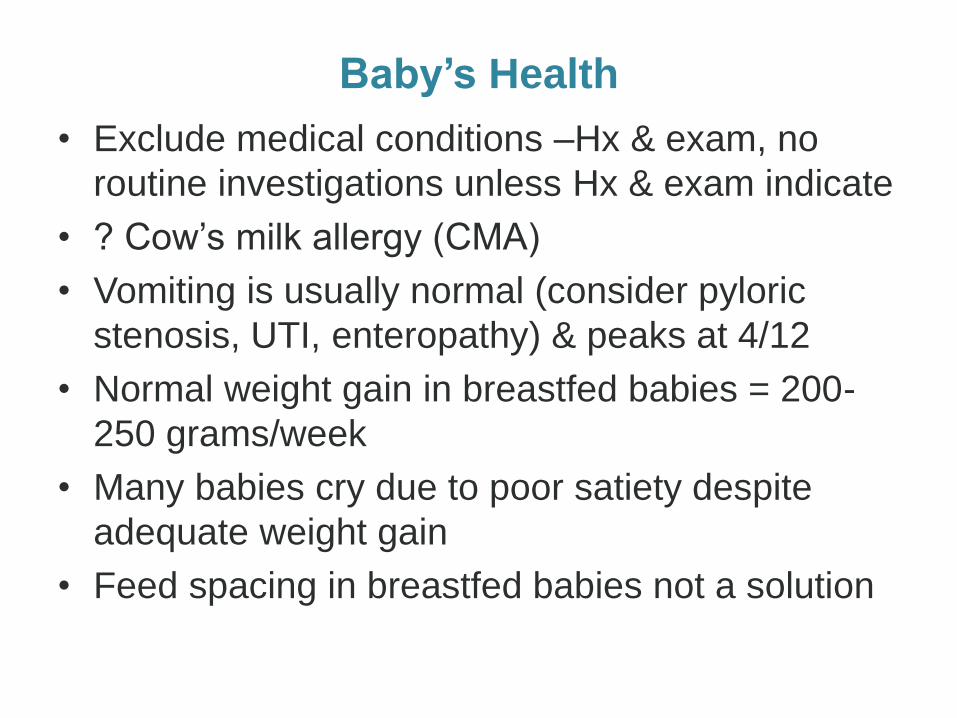
Baby’s Health
• Exclude medical conditions –Hx & exam, no
routine investigations unless Hx & exam indicate
• ? Cow‘s milk allergy (CMA)
• Vomiting is usually normal (consider pyloric
stenosis, UTI, enteropathy) & peaks at 4/12
• Normal weight gain in breastfed babies = 200-
250 grams/week
• Many babies cry due to poor satiety despite
adequate weight gain
• Feed spacing in breastfed babies not a solution

Baby’s health: GORD?
312
Proton pump inhibitors No better than placebo1
Increase risk of infection2
Predispose to food allergies3,4
1van der Pol R, Smits MJ, van Wijt MP, Omaria TI, Tabbers MM, Beninga MA. Efficacy of proton-pump inhibitors in children with gastroesophageal reflux disease: a systematic review. Pediatrics. 2011;127:925-935. 2Orenstein S, Hassall E, Furmaga-Jablonksa W, Atkinson S, Raanan M. Multicenter, double-blind, randomized, placebo-controlled trial assessing the efficacy and safety of proton pump inhibitor lansoprazole in infants with symptoms of gastroesophageal reflux disease. Journal of Pedatrics. 2009;154:514-520. 3Trikha A, Baillargeon J, Kuo Y, Tan A, Pierson K, Sharma G, et al. Development of food allergies in patients with gastroesophageal reflux disease treated with gastric acid suppressive medications. Pediatric Allergy and Immunology. 2013;24:582-588. 4Merwat SN, Spechler SJ. Might the use of acid-suppressive medications predispose to the development of eosinophilic esophagitis? Am J Gastroenterol. 2009;104:1897-1902.

Baby’s health: Allergy?
313
Signs of CMA Constipation Blood in stool Skin rashes – urticarial, eczema
CMA may cause oesophagitis (GORD) but takes time to develop (older infants and children)
CMA is the only allergy linked with cry-fuss problems in first 16 weeks
Bergmann MM, Caubet J-C, McLin V, Belli D, Schappi M, Eigenmann P. Common colic, gastroesophageal reflux and constipation in infants under 6 months do not necessitate an allergy work-up. Pediatric Allergy and Immunology. 2014:doi: 10.1111/pai.12199. Muraro A, Halken S, Arshad SH, Beyer K, Dubois AEJ, Du Toit G, et al. EEACI Food allergy and anaphylaxis guidelines. Primary prevention of food allergy. Allergy 2014;69:590-601.

Baby’s health: Allergy?
314
After all other domains addressed: Breastfed babies may benefit from trial of 2
week maternal elimination diet Formula-fed fussy babies improve with
extensively hydrolysed formula1
1Allen KJ, Davidson GP, Day AS, Hill DJ, Kemp As, Peake JE, et al. Management of cow's milk protein allergy in infants and young children: an expert panel perspective. J Paediatr Child Health. 2009;45:481-486.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Baby’s health: Other treatments?
315
No benefit from Homeopathic medicines1,2
Acute respiratory problems Acupuncture3
‘Infacol’ (simethicone)4
Herbal preparations5
1Aviner S, Berkovitch M, H D. Use of a homeopathic preparation for 'infantile colic' and an apparent life-threatening event. Pediatrics. 2010;125:318-323. 2Glatstein M. Choking caused by a homeopathic drug in a previously healthy infant. Canadian Family Physician. 2013;59:848-850. 3Landgren K, Kvorning N, Hallstrom I. Feeding, stooling and sleeping patterns in infants with colic - a randomized controlled trial of minimal acupuncture. BMC Complementary and Alternative Medicine. 2011;11:93. 4Hall B, Chesters J, Robinson A. Infantile colic: a systematic review of medical and conventional therapies. Journal of Paediatrics and Child Health. 2012;48:128-137. 5Perry R, Hunt K, Ernst E. Nutritional supplements and other complementary medicines for infantile colic: a systematic review. Pediatrics. 2011;127:720-733.

Mother’s health
316
Cued care Screen for postnatal depression Healthy biopsychosocial rhythms

Mother’s health
317
Exclude medical conditions (e.g. anaemia, hypothyroidism)
Screen with Edinburgh Postnatal Depression Scale
Daylight Physical activity Focus on meeting own needs out of the house during day
Cued care Screen for postnatal depression Healthy biopsychosocial rhythms

Feeds
318
Identify and manage feeding problems No feed spacing

Feeds Functional lactose overload1,2
319
Not enough cream causes: Frothy poo Tight tummy Copious belches and
flatus Very frequent waking Excessive feeding
1Smillie CM, Campbell SH, Iwinski S. Hyperlactation: how 'left brained' rules for breastfeeding can wreak havoc with a natural process. Newborn and Infant Nursing Reviews. 2005;5:49-58. 2Evans K, Evans R, Simmer K. Effect of the method of breastfeeding on breast engorgement, mastitis and infantile colic. Acta Paediatr. 1995;84(8):849-852.
Feeds Poor satiety
320
If breastfeeding impaired milk transfer not enough cream insufficient milk supply If bottle-feeding impaired milk transfer not enough cream (breastmilk) Breast and formula feeding feed spacing

Feeds Poor satiety
321
Positional instability1,2 causes: Poor satiety
Cry-fuss behaviours Very frequent waking Excessive feeding
Back arching Feeding refusal
1Smillie CM. How infants learn to feed: a neurobehavioral model. In: Watson CG, editor. Supporting sucking skills. New York: Jones and Bartlett Learning; 2012. p. 83-104. 2Colson SD, Meek JH, Hawdon JM. Optimal positions for the release of primitive neonatal reflexes stimulating breastfeeding. Early Hum Dev. 2008;84:441-449.

Sensory
322
Healthy caregiver biopsychosocial rhythms Physical contact 10 hrs/day (awake or asleep)
With permission “Mummy and me yoga”, www.yogababy.com.au

Sensory A healthy sensory diet
323
Babies need a rich and healthy sensory diet
Sight Taste Touch Hearing Smell Vestibular Proprioceptive Acquired through Caregiver pursuing enjoyable social activities outside the house Outdoor activities e.g. walking Physical contact Sibling activity
Babies often cry because they hunger for change in sensory environment (often misinterpreted as ‘tired cue’)

Sensory Other approaches?
324
Pacifiers don’t interfere with breastfeeding duration1
The following do not make infants more settled: Massage2
Manipulative therapies (including craniosacral therapies)3,4
Wrapping5
↑hip dysplasia Poorer weight gains6
Jaafar SH, Jahanfar S, Angolkar M, Ho JJ. Pacifier use versus no pacifier use in breastfeeding term infants for increasing duration of breastfeeding. Cochrane Database Syst Rev. 2011:Issue 3. Art. No.: CD007202. DOI: 007210.001002/14651858.CD14007202.pub14651852. 2Bennett C, Underdown A, Barlow J. Massage for promoting mental and physical health in typically developing infants under the age of six months. Cochrane Database of Systematic Reviews. 2013;4:CD005038. doi: 005010.001002/14651858.CD14005038.pub14651853. 3Ernst E. Chiropractic spinal manipulation for infant colic: a systematic review of randomised clinical trials. The International Journal of Clinical Practice. 2009;63:1351 - 1353. 4Posadzki P, Ernst E. Is spinal manipulation effective for paediatric conditions? An overview of systematic reviews. Focus on Alternative and Complementary Therapies. 2012;17:22-26. 5Clarke N. Swaddling and hip dysplasia: an orthopaedic perspective. Archives of Disease in Childhood. 2014;99:5-6. 6Bystrova K, Matthiesen AS, Wistrom AM, Ransjo-Arvidson A, Welles-Nystrom B, Vorontsov I, et al. The effect of Russian Maternity Home routines on breastfeeding and neonatal weight loss with special reference to swaddling. Early Human Development. 2007;83:29-39.

1Wolke D, Samara M, Alvarez Wolke M. Meta-analysis of fuss/cry durations and colic prevalence across countries. 2011: Presented at the 11th International Infant Cry Research Workshop, 18-10 June 2011, Netherlands
325
1
Sleep
326

1 1
vulnerable maternal personality
increased risk of postnatal depression
327

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Sleep
328
Postnatal depression correlates with poor maternal sleep
efficiency, not number of times of waking in the night.1,2
1Dorheim SK, Bondevik GT, Eberhard-Gran M, Bjorvatn B. Sleep and Depression in Postpartum Women: A Population-Based Study. Sleep. 2009;32:847-855. 2Goyal D, Gay CL, Lee K. Fragmented maternal sleep is more strongly correlated with depressive symptoms than infant temperament at three months postpartum. Arch Womens Ment Health. 2009;12:229-237.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Sleep
329
Marathon feeds and excessive night-waking signal a feeding
problem

Sleep needs are highly variable between babies, and in any one baby
from day to day
330
Galland BC, Taylor BJ, Elder DE, Herbison P. Normal sleep patterns in infants and children: a systematic review of observational studies. Sleep Medicine Reviews. 2012;16:213-222.

Sleep Safe sleep
331
Supine Safest place to sleep baby day and
night is in same room as caregiver Paradox: Putting baby to sleep in separate room
(<6/12) puts baby at increased risk of SIDS
Bed-sharing does not appear to increase risk if done safely1
1Bergman AB. Bed sharing per se is not dangerous. JAMA Pediatrics. 2013;167:998-999.

Resources For parents
332
Community resources The Possums Clinic www.possumsonline.com includes Song and Sensory Programs Group Sessions
Community Child Health Services Australian Breastfeeding Association Helpline PANDA 1300 726 306 Web-based SIDS and Kids www.isisonline.org.uk http://www.mothersmatter.co.nz/ www.beyondblue.com.au www.bottlebabies.org Books The Discontented Little Baby Book Dr Pamela Douglas Becoming Mum Dr Koa Whittingham

Douglas PS, Whittingham K. Response to 'Sleeping like a baby? Infant sleep impact on care givers and current controversies'. Journal of Paediatrics and Child Health. 2015;51:234. Whittingham K, Douglas P. Optimising parent-infant sleep in the first 6 months: a new paradigm. Infant Mental Health Journal. 2014;35:614-623. Douglas P. Diagnosing gastro-oesophageal reflux disease or lactose intolerance in babies who cry alot in the first few months overlooks feeding problems. J Paediatr Child Health. 2013;49:e252-256. Douglas P, Hill PS. Behavioural sleep interventions in the first six months of life do not improve outcomes for mothers or infants: a systematic review. J Dev Behav Pediatr. 2013;34:497–507. Douglas P, Shirley B. How to Treat: The Crying Baby. Australian Doctor. 2013; 24 May 31-38. Douglas PS, Hill PS. A neurobiological model for cry-fuss problems in the first three to four months of life. Med Hypotheses. 2013;81:816-822.. Douglas PS. Re-thinking 'posterior' tongue-tie. Breastfeed Med. 2013;8(6):1-4. Douglas P, Miller Y, Bucetti A, Hill PS, Creedy D. Preliminary evaluation of a primary care intervention for cry-fuss behaviours in the first three to four months of life ("The Possums Approach"): effects on cry-fuss behaviours and maternal mood. Australian Journal of Primary Health. 2013; 18:332-338. Douglas P, Mares R, Hill P. Interdisciplinary perspectives on the management of the unsettled baby: key strategies for improved outcomes. Australian Journal of Primary Health. 2012;18:332-338. Douglas PS, Hill PS. The crying baby: what approach? Curr Opin Pediatr. 2011;23:523-529. Douglas P, Hill P. Managing infants who cry excessively in the first few months of life. BMJ. 2011;343:d7772. Douglas P. The rise and fall of infant reflux. Griffith Review. 2011;32:241-254. Douglas PS, Hill PS, Brodribb W. The unsettled baby: how complexity science helps. Arch Dis Child. 2011;96:793-797. Douglas P, Hiscock H. The unsettled baby: crying out for an integrated, multidisciplinary, primary care intervention. Med J Aust. 2010;193:533-536. Douglas PS. Excessive crying and gastro-oesophageal reflux disease in infants: misalignment of biology and culture. Med Hypotheses. 2005;64:887-898.
333

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.possumsonline.com

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.childrens.health.qld.gov.au/community-health/child-health-service/

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Common neonatal presentations
Time Task Who
3:15 Updates Dr Wendy Burton
3.30 pm Breastfeeding Kathleen Goldsmith, LC
4:00 Neonatal cases All
4:10 Neonatal examination Dr David Cartwright
Dr Andrea McGlade
4:40 Common neonatal presentations Dr Andrea McGlade
4:55-5.00pm Conclusion All
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Common neonatal presentations
• Tongue tie
• Skin rashes
• Nappy rash
• Plagiocephaly
• The circumcision question

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Tongue Tie

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Tongue Tie : Definition
• congenital anomaly where short, lingual frenulum or a
highly attached genioglossus muscle restricts tongue
movement
• definition not standardised, so wide variation of opinion
regarding clinical significance and optimal management
(eg. snip vs. observe)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Tongue Tie : Clinical Features
• Inability to lift the tongue
to the upper dental alveolus
• Inability to protrude tongue
• >1-2 mm past the lower central
incisors
• Impaired side-to-side movement

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Tongue Tie : Potential Sequelae
• Difficulty breastfeeding (poor latch, maternal nipple pain)
• Speech articulation difficulty (NOT speech and language
delay)
• Mechanical problems (inability to lick the lips or sweep
food debris from the teeth)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Tongue Tie: Indications for Surgery
• Breastfeeding difficulty
• Articulation problems
• Psychological problems
• Periodontal disease

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Tongue Tie : Surgery
• Given lack of consensus about surgery, decision should
be made on a case-by-case basis with involvement of the
parents
• Frenotomy should be performed by appropriately trained
personnel

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Neonatal Skin Rashes

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What is this rash?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Erythema Toxicum Neonatorum
• harmless neonatal skin condition
• erythematous base with a central tiny yellow papule, seen anywhere - except the palms and soles
• lesions are packed with eosinophils, and there may be accompanying eosinophilia in the blood count.
• cause unknown, no treatment is required
• usually disappears after 1-2 weeks, but can come and go until 3 months of age

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What is this rash?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Milaria
• prickly heat, sweat rash
• many red macules with central papules, vesicles or
pustules
• may be on the trunk, nappy area, head or neck

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What is this rash?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Milia
• epidermal inclusion cysts
• pearly, yellow 1-3mm diameter papules on face, chin, and
forehead
• 50% newborns
• usually resolve in first month without treatment, but may
persist for several months

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What is this rash?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Seborrhoeic Dermatitis
• mild baby oils (eg. Aveeno, Hamilton‘s bath oil),
then moisturise (sorbolene)
• brush cradle cap softly to remove scales
• if fails to improve, can try steroid ointments

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What are these?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Capillary malformations • Common (40% newborns)
• Small flat patches pink or red, poorly defined borders
• Nape of neck (stork mark), forehead ( angel kiss),
eyelids and scrotum
• Worse with crying
• Not associated with extracutaneous findings

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What is this rash?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Infantile Eczema
• infants often have widely distributed eczema,
cheeks often first affected
• skin is often dry, scaly, with small scratch
marks made by sharp baby nails
• nappy area is often spared due to moisture
retention of nappies (but they can still get
nappy rash)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Eczema Distribution by age

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What is this rash?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Irritant Nappy Dermatitis
• Rash confined to convex surfaces of the
buttocks, perineal area, lower abdomen, and
proximal thighs, sparing the intertrigous creases
• Caused by combination of factors, irritation to
the skin by urine, faeces, excessive heat, and
occlusion
• Beware secondary Staph or Candida infection

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Irritant Nappy Dermatitis :
Prevention and Treatment • Nappy off!!!
• Change nappy frequently
• Wash bottom at each change
• Use emollient (aqueous cream) and barrier cream (zinc oxide, eg. Sudo-cream)
• Low potency topical steroid (hydrocortisone) in more significant cases

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What is this rash?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Candidal Dermatitis
• starts off in deep flexures with widespread
erythema on the buttocks (beefy red color)
• also raised edge, sharp marginisation and white
scale at the border lesions, with pinpoint pustulo-
vesicular satellite lesions
• treat antifungal, can add low potency steroid for a
few days

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
What are these?

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Infantile Haemangioma • Most common benign tumours of infancy
• Begin as barely visible telangieactasia or red macules and grow
into 0.5-4cm bright red partially compressible tumours
• 60% occur on head and neck area
- if neck area, consider intra-tracheal lesions
- if multiple, consider systemic lesions (eg. Liver haemangioma)
• Most spontaneously resolve by age 5 years; if aggressive growth
or significant size, may consider treatment with propanolol (vs.
intralesional steroids or laser)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Common neonatal discussions

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Plagiocephaly

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Plagiocephaly
• Deformational plagiocephaly is a non -surgical problem most often related to a supine sleeping position
• Conservative measures to prevent ongoing pressure to the affected area is main premise of treatment
- physiotherapist often very useful
- encourage ― tummy‖ time when awake
- alternate direction head is facing when laid to sleep
• Occasionally helmet is required (before 8 months); GB Orthopaedics, and Brisbane Prosthetics and Orthotics

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Plagiocephaly Helmets

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Plagiocephaly helmets
Helmet therapy in infants with positional skull deformation: randomised controlled trial
BMJ 2014; 348 doi: http://dx.doi.org/10.1136/bmj.g2741 (Published 1 May 2014)
http://www.bmj.com/content/348/bmj.g2741
"Positional" or "deformational" plagiocephaly or brachycephaly are the result of head moulding when a foetus or infant lies in a persisting head posture. It has become much very more prevalent since the recommendation that babies should not be placed in the prone position for sleeping to help avoid SIDS. Such positional moulding of the head can produce quite dramatic flattening in the occipital region associated with misalignment of the ears and other compensatory skull changes. Parents are commonly very concerned about these perceived abnormalities.
The study was an RCT of 84 infants with moderate to severe skull deformation. They excluded those with syndromic causes, craniosynostosis and muscular Torticollis.
In short the study showed no benefit from the use of helmets.

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Pathological Plagiocephaly
• Occasionally related to torticollis, refer to
physio in first instance orthopaedic
surgeon
• If concerned re craniosynostosis, get a
plain skull X-Rays and refer to plastic
surgeon or neurosurgeon

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Circumcision
• Undertaken for religious and cultural reasons for
many thousands of years
• Based on current available evidence, RACP do
not recommend routine infant circumcision in
Australia and New Zealand

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
To Circumcise or not to Circumcise
Potential benefits
• Connectedness for particular socio-cultural groups
• Decreased risk of some diseases
Potential harms
• Contravention of individual rights
• Loss of choice
• Loss of function
• Procedural/psychological complications

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Contraindications to circumcision
• Hypospadius and other congenital anomalies of penis
• Chordee(ventral angulation penis)
• Buried penis
• Sick and unstable infants
• Personal/family history bleeding disorder
• Inadequate expertise/facilities

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Circumcision Complications
• 1-4%
• Haemorrhage
• Fistula formation
• Infection
• Penile amputation
• Meatal stenosis
• Secondary phimosis or chordee
• Poor cosmetic appearance

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Role of circumcision in preventing
disease • UTI: circumcision provides some benefit in preventing UTI
in boys, particularly in those with underlying anomalies of
the urogenital tract
• STI/HIV: in low prevalence populations such as Australia
and NZ circumcision does not provide significant
protection against STI‘s and HIV, and is less effective than
safe sex practices
• HPV: may reduce risk, but more benefit from HPV vaccine
• Penile cancer: decreases risk (but rare to begin with)
• Doesn‘t decrease prostate cancer

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
A few extras….
Labial fusion
• Usually presents between 3-6 months of age
• Irritation + low oestrogen levels thought to be the
cause
• Typically resolves spontaneously once out of
nappies
• Consider oestrogen cream if still present as
puberty approaches or if urination is affected or
UTIs occurring

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Flat feet
• When the arch on the inner border of the foot is
not as high
• Normal development in 97% of children
• Insoles or arch supports do not make a
difference
• Walking barefoot before the age of 6 years helps
develop normal foot arches as the feet mature Thanks to Dr Haseena Mohamed for this and the following 2 slides

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
In-toeing
• Due to internal rotation of the
femur at the hip joint
• Occurs in 1 in 6 children
• Usually corrects in children
under 8 years old
• Prevent children from sitting
in the W-position

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Knock knees
• All children have bow legs until the age
of 2 years
• After this they become knock kneed between 3-4
years
• Legs slowly straighten to adult shape by 10-12
years
• Important to exclude rickets due to vitamin D
deficiency as a cause
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
http://metrosouth.health.qld.gov.au/oral-health
Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
http://metrosouth.
health.qld.gov.au/
dental-health
-children


Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
www.childrens.health.qld.gov.au


Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
LCCH
• Children should be referred to their local service
where available and appropriate
• New referral templates, to replace the MCH and
RCH templates, are available to download from
www.childrens.health.qld.gov.au/referapatient/
• Further information about the services available
at LCCH is also available on this website

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Please be aware of PEDS
• As of July 1, 2015, new Red Books (the paediatric
personal health record) incorporate a parents‘
evaluation of developmental status (PEDS) into the
questions at 6, 12, 18 months, 2 ½ and 4 years
• Parents who raise concerns should be directed into
appropriate follow up services e.g. use
www.raisingchildren.net.au to check the child‘s
developmental status against milestones or use the
Red Flags tool and refer publically or privately prn

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
PEDS
• BSPHN is partnering with local childcare centers
in the roll out of PEDS = Parents‘ Evaluation of
Developmental Status to try and identify early if
a child has a developmental delay
• Watch the newsletter for upcoming events which
will inform you about this evidence based tool
and how to interpret the information it provides
• BSPHN is also hosting Paediatric Pathways on
June 4, 2016 at LCCH

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
In conclusion….
The Mater Mothers Alignment program has
created a significant number of resources which
are available online for all to use and to share
We have worked with our colleagues in other
hospitals and in general practice to create affiliated
programs at Beaudesert, Logan, Redland, RBWH,
Redcliffe/Caboolture, Nambour, Ipswich and
Emerald Hospitals
Please use and share these resources

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Available now….
• Online options to realign
• Bridging option for GPs who complete an
Alignment event at an affiliated hospital
• VOPP of some of the presentations
• Video clips with Dr Treasure McGuire,
pharmacologist


Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
GPs referring to MSHHS? Online resources including power points with
information on local referral pathways are hosted
at www.bsphn.org.au/education-events/
maternal-shared-care/

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
GPs referring to MNHHS? Contact information for the MNHHS Alignment:
Brigid Wheaton Program Coordinator Metro North
Maternity GP Alignment Program
Phone: (07) 3646 4421
Email: [email protected]
Online resources are currently being hosted at
http://www.brisbanenorthphn.org.au/page/news-and-
events/metro-north-maternity-gp-alignment-program-
resources/

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Contact details
Maternity Share Care issues?
• GP Liaison Midwife Phone: 3163 1861
• E-mail: [email protected]
• Mobile: 0466 205 710
•If you are uncertain about the best approach to
take in caring for or referring a woman, or if she
requires urgent review, phone the on call consultant
(3163 6009), registrar (3163 6611) or the GPLM

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Contact details
Alignment status, contact details & evaluation enquiries?
Sarah Renals
Phone 3163 1967
Email [email protected]
Training & RACGP enquiries?
Mater Marketing
Phone: 07 3163 1524
Email: [email protected]

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Item numbers for MSC
16500 Rebate $40.10 ($47.15) Antenatal Attendance
16591 Rebate $121.30 ($142.65) “Planning and management of a pregnancy that has progressed beyond 20 weeks provided the fee does not include any amount for the management of the labour and delivery if the care of the patient will be transferred to another medical practitioner, payable once only for any pregnancy that has progressed beyond 20 weeks, not being a service to which item 16590 applies” (16590 = planning to undertake the delivery for a privately admitted patient)

Alignment 2 by Mater Alignment Program is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Don’t forget…
• To complete your feedback document
• To complete your questionnaire – the pass mark
is 80% and yes, you can mail it in
• To get your pass for the car park!
• Do expect up to 8 weeks for processing of the
paperwork

Happy 5th Birthday, MMH Alignment!




















