
Masitinib (AB1010), from canine tumor model to human clinical development: Where we are?
14
Please cite this article in press as: Marech I, et al. Masitinib (AB1010), from canine tumor model to human clinical development: Where we are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.critrevonc.2013.12.011 ARTICLE IN PRESS ONCH-1825; No. of Pages 14 Critical Reviews in Oncology/Hematology xxx (2014) xxx–xxx Masitinib (AB1010), from canine tumor model to human clinical development: Where we are? Ilaria Marech a , Rosa Patruno b , Nicola Zizzo c , Claudia Gadaleta c , Marcello Introna c , Alfredo Francesco Zito d , Cosmo Damiano Gadaleta a , Girolamo Ranieri a,∗ a Interventional Radiology Unit with Integrated Section of Translational Medical Oncology, National Cancer Research Centre “Giovanni Paolo II”, Bari, Italy b Department of Prevention and Animal Health, ASL BAT, Barletta, Bari, Italy c Chair of Pathology, Veterinary Medical School, University of Bari, Valenzano, Bari, Italy d Pathology Unit, ASL BA, Bari, Italy Accepted 9 December 2013 Contents 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 2. Structure–activity. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 3. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 4. Targeting c-Kit receptor tyrosine kinase . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 5. Escape/resistance mechanisms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 6. Preclinical studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 7. Masitinib approval in canine mast cell tumors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 8. Human clinical trials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 9. Toxicity in human clinical trials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 10. Ongoing human clinical trials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 11. Concluding remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 Conflict of interest statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 Reviewers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 Biographies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 Abstract Masitinib mesylate (AB1010) is a novel potent and selective tyrosine kinase inhibitor, targeting mainly wild-type and mutated c-Kit receptor (c-KitR), Platelet Derived Growth Factor Receptor-alfa/beta (PDGFR/), Lymphocyte-specific kinase (Lck), Lck/Yes-related protein (LYn), Fibroblast Growth Factor Receptor 3 (FGFR3) and Focal Adhesion Kinase (FAK). It is the first anticancer therapy approved in veterinary medicine for the treatment of unresectable canine mast cell tumors (CMCTs), harboring activating c-KitR mutations, at dose of 12.5 mg/kg once daily. Considering its anti-proliferative action, principally given by inhibiting the MCs c-KitR anti-angiogenic pathway that leads cancer progression, and its role as chemosensitizer, masitinib is under clinical investigation in several human malignancies (Gastro-Intestinal Stromal Tumors, acute myeloid leukemia, systemic mastocytosis, pancreatic cancer, multiple myeloma, non-small cell lung cancer, melanoma, ovarian and prostate cancer), which are characterized by similar canine c-KIT proto-oncogene mutations. Here, we analyze masitinib structure activity, ∗ Corresponding author at: Interventional Radiology Unit with Integrated Section of Translational Medical Oncology, National Cancer Research Centre “Giovanni Paolo II” of Bari, Via Orazio Flacco 65, 70100 Bari, Italy. Tel.: +39 080 5555561; fax: +39 080 5555563. E-mail addresses: [email protected], [email protected] (G. Ranieri). 1040-8428/$ – see front matter © 2013 Elsevier Ireland Ltd. All rights reserved. http://dx.doi.org/10.1016/j.critrevonc.2013.12.011
Transcript of Masitinib (AB1010), from canine tumor model to human clinical development: Where we are?
O
a
C
12345678911
A
(FmopTa
“
1h
ARTICLE IN PRESSNCH-1825; No. of Pages 14
Critical Reviews in Oncology/Hematology xxx (2014) xxx–xxx
Masitinib (AB1010), from canine tumor model to human clinicaldevelopment: Where we are?
Ilaria Marech a, Rosa Patruno b, Nicola Zizzo c, Claudia Gadaleta c, Marcello Introna c,Alfredo Francesco Zito d, Cosmo Damiano Gadaleta a, Girolamo Ranieri a,∗
Interventional Radiology Unit with Integrated Section of Translational Medical Oncology, National Cancer Research Centre “Giovanni Paolo II”, Bari, Italyb Department of Prevention and Animal Health, ASL BAT, Barletta, Bari, Italy
c Chair of Pathology, Veterinary Medical School, University of Bari, Valenzano, Bari, Italyd Pathology Unit, ASL BA, Bari, Italy
Accepted 9 December 2013
ontents
. Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
. Structure–activity. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
. Targeting c-Kit receptor tyrosine kinase . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
. Escape/resistance mechanisms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
. Preclinical studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
. Masitinib approval in canine mast cell tumors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
. Human clinical trials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
. Toxicity in human clinical trials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000. Ongoing human clinical trials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 001. Concluding remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
Conflict of interest statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Reviewers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Biographies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
bstract
Please cite this article in press as: Marech I, et al. Masitinib (AB1010), from canine tumor model to human clinical development: Wherewe are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.critrevonc.2013.12.011
Masitinib mesylate (AB1010) is a novel potent and selective tyrosine kinase inhibitor, targeting mainly wild-type and mutated c-Kit receptorc-KitR), Platelet Derived Growth Factor Receptor-alfa/beta (PDGFR�/�), Lymphocyte-specific kinase (Lck), Lck/Yes-related protein (LYn),ibroblast Growth Factor Receptor 3 (FGFR3) and Focal Adhesion Kinase (FAK). It is the first anticancer therapy approved in veterinaryedicine for the treatment of unresectable canine mast cell tumors (CMCTs), harboring activating c-KitR mutations, at dose of 12.5 mg/kg
nce daily. Considering its anti-proliferative action, principally given by inhibiting the MCs c-KitR anti-angiogenic pathway that leads cancerrogression, and its role as chemosensitizer, masitinib is under clinical investigation in several human malignancies (Gastro-Intestinal Stromalumors, acute myeloid leukemia, systemic mastocytosis, pancreatic cancer, multiple myeloma, non-small cell lung cancer, melanoma, ovariannd prostate cancer), which are characterized by similar canine c-KIT proto-oncogene mutations. Here, we analyze masitinib structure activity,
∗ Corresponding author at: Interventional Radiology Unit with Integrated Section of Translational Medical Oncology, National Cancer Research CentreGiovanni Paolo II” of Bari, Via Orazio Flacco 65, 70100 Bari, Italy. Tel.: +39 080 5555561; fax: +39 080 5555563.
E-mail addresses: [email protected], [email protected] (G. Ranieri).
040-8428/$ – see front matter © 2013 Elsevier Ireland Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.critrevonc.2013.12.011

O
2
intor©
K
1
aihid[
s(wmDwtp((ooti2m(v[
aofdaraaC(nKoeTm
ARTICLE IN PRESSNCH-1825; No. of Pages 14
I. Marech et al. / Critical Reviews in Oncology/Hematology xxx (2014) xxx–xxx
ts pharmacokinetics compared to imatinib, the c-KitR pathway referring to the most frequent c-KIT mutations sensitive or resistant to thisovel drug compared to imatinib, and masitinib safety profile. We, also, explore preclinical and clinical (completed and ongoing) trials withhe aim to emphasize as this recent anti-angiogenic therapy, at first approved in CMCTs and, currently in development for the treatmentf several human neoplasms, could be represent a milestone in translational oncology, in which the murine experimental model of canceresearch could be integrated by canine spontaneous tumor model.
2013 Elsevier Ireland Ltd. All rights reserved.
ro-Intes
tbp[isDt
mt5waitCcu
toStn((alti[
pcsogaOm
eywords: Canine tumor model; c-Kit receptor; Dog mast cell tumors; Gast
. Introduction
The knowledge of biochemical cellular dysfunctionsdvanced the discovery of targeted therapy, such as masitinib,n several fields of research both in veterinarian anduman medicine, from inflammatory (rheumatoid arthritis,nflammatory bowel disease, asthma, atopic dermatitis) oregenerative-chronic disease (Alzheimer’s disease) to cancer1–5].
Masitinib mesylate (AB1010) is an oral novel, potent andelective phenylaminothiazole-type tyrosine kinase inhibitorTKI) targeting mainly c-Kit receptor (c-KitR). It inhibits theild-type (WT) c-KitR form, as its constitutively activatedutated form (in the juxtamembrane region), the Plateleterived Growth Factor Receptor-alfa/beta (PDGFR�/�),eakly the Fibroblast Growth Factor Receptor 3 (FGFR3),
he Lymphocyte-specific kinase (Lck), the Lck/Yes-relatedrotein (LYn), and, weakly, the Focal Adhesion KinaseFAK), also. The latter three TKs belong to the SarcomaSrc) family proteins [6]. Although masitinib has previ-usly been assessed to enhance the anti-proliferative effectsf gemcitabine in human pancreatic cancer [7] showingo be a potential strong chemosensitizer, however, surpris-ngly, at first it was approved (Masivet®) on 17 November008 by EMA (European Medicine Agency) in veterinaryedicine for treatment of recurrent or unresectable grade
G) 2/3 canine mast cell tumors (CMCTs), that harbor acti-ating c-KitR mutations, at dose of 12.5 mg/kg once daily8].
CMCT is the most frequent cutaneous tumor in the dog,ccounting for 7–21% of all canine skin tumors [9]. Basedn grading, CMCT is classified in three subgroups: well dif-erentiated (G1) which is a benign disease, intermediatelyifferentiated (G2), which is a malignant borderline tumornd finally poorly differentiated (G3), corresponding to aeally malignant disease [10]. For G2/G3 CMCTs the over-ll response rate (RR) to conventional chemotherapy is onlybout 47% [11]. Thus, in recurrent or unresectable G2/G3MCTs the results given by the common therapeutic options
such as chemotherapy and radiation therapy) utilized wereot satisfactory. Several canine studies showed that the c-itR mutated form is expressed in 20–30% of all CMCTs;n the other hand it is known that c-KitR mutated form is
Please cite this article in press as: Marech I, et al. Masitinib (AB1010),
we are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.crit
xpressed in almost 60% of high grade CMCTs [12,13].herefore, these data led to masitinib development from aedicinal chemistry point of view to clinical investigation.
spm
tinal Stromal Tumors; Masitinib; Pancreatic cancer; Systemic mastocytosis
C-KitR, a type III transmembrane tyrosine kinase pro-ein encoded by c-KIT proto-oncogene, is normally activatedy the stem cell factor (SCF), leading to mast cells (MCs)roliferation and degranulation [14,15]. C-KitR mutations16], mainly, induce a constitutive activation of c-KitR, lead-ng to MCs secretion of numerous pro-angiogenic factors,uch as Vascular Endothelial Growth Factor (VEGF), Plateleterived Growth Factor (PDGF), and Fibroblast Growth Fac-
or (FGF) stored in their secretory granules [17,18].In CMCTs it has been demonstrated that the most frequent
utations activating c-KitR are mainly localized in the jux-amembrane (JM) region of receptor (though mutations of theth immunoglobulin-like portion of the extracellular domainere not rare) causing TK activation [19]. These mutations
ctivate constitutively the c-KitR, conferring it a key rolen CMCTs pathogenesis. Moreover, these activating muta-ions of c-KitR are associated with higher histologic grade ofMCTs and poor prognosis [13]. In particular, tandem dupli-ations in the c-KitR JM subunit have been individuated inp to 12% of all CMCTs and in 40% of G3 CMCTs [12,13].
CMCTs have a higher incidence than human MCTshat interestingly show similar activating c-KitR mutationsbserved in several dogs and in human Gastro-Intestinaltromal Tumor (GIST) [5,20]. Although the mutations or
he alterations of c-KitR are found in other human malig-ancies such as acute myeloid leukemia, multiple myelomaNCT00866138), non-small cell lung cancer, melanomaNCT01280565), ovarian cancer and prostate cancer; theselterations are probably over estimated and not confirmed inarge cohorts of patients. In addition, several recent clinicalrials not showed benefit from therapies that target c-KitRn non-small cell lung cancer or prostate cancer patients21–26].
Studies in vitro have demonstrated that masitinib is moreowerful than imatinib, inhibiting human recombinant WT-KitR [6]. Moreover, it was hypothesized that the highelectivity of masitinib involves a better safety profile thanther TKI, in fact, in preclinical studies cardiotoxicity andenotoxicity (given by the presence of positive chromosomeberration test in human lymphocytes in Chinese Hamstervary (CHO) cells and in a bacterial reverse mutation test)asitinib-induced have not been showed [6].This review will shed light on masitinib considering: the
from canine tumor model to human clinical development: Whererevonc.2013.12.011
tructure–activity, the pharmacokinetics, the c-KitR activatedathway, potential resistance mechanisms to masitinib treat-ent, and the safety profile. We, also, explore preclinical

ARTICLE IN PRESSONCH-1825; No. of Pages 14
I. Marech et al. / Critical Reviews in Oncolo
Table 1Masitinib effects on the activity of protein kinases receptors.
Protein kinase receptor Enzyme IC50 (mM) Assay IC50 (mM)
KIT wild-type 0.20 ± 0.04 0.15KIT (exon 9) –a 0.1KIT V559D (exon 11) –a 0.003 ± 0.0001KIT (exon 13) –a 0.04KIT D816V (exon 17) >10 5 ± 2KIT D814V (murine) –a 0.005 ± 0.0003P
atatats
2
oWt
[bWibhTtdtoCbLmap
3
mtmcbte
aep[dtt
pragmp[[fi
lorufgsaataafmr[
dCaapcASok2
4
DGFR� 0.80 ± 0.12 0.005 ± 0.002a Not assessed.
nd clinical (completed and ongoing) trials with the aimo emphasize as this recent anti-angiogenic therapy, at firstpproved in CMCTs and, currently in development for thereatment of several human neoplasms, could be representn intriguingly setting in translational oncology, in whichhe murine model of cancer research could be integrated bypontaneous canine tumor model [27].
. Structure–activity
Masitinib mesylate is the orally bioavailable mesylate saltf masitinib, that selectively binds to and inhibits both theT and mutated forms of c-KitR, PDGFR�/�, FGFR3 and,
o a lesser extent, FAK (Table 1) [6,31].Masitinib is a 4-[(4-methylpiperazin-1-yl)methyl]-N-
4-methyl-3-[(4-pyridin-3-yl-1,3-thiazol-2 l)amino]phenyl]enzamide [28–30]. It docked into the ATP-binding site ofT c-KitR and, as a consequence, coordinates the c-KitR
n the inactive conformation. When docked into the c-KitRinding site, the aminothiazole of masitinib participates in aydrogen bond with the side-chain of the gatekeeper residuehr670 [6,31]. The amide NH forms a hydrogen bond to
he side-chain of Glu640, and the meta-nitrogen of the pyri-ine ring interacts with the backbone NH of Cys673. Forhe methylpiperazine group, an additional hydrogen bond isbserved between the protonated CH3-NH and the backbone-O of His790. The thiazole ring of masitinib packs looselyetween the aliphatic portions of the side-chains of Ala621,eu799, Cys809, and Phe811 [29]. The thiazole ring ofasitinib is strongly hydrophobic and it is unable to mediate
hydrogen bond to the water molecules. In this manner, thereferred binding of masitinib by c-KitR is observed.
. Pharmacokinetics
In vivo the intraperitoneal or oral administration ofasitinib inhibits tumor proliferation in mice with subcu-
aneous grafts of Ba/F3 cells expressing the D27 c-KitRutant [6]. In an intraperitoneal model, masitinib signifi-
Please cite this article in press as: Marech I, et al. Masitinib (AB1010),
we are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.crit
antly enhanced survival with a good safety profile, as showedy a lack of weight loss at the administered doses [6]. Thus,hese data emphasize masitinib orally bioavailability and itsfficacy to block cancer proliferation in vivo models [8].
ptf
gy/Hematology xxx (2014) xxx–xxx 3
Based on these studies, masitinib has been subsequentlydministered orally in pets and humans. With special refer-nce to pets, it has been demonstrated that masitinib reacheseak concentration approximately 1–2 h after administration31]. In particular, the oral bioavailability is 83%, with wideistribution throughout the body and rapid elimination (onlyrace amounts detectable 24 h post-dose). It is highly boundo plasma proteins (about 93%) [32].
The excretion is predominately intestinal (90%), with thearent compound accounting for nearly 50% of the mate-ial excreted. Its principal metabolites with biologic activityre: in feces N-desmethyl derivative, which is formed byut microflora and a sulfate conjugate of mono-hydroxy-asitinib; while in urine a carboxylic acid metabolite of the
arent compound after hydrolysis of the central amid linkage32,33]. Masitinib is mainly metabolized by N-dealkylation34]. Globally, 8 metabolites are identified in feces, and a partrom the parent compound up to 12 metabolites is detectedn urine [34].
Masitinib concentration increases with increasing dose-evels in a nearly dose proportional manner. No evidencef saturation or a time-dependent effect of absorption isecorded. In rats time to maximal concentration (tmax) val-es is between 2 and 7 h after repeated dose administrationsor 4, 13 and 26 weeks. Curiously, in rats, it was showed aender-dependent effect leading to a twofold higher expo-ure of females. Also in dogs this effect, it was observed alsofter single dose administration to a lesser extent. Both in ratsnd dogs masitinib mean half-life (t½) after single adminis-ration is about 5 h, whereas in humans after repeated dosepplication t½ values is about 13 h, increasing up to 33 h withscending doses. In rats, terminal half-life is slightly shorteror masitinib (range 2.72–3.16 h) than for AB3280, a majoretabolite (range 3.55–4.23 h), and is not showed variation
elated to gender or over time after repeated doses for 14 days32,33].
In humans, although masitinib is not able to induceifferent cytochrome P450 isoforms, it inhibits reversiblyYP3A4, 2C9 and 2D6 with IC50 values of 14 �M, 20 �Mnd >30 �M, respectively. However, this inhibition, as wells the high protein binding, may be of concern because of theotentials for drug-drug interactions, which are frequent inancer patients who receive commonly more than one drug.B3280 is not able to inhibit/induce these CYP isoforms.tudies concerning masitinib tissue distribution (given oncerally) in rats reveal an enrichment of the test item in adrenals,idneys, spleen and intestine (0.006–6.43% of the dose at4 h) [33,35].
. Targeting c-Kit receptor tyrosine kinase
from canine tumor model to human clinical development: Whererevonc.2013.12.011
The c-KitR, also called CD117 and encoded by c-KITroto-oncogene (localized on chromosome q4), belongso the class III of tyrosine kinase receptor (TKR)amily [36,37]. This family includes the PDGFR, and

ARTICLE IN PRESSONCH-1825; No. of Pages 14
4 Oncolo
mfipm
oJs
rhcP(
mebamvpbacvms(
dsam
(Toam
pawiaosptBt[
d
sai[mlbD
5
idtc
arahac1isKmtNmpris
teocitasmmcicat
I. Marech et al. / Critical Reviews in
acrophage colony-stimulating Factor/colony-stimulatingactor-1 Receptor (c-FmsR). SCF (overexpressed in variousnflammatory diseases) [38] and c-KitR regulate erythro-oiesis, lymphopoiesis, megakaryopoiesis, gametogenesis,elanogenesis, and MCs/eosinophils activations [37,39].The c-KitR includes: an extracellular region, consisting
f five immunoglobulin-like domains, a trans-membrane orM region, and an intracellular TK domain separated in twoubdomains by an insert region (Fig. 1) [14].
The interaction between c-KitR and SCF occurs theeceptor phosphorylation and the formation of variousomo/heterodimers with the activation of specific intra-ellular signaling pathways, including Mitogen Activatedrotein Kinase (MAPK) and Phosphatidyl Inositol 3-KinasePI3K)/Protein Kinase B (AKt) (Fig. 1) [40,41].
It has been found two forms of c-KitR: WT (145 kDa) andutant-type (125 kDa) [42,43]. The deregulation and over-
xpression of the complex c-Kit signaling network, inducedy mutant-type form of c-KitR, have been discovered to bessociated with cancer transformation in a variety of humanalignancies [42–47], as previously said. The increased acti-
ation of c-KitR pathway leads the MCs activation, thatlays a key role in human and canine tumor angiogenesisy means of pro-angiogenic cytokines degranulation, suchs VEGF, PDGF, FGF, and tryptase, all factors stored in theirytoplasmic secretory granules [48–50]. MCs c-KitR acti-ation induces the cross-talk between MCs the tumor cellsicroenvironment (endothelial and other cells) leading to the
trengthening of pro-angiogenic signaling, consequentiallyFig. 1) [14].
C-KitR mutations can be localized in the fifth extracellularomain (exon 8 and exon 9, f.e. Ala502-Tyr503 duplicationpecific in GIST) [51], in the JM region (exon 11, f.e. V559D,
deletion of nine aminoacids in the JM domain, called D27utant), and in the kinase domain (exon 17) [52].Imatinib mesylate (Gleevec®) was the first c-KitR TKI
targeting PDGFR�/�, BCR/ABL TK, CSF-1R, and SpleenK (SyK)) approved in human cancer for the treatmentf chronic myelogenous leukemia (CML) and unresectablend/or malignant GIST in patients with Philadelphia chro-osome and c-KIT positive, respectively [53].Regarding to molecular targeting, masitinib, inhibiting
articularly c-KitR, but also PDGFR�/� and Lck/LYn TK,s well as, in a lesser extent, FGFR3 and FAK, demonstratedeak inhibition of BCR/ABL TK and CSF-1R, compared to
matinib. In fact, it has been demonstrated in experimentalnimal models that masitinib has low risk of cardiotoxicityr genotoxicity compared to imatinib, due to masitinib highlyelective activity, given by the absence of its interference onroteins involved in cardiotoxicity (left ventricular dysfunc-ion or congestive heart failure), such as SRC family kinases,CR/ABL TK, Vascular Endothelial Growth Factor Recep-
Please cite this article in press as: Marech I, et al. Masitinib (AB1010),
we are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.crit
ors (VEGFR), Epidermal Growth Factor Receptors (EGFR)54].
Regarding to c-KitR activating mutations eventually pre-ictive of resistance to TKI therapy, patients harboring
ipde
gy/Hematology xxx (2014) xxx–xxx
pecific c-KIT mutations, including those of the exon 9nd the exon 17 (e.g. D816V mutant, frequently involvedn mastocytosis), develop resistance to imatinib treatment52,55,56]. Conversely to imatinib, in a preclinical studyasitinib showed the growth inhibition of a particular cellular
ine (Ba/F3 cells) carrying several c-KIT exon 11 mutations,ut also the proliferation of the same cell line expressing the816V mutation of exon 17 [6].
. Escape/resistance mechanisms
In several cancer diseases harboring c-KitR mutations,t was observed in malignant subclones the possibility toevelop additional c-KitR mutations that could confer resis-ance to masitinib treatment with an unknown mechanism,urrently.
At regard to this point, Hadzijusufovic et al. proposed particular experimental model to investigate the possibleesistance mechanisms to masitinib treatment [57]. They cre-ted NI-1 cell line from canine mastocytoma carrying variousomozygous c-KIT mutations, including missense mutationst nucleotides 107(C→T) and 1187(A→G), a 12-bp dupli-ation (nucleotide 1263), and a 12-bp deletion (nucleotide550). NI-1 cells were utilized to induce mastocytoma lesionsn NOD/SCID IL-2Rgammanull mice. NI-1 cells expressedeveral MCs differentiation antigens, including tryptase, c-itR, and a functional IgE receptor. Compared to the C2astocytoma cell line (harboring a c-KIT exon 11 muta-
ion, normally responsive to masitinib and imatinib therapy),I-1 cells were found to be less responsive against com-on c-KitR TKI, but they were even more sensitive against
roliferation-inhibitory effects of the mammalian target ofapamycin (mTOR) block everolimus and of PI3K/mTORnhibitors, including midostaurin, dasatinib, sunitinib, toza-ertib, and NVP-BEZ235 [57].
To individuate the downstream intracellular events dueo c-KitR inhibition after masitinib therapy, Klopfleischt al. assessed the transcriptional and translational changesf c-KIT-mutant canine C2 mast cells (a particular mastell line with a tandem duplication in the JM unit lead-ng c-KitR constitutive activation) after masitinib treatmento identify the signal transduction pathways, target genesnd cell functions correlated to c-KitR activity by tran-criptome and proteome analysis [58]. After three days ofasitinib (100 nM) treatment, it was observed a decreasedetabolic activity of C2 cells up to 40%. Therefore, the
-KitR inhibition caused a strong shut off of gene activ-ty in masitinib treated cells. Transcriptome analysis of C2ell line treated with masitinib for up to 72 h demonstrated
significant change of mRNA expression levels of morehan 3500 genes (about 16% of the 22,000 suspected genes
from canine tumor model to human clinical development: Whererevonc.2013.12.011
n the canine genome, corresponding to 16% of the com-lete coding genome in humans) [58], 60% of which withown-regulated expression correlating with reduced prolif-ration. On the other hand, about 40% of remaining genes

ARTICLE IN PRESSONCH-1825; No. of Pages 14
I. Marech et al. / Critical Reviews in Oncology/Hematology xxx (2014) xxx–xxx 5
tivated
hfisrt(AtwiI1r(sf1(
aCiatlaba[
6
olPFPcpgtmaosP
c(wnp
n
Fig. 1. The signaling network induced by ac
ad increased mRNA expression levels. These genes codi-es for 15 receptors, involved in pro-proliferative pathways,uch as: B- and T-cell receptors, insulin receptor, chemokineeceptors, steroid hormone and ErythroPOietin (EPO) recep-ors, Rat SArcoma (RAS) and Mitogen-Activated ProteinMAP) kinases, Phosphatase and TEnsiN homolog (PTEN).fter three days of masitinib treatment on C2 cells, the pro-
eome analysis of C2 cells identified only few 24 proteinsith changed expression levels, most of which being involved
n gene transcription: down-regulated Eukaryotic translationnitiation Factor 3/4A (EIF3, EIF4A), T-Complex Protein� (TCP1�) and inorganic PyrophosPhAtase 1 (PPA1); up-egulated protein folding, such as Heat Shock Protein ß1HSP-ß1), Protein Disulfide Isomerase-Associated 3 precur-or (PDIA3); up-regulated proteins involved in protectionrom oxidative stress, such as SELENium Binding Protein
(SELENBP1), Ubiquitin Carboxyl-terminaL esterase L3UCHL3) and ANneXin A6 (ANXA6) [57].
In conclusion, the alteration in mRNA expression levels of numerous genes demonstrated that in the masitinib treated2 cells several active genes were inactivated due to c-KitR
nhibition. Instead, most of receptor pathways up-regulatedfter masitinib treatment had pro-proliferative activity: thus,hese alternative activated pathways could represent cel-ular attempts to bypass the tumor growth arrest. These
Please cite this article in press as: Marech I, et al. Masitinib (AB1010),
we are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.crit
lternative signaling pathways (RAS, MAP, PTEN) couldecome crucial targets for the masitinib association ther-py or for subsequent therapy in resistant-masitinib patients57].
ti
c
c-Kit receptor tyrosine kinase in mast cell.
. Preclinical studies
In human pancreatic tumor cell lines model the associationf masitinib plus gemcitabine demonstrated to enhance pro-iferation inhibition of gemcitabine-refractory cell lines (Miaaca2 expressing SRC, LYn, FGFR3, Epidermal Growthactor Receptor 2 (ERBB2), and Panc1 expressing c-KitR,DGFR�/�), and to enhance in a lesser manner Mia Paca2ell tumor growth inhibition in a mouse model of humanancreatic cancer [7]. Moreover, it was observed increasedemcitabine cytotoxicity after reductions (400-fold reduc-ion) in gemcitabine IC50 on Mia Paca2 cells pre-treated with
asitinib (at dose between 5 and 10 nM), whereas a moder-te sensibility on Panc1 cells after a gemcitabine reductionf 10-fold. Interestingly, it was not shown an enhanced sen-itivity on proliferation inhibition to gemcitabine after Miaaca2 cells pre-treatment with imatinib [7].
In a Nog-SCID mouse model of human pancreatic can-er (28 days after the Mia Paca-2 cells injection) masitinib100 mg/kg daily oral) plus gemcitabine (50 mg/kg twiceeekly) demonstrated anti-tumor activity that, although wasot statistically significant (p > 0.05), it seemed to be moreotent compared to gemcitabine activity alone [7].
The analysis of 1412 genes expression showed an inferiorumber of deregulated genes after masitinib alone (n = 354)han gemcitabine alone (n = 1161) or masitinib plus gemc-
from canine tumor model to human clinical development: Whererevonc.2013.12.011
tabine therapy (n = 971) [7].Transcriptional analysis identified no pathway signifi-
antly over-expressed among the up-regulated genes, while
ARTICLE IN PRESSONCH-1825; No. of Pages 14
6 Oncolo
issa(P[cpg[
tthdod(uc
ignib
oiop[
dcmpl[
7
bipiraatdod
s(mmdni
fscd
ms31
iar[nmran(3v((
8
s4TOct(((imuppd
I. Marech et al. / Critical Reviews in
t individuated the WiNgless InTegrase-1(Wnt)/b-cateninignaling pathway as down-regulated in the cell lines resen-itised by the masitinib/gemcitabine combination (p < 0.001)nd in a lesser extent Extracellular-signal Regulated KinaseERK)/MAPK, Cell Division protein Kinase 5 (CDK5), andI3K/AKT signaling (p = 0.016, 0.025, 0.039, respectively)7]. The Wnt/b-catenin pathway, involved in pancreaticancer development, re-activates during pancreatic cancerrogression [59,60] and the association of masitinib plusemcitabine contributed to increase death in Mia Paca-2 cells7].
Thamm et al. achieved the potential of masitinibo sensitize several canine cancer cell lines (mastocy-oma, osteosarcoma, breast carcinoma, B-cell lymphoma,emangiosarcoma, histiocytic sarcoma, melanoma, and blad-er carcinoma) to antineoplastic agents [61]. The abilityf masitinib to synergize with various chemotherapeuticrugs, including gemcitabine (0.01–100 �M), doxorubicin0.4–1000 ng/mL), or vinblastine (0.1–10 �g/mL), is eval-ated with or without masitinib, administered at twooncentrations near its IC50 for each cell type.
Masitinib (at dose between 5 and 10 �M over a 72 hncubation time – conditions) enhanced gemcitabine-inducedrowth inhibition in canine osteosarcoma and breast carci-oma cell lines, while it increased doxorubicin/vinblastine-nduced growth inhibition in canine hemangiosarcoma,ladder carcinoma and histiocytic sarcoma cell lines [61].
Moreover, masitinib enhanced anti-proliferative effectn doxorubicin-resistant canine lymphoid GL-40 cells bynhibiting the function of P-glycoprotein, that is consideredne of the most important multidrug resistance mechanismsreventing intracellular distribution of antineoplastic agents62].
Interestingly, Lyles et al. showed a dose and time depen-ent proliferation decrease in canine hemangiosarcomaell lines after treatment with increasing concentrations ofasitinib (0.01–100 �M) for 24, 48 and 72 h inducing apo-
tosis through caspase-3/7 activation, as it was demonstratedikewise in feline sarcoma and canine osteosarcoma cells63–65].
. Masitinib approval in canine mast cell tumors
The pivotal multicenter, randomized-controlled, doubleind, phase III clinical trial has achieved masitinib (admin-stered with an intent-to-treat period of 6 months unlessrogressive disease, at dose between 12.5 and 6 mg/kg/day –n case of toxicity) efficacy in 202 dogs with unresectable orecurrent G2/3 metastatic CMCTs [8]. 25% of 191 dogs had
mutated form of c-KitR (in exons 11, 8, and 9) in both ofrms. Treatment with masitinib significantly prolonged time
Please cite this article in press as: Marech I, et al. Masitinib (AB1010),
we are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.crit
o progression (TTP) in all dogs compared to placebo (118ays vs 75 days; p = 0.038). By subgroup analysis it is clearlybserved that TTP is more increased in naïve than pretreatedogs (178 days vs 75 days, respectively; p = 0.001), and this
mttt
gy/Hematology xxx (2014) xxx–xxx
ignificant result is not correlated to c-KitR expression statusmutant or WT form). Thus, also in dogs, which have receivedasitinib as subsequent lines of treatment, harboring c-KitRutant form had a longer TTP compared to placebo (202
ays vs 97 days, respectively), although the difference wasot statistically significant because of small number of dogsn this subgroup (n = 25) [8].
Moreover, in masitinib arm it has been showed a trend inavor of increased overall survival (OS), despite there was aignificant increase of OS in masitinib treated dogs carrying-KitR mutant form compared to placebo (417 days vs 182ays, respectively; p = 0.015) [8]
In a subsequent study Hahn et al. demonstrated thatasitinib (12.5 mg/kg/day) compared to placebo increased
ignificantly OS at 12 months (masitinib 63% vs placebo9.8%) and at 24 months (masitinib 36% vs placebo 15%) in39 unresectable G2/3 CMCTs [66].
In the pivotal study there was not significant differencen terms of overall response (OR) assessed at 6 monthsfter initiation of treatment between two arms (completeesponse: 11.2% vs 4.9% and partial response: 4.6% vs 9.8%)8]. Considering safety, the toxicity masitinib-related sig-ificantly more frequent (72.6%) was that gastrointestinal,ainly of G 1–2 and reversible. Other side effects masitinib-
elated were: edema (14.9%), renal toxicity (10%), decreasedppetite (6.2%), lipoma (6.2%), asthenia (4.3%). Neutrope-ia and anemia were observed in 6.2% and in 5.6% of dogsmainly of G 1–2) treated with masitinib, respectively. The G–4 adverse events were: vomiting (4.3%) diarrhea (1.9%),omiting/diarrhea (5%), renal insufficiency (5%), and edema2.5%). The incidence of death between two arms was similar14.9% in masitinib group and 17.1% in placebo group) [8].
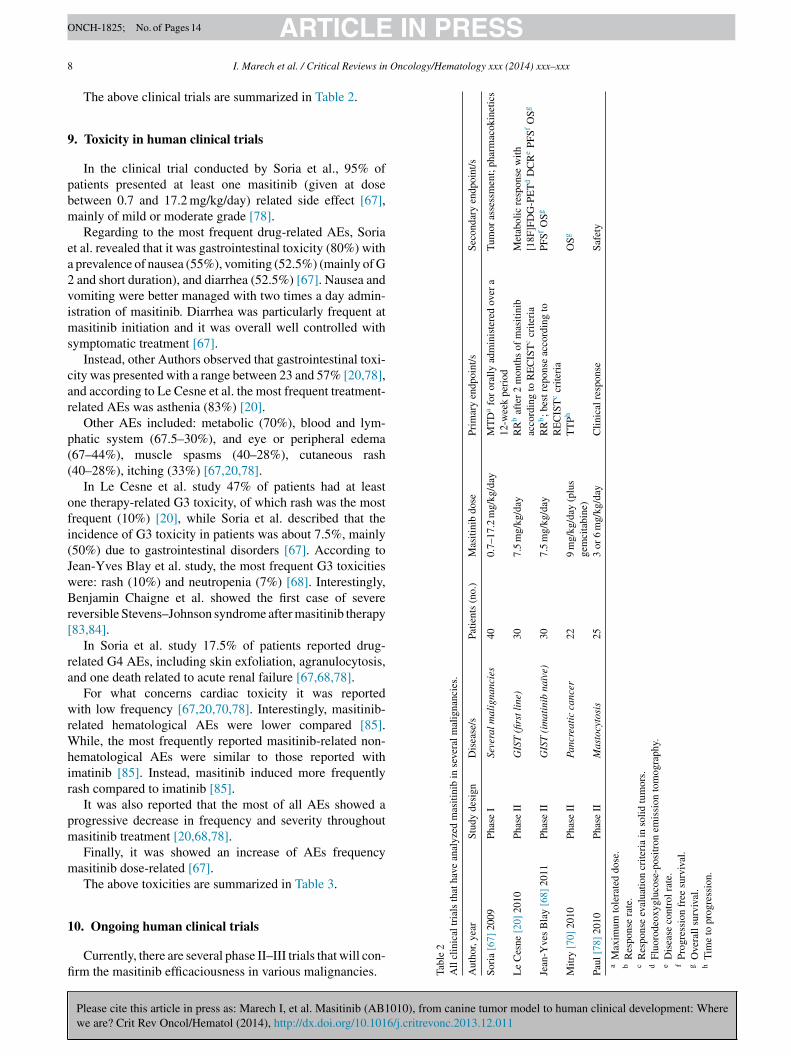
. Human clinical trials
The first phase I multicenter, non-randomized, open labeltudy achieved masitinib maximum tolerated dose (MTD) in0 patients with various advanced or metastatic solid cancers.he majority of patients (47.5%) were affected by GIST [67].ther patients had: mesothelioma (12.5%), thymoma (7.5%),
ortico-suprarenal cancer (5%), thyroid cancer (5%), colorec-al cancer (5%), bladder (2.5%), not differentiated cancer2.5%), non-small cell lung cancer (2.5%), prostate cancer2.5%), duodenum carcinoma (2.5%), neuroendocrine tumor2.5%), cystic adenoid carcinoma (2.5%). All patients hav-ng c-KitR expression status positive received oral dose of
asitinib between 0.7 and 17.2 mg/kg/day up to 12 weeksntil unacceptable toxicity or disease progression. 98% ofatients received at least one prior therapy, while 45% ofatients had previously been treated with imatinib [67]. Theose of 12 mg/kg/day was considered as the maximal recom-
from canine tumor model to human clinical development: Whererevonc.2013.12.011
ended dose in long-term treatment because of higher doseshan 12 mg/kg/day increased the incidence of gastrointestinaloxicity [67]. Tumor response assessed by Response Evalua-ion Criteria in Solid Tumors (RECIST) criteria. The clinical
ARTICLE IN PRESSONCH-1825; No. of Pages 14
Oncolo
bpriFcin
altmsdiTRPRs3o(ayd(ip[t(wKCp(rta[
tctlwpP3opp
(
gs[miS8
amt8rla
oadm4mMo[
d6tC(thtDltnwaom
mtt(sir
i
I. Marech et al. / Critical Reviews in
enefit rate (CBR) was 50% considering all patients. In GISTatients CBR was overall 36.9%, while in the imatinib-esistant group (17/40 patients) was 29.4% and in thematinib-intolerant group (only 2/40 patients) was 100% [67].inally, from this clinical trial emerges the strong rationale toonsider masitinib in first-line treatment of GIST (interest-ngly in imatinib-resistant patients) whether in other malig-ancies in association eventually with chemotherapy [67].
A phase II study analyzed efficacy of masitinib (givent 7.5 mg/kg/day in two intakes) in 30 naïve patients withocally advanced or metastatic GIST (c-KitR expression sta-us positive) during a median follow-up of 3 years [20]. The
utational analysis of c-KitR status in 15 of 30 patientshowed c-KitR exon 11 single mutation, c-KitR exon 11ouble mutations, WT c-KitR, PDGFR� mutation (D842V)n 33.3%, 3.3%, 10%, 3.3% of patients, respectively [20].he response rate (RR) at 2 months was 20% according toECIST criteria, while it was 85.7% according to FDG-ET Response Criteria [20]. Best response according toECIST criteria were a complete response, partial response,
table disease, progressive disease in 3.3%, 50%, 43.3%,.3% of patients with an overall disease control rate (DCR)f 96.7% [20]. Estimated median progression-free survivalPFS) was 41.3 months with PFS rate of 76.8% and 27.7%t 1 year and 3.5 years, respectively; the OS at 1 and 3ears was 96.7% and 89.9%, respectively [20].A preliminaryata of phase II, non-randomized trial evaluated masitinib7.5 mg/kg/day) administered until progression without clin-cal benefit, refusal or toxicity as first-line therapy in 30atients with inoperable, locally advanced or metastatic GIST68]. Almost all patients (97%) harbored positive c-KitR sta-us. The most frequent c-KitR mutation was that of exon 1156%), while the remaining were that of exon 11 togetherith exon 13 (13%), PDGFR� (6%), and other (6%). C-itR WT status was found in 19% of patients [68]. TheBR assessed by RECIST criteria was 23%. 77% of allatients withdrew from the study due to progression (50%)according to RECIST criteria), toxicity (17%) or othereasons (10%). This study showed a significant benefit inerms of median PFS (at 3.4 years in 50% of all patients)nd in median OS (at 4.3 years in 70% of all patients)68].
Although masitinib do not seem superior to imatinib inhese phase II clinical trials, however it appears a potentialandidate to compare it with imatinib in a phase III clinicalrial ongoing (NCT00812240). For what concern the secondine therapy in imatinib-resistant advanced GIST, masitinibas compared to sunitinib in a randomized phase II trial in 44atients [69]. After a median follow up of 14 months, medianFS (primary endpoint) was 3.9 months for masitinib arm and.8 months for sunitinib arm [69]. Based on similar valuesf PFS between two arms, masitinib could be considered as
Please cite this article in press as: Marech I, et al. Masitinib (AB1010),
we are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.crit
otential novel treatment worthy to a further evaluation inhase III clinical trials.
A phase II, non-randomized study achieved oral masitinib9 mg/kg/day, corresponding to about 600 mg/day) plus
etap
gy/Hematology xxx (2014) xxx–xxx 7
emcitabine as first-line treatment in 22 patients with unre-ectable, locally advanced or metastatic pancreatic cancer70]. TTP was 6.4 months and for locally advanced andetastatic patients was 8.3 and 2.7 months, respectively. TTP
n a subgroup analysis according to Karnofsky Performancetatus (KPS) was 6.4 and 0.8 months for patients with KPS0–100 or KPS 70, respectively [70].
Median OS was 7.1 months and, according to subgroupnalysis based on stage of disease, it was 8.4 and 6.8onths for locally advanced or metastatic disease, respec-
ively. According to subgroup analysis based on PS, OS was and 4.4 months in patients with KPS 80–100 or KPS 70,espectively. The 18-month observed survival rate was simi-ar for locally advanced (22%) and metastatic patients (23%)nd reached 28% for KPS 80–100 patients.
Georgin-Lavialle et al. described a bright early responsef one symptomatic patient having mast cell leukemia (MCL)fter 3 months of masitinib treatment 6.5 mg/kg/day, evi-enced by clinical benefit, the disappearance of circulatingast cells (from 7% to 0%) and c-KIT expressing cells (from
6% to 2%) [71]. This patient harbored a rare and specificutation: the duplication 501–502 located in c-KIT exon 9.ainly, in MCL patients treated with moderate success using
ther TKI it was found c-KIT mutation D816V in exon 1772–77].
A phase II2a, multicenter, open-label trial achieved theose response of masitinib (administered at dose of 3 or
mg/kg/day in two daily intakes for 3 months) in 25 symp-omatic mastocytosis patients (IM with “handicap”) [78].-KIT mutation status revealed that 76% of all patients
belonging to one arm: group 1) had not D816V mutation (ofhese group 1 patients: 32% harbored WT c-KIT status; 44%ad unknown c-KIT status), while 24% of patients (belongingo other arm: group 2) had at least one organ infiltrated with a816V, i.e. a mixed c-KIT status. 84% of patients presented at
east one-suspected masitinib-related adverse events duringhe initial 12-week phase. Results indicated that masitinib sig-ificantly reduced disability (depression, flushes and itchingith clinical response rates of 60, 50%, 25%, respectively)
fter 12 weeks in 56% of patients and improved quality-f-life in patients suffering from IM with handicap after 3onths [6,78–81].Regarding to symptoms improvement after masitinib in
astocytosis patients, Moura et al. analyzed in 288 patientshe therapeutic impact of this novel drug in depression symp-oms. This study demonstrated beyond that there was a high64%) prevalence of depression in this specific patients sub-et, but also that masitinib treatment induced a significantmprovement (67% of the cases) of depression, and 75% ofecovery cases [82].
Although published data seem promising, however it ismportant to remark the small size of the series of patients
from canine tumor model to human clinical development: Whererevonc.2013.12.011
nrolled (from 25 to 40) and as a consequence the weak statis-ical significance of studies results. Further studies enrolling
more large series of patient are awaited to confirm thesereliminary results [67,20,68,69,78,82].
ARTICLE IN PRESSONCH-1825; No. of Pages 14
8 Oncology/Hematology xxx (2014) xxx–xxx
9
pbm
ea2vims
car
p((
ofi(JwBr[
ra
wrWhir
pm
m
1
fi
tria
ls
that
have
anal
yzed
mas
itini
b
in
seve
ral m
alig
nanc
ies.
r
Stud
y
desi
gn
Dis
ease
/s
Patie
nts
(no.
)
Mas
itini
b
dose
Prim
ary
endp
oint
/s
Seco
ndar
y
endp
oint
/s
009
Phas
e
ISe
vera
l mal
igna
ncie
s
40
0.7–
17.2
mg/
kg/d
ay
MT
Da
for
oral
ly
adm
inis
tere
d
over
a12
-wee
k
peri
odT
umor
asse
ssm
ent;
phar
mac
okin
etic
s
0]
2010
Phas
e
II
GIS
T
(firs
t lin
e)
30
7.5
mg/
kg/d
ay
RR
baf
ter
2
mon
ths
of
mas
itini
bac
cord
ing
to
RE
CIS
Tc
crite
ria
Met
abol
ic
resp
onse
with
[18F
]FD
G-P
ET
dD
CR
ePF
SfO
Sg
lay
[68]
2011
Phas
e
II
GIS
T
(im
atin
ib
naïv
e)
30
7.5
mg/
kg/d
ay
RR
b; b
est r
epon
se
acco
rdin
g
toR
EC
IST
ccr
iteri
aPF
SfO
Sg
010
Phas
e
II
Panc
reat
ic
canc
er
22
9
mg/
kg/d
ay
(plu
sge
mci
tabi
ne)
TT
PhO
Sg
10
Phas
e
II
Mas
tocy
tosi
s
25
3
or
6
mg/
kg/d
ay
Clin
ical
resp
onse
Safe
ty
m
tole
rate
d
dose
.e
rate
.e
eval
uatio
n
crite
ria
in
solid
tum
ors.
eoxy
gluc
ose-
posi
tron
emis
sion
tom
ogra
phy.
cont
rol r
ate.
sion
free
surv
ival
.su
rviv
al.
prog
ress
ion.
I. Marech et al. / Critical Reviews in
The above clinical trials are summarized in Table 2.
. Toxicity in human clinical trials
In the clinical trial conducted by Soria et al., 95% ofatients presented at least one masitinib (given at doseetween 0.7 and 17.2 mg/kg/day) related side effect [67],ainly of mild or moderate grade [78].Regarding to the most frequent drug-related AEs, Soria
t al. revealed that it was gastrointestinal toxicity (80%) with prevalence of nausea (55%), vomiting (52.5%) (mainly of G
and short duration), and diarrhea (52.5%) [67]. Nausea andomiting were better managed with two times a day admin-stration of masitinib. Diarrhea was particularly frequent atasitinib initiation and it was overall well controlled with
ymptomatic treatment [67].Instead, other Authors observed that gastrointestinal toxi-
ity was presented with a range between 23 and 57% [20,78],nd according to Le Cesne et al. the most frequent treatment-elated AEs was asthenia (83%) [20].
Other AEs included: metabolic (70%), blood and lym-hatic system (67.5–30%), and eye or peripheral edema67–44%), muscle spasms (40–28%), cutaneous rash40–28%), itching (33%) [67,20,78].
In Le Cesne et al. study 47% of patients had at leastne therapy-related G3 toxicity, of which rash was the mostrequent (10%) [20], while Soria et al. described that thencidence of G3 toxicity in patients was about 7.5%, mainly50%) due to gastrointestinal disorders [67]. According toean-Yves Blay et al. study, the most frequent G3 toxicitiesere: rash (10%) and neutropenia (7%) [68]. Interestingly,enjamin Chaigne et al. showed the first case of severe
eversible Stevens–Johnson syndrome after masitinib therapy83,84].
In Soria et al. study 17.5% of patients reported drug-elated G4 AEs, including skin exfoliation, agranulocytosis,nd one death related to acute renal failure [67,68,78].
For what concerns cardiac toxicity it was reportedith low frequency [67,20,70,78]. Interestingly, masitinib-
elated hematological AEs were lower compared [85].hile, the most frequently reported masitinib-related non-
ematological AEs were similar to those reported withmatinib [85]. Instead, masitinib induced more frequentlyash compared to imatinib [85].
It was also reported that the most of all AEs showed arogressive decrease in frequency and severity throughoutasitinib treatment [20,68,78].Finally, it was showed an increase of AEs frequency
asitinib dose-related [67].The above toxicities are summarized in Table 3.
Please cite this article in press as: Marech I, et al. Masitinib (AB1010), from canine tumor model to human clinical development: Wherewe are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.critrevonc.2013.12.011
0. Ongoing human clinical trials
Currently, there are several phase II–III trials that will con-rm the masitinib efficaciousness in various malignancies. Ta
ble
2A
ll
clin
ical
Aut
hor,
yea
Sori
a
[67]
2
Le
Ces
ne
[2
Jean
-Yve
s
B
Mitr
y
[70]
2
Paul
[78]
20a
Max
imu
bR
espo
nsc
Res
pons
dFl
uoro
de
Dis
ease
fPr
ogre
sg
Ove
rall
hT
ime
to

ARTICLE IN PRESSONCH-1825; No. of Pages 14
I. Marech et al. / Critical Reviews in Oncology/Hematology xxx (2014) xxx–xxx 9
Table 3All toxicities that are reported in clinical studies mentioned above.
Adverse event, n (%) all grades Soria [67] pts no. 40 Le Cesne [20] pts no. 30 Mitry [70] pts no. 22 Paul [78] pts no. 25
Nausea 22 (55%) 15 (50%) 14 (63.6%) 11 (44%)Vomiting 21 (52.5%) 10 (33.3%) 11 (50%) 18 (72%)Diarrhea 21 (52.5%) 18 (60%) 11 (50%) 3 (12%)Constipation –a –a 2 (9.1) –a
Metabolic toxicity 28 (70%) – – –Eye or peripheral edema 9 (22.5%) 23 (76.7%) 8 (36.4%) 11 (44%)Muscle spasms 9 (22.5%) 12 (40%) –a 7 (28%)Cutaneous rash n.r.b 12 (40%) 11 (50%) 7 (28%)Itching n.r.b 11 (36.7%) –a –a
Anemia n.r.b 5 (16.7%) 8 (36.4%) –a
Neutropenia n.r.b 6 (20%) 6 (27.3%) –a
Thrombocytopenia –a –a 6 (27.3%) –a
Abdominal pain n.r.b 16 (53%) 4 (18.2%) 4 (16%)Cutaneous toxicity n.r.b –a –a –a
Asthenia n.r.b 27 (90%) 6 (27.3) 6 (24%)Headache –a –a –a 5 (20%)Eructation –a –a –a 3 (12%)Cardiac toxicity 3 (7.5%) –a –a –a
Vascular disorders 4 (10%) –a –a –a
Nervous system disorders 4 (10%) –a –a –a
Psychiatric disorders 1 (2.5%) –a –a –a
Renal and urinary disorders 9 (22.5%) –a –a –a
Haepatobiliary disorders 11 (27.5%) –a 10 (45.3%) –a
General disorders and administration site conditions 26 (65%) –a 9 (40.9%) –a
Respiratory disorders 1 (2.5%) –a 1 (4.5%) 3 (12%)Reproductive and breast disorders 1 (2.5%) –a –a –a
Hematological and lymphatic system disorders 27 (67.5%) 11 (36.7%) 20 (91%) –a
Skin and subcutaneous tissue disorders 14 (35%) 27 (50%) –a –a
Musculoskeletal and connective tissue disorders 9 (22.5%) 4 (13.3%) –a –a
Lacrimation increased –a 4 (13.3%) –a –a
a
tGptrmi(li
dsosSdtt(sew
g[mtiNgo[
pre6I(
ipIw
Noneb Not reported.
A phase II study will evaluate masitinib as second-linereatment at dose of 12 mg/kg/day compared to sunitinib inIST imatinib-resistant patients (NCT01506336). Anotherhase II study refers to Jean-Yves Blay et al. completerial (NCT00998751). It will be interesting to see finalesults of two phase III clinical trials that are consideringasitinib (7.5 mg/kg/day) as first-line therapy compared to
matinib (400 or 600 mg/day) therapy in GIST naïve patientsNCT00812240) and masitinib (12 mg/kg/day) as second-ine therapy compared to sunitinib (50 mg/day) in GISTmatinib-pretreated patients (NCT01694277).
Although the combination of masitinib plus gemcitabineid not showed promising results obtained from phase IItudy in pancreatic cancer [70], a large phase III study is nowngoing (NCT00789633). Preliminary data of this ongoingtudy (NCT00789633) presented at Gastrointestinal Cancersymposium of ASCO 2013 did not showed any statisticalifference in terms of median OS between the patients groupreated with gemcitabine plus masitinib (7.7 months) andhe patients group treated with gemcitabine plus placebo7 months; p = 0.74) [86]. However, in subgroup of patients
Please cite this article in press as: Marech I, et al. Masitinib (AB1010),
we are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.crit
elected with an unspecified genomic biomarker this differ-nce was significant (11 months in the patients group treatedith gemcitabine plus masitinib vs 5 months in the patients
p
(
roup treated with gemcitabine plus placebo; p = 0.000038)86]. Although this data showed some degree of interest, theain weakness of the reported result is a lack of the charac-
erization of the genomic biomarker employed [86]. Finally,n the global population of pancreatic cancer FOLFIRI-OX regimen is the gold standard treatment in patients withood PS [87] and, up to now, no advantage seems to beffered by the combination of masitinib plus gemcitabine86].
With regard to systemic mastocytosis, there are twohase II studies that will assess both of symptomsesponse then hematic biomarkers, including tryptase, TNF�,osinophils, and histamine under masitinib dose of 3 or
mg/kg/day (NCT01266369, NCT00814073), while a phaseII trial will confirm efficacy of 6 mg/kg/day masitinib doseNCT00831974).
Interestingly, masitinib at dose of 9 mg/kg/day is undernvestigation in a phase II trial in relapse or refractory multi-le myeloma (MM) patients (NCT00866138) and in a phaseII trial in relapse or refractory MM patients in associationith bortezomib and dexamethasone compared to placebo
from canine tumor model to human clinical development: Whererevonc.2013.12.011
lus bortezomib and dexamethasone (NCT01470131).Another phase III trial will achieve masitinib
5 mg/kg/day) plus dacarbazine in unresectable or metastatic

Please cite
this article
in press
as: M
arech I,
et al.
Masitinib
(AB
1010), from
canine tum
or m
odel to
human
clinical developm
ent: W
herew
e are?
Crit
Rev
Oncol/H
ematol
(2014), http://dx.doi.org/10.1016/j.critrevonc.2013.12.011
AR
TIC
LE
IN P
RE
SS
ON
CH
-1825;
No.
of Pages
14
10
I. M
arech et
al. /
Critical
Review
s in
Oncology/H
ematology
xxx (2014)
xxx–xxxTable 4All ongoing phase II/III trials mentioned above that are considering masitinib in several malignancies.
ClinicalTrials. gov Identifier Study design Arm/s Disease Target recruitment (no.) Masitinib dose Primary endpoint/s Secondary endpoint/s
NCT00866138 Phase II Masitinib Multiple myeloma 14 9 mg/kg/day TRRa TTPb; duration of response inresponder patients
NCT01506336 Phase II (1) Masitinib(2) Sunitinib
GIST 44 12 mg/kg/day Overall PFSc OSd
NCT00998751 Phase II Masitinib GIST 30 7.5 mg/kg/day ORRe according to RECISTcriteria
PFSc
NCT00831974 Phase II (1) Masitinib(2) Masitinib
Mastocytosis 23 (1) 6 mg/kg/day(2) 3 mg/kg/day
Response on symptoms AFIRMM scoref; reductionof: organ infiltration, level oftryptase, biomarkers (TNF�,eosinophils, histamine levels)pharmacokinetic profile
NCT01266369 Phase II (1) Masitinib(2) Masitinib
Mastocytosis 21 (1) 6 mg/kg/day(2) 3 mg/kg/day
Efficacy on handicaps;pruritus score; number offlushes per week; Hamiltonand Fatigue Impact scaleg atweek 12
None
NCT00814073 Phase III (1) Masitinib(2) Placebo
Mastocytosis 200 6 mg/kg/day Responder rate at week 24 Response in symptoms, mastcell infiltration, serumtryptase level; safetyprofile
NCT01470131 Phase III (1) Masitinib(2) Placebo(1) and (2) Plusbortezomib anddexamethasone
Multiple myeloma 300 6 mg/kg/day PFSc Overall TTPb; OSd
NCT00812240 Phase III (1) Masitinib(2) Imatinib
GIST 222 7.5 mg/kg/day PFSc OSd
NCT00789633 Phase III (1) Masitinib(2) Placebo(1) and (2) Plusgemcitabine
Pancreatic cancer 320 9 mg/kg/day OSd Survival rate, ORRe, controldisease rate, best response,serum level of CA19-9, PFSc,TTPb,time to response, quality oflife, questionnaires pain andanalgesics consumption
NCT01280565 Phase III (1) Masitinib(2) Dacarbazine
Melanoma 200 5 mg/kg/day Overall PFSc OS
NCT01694277 Phase III (1) Masitinib(2) Sunitinib
GIST 208 12 mg/kg/day OSd TTPb; overall PFSc; survivalrate; ORRe; control diseaserate
a Tumor response rate.b Time to tumor progression.c Progression free survival.d Overall survival.e Objective response rate.f Standard score to misure disability.g Scales to misure depression and fatigue.

ARTICLE IN PRESSONCH-1825; No. of Pages 14
Oncolo
s(
T
1
tPtooiN
t(rco
brpfiRa(i9cTmem
icf[2aas(aj
tiacct
ndidtmb
tah
C
R
DC
iG
C
R
I. Marech et al. / Critical Reviews in
tage 3–4 melanoma patients carrying c-KitR JM mutationNCT01280565).
The above ongoing clinical trials are summarized inable 4.
1. Concluding remarks
Masitinib mesylate (AB1010) is a novel selective TKI,hat inhibits mainly c-KitR (both of WT and mutated form),DGFR�/�, Lck, Lyn, weakly FGFR3 and FAK [6]. At first
ime it was approved in veterinary medicine for the treatmentf unresectable CMCTs [8]. Based on its favorable resultsn CMCTs [8,48,50,14,19], masitinib is under investigationn several human malignancies [68,21–26] (NCT00814073,CT00789633, NCT00866138, NCT01280565) [5].In human clinical development, there are several points
hat can be discussed about future masitinib application:1) the influence of c-KitR expression status on its clinicalesponse compared to imatinib; (2) the criteria to evaluatelinical outcome; (3) its role as chemosensitizer; (4) the rec-mmended dose and its administration mode.
Regarding to the first point, imatinib is less powerful inlocking WT c-KitR than masitinib [53]. Thus, it could beationale to consider masitinib in human cancers c-KIT+
referably to imatinib considering, also, its better safety pro-le regards to lower or absent cardiotoxicity [67,20,70,78].egards to the prediction of clinical response consideringctivating c-KIT mutations, the presence of exon 9, 17D816V), and 11 (some) mutations, could confer resistance tomatinib treatment [6,52,55,56]. Instead, the presence of exon
(duplication 501–502), 11, 13, 17 (D816V) mutations, notonfers resistance to masitinib treatment [6,67,68,70,71,78].hese data will be essential to evaluate the optimal use ofasitinib in further phase III clinical trials, according to
fficaciousness (toward the most frequent activating c-KITutations) and good safety profile.Regarding to the second point, the RECIST criteria are
nadequate to evaluate response in GIST patients [88]. Theseriteria must be replaced by CHOI criteria, which reflectully clinical outcome assessing the real tumor metabolism89,90]. In fact, in Le Cesne et al. trial it was observed a RR at
months of 20% according to RECIST criteria and of 85.7%ccording to CHOI criteria, in agreement with observed OSt 3 years (89.9%) [20]. Interestingly, it was recently demon-trated that Dynamic Contrast-Enhanced UltrasonographyDCE-US), like FDG-PET, is able to provide a quantitativessessment of GIST tumor perfusion giving a real responseudgment of masitinib efficacy also [91].
Regarding to the third point, the masitinib peculiarity iso synergize strongly with several antineoplastic agents inn vitro cell lines [7], especially with gemcitabine in pancre-
Please cite this article in press as: Marech I, et al. Masitinib (AB1010),
we are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.crit
tic cancer, unlike other TKIs. These preclinical data wereonfirmed by good TTP and OS observed in all human pan-reatic cancer patients after masitinib plus gemcitabine wellolerated treatment [70].
gy/Hematology xxx (2014) xxx–xxx 11
Considering the last point, there are two aspects that haveot yet been fully elucidated: the masitinib recommendedose (9 or 7.5 or 6 mg/kg/day [20,68–70,78]) and its admin-stration mode (in two daily intakes [67,20,78] or in one dailyose [70,68]). Further clinical studies are awaited to assesshe masitinib recommended dose and its administrationode, considering acceptable balance between therapeutic
enefit and risk to develop toxicity.In conclusion, masitinib represents the first widely selec-
ive and potent drug developed for c-KIT canine driven tumornd then translated to human cancer therapy worthy to furtheruman investigation.
onflict of interest statement
Authors have no conflict of interest to be declared.
eviewers
Jean-Yves Blay, M.D., Ph.D. Chair, Centre Leon Berard,epartment of Medicine, 28, rue Laennec, F-69008 Lyonedex 03, France.
Domenico Ribatti, Full Professor, University of Bari Med-cal School, Department of Basic Medical Sciences, Piazza. Cesare, 11, Bari, Italy.Jean-Charles Soria, M.D. Ph.D., Professor, IGR, 39 rue
amille Desmoulins, F-94800 Villejuif, France.
eferences
[1] Tebib J, Mariette X, Bourgeois P, et al. Masitinib in the treatment ofactive rheumatoid arthritis: results of a multicentre, open-label, dose-ranging, phase 2a study. Arthritis Research & Therapy 2009;11(3):R95.
[2] Procoli F. Clinical trial on the efficacy of masitinib in canine IBD.Veterinary Record 2010;167(19):760.
[3] Humbert M, de Blay F, Garcia G, et al. Masitinib, a c-kit/PDGFreceptor tyrosine kinase inhibitor, improves disease control in severecorticosteroid-dependent asthmatics. Allergy 2009;64(8):1194–201;Olivry T, Bizikova PA. Systematic review of randomized controlled tri-als for prevention or treatment of atopic dermatitis in dogs: 2008–2011update. Veterinary Dermatology 2013;24(1):97–117.
[4] Piette F, Belmin J, Vincent H, et al. Masitinib as an adjunct therapyfor mild-to-moderate Alzheimer’s disease: a randomised, placebo-controlled phase 2 trial. Alzheimer’s Research & Therapy 2011;3(2):16.
[5] Ranieri G, Gadaleta CD, Patruno R, et al. A model of study for humancancer: spontaneous occurring tumors in dogs. Biological features andtranslation for new anticancer therapies. Critical Reviews in Oncol-ogy/Hematology 2013. pii:S1040-8428(13)00065-6.
[6] Dubreuil P, Letard S, Ciufolini M, et al. Masitinib (AB1010), a potentand selective tyrosine kinase inhibitor targeting KIT. PLoS ONE2009;4(9):e7258.
from canine tumor model to human clinical development: Whererevonc.2013.12.011
[7] Humbert M, Castéran N, Letard S, et al. Masitinib combined with stan-dard gemcitabine chemotherapy: in vitro and in vivo studies in humanpancreatic tumour cell lines and ectopic mouse model. PLoS ONE2010;5(3):e9430.

ARTICLE IN PRESSONCH-1825; No. of Pages 14
1 Oncolo
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[[[
[
[
[
[
[[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
2 I. Marech et al. / Critical Reviews in
[8] Hahn KA, Ogilvie G, Rusk T, et al. Masitinib is safe and effective forthe treatment of canine mast cell tumors. Journal of Veterinary InternalMedicine 2008;22(6):1301–9.
[9] London CA, Seguin B. Mast cell tumors in the dog. Veterinary Clinicsof North America: Small Animal Practice 2003;33(3):473–89.
10] Takeuchi Y, Fujino Y, Watanabe M, et al. Validation of the prog-nostic value of histopathological grading or c-kit mutation in caninecutaneous mast cell tumours: a retrospective cohort study. VeterinaryJournal 2013, http://dx.doi.org/10.1016/j.tvjl.2012.11018. pii:S1090-0233(12)00522-9.
11] Thamm DH, Mauldin EA, Vail DM. Prednisone and vinblastinechemotherapy for canine mast cell tumor—41 cases (1992–1997). Jour-nal of Veterinary Internal Medicine 1999;13(5):491–7.
12] Letard S, Yang Y, Hanssens K, et al. Gain-of-function mutations in theextracellular domain of KIT are common in canine mast cell tumors.Molecular Cancer Research 2008;6(7):1137–45.
13] Zemke D, Yamini B, Yuzbasiyan-Gurkan V. Mutations in the jux-tamembrane domain of KIT are associated with higher grade mast celltumors in dogs. Veterinary Pathology 2002;39(5):529–35.
14] Kitamura Y, Hirotab S. Kit as a human oncogenic tyrosine kinase.Cellular and Molecular Life Sciences 2004;61(23):2924–31.
15] London CA, Galli SJ, Yuuki T, Hu ZQ, Helfand SC, Geissler EN.Spontaneous canine mast cell tumors express tandem duplicationsin the proto-oncogene c-kit. Experimental Hematology 1999;27(4):689–97.
16] Kim KH, Nelson SD, Kim DH, et al. Diagnostic relevance of overex-pressions of PKC-� and DOG-1 and KIT/PDGFRA gene mutations inextragastrointestinal stromal tumors: a Korean six-centers study of 28cases. Anticancer Research 2012;32(3):923–37.
17] Patruno R, Arpaia N, Gadaleta CD, et al. VEGF concentration fromplasma-activated platelets rich correlates with microvascular densityand grading in canine mast cell tumour spontaneous model. Journal ofCellular and Molecular Medicine 2009;13(3):555–61.
18] Ranieri G, Passantino L, Patruno R, et al. The dog mast cell tumour as amodel to study the relationship between angiogenesis, mast cell densityand tumour malignancy. Oncology Reports 2003;10(5):1189–93.
19] Takeuchi Y, Fujino Y, Watanabe M, et al. Aberrant autophosphoryla-tion of c-Kit receptor in canine mast cell tumor cell lines. VeterinaryImmunology and Immunopathology 2010;137(3-4):208–16.
20] Le Cesne A, Blay JY, Bui BN, et al. Phase II study of oral masitinibmesilate in imatinib-naïve patients with locally advanced or metastaticgastro-intestinal stromal tumour (GIST). European Journal of Cancer2010;46(8):1344–51.
21] Nick HJ, Kim HG, Chang CW, Harris KW, Reddy V, Klug CA.Distinct classes of c-Kit-activating mutations differ in their abilityto promote RUNX1-ETO-associated acute myeloid leukemia. Blood2012;119(6):1522–31.
22] López-Martin A, Ballestín C, Garcia-Carbonero R, et al. Prognos-tic value of KIT expression in small cell lung cancer. Lung Cancer2007;56(3):405–13.
23] Chau WK, Ip CK, Mak AS, Lai HC, Wong AS. C-Kit mediateschemoresistance and tumor-initiating capacity of ovarian cancer cellsthrough activation of Wnt/�-catenin-ATP-binding cassette G2 signal-ing. Oncogene 2013;32(22):2767–81.
24] Wiesner C, Nabha SM, Dos Santos EB, et al. C-kit and its ligand stemcell factor: potential contribution to prostate cancer bone metastasis.Neoplasia 2008;10(9):996–1003.
25] Bajaj GK, Zhang Z, Garrett-Mayer E, et al. Phase II study of imatinibmesylate in patients with prostate cancer with evidence of biochemicalrelapse after definitive radical retropubic prostatectomy or radiotherapy.Urology 2007;69(3):526–31.
26] Huang CH, Williamson SK, Van Veldhuizen PJ, et al. Potential roleof platelet-derived growth factor receptor inhibition using imatinib in
Please cite this article in press as: Marech I, et al. Masitinib (AB1010),
we are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.crit
combination with docetaxel in the treatment of recurrent non-small celllung cancer. Journal of Thoracic Oncology 2011;6(2):372–7.
27] Ranieri G, Pantaleo M, Piccinno M, et al. Tyrosine kinase inhibitors(TKIs) in human and pet tumours with special reference to
[
gy/Hematology xxx (2014) xxx–xxx
breast cancer: a comparative review. Critical Reviews in Oncol-ogy/Hematology 2013. pii:S1040-8428(13)00103-0.
28] RichmanChemicalCustom Solutions. www.RichmanChemical.com29] ChemicalBoock. www.chemicalbook.com/ChemicalProductProperty30] Masitinib Mesylate – NCI Drug Dictionary – National Cancer Institute.
www.cancer.gov/drugdictionary?cdrid=62910931] Bellamy F, Bader T, Moussy A, Hermine O. Pharmacokinet-
ics of masitinib in cats. Veterinary Research Communications2009;33(8):831–7.
32] U.S. Food and Drug Administration. http://www.fda.gov/downloads/AnimalVeterinary/Products/ApprovedAnimalDrugProducts/FO IADrugSummaries/UCM245243.pdf
33] Masivet – European Drugs Reference Encyclopedia.http://www.theodora.com/drugs/eu/masivet veterinary.html
34] Dog Aware. http://www.dogaware.com/health/cancer.html#newmastcell
35] VCS Veterinary Cancer Society. http://www.vetcancersociety.org/36] Cools J, De Angelo DJ, Gotlib J, et al. A tyrosine kinase created by
fusion of the PDGFRA and FIP1L1 genes as a therapeutic target of ima-tinib in idiopathic hypereosinophilic syndrome. New England Journalof Medicine 2003;348(13):1201–14.
37] Ranieri G. Hot topic: targeting tumor angiogenesis: an update. CurrentMedicinal Chemistry 2012;19(7):937.
38] Ribatti D, Ranieri G, Basile A, Azzariti A, Paradiso A, Vacca A. Tumorendothelial markers as a target in cancer. Expert Opinion on TherapeuticTargets 2012;16(12):1215–25.
39] Broudy VC. Stem cell factor and hematopoiesis. Blood1997;90(4):1345–64.
40] Ranieri G, Gadaleta-Caldarola G, Goffredo V, et al. Sorafenib(BAY 43-9006) in hepatocellular carcinoma patients: from discov-ery to clinical development. Current Medicinal Chemistry 2012;19(7):938–44.
41] Reith AD, Ellis C, Lyman SD, et al. Signal transduction by normalisoforms and W mutant variants of the Kit receptor tyrosine kinase.EMBO Journal 1991;10(9):2451–9.
42] Wypych J, Bennett LG, Schwartz MG, et al. Soluble kit receptor inhuman serum. Blood 1995;85(1):66–73.
43] Broudy VC, Lin NL, Sabath DF. The fifth immunoglobulin-like domainof the kit receptor is required for proteolytic cleavage from the cellsurface. Cytokine 2001;15(4):188–95.
44] Cohen PS, Chan JP, Lipkunskaya M, Biedler JL, Seeger RC. Expressionof stem cell factor and c-kit in human neuroblastoma The Children’sCancer Group. Blood 1994;84(10):3465–72.
45] Hassan S, Kinoshita Y, Kawanami C, et al. Expression of proto-oncogene c-kit and its ligand stem cell factor (SCF) in gastriccarcinoma cell lines. Digestive Disease and Sciences 1998;43(1):8–14.
46] Hines SJ, Organ C, Kornstein MJ, Krystal GW. Coexpression of thec-kit and stem cell factor genes in breast carcinomas. Cell Growth &Differentiation 1995;6(6):769–79.
47] Inoue M, Kyo S, Fujita M, Enomoto T, Kondoh G. Coexpression of thec-kit receptor and the stem cell factor in gynecological tumors. CancerResearch 1994;54(11):3049–53.
48] Giantin M, Aresu L, Benali S, et al. Expression of matrix met-alloproteinases, tissue inhibitors of metalloproteinases and vascularendothelial growth factor in canine mast cell tumours. Journal of Com-parative Pathology 2012;147(4):419–29.
49] Mederle O, Mederle N, Bocan EV, Ceausu R, Raica M. VEGF expres-sion in dog mastocytoma. Revista medico-chirurgicala a Societatii deMedici siNaturalisti din Iasi 2011;114(1):185–8.
50] Ranieri G, Patruno R, Ruggieri E, Montemurro S, Valerio P, Ribatti D.Vascular endothelial growth factor (VEGF) as a target of bevacizumabin cancer: from the biology to the clinic. Current Medicinal Chemistry2006;13(16):1845–57.
from canine tumor model to human clinical development: Whererevonc.2013.12.011
51] Sleijfer S, Wiemer E, Verweij J. Drug Insight: gastrointestinal stromaltumors (GIST)—the solid tumor model for cancer-specific treatment.Nature Reviews Clinical Oncology 2008;5(2):102–11.
ARTICLE IN PRESSONCH-1825; No. of Pages 14
Oncolo
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
I. Marech et al. / Critical Reviews in
52] Orfao A, Garcia-Montero AC, Sanchez L, Escribano L. Recentadvances in the understanding of mastocytosis: the role of KIT muta-tions. British Journal of Haematology 2007;138(1):12–30.
53] Buchdunger E, Zimmermann J, Mett H, et al. Inhibition ofthe Abl protein-tyrosine kinase in vitro and in vivo by a 2-phenylaminopyrimidine derivative. Cancer Research 1996;56(1):100–4.
54] Kerkelä R, Grazette L, Yacobi R, et al. Cardiotoxicity of the cancer ther-apeutic agent imatinib mesylate. Nature Medicine 2006;12(8):908–16.
55] Rubin BP, Duensing A. Mechanisms of resistance to small moleculekinase inhibition in the treatment of solid tumours. Laboratory Investi-gation 2006;86(10):981–6.
56] Ma Y, Zeng S, Metcalfe DD, et al. The c-KIT mutation causing humanmastocytosis is resistant to STI571 and other KIT kinase inhibitors;kinases with enzymatic site mutations show different inhibitor sensi-tivity profiles than wild-type kinases and those with regulatory-typemutations. Blood 2002;99(5):1741–4.
57] Hadzijusufovic E, Peter B, Herrmann H, et al. NI-1: a novel caninemastocytoma model for studying drug resistance and IgER-dependentmast cell activation. Allergy 2012;67(7):858–68.
58] Klopfleisch R, Meyer A, Schlieben P, et al. Transcriptome and pro-teome analysis of tyrosine kinase inhibitor treated canine mast celltumour cells identifies potentially kit signaling-dependent genes. BMCVeterinary Research 2012;8:96.
59] Osborne CS, Chakalova L, Brown KE, et al. Active genes dynamicallycolocalize to shared sites of ongoing transcription. Nature Genetics2004;36(10):1065–71.
60] Murtaugh LC. The what, where, when and how of Wnt/beta-cateninsignaling in pancreas development. Organogenesis 2008;4(2):81–6.
61] Thamm DH, Rose B, Kow K, et al. Masitinib as a chemosensitizerof canine tumor cell lines: proof of concept study. Veterinary Journal2012;191(1):131–4.
62] Zandvliet M, Teske E, Chapuis T, Fink-Gremmels J, Schrickx JA.Masitinib reverses doxorubicin resistance in canine lymphoid cells byinhibiting the function of P-glycoprotein. Journal of Veterinary Phar-macology and Therapeutics 2013, http://dx.doi.org/10.1111/jvp.12039.
63] Lyles SE, Milner RJ, Kow K, Salute ME. In vitro effects of the tyrosinekinase inhibitor, masitinib mesylate, on canine hemangiosarcoma celllines. Veterinary and Comparative Oncology 2012;10(3):223–35.
64] Lawrence J, Saba C, Gogal Jr R, et al. Masitinib demonstrates anti-proliferative and pro-apoptotic activity in primary and metastatic felineinjection-site sarcoma cells. Veterinary and Comparative Oncology2012;10(2):143–54.
65] Fahey CE, Milner RJ, Kow K, Bacon NJ, Salute ME. Apoptotic effectsof the tyrosine kinase inhibitor, masitinib mesylate, on canine osteosar-coma cells. Anticancer Drugs 2013;24(5):519–26.
66] Hahn KA, Legendre AM, Shaw NG, et al. Evaluation of 12- and24-month survival rates after treatment with masitinib in dogs with non-resectable mast cell tumors. American Journal of Veterinary Research2010;71(11):1354–61.
67] Soria JC, Massard C, Magné N, et al. Phase 1 dose-escalation study oforal tyrosine kinase inhibitor masitinib in advanced and/or metastaticsolid cancers. European Journal of Cancer 2009;45(13):2333–41.
68] Blay JY, Le Cesne A, Nguyen BB, et al. Overall survival benefit withmasitinib mesylate in imatinib-naïve locally advanced or metastaticgastro-intestinal stromal tumor (GIST): 4 years follow-up of the FrenchSarcoma Group phase II trial. In: ASCO Gastrointestinal Cancers Sym-posium. 2011 [abstract].
69] Adenis A, Le Cesne A, Nguyen BB, et al. Masitinib mesylate inimatinib-resistant advanced GIST: a randomized phase II trial. Journalof Clinical Oncology 2012;30.(Suppl.) [abstr. 10007].
70] Mitry E, Hammel P, Deplanque G, et al. Safety and activity of masitinibin combination with gemcitabine in patients with advanced pancre-
Please cite this article in press as: Marech I, et al. Masitinib (AB1010),
we are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.crit
atic cancer. Cancer Chemotherapy and Pharmacology 2010;66(2):395–403.
71] Georgin-Lavialle S, Lhermitte L, Suarez F, et al. Mast cell leukemia:identification of a new c-Kit mutation, dup(501–502), and response
[
gy/Hematology xxx (2014) xxx–xxx 13
to masitinib, a c-Kit tyrosine kinase inhibitor. European Journal ofHaematology 2012;89(1):47–52.
72] Gotlib J, Berubé C, Growney JD, et al. Activity of the tyrosine kinaseinhibitor PKC412 in a patient with mast cell leukemia with the D816VKIT mutation. Blood 2005;106(8):2865–70.
73] Noack F, Sotlar K, Notter M, Thiel E, Valent P, Horny HP. A leukemicmast cell leukemia with abnormal immunophenotype and c-kit muta-tion D816V. Leukemia & Lymphoma 2004;45(11):2295–302.
74] Akin C, Fumo G, Yavuz AS, Lipsky PE, Neckers L, MetcalfeDD. A novel form of mastocytosis associated with a transmem-brane c-kit mutation and response to imatinib. Blood 2004;103(8):3222–5.
75] Zhang LY, Smith ML, Schultheis B, et al. A novel K509I muta-tion of KIT identified in familial mastocytosis—in vitro and in vivoresponsiveness to imatinib therapy. Leukemia Research 2006;30(4):373–8.
76] Mital A, Piskorz A, Lewandowski K, Wasag B, Limon J, Hell-mann A. A case of mast cell leukaemia with exon 9 KIT mutationand good response to imatinib. European Journal of Haematology2011;86(6):531–5.
77] Spector MS, Iossifov I, Kritharis A, et al. Mast-cell leukemia exomesequencing reveals a mutation in the IgE mast-cell receptor beta chainand KIT V654A. Leukemia 2011;26(6):1422–5.
78] Paul C, Sans B, Suarez F, et al. Masitinib for the treatment of systemicand cutaneous mastocytosis with handicap: a phase 2a study. AmericanJournal of Hematology 2010;85(12):921–5.
79] Droogendijk HJ, Kluin-Nelemans HJ, van Doormaal JJ, Oranje AP,van de Loosdrecht AA, van Daele PL. Imatinib mesylate in the treat-ment of systemic mastocytosis: a phase II trial. Cancer 2006;107(2):345–51.
80] Vega-Ruiz A, Cortes JE, Sever M, et al. Phase II study of imatinibmesylate as therapy for patients with systemic mastocytosis. LeukemiaResearch 2009;33(11):1481–4.
81] Gilfillan AM, Tkaczyk C. Integrated signalling pathways for mast-cellactivation. Nature Reviews Immunology 2006;6(3):218–30.
82] Moura DS, Sultan S, Georgin-Lavialle S, et al. Depression in patientswith mastocytosis: prevalence, features and effects of masitinib therapy.PLoS ONE 2011;6(10):e26375.
83] Chaigne B, Lagier L, Aubourg A, et al. Stevens–Johnson Syndromeinduced by masitinib. Acta Dermato-Venereologica 2012;92(2):210–2.
84] Hsiao LT, Chung HM, Lin JT, et al. Stevens–Johnson syndrome aftertreatment with STI571: a case report. British Journal of Haematology2002;117(3):620–2.
85] Verweij J, Casali PG, Zalcberg J, et al. Progression-free survival ingastrointestinal stromal tumours with high-dose imatinib: randomisedtrial. Lancet 2004;364(9440):1127–34.
86] Deplanque G, Demarchi M, Hebbar M, et al. Masitinib in nonresectablepancreatic cancer: results of a phase III randomized placebo-controlledtrial. Journal of Clinical Oncology 2012;30(Suppl. 34) [abstr. 158].
87] Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gem-citabine for metastatic pancreatic cancer. New England Journal ofMedicine 2011;364(19):1817–25.
88] Benjamin RS, Choi H, Macapinlac HA, et al. We should desistusing RECIST, at least in GIST. Journal of Clinical Oncology2007;25(13):1760–4.
89] Choi H, Charnsangavej C, Faria SC, et al. Correlation of com-puted tomography and positron emission tomography in patients withmetastatic gastrointestinal stromal tumor treated at a single institu-tion with imatinib mesylate: proposal of new computed tomographyresponse criteria. Journal of Clinical Oncology 2007;25(13):1753–9.
90] Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to eval-uate the response to treatment in solid tumors. European Organizationfor Research and Treatment of Cancer, National Cancer Institute of
from canine tumor model to human clinical development: Whererevonc.2013.12.011
the United States, National Cancer Institute of Canada. Journal of theNational Cancer Institute 2000;92(3):205–16.
91] Lassau N, Chami L, Koscielny S, et al. Quantitative functional imag-ing by dynamic contrast enhanced ultrasonography (DCE-US) in

ARTICLE IN PRESSONCH-1825; No. of Pages 14
1 Oncolo
B
uoOvtm
inarp
ivia
dVp
eBa
oi
aINHt
oo
4 I. Marech et al. / Critical Reviews in
GIST patients treated with masatinib. Investigational New Drugs2012;30(2):765–71.
iographies
Ilaria Marech is a medical oncologist specialized inltrasonography. She works in the Interventional Radiol-gy Unit with Integrated Section of Translational Medicalncology at the National Cancer Research Center “Gio-
anni Paolo II” in Bari, Italy. Her research interests include:umor angiogenesis, targeted therapies, and pet animal
odels.
Rosa Patruno is a veterinary medical doctor specializedn infective disease, veterinary prophylaxis, and in veteri-ary public health. She works in Department of Preventionnd Animal Health at the ASL BAT in Barletta, Italy. Heresearch interests include pet tumor angiogenesis and com-arative oncology.
Nicola Zizzo is a veterinary medical doctor and professorn Veterinary Pathology in Veterinary Medical School at Uni-
Please cite this article in press as: Marech I, et al. Masitinib (AB1010),
we are? Crit Rev Oncol/Hematol (2014), http://dx.doi.org/10.1016/j.crit
ersity of Bari in Valenzano, Bari, Italy. His research interestsnclude: animal pathology, comparative oncology, and tumorngiogenesis.
Rra
gy/Hematology xxx (2014) xxx–xxx
Claudia Gadaleta is a student in science of animal repro-uction at Veterinary Medical School at University of Bari inalenzano, Bari, Italy. Her research interests include animalathology and comparative oncology.
Marcello Introna is a veterinary medical doctor in Vet-rinary Medical School at University of Bari in Valenzano,ari, Italy. His research interests include animal pathologynd comparative oncology.
Alfredo Francesco Zito is a medical pathologist in Pathol-gy Unit at ASL BA in Bari, Italy. His research interestsnclude: tumor angiogenesis and comparative oncology.
Cosmo Damiano Gadaleta is an interventional radiologistnd the director of the Interventional Radiology Unit, withntegrated Section of Translational Medical Oncology at theational Cancer Institute “Giovanni Paolo II” of Bari, Italy.is research interests include: transarterial chemoemboliza-
ion of lung and liver tumors, and pet animal models.
Girolamo Ranieri is a medical oncologist and vice directorf the Interventional Radiology Unit with Integrated Sectionf Translational Medical Oncology at the National Cancer
from canine tumor model to human clinical development: Whererevonc.2013.12.011
esearch Centre “Giovanni Paolo II” in Bari, Italy. Hisesearch interests include: tumor angiogenesis, targeted ther-pies, and pet animal models.




















