Managing Patients with Pain in Primary Care – Part 1 - Gov.bc ...
50
Managing Patients with Pain in Primary Care – Part 1 1 DRAFT FOR EXTERNAL REVIEW 2 Online questionnaire available at: surveymoh.health.gov.bc.ca/public/survey/external-review-questionnaire- 3 managing-pain 4 Line numbers are included for ease of reference while providing feedback 5 Effective Date: TBD 6 Preamble 7 Managing patients with pain, especially chronic non-cancer pain (CNCP) is challenging given current practice 8 realities. Practice patterns have changed with more patients receiving episodic care from walk-in-clinics and 9 emergency departments, and group or team-based clinics with a variety of participating clinicians. Clinicians can be 10 overwhelmed by guidelines, updates, algorithms, portals, and on-line journals. The overdose crisis has permeated 11 our day-to-day practice and often create prescribing uncertainty. Many have fears (often misplaced) about 12 disciplinary and legal consequences from licensing and legislative bodies. Patients also have access to many sources 13 of information, may come with a history of past trauma and unequal treatment by the health care system, and 14 struggle with reduced function and ability because of their pain. 15 The intent of this guideline is to provide practical, accessible, and BC specific guidance. It’s a distillation of many 16 guidelines and expert recommendations. There is no clear or absolute clinical pathway to managing pain and many 17 controversies persist especially in the use of opioid and cannabis. The guideline development committee 18 recommends reasonable clinical judgement, documenting well and reassessing often. 19 Scope 20 This guideline comprises of 2 parts: 21 1. Pain Assessment and Management Approaches 22 2. Pain Management – Pharmacological and Procedural 23 24 Within Scope of this guideline: 25 • Practical recommendations within the primary care setting for a graded, multimodal approach to supporting 26 adult patients (≥ 19 years) with pain on a continuum from acute, subacute to chronic pain. A multimodal 27 approach is one where patients with pain receive multiple interventions and supports, both concurrently 28 and sequentially. 29 • General approaches to treating patients with pain and links to supportive resources. 30 31 Out of scope of this guideline: 32 • Detailed recommendations for condition-specific pain 33 • Pain in palliative care or as part of an advanced life-limiting disease 34 - refer to BC Guidelines: Palliative Care Part 2: Pain and Symptom Management. Patients with pain 35 associated with serious or advanced illness may benefit from both the Palliative Care and Managing Pain 36 guidelines. 37 • Pain in children or young adults. Consider accessing the Pain Service at BC Children’s Hospital for more 38 specific assistance in managing pain in this age group. 39
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of Managing Patients with Pain in Primary Care – Part 1 - Gov.bc ...
Managing Patients with Pain in Primary Care – Part 1 1 DRAFT FOR EXTERNAL REVIEW 2
Online questionnaire available at: surveymoh.health.gov.bc.ca/public/survey/external-review-questionnaire-3 managing-pain 4
Line numbers are included for ease of reference while providing feedback 5 Effective Date: TBD 6
Preamble 7
Managing patients with pain, especially chronic non-cancer pain (CNCP) is challenging given current practice 8 realities. Practice patterns have changed with more patients receiving episodic care from walk-in-clinics and 9 emergency departments, and group or team-based clinics with a variety of participating clinicians. Clinicians can be 10 overwhelmed by guidelines, updates, algorithms, portals, and on-line journals. The overdose crisis has permeated 11 our day-to-day practice and often create prescribing uncertainty. Many have fears (often misplaced) about 12 disciplinary and legal consequences from licensing and legislative bodies. Patients also have access to many sources 13 of information, may come with a history of past trauma and unequal treatment by the health care system, and 14 struggle with reduced function and ability because of their pain. 15 The intent of this guideline is to provide practical, accessible, and BC specific guidance. It’s a distillation of many 16 guidelines and expert recommendations. There is no clear or absolute clinical pathway to managing pain and many 17 controversies persist especially in the use of opioid and cannabis. The guideline development committee 18 recommends reasonable clinical judgement, documenting well and reassessing often. 19
Scope 20
This guideline comprises of 2 parts: 21
1. Pain Assessment and Management Approaches 22 2. Pain Management – Pharmacological and Procedural 23
24 Within Scope of this guideline: 25
• Practical recommendations within the primary care setting for a graded, multimodal approach to supporting 26 adult patients (≥ 19 years) with pain on a continuum from acute, subacute to chronic pain. A multimodal 27 approach is one where patients with pain receive multiple interventions and supports, both concurrently 28 and sequentially. 29
• General approaches to treating patients with pain and links to supportive resources. 30 31 Out of scope of this guideline: 32
• Detailed recommendations for condition-specific pain 33 • Pain in palliative care or as part of an advanced life-limiting disease 34
refer to BC Guidelines: Palliative Care Part 2: Pain and Symptom Management. Patients with pain 35 associated with serious or advanced illness may benefit from both the Palliative Care and Managing Pain 36 guidelines. 37
• Pain in children or young adults. Consider accessing the Pain Service at BC Children’s Hospital for more 38 specific assistance in managing pain in this age group. 39
BC Guidelines: Managing Pain – DRAFT for External Review 2
Key Recommendations 40
• Patients with moderate to severe acute injury should receive adequate pain control and consideration of 41 early referral to specialized services where indicated and available. 42
• Consider improving function and reducing disability, rather than the elimination of pain, as the goal of pain 43 management strategies, especially when pain progresses into the chronic pain continuum. 44
• A supportive longitudinal therapeutic relationship is a foundation of pain management. Given the changing 45 face of primary care with team-based care, walk-in care, and virtual care, use of databases such as EMR, 46 Pharmanet/CareConnect is increasingly important. 47
• Throughout the pain continuum, especially in subacute and chronic, assess for biopsychosocial factors 48 (yellow flags), and co-morbid conditions. Be alert to addressing the risk factors for development of chronic 49 pain. 50
• Complex Regional Pain Syndrome (CRPS) is often considered a pain emergency and warrants an urgent 51 referral or consultation to a pain specialist and consideration of early intervention with steroids. 52
• Consider all forms of interventions, including non-pharmacological and pharmacological, as a ‘trial’ to be 53 reassessed for effectiveness on a regular basis. 54
• For people with chronic pain not already on opioid therapy, optimize non-pharmacotherapy and non-opioid 55 pharmacotherapy first before considering a trial of opioid therapy. 56
• For all medication, aim for the optimal dose (and be aware of the recommended maximal dose) with fewest 57 side effects and do regular, recurrent evaluation to assess for meaningful improvement in pain and function. 58 See Managing Pain in Primary Care – Part 2: Pharmacological Management. 59
Definition 60
The International Association for the Study of Pain (IASP) defines pain as an unpleasant sensory and emotional 61 experience associated with actual or potential tissue damage or described in terms of such damage. 62
While it is convenient to try and categorize pain in terms of mechanism, duration or origin, there can be significant 63 differences in how individuals experience pain and how tissues may heal. The parameters for defining pain as acute 64 or chronic may vary depending on the type of trauma and past history, which suggests that a more nuanced 65 approach to applying a framework for resolution of the pain is often required. 66
Acute pain is pain generally expected to last less than 4 weeks and occurs within the context of tissue damage and 67 repair, resolving with tissue healing. 68
Subacute pain (transition zone between acute and chronic) is defined as pain not resolving or diminishing as 69 expected in 4-12 weeks after initial onset. The ‘subacute’ timeframe should trigger practitioners to pause and reflect 70 on progress of pain management and take steps to reduce the likelihood of transition to chronic pain. 71
Chronic or persistent pain is pain persisting for greater than 3 months. It can arise from long-term medical 72 conditions not expected to improve such as osteoarthritis, scoliosis, and multiple sclerosis, or it can also be pain that 73 persists beyond expected time of healing. 74
Pain can be described in terms of mechanisms. Treatment modalities, including adjuvants, may differ significantly 75 depending on the mechanism of pain. 76
• Nociceptive: arises from actual or threatened damage to underlying tissue (e.g. soft tissue, bone, viscera) 77 • Inflammatory: perception of noxious stimuli that occur during an inflammatory or immune response. 78 • Neuropathic: results from damaged or dysfunctional nerves (leads to misfiring pain signals). 79 • Nociplastic: altered pain perception without clear evidence of actual or threatened tissue damage such as in 80
fibromyalgia. 81 82
3 BC Guidelines: Managing Pain – DRAFT for External Review
When considering a patient’s experience of pain, it can help to remember: 83 • Pain is always a personal, learned experience that is influenced to varying degrees by biological, psychological, 84
social, and cultural factors and life experiences. 85 • A person’s report of their subjective experience of pain should be respected. 86 • Although pain usually serves an adaptive role, it may have adverse effects on function, and on social and 87
psychological well-being. 88 • Verbal description is only one of several ways to express pain; inability to communicate does not negate the 89
possibility that a person experiences pain. 90
Epidemiology of Chronic Pain 91
According to Statistics Canada, an estimated 7.6 million, or one in five people (across their lifespan) in Canada, live 92 with chronic pain.1 It is estimated that 1 in 5 adults in BC suffer with chronic pain.2 93
Approach to Care 94
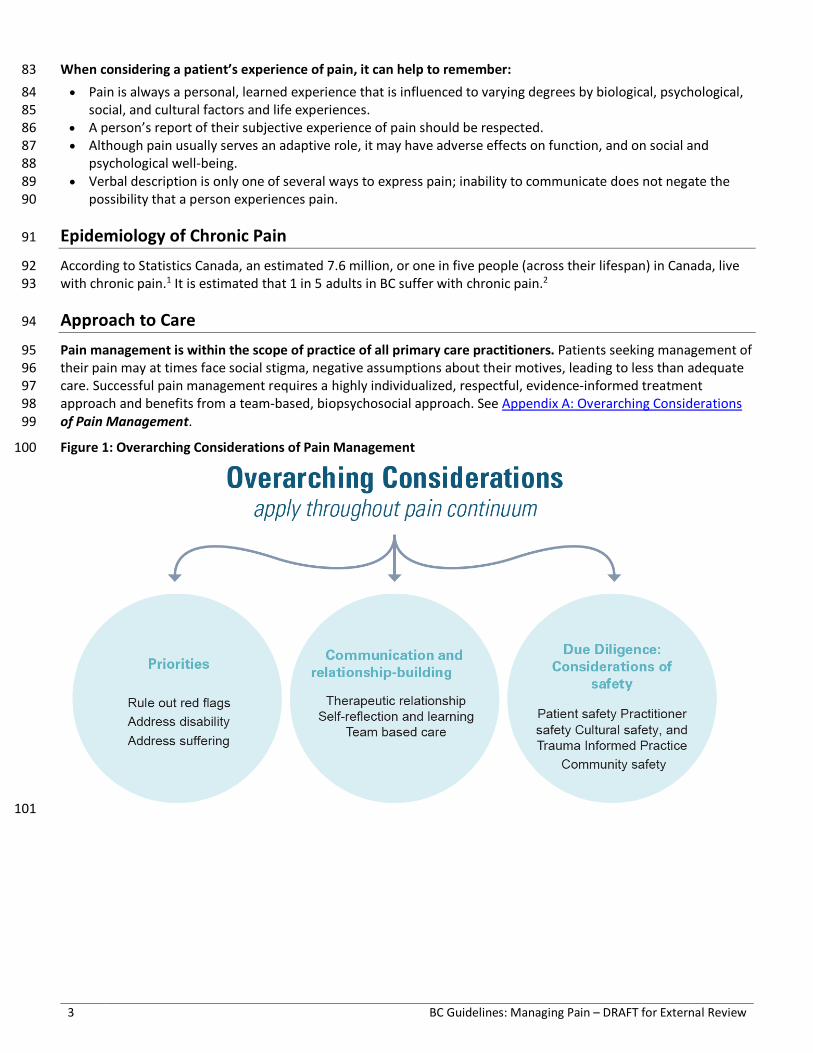
Pain management is within the scope of practice of all primary care practitioners. Patients seeking management of 95 their pain may at times face social stigma, negative assumptions about their motives, leading to less than adequate 96 care. Successful pain management requires a highly individualized, respectful, evidence-informed treatment 97 approach and benefits from a team-based, biopsychosocial approach. See Appendix A: Overarching Considerations 98 of Pain Management. 99
Figure 1: Overarching Considerations of Pain Management 100
101
BC Guidelines: Managing Pain – DRAFT for External Review 4
General Principles 102
While clinicians may see a patient at any point along the pain 103 continuum, the principles for managing pain remain 104 consistent. It is important to develop a positive, supportive, 105 and respectful therapeutic relationship. Strong consideration 106 should be given to using a trauma informed approach, 107 especially in people experiencing chronic pain. 108
• Emphasis on addressing ongoing impact of pain, disability, 109 and suffering. The goal is improved function – use 110 functional assessments for personal and occupational 111 functioning. 112
• Unattached patients and those in team-based practices 113 with a variety of care providers present a challenge to the traditional long-term relationship that clinicians 114 have previously had. Use of the EMR and shared databases such as Pharmanet and CareConnect are 115 increasingly important to connect the information relating to patient’s history and past care interventions. 116
• Encourage supported self-management strategies (See Resources: Resources for Patients) and incorporate 117 into daily lives. 118
• Consider all interventions and therapies as therapeutic trials. 119 • Consistent re-evaluation of progress is important. Address early if progress is delayed. 120 • Red flags suggest a more urgent need for investigations or referral (Table 1: Pain Red Flags). 121 • Yellow flags are physical, psychological and social Factors that may affect development of chronic pain (Table 122
2: Pain Yellow Flags) 123 • Be alert to red and yellow flags - assess and re-assess concurrent disorders and biopsychosocial factors that 124
increase the risk of the pain becoming chronic. Be mindful of patient, practitioner, and community safety. 125 • Document well - improvements/changes in symptoms and function, and patient assessment of effects of 126
individual modalities. This is especially important when using opioids and if exceeding recommended 127 prescribing standards. 128
Assessing and Managing Pain 129
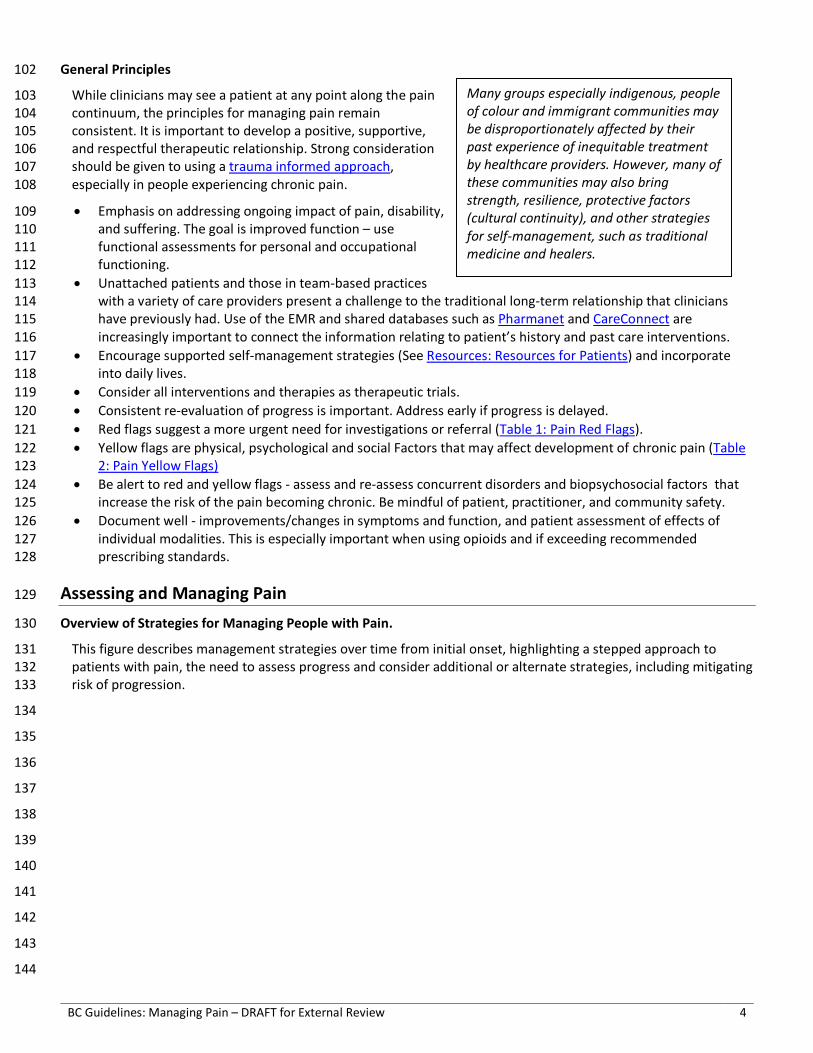
Overview of Strategies for Managing People with Pain. 130
This figure describes management strategies over time from initial onset, highlighting a stepped approach to 131 patients with pain, the need to assess progress and consider additional or alternate strategies, including mitigating 132 risk of progression. 133
134
135
136
137
138
139
140
141
142
143
144
Many groups especially indigenous, people of colour and immigrant communities may be disproportionately affected by their past experience of inequitable treatment by healthcare providers. However, many of these communities may also bring strength, resilience, protective factors (cultural continuity), and other strategies for self-management, such as traditional medicine and healers.
5 BC Guidelines: Managing Pain – DRAFT for External Review
145
Figure 2: Strategies for Pain Management 146
147 148
149 150 151
152
153
BC Guidelines: Managing Pain – DRAFT for External Review 6
Acute pain 154
Assessment 155
• Identify the source of the pain. Consider pain mechanism and location. 156 • Take a structured pain history. Consider one of the following strategies: 157
o OPQRST – Onset, Provoking/Palliating, Quality of pain, Region/Radiation, Severity, Timing/Treatment 158 o AAA - Alleviating/aggravating factors, Associated symptoms, Attributions/adaptation. 159
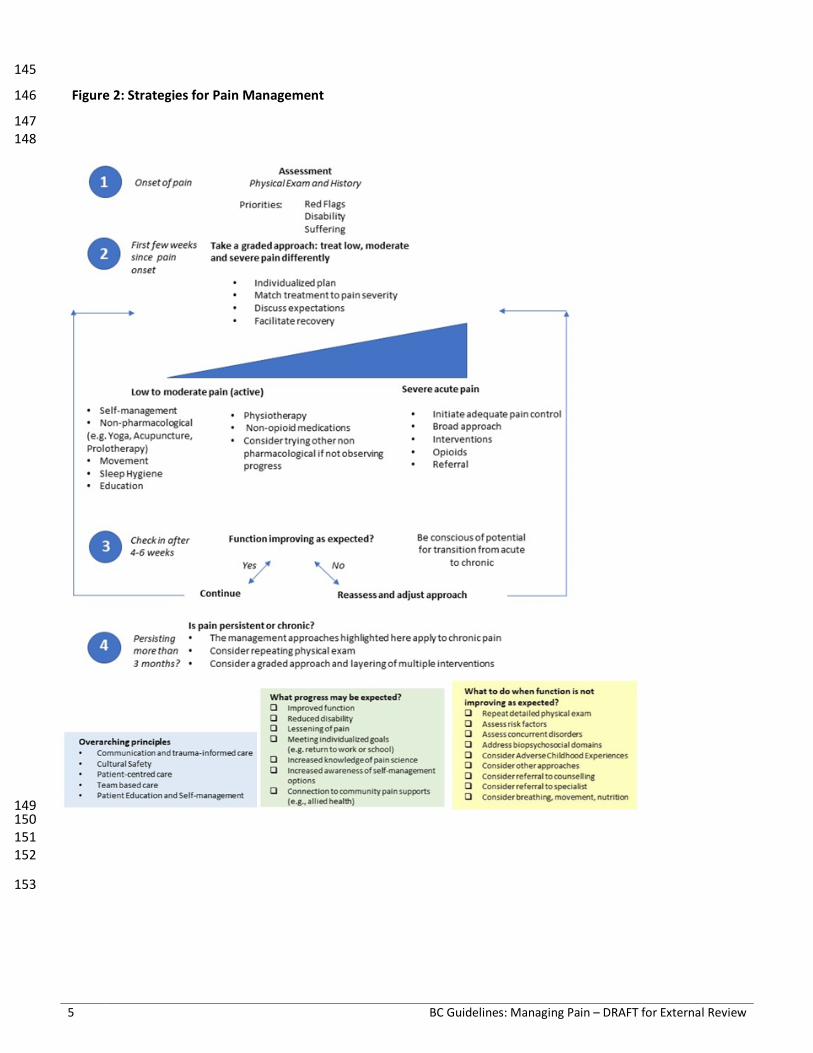
• Assess early for Red Flags. See Table 1: Pain Red Flags below. 160 161
Table 1: Pain Red Flags3 Red Flags suggest a more urgent need for investigations and/or referral (adapted from 162 Centre for Effective Practice ‘Management of Non-Cancer Pain’) 163
164
Functional and Occupational Assessment 165
Support work rehabilitation, occupational review and return to work or education. Explore work accommodation 166 options (e.g. part-time, modified duties) if appropriate rather than complete disability. 167 • For WorkSafeBC and ICBC injuries, consider early intervention support and consultation. 168 • Many occupational groups, employers or insurance companies have occupational health departments and 169
clinician experts. Engage early if complex pain or extended disability is anticipated. 170 Management 171
• Patients with painful acute injury or illness should receive appropriate pain control. See Managing Pain in 172 Primary Care – Part 2: Pharmacological Management. 173
• To help reduce the pain burden consider focusing on medication in the first few weeks. This may allow the 174 patient the time and confidence to begin to engage in other pain treatment modalities that are not medication 175 based. See Appendix B: Non-pharmacological Treatment Modalities for Pain. 176
• Consider non-opioid medications first unless pain is severe. 177 • If considering prescribing opioids, assess for active and past substance use disorder (SUD) (including nicotine, 178
alcohol, opioids, marijuana) and psychiatric disorders. The presence of these disorders is not a reason to not 179
Red Flag Category Clinical Features
Neurological Diffuse motor/sensory loss; progressive neurological deficits; Cauda Equina Syndrome
Infection Fever, chills, weight loss, IV drug use, immunocompromised (including steroids)
Fracture History of physical trauma; minor trauma in elderly or with osteoporosis risk (consider acute vertebral fractures)
Malignancy Past history of cancer; age >50; unexplained weight loss; night pain or supine pain; severe fatigue
Inflammatory Acute monoarthritis; Arteritis-giant cell/temporal; acute vasculitis; acute flare up of connective tissue disease
Vascular History of significant vascular risk factors, clotting disorders, and cardiovascular disease; hemodynamic instability; abdominal pain suggestive of AAA; unilateral limb symptoms including swelling and absence of pulses, coldness
Constitutional Unexplained fever (>38); unexplained weight loss; night sweats
Complex Regional Pain Syndrome (CRPS)
Previously known as Reflex Sympathetic Dystrophy, an evolving CRPS is usually considered an emergency by pain specialists with a strong suggestion for at least a phone consultation and consideration of an urgent referral. While considered rare, it is occasionally progressive involving the arm, leg, hand, or foot. Symptoms may include excessive pain, swelling, and changes in skin colour, texture, and temperature. A subset of patients may benefit from early steroid therapy so again consider an urgent consultation and referral.
7 BC Guidelines: Managing Pain – DRAFT for External Review
prescribe but suggest a need to proceed with caution and to have a clear discussion with patient about risks. 180 Indeed, the presence of any SUD is not a contraindication to prescribe opioids. Untreated pain is also a risk for 181 SUD. 182
• If opioids are prescribed for acute pain, suggest limiting the size of the first prescription of opioids to less than 7 183 days, and use short-acting agents only.4 184
• If patient is not progressing, try alternate interventions and assess if pain is becoming more complex (refer to 185 Subacute section below). 186
Subacute (4 weeks - 3 months) - Transition from acute to chronic pain 187
Assessment 188
If the patient is not progressing as expected after 4-6 weeks (e.g. severe pain, pain is increasingly complex, multiple 189 pain sites), assess for biopsychosocial factors (Yellow Flags) that may indicate risk for developing persistent pain and 190 disability (See Table 2: Yellow Flags). Consider asking “How is the pain affecting the rest of your life?” 191
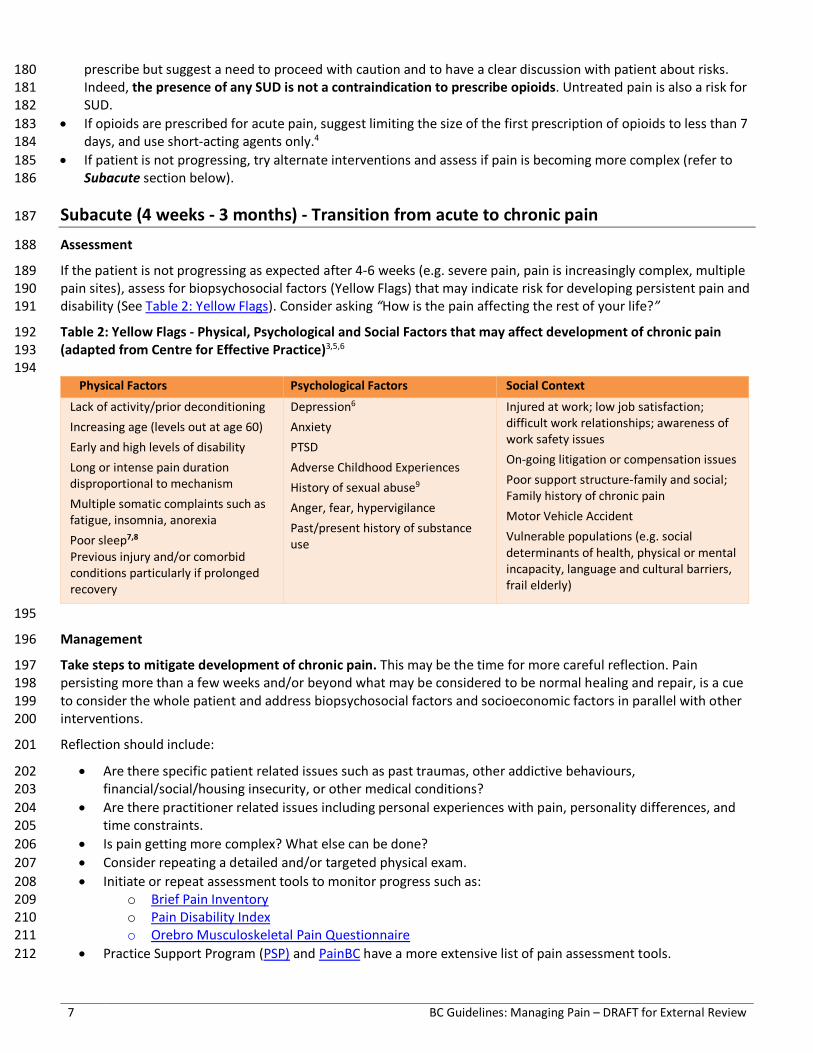
Table 2: Yellow Flags - Physical, Psychological and Social Factors that may affect development of chronic pain 192 (adapted from Centre for Effective Practice)3,5,6 193 194
Physical Factors Psychological Factors Social Context
Lack of activity/prior deconditioning Increasing age (levels out at age 60) Early and high levels of disability Long or intense pain duration disproportional to mechanism Multiple somatic complaints such as fatigue, insomnia, anorexia Poor sleep7,8 Previous injury and/or comorbid conditions particularly if prolonged recovery
Depression6 Anxiety PTSD Adverse Childhood Experiences History of sexual abuse9 Anger, fear, hypervigilance Past/present history of substance use
Injured at work; low job satisfaction; difficult work relationships; awareness of work safety issues On-going litigation or compensation issues Poor support structure-family and social; Family history of chronic pain Motor Vehicle Accident Vulnerable populations (e.g. social determinants of health, physical or mental incapacity, language and cultural barriers, frail elderly)
195
Management 196
Take steps to mitigate development of chronic pain. This may be the time for more careful reflection. Pain 197 persisting more than a few weeks and/or beyond what may be considered to be normal healing and repair, is a cue 198 to consider the whole patient and address biopsychosocial factors and socioeconomic factors in parallel with other 199 interventions. 200
Reflection should include: 201
• Are there specific patient related issues such as past traumas, other addictive behaviours, 202 financial/social/housing insecurity, or other medical conditions? 203
• Are there practitioner related issues including personal experiences with pain, personality differences, and 204 time constraints. 205
• Is pain getting more complex? What else can be done? 206 • Consider repeating a detailed and/or targeted physical exam. 207 • Initiate or repeat assessment tools to monitor progress such as: 208
o Brief Pain Inventory 209 o Pain Disability Index 210 o Orebro Musculoskeletal Pain Questionnaire 211
• Practice Support Program (PSP) and PainBC have a more extensive list of pain assessment tools. 212
BC Guidelines: Managing Pain – DRAFT for External Review 8
• When using the assessment tools, some pain specialists have noted that many patients will label every 213 domain as 10/10. While it may not be an accurate reflection of the actual pain, it may reflect the patient’s 214 overall frustration and hopelessness and should not be dismissed as malingering or over-exaggeration. 215 Consider that multiple pain mechanisms may now be involved in patients experience of pain. 216
• Re-emphasize that total elimination of pain may not be the goal. Improving function and managing suffering 217 are the priorities. Provide information on pain education and self-management. See Resources: Resources for 218 Patients. 219
• If recovery is delayed, refer to specialists for expedited assessment or for specialized treatments or 220 procedures (e.g. epidural or nerve root injections, facet or SI joint injections, joint injections or 221 vertebroplasty). For some conditions such as CRPS and worsening neuropathic pain, referral to specialty 222 services should be as early as possible. This may be especially true in frail older adults as they experience 223 greater functional impairment which can worsen frailty. 224
• As complexity increases, consider combinations of treatments rather than a sequence of treatments. 225 Consider other options, in addition to medications and non-pharmacological interventions. Consider 226 involvement of allied health professionals and/or teams where available. 227
• Explore accommodations for work/school such as the WorkSafeBC Physician's Report. 228 • For patients involved in motor vehicle accidents, who are not recovering as expected or have an unknown 229
diagnosis or complicating factors, consider referral to an ICBC registered care advisor (RCA) within 90 days of 230 the accident for an expedited medical consultation. 231
Chronic pain (3+ months) 232
Assessment 233
It may be worthwhile considering a slightly different approach if the patient has long standing and well documented 234 pain versus the patient who has recently developed chronic pain after an acute event. Many strategies are the same 235 but, a patient with long standing chronic pain may have adapted to achieve some stable level of function and ability, 236 while a patient with new onset of chronic pain may still be uncertain about work options and activities of daily living 237 (ADL) adaptations. 238 239 Evaluating and managing patients with chronic pain requires repeat history and physical exams as well as evaluation 240 of disability and psychosocial domains. This can be beneficial even for long-term patients who appear stable. This 241 process can be conducted over multiple office visits and may at different times include: 242 • Repeat / review history, physical exam 243 • Consider asking yourself: 244
1. What is going on? 245 2. Could it be something else? 246 3. Could two things be going on at once? 247 4. Is the diagnosis still supported by the available evidence? 248
• Review medication history including OTC and “off label” products (including use of cannabis) 249 • Repeat / review pain assessment tools, including functional and occupational assessments 250 • Assess / reassess for mental health conditions (e.g. use screening tools for anxiety, depression, PTSD). 251
Both chronic pain and depression may frequently co-exist, especially in old age, and may be risk factors for 252 each other10. Consider exploring other life changes as possible contributors to depression and/or pain 253 symptoms. What other things are going on in your life?” 254
• Assess / reassess concurrent disorders and other medical conditions: 255 o Substance use disorders (e.g. opioid, alcohol) 256 o Sleep disorders 257 o Chronic diseases (diabetes, chronic heart failure, obesity, cancer, osteoporosis) 258 o Falls and falls risks, especially in frail elderly (refer to BCGuidelines: Falls Prevention) 259 o Polypharmacy including OTC medications 260
9 BC Guidelines: Managing Pain – DRAFT for External Review
o Cognitive and/or sensory impairment 261 • Assess / reassess risk factors and biopsychosocial domains (Red and Yellow Flags) 262 • Consider referral to specialists or allied healthcare. 263 • Consider strategies such as breathing, movement, and nutrition. All strategies may add to the layering effect 264
that improves function and reduces suffering and disability. See Appendix B: Non-pharmacological Treatment 265 Modalities for Pain. 266
267
Management 268
• Match non-pharmacological interventions that are best suited to patient’s specific pain mechanism and history, 269 such as physiotherapy or chiropractic therapy for mechanical low back pain (LBP); psychological intervention if 270 there is a possible history of PTSD or ACEs; Cognitive Behavioural Therapy (CBT) for depression and anxiety; 271 and social work or occupational therapy if housing/financial/job insecurity are present. Using a layered and 272 multimodal approach may be more effective than trying a single intervention at a time. 273
• Discuss goals of care. Specifically, improved function, reduced suffering, patient’s other individual goals and not 274 necessarily removal of all pain. 275
• Review patient expectations for treatment outcomes and address misconceptions or unrealistic expectations. 276 • Over multiple visits, develop an Individualized Care Plan or chronic pain flow sheet3 to encourage a better 277
system approach to chronic pain. Share and review the plan with the patient. 278 • Provide guidance for practical steps that can be addressed in next visit. 279 • If a patient has been adherent to therapy for 3-4 months and is not responding, consider an alternative 280
approach. 281 • Educate patients about chronic pain and the multidimensionality of pain. See Resources : Resources for 282
Patients. It is often assumed that tissue damage will continue to heal, but there may be other interfering 283 factors. 284
• Educate patients that non-opioid treatment gives equal pain control and fewer side effects than opioid 285 treatment for most types of chronic LBP and knee and hip arthritic pain.11 286
• Educate patients that opioid use may increase pain sensitivity and add to pain at injury sites during 287 withdrawal.12,13 288
• Best practice treatment plans involve primary care providers working closely with allied health care providers, 289 including physiotherapists, occupational therapists, psychologists, chiropractors, massage therapists, and social 290 workers, and should be centred around patient education and self-management. Most of the services are not 291 covered directly by MSP, however, explore possible coverage through ICBC, Worksafe BC and patient’s work 292 disability services. Refer to Pain BC and PathwaysBC for listings of providers, self-management groups and 293 clinics with experience and training in managing chronic pain. 294
Procedural Treatment for patients with pain in primary care settings 295
Within the context of primary care, there are a number of procedures that can be within the scope of most 296 clinicians. These may include: 297
• Trigger point injections 298 • Bursa injections 299 • Intra-articular injections excluding the hip and intra-articular glenohumeral joints 300 • Mid-sized peripheral nerve blocks 301
These procedures generally don’t require imaging, can be performed in an office setting and are not restricted to an 302 accredited facility. It is beyond the scope of this guideline to describe these procedures in detail and their 303 indications, but they tend to be self-explanatory and a number of online instruction resources exist. 304 For more complex procedures (e.g. intra articular hip and shoulder injections, epidural injections) the CPSBC has 305 described these procedures as Advanced Level I and II, which are required to be done in an approved facility. Refer 306 to the CPSCBC website for more information. 307
BC Guidelines: Managing Pain – DRAFT for External Review 10
Substance Use Reduction 308
A number of different psychoactive substances have been shown to temporarily supress pain perception in the 309 euphoric phase (the reason the patient with pain may like the feel of the substance). Yet, these same substances can 310 increase pain sensitivity and add to chronic pain in the long run. Alcohol, tobacco, and opioids are all examples.13–16 311 Patient education on this topic then a trial of tapering down or off of these substances may be needed to help pain 312 perception. In those with CNCP, opioids can produce a dose-dependent pain sensitization that temporarily worsens 313 during tapering.12,17,18 For those with chronic pain or an opioid use disorder, previous injury sites can hurt again 314 during abrupt withdrawal and add to the risk of opioid re-initiation. Thus, slow tapering along with the use of 315 adjuvant medications like NSAIDS or gabapentinoids may be helpful in adults. This does not include tapering 316 previously stable OAT or opioids used for the treatment of OUD. 317
Supported Self-Management 318 • Provide or refer patient to educational resources about science of pain. Pain education has been shown to 319
decrease disability and increase self-efficacy.19 Refer to Resources: Resources for Patients for helpful resources. 320 • Provide patient with information about self-management (including focused breathing, nutrition, gentle 321
movement, mindfulness meditation, sleep hygiene) connecting to additional support (community physical 322 activity programs, dietitians) 323
• Consider goal setting, including return to work and Brief Action Planning (BAP). 324
Allied Health Professionals to support non-pharmacological pain management 325 Pain BC has developed an overview of Allied Health Approaches To Chronic Pain Management-A Tool For 326 Primary Care Providers. Many non-pharmacological interventions may be partially or fully covered by third party 327 insurers, ICBC or WorkSafe, or if patient is on disability or income assistance. See Appendix C: Allied Health 328 Professionals to Support Pain Management for more details on allied practitioners. 329
Considerations for Referral or Request for Expert Input 330
When patients DO NOT experience ongoing improvement in function and decrease in suffering then consider: 331 • Consultation with an appropriate specialist 332 • Structural cause such as a compression fracture 333 • Psychological services if history of PTSD or ACEs or catastrophizing 334 • Pain clinic if pain appears to have a nociplastic component 335
336 Guiding principles for referral or request for expert input. 337
• Not seeing appropriate progress and pain looks likely to persist longer than expected 338 • Neuropathic features develop, persist or worsen. 339 • Post-op patients unable to reduce or discontinue opioid use. 340 • If patient is continuing to show biopsychosocial factors that increase risk of progression to chronic pain. 341 • Complex Regional Pain Syndrome-CRPS. Some pain specialists suggest that the emergence of CRPS 342
symptoms warrants at least a phone consultation to assess the need for urgent referral. If WorkSafe or ICBC 343 involved, phone the worker’s medical advisor and ask for an expedited appointment. 344
• If an interventional or surgical procedure is likely. 345 • If chronic non-cancer pain and OUD coexist a referral to an addiction specialist is warranted. 346
Managing Pain in the Older Adult 347
Managing pain in the “Older Adult”, especially the Frail Older Adult, often requires modifications and adjustments in 348 both approach and dosages. While there is no specific definition of the Older Adult, many experts suggest that age 349 greater than 70 may be an appropriate age to consider age related factors in assessing and managing pain. The 350 definition of frailty is still being fully defined but its current definition is a medical syndrome with multiple causes 351
11 BC Guidelines: Managing Pain – DRAFT for External Review
and contributors, characterized by diminished strength and endurance and reduced physiological function, leading 352 to increased vulnerability for adverse health outcomes such as functional decline and early mortality. While frailty is 353 common with increasing age, it is not an inevitable part of aging. Additional information about Healthy Aging and 354 Preventing Frailty, can be found in the updated provincial healthy aging strategy. 355 Guiding Principles: 356 • The frail older adult may require adjustments in medications and dosages, but the use of opioids is not 357
contraindicated. See Part 2: Pharmacological Treatment for more specific guidance. 358 • Persistent pain in frail older adults increases morbidity and poor health outcomes, making treatment a priority. 359 • Multiple morbidity, cognitive impairment and altered pharmacokinetics and dynamics mandate an individual 360
approach. Some basic bloodwork including renal function may be appropriate in the initial assessment phase 361 and intermittently if the use of medication persists. 362
• As cognition worsens, pain is less likely to be reported and may manifest as other distress behaviours 363 (agitation, resisting care, insomnia, poor appetite). 364
• Older adults are more likely to be taking multiple medications (polypharmacy) and have co-morbidities, 365 therefore, assess individual patients for drug and disease interactions when prescribing NSAIDs and other 366 medications. 367
• Risk of falls is elevated. However, pain and decreased attention or poor sleep due to chronic pain can also 368 increase the risk of falls. Monitoring the increased risk for managing pain in the elderly is necessary to reduce 369 suffering and increased function. 370
371
References 372
1. Canada H. Canadian Pain Task Force Report: March 2021 [Internet]. 2021 [cited 2021 Jun 17]. Available from: https://www.canada.ca/en/health-373 canada/corporate/about-health-canada/public-engagement/external-advisory-bodies/canadian-pain-task-force/report-2021.html 374
2. Schopflocher D, Taenzer P, Jovey R. The prevalence of chronic pain in Canada. Pain Res Manag. 2011 Dec;16(6):445–50. 375 3. Centre for Effective Practice. (Updated May 2018). Management of Chronic Non-Cancer Pain (CNCP): Ontario. Toronto: Centre for Efective Practice. 376 4. Ccfp CK, Perry D, Ton J, Ccfp MRK, Ccfp SG, BScPharm BT, et al. Managing opioid use disorder in primary care. :10. 377 5. Kendall NAS, Linton SJ, Main C. Psychosocial Yellow Flags for acute low back pain: ‘Yellow Flags’; as an analogue to ‘Red Flags’; Eur J Pain. 1998 378
Mar;2(1):87–9. 379 6. Hruschak V, Cochran G. Psychosocial predictors in the transition from acute to chronic pain: a systematic review. Psychol Health Med. 380
2018;23(10):1151–67. 381 7. Olson KA, PhD. Pain and Sleep: Understanding the Interrelationship [Internet]. Practical Pain Management. [cited 2021 Jan 15]. Available from: 382
https://www.practicalpainmanagement.com/pain/other/co-morbidities/pain-sleep-understanding-interrelationship 383 8. Pain and Sleep: Common Sleep Disturbances & Tips [Internet]. Sleep Foundation. [cited 2021 Jan 15]. Available from: 384
https://www.sleepfoundation.org/physical-health/pain-and-sleep 385 9. Spiegel DR, Shaukat AM, Mccroskey AL, Chatterjee A, Ahmadi T, Simmelink D, et al. Conceptualizing a subtype of patients with chronic pain: The 386
necessity of obtaining a history of sexual abuse. Int J Psychiatry Med. 2016;51(1):84–103. 387 10. Zis P, Daskalaki A, Bountouni I, Sykioti P, Varrassi G, Paladini A. Depression and chronic pain in the elderly: links and management challenges. Clin Interv 388
Aging. 2017;12:709–20. 389 11. Krebs EE, Gravely A, Nugent S, Jensen AC, DeRonne B, Goldsmith ES, et al. Effect of Opioid vs Nonopioid Medications on Pain-Related Function in 390
Patients With Chronic Back Pain or Hip or Knee Osteoarthritis Pain: The SPACE Randomized Clinical Trial. JAMA. 2018 Mar 6;319(9):872–82. 391 12. Rieb LM, Norman WV, Martin RE, Berkowitz J, Wood E, McNeil R, et al. Withdrawal-associated injury site pain (WISP): a descriptive case series of an 392
opioid cessation phenomenon. Pain. 2016;157(12):2865–74. 393 13. Rivat C, Ballantyne J. The dark side of opioids in pain management: basic science explains clinical observation. Pain Rep [Internet]. 2016 Sep 8 [cited 394
2020 Nov 24];1(2). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5741356/ 395 14. Apkarian AV, Neugebauer V, Koob G, Edwards S, Levine JD, Ferrari L, et al. Neural mechanisms of pain and alcohol dependence. Pharmacol Biochem 396
Behav. 2013 Nov;112:34–41. 397 15. Baiamonte BA, Valenza M, Roltsch EA, Whitaker AM, Baynes BB, Sabino V, et al. Nicotine dependence produces hyperalgesia: role of corticotropin-398
releasing factor-1 receptors (CRF1Rs) in the central amygdala (CeA). Neuropharmacology. 2014 Feb;77:217–23. 399 16. Egli M, Koob GF, Edwards S. Alcohol dependence as a chronic pain disorder. Neurosci Biobehav Rev. 2012 Nov;36(10):2179–92. 400 17. Rieb LM, DeBeck K, Hayashi K, Wood E, Nosova E, Milloy M-J. Withdrawal-associated injury site pain prevalence and correlates among opioid-using 401
people who inject drugs in Vancouver, Canada. Drug Alcohol Depend. 2020 Nov 1;216:108242. 402 18. Associations between Heat Pain Perception and Opioid Dose among Patients with Chronic Pain Undergoing Opioid Tapering. :12. 403 19. Louw A, Nijs J, Puentedura EJ. A clinical perspective on a pain neuroscience education approach to manual therapy. J Man Manip Ther. 2017 404
Jul;25(3):160–8. 405 20. Mistiaen P, van Osch M, van Vliet L, Howick J, Bishop FL, Di Blasi Z, et al. The effect of patient-practitioner communication on pain: a systematic review. 406
Eur J Pain. 2016 May;20(5):675–88. 407 21. Van der Kolk BA, Ducey CP. The psychological processing of traumatic experience: Rorschach patterns in PTSD. J Trauma Stress. 1989;2(3):259–74. 408 22. Trauma-Informed Practice Guide [Internet]. 2013 [cited 2019 Nov 14]. Available from: http://bccewh.bc.ca/wp-content/uploads/2012/05/2013_TIP-409
Guide.pdf 410 23. Skelly AC, Chou R, Dettori JR, Turner JA, Friedly JL, Rundell SD, et al. Noninvasive Nonpharmacological Treatment for Chronic Pain: A Systematic Review 411
BC Guidelines: Managing Pain – DRAFT for External Review 12
Update [Internet]. Agency for Healthcare Research and Quality (AHRQ); 2020 Apr [cited 2021 May 5]. Available from: 412 https://effectivehealthcare.ahrq.gov/products/noninvasive-nonpharm-pain-update/research 413
24. Brain K, Burrows TL, Rollo ME, Chai LK, Clarke ED, Hayes C, et al. A systematic review and meta-analysis of nutrition interventions for chronic noncancer 414 pain. J Hum Nutr Diet. 2019 Apr;32(2):198–225. 415
25. Rondanelli M, Faliva MA, Miccono A, Naso M, Nichetti M, Riva A, et al. Food pyramid for subjects with chronic pain: foods and dietary constituents as 416 anti-inflammatory and antioxidant agents. Nutr Res Rev. 2018 Jun;31(1):131–51. 417
26. Guo R, Chen L-H, Xing C, Liu T. Pain regulation by gut microbiota: molecular mechanisms and therapeutic potential. Br J Anaesth. 2019 Nov 418 1;123(5):637–54. 419
27. Cheatle MD, Foster S, Pinkett A, Lesneski M, Qu D, Dhingra L. Assessing and Managing Sleep Disturbance in Patients with Chronic Pain. Anesthesiol Clin. 420 2016 Jun 1;34(2):379–93. 421
28. Jafari H, Courtois I, Van den Bergh O, Vlaeyen JWS, Van Diest I. Pain and respiration: a systematic review. PAIN. 2017 Jun;158(6):995–1006. 422 29. Busch V, Magerl W, Kern U, Haas J, Hajak G, Eichhammer P. The effect of deep and slow breathing on pain perception, autonomic activity, and mood 423
processing--an experimental study. Pain Med Malden Mass. 2012 Feb;13(2):215–28. 424 30. Hilton L, Hempel S, Ewing BA, Apaydin E, Xenakis L, Newberry S, et al. Mindfulness Meditation for Chronic Pain: Systematic Review and Meta-analysis. 425
Ann Behav Med. 2017 Apr;51(2):199–213. 426 31. Majeed MH, Ali AA, Sudak DM. Mindfulness-based interventions for chronic pain: Evidence and applications. Asian J Psychiatry. 2018 Feb;32:79–83. 427 32. Geneen LJ, Moore RA, Clarke C, Martin D, Colvin LA, Smith BH. Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews. 428
Cochrane Database Syst Rev. 2017 14;1:CD011279. 429 33. Bidonde J, Busch AJ, Webber SC, Schachter CL, Danyliw A, Overend TJ, et al. Aquatic exercise training for fibromyalgia. Cochrane Musculoskeletal Group, 430
editor. Cochrane Database Syst Rev [Internet]. 2014 Oct 28 [cited 2019 Oct 1]; Available from: http://doi.wiley.com/10.1002/14651858.CD011336 431 34. Bidonde J, Busch AJ, Schachter CL, Webber SC, Musselman KE, Overend TJ, et al. Mixed exercise training for adults with fibromyalgia. Cochrane 432
Musculoskeletal Group, editor. Cochrane Database Syst Rev [Internet]. 2019 May 24 [cited 2019 Oct 1]; Available from: 433 http://doi.wiley.com/10.1002/14651858.CD013340 434
35. Bidonde J, Busch AJ, Schachter CL, Overend TJ, Kim SY, Góes SM, et al. Aerobic exercise training for adults with fibromyalgia. Cochrane Musculoskeletal 435 Group, editor. Cochrane Database Syst Rev [Internet]. 2017 Jun 21 [cited 2019 Oct 1]; Available from: 436 http://doi.wiley.com/10.1002/14651858.CD012700 437
36. Hurley M, Dickson K, Hallett R, Grant R, Hauari H, Walsh N, et al. Exercise interventions and patient beliefs for people with hip, knee or hip and knee 438 osteoarthritis: a mixed methods review. Cochrane Database Syst Rev. 2018 17;4:CD010842. 439
37. Chronic Pain and exercise, Exercise Is Medicine Australia Factsheet, 2014, http://exerciseismedicine.com.au/wp-content/uploads/2018/06/2014-440 Chronic-Pain-FULL-1.pdf. 441
38. Nielsen A, Wieland LS. Cochrane reviews on acupuncture therapy for pain: A snapshot of the current evidence. EXPLORE. 2019 Nov 1;15(6):434–9. 442 39. Acupuncture for neuropathic pain in adults [Internet]. [cited 2020 Dec 9]. Available from: /CD012057/SYMPT_acupuncture-neuropathic-pain-adults 443 40. Lee MS, Ernst E. Acupuncture for pain: an overview of Cochrane reviews. Chin J Integr Med. 2011 Mar;17(3):187–9. 444 41. Acupuncture for Chronic Non-Cancer Pain: A Review of Clinical Effectiveness, Cost Effectiveness and Guidelines [Internet]. CADTH.ca. 2019 [cited 2021 445
May 5]. Available from: https://www.cadth.ca/acupuncture-chronic-non-cancer-pain-review-clinical-effectiveness-cost-effectiveness-and-0 446 447
Practitioner Resources 448
• Pathways is Division of Family Practice Resource that provides access to referral information as well as 449 patient and physician resources and local community resources. Available at https://pathwaysbc.ca/login. 450 Pain Management resources video at Pathways is available at https://vimeo.com/528999461 451
• RACE line Available at http://www.raceconnect.ca/. Pain is not listed as a specific speciality area, however, 452 consider a RACE consult to a specialist if the pain is related to a specific specialty area. There is a provincial 453 line for Addictions Medicine that can respond to questions related to co-occurring pain and opioid use 454 disorder. Specialist Pain Clinics (Health Authority and Private clinics) can be found on PathwaysBC. 455
• WorkSafe BC Physician’s Hotline 1-855-476-3049 to speak with an agent about access to WorkSafeBC funded 456 programs including the following: Occupational Rehabilitation (OR1 and 2); Pain and Medication 457 Management Program (PMMP); Resiliency over perceived trauma (ROPT); Community Pain and Addiction 458 Services (CPAS). 459
• ICBC: Claims 460
• Self-Management BC is part of University of Victoria’s Institute on Aging & Lifelong Health and is supported 461 by the Patients as Partners Initiative Primary Care Division, B.C. Ministry of Health. It offers three peer-462 delivered chronic pain programs free to British Columbia residents. A description of each program can be 463 accessed at www.selfmanagementbc.ca 464
The Chronic Pain Self-Management Program 465 Tool Kit for Active Living with Chronic Pain 466 The Self-Management Health Coach Program 467
13 BC Guidelines: Managing Pain – DRAFT for External Review
Resources for Patients 468
• Pain BC 469
Support and Information for Patients and Caregivers 470 Coaching for Health – individual phone coaching, free service. Requires MD referral. 471 Pain Support Line, Patient Education and more: 472 Find Help Near You – - includes listings of providers, self management groups and clinics with 473
experience and training in managing chronic pain 474 Pain BC’s Live Plan Be 475 Chronic Pain Road Map 476
• Self-Management BC (www.selfmanagementbc.ca) 477 The Chronic Pain Self-Management Program 478 The Chronic Pain Toolkit and Calls program 479 The Telephone Self-Management Health Coach Program 480
• AnxietyBC 481
• Toronto Academic Pain Medicine Institute 482
• Wellness Together Canada 483
• Youtube videos on pain are available including: Explain pain in 5 minutes, What is chronic pain?, Why things 484 hurt?, Pain, Is it all in your mind?, Treating Pain Using the Brain. 485
• HealthLinkBC 486
Chronic Pain 487 Insomnia: Improving your sleep 488 Stress Management: Breathing Exercises for Relaxation 489 Physical Activity Line – Call 8-1-1 to speak to a qualified exercise professional 490 Dietitians – Call or Email to speak to a registered dietitian 491
• Work Wellness and Disability Prevention Institute 492 • Self Management apps 493 mySleepButton “mySleepButton is an app designed to help you fall asleep. It’s based on our 494
contribution to cognitive science. Just press the “Put Me to Sleep” button, close your eyes, and imagine 495 the various things mySleepButton reads to you as you fall asleep.” 496
MindShift “MindShift CBT uses scientifically proven strategies based on Cognitive Behavioural Therapy 497 (CBT) to help you learn to relax and be mindful, develop more effective ways of thinking, and use active 498 steps to take charge of your anxiety.” 499
Woebot “Woebot sends over a Million messages per week to help users with everyday stress and 500 challenges such as symptoms of depression, anxiety, relationship problems, procrastination, loneliness, 501 grief, addiction, pain management and more! Woebot checks-in with you every day and guides you 502 through practical techniques based on tried and tested approaches such as Cognitive Behavioral Therapy 503 (CBT), Mindfulness, and Dialectical Behavior Therapy (DBT).” 504
Calm.com “Calm is the #1 app for meditation and mindfulness. Enjoy 100+ guided meditations to help 505 you manage anxiety, lower stress and sleep better.” 506
Curable app “an online pain psychology program. The entire program takes place online via a personal 507 computer, tablet device, or smartphone and is delivered via a virtual pain coach.” 508
Appendices 509 Appendix A: Overarching Considerations of Pain Management 510 Appendix B: Non-pharmacological Treatment Modalities for Pain 511 Appendix C: Allied Health Professionals to Support Pain Management 512
BC Guidelines: Managing Pain – DRAFT for External Review 14
This guideline is based on scientific evidence current as of the effective date. 513
The guideline was developed by the Guidelines and Protocols Advisory Committee and would be adopted by the 514 Medical Services Commission. 515
For more information about how BC Guidelines are developed, refer to the GPAC Handbook available at 516 BCGuidelines.ca: GPAC Handbook. 517
518
519
THE GUIDELINES AND PROTOCOLS ADVISORY COMMITTEE 520
The principles of the Guidelines and Protocols Advisory Committee are to: • encourage appropriate responses to common medical situations • recommend actions that are sufficient and efficient, neither excessive nor deficient • permit exceptions when justified by clinical circumstances
Contact Information: Guidelines and Protocols Advisory Committee PO Box 9642 STN PROV GOVT Victoria, BC V8W 9P1 Email: [email protected] Website: www.BCGuidelines.ca
Disclaimer
The Clinical Practice Guidelines (the “Guidelines”) have been developed by the Guidelines and Protocols Advisory Committee on behalf of the Medical Services Commission. The Guidelines are intended to give an understanding of a clinical problem, and outline one or more preferred approaches to the investigation and management of the problem. The Guidelines are not intended as a substitute for the advice or professional judgment of a health care professional, nor are they intended to be the only approach to the management of clinical problem. We cannot respond to patients or patient advocates requesting advice on issues related to medical conditions. If you need medical advice, please contact a health care professional.
521
15 BC Guidelines: Managing Pain – DRAFT for External Review
Appendix A: Overarching Considerations of Pain Management 522
Communication and Relationship Building 523
Self-reflection and learning 524 o Reflect on potential bias or stigma related to treating complex pain patients. Treating patients with complex 525
pain is challenging and can be frustrating. Recognize your own triggers and be aware of one’s own bias towards 526 people in pain in general and specific patients in pain. Consider strategies for responding in a way that can 527 create more successful relationships. 528
o Reflect on your current pain management practices and consider both new 529 approaches and the reassessment of previous strategies that may have been 530 less effective. Be conscious of slowing down, listening and taking time with 531 people with pain. The extra time needed at the start can decrease time in the 532 future. (Maintaining a “remote, non-reactive” demeanour, or the opposite of 533 an overtly engaged desire to eliminate all pain and suffering may be an 534 example of an approach that could influence management). 535 Reflect on the barriers preventing early referral. 536 Reflect on proactive measure for ‘pre-pain’ symptoms like stiffness, swelling, ‘mild pain,’ self-resolved but 537
intermittent pain. 538 o Learn about pain science and new approaches to pain management 539
Refer to UBC CPD Practice Support Program, PainBC, Pain BC – Pain Foundations Online course, and the BC 540 ECHO for chronic pain 541
Therapeutic Relationship 542 Supportive patient-provider relationships that are empathetic, are culturally safe, promote positive 543 expectations, and provide information in advance of procedures ( e.g. what to expect and how to recover) 544 may have a small but positive effect on acute pain.20 545
Consider a trauma-informed approach for all patients, regardless of their trauma history 546 o In this case, trauma is defined as the psychological effects of a life event (or events) that is/are out of an 547
individual’s control and overwhelms an individual’s capacity to cope.21,22 As such, trauma refers to the 548 psychological impact of events rather than to the acute physical trauma (e.g. car accident). 549
o The aim of trauma-informed practice recognizes the impact on health and uses a strengths-based approach to 550 build a safe, trusting and collaborative relationship between patient and provider. 551
o Consider reframing your perspective. Practitioners who apply a trauma-informed approach may find it helpful to 552 think ‘What happened to you?’ when reflecting on complex, challenging patients instead of ‘What’s wrong with 553 you?’. 554
o Refer to BC Guideline: Adverse Childhood Experiences (ACEs) and Trauma-Informed Practice [in development] 555 and BC Trauma-Informed Practice Guide for more information about trauma-informed practice. The learning 556 module addresses strategies primary care providers can use to identify patients who have been impacted by 557 trauma, to provide additional support, and to help patients build resilience. 558
o Recognize the patient as an expert in their pain. Consider a person-centred approach to empower patients. 559 o Focus on actively listening to and validating the patient’s experience of pain. 560 o Use evidence-informed tools to assess the level of suffering and disability that the patient with pain is 561
experiencing. 562 o Engage the patient in shared decision making and work together to integrate the values, goals, and concerns of 563
the patient with the best available evidence about the benefits, risks of the treatment and/or care. The 564 objective advice and expertise of the practitioner and the preferences of the patients should work in a 565 complimentary manner to achieve an optimal decision to decrease suffering, improve function, and general 566 wellbeing. 567
“You can’t expect different results if you keep acting and reacting the same way”
BC Guidelines: Managing Pain – DRAFT for External Review 16
o Collaboratively support patient with pain’s choice in their self-management strategies. 568
Team Based Care 569 o Pain management benefits from a multimodal approach (receiving multiple interventions at the same time e.g. 570
yoga, physiotherapy, occupational therapy, counselling, medication). 571 o Get to know pain practitioners in your local community who have training in the management of people with 572
pain and build a network of resources, including low and no cost options and awareness of financial supports. 573 Consider connecting with providers whom the patient has identified as part of their care team or recommend a 574 local practitioner from your network. We acknowledge that access to care may be limited by geography and 575 resources. 576
o Team members may include pharmacists, physiotherapists, massage therapists, acupuncturists, chiropractors, 577 osteopaths, occupational therapists, counsellors, social workers, lifestyle coaches, support for substance use 578 and mental health, psychologists, cognitive behavioural therapists, indigenous cultural and wellness supports, 579 dietitians and qualified exercise professionals. Team members can also be your own office staff, who may assist 580 with assessment using various tools such as the brief pain inventory and the pain disability index. This can make 581 this complex and sometimes challenging care more manageable. 582
o Refer to Health Link BC (8-1-1), Pathways, or Pain BC for local practitioners and resources. Check the scope of 583 the organization to ensure proper referral. Refer to Health Link BC (8-1-1) where providers and patients can 584 speak with dietitians and qualified exercise professionals. Pain BC support line can help identify local pain 585 providers including practitioners who can provide guidance and support for self-management. 586
o Involve caregiver/family members as part of the team for frail older adults in pain, particularly if there is 587 cognitive impairment present. 588
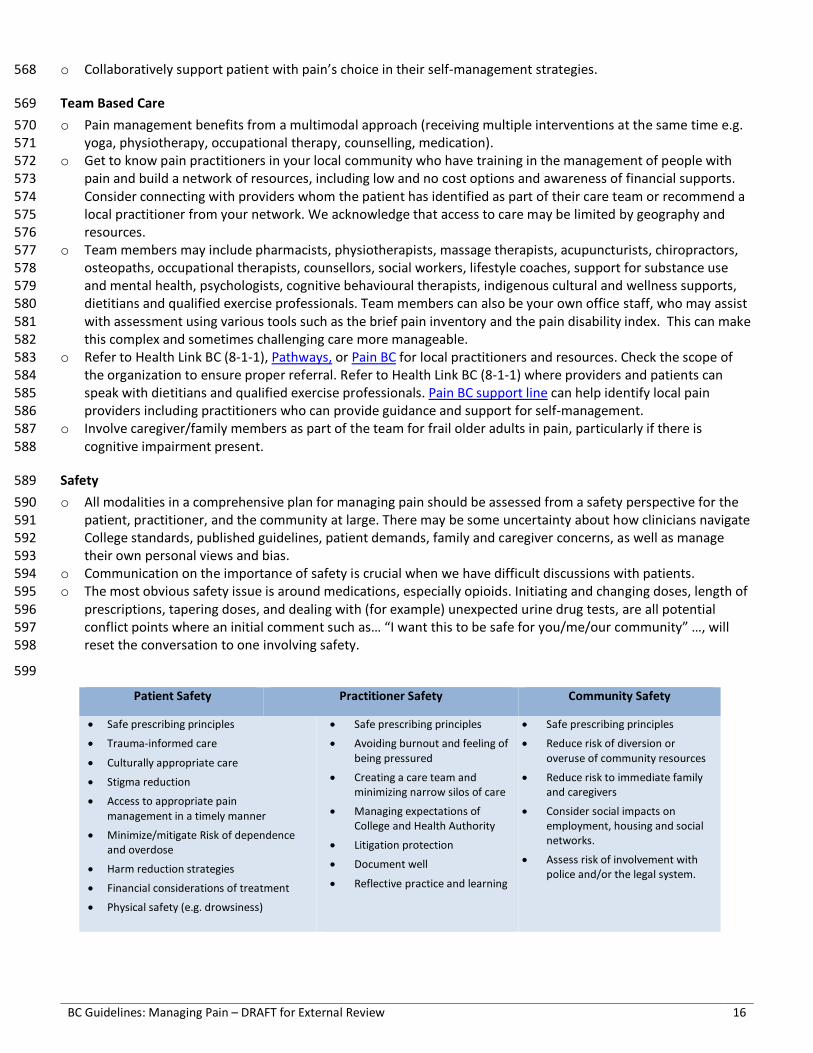
Safety 589 o All modalities in a comprehensive plan for managing pain should be assessed from a safety perspective for the 590
patient, practitioner, and the community at large. There may be some uncertainty about how clinicians navigate 591 College standards, published guidelines, patient demands, family and caregiver concerns, as well as manage 592 their own personal views and bias. 593
o Communication on the importance of safety is crucial when we have difficult discussions with patients. 594 o The most obvious safety issue is around medications, especially opioids. Initiating and changing doses, length of 595
prescriptions, tapering doses, and dealing with (for example) unexpected urine drug tests, are all potential 596 conflict points where an initial comment such as… “I want this to be safe for you/me/our community” …, will 597 reset the conversation to one involving safety. 598
599
Patient Safety Practitioner Safety Community Safety
• Safe prescribing principles
• Trauma-informed care
• Culturally appropriate care
• Stigma reduction
• Access to appropriate pain management in a timely manner
• Minimize/mitigate Risk of dependence and overdose
• Harm reduction strategies
• Financial considerations of treatment
• Physical safety (e.g. drowsiness)
• Safe prescribing principles
• Avoiding burnout and feeling of being pressured
• Creating a care team and minimizing narrow silos of care
• Managing expectations of College and Health Authority
• Litigation protection
• Document well
• Reflective practice and learning
• Safe prescribing principles
• Reduce risk of diversion or overuse of community resources
• Reduce risk to immediate family and caregivers
• Consider social impacts on employment, housing and social networks.
• Assess risk of involvement with police and/or the legal system.
17 BC Guidelines: Managing Pain – DRAFT for External Review
Appendix B: Non-pharmacological Treatment Modalities for Pain 600
Lifestyle Interventions and Strategies23 601 A good overall management tool for non-pharmacological management can be found at the CEP Management of 602 Chronic Non-Cancer Pain: Non-Pharmacological Therapies. 603
Nutritional Support 604 o Nutrition plays a key role in fighting infection, healing, managing chronic conditions that involve pain, and 605
optimizing overall health and well-being.24,25 The evidence base for therapeutic diets varies depending on the 606 condition. 607
o Emerging research suggests an association between some chronic pain conditions such as fibromyalgia and a 608 disordered gut “microbiome” (the totality of microorganisms including bacteria, viruses, protozoa and fungi). 609 Understanding of the role of gut microbiota in pain is still in the early stages with varying levels of support, 610 though emerging evidence suggests that dysregulation of gut microbiota participates in visceral pain, 611 inflammatory pain, neuropathic pain, migraine and opioid tolerance26. 612
o Consider the impact of acute and chronic pain on the patient’s ability to plan, shop for, and prepare healthy 613 meals. Pain can also impact appetite, dietary intake, and nutritional status. 614
o Registered Dietitians at HealthLinkBC (8-1-1) offer nutrition assessments, advice and guidance, counselling, care 615 plans and therapeutic diets care coordination. 616
Sleep 617 There is increasing evidence that pain and sleep have a bidirectional relationship. Poor sleep commonly occurs 618 in those with chronic pain and may in turn lead to additional fatigue and exacerbate pain.27 both non-619 pharmacological and pharmacological interventions can help those with pain obtain a better sleep.8,27 When 620 appropriate assess for obstructive sleep apnea. 621
Breath 622 Pain, especially acute pain, can cause breath holding and hyperventilation which may accentuate the pain. More 623 consideration is now being given to the importance of “breath work” as an integral component of self-624 management of pain.28,29 While the exact mechanism is not well understood, the effect of “paced slow deep 625 breathing” on vagal nerve stimulation may contribute to modulating pain as well as improving the V/Q match 626 and improving oxygenation. See Resources: Resources for Patients for breathing techniques and integration with 627 meditation and yoga practices. 628
Mindfulness-Based Interventions 629 o Mindfulness meditation is demonstrated to work by paying attention, on purpose, in the present moment and 630
non-judgementally, and increasing awareness of one’s external surroundings and inner sensations, allowing the 631 individual to step back and reframe experiences.30 Clinical use of mindfulness has included applications in 632 substance use disorders, tobacco cessation, stress reduction, and treatment of chronic pain.30 The goal of this 633 approach is to reduce pain, increase functioning and improve the quality of life, by empowering the patient with 634 skills to live a productive life despite the presence of discomfort or disability. 635
o Multiple reviews of mindfulness interventions suggest the quality of evidence varies considerably depending on 636 the outcome of interest.30,31 637
o Refer to Pain Education material on Pain BC’s Live Plan Be or the Toronto Academic Pain Medicine Institute for 638 information on mind-body therapies and techniques. 639
Physical Activity and Therapeutic Movement 640 o Recent systematic reviewers suggest physical activity alone can decrease severity of pain and improve physical 641
function in adults with chronic non-cancer pain.32 . It can improve symptoms of stiffness33, fatigue34, health-642 related fitness33, and/or quality of life34,35 in those with fibromyalgia, and depression as well as self-efficacy and 643

BC Guidelines: Managing Pain – DRAFT for External Review 18
social function for patients with chronic hip and knee pain from osteoarthritis36. 644 o The main goal is restoration of movement and activity. There is no optimal type of physical activity for chronic 645
pain,37 and interventions should be individualized. 646 o Spending time in nature has a wide range of positive effects on human health. A BC specific program in 647
conjunction with BC Parks Foundation called PaRx encourages clinicians to formally prescribes time in nature. 648 o Consider referring to allied health care providers, especially those with expertise in exercise prescription for 649
chronic pain conditions, for customized, supervised, physical activity programs tailored to individuals’ health 650 status and goals and physical activity levels and preferences. 651
652
19 BC Guidelines: Managing Pain – DRAFT for External Review
Appendix C: Allied Health Professionals to Support Pain Management 653
654 The following is a summary of allied health professionals and evidenced-based approaches. Evidence summaries, 655 tools, resources for practitioners and patients are available in CADTH: Non-Drug Ways to Manage Chronic Pain and 656 Agency for Healthcare Research and Quality: Noninvasive Nonpharmacological Treatment for Chronic Pain. 657
• Acupuncture or TENS: Evidence for reducing pain, mitigate withdrawal side effects.38–40 Acupuncture may be 658 beneficial in certain conditions.41 659
• Chiropractic Services: Pain related to musculoskeletal and axial pathology, but other types of chronic pain may 660 respond to chiropractic treatment. 661
• Occupational Therapy: Referral highly recommended when a patient’s function in daily activities is disrupted by 662 pain; e.g. the ability to take care of themselves, family/home responsibilities, work, school, etc. 663
• Physiotherapy: For active acute MSK type injuries; some physiotherapists may have skills at managing chronic 664 pain. Evidence for an activity/exercise plan. Passive modalities i.e. hot compresses and use of TENS machines 665 can complement and not replace the mobility programs. 666
667 • Registered Massage Therapy. Help in desensitizing affected areas and helping to restore and/or maintain 668
optimum movement and function. 669 670
• Osteopathic Therapy. Osteopathy follows the principle that there is a strong relationship between structure and 671 function of the body. As the body possesses its own self-healing mechanisms; manual osteopathy aids these 672 mechanisms by using techniques to restore the body to harmony with the aim of relieving pain and improving 673 mobility. 674
675 • Psychological Services: Patients with chronic pain very often have depression and anxiety. Useful for improved 676
self-management, goal setting, sleep hygiene ; approaches include cognitive behavioral therapy, PTSD 677 counselling, mindfulness and biofeedback. Consider when chronic pain has other variables such as relationship 678 instability, financial and work insecurity, past traumas or other medical co-morbidities. 679
680 • Social Work. provide a safe supportive environment to deal with issues such as work impacts, personal and 681
social relationships, accessing benefits, drug and alcohol misuse and cultural perspectives. 682 683
• Traditional Healers. For many indigenous people and others from different cultural backgrounds, the continuity 684 of their community culture and the inclusion of traditional healing will add a layer of support to the 685 management of pain. This is rarely an either/or decision, rather an exploration of ways to complement the on-686 going plan. This may already be going on “in the background” if the patient is unsure of the reaction of other 687 caregivers, so ask about what resources are available through their own indigenous / cultural community. 688
Managing Patients with Pain in Primary Care – Part 2 1 DRAFT FOR EXTERNAL REVIEW 2
Online questionnaire available at: surveymoh.health.gov.bc.ca/public/survey/external-review-3 questionnaire-managing-pain 4
Line numbers are included for ease of reference while providing feedback 5 Effective Date: TBD 6 7 This guideline is Part 2 of the Managing Patients with Pain in Primary Care Guideline. For Pain 8 Assessment and Management Approaches see Part 1 of the guideline. 9
Pharmacological Treatment 10
For many patients with acute, subacute, and chronic pain, pharmacological management is part of 11 overall care. Indeed, it is imperative to get acute pain under control early and effectively but with a clear 12 goal of reassessing its effectiveness and presenting a well-articulated anticipated plan to taper and stop 13 medications. The benefits of long-term medications, especially opioids, are less well understood. For 14 longer term non-cancer pain, ensure that non-opioid and non-pharmacological therapies have been 15 effectively optimized first.1 The management of cancer and end-of-life pain usually requires a different 16 strategy that may more appropriately include opioids. 17
Managing patients with most types of pain is not necessarily an “either/or” strategy but rather a 18 layering of interventions including non-pharmacological management, self-management, and 19 pharmacological management. 20
Considerations and Controversies of Care 21
• Many guidelines on pain management exist, including those from national, provincial, regulatory 22 authority, advocacy, and academic institutions. They may not all align, and the levels of evidence 23 and evidence review process used to create those guidelines may appear unclear in terms of clinical 24 decision making. 25
• Evidence may include large systemic reviews, randomized control trials, and expert opinion. 26 Evidence may come from high quality studies, but the strength of the evidence may be described as 27 poor, e.g., simply because of small study numbers. An effect may be described as statistically 28 significant, but the magnitude of the clinical impact maybe small. 29
• Guidelines are generally considered to be based on strong clinical evidence, yet some 30 recommendations clearly state the evidence is weak. However, weak evidence may be the only 31 evidence available and is intended to give the clinician an option to consider. 32
• The number needed to treat (NNT), and the number needed to harm (NNH) are important concepts 33 to help weigh the benefit and harm of a drug or treatment. They are used to inform a clinician about 34 a specific condition response. However, an intervention may be used in several conditions but be 35 more effective in one condition than another. 36
• Pain is a symptom and not a specific condition with clearly defined parameters like blood pressure 37 and spirometry. Clinicians who need to treat patients with pain need information on how to do this 38 as safely and effectively as possible for that patient. 39
• It is important to use medications with caution for any patient who may have reduced renal, 40
BC Guidelines: Managing Pain – DRAFT for External Review 2
hepatic, or cardiac function. Likewise, patients with reduced lean body mass (increased fat 41 concentration), malnourishment (reduced albumin), concomitant disease, and multiple medications, 42 may need dose adjustments. Consult product monographs for specific drugs and check Appendix A: 43 Medication Table. 44
Non-opioid medications2 45 Acetaminophen 46 Indications: Consider for initial management of patients with mild-moderate pain.3 Use the lowest 47 effective dose and stop therapy if minimal or no effect. 48 Cautions: Higher doses, chronic use, increasing age, renal disfunction and alcohol use increase risk of 49 hepatic toxicity. 50 51 Nonsteroidal Anti-inflammatory Drugs (NSAIDs) 52 Indications: Consider for patients with mild-moderate musculoskeletal pain and inflammation. Use the 53 lowest effective dose for the shortest duration to reduce adverse events and reassess effectiveness 54 within the first few weeks. 55 Cautions: 56
o The risk of GI complications is unlikely, but possible, within the first week. The risk increases 57 with longer duration of therapy. Patients at high risk of GI complications may benefit from a 58 COX-2 inhibitor (i.e., celecoxib), and/or the addition of a PPI (i.e., rabeprazole) even for short 59 term use. 60
o Patients at high risk or with established cardiovascular disease may be at increased risk of CV 61 events with NSAIDs. Risk appears to be dose and duration dependent. 62
o Contraindicated in patients with a Creatinine Clearance (CrCl ≤30 ml/min. NSAIDs may cause 63 further deterioration in renal function in patients with mild-moderate or declining renal 64 function, use with caution. 65
o Older adults have a greater frequency of impaired renal function, existing electrolyte 66 imbalances, comorbid conditions (including CV disease), and multiple medications including OTC 67 products. Take a full history and assess individual patients’ appropriateness for NSAIDs. 68
69 Combining classes of drugs and combination products. 70 Indications: There is some evidence that in the setting of patients with acute pain, low back pain, and 71 hip/knee osteoarthritis pain, an NSAID +/- acetaminophen (but not acetaminophen alone) is equally 72 effective as an opioid +/-acetaminophen.4,5 Evidence in post-surgical situations support lower opioid 73 doses for those on an NSAID +/- acetaminophen. Addition of an opioid to acetaminophen/NSAID 74 combination does not result in additional pain relief.6,7 75 76 Topical NSAIDs 77 Indications: Consider for acute conditions such as when patients have sprains, strains and overuse 78 injuries.8 and in some chronic conditions such as osteoarthritis, particularly of the hand or knee. Re-79 evaluate every 3 months and continue only in responders.8 80 Topical formulations with diclofenac (1-4%), ibuprofen (5-10%) or ketoprofen (1-5%) have the best 81 evidence8 and are available over the counter (diclofenac 1.16-2.32%) or through a compounding 82 pharmacy (generally in the 5-10% range). These can be expensive and are not a PharmaCare benefit. 83 While increased concentrations are seen in practice, they have not been studied. 84 Cautions: Systemic absorption from topic NSAIDs is low (approximately 6-23%) compared to oral forms 85 however systemic adverse events have been reported. Generally, well tolerated by all patients including 86
BC Guidelines: Managing Pain – DRAFT for External Review 3
those over 65 years of age. 87 Skeletal Muscle Relaxants 88 Indications: For acute MSK pain only. There is insufficient evidence to support the use of 89 cyclobenzaprine for chronic myofascial pain.9 90 Cautions: Due to the risk of long-term dependence and high incidence of adverse effects (sedation, 91 dizziness, dry mouth), consider short term use only (1-2 weeks). Adverse effects may be more 92 pronounced and may cause falls in frail older adults. 93 94 Gabapentinoids10 95 Indications: Consider for patients with neuropathic pain conditions such as post herpetic neuralgia or 96 painful diabetic neuropathy. Benefits/harms can often be seen and assessed as early as 1 week. Higher 97 doses (gabapentin >1800 mg/d; pregabalin >300 mg/d) may not provide additional significant benefit 98 relative to the increased risk of adverse events.10 A good summary is provided by the B.C. Provincial 99 Academic Detailing Service. 100 Cautions: Due to the risk of severe respiratory depression and sedation, use with caution with opioids 101 and other CNS depressants.11 Adverse effects (drowsiness, dizziness, etc.,) may be more pronounced 102 and may cause falls in frail older adults. Gabapentinoids have been identified as drugs of potential 103 misuse.12 These drugs are renally excreted, therefore use with caution in patients with renal 104 impairment. 105 106 Serotonin norepinephrine reuptake inhibitors (SNRIs) 107 Indications: Consider for patients with neuropathic pain conditions (diabetic neuralgia, post herpetic 108 neuralgia). Evidence of benefit is stronger for duloxetine than for venlafaxine.13–15 109 Benefits/harms can often be seen and assessed within 1 week. Higher doses (duloxetine >60 mg/d) do 110 not produce better analgesia). SNRIs are better tolerated than TCAs in frail older adults.16 111 112 Tricyclic antidepressants (TCAs) 113 Indications: Low quality evidence suggests TCAs may result in a 30% reduction in pain for some patients. 114 TCAs do not appear to be more effective than placebo in chronic low-back pain. There is a lack of 115 evidence to evaluate the role of TCAs in fibromyalgia.17 116 Cautions: Due to high incidence of anticholinergic side effects (drowsiness, dry mouth, constipation), 117 consider alternatives in frail older adults. However, if there is a distinct mood disorder in a patient with 118 pain, it is always a consideration to add an antidepressant/anxiety medication to help reduce the 119 “disability burden”. 120
Opioid Therapy 121 This section provides guidance for managing patients who are both opioid-naïve and those already on 122 long-term opioid therapy. Indications for tapering / cessation of opioids are also included. 123
Controversies of Care 124
The use of opioids is one of the more controversial issues for many clinicians. 125
o There are national guidelines as well as regulatory authority directives that give clear guidance 126 about the use of opioids but to some clinicians, these appear excessively harsh and restrictive. Some 127 clinicians are concerned about disciplinary action if they prescribe opioids or exceed the 128 recommended daily maximum. 129
o Virtually all guidelines distinguish between non-cancer and palliative end-of-life care, yet some 130 clinicians fail to properly consider that distinction and restrict appropriate comfort measures. 131
BC Guidelines: Managing Pain – DRAFT for External Review 4
o The 2017 Canadian Guideline for Opioids for Non-Cancer Pain is the current standard, yet a follow 132 up review of those guidelines by the main author suggests that 1/3 of clinicians mistakenly believed 133 the guideline suggested mandatory tapering and that 2/3 of respondents highlighted resistance by 134 patients and lack of access to effective non-opioid treatment.18 135
o Consensual tapers may lead to improved or at least no worse pain management (though in a 136 significant minority of patients this might not be the case), while forced tapers may increase risk of 137 OUD, overdose, and suicide.19 138
o A 2018 review by the same author looking at 96 clinical trials, concluded “use of opioids was 139 associated with significantly less pain and significantly improved physical functioning…but the 140 magnitude of the association was small”. The mean follow up of the studies was 60 days.20 141
o The 2017 National Guidelines that describe maximum daily doses, also suggest that some patients 142 may benefit from higher doses. 143
o Clinicians may hesitate to prescribe opioids to elderly patients yet many of the elderly have 144 significant debilitating conditions that would benefit from an opioid. Considerations for safely 145 prescribing opioids for the elderly are described below. 146
o There are several screening tools available to try and identify the risk of developing OUD when 147 initiating opioids, but the evidence suggest they may not help identify those at low risk. Only the 148 absence of a mood disorder was associated with low risk. Previous OUD, certain mental health 149 conditions(e.g. personality disorder), and the use of certain psychiatric medications such as atypical 150 anti-psychotics, were associated with high risk of developing OUD.21 151
o The most commonly prescribed opioids in 2018/19, in order of most to least, are codeine, 152 hydromorphone, tramadol, morphine, and oxycodone.22 However, the analgesic activity of codeine 153 (and to a lesser extent tramadol) is dependent on genetic polymorphisms, making them more 154 difficult to dose adjust in patients requiring additional dose adjustments due to renal or hepatic 155 impairment. 156
o TRAMADOL: There is a perception that tramadol is a safer opioid as it is not currently a Schedule 1 157 narcotic, however, Health Canada has added tramadol to the Controlled Drugs and Substances 158 Act effective March 31, 2022, to reflect the fact it is an opioid with the same risks as other opioids.23 159 Tramadol’s analgesic activity, much like codeine, is dependent on CYP2D6 metabolism which is 160 altered in approximately 28% of patients.24 In addition, tramadol acts as a serotonin and 161 norepinephrine reuptake inhibitor (SNRI), increasing the risk of drug interactions and side effects 162 (including serotonin syndrome and seizures) over that of other opioids.25 163
164 Considerations for initiation of opioid therapy for opioid-naïve patients 165
Indications for opioid medications: 166
o Moderate to severe acute pain (e.g., post-operative, 167 injuries) expected to resolve. 168
o Palliative and life-limiting conditions (e.g., end-stage 169 heart failure / COPD / cancers) – for these settings, 170 refer to Palliative Care Guideline as the benefits and 171 risks are different in these patients who will need 172 longer and likely escalating doses. Palliative care 173 patients should never be denied opioid medications 174 when required. 175
Opioids are a potent and useful class of medications for the treatment of pain and end-of-life symptoms when used appropriately. However, while supporting the patient with pain management, clinicians need to be aware of appropriate prescribing guidelines to mitigate the risks of opioid harms and dependence.
BC Guidelines: Managing Pain – DRAFT for External Review 5
Despite previous practice, there is limited or weak evidence for the value of initiating opioids for 176 patients with chronic non cancer pain (CNCP). In many instances, the risks of prescription opioid-use 177 disorder (OUD) or adverse effects outweigh the potential benefits. The long-term use of opioids for 178 managing pain has a potentially higher risk of harm and has limited evidence for benefit. A classic 179 example of this type is a young patient with gradually worsening degenerative back or joint pain. 180
Prescribing considerations: 181
o The initiation of an opioid should always be considered as a “therapeutic trial”. Document well 182 the initial discussion and rationale for use of opioids. Encourage patients to self-limit where 183 possible. 184
o Limit prescriptions. Consider a trial for 7 days or less at a time. Increase interval as patient 185 stabilizes on a dose that does not compromise function. An oral dose of morphine 5-10 mg, or 186 hydromorphone 1-2 mg are common adult starting doses, especially in the immediate post-op 187 period. 188
o Start patients, especially those who are opioid naïve, on lowest effective dose and titrate as 189 needed with close monitoring of efficacy and side effects. A particularly useful tool is: Centre for 190 Effective Practice ‘Opioid Manager’. The Opioid Manager is a practical tool and checklist for 191 opioid prescribing decisions including opioid therapy trials, maintenance, and monitoring, 192 switching, and tapering. 193
o Consider and minimise drug interactions (e.g., CNS depressants, serotonin concerns with 194 tramadol). See Appendix A: Medication Table for specific drug interactions. 195
o Be aware of CPSBC Safe Prescribing Standards. The College also has a list of Prescribing tools and 196 resources on their website. 197
o Fully inform patients of the risks and benefits of using opioids and discuss plans for the possible 198 tapering and/or discontinuation of the medication. Document this discussion. 199
o A patient handout is encouraged. Refer to Appendix B: Patient Handout – Initiating Opioids 200 o Frail older adults with moderate to severe pain and functional impairment, or poor quality of life 201
should not be excluded from consideration of opioid therapy. See Pharmacological Pain 202 Management in the Older Adult below. 203
o An additional resource is a detailed review on Opioid Metabolism by Howard Smith26. 204 o For BC specific information and coverage, see Appendix A: Medication Table. 205
206
Contraindications and Cautions 207
Absolute Contraindications. 208 o Documented opioid allergy 209 o Severe respiratory instability 210 o Acute psychiatric instability or increased risk of suicide 211 o Previously known opioid intolerance 212
Relative Contraindications. 213 o Concurrent use of benzodiazepines and “z” drugs like zopiclone 214 o Addition or increasing dose of methadone in a person with documented prolonged QTc interval 215 o Known on-going alcohol or other substance use disorder 216 o Documented history of diversion 217
Use with Caution. 218 o Concurrent use with CYP3A4 inhibitors/inducers (e.g., clarithromycin, diltiazem, “azoles” such as 219
ketoconazole, certain ARV’s such as ritonavir, phenobarbital and phenytoin). See Appendix A: 220 Medication Table. 221
BC Guidelines: Managing Pain – DRAFT for External Review 6
o Codeine is metabolized by CYP2D6 to its active form, morphine. Up to 23% of the population may 222 produce significantly more or less morphine than expected based on the dose.27 Monitor for increased 223 side effects/ decreased efficacy or select alternative drug. 224
o Concurrent use of potentially sedating medications such as gabapentinoids11 cyclobenzaprine, 225 diphenhydramine and dimenhydrate. 226
o Hepatic and renal impairment may change the pharmacokinetics of medications, reducing elimination 227 and increasing availability of that drug. 228
o Use of alcohol with opioids should be actively discouraged. 229 o When patients have co-existing mental health conditions such as mood or thought disorders, 230
consider the extent to which they may be exacerbating or coexisting with the pain. Use caution 231 when considering an opioid and reflect on the concomitant need to manage the mental health 232 condition as well. The Canadian National Guideline for Opioids for Chronic Non-Cancer Pain 233 recommends stabilizing active psychiatric disorder before initiating a trial of opioids (Weak 234 recommendation). 235
236 Considerations for patients already on opioid therapy 237
Most primary care practitioners see patients who are already on long-term opioid therapy for chronic 238 pain, regardless of initial indications. These considerations apply whether the patients are long 239 established or new to the practice. Again, it is not appropriate to refuse to accept or continue to care for 240 patients on opioids and it is not appropriate to abruptly stop prescribing. 241
Indications for long-term use of opioid medications: 242
o Palliative care and end-of-life conditions 243 o Conditions not expected to improve and not well managed with non-opioid medications. Some 244
examples may include worsening scoliosis, degenerative disc disease or vertebral fractures not 245 amenable to other interventions. 246
o Some patients with chronic pain already on opioids may be stable, and functional with minimal 247 disability and side effects. Maintaining them on opioids may be appropriate and indicated. A forced 248 taper may worsen pain and reduce stability. 249
Ongoing Management 250
o Reassess regularly to ensure that non-opioid and non-pharmacological therapies have been 251 maximized. Document the reassessment. 252
o Self-Reflection: “If you are feeling pressured to prescribe opioids, ask yourself where this pressure is 253 coming from and how you might respond”. 254
o There is not a defined target morphine equivalent daily dose- MEDD, but clinicians should prescribe 255 the lowest effective dose. 256
o The CPSBC Safe Prescribing Standards, suggests that doses above 90 MEDD require “substantive 257
Pandemic Considerations.
During the Covid pandemic and the opiate epidemic, consideration may be needed to reduce the risk of harm from both. In an effort to reduce the spread of Covid, the BCCSU has a document outlining many related changes in prescribing policy. There are provincial policy changes that reduce risk of exposure such as phone orders and transferring scripts between pharmacies. Longer prescriptions and potentially delaying or slowing tapers may also be strategies to avoid destabilizing already vulnerable patients.
BC Guidelines: Managing Pain – DRAFT for External Review 7
evidence of exceptional need and benefit”. The standards do not say that higher doses cannot or 258 should not be prescribed, just documenting the evidence and need for a higher dose. In addition the 259 guidelines do not suggest mandatory tapering.18,28 Clinical examples may include patients with 260 severe pain for which higher doses of opioids are needed and patients who present with existing 261 prescription doses which exceed 90 MEDD for whom abrupt tapering or cessation would cause 262 harm. Documentation is critical. 263
o Consider using long-acting opioids after stabilizing the patient on immediate release opioid. Even in 264 this situation, be aware that there is poor evidence supporting long-term use of opioids and discuss 265 and document the risk of long-acting opioids in advance. 266
o For anticipated longer term prescriptions, a written treatment agreement is encouraged. Samples 267 available at CPSBC Prescription Review Program and others in Resources section. 268
o Divergence from the treatment agreement may suggest a need to re-evaluate the clinical situation 269 and taking into account the biopsychosocial stressors that may be present. Agreements are not 270 meant to be punitive so it does not necessarily indicate that opioids must be tapered or stopped. 271 Breach of agreements should not be used as a method to justify termination of opioid therapy nor 272 should they be used to support discharging a patient from a practice. Instead, they should be used 273 to support opening a conversation about appropriate and safe opioid use. Consider discussion with 274 a pain/addiction medicine specialist. 275
o All patients on opioids for chronic pain could be considered for random rUDT. However, there is 276 uncertain evidence about the effect of urine drug screening on the risk of opioid overdose.1 A urine 277 drug test may be used in the context of patient education and safety to identify additional drugs 278 (sometimes taken unknowingly) that may put patients at higher risk. Absence of the prescribed 279 opioid in random urine testing should be a red flag for possible diversion. A respectful discussion of 280 results may be useful before any action is taken. Refer to BCCSU’s Opioid Use Disorder, see Urine 281 Drug Testing for more information. 282
o Ideally, patients should be prescribed opioids by their primary care provider only. Where possible, 283 only one consistent provider/team should be providing the prescriptions. However, the current 284 reality in BC is that some patients may see multiple providers; therefore, make good use of 285 documentation and EMR functions including ready access to patient agreements, current 286 medications and any “cautions” or “flags” that are attached. 287
o Pharmanet provides an up-to-date list of filled prescriptions and should be used prior to every 288 opioid prescription and refill. CareConnect provides recent clinical encounters including ER visits and 289 prescriptions written. 290
o Consider blister-packs and controlled dispensing strategies if there is concern about misuse. 291 o Consider offering a naloxone kit and education to patient and family on how to administer and 292
respond to overdose. Refer to towardtheheart.com produced by BCCDC for naloxone kit guidance. 293 o For safety of children, pets and opioid-naïve adults and prevention of theft, educate patients on safe 294
storage and disposal of opioid medications. 295 o Reassess regularly and be vigilant for incipient or existing prescription OUD, e.g., escalating dosages, 296
increasing pain complaints, multi-doctoring. 297
When to Taper and/or Stop Opioids 298 o For patients prescribed opioids for short-term, acute pain (e.g. post-operative or injuries), 299
recommend a tapering and discontinuation plan including dosage, frequency and duration. Confirm 300 the follow-up plan. 301
o Opioid tapering and discontinuation may be difficult for the patient who fear worsening of the pain 302 and withdrawal symptoms. Patients should be actively engaged in a discussion about the merits of 303
BC Guidelines: Managing Pain – DRAFT for External Review 8
gradual dose reduction, including the potential for equivalent or better pain control with less opioid-304 associated risks (reduced risk of MI, MVA, sleep apnea, sexual dysfunction, falls, depression, 305 addiction, unintended overdose). ‘I think we can work towards giving you just as much pain control 306 with less medication risks’. However, a percentage of people will not experience these benefits and 307 the taper may not be appropriate. 308
Indications for tapering: 309 When there is a loss of therapeutic effect on pain and function. 310 When there are intolerable side effects such as sedation. 311 When there is non-adherence to the agreed plan or evidence of diversion. Diversion is often 312
challenging to manage as a patient may only be misusing apportion of the script. 313 Patient request 314 When clear evidence of SUD is present or worsening it maybe more appropriate to refer to 315
addiction specialist instead of attempting to taper. 316 • Many guidelines suggest that a taper be considered for patients whose MEDD is above 90. This is not 317
a strict limit and clinical judgement is always warranted. This does not apply to cancer/palliative 318 patients. 319
Opioid-induced hyperalgesia is an adverse effect that is characterized by decreasing efficacy that is 320 not improved by increasing the dose of the opioid.56 When it happens, it happens at high doses and 321 has been reported with a number of different opioids.57–59 Symptoms include spreading or burning 322 pain and allodynia (pain due to a stimulus such as light touch that does not usually provoke pain). It 323 may also be accompanied by other signs of opioid toxicity such as myoclonus, delirium, and seizures. 324 Symptoms improve by reducing or eliminating the drug. Consider opioid rotation in cases of opioid 325 toxicity. See Opioid Switching section below. 326
Tapering Strategies 327 There is no evidence for any specific tapering strategy. However, a commonly described strategy is: 328 o A reduction of 5-10% of the daily dose 329 o A dose reduction every 2-4 weeks 330 o Beginning with just a 2-3% drop can build confidence and let the person gain insight into any 331
anticipatory anxiety-related pain symptoms. 332 o Patients habituated to high-dose, long-term opioids may need longer intervals between drops in 333
dose, e.g., 5% every 1-3 months. 334 o Monitor the patient for withdrawal symptoms and consider withdrawal management medications 335
such as clonidine, Imodium and NSAIDs. 336 A good Canadian opioid reduction guide is Centre for Effective Practice ‘Opioid’ Manager-Opioid 337 Tapering Template 338
Cautions while tapering / discontinuing long-term opioids: 339 o Never abruptly stop opioids with patients on chronic opioid therapy. 340 o Tapering (especially rapidly) can paradoxically increase the risk of overdose, OUD and suicide if 341
underlying pain is not well managed. Consider switching to an alternative opioid including 342 methadone or opiate agonist such as buprenorphine. 343
o A clinician needs to differentiate between worsening or non-responsive chronic pain, and untreated 344 or unmasked OUD. The concomitant existence of OUD and chronic pain may require a referral to an 345 addiction’s specialist, whereas worsening chronic pain should prompt an overall evaluation of the 346 pharmacologic and non-pharmacologic strategy. 347
BC Guidelines: Managing Pain – DRAFT for External Review 9
Opioid Switching 348 For patients on opioids who have significant side effects or reduced effectiveness, consider switching 349 to another opioid. See Appendix A for opioids medications profiles and the below resources: 350
o Centre for Effective Practice ‘Opioid’ Manager 351 o Opioid Manager (National Pain Centre) – Opioid Switching 352 o McMaster Opioid Manager 353
Opioid Use Disorder-OUD 354
Prescribing opioids for pain is associated with a risk for developing prescription opioid use disorder.29 355 Despite a number of screening tools available to identify patients at increased risk, there are few valid 356 ways to identify those who can be safely prescribed opioid analgesics.21 357
This guideline is not intended to provide guidance on diagnosing and managing OUD. For full guidance, 358 see BC Guidelines: Opioid Use Disorder and BCCSU 359
Providing opioids for analgesia for patients with OUD is complex. Still, almost all the principles in the 360 guideline can be applied to patients with an OUD who are in need of pain management. 361
o For patients already on long-acting opioids for years, consider whether they may have a prescription 362 opioid use disorder, and, if evidence of OUD (versus increasing opioid tolerance), consider opioid 363 agonist treatment (e.g., buprenorphine/naloxone or other available therapies). 364
o Managing patients with prescription opioid use disorder who also have complex chronic pain is 365 challenging. Consider consulting with the RACE line and BC Centre on Substance Use Provincial 366 Guideline Opioid Use Disorder: Diagnosis and Management in Primary Care and The Canadian 367 Guideline for Opioid Use Disorder in Older adults. Additional information and training on Opioid Use 368 Disorder can be found at the BCCSU: www.bccsu.ca/about-the-addiction-care-and-treatment-369 online-certificate/ and their ECHO site on OUD: www.bccsu.ca/bcechoonsubstanceuse-oud/ 370
o Patients with active mental health issues (e.g. anxiety, depression, PTSD) may be at increased risk of 371 prescription OUD.29 372
Cannabis 373
Cannabis and cannabinoid use for medical purposes can be another controversial topic. As with opioids, 374 views and authorization practices may be influenced by media, social justice issues, personal experience 375 and at times conflicting evidence. Complicating its use in a medical setting is the proportion of 376 Canadians who indicated they had consumed cannabis within the last 12 months rose from 9.4% to 377 14.8% between 2004 and 2017, and in the year following legalization (2018-2019) that number 378 increased to 17.5%.30 Statistics Canada reported in 2018 that 45% of Canadians had tried cannabis at 379 least once in the lifetime, and that 50% of the people who self-reported using it for medical reasons, did 380 so for managing pain. 381
The challenge for clinicians is weighing the evidence for medical use, managing the potential biases 382 (including their own) from all sides of the debate, and being aware that many of their patients are and 383 will be using it for managing pain. Be aware of simply switching one dependency (opioids) for another 384 (cannabis) and be aware that evidence regarding cannabis use is still evolving. 385 386 387
BC Guidelines: Managing Pain – DRAFT for External Review 10
Cannabis for chronic pain 388
Recent guidance intended for the Canadian clinician highlights that more research is needed to 389 determine the role of cannabis in managing chronic pain. However, the Simplified Guideline for 390 Prescribing Medical Cannabinoids in Primary Care31 suggests that cannabinoids may be useful for 391 chronic neuropathic pain, chemotherapy induced nausea and vomiting, and spasticity of multiple 392 sclerosis and spinal cord injury, but not as a first line therapy. 393
In contrast, a recent review by the National Academies of Sciences, Engineering and Medicine found 394 there was conclusive or substantial evidence that cannabis or cannabinoids are effective for the 395 treatment of chronic pain in adults.32 396
The Canadian National Guideline for Opioids for Chronic Non-Cancer Pain notes that nabilone may have 397 similar effects on pain relief when compared to opioids, NSAIDs, or tricyclic antidepressants29 (Low 398 Quality Evidence). Evidence comparing opioids to nabilone was from a single study.33 399
In summary, while cannabis is now legal, consumed by many patients and may prove effective for some 400 conditions, it is difficult to provide broader evidence informed indications for its use. More clarity is 401 needed for specific therapeutic products and dosing schedules. 402
The Lower-Risk Cannabis Use Guideline34 provides 10 recommendations of modifiable behaviours to 403 reduce the risk of adverse effects of cannabis use, including avoiding early age initiation, using lower 404 potency THC products, avoiding synthetic cannabinoids, and preferring non-smoking methods. 405
Health care providers need to be knowledgeable and non-judgmental when informing 406 patients about cannabis and cannabinoids. 407
UBC CPD elearning has a free on-line module Cannabis Education for Health Care Providers as well as a 408 Cannabis Education Toolkit. 409
Pharmacological Pain Management in the Older Adult 410
Managing ‘Older Adults’ with pain, especially the Frail Older Adult, often requires modifications and 411 adjustments in both approach and dosages. Many experts suggest that age greater than 70 and/or 412 frailty require awareness of additional factors when assessing and managing pain. Frailty is a medical 413 syndrome with multiple causes and contributors, characterized by diminished strength and endurance 414 and reduced physiological function, leading to increased adverse health outcomes such as functional 415 decline and early mortality. However, frailty is not inevitable in ageing and can be prevented or 416 reversed. Additional information about Healthy Aging and Preventing Frailty, can be found in the 417 updated provincial healthy aging strategy. 418
Guiding principles when prescribing for frail / older patients: 419
o In general, dose selection for an elderly patient should be cautious, usually starting at the low end of 420 the dosing range, reflecting the greater frequency of decreased hepatic, renal or cardiac function, 421 and of concomitant disease or other drug therapy. 422
o Persistent pain in frail older adults increases morbidity and poor health outcomes, making treatment 423 a priority. 424
o As cognition worsens, pain is less likely to be reported and may manifest as other distress 425 behaviours (agitation, resisting care, insomnia, poor appetite). 426
o Risk of falls is elevated. However, pain, decreased attention or poor sleep due to chronic pain can 427 also increase the risk of falls. 428
o Multiple morbidity, cognitive impairment and altered pharmacokinetics mandate an individualized 429
BC Guidelines: Managing Pain – DRAFT for External Review 11
approach. Bloodwork as needed (e.g., renal function) in the initial assessment phase and 430 intermittently if the use of medication persists. 431
o Opioid naive patients should be started at the lowest recommended dose and titrated as needed. 432
Choices of Opioid for Frail Older Adults. 433
o The use of opioids is not contraindicated in frail older adults but starting doses should be at the low 434 end of the dosing range reflecting the greater frequency of decreased hepatic, renal or cardiac 435 function, and of concomitant disease or other drug therapy. Ongoing dosing, when needed, should 436 be titrated slowly based on efficacy and adverse effects. Please consult product monographs for 437 more information. 438
o The most commonly prescribed opioids in 2018/19, in order of most to least, are codeine, 439 hydromorphone, tramadol, morphine, and oxycodone.22 440
o The analgesic activity of codeine (and to a lesser extent tramadol) is dependent on genetic 441 polymorphisms, making them more difficult to dose adjust in patients requiring additional dose 442 adjustments due to renal or hepatic impairment. See the cautionary note regarding Tramadol in the 443 Opioid Therapy: Controversies of Care section above. 444
o In addition to starting at the low end of the dosing range for hydromorphone, morphine and 445 oxycodone for all older adults, additional dose adjustments are needed for patients with impaired 446 hepatic or renal function. Please consult product monographs for more information. 447
o Methadone, fentanyl, and buprenorphine are also used in managing pain, but less frequently and 448 may require more experience or expert guidance. 449
o Gabapentinoids may have a higher rate of side effects including respiratory depression and 450 sedation, and therefore should be used with caution in the older adult especially in those with 451 reduced renal function. 452
References 453 1. Busse J. The 2017 Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Cancer Pain. 2017;105. 454 2. Wood L, Hendrick PA. A systematic review and meta-analysis of pain neuroscience education for chronic low back pain: Short-and long-455
term outcomes of pain and disability. European Journal of Pain. 2019;23(2):234–49. 456 3. Enthoven WT, Roelofs PD, Deyo RA, van Tulder MW, Koes BW. Non-steroidal anti-inflammatory drugs for chronic low back pain. 457
Cochrane Back and Neck Group, editor. Cochrane Database of Systematic Reviews [Internet]. 2016 Feb 10 [cited 2019 Nov 14]; Available 458 from: http://doi.wiley.com/10.1002/14651858.CD012087 459
4. Chang AK, Bijur PE, Esses D, Barnaby DP, Baer J. Effect of a Single Dose of Oral Opioid and Nonopioid Analgesics on Acute Extremity Pain 460 in the Emergency Department: A Randomized Clinical Trial. JAMA. 2017 Nov 7;318(17):1661. 461
5. Krebs EE, Gravely A, Nugent S, Jensen AC, DeRonne B, Goldsmith ES, et al. Effect of Opioid vs Nonopioid Medications on Pain-Related 462 Function in Patients With Chronic Back Pain or Hip or Knee Osteoarthritis Pain: The SPACE Randomized Clinical Trial. JAMA. 2018 Mar 463 6;319(9):872–82. 464
6. Best AD, De Silva RK, Thomson WM, Tong DC, Cameron CM, De Silva HL. Efficacy of Codeine When Added to Paracetamol 465 (Acetaminophen) and Ibuprofen for Relief of Postoperative Pain After Surgical Removal of Impacted Third Molars: A Double-Blinded 466 Randomized Control Trial. J Oral Maxillofac Surg. 2017 Oct;75(10):2063–9. 467
7. Thybo KH, Hägi-Pedersen D, Dahl JB, Wetterslev J, Nersesjan M, Jakobsen JC, et al. Effect of Combination of Paracetamol 468 (Acetaminophen) and Ibuprofen vs Either Alone on Patient-Controlled Morphine Consumption in the First 24 Hours After Total Hip 469 Arthroplasty: The PANSAID Randomized Clinical Trial. JAMA. 2019 Feb 12;321(6):562–71. 470
8. Derry S, Moore AR, Gaskell H, McIntyre M, Wiffen PJ. Topical NSAIDs for acute musculoskeletal pain in adults [Systematic Review]. 471 Cochrane Database of Systematic Reviews 2018. 2018; 472
9. Leite FM, Atallah ÁN, Dib RE, Grossmann E, Januzzi E, Andriolo RB, et al. Cyclobenzaprine for the treatment of myofascial pain in adults. 473 Cochrane Database of Systematic Reviews [Internet]. 2009 [cited 2020 Nov 24];(3). Available from: 474 https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD006830.pub3/abstract 475
10. B.C. Provincial Academic Detailing Service. Medications for Neuropathic Pain. [Internet]. 2018 Dec. Available from: 476 https://www2.gov.bc.ca/assets/gov/health/practitioner-pro/provincial-academic-detailing-service/medications-neuropathic-pain-477 newsletter.pdf 478
11. Gomes T, Juurlink DN, Antoniou T, Mamdani MM, Paterson JM, van den Brink W. Gabapentin, opioids, and the risk of opioid-related 479 death: A population-based nested case–control study. Tsai AC, editor. PLoS Med. 2017 Oct 3;14(10):e1002396. 480
12. Molero Y, Larsson H, D’Onofrio BM, Sharp DJ, Fazel S. Associations between gabapentinoids and suicidal behaviour, unintentional 481 overdoses, injuries, road traffic incidents, and violent crime: population based cohort study in Sweden. BMJ [Internet]. 2019 Jun 12 482
BC Guidelines: Managing Pain – DRAFT for External Review 12
[cited 2020 Nov 24];365. Available from: https://www.bmj.com/content/365/bmj.l2147 483 13. Moore RA, Derry S, Aldington D, Cole P, Wiffen PJ. Amitriptyline for neuropathic pain in adults. Cochrane Database of Systematic 484
Reviews [Internet]. 2015 [cited 2020 Dec 9];(7). Available from: 485 https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD008242.pub3/full 486
14. Hearn L, Derry S, Phillips T, Moore RA, Wiffen PJ. Imipramine for neuropathic pain in adults. Cochrane Database of Systematic Reviews 487 [Internet]. 2014 [cited 2020 Dec 9];(5). Available from: 488 https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD010769.pub2/full 489
15. Derry S, Wiffen PJ, Aldington D, Moore RA. Nortriptyline for neuropathic pain in adults. Cochrane Database Syst Rev [Internet]. 2015 Jan 490 8 [cited 2020 Dec 9];2015(1). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6485407/ 491
16. Crocco EA, Jaramillo S, Cruz-Ortiz C, Camfield K. Pharmacological Management of Anxiety Disorders in the Elderly. Curr Treat Options 492 Psychiatry. 2017 Mar;4(1):33–46. 493
17. Moore RA, Derry S, Aldington D, Cole P, Wiffen PJ. Amitriptyline for fibromyalgia in adults. Cochrane Database of Systematic Reviews 494 [Internet]. 2015 [cited 2020 Dec 9];(7). Available from: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD011824/full 495
18. Busse JW, Douglas J, Chauhan TS, Kobeissi B, Blackmer J. Perceptions and Impact of the 2017 Canadian Guideline for Opioid Therapy 496 and Chronic Noncancer Pain: A Cross-Sectional Study of Canadian Physicians. Pain Research and Management. 2020 Feb 497 17;2020:e8380171. 498
19. Kroenke K, Alford DP, Argoff C, Canlas B, Covington E, Frank JW, et al. Challenges with Implementing the Centers for Disease Control and 499 Prevention Opioid Guideline: A Consensus Panel Report. Pain Medicine. 2019 Apr 1;20(4):724–35. 500
20. Busse JW, Wang L, Kamaleldin M, Craigie S, Riva JJ, Montoya L, et al. Opioids for Chronic Noncancer Pain: A Systematic Review and 501 Meta-analysis. JAMA. 2018 Dec 18;320(23):2448–60. 502
21. Klimas J, Gorfinkel L, Fairbairn N, Amato L, Ahamad K, Nolan S, et al. Strategies to Identify Patient Risks of Prescription Opioid Addiction 503 When Initiating Opioids for Pain: A Systematic Review. JAMA Netw Open. 2019 May 3;2(5):e193365–e193365. 504
22. British Columbia Ministry of Health. 2018/19 British Columbia Controlled Prescription Drug Atlas [Internet]. Available from: 505 https://www2.gov.bc.ca/assets/gov/health/conducting-health-research/2018-506 2019_british_columbia_controlled_prescription_drug_atlas.pdf 507
23. Order Amending Schedule I to the Controlled Drugs and Substances Act (Tramadol): SOR/2021-44 [Internet]. Available from: 508 https://canadagazette.gc.ca/rp-pr/p2/2021/2021-03-31/html/sor-dors44-eng.html 509
24. Young JWS, Juurlink DN. Tramadol. CMAJ. 2013 May 14;185(8):E352–E352. 510 25. Marks D, Shah M, Patkar A, Masand P, Park G-Y, Pae C-U. Serotonin-Norepinephrine Reuptake Inhibitors for Pain Control: Premise and 511
Promise. CN. 2009 Dec 1;7(4):331–6. 512 26. Smith HS. Opioid metabolism. Mayo Clin Proc. 2009 Jul;84(7):613–24. 513 27. Pratt VM, Scott SA, Pirmohamed M, Esquivel B, Kane MS, Kattman BL, et al., editors. Codeine Therapy and CYP2D6 Genotype. In: 514
Medical Genetics Summaries [Internet]. Bethesda (MD): National Center for Biotechnology Information (US); 2012 [cited 2021 Jun 10]. 515 Available from: http://www.ncbi.nlm.nih.gov/books/NBK100662/ 516
28. L R. Prescribing Opioids for Chronic Pain: Unintended Consequences of the 2016 CDC Guideline. AFP. 2020 Apr 15;101(8):458–9. 517 29. Busse JW, Craigie S, Juurlink DN, Buckley DN, Wang L, Couban RJ, et al. Guideline for opioid therapy and chronic noncancer pain. CMAJ. 518
2017 May 8;189(18):E659–66. 519 30. Rotermann M. Analysis of trends in the prevalence of cannabis use and related metrics in Canada. [cited 2020 Oct 29]; Available from: 520
https://www150.statcan.gc.ca/n1/pub/82-003-x/2019006/article/00001-eng.htm 521 31. Allan GM, Ramji J, Perry D, Ton J, Beahm NP, Crisp N, et al. Simplified guideline for prescribing medical cannabinoids in primary care. 522
Can Fam Physician. 2018 Feb 1;64(2):111. 523 32. National Academies of Sciences, Engineering, and Medicine (U.S.), editor. The health effects of cannabis and cannabinoids: the current 524
state of evidence and recommendations for research. Washington, DC: The National Academies Press; 2017. 468 p. 525 33. Frank B, Serpell MG, Hughes J, Matthews JNS, Kapur D. Comparison of analgesic effects and patient tolerability of nabilone and 526
dihydrocodeine for chronic neuropathic pain: randomised, crossover, double blind study. BMJ. 2008 Jan 26;336(7637):199–201. 527 34. Fischer B, Jeffries V, Hall W, Room R, Goldner E, Rehm J. Lower Risk Cannabis use Guidelines for Canada (LRCUG): a narrative review of 528
evidence and recommendations. Can J Public Health. 2011 Oct;102(5):324–7. 529 530
Practitioner Resources 531 532 Pharmanet: PharmaNet, administered by the Ministry of Health, was developed in consultation with 533 health professionals and the public to improve prescription safety and support prescription claim 534 processing. Available at: www2.gov.bc.ca/gov/content/health/health-drug-coverage/pharmacare-for-535 bc-residents/pharmanet 536 537 CareConnect: secure, view-only Electronic Health Record (EHR) that delivers patient-centric information 538 to support healthcare providers in their delivery of patient care. Available at: my.careconnect.ca/ 539 540 College of Physicians and Surgeons of British Columbia: Drug Programs. Available at: 541 www.cpsbc.ca/registrants/programs/drug-programs 542
https://www2.gov.bc.ca/gov/content/health/health-drug-coverage/pharmacare-for-bc-residents/pharmanet
BC Guidelines: Managing Pain – DRAFT for External Review 13
BC Centre on Substance Use: a provincially networked organization with a mandate to develop, help 543 implement, and evaluate evidence-based approaches to substance use and addiction. Available at: 544 www.bccsu.ca/ 545 Michael G. DeGroote Institute for Pain Research and Care: seeks to fund research and initiatives that 546 will ultimately improve the quality of life for those living with Chronic Pain. Available at: 547 healthsci.mcmaster.ca/pain-institute 548 PainBC: provides wide range of continuing education opportunities are based on a laddered strategy 549 that aims to increase chronic pain capacity among health care providers of all disciplines. Available at: 550 painbc.ca/health-professionals 551 Centre for Effective Practice (CEP): provides many clinical tools including the Management of Chronic 552 Non-Cancer Pain Tool. Available at: cep.health/clinical-products/chronic-non-cancer-pain/ 553
Appendices 554 555 Appendix A: Medication Table 556 Appendix B: Patient Handout: Initiating Opioids 557 Appendix C: Handout for Patients on Long Term Opioids 558
BC Guidelines: Managing Pain – DRAFT for External Review 14
This guideline is based on scientific evidence current as of the effective date. 559
The guideline was developed by the Guidelines and Protocols Advisory Committee and adopted by 560 the Medical Services Commission. 561
For more information about how BC Guidelines are developed, refer to the GPAC Handbook 562 available at BCGuidelines.ca: GPAC Handbook. 563
564
565
THE GUIDELINES AND PROTOCOLS ADVISORY COMMITTEE 566
The principles of the Guidelines and Protocols Advisory Committee are to: • encourage appropriate responses to common medical situations • recommend actions that are sufficient and efficient, neither excessive nor deficient • permit exceptions when justified by clinical circumstances
Contact Information: Guidelines and Protocols Advisory Committee PO Box 9642 STN PROV GOVT Victoria, BC V8W 9P1 Email: [email protected] Website: www.BCGuidelines.ca
Disclaimer
The Clinical Practice Guidelines (the “Guidelines”) have been developed by the Guidelines and Protocols Advisory Committee on behalf of the Medical Services Commission. The Guidelines are intended to give an understanding of a clinical problem, and outline one or more preferred approaches to the investigation and management of the problem. The Guidelines are not intended as a substitute for the advice or professional judgment of a health care professional, nor are they intended to be the only approach to the management of clinical problem. We cannot respond to patients or patient advocates requesting advice on issues related to medical conditions. If you need medical advice, please contact a health care professional.
567
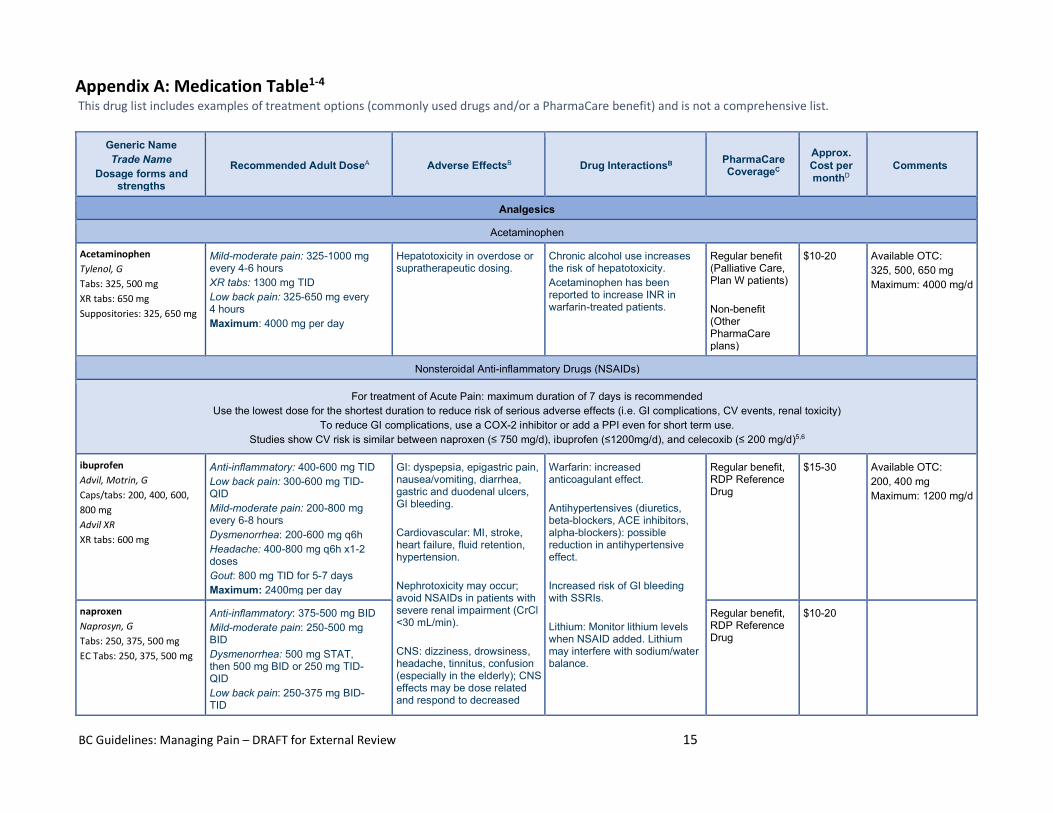
BC Guidelines: Managing Pain – DRAFT for External Review 15
Appendix A: Medication Table1-4
This drug list includes examples of treatment options (commonly used drugs and/or a PharmaCare benefit) and is not a comprehensive list.
Generic Name Trade Name
Dosage forms and strengths
Recommended Adult DoseA Adverse EffectsB Drug InteractionsB PharmaCare CoverageC
Approx. Cost per monthD
Comments
Analgesics
Acetaminophen
Acetaminophen Tylenol, G Tabs: 325, 500 mg XR tabs: 650 mg Suppositories: 325, 650 mg
Mild-moderate pain: 325-1000 mg every 4-6 hours XR tabs: 1300 mg TID Low back pain: 325-650 mg every 4 hours Maximum: 4000 mg per day
Hepatotoxicity in overdose or supratherapeutic dosing.
Chronic alcohol use increases the risk of hepatotoxicity. Acetaminophen has been reported to increase INR in warfarin-treated patients.
Regular benefit (Palliative Care, Plan W patients) Non-benefit (Other PharmaCare plans)
$10-20 Available OTC: 325, 500, 650 mg Maximum: 4000 mg/d
Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
For treatment of Acute Pain: maximum duration of 7 days is recommended Use the lowest dose for the shortest duration to reduce risk of serious adverse effects (i.e. GI complications, CV events, renal toxicity)
To reduce GI complications, use a COX-2 inhibitor or add a PPI even for short term use. Studies show CV risk is similar between naproxen (≤ 750 mg/d), ibuprofen (≤1200mg/d), and celecoxib (≤ 200 mg/d)5,6
ibuprofen Advil, Motrin, G Caps/tabs: 200, 400, 600, 800 mg Advil XR XR tabs: 600 mg
Anti-inflammatory: 400-600 mg TID Low back pain: 300-600 mg TID-QID Mild-moderate pain: 200-800 mg every 6-8 hours Dysmenorrhea: 200-600 mg q6h Headache: 400-800 mg q6h x1-2 doses Gout: 800 mg TID for 5-7 days Maximum: 2400mg per day
GI: dyspepsia, epigastric pain, nausea/vomiting, diarrhea, gastric and duodenal ulcers, GI bleeding. Cardiovascular: MI, stroke, heart failure, fluid retention, hypertension. Nephrotoxicity may occur; avoid NSAIDs in patients with severe renal impairment (CrCl <30 mL/min). CNS: dizziness, drowsiness, headache, tinnitus, confusion (especially in the elderly); CNS effects may be dose related and respond to decreased
Warfarin: increased anticoagulant effect. Antihypertensives (diuretics, beta-blockers, ACE inhibitors, alpha-blockers): possible reduction in antihypertensive effect. Increased risk of GI bleeding with SSRIs. Lithium: Monitor lithium levels when NSAID added. Lithium may interfere with sodium/water balance.
Regular benefit, RDP Reference Drug
$15-30 Available OTC: 200, 400 mg Maximum: 1200 mg/d
naproxen Naprosyn, G Tabs: 250, 375, 500 mg EC Tabs: 250, 375, 500 mg
Anti-inflammatory: 375-500 mg BID Mild-moderate pain: 250-500 mg BID Dysmenorrhea: 500 mg STAT, then 500 mg BID or 250 mg TID-QID Low back pain: 250-375 mg BID-TID
Regular benefit, RDP Reference Drug
$10-20
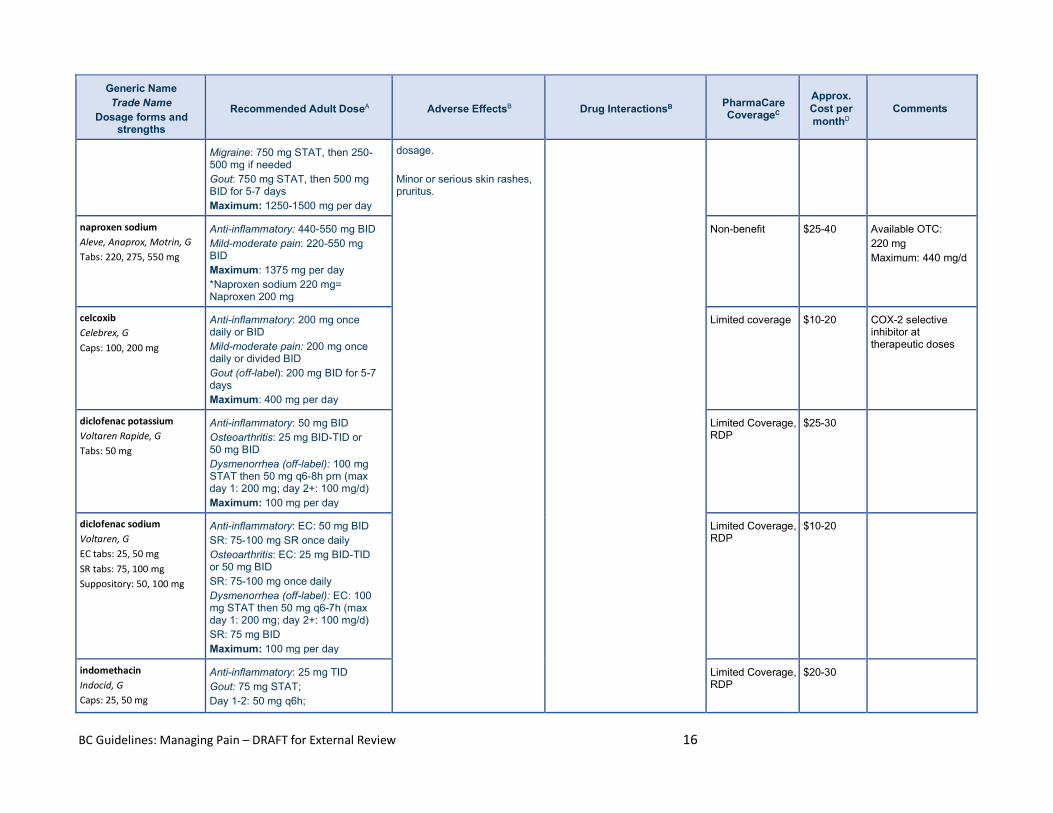
BC Guidelines: Managing Pain – DRAFT for External Review 16
Generic Name Trade Name
Dosage forms and strengths
Recommended Adult DoseA Adverse EffectsB Drug InteractionsB PharmaCare CoverageC
Approx. Cost per monthD
Comments
Migraine: 750 mg STAT, then 250-500 mg if needed Gout: 750 mg STAT, then 500 mg BID for 5-7 days Maximum: 1250-1500 mg per day
dosage. Minor or serious skin rashes, pruritus.
naproxen sodium Aleve, Anaprox, Motrin, G Tabs: 220, 275, 550 mg
Anti-inflammatory: 440-550 mg BID Mild-moderate pain: 220-550 mg BID Maximum: 1375 mg per day *Naproxen sodium 220 mg= Naproxen 200 mg
Non-benefit $25-40 Available OTC: 220 mg Maximum: 440 mg/d
celcoxib Celebrex, G Caps: 100, 200 mg
Anti-inflammatory: 200 mg once daily or BID Mild-moderate pain: 200 mg once daily or divided BID Gout (off-label): 200 mg BID for 5-7 days Maximum: 400 mg per day
Limited coverage $10-20 COX-2 selective inhibitor at therapeutic doses
diclofenac potassium Voltaren Rapide, G Tabs: 50 mg
Anti-inflammatory: 50 mg BID Osteoarthritis: 25 mg BID-TID or 50 mg BID Dysmenorrhea (off-label): 100 mg STAT then 50 mg q6-8h prn (max day 1: 200 mg; day 2+: 100 mg/d) Maximum: 100 mg per day
Limited Coverage, RDP
$25-30
diclofenac sodium Voltaren, G EC tabs: 25, 50 mg SR tabs: 75, 100 mg Suppository: 50, 100 mg
Anti-inflammatory: EC: 50 mg BID SR: 75-100 mg SR once daily Osteoarthritis: EC: 25 mg BID-TID or 50 mg BID SR: 75-100 mg once daily Dysmenorrhea (off-label): EC: 100 mg STAT then 50 mg q6-7h (max day 1: 200 mg; day 2+: 100 mg/d) SR: 75 mg BID Maximum: 100 mg per day
Limited Coverage, RDP
$10-20
indomethacin Indocid, G Caps: 25, 50 mg
Anti-inflammatory: 25 mg TID Gout: 75 mg STAT; Day 1-2: 50 mg q6h;
Limited Coverage, RDP
$20-30
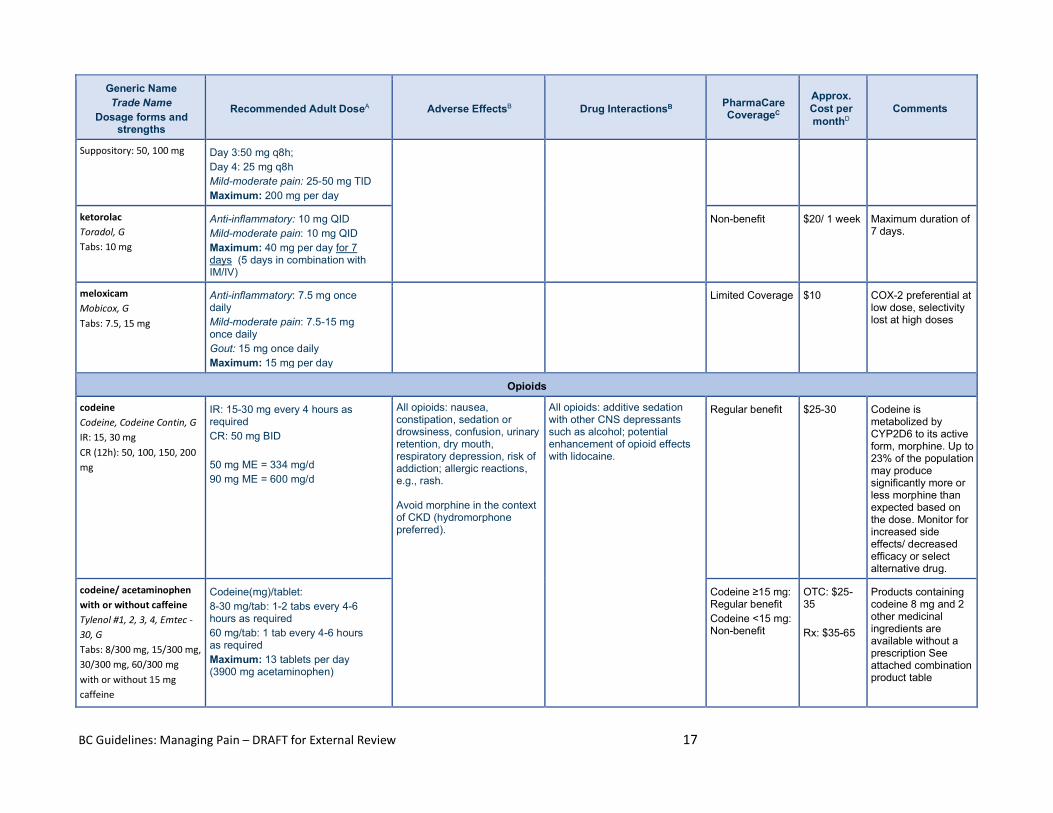
BC Guidelines: Managing Pain – DRAFT for External Review 17
Generic Name Trade Name
Dosage forms and strengths
Recommended Adult DoseA Adverse EffectsB Drug InteractionsB PharmaCare CoverageC
Approx. Cost per monthD
Comments
Suppository: 50, 100 mg Day 3:50 mg q8h; Day 4: 25 mg q8h Mild-moderate pain: 25-50 mg TID Maximum: 200 mg per day
ketorolac Toradol, G Tabs: 10 mg
Anti-inflammatory: 10 mg QID Mild-moderate pain: 10 mg QID Maximum: 40 mg per day for 7 days (5 days in combination with IM/IV)
Non-benefit $20/ 1 week Maximum duration of 7 days.
meloxicam Mobicox, G Tabs: 7.5, 15 mg
Anti-inflammatory: 7.5 mg once daily Mild-moderate pain: 7.5-15 mg once daily Gout: 15 mg once daily Maximum: 15 mg per day
Limited Coverage $10 COX-2 preferential at low dose, selectivity lost at high doses
Opioids
codeine Codeine, Codeine Contin, G IR: 15, 30 mg CR (12h): 50, 100, 150, 200 mg
IR: 15-30 mg every 4 hours as required CR: 50 mg BID 50 mg ME = 334 mg/d 90 mg ME = 600 mg/d
All opioids: nausea, constipation, sedation or drowsiness, confusion, urinary retention, dry mouth, respiratory depression, risk of addiction; allergic reactions, e.g., rash. Avoid morphine in the context of CKD (hydromorphone preferred).
All opioids: additive sedation with other CNS depressants such as alcohol; potential enhancement of opioid effects with lidocaine.
Regular benefit $25-30 Codeine is metabolized by CYP2D6 to its active form, morphine. Up to 23% of the population may produce significantly more or less morphine than expected based on the dose. Monitor for increased side effects/ decreased efficacy or select alternative drug.
codeine/ acetaminophen with or without caffeine Tylenol #1, 2, 3, 4, Emtec -30, G Tabs: 8/300 mg, 15/300 mg, 30/300 mg, 60/300 mg with or without 15 mg caffeine
Codeine(mg)/tablet: 8-30 mg/tab: 1-2 tabs every 4-6 hours as required 60 mg/tab: 1 tab every 4-6 hours as required Maximum: 13 tablets per day (3900 mg acetaminophen)
Codeine ≥15 mg: Regular benefit Codeine <15 mg: Non-benefit
OTC: $25-35 Rx: $35-65
Products containing codeine 8 mg and 2 other medicinal ingredients are available without a prescription See attached combination product table
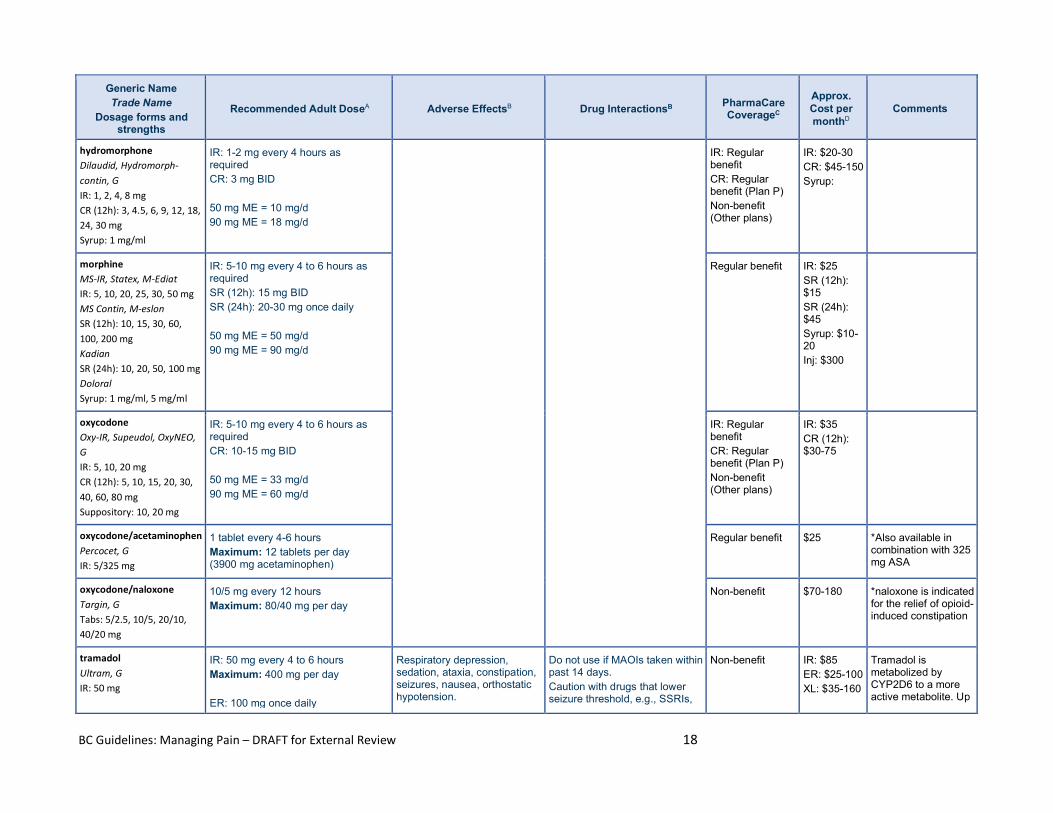
BC Guidelines: Managing Pain – DRAFT for External Review 18
Generic Name Trade Name
Dosage forms and strengths
Recommended Adult DoseA Adverse EffectsB Drug InteractionsB PharmaCare CoverageC
Approx. Cost per monthD
Comments
hydromorphone Dilaudid, Hydromorph-contin, G IR: 1, 2, 4, 8 mg CR (12h): 3, 4.5, 6, 9, 12, 18, 24, 30 mg Syrup: 1 mg/ml
IR: 1-2 mg every 4 hours as required CR: 3 mg BID 50 mg ME = 10 mg/d 90 mg ME = 18 mg/d
IR: Regular benefit CR: Regular benefit (Plan P) Non-benefit (Other plans)
IR: $20-30 CR: $45-150 Syrup:
morphine MS-IR, Statex, M-Ediat IR: 5, 10, 20, 25, 30, 50 mg MS Contin, M-eslon SR (12h): 10, 15, 30, 60, 100, 200 mg Kadian SR (24h): 10, 20, 50, 100 mg Doloral Syrup: 1 mg/ml, 5 mg/ml
IR: 5-10 mg every 4 to 6 hours as required SR (12h): 15 mg BID SR (24h): 20-30 mg once daily 50 mg ME = 50 mg/d 90 mg ME = 90 mg/d
Regular benefit
IR: $25 SR (12h): $15 SR (24h): $45 Syrup: $10-20 Inj: $300
oxycodone Oxy-IR, Supeudol, OxyNEO, G IR: 5, 10, 20 mg CR (12h): 5, 10, 15, 20, 30, 40, 60, 80 mg Suppository: 10, 20 mg
IR: 5-10 mg every 4 to 6 hours as required CR: 10-15 mg BID 50 mg ME = 33 mg/d 90 mg ME = 60 mg/d
IR: Regular benefit CR: Regular benefit (Plan P) Non-benefit (Other plans)
IR: $35 CR (12h): $30-75
oxycodone/acetaminophen Percocet, G IR: 5/325 mg
1 tablet every 4-6 hours Maximum: 12 tablets per day (3900 mg acetaminophen)
Regular benefit $25 *Also available in combination with 325 mg ASA
oxycodone/naloxone Targin, G Tabs: 5/2.5, 10/5, 20/10, 40/20 mg
10/5 mg every 12 hours Maximum: 80/40 mg per day
Non-benefit $70-180 *naloxone is indicated for the relief of opioid-induced constipation
tramadol Ultram, G IR: 50 mg
IR: 50 mg every 4 to 6 hours Maximum: 400 mg per day ER: 100 mg once daily
Respiratory depression, sedation, ataxia, constipation, seizures, nausea, orthostatic hypotension.
Do not use if MAOIs taken within past 14 days. Caution with drugs that lower seizure threshold, e.g., SSRIs,
Non-benefit IR: $85 ER: $25-100 XL: $35-160
Tramadol is metabolized by CYP2D6 to a more active metabolite. Up
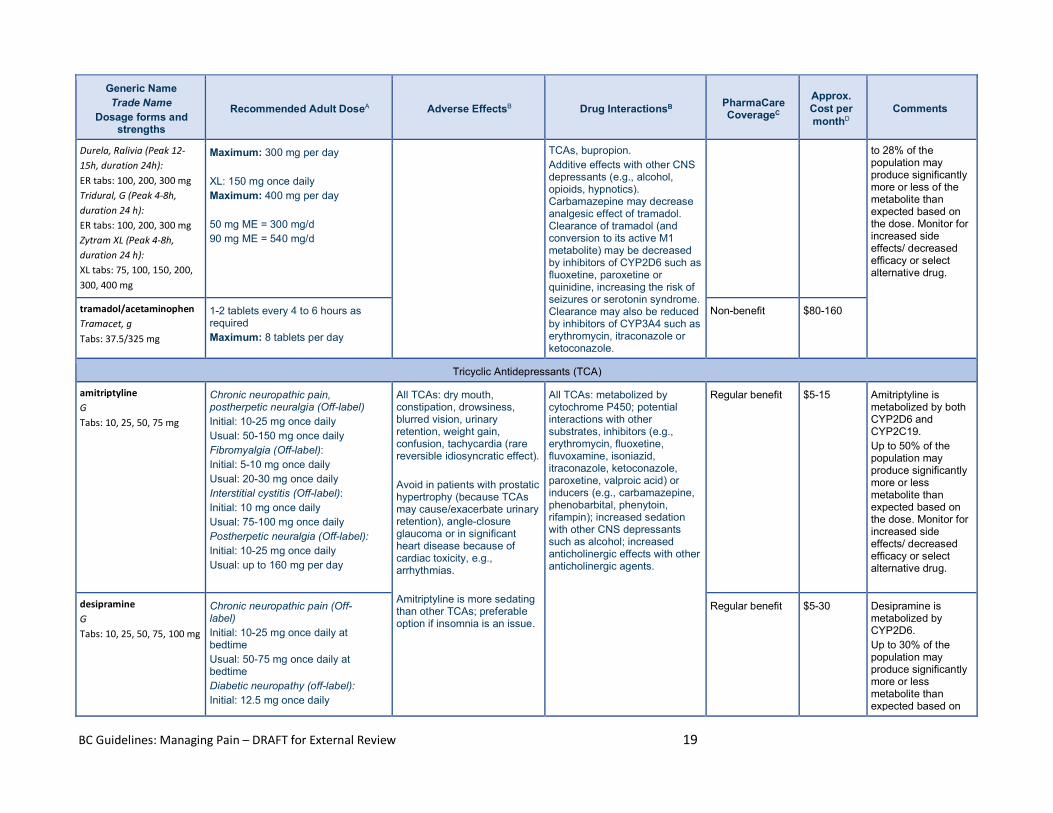
BC Guidelines: Managing Pain – DRAFT for External Review 19
Generic Name Trade Name
Dosage forms and strengths
Recommended Adult DoseA Adverse EffectsB Drug InteractionsB PharmaCare CoverageC
Approx. Cost per monthD
Comments
Durela, Ralivia (Peak 12-15h, duration 24h): ER tabs: 100, 200, 300 mg Tridural, G (Peak 4-8h, duration 24 h): ER tabs: 100, 200, 300 mg Zytram XL (Peak 4-8h, duration 24 h): XL tabs: 75, 100, 150, 200, 300, 400 mg
Maximum: 300 mg per day XL: 150 mg once daily Maximum: 400 mg per day 50 mg ME = 300 mg/d 90 mg ME = 540 mg/d
TCAs, bupropion. Additive effects with other CNS depressants (e.g., alcohol, opioids, hypnotics). Carbamazepine may decrease analgesic effect of tramadol. Clearance of tramadol (and conversion to its active M1 metabolite) may be decreased by inhibitors of CYP2D6 such as fluoxetine, paroxetine or quinidine, increasing the risk of seizures or serotonin syndrome. Clearance may also be reduced by inhibitors of CYP3A4 such as erythromycin, itraconazole or ketoconazole.
to 28% of the population may produce significantly more or less of the metabolite than expected based on the dose. Monitor for increased side effects/ decreased efficacy or select alternative drug.
tramadol/acetaminophen Tramacet, g Tabs: 37.5/325 mg
1-2 tablets every 4 to 6 hours as required Maximum: 8 tablets per day
Non-benefit $80-160
Tricyclic Antidepressants (TCA)
amitriptyline G Tabs: 10, 25, 50, 75 mg
Chronic neuropathic pain, postherpetic neuralgia (Off-label) Initial: 10-25 mg once daily Usual: 50-150 mg once daily Fibromyalgia (Off-label): Initial: 5-10 mg once daily Usual: 20-30 mg once daily Interstitial cystitis (Off-label): Initial: 10 mg once daily Usual: 75-100 mg once daily Postherpetic neuralgia (Off-label): Initial: 10-25 mg once daily Usual: up to 160 mg per day
All TCAs: dry mouth, constipation, drowsiness, blurred vision, urinary retention, weight gain, confusion, tachycardia (rare reversible idiosyncratic effect). Avoid in patients with prostatic hypertrophy (because TCAs may cause/exacerbate urinary retention), angle-closure glaucoma or in significant heart disease because of cardiac toxicity, e.g., arrhythmias. Amitriptyline is more sedating than other TCAs; preferable option if insomnia is an issue.
All TCAs: metabolized by cytochrome P450; potential interactions with other substrates, inhibitors (e.g., erythromycin, fluoxetine, fluvoxamine, isoniazid, itraconazole, ketoconazole, paroxetine, valproic acid) or inducers (e.g., carbamazepine, phenobarbital, phenytoin, rifampin); increased sedation with other CNS depressants such as alcohol; increased anticholinergic effects with other anticholinergic agents.
Regular benefit $5-15 Amitriptyline is metabolized by both CYP2D6 and CYP2C19. Up to 50% of the population may produce significantly more or less metabolite than expected based on the dose. Monitor for increased side effects/ decreased efficacy or select alternative drug.
desipramine G Tabs: 10, 25, 50, 75, 100 mg
Chronic neuropathic pain (Off-label) Initial: 10-25 mg once daily at bedtime Usual: 50-75 mg once daily at bedtime Diabetic neuropathy (off-label): Initial: 12.5 mg once daily
Regular benefit $5-30 Desipramine is metabolized by CYP2D6. Up to 30% of the population may produce significantly more or less metabolite than expected based on
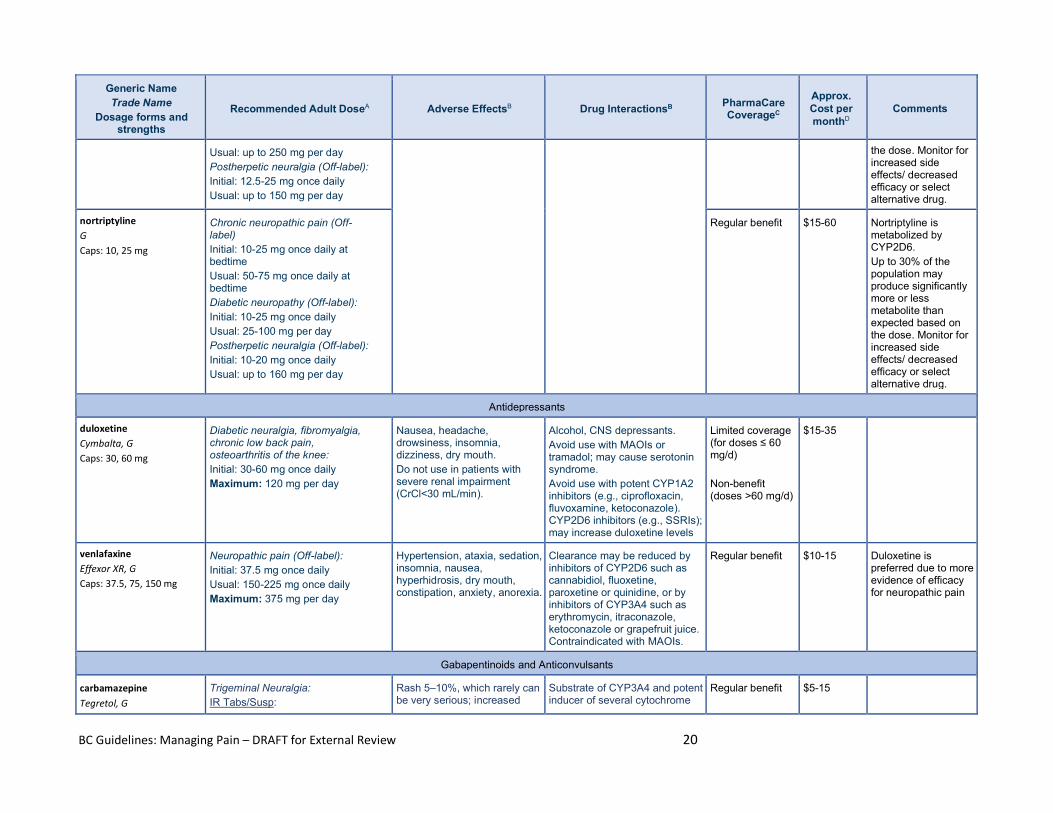
BC Guidelines: Managing Pain – DRAFT for External Review 20
Generic Name Trade Name
Dosage forms and strengths
Recommended Adult DoseA Adverse EffectsB Drug InteractionsB PharmaCare CoverageC
Approx. Cost per monthD
Comments
Usual: up to 250 mg per day Postherpetic neuralgia (Off-label): Initial: 12.5-25 mg once daily Usual: up to 150 mg per day
the dose. Monitor for increased side effects/ decreased efficacy or select alternative drug.
nortriptyline G Caps: 10, 25 mg
Chronic neuropathic pain (Off-label) Initial: 10-25 mg once daily at bedtime Usual: 50-75 mg once daily at bedtime Diabetic neuropathy (Off-label): Initial: 10-25 mg once daily Usual: 25-100 mg per day Postherpetic neuralgia (Off-label): Initial: 10-20 mg once daily Usual: up to 160 mg per day
Regular benefit $15-60 Nortriptyline is metabolized by CYP2D6. Up to 30% of the population may produce significantly more or less metabolite than expected based on the dose. Monitor for increased side effects/ decreased efficacy or select alternative drug.
Antidepressants
duloxetine Cymbalta, G Caps: 30, 60 mg
Diabetic neuralgia, fibromyalgia, chronic low back pain, osteoarthritis of the knee: Initial: 30-60 mg once daily Maximum: 120 mg per day
Nausea, headache, drowsiness, insomnia, dizziness, dry mouth. Do not use in patients with severe renal impairment (CrCl<30 mL/min).
Alcohol, CNS depressants. Avoid use with MAOIs or tramadol; may cause serotonin syndrome. Avoid use with potent CYP1A2 inhibitors (e.g., ciprofloxacin, fluvoxamine, ketoconazole). CYP2D6 inhibitors (e.g., SSRIs); may increase duloxetine levels
Limited coverage (for doses ≤ 60 mg/d) Non-benefit (doses >60 mg/d)
$15-35
venlafaxine Effexor XR, G Caps: 37.5, 75, 150 mg
Neuropathic pain (Off-label): Initial: 37.5 mg once daily Usual: 150-225 mg once daily Maximum: 375 mg per day
Hypertension, ataxia, sedation, insomnia, nausea, hyperhidrosis, dry mouth, constipation, anxiety, anorexia.
Clearance may be reduced by inhibitors of CYP2D6 such as cannabidiol, fluoxetine, paroxetine or quinidine, or by inhibitors of CYP3A4 such as erythromycin, itraconazole, ketoconazole or grapefruit juice. Contraindicated with MAOIs.
Regular benefit $10-15 Duloxetine is preferred due to more evidence of efficacy for neuropathic pain
Gabapentinoids and Anticonvulsants
carbamazepine Tegretol, G
Trigeminal Neuralgia: IR Tabs/Susp:
Rash 5–10%, which rarely can be very serious; increased
Substrate of CYP3A4 and potent inducer of several cytochrome
Regular benefit $5-15
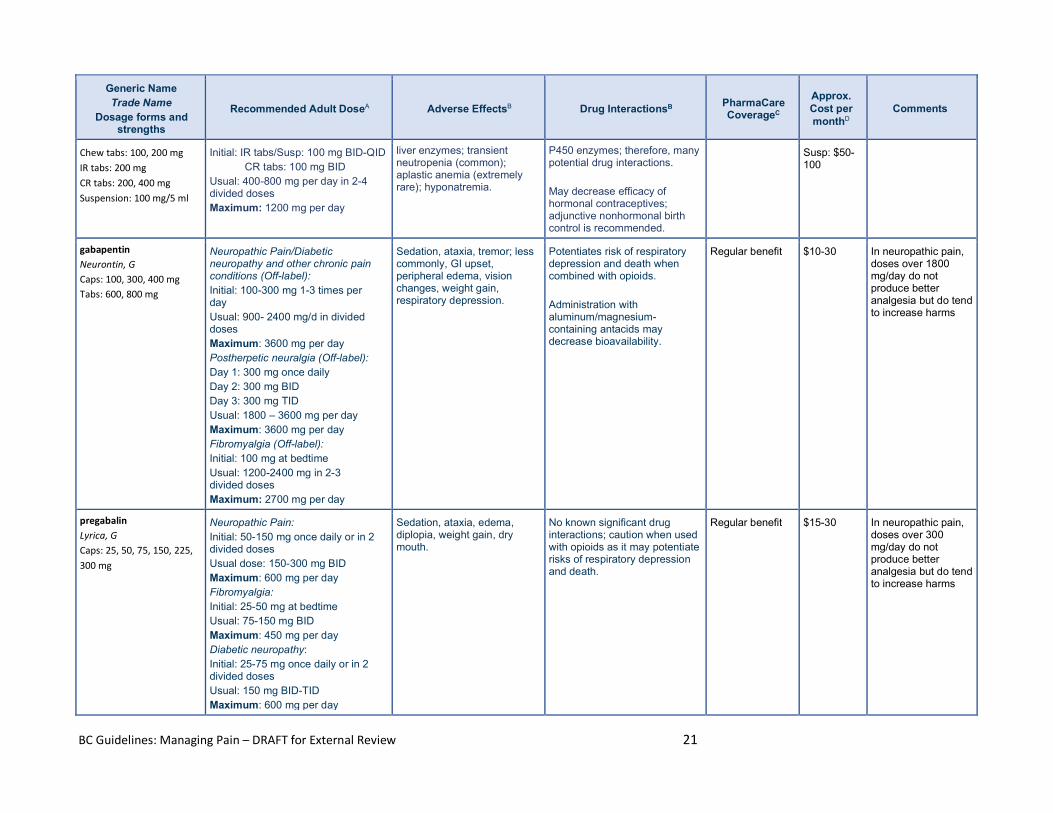
BC Guidelines: Managing Pain – DRAFT for External Review 21
Generic Name Trade Name
Dosage forms and strengths
Recommended Adult DoseA Adverse EffectsB Drug InteractionsB PharmaCare CoverageC
Approx. Cost per monthD
Comments
Chew tabs: 100, 200 mg IR tabs: 200 mg CR tabs: 200, 400 mg Suspension: 100 mg/5 ml
Initial: IR tabs/Susp: 100 mg BID-QID CR tabs: 100 mg BID Usual: 400-800 mg per day in 2-4 divided doses Maximum: 1200 mg per day
liver enzymes; transient neutropenia (common); aplastic anemia (extremely rare); hyponatremia.
P450 enzymes; therefore, many potential drug interactions. May decrease efficacy of hormonal contraceptives; adjunctive nonhormonal birth control is recommended.
Susp: $50-100
gabapentin Neurontin, G Caps: 100, 300, 400 mg Tabs: 600, 800 mg
Neuropathic Pain/Diabetic neuropathy and other chronic pain conditions (Off-label): Initial: 100-300 mg 1-3 times per day Usual: 900- 2400 mg/d in divided doses Maximum: 3600 mg per day Postherpetic neuralgia (Off-label): Day 1: 300 mg once daily Day 2: 300 mg BID Day 3: 300 mg TID Usual: 1800 – 3600 mg per day Maximum: 3600 mg per day Fibromyalgia (Off-label): Initial: 100 mg at bedtime Usual: 1200-2400 mg in 2-3 divided doses Maximum: 2700 mg per day
Sedation, ataxia, tremor; less commonly, GI upset, peripheral edema, vision changes, weight gain, respiratory depression.
Potentiates risk of respiratory depression and death when combined with opioids. Administration with aluminum/magnesium-containing antacids may decrease bioavailability.
Regular benefit $10-30 In neuropathic pain, doses over 1800 mg/day do not produce better analgesia but do tend to increase harms
pregabalin Lyrica, G Caps: 25, 50, 75, 150, 225, 300 mg
Neuropathic Pain: Initial: 50-150 mg once daily or in 2 divided doses Usual dose: 150-300 mg BID Maximum: 600 mg per day Fibromyalgia: Initial: 25-50 mg at bedtime Usual: 75-150 mg BID Maximum: 450 mg per day Diabetic neuropathy: Initial: 25-75 mg once daily or in 2 divided doses Usual: 150 mg BID-TID Maximum: 600 mg per day
Sedation, ataxia, edema, diplopia, weight gain, dry mouth.
No known significant drug interactions; caution when used with opioids as it may potentiate risks of respiratory depression and death.
Regular benefit $15-30 In neuropathic pain, doses over 300 mg/day do not produce better analgesia but do tend to increase harms
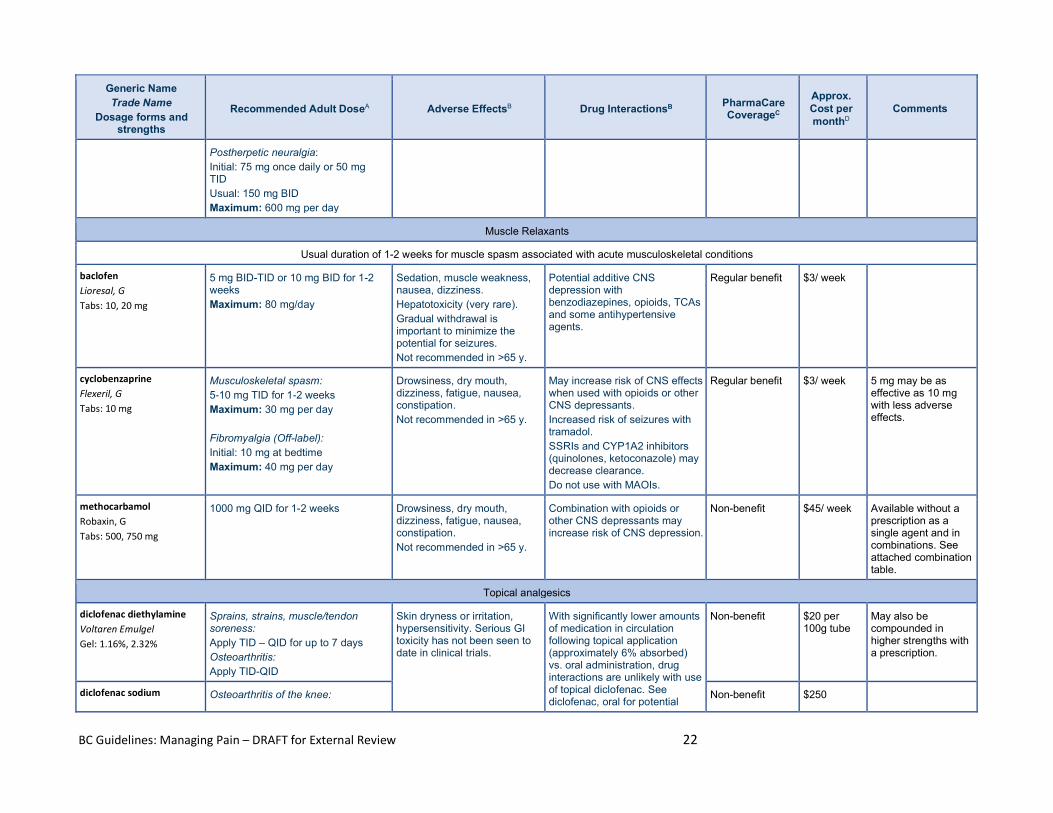
BC Guidelines: Managing Pain – DRAFT for External Review 22
Generic Name Trade Name
Dosage forms and strengths
Recommended Adult DoseA Adverse EffectsB Drug InteractionsB PharmaCare CoverageC
Approx. Cost per monthD
Comments
Postherpetic neuralgia: Initial: 75 mg once daily or 50 mg TID Usual: 150 mg BID Maximum: 600 mg per day
Muscle Relaxants
Usual duration of 1-2 weeks for muscle spasm associated with acute musculoskeletal conditions
baclofen Lioresal, G Tabs: 10, 20 mg
5 mg BID-TID or 10 mg BID for 1-2 weeks Maximum: 80 mg/day
Sedation, muscle weakness, nausea, dizziness. Hepatotoxicity (very rare). Gradual withdrawal is important to minimize the potential for seizures. Not recommended in >65 y.
Potential additive CNS depression with benzodiazepines, opioids, TCAs and some antihypertensive agents.
Regular benefit $3/ week
cyclobenzaprine Flexeril, G Tabs: 10 mg
Musculoskeletal spasm: 5-10 mg TID for 1-2 weeks Maximum: 30 mg per day Fibromyalgia (Off-label): Initial: 10 mg at bedtime Maximum: 40 mg per day
Drowsiness, dry mouth, dizziness, fatigue, nausea, constipation. Not recommended in >65 y.
May increase risk of CNS effects when used with opioids or other CNS depressants. Increased risk of seizures with tramadol. SSRIs and CYP1A2 inhibitors (quinolones, ketoconazole) may decrease clearance. Do not use with MAOIs.
Regular benefit $3/ week 5 mg may be as effective as 10 mg with less adverse effects.
methocarbamol Robaxin, G Tabs: 500, 750 mg
1000 mg QID for 1-2 weeks Drowsiness, dry mouth, dizziness, fatigue, nausea, constipation. Not recommended in >65 y.
Combination with opioids or other CNS depressants may increase risk of CNS depression.
Non-benefit $45/ week Available without a prescription as a single agent and in combinations. See attached combination table.
Topical analgesics
diclofenac diethylamine Voltaren Emulgel Gel: 1.16%, 2.32%
Sprains, strains, muscle/tendon soreness: Apply TID – QID for up to 7 days Osteoarthritis: Apply TID-QID
Skin dryness or irritation, hypersensitivity. Serious GI toxicity has not been seen to date in clinical trials.
With significantly lower amounts of medication in circulation following topical application (approximately 6% absorbed) vs. oral administration, drug interactions are unlikely with use of topical diclofenac. See diclofenac, oral for potential
Non-benefit $20 per 100g tube
May also be compounded in higher strengths with a prescription.
diclofenac sodium Osteoarthritis of the knee: Non-benefit $250
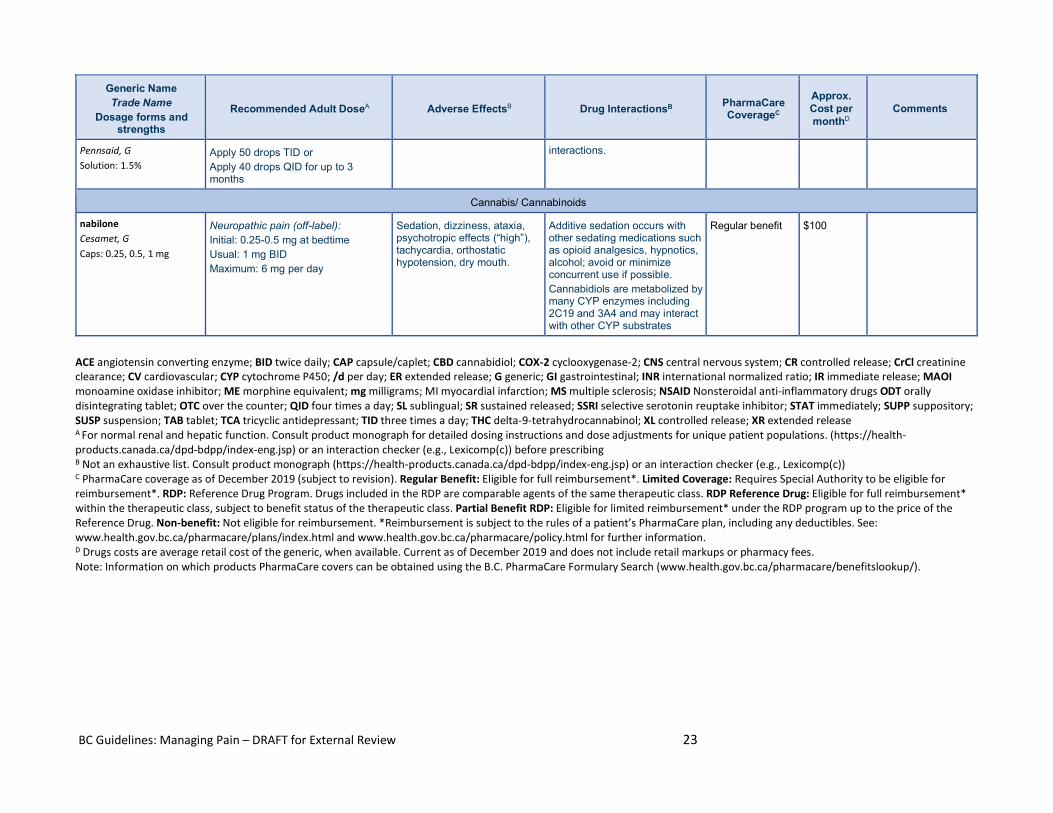
BC Guidelines: Managing Pain – DRAFT for External Review 23
Generic Name Trade Name
Dosage forms and strengths
Recommended Adult DoseA Adverse EffectsB Drug InteractionsB PharmaCare CoverageC
Approx. Cost per monthD
Comments
Pennsaid, G Solution: 1.5%
Apply 50 drops TID or Apply 40 drops QID for up to 3 months
interactions.
Cannabis/ Cannabinoids
nabilone Cesamet, G Caps: 0.25, 0.5, 1 mg
Neuropathic pain (off-label): Initial: 0.25-0.5 mg at bedtime Usual: 1 mg BID Maximum: 6 mg per day
Sedation, dizziness, ataxia, psychotropic effects (“high”), tachycardia, orthostatic hypotension, dry mouth.
Additive sedation occurs with other sedating medications such as opioid analgesics, hypnotics, alcohol; avoid or minimize concurrent use if possible. Cannabidiols are metabolized by many CYP enzymes including 2C19 and 3A4 and may interact with other CYP substrates
Regular benefit $100
ACE angiotensin converting enzyme; BID twice daily; CAP capsule/caplet; CBD cannabidiol; COX-2 cyclooxygenase-2; CNS central nervous system; CR controlled release; CrCl creatinine clearance; CV cardiovascular; CYP cytochrome P450; /d per day; ER extended release; G generic; GI gastrointestinal; INR international normalized ratio; IR immediate release; MAOI monoamine oxidase inhibitor; ME morphine equivalent; mg milligrams; MI myocardial infarction; MS multiple sclerosis; NSAID Nonsteroidal anti-inflammatory drugs ODT orally disintegrating tablet; OTC over the counter; QID four times a day; SL sublingual; SR sustained released; SSRI selective serotonin reuptake inhibitor; STAT immediately; SUPP suppository; SUSP suspension; TAB tablet; TCA tricyclic antidepressant; TID three times a day; THC delta-9-tetrahydrocannabinol; XL controlled release; XR extended release A For normal renal and hepatic function. Consult product monograph for detailed dosing instructions and dose adjustments for unique patient populations. (https://health-products.canada.ca/dpd-bdpp/index-eng.jsp) or an interaction checker (e.g., Lexicomp(c)) before prescribing B Not an exhaustive list. Consult product monograph (https://health-products.canada.ca/dpd-bdpp/index-eng.jsp) or an interaction checker (e.g., Lexicomp(c)) C PharmaCare coverage as of December 2019 (subject to revision). Regular Benefit: Eligible for full reimbursement*. Limited Coverage: Requires Special Authority to be eligible for reimbursement*. RDP: Reference Drug Program. Drugs included in the RDP are comparable agents of the same therapeutic class. RDP Reference Drug: Eligible for full reimbursement* within the therapeutic class, subject to benefit status of the therapeutic class. Partial Benefit RDP: Eligible for limited reimbursement* under the RDP program up to the price of the Reference Drug. Non-benefit: Not eligible for reimbursement. *Reimbursement is subject to the rules of a patient’s PharmaCare plan, including any deductibles. See: www.health.gov.bc.ca/pharmacare/plans/index.html and www.health.gov.bc.ca/pharmacare/policy.html for further information. D Drugs costs are average retail cost of the generic, when available. Current as of December 2019 and does not include retail markups or pharmacy fees. Note: Information on which products PharmaCare covers can be obtained using the B.C. PharmaCare Formulary Search (www.health.gov.bc.ca/pharmacare/benefitslookup/).
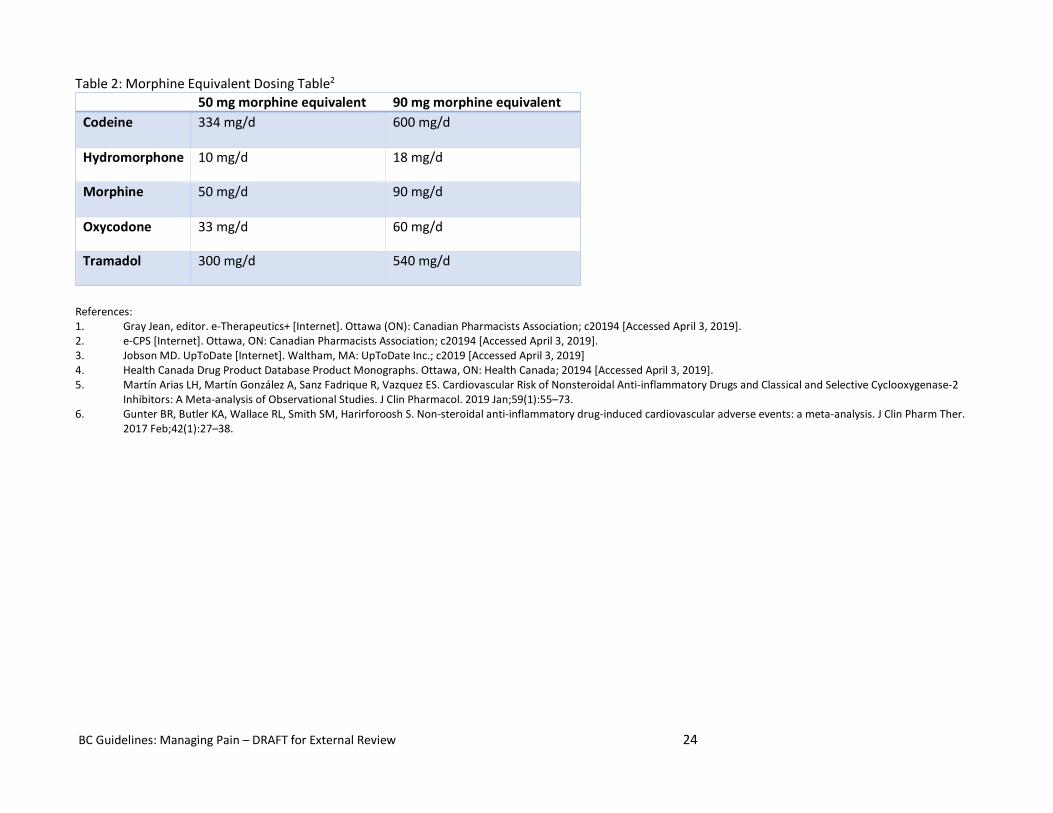
BC Guidelines: Managing Pain – DRAFT for External Review 24
Table 2: Morphine Equivalent Dosing Table2
50 mg morphine equivalent 90 mg morphine equivalent Codeine 334 mg/d 600 mg/d
Hydromorphone 10 mg/d 18 mg/d
Morphine 50 mg/d 90 mg/d
Oxycodone 33 mg/d 60 mg/d
Tramadol 300 mg/d 540 mg/d
References: 1. Gray Jean, editor. e-Therapeutics+ [Internet]. Ottawa (ON): Canadian Pharmacists Association; c20194 [Accessed April 3, 2019]. 2. e-CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; c20194 [Accessed April 3, 2019]. 3. Jobson MD. UpToDate [Internet]. Waltham, MA: UpToDate Inc.; c2019 [Accessed April 3, 2019] 4. Health Canada Drug Product Database Product Monographs. Ottawa, ON: Health Canada; 20194 [Accessed April 3, 2019]. 5. Martín Arias LH, Martín González A, Sanz Fadrique R, Vazquez ES. Cardiovascular Risk of Nonsteroidal Anti-inflammatory Drugs and Classical and Selective Cyclooxygenase-2
Inhibitors: A Meta-analysis of Observational Studies. J Clin Pharmacol. 2019 Jan;59(1):55–73. 6. Gunter BR, Butler KA, Wallace RL, Smith SM, Harirforoosh S. Non-steroidal anti-inflammatory drug-induced cardiovascular adverse events: a meta-analysis. J Clin Pharm Ther.
2017 Feb;42(1):27–38.
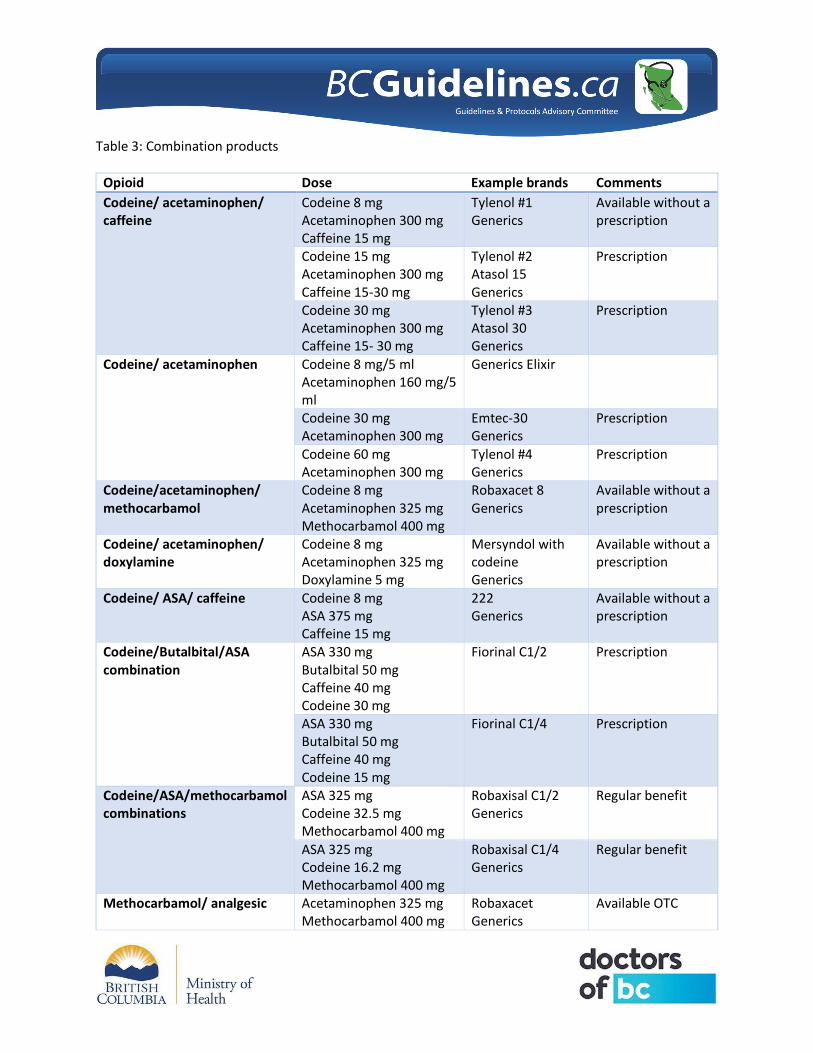
Table 3: Combination products
Opioid Dose Example brands Comments Codeine/ acetaminophen/ caffeine
Codeine 8 mg Acetaminophen 300 mg Caffeine 15 mg
Tylenol #1 Generics
Available without a prescription
Codeine 15 mg Acetaminophen 300 mg Caffeine 15-30 mg
Tylenol #2 Atasol 15 Generics
Prescription
Codeine 30 mg Acetaminophen 300 mg Caffeine 15- 30 mg
Tylenol #3 Atasol 30 Generics
Prescription
Codeine/ acetaminophen Codeine 8 mg/5 ml Acetaminophen 160 mg/5 ml
Generics Elixir
Codeine 30 mg Acetaminophen 300 mg
Emtec-30 Generics
Prescription
Codeine 60 mg Acetaminophen 300 mg
Tylenol #4 Generics
Prescription
Codeine/acetaminophen/ methocarbamol
Codeine 8 mg Acetaminophen 325 mg Methocarbamol 400 mg
Robaxacet 8 Generics
Available without a prescription
Codeine/ acetaminophen/ doxylamine
Codeine 8 mg Acetaminophen 325 mg Doxylamine 5 mg
Mersyndol with codeine Generics
Available without a prescription
Codeine/ ASA/ caffeine Codeine 8 mg ASA 375 mg Caffeine 15 mg
222 Generics
Available without a prescription
Codeine/Butalbital/ASA combination
ASA 330 mg Butalbital 50 mg Caffeine 40 mg Codeine 30 mg
Fiorinal C1/2 Prescription
ASA 330 mg Butalbital 50 mg Caffeine 40 mg Codeine 15 mg
Fiorinal C1/4 Prescription
Codeine/ASA/methocarbamol combinations
ASA 325 mg Codeine 32.5 mg Methocarbamol 400 mg
Robaxisal C1/2 Generics
Regular benefit
ASA 325 mg Codeine 16.2 mg Methocarbamol 400 mg
Robaxisal C1/4 Generics
Regular benefit
Methocarbamol/ analgesic Acetaminophen 325 mg Methocarbamol 400 mg
Robaxacet Generics
Available OTC
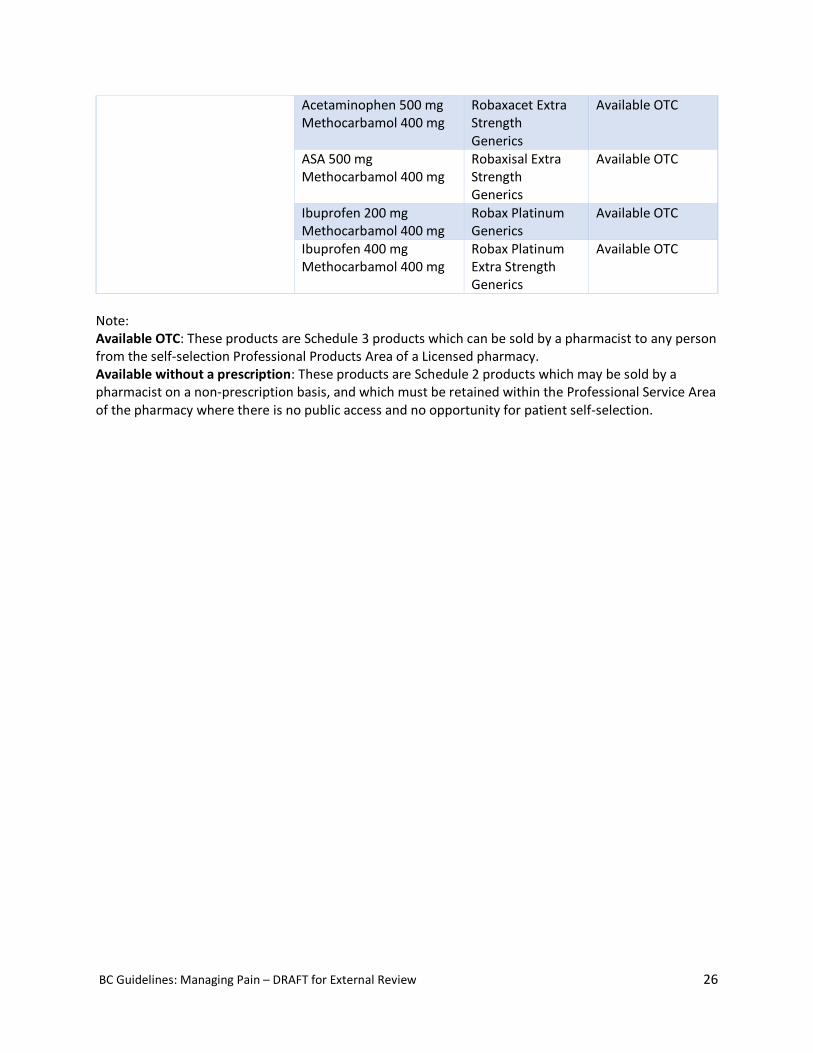
BC Guidelines: Managing Pain – DRAFT for External Review 26
Acetaminophen 500 mg Methocarbamol 400 mg
Robaxacet Extra Strength Generics
Available OTC
ASA 500 mg Methocarbamol 400 mg
Robaxisal Extra Strength Generics
Available OTC
Ibuprofen 200 mg Methocarbamol 400 mg
Robax Platinum Generics
Available OTC
Ibuprofen 400 mg Methocarbamol 400 mg
Robax Platinum Extra Strength Generics
Available OTC
Note: Available OTC: These products are Schedule 3 products which can be sold by a pharmacist to any person from the self-selection Professional Products Area of a Licensed pharmacy. Available without a prescription: These products are Schedule 2 products which may be sold by a pharmacist on a non-prescription basis, and which must be retained within the Professional Service Area of the pharmacy where there is no public access and no opportunity for patient self-selection.
BC Guidelines: Managing Pain – DRAFT for External Review 27
Appendix B: Patient Handout: Initiating Opioids
What you need to know about taking opioid medication
Opioids are a group of medications that are used to help with pain. They include drugs such as morphine, codeine, oxycodone, hydromorphone, tramadol and fentanyl. Methadone is also an opioid. Opioids can be prescribed as a single drug or in combination with other medications including acetaminophen.
1. Opioids are used to reduce disability, improve function and reduce pain. • They may best be used to treat pain, especially acute pain, for a short period of time, if non-
opioid medications are inadequate. • In general, they are less effective for treating chronic pain and may present more risk than non-
opioid and non-pharmacologic treatments. • They are best used in combination with other pain management strategies such as (for example)
manual therapy, exercise and mind-body directed therapies. • We will set goals of treatment and ensure the medication is effective in achieving these goals in
a timely manner. That may include returning to previous activity level or simply becoming more active. Improving activities of daily living function or returning to work may also be important goals to achieve.
• You will need to see your clinician on a regular basis to make sure you are making progress and make sure there are no problematic side effects. If effective the medication may be continued but if it’s not effective or proving unsafe, then a plan to change or taper and stop the medication will occur.
• We will regularly assess whether the medication is still needed, or a dose adjustment is indicated
• If the medication is felt to be not effective or not being safely used, a trial to taper the medication will be suggested, with a goal of reducing or stopping the medication if needed.
2. There may be side effects from opioids, but they can usually be managed by careful initiation and dosage changes.
• Side effects tend to occur when an opioid is initiated. Common ones such as drowsiness and nausea often improve while constipation tends to persist and often needs to be actively managed with laxatives. (Diet is generally not effective, and stool softeners can be added if stools become dry and hard.) If symptoms such as drowsiness, dizziness, nausea or itchy skin persist or are severe, then the drug may just not be tolerated (toxicity or “poor fit”). Stopping the medication is appropriate and consideration of an alternative opioid, is reasonable.
• When initiating or increasing the dose of opioids, drowsiness or mental clouding can occur resulting in a greater risk of car accidents, falls, or fractures. Opioid related drowsiness and mental clouding look different in different patients. Some may experience anxiety and depression, while others may show signs of inattention, fatigue, disorientation and confusion.
• Less common side effects described in a small number of patients include reduced sexual interest and performance, and diminished muscle mass. Both high and low blood sugars and weight gain have been seen in patients treated with methadone, however the relevance of these observations to patients on other opioids for pain is uncertain but reinforces the need for all patients to maximize a healthy balanced diet and maintain a healthy weight.
• The challenge with assessing these risks for individuals is that many variables such as age, pe-existing medical conditions, genetics, kidney function, type of opioid, reason for its use, duration
BC Guidelines: Managing Pain – DRAFT for External Review 28
of use, existing pain and dysfunction (for e.g.) may all impact one’s individual risk of these side effects.
• There is a small risk that taking an opioid may make the pain worse (hyper analgesia) and if that happens the medication will be tapered and stopped.
• Special precautions are usually required if you have sleep apnea, kidney and liver problems, on-going mental health conditions, a history of substance use disorder or are pregnant. Opioids can safely be used in the elderly, but certain opioids are better tolerated and side effects such as dizziness need to be closely monitored.
3. Opioids can be improperly used, especially with prolonged use, including the potential risk of developing a substance use disorder. Your safety is very important, and we will work with you to keep you safe. Everyone who takes opioids regularly will progress to eventual dependence; that is physiologic. There is a small but measurable risk of developing a substance use disorder with the use of prescribed opioids, that it can be difficult to identify who might be at higher risk. While a past history of substance use and/or other mental health diagnoses may indicate a slightly higher risk, by no means does this suggest that opioids cannot be used, it just requires a careful discussion on risks and benefits.
• Addiction usually means you have lost the ability to use the medication in a safe and effective manner, creating danger to yourself and others.
• It is possible that even a short course of opioids can lead to using more or in ways other than prescribed of and dependence on opioids.
• To assist with harm reduction, we can provide you with a take home naloxone kit. Resources for getting help with opioid use disorder are listed at the bottom of this handout.
4. Opioid risks can be reduced by working cooperatively with your clinician. • Take your medication as your clinician prescribed it. Taking more than the prescribed dose puts
you at a greater risk of adverse effects, addiction and overdose. Tell your clinician if you feel unwell or are experiencing side effects.
• Do not drive while your dose is being increased or if the medication is making you drowsy. • Do not use alcohol while on opioids. • Ideally only one clinician should prescribe your opioid medication. In the case your regular
clinician is unavailable, it may be best to see another clinician in the same clinic, so they have access to your records.
• Do not take opioids from someone else and do not share your medication. What is a pain relieving dose for one person can be an overdose for a different person?
• In discussion with your clinician, you will be given a sufficient supply of opioids to last until your next appointment. It is important that you keep your medication in a secure place (especially childproof) and take care to ensure they are not lost or stolen. Random urine drug screens are commonly used and provide an element of safety for you.
5. If you suddenly stop your medication, you will likely experience symptoms of withdrawal. This may include nausea, muscle cramping, agitation, anxiety, runny nose, sweating and yawning.
• Experiencing withdrawal symptoms does not mean you are addicted; just that your body has gotten used to the medication and you stopped too quickly.
• Usually, withdrawal from opioids is not dangerous but for those with other medical conditions including heart problems and the elderly, pregnancy, withdrawal may present a significant health risk.
BC Guidelines: Managing Pain – DRAFT for External Review 29
• If you do stop your medication, especially if you’ve experienced withdrawal symptoms, do not restart your medication without consulting your clinician. There is a significant risk of overdose in that early restarting phase as tolerance to the opioids has been reduced.
6. Overdose from taking opioids as prescribed is very uncommon but you and your family should be aware of the signs.
• The most worrisome signs are loss of consciousness, slowed and difficult breathing or absent breathing and heart rate. Drowsiness progressing to slurred speech, slow breathing and not responding to voice or light touch, may suggest the early signs of an overdose. An overdose tends to occur when the medication is having its peak effect and that is usually within the first 1-3 hrs after an oral dose or within the first 12-30 hrs of starting a fentanyl patch.
• Mixing opioids with alcohol and sedating drugs such as benzodiazepines significantly increase the risk of an overdose. Ensure your clinician knows all the medications you are taking, including over the counter medications or medications you are receiving from other clinicians.
• Overdose is more likely when the dose is increased or restarting after recently stopping. • Make sure that your family and close contacts are aware of the signs of an overdose and call 9-
1-1 as needed. • Speak with your clinician about Narcan (naloxone) – a medication that can reverse opioid
overdose. Discuss how to obtain a kit and ensure family members or others you live with know how to use the kit, if needed in an emergency. Your prescribed opioid medication can be dangerous to others.
• Do not share your medication with others. Your body will get used to the dose your clinician prescribes for you, but it may be dangerous or fatal to others.
• Keep your medication securely stored at home. A bathroom medicine cabinet is not secure. Friends and relatives (including children and teenagers) will have easy access to your medication unless they are safely stored and secured (such as a medication lock box).
Additional Resources • Best Advice for People Taking Opioid medication (Doc Mike Evans video)
o https://www.youtube.com/watch?v=7Na2m7lx-hU • Health Canada Listing of resources for problematic substance use
o https://www.canada.ca/en/health-canada/services/substance-use/get-help/get-help-problematic-substance-use.html?utm_source=Youtube&utm_medium=Video&utm_campaign=EOACSeekHelpCreative2&utm_term=OpioidDrugTreatment
• Mayo Clinic – Patient Information about how Opioid Addiction Occurs o https://www.mayoclinic.org/diseases-conditions/prescription-drug-abuse/in-depth/how-opioid-
addiction-occurs/art-20360372 • Harm Reduction – Where to find a naloxone kit and how to use naloxone
o https://towardtheheart.com/ • Health Link BC
o https://www.healthlinkbc.ca/health-topics/abs2147 • TowardstheHeart • https://towardtheheart.com/naloxone-training
BC Guidelines: Managing Pain – DRAFT for External Review 30
Appendix C: Handout for Patients on Long Term Opioids
A lot has been learned in the past 10-15 years about the use of opioid medication, its uses for chronic pain and the risk of overdose and risk of developing opioid use disorder. We now know that in many cases, the use of opioids for chronic pain is less effective than we thought and that there are many underutilized strategies that can be more effective. As clinicians we also are concerned about the misuse and inappropriate use of opioids. The College of Physicians and Surgeons of BC has created a standard that requires safe, and effect use of narcotics and other medications to manage chronic pain. As clinicians we share this concern for the well-being of our patients and society overall. We have undertaken more training to help us make changes in managing chronic pain, and in particular the prescribing of opioid medication. The main focus of this training is improved patient safety and effective management of chronic pain as part of a provincial, national and international strategy. This review will help you to understand these changes. If you are currently taking or planning to take opioid medications, the process of determining the best medication and dose for you will take some time to do it safely and effectively. If you are joining this practice and are already on opioid medication, then welcome and we trust you will appreciate our concern for your safety and making sure the medications continue to be effective. What will these changes be and how will they affect your care? Education and Medication Review: • We will make sure you fully understand the risks and benefits of all the medication you are taking. • Your care team will make sure that you have an up-to-date care plan and that all the strategies used
to manage your pain are effective. • We will encourage you to review the educational materials we suggest to help manage your pain.
Self-management is the cornerstone of a long-term pain management strategy. • We will need to increase our efforts to make sure we have maximized the use of non-opioid, non-
sedating and non-pharmacological treatment strategies. If something didn’t work in the past it doesn’t mean we can’t reconsider it again or in a different way.
• We will do a Pharmanet search to review all the medications you’ve been prescribed, and this will require your consent. There are many drug interactions that need to be considered as well as some factors such as kidney function and age
Ongoing Monitoring • We will prescribe opioids in a way that will require regular visits to the pharmacy in between regular
visits back to see your prescriber to assess your progress and rewrite your prescription as needed. • We may require random urine drug screens to make sure we both know the medications, both
prescription and non-prescription, you are taking as they may affect the medication we are prescribing for your treatment plan.
Assessing Effectiveness • We will regularly review your need for opioid medication to make sure it remains effective and is
not compromising your safety. • If a medication is not effective or has side effects that persist, we will make a plan to reduce and
discontinue the medication. It is not recommended to suddenly stop a medication until you’ve discussed it with your clinician as this may result in withdrawal symptoms.
BC Guidelines: Managing Pain – DRAFT for External Review 31
• If prescribing a medication to you is proving problematic in terms of personal safety , we will work with you to develop a better safety plan or a strategy to taper and discontinue that medication, while seeking alternative pain management strategies
• Our goal is always to increase function, minimize your disability and keep you safe.
When will these changes take place? • We will be implementing these changes over the next few visits to the clinic. • We will review your medications on a regular basis and always discuss the need for continuing the
opioid, as well as reviewing the effectiveness of these medications.
Why am I being asked to sign a consent to review my medications on Pharmanet? • Pharmanet reviews and the use of random urine drug screens are now part of the College of
Physicians and Surgeons of BC’s standards of care for your safety. Your consent for this review is a requirement of the privacy legislation.
• The goal is to ensure that your clinician has complete and up to date information on all the medications you’ve been prescribed from any source. This includes other family physicians, ER departments, and walk in clinics.
• This information will be treated with the same confidentiality as all your other medical information and will only be shared by other health care providers on a clinical need-to-know basis.
• If you refuse to provide consent to access this information, it will not be safe to prescribe medications to you.
Why am I being asked to do random urine drug screens? What will happen if I test positive for other drugs? What happens if I decline to give a urine sample? • Random urine drug screens may identify drugs in your body that could interact with other
medications and increase your risk of harm. It’s now a standard of care for patients on long-term opioids. It is important to tell your clinician about all the medication you are taking, both prescription and non-prescription.
• If any tests results are unexpected, your clinician will review the results with you and decide what appropriate action to take. You should come to your visits prepared to provide a urine sample if requested. If you are unable to provide a sample when requested, you will likely be asked to provide a sample within a few hours before your prescription is renewed.
• A positive screen does not mean you will be punished or have your medications stopped abruptly. We both need to be very clear we know what drugs you are taking in order to provide the best care possible.
• If you refuse to provide a urine sample, then your clinician will have to reassess their ability to continue to prescribe opioid medication. Ultimately, it’s about your safety and making sure that we are not increasing your risk of harm from taking these medications. Your medications will not be stopped abruptly but a plan will be developed to increase our confidence that we are not putting you at risk. It may involve a change in dispensing protocol to fewer tablets being dispensed, witnessed ingestion or a planned taper and discontinuation.