Agonizing Cancer Pain: Effective Interventional Pain Management
6
255 JIMSA October-December 2013 Vol. 26 No. 4 Agonizing Cancer Pain: Effective Interventional Pain Management Neeraj Jain, Rajeshree Jain 1 Senior Consultant Spine & Pain Specialist, Spine & Pain Clinics & Sri Balaji Action Medical Institute, Max Hospital, Pitampura, New Delhi & Sant Parmanand Hospital, New Delhi. 1 Senior Consultant Gynecologist, Max Hospital, New Delhi. Abstract :Pain is one of the most common symptoms associated with cancer. Pain is defined as “an independent and emotional experience associated with actual or potential tissue damage or described in terms of such damage.” Cancer pain or cancer-related pain distinguishes pain experienced by cancer patients from that experienced by patients without malignancies. Pain occurs in approximately one quarter of patients with newly diagnosed malignancies, one third of patients undergoing treatment, and three quarters of patients with advanced disease. In addition, this is one of the symptoms patients fear most. Unrelieved pain denies them comfort and greatly affects their activities, motivation, interactions with family and friends, and overall quality of life. The importance of relieving pain and the availability of excellent therapies make it imperative that physicians and nurses caring for these patients be adept at the assessment and treatment of cancer pain. This requires familiarity with the pathogenesis of cancer pain; pain assessment techniques; common barriers to the delivery of appropriate analgesia; and pertinent pharmacologic, anesthetic, neurosurgical, and behavioral approaches to the treatment of cancer pain. INTRODUCTION Pain is most agonizing symptom of cancer, the menace. In addition, pain is usually a hallmark of progression or metastatic spread, and 65 to 85 percent of people with cancer have pain when they develop advanced disease. Residual pain is an increasing burden in cancer survivors as well. In 10 to 20 percent of cancer cases, pain is difficult to treat, frustrating, and poorly controlled. Currently, opioid pharmacotherapy is the principal weapon in the fight against cancer pain; but when conservative treatments are unsuccessful, least invasive interventions should be added to optimize pain relief. Interventional pain procedures target neural and non-neural pain generators and neural blockade techniques provide excellent pain relief for neuropathic, sympathetic, nociceptive somatic, or visceral pain. Neural blockade techniques are broadly categorized into non-neurolytic and neurolytic blocks. techniques are employed in sympathetically maintained pain states, ischemic pain, postherpetic neuralgia, and radiation plexopathy NEUROLYTIC BLOCKS Alcohol and phenol are the preferred agents for neurolytic procedures because they cause axonal degeneration within minutes and effectively interrupt the central transmission of pain impulses. Chemical neurolysis can result in immediate and total pain relief in selected patients with localized or regional pain. Opioid requirements decrease sharply, and patients on high doses of opioids will require careful tapering to avoid respiratory depression. Other indications for neurolysis are costopleural syndrome and sympathetically maintained pain in Pancoast’s syndrome. Unfortunately, potentially unacceptable side effects limit the utility of neurolytic blocks; but neurolytic blocks are still preferred over standard opioid analgesia to control intractable abdominal, pelvic, and perineal pain. The following four criteria must be met before a nerve block is considered appropriate: —Limited lifespan of three to six months —A favorable risk to benefit ratio (i.e., the block will not impair bladder or bowel function or cause limb paralysis) — A poor response to primary antitumor treatment, which has not been able to reduce the tumor burden — A good analgesic response and acceptable side effects with prognostic blocks. Advantages: The neurolytic blocks have the following advantages in home care by relatives of patients particularly in rural area of India: 1). Neurolytic blocks provide longer duration of pain relief. 2).Drugs and inexpensive equipment required are readily available.Elaborate equipment is not mandatory. 3). Long-term indoor ward treatment is avoided, repeated visits to the urban pain center are not required. 4). Patient can remain at home pain free even in rural areas where medical help is scarce. Just sympathy is not enough Proactive higher approach is the answer NON-NEUROLYTIC BLOCKS Local anesthetic and corticosteriod blocks are used to treat a variety of pain syndromes. A good response to a prognostic non-neurolytic interventions usually suggest that the patient will benefit from neurolytic procedures as well. Fluoroscopic guidance improves the accuracy of these blocks and minimizes complications. Somatic, sympathetic, and neuropathic pain respond to local anesthetic injections or the continuous administration of anesthetic drugs through a catheter. Intercostal nerve blocks or interpleural analgesia are indicated in post-thoracotomy chest wall pain/intercostal neuralgia, and radiculopathy requires selective nerve root blocks or transforaminal epidural injections when non-invasive treatments fail. Sympathetic blocks and other regional anesthetic Correspondence: Dr Neeraj Jain, Senior Consultant Spine & Pain Specialist, Spine & Pain Clinics & Sri Balaji Action Medical Institute, Max Hospital, Pitampura, New Delhi & Sant Parmanand Hospital, New Delhi. e-mail: [email protected] www.spinenpain.com Table 1. Autonomic Nerve Blocks
-
Upload
maxhealthcare -
Category
Documents
-
view
1 -
download
0
Transcript of Agonizing Cancer Pain: Effective Interventional Pain Management

255JIMSA October-December 2013 Vol. 26 No. 4
Agonizing Cancer Pain:Effective Interventional Pain Management
Neeraj Jain, Rajeshree Jain1
Senior Consultant Spine & Pain Specialist, Spine & Pain Clinics & Sri Balaji Action Medical Institute,Max Hospital, Pitampura, New Delhi & Sant Parmanand Hospital, New Delhi.
1Senior Consultant Gynecologist, Max Hospital, New Delhi.
Abstract:Pain is one of the most common symptoms associated with cancer. Pain is defined as “an independent and emotional experience associatedwith actual or potential tissue damage or described in terms of such damage.” Cancer pain or cancer-related pain distinguishes pain experienced bycancer patients from that experienced by patients without malignancies. Pain occurs in approximately one quarter of patients with newly diagnosedmalignancies, one third of patients undergoing treatment, and three quarters of patients with advanced disease. In addition, this is one of the symptomspatients fear most. Unrelieved pain denies them comfort and greatly affects their activities, motivation, interactions with family and friends, and overallquality of life. The importance of relieving pain and the availability of excellent therapies make it imperative that physicians and nurses caring for thesepatients be adept at the assessment and treatment of cancer pain. This requires familiarity with the pathogenesis of cancer pain; pain assessmenttechniques; common barriers to the delivery of appropriate analgesia; and pertinent pharmacologic, anesthetic, neurosurgical, and behavioralapproaches to the treatment of cancer pain.
INTRODUCTIONPain is most agonizing symptom of cancer, the menace. In addition, painis usually a hallmark of progression or metastatic spread, and 65 to 85percent of people with cancer have pain when they develop advanceddisease. Residual pain is an increasing burden in cancer survivors aswell. In 10 to 20 percent of cancer cases, pain is difficult to treat,frustrating, and poorly controlled. Currently, opioid pharmacotherapy isthe principal weapon in the fight against cancer pain; but whenconservative treatments are unsuccessful, least invasive interventionsshould be added to optimize pain relief. Interventional pain procedurestarget neural and non-neural pain generators and neural blockadetechniques provide excellent pain relief for neuropathic, sympathetic,nociceptive somatic, or visceral pain. Neural blockade techniques arebroadly categorized into non-neurolytic and neurolytic blocks.
techniques are employed in sympathetically maintained pain states,ischemic pain, postherpetic neuralgia, and radiation plexopathy
NEUROLYTIC BLOCKSAlcohol and phenol are the preferred agents for neurolytic proceduresbecause they cause axonal degeneration within minutes and effectivelyinterrupt the central transmission of pain impulses. Chemical neurolysiscan result in immediate and total pain relief in selected patients withlocalized or regional pain. Opioid requirements decrease sharply, andpatients on high doses of opioids will require careful tapering to avoidrespiratory depression. Other indications for neurolysis are costopleuralsyndrome and sympathetically maintained pain in Pancoast’s syndrome.Unfortunately, potentially unacceptable side effects limit the utility ofneurolytic blocks; but neurolytic blocks are still preferred over standardopioid analgesia to control intractable abdominal, pelvic, and perinealpain. The following four criteria must be met before a nerve block isconsidered appropriate: —Limited lifespan of three to six months —Afavorable risk to benefit ratio (i.e., the block will not impair bladder orbowel function or cause limb paralysis) — A poor response to primaryantitumor treatment, which has not been able to reduce the tumor burden— A good analgesic response and acceptable side effects with prognosticblocks.Advantages: The neurolytic blocks have the following advantages inhome care by relatives of patients particularly in rural area of India: 1).Neurolytic blocks provide longer duration of pain relief. 2).Drugs andinexpensive equipment required are readily available.Elaborate equipmentis not mandatory. 3). Long-term indoor ward treatment is avoided, repeatedvisits to the urban pain center are not required. 4). Patient can remain athome pain free even in rural areas where medical help is scarce.
Just sympathy is not enough Proactive higher approach is the answer
NON-NEUROLYTIC BLOCKSLocal anesthetic and corticosteriod blocks are used to treat a variety ofpain syndromes. A good response to a prognostic non-neurolyticinterventions usually suggest that the patient will benefit from neurolyticprocedures as well. Fluoroscopic guidance improves the accuracy of theseblocks and minimizes complications. Somatic, sympathetic, andneuropathic pain respond to local anesthetic injections or the continuousadministration of anesthetic drugs through a catheter. Intercostal nerveblocks or interpleural analgesia are indicated in post-thoracotomy chestwall pain/intercostal neuralgia, and radiculopathy requires selective nerveroot blocks or transforaminal epidural injections when non-invasivetreatments fail. Sympathetic blocks and other regional anesthetic
Correspondence: Dr Neeraj Jain, Senior Consultant Spine & PainSpecialist, Spine & Pain Clinics & Sri Balaji Action Medical Institute,Max Hospital, Pitampura, New Delhi & Sant Parmanand Hospital, NewDelhi. e-mail: [email protected] www.spinenpain.com
Table 1. Autonomic Nerve Blocks

256256 JIMSA October-December 2013 Vol. 26 No. 4
Ganglion Impar Neurolytic Blocks relieve perineal pain from cancerof the cervix, endometrium, bladder, and rectum. The ganglion is a single,midline structure ventral to the sacrococcygeal junction and can beaccessed by a midline trans-sacral approach.Painful input from somatic and visceral structures can producesympathetically maintained pain (SMP) that may be visceral orneuropathic in nature. Sympathetic Ganglion Neurolysis relieves SMPand improves blood flow and is used to treat pain from radiationplexopathy, phantom pain, herpes zoster, vascular insufficiency secondaryto malignancy, and complex regional pain syndromes (reflex sympatheticdystrophy and causalgia), with little risk of motor or sensory loss ordeafferentation pain. The trigeminal nerve receives sensory input from the skin of the face,anterior two-thirds of the tongue, and oronasal mucosa. AnestheticBlockade Or Chemical Rhizolysis of the trigeminal ganglion or itsindividual branches is indicated in orofacial malignancies with intractablehead and face pain.Neurolytic Spinal Blockade can produce profound segmental analgesia.Nociceptive input is interrupted by selectively destroying the dorsal rootsand rootlets between the spinal cord and the dorsal root ganglia. Theprocedure is reserved for terminally ill patients with cancer who have ashort life expectancy and unilateral somatic pain localized to a fewadjacent dermatomes, ideally in the trunk and distant from sphincter orlimb innervation. Combined with a unilateral cordotomy, subarachnoidalcohol/ phenol blocks effectively control pain in costopleural syndrome,which is caused by invasion of the pleural cavity and thoracic wall.Adverse effects include PDPH, meningitis (rarely), persistent numbnessand paresthesia, loss of motor function due to the unintended neurolysis
Phenol Intrathecal Neurolysis Alcohol Intraspinal Tunneled Catheter
Neurolytic Celiac Plexus Blocks (NCPB) And Splanchnic NerveBlocks (SNB) are routinely performed (and are preferred over standardanalgesic therapies) for patients with intractable pain from hepato-biliary,pancreatic and upper gastrointestinal cancer. NCPBs provide immediateand substantial pain relief in 70 to 90 percent of cases, improve the patient’squality of life, and significantly reduce opioid intake. The procedure canbe repeated in three to six months if the effect of the initial block wearsoff. NCPBs are performed percutaneously or intraoperatively. Underradiologic guidance, 50-100% alcohol or 6% phenol is instilled anteriorto the aorta at the level of the L1 vertebral body. Injection site pain, diarrhea,and temporary hypotension are transient adverse effects. A lowcomplication rate is observed, since the risk of the neurolytic agentspreading to the somatic nerves supplying the lower limbs, bladder, andbowel is minimal.Superior Hypogastric Plexus Blocks (SHPB) are indicated forunrelenting pain from cancer of the pelvic viscera. This plexus lies infront of the L5 and S1 vertebrae in the prevertebral space. A spinal needleis placed percutaneously in this space from the back under radiologicguidance. Excellent analgesia is reported by 70 percent of patients after aSHPB. Reductions in pain scores and opioid consumption are reported tobe significant, even in patients with advanced disease. No majorcomplications have been reported following SHPBs, although a potentialrisk exists for the spread of neurolytic agents to the nerve fibers controllingmicturition, bowel motility, and sexual function. The SHPB block can berepeated if pain recurs. Patients who fail two consecutive attempts arecandidates for intraspinal opioid analgesia.
TRANS-SPHENOID PITUITARYNEUROABLATIONVery useful simple intervention with 70-80% success rate in diffuse cancers ofadvanced stage with multiple bony & spinal metastasis especially hormonedependent cancers not responding to all other measures.Intraspinal Opioid Therapy continued administration of opioids intrathecallyor epidurally with or without lower concentration of local anesthetic & adjuvantdrugs is an important option for patients with thoracic, abdominal or pelviccancer pain that is refractory to conventional pharmacologic management.Advantages include profound analgesia, often at a much lower opioid dosewithout the motor, sensory, or sympathetic block. However combinations oflow-dose opioids given epidurally with a local anesthetic act synergistically toproduce effective analgesia while decreasing their side effects. Administrationcan be carried out using a variety of drug-delivery systems ranging from atemporary percutaneous epidural catheter to a totally implanted pump system.The effectiveness of preimplantation procedure and reversibility of effect makesthis an attractive treatment option.Vertebroplasty for Metastatic VB #, Multiple Myeloma VB # (3%).Approximately 30% of patients with various neoplastic conditions developsymptomatic spinal metastases during the course of their illness & pain is thepresenting complaint in the majority of cases.
CONCLUSIONThe management of patients with cancer pain can be a challenging task, evenfor physicians trained in cancer pain management Effectively relieving pain incancer patients requires a range of treatment alternatives, including neuralblockade when the patient’s pain no longer responds to opioid analgesia. Thetype of neural block selected is determined by the location and mechanism ofthe pain, the physical status of the patient, the extent of tumor spread, and thetechnical skill and experience of the doctor performing the intervention. Non-neurolytic blocks can provide safe and effective analgesia for the less seriousconditions indicated above. Neurolytic blocks, with their potential forcomplications, are reserved for select patients who are unresponsive to standardanalgesic pharmacotherapy and/or are at a more advanced stage of disease.However, only few would question that aggressive intervention is oftenappropriate. Neurolytic nerve blocks offer an excellent option for the physicianin the fight to control cancer pain. Such blocks can be easily utilized to helpprovide pain relief in most of the cancer patients at the utmost needed times.
BIBLIOGRAPHY1. Hewitt DJ. The management of pain in the oncology patient. Obstetrics and Gynecology clinics of
North America 2001;28(4):819-46.2. Cohen MZ, Easley MK, Ellis C et al. Cancer pain management and the JCAHO’s pain standards:
an institutional challenge. J Pain Symptom Manage 2003;25(6):519-27.3. Goudas LC, Bloch R, Gialeli-Goudas M et al. The epidemiology of cancer pain. Cancer Invest
2005;23(2):182-90.4. Svendsen KB, Andersen S, Arnason S et al. Breakthrough pain in malignant and non-malignant
diseases: a review of prevalence, characteristics and mechanisms. Eur J Pain 2005;9(2):195-206.5. Cleeland CS, Gonin R, Hatfield AK et al. Pain and its treatment in outpatients with metastatic
cancer. N Engl J Med 1994;330:592-596.6. Martin LA, Hagen NA. Neuropathic pain in cancer patients: Mechanisms, syndromes, and clini-
cal controversies. J Pain Symptom Manage 1997;14:99-117.7. Panchal SJ. Intrathecal Pumps. Techniques in Regional Anesthesia and Pain Management
2000;4(3):137-142.
of ventral rootlets, and sphincter and limb weakness.
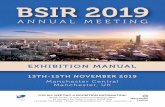
CT Guided Celiac Superior Hypogastric Pituitary NeuroablationPlexus Block Block

257JIMSA October-December 2013 Vol. 26 No. 4

258258 JIMSA October-December 2013 Vol. 26 No. 4

259JIMSA October-December 2013 Vol. 26 No. 4
AAbdominal Cocoon: A Rare Cause of Intestinal Obstruction: A Case Report. 110
A Double-Blind, Placebo Controlled, Randomised Comparison of Pre& Post operative administration of Tramadol for Dental Extraction Pain. 97
Agonizing Cancer Pain: Effective Interventional Pain Management 255
Anesthetic Considerations in Paediatric Patients. 127Angiofibroma masquerading as a Cheek Swelling – A Diagnostic Dilemma. 111
Anomalous third head of Biceps brachii and Pronator teres in Single Cadaver. 224
Anorectal Manometry: Current Techniques and Indications. 169Anterior Jugular Phlebectasia: Diagnosis by Multislice CT 157
An Unusual Presentation of Acute Gastroenteritis Caused by Elizabethkingia
Meningoseptica in a Child with Sepsis from Rural Karnataka-A Case Report. 114A randomized, placebo controlled study evaluating preventive role of ondansetron, 217
dexamethasone and ondansetron plus dexamethasone for postoperative
nausea and vomiting (PONV) in patients undergoing laparoscopiccholecystectomy
Arthrogryposis : A Case Report 221
Association of HepatitisB&C with HIV / AIDS: Management Issues. 89A Study of Clinical Profile of Neurofibromatosis. 103
Atracurium Anaphylaxis: A Case Report and Review of Literature. 115
B
Bariatric Surgery: An Overview. 137
Bariatric Surgery for Treatment of Obstructive Sleep Apnea. 142Bariatric Surgical Procedures. 138
Biofeedback in Obstructed Defaecation Syndrome. 195
Botulinum Toxin treatment for Anal Fissures – An overview & The first report 197on experience of BTX from India
Bronchial Artery Embolozation in Pulmonary Diseases: Current Scenario 69
C
Choledochoduodenal Fistula: A Rare Case Report With Review Of Literature 226Computed Tomography in the 21st Century: Current Status & Future Prospects... 35
Computers in Radiology: Few Recent Advance 17
Conjoined Twins : Parapagus Twins 229Congenital Black Hairy Nevus 230
Coronary Artery Disease and Periodontitis: A Prospective Study. 93
Current Perspectives in Management of Rectal Prolapse. 179
D
Derriere Distress - Defecation - Deification 155
Doppler Changes In Pre-Eclampsia 215
Dynamic Musculoskeletal Sonography 21
E
Elastography: A New Imaging Technique and its Application 25Entrance Skin Dose Estimation In X-Ray Lumbar Spine Lateral Procedure: 219Coventional Vs Digital X-Ray Units
Evaluation of Obstructed Defaecation Syndrome 167
F
Fusion Imaging: Current Trends 73Future of Pediatric Radiology in India 77
G
Gullian- Barre Syndrome associated with Herpes Zoster Virus - Infection 123- A Case Report.
H
Hamartomatous Duodenal Polyp leading to Duodeno - Jejunal Intussusception - 121A Rare Case Report.
I
Idiopathic Hypogonadotrophic Hypogonadism (IHH) With Pickwikian Syndrome, 227Cor Pulmonale and Insulin Resistance.
Ileal Pouch Anal Anastomosis. 191
Subject Index
Imaging of Obstructed Defaecation Syndrome. 163Imaging in Obstructive Jaundice: A Review with Our Experience. 43
Infective Arthritis of Hip: Role of Sonography 15
Indications and Risks of Vacuum Assisted Deliveries 213Intussusception due to Jejunal Lipoma: A Case Report 112
Isolated Spontaneous Gall Bladder Perforation in a Child – A Rare Case Report. 109
Is Severity of Cholecystitis related to Body Mass Index? 101
M
Management of Constipation. 173
Management of Lefort Fractures using External Skeletal Fixator : 124
Two Case Reports.Meckel’s Diverticulum Presenting as Intestinal Obstruction due 122
to Faecal Impaction – A Rare Case Report.
N
New Advances in MRI. 59
O
Open versus Closed Lateral Internal Anal Sphincterotomy for 177the Treatment of Fissure in ANO - A Rural Indian Experience.
P
Pain Management: A New Super-Specialty 243Pictorial CME 239
Pitting Edema in Hypothyroidism. 133
Primary adenocarcinoma ileum presenting as perforation – A review of literature 223Prophylactic Antibiotics in Surgery 207
R
Radiological Imaging in Trigeminal Nerve Schwannoma: A Case Report 117
and Review of Literature.Recurremt Chronic Pancreatitis due to Pancreas Divisum: Diagnosis By 55
Multislice CT
Refractory Hypokalemia: A Rare Presentation of Hypomagnesemia 107Role of antibiotic prophylaxis in laparoscopic cholecystectomy ?
Role of Imaging in Subclinical Atherosclerosis 31
Role of Multi Slice CT in Abdominal Tuberculosis. 47Role of Multi Spiral C.T. in the Evaluation of Neck Masses 51
S
Sacrococcygeal Teratoma: A Case Report 222
Scenario-specific, statistically sound, problem- driven approach to 235data analysis – a robust tool for future health managers
Seroprevalence of Hepatitis B and C Co-Infection in HIV Positive Patients 91
from a Tertiary Care Hospital.“Slip Disc with Sciatica – Newer Non-Surgical Treatment” 249
Sonographic Evaluation of Clubfoot 9
Stapled Anopexy- How I Do It? 183STARR Procedure for Obstructed Defecation Syndrome. How I do it? 171
Staged Surgical Management Of Rheumatoid Arthiritis Of Wrist 231
Surgical Approach to an Adult with Altered Bowel Habit. 185Surgical Cure for Type II Diabetes-From Bariatric Surgery to Metabolic Surgery. 140
Surgeon’s Domain: From Organic Constipation to Idiopathic Constipation. 161
T
The Management Of Intractable Low Back Pain: Recent Advances 245
The Prayer Sign. 133The Young And The Bold 157
Transverse Testicular Ectopia-A Case Report and A Review of Literature. 119
Trifid Tongue 228
V
Vascular Imaging: Past, Present & Future 65
Vertebroplasty/Kyphoplasty: A Novel Approach for Treatment of Spine Fractures 251

260260 JIMSA October-December 2013 Vol. 26 No. 4
A
Acharya Sourya 227Agarwal Brij B. 155, 161, 171,207Aggarwal H. K. 107Agarwal Krishna Adit 157Aggarwal Sandeep 137, 138, 140, 142Ahuja Ruchi 124Ahuja Sanjiv 91Anand Santosh 138Angelina J. Tracy Tina 219Arora Anil 169Arora Aparajita 157Arora Shobha S. 9Aroor Shrikiran 114Ashish S. R 215, 226
B
Badar Nazia 213Bal M.S. 223Balakrishnan Abirhami 114Ballal Mamatha 114Bansal J K 115Bansal Naresh 169Bansal Teena 127Bhalla Ashu 69Bhargava Satish Kumar 9,15,21,25,43,47,51,55,57Bhargava Sumeet 9,15,21,25,43,47,51,55,57Bhaskar M. 119Bhatt Shuchi 9,21,31,43,5Bhattacharjee Hemanga 142
C
Chakraborty Rituparna 114Chandra Hem 235Chaudhry Navneet 121Chauhan Ankit 91Chintamani 155
D
Dabar S. S. 112Dey Ashish 183Dhawan Mrinal 157Dubhashi Siddharth P. 101
G
Garg Dinesh 115Garg Kamlesh 173Garga U.C. 117Gautam R. M. 177Gore Pravin P. 197Ghonge Nitin P. 35Gupta Pushpender 51,55,57Gupta Ridhima 55, 57Gupta PC 65Gupta Tarana 107Govindasamy Mahendran 191Gupta Himanshu 123, 239Gupta Renu 224Gupta Vikas 231
H
Hans Charoo 91Hafeez Maimoona 213Harish H. 215Hooda Sarla 127
I
Inderjit I.K 17
Author Index
J
JadhavVijay 59Jagadeesan K. 219Jagadeesan Kesav 219Jathar Chetan 59Jana Manisha 69Jain Ashok 245Jain Deepak 107Jain Neeraj 243, 245, 249, 251, 255Jain Pankaj 169Jain Rajeshree 255Jain Seema 243Jindal Saurabh 109, 110, 122J. Rajasekar Sandeep 119
K
K. Mohandas 219Kalaiselvan Dhinesh B. 119Kalayarasan R. 185Kamaldeep 228Kar Premashis 89Kamat Ritesh 163Kaur Vineet 112, 115Khan Farhan Ahamad 97Khandelwal Niranjan 77Kishore LT 65Koirala Rabin 191Korath M.Kaul 219Kothari Nirmesh 227Kumar Ashwani 43,209,217, 221Kumar Pradeep 47Kumari Rima 43Kumaran Vinay 191Kuldish 230
M
Mahajan Amit 121Mahajan K. C. 155Mahajan S. N. 227Malhotra Shalini 91Malhotra Sumit 93Mallarajapatna Govindarajan Janardan 73Malik Vinod K 183Mallikarjunappa B. 215, 221, 222, 227Masih Leela 235Mehra P. 124Mehra Shibani 117Mehta Naimish 191Mehrotra Gopesh 51Mishra Hitesh 97Mundkur Suneel 114
N
Nabi Tauqeer 235Nag Hirdaya H. 185Nagaraja BT 222Narayanan Vivek 231Neki N. S. 123, 133, 239Nundy Samiran 191
PPahwa Siddharth 209Pandey Sharad 109Pandove P. K. 209, 217, 223Pant Pooja 157Panicker T.M.R. 219Parkash Hari 93Patkar Deepak 59Patankar Roy 167, 195Patel Shruti 110Patodia Madhusudan 209, 217,223
Poonia Anil Kumar 229Prakash Meenakshi 9, 25Puri Neerja 103Pukale Ravindra S 215
RRahesuddin 235Rajalingam Vijianthy 114Ranjan Piyush 169Rathi Vineeta 51Rastogi Rajul 73Ravinthar A. 119Ray S.B. 224Rinkoo Arvind Vashishta 235Rohilla Kshitiz 111
S
Sachdeva Munish 169Sanjeev 230Sandhu Sartaj 122Saravanan P. S. 119Saxena Akshay Kumar 77Setia Suman 112Sharda V. K. 209, 217, 223Sharma Aditya P 137Sharma S 69Sharma Sanjay 25Sharma Shruti 161Singh Gurinder 115Singh Ishu 123Singh Kuldip 109Singh Jaswir 228, 229, 230Singh Mohinder 109, 110Singh Sarabjit 112, 115Singh Surendra Pratap 235Singh Vineet 111Sircar Pankaj 121Shruthi K M. 221Shukla Samarth 227Sodhi Kushaljit Singh 77Sood Dinkar 109Sriram K 111Srivastava Deep Narayan 69Suresh 117
T
T. Trinath 101Tamilmani 123, 239Tandon Anupama 9, 21, 31Thakur Mukund 179Thapar Ravi 163Thulkar S 69Thingujam Usha 43Tripathi C. D. 173
U
Upadhyay Shekhar 121Upasani Abhay 195
VV. Ramesh 111Varma Vibha 191
WWahal Akshat 140Wani Sachin 167, 195
YYadav R. K. 107Yasin Asma 213