
The Next Phase of IT Outsourcing - Utility Computing: Understanding Utility Computing Acceptance

lable at ScienceDirect
Manual Therapy xxx (2014) 1e9
Contents lists avai
Manual Therapy
journal homepage: www.elsevier .com/math
Original article
The clinical utility of pain classification in non-specific arm pain
Niamh A. Moloney a, b, *, Toby M. Hall c, d, Andrew M. Leaver b, Catherine M. Doody a
a UCD School of Public Health, Physiotherapy and Population Science, University College Dublin, Belfield, Dublin 4, Irelandb Discipline of Physiotherapy, Faculty of Health Sciences, The University of Sydney, PO Box 170, Lidcombe, NSW 1825, Australiac School of Physiotherapy, Curtin Health Innovation Research, Curtin University of Technology, G.P.O. Box U1987, Perth, WA 6845, Australiad Manual Concepts, P.O. Box 1236, Booragoon, WA 6954, Australia
a r t i c l e i n f o
Article history:Received 18 February 2014Received in revised form4 August 2014Accepted 26 August 2014
Keywords:Pain classificationNon-specific arm painInter-rater agreementNeuropathic pain
* Corresponding author. Discipline of PhysiotherapThe University of Sydney, PO Box 170, Lidcombe, NSW9351 9266; fax: þ61 293519278.
E-mail address: [email protected] (N
http://dx.doi.org/10.1016/j.math.2014.08.0101356-689X/© 2014 Elsevier Ltd. All rights reserved.
Please cite this article in press as: Moloney Nhttp://dx.doi.org/10.1016/j.math.2014.08.010
a b s t r a c t
Mechanisms-based pain classification has received considerable attention recently for its potential use inclinical decision making. A number of algorithms for pain classification have been proposed. Non-specificarm pain (NSAP) is a poorly defined condition, which could benefit from classification according to painmechanisms to improve treatment selection. This study used three published classification algorithms(hereafter called NeuPSIG, Smart, Schafer) to investigate the frequency of different pain classifications inNSAP and the clinical utility of these systems in assessing NSAP.
Forty people with NSAP underwent a clinical examination and quantitative sensory testing. Findingswere used to classify participants according to three classification algorithms. Frequency of pain clas-sification including number unclassified was analysed using descriptive statistics. Inter-rater agreementwas analysed using kappa coefficients.
NSAP was primarily classified as ‘unlikely neuropathic pain’ using NeuPSIG criteria, ‘peripheralneuropathic pain’ using the Smart classification and ‘peripheral nerve sensitisation’ using the Schaferalgorithm. Two of the three algorithms allowed classification of all but one participant; up to 45% ofparticipants (n ¼ 18) were categorised as mixed by the Smart classification. Inter-rater agreement wasgood for the Schafer algorithm (к ¼ 0.78) and moderate for the Smart classification (к ¼ 0.40). A kappavalue was unattainable for the NeuPSIG algorithm but agreement was high.
Pain classification was achievable with high inter-rater agreement for two of the three algorithmsassessed. The Smart classification may be useful but requires further direction regarding the use ofclinical criteria included. The impact of adding a pain classification to clinical assessment on patientoutcomes needs to be evaluated.
© 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Classification of pain based on pathophysiological mechanismshas received considerable attention (Woolf et al., 1998; Hansson,2002; Freynhagan et al., 2008; Scholz et al., 2009; Nijs et al.,2010; Kindler et al., 2011; Schafer et al., 2011; Woolf, 2011; Smartet al., 2012) and is increasingly used in diagnosis and manage-ment of musculoskeletal conditions. In musculoskeletal conditions,there is often a poor relationship between pathology, pain anddisability (Kanayama et al., 2009), as well as high prevalence ofundiagnosed disorders (Walker-Bone et al., 2004; Beaudet et al.,2013), suggesting the potential clinical value of mechanisms-based pain classification (Woolf et al., 1998).
y, Faculty of Health Sciences,1825, Australia. Tel.: þ61 2
.A. Moloney).
A, et al., The clinical utility o
In the absence of a gold standard classification, a number ofmechanisms based algorithms have been proposed (Schafer et al.,2009; Haanp€a€a et al., 2011; Smart et al., 2012). The classificationalgorithm endorsed by the Neuropathic Pain Special Interest Group(NeuPSIG) of the International Association for the Study of Pain(Treede et al., 2008; Haanp€a€a et al., 2011) classifies patients into oneof four groups; Definite-, Probable-, Possible-, and Unconfirmed-Neuropathic pain, based on the number of corroborative signs(Fig. 1). The ‘NeuPSIG algorithm’ is a consensus document of Neu-PSIG and its reliability or validity have not been formally tested.
Classification criteria outlined by Smart et al. (2012), for chroniclow back pain (± leg pain), classifies patients into three groups(nociceptive-, peripheral neuropathic- and central sensitisationpain) (Fig. 2). There is preliminary evidence for the validity of the‘Smart classification’ when used in a low back pain population(Smart et al., 2012).
The algorithm of Schafer et al. (2009) for classification of low-back related leg pain classifies patients into four groups
f pain classification in non-specific arm pain, Manual Therapy (2014),
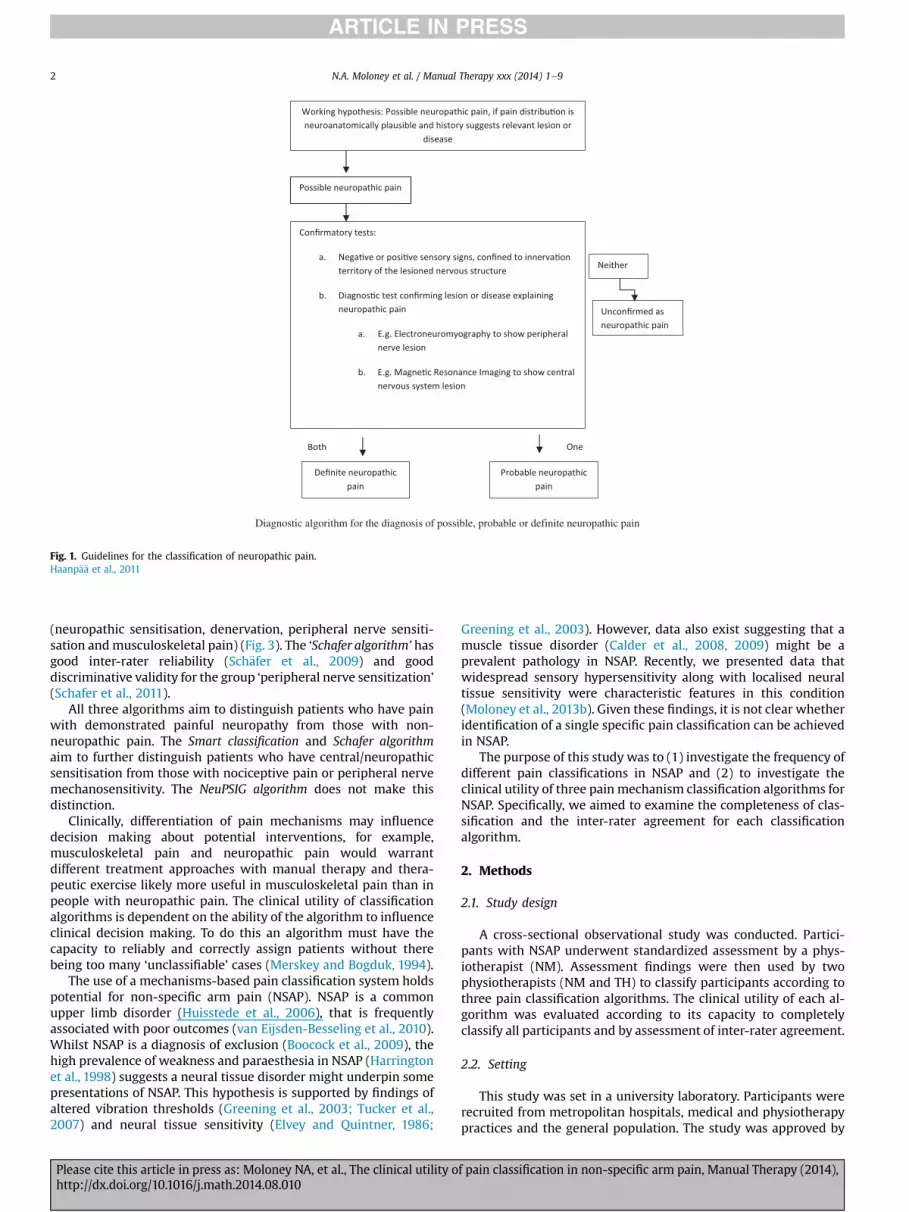
Diagnostic algorithm for the diagnosis of possible, probable or definite neuropathic pain
Fig. 1. Guidelines for the classification of neuropathic pain.Haanp€a€a et al., 2011
N.A. Moloney et al. / Manual Therapy xxx (2014) 1e92
(neuropathic sensitisation, denervation, peripheral nerve sensiti-sation andmusculoskeletal pain) (Fig. 3). The ‘Schafer algorithm’ hasgood inter-rater reliability (Sch€afer et al., 2009) and gooddiscriminative validity for the group ‘peripheral nerve sensitization’(Schafer et al., 2011).
All three algorithms aim to distinguish patients who have painwith demonstrated painful neuropathy from those with non-neuropathic pain. The Smart classification and Schafer algorithmaim to further distinguish patients who have central/neuropathicsensitisation from those with nociceptive pain or peripheral nervemechanosensitivity. The NeuPSIG algorithm does not make thisdistinction.
Clinically, differentiation of pain mechanisms may influencedecision making about potential interventions, for example,musculoskeletal pain and neuropathic pain would warrantdifferent treatment approaches with manual therapy and thera-peutic exercise likely more useful in musculoskeletal pain than inpeople with neuropathic pain. The clinical utility of classificationalgorithms is dependent on the ability of the algorithm to influenceclinical decision making. To do this an algorithm must have thecapacity to reliably and correctly assign patients without therebeing too many ‘unclassifiable’ cases (Merskey and Bogduk, 1994).
The use of a mechanisms-based pain classification system holdspotential for non-specific arm pain (NSAP). NSAP is a commonupper limb disorder (Huisstede et al., 2006), that is frequentlyassociated with poor outcomes (van Eijsden-Besseling et al., 2010).Whilst NSAP is a diagnosis of exclusion (Boocock et al., 2009), thehigh prevalence of weakness and paraesthesia in NSAP (Harringtonet al., 1998) suggests a neural tissue disorder might underpin somepresentations of NSAP. This hypothesis is supported by findings ofaltered vibration thresholds (Greening et al., 2003; Tucker et al.,2007) and neural tissue sensitivity (Elvey and Quintner, 1986;
Please cite this article in press as: Moloney NA, et al., The clinical utility ohttp://dx.doi.org/10.1016/j.math.2014.08.010
Greening et al., 2003). However, data also exist suggesting that amuscle tissue disorder (Calder et al., 2008, 2009) might be aprevalent pathology in NSAP. Recently, we presented data thatwidespread sensory hypersensitivity along with localised neuraltissue sensitivity were characteristic features in this condition(Moloney et al., 2013b). Given these findings, it is not clear whetheridentification of a single specific pain classification can be achievedin NSAP.
The purpose of this study was to (1) investigate the frequency ofdifferent pain classifications in NSAP and (2) to investigate theclinical utility of three pain mechanism classification algorithms forNSAP. Specifically, we aimed to examine the completeness of clas-sification and the inter-rater agreement for each classificationalgorithm.
2. Methods
2.1. Study design
A cross-sectional observational study was conducted. Partici-pants with NSAP underwent standardized assessment by a phys-iotherapist (NM). Assessment findings were then used by twophysiotherapists (NM and TH) to classify participants according tothree pain classification algorithms. The clinical utility of each al-gorithm was evaluated according to its capacity to completelyclassify all participants and by assessment of inter-rater agreement.
2.2. Setting
This study was set in a university laboratory. Participants wererecruited from metropolitan hospitals, medical and physiotherapypractices and the general population. The study was approved by
f pain classification in non-specific arm pain, Manual Therapy (2014),
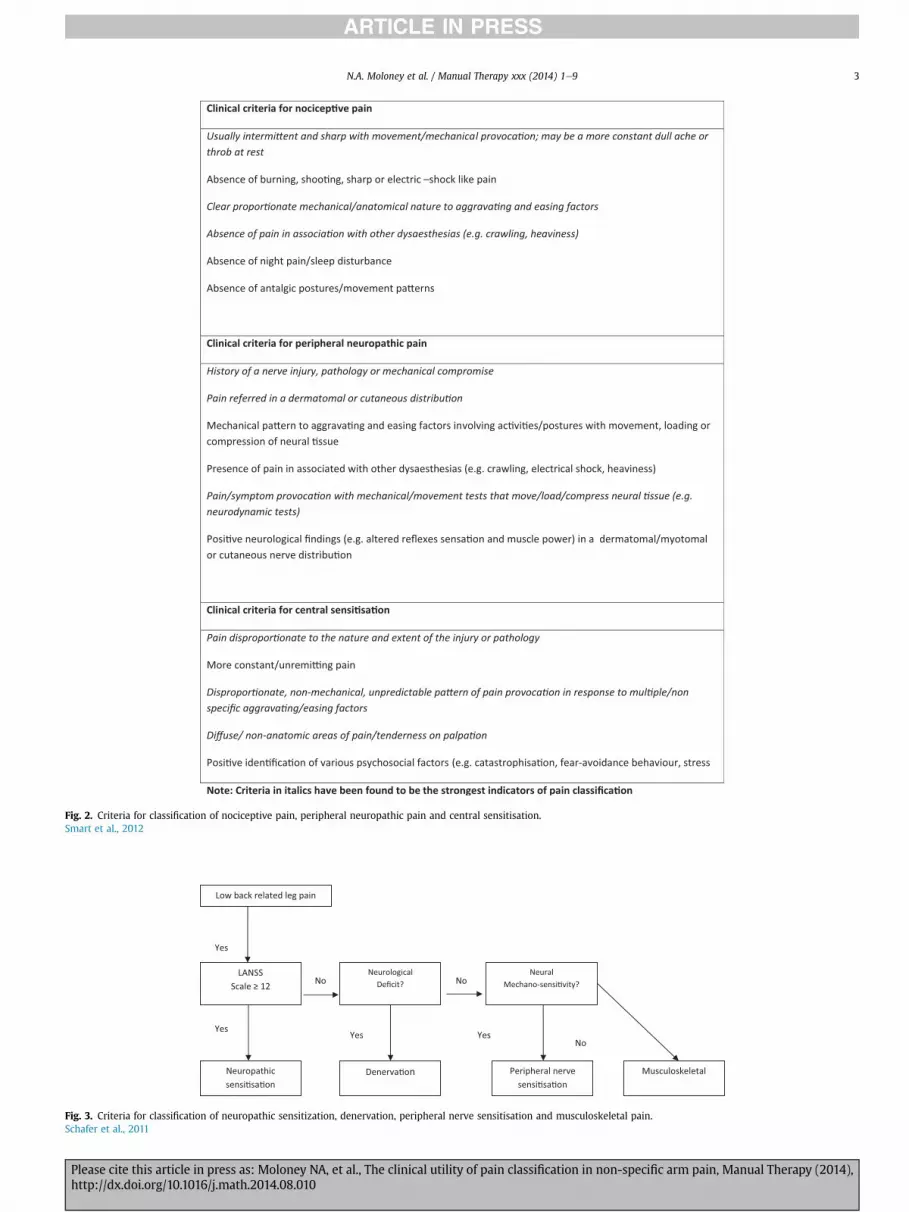
Fig. 2. Criteria for classification of nociceptive pain, peripheral neuropathic pain and central sensitisation.Smart et al., 2012
Fig. 3. Criteria for classification of neuropathic sensitization, denervation, peripheral nerve sensitisation and musculoskeletal pain.Schafer et al., 2011
N.A. Moloney et al. / Manual Therapy xxx (2014) 1e9 3
Please cite this article in press as: Moloney NA, et al., The clinical utility of pain classification in non-specific arm pain, Manual Therapy (2014),http://dx.doi.org/10.1016/j.math.2014.08.010

N.A. Moloney et al. / Manual Therapy xxx (2014) 1e94
the Human Research Ethics Committee for Life Sciences, UniversityCollege Dublin, and participating hospitals. All participants wereunpaid volunteers who provided written informed consent.
2.3. Participants
Forty volunteers with arm pain, aged between 18 and 65 yearswere recruited. Participants were included if they had pain�3/10 of>3 months duration, who used desktop equipment for more than40% of their working week (Greening et al., 2003) and had beenemployed using desk-top equipment for at least two years(Johnston et al., 2008). Participants were excluded if they had adiagnosed specific musculoskeletal condition or any of thefollowing: generalized neurological or musculoskeletal disorders,low back pain or migraine over the previous 6 months, significantupper quadrant trauma, diabetes, endocrine disorders, epilepsy orsignificant mental health disorders.
2.4. Investigators
Clinical assessment of the participants and collection of baselinedata and allocation of participants to pain classification groups wasconducted by the lead author (NM). A second investigator (TH)independently verified assessment findings and independentlyallocated participants to pain classification groups. Data entry andanalysis was conducted by a third investigator (AL). All in-vestigators were physiotherapists with post-graduate qualificationin musculoskeletal physiotherapy, with more than 11 years clinicalexperience and training in quantitative sensory testing (QST).
2.5. Procedure
Participants attended a one-off clinical assessment that includedquantitative sensory testing (Fig. 4). The diagnosis of ‘NSAP’ was
Fig. 4. Study
Please cite this article in press as: Moloney NA, et al., The clinical utility ohttp://dx.doi.org/10.1016/j.math.2014.08.010
confirmed by excluding alternative diagnoses including cervicalreferred pain and upper limb neuropathies (see Appendix 1).Neurological function and nervous system sensitisation (localisedand widespread) was also assessed. Participants completed ques-tionnaires to assess pain and disability. Assessment findings wereevaluated by two independent investigators. Participants wereclassified according to the three algorithms by two independentinvestigators (Figs. 1e3).
2.6. Variables
Variables used to classify participants for each algorithm wereextracted from the patient history, written questionnaires, physicalexamination and QST findings. The interpretation of each variablewithin each classification algorithm is detailed in Table 1.
2.6.1. HistoryVariables extracted from the patient history included the pre-
senting complaint, pain features, pattern of aggravating and easingfactors, and signs and symptoms of nerve injury or compromise.
2.6.2. QuestionnairesParticipants completed the Leeds Assessment for Neuropathic
Symptoms and Signs (LANSS) questionnaire, Tampa Scale forKinesiophobia (TSK) (Kori et al., 1990; Vlaeyen et al., 1995), andShort-Form McGill Pain Questionnaire (SFMPQ) (McGill, 1987). ALANSS of �12 was considered an indicator of possible neuropathicpain (Bennett, 2001). A TSK score of �37 was considered an indi-cator of significant fear avoidance beliefs (Vlaeyen et al., 1995). Inaddition, the disability of arm, shoulder and hand (DASH) ques-tionnaire was administered (Kitis et al., 2009). Pain descriptors inthe MPQ, in addition to descriptors nominated by participants, andresults from these questionnaires were used for completion ofclinical algorithms (Table 1).
design.
f pain classification in non-specific arm pain, Manual Therapy (2014),

Table 1Interpretation of variables within each algorithm.
Variable NeuPSIG algorithm Smart classification Schafer algorithm
1.Symptom frequency and descriptorsof pain quality including those outlinedin the MPQ2.Pattern of aggravating and easingfactors
N/A Used for all 3 pain classifications N/A
3.Symptom distribution Neuroanatomical distribution isan essential criterion for classificationof neuropathic pain
Pain in a dermatomal cutaneous nervedistribution supports the classificationof peripheral neuropathic pain
N/A
4.History of a nerve injury ormechanical compromise of a nerve
History of a nerve injury is anessential criterion for classificationof neuropathic pain
History of a nerve injury or mechanicalcompromise supports the classificationof peripheral neuropathic pain
N/A
5.Questionnairesa. LANSS � 12b. DASH � 50c. TSK � 37
N/A High levels of disability and fearavoidance support the classificationof central sensitisation pain
A LANSS score of �12 is used forthe classification of neuropathicsensitisation
d. Neurological examination The presence of neurological deficitwithin the affected area supports theclassification of neuropathic pain
The presence of neurological deficitwithin the affected area supports theclassification of peripheral neuropathicpain
The presence of 2 or more signsof neurological deficit within theaffected area supports the classificationof denervation
e. Assessment of hyperalgesia and/or allodynia
The presence of hyperalgesia and/orallodynia within the affected areasupports the classification ofneuropathic pain
The presence of widespread hyperalgesiaand/or allodynia (tenderness on palpation)supports the classification of centralsensitisation pain
Hyperalgesia and allodynia areassessed as part of the LANSS andsupport a classification of neuropathicsensitisation if present with a LANSSscore � 12
f. Neural tissue provocation tests N/A The presence of positive neural tissueprovocation tests supports theclassification of peripheral neuropathicpain
The presence of positive neuraltissue provocation tests supportsa classification of peripheral nervesensitisation
g. Quantitative sensory testing The presence of increased pressureor thermal pain sensitivity and/orthermal or vibration hypoaesthesiawithin a relevant neuroanatomicaldistribution supports a classificationof neuropathic pain
The presence of widespread pressure orthermal pain sensitivity supports theclassification of central sensitisation pain
N/A
MPQ: McGill Pain Questionnaire; LANSS: Leeds assessment of neuropathic symptoms and signs; DASH: Disability of the arm, shoulder and hand; TSK: Tampa Scale ofKinesiophobia.
N.A. Moloney et al. / Manual Therapy xxx (2014) 1e9 5
2.6.3. Physical examinationPhysical examination included:
� Neurological examination (reflexes, myotomes, dermatomes)(Malanga, 1997)
� Neural tissue sensitivity tests including the upper limb neuro-dynamic test 1 and palpation of the median, ulnar and radialnerves. The neurodynamic test was considered positive if armsymptoms (at least in part) were reproduced along with positivestructural differentiation tests (Elvey, 1997; Butler, 2000).
� Assessment of pin-prick hyperalgesia and brush-stroke allody-nia over symptomatic and remote asymptomatic regions
� Assessment of general tenderness to light touch.
2.6.4. Quantitative sensory testingA previously published QST protocol (Moloney et al., 2010) was
implemented to test the following: cold, warm and vibrationdetection thresholds; cold, heat and pressure pain thresholds. Allmeasures were recorded bilaterally over three upper limb sites. Thetibialis anterior region was used as a remote reference point forthermal testing and pressure pain thresholds (recorded unilater-ally). QST data were used during analyses for evidence of alteredsensation either locally and/or at remote sites from the pain.
Sensory phenotypes were determined for each participant bygenerating z-score profiles from QST data (Rolke et al., 2006). QSTdata were log transformed before calculation of z-scores. Z-trans-formation for each variable was generated using the formula: Z-score ¼ (X single participant e Mean controls)/SD controls (Rolkeet al., 2006). Z-scores of >2 z-scores from the mean were
Please cite this article in press as: Moloney NA, et al., The clinical utility ohttp://dx.doi.org/10.1016/j.math.2014.08.010
considered indicative of sensory gain to the tested stimuli, while z-scores of <2 from the mean were considered indicative of sensoryloss (Maier et al., 2010). If a sensory abnormality was detected, itwas sub-grouped as (a) localised, (b) localised within a neuroana-tomical distribution or (c) widespread.
2.7. Analyses
Sample size was calculated using a method reported by Sim andWright (2005). We considered that k ¼ 0.40 would be the leastclinically acceptable agreement measurement. Using the null hy-pothesis of k ¼ 0.40 and assuming a 5% level of significance and apower of 0.8, a sample size of 39 was required.
Participant characteristics and classification frequencies wereanalysed using descriptive statistics. Clinical utility of each algo-rithm was assessed according to the completeness of the classifi-cation according to each algorithm i.e. the proportion ofparticipants classified versus unclassified. The Kappa coefficientwas used to assess inter-rater agreement of classification accordingto each algorithm and was interpreted according to publishedguidelines (Landis and Koch, 1977).
3. Results
Participant characteristics are presented in Table 2.
3.1. Frequency of pain classification
The frequency of assignment to each pain group and inter-rateragreement for each algorithm are presented in Tables 3e5. The
f pain classification in non-specific arm pain, Manual Therapy (2014),

Table 3Frequency data for NeuPSIG classifications and inter-rater agreement for NeuPSIGAlgorithm for NSAP (n ¼ 40).
Algorithm 1 (Haanp€a€a et al., 2011) Rater 1 Rater 2 Kappa p-value
Possible neuropathic pain 3 0 Unable to calculateUnlikely neuropathic pain 37 40
Table 5Frequency data for Schafer classifications and inter-rater agreement for SchaferAlgorithm for NSAP (n ¼ 40).
Rater 1 Rater 2 Kappa p-value
Neuropathic sensitisation 3 4 0.783 <0.001Denervation 2 3Peripheral nerve sensitisation 26 22Musculoskeletal 8 11Mixed 1 0
Table 2Participant characteristics.
Non specific arm pain n ¼ 40
Number female 26Mean age (SD) 36.6 (8.0)Age range 26e56Mean (SD) duration of pain, years 4.3 (8.7)Unilateral arm pain 32Bilateral arm pain 8LANSS Mean (SD) 5.5 (4.3)No � 12 4TSK Mean (SD) 33.7 (5.7)No � 37 11
N.A. Moloney et al. / Manual Therapy xxx (2014) 1e96
dominant pain classification was ‘unlikely neuropathic pain’ usingthe NeuPSIG algorithm, ‘peripheral nerve sensitisation’ using theSchafer algorithm, and ‘peripheral neuropathic pain’ using the Smartclassification.
3.2. Clinical utility
For two classification systems (NeuPSIG and Schafer algorithms)all but one participant could be classified by both observers. Usingthe Smart classification, 20% and 45% of participants were deemedto have mixed pain types by rater 1 and 2 respectively.
A statistical coefficient of agreement was unattainable for theNeuPSIG algorithm; however, visual inspection of the data revealedexcellent agreement between the observers (92% agreement). Theinter-rater agreement was moderate at 40% for the Smart classifi-cation, which was set a priori as the minimal clinically-relevantacceptable agreement. Classification using the Schafer algorithmdemonstrated good agreement at 78.3%.
4. Discussion
This study demonstrates that mechanisms-based pain classifi-cation algorithms developed for back pain ± leg pain (Smart et al.,2012), low back related leg pain (Schafer et al., 2009) and neuro-pathic pain (Haanp€a€a et al., 2011) have potential clinical utility inthe assessment of NSAP. Using the NeuPSIG algorithm, the mostfrequently allocated classification was ‘unlikely neuropathic pain’,while using the Smart and Schafer algorithms this was ‘peripheralneuropathic pain’ and ‘peripheral nerve sensitisation’ respectively.Between five and 11 participants were considered to have muscu-loskeletal/nociceptive pain using these latter algorithms, while fewparticipants were deemed to have central or neuropathic sensiti-sation. The best agreement between raters was achieved using theSchafer algorithm.
Table 4Frequency data for Smart classifications and inter-rater agreement for Smart Algo-rithm for NSAP (n ¼ 40).
Rater 1 Rater 2 Kappa p-value
Nociceptive pain 8 5 0.401 <0.001Peripheral neuropathic pain 23 15Central pain 1 2Mixed 8 18
Please cite this article in press as: Moloney NA, et al., The clinical utility ohttp://dx.doi.org/10.1016/j.math.2014.08.010
4.1. Pain classifications in NSAP
The results of this study indicate that NSAP may be considered a‘peripheral neuropathic pain’ condition when using the Smart algo-rithm but was considered ‘unlikely neuropathic pain’ using the Neu-PSIG algorithm (Haanp€a€a et al., 2011). This highlights discord in theclinical criteria used to classify neuropathic pain. The NeuPSIG algo-rithm requires that evidence of a lesion or disease of the nervoussystem is obtained through the history, pain distribution and furthertesting and provides a stepwise approach to the classification ofneuropathic pain, from probable to definite. There are two key dif-ferences to the way we used the criteria outlined by Smart et al.(2012). Firstly, because a hierarchy of the clinical criteria has notbeen indicated, all of the criteria were treated with equal weightwhen classifying patients. Secondly, signs and symptoms of neuraltissuemechanosensitivity, even in the absence of neurological deficit,were assigned to peripheral neuropathic pain. This may explain thediscrepancy between the results of the Smart classification and theNeuPSIG algorithm. Furthermore, the Schafer algorithm allows forseparation of those with neurological deficit and those with neuraltissue mechanosensitivity under the headings ‘denervation’ and‘peripheral nerve sensitisation’; this resulted in 65% of participantsfalling into the latter category. The presence of peripheral nervesensitisation inNSAP is consistentwith our previous report (Moloneyet al., 2013b) and other studies (Elvey andQuintner,1986; Byng,1997;Greening et al., 2003; Jepsen, 2004). Thesefindings hold relevance forclinical decision making, discussed later in this paper.
With respect to other classifications of pain, up to 28% of partic-ipants were classified as having nociceptive/musculoskeletal pain,but few were identified with widespread sensitisation (central orneuropathic sensitisation) (�10%). The infrequent identification ofwidespread sensitisation in NSAP using these algorithms is surpris-ing and contrasts with data from QST in this group that highlightedwidespread sensitisation as a key characteristic (Moloney et al.,2013b). To our knowledge, correlations between the clinicalappraisal of the presence of widespread sensitisation and resultsfrom QST have not been yet been reported; however, quantitativemeasures of pain sensitivity have previously been shown to correlatepoorly with self-reported pain and disability (Hübscher et al., 2013).Hübscher et al. (2013) proposed one reason for this poor correlationmay be the fact that none of the included studies in that reviewspecifically recruited people deemed clinically to present withwidespread sensitisation and as such, correlations between QST andclinical presentation of pain may have been diluted. Interestingly,while widespread hypersensitivity is acknowledged as an importantmechanism underpinning some chronic pain states e.g. whiplashand fibromyalgia (Sterling et al., 2003; Staud et al., 2009; VanOosterwijck et al., 2012), both its status as a distinct pain classifica-tion and criteria for its classification are not yet fully established.
4.2. Appraisal of each algorithm
In consideration of the NeuPSIG algorithm, it is unsurprising thatthe majority of the participants were deemed unlikely to have
f pain classification in non-specific arm pain, Manual Therapy (2014),

N.A. Moloney et al. / Manual Therapy xxx (2014) 1e9 7
neuropathic pain, with only three participants allocated to the‘possible’ category by one observer. No participant was classified asprobable or definite in this group. Our participants were screenedfor the presence of specific diagnoses prior to inclusion in thisstudy, and neurological injury would have meant exclusion. TheNeuPSIG algorithmwas therefore accurate in this respect; however,its use may have been redundant in this group. The purpose of theNeuPSIG algorithm is to provide a framework for classification ofneuropathic pain, which relies on the diagnosis of neuropathy(Haanp€a€a et al., 2011). There has been some debate about thisapproach and a view that neuropathic pain may be a broader entity(Lynch et al., 2011). Nonetheless, the benefit of this algorithm forguiding clinical decision making in primary care lies in its ability toidentify patients who may warrant further investigation or morespecific management for neuropathy (Bono et al., 2011). The limi-tation of this algorithm is that in the absence of neuropathic pain,other guidelines are required for further classification and directionfor management.
The Smart classification resulted in the highest number of par-ticipants classified with mixed pain presentations and the lowestconsistency between raters. This was largely influenced by thenumber of participants classified as mixed by one rater. Improve-ment in inter-rater agreement might be achieved with more spe-cific instruction about interpreting assessment findings in light ofthe classification criteria. Inter-rater agreement in the current studywas considerably lower than previously reported (Smart et al.,2010); however, that study used different methodology. Smartet al. (2010) assessed agreement of a larger suite of clinicalcriteria items that were used in an earlier phase of their study.Further, Smart et al. (2010) tested decisions made immediatelyfollowing patient assessment rather than post-hoc as they were inthis study. The clinical criteria for selection in each categoryincorporate a combination of subjective and objective features, theabsence of a hierarchical model meant that many participants wereclassified as ‘mixed’. Whilst this makes clinical decision makingdifficult, it may reflect the real-life clinical situation, where patientsare likely to present with a mix of pain types and where pain statesare a continuum rather than discrete entities. However, developingthis classification system into a stepwise clinical algorithm mightbe beneficial.
The dominant classification of the Smart classification was pe-ripheral neuropathic pain despite this cohort being screened andcleared of neuropathy. The inclusion of both neurological deficitand signs and symptoms of neural tissue mechanosensitivitywithin the same category in this algorithm diminishes the capacityof this algorithm to guide clinical decision making as it is necessaryto segregate those with neurological deficit from those without forthe purpose of guiding further investigation and possibletreatment.
The Schafer algorithm was considered the most clinically usefulalgorithm for NSAP, both due to the high number of people clas-sified and the good inter-rater agreement. This is likely due to twofactors; firstly the hierarchical nature of the algorithm forces acategory selection that is based on limited but key information.Secondly, the presence of a separate category for neural tissuemechanosensitivity i.e. peripheral nerve sensitisation was useful inNSAP. The identification of peripheral nerve sensitisation as adistinct category may be controversial from a mechanisms-basedpain classification perspective. As is apparent from the Smart clas-sification, it has become common to describe neural tissuemechanosensitivity as a neuropathic pain condition. This descrip-tion reflects the inconsistency across some disciplines in the se-mantic use of the term 'neuropathic'. Whilst neural tissueprovocation tests have demonstrated validity (Selvaratnam et al.,1988; Kleinrensink et al., 2000), whether peripheral nerve
Please cite this article in press as: Moloney NA, et al., The clinical utility ohttp://dx.doi.org/10.1016/j.math.2014.08.010
sensitisation is a discrete neuropathic pain condition is debatable.Certainly, neural tissue sensitisation frequently occurs with painfulneuropathies (Wainner et al., 2003); however, in the absence of adistinct neuropathy, a number of mechanisms to explain sensiti-sation of neural tissue include neuritis (Eliav et al., 2001; Dilleyet al., 2005), sensitisation of nervi nervorum (Quintner and Bove,2001) and minor neuropathy (Greening et al., 2003). Regardlessof the semantic arguments, arm painwith neuropathy and arm painwithout neuropathy but with neural tissue sensitivity usuallyrequire different treatment approaches so distinguishing betweenthese conditions is important.
4.3. Clinical value of pain classification algorithms
It is important to consider how pain classification might influ-ence clinical decision-making. From the algorithms outlined, foursub-groups are evident: (1) Neuropathic pain; (2) Musculoskeletalpain; (3) Widespread sensitisation and (4) Peripheral nerve sensi-tisation (i.e. localised neural tissue mechanosensitivity). Animportant caveat in discussing sub-grouping is whether it results inimproved outcomes. Whilst sub-grouping is attractive for thestratification of healthcare and appears logical, as will be outlined,the impact of sub-grouping on treatment outcomes is, as yet,inconsistent (Hill et al., 2011; Jull et al., 2013; Wand and O'Connell,2008).
4.3.1. Neuropathic painA key task when triaging a patient is the identification of specific
pathologies including neuropathy ± neuropathic pain. Such pa-tients often require specific investigations and sometimes surgicalintervention (Bono et al., 2011). Conservative management in thisgroup including physical therapies (Salt et al., 2011), and anti-convulsant medications (Wiffen et al., 2013) might also beconsidered.
4.3.2. Peripheral nerve sensitisationThe mechanisms underpinning peripheral nerve sensitisation
are still open to debate. Nonetheless, identification of peripheralnerve sensitisation as a distinct entity is potentially beneficial.Emerging data demonstrate positive responses to therapies spe-cifically targeting neural tissue sensitivity i.e. non-provocativeneural mobilisation in those classified with peripheral nervesensitisation (Allison et al., 2002; Hall and Elvey, 2004; Schaferet al., 2011; Nee et al., 2012).
4.3.3. Nociceptive painThe identification of musculoskeletal (nociceptive) pain, in the
absence of neuropathy or central sensitisation, suggests that clini-cians should focus on conservative interventions, such as, educa-tion, simple analgesic/anti-inflammatory medication and physicaltreatments such as exercise andmanual therapy (Green et al., 2003;Brennan et al., 2010; Kay et al., 2012; Pattanittum et al., 2013).
4.3.4. Widespread sensitisationWidespread sensitisation involves peripheral and central ner-
vous system sensitisation which poses a particular challenge inclinical practice. There is growing research evidence that manypeople with chronic musculoskeletal conditions display signs ofwidespread sensitisation (Zusman, 2002; Sterling et al., 2003;Tampin et al., 2012; Van Oosterwijck et al., 2012; Wylde et al.,2012; Moloney et al., 2013a). Evidence based management ap-proaches remain elusive in this group (Sterling et al., 2003; Jullet al., 2013); however, comprehensive, multi-disciplinary ap-proaches incorporating pain science education, are likely war-ranted (Zusman, 2002; Nijs et al., 2011).
f pain classification in non-specific arm pain, Manual Therapy (2014),

N.A. Moloney et al. / Manual Therapy xxx (2014) 1e98
4.4. Study limitations
Further studies on a larger sample size and by researchers whohave not been involved in the development of the classificationsystems are warranted.
5. Conclusion
This study explored the clinical utility for NSAP of three painalgorithms that classify patients according to painmechanisms. Theresults indicate that theNeuPSIG algorithm is effective in identifyingthose with neuropathic pain resulting from an identifiable neuro-logical lesion. The Schafer algorithm was demonstrated to have thebest clinical utility in terms of number of participants classified andinter-rater agreement. Finally the Smart classification resulted in themost participants classified with ‘mixed pain’ in this cohort, whichalso largely accounted for the lower inter-rater rates using thismethod. The results from this study support previous reports ofperipheral nerve sensitisation as a key characteristic of NSAP.
Conflicts of interest
None declared.
Acknowledgements
The authors would like to acknowledge the late Max Zusman forhis contribution to the body of research from which this paper isderived. This research was funded by the Irish Research Council forScience, Engineering and Technology: Embase PhD Scholarship;Chartered Physiotherapists in Musculoskeletal Therapy, Ireland:Research Bursary; Chartered Physiotherapists in OccupationalHealth and Ergonomics, Ireland: Research Bursary.
Appendix A. Supplementary data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.math.2014.08.010.
References
Allison GT, Nagy BM, Hall T. A randomized clinical trial of manual therapy forcervico-brachial pain syndrome e a pilot study. Man Ther 2002;7:95e102.
Beaudet N, Courteau J, Sarret P, Vanasse A. Prevalence of claims-based recurrent lowback pain in a Canadian population: a secondary analysis of an administrativedatabase. BMC Musculoskelet Disord 2013;14.
Bennett M. The LANSS Pain Scale: the Leeds assessment of neuropathic symptomsand signs. Pain 2001;92:147e57.
Bono CM, Ghiselli G, Gilbert TJ, Kreiner DS, Reitman C, Summers JT, et al. Anevidence-based clinical guideline for the diagnosis and treatment of cervicalradiculopathy from degenerative disorders. Spine J 2011;11:64e72.
Boocock MG, Collier JM, McNair PJ, Simmonds M, Larmer PJ, Armstrong B.A framework for the classification and diagnosis of work- related upper ex-tremity conditions: systematic review. Semin Arthritis Rheum 2009;38:296e311.
Brennan GP, Parent EC, Cleland JA. Description of clinical outcomes and post-operative utilization of physical therapy services within 4 categories of shouldersurgery. J Orthop Sports Phys Ther 2010;40:20e9.
Butler DS. The sensitive nervous system. Adelaide: Noigroup Publications; 2000.Byng J. Overuse syndromes of the upper limb and the upper limb tension test: a
comparison between patients, asymptomatic keyboard workers and asymp-tomatic non-keyboard workers. Man Ther 1997;2:157e64.
Calder KM, Gabriel DA, McLean L. Differences in EMG spike shape between in-dividuals with and without non-specific arm pain. J Neurosci Methods2009;178:148e56.
Calder KM, Stashuk DW, McLean L. Motor unit potential morphology differences inindividuals with non-specific arm pain and lateral epicondylitis. J NeuroEngRehabil 2008;5.
Dilley A, Lynn B, Pang SJ. Pressure and stretch mechanosensitivity of peripheralnerve fibres following local inflammation of the nerve trunk. Pain 2005;117:462e72.
Please cite this article in press as: Moloney NA, et al., The clinical utility ohttp://dx.doi.org/10.1016/j.math.2014.08.010
Eliav E, Benoliel R, Tal M. Inflammationwith no axonal damage of the rat saphenousnerve trunk induces ectopic discharge and mechanosensitivity in myelinatedaxons. Neurosci Lett 2001;311:49e52.
Elvey R. Physical evaluation of the peripheral nervous system in disorders of painand dysfunction. J Hand Ther 1997;10:122e9.
Elvey RL, Quintner JL. A clinical study of RSI. Aust Fam Physician 1986;15:1312e4.Freynhagan R, Rolke R, Baron R, Tolle TR, Rutjes A, Schu S, et al. Pseudoradicular and
radicular low- back pain- a disease continuum rather than different entities?Answers from quantitative sensory testing. Pain 2008;135:65e74.
Green S, Buchbinder R, Hetrick S. Physiotherapy interventions for shoulder pain.Cochrane Database Syst Rev 2013 2003;2.
Greening J, Lynn B, Leary R. Sensory and autonomic function in the hands of pa-tients with non-specific arm pain (NSAP) and asymptomatic office workers.Pain 2003;104:275e81.
Haanp€a€a M, Attal N, Backonja M, Baron R, Bennett M, Bouhassira D, et al. NeuPSIGguidelines on neuropathic pain assessment. Pain 2011;152:14e27.
Hall TM, Elvey RL. Management of mechanosensitivity of the nervous system inspinal pain syndromes. In: Boyling JD, Jull GA, editors. Grieve's modern manualtherapy. 3rd ed. Churchill Livinstone; 2004. p. 413e32.
Hansson P. Neuropathic pain: clinical characteristics and diagnostic workup. Eur JPain 2002;6(Suppl. A):47e50.
Harrington J, Carter J, Birrell L, Gromptez D. Surveillance case definitions for workrelated upper limb pain syndromes. Occup Environ Med 1998;55:264e71.
Hill JC, Whitehurst DG, Lewis M, Bryan S, Dunn KM, Foster NE, et al. Comparison ofstratified primary care management for low back pain with current bestpractice (STarT Back): a randomised controlled trial. Lancet 2011;378:1560e71.
Hübscher M, Moloney N, Leaver A, Rebbeck T, McAuley J, Refshauge K. Relationshipbetween quantitative sensory testing and pain or disability in people withspinal pain e a systematic review and meta-analysis. Pain 2013;154:1497e504.
Huisstede BM, Bierma-Zeinstra SM, Koes BW, Verhaar JA. Incidence and prevalenceof upper-extremity musculoskeletal disorders. A systematic appraisal of theliterature. BMC Musculoskelet Disord 2006;7.
Jepsen JR. Upper limb neuropathy in computer operators? A clinical case study of 21patients. BMC Musculoskelet Disord 2004;5.
Johnston V, Jimmieson NL, Jull G, Souvlis T. Quantitative sensory measures distin-guish office workers with varying levels of neck pain and disability. Pain2008;137:257e65.
Jull G, Kenardy J, Hendrikz J, Cohen M, Sterling M. Management of acute whiplash: arandomized controlled trial of multidisciplinary stratified treatments. Pain2013;154:1798e806.
Kanayama M, Togawa D, Takahashi C, Terai T, Hashimoto T. Cross-sectional magneticresonance imaging study of lumbar disc degeneration in 200 healthy in-dividuals. J Neurosurg Spine 2009;11:501e7.
Kay TM, Gross A, Goldsmith CH, Rutherford S, Voth S, Hoving JL, et al. Exercises formechanical neck disorders. Cochrane Database Syst Rev 2012;15.
Kindler LL, Bennett RM, Jones KD. Central sensitivity syndromes: mounting path-ophysiologic evidence to link fibromyalgia with other common chronic paindisorders. Pain Manag Nurs 2011;12:15e24.
Kitis A, Celik E, Aslan UB, Zencir M. DASH questionnaire for the analysis of musu-closkeletal symptoms in industrial workers: a validity and reliability study. ApplErgon 2009;40:251e5.
Kleinrensink GJ, Stoeckart R, Mulder PGH, Hoek Gvd, Broek T, Vleeming A, et al.Upper limb tension tests as tools in the diagnosis of nerve and plexus lesions.Anatomical and biomechanical aspects. Clin Biomech 2000;15:9e14.
Kori S, Miller R, Todd D. Kinesphobia: a new view of chronic pain behaviour. PainManag 1990;3.
Landis J, Koch G. The measurement of observer agreement for categorical data.Biometrics 1977;33:159e74.
Lynch ME, Clark AT, Moulin DE, WAtson CPN. Letter to the Editor: modifications aresuggested for the Special Interest Group (SIG) on Neuropathic Pain proposeddefinition and guidelines for neuropathic pain. Pain 2011;152:1682.
Maier C, Baron R, T€olle TR, Binder A, Birbaumer N, Birklein F, et al. Quantitativesensory testing in the German Research Network on Neuropthaic Pain (DFNS):somatosensory abnormalities in 1236 patients with difference neuropathic painsyndromes. Pain 2010;150:439e50.
Malanga GA. The diagnosis and treatment of cervical radiculopathy. Med Sci SportsExerc 1997;29:236e45.
McGill R. The short-form McGill pain questionnaire. Pain 1987;30:191e7.Merskey H, Bogduk N. Classification of chronic pain. 2nd ed. Seattle: IASP Press;
1994.Moloney N, Hall T, Doody C. An investigation of somatosensory profiles in work
related upper limb disorders: a case control observational study protocol. BMCMusculoskelet Disord 2010;11.
Moloney N, Hall T, Doody C. Sensory hyperalgesia is characteristic of nonspecificarm pain: a comparison with cervical radiculopathy and pain-free controls. ClinJ Pain 2013a;29:948e56.
Moloney NA, Hall TM, Doody CM. Sensory hyperalgesia is characteristic of non-specific arm pain. Clin J Pain 2013b;29:948e56.
Nee R, Vicenzino B, Jull G, Cleland J, Coppieters MW. Neural tissue managementprovides immediate clinically relevant benefits without harmful effects forpatients with nerve-related neck and arm pain: a randomized controlled trial.J Physiother 2012;58:23e31.
Nijs J, Meeus M, Van Oosterwijck J, Roussel N, De Kooning M, Ickmans K, et al.Treatment of central sensitization in patients with ‘unexplained’ chronic pain:what options do we have? Expert Opin Pharmacother 2011;12:1087e98.
f pain classification in non-specific arm pain, Manual Therapy (2014),
N.A. Moloney et al. / Manual Therapy xxx (2014) 1e9 9
Nijs J, Van Houdenhove B, Oostendorp RAB. Recognition of central sensitization inpatients with musculoskeletal pain: application of pain neurophysiology inmanual therapy practice. Man Ther 2010;15:135e41.
Pattanittum P, Turner T, Green S, Buchbinder R. Non-steroidal anti-inflammatorydrugs (NSAIDs) for treating lateral elbow pain in adults. Cochrane DatabaseSyst Rev 2013;5.
Quintner JL, Bove GM. From neuralgia to peripheral neuropathic pain: evolution of aconcept. Reg Anesth Pain Med 2001;26:368e72.
Rolke R, Magel W, Campbell, Andrews K, et al. Quantitative sensory testing: acomprehensive protocol for clinical trials. Eur J Pain 2006;10:77e88.
Salt E, Wright C, Kelly S, Dean A. A systematic review on the effectiveness of non-invasive therapy for cervicobrachial pain. Man Ther 2011;16:53e65.
Schafer A, Hall T, Briffa K. Classification of low back-related leg pain e a proposedpatho-mechanism based approach. Man Ther 2009;14:222e30.
Schafer A, Hall T, Muller G, Briffa K. Outcomes differ between subgroups of patientswith low back and leg pain following neural manual therapy: a prospectivecohort study. Eur Spine J 2011;20:482e90.
Sch€afer A, Hall TM, Lüdtke K, Mallwitz JKBN. Interrater reliability of a new classi-fication system for patients with neural low back-related leg pain. J Man ManipTher 2009;17:109e17.
Scholz J, Mannion RJ, Hord DE, Griffin RS, Rawal B, Zheng H, et al. A Novel Tool forthe assessment of pain: validation in low back pain. PLoS Med 2009;6.
Selvaratnam P, Glasgow E, Matyas T. Strain effects in the nerve roots of the brachialplexus. J Anat 1988;161:260e4.
Sim J, Wright CC. The kappa statistics in reliability studies: use, interpretation, andsample size requirements. Physical Therapy 2005;85:257e68.
Smart KM, Blake C, Staines A, Doody CM. The discriminative validity of “nocicep-tive”, “peripheral neuropathic” and “central sensitisation” as mechanisms-based classifications of musculoskeletal pain. Clin J Pain 2012;28:655e63.
Smart KM, Curley A, Blake C, Staines A, Doody C. The reliability of clinical judgmentsand criteria associated with mechanisms-based classifications of pain in pa-tients with low back pain disorders: a preliminary reliability study. J ManManip Ther 2010;18:102e9.
Staud R, Nagel S, Robinson ME, Price DD. Enhanced central pain processing of fi-bromyalgia patients is maintained by muscle afferent input: a randomized,double-blind, placebo-controlled study. Pain 2009;145:96e104.
Sterling M, Jull G, Vicenzino B, Kenardy J. Sensory hypersensitivity occurs soon afterwhiplash injury and is associated with poor recovery. Pain 2003;104:509e17.
Please cite this article in press as: Moloney NA, et al., The clinical utility ohttp://dx.doi.org/10.1016/j.math.2014.08.010
Tampin B, Slater H, Hall T, Lee G, Briffa NK. Quantitative sensory testing somato-sensory profiles in patients with cervical radiculopathy are distinct from thosein patients with nonspecific neck-arm pain. Pain 2012;153:2403e14.
Treede R-D, Jensen TS, Campbell JN, Cruccu G, Dostrovsky JO, Griffin JW, et al.Neuropathic pain: redefinition and a grading system for clinical and researchpurposes. Neurology 2008;70:1630e5.
Tucker AT, White PD, Kosek E, Pearson RM, Henderson M, Coldrick AR, et al.Comparison of vibration perception thresholds in individuals with diffuse up-per limb pain and carpal tunnel syndrome. Pain 2007;127:263e9.
van Eijsden-Besseling MDF, van der Bergh KA, Staal JB, De Bie RA, van derHeuvel WJ. The course of non-specific work-related upper limb disorders andthe influence of demographic factors, psychologic factors and physical fitnesson clinical status and disability. Arch Phys Med Rehabil 2010;91:862e7.
Van Oosterwijck J, Nijs J, Meeus M, Van Loo M, Paul L. Lack of endogenous paininhibition during exercise in people with chronic whiplash associated disor-ders: an experimental study. J Pain 2012;13:242e54.
Vlaeyen JWS, Kole-Snijders AMJ, Boeren RGB, van Eek H. Fear of movement/(re)injury in chronic low back pain and its relation to behavioral performance. Pain1995;62:363e72.
Wainner LR, Fritz JM, Irrgang JJ, Boninger ML, Delitto A, Allison CS. Reliability anddiagnostic accuracy of the clinical examination and patient self-report mea-sures for cervical radiculopathy. Spine 2003;28:52e62.
Walker-Bone K, Palmer KT, Reading I, Coggon D, Cooper C. Prevalence and impact ofmusculoskeletal disorders or the upper limb in the general population. ArthritisRheum 2004;51:642e51.
Wand BM, O'Connell NE. Chronic non-specific low back pain e sub-groups or asingle mechanism? BMC Musculoskelet Disord 2008;9:1471e2474.
Wiffen P, Derry S, Moore R, Aldington D, Cole P, Rice AC, et al. Antiepileptic drugs forneuropathic pain and fibromyalgia - an overview of Cochrane reviews.Cochrane Database Syst Rev 2013;12.
Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain.Pain 2011;15:S2e15.
Woolf CJ, Bennett GJ, Doherty M, Dubner R, Kidd BL, Koltzenberg M, et al. Towards amechanism-based-classification of pain? Pain 1998;77:227e9.
Wylde V, Palmer ST, Learmonth ID, Dieppe P. Somatosensory abnormalities in kneeOA. Rheumatology 2012;51:535e43.
Zusman M. Forebrain-mediated sensitization of central pain pathways: ‘non-spe-cific’ pain and a new image for MT. Man Ther 2002;7:80e8.
f pain classification in non-specific arm pain, Manual Therapy (2014),
Copyright © 2022 FDOKUMEN




















