On the origin of asymmetries in bilateral supernova remnants

Journal of Cranio-Maxillofacial Surgery (i996) 24, 96-I03 © 1996 European Association for Cranio-Maxillofacial Surgery
Bird face deformity secondary to bilateral temporomandibular joint ankylosis
M. M. El-Sheikh, A. M. Medra, M. H. Warda
Cranio-Maxillo-Facial and Plastic Surgery Department, Faculty of Dentistry, Alexandria University, Egypt
SUMMARY. This paper describes our experience in the treatment of 10 patients with bilateral longstanding temporomandibular joint ankylosis occurring during the active growth period and causing severe bird face deformity. The clinical manifestations were: (1) upper airway obstruction in the form of either severe night snoring or obstructive sleep apnoea; (2) inability to open the mouth and (3) severely convex facial profile. Surgery consists of simultaneous release of the ankylosed joints, advancement of the mandible and insertion of posterior mandibular costochondral graft struts. A Le Fort I osteotomy was performed concomitantly in marked deformities to help in the restoration of the posterior facial height. Dramatic improvement in the airway, facial profile and jaw function were obtained by this programme.
INTRODUCTION
Patients with longstanding bilateral temporomandib- ular joint (TMJ) ankylosis caused by joint trauma during the active growth period in early childhood present mainly with: (a) severe bird face deformity, (b) inability to open the mouth and (c) manifestations of upper airway obstruction in the form of either snoring during sleep or obstructive sleep apnoea.
The term bird face deformity was coined by Obwegser and Hadjianghelou (1987, 1988) to describe a clinical state of micrognathic mandible with receding chin and steep occlusal plane. The maxilla is usually secondarily affected, with shortening of the posterior facial height. Also, secondary effects on the soft tissues enveloping the mandible occur in the form of shorten- ing of the pterygo-masseteric muscle sling and other ligaments attaching the mandible to the skull base (sphenomandibular and stylomandibular ligaments). The temporalis muscle and coronoid process become more strong and hypertrophied. The suprahyoid muscle group is also short and hypertrophied.
The oropharyngeal airway is narrowed in the cephalo-caudal, transverse, as well as in the postero- anterior directions, secondary to shortening of the mandibular rami and narrowing of the space between the mandibular angles.
In planning the surgical treatment of patients with long standing bilateral TMJ ankylosis with bird face deformity, the above mentioned secondary effects must be born in mind and corrected at the same time when operating on the TMJs to release their ankyloses.
MATERIALS AND METHODS
The material of this work comprises 10 patients who presented to the Cranio-Maxillofacial department of
the Alexandria University Hospital during the period January 1990-March 1994 with bird face deformity secondary to longstanding bilateral TMJ ankylosis. Six patients were female and four male, the youngest was 8 and the oldest 37 years of age with a mean of 25 years. All patients gave histories of trauma as a cause of their ankylosed joints. The trauma was inflicted on all patients during the first decade except patients number 8 and 9 where trauma occurred at the ages of 11 and 13 years respectively (Table 1), i.e. during the period of active growth of the facial skeleton. The duration of symptoms varied between 6 and 25 years with an average of 17 years. The younger the patient at the time of trauma and the longer the period of suffering, the more severe was the deformity.
Six patients had had previous operations. One had had silastic implants inserted to replace the resected ccondyles and five were treated by the so called 'gap arthroplasty' with or without the insertion of a tem- poralis muscle flap. The coronoid process was found to be unresected in almost all patients.
Four patients had been previously operated on in the same department, at variable periods ranging between 6 and 10 years before the study period. Two were operated on elsewhere and two patients pre- sented for the first time and had had no previous surgical intervention.
In seven patients, mandibular surgery alone was performed while in the remaining three patients bimaxillary surgery was done in one session.
96
Clinical features
All patients presented with features of the classic bird face syndrome in the form of: (1) limited or absent mouth opening, (2) convex facial profile, (3) respir- atory insufficiency with either severe night snoring
Bird face deformity secondary to bilateral TMJ ankylosis 97
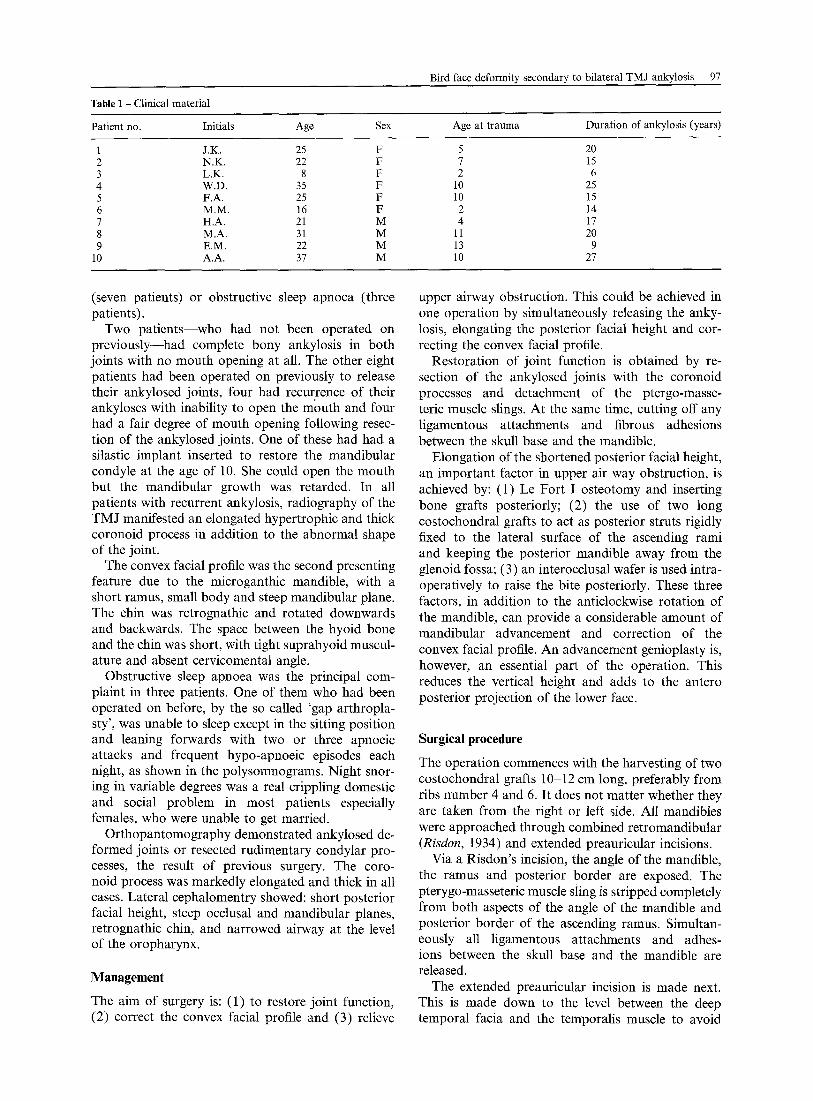
Table 1 - Clinical material
Patient no. Initials Age Sex Age at t rauma Durat ion of ankylosis (years)
1 J.K. 25 F 5 20 2 N.K. 22 F 7 15 3 L.K. 8 F 2 6 4 W.D. 35 F 10 25 5 F.A. 25 F 10 15 6 M.M. 16 F 2 14 7 H.A. 21 M 4 17 8 M.A. 31 M 11 20 9 E.M. 22 M 13 9
10 A.A. 37 M 10 27
(seven patients) or obstructive sleep apnoea (three patients).
Two patients--who had not been operated on previously--had complete bony ankylosis in both joints with no mouth opening at all. The other eight patients had been operated on previously to release their ankylosed joints, four had recurrence of their ankyloses with inability to open the mouth and four had a fair degree of mouth opening following resec- tion of the ankylosed joints. One of these had had a silastic implant inserted to restore the mandibular condyle at the age of 10. She could open the mouth but the mandibular growth was retarded. In all patients with recurrent ankylosis, radiography of the TMJ manifested an elongated hypertrophic and thick coronoid process in addition to the abnormal shape of the joint.
The convex facial profile was the second presenting feature due to the microganthic mandible, with a short ramus, small body and steep mandibular plane. The chin was retrognathic and rotated downwards and backwards. The space between the hyoid bone and the chin was short, with tight suprahyoid muscul- ature and absent cervicomental angle.
Obstructive sleep apnoea was the principal com- plaint in three patients. One of them who had been operated on before, by the so called 'gap arthropla- sty', was unable to sleep except in the sitting position and leaning forwards with two or three apnoeic attacks and frequent hypo-apnoeic episodes each night, as shown in the polysomnograms. Night snor- ing in variable degrees was a real crippling domestic and social problem in most patients especially females, who were unable to get married.
Orthopantomography demonstrated ankylosed de- formed joints or resected rudimentary condylar pro- cesses, the result of previous surgery. The coro- noid process was markedly elongated and thick in all cases. Lateral cephalomentry showed: short posterior facial height, steep occlusal and mandibular planes, retrognathic chin, and narrowed airway at the level of the oropharynx.
Management
The aim of surgery is: (1) to restore joint function, (2) correct the convex facial profile and (3) relieve
upper airway obstruction. This could be achieved in one operation by simultaneously releasing the anky- losis, elongating the posterior facial height and cor- recting the convex facial profile.
Restoration of joint function is obtained by re- section of the ankylosed joints with the coronoid processes and detachment of the ptergo-masse- teric muscle slings. At the same time, cutting off any ligamentous attachments and fibrous adhesions between the skull base and the mandible.
Elongation of the shortened posterior facial height, an important factor in upper air way obstruction, is achieved by: (1) Le Fort I osteotomy and inserting bone grafts posteriorly; (2) the use of two long costochondral grafts to act as posterior struts rigidly fixed to the lateral surface of the ascending rami and keeping the posterior mandible away from the glenoid fossa; (3) an interocclusal wafer is used intra- operatively to raise the bite posteriorly. These three factors, in addition to the anticlockwise rotation of the mandible, can provide a considerable amount of mandibular advancement and correction of the convex facial profile. An advancement genioplasty is, however, an essential part of the operation. This reduces the vertical height and adds to the antero posterior projection of the lower face.
Surgical procedure
The operation commences with the harvesting of two costochondral grafts 10-12 cm long, preferably from ribs number 4 and 6. It does not matter whether they are taken from the right or left side. All mandibles were approached through combined retromandibular (Risdon, 1934) and extended preauricular incisions.
Via a Risdon's incision, the angle of the mandible, the ramus and posterior border are exposed. The pterygo-masseteric muscle sling is stripped completely from both aspects of the angle of the mandible and posterior border of the ascending ramus. Simultan- eously all ligamentous attachments and adhes- ions between the skull base and the mandible are released.
The extended preauricular incision is made next. This is made down to the level between the deep temporal facia and the temporalis muscle to avoid

98 Journal of Cranio-Maxillofacial Surgery
dissection near the frontal branch of the facial nerve, Norman and Bramley (1990). The dissection is carried downwards to the level of the zygomatic arch and anteriorly to the zygomatic bone, cutting through the deep layer of the temporal facia which is attached to the deep aspect of the zygomatic arch and bone. The posterior fibres of the masseter muscle are cut with a diathermy knife. By connecting this wound to that previously made through the Risdon's incision, the ankylosed joint and the coronoid process can be easily exposed. The ankylosed mandibular condyle with the surrounding callus tissue, together with the coronoid process, are now resected and removed using different sizes of rosehead tungsten carbide burs, taking absolute care not to injure the internal maxillary artery or any of its branches behind and deep to the callus mass. Any residual bone left deep in this surgical field may hinder free mandibular movements and might contribute to recurrence of the process of ankylosis. The site of the glenoid fossa must be trimmed from any remnants of callus tissue using a suitable rosehead bur until a reasonably formed new glenoid cavity is created. A temporalis muscle flap is hinged down to fill the resulting cavity. The same procedure is repeated on the opposite side. The mandible should now be freely mobile with full and easy mouth opening. The retromolar region is inspected intraorally for any mucosal tears and these must be tightly sutured to prevent contamination of the operation site by any contents of the oral cavity.
Le Fort I osteotomy is performed next and the maxilla is set down posteriorly according to the prediction tracing and the gap is filled with a bone graft and fixed with miniplates and screws.
The mandible is advanced and rotated in an anti- clockwise manner and fixed to the maxilla using an occlusal wafer, which is fashioned so that the bite is raised posteriorly by few millimetres.
Two posterior struts of costo-chondral grafts are then applied and fixed to the mandibular rami. The chondral part of the graft (3-5 mm long) must lie in the newly fashioned glenoid fossa. The grafts are lightly decorticated to promote revascularization and fixed to the lateral surface of the mandible by two bicortical 2.7 mm screws 12-16 mm long. The man- dibular surfaces are lightly decorticated too before applying the grafts. Good contact between the graft and the mandible is necessary.
Before closing the wounds, the pterygo-masseteric muscle slings are draped over the mandibular rami and no attempt is made to suture these muscles back in place. Drains are then inserted; two on each side, to drain the upper and lower wounds through separ- ate stab incisions. An advancement genioplasty is now performed to complete the operation and it is fixed either by wires or preferably by two plates on either side. Intraoperatively the patient is given 1 g of Claforan 2-hourly; this is continued 8-hourly in
the postoperative period for 5 days. Intermaxillary fixation is kept for 6-8 weeks, after which the patient is kept under a strict active training program to open and close the mouth, for at least 1 year.
The steps of the surgical procedure can be summar- ized as follows:
1. Release of the ankylosed joints bilaterally: (i) stripping of pterygo-masseteric slings (ii) resection of the ankylosed mass (iii) resection of the enlarged coronoid processes.
2. Le Fort 1 osteotomy, lowering of the maxilla posteriorly, insertion of bone grafts and rigid internal fixation
3. mandibular advancement with rotation in an anti- clockwise manner and intermaxillary fixation using an occlusal wafer
4. insertion of bilateral costochondral grafts 5. advancement genioplasty.
Postoperative treatment
Soon after release of maxillo-mandibular fixation, active mouth opening exercises using a gradually increasing number of wooden tongue spatulae accord- ing to the patient's tolerance, avoiding any force until full mouth opening is achieved. The patient has to do these exercises for 15 min, six times a day. Regular follow-up visits are arranged; once per week for a month, biweekly for 3 months and then monthly for 1 year (Bradley, 1985).
RESULTS
Dramatic and immediate improvements in airway function was noted in the immediate postoperative period with disappearance of all hypopnoeic and apnoeic attacks, i.e. obstructive sleep apnoea and the noisy night snoring. However, two of those patients for whom monomaxillary surgery was done still had slight night snoring after 1 year, otherwise all patients had comfortable sleep for up to 3 years.
The facial profile was satisfactory in almost all patients, both in early as well as in late follow up periods.
A certain degree of relapse in the airway space was noted in the lateral cephalogram in two of those patients in whom mon0maxillary surgery was done, this was probably the cause of the return of mild snoring in the late follow-up period.
Infection was negligible. Two of our patients are shown in Figures 1 and 2,
and the overall results are shown in Table 2.
DISCUSSION
Trauma to the TMJ occurring in early childhood, if left untreated, will lead to TMJ ankylosis. This hin-

Bird face deformity secondary to bilateral TMJ ankylosis 99
Fig. 1 - Female, 24 years of age who had bilateral recurrent TMJ ankylosis treated in early childhood by resection of the ankylosed joint and insertion of silastic prostheses, she presented with a bird face appearance and night snoring. (A) Preoperative frontal view. (B) Preoperative profile. (C) Preoperative occlusal view. (D) Postoperative frontal view. (E) Postoperative profile. (F) Postoperative occlusion and mouth opening. (G) Preoperative orthopantomogram tracing. Right side: residual callus, elongated coronoid process. Left side: silastic implant fixed by wire and elongated coronoid process. (H) Preoperative lateral cephalogram. Micrognathic mandible, elongated receding chin, steep occlusal and mandibular planes and narrow airway. (I) Preoperative lateral cephalogram tracing. (J) Postoperative lateral cephalogram of the same patient, note the increase in the width of airway space.
100 Journal of Cranio-Maxillofacial Surgery
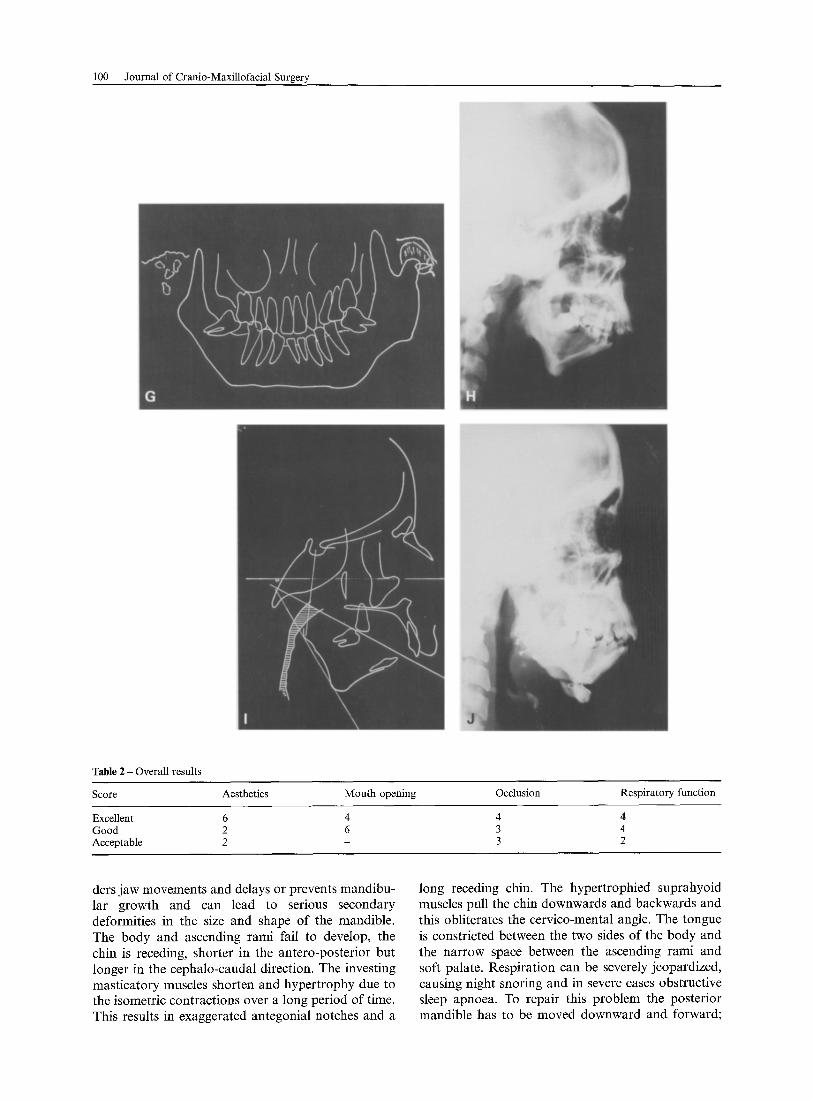
Table 2 - Overall results
Score Aesthetics Mouth opening Occlusion Respiratory function
Excellent 6 4 4 4 Good 2 6 3 4 Acceptable 2 - 3 2
ders jaw movements and delays or prevents mandibu- lar growth and can lead to serious secondary deformities in the size and shape of the mandible. The body and ascending rami fail to develop, the chin is receding, shorter in the antero-posterior but longer in the cephalo-caudal direction. The investing masticatory muscles shorten and hypertrophy due to the isometric contractions over a long period of time. This results in exaggerated antegonial notches and a
long receding chin. The hypertrophied suprahyoid muscles pull the chin downwards and backwards and this obliterates the cervico-mental angle. The tongue is constricted between the two sides of the body and the narrow space between the ascending rami and soft palate. Respiration can be severely jeopardized, causing night snoring and in severe cases obstructive sleep apnoea. To repair this problem the posterior mandible has to be moved downward and forward;
Bird face deformity secondary to bilateral TMJ ankylosis 101
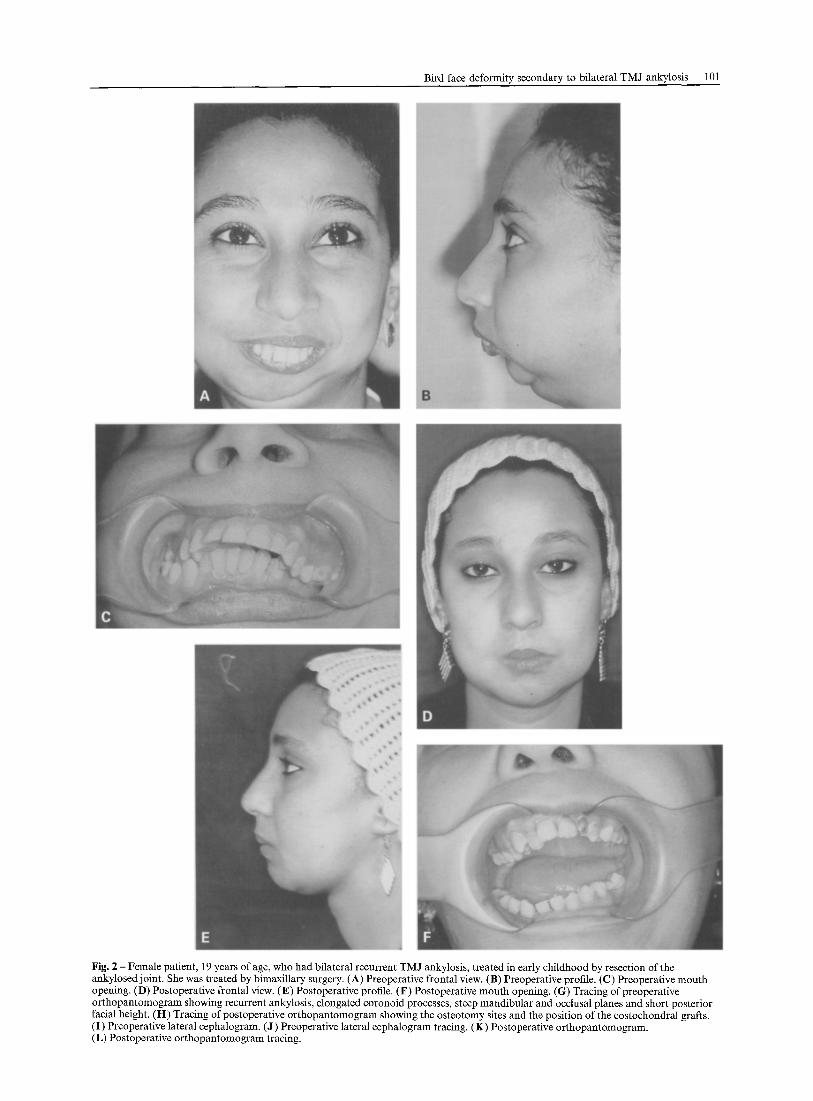
Fig. 2 - Female patient, 19 years of age, who had bilateral recurrent TMJ ankylosis, treated in early childhood by resection of the ankylosed joint. She was treated by bimaxillary surgery. (A) Preoperative frontal view. (B) Preoperative profile. (C) Preoperative mouth opening. (D) Postoperative frontal view. (E) Postoperative profile. (F) Postoperative mouth opening. (G) Tracing of preoperative orthopantomogram showing recurrent ankylosis, elongated coronoid processes, steep mandibular and occlusal planes and short posterior facial height. (H) Tracing of postoperative orthopantomogram showing the osteotomy sites and the position of the eostochondral grafts. (I) Preoperative lateral eephalogram. (J) Preoperative lateral cephalogram tracing. (K) Postoperative orthopantomogram. (L) Postoperative orthopantomogram tracing.

102 Journal of Cranio-Maxillofacial Surgery
G

Bird face deformity secondary to bilateral TMJ ankylosis 103
this can be achieved by releasing the ankylosis, man- dibular advancement and insertion of two costochon- dral grafts to restore the posterior facial height.
The maxillary size, shape and position are altered too. In unilateral cases there is canting of the occlusal plane. In bilateral cases, the posterior maxillary height gets shorter, and together with the short mandibular rami, contributes to the shortened posterior facial height, hence the bird face deformity.
The sagittal splitting of the ramus as described by Obwegeser and Hadjianghelou (1987) for correction of bird face deformity is applicable in cases of minimal ramus shortening. Up to 10 mm of posterior ramus height can be obtained by the sagittal splitting tech- nique. The ramus must be sufficiently broad, thick and well developed even though it is short. The abnormally short ramus is rendered shorter after resection of the ankylosed joint with the coronoid process, these two factors will leave a residual ramus unfit for sagittal splitting (Carlotti and Schendel, 1992). The pterygo-masseteric sling, which is hyper- trophic and short, must be stripped completely from the mandible and not re-attached during wound closure, this cannot be done via an intraoral approach.
The spheno- and stylo-mandibular ligaments, together with fibrosis deep to the mandible which is the result of old trauma or previous surgery on the condyle, must be released and detached from the mandible. This also must be done via an extraoral approach. In advanced cases the coronoid process must be resected, to destroy the function of the temporalis muscle; an important factor contributing to recurrence of the ankylosing process.
The costochondral graft is our preferred autograft for reconstructing the posterior mandible, for the following reasons: (a) it acts as a posterior strut of the jaw against the skull base; this opens up the obstructed airway; (b) it can restore any amount of shortening in the posterior facial height; (c) it pro- vides a potential source of growth in young children; (d) it is an autogenous material compatible with the local tissue, less liable to infection and does not need to be removed.
Fixation of the costochondral graft to the posterior border of the mandible gives it an oblique and forward direction and can bring the cartilage part forward in front of the glenoid eminence. This will not correct the posterior facial height. Therefore, this graft should be applied to the lateral surface of the residual ramus, and fixed rigidly by screws, the carti- lage part must lie in the glenoid fossa.
Release of the ankylosis and restoration of the mandibular ramus and joint by costochondral grafts give satisfactory results in moderate cases. Ortho- dontic treatment is mandatory in the postoperative period to maintain an acceptable occlusion. How- ever, in severe degrees of bird face deformity with marked shortening of the posterior facial height and steep mandibular and occlusal planes, bimaxillary surgery gives better results (Rosen, 1994). Genioplasty markedly improves the convex profile. It can be done primarily during this surgical procedure, or 6 months later according to the case; i.e. if the chief complaint is aesthetics, genioplasty must be an integral part of the operation. However, if the problem is mainly that of respiratory insufficiency, genioplasty can be deferred according to the patient's need.
Simultaneous correction of ankylosis and facial deformity has several beneficial effects. In one oper- ation, the patient gains both the immediate psycho- logical benefit of having a nearly normal appearance and ultimate mouth opening. It is not possible to maintain the corrected position of the jaws unless there is a mechanically stable ascending ramus and a pseudocondyle that cannot slide backwards (Munro et al., 1966).
References
Bradley, P. F.: Injuries of the condylar and coronoid processes. In: Rowe, William, eds. Maxillo-facial injuries, vol. 1. Churchill Livingstone 1985, 337
Carlotti, A. E., S. A. Schendek Mandibular ramus deformities. In: Bell, W. H., ed. Modern practice in orthognathic and reconstructive surgery, vol. 3. W.B. Saunders, Philadelphia 1992, 1996-2019
Munro, L R., Y. R. Chen, B. Y. Park. Simultaneous total correction of temporo-mandibular ankylosis and facial asymmetry. Plast. Reconst. Surg. 77 (1986) 715
Norman, J. E., P. Bramley: A text book and colour atlas of the temporomandibular joint. Wolfe Medical publications Ltd 1990, 26
Obwegeser, H. L., O. Hadjianghelou: Two ways to correct bird face deformity. Oral Surg. 64 1987 507
Obwegeser, H. L., O. Hadjianghelou: Variations of a standard approach for correction of the bird face deformity. J. Cranio- Max. Fac. Surg. 16 1988 265
Risdon, F: Ankylosis of the temporomandibular joint. J. Am. Dent. Assoc. 21 1934 1933-1937
Rosen, M. H.: Bimaxillary surgery. In: Advances in plastic and reconstructive surgery. M. Mosby 1994, 93
Prof. M. M. El-Sheikh FRCS Cranio-Maxillo-Facial and Plastic Surgery Department Faculty of Dentistry Alexandria University Shamplion Street A1-Azarita Egypt
Paper received 16 November 1995 Accepted 5 February 1996
Copyright © 2022 FDOKUMEN