Lyme disease surveillance in Maryland, 1992
6
ELSEVIER Lyme Disease Surveillance in Maryland, 1992 SUZANNE H. STEINBERG, MD, MS, G. THOMAS STRICKLAND, MD, PHD, DCMT, CESAR PENA, DVM, MS, AND EBENEZER ISRAEL, MD, MPH 7’he incidence of Lyme disease (LO) reported to the Maryland Department of Health and Mental Hygiene during 1992 was 6.5/l 00,000 population, ranging from 29.3 cases/lOO,OOO on the Eastern Shore (74.4% of all cases)to no cases in the mountains of western Maryland. Among the 317 reported patients, 44.4% gave a history of tick exposure and 78.9% had positive serologic test results. For the 187 (59.0%) patients meeting the Centers for Disease Control and Prevention (CDC) surveillance casedefinition, erythemamigrans (EM) occurred in69.5%, witharthritic (26.7%), neurologic (13.4%), and cardiac (2.1%) manifestations being less frequent. Patients not meeting the surveillance case definition were significantly more likely to have influenza-like symptoms, a smaller rash, and arthralgia. Patients meeting the CDC criteria were more likely to have an onset during the major transmission season in the summer (odds ratio (OR): 2.1; confidence interval (CI): 1.2 to 3.6) since this was the time when most (115/130) patients with EM were detected. Positive serologic results were more likely (OR: 2.2; Cl: 1.2 to 4.2) in those not meeting the case definition. ‘The treatment given to patients thought to have LD was almost always that recommended in the literature and there was no difference between treatment prescribed for patients meeting and those not meeting the case definition. These data show that physicians in Maryland are treating many patients for LD who are clinically diagnosed as having LD (e.g., febrile patients with flulike symptoms, patients with arthralgius or erythematous rashes < 5 cm in size) and who have gositive serologic test results but who do not meet the CDC surveillance case definition. These patients and the large number of unreported paatients being seen and treated for LD wr tick bites must be added to the overall burden of LD in the state. Ann Epiakmiol 19%;6:24-29. KEY WORDS: Lyme disease, epidemiology, surveillance, diagnosis, manifestations, treatment. INTRODUCTION Lyme disease (LD) is a tick-borne zoonotic infection caused by the spirochete &reZia burgdorferi. It accounts for 90% of all reported vector-borne illnesses in the United States (I). It is seasonally transmitted, with most infections in the United States occurring during the months of May through August when nymphal tick and human outdoor activities are at a peak. Ninety percent of these cases occur in the Northeast, the upper Midwest, and northern California (2, 3). The acute illness is manifested by nonspecific constitu- tional symptoms (fever, headache, myalgia, fatigue, and ar- thralgia) and a characteristic skin rash, erythema migrans (EM). The chronic stages of the disease include arthritic, cardiac, and neurologic complications. Based on clinical history and physical examination, the diagnosis of LD can From the Department of Epidemiology and Preventive Medicine, Uni- versity ofMaryland at Baltimore (S.H.S., G.T.S., C.P.), and the Epidemiol- ogy and Disease Control Program, Maryland Department of Health and Mental Hygiene (EL), Baltimore, MD. Addr&&prin~ re&ests to: G.-Zhomas Strickland, MD, PhD, DCMT. Department of Epidemiology and Preventive Medicine, University of Maryland School of Medicine, Baltimore, MD 21201. Received July 18, 1994; accepted April 18, 1995. 0 1996 by Elsevier Science Inc. 655 Avenue of the Americas, New York, NY 10010 be difficult to make. The most frequently used diagnostic test, an enzyme immunoassay (EJA) to detect B. burgdorferi antibodies in the patient’s serum, has poor sensitivity for acute infections and lacks specificity for chronic infections and has a wide intralaboratory and interlaboratory variabil- ity (4-6). The State of Maryland has required the reporting of LD cases since 1989. About 500 cases meeting the Centers for Disease Control and Prevention (CDC) surveillance case definition were reported to the State Department of Health and Mental Hygiene (DHMH) prior to 1991 (7, 8), and another 283 cases were reported in 1991 (9). This study describes some epidemiologic and clinical characteristics and antibiotii: treatment regimens for the ID patients, both those who met and those who did not meet the CDC surveil- lance case definition, reported to the DHMH in 1992. In addi- tion, it contrasts findings in patients meeting the CDC sur- veillance case definition with those in patients who did not. METHODS Surveillance Methods This study includes all patients with LD in Maryland re- ported to the DHMH who were diagnosed from January 1047-2797/96/$15.00 SSDI 1047-2797(95)00096-B
Transcript of Lyme disease surveillance in Maryland, 1992

ELSEVIER
Lyme Disease Surveillance in Maryland, 1992
SUZANNE H. STEINBERG, MD, MS, G. THOMAS STRICKLAND, MD, PHD, DCMT,
CESAR PENA, DVM, MS, AND EBENEZER ISRAEL, MD, MPH
7’he incidence of Lyme disease (LO) reported to the Maryland Department of Health and Mental Hygiene during 1992 was 6.5/l 00,000 population, ranging from 29.3 cases/lOO,OOO on the Eastern Shore (74.4% of all cases) to no cases in the mountains of western Maryland. Among the 317 reported patients, 44.4% gave a history of tick exposure and 78.9% had positive serologic test results. For the 187 (59.0%) patients meeting the Centers for Disease Control and Prevention (CDC) surveillance casedefinition, erythemamigrans (EM) occurred in69.5%, witharthritic (26.7%), neurologic (13.4%), and cardiac (2.1%) manifestations being less frequent. Patients not meeting the surveillance case definition were significantly more likely to have influenza-like symptoms, a smaller rash, and arthralgia. Patients meeting the CDC criteria were more likely to have an onset during the major transmission season in the summer (odds ratio (OR): 2.1; confidence interval (CI): 1.2 to 3.6) since this was the time when most (115/130) patients with EM were detected. Positive serologic results were more likely (OR: 2.2; Cl: 1.2 to 4.2) in those not meeting the case definition. ‘The treatment given to patients thought to have LD was almost always that recommended in the literature and there was no difference between treatment prescribed for patients meeting and those not meeting the case definition. These data show that physicians in Maryland are treating many patients for LD who are clinically diagnosed as having LD (e.g., febrile patients with flulike symptoms, patients with arthralgius or erythematous rashes < 5 cm in size) and who have gositive serologic test results but who do not meet the CDC surveillance case definition. These patients and the large number of unreported paatients being seen and treated for LD wr tick bites must be added to the overall burden of LD in the state. Ann Epiakmiol 19%;6:24-29.
KEY WORDS: Lyme disease, epidemiology, surveillance, diagnosis, manifestations, treatment.
INTRODUCTION Lyme disease (LD) is a tick-borne zoonotic infection caused by the spirochete &reZia burgdorferi. It accounts for 90% of all reported vector-borne illnesses in the United States (I). It is seasonally transmitted, with most infections in the United States occurring during the months of May through August when nymphal tick and human outdoor activities are at a peak. Ninety percent of these cases occur in the Northeast, the upper Midwest, and northern California (2, 3).
The acute illness is manifested by nonspecific constitu- tional symptoms (fever, headache, myalgia, fatigue, and ar- thralgia) and a characteristic skin rash, erythema migrans (EM). The chronic stages of the disease include arthritic, cardiac, and neurologic complications. Based on clinical history and physical examination, the diagnosis of LD can
From the Department of Epidemiology and Preventive Medicine, Uni- versity ofMaryland at Baltimore (S.H.S., G.T.S., C.P.), and the Epidemiol- ogy and Disease Control Program, Maryland Department of Health and Mental Hygiene (EL), Baltimore, MD.
Addr&&prin~ re&ests to: G.-Zhomas Strickland, MD, PhD, DCMT. Department of Epidemiology and Preventive Medicine, University of Maryland School of Medicine, Baltimore, MD 21201.
Received July 18, 1994; accepted April 18, 1995.
0 1996 by Elsevier Science Inc. 655 Avenue of the Americas, New York, NY 10010
be difficult to make. The most frequently used diagnostic test, an enzyme immunoassay (EJA) to detect B. burgdorferi antibodies in the patient’s serum, has poor sensitivity for acute infections and lacks specificity for chronic infections and has a wide intralaboratory and interlaboratory variabil- ity (4-6).
The State of Maryland has required the reporting of LD cases since 1989. About 500 cases meeting the Centers for Disease Control and Prevention (CDC) surveillance case definition were reported to the State Department of Health and Mental Hygiene (DHMH) prior to 1991 (7, 8), and another 283 cases were reported in 1991 (9). This study describes some epidemiologic and clinical characteristics and antibiotii: treatment regimens for the ID patients, both those who met and those who did not meet the CDC surveil- lance case definition, reported to the DHMH in 1992. In addi- tion, it contrasts findings in patients meeting the CDC sur- veillance case definition with those in patients who did not.
METHODS Surveillance Methods This study includes all patients with LD in Maryland re- ported to the DHMH who were diagnosed from January
1047-2797/96/$15.00 SSDI 1047-2797(95)00096-B

AEP Vol. 6, No. 1 Stemberg et al. 25 lanumy 19%: 24-29 LYME DISEASE SURVEILLANCE
1, 1992, through December 31, 1992. Cases were received as reports from physicians using the Maryland Confidential Morbidity Report (MCMR) or from diagnostic laboratories reporting positive serologic test results. Physicians identified by either of these two means were then sent a one-page questionnaire to obtain information on their patient’s age, gender, race, residence, tick bite exposure, time of onset of illness, clinical symptoms and signs, serologic test results, and antibiotic therapy prescribed. If there was no response within 3 weeks, the physician’s office was called and re- minded to return the questionnaire. Patients for whom the information was incomplete were investigated further by telephone interview.
Case Definition
Patients were classified as having met the CDC national surveillance case definition if a physician diagnosed EM of at least 5 cm in diameter or if the patient had a specific rheumatologic, neurologic, or cardiac manifestation com- bined with a positive serologic test result for LD (10).
Statistical Analysis
Differences in proportions were assessed by the x2 test and means were compared by t tests. Odds ratios (ORs) were used to compare risk factors or symptoms between patients meeting and those not meeting the CDC surveillance case definition, with 95% confidence intervals (CIs) calculated using the Mantel-Haenszel method.
RESULTS
Demographics and Tick Exposure
A total of 385 questionnaires were sent to physicians; 337 (87.5%) of these were returned. Ten patients identified by positive serology but not believed by their physicians to have had LD were excluded. Ten patients reported to the DHMH for the first time in 1992, but who had been diag- nosed in earlier years were also excluded. Of the remaining 3 17, all believed by the attending physicians to be patients with LD, 187 (59.0%) met the CDC surveillance case defini- tion for LD.
Of the 317 patients in this report, 56.8% were males. The median age was 34, with a range of 1 to 81 years. Of the 295 patients for whom information on race was available, whites represented 89.2%; blacks, 9.8%; and Asians or His- panics, 1.0%. Forty-four percent of patients gave a history of tick exposure. There was no statistical difference between patients who met the CDC surveillance case definition for LD and those who did not with respect to the mean
TABLE 1. Some characteristics of 317 patients reported to the Maryland Department of Health and Mental Hygiene in 1992 who met or did not meet the CDC surveillance case definition for Lyme disease
Surveillance case definition
Characteristics Met Not met Total
No. (%) 187 (59.0) 130 (41.0) 11: Mean age (SD) 34.0 (22.1) 34.7 (20.0) 34.3 (21.2) Males (%) 112/187 (59.9) 681130 (52.3) 180/317 (56.8) White (96) 160/177 (90.4) 103/118 (67.3) 261/295 (89.2) Tick exposure (%) 65/144 (45.1) 51i117 (43 i-$ 116/261 (44.4) Onset in May-
August (%) 1431187 (76.5) 69/113 (61.0) LW300 (70.7)
n Difference between groups statistically significant; P < 0 00 I
age, or proportion by gender, race, or rick bite exposure (Table 1).
Season& Pattern
The majority (70.7%) of LD patients had onset of symptoms during the transmission season, May through August (Ta- ble 1, Figure 1). Patients meeting the CDC surveillance case definition for LD were more likely to have had an onset during these summer months than during the other 8 months (OR: 2.1; CI: 1.2 to 3.6) since this period was marked by an increase in the number of patients with EM, that is, 115 (87.1%) of 132 compared with 15 (27.3%) of 55 from September through April (OR: 18.0; CI: 8.3 to 39.4). There was no statistically significant (OR: 0.8; CI: 0.4 to 1.5) seasonal variation in onset of illness among the 57 patients who had systemic manifestations of LD in the absence of EM.
Geographic Distribution
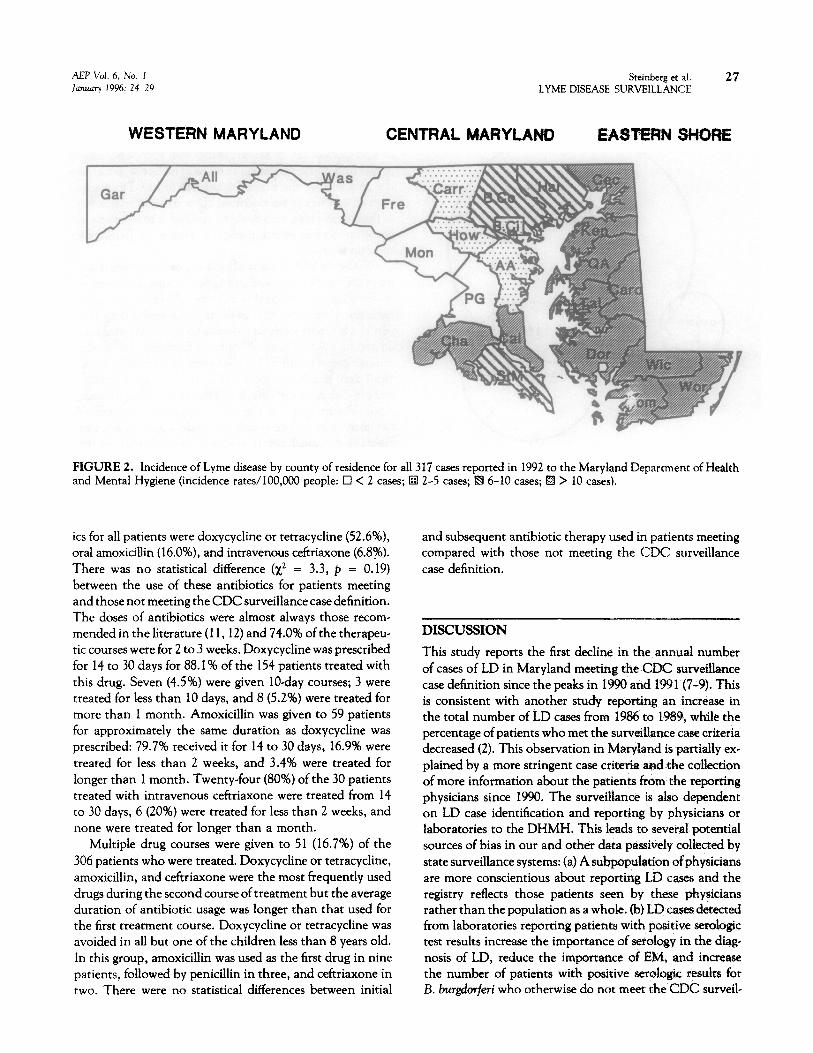
Based on the 1992 population of 4.84 million, the statewide incidence of LD reported to DHMH was 6.5/100,000. It was reported in residents of all but the two most western counties in the state (Figure 2). The highest incidence oc- curred on the Eastern Shore, which had a rate of 29.3 cases/ 100,000, and included 74.4% of all cases reported during 1992. The two counties with the highest incidence rates per 100,000 were Kent (145) and Queen Anne’s (94.5). There was no geographic variability in the ratio of reported pa- tients meeting to those not meeting the CDC surveillance case definition.
Clinical Characteristics
Influenza-like symptoms, including headache, fatigue, myal- gia, or fever, occurred in almost half of the patients and were more frequent (OR: 1.7; CI: 1.1 to 2.7) in patients not meeting CDC surveillance case criteria than in those who did. For the 130 patients not meeting the case definition, the most common (n = 47,36.2%) manifestation was arthralgia

26 Steinberg et al. AEP Vol. 6, No. I LYME DISEASE SURVEILLANCE January 1996: 24-29
80”
60-,
< JanJan Feb Mar Apr May Jun Jul Aug Sep Ott Nov Dee Time (Months)
FIGURE 1. Cases of Lyme disease reported to the Maryland Department of Health and Mental Hygiene in 1992 by month of onset of symptoms (a met CDC criteria; n not met CDC criteria).
(e.g., joint pain but no reported joint swelling). The knees were affected much more frequently (OR: 6.8; CI: 2.6 to 1.5) in those complaining of joint pain who met (70.0%) than in those who did not meet (25.5%) the CDC surveil- lance case definition. As expected, patients reported with neurologic symptoms almost always (25/26) met the CDC surveillance case definition.
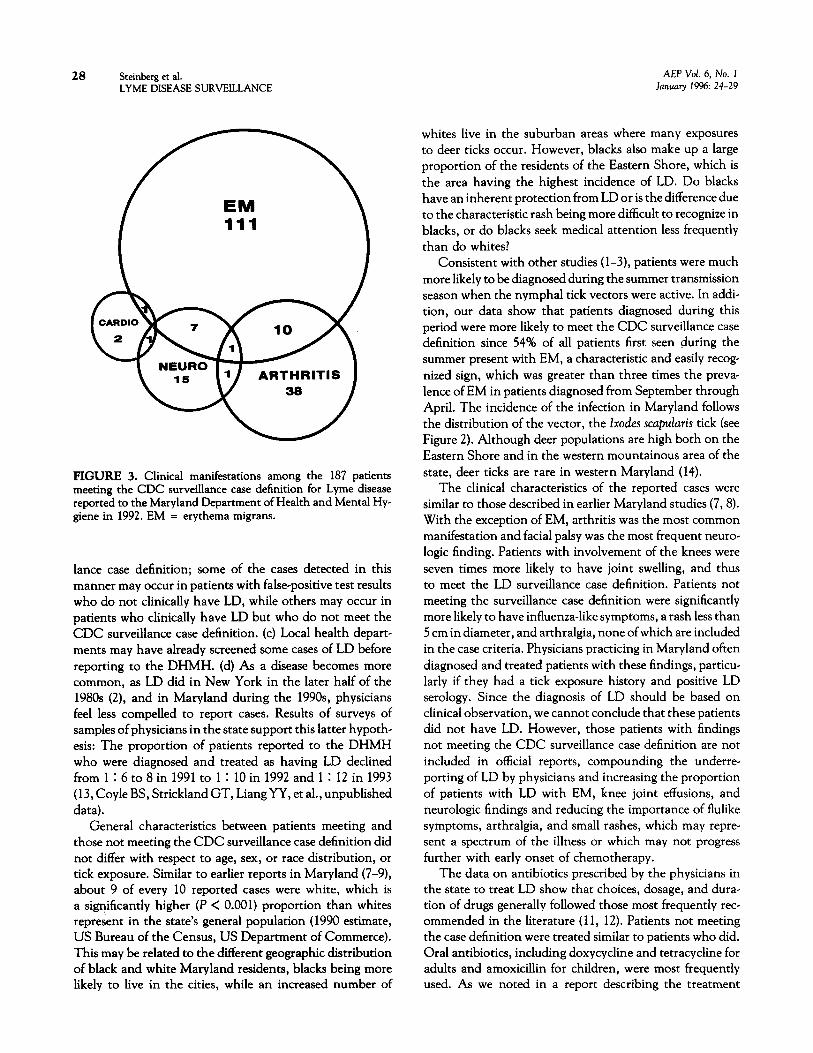
Among the 187 patients meeting the CDC surveillance case definition, (a) EM 5 cm or larger occurred in almost 70%, (b) arthritis was reported in 26.7%, and (c) neurologic findings were present in 13.4% (Figure 3). Four (2.1%) adult male patients had cardiac involvement on the basis of an atrioventricular block noted on the electrocardiogram. The mean size (+ standard deviation) of the EM was reported as 9.4 f 5.6 cm. The knees were the most common (35/ 50) site of arthritis. Sixteen (64%) of the patients with neuro- logic symptoms had facial palsy while 6 had radiculopathies and 3 had encephalitis. Neurologic symptoms occurred more frequently (OR: 3.3; CI: 1.1 to 10.3) in males (20) than in females (5). Twenty-one (11.2%) patients had more than one manifestation (see Figure 3): 10 individuals had EM and arthritis; 7 had neurologic symptoms and EM, 1 had atrioventricular block and EM; 1 had cardiac and neuro-
logic findings; and 2 individuals had arthritic and neuro- logic symptoms, one with and one without EM.
Serologic Response
Criteria for a positive serology result were provided by the laboratory where the physician sent the specimen. Most physician case reports were based on a positive result of a screening EIA without a confirmatory Western blot. Pa- tients not meeting the CDC surveillance case definition were more likely (OR: 2.2; CI: 1.2 to 4.2) to have positive serology (112/130, 86.3%) than were patients meeting the case criteria (138/187,73.8%). Ofthe 130 patients with EM, 81 (62.3%) were reported as having positive serology and by definition, all 57 patients not having EM who met the CDC surveillance case definition had positive serologic test results.
Treatment
Eleven (3.5%) of the 3 17 patients were not given antibiotics by the time they were reported to the DHMH; 255 of the remaining 306 received only one antibiotic course by the time of reporting. The most frequently prescribed antibiot-
AEP Vol. 6, No. I Steinberg et al. January 19%: 24-29 LYME DISEASE SURVEILLAFJCE
27
WESTERN MARYLAND CENTRAL MARYLAND EASTERN SHORE
FIGURE 2. Incidence of Lyme disease by county of residence for all 317 cases reported in 1992 to the Maryland Department of Health and Mental Hygiene (incidence rates/lOO,OOO people: Cl < 2 cases; q 2-5 cases; m 6-10 cases; fE > 10 cases).
its for all patients were doxycycline or tetracycline (52.6%), oral amoxicillin (16.0%), and intravenous ceftriaxone (6.8%). There was no statistical difference (x2 = 3.3, p = 0.19) between the use of these antibiotics for patients meeting and those not meeting the CDC surveillance case definition. The doses of antibiotics were almost always those recom- mended in the literature ( 11,12) and 74.0% of the therapeu- tic courses were for 2 to 3 weeks. Doxycycline was prescribed for 14 to 30 days for 88.1% of the 154 patients treated with this drug. Seven (4.5%) were given IO-day courses; 3 were treated for less than 10 days, and 8 (5.2%) were treated for more than 1 month. Amoxicillin was given to 59 patients for approximately the same duration as doxycycline was prescribed: 79.7% received it for 14 to 30 days, 16.9% were treated for less than 2 weeks, and 3.4% were treated for longer than 1 month. Twenty-four (80%) of the 30 patients treated with intravenous ceftriaxone were treated from 14 to 30 days, 6 (20%) were treated for less than 2 weeks, and none were treated for longer than a month.
Multiple drug courses were given to 51 (16.7%) of the 306 patients who were treated. Doxycycline or tetracycline, amoxicillin, and ceftriaxone were the most frequently used drugs during the second course of treatment but the average duration of antibiotic usage was longer than that used for the first treatment course. Doxycycline or tetracycline was avoided in all but one of the children less than 8 years old. In this group, amoxicillin was used as the first drug in nine patients, followed by penicillin in three, and ceftriaxone in two. There were no statistical differences between initial
and subsequent antibiotic therapy used in patients meeting compared with those not meeting the CDC surveillance case definition.
DISCUSSION
This study reports the first decline in the annual number of cases of LD in Maryland meeting the CDC surveillance case definition since the peaks in 1990 and 1991(7-9). This is consistent with another study reporting an increase in the total number of LD cases from 1986 to 1989, while the percentage of patients who met the surveillance case criteria decreased (2). This observation in Maryland is partially ex- plained by a more stringent case criteria and the collection of more information about the patients from the reporting physicians since 1990. The surveillance is also dependent on LD case identification and reporting by physicians or laboratories to the DHMH. This leads to several potential sources of bias in our and other data passively collected by state surveillance systems: (a) A subpopulation of physicians are more conscientious about reporting LD cases and the registry reflects those patients seen by these physicians rather than the population as a whole. (b) LD cases detected from laboratories reporting patients with positive serologic test results increase the importance of seroiogy in the diig- nosis of LD, reduce the importance of EM, and increase the number of patients with positive serologic results for B. burgdorjeri who otherwise do not meet rhe CDC surveil-
28 Steinberg e.t al. AEP Vol. 6, No. 1 LYME DISEASE SURVEILLANCE January 19%: 24-29
FIGURE 3. Clinical manifestations among the 187 patients meeting the CDC surveillance case definition for Lyme disease reported to the Maryland Department of Health and Mental Hy- giene in 1992. EM = erythema migrans.
lance case definition; some of the cases detected in this manner may occur in patients with false-positive test results who do not clinically have LD, while others may occur in patients who clinically have LD but who do not meet the CDC surveillance case definition. (c) Local health depart- ments may have already screened some cases of LD before reporting to the DHMH. (d) As a disease becomes more common, as LD did in New York in the later half of the 1980s (2), and in Maryland during the 199Os, physicians feel less compelled to report cases. Results of surveys of samples of physicians in the state support this latter hypoth- esis: The proportion of patients reported to the DHMH who were diagnosed and treated as having LD declined from 1 1 6 to 8 in 1991 to 1 : 10 in 1992 and 1 1 12 in 1993 (13, Coyle BS, Strickland GT, Liang YY, et al., unpublished data).
General characteristics between patients meeting and those not meeting the CDC surveillance case definition did not differ with respect to age, sex, or race distribution, or tick exposure. Similar to earlier reports in Maryland (7-9), about 9 of every 10 reported cases were white, which is a significantly higher (P < 0.001) proportion than whites represent in the state’s general population (1990 estimate, US Bureau of the Census, US Department of Commerce). This may be related to the different geographic distribution of black and white Maryland residents, blacks being more likely to live in the cities, while an increased number of
whites live in the suburban areas where many exposures to deer ticks occur. However, blacks also make up a large proportion of the residents of the Eastern Shore, which is the area having the highest incidence of LD. Do blacks have an inherent protection from LD or is the difference due to the characteristic rash being more difficult to recognize in blacks, or do blacks seek medical attention less frequently than do whites?
Consistent with other studies (l-3), patients were much more likely to be diagnosed during the summer transmission season when the nymphal tick vectors were active. In addi- tion, our data show that patients diagnosed during this period were more likely to meet the CDC surveillance case definition since 54% of all patients first seen during the summer present with EM, a characteristic and easily recog nized sign, which was greater than three times the preva- lence of EM in patients diagnosed from September through April. The incidence of the infection in Maryland follows the distribution of the vector, the Zxodes sc+4luris tick (see Figure 2). Although deer populations are high both on the Eastern Shore and in the western mountainous area of the state, deer ticks are rare in western Maryland (14).
The clinical characteristics of the reported cases were similar to those described in earlier Maryland studies (7,8). With the exception of EM, arthritis was the most common manifestation and facial palsy was the most frequent neuro- logic finding. Patients with involvement of the knees were seven times more likely to have joint swelling, and thus to meet the LD surveillance case definition. Patients not meeting the surveillance case definition were significantly more likely to have influenza-like symptoms, a rash less than 5 cm in diameter, and arthralgia, none of which are included in the case criteria. Physicians practicing in Maryland often diagnosed and treated patients with these findings, particu- larly if they had a tick exposure history and positive LD serology. Since the diagnosis of LD should be based on clinical observation, we cannot conclude that these patients did not have LD. However, those patients with findings not meeting the CDC surveillance case definition are not included in official reports, compounding the underre- porting of LD by physicians and increasing the proportion of patients with LD with EM, knee joint effusions, and neurologic findings and reducing the importance of flulike symptoms, arthralgia, and small rashes, which may repre- sent a spectrum of the illness or which may not progress further with early onset of chemotherapy.
The data on antibiotics prescribed by the physicians in the state to treat LD show that choices, dosage, and dura- tion of drugs generally followed those most frequently rec- ommended in the literature (11, 12). Patients not meeting the case definition were treated similar to patients who did. Oral antibiotics, including doxycycline and tetracycline for adults and amoxicillin for children, were most frequently used. As we noted in a report describing the treatment

AEF’ Vol. 6, No. 1 Steinberg et al. 29 January 1996: 24-29 LYME DISEASE SIJRVFILLANCE
of LD during 1991 (9), intravenous therapy, mostly with ceftriaxone, was almost exclusively used for those who had arthritic, neurologic, or cardiac manifestations. Four (79.7%) of every five patients with LD were treated with antibiotics for a duration ranging from 14 to 30 days. A very few were treated longer than 1 month. However, over one (16.9%) of every six was treated for less than 2 weeks, which may be an insufficient period to completely eradicate B. burgdorfen’.
REFERENCES 1. Centers for Disease Control. Lyme Disease.-Ilnited States, 1991-
1992, MMWR. 1993;42:345-348,
2. White DJ, Chang H-H, Benach JL, et al. The geographic spread and temporal increase of the Lyme disease epidemic, JAMA. lY91;266: 1230-1236.
3.
There is no clinically practical gold standard for diagnos- ing all cases of LD (15-18). Our results bolster the conclusion that physicians in Maryland were often diagnosing and treating patients not meeting the CDC surveillance case definition for LD in 1992. Case definitions for diseases in which there are no gold standards for diagnosis are usually narrowly set to provide internal and external validity so that clinical decisions and comparisons between groups of patients can be reliably made. In the case of LD, it has not been possible to broaden this definition to include the many patients who have positive LD serology and uncharacteristic symptoms, including arthralgia, flulike symptoms, chronic fatigue syndrome, and fibromyalgia (15-19). However, resi- dents of endemic areas are so sensitized to the risk for LD that they often seek medical attention with these symp tom complexes or for tick exposure, and the physician is often under intense pressure to treat them for LD. Our data show that 40% of the patients in Maryland reported to the DHMH fall within that category and many more are treated for LD and not reported (Coyle BS, Strickland GT, Liang YY, et al., unpublished data). This clearly documents the need to provide practicing physicians in the state guidelines for ordering screening serologic tests and encouragement to obtain Western blot confirmation before treating sero- logically positive patients with atypical findings of LD (6, 15-19).
4.
5.
Spach DH, Lilies WC, Campbell GL, et al. Tick-borne disease in the United States, N Engl J Med. 1993;329:93&93Q.
Luger SW, Krauss E. Serologic tests for Lyme disease: Inrerlaboratory variability, Arch Intern Med. 1990;150:761-76!.
Bakken LL, Case KL, Callister SM, et al. Performance of 45 labora- tories participating in a proficiency program for Lyme disease serology, JAMA. 1992;268:891-895.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
This research was partially supported by the Maryland Department of Health and Mental Hygiene Disease Control Program and by the Agency for Health Care Policy and Research grant 5 ROI HS07813. In addition, Dr. Steinberg received a CDC/Association of Teachers of Preventive Med- icine Public Health Internship during part of the time she worked on the project.
18.
19.
Golightly MG. Laboratory considerations in the diagnosis and man- agement of Lyme borreliosis, Am J Clin Parhol. 1993;99:168-173.
Thambidurai RM, Grigor JK, Herman JT, Israel E. Lyme disew: Epidemiological characteristics in Marvland, 1984 - ! 986, h4d Med 1. 1988;37:465-467.
Mitchell CS, Cloeren M, Israel E, et al. Lyme disease in Maryland: 1987-1990, Md Med J. 1992;40:391- 396.
Strickland GT, Caisley 1, Woubeshet M, Israel 1. AntibiotIc therapy for Lyme disease in Maryland, Public Health Rep. 1994;109:745-749.
Centers for Disease Control. Case definitions for public he&h surveil- lance, MMWR 1990;39(No. RR-13):19-21.
Rahn DW, Malawista SE. Lyme disease; recommendanons for diagno- sis and treatment, Ann Intern Med. 1991;114 4% 481.
Anonymous. Treatment of Lyme disease, Med Let<. 199L;34:95-97.
Jung PI, Nahas JN, Strickland GT, et al. Marylatid physicIan’s survey on Lyme disease, Md Med J. 1994;43:447-450
Amerasinghe FP, Breisch NL, Neidhardt K, er aI. Increasing density and Borrelia burgdorferi infection ofdeer-infesting lx&s dammini (acari: Ixodidae) in Maryland, J Med Entomol. 1993;30:858-864.
Blaaus AA, Nohlmans MK, van den Bogaard BE, van der Linden S. Diagnostic tools in Lyme borreliosis: Clinical history compared with serology, J Clin Epidemiol. 1992;11:1129--1 I ic.
Sigal L. Summary of the first 100 patients see!: at 21 Lwne disease referral center, Am J Med. 1990;88;577-581
Burdge DR, O’Hanlon DP. Experience at a referral center for patients with suspected Lyme disease in an area of nonendemicity: First 65 patients, Clin Infect Dis. 1993;16:558-560.
Steere AC, Taylor E, McHugh GL, Logigian IX The overdiagnosis of Lyme disease, JAMA. 1993;269:1812-1816.
Lightfoot RW, Luft BJ, Rahn DW, et ai. Empiric parenteral antibiotic treatment of patients with fibromyalgia and fatigue and a positive serologic result for Lyme disease: A cost-effecriT;eness analysis, Ann Intern Med. lYY3;119:5@3-509.