Mathematical modelling of atherosclerosis as an inflammatory disease

lable at ScienceDirect
Atherosclerosis 239 (2015) 328e334
Contents lists avai
Atherosclerosis
journal homepage: www.elsevier .com/locate/atherosclerosis
Low estimated glomerular filtration rate is associated with pooroutcomes in patients who suffered a large artery atherosclerosisstroke
Shin-Joe Yeh a, Jiann-Shing Jeng a, Sung-Chun Tang a, Chung-Hsiang Liu b, Shih-Pin Hsu c,Chih-Hung Chen d, Li-Ming Lien e, Huey-Juan Lin f, Chiu-Mei Chen g, Ruey-Tay Lin h,Siu-Pak Lee i, Ching-Huang Lin j, Chung-Hsin Yeh k, Yu Sun l, Ming-Hui Sun m,Jiu-Haw Yin n, Che-Chen Lin o, Chi-Pang Wen p, Li-Kai Tsai a, *, Fung-Chang Sung o, **,Chung Y. Hsu q, Taiwan Stroke Registry Investigatorsa Stroke Center and Department of Neurology, National Taiwan University Hospital, Taipei, Taiwan, ROCb Department of Neurology, China Medical University Hospital, Taichung, Taiwan, ROCc Department of Neurology, E Da Hospital, Kaohsiung, Taiwan, ROCd Department of Neurology, National Cheng Kung University Hospital, Tainan, Taiwan, ROCe Department of Neurology, Shin Kong Wu-Ho-Su Memorial Hospital, Taipei, Taiwan, ROCf Department of Neurology, Chi Mei Medical Center, Tainan, Taiwan, ROCg Department of Neurology, Chung Shan Medical University Hospital, Taichung, Taiwan, ROCh Department of Neurology, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan, ROCi Department of Neurology, Far Eastern Memorial Hospital, New Taipei City, Taiwan, ROCj Section of Neurology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, ROCk Department of Neurology, Show Chwan Memorial Hospital, Changhua, Taiwan, ROCl Department of Neurology, En Chu Kong Hospital, New Taipei City, Taiwan, ROCm Department of Neurology, Kuang Tien General Hospital, Taichung, Taiwan, ROCn Department of Neurology, Cheng-Hsin General Hospital, Taipei, Taiwan, ROCo Department of Public Health, China Medical University, Taichung, Taiwan, ROCp Institute of Population Science, National Health Research Institute, Miaoli, Taiwan, ROCq Graduate Institute of Clinical Medical Science, China Medical University and Hospital, Taichung, Taiwan, ROC
a r t i c l e i n f o
Article history:Received 18 August 2014Received in revised form11 January 2015Accepted 31 January 2015Available online 7 February 2015
Keywords:AtherosclerosisBrain infarctionGlomerular filtration rate
* Corresponding author. Department of NeurologyHospital, No 7, Chung-Shan South Road, Taipei 100, T** Corresponding author. Department of Public Hea91 Hsueh-Shih Road, Taichung 404, Taiwan, ROC.
E-mail addresses: [email protected] (L.-K. T(F.-C. Sung).
http://dx.doi.org/10.1016/j.atherosclerosis.2015.01.0380021-9150/© 2015 Elsevier Ireland Ltd. All rights rese
a b s t r a c t
Objectives: The relationship between low estimated glomerular filtration rate (eGFR) and the outcome ofischemic stroke remains controversial, despite the close association between kidney dysfunction andatherosclerosis.Methods: This study conducted subgroup analysis using data from the prospective Taiwan Stroke Reg-istry to investigate the relationship between eGFR at the time of admission and 6-month functionaloutcomes in patients with the large artery atherosclerotic (LAA) subtype of acute ischemic stroke. Strokeseverity was assessed using the National Institutes of Health Stroke Scale (NIHSS), and outcomes weredefined as modified Rankin Scale and mortality status at 6 months post stroke.Results: Of the 8052 patients with the LAA subtype of acute ischemic stroke in this study, 3312 (41.1%)had eGFR <60 mL/min/1.73 m2. The adjusted odds ratios of worse functional outcomes following a strokewere 1.10 (95% confidence interval [CI], 0.95e1.28), 1.60 (95% CI, 1.22e2.11) and 1.60 (95% CI, 1.10e2.33) inpatients with eGFR 30e59, 15e29, and <15 as compared with those with eGFR 60e119 mL/min/1.73 m2,respectively. Increased risk of mortality was closely and independently related to high NIHSS scores andlow eGFR levels. Stroke severity and eGFR were also synergistically related to 6-month mortality, with an
, National Taiwan Universityaiwan, ROC.lth, China Medical University,
sai), [email protected]
rved.

S.-J. Yeh et al. / Atherosclerosis 239 (2015) 328e334 329
adjusted hazard ratio of 21.19 (95% CI, 9.69e46.35) in patients with NIHSS >15 and eGFR <15 mL/min/1.73 m2, compared with those with NIHSS 0e5 and eGFR 60e119 mL/min/1.73 m2.Conclusions: Low eGFR was significantly and independently associated with 6-month functional out-comes and mortality in patients with the LAA subtype of acute ischemic stroke. The deleterious rela-tionship between low eGFR levels and mortality following stroke was exacerbated by its synergisticassociation with stroke severity.
© 2015 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Stroke is the leading cause of chronic disability and the thirdleading cause of mortality worldwide [1]. Kidney dysfunction isalso being recognized as an important public health concern [2],and patients with dysfunctional kidneys face a higher risk of car-diovascular disease and stroke [3,4]. For example, in a large cohortstudy in China, 14%e16% of stroke patients were shown to havekidney dysfunction [5]. A previous meta-analysis study furtherrevealed that the relative risk of stroke was 1.43 among patientswith an estimated glomerular filtration rate (eGFR) of <60 ml/min/1.73 m2 [6]. The close association between stroke and kidneydysfunction is partly explained by their common vascular riskfactors [7]. In addition, kidney dysfunction has been shown to be anindependent risk factor for atherosclerosis in both humans andanimals [8,9], and patients with kidney dysfunction are more likelyto have unstable atherosclerotic plaques [10]. Thus, kidneydysfunction increases the risk of suffering from the large arteryatherosclerosis (LAA) subtype of ischemic stroke [11].
The precise nature of the relationship between low eGFR andischemic stroke outcomes remains controversial [12e15]. Someresearchers have claimed that the functional outcome ofischemic stroke is worse in patients with low eGFR [12,13], whileother researchers have been unable to identify such an associa-tion [14,15]. These mixed results may be related to heterogeneityof stroke subtypes among study populations. In addition, notonly low eGFR but also high eGFR (�120 ml/min/1.73 m2) wasassociated with higher post-stroke mortality [13], but its influ-ence on specific stroke subtypes is still not clear. The knownassociation between kidney dysfunction and atherosclerosis[8,9], as well as between LAA and high stroke mortality [16,17],compelled us to explore the impact that eGFR level has on strokeoutcomes, with a particular focus on the LAA subtype. We hy-pothesized that both low and high eGFR levels have negativeimpact on the outcome after LAA subtype ischemic stroke. Wealso evaluated the combined effects of eGFR levels and strokeseverity on the risk of mortality.
2. Methods
2.1. Patients
Between May 2006 and April 2009, 42,610 patients with acutestroke were prospectively registered with the Taiwan Stroke Reg-istry (TSR) [18]. The TSR is a nationwide program, which wasestablished to provide a reliable national stroke database. A total of39 academic and community hospitals participated in the program,and a 4-step quality control regimen was followed to ensure thereliability of data [18]. Patients were registered within 10 days fromthe onset of stroke, and the stroke was defined according to theWorld Health Organization as rapid developing focal neurologicaldeficit lasting for longer than 24 h [19]. Study protocol wasapproved by the ethics committee at each participating hospital,and written informed consent was obtained from all participants. If
a subject was incommunicable, we obtained informed consentfrom his/her family.
To be included in our study, patients should have received aneurological assessment and computerized tomography (CT) and/or magnetic resonance imaging (MRI) to clarify ischemic strokefrom hemorrhagic stroke. A total of 31,336 patients with acuteischemic stroke were identified in the TSR database, and they weredivided into 5 subtypes according toTOAST criteria (The Trial of Org10,172 in Acute Stroke Treatment) [20]. Among them, 8215 patientspresented the LAA subtype. The LAA subtype was defined by eithersignificant (>50%) stenosis or occlusion of a major cervical or ce-rebral artery based on carotid duplex sonography, transcranialcolor-coded sonography, CT/MRI angiography, or conventionalangiography. Patients without serum creatinine data at the time ofadmissionwere excluded, which resulted in a total of 8052 patientsincluded in the study.
2.2. Data collection
Clinical data were compiled prospectively by TSR-trained neu-rologists and nurses (Supplementary data). To assess the impact ofeGFR on stroke outcomes, we collected data related to the followingparts: (1) preadmission demographic profile, previous medicalhistory, and medications taken prior to admission; (2) score on theNational Institutes of Health Stroke Scale (NIHSS) at the time ofadmission, risk factors of stroke, serum creatinine levels, electro-cardiogram results, CT/MRI findings, and duplex sonographic re-sults; and (3) mortality and modified Rankin scale (mRS) score 6months after onset of stroke, which were obtained via phoneinterview. Those who were followed up for less than 6 months andwithout event (mortality) were censored. The number of lost tofollow-up at 6 months was 2844. Serum creatinine level and otherlab data were collected at individual hospitals upon admission.
We calculated eGFR using the CKD-EPI (Chronic Kidney DiseaseEpidemiology Collaboration) equation, specifically:
eGFR ¼ 141�minðSCr=k;1Þa �maxðSCr=k;1Þ�1:209 � 0:993Age
� ½1:018 if Female� � ½1:1 in Chinese population�;
where SCr is serum creatinine level on admission; k is 0.7 for fe-males and 0.9 is for males; a is �0.329 for females and �0.411 is formales; min indicates the minimum of SCr/k or 1; andmax indicatesthe maximum of SCr/k or 1 [21]. Our classification of kidneydysfunction was in accordance with that of the K/DOQI ClinicalPractice Guidelines, in which low eGFR was defined as eGFR<60 mL/min/1.73 m2 [22], and high eGFR as eGFR �120 mL/min/1.73 m2 [13].
2.3. Statistical analysis
Eligible patients with LAA ischemic stroke were stratified into 5subgroups according to eGFR level (�120 mL/min/1.73 m2,60e119 mL/min/1.73 m2, 30e59 mL/min/1.73 m2, 15e29 mL/min/

Table 1Characteristics of patients with LAA subtype ischemic stroke by eGFR level.
eGFR (mL/min/1.73 m2) P-value
�120 60e119 30e59 15e29 <15
(n ¼ 41) (n ¼ 4699) (n ¼ 2645) (n ¼ 443) (n ¼ 224)
Age in years 41 (15.1) 65 (12.1) 74.0 (10.4) 74.3 (10.5) 70.4 (11.9) <0.0001Body mass index in kg/m2 23.4 (3.8) 24.5 (3.8) 24.3 (3.9) 24.6 (3.9) 23.5 (4.2) 0.0005Number of males 18 (43.9) 3000 (63.8) 1574 (59.5) 250 (56.4) 101 (45.1) <0.0001NIHSS 0e5 17 (41.5) 2541 (54.1) 1250 (47.3) 200 (45.1) 98 (43.8) <0.0001
6e15 18 (43.9) 1541 (32.8) 942 (35.6) 155 (35) 76 (33.9) <0.0001>15 6 (14.6) 617 (13.1) 453 (17.1) 88 (19.9) 50 (22.3) <0.0001
Hypertension <0.0001No 23 (56.1) 1032 (22.0) 349 (13.2) 37 (8.4) 22 (9.8)Yes 16 (39.0) 3646 (77.6) 2284 (86.4) 403 (91.0) 202 (90.2)Missing value 2 (4.9) 21 (0.5) 12 (0.5) 3 (0.7) 0
Diabetes <0.0001No 25 (61.0) 2683 (57.1) 1394 (52.7) 201 (45.4) 92 (41.1)Yes 15 (36.6) 1980 (42.1) 1234 (46.7) 241 (54.4) 132 (58.9)Missing value 1 (2.4) 36 (0.8) 17 (0.6) 1 (0.2) 0
Dyslipidemia 0.0234No 26 (63.4) 2026 (43.1) 1092 (41.3) 181 (40.9) 103 (46.0)Yes 12 (29.3) 2406 (51.2) 1375 (52.0) 242 (54.6) 105 (46.7)Missing value 3 (7.3) 267 (5.7) 178 (6.7) 20 (4.5) 16 (7.2)
Ischemic heart disease <0.0001No 40 (97.6) 4200 (89.4) 2252 (85.2) 355 (80.2) 177 (79.0)Yes 1 (2.4) 499 (10.6) 393 (14.9) 88 (19.9) 47 (21.0)
Previous stroke <0.0001No 34 (82.9) 3441 (73.2) 1729 (65.4) 262 (59.1) 147 (65.6)Yes 5 (12.2) 1238 (26.4) 897 (33.9) 179 (40.4) 77 (34.4)Missing value 2 (4.9) 20 (0.4) 19 (0.7) 2 (0.5) 0
Smoking <0.0001No 25 (61.0) 2517 (53.6) 1592 (60.2) 283 (63.9) 164 (73.2)Yes 15 (36.6) 2166 (46.1) 1039 (39.3) 159 (35.9) 60 (26.8)Missing value 1 (2.4) 16 (0.3) 14 (0.5) 1 (0.2) 0
Alcohol <0.0001No 34 (82.9) 3819 (8.13) 2305 (87.2) 407 (91.9) 206 (92.0)Yes 6 (14.6) 865 (18.4) 328 (12.4) 35 (7.9) 18 (8.0)Missing value 1 (2.4) 15 (0.3) 12 (0.5) 1 (0.2) 0
Abbreviations: LAA, large artery atherosclerosis; eGFR, estimated glomerular filtration rate; NIHSS, National Institutes of Health Stroke Scale.Data are presented as number (percent), except for age and body mass index, which are presented as mean (standard deviation).
Fig. 1. Outcomes at six months post-large artery atherosclerotic (LAA) ischemic strokedefined by modified Rankin Scale (0e1, 2e3, 4e5, death), according to eGFR level.
S.-J. Yeh et al. / Atherosclerosis 239 (2015) 328e334330
1.73 m2, and <15 mL/min/1.73 m2), and baseline information wascompared. For this, we considered age, gender, body mass index,initial NIHSS score, prevalence of comorbidities (hypertension,diabetes, dyslipidemia, old ischemic stroke, and ischemic heartdisease), smoking habits, and alcohol consumption. Chi-squaretests and ANOVA were used to determine among-group differ-ences in categorical data and continuous data, respectively. Weidentified key variables influencing poor functional outcome (mRS>3) and mortality 6 months after onset of stroke using a logisticregression model. For regression analysis, we adjusted all of thesignificant determinants in the baseline information analysis.Multivariable Cox proportional hazards regression analysis wasused to estimate the adjusted hazard ratio (HR) and its 95% confi-dence interval (CI) of death among stroke patients with low or higheGFR levels, high NIHSS scores, or female gender.We also tested theincreased trend of the mortality risk in different levels of eGFR andNIHSS. We considered eGFR as a continuous variable and used theCox model to estimate the effect of eGFR by different levels ofNIHSS. On the other hand, we considered NIHSS score as acontinuous variable and estimated the effect of NIHSS score bydifferent level of eGFR with Cox model. KaplaneMeier analysis wasused to estimate the survival of LAA stroke patients according toeGFR level or initial NIHSS score. A log-rank test was used todetermine differences among groups. Two-tailed P values of lessthan 0.05 were considered statistically significant. Data manage-ment and analysis were performed using SAS 9.3 software (SASInstitute, Cary, NC, USA), and the cumulative incidence curve was
drawn using R software (R Foundation for Statistical Computing,Vienna, Austria).
3. Results
3.1. Patient characteristics
Among the 8052 subjects with the LAA subtype of acuteischemic stroke, 3312 (41.1%) had eGFR <60 mL/min/1.73 m2,

Table 2Logistic regression analysis for determinants of poor outcomes and mortality at 6months after LAA subtype ischemic stroke.
N Poor outcomea Mortalityb
No. ofcases
OR (95% CI) No. ofcases
OR (95% CI)
eGFRlevel
�120 41 8 0.33 (0.07e1.63) 3 ec
60e119 4699 1062 1.00 (Reference) 173 1.00 (Reference)30e59 2645 837 1.10 (0.95e1.28) 178 1.48 (1.13e1.92)15e29 443 167 1.60 (1.22e2.11) 53 2.68 (1.79e4.02)<15 224 90 1.60 (1.10e2.33) 33 3.56 (2.16e5.87)
InitialNIHSS
<6 4106 427 1.00 (Reference) 102 1.00 (Reference)
6e15 2732 938 4.05 (3.49e4.71) 134 1.53 (0.99e2.37)>15 1214 799 16.25 (13.4e19.71) 204 2.34 (1.57e3.48)
Gender Female 3109 1002 1.00 (Reference) 182 1.00 (Reference)Male 4943 2164 1.22 (1.03e1.44) 258 0.84 (0.63e1.13)
Data are presented as adjusted odds ratios (95% confidence intervals).The adjusted model included eGFR levels, age, gender, body mass index, initialNIHSS score, hypertension, diabetes, dyslipidemia, old ischemic stroke, ischemicheart disease, smoking, and alcohol consumption.Abbreviations: LAA, large artery atherosclerosis; eGFR, estimated glomerularfiltration rate; NIHSS, National Institutes of Health Stroke Scale; N, number ofparticipants.
a Adjusted odds ratios for a poor outcome (mRS >3) compared with a goodoutcome (mRS �3).
b Adjusted odds ratios for death compared to survival.c Without an odds ratio due to relatively few cases in this subgroup.
S.-J. Yeh et al. / Atherosclerosis 239 (2015) 328e334 331
including 2645 (32.8%) with eGFR 30e59, 443 (5.5%) with eGFR15e29, and 224 (2.8%) with eGFR <15 mL/min/1.73 m2, while 41(0.5%) had eGFR �120 mL/min/1.73 m2. We determined that eGFRlevels were greatly decreased among patients who: (1) were older,(2) were female, (3) had a high NIHSS score, (4) had previouslysuffered from ischemic stroke, (5) had previously suffered fromischemic heart disease, or (6) currently suffered from hypertensionor diabetes (P < 0.0001) (Table 1).
3.2. Kidney function and stroke outcome
Patients with low eGFR levels tended to have higher mRS scoresat 6 months post-LAA ischemic stroke, while the high eGFR sub-group (eGFR �120 mL/min/1.73 m2) had higher percentages ofmortality and lower percentage of mRS 0e1, as compared witheGFR 60e119 mL/min/1.73 m2 subgroup (Fig. 1). Poor functionaloutcome (mRS >3) following stroke was associated with loweringin eGFR levels as well as with increase in NIHSS scores (Table 2). Theadjusted odds ratios (aORs) for a poor outcome associated witheGFR 30e59, 15e29, and <15 mL/min/1.73 m2 were 1.10 (95% CI,0.95e1.28), 1.60 (95% CI, 1.22e2.11), and 1.60 (95% CI, 1.10e2.33),respectively. High eGFR level did not have significant influence onthe outcome. Elevated NIHSS score was shown to be a significantdeterminant of poor outcome, with an adjusted OR of 4.05 (95% CI,3.49e4.71) in patients with NIHSS scores of 6e15 and 16.25 (95% CI,13.4e19.71) in patients with NIHSS scores >15. In addition, mor-tality risk at 6 months post-stroke increased with a low eGFR levelor a high NIHSS score (Table 2). The adjusted ORs of death in pa-tients with eGFR 30e59,15e29, and <15mL/min/1.73 m2 were 1.48(95% CI, 1.13e1.92), 2.68 (95% CI, 1.79e4.02), and 3.56 (95% CI,2.16e5.87), respectively. Female patients had higher risk to havepoor outcome (aOR, 1.22; 95% CI, 1.03e1.44) but not with highermortality (aOR, 0.84; 95% CI, 0.63e1.13). KaplaneMeier analysisrevealed that higher NIHSS score with any level of eGFR wasindependently associated with higher mortality rates at 6 monthspost-LAA subtype ischemic stroke (P < 0.0001), and this relation-ship was exaggerated by the worsening of eGFR (Fig. 2AeD).
3.3. Kidney function and stroke severity synergistically associatedwith stroke mortality
Mortality rates at 6 months after LAA subtype ischemic strokeshowed a significant and proportional increase with initial NIHSSscore and an inverse increase with eGFR level (Table 3). In a Coxregression model using stroke patients with NIHSS scores 0e5 andeGFR 60e119 mL/min/1.73 m2 as the reference group, the adjustedHR of death increased to 2.81 (95% CI, 1.40e5.64) and 1.73 (95% CI,0.52e5.74) in patients with NIHSS score 0e5 combined with eGFR15e29 and eGFR <15 mL/min/1.73 m2, respectively (P value fortrend ¼ 0.028). In addition, the adjusted HR of death increased to5.17 (95% CI, 3.38e7.92) in patients with NIHSS score >15 and eGFR60e119 mL/min/1.73 m2 (P value for trend <0.0001). Of note, theadjusted HR of death increased to 21.19 (95% CI, 9.69e46.35) inpatients with NIHSS score >15 and eGFR <15 mL/min/1.73 m2,indicating that kidney dysfunction and stroke severity had syner-gistic effects on the risk of mortality due to stroke.
4. Discussion
A high incidence of low eGFR was observed in this large cohortof patients with the LAA subtype of ischemic stroke. In addition,low eGFR was associated with a worse functional outcome and ahigher mortality rate at 6 months post-stroke. The adverse rela-tionship between kidney dysfunction and stroke mortality wasexacerbated by stroke severity. These results confirmed the
significant and independent relationship between low eGFR andpoor stroke outcome in patients with LAA stroke subtype.
The percentage of eGFR <60 mL/min/1.73 m2 in our cohort ofLAA subtype ischemic stroke patients (41.4%) wasmuch higher thanthat observed in a previous report (18%) [3]. This finding highlightsthe key role of kidney dysfunction, particularly among patientswith the LAA subtype of ischemic stroke. Kidney dysfunction isusually an indicator of the severity and duration of vascular riskfactors, most commonly hypertension and diabetes [13], and thesevascular risk factors promote atherosclerosis [23]. Kidneydysfunction can also exacerbate hypertension, which leads to avicious cycle [15]. In addition, uremic toxins can facilitate thedevelopment and progression of atherosclerosis through endo-thelial dysfunction, and this is heightened by oxidative stress andinflammatory reaction [24,25]. Finally, many patients with kidneydysfunction present with vascular calcification, which could pro-mote plaque ruptures and arterial stiffness [26]. In this manner,kidney dysfunction is strongly associated with LAA subtype ofischemic stroke.
After adjusting for covariates including stroke severity, loweGFR level was significantly associated with worse functionaloutcome and higher mortality at 6 months post-stroke. There areseveral possible explanations for this phenomenon. For example,patients with kidney dysfunction may have higher risk of neuro-logical deterioration and hemorrhagic transformation followingischemic stroke [14,27]. In addition, patients with kidneydysfunction tend to face higher risk of subsequent myocardialinfarction or recurrent stroke [6,28].
High eGFR (�120 mL/min/1.73 m2) has been revealed to beassociated with adverse outcome in ischemic stroke patients [13].In the LAA population in this study, patients with high eGFR tendedto be at a higher risk of death, but it was not significantly associatedwith poor outcome. Patients with high eGFR were younger and atan elevated risk of mortality after stroke, whichwas consistent witha Finland study reported by Putaala et al. [13]. Our study furthershowed that the diabetic prevalence was lower in patients withhigh eGFR than those with normal eGFR (37.5% vs. 42.5%). However,
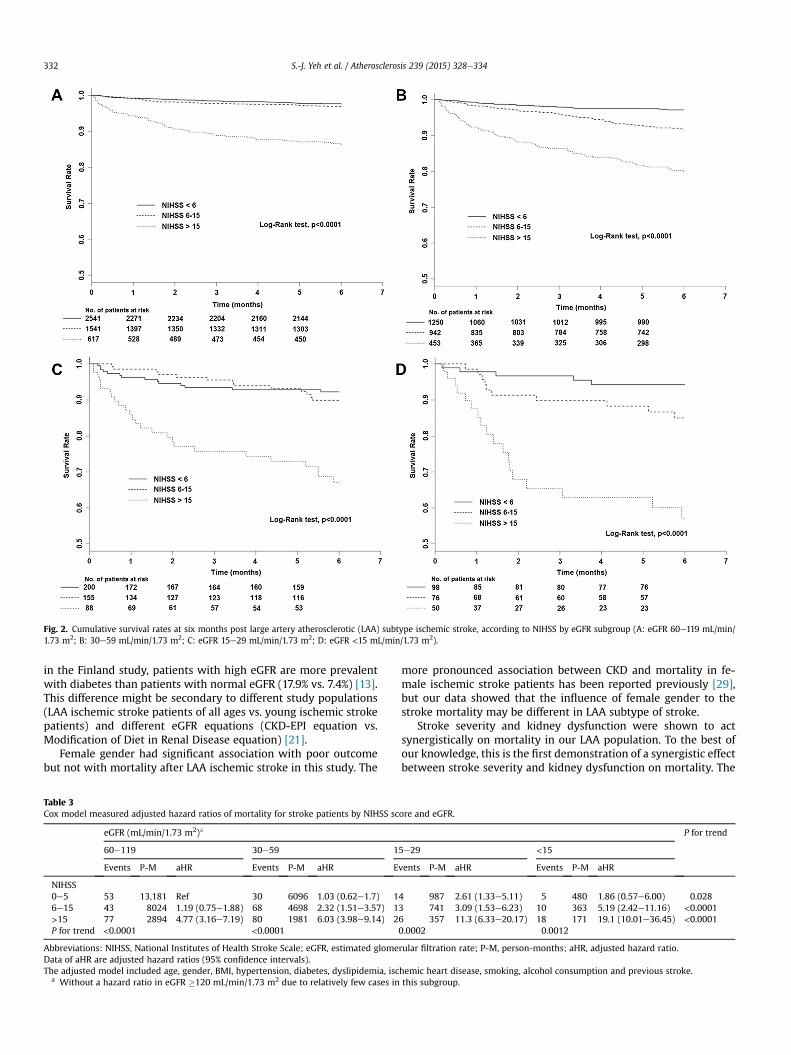
Fig. 2. Cumulative survival rates at six months post large artery atherosclerotic (LAA) subtype ischemic stroke, according to NIHSS by eGFR subgroup (A: eGFR 60e119 mL/min/1.73 m2; B: 30e59 mL/min/1.73 m2; C: eGFR 15e29 mL/min/1.73 m2; D: eGFR <15 mL/min/1.73 m2).
S.-J. Yeh et al. / Atherosclerosis 239 (2015) 328e334332
in the Finland study, patients with high eGFR are more prevalentwith diabetes than patients with normal eGFR (17.9% vs. 7.4%) [13].This difference might be secondary to different study populations(LAA ischemic stroke patients of all ages vs. young ischemic strokepatients) and different eGFR equations (CKD-EPI equation vs.Modification of Diet in Renal Disease equation) [21].
Female gender had significant association with poor outcomebut not with mortality after LAA ischemic stroke in this study. The
Table 3Cox model measured adjusted hazard ratios of mortality for stroke patients by NIHSS sc
eGFR (mL/min/1.73 m2)a
60e119 30e59 1
Events P-M aHR Events P-M aHR E
NIHSS0e5 53 13,181 Ref 30 6096 1.03 (0.62e1.7) 16e15 43 8024 1.19 (0.75e1.88) 68 4698 2.32 (1.51e3.57) 1>15 77 2894 4.77 (3.16e7.19) 80 1981 6.03 (3.98e9.14) 2P for trend <0.0001 <0.0001
Abbreviations: NIHSS, National Institutes of Health Stroke Scale; eGFR, estimated glomeData of aHR are adjusted hazard ratios (95% confidence intervals).The adjusted model included age, gender, BMI, hypertension, diabetes, dyslipidemia, isc
a Without a hazard ratio in eGFR �120 mL/min/1.73 m2 due to relatively few cases in
more pronounced association between CKD and mortality in fe-male ischemic stroke patients has been reported previously [29],but our data showed that the influence of female gender to thestroke mortality may be different in LAA subtype of stroke.
Stroke severity and kidney dysfunction were shown to actsynergistically on mortality in our LAA population. To the best ofour knowledge, this is the first demonstration of a synergistic effectbetween stroke severity and kidney dysfunction on mortality. The
ore and eGFR.
P for trend
5e29 <15
vents P-M aHR Events P-M aHR
4 987 2.61 (1.33e5.11) 5 480 1.86 (0.57e6.00) 0.0283 741 3.09 (1.53e6.23) 10 363 5.19 (2.42e11.16) <0.00016 357 11.3 (6.33e20.17) 18 171 19.1 (10.01e36.45) <0.00010.0002 0.0012
rular filtration rate; P-M, person-months; aHR, adjusted hazard ratio.
hemic heart disease, smoking, alcohol consumption and previous stroke.this subgroup.

S.-J. Yeh et al. / Atherosclerosis 239 (2015) 328e334 333
group with both eGFR <15 mL/min/1.73 m2 and NIHSS score >15had the highest hazard ratio for mortality. This synergistic effect onmortality highlights the importance of screening acute ischemicstroke patients early in order to identify kidney dysfunction. Earlyidentification of CKD may facilitate early initiation of kidney-protection strategies, such as optimal control of blood glucoseand blood pressure, or blockade of renin-angiotensin-aldosteronesystem [30,31]. Besides, the choice of antiplatelet agents inischemic stroke patients with CKD may influence the thrombotictendency and CKD course. For example, phosphodiesterase in-hibitors may offer better platelet inhibition and restore endothelialdysfunction in CKD patients, while aspirin may accelerate CKDdeterioration [32].
There are several limitations to the present study. First, we didnot seek to assess the causes of mortality due to lack of this infor-mation in the registration data. Second, serum creatinine levelswere only determined at the time of admission; therefore, wewereunable to differentiate the chronicity of kidney dysfunction. Third,this observational study provided no evidence for a causal mech-anism underlying the effect of low eGFR on worsening stroke out-comes. Forth, the rate of lost to follow-up at 6-months in this studywas 35.3%. The follow-up group had slightly higher percentage ineGFR �60 mL/min/1.73 m2 (59.9% vs. 57.1%) and lower percentagein NIHSS<6 (49.9% vs. 53.0%) than the lost to follow-up group,which might influence the prognosis estimation of the LAA popu-lation. Fifth, the information on types of diabetes was unavailable inTSR, so we were unable to analyze our data by diabetic type. Sixth,the percentages of missing data for comorbidities in this studyranged from 0 to 7.3%, which might influence the interpretation forthe distribution of comorbidities (especially dyslipidemia) indifferent eGFR subgroups. Finally, TSR data did not include infor-mation related to the extent of proteinuria, which may have led toan underestimation in the percentage of patients with kidneydysfunction.
In conclusion, low eGFR level at the time of admission wasshown to be significantly associated with poor outcomes in the LAAsubtype of acute ischemic stroke. The relationship between loweGFR level and stroke mortality was further exacerbated by asynergistic interaction between kidney dysfunction and strokeseverity. When treating patients with acute ischemic stroke of theLAA subtype, close attention should be paid to eGFR levels. Iden-tifying CKD in patients with ischemic stroke may facilitate earlyinitiation of kidney-protection strategies to prevent deteriorationof CKD and poor outcomes.
Competing interests
The authors declare that they have no competing interests.
Acknowledgments
This project was funded by the Bureau of Health Promotion,Department of Health Taiwan Stroke Registry grant (DOH-95e98-HP-1102); Taiwan Ministry of Health and Welfare Clinical Trialand Research Center of Excellence (Grant Numbers MOHW103-TDU-B-212-113002); Academia Sinica, Biosignature(BM102021169), National Taiwan University Hospital grants (103-2544 and 104-2871), Tseng-Lien Lin Foundation, Taichung, Taiwanand Katsuzo and Kiyo Aoshima Memorial Funds.
Appendix A. Supplementary data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.atherosclerosis.2015.01.038.
References
[1] M.S. Elkind, Epidemiology and risk factors, Continuum 17 (2011) 1213e1232.[2] V. Jha, G. Garcia-Garcia, K. Iseki, Z. Li, S. Naicker, B. Plattner, et al., Chronic
kidney disease: global dimension and perspectives, Lancet 382 (2013)260e272.
[3] M.J. Holzmann, A. Aastveit, N. Hammar, I. Jungner, G. Walldius, I. Holme, Renaldysfunction increases the risk of ischemic and hemorrhagic stroke in thegeneral population, Ann. Med. 44 (2012) 607e615.
[4] R.T. Gansevoort, R. Correa-Rotter, B.R. Hemmelgarn, T.H. Jafar, H.J. Heerspink,J.F. Mann, et al., Chronic kidney disease and cardiovascular risk: epidemiology,mechanisms, and prevention, Lancet 382 (2013) 339e352.
[5] X. Wang, Y. Luo, Y. Wang, C. Wang, X. Zhao, D. Wang, , et al.China NationalStroke Registry Investigators, Comparison of associations of outcomes afterstroke with estimated GFR using Chinese modifications of the MDRD studyand CKD-EPI creatinine equations: results from the China National StrokeRegistry, Am. J. Kidney Dis. 63 (2014) 59e67.
[6] M. Lee, J.L. Saver, K.H. Chang, H.W. Liao, S.C. Chang, B. Ovbiagele, Lowglomerular filtration rate and risk of stroke: meta-analysis, BMJ 341 (2010)c4249.
[7] G. Yahalom, R. Schwartz, Y. Schwammenthal, O. Merzeliak, M. Toashi,D. Orion, et al., Chronic kidney disease and clinical outcome in patients withacute stroke, Stroke 40 (2009) 1296e1303.
[8] S. Zoungas, S. Ristevski, P. Lightfoot, Y.L. Liang, P. Branley, L.M. Shiel, et al.,Carotid artery intima-medial thickness is increased in chronic renal failure,Clin. Exp. Pharmacol. Physiol. 27 (2000) 639e641.
[9] K. Amann, R. Neususs, E. Ritz, T. Irzyniec, G. Wiest, G. Mall, Changes of vasculararchitecture independent of blood pressure in experimental uremia, Am. J.Hypertens. 8 (1995) 409e417.
[10] J. Pelisek, I.N. Hahntow, H.H. Eckstein, S. Ockert, C. Reeps, P. Heider, et al.,Impact of chronic kidney disease on carotid plaque vulnerability, J. Vasc. Surg.54 (2011) 1643e1649.
[11] Y. Tsukamoto, W. Takahashi, S. Takizawa, S. Kawada, S. Takagi, Chronic kidneydisease in patients with ischemic stroke, J. Stroke Cerebrovasc. Dis. 21 (2012)547e550.
[12] Y. Luo, X. Wang, Y. Wang, C. Wang, H. Wang, D. Wang, , et al.CNSR In-vestigators, Association of glomerular filtration rate with outcomes of acutestroke in type 2 diabetic patients: results from the China National StrokeRegistry, Diabetes Care 37 (2014) 173e179.
[13] J. Putaala, E. Haapaniemi, D. Gordin, R. Liebkind, P.H. Groop, M. Kaste, et al.,Factors associated with impaired kidney function and its impact on long-termoutcome in young ischemic stroke, Stroke 42 (2011) 2459e2464.
[14] Y. Kumai, M. Kamouchi, J. Hata, T. Ago, J. Kitayama, H. Nakane, , et al.FSRInvestigators, Proteinuria and clinical outcomes after ischemic stroke,Neurology 78 (2012) 1909e1915.
[15] Z. Hao, B. Wu, S. Lin, F.Y. Kong, W.D. Tao, D.R. Wang, et al., Association be-tween renal function and clinical outcome in patients with acute stroke, Eur.Neurol. 63 (2010) 237e242.
[16] K.S. Wong, H. Li, Long-term mortality and recurrent stroke risk among Chi-nese stroke patients with predominant intracranial atherosclerosis, Stroke 34(2003) 2361e2366.
[17] J.F. Arenillas, C.A. Molina, J. Montaner, S. Abilleira, M.A. Gonz�alez-S�anchez,J. Alvarez-Sabín, Progression and clinical recurrence of symptomatic middlecerebral artery stenosis: a long-term follow-up transcranial Doppler ultra-sound study, Stroke 32 (2001) 2898e2904.
[18] F.I. Hsieh, L.M. Lien, S.T. Chen, C.H. Bai, M.C. Sun, H.P. Tseng, et al., Get with theguidelines-stroke performance indicators: surveillance of stroke care in thetaiwan stroke registry: get with the guidelines-stroke in taiwan, Circulation122 (2010) 1116e1123.
[19] S. Hatano, Experience from a multicentre stroke register: a preliminary report,Bull. World Health Organ. 54 (1976) 541e553.
[20] H.P.J. Adams, R.F. Woolson, J. Biller, W. Clarke, Studies of Org 10172 in patientswith acute ischemic stroke. TOAST study Group, Haemostasis 22 (1992)99e103.
[21] A.S. Levey, L.A. Stevens, C.H. Schmid, Y.L. Zhang, A.F. Castro 3rd, H.I. Feldman,et al., CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration), A newequation to estimate glomerular filtration rate, Ann. Intern Med. 150 (2009)604e612.
[22] National Kidney Foundation, K/DOQI clinical practice guidelines for bonemetabolism and disease in chronic kidney disease, Am. J. Kidney Dis. 42(2003) S1eS201.
[23] Y. Kokubo, Carotid atherosclerosis in kidney disease, Contrib. Nephrol. 179(2013) 35e41.
[24] A. Recio-Mayoral, D. Banerjee, C. Streather, J.C. Kaski, Endothelial dysfunction,inflammation and atherosclerosis in chronic kidney diseaseea cross-sectionalstudy of predialysis, dialysis and kidney-transplantation patients, Athero-sclerosis 216 (2011) 446e451.
[25] W.E. Moody, N.C. Edwards, M. Madhani, C.D. Chue, R.P. Steeds, C.J. Ferro, et al.,Endothelial dysfunction and cardiovascular disease in early-stage chronickidney disease: cause or association? Atherosclerosis 223 (2012) 86e94.
[26] M. Rogers, C. Goettsch, E. Aikawa, Medial and intimal calcification in chronickidney disease: stressing the contributions, J. Am. Heart Assoc. 2 (2013)e000481.
[27] J.G. Lee, K.B. Lee, I.M. Jang, H. Roh, M.Y. Ahn, H.Y. Woo, et al., Low glomerular
S.-J. Yeh et al. / Atherosclerosis 239 (2015) 328e334334
filtration rate increases hemorrhagic transformation in acute ischemic stroke,Cerebrovasc. Dis. 35 (2013) 53e59.
[28] D. Bernaudo, R. Coll, J.F. S�anchez Mu~noz-Torrero, M.T. Pascual, A.M. García-Díaz, L.R. Alvarez, , et al.FRENA Investigators, Renal function and short-termoutcome in stable outpatients with coronary, cerebrovascular or peripheralartery disease, Atherosclerosis 229 (2013) 258e262.
[29] B. Ovbiagele, Chronic kidney disease and risk of death during hospitalizationfor stroke, J. Neurol. Sci. 301 (2011) 46e50.
[30] J. Lv, P. Ehteshami, M.J. Sarnak, H. Tighiouart, M. Jun, T. Ninomiya, et al., Effectsof intensive blood pressure lowering on the progression of chronic kidneydisease: a systematic review and meta-analysis, CMAJ 185 (2013) 949e957.
[31] L. Tylicki, S. Lizakowski, B. Rutkowski, Renin-angiotensin-aldosterone systemblockade for nephroprotection: current evidence and future directions,J. Nephrol. 25 (2012) 900e910.
[32] S.J. Kim, O.Y. Bang, Antiplatelet therapy for preventing stroke in patients withchronic kidney disease, Contrib. Nephrol. 179 (2013) 119e129.
Copyright © 2022 FDOKUMEN