
Benefits and Harms of Doxycycline Treatment for Gulf War Veterans' Illnesses
Upload
independentCategory
view
4download
0
http://adr.sagepub.com/Advances in Dental Research
http://adr.sagepub.com/content/12/1/32The online version of this article can be found at:
DOI: 10.1177/08959374980120011601
1998 12: 32ADRJ.G. Thomas, R.J. Metheny, J.M. Karakiozis, J.M. Wetzel and R.J. Crout
Periodontitis: Effects on Subgingival Bacterial Population DynamicsLong-Term Sub-Antimicrobial Doxycycline (Periostat®) as Adjunctive Management in Adult
Published by:
http://www.sagepublications.com
On behalf of:
International and American Associations for Dental Research
can be found at:Advances in Dental ResearchAdditional services and information for
http://adr.sagepub.com/cgi/alertsEmail Alerts:
http://adr.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
by guest on July 13, 2011 For personal use only. No other uses without permission.adr.sagepub.comDownloaded from

LONG-TERM SUB-ANTIMICROBIAL DOXYCYCLINE(PERIOSTAT®) AS ADJUNCTIVE MANAGEMENT
IN ADULT PERIODONTITIS: EFFECTS ONSUBGINGIVAL BACTERIAL POPULATION DYNAMICS
J.G. THOMAS*
R.J. METHENY
J.M. KARAKIOZIS
J.M. WETZEL
R.J. CROUT
Departments of Pathology and Periodontics, West VirginiaUniversity, Robert C. Byrd HSC-North, Morgantown, WestVirginia 26506-9203; Corresponding author
Adv Dent Res 12:32-39, November, 1998
Abstract—Previous trials had indicated that variousschedules of sub-antimicrobial doxycycline significantlyreduced gingival crevicular fluid (GCF) collagenase activityin adult patients with periodontitis with no evidence ofemergent tetracycline-resistant (Tcr) marker oral flora. Thepurpose of this nine-month study was to expand theseobservations, emphasizing newer microbial diagnosticmethods. Subgingival paper point samples were obtained atbaseline (BL), 3, 6, and 9 months. Four subject treatmentgroups in a double-blind design were evaluated bymechanical scaling and root planing (SRP) and/or 20 mgdoxycycline BID (Periostat®). Thirty-eight patients enteredthe study at baseline (BL). Dark-field microscopy on 260samples showed that morphotype distribution wasindependent of treatment schedule. Culture analysis of the 3most prevalent isolates recovered showed that Streptococcusand Prevotella species accounted for approximately 85% ofthe 724 cultures. There did not appear to be any overgrowthor replacement by opportunistic oral flora. Of 658susceptibility patterns evaluated by Etest, the MIC50/90 andmode MIC showed stable patterns, independent of treatmentgroup. Our findings were different from those of previouslypublished reports, but may be partly explained by the lack ofuniversally standardized methods in oral microbiology andinterpretive criteria for susceptibility testing.
Key words: Periodontal disease, microbiology, putativepathogens, sub-antimicrobial, susceptibility testing.
Presented at the Workshop on the "Non-AntibioticProperties of Tetracyclines", held November 13-14, 1997, inGarden City, New York, sponsored by the Long Island JewishMedical Center, CollaGenex Pharmaceuticals, Inc., and theNational Institute of Dental Research (NIH).
Periodontal disease is described as a disruption of thesymbiotic and heterogeneous ecosystem (Marsh,1994; Socransky and Haffajee, 1997), resulting in animbalance favoring the selection of certain putative
periopathogens (Thomas and Walker, 1996). Golub et al.(1983) were the first to report that tetracyclines (Tcs)inhibited the mature collagenases by a mechanismindependent of the antimicrobial properties of theseantibiotics. He and others (Golub et al., 1990; Crout andSchroeder, 1992; Thomas et al, 1995; Caton et al, 1997)subsequently evaluated the impact of the Tcs in periodontaldisease on selected marker organisms. Their preliminarystudies found that at sub-antimicrobial doses or low-dosedoxycycline (LDD), there was a dramatic reduction in hostcollagenase, elastase, and (3-glucuronidase withoutconcomitant changes in the subgingival flora or pathogensresistant to Tcs (Tcr). However, this was not withoutcontroversy. Other investigators, using a variety of differentculture and molecular techniques, found changes in the oralflora and development of simultaneous antibiotic resistancewhen evaluating therapeutic concentrations of doxycycline(Haffajee et al, 1995; Olsvik et al, 1995; Edlund et al,1996; Magnusson and Lindhe, 1996). It was the purpose ofthis study to evaluate further long-term, sub-antimicrobialdoxycycline (Periostat®) as an adjunct in the management ofadult periodontitis by measuring expanded biologicalmarkers of the subgingival flora. This included: (1)measuring the bacterial load and microbial flora compositionas a component of "colonization resistance"; (2) replacementor overgrowth of Staphylococcus aureus, enteric species, oryeast; and (3) changes in resistant patterns to 6 antibiotics,measuring drift, shift, and multi-drug resistance.
MATERIALS and METHODS
Thirty-eight subjects were entered at baseline (BL) and wererandomly assigned to receive 20 mg BID doxycycline(Periostat®) or a placebo. Subjects were medically screenedand selected for periodontal pocket depths of > 5 mm but < 9mm. Each subject, regardless of assigned Group (A,B,C,D)received a scaling and root planing (SRP) in two quadrantson one side of the mouth (split mouth), while the oppositeside was left unsealed. Hence, there were 4 potentialmanagements provided (1-4): (1) Periostat® and SRP, (2)Periostat® alone, (3) placebo and SRP, and (4) placebo alone.The microbial analyses were performed without theinvestigators knowing which subject group (A,B,C,D)
32 by guest on July 13, 2011 For personal use only. No other uses without permission.adr.sagepub.comDownloaded from
VOL. 12 DOXYCYCLINE IMPACT ON PERIODONTAL BACTERIA 33
Incubation Conditions Species
3-5 days, aerobic, 37°C
3-5 days, 5% CO,, 37°C
5-7 days, anaerobic, 37°C
corresponded to whichtreatment group (1,2,3,4).However, it was knownthat Group A was pairedwith Group C and GroupB with Group D. Sampleswere collected at baseline(BL), 3, 6, and 9 monthsfor each patient.
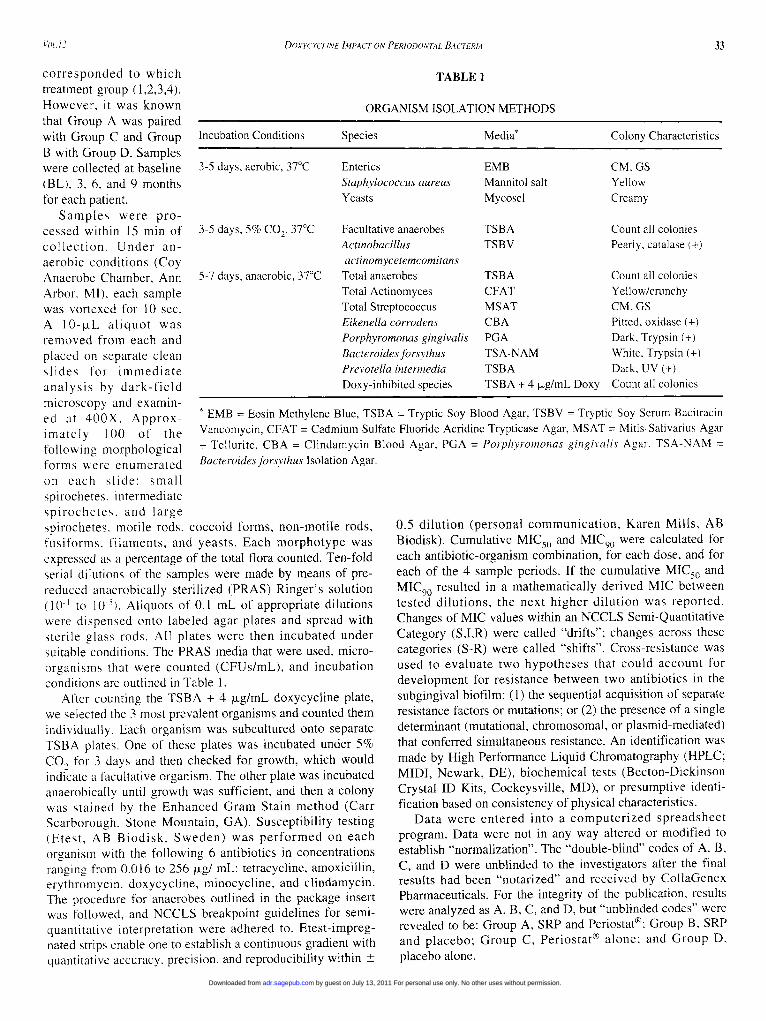
Samples were pro-cessed within 15 min ofcollection. Under an-aerobic conditions (CoyAnaerobe Chamber, AnnArbor, MI), each samplewas vortexed for 10 sec.A 10-jxL aliquot wasremoved from each andplaced on separate cleanslides for immediateanalysis by dark-fieldmicroscopy and examin-ed at 400X. Approx-imately 100 of thefollowing morphologicalforms were enumeratedon each slide: smallspirochetes, intermediatespirochetes, and largespirochetes. motile rods, coccoid forms, non-motile rods,fusiforms, filaments, and yeasts. Each morphotype wasexpressed as a percentage of the total flora counted. Ten-foldserial dilutions of the samples were made by means of pre-reduced anaerobically sterilized (PRAS) Ringer's solution(10"1 to 10~\). Aliquots of 0.1 mL of appropriate dilutionswere dispensed onto labeled agar plates and spread withsterile glass rods. All plates were then incubated undersuitable conditions. The PRAS media that were used, micro-organisms that were counted (CFUs/mL), and incubationconditions are outlined in Table 1.
After counting the TSBA + 4 |xg/mL doxycycline plate,we selected the 3 most prevalent organisms and counted themindividually. Each organism was subcultured onto separateTSBA plates. One of these plates was incubated under 5%CO2 for 3 days and then checked for growth, which wouldindicate a facultative organism. The other plate was incubatedanaerobically until growth was sufficient, and then a colonywas stained by the Enhanced Gram Stain method (CarrScarborough, Stone Mountain, GA). Susceptibility testing(Etest, AB Biodisk, Sweden) was performed on eachorganism with the following 6 antibiotics in concentrationsranging from 0.016 to 256 \xg/ mL: tetracycline, amoxicillin,erythromycin, doxycycline, minocycline, and clindamycin.The procedure for anaerobes outlined in the package insertwas followed, and NCCLS breakpoint guidelines for semi-quantitative interpretation were adhered to. Etest-impreg-nated strips enable one to establish a continuous gradient withquantitative accuracy, precision, and reproducibility within ±
TABLE 1
ORGANISM ISOLATION METHODS
Media* Colony Characteristics
EntericsStaphylococcus aureusYeasts
Facultative anaerobesActinobacillusactinomycetemcomitans
Total anaerobesTotal ActinomycesTotal StreptococcusEikenella corrodensPorphyromonas gingivalisBacteroides forsythusPrevotella intermediaDoxy-inhibited species
EMBMannitol saltMycosel
TSBATSBV
TSBACFATMSATCBAPGATSA-NAMTSBATSBA + 4 jjig/mL Doxy
CM,GSYellowCreamy
Count all coloniesPearly, catalase (+)
Count all coloniesYellow/crunchyCM, GSPitted, oxidase (+)Dark, Trypsin (+)White, Trypsin (+)Dark, UV (+)Count all colonies
* EMB = Eosin Methylene Blue, TSBA = Tryptic Soy Blood Agar, TSBV = Tryptic Soy Serum BacitracinVancomycin, CFAT = Cadmium Sulfate Fluoride Acridine Trypticase Agar, MSAT = Mitis-Salivarius Agar+ Tellurite, CBA = Clindamycin Blood Agar, PGA = Porphyromonas gingivalis Agar. TSA-NAM =Bacteroides forsythus Isolation Agar.
0.5 dilution (personal communication, Karen Mills, ABBiodisk). Cumulative MIC50 and MIC90 were calculated foreach antibiotic-organism combination, for each dose, and foreach of the 4 sample periods. If the cumulative MIC50 andMIC90 resulted in a mathematically derived MIC betweentested dilutions, the next higher dilution was reported.Changes of MIC values within an NCCLS Semi-QuantitativeCategory (S,I,R) were called "drifts"; changes across thesecategories (S-R) were called "shifts". Cross-resistance wasused to evaluate two hypotheses that could account fordevelopment for resistance between two antibiotics in thesubgingival biofilm: (1) the sequential acquisition of separateresistance factors or mutations; or (2) the presence of a singledeterminant (mutational, chromosomal, or plasmid-mediated)that conferred simultaneous resistance. An identification wasmade by High Performance Liquid Chromatography (HPLC;MIDI, Newark, DE), biochemical tests (Becton-DickinsonCrystal ID Kits, Cockeysville, MD), or presumptive identi-fication based on consistency of physical characteristics.
Data were entered into a computerized spreadsheetprogram. Data were not in any way altered or modified toestablish "normalization". The "double-blind" codes of A, B,C, and D were unblinded to the investigators after the finalresults had been "notarized" and received by CollaGenexPharmaceuticals. For the integrity of the publication, resultswere analyzed as A, B, C, and D, but "unblinded codes" wererevealed to be: Group A, SRP and Periostat®; Group B, SRPand placebo; Group C, Periostat® alone; and Group D,placebo alone.
by guest on July 13, 2011 For personal use only. No other uses without permission.adr.sagepub.comDownloaded from

34 THOMAS ET AL. ADV DENT RES NOVEMBER 1998
TABLE 2
STUDY SUMMARY
Study Parameters
Total # of patientsDrop-outs*Exits**Total # of Patients per
treatment group:A&C pairedB&D paired
Total # of patient samples(@ 2 samples/patient)
Maximum # isolates(@ 3 isolates/sampleor 6 isolates/patient)
Total # organisms isolatedTotal # organisms identifiedTotal # susceptibility tests
performed (Etests)
Baseline
3800
1820
76
228
225211
183
3 Months
3261
1517
64
192
177177
163
6 Months
3101
1516
62
186
178178
166
9 Months
2910
1415
58
174
164156
146
* Left study** Left study with culture at exit.
RESULTS and DISCUSSION
Of the 38 patients initially enrolled in the study (BL), 32were cultured at 3 months, 31 at 6 months, and 29 at 9months. The N value was the total samples for each periodrather than individual patients (Table 2). Because the 3 mostfrequent organisms were identified per sample, there was a
MEAN PERCENT SPIROCHETE DISTRIBUTION BY DARKFIELD MICROSCOPY
50%
45%
A B
6Months
Fig. 1—Mean percent distribution of small, intermediate, large, and totalspirochetal morphotypes analyzed by dark-field microscopy.
maximum number of isolates for eachof the sample periods of 228 results atBL, 192 at 3 mos, 186 at 6 mos, and174 at 9 mos. All organisms were notcultivable, nor could they all beidentified by either HPLC or theCrystal ID System. This was notsurprising, since anaerobes do loseviability, even under the most stringentof anaerobic maintenance. They mayfail to thrive upon continued subculturewhen removed from the symbioticecosystem, where biosynergy is atrademark of the subgingival biofilm orplaque.
Significantly, no single group(A,B,C,D), paired groups (A+C orB+D), or any sample period (BL, 3, 6,and 9 mos) showed a marked decreasein organism recovery or species identi-fication. There was an overall decrease,from 211 species recovered andidentified at BL to 156 at 9 mos. Thisreflected a decrease in patientparticipation, from 38 patients at BL to29 at 9 mos. To account for drop-outand exit patients, we expressed resultsas a percentage of the N value. There
was a grand total of 260 samples, resulting in 744 recoveredand 724 identified to species level, of which 658 gaveinterpretable MIC results for 6 different antibiotics.
Fig. 1 shows results of dark-field microscopy listing meanpercent distribution of small, intermediate, large, and totalspirochetes. Dark-field microscopy was performed because
there is no routine cultivablemethodology for spirochetes. In ourstudy, the largest number of all 3spirochete morphotypes was observedat Baseline. Over time, the distributiondecreased slightly, with the largestchange occurring between BL and 3mos. Generally, large spirochetesrepresented the smallest numbers ofspirochetes, while intermediate andsmall spirochetes remained stable forthree-, six-, and nine-month samples.Spirochetes comprised approximatelyhalf of the 9 dark-field morphotypes atBL to less than one-quarter at 9 mos.These trends were uninfluenced bytreatment category, either singularly(A,B,C,D) or paired (A+C vs. B+D).
We calculated the percent of totalplaque population inhibited by 4 |xgdoxycycline/mL by dividing the totaldoxycycline count (CFU's/mL) by thetotal anaerobic count (CFU's/mL).Total number of samples screened was
TOTAL % OF SP
LARGE SP
INTERMEDIATE SP
SMALL SP
by guest on July 13, 2011 For personal use only. No other uses without permission.adr.sagepub.comDownloaded from

VOL.12DOXYCYCLINE IMPACT ON PERIODONTAL BACTERIA
35
30.00%
25.00%
20.00%
15.00%
10.00%
5.00%
0.00%
260, with 76 samples at baseline, 64 samples at 3mos, 62 samples at 6 mos, and 58 samples at 9mos (Table 1). Both mean and median werecalculated for % inhibition, with the latter beingshown in Fig. 2. All 4 treatment groups showedessentially parallel median inhibitions. Thehighest percentage of doxycycline inhibition wasat 9 mos, when there were 5 out of 164recovered isolates whose calculated inhibitionwas greater than 100%. These "outliers"increased from 0 at BL to 1 at 3 mos, 3 at 6 mos,and 5 at 9 mos. The organisms recovered inthese patients were Gram-positive morphotypes,historically known to be resistant to Tcs. In allcases, the outliers were never > 100% inhibitionfor the paired samples. Most outliers wererecovered from treatment group A and its pair C.Of the 9 total outliers, 4 were group A and 3were C. Interestingly, A and C showed similarvalues and parallel changes when compared withB and D.
It is also interesting to note that of theorganisms originally recovered in mixed cultureon 4 |xg/mL doxycycline per mL, a portion lostthat capability and reported MICs to doxycyclineof < 4 |xg/mL in pure culture. As an example, ofthe 9 outliers, all had MICs < 4 |xg/mL when sub-cultured—hence the idea that indirect testing ofplaque samples, destroying the symbioticenvironment, does influence the reportedresistance of the population as a whole.
Fig. 3 highlights mean percentages ofmorphotypes recovered from the doxycyclineplates that were Gram-positive cocci (GPC), Gram-negativerods (GNR), Gram-positive rods (GPR), Gram-negative cocci(GNC), and yeasts, according totreatment group and sampleperiod. A total of 724 organismswas analyzed, 211 at BL, 177 at3 mos, 178 at 6 mos, and 158 at9 mos. The most prevalentisolates were GPC followed byGNR, which together constituteabout 85% of the morphotypesrecovered. Although generallystable, there was a suggestionthat the GPC increased slightly(49-61%), while GNR decreased15% between 6 and 9 mos.
We also analyzed individualspecies for each morphotype tocompare the most prevalentspecies by treatment group andsample period, and to unmaskany trend that would be evidentwhen all species werecatalogued. Several observationsheld true for treatment groups
Median Percent Inhibition of Organisms
Baseline
3 MONTHS
6 MONTHS
9 MONTHS
Fig 2—Median percent inhibition of organisms (CFU's) isolated frommedia containing 4 /xg/mL of doxycycline relative to total anaerobic count.
(single or paired) and for all sample periods. There was noevidence of organism selection or of any selective
MEAN PERCENT GRAM STAIN MORPHOLOGY - BY TREATMENT GROUPS
Gram Positive Cocci
am Negative Rods
Gram Positive Rods
Gram Negative Cocci
fig, j _ Comparative distribution of mean percent Gram-stain morphotypes.
by guest on July 13, 2011 For personal use only. No other uses without permission.adr.sagepub.comDownloaded from
36 THOMAS ET AL. ADV DENT RES NOVEMBER 1998
DOCYCLINE MIC INTERPRETATIONS
80%
70%
10%
0°/c
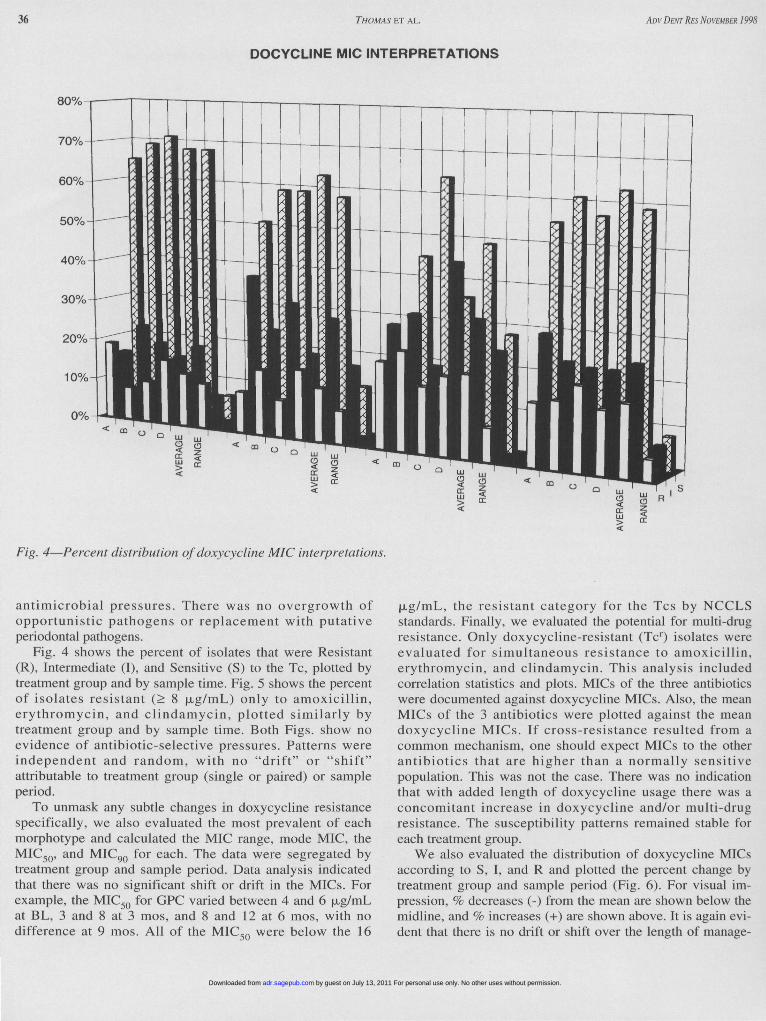
Fig. 4—Percent distribution of doxycycline MIC interpretations.
antimicrobial pressures. There was no overgrowth ofopportunistic pathogens or replacement with putativeperiodontal pathogens.
Fig. 4 shows the percent of isolates that were Resistant(R), Intermediate (I), and Sensitive (S) to the Tc, plotted bytreatment group and by sample time. Fig. 5 shows the percentof isolates resistant (> 8 |xg/mL) only to amoxicillin,erythromycin, and clindamycin, plotted similarly bytreatment group and by sample time. Both Figs, show noevidence of antibiotic-selective pressures. Patterns wereindependent and random, with no "drift" or "shift"attributable to treatment group (single or paired) or sampleperiod.
To unmask any subtle changes in doxycycline resistancespecifically, we also evaluated the most prevalent of eachmorphotype and calculated the MIC range, mode MIC, theMIC50, and MIC90 for each. The data were segregated bytreatment group and sample period. Data analysis indicatedthat there was no significant shift or drift in the MICs. Forexample, the MIC50 for GPC varied between 4 and 6 jjig/mLat BL, 3 and 8 at 3 mos, and 8 and 12 at 6 mos, with nodifference at 9 mos. All of the MIC50 were below the 16
(xg/mL, the resistant category for the Tcs by NCCLSstandards. Finally, we evaluated the potential for multi-drugresistance. Only doxycycline-resistant (Tcr) isolates wereevaluated for simultaneous resistance to amoxicillin,erythromycin, and clindamycin. This analysis includedcorrelation statistics and plots. MICs of the three antibioticswere documented against doxycycline MICs. Also, the meanMICs of the 3 antibiotics were plotted against the meandoxycycline MICs. If cross-resistance resulted from acommon mechanism, one should expect MICs to the otherantibiotics that are higher than a normally sensitivepopulation. This was not the case. There was no indicationthat with added length of doxycycline usage there was aconcomitant increase in doxycycline and/or multi-drugresistance. The susceptibility patterns remained stable foreach treatment group.
We also evaluated the distribution of doxycycline MICsaccording to S, I, and R and plotted the percent change bytreatment group and sample period (Fig. 6). For visual im-pression, % decreases (-) from the mean are shown below themidline, and % increases (+) are shown above. It is again evi-dent that there is no drift or shift over the length of manage-
by guest on July 13, 2011 For personal use only. No other uses without permission.adr.sagepub.comDownloaded from

VOL. 12 DOXYCYCLINE IMPACT ON PER1ODONTAL BACTERIA 37
PERCENT OF ISOLATES WITH MIC >8mg/ml FOR LISTED ANTIBIOTICS
35%
30%
25%
15%
10%
0%
BASELINE ^ D
3 MONTHS
6 MONTHS
B9 MONTHS
' ERYTHROMYCIN" CLINDAMYCIN
' AMOXICILLIN
Fig. 5—Percent distribution of isolates with resistant MICs (> 8 /xg/mL)for amoxicillin, clindamycin, and erythromycin.
PERCENT CHANGE IN DOXYCYCLINE MIC INTERPRETATION
Fig. 6—Percent change in doxycyclinc MIC interpretation.
by guest on July 13, 2011 For personal use only. No other uses without permission.adr.sagepub.comDownloaded from
38 THOMAS ET AL. ADV DENT RES NOVEMBER 1998
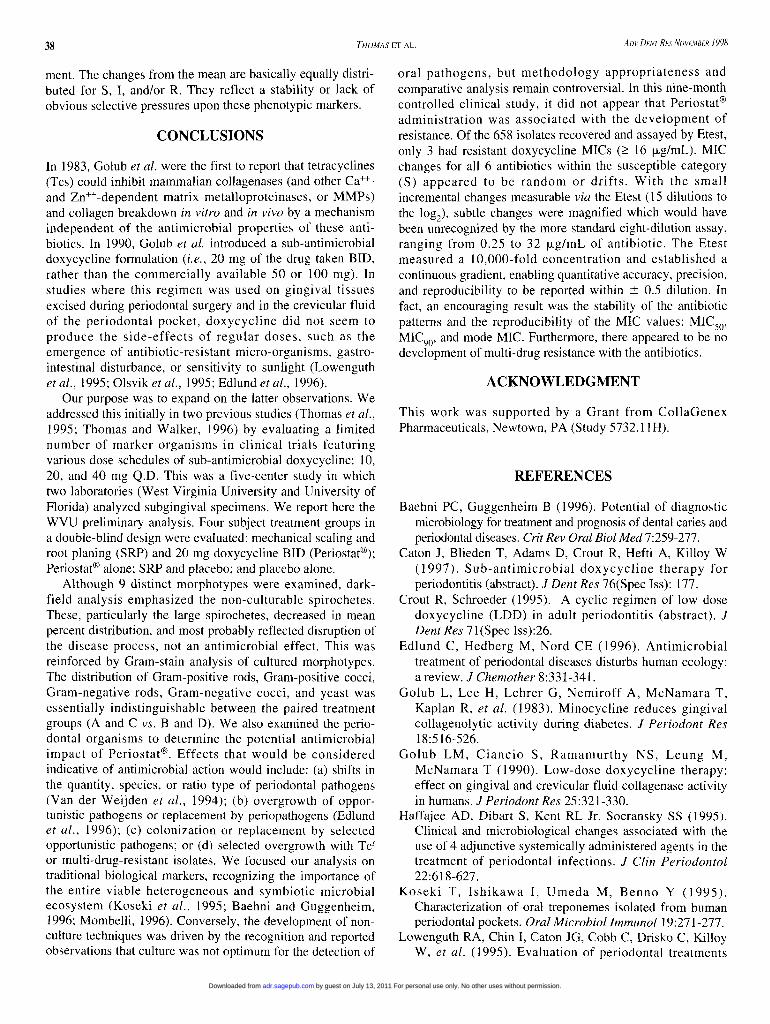
ment. The changes from the mean are basically equally distri-buted for S, I, and/or R. They reflect a stability or lack ofobvious selective pressures upon these phenotypic markers.
CONCLUSIONS
In 1983, Golub et al. were the first to report that tetracyclines(Tcs) could inhibit mammalian collagenases (and other Ca++-and Zn++-dependent matrix metalloproteinases, or MMPs)and collagen breakdown in vitro and in vivo by a mechanismindependent of the antimicrobial properties of these anti-biotics. In 1990, Golub et al. introduced a sub-antimicrobialdoxycycline formulation (i.e., 20 mg of the drug taken BID,rather than the commercially available 50 or 100 mg). Instudies where this regimen was used on gingival tissuesexcised during periodontal surgery and in the crevicular fluidof the periodontal pocket, doxycycline did not seem toproduce the side-effects of regular doses, such as theemergence of antibiotic-resistant micro-organisms, gastro-intestinal disturbance, or sensitivity to sunlight (Lowenguthet al, 1995; Olsvik et al, 1995; Edlund et al, 1996).
Our purpose was to expand on the latter observations. Weaddressed this initially in two previous studies (Thomas et al,1995; Thomas and Walker, 1996) by evaluating a limitednumber of marker organisms in clinical trials featuringvarious dose schedules of sub-antimicrobial doxycycline: 10,20, and 40 mg Q.D. This was a five-center study in whichtwo laboratories (West Virginia University and University ofFlorida) analyzed subgingival specimens. We report here theWVU preliminary analysis. Four subject treatment groups ina double-blind design were evaluated: mechanical scaling androot planing (SRP) and 20 mg doxycycline BID (Periostat®);Periostat® alone; SRP and placebo; and placebo alone.
Although 9 distinct morphotypes were examined, dark-field analysis emphasized the non-culturable spirochetes.These, particularly the large spirochetes, decreased in meanpercent distribution, and most probably reflected disruption ofthe disease process, not an antimicrobial effect. This wasreinforced by Gram-stain analysis of cultured morphotypes.The distribution of Gram-positive rods, Gram-positive cocci,Gram-negative rods, Gram-negative cocci, and yeast wasessentially indistinguishable between the paired treatmentgroups (A and C vs. B and D). We also examined the perio-dontal organisms to determine the potential antimicrobialimpact of Periostat®. Effects that would be consideredindicative of antimicrobial action would include: (a) shifts inthe quantity, species, or ratio type of periodontal pathogens(Van der Weijden et al, 1994); (b) overgrowth of oppor-tunistic pathogens or replacement by periopathogens (Edlundet al, 1996); (c) colonization or replacement by selectedopportunistic pathogens; or (d) selected overgrowth with Tcr
or multi-drug-resistant isolates. We focused our analysis ontraditional biological markers, recognizing the importance ofthe entire viable heterogeneous and symbiotic microbialecosystem (Koseki et al, 1995; Baehni and Guggenheim,1996; Mombelli, 1996). Conversely, the development of non-culture techniques was driven by the recognition and reportedobservations that culture was not optimum for the detection of
oral pathogens, but methodology appropriateness andcomparative analysis remain controversial. In this nine-monthcontrolled clinical study, it did not appear that Periostat®administration was associated with the development ofresistance. Of the 658 isolates recovered and assayed by Etest,only 3 had resistant doxycycline MICs (> 16 |jLg/mL). MICchanges for all 6 antibiotics within the susceptible category(S) appeared to be random or drifts. With the smallincremental changes measurable via the Etest (15 dilutions tothe log2), subtle changes were magnified which would havebeen unrecognized by the more standard eight-dilution assay,ranging from 0.25 to 32 (jug/mL of antibiotic. The Etestmeasured a 10,000-fold concentration and established acontinuous gradient, enabling quantitative accuracy, precision,and reproducibility to be reported within ± 0.5 dilution. Infact, an encouraging result was the stability of the antibioticpatterns and the reproducibility of the MIC values: MIC50,MIC90, and mode MIC. Furthermore, there appeared to be nodevelopment of multi-drug resistance with the antibiotics.
ACKNOWLEDGMENT
This work was supported by a Grant from CollaGenexPharmaceuticals, Newtown, PA (Study 5732.11H).
REFERENCES
Baehni PC, Guggenheim B (1996). Potential of diagnosticmicrobiology for treatment and prognosis of dental caries andperiodontal diseases. Crit Rev Oral Biol Med 7:259-277.
Caton J, Blieden T, Adams D, Crout R, Hefti A, Killoy W(1997). Sub-antimicrobial doxycycline therapy forperiodontitis (abstract). J Dent Res 76(Spec Iss): 177.
Crout R, Schroeder (1995). A cyclic regimen of low dosedoxycycline (LDD) in adult periodontitis (abstract). JDent Res 71(Spec Iss):26.
Edlund C, Hedberg M, Nord CE (1996). Antimicrobialtreatment of periodontal diseases disturbs human ecology:a review. / Chemother 8:331-341.
Golub L, Lee H, Lehrer G, Nemiroff A, McNamara T,Kaplan R, et al. (1983). Minocycline reduces gingivalcollagenolytic activity during diabetes. J Periodont Res18:516-526.
Golub LM, Ciancio S, Ramamurthy NS, Leung M,McNamara T (1990). Low-dose doxycycline therapy:effect on gingival and crevicular fluid collagenase activityin humans. J Periodont Res 25:321-330.
Haffajee AD, Dibart S, Kent RL Jr, Socransky SS (1995).Clinical and microbiological changes associated with theuse of 4 adjunctive systemically administered agents in thetreatment of periodontal infections. J Clin Periodontol22:618-627.
Koseki T, Ishikawa I, Umeda M, Benno Y (1995).Characterization of oral treponemes isolated from humanperiodontal pockets. Oral Microbiol Immunol 19:271-277.
Lowenguth RA, Chin I, Caton JG, Cobb C, Drisko C, KilloyW, et al (1995). Evaluation of periodontal treatments
by guest on July 13, 2011 For personal use only. No other uses without permission.adr.sagepub.comDownloaded from

VOL. 12 DOXYCYCLINE IMPACT ON PERIODONTAL BACTERIA 39
using controlled release tetracycline fibers:microbiological response. J Periodontol 66:700-707.
Magnusson I, Lindhe J (1996). Current concepts in diagnosisand treatment of periodontitis. Sem Orthod 2(l):13-20.
Marsh PD (1994). Microbial ecology of dental plaque and itssignificance in health and disease. Adv Dent Res 8:263-271.
Mombelli A (1996). Microbiological monitoring. J ClinPeriodontol 23(3 Pt 2):251-257.
Olsvik B, Hansen BF, Tenover FC, Olsen I (1995).Tetracycline-resistant micro-organisms recovered frompatients with refractory periodontal disease. J ClinPeriodontol 22:391-396.
Socransky SS, Haffajee AD (1997). The nature of periodontal
diseases. Ann Periodontol 2(l):3-10.Thomas J, Walker C (1996). Impact of bacterial antibiotic
resistance on oral health: what is the relevance? (abstract).Seattle, WA: University of Washington, Department ofPathobiology, September 3-5.
Thomas J, Crout RJ, Crout RM, et al. (1995). Antibioticresistance evaluation with low dose doxycycline (LDD) inadult periodontitis (abstract). J Dent Res 74(Spec Iss):575.
Van der Weijden GA, Timmerman MF, Reijerse E, WolffeGN, Van Winkelhoff AJ, Van der Velden U (1994). Theprevalence of A. actinomycetemcomitans, P. gingivalis,and P. intermedia in selected subjects with periodontitis. JClin Periodontol 21:583-588.
by guest on July 13, 2011 For personal use only. No other uses without permission.adr.sagepub.comDownloaded from
Copyright © 2022 FDOKUMEN




















