
The Efficacy and Safety of Aripiprazole as Adjunctive Therapy in Major Depressive Disorder: A...
10
The Efficacy and Safety of Aripiprazole as Adjunctive Therapy in Major Depressive Disorder A Second Multicenter, Randomized, Double-Blind, Placebo-Controlled Study Ronald N. Marcus, MD,* Robert D. McQuade, PhD, y William H. Carson, MD, y Delphine Hennicken, MS, z Maurizio Fava, MD, x Jeffrey S. Simon, MD, k Madhukar H. Trivedi, MD, { Michael E. Thase, MD,** and Robert M. Berman, MD* Abstract: Nonresponse to one or more antidepressants is common and an important public health problem. This study evaluated the efficacy and safety of adjunctive aripiprazole or placebo to standard antidepressant therapy (ADT) in patients with major depressive disorder who showed an inadequate response to at least 1 and up to 3 historical and 1 additional prospective ADT. The study comprised a 7–28-day screening, an 8-week prospective treatment, and a 6-week randomization phase. During prospective treatment, patients experiencing a major depressive episode (17-item Hamilton Rating Scale for Depression total score Q18) received single-blind adjunc- tive placebo plus clinicians’ choice of ADT (escitalopram, fluox- etine, paroxetine controlled-release, sertraline, or venlafaxine extended-release). Subjects with inadequate response were random- ized to adjunctive placebo (n = 190) or adjunctive aripiprazole (n = 191) (starting dose 5 mg/d, dose adjustments 2–20 mg/d, mean end- point dose of 11.0 mg/d). The primary efficacy endpoint was the mean change in Montgomery-A ˚ sberg Depression Rating Scale total score from end of prospective treatment phase to end of randomized treatment phase (last observation carried forward). Mean change in Montgomery-A ˚ sberg Depression Rating Scale total score was significantly greater with adjunctive aripiprazole than placebo (j8.5 vs j5.7; P = 0.001). Remission rates were significantly greater with adjunctive aripiprazole than placebo (25.4% vs 15.2%; P = 0.016) as were response rates (32.4% vs 17.4%; P < 0.001). Adverse events occurring in 10% of patients or more with adjunctive placebo or aripiprazole were akathisia (4.2% vs 25.9%), headache (10.5% vs 9.0%), and fatigue (3.7% vs 10.1%). Incidence of adverse events leading to discontinuation was low (adjunctive placebo [1.1%] vs adjunctive aripiprazole [3.7%]). Aripiprazole is an effective and safe adjunctive therapy as demonstrated in this short-term study for patients who are nonresponsive to standard ADT. (J Clin Psychopharmacol 2008;28:156–165) N onresponse to antidepressant therapy (ADT) is a common occurrence in clinical practice and a major public health challenge, with up to 60% of patients not achieving adequate response following ADT. 1 A range of augmentation and combination strategies has been used in an attempt to improve outcomes in patients who show an inadequate antidepressant response or to increase the chance of achieving remission. 2 In particular, atypical antipsychotics are being increasingly used as adjunctive agents in clinical practice, although randomized controlled trials with olanzapine/ fluoxetine combination 3,4 or risperidone/citalopram combina- tion 5 have yielded mixed results. Aripiprazole is pharmacologically distinct from other antipsychotics acting as a partial agonist at dopamine D 2 ,D 3 , and serotonin 5-HT 1A receptors and as an antagonist at 5-HT 2A receptors. 6–9 This profile provides a pharmacological rationale for the use of aripiprazole in depression, as activity at these receptors is shared by several agents that have demon- strated efficacy as adjunctive therapy in clinical trials. 10 Several open-label studies have previously reported the efficacy of adjunctive aripiprazole in patients with treatment- resistant depression 11–13 and partial response to ADT, 14–16 providing empirical support for the efficacy of adjunctive aripiprazole in the treatment of depression. The study reported here is the second of 2 identical, large, multicenter, randomized, double-blind, placebo-controlled trials compar- ing the efficacy, safety, and tolerability of aripiprazole with placebo as an adjunctive treatment to ADT in patients who have demonstrated an inadequate response to a prospective 8-week trial of the same antidepressant agent and at least 1 historical ADT trial. The first of these has recently been published and showed that adjunctive aripiprazole was Original Contribution Journal of Clinical Psychopharmacology Volume 28, Number 2, April 2008 156 *Bristol-Myers Squibb, Wallingford, CT; yOtsuka Pharmaceutical Develop- ment & Commercialization, Inc, Princeton, NJ; zBristol-Myers Squibb, Braine-l’Alleud, Belgium; xDepression Clinical and Research Program, Massachusetts General Hospital, Boston, MA; kNorthbrooke Research Center, Brown Deer, WI; {The University of Texas Southwestern Medical Center, Dallas, TX; and **Department of Psychiatry, University of Pittsburgh Medical Center, University of Pennsylvania School of Medicine, and the Philadelphia Veterans Affairs Medical Center, Pennsylvania, PA. Received August 29, 2007; accepted after revision January 7, 2008. This study was supported by Bristol-Myers Squibb (Princeton, NJ) and Otsuka Pharmaceutical Co, Ltd (Tokyo, Japan). Editorial support for the preparation of this manuscript was provided by Michelle O’Donovan, PhD, Ogilvy Healthworld Medical Education (London, UK); funding was provided by Bristol-Myers Squibb. Address correspondence and reprint requests to Robert M. Berman, MD, Bristol-Myers Squibb, 5 Research Parkway, Wallingford, CT 06492. E-mail: [email protected]. Copyright * 2008 by Lippincott Williams & Wilkins ISSN: 0271-0749/08/2802-0156 DOI: 10.1097/JCP.0b013e3181677489 Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
-
Upload
iiserbhopal -
Category
Documents
-
view
2 -
download
0
Transcript of The Efficacy and Safety of Aripiprazole as Adjunctive Therapy in Major Depressive Disorder: A...

The Efficacy and Safety of Aripiprazole as AdjunctiveTherapy in Major Depressive Disorder
A Second Multicenter, Randomized, Double-Blind,Placebo-Controlled Study
Ronald N. Marcus, MD,* Robert D. McQuade, PhD,y William H. Carson, MD,yDelphine Hennicken, MS,z Maurizio Fava, MD,x Jeffrey S. Simon, MD,k Madhukar H. Trivedi, MD,{
Michael E. Thase, MD,** and Robert M. Berman, MD*
Abstract: Nonresponse to one or more antidepressants is common
and an important public health problem. This study evaluated the
efficacy and safety of adjunctive aripiprazole or placebo to standard
antidepressant therapy (ADT) in patients with major depressive
disorder who showed an inadequate response to at least 1 and up to
3 historical and 1 additional prospective ADT. The study comprised
a 7–28-day screening, an 8-week prospective treatment, and a
6-week randomization phase. During prospective treatment, patients
experiencing a major depressive episode (17-item Hamilton Rating
Scale for Depression total score Q18) received single-blind adjunc-
tive placebo plus clinicians’ choice of ADT (escitalopram, fluox-
etine, paroxetine controlled-release, sertraline, or venlafaxine
extended-release). Subjects with inadequate response were random-
ized to adjunctive placebo (n = 190) or adjunctive aripiprazole (n =
191) (starting dose 5 mg/d, dose adjustments 2–20 mg/d, mean end-
point dose of 11.0 mg/d). The primary efficacy endpoint was the
mean change in Montgomery-Asberg Depression Rating Scale total
score from end of prospective treatment phase to end of randomized
treatment phase (last observation carried forward). Mean change in
Montgomery-Asberg Depression Rating Scale total score was
significantly greater with adjunctive aripiprazole than placebo
(j8.5 vs j5.7; P = 0.001). Remission rates were significantly
greater with adjunctive aripiprazole than placebo (25.4% vs 15.2%;
P = 0.016) as were response rates (32.4% vs 17.4%; P < 0.001).
Adverse events occurring in 10% of patients or more with adjunctive
placebo or aripiprazole were akathisia (4.2% vs 25.9%), headache
(10.5% vs 9.0%), and fatigue (3.7% vs 10.1%). Incidence of adverse
events leading to discontinuation was low (adjunctive placebo [1.1%]
vs adjunctive aripiprazole [3.7%]). Aripiprazole is an effective and
safe adjunctive therapy as demonstrated in this short-term study for
patients who are nonresponsive to standard ADT.
(J Clin Psychopharmacol 2008;28:156–165)
Nonresponse to antidepressant therapy (ADT) is a
common occurrence in clinical practice and a major
public health challenge, with up to 60% of patients not
achieving adequate response following ADT.1 A range of
augmentation and combination strategies has been used in an
attempt to improve outcomes in patients who show an
inadequate antidepressant response or to increase the chance
of achieving remission.2 In particular, atypical antipsychotics
are being increasingly used as adjunctive agents in clinical
practice, although randomized controlled trials with olanzapine/
fluoxetine combination3,4 or risperidone/citalopram combina-
tion5 have yielded mixed results.Aripiprazole is pharmacologically distinct from other
antipsychotics acting as a partial agonist at dopamine D2, D3,and serotonin 5-HT1A receptors and as an antagonist at5-HT2A receptors.6–9 This profile provides a pharmacologicalrationale for the use of aripiprazole in depression, as activity atthese receptors is shared by several agents that have demon-strated efficacy as adjunctive therapy in clinical trials.10
Several open-label studies have previously reported theefficacy of adjunctive aripiprazole in patients with treatment-resistant depression11–13 and partial response to ADT,14–16
providing empirical support for the efficacy of adjunctivearipiprazole in the treatment of depression. The studyreported here is the second of 2 identical, large, multicenter,randomized, double-blind, placebo-controlled trials compar-ing the efficacy, safety, and tolerability of aripiprazole withplacebo as an adjunctive treatment to ADT in patients whohave demonstrated an inadequate response to a prospective8-week trial of the same antidepressant agent and at least 1historical ADT trial. The first of these has recently beenpublished and showed that adjunctive aripiprazole was
Original Contribution
Journal of Clinical Psychopharmacology � Volume 28, Number 2, April 2008156
*Bristol-Myers Squibb, Wallingford, CT; yOtsuka Pharmaceutical Develop-ment & Commercialization, Inc, Princeton, NJ; zBristol-Myers Squibb,Braine-l’Alleud, Belgium; xDepression Clinical and Research Program,Massachusetts General Hospital, Boston, MA; kNorthbrooke ResearchCenter, Brown Deer, WI; {The University of Texas SouthwesternMedical Center, Dallas, TX; and **Department of Psychiatry, Universityof Pittsburgh Medical Center, University of Pennsylvania School ofMedicine, and the Philadelphia Veterans Affairs Medical Center,Pennsylvania, PA.
Received August 29, 2007; accepted after revision January 7, 2008.This study was supported by Bristol-Myers Squibb (Princeton, NJ) and
Otsuka Pharmaceutical Co, Ltd (Tokyo, Japan). Editorial support for thepreparation of this manuscript was provided by Michelle O’Donovan,PhD, Ogilvy Healthworld Medical Education (London, UK); funding wasprovided by Bristol-Myers Squibb.
Address correspondence and reprint requests to Robert M. Berman, MD,Bristol-Myers Squibb, 5 Research Parkway, Wallingford, CT 06492.E-mail: [email protected].
Copyright * 2008 by Lippincott Williams & WilkinsISSN: 0271-0749/08/2802-0156DOI: 10.1097/JCP.0b013e3181677489
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

significantly more effective than adjunctive placebo for theimprovement of depression symptoms and was relatively welltolerated.17
MATERIALS AND METHODSThe study was a multicenter, randomized, double-blind,
placebo-controlled trial conducted at 36 sites in the UnitedStates between September 2004 and December 2006. Theprotocol was approved by the ethics committee at each site,and the study was conducted in accordance with theDeclaration of Helsinki.
The study consisted of 3 phases. Patients first entereda 7–28-day screening phase, in which prohibited psy-chotropic medications (ADTs, benzodiazepines, and mosthypnotic agents) were discontinued. Those patients experi-encing a major depressive episode — including a totalscore of Q18 17-item Hamilton Rating Scale for Depression(HAM-D17) — then qualified for an 8-week prospectivetreatment phase. This phase was designed to establish thatpatients had an inadequate response to standard ADT beforebeing randomized to adjunctive aripiprazole or placebo.During this phase, all patients received single-blind (theinvestigator, but not the patient, knew of the treatmentassignment), adjunctive placebo, so patients were unaware ofthe transition into the randomization phase. In addition, allpatients received ADT in accordance with current productlabeling, targeting the following doses by the beginning of thefourth week: escitalopram (10 or 20 mg/d), fluoxetine (20 or40 mg/d), paroxetine controlled-release (37.5 or 50 mg/d),sertraline (100 or 150 mg/d), or venlafaxine extended-release(150 or 225 mg/d). Assignment of ADT was based oninvestigator assessment of clinical factors (eg, prior antide-pressant use, response, and tolerability), although use of anysingle ADT at a given site was limited to <40% of patients.Treatment response was defined as a Q50% reduction in theHAM-D17 total score from baseline to the end of theprospective treatment phase, a HAM-D17 total score of <14,or a Clinical Global Impression Improvement (CGI-I) score of<3. Patients who did not meet these response criteria wereeligible to enter a 6-week, randomized, double-blind phase(actual study visits weeks 8–14), in which participants wererandomized (1:1) to continue the same ADT (no dose adjust-ment was permitted) plus either adjunctive placebo oraripiprazole. Patients randomized to receive aripiprazolestarted with a dose of 5 mg/d, which could be decreased to2 mg/d if the original dose was not tolerated. The dose wasincreased to at least 10 mg/d if well tolerated. Investigatorscould also increase the dose by 5 mg/d once per week, to amaximum of 20 mg/d (15 mg/d for patients on fluoxetine orparoxetine, due to the associated cytochrome P450 2D6inhibition). No dose increases were allowed after the fourthweek of this phase (study Week 12), although dose reductionfor tolerability reasons was permitted at any visit.
All patients gave written informed consent to partic-ipate in the study. Patients eligible for inclusion wereoutpatients aged 18–65 years who met the Diagnostic andStatistical Manual of Mental Disorders, Fourth Edition—Text Revision criteria for a major depressive episode that
had lasted Q8 weeks. Patients were also required to havereported an inadequate response to previous ADT, asdetermined by the Antidepressant Treatment ResponseQuestionnaire.1 Specifically, inadequate response wasdefined as the patients’ reporting of <50% reduction inseverity of depression to at least 1 and no more than 3 ADTtrials of >6 weeks’ duration (>3 weeks for combinationtreatments) at the minimum acceptable dose specified in theAntidepressant Treatment Response Questionnaire (typicallyequal or greater than the minimal efficacious dose reflected inthe prescribing information). Patients who had a Q50%reduction in depressive symptoms after previous ADT couldalso qualify for inclusion if they had experienced <50%reduction in depressive symptoms relative to their last wellperiod and an inadequate response to a subsequent ADT. If apatient had only 1 adequate antidepressant trial in the currentepisode, they were not assigned that antidepressant in theprospective treatment phase. The exclusion criteria were thesame as those used in a previously reported study.17
During the 8-week prospective treatment phase,patients were seen weekly for the first 4 weeks and every 2weeks thereafter to assess efficacy and safety. Patients werethen assessed weekly for the 6-week duration of double-blindtreatment. The primary efficacy endpoint was the mean changefrom end of the prospective treatment phase to the end of therandomized, double-blind phase in the Montgomery-AsbergDepression Rating Scale (MADRS) total score.18 A key sec-ondary endpoint was the change in mean Sheehan DisabilityScale (SDS) scores during the randomized, double-blindphase.19 The SDS evaluates the extent to which depressioninterferes with work, family, and social life; each aspect isscored on a scale of 1–10, and a mean score of 1–10is generated from the individual items.19 Other secondaryefficacy measures included the CGI-I and CGI Severity ofIllness (CGI-S),20 the Inventory of Depressive Symptomatol-ogy Self-Report Scale (IDS-SR),21 and the Quick Inventoryof Depressive Symptoms Self-Report Scale (QIDS-SR).22
Safety was evaluated by monitoring of adverse events (AEs),body weight, vital signs, laboratory parameters, and 12-leadelectrocardiogram. In addition, extrapyramidal symptomsrating scale evaluations included changes in Simpson-AngusScale,23 the Abnormal Involuntary Movement Scale,24 andthe Barnes Akathisia Clinical Assessment.25 The self-reported Massachusetts General Hospital Sexual FunctioningInventory (SFI) Scale was also evaluated.26
The randomized sample comprised all patients whowererandomized in the double-blind treatment phase; the safetysample included those randomized patients who received atleast 1 dose of double-blind study medication; and the efficacysample included those patients in the safety sample who had atleast 1 post-randomization efficacy evaluation.
The primary efficacy outcome measure, mean changefrom the end of the prospective treatment phase (Week 8visit) to the end of the randomized, double-blind treatmentphase (Week 14 visit, last observation carried forward[LOCF]) in MADRS total score, was assessed by analysisof covariance, with end of prospective treatment phase scoreas covariate and treatment, and study center as main effects.All secondary outcome measures and safety analysis were
Journal of Clinical Psychopharmacology � Volume 28, Number 2, April 2008 Adjunctive Aripiprazole in Major Depression
* 2008 Lippincott Williams & Wilkins 157
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

conducted as previously described.17 All statistical tests areinterpreted at the 5% significance level.
RESULTSIn total, 1151 patients were screened, of whom 830
were eligible and entered the prospective treatment phase,and 651 patients completed this treatment phase (Fig. 1). Ofthese, 266 patients (41%) met the criteria for response(HAM-D17 improvement Q50%, HAM-D17 <14, or CGI-I<3) during the prospective ADT treatment and did notproceed to double-blind treatment. In total, 381 patients wererandomized to adjunctive placebo (n = 190) or adjunctivearipiprazole (n = 191) in the randomized, double-blindtreatment phase. The randomized, double-blind treatmentphase was completed by 85% of patients in both treatmentgroups, and the reasons for treatment discontinuation areshown in Figure 1.
The treatment groups were well balanced with respectto baseline demographics and disease characteristics(Table 1).
At randomization to double-blind treatment, the overalldistribution of specific ADTs was as follows: escitalopram,30.4%; venlafaxine extended-release, 28.1%; sertraline, 19.7%;fluoxetine, 14.7%; and paroxetine controlled-release, 7.1%.This was representative of the ADTs chosen overall duringthe initial prospective treatment phase, and there wasa similar distribution between the placebo and aripiprazoletreatment arms.
The mean dose of aripiprazole during the last weekof the randomized, double-blind treatment phase was 11.0mg/d and was similar between ADT groups, ranging from10.0 mg/d with fluoxetine to 11.7 mg/d with escitalopram.
For patients in the placebo group, the mean dose equivalentwas 15.3 mg/d.
Patients receiving adjunctive aripiprazole experienceda significantly greater improvement at endpoint in meanMADRS total score (j8.5) than those receiving adjunctiveplacebo (j5.7; P = 0.001) in the randomized, double-blindtreatment phase (Fig. 2). This provided a standardizedtreatment effect size of 0.35 in favor of aripiprazole. Thedifference between adjunctive aripiprazole and adjunctiveplacebo was significant from Week 1 of double-blind treat-ment (j3.7 vs j2.2; P = 0.007) with continued improvementthroughout the duration of treatment. As the MADRS totalscores showed a statistically significant treatment differencebetween the adjunctive placebo and adjunctive aripiprazoletreatment groups at the end of prospective treatment (double-blind baseline) (efficacy sample: 26.6 vs 24.6 respectively;P < 0.001), a sensitivity analysis was conducted to confirmthe validity of the primary efficacy findings. A significanttreatment difference was found in favor of aripiprazole,regardless of whether the model was adjusted for thedifference in baseline MADRS total scores.
Subgroup analyses of mean change in MADRS totalscore from the end of the prospective treatment phase to theend of double-blind treatment showed no statistically signifi-cant interaction effects for sex (P = 0.374), ADT (P = 0.526),age group (<37, e37 to <45, e45 to <53, and Q53 years;P = 0.718), or MADRS response at the end of the prospectivetreatment phase (<25% vs Q25% improvement in MADRStotal score from baseline; P = 0.960).
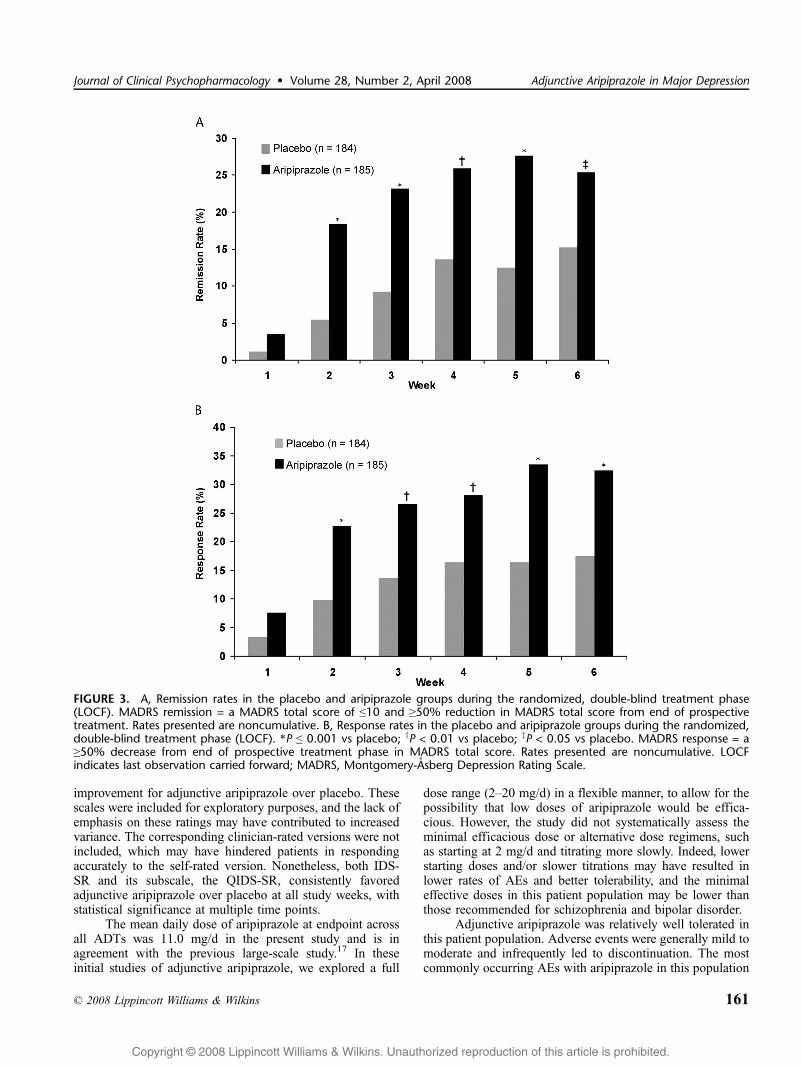
Compared with adjunctive placebo, adjunctive aripi-prazole also produced significantly greater remission ratesduring the double-blind treatment from week 2 through toendpoint (15.2% vs 25.4%; P = 0.016) (Fig. 3A), providing
FIGURE 1. Patient disposition.
Marcus and Associates Journal of Clinical Psychopharmacology � Volume 28, Number 2, April 2008
* 2008 Lippincott Williams & Wilkins158
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

a number needed-to-treat for remission of 10. Response,defined as Q50% reduction in MADRS total score, was alsoobserved in significantly more adjunctive aripiprazole-treated(32.4%) compared with the adjunctive placebo-treatedpatients (17.4%) at Week 6 (P < 0.001; Fig. 3B), providinga number needed to treat for response of 7.
The mean SDS total score— the key secondary outcomemeasure — improved significantly more with adjunctivearipiprazole than adjunctive placebo at endpoint (j1.3 vsj0.7; P = 0.012) (Fig. 4). Significant improvements overadjunctive placebo in social and family life score items wereobserved with adjunctive aripiprazole (Fig. 4). Differences inthe work/school score item numerically favored adjunctivearipiprazole over adjunctive placebo, although the differenceswere not statistically significant (P = 0.615).
Adjunctive aripiprazole also produced significantlygreater improvements from end of prospective treatmentfor the CGI-S scores (P < 0.001) and end-point CGI-I scores(P < 0.001) than adjunctive placebo (Table 2). Both showedstatistically significantly greater improvement from Week 1onwards (data not shown), confirming the findings on the
primary endpoint. Numerically greater improvements in IDS-SR and QIDS-SR were seen with adjunctive aripiprazole, butthese were not statistically significant at endpoint.
During the double-blind phase, 120 (63.2%) patientsin the placebo group and 154 (81.5%) patients in theadjunctive aripiprazole group experienced at least 1 AE.Adverse events occurring at an incidence Q5% in either groupare shown in Table 3. In the adjunctive aripiprazole group,AEs reported at an incidence of Q5% and at least twice that ofadjunctive placebo were akathisia (25.9% vs 4.2%), fatigue(10.1% vs 3.7%), restlessness (9.5% vs 0.5%), insomnia(7.4% vs 1.6%), tremor (6.3% vs 2.6%), and constipation(5.3% vs 2.6%). Only 1 serious AE occurred during therandomized, double-blind treatment phase (an event ofcellulitis in a patient receiving adjunctive aripiprazole thatwas deemed not to be related to study medication); nodeaths were reported. Discontinuation from double-blindtreatment because of AEs occurred in 2 patients (1.1%) inthe placebo group and 7 patients (3.7%) in the adjunctivearipiprazole group. Of the AEs occurring in Q5% ofpatients, only fatigue (2 patients), akathisia (2 patients),and restlessness (1 patient) led to discontinuation. Nosuicide-related AEs were reported with either adjunctivearipiprazole or placebo during the double-blind randomizedphase.
By the last study visit, continuing akathisia wasreported in 25 (51%) of the 49 patients who had everreported this symptom. Furthermore, the majority of akathisia(n = 38/49; 78%) was first reported during the first 3 weeksof treatment. Akathisia, at its maximum, was generally mild(n = 12/49; 25%) or moderate (n = 33/49; 67%) in severity,with few patients reporting akathisia as severe (n = 4/49;8%). For those subjects whose akathisia resolved during thestudy (n = 24), 58% (n = 14/24) received dose reduction, and42% (n = 10/24) received no interventions.
During the double-blind phase, minimal changes fromthe end of prospective treatment phase were seen at endpoint(LOCF) on the Simpson-Angus Scale total score (adjunctiveplacebo, 0.08; adjunctive aripiprazole, 0.42; P < 0.001),Abnormal Involuntary Movement Scale total score (adjunc-tive placebo, 0.04; adjunctive aripiprazole, 0.04; P = 0.986),and the Barnes Akathisia Rating Scale Global ClinicalAssessment of Akathisia score (adjunctive placebo, 0.02;adjunctive aripiprazole, 0.22; P = 0.002). The distribution ofBarnes Akathisia Rating Scale Global Clinical Assessmentof Akathisia scores in the adjunctive aripiprazole group atthe end of the double-blind treatment was similar to placebo(absent, 82% vs 90%; questionable, 10% vs 8%; mildakathisia, 5% vs 2%; moderate or marked akathisia, 3% vs1%; and severe akathisia, both 0%).
Analysis of mean weight change over the course ofdouble-blind treatment showed that the mean (SE) weight gainin the adjunctive aripiprazole group (1.47 T 0.16 kg) wassignificantly greater than the placebo group (0.42 T 0.17 kg;P < 0.001; LOCF). There was also a statistically significantdifference in the proportion of patients showing clinicallysignificant weight gain (Q7% from double-blind baseline;LOCF) (adjunctive placebo, 0%, vs adjunctive aripiprazole,3.4%; P = 0.031, Fisher exact test).
TABLE 1. Baseline Demographic and Disease Characteristics ofRandomized Patients
Characteristic Placebo Aripiprazole
Patients, n 190 191
Sex, n (%)
Male 62 (32.6) 65 (34.0)
Female 128 (67.4) 126 (66.0)
Age, mean (SD), yrs 44.4 (10.7) 44.6 (11.0)
Weight,* mean (SD), kg 87.7 (23.2) 86.5 (20.8)
BMI,* mean (SD), kg/m2 30.8 (7.5) 30.7 (7.4)
Race, n (%)
White 169 (88.9) 170 (89.0)
Black/African American 14 (7.4) 14 (7.3)
Asian 4 (2.1) 3 (1.6)
American Indian/Alaskan native 1 (0.5) 1 (0.5)
Native Hawaiian/other Pacific Islander 0 1 (0.5)
Other 2 (1.1) 2 (1.0)
Duration of current episode, mo
Mean (SD) 48.5 (88.8) 43.7 (68.0)
Median (range) 19.6 (2.1–678.8) 17.2 (2.5–430.4)
No. depressive episodes
Mean (SD) 7.3 (15.2) 6.3 (11.8)
Median (range) 3.0 (1.0–99.0) 3.0 (1.0–99.0)
No. adequate antidepressant trials in the current episode, n (%)
1 trial 128 (67.7) 135 (71.1)
2 trials 51 (27.0) 49 (25.8)
3 trials 10 (5.3) 5 (2.6)
4 trials 0 1 (0.5)
Single depressive episode, n (%) 34 (17.9) 32 (16.8)
MADRS total score,* mean (SD) 27.0 (5.5) 25.2 (6.2)
*Assessed at end of prospective treatment phase.
MADRS indicates Montgomery-Asberg Depression Rating Scale.
Journal of Clinical Psychopharmacology � Volume 28, Number 2, April 2008 Adjunctive Aripiprazole in Major Depression
* 2008 Lippincott Williams & Wilkins 159
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

There were no clinically meaningful differencesbetween adjunctive aripiprazole and adjunctive placebo invital signs, electrocardiographic findings, or laboratoryabnormalities.
During the double-blind randomization phase, there was astatistically significant treatment difference in favor of adjunc-tive aripiprazole over placebo on 2 SFI Scale items: interest insex (P < 0.001) and sexual satisfaction (P = 0.015). There wasno significant difference on the overall improvement score orother items of the scale. The mean baseline serum prolactinlevels for both placebo and aripiprazole groups were withinnormal serum levels at baseline and at the end of prospectivephase. A small reduction in prolactin levels was noted in theadjunctive aripiprazole group (median,j1.0 ng/mL) comparedwith no change in the adjunctive placebo group.
DISCUSSIONThis study shows that the addition of aripiprazole to
standard ADT is significantly more effective than placebo forthe improvement of depressive symptoms in patients withmajor depressive disorder who have failed to achieve anadequate response following at least 1 historic and 1 prospec-tive ADT during the current episode. This is the second study toconfirm the efficacy and safety of adjunctive aripiprazole in thetreatment of this patient population and further supports its useas a short-term augmentation strategy. In a clear replication ofthe positive findings of the first double-blind, placebo-controlled study,17 adjunctive aripiprazole was statisticallysignificantly superior to adjunctive placebo in the primaryendpoint (mean change in MADRS total score at week 6) andseveral key secondary endpoints. In both studies, onset ofactivity was found to be rapid, and continued improvementwas observed with adjunctive aripiprazole.
Adjunctive aripiprazole was associated with signifi-cantly higher remission rates than adjunctive placebo fromweek 2 onward. At endpoint, there was a 1.7-fold greaterlikelihood of remission with adjunctive aripiprazole thanplacebo; this clearly confirms the clinical relevance of thesefindings. Although there are inherent limitations to compar-isons across studies, the remission rates shown in this studycompare favorably with the STAR*D study, for which aremission rate of 20.5% was reported for patients at a similarstage of treatment as those in the present study (ie, level 3augmentation strategy in the 4-step treatment algorithm;previous treatment with 2 ADTs).27 The results of this studyare also consistent with smaller-scale, open-label or retro-spective studies of aripiprazole augmentation.11,12,14–16,28
As well as improvements seen on clinical outcomes,adjunctive aripiprazole was also significantly more effectivethan placebo for the improvement of disability associated withdepression, as measured using the SDS. The overall SDS datafrom both studies show a consistent and favorable impact ofaripiprazole treatment on functioning. Results from this and theprevious study17 show statistically significant improvement onthe family and social life items. These findings are important,given the known impact of residual symptoms on impairedpsychosocial functioning.29,30 Although improvements inwork/school functioning were not significant, 6 weeks maybe too short to detect improvement in this area. As there wasno statistically significant interaction effect for MADRSresponse at the end of the prospective treatment phase, thesedata suggest that both patients with partial response or thosewith nonresponse to ADT can benefit from augmentation.
Whereas clinician-rated scales and patient-ratings offunctioning both showed statistically significant differencesbetween treatment groups, the patient self-rated symptomscales (IDS-SR and QIDS-SR) failed to show a significant
FIGURE 2. Change in mean (TSE) MADRS total score during the randomized, double-blind treatment phase (LOCF). *P < 0.01 vsplacebo; yP e 0.001 vs placebo. Baseline MADRS total scores (end of prospective treatment phase): aripiprazole, 24.6; placebo,26.6 (P < 0.001). LOCF indicates last observation carried forward; MADRS, Montgomery-Asberg Depression Rating Scale; SE,standard error.
Marcus and Associates Journal of Clinical Psychopharmacology � Volume 28, Number 2, April 2008
* 2008 Lippincott Williams & Wilkins160
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
improvement for adjunctive aripiprazole over placebo. Thesescales were included for exploratory purposes, and the lack ofemphasis on these ratings may have contributed to increasedvariance. The corresponding clinician-rated versions were notincluded, which may have hindered patients in respondingaccurately to the self-rated version. Nonetheless, both IDS-SR and its subscale, the QIDS-SR, consistently favoredadjunctive aripiprazole over placebo at all study weeks, withstatistical significance at multiple time points.
The mean daily dose of aripiprazole at endpoint acrossall ADTs was 11.0 mg/d in the present study and is inagreement with the previous large-scale study.17 In theseinitial studies of adjunctive aripiprazole, we explored a full
dose range (2–20 mg/d) in a flexible manner, to allow for thepossibility that low doses of aripiprazole would be effica-cious. However, the study did not systematically assess theminimal efficacious dose or alternative dose regimens, suchas starting at 2 mg/d and titrating more slowly. Indeed, lowerstarting doses and/or slower titrations may have resulted inlower rates of AEs and better tolerability, and the minimaleffective doses in this patient population may be lower thanthose recommended for schizophrenia and bipolar disorder.
Adjunctive aripiprazole was relatively well tolerated inthis patient population. Adverse events were generally mild tomoderate and infrequently led to discontinuation. The mostcommonly occurring AEs with aripiprazole in this population
FIGURE 3. A, Remission rates in the placebo and aripiprazole groups during the randomized, double-blind treatment phase(LOCF). MADRS remission = a MADRS total score of e10 and Q50% reduction in MADRS total score from end of prospectivetreatment. Rates presented are noncumulative. B, Response rates in the placebo and aripiprazole groups during the randomized,double-blind treatment phase (LOCF). *P e 0.001 vs placebo; yP < 0.01 vs placebo; zP < 0.05 vs placebo. MADRS response = aQ50% decrease from end of prospective treatment phase in MADRS total score. Rates presented are noncumulative. LOCFindicates last observation carried forward; MADRS, Montgomery-Asberg Depression Rating Scale.
Journal of Clinical Psychopharmacology � Volume 28, Number 2, April 2008 Adjunctive Aripiprazole in Major Depression
* 2008 Lippincott Williams & Wilkins 161
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

were also generally similar to those reported previously witharipiprazole. Adjunctive aripiprazole was associated with ahigher rate of akathisia than placebo; however, only 2 patientsdiscontinued this study due to this AE, and only 1 patientdiscontinued in the previous study of a similar size.17 As alsoseen previously, akathisia was generally mild to moderate inseverity and resolved, often without intervention, before theend of the study for approximately half of the patients.
Treatment with adjunctive aripiprazole was associatedwith greater weight gain than adjunctive placebo duringthe 6-week treatment period, although clinically significantweight gain was seen in only 3% of patients. Weight gaincan be readily assessed clinically in the context of risk-
benefit management and should be proactively managed shouldit occur. While weight gain is not uncommon with atypicalaugmentation, the incidence observed in the current study witharipiprazole is similar to or less than that observed in similarstudies using risperidone or olanzapine augmentation.3–5
Adjunctive aripiprazole treatment did not confer anyadverse effects on sexual functioning as measured on the SFIScale and resulted in improvements in Binterest in sex[ andBsexual satisfaction[ items during the double-blind treatment.Adjunctive aripiprazole also had no adverse effects onprolactin levels. Taken together, these findings suggest thataripiprazole augmentation does not worsen any potential forhyperprolactinemia that has been suggested following treat-ment with selective serotonin reuptake inhibitors.31
Strengths of the current study include the large patientpopulation, the randomized and placebo-controlled study
FIGURE 4. Mean change in SDS scores from end of prospective treatment during the randomized, double-blind treatment phase(LOCF). *P e 0.05 vs placebo; yP e 0.01 vs placebo. LOCF indicates last observation carried forward; SDS, Sheehan Disability Scale.
TABLE 2. Mean (SE) Change* in Secondary Efficacy EndPointsin the Double-Blind, 6-Week Study (LOCF)
Rating ScalePlacebo(n = 184)
Aripiprazole(n = 185) P
CGI-S
Double-blind baseline 4.1 (0.04) 4.0 (0.04) 0.359
Change to Week 6 j0.6 (0.08) j1.1 (0.08) <0.001
End-point CGI-I score* 2.9 (0.08) 2.4 (0.08) <0.001
IDS-SR
Double-blind baseline 32.3 (0.94) 30.3 (0.93) 0.093
Change to Week 6 j4.6 (0.73) j6.0 (0.73) 0.126
QIDS-SR
Double-blind baseline 12.3 (0.36) 11.6 (0.36) 0.120
Change to Week 6 j1.8 (0.31) j2.3 (0.30) 0.213
*CGI-I is presented as the end-point mean score, not change from baseline.
CGI-I indicates Clinical Global Impression Improvement; CGI-S, CGI Severity of
Illness; IDS-SR, Inventory of Depressive Symptomatology Self-Report Scale; QIDS-
SR, Quick Inventory of Depressive Symptoms Self-Report Scale.
TABLE 3. Treatment-Emergent Adverse Events Occurring at anIncidence of Q5% in Either Treatment Group During theRandomized, Double-Blind Treatment Phase (Safety Sample)
Placebo (n = 190) Aripiprazole (n = 189)
Adverse Event n (%) n (%)
Akathisia 8 (4.2) 49 (25.9)
Fatigue 7 (3.7) 19 (10.1)
Restlessness 1 (0.5) 18 (9.5)
Headache 20 (10.5) 17 (9.0)
Insomnia 3 (1.6) 14 (7.4)
Somnolence 7 (3.7) 13 (6.9)
Tremor 5 (2.6) 12 (6.3)
Constipation 5 (2.6) 10 (5.3)
Nausea 8 (4.2) 10 (5.3)
Marcus and Associates Journal of Clinical Psychopharmacology � Volume 28, Number 2, April 2008
* 2008 Lippincott Williams & Wilkins162
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

design, and the use of historical ADT failure combined with arobust prospective treatment failure (8-week ADT treatmentat target doses above the minimal physician desk reference–recommended doses) in establishing antidepressant unrespon-siveness. Because of these design features, the findings fromthis study are eminently generalizable to routine clinicalpractice. Furthermore, the study used a number of methodo-logical innovations aimed at enhancing signal detection,avoiding study bias and focusing the study centers on goodstudy conduct. These included use of different entry (HAM-D17) and outcome (MADRS) severity scales; patient blindingto the point of randomization and site support to maintain thisblind; continuation of nonrandomized patients; use of feasibleentry criteria; intensive rater training requiring demonstration ofproficient interview techniques using simulated patients; ongoingevaluation of internal rating consistency by analysis of HAM-D17, MADRS, and IDS-SR scores; and frequent site contact andreview of protocol conduct. The reliability of results observedacross this study and the previously reported trial of identicaldesign17 suggest that these methodologies were successful.
Limitations include the fact that patients were notrandomized to ADT during prospective treatment and therelatively small sample sizes of patients assigned to each ADTregimen, which preclude evaluation of the effects of aripiprazoleaugmentation by ADT treatment assignment. In addition, thegeneral application of the findings is somewhat limited by theexclusion of patients who had failed >3 prior antidepressanttrials, as many patients in real-world practice may have receivedmore antidepressants than this. However, it should be noted thatthe antidepressant trials in this study were of adequate dosageand duration, which may not always be the case in real-worldpractice. Furthermore, the trial duration of 6 weeks does notallow for conclusions on the long-term benefit of aripiprazoleaugmentation on remission in this difficult-to-treat population;this remains to be established in further studies.
In summary, this study replicates previous findingsdemonstrating the efficacy of adjunctive aripiprazole as anaugmentation strategy to standard ADT therapy in patientswith a history of nonresponse to antidepressant medication.Given the public health challenge of antidepressant non-response, this is a significant clinical finding.
ACKNOWLEDGMENTSWe would like to thank all of the principal investigators
who participated in this study: Alison Baker MD, ClinicalNeuroscience Solutions Inc, Memphis, TN; Ari Kiev, MD,Social Psychiatry Research Institute, New York, NY; ArifullaKhan, MD, Northwest Clinical Research Center, Bellevue,WA; Boadie W. Dunlop, MD, Emory University, Departmentof Psychiatry & Behavioral Sciences, Atlanta, GA; CarolineM. Dupont, MD, Dupont Clinical Research, Rockville, MD;Charles Bailey, MD, Clinical Neuroscience Solutions Inc,Orlando, FL; Craig McCarthy, MD, Pivotal ResearchCenters, Mesa, AZ; David L. Dunner, MD, University ofWashington, Center for Anxiety & Depression, Seattle, WA;Dennis J. Munjack, MD, Southwestern Research Inc,Burbank, CA; G. Michael Dempsey, MD, AlbuquerqueNeuroscience Inc, Albuquerque, NM; Gary Gerard, MD,
Neurology & Neuroscience Center of Ohio, Toledo, OH;George Joseph, MD, Clinical Neuroscience Solutions Inc,Jacksonville, FL; Irish Crisanto, MD, Pacific ClinicalResearch Medical Group, Orange, CA; Jayesh Kamath,MD, PhD, University of Connecticut Health Center, Depart-ment of Psychiatry, Farmington, CT; Jeffrey S. Simon, MD,Northbrooke Research Center, Brown Deer, WI; Jerry C.Steiert, MD, Summit Research Network (Seattle) LLC,Seattle, WA; Joachim D. Raese, MD, Pacific ClinicalResearch Medical Group, Orange, CA; John J. Murphy,MD, Southwestern Research Inc, Beverly Hills, CA; Keith E.Saylor PhD, Neuroscience Inc, Herndon, VA; Lawrence D.Ginsberg, MD, Red Oak Psychiatry Associates, PA, Houston,TX; Leslie Moldauer, MD, Radiant Research, Denver, CO;Leslie Vh. Taylor, MD, Dean Foundation for Health,Research & Education, Middleton, WI; Louis C. Kirby II,MD, Pivotal Research Centers, Peoria, AZ; Madhukar H.Trivedi, MD, UT Southwestern Medical Center, Dallas, TX;Mary J. Stoller, MD, Pacific Clinical Research MedicalGroup, Orange, CA; Michael E. Thase, MD, WesternPsychiatric Institute and Clinic, Pittsburgh, PA; MohammedBari, MD, Synergy Clinical Research Center, National City,CA; Neil S. Dubin, MD, Patient Priority Clinical Sites LLC,Cincinnati, OH; Nicholas A. Demartinis, MD, University ofConnecticut Health Center, Department of Psychiatry, Farm-ington, CT; Nick Vatakis, MD, Social Psychiatry ResearchInstitute, Brooklyn, NY; Norman E. Rosenthal, MD, CapitalClinical Research Associates, Rockville, MD; Paul R. Miller,MD, Pacific Clinical Research Medical Group, Pasadena,CA; Philip T. Ninan, MD, Emory University, Department ofPsychiatry & Behavioral Sciences, Atlanta, GA; Ram K.Shrivastava, MD, Eastside Comprehensive Medical Center,New York, NY; Ramanath Gopalan, MD, ComprehensiveNeuroscience of Northern Virginia, Arlington, VA; RichardWilliam Brown, MD, Patient Priority Clinical Sites LLC,Cincinnati, OH; Robert B. Pohl, MD, Wayne State University,Psychiatric Center, Detroit, MI; Ronald R. Fieve, MD, FieveClinical Services Inc, New York, NY; Stephen Poland, MD,Hartford Research Group, Florence, KY; Susan G. Kornstein,MD, VCU Mood Disorders Institute, Richmond, VA; ValerieK. Arnold, MD, Clinical Neuroscience Solutions Inc,Memphis, TN; Ward T. Smith, MD, Summit Research Network(Oregon) Inc, Portland, OR.
AUTHOR DISCLOSURE INFORMATIONRobert M. Berman, Ronald N. Marcus, and Delphine
Hennicken are employees of Bristol-Myers Squibb. DrsBerman and Marcus are also Bristol-Myers Squibb share-holders. Robert D. McQuade and William H. Carson areemployees of Otsuka Pharmaceutical Development & Com-mercialization Inc. Robert D. McQuade is an ex-employeeof Bristol-Myers Squibb and is a Bristol-Myers Squibbshareholder.
Maurizio Fava receives research support from AbbottLaboratories, Alkermes, Aspect Medical Systems, Astra-Zeneca, Bristol-Myers Squibb, Cephalon, Eli Lilly & Co,Forest Pharmaceuticals Inc, GlaxoSmithkline, J&J Pharma-ceuticals, Lichtwer Pharma GmbH, Lorex Pharmaceuticals,
Journal of Clinical Psychopharmacology � Volume 28, Number 2, April 2008 Adjunctive Aripiprazole in Major Depression
* 2008 Lippincott Williams & Wilkins 163
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Novartis, Organon Inc, PamLab LLC, Pfizer Inc, Pharmavite,Roche, Sanofi/Synthelabo, Solvay Pharmaceuticals Inc,Wyeth-Ayerst Laboratories; is an advisor/consultant forAspect Medical Systems, AstraZeneca, Bayer AG, BestPractice Project Management Inc, Biovail PharmaceuticalsInc, BrainCells Inc, Bristol-Myers Squibb, Cephalon, Com-pellis, Cypress Pharmaceuticals, Dov Pharmaceuticals, EliLilly & Co, EPIX Pharmaceuticals, Fabre-Kramer Pharma-ceuticals Inc, Forest Pharmaceuticals Inc, GlaxoSmithkline,Grunenthal GmBH, Janssen Pharmaceutica, Jazz Pharma-ceuticals, J&J Pharmaceuticals, Knoll Pharmaceutical Co,Lundbeck, MedAvante Inc, Merck, Neuronetics, Novartis, Nu-trition 21, Organon Inc, PamLab LLC, Pfizer Inc, PharmaStar,Pharmavite, Roche, Sanofi/Synthelabo, Sepracor, SolvayPharmaceuticals Inc, Somaxon, Somerset Pharmaceuticals,Takeda, Wyeth-Ayerst Laboratories; participates in speakers’bureau for AstraZeneca, Boehringer-Ingelheim, Bristol-MyersSquibb, Cephalon, Eli Lilly & Co, Forest Pharmaceuticals Inc,GlaxoSmithkline, Novartis, Organon Inc, Pfizer Inc, Phar-maStar, Wyeth-Ayerst Laboratories; and has equity holdingswith Compellis, MedAvante.
Jeffrey S. Simon has been a consultant for Pfizer,Bristol-Meyers Squibb, Wyeth Research, Abbott, Tap, andCephalon. He has received research/grant support fromBristol-Meyers Squibb, Pfizer, Wyeth Research, Sanofi, Lilly,Cephalon, Forest, GlaxoSmithKline, Otsuka, AstraZeneca, andOrganon, and he is on the speakers’ bureau of Wyeth Re-search and GlaxoSmithKline.
Madhukar Trivedi has received research support from,or served as a consultant to, or has been on the speakers’boards of the following: Abdi Brahim; Abbott LaboratoriesInc; Akzo (Organon Pharmaceuticals Inc); AstraZeneca;Bayer; Bristol-Myers Squibb; Cephalon Inc; Corcept Ther-apeutics Inc; Cyberonics Inc; Eli Lilly & Co; Fabre KramerPharmaceuticals Inc; Forest Pharmaceuticals; Glaxo-SmithKline; Janssen Pharmaceutica Products, LP; Johnson& Johnson PRD; Meade Johnson; Merck; National Institute ofMental Health; National Alliance for Research in Schizophre-nia and Depression; Neuronetics; Novartis; Parke-DavisPharmaceuticals Inc; Pfizer Inc; Pharmacia & Upjohn;Predix Pharmaceuticals; Sepracor; Solvay PharmaceuticalsInc; VantagePoint; and Wyeth-Ayerst Laboratories.
Michael E. Thase is an advisor/consultant for: Astra-Zeneca, Bristol-Myers Squibb, Cephalon Inc, Cyberonics Inc,Eli Lilly & Co, GlaxoSmithKline; Janssen Pharmaceutica,MedAvante Inc, Neuronetics Inc, Novartis; Organon Inc,Sepracor Inc, Shire US Inc, and Wyeth Pharmacueticals. DrThase participates in speakers’ bureaus for AstraZeneca,Bristol-Myers Squibb, Cyberonics Inc, Eli Lilly & Co,GlazoSmithKline, Organon Inc, Sanofi Aventis, and WyethPharmacueticals. Dr Thase does not receive any grants frompharmaceutical companies. He has equity holdings inMedAvante Inc and receives income from royalties, patents,or other sources from American Psychiatric Publishing Inc,Guildford Publications, and Herald House.
REFERENCES1. Fava M. Diagnosis and definition of treatment-resistant depression. Biol
Psychiatry. 2003;53:649–659.
2. Fava M, Rush AJ. Current status of augmentation and combinationtreatments for major depressive disorder: a literature review and a pro-posal for a novel approach to improve practice. Psychother Psychosom.2006;75:139–153.
3. Thase ME, Corya SA, Osuntokun O, et al. A randomized, double-blindcomparison of olanzapine/fluoxetine combination, olanzapine, andfluoxetine in treatment-resistant major depressive disorder. J ClinPsychiatry. 2007;68:224–236.
4. Shelton RC, Williamson DJ, Corya SA, et al. Olanzapine/fluoxetinecombination for treatment-resistant depression: a controlled studyof SSRI and nortriptyline resistance. J Clin Psychiatry. 2005;66:1289–1297.
5. Rapaport MH, Gharabawi GM, Canuso CM, et al. Effects of risperidoneaugmentation in patients with treatment-resistant depression: results ofopen-label treatment followed by double-blind continuation. Neuropsy-chopharmacology. 2006;31:2505–2513.
6. Burris KD, Molski TF, Xu C, et al. Aripiprazole, a novel antipsychotic,is a high-affinity partial agonist at human dopamine D2 receptors.J Pharmacol Exp Ther. 2002;302:381–389.
7. Jordan S, Koprivica V, Chen R, et al. The antipsychotic aripiprazole is apotent, partial agonist at the human 5-HT(1A) receptor. Eur J Pharmacol.2002;441:137–140.
8. Shapiro DA, Renock S, Arrington E, et al. Aripiprazole, a novel atypicalantipsychotic drug with a unique and robust pharmacology. Neuro-psychopharmacology. 2003;28:1400–1411.
9. Stark AD, Jordan S, Allers KA, et al. Interaction of the novelantipsychotic aripiprazole with 5-HT(1A) and 5-HT(2A) receptors:functional receptor-binding and in vivo electrophysiological studies.Psychopharmacology (Berl). 2007;190:373–382.
10. Fava M. Augmentation and combination strategies in treatment-resistantdepression. J Clin Psychiatry. 2001;62(suppl 18):4–11.
11. Patkar AA, Peindl K, Mago R, et al. An open-label, rater-blinded,augmentation study of aripiprazole in treatment-resistant depression.Prim Care Companion J Clin Psychiatry. 2006;8:82–87.
12. Papakostas GI, Petersen TJ, Kinrys G, et al. Aripiprazole augmentationof selective serotonin reuptake inhibitors for treatment-resistant majordepressive disorder. J Clin Psychiatry. 2005;66:1326–1330.
13. Barbee JG, Conrad EJ, Jamhour NJ. Aripiprazole augmentation intreatment-resistant depression. Ann Clin Psychiatry. 2004;16:189–194.
14. Pae CU, Patkar AA, Jun TY, et al. Aripiprazole augmentation for treat-ment of patients with inadequate antidepressants response. DepressAnxiety. 2007;24:522–526.
15. Simon JS, Nemeroff CB. Aripiprazole augmentation of antidepres-sants for the treatment of partially responding and nonrespondingpatients with major depressive disorder. J Clin Psychiatry. 2005;66:1216–1220.
16. Worthington JJ 3rd, Kinrys G, Wygant LE, et al. Aripiprazole asan augmentor of selective serotonin reuptake inhibitors in depressionand anxiety disorder patients. Int Clin Psychopharmacol. 2005;20:9–11.
17. Berman RM, Marcus RN, Swanink R, et al. The efficacy and safety ofaripiprazole as adjunctive therapy in major depressive disorder: amulticenter, randomized, double-blind, placebo-controlled study. J ClinPsychiatry. 2007;68:843–853.
18. Montgomery SA, Asberg M. A new depression scale designed to besensitive to change. Br J Psychiatry. 1979;134:382–389.
19. Leon AC, Shear MK, Portera L, et al. Assessing impairment in patientswith panic disorder: the Sheehan Disability Scale. Soc PsychiatryPsychiatr Epidemiol. 1992;27:78–82.
20. Guy W. ECDEUAssessment Manual for Psychopharmacology—Revised.Rockville, MD: US Department of Health Services; 1976.
21. Rush AJ, Gullion CM, Basco MR, et al. The Inventory of DepressiveSymptomatology (IDS): psychometric properties. Psychol Med. 1996;26:477–486.
22. Rush A, Trivedi M, HM I. The 16-item Quick Inventory of DepressiveSymptomatology (QIDS), clinician rating (QIDS-C) and self-report(QIDS-SR16): a psychometric evaluation in patients with chronic majordepression. Biol Psychiatry Res. 2003;56:573–583.
23. Simpson GM, Angus JW. A rating scale for extrapyramidal side effects.Acta Psychiatr Scand Suppl. 1970;212:11–19.
24. Guy W. Abnormal Involuntary Movement Scale (AIMS). ECDEUAssessment Manual for Psychopharmacology. US Department of Health,
Marcus and Associates Journal of Clinical Psychopharmacology � Volume 28, Number 2, April 2008
* 2008 Lippincott Williams & Wilkins164
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Education, and Welfare publication (ADM) 76–338. Rockville, MD:National Institute of Mental Health; 1976:534–537.
25. Barnes TR. A rating scale for drug-induced akathisia. Br J Psychiatry.1989;154:672–676.
26. Labbate LA, Lare SB. Sexual dysfunction in male psychiatric out-patients: validity of the Massachusetts General Hospital Sexual Func-tioning Questionnaire. Psychother Psychosom. 2001;70:221–225.
27. Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-termoutcomes in depressed outpatients requiring one or several treatmentsteps: a STAR*D report. Am J Psychiatry. 2006;163:1905–1917.
28. Adson DE, Kushner MG, Fahnhorst TA. Treatment of residualanxiety symptoms with adjunctive aripiprazole in depressed patients
taking selective serotonin reuptake inhibitors. J Affect Disord. 2005;86:99–104.
29. Van Londen L, Molenaar RP, Goekoop JG, et al. Three- to 5-yearprospective follow-up of outcome in major depression. Psychol Med.1998;28:731–735.
30. Judd LL, Akiskal HS, Zeller PJ, et al. Psychosocial disability during thelong-term course of unipolar major depressive disorder. Arch GenPsychiatry. 2000;57:375–380.
31. Papakostas GI, Miller KK, Petersen T, et al. Serum prolactin levelsamong outpatients with major depressive disorder during the acutephase of treatment with fluoxetine. J Clin Psychiatry. 2006;67:952–957.
Journal of Clinical Psychopharmacology � Volume 28, Number 2, April 2008 Adjunctive Aripiprazole in Major Depression
* 2008 Lippincott Williams & Wilkins 165
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.




















