
Long-Term Safety and Efficacy of Percutaneous Coronary Intervention With Stenting and Coronary...
10
Long-Term Safety and Efficacy of Percutaneous Coronary Intervention With Stenting and Coronary Artery Bypass Surgery for Multivessel Coronary Artery Disease A Meta-Analysis With 5-Year Patient-Level Data From the ARTS, ERACI-II, MASS-II, and SoS Trials Joost Daemen, MD; Eric Boersma, PhD; Marcus Flather, MBBS; Jean Booth, MSc; Rod Stables, MA, DM, FRCP; Alfredo Rodriguez, MD; Gaston Rodriguez-Granillo, MD, PhD; Whady A. Hueb, MD; Pedro A. Lemos, MD, PhD; Patrick W. Serruys, MD, PhD Background—Randomized trials that studied clinical outcomes after percutaneous coronary intervention (PCI) with bare metal stenting versus coronary artery bypass grafting (CABG) are underpowered to properly assess safety end points like death, stroke, and myocardial infarction. Pooling data from randomized controlled trials increases the statistical power and allows better assessment of the treatment effect in high-risk subgroups. Methods and Results—We performed a pooled analysis of 3051 patients in 4 randomized trials evaluating the relative safety and efficacy of PCI with stenting and CABG at 5 years for the treatment of multivessel coronary artery disease. The primary end point was the composite end point of death, stroke, or myocardial infarction. The secondary end point was the occurrence of major adverse cardiac and cerebrovascular accidents, death, stroke, myocardial infarction, and repeat revascularization. We tested for heterogeneities in treatment effect in patient subgroups. At 5 years, the cumulative incidence of death, myocardial infarction, and stroke was similar in patients randomized to PCI with stenting versus CABG (16.7% versus 16.9%, respectively; hazard ratio, 1.04, 95% confidence interval, 0.86 to 1.27; P0.69). Repeat revascularization, however, occurred significantly more frequently after PCI than CABG (29.0% versus 7.9%, respectively; hazard ratio, 0.23; 95% confidence interval, 0.18 to 0.29; P0.001). Major adverse cardiac and cerebrovascular events were significantly higher in the PCI than the CABG group (39.2% versus 23.0%, respectively; hazard ratio, 0.53; 95% confidence interval, 0.45 to 0.61; P0.001). No heterogeneity of treatment effect was found in the subgroups, including diabetic patients and those presenting with 3-vessel disease. Conclusions—In this pooled analysis of 4 randomized trials, PCI with stenting was associated with a long-term safety profile similar to that of CABG. However, as a result of persistently lower repeat revascularization rates in the CABG patients, overall major adverse cardiac and cerebrovascular event rates were significantly lower in the CABG group at 5 years. (Circulation. 2008;118:1146-1154.) Key Words: bypass coronary disease prognosis stents surgery C oronary artery bypass grafting (CABG) has been con- sidered the gold standard for treating multivessel coro- nary artery disease, mainly because of its higher rate of complete revascularization, reflected by a lower need for repeat revascularizations compared with percutaneous coro- nary intervention (PCI). 1–4 Clinical Perspective p 1154 Whereas the risk difference of CABG versus balloon angioplasty for repeat revascularization in a large-scale meta- analysis proved to be 34% at 3 years, this difference de- creased to 15% when coronary stents were used. 1 In terms of clinical safety end points, the recently reported 5-year follow-up of the Arterial Revascularization Therapies Study (ARTS), 5 Argentine Randomized Trial of Coronary Angio- plasty With Stenting Versus Coronary Bypass Surgery in Patients With Multiple Vessel Disease (ERACI-II), 6 and the Medicine, Angioplasty or Surgery Study for Multi-Vessel Coronary Artery Disease (MASS-II) 7 reported no difference in death rates between the 2 revascularization strategies. Continuing medical education (CME) credit is available for this article. Go to http://cme.ahajournals.org to take the quiz. Received November 13, 2007; accepted June 30, 2008. From Thoraxcenter, Erasmus Medical Center, Rotterdam, the Netherlands (J.D., E.B., P.W.S.); Clinical Trials and Evaluation Unit, Royal Brompton Hospital, London, UK (M.F., J.B., R.S.); Otamendi Hospital, Buenos Aires, Argentina (A.R., G.R.-G.); and Heart Institute (InCor), University of São Paulo Medical School, São Paulo, Brazil (W.A.H., P.A.L.). Correspondence to Professor P.W. Serruys, MD, PhD, Thoraxcenter, Ba-583, Dr Molewaterplein 40, 3015 GD Rotterdam, Netherlands. E-mail [email protected] © 2008 American Heart Association, Inc. Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.107.752147 1146 by guest on January 6, 2015 http://circ.ahajournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Long-Term Safety and Efficacy of Percutaneous Coronary Intervention With Stenting and Coronary...

Long-Term Safety and Efficacy of Percutaneous CoronaryIntervention With Stenting and Coronary Artery Bypass
Surgery for Multivessel Coronary Artery DiseaseA Meta-Analysis With 5-Year Patient-Level Data From the ARTS,
ERACI-II, MASS-II, and SoS Trials
Joost Daemen, MD; Eric Boersma, PhD; Marcus Flather, MBBS; Jean Booth, MSc;Rod Stables, MA, DM, FRCP; Alfredo Rodriguez, MD; Gaston Rodriguez-Granillo, MD, PhD;
Whady A. Hueb, MD; Pedro A. Lemos, MD, PhD; Patrick W. Serruys, MD, PhD
Background—Randomized trials that studied clinical outcomes after percutaneous coronary intervention (PCI) with baremetal stenting versus coronary artery bypass grafting (CABG) are underpowered to properly assess safety end points likedeath, stroke, and myocardial infarction. Pooling data from randomized controlled trials increases the statistical powerand allows better assessment of the treatment effect in high-risk subgroups.
Methods and Results—We performed a pooled analysis of 3051 patients in 4 randomized trials evaluating the relativesafety and efficacy of PCI with stenting and CABG at 5 years for the treatment of multivessel coronary artery disease.The primary end point was the composite end point of death, stroke, or myocardial infarction. The secondary end pointwas the occurrence of major adverse cardiac and cerebrovascular accidents, death, stroke, myocardial infarction, andrepeat revascularization. We tested for heterogeneities in treatment effect in patient subgroups. At 5 years, thecumulative incidence of death, myocardial infarction, and stroke was similar in patients randomized to PCI with stentingversus CABG (16.7% versus 16.9%, respectively; hazard ratio, 1.04, 95% confidence interval, 0.86 to 1.27; P�0.69).Repeat revascularization, however, occurred significantly more frequently after PCI than CABG (29.0% versus 7.9%,respectively; hazard ratio, 0.23; 95% confidence interval, 0.18 to 0.29; P�0.001). Major adverse cardiac andcerebrovascular events were significantly higher in the PCI than the CABG group (39.2% versus 23.0%, respectively;hazard ratio, 0.53; 95% confidence interval, 0.45 to 0.61; P�0.001). No heterogeneity of treatment effect was found inthe subgroups, including diabetic patients and those presenting with 3-vessel disease.
Conclusions—In this pooled analysis of 4 randomized trials, PCI with stenting was associated with a long-term safetyprofile similar to that of CABG. However, as a result of persistently lower repeat revascularization rates in the CABGpatients, overall major adverse cardiac and cerebrovascular event rates were significantly lower in the CABG group at5 years. (Circulation. 2008;118:1146-1154.)
Key Words: bypass � coronary disease � prognosis � stents � surgery
Coronary artery bypass grafting (CABG) has been con-sidered the gold standard for treating multivessel coro-
nary artery disease, mainly because of its higher rate ofcomplete revascularization, reflected by a lower need forrepeat revascularizations compared with percutaneous coro-nary intervention (PCI).1–4
Clinical Perspective p 1154Whereas the risk difference of CABG versus balloon
angioplasty for repeat revascularization in a large-scale meta-
analysis proved to be 34% at 3 years, this difference de-creased to 15% when coronary stents were used.1 In terms ofclinical safety end points, the recently reported 5-yearfollow-up of the Arterial Revascularization Therapies Study(ARTS),5 Argentine Randomized Trial of Coronary Angio-plasty With Stenting Versus Coronary Bypass Surgery inPatients With Multiple Vessel Disease (ERACI-II),6 and theMedicine, Angioplasty or Surgery Study for Multi-VesselCoronary Artery Disease (MASS-II)7 reported no differencein death rates between the 2 revascularization strategies.
Continuing medical education (CME) credit is available for this article. Go to http://cme.ahajournals.org to take the quiz.Received November 13, 2007; accepted June 30, 2008.From Thoraxcenter, Erasmus Medical Center, Rotterdam, the Netherlands (J.D., E.B., P.W.S.); Clinical Trials and Evaluation Unit, Royal Brompton
Hospital, London, UK (M.F., J.B., R.S.); Otamendi Hospital, Buenos Aires, Argentina (A.R., G.R.-G.); and Heart Institute (InCor), University of SãoPaulo Medical School, São Paulo, Brazil (W.A.H., P.A.L.).
Correspondence to Professor P.W. Serruys, MD, PhD, Thoraxcenter, Ba-583, Dr Molewaterplein 40, 3015 GD Rotterdam, Netherlands. [email protected]
© 2008 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.107.752147
1146 by guest on January 6, 2015http://circ.ahajournals.org/Downloaded from

Conversely, the Stent or Surgery (SoS) trial recently demon-strated a significantly lower survival in patients treated withPCI compared with CABG at 6 years.7a
In the present study, patient-level data of the above-mentioned randomized trials were pooled to make a moreprecise estimate of the relative long-term safety and efficacyof PCI with stenting and CABG for multivessel coronaryartery disease, to assess the relative treatment effect in severalhigh-risk subgroups, and to assess the heterogeneity of thetreatment effect.
MethodsStudy Design and Patient PopulationThe methodology of the present meta-analysis has been describedpreviously.8 In brief, a MEDLINE search using the keywordscoronary stenting, coronary artery bypass surgery, and multisystem/multivessel disease was performed with the intention of selecting andincluding all randomized clinical trials comparing PCI with stentingand CABG in patients with multivessel coronary artery disease. Fourtrials were selected: ARTS,9 SoS,10 ERACI-II,11 and MASS-II.12
Principal investigators of each study group were contacted, andindividual patient data were requested on a broad range of baselinecharacteristics, medication usage, procedural results, and clinicaloutcome at 5 years. Clinical outcome included data on death, stroke,myocardial infarction (MI), and repeat revascularization (either PCIor CABG) at 5 years for ARTS, MASS-II, and ERACI-II. For theSoS trial, 5-year follow-up data were restricted to survival data. Dataon the occurrence of stroke, MI, and repeat revascularizationbetween 1 and 5 years were not collected by the SoS investigators.
Clinical events were adjudicated by independent clinical eventcommittees. The patient-level–based data were subsequently trans-ferred to Erasmus University Medical Center (Rotterdam, the Neth-erlands; E.B.) to 2 researchers (J.D., P.W.S.) who analyzed andinterpreted the data.
Definitions and Clinical End PointsNo attempt was made to readjudicate the events in the different trialsto compensate for the differences in the individual end-point defini-tions. Given the randomized design of the 4 trials, no bias wasexpected. The primary end point was the composite end point ofdeath, stroke, or MI at 5 years. The secondary end points includedmajor adverse cardiac and cerebrovascular events (defined as theoccurrence of major adverse cardiac and cerebrovascular accidents:all-cause death, stroke, MI, and repeat revascularization); the com-bined end point of all-cause death, MI, or repeat revascularization;and the itemized end points of death, stroke, MI, and repeatrevascularization (PCI or CABG).
Statistical AnalysisAll analyses were performed on an intention-to-treat population.Most continuous variables had nonnormal distribution (as evaluatedby Kolmogorov-Smirnov tests). For reasons of uniformity, summarystatistics for all continuous variables are therefore presented asmedians and 25th and 75th percentiles. Categorical data are summa-rized as frequencies and percentages. Differences in baseline char-acteristics between patients randomized to PCI with stenting versusCABG were analyzed with Wilcoxon–Mann–Whitney tests or Fish-er’s exact tests as appropriate.
The incidence of events over time was studied by the Kaplan–Meier method, and log-rank tests were applied to evaluate differ-ences between patients allocated to PCI with stenting or CABG.Additionally, Cox proportional-hazards regression models wereapplied to further evaluate the effects of allocated treatment on theincidence of events over time. Because aggregated estimates oftreatment effect that are based on small numbers of studies aresensitive to the chosen pooling method, we applied a variety of suchmethods, which showed quite consistent results. First, hazard ratios
(HRs) for study end points were determined from the proportional-hazards model stratified by trial with a single fixed effect accordingto the Yusuf–Peto13 approach. Subsequently, nonstratified modelswere fitted with study membership as a covariate in the model,allowing for the adjustment of trial effects and variations in thestandards of practice across participating institutions.14 Then, trial-by-treatment interaction terms were added to evaluate heterogeneityin treatment effect across trials. Interaction terms also were added tostudy heterogeneities in treatment effects according to clinicallyrelevant characteristics, including age, gender, diabetes, dyslipid-emia, hypertension, prior MI, number of diseased vessels, leftventricular ejection fraction, and peripheral vascular disease. Be-cause the �2 log likelihood of the regression models was notimproved by adding interaction terms (except for death in relation totrial; see the Results section), we decided to stick to the fixed-effectsapproach and to remove any interaction term from further models.The HRs that are finally reported (together with the 95% confidenceintervals [CIs]) are based on regression models with allocatedtreatment as the main effect and with the above-mentioned clinicalcharacteristics as covariates.15
All tests are 2 sided with a significance level of 0.05. All statisticalanalyses were performed with the SAS System version 8.2 (SASInstitute Inc, Cary, NC).
The authors had full access to and take full responsibility for theintegrity of the data. All authors have read and agree to themanuscript as written.
ResultsPatients, Baseline, and Procedural CharacteristicsA total of 3051 patients were included in this analysisbetween June 1995 and June 2000 (1205 in ARTS, 450 inERACI-II, 408 in MASS-II, and 988 in SoS). In total, 1533were randomized to CABG, and 1518 were randomized toPCI. Eighty-nine percent of patients allocated to PCI under-went the assigned treatment compared with 96% of thoseassigned to CABG.
Baseline and procedural characteristics are summarized inTable 1. Although 3-vessel disease was more frequent in theCABG group compared with the PCI group (40.0% versus36.1%, respectively; P�0.017), complete revascularizationwas performed in 89.4% of the CABG patients comparedwith 62.0% of the PCI patients (P�0.001). The hospital staywas significantly longer in the CABG group (median, 8 days;interquartile range, 1 to 4 days) compared with the PCI group(median, 3 days; interquartile range, 6 to 11) (P�0.001).
Clinical OutcomeClinical event rates are summarized in Table 2 and Figure 1.Five-year follow-up was complete for 97% of all patients(100% in ARTS and ERACI-II, 97.5% in MASS-II, and91.6% in SoS). At 5 years, the cumulative incidence of death,MI, and stroke was similar in patients randomized to PCI withstenting versus CABG (16.7% versus 16.9%, respectively;HR, 1.04; 95% CI, 0.86 to 1.27; P�0.69). Repeat revascu-larization, however, occurred significantly more frequentlyafter PCI compared with CABG (29.0% versus 7.9%, respec-tively; HR, 0.23; 95% CI, 0.18 to 0.29; P�0.001). Because ofthe substantial difference in the repeat revascularization ratesbetween both treatment modalities, major adverse cardiac andcerebrovascular event rates were significantly higher in thePCI group than in the CABG group (39.2% versus 23.0%,respectively; HR, 0.53; 95% CI, 0.45 to 0.61; P�0.001).
Daemen et al PCI Versus CABG for Multivessel Disease 1147
by guest on January 6, 2015http://circ.ahajournals.org/Downloaded from

Table 1. Baseline and Procedural Characteristics and Medications
PCI With Stenting(n�1518 Patients)
CABG(n�1533 Patients) P
Age, y
Median 61.6 61.6 0.37
IQR 53.5–68.0 54.6–68.3
Range 30.2–85.4 31.9–86.0
Men, % 76.5 (1162/1518) 77.1 (1182/1533) 0.73
Diabetes mellitus, % 18.1 (275/1518) 17.5 (268/1533) 0.67
Hyperlipidemia, % 60.1 (910/1515) 56.5 (866/1532) 0.051
Hypertension, % 50.5 (766/1518) 51.7 (792/1533) 0.52
Family history of CAD, % 38.1 (498/1307) 38.7 (514/1327) 0.75
Current smoker, % 28.3 (429/1516) 26.5 (406/1533) 0.27
Previous MI, % 42.8 (650/1518) 41.4 (635/1533) 0.44
Peripheral vascular disease, % 7.0 (107/1518) 8.2 (126/1533) 0.25
Aspirin, % 93.5 (1419/1518) 90.2 (1382/1533) 0.001
�-Blockers, % 79.4 (1205/1518) 81.7 (1252/1533) 0.11
Calcium channel blockers, % 37.3 (566/1518) 40.2 (617/1533) 0.095
Nitrates, % 68.1 (1033/1518) 69.7 (1068/1533) 0.35
Statins, % 40.9 (621/1517) 39.5% (606/1533) 0.44
Enrollment diagnosis, %*
Stable angina 68.2 (1036/1518) 68.9 (1057/1533) 0.70
Unstable angina 28.5 (432/1518) 27.3 (418/1533) 0.47
Silent ischemia 3.5 (48/1358) 2.6 (34/1330) 0.15
Ejection fraction, % 0.91
Median 60 60
IQR 52–68 51–67
Range 27–92 26–91
Segments with �50% stenosis, n 0.92
Median 3 3
IQR 2–3 2–3
Range 1–9 1–8
Diseased vessels, n 0.017
1 4.6 (70/1518) 3.0 (46/1533)
2 59.3 (900/1518) 57.0 (874/1533)
3 36.1 (548/1518) 40.0 (613/1533)
Vessel territory with stenosis, %
RCA 74.2 (1127/1518) 78.0 (1195/1533) 0.017
LAD 89.9 (1364/1518) 91.8 (1408/1533) 0.06
LCx 63.2 (959/1518) 67.7 (1038/1533) 0.009
LMCA 1.0 (15/1518) 0.7 (10/1533) 0.32
Length of hospital stay, d �0.001
Median 3 8
IQR 1–4 6–11
Range 1–70 1–110
Complete revascularization, % 62.0 (809/1304) 89.4 (1180/1320) �0.001
IQR indicates interquartile range; CAD, coronary artery disease; RCA, right coronary artery; LAD, leftanterior descending artery; LCx, left circumflex artery; and LMCA, left main coronary artery. Valuesare mean�SD when appropriate. The difference between the total number in each group and thedenominator used to calculate the percentages for each variable is due to missing data.
*Stable angina was defined according to the Canadian Cardiovascular Society system; unstableangina was classified according to the Braunwald classification.
1148 Circulation September 9, 2008
by guest on January 6, 2015http://circ.ahajournals.org/Downloaded from
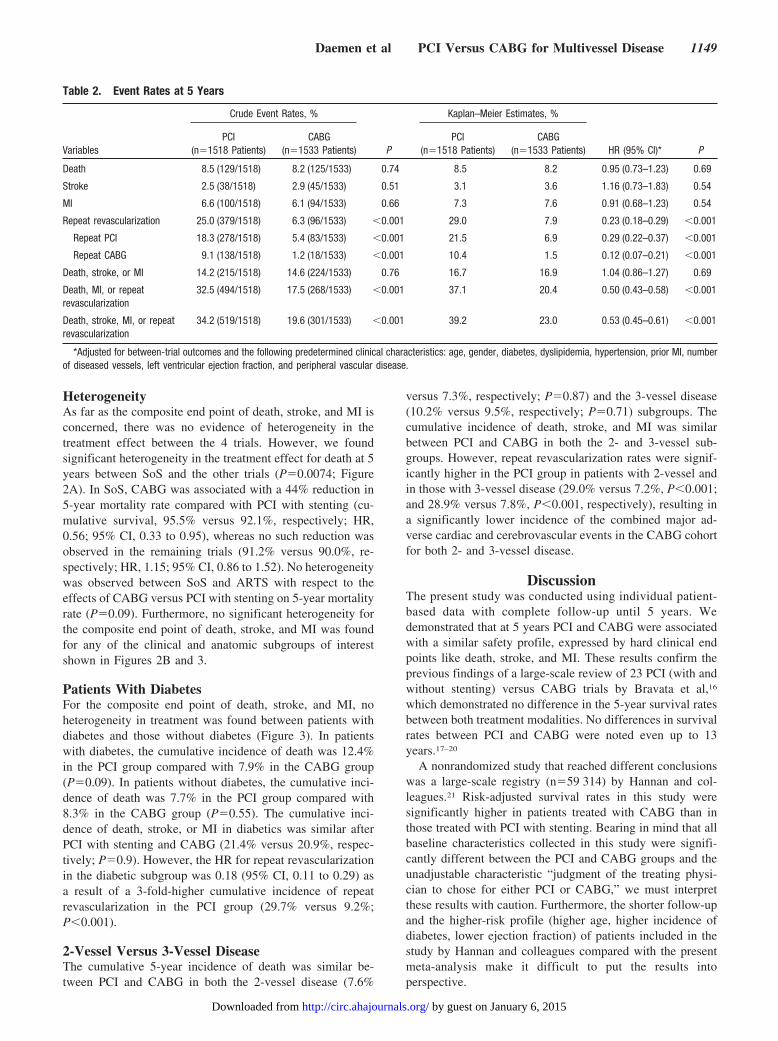
HeterogeneityAs far as the composite end point of death, stroke, and MI isconcerned, there was no evidence of heterogeneity in thetreatment effect between the 4 trials. However, we foundsignificant heterogeneity in the treatment effect for death at 5years between SoS and the other trials (P�0.0074; Figure2A). In SoS, CABG was associated with a 44% reduction in5-year mortality rate compared with PCI with stenting (cu-mulative survival, 95.5% versus 92.1%, respectively; HR,0.56; 95% CI, 0.33 to 0.95), whereas no such reduction wasobserved in the remaining trials (91.2% versus 90.0%, re-spectively; HR, 1.15; 95% CI, 0.86 to 1.52). No heterogeneitywas observed between SoS and ARTS with respect to theeffects of CABG versus PCI with stenting on 5-year mortalityrate (P�0.09). Furthermore, no significant heterogeneity forthe composite end point of death, stroke, and MI was foundfor any of the clinical and anatomic subgroups of interestshown in Figures 2B and 3.
Patients With DiabetesFor the composite end point of death, stroke, and MI, noheterogeneity in treatment was found between patients withdiabetes and those without diabetes (Figure 3). In patientswith diabetes, the cumulative incidence of death was 12.4%in the PCI group compared with 7.9% in the CABG group(P�0.09). In patients without diabetes, the cumulative inci-dence of death was 7.7% in the PCI group compared with8.3% in the CABG group (P�0.55). The cumulative inci-dence of death, stroke, or MI in diabetics was similar afterPCI with stenting and CABG (21.4% versus 20.9%, respec-tively; P�0.9). However, the HR for repeat revascularizationin the diabetic subgroup was 0.18 (95% CI, 0.11 to 0.29) asa result of a 3-fold-higher cumulative incidence of repeatrevascularization in the PCI group (29.7% versus 9.2%;P�0.001).
2-Vessel Versus 3-Vessel DiseaseThe cumulative 5-year incidence of death was similar be-tween PCI and CABG in both the 2-vessel disease (7.6%
versus 7.3%, respectively; P�0.87) and the 3-vessel disease(10.2% versus 9.5%, respectively; P�0.71) subgroups. Thecumulative incidence of death, stroke, and MI was similarbetween PCI and CABG in both the 2- and 3-vessel sub-groups. However, repeat revascularization rates were signif-icantly higher in the PCI group in patients with 2-vessel andin those with 3-vessel disease (29.0% versus 7.2%, P�0.001;and 28.9% versus 7.8%, P�0.001, respectively), resulting ina significantly lower incidence of the combined major ad-verse cardiac and cerebrovascular events in the CABG cohortfor both 2- and 3-vessel disease.
DiscussionThe present study was conducted using individual patient-based data with complete follow-up until 5 years. Wedemonstrated that at 5 years PCI and CABG were associatedwith a similar safety profile, expressed by hard clinical endpoints like death, stroke, and MI. These results confirm theprevious findings of a large-scale review of 23 PCI (with andwithout stenting) versus CABG trials by Bravata et al,16
which demonstrated no difference in the 5-year survival ratesbetween both treatment modalities. No differences in survivalrates between PCI and CABG were noted even up to 13years.17–20
A nonrandomized study that reached different conclusionswas a large-scale registry (n�59 314) by Hannan and col-leagues.21 Risk-adjusted survival rates in this study weresignificantly higher in patients treated with CABG than inthose treated with PCI with stenting. Bearing in mind that allbaseline characteristics collected in this study were signifi-cantly different between the PCI and CABG groups and theunadjustable characteristic “judgment of the treating physi-cian to chose for either PCI or CABG,” we must interpretthese results with caution. Furthermore, the shorter follow-upand the higher-risk profile (higher age, higher incidence ofdiabetes, lower ejection fraction) of patients included in thestudy by Hannan and colleagues compared with the presentmeta-analysis make it difficult to put the results intoperspective.
Table 2. Event Rates at 5 Years
Variables
Crude Event Rates, %
P
Kaplan–Meier Estimates, %
HR (95% CI)* PPCI
(n�1518 Patients)CABG
(n�1533 Patients)PCI
(n�1518 Patients)CABG
(n�1533 Patients)
Death 8.5 (129/1518) 8.2 (125/1533) 0.74 8.5 8.2 0.95 (0.73–1.23) 0.69
Stroke 2.5 (38/1518) 2.9 (45/1533) 0.51 3.1 3.6 1.16 (0.73–1.83) 0.54
MI 6.6 (100/1518) 6.1 (94/1533) 0.66 7.3 7.6 0.91 (0.68–1.23) 0.54
Repeat revascularization 25.0 (379/1518) 6.3 (96/1533) �0.001 29.0 7.9 0.23 (0.18–0.29) �0.001
Repeat PCI 18.3 (278/1518) 5.4 (83/1533) �0.001 21.5 6.9 0.29 (0.22–0.37) �0.001
Repeat CABG 9.1 (138/1518) 1.2 (18/1533) �0.001 10.4 1.5 0.12 (0.07–0.21) �0.001
Death, stroke, or MI 14.2 (215/1518) 14.6 (224/1533) 0.76 16.7 16.9 1.04 (0.86–1.27) 0.69
Death, MI, or repeatrevascularization
32.5 (494/1518) 17.5 (268/1533) �0.001 37.1 20.4 0.50 (0.43–0.58) �0.001
Death, stroke, MI, or repeatrevascularization
34.2 (519/1518) 19.6 (301/1533) �0.001 39.2 23.0 0.53 (0.45–0.61) �0.001
*Adjusted for between-trial outcomes and the following predetermined clinical characteristics: age, gender, diabetes, dyslipidemia, hypertension, prior MI, numberof diseased vessels, left ventricular ejection fraction, and peripheral vascular disease.
Daemen et al PCI Versus CABG for Multivessel Disease 1149
by guest on January 6, 2015http://circ.ahajournals.org/Downloaded from

All 4 randomized trials included in the present meta-anal-ysis studied the safety and effectiveness of PCI with baremetal stents. Since 2002, drug-eluting stents have been shownto halve repeat reinterventions rates without affecting theshort- and long-term safety of the treatment.22–25 Moreover,because of their significantly lower revascularization rates,sirolimus-eluting stents proved to be capable of narrowing thegap in major adverse cardiac event rates between PCI andCABG, as demonstrated by the ARTS-II and ERACI-IIIstudies.26,27 In contrast to the ARTS-I study, the recentlypresented 3-year results of the ARTS-II study showed similarmajor adverse cardiac event rates after PCI with sirolimus-eluting stents and CABG. However, the need for repeatrevascularization was still significantly lower after CABG.28
Although both ERACI-III and ARTS-II showed a clearimpact of drug-eluting stents on the relative efficacy of PCI
and CABG, it must be noted that both studies were nonran-domized comparisons. Along these lines, a recent registry byJavaid et al29 reported significantly higher mortality rates anda trend toward higher MI rates in patients treated with PCIwith drug-eluting stents compared with those treated withCABG at 1 year regardless of the amount of vessels diseasedand the presence of diabetes.29 It is worth mentioning that the1-year results of none of the 4 randomized trials in the presentstudy concurred with these latter findings.9–12 Given thesimilar, if not superior, safety profile of drug-eluting stentscompared with bare metal stents, it is unlikely that the use ofdrug-eluting stents in this study accounted for this dissimi-larity.22,23,30 Several large-scale randomized trials such asFuture Revascularization Evaluation in Patients With Diabetes:Optimal Management of Multivessel Disease (FREEDOM),Coronary Artery Revascularization in Diabetics (CARDIA), and
Days
Logrank p-value 0.78
0 365 730 1095 1460 1825
50
60
70
80
90
100
Ove
rall
surv
ival
(%) PCI 91.5%
CABG 91.8%
Group 0 365 730 1095 1460 1825
PCI 1518 1472 1456 1440 1406 1347
CABG 1533 1479 1457 1439 1412 1349
Group 0 365 730 1095 1460 1825
PCI 1518 1381 913 896 872 846
CABG 1533 1377 908 891 868 845
PCI 83.3%
CABG 83.1%
Logrank p-value 0.6450
60
70
80
90
100
Surv
ival
free
of d
eath
, str
oke
and
myo
card
ial
infa
rctio
n (%
)
Days0 365 730 1095 1460 1825
Group 0 365 730 1095 1460 1825
PCI 1518 1204 772 740 707 665
CABG 1533 1428 927 911 882 855
PCI 71.0%
CABG 92.1%
Logrank p-value <0.000150
60
70
80
90
100
Surv
ival
free
of r
epea
t rev
ascu
lariz
atoi
n (%
)
Days0 365 730 1095 1460 1825
Group 0 365 730 1095 1460 1825
PCI 1518 1153 729 691 657 616
CABG 1533 1332 867 846 812 785
PCI 60.8%
CABG 77.0%
Logrank p-value <0.000150
60
70
80
90
100Su
rviv
al fr
ee o
f dea
th, s
trok
e, m
yoca
rdia
l inf
arct
ion
and
repe
at re
vasc
ular
izat
ion
(%)
Days0 365 730 1095 1460 1825
A B
C D
Figure 1. Kaplan–Meier event-free survival analysis of death (A); death, stroke, or MI (B); repeat revascularization (C); and majoradverse cardiac and cerebrovascular events (death, stroke, MI, and repeat revascularization (D).
1150 Circulation September 9, 2008
by guest on January 6, 2015http://circ.ahajournals.org/Downloaded from

Synergy Between Percutaneous Coronary Intervention WithTaxus and Cardiac Surgery (SYNTAX) are currently comparingthe safety and effectiveness of CABG and PCI with drug-elutingstents.31
Of note, despite the improvement in durability of morecontemporary PCI with (drug-eluting) stents, long-term sur-vival rates do not seem to improve in a similar fashion andremain equal between PCI and CABG. This finding recalls amajor goal of treating (multivessel) coronary artery disease:the relief of angina. Despite the fact that at 1 year after CABGsignificantly more patients were free of angina comparedwith PCI in all 4 trials,9–12 5-year reports of the ARTS,ERACI-II, and MASS-II demonstrated similar incidences ofangina at 5 years after CABG and PCI.5–7 Additionally, thefinal results from the Bypass Angioplasty RevascularizationInvestigation (BARI) trial proved that even up to 10 years,angina rates were still equal between both treatment modal-ities.17 However, in the PCI group, these similar angina rateswere achieved only after a significantly higher rate of repeatrevascularizations compared with the CABG group.
Significant heterogeneity in treatment effect was notedbetween SoS and the remaining trials with respect to survivalat 5 years. Although the 5-year cumulative survival in the PCIarm of SoS (92.1%) was similar to the ARTS, ERACI-II, andMASS-II trials (92.2%, 92.9%, and 86.3% respectively), thesurvival in the CABG arm of SoS (95.5%) was remarkablyhigher than in ARTS, ERACI-II, and MASS-II (92.6%,88.5%, and 84.1%, respectively). The exact reason for thissuperior survival rate remains puzzling, and a play of chancecannot be excluded. A speculative reason for the heterogene-ity might be the difference in the inclusion criteria andprocedural requirements in the different studies. In ARTS,higher-risk patients were excluded; 67% of the patients had2-vessel disease; and an equivalent revascularization rate was
required.9,32 Conversely, in MASS-II, almost 58% of thepatients had 3-vessel disease, and a proximal left anteriordescending artery lesion was required.12 Additionally, theSoS trial protocol stated that the study was intended to be a“pragmatic trial,” including enrollment of a wide range ofpatients with minimal restriction on postrandomization pa-tient management. However, both patient groups in SoS werewell matched, and it is unlikely that the pragmatic nature ofthe trial was the reason for the unexpected difference in deathrates, which are not confirmed by the larger sample of thismeta-analysis.10
Coronary artery disease in diabetics has been shown to bemore aggressive and to be associated with an impairedevent-free survival after both CABG and PCI because ofsmaller vessel sizes, longer lesion length, greater plaqueburden, and a possibly differently acting restenotic cascadethan in nondiabetics.33–38 Given this higher-risk profile,which is most often associated with multivessel disease,CABG was regarded as the preferred revascularizationmethod because of its ability to bypass this large amount ofplaque burden and to achieve more complete revasculariza-tion rates, making the need for repeat revascularizations lesslikely. Attempting to demonstrate the most optimal treatmentstrategy for diabetics, a subgroup analysis of the randomizedBARI trial and a large observational registry demonstratedsignificantly impaired survival among patients treated withPCI compared with those treated with CABG.36,39 Interest-ingly, in the BARI registry, all-cause survival was notsignificantly different between both groups.40 Furthermore,all the above-mentioned studies were performed in theprestent era and may no longer be applicable in currentclinical practice. In the present analysis, using pooled patient-level–based 5-year follow-up data from 4 randomized con-trolled trials, we found no significant heterogeneity of the
Adjusted hazard ratio and 95% CI for death at 4Y
0.1 1.0 100.5 2.0
Favors PCIFavors CABG
HR 0.56, 95% CI 0.33 – 0.95
HR 0.95, 95% CI 0.63 - 1.43
HR 1.18, 95% CI 0.71 – 1.96
HR 1.69, 95% CI 0.91 – 3.16
HR 0.97, 95% CI 0.76 – 1.24
SoS
ARTS
MASS-II
ERACI-II
All patients
SoS
ARTS
MASS-II
ERACI-II
All patients
Adjusted hazard ratio and 95% CI for death, stroke or MI at 4Y
0.1 1.0 100.5 2.0
Favors PCIFavors CABG
HR 1.24, 95% CI 0.80 – 1.93
HR 0.80, 95% CI 0.60 – 1.06
HR 1.08, 95% CI 0.72 – 1.61
HR 1.74, 95% CI 1.07 – 2.83
HR 1.05, 95% CI 0.87 – 1.26
A B
Figure 2. HRs for each trial individually and the pooled estimate for all trials (corrected for between-trial outcome) for the end points ofall-cause mortality (A) and all-cause death, stroke, and MI (B).
Daemen et al PCI Versus CABG for Multivessel Disease 1151
by guest on January 6, 2015http://circ.ahajournals.org/Downloaded from

treatment effect in diabetics compared with nondiabetics,although our analysis might have suffered from a lack ofpower. The ongoing FREEDOM and CARDIA trials willfurther address the relative safety and efficacy of CABG andmore contemporary PCI with drug-eluting stents in diabetics.
Two randomized controlled trials comparing PCI withCABG, the Angina With Extremely Serious Operative MortalityEvaluation (AWESOME) and a Randomized Comparison ofStent Implantation and Off-Pump Bypass Surgery in PatientsReferred for Coronary Angioplasty (OCTOSTENT) trials,41,42
were excluded from the present meta-analysis. The AWESOMEtrial (n�454) included only high-risk patients with refractorymyocardial ischemia and a high risk of adverse outcomes,generating a study population clearly different from the presentone. Moreover, 54% of the patients in AWESOME were treatedwith balloon angioplasty only. The OCTOSTENT trial(n�280), with only 30% of the population having multives-sel disease, was not yet published when the initial meta-analysis by Mercado et al8 was performed. Of note, neither
AWESOME nor OCTOSTENT completed the 5-year follow-upat the time of the present meta-analysis.
Pooling data from 4 multicenter randomized controlledtrials with diversity in inclusion and exclusion criteria re-sulted in a diverse and high-risk patient population. However,patients with severe 3-vessel disease presenting with an acutecoronary syndrome, left main lesions, previous coronaryinterventions, heart failure, or renal disease were excluded inall 4 trials. Although no heterogeneity in the treatment effectwas found among several high-risk subgroups in the presentanalysis, the results of several large-scale, dedicated, random-ized controlled trials are eagerly awaited to determine theexternal validity of our findings. Until the relatively short-term findings of these large trials are presented, the resultsfrom the present meta-analysis constitute the highest amountof clinical evidence regarding the relative long-term safety ofPCI using stents and CABG.
ConclusionsIn this pooled analysis of 4 randomized trials, PCI wasassociated with a long-term safety profile, expressed bydeath, stroke, and MI, similar to that of CABG. However,because of the persistently lower repeat revascularizationrates in the CABG patients, overall major adverse cardiac andcerebrovascular event rates were significantly lower in theCABG group at 5 years. Dedicated trial data on the impact ofdrug-eluting stents, the relief of angina, and the role of PCI inhigher-risk patients are warranted.
DisclosuresDr Stables received research grants from Cordis, Boston Scientific,Medtronic, and Abbott and has served as a consultant or on theadvisory board for Cordis, Boston Scientific, Medtronic, and Abbott.The other authors report no conflicts.
References1. Hoffman SN, TenBrook JA, Wolf MP, Pauker SG, Salem DN, Wong JB.
A meta-analysis of randomized controlled trials comparing coronaryartery bypass graft with percutaneous transluminal coronary angioplasty:one- to eight-year outcomes. J Am Coll Cardiol. 2003;41:1293–1304.
2. van der Hoeven BL, Schalij MJ, van der Wall EE. Percutaneous coronaryintervention with stent placement versus bypass operation in symptomaticmultiple-vessel disease: lessons from an observational study [in Dutch].Ned Tijdschr Geneeskd. 2005;149:2837–2840.
3. Bell MR, Gersh BJ, Schaff HV, Holmes DR Jr, Fisher LD, Alderman EL,Myers WO, Parsons LS, Reeder GS. Effect of completeness of revascu-larization on long-term outcome of patients with three-vessel diseaseundergoing coronary artery bypass surgery: a report from the CoronaryArtery Surgery Study (CASS) Registry. Circulation. 1992;86:446–457.
4. van den Brand MJ, Rensing BJ, Morel MA, Foley DP, de Valk V,Breeman A, Suryapranata H, Haalebos MM, Wijns W, Wellens F, BalconR, Magee P, Ribeiro E, Buffolo E, Unger F, Serruys PW. The effect ofcompleteness of revascularization on event-free survival at one year in theARTS trial. J Am Coll Cardiol. 2002;39:559–564.
5. Serruys PW, Ong AT, van Herwerden LA, Sousa JE, Jatene A, BonnierJJ, Schonberger JP, Buller N, Bonser R, Disco C, Backx B, HugenholtzPG, Firth BG, Unger F. Five-year outcomes after coronary stenting versusbypass surgery for the treatment of multivessel disease: the final analysisof the Arterial Revascularization Therapies Study (ARTS) randomizedtrial. J Am Coll Cardiol. 2005;46:575–581.
6. Rodriguez AE, Baldi J, Fernandez Pereira C, Navia J, Rodriguez Ale-mparte M, Delacasa A, Vigo F, Vogel D, O’Neill W, Palacios IF.Five-year follow-up of the Argentine randomized trial of coronary angio-plasty with stenting versus coronary bypass surgery in patients withmultiple vessel disease (ERACI II). J Am Coll Cardiol. 2005;46:582–588.
HypercholesterolemiaNo hypercholesterolemia
DiabetesNo diabetes
Previous MINo previous MI
LVEF ≤60LVEF >60
Two vessel diseaseThree vessel disease
Peripheral vascular diseaseNo peripheral vascular disease
All patients
0.95
0.06
0.58
0.65
0.84
0.54
0.84
0.12
P for interaction
Adjusted hazard ratio and 95% CI for all-cause death, stroke of MI
0.1 1.0 100.5 2.0
Favors PCI Favors CABG
Age ≤62 yearsAge >62 years
MenWomen
HypertensionNo hypertension
0.08
0.64
Figure 3. Primary end point of death, stroke, or MI in selectedsubgroups. Exploratory analyses to evaluate possible heteroge-neity in treatment effects on 5-year event rates according to 2 ofthe 3 treatment cohorts and the following clinically relevantcharacteristics: age, gender, hypertension, diabetes, previousMI, left ventricular ejection fraction (LVEF), vessel disease, andperipheral vascular disease. For the continuous variables (ageand total stented length), medians were used as cutoffs. Resultsof tests for heterogeneity in treatment effect were consideredsignificant at P�0.01.
1152 Circulation September 9, 2008
by guest on January 6, 2015http://circ.ahajournals.org/Downloaded from

7. Hueb W, Lopes NH, Gersh BJ, Soares P, Machado LA, Jatene FB,Oliveira SA, Ramires JA. Five-year follow-up of the Medicine, Angio-plasty, or Surgery Study (MASS II): a randomized controlled clinicaltrial of 3 therapeutic strategies for multivessel coronary artery disease.Circulation. 2007;115:1082–1089.
7a.Booth J, Clayton T, Pepper J, Nugara F, Flather M, Sigwart U, StablesRH, SoS Investigators. Randomized, controlled trial of coronary arterybypass surgery versus percutaneous coronary intervention in patients withmultivessel coronary artery disease: six-year follow-up from the Stent orSurgery Trial (SoS). Circulation. 2008;118:381–388.
8. Mercado N, Wijns W, Serruys PW, Sigwart U, Flather MD, Stables RH,O’Neill WW, Rodriguez A, Lemos PA, Hueb WA, Gersh BJ, Booth J,Boersma E. One-year outcomes of coronary artery bypass graft surgeryversus percutaneous coronary intervention with multiple stenting formultisystem disease: a meta-analysis of individual patient data fromrandomized clinical trials. J Thorac Cardiovasc Surg. 2005;130:512–519.
9. Serruys PW, Unger F, Sousa JE, Jatene A, Bonnier HJ, Schonberger JP,Buller N, Bonser R, van den Brand MJ, van Herwerden LA, Morel MA,van Hout BA. Comparison of coronary-artery bypass surgery and stentingfor the treatment of multivessel disease. N Engl J Med. 2001;344:1117–1124.
10. Stables R. Coronary artery bypass surgery versus percutaneous coronaryintervention with stent implantation in patients with multivessel coronaryartery disease (the Stent or Surgery trial): a randomised controlled trial.Lancet. 2002;360:965–970.
11. Rodriguez A, Bernardi V, Navia J, Baldi J, Grinfeld L, Martinez J, VogelD, Grinfeld R, Delacasa A, Garrido M, Oliveri R, Mele E, Palacios I,O’Neill W. Argentine Randomized Study: Coronary Angioplasty WithStenting Versus Coronary Bypass Surgery in Patients With Multiple-Vessel Disease (ERACI II): 30-day and one-year follow-up results:ERACI II Investigators. J Am Coll Cardiol. 2001;37:51–58.
12. Hueb W, Soares PR, Gersh BJ, Cesar LA, Luz PL, Puig LB, MartinezEM, Oliveira SA, Ramires JA. The Medicine, Angioplasty, or SurgeryStudy (MASS-II): a randomized, controlled clinical trial of three thera-peutic strategies for multivessel coronary artery disease: one-year results.J Am Coll Cardiol. 2004;43:1743–1751.
13. Yusuf S, Peto R, Lewis J, Collins R, Sleight P. Beta blockade during andafter myocardial infarction: an overview of the randomized trials. ProgCardiovasc Dis. 1985;27:335–371.
14. Michiels S, Baujat B, Mahe C, Sargent DJ, Pignon JP. Random effectssurvival models gave a better understanding of heterogeneity in indi-vidual patient data meta-analyses. J Clin Epidemiol. 2005;58:238–245.
15. Steyerberg EW, Bossuyt PM, Lee KL. Clinical trials in acute myocardialinfarction: should we adjust for baseline characteristics? Am Heart J.2000;139:745–751.
16. Bravata DM, Gienger AL, McDonald KM, Sundaram V, Perez MV,Varghese R, Kapoor JR, Ardehali R, Owens DK, Hlatky MA. Systematicreview: the comparative effectiveness of percutaneous coronary inter-ventions and coronary artery bypass graft surgery. Ann Intern Med.2007;147:703–716.
17. BARI Investigators. The final 10-year follow-up results from the BARIrandomized trial. J Am Coll Cardiol. 2007;49:1600–1606.
18. King SB 3rd, Kosinski AS, Guyton RA, Lembo NJ, Weintraub WS.Eight-year mortality in the Emory Angioplasty Versus Surgery Trial(EAST). J Am Coll Cardiol. 2000;35:1116–1121.
19. Kaehler J, Koester R, Billmann W, Schroeder C, Rupprecht HJ, IschingerT, Jahns R, Vogt A, Lampen M, Hoffmann R, Riessen R, Berger J,Meinertz T, Hamm CW. 13-Year follow-up of the German angioplastybypass surgery investigation. Eur Heart J. 2005;26:2148–2153.
20. Henderson RA, Pocock SJ, Sharp SJ, Nanchahal K, Sculpher MJ, BuxtonMJ, Hampton JR. Long-term results of RITA-1 trial: clinical and costcomparisons of coronary angioplasty and coronary-artery bypass grafting:Randomised Intervention Treatment of Angina. Lancet. 1998;352:1419–1425.
21. Hannan EL, Racz MJ, Walford G, Jones RH, Ryan TJ, Bennett E,Culliford AT, Isom OW, Gold JP, Rose EA. Long-term outcomes ofcoronary-artery bypass grafting versus stent implantation. N Engl J Med.2005;352:2174–2183.
22. Tu JV, Bowen J, Chiu M, Ko DT, Austin PC, He Y, Hopkins R, TarrideJE, Blackhouse G, Lazzam C, Cohen EA, Goeree R. Effectiveness andsafety of drug-eluting stents in Ontario. N Engl J Med. 2007;357:1393–1402.
23. Stettler C, Wandel S, Allemann S, Kastrati A, Morice MC, Schomig A,Pfisterer ME, Stone GW, Leon MB, de Lezo JS, Goy JJ, Park SJ, SabateM, Suttorp MJ, Kelbaek H, Spaulding C, Menichelli M, Vermeersch P,
Dirksen MT, Cervinka P, Petronio AS, Nordmann AJ, Diem P, Meier B,Zwahlen M, Reichenbach S, Trelle S, Windecker S, Juni P. Outcomesassociated with drug-eluting and bare-metal stents: a collaborativenetwork meta-analysis. Lancet. 2007;370:937–948.
24. Kastrati A, Mehilli J, Pache J, Kaiser C, Valgimigli M, Kelbaek H,Menichelli M, Sabate M, Suttorp MJ, Baumgart D, Seyfarth M, PfistererME, Schomig A. Analysis of 14 trials comparing sirolimus-eluting stentswith bare-metal stents. N Engl J Med. 2007;356:1030–1039.
25. Stone GW, Moses JW, Ellis SG, Schofer J, Dawkins KD, Morice MC,Colombo A, Schampaert E, Grube E, Kirtane AJ, Cutlip DE, Fahy M,Pocock SJ, Mehran R, Leon MB. Safety and efficacy of sirolimus- andpaclitaxel-eluting coronary stents. N Engl J Med. 2007;356:998–1008.
26. Serruys PW, Ong AT, Morice MC, De Bruyne B, Colombo A, Macaya C,Richardt G, Fajadet J, Hamm CW, Dawkins K, O’Malley AJ, BressersM, Donohoe DJ. Arterial Revascularisation Therapies Study part II:Sirolimus-eluting stents for the treatment of patients with multivesselde novo coronary artery lesions. Eurointervention. 2005;1:147–156.
27. Rodriguez AE, Maree AO, Grinfeld L, Fernandez Pereira C, Mieres J,Rodriguez Alemparte M, Berrocal D, Rodriguez Granillo AM, VigoCS, Russo Felsen M, O’Neill W, Palacios I. Revascularizationstrategies of coronary multivessel disease in the drug-eluting stent era:one year follow-up results of the ERACI-III trial. Eurointervention.2006;2:53– 60.
28. Serruys PW. Arterial Revascularization Therapies Study Part II: thesirolimus-eluting stent in the treatment of patients with multivessel denovo coronary artery lesions: three-year clinical outcome. Paper present-ed at: Annual Scientific Sessions of the American College of Cardiology;March 24–27, 2007; New Orleans, La.
29. Javaid A, Steinberg DH, Buch AN, Corso PJ, Boyce SW, Pinto SlottowTL, Roy PK, Hill P, Okabe T, Torguson R, Smith KA, Xue Z, GevorkianN, Suddath WO, Kent KM, Satler LF, Pichard AD, Waksman R.Outcomes of coronary artery bypass grafting versus percutaneouscoronary intervention with drug-eluting stents for patients with mul-tivessel coronary artery disease. Circulation. 2007;116(suppl):I-200–I-206.
30. Daemen J, Van Domburg R, Boersma E, de Jaegere P, Serruys P.A long-term survival analysis of 3 sequential cohorts of consecutive allcomers (n�6129) treated with either bare-metal, sirolimus- or paclitaxel-eluting stents: an epidemiological analysis requested by the directingboard of a Dutch tertiary medical center. Paper presented at: EuropeanSociety of Cardiology; September 3, 2007; Vienna, Austria.
31. Ong AT, Serruys P, Mohr FW, Morice MC, Kappetein AP, Holmes DR,Mack MJ, van den Brand MJ, Morel MA, van Es GA, Kleijne J, KoglinJ, Russell ME. The Synergy Between Percutaneous Coronary Inter-vention With Taxus and Cardiac Surgery (SYNTAX) Study: design,rationale and run-in phase. Am Heart J. 2006;131:1194–1204.
32. Serruys PW, Unger F, van Hout BA, van den Brand MJ, van HerwerdenLA, van Es GA, Bonnier JJ, Simon R, Cremer J, Colombo A, Santoli C,Vandormael M, Marshall PR, Madonna O, Firth BG, Breeman A, MorelMA, Hugenholtz PG. The ARTS Study (Arterial RevascularizationTherapies Study). Semin Interv Cardiol. 1999;4:209–219.
33. Kip KE, Faxon DP, Detre KM, Yeh W, Kelsey SF, Currier JW. Coronaryangioplasty in diabetic patients: the National Heart, Lung, and BloodInstitute Percutaneous Transluminal Coronary Angioplasty Registry.Circulation. 1996;94:1818 –1825.
34. Thourani VH, Weintraub WS, Stein B, Gebhart SS, Craver JM, Jones EL,Guyton RA. Influence of diabetes mellitus on early and late outcome aftercoronary artery bypass grafting. Ann Thorac Surg. 1999;67:1045–1052.
35. West NE, Ruygrok PN, Disco CM, Webster MW, Lindeboom WK,O’Neill WW, Mercado NF, Serruys PW. Clinical and angiographicpredictors of restenosis after stent deployment in diabetic patients.Circulation. 2004;109:867– 873.
36. Niles NW, McGrath PD, Malenka D, Quinton H, Wennberg D,Shubrooks SJ, Tryzelaar JF, Clough R, Hearne MJ, Hernandez F Jr,Watkins MW, O’Connor GT. Survival of patients with diabetes andmultivessel coronary artery disease after surgical or percutaneouscoronary revascularization: results of a large regional prospective study:Northern New England Cardiovascular Disease Study Group. J Am CollCardiol. 2001;37:1008–1015.
37. Lincoff AM. Important triad in cardiovascular medicine: diabetes,coronary intervention, and platelet glycoprotein IIb/IIIa receptorblockade. Circulation. 2003;107:1556–1559.
Daemen et al PCI Versus CABG for Multivessel Disease 1153
by guest on January 6, 2015http://circ.ahajournals.org/Downloaded from

38. Aronson D, Bloomgarden Z, Rayfield EJ. Potential mechanisms pro-moting restenosis in diabetic patients. J Am Coll Cardiol. 1996;27:528–535.
39. Comparison of coronary bypass surgery with angioplasty in patients withmultivessel disease: the Bypass Angioplasty Revascularization Investi-gation (BARI) Investigators. N Engl J Med. 1996;335:217–225.
40. Detre KM, Guo P, Holubkov R, Califf RM, Sopko G, Bach R, BrooksMM, Bourassa MG, Shemin RJ, Rosen AD, Krone RJ, Frye RL, Feit F.Coronary revascularization in diabetic patients: a comparison of therandomized and observational components of the Bypass AngioplastyRevascularization Investigation (BARI). Circulation. 1999;99:633–640.
41. Eefting F, Nathoe H, van Dijk D, Jansen E, Lahpor J, Stella P, Suyker W,Diephuis J, Suryapranata H, Ernst S, Borst C, Buskens E, Grobbee D, de
Jaegere P. Randomized comparison between stenting and off-pumpbypass surgery in patients referred for angioplasty. Circulation. 2003;108:2870–2876.
42. Morrison DA, Sethi G, Sacks J, Henderson W, Grover F, Sedlis S,Esposito R, Ramanathan K, Weiman D, Saucedo J, Antakli T, ParameshV, Pett S, Vernon S, Birjiniuk V, Welt F, Krucoff M, Wolfe W, Lucke JC,Mediratta S, Booth D, Barbiere C, Lewis D. Percutaneous coronaryintervention versus coronary artery bypass graft surgery for patients withmedically refractory myocardial ischemia and risk factors for adverseoutcomes with bypass: a multicenter, randomized trial: Investigators ofthe Department of Veterans Affairs Cooperative Study #385, the AnginaWith Extremely Serious Operative Mortality Evaluation (AWESOME).J Am Coll Cardiol. 2001;38:143–149.
CLINICAL PERSPECTIVERandomized trials that studied clinical outcome after percutaneous coronary intervention (PCI) with bare metal stentingversus coronary artery bypass grafting (CABG) are underpowered to properly assess safety end points like death, stroke,and myocardial infarction. Pooling data from randomized controlled trials increases the statistical power and allows betterassessment of the treatment effect in high-risk subgroups. The present pooled analysis of 3051 patients in 4 randomizedtrials evaluating the relative safety and efficacy of PCI with stenting and CABG for the treatment of multivessel coronaryartery disease demonstrates that both treatment modalities provided similar long-term safety profiles. At 5 years, thecumulative incidence of death, myocardial infarction, and stroke was similar in patients randomized to PCI with stentingversus CABG (16.7% versus 16.9%, respectively; hazard ratio, 1.04; 95% confidence interval, 0.86 to 1.27; P�0.69).Repeat revascularization, however, occurred significantly more frequently after PCI than CABG (29.0% versus 7.9%,respectively; hazard ratio, 0.23; 95% confidence interval, 0.18 to 0.29; P�0.001). Several large-scale randomized trials likethe Future Revascularization Evaluation in Patients With Diabetes: Optimal Management of Multivessel Disease, andSynergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery are currently comparing the safetyand effectiveness of CABG and PCI with drug-eluting stents. Whether drug-eluting stents will tip the balance betweensafety and efficacy of PCI and CABG is to be examined.
Go to http://cme.ahajournals.org to take the CME quiz for this article.
1154 Circulation September 9, 2008
by guest on January 6, 2015http://circ.ahajournals.org/Downloaded from
Gaston Rodriguez-Granillo, Whady A. Hueb, Pedro A. Lemos and Patrick W. SerruysJoost Daemen, Eric Boersma, Marcus Flather, Jean Booth, Rod Stables, Alfredo Rodriguez,
SoS TrialsMeta-Analysis With 5-Year Patient-Level Data From the ARTS, ERACI-II, MASS-II, and
Coronary Artery Bypass Surgery for Multivessel Coronary Artery Disease: A Long-Term Safety and Efficacy of Percutaneous Coronary Intervention With Stenting and
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2008 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.107.752147
2008;118:1146-1154; originally published online August 25, 2008;Circulation.
http://circ.ahajournals.org/content/118/11/1146World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on January 6, 2015http://circ.ahajournals.org/Downloaded from




















