
Light scattering and light transmittance in a series of calcified single-piece hydrophilic acrylic...
8
Light scattering and light transmittance in a series of calcified single-piece hydrophilic acrylic intraocular lenses of the same design Daniel Barra, MD, Liliana Werner, MD, PhD, Jo~ ao Luiz Pacini Costa, MD, Caleb Morris, BS, Tiago Ribeiro, MD, Bruna Vieira Ventura, MD, F abio Dornelles, MD PURPOSE: To evaluate light scattering and light transmittance of Ioflex hydrophilic acrylic intraoc- ular lenses (IOLs) explanted because of clinically significant opacification secondary to calcification. SETTING: John A. Moran Eye Center, University of Utah, Salt Lake City, Utah, USA. DESIGN: Experimental study. METHODS: Seven explanted and 8 control Ioflex IOLs were studied. Gross and light microscopy of all the IOLs were performed. Light scattering was measured with a Scheimpflug camera, and light transmittance was assessed with a spectrophotometer. Analyses were performed at room temperature in the hydrated state, and findings of the explanted and control IOLs were compared. RESULTS: Light scattering was 219.71 computer compatible tape (CCT) G 2.62 (SD) for explanted IOLs and 4.75 G 2.50 CCT for controls. The mean light transmittance in the visible light spectrum was 75.94% to 87.25% for explanted IOLs and 97.54% to 98.97% for controls. The most striking finding was variable degrees of light transmittance between 290 nm and 350 nm (ultraviolet-A and B radiation) in the explanted and control IOLs with expiration dates in 2009/2010 but 0% transmit- tance in this region in all controls with expiration dates in 2011/2012. CONCLUSIONS: Light scattering was extremely high and transmittance was significantly reduced in calcified IOLs. Differences in transmittance observed in the 290 to 350 nm region between IOLs with different expiration dates were related to use of different hydrophilic acrylic raw material suppliers in the manufacture of the IOLs, highlighting the complexity of IOL calcification investigations. Financial Disclosure: No author has a financial or proprietary interest in any material or method mentioned. J Cataract Refract Surg 2014; 40:121–128 Q 2013 ASCRS and ESCRS Implantation of an intraocular lens (IOL) after cataract surgery has evolved into a very successful procedure since its introduction by Sir Harold Ridley. 1 Despite considerable progress in IOL manufacture, complica- tions related to postoperative optic changes have continually been described in the literature. Calcifica- tion is one of these complications, and its pathogenesis is not yet completely understood. 2,3 Possible contri- butors to the development of postoperative IOL calcification include packaging containing silicone compounds, patient metabolic conditions, surgical techniques, and adjuvants. 2–6 The Ioflex IOL (Mediphacos Ltda.) is a foldable hydrophilic acrylic single-piece IOL with an optic diameter of 5.7 mm and an overall diameter of 12.5 mm. The material used for the IOL is a copolymer of poly(hydroxyethyl methacrylate) with 25% water content. Since its introduction in the Brazilian market in 2001, more than 1.5 million units have been distri- buted in Brazil and other countries. Two recent studies have described opacification resulting from calcifica- tion of the Ioflex IOL. 7–9 According to investigations performed by the manufacturer, the opacification could also be related to the presence of silicone com- pounds found in the packaging of some IOL lots. 2,A In a previous study, 10 we measured light scattering and light transmittance in poly(methyl methacrylate) (PMMA), various hydrophilic acrylic, and silicone IOLs that were explanted because of clinically signifi- cant optic opacification resulting from various patho- logic processes. The present study performed the same measurements in a series of explanted Ioflex Q 2013 ASCRS and ESCRS Published by Elsevier Inc. 0886-3350/$ - see front matter 121 http://dx.doi.org/10.1016/j.jcrs.2013.10.015 LABORATORY SCIENCE
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Light scattering and light transmittance in a series of calcified single-piece hydrophilic acrylic...

LABORATORY SCIENCE
Light scattering and ligh
t transmittance in a seriesof calcified single-piece hydrophilic acrylicintraocular lenses of the same designDaniel Barra, MD, Liliana Werner, MD, PhD, Jo~ao Luiz Pacini Costa, MD, Caleb Morris, BS,
Tiago Ribeiro, MD, Bruna Vieira Ventura, MD, F�abio Dornelles, MD
Q 2013 A
Published
SCRS an
by Elsev
PURPOSE: To evaluate light scattering and light transmittance of Ioflex hydrophilic acrylic intraoc-ular lenses (IOLs) explanted because of clinically significant opacification secondary to calcification.
SETTING: John A. Moran Eye Center, University of Utah, Salt Lake City, Utah, USA.
DESIGN: Experimental study.
METHODS: Seven explanted and 8 control Ioflex IOLs were studied. Gross and light microscopyof all the IOLs were performed. Light scattering was measured with a Scheimpflug camera, andlight transmittance was assessed with a spectrophotometer. Analyses were performed at roomtemperature in the hydrated state, and findings of the explanted and control IOLs were compared.
RESULTS: Light scattering was 219.71 computer compatible tape (CCT)G 2.62 (SD) for explantedIOLs and 4.75 G 2.50 CCT for controls. The mean light transmittance in the visible light spectrumwas 75.94% to 87.25% for explanted IOLs and 97.54% to 98.97% for controls. The most strikingfinding was variable degrees of light transmittance between 290 nm and 350 nm (ultraviolet-A and Bradiation) in the explanted and control IOLs with expiration dates in 2009/2010 but 0% transmit-tance in this region in all controls with expiration dates in 2011/2012.
CONCLUSIONS: Light scattering was extremely high and transmittance was significantly reduced incalcified IOLs. Differences in transmittance observed in the 290 to 350 nm region between IOLs withdifferent expiration dates were related to use of different hydrophilic acrylic raw material suppliersin the manufacture of the IOLs, highlighting the complexity of IOL calcification investigations.
Financial Disclosure: No author has a financial or proprietary interest in any material or methodmentioned.
J Cataract Refract Surg 2014; 40:121–128 Q 2013 ASCRS and ESCRS
Implantation of an intraocular lens (IOL) after cataractsurgery has evolved into a very successful proceduresince its introduction by Sir Harold Ridley.1 Despiteconsiderable progress in IOL manufacture, complica-tions related to postoperative optic changes havecontinually been described in the literature. Calcifica-tion is one of these complications, and its pathogenesisis not yet completely understood.2,3 Possible contri-butors to the development of postoperative IOLcalcification include packaging containing siliconecompounds, patient metabolic conditions, surgicaltechniques, and adjuvants.2–6
The Ioflex IOL (Mediphacos Ltda.) is a foldablehydrophilic acrylic single-piece IOL with an opticdiameter of 5.7 mm and an overall diameter of12.5 mm. The material used for the IOL is a copolymer
d ESCRS
ier Inc.
of poly(hydroxyethyl methacrylate) with 25% watercontent. Since its introduction in the Brazilian marketin 2001, more than 1.5 million units have been distri-buted in Brazil and other countries. Two recent studieshave described opacification resulting from calcifica-tion of the Ioflex IOL.7–9 According to investigationsperformed by the manufacturer, the opacificationcould also be related to the presence of silicone com-pounds found in the packaging of some IOL lots.2,A
In a previous study,10 we measured light scatteringand light transmittance in poly(methyl methacrylate)(PMMA), various hydrophilic acrylic, and siliconeIOLs that were explanted because of clinically signifi-cant optic opacification resulting from various patho-logic processes. The present study performed thesame measurements in a series of explanted Ioflex
0886-3350/$ - see front matter 121http://dx.doi.org/10.1016/j.jcrs.2013.10.015
122 LABORATORY SCIENCE: LIGHT SCATTERING AND TRANSMITTANCE IN CALCIFIED IOLS
IOLs to obtain a more comprehensive assessment andcharacterization of the opacification process in thisIOL design.
MATERIALS AND METHODS
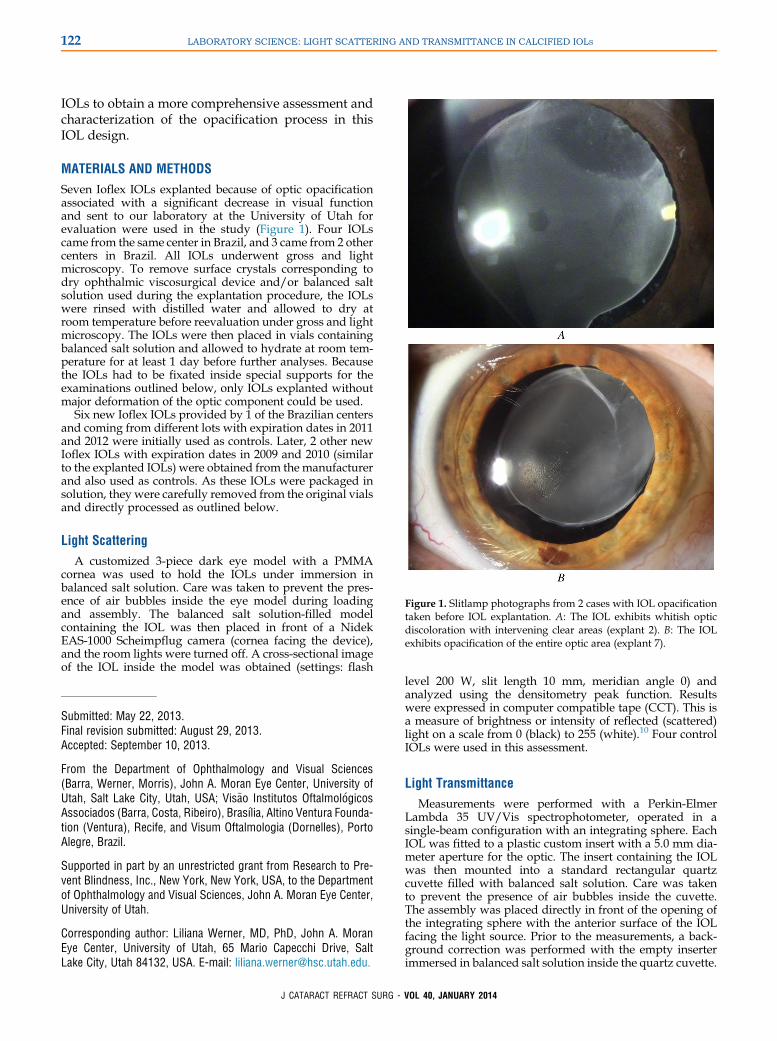
Seven Ioflex IOLs explanted because of optic opacificationassociated with a significant decrease in visual functionand sent to our laboratory at the University of Utah forevaluation were used in the study (Figure 1). Four IOLscame from the same center in Brazil, and 3 came from 2 othercenters in Brazil. All IOLs underwent gross and lightmicroscopy. To remove surface crystals corresponding todry ophthalmic viscosurgical device and/or balanced saltsolution used during the explantation procedure, the IOLswere rinsed with distilled water and allowed to dry atroom temperature before reevaluation under gross and lightmicroscopy. The IOLs were then placed in vials containingbalanced salt solution and allowed to hydrate at room tem-perature for at least 1 day before further analyses. Becausethe IOLs had to be fixated inside special supports for theexaminations outlined below, only IOLs explanted withoutmajor deformation of the optic component could be used.
Six new Ioflex IOLs provided by 1 of the Brazilian centersand coming from different lots with expiration dates in 2011and 2012 were initially used as controls. Later, 2 other newIoflex IOLs with expiration dates in 2009 and 2010 (similarto the explanted IOLs) were obtained from the manufacturerand also used as controls. As these IOLs were packaged insolution, they were carefully removed from the original vialsand directly processed as outlined below.
Light Scattering
Figure 1. Slitlamp photographs from 2 cases with IOL opacificationtaken before IOL explantation. A: The IOL exhibits whitish opticdiscoloration with intervening clear areas (explant 2). B: The IOLexhibits opacification of the entire optic area (explant 7).
A customized 3-piece dark eye model with a PMMAcornea was used to hold the IOLs under immersion inbalanced salt solution. Care was taken to prevent the pres-ence of air bubbles inside the eye model during loadingand assembly. The balanced salt solution-filled modelcontaining the IOL was then placed in front of a NidekEAS-1000 Scheimpflug camera (cornea facing the device),and the room lights were turned off. A cross-sectional imageof the IOL inside the model was obtained (settings: flash
Submitted: May 22, 2013.Final revision submitted: August 29, 2013.Accepted: September 10, 2013.
From the Department of Ophthalmology and Visual Sciences(Barra, Werner, Morris), John A. Moran Eye Center, University ofUtah, Salt Lake City, Utah, USA; Vis~ao Institutos Oftalmol�ogicosAssociados (Barra, Costa, Ribeiro), Bras�ılia, Altino Ventura Founda-tion (Ventura), Recife, and Visum Oftalmologia (Dornelles), PortoAlegre, Brazil.
Supported in part by an unrestricted grant from Research to Pre-vent Blindness, Inc., New York, New York, USA, to the Departmentof Ophthalmology and Visual Sciences, John A. Moran Eye Center,University of Utah.
Corresponding author: Liliana Werner, MD, PhD, John A. MoranEye Center, University of Utah, 65 Mario Capecchi Drive, SaltLake City, Utah 84132, USA. E-mail: [email protected].
J CATARACT REFRACT SURG -
level 200 W, slit length 10 mm, meridian angle 0) andanalyzed using the densitometry peak function. Resultswere expressed in computer compatible tape (CCT). This isa measure of brightness or intensity of reflected (scattered)light on a scale from 0 (black) to 255 (white).10 Four controlIOLs were used in this assessment.
Light Transmittance
Measurements were performed with a Perkin-ElmerLambda 35 UV/Vis spectrophotometer, operated in asingle-beam configuration with an integrating sphere. EachIOL was fitted to a plastic custom insert with a 5.0 mm dia-meter aperture for the optic. The insert containing the IOLwas then mounted into a standard rectangular quartzcuvette filled with balanced salt solution. Care was takento prevent the presence of air bubbles inside the cuvette.The assembly was placed directly in front of the opening ofthe integrating sphere with the anterior surface of the IOLfacing the light source. Prior to the measurements, a back-ground correction was performed with the empty inserterimmersed in balanced salt solution inside the quartz cuvette.
VOL 40, JANUARY 2014
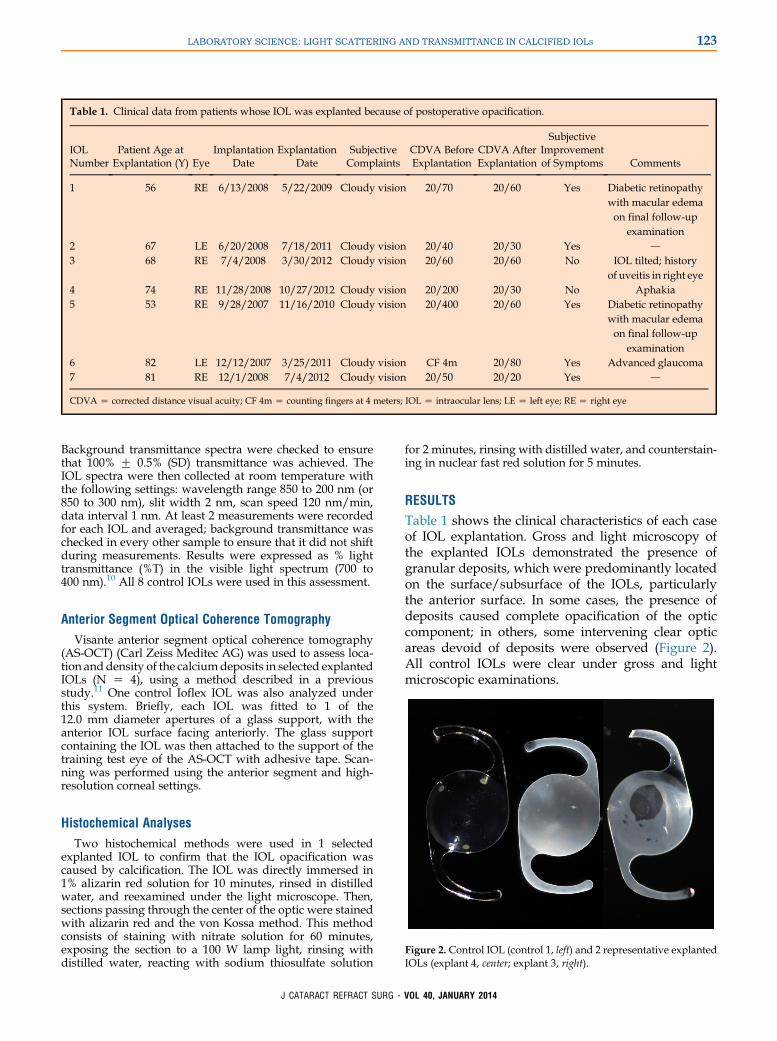
Table 1. Clinical data from patients whose IOL was explanted because of postoperative opacification.
IOLNumber
Patient Age atExplantation (Y) Eye
ImplantationDate
ExplantationDate
SubjectiveComplaints
CDVA BeforeExplantation
CDVA AfterExplantation
SubjectiveImprovementof Symptoms Comments
1 56 RE 6/13/2008 5/22/2009 Cloudy vision 20/70 20/60 Yes Diabetic retinopathywith macular edemaon final follow-up
examination2 67 LE 6/20/2008 7/18/2011 Cloudy vision 20/40 20/30 Yes d
3 68 RE 7/4/2008 3/30/2012 Cloudy vision 20/60 20/60 No IOL tilted; historyof uveitis in right eye
4 74 RE 11/28/2008 10/27/2012 Cloudy vision 20/200 20/30 No Aphakia5 53 RE 9/28/2007 11/16/2010 Cloudy vision 20/400 20/60 Yes Diabetic retinopathy
with macular edemaon final follow-up
examination6 82 LE 12/12/2007 3/25/2011 Cloudy vision CF 4m 20/80 Yes Advanced glaucoma7 81 RE 12/1/2008 7/4/2012 Cloudy vision 20/50 20/20 Yes d
CDVA Z corrected distance visual acuity; CF 4m Z counting fingers at 4 meters; IOL Z intraocular lens; LE Z left eye; RE Z right eye
123LABORATORY SCIENCE: LIGHT SCATTERING AND TRANSMITTANCE IN CALCIFIED IOLS
Background transmittance spectra were checked to ensurethat 100% G 0.5% (SD) transmittance was achieved. TheIOL spectra were then collected at room temperature withthe following settings: wavelength range 850 to 200 nm (or850 to 300 nm), slit width 2 nm, scan speed 120 nm/min,data interval 1 nm. At least 2 measurements were recordedfor each IOL and averaged; background transmittance waschecked in every other sample to ensure that it did not shiftduring measurements. Results were expressed as % lighttransmittance (%T) in the visible light spectrum (700 to400 nm).10 All 8 control IOLs were used in this assessment.
Anterior Segment Optical Coherence Tomography
Visante anterior segment optical coherence tomography(AS-OCT) (Carl Zeiss Meditec AG) was used to assess loca-tion and density of the calciumdeposits in selected explantedIOLs (N Z 4), using a method described in a previousstudy.11 One control Ioflex IOL was also analyzed underthis system. Briefly, each IOL was fitted to 1 of the12.0 mm diameter apertures of a glass support, with theanterior IOL surface facing anteriorly. The glass supportcontaining the IOL was then attached to the support of thetraining test eye of the AS-OCT with adhesive tape. Scan-ning was performed using the anterior segment and high-resolution corneal settings.
Histochemical Analyses
Figure 2. Control IOL (control 1, left) and 2 representative explantedIOLs (explant 4, center; explant 3, right).
Two histochemical methods were used in 1 selectedexplanted IOL to confirm that the IOL opacification wascaused by calcification. The IOL was directly immersed in1% alizarin red solution for 10 minutes, rinsed in distilledwater, and reexamined under the light microscope. Then,sections passing through the center of the optic were stainedwith alizarin red and the von Kossa method. This methodconsists of staining with nitrate solution for 60 minutes,exposing the section to a 100 W lamp light, rinsing withdistilled water, reacting with sodium thiosulfate solution
J CATARACT REFRACT SURG -
for 2 minutes, rinsing with distilled water, and counterstain-ing in nuclear fast red solution for 5 minutes.
RESULTS
Table 1 shows the clinical characteristics of each caseof IOL explantation. Gross and light microscopy ofthe explanted IOLs demonstrated the presence ofgranular deposits, which were predominantly locatedon the surface/subsurface of the IOLs, particularlythe anterior surface. In some cases, the presence ofdeposits caused complete opacification of the opticcomponent; in others, some intervening clear opticareas devoid of deposits were observed (Figure 2).All control IOLs were clear under gross and lightmicroscopic examinations.
VOL 40, JANUARY 2014
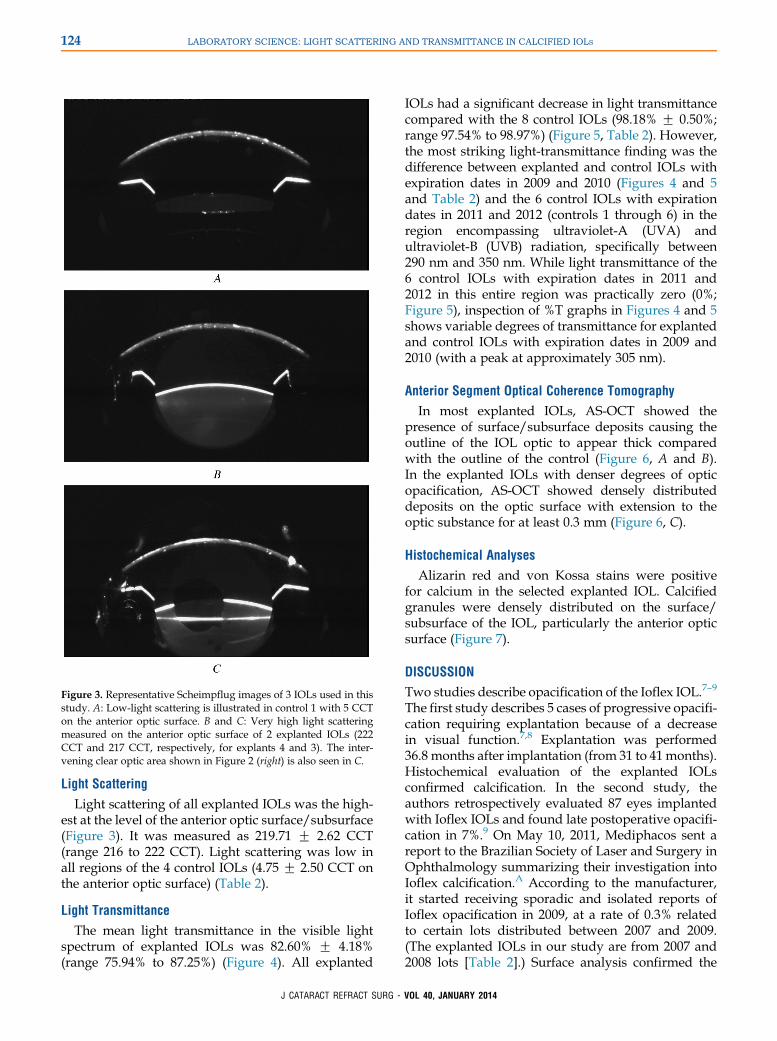
Figure 3. Representative Scheimpflug images of 3 IOLs used in thisstudy. A: Low-light scattering is illustrated in control 1 with 5 CCTon the anterior optic surface. B and C: Very high light scatteringmeasured on the anterior optic surface of 2 explanted IOLs (222CCT and 217 CCT, respectively, for explants 4 and 3). The inter-vening clear optic area shown in Figure 2 (right) is also seen in C.
124 LABORATORY SCIENCE: LIGHT SCATTERING AND TRANSMITTANCE IN CALCIFIED IOLS
Light Scattering
Light scattering of all explanted IOLs was the high-est at the level of the anterior optic surface/subsurface(Figure 3). It was measured as 219.71 G 2.62 CCT(range 216 to 222 CCT). Light scattering was low inall regions of the 4 control IOLs (4.75 G 2.50 CCT onthe anterior optic surface) (Table 2).
Light Transmittance
The mean light transmittance in the visible lightspectrum of explanted IOLs was 82.60% G 4.18%(range 75.94% to 87.25%) (Figure 4). All explanted
J CATARACT REFRACT SURG -
IOLs had a significant decrease in light transmittancecompared with the 8 control IOLs (98.18% G 0.50%;range 97.54% to 98.97%) (Figure 5, Table 2). However,the most striking light-transmittance finding was thedifference between explanted and control IOLs withexpiration dates in 2009 and 2010 (Figures 4 and 5and Table 2) and the 6 control IOLs with expirationdates in 2011 and 2012 (controls 1 through 6) in theregion encompassing ultraviolet-A (UVA) andultraviolet-B (UVB) radiation, specifically between290 nm and 350 nm. While light transmittance of the6 control IOLs with expiration dates in 2011 and2012 in this entire region was practically zero (0%;Figure 5), inspection of %T graphs in Figures 4 and 5shows variable degrees of transmittance for explantedand control IOLs with expiration dates in 2009 and2010 (with a peak at approximately 305 nm).
Anterior Segment Optical Coherence Tomography
In most explanted IOLs, AS-OCT showed thepresence of surface/subsurface deposits causing theoutline of the IOL optic to appear thick comparedwith the outline of the control (Figure 6, A and B).In the explanted IOLs with denser degrees of opticopacification, AS-OCT showed densely distributeddeposits on the optic surface with extension to theoptic substance for at least 0.3 mm (Figure 6, C).
Histochemical Analyses
Alizarin red and von Kossa stains were positivefor calcium in the selected explanted IOL. Calcifiedgranules were densely distributed on the surface/subsurface of the IOL, particularly the anterior opticsurface (Figure 7).
DISCUSSION
Two studies describe opacification of the Ioflex IOL.7–9
The first study describes 5 cases of progressive opacifi-cation requiring explantation because of a decreasein visual function.7,8 Explantation was performed36.8 months after implantation (from 31 to 41months).Histochemical evaluation of the explanted IOLsconfirmed calcification. In the second study, theauthors retrospectively evaluated 87 eyes implantedwith Ioflex IOLs and found late postoperative opacifi-cation in 7%.9 On May 10, 2011, Mediphacos sent areport to the Brazilian Society of Laser and Surgery inOphthalmology summarizing their investigation intoIoflex calcification.A According to the manufacturer,it started receiving sporadic and isolated reports ofIoflex opacification in 2009, at a rate of 0.3% relatedto certain lots distributed between 2007 and 2009.(The explanted IOLs in our study are from 2007 and2008 lots [Table 2].) Surface analysis confirmed the
VOL 40, JANUARY 2014

Table 2. Surface light scattering and light transmittance of IOLs included in the study.
IOL Serial Number Lot Expiration Date Light Scattering (CCT) % T
Explant 1 080401380126700019686 E0812906 12/05/2010 216 78.42264074Explant 2 080301480126300014553 G0818459 18/07/2010 221 83.80042707Explant 3 080301480126300014552 G0818459 18/07/2010 217 85.49597249Explant 4 080700280126600030560 C0807215 07/03/2010 222 87.25728315Explant 5 070700830126100012194 J0729351 29/10/2009 222 81.48994182Explant 6 071000780126300010383 G0824531 24/07/2010 222 85.81662468Explant 7 080501420126500013046 F0827825 27/06/2010 218 75.94432882Control 1 0000027175 K092301 11/23/2011 5 98.97091734Control 2 0000027174 K092301 11/23/2011 8 98.24288611Control 3 0000036815 H090705 08/30/2011 NM 98.12172529Control 4 0000280040 K092605 11/26/2011 NM 97.54277189Control 5 0000040757 J092205 12/30/2011 NM 97.83966871Control 6 0000034696 C102401 03/30/2012 NM 97.62428945Control 7 071001910129400000979 K0729195 November 2009 2 98.60748267Control 8 080600400129500004667 G0810328 July 2010 4 98.56371685
CCT Z computer-compatible tape; IOL Z intraocular lens; NM Z not measured; %T Z % light transmittance in the visible light spectrum (700-400 nm)
125LABORATORY SCIENCE: LIGHT SCATTERING AND TRANSMITTANCE IN CALCIFIED IOLS
presence of calcium/phosphate precipitation, as wellas the presence of poly(dimethyl siloxane) on the sur-faces of the analyzed IOLs. Poly(dimethyl siloxane)was found to come from the packaging of the IOLlots manufactured during the period in question. Themanufacturer withdrew the IOLs from those lotsfrom the market, and the packaging was changed in2010.A Since this change, the manufacturer has distrib-uted more than 400 000 IOLs, which currently have aclinical follow-up of up to 3 years with no reports ofcalcification.
In our series of 7 explanted IOLs, the opacificationwas caused by the presence of calcified deposits onthe optic surface/subsurface primarily, as confirmed
Figure 4. Percentage of light transmittance between 850 nm and200 nm in 4 IOLs explanted in the same center in Brazil because oflate postoperative opacification (explants 1 through 4).
J CATARACT REFRACT SURG -
by the AS-OCT and by microscopic findings beforeand after histochemical staining. This pattern is similarto that described in the previous studies with thissame IOL design.7–9 Light scattering due to calcifica-tion of the Ioflex IOLs was high in this study(219.71 G 2.62 CCT). On average, these values werehigher than those obtained in a previous study inwhich other types of hydrophilic acrylic IOLsexhibited a similar pattern of calcification (200.54 G49.58 CCT).10 The decrease in average % light trans-mittance in the visible light spectrum due to the calci-fication was significant (82.60% G 4.18%) and moresignificant on average than the decrease in other calci-fied IOLs (90.31% G 5.10%).10
Figure 5. Percentage of light transmittance between 850 nm and200 nm in the 8 control Ioflex IOLs. The curves of control IOLsnumber 7 and 8 (with expiration dates in 2009/2010) differ fromthe other controls (with expiration dates in 2011/2012) in the regionencompassing UVA and UVB radiation.
VOL 40, JANUARY 2014

Figure 6.Anterior segmentOCTof representative IOLs.A: Control 1;the outline of the optic surface is thin. B: Explant 2; the outline of theoptic surface is thicker than inA. C: Explant 4; besides a thick outlineof the optic surface, the scan shows deposits/granules denselydistributed within the optic substance.
126 LABORATORY SCIENCE: LIGHT SCATTERING AND TRANSMITTANCE IN CALCIFIED IOLS
The most striking finding of the present study wasthe difference between explanted and control IOLs(controls 7 and 8) with expiration dates in 2009 and2010 and the 6 control IOLs with expiration dates in2011 and 2012 (controls 1 through 6) in the region be-tween 290 nm and 350 nm (Figures 4 and 5, Table 2).The natural crystalline lens absorbs a large portion ofthe UVA and UVB spectra, up to 390 nm in the youngeye and up to 400 nm in a 63-year-old lens.12 Therefore,UV absorber molecules have been incorporated intoIOLs manufactured from different materials.13–15 Inour study, while light transmittance of the 6 controlIOLs with expiration dates in 2011 and 2012 in theentire region between 290 nm and 350 nm was practi-cally 0% (Figure 5), inspection of %T graphs inFigures 4 and 5 showed variable degrees of transmit-tance in explanted and control IOLs with expirationdates in 2009 and 2010 (with a peak at approximately305 nm). In our previous study comparing light scat-tering and light transmittance of opacified IOLs andnonopacified controls, although light transmittancewas also decreased in calcified hydrophilic acrylic
J CATARACT REFRACT SURG -
IOLs, no design exhibited this alteration in the lighttransmittance curves; this alteration was also notfound in any of the control hydrophilic acrylic IOLsused.10 Figure 8 shows representative curves of 4different hydrophilic acrylic IOL designs explantedbecause of calcification and analyzed in our previousstudy. The curves were obtained using the methodol-ogy and equipment described in the current study.10
We initially hypothesized that this alteration mightrepresent a form of degradation of the UV absorberused in the Ioflex design, as it was observed in IOLswith earlier expiration dates (2009/2010 versus2011/2012), and the level of transmittance in the 290to 350 nm region was variable among the IOLs.Further studies are necessary to confirm this hypothe-sis. Studies should include techniques to evaluate thechemical composition of the IOLs, such as Fouriertransform infrared spectroscopy.16 Ideally, never-used Ioflex IOLs should also undergo a process ofin vitro accelerated aging by immersion in balancedsalt solution at high temperatures with subsequent an-alyses of light transmittance as well as gas and liquidchromatography to determine whether any moleculesare leaching out or degrading over time.17 However,according to the manufacturer, in the period 2007and 2008, 2 hydrophilic acrylic raw material supplierswere used to manufacture the Ioflex IOLs. Thebehavior of the IOLs manufactured from the 2different raw material sources is depicted under UV/Vis spectrophotometry in Figure 5; 1 group is repre-sented by control numbers 1 through 6 and the secondgroup is represented by control numbers 7 and 8. Itappears that all explanted IOLs in this current studywere manufactured from the material in the secondgroup. We also speculated whether this alterationhad any relationship with the calcification process ofthis IOL design, but according to the manufacturer,there were cases of Ioflex calcification with bothtypes of raw materials.B A previous study of opacifiedhydrophilic acrylic IOLs suggests premature agingof the UV-light filter.18 Frohn et al.18 analyzed 41SC60B-OUV IOLs using different techniques,including light microscopy, high performance liquidchromatography, sodium dodecyl sulfate polyacryl-amide gel electrophoresis, and spectrometric analysis.The latter yielded alterations in the UV spectral range.In our previous study, 6 of the 22 calcified IOLs werealso of the SC60B-OUV design. However, we did notfind any alteration in the UV spectral range of the lighttransmittance curves of those IOLs (an example isshown in Figure 8).10
In conclusion, we describe the findings of 7 cases ofcalcification of Ioflex hydrophilic acrylic IOLs. Levelsof light scattering were extremely high and light trans-mittance was significantly reduced in all IOLs
VOL 40, JANUARY 2014
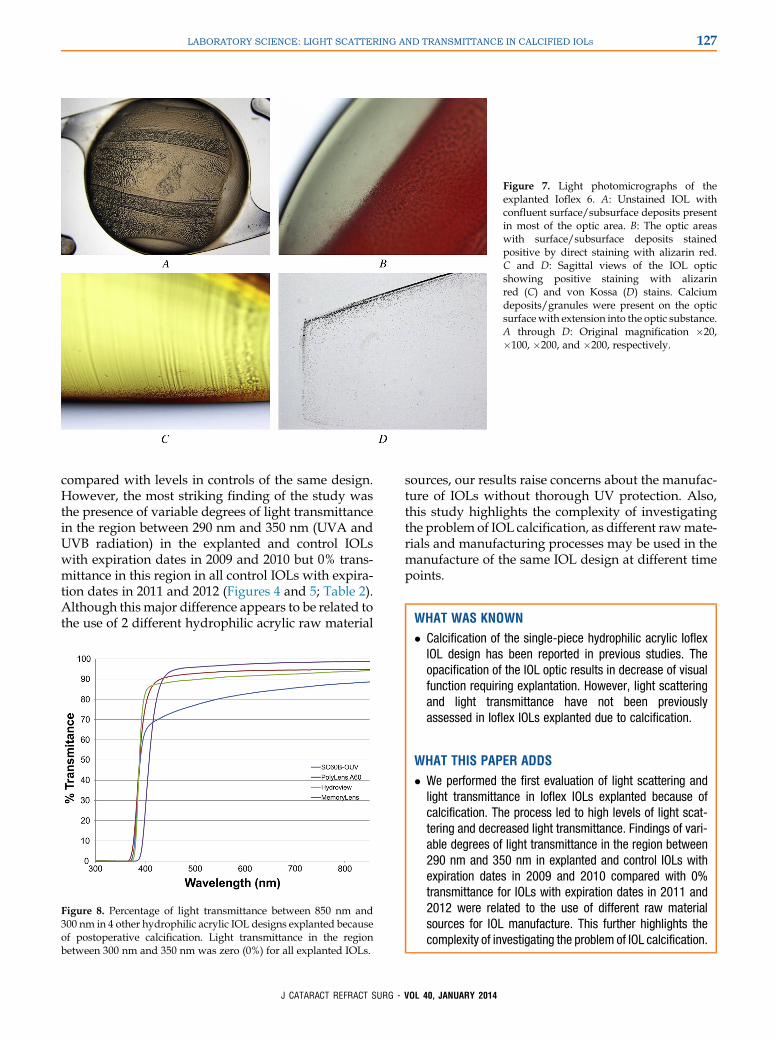
Figure 7. Light photomicrographs of theexplanted Ioflex 6. A: Unstained IOL withconfluent surface/subsurface deposits presentin most of the optic area. B: The optic areaswith surface/subsurface deposits stainedpositive by direct staining with alizarin red.C and D: Sagittal views of the IOL opticshowing positive staining with alizarinred (C) and von Kossa (D) stains. Calciumdeposits/granules were present on the opticsurfacewith extension into the optic substance.A through D: Original magnification �20,�100, �200, and �200, respectively.
127LABORATORY SCIENCE: LIGHT SCATTERING AND TRANSMITTANCE IN CALCIFIED IOLS
compared with levels in controls of the same design.However, the most striking finding of the study wasthe presence of variable degrees of light transmittancein the region between 290 nm and 350 nm (UVA andUVB radiation) in the explanted and control IOLswith expiration dates in 2009 and 2010 but 0% trans-mittance in this region in all control IOLs with expira-tion dates in 2011 and 2012 (Figures 4 and 5; Table 2).Although this major difference appears to be related tothe use of 2 different hydrophilic acrylic raw material
Figure 8. Percentage of light transmittance between 850 nm and300 nm in 4 other hydrophilic acrylic IOL designs explanted becauseof postoperative calcification. Light transmittance in the regionbetween 300 nm and 350 nm was zero (0%) for all explanted IOLs.
J CATARACT REFRACT SURG -
sources, our results raise concerns about the manufac-ture of IOLs without thorough UV protection. Also,this study highlights the complexity of investigatingthe problem of IOL calcification, as different rawmate-rials and manufacturing processes may be used in themanufacture of the same IOL design at different timepoints.
VO
WHAT WAS KNOWN
� Calcification of the single-piece hydrophilic acrylic IoflexIOL design has been reported in previous studies. Theopacification of the IOL optic results in decrease of visualfunction requiring explantation. However, light scatteringand light transmittance have not been previouslyassessed in Ioflex IOLs explanted due to calcification.
WHAT THIS PAPER ADDS
� We performed the first evaluation of light scattering andlight transmittance in Ioflex IOLs explanted because ofcalcification. The process led to high levels of light scat-tering and decreased light transmittance. Findings of vari-able degrees of light transmittance in the region between290 nm and 350 nm in explanted and control IOLs withexpiration dates in 2009 and 2010 compared with 0%transmittance for IOLs with expiration dates in 2011 and2012 were related to the use of different raw materialsources for IOL manufacture. This further highlights thecomplexity of investigating the problem of IOL calcification.
L 40, JANUARY 2014

128 LABORATORY SCIENCE: LIGHT SCATTERING AND TRANSMITTANCE IN CALCIFIED IOLS
REFERENCES1. Apple DJ. Harold Ridley, MA, MD, FRCS: a golden anniversary
celebration and a golden age [editorial]. Arch Ophthalmol 1999;
117:827–828
2. Werner L. Causes of intraocular lens opacification or discolor-
ation. J Cataract Refract Surg 2007; 33:713–726
3. Werner L. Calcification of hydrophilic acrylic intraocular lenses
[editorial]. Am J Ophthalmol 2008; 146:341–343
4. Werner L, Apple DJ, Escobar-Gomez M, €Ohrstr€om A,
Crayford BB, Bianchi R, Pandey SK. Postoperative deposition
of calcium on the surfaces of a hydrogel intraocular lens.
Ophthalmology 2000; 107:2179–2185
5. Werner L, Apple DJ, Kaskaloglu M, Pandey SK. Dense opacifi-
cation of the optical component of a hydrophilic acrylic intraoc-
ular lens; a clinicopathological analysis of 9 explanted lenses.
J Cataract Refract Surg 2001; 27:1485–1492
6. Werner L, Hunter B, Stevens S, Chew JJ, Mamalis N. Role of sil-
icon contamination on calcification of hydrophilic acrylic intraoc-
ular lenses. Am J Ophthalmol 2006; 141:35–43
7. Ventura BV, Ventura M, Lira W, Ventura CV, Santhiago MR,
Werner L. Microscopic analysis of opacification in Ioflex� hydro-
philic acrylic intraocular lenses. Rev Bras Oftalmol 2012;
71:149–154. Available at: http://www.scielo.br/pdf/rbof/v71n3/
a02v71n3.pdf. Accessed October 5, 2013
8. Ventura BV, Ventura M, Werner L, Santhiago MR. Calcium de-
posits on hydrophilic acrylic intraocular lenses. J Cataract
Refract Surg 2013; 39:142–143
9. De Almeida Jorge P, Jorge D, Ventura CV, Ventura BV, Lira W,
VenturaMC,Werner L, Kara-Junior N. Late opacification in hydro-
philic acrylic intraocular lenses: analysis of 87 eyes in a random
sample of 102patients. JCataractRefract Surg 2013; 39:403–407
10. Michelson J, Werner L, Ollerton A, Leishman L, Bodnar Z. Light
scattering and light transmittance in intraocular lenses explanted
because of optic opacification. J Cataract Refract Surg 2012;
38:1476–1485
11. Werner L, Michelson J, Ollerton A, Leishman L, Bodnar Z. Ante-
rior segment optical coherence tomography in the assessment
of postoperative intraocular lens optic changes. J Cataract
Refract Surg 2012; 38:1077–1085
J CATARACT REFRACT SURG -
12. Boettner EA, Wolter JR. Transmission of the ocular media.
Invest Ophthalmol 1962; 1:776–783. Available at: http://www.
iovs.org/cgi/reprint/1/6/776.pdf. Accessed October 5, 2013
13. Ernest PH. Light-transmission-spectrum comparison of fold-
able intraocular lenses. J Cataract Refract Surg 2004;
30:1755–1758
14. Tanito M, Okuno T, Ishiba Y, Ohira A. Transmission spectrums
and retinal blue-light irradiance values of untinted and yellow-
tinted intraocular lenses. J Cataract Refract Surg 2010;
36:299–307
15. Laube T, Apel H, Koch H-R. Ultraviolet radiation absorption of
intraocular lenses. Ophthalmology 2004; 111:880–885
16. Ong MD, Callaghan TA, Pei R, Karakelle M. Etiology of surface
light scattering on hydrophobic acrylic intraocular lenses.
J Cataract Refract Surg 2012; 38:1833–1844
17. Yang S, Makker H, Christ FR. Accelerated ultraviolet aging of
intraocular lens optic materials: a 50 year simulation.
J Cataract Refract Surg 1997; 23:940–947
18. Frohn A, Dick HB, Augustin AJ, Grus FH. Late opacification of
the foldable hydrophilic acrylic lens SC60B-OUV. Ophthal-
mology 2001; 108:1999–2004
OTHER CITED MATERIALA. Soares M, “Nota de Esclarecimento,” report sent on May 10,
2011 to the Brazilian Society of Laser and Surgery in Ophthal-
mology. Available from Dr. Werner.
B. Ana Paula Castro, Mediphacos Ltda. E-mail communication
June 13, 2013
VOL
40, JANUARY 2014First author:Daniel Barra, MD
Department of Ophthalmology andVisual Sciences, John A. Moran EyeCenter, University of Utah, Salt LakeCity, Utah, USA



















