
Lasers on the skin - a book chapter
32
Use of The Laser in Facial Plastic Surgery Mr Mike G Dilkes MS, FRCSEd, FRCS, FRCS(ORL-HNS). Consultant Ear Nose and Throat Surgeon St. Bartholomew’s Hospital, London EC1Y 0DT, UK. Chapters 1) History 2) Physics 3) Lasers used in Facial Plastics 4) Clinical areas in Facial Plastics where the laser is effective. 5) Pigmentation problems 6) Safety 7) References 1) History Light has been used as a therapeutic tool for the skin since the Finsen lamp was invented in 1899, when it was used initially for Lupus Vulgaris. In 1901 an ultraviolet lamp was used to treat Rickets, and scar tissue, followed by PUVA treatment for Psoriasis in 1925. It was therefore natural that skin became the first area where lasers were used. Lasers were first used on the skin soon after Maiman’s breakthrough at
Transcript of Lasers on the skin - a book chapter
Use of The Laser in Facial Plastic Surgery
Mr Mike G Dilkes MS, FRCSEd, FRCS, FRCS(ORL-HNS).
Consultant Ear Nose and Throat Surgeon
St. Bartholomew’s Hospital, London EC1Y 0DT, UK.
Chapters
1) History
2) Physics
3) Lasers used in Facial Plastics
4) Clinical areas in Facial Plastics where the laser is effective.
5) Pigmentation problems
6) Safety
7) References
1) History
Light has been used as a therapeutic tool for the skin since the
Finsen lamp was invented in 1899, when it was used initially for Lupus
Vulgaris. In 1901 an ultraviolet lamp was used to treat Rickets, and
scar tissue, followed by PUVA treatment for Psoriasis in 1925. It
was therefore natural that skin became the first area where lasers
were used.
Lasers were first used on the skin soon after Maiman’s breakthrough at

Massachusetts Institue of Technology in 1960(1), when the Ruby laser
became the first laser ever produced. Leon Goldman was a dermatologist
in Cincinnati, and he heard early on about Maiman’s work. He had the
vision to set up a biomedical laser laboratory at the University of
Cincinnati in 1961. At the time the Ruby laser was the only system
available, and although good results were seen on a variety of skin
conditions, there was too much scarring found to establish this as a
mainstay of skin treatment(2). In 1964 the Carbon Dioxide laser,
highly absorbed by water, was made available, and this allowed tissue
such as skin to be cut in a bloodless manner. The same year the Argon
laser also appeared, and this was preferentially absorbed by
haemoglobin, leading to work on port wine stains and other skin
vascular lesions. At the same time this laser was also developed by
Ophthalmic surgeons to successfully treat neovascularisation of the
retina, without damaging eyesight, which was a major breakthrough(3).
The next big step for skin laser treatment was with the advent of Q-
switched lasers(4), in particular the q switched Nd-YAG laser.This was
able to produce ultra short pulses of light in the giga watt range of
peak energy. Tattoo destruction became possible because ink pigment
absorbed well at this wavelength, so producing superheated water and
plasma wave formation, which could disrupt the tattoo and lead to its
dissolution. Q switching was invented in 1961, but it was not used
clinically until 1967, although the Nd-YAG laser had been produced in
1964.
During the 1970’s all of these systems were extensively used on
dermatological patients, with varying degrees of success, the use of
the Nd-YAG laser in angioma treatment being published, again by
Goldman, in 1973. The next major breakthrough came in the early
1980’s, when Anderson and Parrish published their theory of Selective
Photothermolysis(5). At the same time the pulsed dye laser was
produced, and this led to much more successful treatment of skin
vascular lesions, and spawned the development of other long pulse
systems such as the KTP (potassium titanyl phosphate - a frequency
doubling crystal used with Nd-YAG), Alexandrite, and long pulse Ruby.
These systems allowed the selective treatment of hair follicles, and
led to laser hair removal, approved by the FDA in 1989(6). More than
25 years after it had become the first laser ever created, the Ruby
resurfaced as the first laser licenced for this application by the
FDA.
Flash scanner technology, mainly used with the Carbon Dioxide laser,
was also invented in the late 1980’s and this allowed safe non
scarring laser skin resurfacing and skin blemish vapourisation(7). The
advent of the Erbium-YAG laser in 1996 led to fractional
photothermolysis and fractional skin resurfacing for lines and
wrinkles.
From the mid 1970’s onwards, an additional technique, Photodynamic
Therapy, was developed, and was initially used in urology and head
and neck cancer, newer more powerful photosensitising drugs making
treatment more effective(8). Development of this technique for skin
has created a large workload in skin premalignancy and malignancy.

2) Physics
Maiman produced the first ever laser in 1960, following its
postulation in 1916’s theory of stimulated emission by Einstein(9).
Maiman’s was a Ruby laser, producing photons of 694 nanometres (nm)
wavelength. There are many different types of laser, all producing
different wavelength (colour) of light. Table 1 is not an exhaustive
list, but demonstrates the range of wavelengths available, from 193nm
to 10,600 nm. The name of the laser tends to be called after the
lasing medium, ie the substance that is creating the laser light, such
as Carbon Dioxide (CO2). Not all compounds can be lasing media, there
is a unique property of lasing compounds that others do not have. This
is the ability to maintain a metastable state when excited.
The acronym LASER stands for light amplification by the stimulated
emission of radiation. This means that a situation is created where
stimulated emission can occur - which is when more than half of the
photons in a population are in their excited state, and by being
metastable they are able to stay there. Stimulated emission itself is
a physical situation whereby photons spontaneously emitted as an
excited atom returns to its ground state (after Plank’s law that
energy is constant - ie if an excited, energised atom returns to a
lower energy state, then the energy difference must be emitted as
something exactly equal, such as a photon in this case), then the
emitted photon can interact with other excited atoms and produce its
own identical clone - one photon stimulates the emission of another.

If this process occurs inside an optical cavity, where there is a
cylinder containing the lasing medium, and two mirrors at either end,
both exactly lined up with each other, then those photons produced
directly in line with the mirrors will bounce back and forwards
between the mirrors, stimulating their clones to be produced by
stimulated emission, all happening at the speed of light, such that
very quickly there are billions of identical photons oscillating
between the 2 mirrors. If one mirror is then made fractionally less
than 100% reflecting, ie allowing some photons to escape through a
small 99.7% reflecting area, you suddenly have an external beam of
light - a laser beam.
This light beam will have these 3 very useful properties, ones that
separate it from non-laser light sources, even high intensity ones:
1) The light will be monochromatic - which means the same colour, or
the same wavelength. This is very important when using the principle
of selective photothermolysis (see later) to treat hair or vascular
anomalies.
2) The light will be coherent - which means all the photons will be in
phase, and more importantly for medical applications, the photons will
be collimated - in parallel with each other. This means that if the
laser light is shone onto a high quality lens, the entire light beam
can be focussed onto a tiny spot, measured in microns, giving
extremely high energy densities. This is very useful in techniques
using the principle of thermal relaxation (see later), such as laser
skin resurfacing.
3) The light is high intensity, due to the amplification process (see
above). Extremely high intensity pulses can be produced by using Q
(quality) switching, a process in which a very short duration switch
is placed in the laser cavity, causing huge energy pulses of extremely
short length. This technique is used mainly in tattoo removal (see
later).
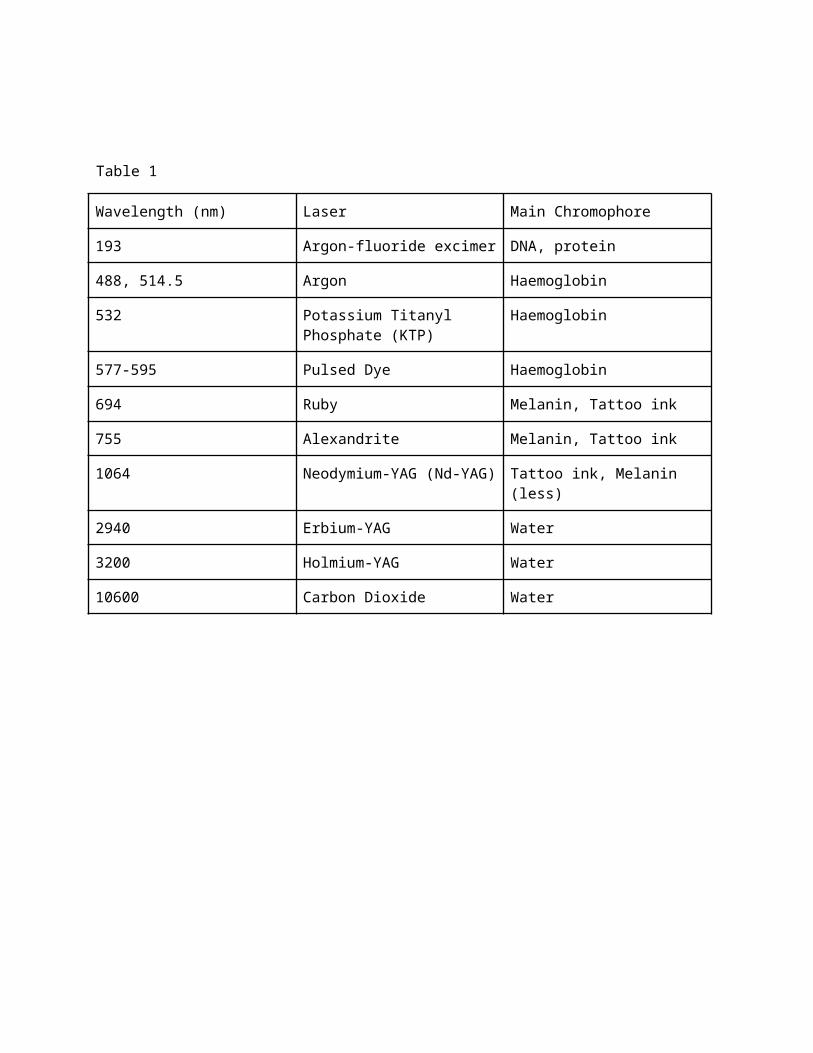
Table 1
Wavelength (nm) Laser Main Chromophore
193 Argon-fluoride excimer DNA, protein
488, 514.5 Argon Haemoglobin
532 Potassium Titanyl Phosphate (KTP)
Haemoglobin
577-595 Pulsed Dye Haemoglobin
694 Ruby Melanin, Tattoo ink
755 Alexandrite Melanin, Tattoo ink
1064 Neodymium-YAG (Nd-YAG) Tattoo ink, Melanin (less)
2940 Erbium-YAG Water
3200 Holmium-YAG Water
10600 Carbon Dioxide Water
Understanding the interaction of laser light and skin will supply the
reader with an excellent background to understand the application of
laser technology all over the body. Because facial skin is directly
visible - its what we mainly see when we look at people, the need to
avoid scarring during treatment was paramount in the development of
the laser in Facial Plastics. After Goldman’s initial experimentation
in the 60’s and 70’s, this development work was carried out
substantially at Harvard Medical School by John Parrish, a physician
at Massachusetts General Hospital, and Rox Anderson, a laboratory
technician and then medical student(10). Initially they looked at the
properties of skin from an optical point of view, then in the mid
eighties they developed 2 important physics principles of particular
relevance to the skin, namely:
1) Selective photothermolysis
2) Thermal relaxation time
1) The principle of Selective Photothermolysis was published in
Science(5). In this article, it was shown that short duration of
light, at a specific wavelength matched to the chromophore (light
absorbing tissue) make up of the target disease, could cause severe
damage to the target if energy levels were sufficiently high, but less
damage to the surrounding normal tissue. This paved the way for
selective treatment of haemangiomas, tattoos and hair removal, amongst
others, by destroying the disease but leaving the overlying skin and
subcutaneous tissue undamaged..
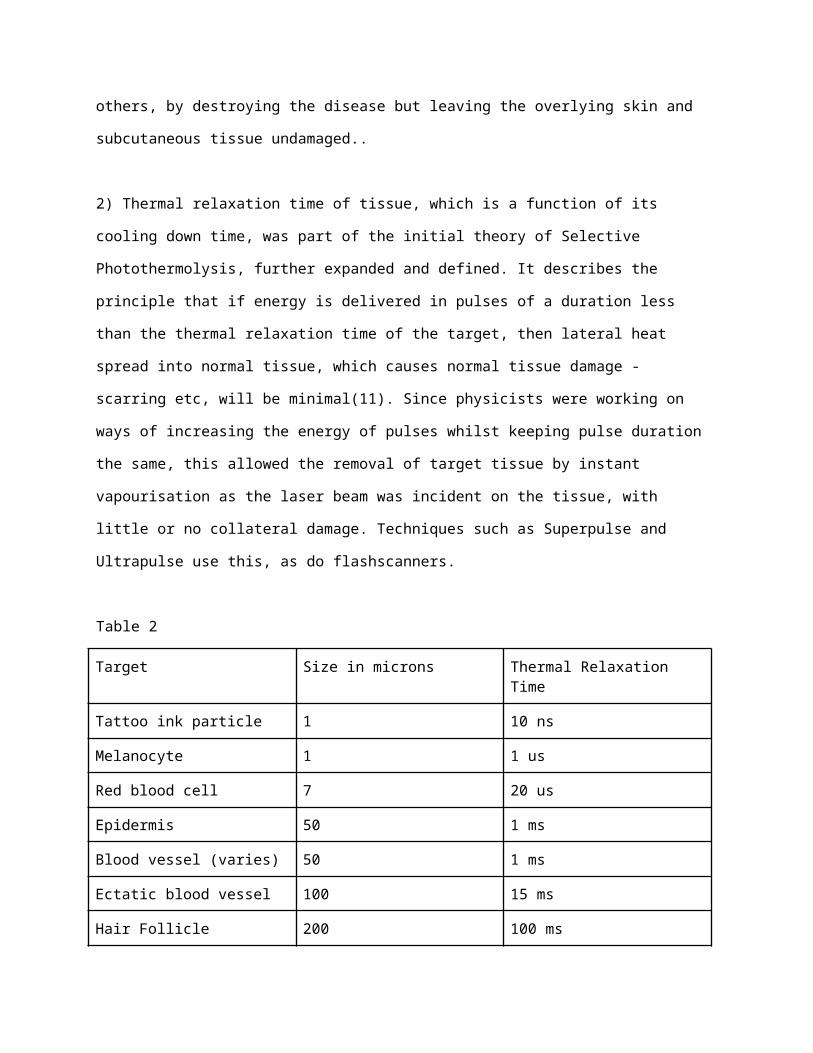
2) Thermal relaxation time of tissue, which is a function of its
cooling down time, was part of the initial theory of Selective
Photothermolysis, further expanded and defined. It describes the
principle that if energy is delivered in pulses of a duration less
than the thermal relaxation time of the target, then lateral heat
spread into normal tissue, which causes normal tissue damage -
scarring etc, will be minimal(11). Since physicists were working on
ways of increasing the energy of pulses whilst keeping pulse duration
the same, this allowed the removal of target tissue by instant
vapourisation as the laser beam was incident on the tissue, with
little or no collateral damage. Techniques such as Superpulse and
Ultrapulse use this, as do flashscanners.
Table 2
Target Size in microns Thermal Relaxation Time
Tattoo ink particle 1 10 ns
Melanocyte 1 1 us
Red blood cell 7 20 us
Epidermis 50 1 ms
Blood vessel (varies) 50 1 ms
Ectatic blood vessel 100 15 ms
Hair Follicle 200 100 ms
Characteristics of light as it interacts with tissue.
When light is shone on living tissue such as the skin, it does all of
the following.
1) It reflects off the surface and hits something else
2) It is absorbed by the tissue, causing an effect - this is mostly
what we are after (Grotthus-Draper law).
3) It transmits through the tissue, possibly being absorbed deeper in.
4) It scatters, so reducing the energy density and giving a wider,
less predictable effect.

3) Lasers Used in Facial Plastics
The Carbon Dioxide (CO2) Laser. This is an infrared laser, producing
light at 10,600nm wavelength. It is well outside the visible range,
and therefore needs to be combined with a visible low power aiming
beam laser, the Helium-Neon laser, which produces light at 630 nm
wavelength, in the middle of the red spectrum. The Carbon Dioxide
laser light is very highly absorbed by water, which means it has
minimal penetration in most tissue, hence it is good for superficial,
delicate effects, in particular skin and vocal cords. It will not pass
down solid quartz laser fibres however, and this can limit its
delivery deep into tissue. Flash scanning technology has greatly
helped the application of this laser in Facial Plastics(12). Flash
Scanners enable a highly focussed small laser spot (0.2mm diameter) to
be rapidly moved around a much larger area, so that the whole area is
covered in a given time, but the dwell time of the smaller spot of
0.2mm diameter is 1 millisecond or less. The dwell time if the amount
of time the laser light was actually incident on the tissue, and is
very important in minimising deeper damage, as per the theory of
thermal relaxation. For skin, the thermal relaxation time is thought
to be around 1 millisecond, so this scanner allows treatment diameters
from 3 to 10 mm to be treated quickly and evenly, all within the
thermal relaxation time, hence with minimal deep damage. The

flashscanner system relies on 2 mirrors rotating opposite each other,
but not directly opposite, so an even beam is created with even light
distribution around the entire area of the visible spot.
Superpulsing is an electronic way of stacking pulses to create pulses
of light of very high intensity and short duration - another way of
ensuring the dwell time is less than 1 msec, avoiding collateral
damage but causing a vapourising effect.
The Erbium YAG laser. This is a solid state, crystal laser, where the
lasing medium is Erbium incorporated into a garnet made from Ytrrium
and Aluminium (a garnet is a form of crystal). This is doped with
Erbium to produce light at 2,300nm wavelength. This has an even higher
water absorption peak than CO2, and is therefore even more delicate.
Er-YAG laser light passes well down solid fibres, so can be used
deeper in the body.
Vascular lasers. There are more than one lasers which fill this role.
They are all based on a wavelength between 480 and 530 nm, the yellow-
green part of the visible spectrum, which coincides with the peak of
absorption of oxygenated and deoxygenated haemoglobin - the key
chromophore in blood vessels. They include the flashlamp pumped dye
laser, the KTP (potassium titanyl phosphate), the argon laser and the
copper vapour laser. Nowadays the mainstay vascular lasers are the
first two.
Q-switched lasers. These lasers are mainly used for tattoo removal, so
do not have a big role in facial plastics. Q (quality) switching uses
an electronic switch within the laser cavity, which turns on and off
at very high frequency, causing very high energy pulses of extremely
short duration to be created. When these very high energies hit an
absorbing medium (chromophore) of the correct wavelength, explosions
of plasma are produced within the target tissue, which shatter the ink
particles within the tattoo, and are then taken away by the lymphatic
system. These laser will not be further discussed in this chapter.
Long pulsed penetrating lasers for hair removal. As their name
suggests, these lasers have a wavelength in the near infrared region,
which maximises penetration through tissue. They are used to treat
melanin accumulation in the hair follicles, causing extreme heating
and destruction of the follicle, without significantly damaging skin.
Melanin has its peak of absorption at a lower wavelength, but if these
wavelengths were used, there would be insufficient penetration to
damage the follicles, which lie quite deep in the dermis. The longer
wavelength is therefore a compromise between penetration and effect.
The main lasers in this area are the Ruby, Alexandrite, Neodymium-YAG
and Diode systems.

Photodynamic Therapy (PDT)
This is a cancer based treatment using a drug light combination to
destroy cancers at a cellular level, hence enabling retention of
tissue architecture, allowing non ablative cancer tissue removal, with
an additional selective effect due to cancer cells being more avid for
photosensitising compounds than normal tissue. Lasers for PDT are
designed for the peaks of the photosensiting compounds, mainly in the
red spectrum. Mostly nowadays they are Diode based (13), although
originally tuneable dye laser were used.
Intense Pulsed Light
A non-laser light system, it has a role to play in Facial Plastic
surgery, and so should be included in this chapter.
IPL systems use broadband flashlamps, rather like an arc light one
might use at home for exterior lighting. Emitted light tends to be in
the 500-1300 nm range, and can be modulated by cutoff filters to
narrow the emitted band. this is particularly useful if heating is to
be avoided, as infrared wavelengths above 1000 nm will be absorbed by
water, as this can cause thermal damage. Also, when treating pigmented
skin, filters can cut off the shorter wavelengths where Melanin
absorption is highest. Multiple problems can be addressed in one
treatment, such as hair removal, photorejuvenation and vascular
disorders(14).
4) Clinical areas in Facial Plastics where the laser is effective.
Benign facial lesion removal.
Many cases in facial plastics are for the removal of unsightly
blemishes, raised lumps, nodules etc. If they are removed surgically,
even with the best hands there will be a scar, and usually small
stitch marks. In the middle third of the face, this can leave long
standing mild disfigurement. Use of the CO2 laser in flash scanned
mode or Erbium-YAG delivered within a scanning module means that
facial lesions can be accurately vapourised down to the dermis, from
where skin will regenerate and form a new epidermis, with barely any
noticeable residual cosmetic defect. This is performed under local
anaesthetic with local infiltration of xylocaine 2% and adrenaline
1:200,000. Care needs to be taken that the lesion treated does not
represent anything more serious - for this a good history and
examination under the microscope or dermatoscope is required. In
particular it is important that the area treated has been present for
several years, is very slow growing / not growing at all, it has not
changed shape or colour/ darkened, or bled on minor contact. It should
also have an intact covering with no raised edge or ulceration. If
these parameters are correct, it is reasonable to go ahead and perform
laser vapourisation, there is no specimen with this procedure. If you
are worried about skin cancer or dysplasia, a biopsy may be required
before vapourisation. If malignant melanoma is suspected, wide

excision by a dermatological oncologist should be performed.
Rhinophyma
This condition, usually associated with Acne Rosacea, is characterised
by hypertrophic skin thickening on the external nose, most prominent
at the nasal tip. The thickening is mainly epidermal, and this lends
itself to vapourisation much more deeply than one could risk when
treating facial moles, as the underlying dermis may be 20 mm or more
away. The aim of treatment is to avoid deep dermal damage which would
cause scarring, but remove all of the excessive and disfiguring skin
tissue. This can be easily achieved using the scanned Carbon Dioxide
laser in high power mode, stopping when the deeper tissues are
uncovered. This sculpting mode of use has replaced the old fashioned
way of treating this disease by slicing off the redundant tissue with
a scalpel, a technique that was bloody and uneven at best.
Laser skin resurfacing
The ability to accurately remove superficial layers of skin without
significant deep dermal damage by using flash scanners has become one
of the main applications of the CO2 and Erbium-YAG laser in facial
plastics. Using the correct parameters, keeping energy delivery to
within the thermal relaxation time of the tissue (for skin,
approximately 1 millisecond) skin can be bloodlessly removed in 30
micron (um) deep layers (15). With each pass of laser light, heat is
delivered deeper into tissue, such that the epidermis vapourises away
and is removed by using cotton wool soaked in saline, leaving the

papillary dermis. Since this has different light absorption
characteristics, and much higher collagen content, instead of being
vapourised, it is mainly heated, causing visible dermal collagen
contraction, and significant skin tightening (16). The dermis and
epidermis then reforms due to migration of dermal cells from skin
appendages, leaving the area treated with a new, fresher outer layer
of skin, and dermal collagen tightening (17). It is a very effective
rejuvenating treatment. Postoperative healing can take weeks however,
and its is not a procedure for the faint hearted, particularly if the
whole face is treated. Quite elaborate pre and post treatment
protocols are followed to minimise the risk of damage and scarring.
Most resurfacing is done for the ageing face (lines and wrinkles),
although results from acne treatment with mild to moderate pitting are
also excellent.
Newer techniques use lasers to drill holes in the skin, rather than
completely removing the superficial layers. This is called fractional
photoablation and has less post operative effect in terms of redness
and swelling. It is less effective however, and studies have looked
into using a combination of traditional laser resurfacing for the
epidermis (1 pass) followed by fractional treatment of the reticular
and papillary dermis. This is called ablative fractional
photothermolysis(18). The Erbium-YAG laser can also be used for skin
resurfacing, although it has generally been found to be too slow and
ineffective as its penetration through skin is significantly less than
the CO2 laser, so less effect/damage is achieved. Multiple pass
techniques with this laser have been found to be nearly as effective

as the CO2 laser however and with better healing (19). Non-ablative
tissue remodelling uses deeper penetrating lasers to damage collagen
and cause it to shrink, without causing a significant epidermal
injury. Tissue cooling is important in this area (20). Lasers such as
the 1320 nm Nd-Yag, 1540 Erbium-glass and 1450 nm diode have been used
for this (21).
Transconjunctival blepharoplasty
In this procedure, the CO2 laser can be used to incise the inferior
(caudal) conjunctiva allowing access to the fat pad beneath. The
advantages of using the laser as a knife is that it cuts the slightly
loose conjunctiva easily, avoiding bleeding and haematoma / black
eyes, and also preventing shearing and tearing of the conjunctiva
which happen when the scalpel or scissor is used. Care has to be
taken with the proximity of the cornea, and corneal protectors are
recommended.
Vascular lesions
Because the absorption spectrum of oxygenated and deoxygenated
haemoglobin is relatively wide, a number of lasers fit into this
category. What is key about the treatment of vascular lesions on the
face is that the size and depth of the lesion be accurately assessed,
and that the laser used can provide a variable spot size and pulse
duration to allow effective treatment. The use of ultrasound can help
in this area. Vascular lesions on the face range from thread veins
over the cheek and nose, often caused by sun damage, to port wine
stains. The smaller lesions, such as thread veins, spider naevi,
arterio-venous malformations are easy to treat, and the 532 nm KTP
Aura laser gives an adequate range of pulse duration, energy and spot
size for most of these. Larger lesions such as haemangiomas contain
significantly bigger blood vessels, so longer pulses and therefore
more power is needed. The flashlamp pumped dye laser gives better
penetration and coverage for these (22).

Hair removal
Permanent hair removal is possible if selective photothermolysis (5)
is used to irreversibly damage a chromophore in the hair follicle,
whilst minimally damaging the same chromophore in the skin around the
follicle. The main chromophore found in hair follicles is melanin,
therefore all lasers used in this area emit light at the near infrared
end of the spectrum, where there is reasonable melanin absorption and
good penetration.This is now the biggest area for the use of lasers on
the skin. Facial hair, particularly in females, can be a big problem.
Female hirsutism affects 2-10% of the female population.
Up until the introduction of laser hair removal by Noren in 1996
(pers comm.), facial hair treatment, apart from shaving, essentially
involved pulling the hairs out, only for further growth to occur soon
after. Depilatory creams and electrolysis were also used, to limited
effect. Hypertrichosis, in which hair growth suddenly increases,
usually in patches, may be caused by drugs such as Phenytoin or
Cyclosporine, although it can also be a sign of internal malignancy.
Full investigation is required before treating these patients. General
facial hair problems in females is often linked to polycystic ovaries,
but does not require further investigation.
There is a choice of lasers which can be used for this procedure.
Which one the doctor chooses often depends on his or her population to
be treated. The ideal patients has white skin containing no melanin,
and black hair, with lots of melanin in the hair and its follicle. In

these cases high energies can be used, as there will be no chance of
dermal-epidermal melanin being damaged. The Fitzpatrick skin type
classification is useful in choosing which laser system to use. It is
based on a scoring system looking at eye and hair colour, skin colour
and its reaction to sunlight.
The Fitzpatrick Scale:
● Type I Light, pale white. Always burns, never tans
● Type II White; fair. Usually burns, tans with difficulty
● Type III Medium, white to olive. Sometimes mild burn, gradually
tans to olive.
● Type IV Olive, moderate brown. Rarely burns, tans with ease to a
moderate brown.
● Type V Brown, dark brown. Very rarely burns, tans very easily
● Type VI Black, very dark brown to black. Never burns, tans very
easily, deeply pigmented
Many techniques have been used to try and avoid skin heating in
Fitzpatrick types 2 and above. These include cooled air blowing, cold
spray blowing, frozen glass slides, ice packs, topical steroids (23).
It remains a problem as superficial skin damage may cause disordered
pigmentation, which is cosmetically difficult to cover/treat.

Table 3
Laser Skin type Wavelength nm
Long pulse Ruby 1-3 694
Long pulse Alexandrite 1-4 755
Pulsed diode 1-4 800-810
Long pulse Nd-YAG 1-6 1064
IPL 1-4 590-1200
As the table shows, increase in wavelength means darker skin can be
treated, as Melanin absorbs at lower wavelengths. When choosing energy
density measured in Joules/cm2, thjis depends on the immediate
treatment response, in which perifollicular oedema and mild erythema
should be seen, both of which resolve after 60 minutes. Test
treatments are often used to identify the correct treatment
parameters.
Skin Cancer
Non-Melanoma skin cancers can be effectively treated using the carbon
dioxide laser, or photodynamic therapy.
The Carbon Dioxide laser can be used as a bloodless knife to closely
follow surgical markings around skin cancers, allowing accurate
raising of flaps and z plasties. The spot size of 200 microns, when
used in Superpulse mode allows a neat scar with almost no collateral

damage. The lack of bleeding means that it is easier for the operator
to follow premarked lines for incision, which can often be complicated
in facial plastic surgery, and minor bleeding into the wound after
suturing, which is often the cause of poor scars, is also avoided.
The Carbon Dioxide laser in Flash Scanned mode, using spot sizes of
around 3 mm diameter, can also be used to superficially vapourise
areas of dysplasia, which heal without scarring. Also small basal and
squamous cell carcinomas can be vapourised away down to normal tissue
as in the Moh’s technique. Reconstruction is often not necessary as
the resultant defect, a depression in the skin, is less cosmetically
disfiguring than reconstruction with local flaps.
Photodynamic Therapy is a relatively new technique used for BCC’s or
SCC’s (24). It relies on a drug-light interaction causing activation
of a previously inert substance (the photosensitiser) so that it
reaches a triplet state, subsequently decaying in 2 stages back down
to the ground state, with resultant release of energy at the correct
level to break the covalent bond of the oxygen molecule. This causes
singlet oxygen to be produced, which immediately oxidises vital
intracytoplasmic organelles, causing cell death in a manner which
mimics apoptosis. This all means the tissue architecture is preserved,
since this is a non-ablative treatment and allows migration of
adjacent cells into the area where PDT was performed, with resultant
healing superior to secondary intention, and with no scar as would be
seen with excision and primary intention healing. Selectivity can
occur with respect to the cancer and normal tissue. This is highly
desirable as it minimises normal tissue damage. The best way to gain
selectivity is to paint the photosensitising agent directly onto the
tumour. This is the basis of treatment with d-Amino Laevulinic acid,
which absorbs well into tumours, and causes build up of Protoporphyrin
IX, which is an endogenous photosensisitiser(25). Unfortunately no
other photosensitisers will absorb directly into tissue.
Their delivery is therefore systemic, either orally (ALA again) or
intravenously - most of the mainstream photosensitising agents.
Systemic delivery will lead to some selectivity, as there is increased
affinity for photosensitisers by cancer cells when compared to normal
tissue. Once the peak levels of drug are in the cancer (this can be
measured using fluorescence), activating light of the correct
wavelength, intensity and fluence is shone at the skin cancer. The
method of cell death and healing leaves little residual
scar/deformity.
Photodynamic therapy is limited in its efficacy as specific energy
transfer in the formation of singlet oxygen means that the maximum
wavelength of light that can be used is at around 740 nm. This limits
tissue penetration and therefore depth of effect, to about 7 mm when
using the most powerful second generation photosensitisers.

5) Pigmentation Problems
One of the inherent features of skin is its ability to react to light
by producing melanin, from Melanocytes, which are cells of the Dermis-
Epidermis border. This is a protective function, mainly aimed at
preventing ultraviolet radiation damaging the skin.
Lasers, being light, have the ability to stimulate superficial
melanocytes. They may either cause overproduction or underproduction
of melanin, leading to Hyperpigmentation (over) in the treated area,
or hypopigmentation (under). The lasers that are most dangerous are
those whose wavelength is around 500 nm - 600 nm, where the pigment
Melanin absorbs light the most strongly. Other damaging lasers are the
ablative ones, such as the Carbon Dioxide laser in skin resurfacing.
Although this do not cause a direct light-chromophore effect on
Melanin, the Carbon Dioxide laser causes an intense inflammatory
effect, and that can also cause hyper or hypo pigmentation. Those of
Fitzpatrick skin types 3 and 4 have the most active melanocytes, and
are most prone to damage. People with a recent sun tan will also have
active melanocytes and should not be treated with any skin laser until
the tan has faded significantly. The Cycline family of antibiotics,
particularly tetracycline, are associated with skin pigment changing
after laser treatment. A 6 month gap between the last antibiotic
treatment and the commencement of laser treatment is usually required.

6) Safety
Standard laser safety procedures should be in practice at all times
when class 4 (all medical) lasers are in use. Eye protection for those
in the treatment rooms, locked doors and proper signage are all
required. The wavelength range 400-1400 nm can cause retinal damage,
and the adage never look at a laser beam must be adhered to.
When operating very close to the eyes use stainless steel corneal
protectors, as sudden head movements in response to pain can cause the
laser beam to hit directly onto the cornea, causing corneal scarring
and partial blindness, particularly with the Carbon Dioxide laser.
Other issues such as use of inflammable materials near the laser beam
need to be considered, particularly when 100% oxygen is around, as
this can pool since it is heavier than air. The laser beam is a very
good igniter, particularly the Carbon Dioxide laser.
Skin healing after laser treatment is obviously very important. Often
the skin appendages are very involved in this. The recent use of
retinoids such as Accutane or Roaccutane precludes most laser
treatments as this drug reduces the number of sebaceous glands which
can be vital for skin healing. Generally a 6 month gap is required
before treatment.
7) References
1) Maiman T.H. (2000). The laser odyssey. Blane, Laser Press.
2) Goldman L, Blaney D.J., Kindel D.J Frankie E.K. (1963) Effect of
the laser beam on the skin. J. Invest. Dermatol. 40:121-122
3) Campbell C.J., Noyori K.S., Rittler M.C., Koester C. (1965) Retinal
coagulation: Clinical studies. Ann. N.Y. Acad Sci. 122:780
4) Hellwarth R.W., McClung F.J. (1962) Giant pulsations from Ruby.
Appl. Phys. 33:838-841
5) R. Rox Anderson and John A. Parrish (1983) Selective
Photothermolysis: precise microsurgery by selective absorption of
pulsed radiation
Science Vol. 220, No. 4596, pp. 524-527
6) Sherwood K.A., Murray S., Kurban A.K., Tan O.T. (1989) Effect of
wavelength on cutaneous pigment using pulsed irradiation. J. Invest.
Dermatol. 92:717-720
7) Pulsed CO2 laser tissue ablation: Effect of tissue type and pulse
duration on thermal damage Joseph T. Walsh,Thomas J. Flotte, R. Rox
Anderson,Thomas F. Deutsch. Lasers in Surgery and Medicine. Volume 8,
Issue 2, pages 108–118, 1988
8) Dilkes MG, DeJode ML, Gardiner Q, Kenyon GS, McKelvie P. Treatment
of head and neck cancer with photodynamic therapy: results after one
year.
J Laryngol Otol. 1995 109(11):1072-6.
9) Einstein A., Zur quantumtheorie der Strahlung. (1917) Physikalishe Gesellschaft Zurich. 18:47-62
10) R Rox Anderson and John A Parrish. The Optics of Human Skin.
Journal of Investigative Dermatology (1981) 77, 13–19
11) Anderson RR, Parrish JA. Microvasculature can be selectively
damaged using dye lasers: a basic theory and experimental evidence in
human skin. Lasers Surg Med.1986;122:1016-1022
12) Lach E. Flash scanning the CO2 laser: a revival of the CO2 laser
in plastic surgery (1994) , Proc. SPIE 2128, Laser Surgery: Advanced
Characterization, Therapeutics, and Systems IV, 211
13) An in vivo comparison of the photodynamic action of a new diode
laser and a copper vapour dye laser at 652 nm (1996)
DeJode, M. L.; Mcgilligan, J. A.; Dilkes, M. G.
Lasers in medical science 11 (1996), S. 117-121
14) Schoenewolf N., Barysch M and Dummer R. 2011. Intense Pulsed
Light. In: Curr Probl dermatol. 42:166-172
15) Alster T, Kauvar A, and Geronimus R. (1996) Histology of high
energy pulsed CO2 laser resurfacing. Semin Cutan Med Surg; 15:189-93
16) Green J, Burd E., Nishioka N (1992) Middermal wound healing. A
comparison between dermatomal excision and pulsed carbon dioxide laser
ablation. Arch Dermatol.;128:639-45
17) Ross E, Naseef G, Skrobal M. (1996). In vivo dermal collagen
shrinkage and remodeling following CO2 laser skin resurfacing. Lasers
Surg Med;8:38
18) Cohen S, Henssler C, Johnston J (2009) Fractional photothermolysis
for skin rejuvenation. ... In vivo histopathologic comparison of the
acute injury following treatment with five fractional ablative laser
devices.Dermatol Surg 37(6):776–781
19) Tanzi EL, Alster TS (2003) Single pass carbon dioxide versus
multiple-pass Er:YAG laser skin resurfacing. Comparison of
postoperative wound healing and side effect rates. Dermatol Surg 29 :
80-84 35.
20) Anderson R.R. (2000) Lasers in dermatology: A critical update. J
dermatol;27:700-5
21) Hardaway C and Ross E. (2002) Nonablative laser skin remodelling.
Dermatol Clin.;20:97-111
22) Garden J, Polla L, Tan O. (2006) Laser treatment of vascular
lesions. Clin Dermatol.;24:8-15. 9.
23) Drosner M and Adatto M. (2005) Photoepilation: Guidelines for care
from the European Society for Laser Dermatology. I. Cosmetic Laser
Ther;7:33-38
24) Wilson B and Mang T. (1995) Photodynamic therapy for cutaneous
malignancies. Clin. dermatol.;13:91-6
25) Kennedy J. Pottier R., Pross D. (1990) Photodynamic therapy with
endogenous protoporphyrin IX: Basic principles and present clinical
experience. J. Photochem. Photobiol B;14:275-92




![Menschenhaut [Human skin]](https://static.fdokumen.com/doc/165x107/6326d24f24adacd7250b1364/menschenhaut-human-skin.jpg)















