
Language improvements after TMS plus modified CILT: Pilot, open-protocol study with two, chronic...
23
AUTHOR COPY Restorative Neurology and Neuroscience 32 (2014) 483–505 DOI 10.3233/RNN-130365 IOS Press 483 Language improvements after TMS plus modified CILT: Pilot, open-protocol study with two, chronic nonfluent aphasia cases Paula I. Martin a,∗ , Ethan Treglia a , Margaret A. Naeser a , Michael D. Ho a , Errol H. Baker a , Elizabeth G. Martin a , Shahid Bashir b and Alvaro Pascual-Leone b,c a Veterans Affairs Boston Healthcare System and the Harold Goodglass Boston University Aphasia Research Center, Department of Neurology, Boston University School of Medicine, Boston, MA, USA b Berenson-Allen Center for Noninvasive Brain Stimulation, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA c Institut Universitari de Neurorehabilitaci´ o Guttmann-UAB, Badalona, Spain Abstract. Purpose: The purpose of this study was to investigate: 1) the feasibilty of administering a modified CILT (mCILT) treatment session immediately after TMS; and 2) if this combined therapy could improve naming and elicited propositional speech in chronic, nonfluent aphasia. Methods: Two chronic stroke patients with nonfluent aphasia (mild-moderate and severe) each received twenty minutes of rTMS to suppress the right pars triangularis, followed immediately by three hours of mCILT (5 days/week, 2 weeks). (Each patient had received TMS alone, 2–6 years prior.) Language evaluations were performed pre- TMS+mCILT, and post- at 1-2 months, and 6 or 16 months. Results: Both patients showed significant improvements in naming pictures, and elicited propositional speech at 1-2 months post- TMS+mCILT. The improved naming was still present at 6 months post- TMS+mCILT for P2; but not at 16 months post- TMS+mCILT for P1. Conclusions: It is feasible to administer mCILT for three hours immediately after a TMS session. It is unknown if the significant improvements in naming pictures, and elicited propositional speech were associated with the second series of TMS, or this first series of mCILT, or a combination of both. A larger, sham controlled clinical trial is warranted. Keywords: TMS, speech therapy, constraint-induced language therapy, aphasia, stroke rehabilitation 1. Introduction 1.1. Transcranial magnetic stimulation Transcranial magnetic stimulation (TMS) has been applied to promote poststroke recovery in the domains ∗ Corresponding author: Paula I. Martin, PhD, Aphasia Research Center 12-A, VA Boston Healthcare System, 150 So. Huntington Ave., Boston, MA 02130, USA. Tel.: +1 857 364 4029; Fax: +1 617 739 8926; E-mail: [email protected]. of 1) motor deficits (Fregni et al., 2006); 2) visuospa- tial neglect following right hemisphere (RH) stroke (Brighina et al., 2003; Koch et al., 2008); and 3) apha- sia following left hemisphere (LH) stroke (Barwood et al., 2010; Hamilton et al., 2010; Martin et al., 2009a; Medina et al., 2012; Naeser et al., 2010a, 2005a, 2005b; Turkeltaub et al., 2012; Weiduschat et al., 2011). One principle supporting these improvements post- stroke is that TMS may be used to modulate abnormal interhemispheric inhibition in chronic stroke, where 0922-6028/14/$27.50 © 2014 – IOS Press and the authors. All rights reserved
-
Upload
hms-harvard -
Category
Documents
-
view
2 -
download
0
Transcript of Language improvements after TMS plus modified CILT: Pilot, open-protocol study with two, chronic...

AU
THO
R C
OP
Y
Restorative Neurology and Neuroscience 32 (2014) 483–505DOI 10.3233/RNN-130365IOS Press
483
Language improvements after TMS plusmodified CILT: Pilot, open-protocol studywith two, chronic nonfluent aphasia cases
Paula I. Martina,∗, Ethan Tregliaa, Margaret A. Naesera, Michael D. Hoa, Errol H. Bakera,Elizabeth G. Martina, Shahid Bashirb and Alvaro Pascual-Leoneb,c
aVeterans Affairs Boston Healthcare System and the Harold Goodglass Boston University Aphasia Research Center,Department of Neurology, Boston University School of Medicine, Boston, MA, USAbBerenson-Allen Center for Noninvasive Brain Stimulation, Beth Israel Deaconess Medical Center, Harvard MedicalSchool, Boston, MA, USAcInstitut Universitari de Neurorehabilitacio Guttmann-UAB, Badalona, Spain
Abstract.Purpose: The purpose of this study was to investigate: 1) the feasibilty of administering a modified CILT (mCILT) treatmentsession immediately after TMS; and 2) if this combined therapy could improve naming and elicited propositional speech inchronic, nonfluent aphasia.Methods: Two chronic stroke patients with nonfluent aphasia (mild-moderate and severe) each received twenty minutes of rTMSto suppress the right pars triangularis, followed immediately by three hours of mCILT (5 days/week, 2 weeks). (Each patienthad received TMS alone, 2–6 years prior.) Language evaluations were performed pre- TMS+mCILT, and post- at 1-2 months,and 6 or 16 months.Results: Both patients showed significant improvements in naming pictures, and elicited propositional speech at 1-2 monthspost- TMS+mCILT. The improved naming was still present at 6 months post- TMS+mCILT for P2; but not at 16 months post-TMS+mCILT for P1.Conclusions: It is feasible to administer mCILT for three hours immediately after a TMS session. It is unknown if the significantimprovements in naming pictures, and elicited propositional speech were associated with the second series of TMS, or this firstseries of mCILT, or a combination of both. A larger, sham controlled clinical trial is warranted.
Keywords: TMS, speech therapy, constraint-induced language therapy, aphasia, stroke rehabilitation
1. Introduction
1.1. Transcranial magnetic stimulation
Transcranial magnetic stimulation (TMS) has beenapplied to promote poststroke recovery in the domains
∗Corresponding author: Paula I. Martin, PhD, Aphasia ResearchCenter 12-A, VA Boston Healthcare System, 150 So. HuntingtonAve., Boston, MA 02130, USA. Tel.: +1 857 364 4029; Fax: +1 617739 8926; E-mail: [email protected].
of 1) motor deficits (Fregni et al., 2006); 2) visuospa-tial neglect following right hemisphere (RH) stroke(Brighina et al., 2003; Koch et al., 2008); and 3) apha-sia following left hemisphere (LH) stroke (Barwood etal., 2010; Hamilton et al., 2010; Martin et al., 2009a;Medina et al., 2012; Naeser et al., 2010a, 2005a, 2005b;Turkeltaub et al., 2012; Weiduschat et al., 2011).One principle supporting these improvements post-stroke is that TMS may be used to modulate abnormalinterhemispheric inhibition in chronic stroke, where
0922-6028/14/$27.50 © 2014 – IOS Press and the authors. All rights reserved

AU
THO
R C
OP
Y
484 P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia
increased excitability in parts of the undamaged hemi-sphere is present due to release of inhibition from thedamaged hemisphere (Thiel et al., 2006).
Slow, 1 Hz repetitive TMS (rTMS) may be used tosuppress the hyper-excitability of parts of the undam-aged hemisphere in patients who have suffered a stroke,in turn promoting better modulation of both hemi-spheres. In patients with aphasia due to stroke, bettermodulation has been observed to promote improvedlanguage behavior including naming and phrase lengthat 2 months or longer, following suppression of onespecific, target area (1 cm square) in the RH, usuallythe R pars triangularis (PTr) (Barwood et al., 2010;Hamilton et al., 2010; Medina et al., 2012; Naeseret al., 2010a, 2005a, 2005b; Turkeltaub et al., 2012;Weiduschat et al., 2011).
Functional MRI scans during overt naming of pic-tures in a patient with chronic, nonfluent aphasiaobtained pre- and post- a two-week series of TMS treat-ments to suppress the R PTr have shown improvednaming to be associated with increased activation inparts of the LH, lasting up to 4 years post- TMS(Martin et al., 2009a). Weiduschat et al. (2011) usedactivation positron emission tomography (PET) scanspre- and post- a two-week series of rTMS treatments(real rTMS to the R PTr versus control-real rTMSto the vertex of the head) plus 45 minutes of indi-vidualized speech therapy in a heterogeneous groupof patients with subacute aphasia (<4 months post-stroke onset). In that study, significant improvementin the overall Aachen Aphasia Test (AAT) score andin the subtest of naming was observed only in the realrTMS group where 1 Hz rTMS was used to suppressthe R PTr. There was no significant improvement inthe overall AAT score or naming in the control rTMSgroup. In addition, those patients who received realrTMS to suppress the R PTr no longer retained anincreased right-laterality index for increased activationfor the inferior frontal gyrus/Broca’s area (Weiduschatet al., 2011). These results suggest that rTMS to sup-press R PTr, combined with speech therapy can preventretention of RH lateralization in patients with subacuteaphasia; this may in turn, promote better recovery. Asubsequent study by this group (with a larger num-ber of patients) replicated these findings (Thiel et al.,2013). Cotelli et al. (2011) has applied high frequencyrTMS to the L dorsolateral prefrontal cortex, fol-lowed immediately by 25 minutes of speech therapy(anomia treatment), where improved object namingwas observed. Long-term TMS effects are believed to
engage mechanisms of neural plasticity, thus likely ren-dering this technique especially suitable for improvingpoststroke behavior when combined with appropri-ate behavioral intervention (Rossi and Rossini, 2004;Talelli and Rothwell, 2006).
1.2. Constraint-induced language therapy
Constraint-induced language therapy (CILT) wasoriginally based on a therapy developed to treat paral-ysis in patients who had suffered a stroke – e.g.,constraint-induced movement therapy (CIMT) (Cher-ney et al., 2008; Hakkennes and Keating, 2005;Meinzer et al., 2007; Taub et al., 1999). CIMT canproduce an increase in the amount and quality of move-ment of the affected limbs in patients with hemiparesisdue to stroke, which carries over to a real-world envi-ronment (Taub et al., 1999). The principles applied dur-ing CIMT include: 1) restraining the unaffected limbwith a sling, splint, or glove; 2) forcing the use of theaffected limb; 3) intensive shaping and training of theaffected limb through massed practice (6 hours or moreper day for at least 2-3 weeks) (Taub et al., 1999). Afourth core component, the transfer package, has beendesigned to facilitate transfer of gains to real-worldactivities (Gauthier et al., 2008). Three hours versussix, of intensive therapy has been shown to improve useof the affected arm, along with parallel structural brainchanges (increase in grey matter volume in hand andarm regions of the sensory and motor areas, anteriorsupplementary motor area, portions of the premotorarea, and bilateral hippocampi) (Gauthier et al., 2008).
Based on the CIMT approach, constraint-inducedprinciples have been applied to aphasia therapy,and these have been labeled as CILT or intensivelanguage-action therapy (ILAT) (Difrancesco et al.,2012) including constraint-induced aphasia therapy(CIAT). These language therapies have applied thesame basic, initial therapy components as CIMT,including 1) shaping (Taub, 2004; Taub et al., 1994), 2)massed (intensive) practice, and 3) forced use of verballanguage only (Cherney et al., 2008). These constraint-induced language treatment approaches have beenreviewed (Berthier and Pulvermuller, 2011; Meinzeret al., 2012).
Naming was significantly improved following aseries of 10 CILT treatments (Maher et al., 2006;Meinzer et al., 2005). CIAT has been associated withsignificant language improvement following 3-4 hoursof treatment per day for 2 weeks, in patients with

AU
THO
R C
OP
Y
P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia 485
chronic aphasia (Pulvermuller et al., 2001). In an indi-vidual with chronic nonfluent aphasia, an increase inverb production was observed after a modified CIATprogram was administered (Goral and Kempler, 2008).Intensive language therapies have been observed tohave a lasting effect from 1 month (Maher et al., 2006)up to 6 months after therapy (Meinzer et al., 2005).
1.3. Functional imaging Pre-/Post- CILT
Functional imaging studies demonstrate changes inbrain activity associated with CILT (Meinzer and Bre-itenstein, 2008) that suggest these therapies may alsoengage mechanisms of neural plasticity. After 2 weeksof CIAT, the naming performance of eleven patientswith chronic aphasia significantly improved, and wascorrelated with increased activity in perilesional LHbrain areas (Meinzer et al., 2008). Success followingCIAT has also been correlated with a relative decreaseof activation in RH areas, including the IFG/insularcortex (Richter et al., 2008). In 23 patients, usingmagnetoencephalography (MEG), Breier et al. (2009)identified three different patterns of behavioral andneurophysiologic responses to CILT: 1) Lost-Responsein which any gains were lost 3 months post- treatment,and greater RH activation was present compared tothe other response groups, at each MEG scanning ses-sion; 2) Responders who maintained significant gainsat follow-up, and showed an increase in L temporallobe activation after therapy, as well as a decrease inR frontal activation; and 3) Non-responders who didnot improve after CILT and displayed greater L ver-sus R parietal activation, with a decrease in L temporalactivation after therapy (Breier et al., 2009).
1.4. Rationale
The present study examined the effect of TMS plusa modified CILT (mCILT) in two patients with chronic,nonfluent aphasia. Motivation for our design was basedon other stroke studies where improved behavior wasassociated with a combination of treatment modalities– e.g., pharmacological intervention plus speech ther-apy (Berthier et al., 2009; Kessler et al., 2000); TMSor transcranial direct current stimulation (tDCS) plusphysical therapy (Bolognini et al., 2009; Hesse et al.,2007); TMS plus speech therapy (Cotelli et al., 2011;Weiduschat et al., 2011); and tDCS plus concurrentspeech therapy (Baker et al., 2010; Floel et al., 2011;Vines et al., 2011).
Our rationale for including TMS plus mCILT isas follows: 1) Studies have shown that rTMS aloneimproves naming at 2 months or more after the lasttreatment (Naeser et al., 2005a, 2005b; Hamilton et al.,2010); and 2) Studies have shown that CILT alsoimproves naming at 1 month or more after the lasttreatment (Maher et al., 2006; Meinzer et al., 2005).Imaging studies with each of these therapies haveshown changes in activation after treatment. Thesechanges suggest that each therapy engages mecha-nisms of neural plasticity (Meinzer and Breitenstein,2008; Martin, 2009a; Weiduschat et al., 2011). Thus,our hypothesis was that the combination of TMSplus mCILT would optimize improvements induced byeach treatment modality, resulting in further languagerecovery in chronic stroke patients.
2. Methods
2.1. Participants
Two patients with chronic, nonfluent aphasia whohad completed our initial TMS protocol (Naeser et al.,2005b), without concurrent speech therapy, enteredinto this TMS+mCILT study. This is the first studyto examine the effects of TMS alone, and later, TMSplus CILT in the same chronic stroke patients. Thus,the criteria for entry into this study were as follows:1) the patient must have shown significant improve-ment in naming after the first series of TMS treatmentsalone; and 2) the patient must still be able to nameat least 3 pictures on the Boston Naming Test (BNT)(Kaplan et al., 2001). Demographics and clinical char-acteristics for each participant are included in Table 1;the language data are provided in Table 2. InstitutionalReview Board approval, signed informed consent, andHIPAA consent were obtained. In the current study,neither patient received any additional speech therapy(besides mCILT) during the 2-week treatment proto-col, or throughout the follow-up testing.
2.1.1. Patient 1 (P1)P1, Summary of Previous TMS ParticipationAt age 43 he had suffered an embolic L MCA stroke
that resulted in slight R hemiparesis and mild-moderatenonfluent aphasia; intravenous tissue plasminogenactivator had been administered. He had no visualfield defect or hearing problem. Previous medical his-tory was remarkable for obstructive sleep apnea. At

AU
THO
R C
OP
Y
486 P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia
Tabl
e1
Clin
ical
char
acte
rist
ics
for
two
patie
nts
with
nonfl
uent
apha
sia
Age
atY
ears
Tim
ein
terv
alG
ende
rE
duca
tion
CV
AH
emip
ares
isA
phas
iaTy
peN
ativ
eE
nglis
hH
ande
dnes
sO
ther
time
ofPo
st-C
VA
betw
een
last
entr
yin
toat
time
ofT
MS
alon
eT
MS+
mC
ILT
entr
yin
totr
eatm
enta
nd(Y
rs)
TM
S+m
CIL
Ten
try
into
TM
S+m
CIL
T
P147
4Y
r.7
Mo.
2yr
.5M
o.M
2Y
r.Ju
nior
Col
lege
LM
CA
,em
bolic
;tP
Aad
min
iste
red
Rsl
ight
;som
efin
ger
flexi
on/s
past
icity
mild
-mod
erat
eno
nflue
ntN
ativ
eE
nglis
h;Fl
uent
Span
ish
Rig
htO
bstr
uctiv
eSl
eep
Apn
ea;n
ight
lyC
PAP
P263
12Y
r.3
Mo.
5Y
r.10
Mo.
F4
Yr.
Col
lege
LIC
H,w
ithne
uros
urge
ryR
hem
iple
gia
seve
reno
nflue
ntN
ativ
eE
nglis
hR
ight
AU
THO
R C
OP
Y
P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia 487
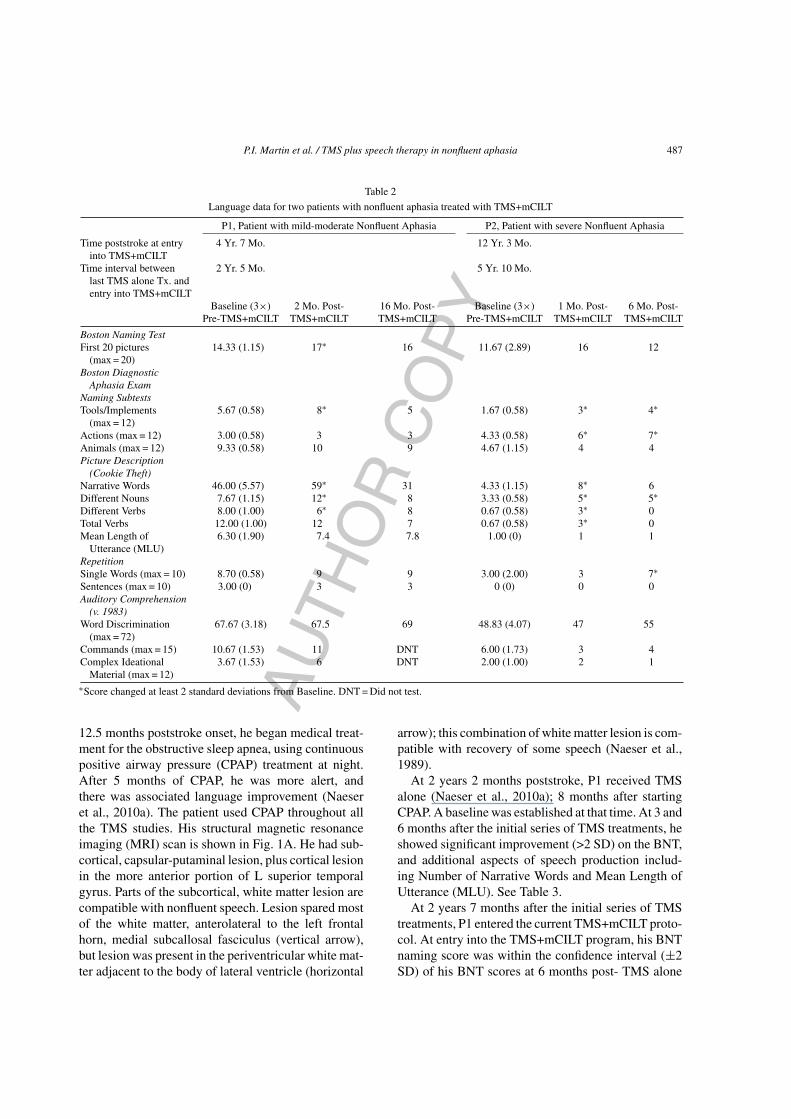
Table 2
Language data for two patients with nonfluent aphasia treated with TMS+mCILT
P1, Patient with mild-moderate Nonfluent Aphasia P2, Patient with severe Nonfluent Aphasia
Time poststroke at entryinto TMS+mCILT
4 Yr. 7 Mo. 12 Yr. 3 Mo.
Time interval betweenlast TMS alone Tx. andentry into TMS+mCILT
2 Yr. 5 Mo. 5 Yr. 10 Mo.
Baseline (3×) 2 Mo. Post- 16 Mo. Post- Baseline (3×) 1 Mo. Post- 6 Mo. Post-Pre-TMS+mCILT TMS+mCILT TMS+mCILT Pre-TMS+mCILT TMS+mCILT TMS+mCILT
Boston Naming TestFirst 20 pictures
(max = 20)14.33 (1.15) 17∗ 16 11.67 (2.89) 16 12
Boston DiagnosticAphasia Exam
Naming SubtestsTools/Implements
(max = 12)5.67 (0.58) 8∗ 5 1.67 (0.58) 3∗ 4∗
Actions (max = 12) 3.00 (0.58) 3 3 4.33 (0.58) 6∗ 7∗Animals (max = 12) 9.33 (0.58) 10 9 4.67 (1.15) 4 4Picture Description
(Cookie Theft)Narrative Words 46.00 (5.57) 59∗ 31 4.33 (1.15) 8∗ 6Different Nouns 7.67 (1.15) 12∗ 8 3.33 (0.58) 5∗ 5∗Different Verbs 8.00 (1.00) 6∗ 8 0.67 (0.58) 3∗ 0Total Verbs 12.00 (1.00) 12 7 0.67 (0.58) 3∗ 0Mean Length of
Utterance (MLU)6.30 (1.90) 7.4 7.8 1.00 (0) 1 1
RepetitionSingle Words (max = 10) 8.70 (0.58) 9 9 3.00 (2.00) 3 7∗Sentences (max = 10) 3.00 (0) 3 3 0 (0) 0 0Auditory Comprehension
(v. 1983)Word Discrimination
(max = 72)67.67 (3.18) 67.5 69 48.83 (4.07) 47 55
Commands (max = 15) 10.67 (1.53) 11 DNT 6.00 (1.73) 3 4Complex Ideational
Material (max = 12)3.67 (1.53) 6 DNT 2.00 (1.00) 2 1
∗Score changed at least 2 standard deviations from Baseline. DNT = Did not test.
12.5 months poststroke onset, he began medical treat-ment for the obstructive sleep apnea, using continuouspositive airway pressure (CPAP) treatment at night.After 5 months of CPAP, he was more alert, andthere was associated language improvement (Naeseret al., 2010a). The patient used CPAP throughout allthe TMS studies. His structural magnetic resonanceimaging (MRI) scan is shown in Fig. 1A. He had sub-cortical, capsular-putaminal lesion, plus cortical lesionin the more anterior portion of L superior temporalgyrus. Parts of the subcortical, white matter lesion arecompatible with nonfluent speech. Lesion spared mostof the white matter, anterolateral to the left frontalhorn, medial subcallosal fasciculus (vertical arrow),but lesion was present in the periventricular white mat-ter adjacent to the body of lateral ventricle (horizontal
arrow); this combination of white matter lesion is com-patible with recovery of some speech (Naeser et al.,1989).
At 2 years 2 months poststroke, P1 received TMSalone (Naeser et al., 2010a); 8 months after startingCPAP. A baseline was established at that time. At 3 and6 months after the initial series of TMS treatments, heshowed significant improvement (>2 SD) on the BNT,and additional aspects of speech production includ-ing Number of Narrative Words and Mean Length ofUtterance (MLU). See Table 3.
At 2 years 7 months after the initial series of TMStreatments, P1 entered the current TMS+mCILT proto-col. At entry into the TMS+mCILT program, his BNTnaming score was within the confidence interval (±2SD) of his BNT scores at 6 months post- TMS alone

AU
THO
R C
OP
Y
488 P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia
Fig. 1. A) and B): T1-weighted structural MRI scans, with axial, and L and R reconstructed lateral views for each patient. White triangle on theR lateral view marks the area of cortex (R PTr) where 1 Hz rTMS was used to suppress that cortical area, in each case. C) Application of rTMSwith the figure 8-shaped, hand-held rTMS coil, using the neuronavigation system, Brainsight (Rogue Industries, Montreal).
(the latest testing time post- TMS alone). His totalnumber of narrative words for the cookie theft pic-ture description was also within the confidence intervalof his number of narrative words at 3 months post-TMS alone. (Propositional speech had not been testedat 6 months post- TMS alone.) Thus, the significantgains in naming and propositional speech that P1 hadmade during TMS alone appeared to remain stable inthe intervening 2 years, 7 months before entry intothis TMS+mCILT program (Table 3). Patient 1 did notreceive individual speech therapy after the initial TMSseries.
2.1.2. Patient 2 (P2)P2, Summary of Previous TMS ParticipationAt age 51, she had suffered a LH intracerebral hem-
orrhage that required surgical intervention and resulted
in severe nonfluent aphasia and R hemiplegia. Shewore a hearing aid and had no visual field defect. Herstructural MRI scan is shown in Fig. 1B. She had pri-marily subcortical white matter lesion. No lesion waspresent in Broca’s or Wernicke’s cortical areas. Whitematter lesion included the medial subcallosal fasci-culus (vertical arrow), and the periventricular whitematter (horizontal arrow). This extensive white matterlesion combination is compatible with severe nonfluentspeech (Naeser et al., 1989).
At 6.5 years poststroke, P2 received TMS alone(Naeser et al., 2005a). At 2 months, and at 4 years3 months after the initial series of TMS treatments,she showed improvement on the BNT, but no changein Phrase Length, which remained 0-1 word. SeeTable 4. P2 had received some speech therapy for a fewmonths, starting at 1 year after the initial TMS alone,

AU
THO
R C
OP
Y
P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia 489Ta
ble
3
Com
pari
son
ofla
ngua
gere
sults
for
TM
Sal
one,
and
Pre-
TM
S+m
CIL
Tte
stin
gfo
rP1
,mild
-mod
erat
eno
nflue
ntap
hasi
a
TM
SA
lone
Com
pari
sons
:TM
SA
lone
,and
TM
S+m
CIL
T
Bas
elin
e+
2SD
−2SD
3M
o.Po
st-
6M
o.Po
st-
Bas
elin
e+
2SD
−2SD
Was
test
ing
2M
o.Po
st-
16M
o.Po
st-
(3×)
TM
Sal
one
TM
Sal
one
(3×)
Pre-
at6
Mo.
Post
-TM
ST
MS+
mC
ILT
TM
S+m
CIL
TPr
e-T
MS
alon
eT
MS+
mC
ILT
alon
e,w
ithin
2SD
ofB
asel
ine,
Pre-
TM
S+m
CIL
T?†
Tim
ePo
stst
roke
Ons
et1
Yr.
5M
o.2
Yr.
5M
o.2
Yr.
9M
o.4
Yr.
7M
o.4
Yr.
11M
o.6
Yr.
1M
o.B
osto
nN
amin
gTe
stFi
rst2
0pi
ctur
es(m
ax=
20)
8.67
(1.4
1)11
.45.
8512
∗13
∗14
.33
(1.1
5)16
.63
12.0
3Y
17∗
16B
osto
nD
iagn
osti
cA
phas
iaE
xam
Nam
ing
Subt
ests
Tool
s/Im
plem
ents
(max
=12
)5.
67(1
.89)
9.45
1.89
52
5.67
(0.5
8)6.
834.
51N
,-2S
D8∗
5A
ctio
ns(m
ax=
12)
3.33
(1.7
1)6.
750
45
3.00
(0.5
8)4.
161.
84N
,+2S
D3
3A
nim
als
(max
=12
)8.
00(2
.06)
12.1
3.88
77
9.33
(0.5
8)10
.49
8.17
N,-
2SD
109
Pic
ture
Des
crip
tion
(Coo
kie
The
ft)
Mea
nL
engt
hof
Utte
ranc
e(M
LU
)2.
9(0
.74)
4.38
1.42
6.9*
DN
T6.
30(1
.9)
10.1
02.
50–
7.4
7.8
Nar
rativ
eW
ords
21.7
5(9
.64)
41.0
2.11
48∗
DN
T46
.00
(5.5
7)57
.14
34.8
6–
59∗
31R
epet
itio
nSi
ngle
Wor
ds(m
ax=
10)
8.67
(0.5
)9.
677.
678
88.
70(0
.58)
9.86
7.54
Y9
9A
udit
ory
Com
preh
ensi
on(v
.198
3)W
ord
Dis
crim
inat
ion
(max
=72
)66
.33
(5.5
0)77
.355
.33
6765
.50
67.6
7(3
.18)
74.0
361
.31
Y67
.569
Com
man
ds(m
ax=
15)
10.6
7(1
.89)
14.4
6.89
1113
.00
10.6
7(1
.53)
13.7
37.
61Y
11D
NT
Com
plex
Idea
tiona
lMat
eria
l(m
ax=
12)
6.00
(1.5
0)9.
003.
006
53.
67(1
.53)
6.73
0.61
Y6
DN
T
∗ Sco
rein
crea
sed
atle
ast2
SDfr
omB
asel
ine
(3×)
,for
each
trea
tmen
tint
erve
ntio
nse
ries
(TM
Sal
one
orT
MS+
mC
ILT
).† T
ime
Inte
rval
betw
een
last
test
ing
Post
-TM
Sal
one
and
entr
yin
toT
MS+
mC
ILT
=1
Yr.
10M
o.D
NT
=D
idno
ttes
t.

AU
THO
R C
OP
Y
490 P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia
Tabl
e4
Com
pari
son
ofla
ngua
gere
sults
for
TM
Sal
one,
and
Pre-
TM
S+m
CIL
Tte
stin
gfo
rP2
,pat
ient
with
seve
reno
nflue
ntap
hasi
a
TM
SA
lone
Com
pari
sons
:TM
SA
lone
,and
TM
S+m
CIL
T
Bas
elin
e2
Mo.
4Y
r.3
Mo.
Bas
elin
e+
2SD
−2SD
Was
last
1M
o.6
Mo.
(1×)
Pre-
Post
-Po
st-
(3×)
Pre-
test
ing
atPo
st-
Post
-T
MS
alon
eT
MS
alon
eT
MS
alon
eT
MS+
mC
ILT
4Y
r.3
Mo.
Post
-T
MS+
mC
ILT
TM
S+m
CIL
TT
MS
alon
e,w
ithin
2SD
ofB
asel
ine,
Pre-
TM
S+m
CIL
T†
Tim
ePo
stst
roke
Ons
et6
Yr.
4M
o.6
Yr.
7M
o.10
Yr.
8M
o.12
Yr.
3M
o.12
Yr.
5M
o.12
Yr.
10M
o.B
osto
nN
amin
gTe
stFi
rst2
0pi
ctur
es(m
ax=
20)
47
1011
.67
(2.8
9)17
.45
5.89
Y16
12B
osto
nD
iagn
osti
cA
phas
iaE
xam
Nam
ing
Subt
ests
Tool
s/Im
plem
ents
(max
=12
)2
32
1.67
(0.5
8)2.
830.
51Y
3∗4∗
Act
ions
(max
=12
)3
43
4.33
(0.5
8)5.
493.
17N
,-2S
D6∗
7∗A
nim
als
(max
=12
)0
12
4.67
(1.1
5)6.
972.
37N
,-2S
D4
4P
ictu
reD
escr
ipti
onC
ooki
eT
heft
Nar
rativ
eW
ords
11
14.
33(1
.15)
6.63
2.03
N,-
2SD
8∗6
Rep
etit
ion
Sing
leW
ords
(max
=10
)4
44
3.00
(2.0
0)7.
000
Y3
7∗A
udit
ory
Com
preh
ensi
on(v
.198
3)W
ord
Dis
crim
inat
ion
(max
=72
)53
5449
.50
48.8
3(4
.07)
56.9
740
.69
Y47
55C
omm
ands
(max
=15
)3
66
6.00
(1.7
3)9.
462.
54Y
34
Com
plex
Idea
tiona
lMat
eria
l(m
ax=
12)
22
42.
00(1
.00)
4.00
0Y
21
∗ Sco
rein
crea
sed
atle
ast2
SDfr
omB
asel
ine
(3×)
,for
trea
tmen
tint
erve
ntio
nse
ries
(TM
S+m
CIL
T).
† Tim
eIn
terv
albe
twee
nla
stte
stin
gPo
st-
TM
Sal
one
and
entr
yin
toT
MS+
mC
ILT
=1
Yr.
6M
o.

AU
THO
R C
OP
Y
P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia 491
treatment series. At that time, she continued to showimprovement in language skills, especially in auditorycomprehension, and in the voluntary use of words andphrases appropriate to her environment (Naeser et al.,2005a).
At 5 years 10 months after the initial series of TMS,P2 entered the current TMS+mCILT protocol. At entryinto the TMS+mCILT program, her mean BNT nam-ing score (11.67) was within the confidence intervalof her previous score (10, at 4 years 3 months post-that initial TMS treatment series). Her number of nar-rative words on the cookie theft picture description hadimproved from 0-1 word at 4 years 3 months post- theinitial series of TMS treatments, to a mean of 4.33, atBaseline testing for TMS+mCILT. The gains that hadbeen made after the initial TMS treatment series (andfollowing the speech therapy intervention at 1 yearpost- TMS), were stable on the BNT or improved onnumber of narrative words, at the time of entry into theTMS+mCILT program (Table 4).
2.2. Treatment methods
2.2.1. Transcranial magnetic stimulationprocedure
The TMS portion of this TMS+mCILT protocol isbased on our initial published TMS treatment proce-dure (Naeser et al., 2005b). Based on each patient’sparticipation in the previous TMS study (withoutspeech therapy), the R PTr was suppressed with 1 HzrTMS (Naeser et al., 2005a, 2010a). This area ismarked on the right lateral MRI view for each casein Fig. 1A and B.
The same TMS equipment that was used in the pre-vious TMS study (without speech therapy), was used inthis current study. On each of the ten days of treatment,1 Hz rTMS was applied for 20 min. using an air-cooled,figure 8-shaped TMS coil (each wing was 7 cm indiameter) (Fig. 1C). The rTMS pulses were deliv-ered at 90% of resting motor threshold for the L firstdorsal interosseus muscle, with a Super-Rapid HighFrequency MagStim Magnetic Stimulator (Magstim,UK). Positioning of the TMS coil on the scalp wasguided using the patient’s own structural MRI scan incombination with the neuronavigation system, Brain-sight (Rogue Industries, Montreal). Patients stayedovernight at the Beth Israel Deaconess Medical Center,General Clinical Research Center for the length of thetreatment series.
2.2.2. Modified constraint-induced languagetherapy procedure
Pre-Testing of Color PicturesPrior to any TMS+mCILT treatment, naming abil-
ity was tested on a set of up to 500 color pictures ofnouns (potential pictures for use during mCILT) (Lan-guage Builder, 2004; Stark, 1998). Before any testing,in order to be sure the patient understood the intendedtarget name, the patient was initially shown each pic-ture card and the tester said aloud the expected name.During the testing sessions, each color picture was pre-sented for 10 sec. on a laptop (Apple iBook). The sizeof each picture was controlled to be 3.5 × 4.8 inches,with a thin black border on a white background.
The color pictures were presented sequentially byfrequency of occurrence, from high frequency-of-occurrence words to low frequency-of-occurrencewords, based on the frequency of nouns fromThe Corpus of Contemporary American English(http://www.americancorpus.org) (Davies, 2008).Testing continued until the pictures became toodifficult to name and 10 pictures were missed in a row.On these color pictures, P1 did not miss 10 picturesin a row until a maximum of 360 pictures had beenpresented. P2 did not miss 10 pictures in a row untila maximum of 250 pictures had been presented. Eachpatient was then tested two more times on his/hermaximum set of pictures (for P1, 360 picture-set; forP2, 250 picture-set), for a total of three testing times.The patients were not trained on the color pictures atthis time, nor did they receive any feedback.
Based on the patient’s responses for each pic-ture at the 3 testing times, the maximum set ofpictures (for later use during mCILT therapy) weredivided as follows: 1) “always-named” (3/3 correct);2) “sometimes-named” (1/3 or 2/3 correct); and 3)“never-named” (0/3 correct).
Administration of mCILTOne hour of mCILT was administered immediately
following each 20-min TMS session. After a 1-hourbreak for lunch, 2 more hours of mCILT were admin-istered, for a total of 3 hours each day of massed,intensive practice.
The patient participated with a Speech-LanguagePathologist (SLP), instead of with another patient orgroup of patients. One patient was treated at a timewith mCILT. The patient was constrained to verballyrespond with a spoken name for a stimulus picture (nogestures, writing or sound effects were permitted). Anopaque screen was placed on a table between the SLP

AU
THO
R C
OP
Y
492 P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia
Fig. 2. mCILT treatment session setup. An opaque screen was placedon the table between the clinician and the patient. There was eyecontact only above the screen. There was a window to pass the cardback and forth (arrow). The patient was expected to name the pictureon the card. No gestures, writing or sound effects were permitted.
and the patient, who were seated across from eachother. The screen had a large opening at the bottomfor passing the cards back and forth between the SLPand the patient (Fig. 2, arrow). There was eye contactabove the screen. Two clinicians were involved in themCILT session. If the patient started to gesture, the sec-ond clinician, who had a view of the patient’s hands,reminded the patient that no gesturing was permittedand asked the patient to “sit on his/her left hand” duringthat response in order to prevent gesturing. The patientwas then able to use his left hand to turn over the nextcard or pass the card through the barrier.
Level of Difficulty (Frequency of Occurrence)within and across mCILT sessions
Pictures were sorted by frequency of occurrence,such that higher frequency-of-occurrence pictureswere presented for naming on day 1, and the lowerfrequency-of-occurrence pictures, on day 10. The pic-tures gradually increased in difficulty both throughouteach day, and across days 1–10 over the two-weekmCILT treatment series. Although different from thetraditional CILT approach by Pulvermuller et al.(2001), increasing the level of difficulty of the taskwas similar to other constraint-induced therapy pro-grams (Breier et al., 2009; Goral and Kempler, 2008;Maher et al., 2006) where behavioral shaping or scalingwas used.
During each mCILT session, 2 of the 6 pictures ina set were from the category of “always-named” at
entry; 2 of the 6 pictures, “sometimes-named”; and 2of the 6 pictures, “never-named”. The “always-named”pictures were included in order to reduce frustrationfor the patient. P2, the severe nonfluent patient didnot have enough “always-named” pictures at entry, topresent during all 10 days of therapy. Therefore, duringdays 5–10, the color pictures presented to P2 consistedonly of those pictures “sometimes-named”, or “never-named”. P2 responded well to therapy even on thesemore difficult pictures.
First and Second hours of mCILTTherapy took the form of a card game during hours
1 and 2 of mCILT. This card game was modeled afterthe dual-card task of Maher et al., 2006. One set of 6different, color picture cards was used at a time, pergame. The same set of 6 color pictures was played forthree games. Each day, three sets of 6 pictures each,were presented (18 different pictures). Picture cards tobe named aloud were turned over one at a time bythe patient, for each set of 6 pictures. The pictureswere individualized to each patient, from his/her maxi-mum set of color pictures from the pre- testing of colorpictures.
Third hour of mCILTThe patient and SLP participated in a different card
game during hour 3. The 18 pictures previously trainedduring hours 1 and 2 were used. The therapist hada board with 9 different pictures. The patient had aboard with the other 9 pictures. The therapist passedthrough the screen one picture card to name. If thepatient named the picture correctly, the patient couldplace a chip over that picture on either his/her board orthe therapist’s board. Play continued until both boardswere completed and all 18 pictures had been namedonce. This constituted one round. In the next round, thetherapist and patient then switched boards. There werethree rounds per day, with the same 18 pictures. There-fore, over the course of one day, each color picture waspresented to the patient 6 times.
ScoringSimilar to other therapy techniques such as ‘cueing
hierarchy’ treatment for anomia (Fridriksson, 2010,2006, 2007), the SLP provided the following structureand sequential cueing after each card was turned over,or presented for naming: 1) The patient was encour-aged to name the picture; 2) If named incorrectly, thepatient was encouraged to name the picture again; 3)If not named, the SLP gave a phonological cue forthe initial phoneme; 4) If still not named, the SLPgave a sentence for completion (from a prepared set

AU
THO
R C
OP
Y
P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia 493
of sentences where the target was the last word); 5)If still not named, the SLP had the patient repeat thecorrect name. A patient completed a set of picturesif he/she had at least one successful response withoutcueing for each of the 6 pictures.
On days 9 and 10, P1 (the mild-moderate patient),had successfully named at least once, without cueingall 360 color pictures presented to him; thus, therapywas focused on sentence production. He was askedto verbalize a new and unique sentence based on thepicture shown to him. All mCILT sessions were audioand videotaped for later reviewing and scoring.
2.3. Design
We utilized a multiple baseline, case study designwhere each patient served as his/her own control.Significant improvement post- treatment was definedas >2 SD above mean Baseline scores, across threeseparate test administrations, for any given test orsubtest.
2.4. Outcome measures
The primary outcome measures included the BNT(Kaplan et al., 2001), the BDAE Picture Naming, andelicited propositional speech for the cookie theft pic-ture description (Goodglass et al., 2001). Although notprimary outcome measures, the Repetition subtests,and all four of the Auditory Comprehension subtestsfrom an earlier version of the BDAE (Goodglass andKaplan, 1983) were also administered. Each test wasadministered three times during separate testing ses-sions at entry in order to establish a Baseline mean andSD; and once, at 1-2 months post- TMS+mCILT. P1was tested again at 16 months post- TMS+mCILT, andP2 was tested again at 6 months post- TMS+mCILT.
Elicited propositional speech (cookie theft picture)was analyzed using Quantitative Production Analy-sis (QPA) to determine changes in the grammaticalstructure, and lexical content of propositional speechsamples (Berndt et al., 2000; Rochon et al., 2000; Saf-fran et al., 1989). Data were collected for the followingaspects of speech production: longest uninterruptedphrase length, total number of narrative words, totalnumber of nouns, number of different nouns, totalnumber of verbs, number of different verbs, and meanlength of utterance. Patients were allowed a maximumof 2 minutes to describe the cookie theft picture.
2.5. Secondary analyses
During each treatment session, accuracy (percentcorrect) for color pictures named correctly withineach category (“always-named” at entry; “sometimes-named”; and “never-named”) was recorded for eachpatient. Secondary analyses were performed for accu-racy within each of these three separate categories, aswell as the total, for each patient, for each day.
3. Results
3.1. Results for P1
3.1.1. P1, outcome measuresAt 2 months post- TMS+mCILT, P1 (patient with
mild-moderate nonfluent aphasia) showed significantimprovement (>2 SD compared to Baseline) on theBNT, and on the BDAE subtest, Tools/Implements(Fig. 3A, B and Table 2). At 16 months post-TMS+mCILT, his score on the BNT was 16, whichcontinued to be higher (but not significantly so) com-pared to Baseline (mean of 14.3; SD, 1.15); and hisscore on the BDAE subtest, Tools/Implements returnedto Baseline.
On the BDAE cookie theft picture description, hispre- TMS+mCILT Baseline mean for longest uninter-rupted phrase length was 10.67 (SD, 4.16), and at 2months post- TMS+mCILT it remained 10. However,there were some quantitative and qualitative differ-ences in his utterances. P1 had a significant increase inthe total number of narrative words produced, from apre- TMS+mCILT Baseline mean of 46 (SD, 5.57), toa 2 month post- TMS+mCILT total of 59 (Fig. 4A andTable 2). He also had a significant increase in numberof different nouns produced from a pre- TMS+mCILTBaseline mean of 7.67 (SD, 1.15), to a 2 month post-TMS+mCILT total of 12 (Fig. 4B and Table 5A). P1showed no significant increase in the number of dif-ferent verbs produced post- TMS+mCILT (Table 5A).At 16 months post- TMS+mCILT he showed no lastingchange in his utterances, including number of narrativewords, or number of different nouns produced.
3.1.2. P1, secondary analysesThe total percent of color pictures named correctly
each day during treatment (Fig. 5) remained relativelyflat across days 1–8 (range, 85–94%, without cueing)despite the increasing level of difficulty (lower fre-quency of occurrence words). The percent of color

AU
THO
R C
OP
Y
494 P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia
Fig. 3. Performance on language outcome measures pre- and post- TMS+mCILT (black bars) for P1 (mild-moderate nonfluent aphasia) on A)BNT, and B) BDAE subtest, Tools/Implements. Previous scores are also shown when intervention was TMS alone (gray bars). *=+2 SD aboveBaseline for each treatment intervention series (TMS alone, or TMS+mCILT). See also Table 3.
pictures named within each of the three categories(“always-named” at entry; “sometimes-named”; and“never-named”), for days 1–8, are shown in Fig. 5.
Table 6A lists the color pictures “never-named” atentry, but successfully named (without cueing) eachday (1–8). The number after each word reflects thenumber of times P1 successfully named that picture,immediately after turning over the card. This rangesfrom 1, to a maximum of 6 for any given day. On day1, for P1, seven words previously “never-named” atentry, were now each named correctly, immediatelyafter turning over the card (6×), without any cueing ortraining, including the first time that picture was shown(e.g., table, team, foot, plate, shirt, chain, bottle).
For P1, performance on naming was also examinedby level of difficulty (frequency of occurrence) during
mCILT, and this was compared to performance on nam-ing by level of difficulty (frequency of occurrence) atentry. The following steps were taken in order to makethis comparison: 1) The maximum set of 360 picturesfor P1 was divided into deciles by frequency of occur-rence; 2) The patient’s performance at entry for eachdecile was calculated, and this is plotted in Fig. 6A(circles). This line shows that the percent of colorpictures named at entry, by decile, was nega-tively correlated with increasing level of difficulty(lower frequency-of-occurrence words), by decile(r = −0.850, p = 0.002); 3) The patient’s performanceduring mCILT for each decile was calculated, and thisis also plotted in Fig. 6A (triangles). This line showsthat the percent of color pictures named correctly, bydecile, during mCILT was also negatively correlated

AU
THO
R C
OP
Y
P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia 495
Table 5
Elicited propositional speech examples- BDAE, cookie theft picture, for P1 and P2
Pre- TMS+mCILT Baseline(3 testing sessions)
2 Months Post- TMS+mCILT(1 testing session)
16 Months Post- TMS+mCILT(1 testing session)
A) P1, Patient with mild-moderate Nonfluent AphasiaNumber of Different
NounsRange: 7–9 boy, stool, cookie jars,
cookies, water, dishes, sink, floor,mother
Total: 12* boys, bench, cookies, jar,hand, sister, bed, mother, water,cabinets, dishes, sink
Total: 8 mother, plates, sink, water,kid, cookie jars, girls, cookies
Number of DifferentVerbs
Range: 7–9 getting, is (3×), selling,was (3×), getting, started, fell,flowing, washing
Total: 7 were, was, going, has,cooking, falling, is
Total: 7 is, was (2×), watching,overflowed, went, fell, going
Pre-TMS+mCILT Baseline(3 testing sessions)
1 Month Post- TMS+mCILT(1 testing session)
6 Months Post- TMS+mCILT(1 testing session)
B) P2, Patient with severe Nonfluent AphasiaNumber of Different
NounsRange: 3-4 picture, water, cookie,
man, boy, towelTotal: 5* cookie, boy, water, man,
dishesTotal: 5* cookie, boy, water, benches,
dishesNumber of Different
VerbsRange: 0-1 falling Total: 3* working, walking, falling Total: 0 None uttered
*Score changed at least 2 SD from Baseline.
Fig. 4. Elements of propositional speech (cookie theft) pre- and post-TMS+mCILT (black bars) for P1 (mild-moderate nonfluent aphasia)for A) total number of narrative words, and B) number of differentnouns. Previous scores are also shown when intervention was TMSalone (gray bars). *=+2 SD above Baseline.
with increasing level of difficulty (lower frequency-of-occurrence words), by decile (r = −0.731, p = 0.016);4) The difference between the percent of color pic-
tures named correctly during mCILT, by decile, and thepercent of color pictures named correctly at entry, bydecile (overall, from highest frequency-of-occurrenceto lowest) was calculated. See Fig. 6B. For P1, thesedifferences in naming performance during mCILT (bydecile), versus at entry (by decile), increased as thelevel of difficulty increased (slope = 3.72, r = 0.721,p = 0.019). This shows that relative to entry nam-ing performance, during each day of TMS+mCILT,naming performance continued to improve, despiteincreasing level of difficulty (lower frequency-of-occurrence) presented for naming (Fig. 6B).
3.2. Results for P2
3.2.1. P2, outcome measuresP2 (patient with severe nonfluent aphasia) showed
significant improvement (>2 SD) on the BDAE sub-tests for Action Naming, and Tools/Implements, at 1and 6 months post- TMS+mCILT (Fig. 7A, B andTable 2); and Single Word Repetition at 6 months post-TMS+mCILT (Fig. 7C and Table 2).
On the cookie theft picture description, at 1 monthpost- TMS+mCILT, P2 showed a significant increasein the total number of narrative words (Fig. 8A),number of different nouns (Fig. 8B), and differentverbs (Table 2). At 6 months post- TMS+mCILT,the number of different nouns remained significant.Examples of her nouns and verbs produced dur-ing elicited propositional speech are provided inTable 5B.

AU
THO
R C
OP
Y
496 P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia
Fig. 5. P1 (mild-moderate nonfluent aphasia), total percent of pictures named correctly (without cueing) during each mCILT treatment day;“Always-named” at entry; “Sometimes-named”; and “never-named”. Note, P1 continued to correctly name pictures never named at entry, evenfor the lower frequency-of-occurrence words. By days 9 and 10, P1 had successfully named his maximum set of 360 color pictures at least oncewithout cueing. mCILT therapy then focused on sentence production.
3.2.2. P2, secondary analysesThe total percent of color pictures named cor-
rectly each day during treatment (Fig. 9) rangedfrom 52–72% (without cueing), despite the increas-ing level of difficulty (lower frequency of occurrencewords). The percent of color pictures named withineach of the three categories (“always-named” at entry;“sometimes-named”; and “never-named”), for days2–10 are shown in Fig. 9. (The data for day 1 wereincomplete.)
Table 6B lists the color pictures “never-named” atentry, but successfully named (without cueing) eachday (days 2–10). The number after each word listedreflects the number of times P2 successfully namedthat picture, immediately after turning over the card.This ranges from 1×, to a maximum of 6×. On day 3,for P2, two words previously “never-named” at entry,
were now named correctly immediately after turningover the card, without any cueing or training (6×),including the first time that picture was shown (e.g.,baseball, boat).
For P2, performance on naming was also examinedby level of difficulty (frequency of occurrence) dur-ing mCILT, and this was compared to performanceon naming by level of difficulty (frequency of occur-rence) at entry. The following steps were taken inorder to make this comparison: 1) The maximum setof 250 pictures for P2 was divided into deciles by fre-quency of occurrence; 2) The patient’s performanceat entry for each decile was calculated, and this isplotted in Fig. 10A (circles). This line shows that thepercent of color pictures named at entry, by decile,was negatively correlated with increasing level ofdifficulty (lower frequency-of-occurrence words), by

AU
THO
R C
OP
Y
P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia 497
Tabl
e6
Lis
tof
colo
rpi
ctur
es‘n
ever
-nam
ed’
aten
try,
buts
ucce
ssfu
llyna
med
atle
asto
nce
duri
ngT
MS+
mC
ILT
(with
outc
uein
g),f
orP1
and
P2
Day
1D
ay2
Day
3D
ay4
Day
5D
ay6
Day
7D
ay8
Day
9*D
ay10
*
A)
P1,P
atie
ntw
ithm
ild-m
oder
ate
Non
fluen
tAph
asia
(max
=6×
per
pict
ure
pres
enta
tion)
tabl
e×
6re
frig
erat
or×
6ra
inbo
w×
6m
aid
×6
neck
lace
×6
type
wri
ter×
6ca
terp
illar
×6
eggp
lant
×6
team
×6
rabb
it×
6ru
g×
6tu
rtle
×6
nood
les×
6ge
m×
5ch
ick
×6
polic
eca
r×
6fo
ot×
6do
ll×
6tr
iang
le×
6su
ngla
sses
×6
pean
uts×
6w
ater
fall
×5
ease
l×5
pick
les×
6pl
ate
×6
oval
×6
oran
ge×
6kn
ot×
5ol
ives
×6
cher
ries
×4
grap
efru
it×
5fa
ucet
×5
shir
t×6
curt
ains
×6
wel
l×5
scar
f×
5ru
ler×
6ra
isin
s×
4re
ctan
gle
×4
saxo
phon
e×
5ch
ain
×6
shor
ts×
5je
ep×
3ho
se×
4st
raw
berr
ies×
6hu
rdle
×2
head
phon
es×
4sw
eats
hirt
×4
bottl
e×
6ho
ok×
5ce
real
×3
robe
×1
napk
in×
6sa
fe×
2le
ash
×4
calc
ulat
or×
3bl
ocks
×5
helm
et×
5ch
ess×
3bu
bble
s×
5ro
oste
r×
3co
oler
×2
pepp
er×
5go
at×
5bu
tterfl
y×
3m
ug×
5re
mot
eco
ntro
l×2
chim
es×
2bl
ocks
×5
foun
tain
×5
tissu
es×
2br
iefc
ase
×5
bead
s×
1bo
wl×
5bo
w×
3ri
bbon
×1
blen
der×
5ri
ng×
4m
agne
t×4
pian
o×
3pl
ug×
4gr
ill×
3co
ffee
tabl
e×
3sh
ell×
2lig
htho
use
×2
mix
er×
2br
acel
et×
1be
etle
×1
B)
P2,P
atie
ntw
ithse
vere
Non
fluen
tAph
asia
(max
=6×
per
pict
ure
pres
enta
tion)
road
×4
base
ball
×6
circ
le×
3ja
cket
×6
dirt
×6
rock
s×
5co
uch
×5
van
×3
crow
n×
6In
com
plet
ew
indo
w×
3bo
at×
6ch
eese
×2
cat×
5de
er×
5so
up×
3w
atch
×5
gym
×2
glov
es×
6D
ata
girl
×3
foot
×5
bask
etba
ll×
1ju
ice
×4
knee
×4
ciga
rette
×2
jean
s×
5tu
nnel
×1
med
al×
2gl
ass×
1be
ach
×4
trai
n×
4st
airs
×4
mus
cle
×2
win
g×
4sh
ell×
1le
af×
1sq
uare
×3
chai
n×
2m
ail×
2ve
geta
bles
×1
*All
pict
ures
wer
esu
cces
sful
lyna
med
atle
asto
nce,
with
outc
uein
g,th
ustr
eatm
entf
ocus
edon
sent
ence
prod
uctio
n.

AU
THO
R C
OP
Y
498 P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia
Fig. 6. P1 (mild-moderate nonfluent aphasia), A) performance on naming by level of difficulty (frequency of occurrence) by decile, duringmCILT (triangles). Performance on naming by level of difficulty (frequency of occurrence) by decile, at entry (circles). B) The black diamondsshow the difference between percent of color pictures named correctly during mCILT intervention by decile, and the percent of color picturesnamed correctly at entry by decile (slope = 3.72, r = 0.721, p = 0.019). Thus, the differences in naming performance during mCILT (by decile),and at entry (by decile), increased as the level of difficulty increased. This suggests a beneficial effect of the TMS+mCILT intervention in namingperformance across the deciles, despite the increasing level of difficulty.
decile (r = −0.73, p = 0.026); 3) The patient’s perfor-mance during mCILT for each decile was calculated,and is plotted in Fig. 10A (triangles). Note, data forthe first decile are not plotted because naming datafor this decile during mCILT were incomplete (day1). This line shows that the percent of color picturesnamed correctly, by decile, during mCILT was flat andnot significantly correlated with increasing level ofdifficulty (lower frequency-of-occurrence), by decile(r = 0.007, n.s.); 4) The difference between the per-cent of color pictures named correctly during mCILT,by decile, and the percent of color pictures namedcorrectly at entry, by decile (overall, from highestfrequency-of-occurrence to lowest) was calculated.See Fig. 10B. For P2, these differences in naming per-formance during mCILT (by decile), versus at entry(by decile) increased as the level of difficulty increased(slope = 4.61, r = 0.71, p = 0.034). This shows that rel-ative to entry naming performance, during each dayof TMS+mCILT, naming performance continued to
improve, despite increasing level of difficulty (lowerfrequency-of-occurrence) presented for naming.
4. Discussion
This study showed that it was feasible to applyrTMS and immediately follow this with three hoursof mCILT. Results showed a significant improvementin naming pictures of objects or actions, and in propo-sitional speech (total number of narrative words anddifferent nouns) at 1-2 months post- TMS+mCILTfor each patient. While this study was not designedto specifically compare the effect of TMS alone ver-sus TMS+mCILT, each patient did show significantlyhigher scores on naming pictures of objects (includingtools/implements) or actions, and in total number ofnarrative words at 1-2 months post- TMS+mCILT, thanhad been previously observed post- the initial seriesof TMS treatments (Tables 3 and 4). It is unknown if

AU
THO
R C
OP
Y
P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia 499
Fig. 7. Performance on language outcome measures pre- and post- TMS+mCILT (black bars) for P2 (severe nonfluent aphasia) on BDAEsubtests: A) Action naming; B) Tools/Implements; and C) Single Word Repetition. Previous scores are also shown when intervention was TMSalone (gray bars). *=+2 SD above Baseline. See also Table 4.
the significant improvements in naming pictures, andelicited propositional speech were associated with thesecond series of TMS, or this first series of mCILT, ora combination of both.
For P1 (mild-moderate nonfluent aphasia), at2 months post- TMS+mCILT, there was signifi-cant improvement on the BNT, the BDAE subtestTools/Implements, and in measures of propositional
speech (total number of narrative words and differentnouns). At 16 months post- TMS+mCILT, the signif-icant gains that had been present at 2 months post-TMS+mCILT no longer remained.
For P2 (severe nonfluent aphasia), there was sig-nificant improvement on the BDAE naming subtestsfor Tools/Implements, and Actions, at 1 and 6 monthspost- TMS+mCILT. At 1 month post- TMS+mCILT,

AU
THO
R C
OP
Y
500 P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia
Fig. 8. Elements of propositional speech (cookie theft) pre- and post-TMS+mCILT (black bars) for P2 (severe nonfluent aphasia) for A)total number of narrative words, and B) number of different nouns.*=+2 SD above Baseline. Her phrase length, pre- and post- TMSalone, was only 0-1 word (not plotted here).
P2 showed significant improvement in measures ofpropositional speech (total number of narrative wordsand different nouns and different verbs). At 6 monthspost- TMS+mCILT the significant improvement onnumber of different nouns remained; there was newimprovement in Single Word Repetition where sherepeated 7 of the 10 words, whereas at Baseline shehad repeated only 3 of the words.
Although verb production was not specifically tar-geted during this mCILT therapy for P2, a significantincrease in the number of different verbs produced dur-ing the cookie theft picture description was observedat the 1-month testing (3 verbs versus mean of 0.67at Baseline). She also showed a significant improve-ment in naming Actions on the BDAE subtest at 1 and6 months post- TMS+mCILT where 6 and 7 Actionpictures were named versus a mean of 4.33 at Base-line. Improvement in naming pictures of Actions wasnot previously observed in this patient following theinitial TMS treatment series alone (Table 4). Verb pro-duction in narrative words for the cookie theft picture
description, however, returned to zero at 6 months afterthe last TMS+mCILT treatment.
Both patients stayed overnight at the Beth IsraelDeaconess Medical Center, General Clinical ResearchCenter for the 10 days of treatment. Despite the inten-sive aspects of mCILT, both patients cooperated fully.There were no adverse events and all treatment hourswere completed. Although the color pictures becameincreasingly difficult (lower frequency-of-occurrence)at each successive day, the total percent of colorpictures named correctly each day (without cueing)remained greater than at entry (Figs. 6A and 10A).Furthermore, both patients began to name picturesthat were previously “never-named.” On day 1, forexample, P1 named (without cueing), seven previously“never-named” pictures. The ability to name these pre-viously “never-named” pictures on day 1 could beattributed to the TMS portion of the treatment that day.However, on subsequent days, in addition to TMS, thecumulative impact of massed practice for naming addi-tional pictures throughout the day (mCILT) could havecontributed. This is unknown.
4.1. Possible mechanisms for TMS
The underlying mechanisms supporting improve-ments in naming and narrative speech following TMSsuppression of the R PTr are not fully known. Neu-roplasticity provides the ability to adapt to change;however, evidence suggests that this adaptation is notalways successful (Pascual-Leone et al., 2005). Thus,patients with chronic aphasia may operate in stable, butmaladaptive states (Belin et al., 1996; Hamilton et al.,2010; Rosen et al., 2000).
The observation of improved language behavior inpatients with aphasia following rTMS to suppress theR PTr has been reported in several studies (Barwoodet al., 2010; Hamilton et al., 2010; Martin et al.,2009a; Naeser et al., 2005a, 2005b, 2010a; Weiduschatet al., 2011). These TMS studies have suggested thatfollowing unilateral stroke, an imbalance in inter-hemispheric inhibition develops (Thiel et al., 2006).Repetitive TMS modulates neural activity, thus pro-moting changes and potential re-organization withinthe language networks resulting in improved behavior(Devlin and Watkins, 2007). Slow, 1 Hz rTMS maybe used to suppress the disinhibition within the Rfrontal region in patients who have suffered a LH strokeincluding L frontal areas, promoting better modula-tion in parts of each hemisphere, resulting in improved

AU
THO
R C
OP
Y
P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia 501
Fig. 9. P2 (severe nonfluent aphasia), total percent of pictures that were named correctly (without cueing) during each mCILT treatment day;“always-named” at entry; “sometimes-named”; and “never-named”. Data were incomplete for day 1. Note, P2 continued to correctly namepictures never named at entry, even for the lowest frequency-of-occurrence words. No color pictures in the “always-named” category from entrytesting were available for presentation during days 5–10.
brain function and behavior. Neither participant in thisstudy was able to participate in 3T functional MRI (dueto medical reasons) that could have provided infor-mation regarding neural network changes after TMSalone, or following TMS+mCILT.
The addition of mCILT immediately after rTMSmay have taken advantage of newly reset networksfrom rTMS, and enhanced these language connectionsfurther. This combined treatment may have promotedadditional improvement not seen with TMS alone, andperhaps even some generalization - i.e., P2 improved inverb production, although verbs were not specificallytrained with her during mCILT.
P1, mild-moderate aphasia, successfully named allpictures at least once without cueing and therefore inthe last two days of treatment, he was asked to createsentences using the picture shown on the card. Thisincrease in level of task difficulty is consistent with
the notion of behavioral shaping. It is unknown howthis increase in task difficulty impacted his naming orpropositional speech.
The optimum 1 cm square cortical area to treat withrTMS is important to consider for each patient. In thisstudy, the RH rTMS target site that had been previ-ously determined as each patient’s “Best Response”area for rTMS treatment alone, was used (Naeser etal., 2005a, 2010a). However, it is possible that this tar-get site was no longer the “optimum” target site, due toneural changes, including changes in functional con-nectivity that may have occurred after the initial TMSseries. This is unknown, however, both patients showedsignificant improvements with this same rTMS targetstimulation site. Some improvements in language havealso been reported after rTMS to other brain regions(Cotelli et al., 2011; Jung et al., 2010; Kakuda et al.,2010).

AU
THO
R C
OP
Y
502 P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia
Fig. 10. P2 (severe nonfluent aphasia), A) performance on naming by level of difficulty (frequency of occurrence) by decile, during mCILT(triangles). Performance on naming by level of difficulty (frequency of occurrence) by decile, at entry (circles). B) The black diamonds showthe difference between percent of color pictures named correctly during intervention by decile, and the percent of color pictures named correctlyat entry by decile (slope = 4.61, r = 0.71, p = 0.034). Thus, the differences in naming performance during mCILT (by decile), and at entry (bydecile), increased as the level of difficulty increased. This suggests a beneficial effect of the TMS+mCILT intervention in naming performanceacross the deciles, despite the increasing level of difficulty.
4.2. Future studies
It was not possible to separate out the relative con-tribution of a second series of TMS treatments fromthe addition of the mCILT treatments to the languageimprovements observed in the two aphasia patientspresented in this report. A larger, controlled clinicaltrial is needed to assess this. Also, further studies areneeded to determine if an additional TMS treatmentseries alone, and/or a language therapy series alonemay be necessary to sustain the new language improve-ments long-term. P2 improved in the Action namingsubtest of the BDAE and in number of different verbsin elicited propositional speech post- TMS+mCILT.CILT programs should be expanded to include targetedverb production (Goral and Kempler, 2008). Factorssuch as lesion site and aphasia severity are also impor-tant to consider in better understanding potential forrecovery (Naeser and Palumbo, 1994). Additionally, afourth core component (a transfer package adapted for
aphasia) should be added. This transfer package wouldbe similar to the fourth core component of CIMT,which facilitates transfer of gains made to real-worldsituations. Thus, carryover of improved functionalcommunication after TMS+mCILT should be docu-mented, including language use, during activities ofdaily living.
Acknowledgments
Research reported in this publication was sup-ported in part under Award Number RO1 DC05672from the National Institute on Deafness and OtherCommunication Disorders of the National Institutesof Health, Bethesda, MD. The content is solely theresponsibility of the authors and does not necessarilyrepresent the official views of the National Insti-tutes of Health; Other support for this publicationincludes a grant from the Medical Research Service,

AU
THO
R C
OP
Y
P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia 503
Department of Veterans Affairs, Washington, D.C.(to M.A.N.); a K24 NIH award (RRO18875), BBVAChair in Translational Medicine, Harvard Clinicaland Translational Science Center (UL1 RR025758),RO1-NS 47754, and RO1-NS 20068 (to A.P.-L.); theHarvard-Thorndike General Clinical Research Cen-ter (NCRR MO1 RR01032); and NIH grant P30DC05207, National Institute on Deafness and OtherCommunication Disorders (to the Harold GoodglassBoston University Aphasia Research Center). Theauthors thank the following people for their contribu-tions to the study: Kristine Lundgren, Sc.D., for CILTstudy and design consultation; Elina Kaplan, B.S., andMallory Finley, B.A., for data collection.
References
Baker, J.M., Rorden, C., & Fridriksson, J. (2010). Using transcranialdirect-current stimulation to treat stroke patients with aphasia.Stroke, 41(6), 1229-1236.
Barwood, C.H., Murdoch, B.E., Whelan, B.M., Lloyd, D., Riek, S.,OSullivan, J.D., Coulthard, A., & Wong, A. (2011). Improvedlanguage performance subsequent to low-frequency rTMS inpatients with chronic non-fluent aphasia post-stroke. Eur J Neu-rol, 18(7), 935-943.
Belin, P., Van Eeckhout, P., Zilbovicius, M., Remy, P., Francois, C.,Guillaume, S., Chain, F., Rancurel, G., & Samson, Y. (1996).Recovery from nonfluent aphasia after melodic intonation ther-apy: A PET study. Neurol, 47(6), 1504-1511.
Berndt, R.S., Wayland, S., Rochon, E., Saffran, E.M., & Schwartz,M.F. (2000). Quantitative Production Analysis: A training man-ual for the analysis of aphasic sentence production. PsychologyPress Ltd.
Berthier, M.L., Green, C., Lara, J.P., Higueras, C., Barbancho,M.A., Davila, G., & Pulvermuller, F. (2009). Memantine andconstraint-induced aphasia therapy in chronic poststroke apha-sia. Ann Neurol, 65(5), 577-585.
Berthier, M.L., & Pulvermuller, F. (2011). Neuroscience insightsimprove neurorehabilitation of poststroke aphasia. Nat RevNeurol, 7(2), 86-97.
Bolognini, N., Pascual-Leone, A., & Fregni, F. (2009). Using non-invasive brain stimulation to augment motor training-inducedplasticity. J Neuroeng Rehabil, 6, 8.
Breier, J.I., Juranek, J., Maher, L.M., Schmadeke, S., Men, D., &Papanicolaou, A.C. (2009). Behavioral and neurophysiologicresponse to therapy for chronic aphasia. Arch Phys Med Reha-bil, 90(12), 2026-2033.
Brighina, F., Bisiach, E., Oliveri, M., Piazza, A., La Bua, V., Daniele,O., & Fierro, B. (2003).1 hz repetitive transcranial magneticstimulation of the unaffected hemisphere ameliorates contrale-sional visuospatial neglect in humans. Neurosci Lett, 336(2),131-133.
Cherney, L.R., Patterson, J.P., Raymer, A., Frymark, T., & Schooling,T. (2008). Evidence-based systematic review, Effects of inten-
sity of treatment and constraint-induced language therapy forindividuals with stroke-induced aphasia. J Speech Lang HearRes, 51(5), 1282-1299.
Cotelli, M., Fertonani, A., Miozzo, A., Rosini, S., Manenti, R.,Padovani, A., Ansaldo, A.I., Cappa, S.F., & Miniussi, C. (2011).Anomia training and brain stimulation in chronic aphasia. Neu-ropsychol Rehabil, 21(5), 717-741.
Davies, M. (2008). The corpus of contemporary Ameri-can English (COCA), 400+ million words, 1990-present.http://www.americancorpus.org
Devlin, J.T., & Watkins, K.E. (2007). Stimulating language: Insightsfrom TMS. Brain, 130(Pt 3), 610-622.
Difrancesco, S., Pulvermuller, F., & Mohr, B. (2012). Intensivelanguage-action therapy (ILAT): The methods. Aphasiology,26(11), 1317-1351.
Floel, A., Meinzer, M., Kirstein, R., Nijhof, S., Deppe, M., Knecht,S., & Breitenstein, C. (2011). Short-term anomia training andelectrical brain stimulation. Stroke, 42(7), 2065-2067.
Fregni, F., Boggio, P.S., Valle, A.C., Rocha, R.R., Duarte, J., Fer-reira, M.J., Wagner, T., Fecteau, S., Rigonatti, S.P., Riberto,M., Freedman, S.D., & Pascual-Leone, A. (2006). A sham-controlled trial of a 5-day course of repetitive transcranialmagnetic stimulation of the unaffected hemisphere in strokepatients. Stroke, 37(8), 2115-2122.
Fridriksson, J. (2010). Preservation and modulation of specific lefthemisphere regions is vital for treated recovery from anomia instroke. J Neurosci, 30(35), 11558-11564.
Fridriksson, J., Morrow-Odom, L., Moser, D., Fridriksson, A., &Baylis, G. (2006). Neural recruitment associated with anomiatreatment in aphasia. Neuroimage, 32(3), 1403-1412.
Fridriksson, J., Moser, D., Bonilha, L., Morrow-Odom, K.L., Shaw,H., Fridriksson, A., Baylis, G.C., & Rorden, C. (2007). Neuralcorrelates of phonological and semantic-based anomia treat-ment in aphasia. Neuropsychologia, 45(8), 1812-1822.
Gauthier, L.V., Taub, E., Perkins, C., Ortmann, M., Mark, V.W.,& Uswatte, G. (2008). Remodeling the brain: Plastic struc-tural brain changes produced by different motor therapies afterstroke. Stroke, 39(5), 1520-1525.
Goodglass, H., Kaplan, E., & Barresi, B. (2001). The assessment ofaphasia and related disorders (3rd Edition). Philadelphia, PA,Lippincott, Williams and Wilkins.
Goral, M., & Kempler, D. (2008). Training verb production incommunicative context: Evidence from a person wtih chronicnon-fluent aphasia. Aphasiology (Sept), 1-15.
Hakkennes, S., & Keating, J.L. (2005). Constraint-induced move-ment therapy following stroke: A systematic review ofrandomised controlled trials. Aust J Physiother, 51(4), 221-231.
Hamilton, R.H., Sanders, L., Benson, J., Faseyitan, O., Norise, C.,Naeser, M., Martin, P., & Coslett, H.B. (2010). Stimulatingconversation: Enhancement of elicited propositional speech ina patient with chronic non-fluent aphasia following transcranialmagnetic stimulation. Brain Lang, 113(1), 45-50.
Hesse, S., Werner, C., Schonhardt, E.M., Bardeleben, A., Jenrich,W., & Kirker, S.G. (2007). Combined transcranial direct currentstimulation and robot-assisted arm training in subacute strokepatients: A pilot study. Restor Neurol Neurosci, 25(1), 9-15.

AU
THO
R C
OP
Y
504 P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia
Jung, T.D., Kim, J.Y., Lee, Y.S., Kim, D.H., Lee, J.J., Seo, J.H.,Lee, H.J., & Chang, Y. (2010). Effect of repetitive transcranialmagnetic stimulation in a patient with chronic crossed aphasia:fMRI study. J Rehabil Med, 42(10), 973-978.
Kakuda, W., Abo, M., Kaito, N., Watanabe, M., & Senoo, A. (2010).Functional MRI-based therapeutic rTMS strategy for aphasicstroke patients: A case series pilot study. Int J Neurosci, 120(1),60-66.
Kaplan, E., Goodglass, H., & Weintraub, S. (2001). The BostonNaming Test. Philadelphia, PA: Lippincott, Williams andWilkins.
Kessler, J., Thiel, A., Karbe, H., & Heiss, W.D. (2000). Piracetamimproves activated blood flow and facilitates rehabilitation ofpoststroke aphasic patients. Stroke, 31(9), 2112-2116.
Koch, G., Oliveri, M., Cheeran, B., Ruge, D., Lo Gerfo, E., Salerno,S., Torriero, S., Marconi, B., Mori, F., Driver, J., Rothwell, J.C.,& Caltagirone, C. (2008). Hyperexcitability of parietal-motorfunctional connections in the intact left-hemisphere of patientswith neglect. Brain, 131(Pt 12), 3147-3155.
Language Builder (2004). Picture noun cards. Chico, CA: StagesLearning Materials.
Maher, L.M., Kendall, D., Swearengin, J.A., Rodriguez, A., Leon,S.A., Pingel, K., Holland, A., & Rothi, L.J. (2006). A pilot studyof use-dependent learning in the context of constraint-inducedlanguage therapy. J Int Neuropsychol Soc, 12(6), 843-852.
Martin, P.I., Naeser, M.A., Ho, M., Doron, K.W., Kurland, J., Kaplan,J., Wang, Y., Nicholas, M., Baker, E.H., Fregni, F., & Pascual-Leone, A. (2009a). Overt naming fMRI pre- and post-TMS:Two nonfluent aphasia patients, with and without improvednaming post-TMS. Brain Lang, 111(1), 20-35.
Martin, P.I., Naeser, M.A., Ho, M., Treglia, E., Kaplan, E., Baker,E.H., & Pascual-Leone, A. (2009b). Research with transcranialmagnetic stimulation in the treatment of aphasia. Curr NeurolNeurosci Rep, 9(6), 451-458.
Medina J., Norise C., Faseyitan O., Coslett H.B., Turkeltaub P.E.,& Hamilton R.H. (2012). Finding the right words: Transcra-nial magnetic stimulation improves discourse productivity innon-fluent aphasia after stroke. Aphasiology, 26(9), 1153-1168.
Meinzer, M., & Breitenstein, C. (2008). Functional imaging studiesof treatment-induced recovery in chronic aphasia. Aphasiology,22(12), 1251-1268.
Meinzer, M., Djundja, D., Barthel, G., Elbert, T., & Rockstroh, B.(2005). Long-term stability of improved language functionsin chronic aphasia after constraint-induced aphasia therapy.Stroke, 36(7), 1462-1466.
Meinzer, M., Elbert, T., Djundja, D., Taub, E., & Rockstroh, B.(2007). Extending the constraint-induced movement therapy(cimt) approach to cognitive functions: Constraint-inducedaphasia therapy (CIAT) of chronic aphasia. NeuroRehab, 22(4),311-318.
Meinzer, M., Flaisch, T., Breitenstein, C., Wienbruch, C., Elbert, T.,& Rockstroh, B. (2008). Functional re-recruitment of dysfunc-tional brain areas predicts language recovery in chronic aphasia.Neuroimage, 39(4), 2038-2046.
Meinzer, M., Rodriguez, A.D., & Gonzalez Rothi, L.J. (2012).First decade of research on constrained-induced treatment
approaches for aphasia rehabilitation. Arch Phys Med Rehabil,93(1 Suppl), S35-S45.
Naeser, M.A., Martin, P.I., Lundgren, K., Klein, R., Kaplan, J.,Treglia, E., Ho, M., Nicholas, M., Alonso, M., & Pascual-Leone, A. (2010a). Improved language in a chronic nonfluentaphasia patient after treatment with CPAP and TMS. CognBehav Neurol, 23(1), 29-38.
Naeser, M.A., Martin, P.I., Nicholas, M., Baker, E.H., Seekins, H.,Helm-Estabrooks, N., Cayer-Meade, C., Kobayashi, M., The-oret, H., Fregni, F., Tormos, J.M., Kurland, J., Doron, K.W.,& Pascual-Leone, A. (2005a). Improved naming after TMStreatments in a chronic, global aphasia patient–case report.Neurocase, 11(3), 182-193.
Naeser, M.A., Martin, P.I., Nicholas, M., Baker, E.H., Seekins, H.,Kobayashi, M., Theoret, H., Fregni, F., Maria-Tormos, J., Kur-land, J., Doron, K.W., & Pascual-Leone, A. (2005b). Improvedpicture naming in chronic aphasia after TMS to part of rightBroca’s area: An open-protocol study. Brain Lang, 93(1), 95-105.
Naeser, M.A., Martin, P.I., Treglia, E., Ho, M., Kaplan, E., Bashir,S., Hamilton, R., Coslett, H.B., & Pascual-Leone, A. (2010b).Research with rTMS in the treatment of aphasia. Restor NeurolNeurosci, 28(4), 511-529.
Naeser, M.A., & Palumbo, C.L. (1994). Neuroimaging and languagerecovery in stroke. J Clin Neurophysiol, 11(2), 150-174.
Naeser, M.A., Palumbo, C.L., Helm-Estabrooks, N., Stiassny-Eder,D., & Albert, M.L. (1989). Severe nonfluency in aphasia. Roleof the medial subcallosal fasciculus and other white matterpathways in recovery of spontaneous speech. Brain, 112(Pt 1),1-38.
Pascual-Leone, A., Amedi, A., Fregni, F., & Merabet, L.B. (2005).The plastic human brain cortex. Annu Rev Neurosci, 28, 377-401.
Pulvermuller, F., Neininger, B., Elbert, T., Mohr, B., Rockstroh, B.,Koebbel, P., & Taub, E. (2001). Constraint-induced therapy ofchronic aphasia after stroke. Stroke, 32(7), 1621-1626.
Richter, M., Miltner, W.H., & Straube, T. (2008). Associationbetween therapy outcome and right-hemispheric activation inchronic aphasia. Brain, 131(Pt 5), 1391-1401.
Rochon, E., Saffran, E.M., Berndt, R.S., & Schwartz, M.F. (2000).Quantitative analysis of aphasic sentence production: Furtherdevelopment and new data. Brain Lang, 72(3), 193-218.
Rosen, H.J., Petersen, S.E., Linenweber, M.R., Snyder, A.Z., White,D.A., Chapman, L., Dromerick, A.W., Fiez, J.A., & Corbetta,M.D. (2000). Neural correlates of recovery from aphasia afterdamage to left inferior frontal cortex. Neurol, 55(12), 1883-1894.
Rossi, S., & Rossini, P.M. (2004). TMS in cognitive plasticity andthe potential for rehabilitation. Trends Cogn Sci, 8(6), 273-279.
Saffran, E.M., Berndt, R.S., & Schwartz, M.F. (1989). The quanti-tative analysis of agrammatic production: Procedure and data.Brain Lang, 37(3), 440-479.
Stark, J. (1998). Everyday life activities photo series. Jentzsch:Vienna.
Talelli, P., & Rothwell, J. (2006). Does brain stimulation after strokehave a future? Curr Opin Neurol, 19(6), 543-550.

AU
THO
R C
OP
Y
P.I. Martin et al. / TMS plus speech therapy in nonfluent aphasia 505
Taub, E. (2004). Harnessing brain plasticity through behavioral tech-niques to produce new treatments in neurorehabilitation. AmPsychol, 59(8), 692-704.
Taub, E., Crago, J.E., Burgio, L.D., Groomes, T.E., Cook, E.W., 3rd,DeLuca, S.C., & Miller, N.E. (1994). An operant approach torehabilitation medicine: Overcoming learned nonuse by shap-ing. J Exp Anal Behav, 61(2), 281-293.
Taub, E., Uswatte, G., & Pidikiti, R. (1999). Constraint-inducedmovement therapy: A new family of techniques with broadapplication to physical rehabilitation–a clinical review. J Reha-bil Res Dev, 36(3), 237-251.
Thiel A., Hartmann A., Rubi-Fessen I., Anglade C., Kracht L., Wei-duschat N., Kessler J., Rommel T., & Heiss W.D. (2013). Effectsof noninvasive brain stimulation on language networks andrecovery in early poststroke aphasia. Stroke, 44(8), 2240-2246.
Thiel, A., Schumacher, B., Wienhard, K., Gairing, S., Kracht,L.W., Wagner, R., Haupt, W.F., & Heiss, W.D. (2006). Directdemonstration of transcallosal disinhibition in language net-works. J Cereb Blood Flow Metab, 26(9), 1122-1127.
Turkeltaub P.E., Coslett H.B., Thomas A.L., Faseyitan O., BensonJ., Norise C., & Hamilton R.H. (2012). The right hemisphereis not unitary in its role in aphasia recovery. Cortex, 48(9),1179-1186.
Vines, B.W., Norton, A.C., & Schlaug, G. (2011). Non-invasive brainstimulation enhances the effects of melodic intonation therapy.Front Psychol, 2, 230.
Weiduschat, N., Thiel, A., Rubi-Fessen, I., Hartmann, A., Kessler, J.,Merl, P., Kracht, L., Rommel, T., & Heiss, W.D. (2011). Effectsof repetitive transcranial magnetic stimulation in aphasic stroke:A randomized controlled pilot study. Stroke, 42(2), 409-415.




















