Investigating Environmental Links Between Parent Depression and Child Depressive/Anxiety Symptoms...
10
NEW RESEARCH Investigating Environmental Links Between Parent Depression and Child Depressive/Anxiety Symptoms Using an Assisted Conception Design Gemma Lewis, B.Sc., Frances Rice, Ph.D., Gordon T. Harold, Ph.D., Stephan Collishaw, Ph.D., Anita Thapar, Ph.D. Objective: Links between maternal and offspring depression symptoms could arise from inherited factors, direct environmental exposure, or shared adversity. A novel genetically sensitive design was used to test the extent of environmental links between maternal depression symptoms and child depression/anxiety symptoms, accounting for inherited effects, shared adversity, and child age and gender. Method: Eight hundred fifty-two families with a child born by assisted conception provided questionnaire data. Mothers and fathers were genetically related or unrelated to the child depending on conception method. Parental depression symptoms were assessed using the Hospital Anxiety and Depression Scale. Child depression/anxiety symptoms were assessed using the Short Mood and Feelings questionnaire and six items tapping generalized anxiety disorder symptoms. Associations between maternal and child symptoms were examined separately for genetically unrelated and related mother– child pairs, adjusting for three measurements of shared adversity: negative life events, family income, and socioeconomic status. Analyses were then run separately for boys and girls and for children and adolescents, and the role of paternal depression symptoms was also examined. Results: Significant associations between parent and child symptoms were found for genetically unrelated mother– child (r 0.32, p .001) and father– child (r 0.17, p .05) pairs and genetically related mother– child (r 0.31, p .001) and father– child (r 0.23, p .001) pairs and were not explained by the shared adversity measurements. Environmental links were present for children and adolescents and were stronger for girls. Conclusions: The transmission of depression symptoms is due in part to environmental processes indepen- dent of inherited effects and is not accounted for by shared adversity measurements. Girls may be more sensitive to the negative effects of maternal depression symptoms than boys through environmental processes. J. Am. Acad. Child Adolesc. Psychiatry, 2011;50(5): 451– 459. Key Words: depression, anxiety, transmission, environmental, genetic C hildren of depressed parents are two to three times more likely than the offspring of nondepressed controls to exhibit ele- vated levels of depression and anxiety symptoms and depressive disorder. 1 Despite consistent ev- idence that depression is familial, few studies have tested the processes underlying intergen- erational transmission of symptoms by teasing apart competing explanations. First, exposure to parent depression symptoms may have a direct environmental effect on children. Second, links between parent and child symptoms could arise through inherited factors. Third, shared exposure to adversities such as bereavement, divorce, or poverty may increase risk for depression in par- ents and children, accounting for observed trans- mission effects. A greater understanding of the pathways involved in intergenerational trans- This article is discussed in an editorial by Dr. David Reiss on page 431. Supplemental material cited in this article is available online. JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY VOLUME 50 NUMBER 5 MAY 2011 451 www.jaacap.org
Transcript of Investigating Environmental Links Between Parent Depression and Child Depressive/Anxiety Symptoms...

NEW RESEARCH
Investigating Environmental Links BetweenParent Depression and Child
Depressive/Anxiety Symptoms Using anAssisted Conception Design
Gemma Lewis, B.Sc., Frances Rice, Ph.D., Gordon T. Harold, Ph.D.,Stephan Collishaw, Ph.D., Anita Thapar, Ph.D.
Objective: Links between maternal and offspring depression symptoms could arise frominherited factors, direct environmental exposure, or shared adversity. A novel geneticallysensitive design was used to test the extent of environmental links between maternaldepression symptoms and child depression/anxiety symptoms, accounting for inheritedeffects, shared adversity, and child age and gender. Method: Eight hundred fifty-twofamilies with a child born by assisted conception provided questionnaire data. Mothersand fathers were genetically related or unrelated to the child depending on conceptionmethod. Parental depression symptoms were assessed using the Hospital Anxiety andDepression Scale. Child depression/anxiety symptoms were assessed using the ShortMood and Feelings questionnaire and six items tapping generalized anxiety disordersymptoms. Associations between maternal and child symptoms were examined separatelyfor genetically unrelated and related mother– child pairs, adjusting for three measurementsof shared adversity: negative life events, family income, and socioeconomic status.Analyses were then run separately for boys and girls and for children and adolescents, andthe role of paternal depression symptoms was also examined. Results: Significantassociations between parent and child symptoms were found for genetically unrelatedmother– child (r � 0.32, p � .001) and father– child (r � 0.17, p � .05) pairs and geneticallyrelated mother– child (r � 0.31, p � .001) and father– child (r � 0.23, p � .001) pairs andwere not explained by the shared adversity measurements. Environmental links werepresent for children and adolescents and were stronger for girls. Conclusions: Thetransmission of depression symptoms is due in part to environmental processes indepen-dent of inherited effects and is not accounted for by shared adversity measurements. Girlsmay be more sensitive to the negative effects of maternal depression symptoms than boysthrough environmental processes. J. Am. Acad. Child Adolesc. Psychiatry, 2011;50(5):451– 459. Key Words: depression, anxiety, transmission, environmental, genetic
C hildren of depressed parents are two tothree times more likely than the offspringof nondepressed controls to exhibit ele-
vated levels of depression and anxiety symptomsand depressive disorder.1 Despite consistent ev-idence that depression is familial, few studies
This article is discussed in an editorial by Dr. David Reiss on page431.
Supplemental material cited in this article is available online.
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011
have tested the processes underlying intergen-erational transmission of symptoms by teasingapart competing explanations. First, exposure toparent depression symptoms may have a directenvironmental effect on children. Second, linksbetween parent and child symptoms could arisethrough inherited factors. Third, shared exposureto adversities such as bereavement, divorce, orpoverty may increase risk for depression in par-ents and children, accounting for observed trans-mission effects. A greater understanding of the
pathways involved in intergenerational trans-451www.jaacap.org

dipam
tatsmwtsrsamp
LEWIS et al.
mission can help in the identification of modifi-able risk factors for child/adolescent depressionsymptoms that could be targeted in preventiveand therapeutic interventions.
Few studies have used genetically sensitivedesigns to estimate the influence of inheritedfactors and separate environmental from geneticeffects.2-5 One study did not assess maternaldepression directly5 and another reported incon-sistent findings depending on the informantused.4 Two studies have directly tested environ-mental transmission of maternal depression.2,3
Tully et al.2 reported significant associations be-tween maternal major depression and child ma-jor depression in adopted and nonadopted fam-ilies, with greater associations in nonadoptedmother–child pairs, suggesting environmentaland genetic effects. Using a children-of-twins de-sign, Silberg et al.3 found that the intergenerationaltransmission of maternal depression symptomswas due to family environmental factors butreported no genetic influence. Findings have sug-gested that parent depression symptoms mayexert environmental risk effects on child depres-sion symptoms. However, previous studies havenot ruled out the possibility that specific mea-surements of shared environmental adversity(affecting parents and offspring) contribute tothis environmental link or account for theassociation between maternal depression andchild symptoms.
Further research on the mechanisms underly-ing intergenerational transmission of depressionis required. In addition to the role of sharedadversity, such research should consider the ef-fects of child gender and age, which have notbeen examined using genetically sensitive de-signs. There is evidence that different factors maybe involved in the etiology and intergenerationaltransmission of depression for boys and girls.6
Some studies have found that the associationbetween maternal and offspring depression isstronger in daughters than in sons.7,8 However,other studies have not reported significant gen-der differences.9 The etiology of child and ado-lescent depression may also vary according to thedevelopmental stage of children. A consistentfinding from twin research has been that geneticinfluences on depression symptoms are greaterin adolescents, whereas shared environment ismore influential in children.10 This suggests thatnoninherited factors could play a more promi-
nent role in the intergenerational transmission ofJOURN
452 www.jaacap.org
epression symptoms for younger children. Theres also consistent evidence that anxiety and de-ression symptoms have shared genetic liabilitynd that, in prepubertal children, this liabilityore commonly manifests as anxiety.11 This sug-
gests the need to examine anxiety and depressionin the offspring of depressed parents.
The present study, based on a sample of childrenconceived by assisted reproduction, aimed to testwhether there are environmentally mediated linksbetween parental depression and child depres-sion/anxiety, and whether they are accountedfor by exposure to three measurements of sharedadversity-negative life events, family income,and socioeconomic status. In addition, the effectsof child age and gender were investigated. Thesample allows tests of environmental and genetictransmission using principles akin to the classicbehavioral genetic adoption design: comparisonsof associations between genetically unrelatedand related parent–child pairs. Associations ofparent and child symptoms in genetically unre-lated dyads indicates the presence of environ-mental transmission, implicating the role of theshared environment (C), whereas evidence forgenetic effects would be shown if associations aregreater in related versus unrelated pairs (G). Arecent study using this sample examined depres-sion and conduct symptoms in children andfound preliminary evidence of environmentallinks.12 However, this study focused on media-ion of the association by parent–child warmthnd hostility and did not rule out the possibilityhat alternative influences such as shared adver-ity may account for effects or that associationsay differ according to child age and gender. Itas hypothesized in the present study that ma-
ernal depression symptoms, in addition tohowing inherited transmission, would have di-ect environmental links not accounted for byhared adversity, with symptoms of depressionnd anxiety in children, and that the environ-ental association would be stronger in girls and
readolescent children younger than 11 years.
METHODSampleThe sample consisted of families recruited from 19fertility clinics across the United Kingdom and one inthe United States who had undergone in vitro fertil-ization (IVF), with children born from 1994 through2002. Twenty-two clinics were approached and 19
agreed to participate, representing a clinic responseAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011

mmcfgcsDtiTt
rspSi
twa
otpe
ENVIRONMENTAL TRANSMISSION OF DEPRESSION SYMPTOMS
rate of 86%. Children included in this report wereconceived by one of four IVF methods: homologous(genetically related to both parents), sperm donation(genetically related to mother only), egg donation (genet-ically related to father only), or embryo donation (genet-ically related to neither parent). All gamete donors wereunrelated to parents. One child from each family partic-ipated. For multiple births, parents were asked to reporton the firstborn child. Data were collected by postalquestionnaire from mothers and fathers on two occasions(Time 1 [T1], 2006; Time 2 [T2], 2009). Questionnairesincluded a range of measurements assessing details ofthe pregnancy, child psychopathology, family environ-ment, and parental psychopathology.
One thousand one hundred fifty-eight familieswere sent questionnaires at T1. Responses were re-ceived from 852 families (74% response rate). Sevenhundred eighty-one families agreed to be contactedabout further studies and these families were mailedfollow-up questionnaires at T2. At T2, responses werereceived from 482 families (62% response rate). Partic-ipants who dropped out at T2 did not differ from thosewho remained in the study in maternal depressionsymptoms at T1 (mean retained in study � 4.24,standard deviation [SD] � 3.04; mean dropped out ofstudy � 4.46, SD � 3.10, t848 � 1.04, p � .30) or childdepression/anxiety as rated by the mother (meanretained in study � 4.68, SD � 3.96; mean dropped outof study � 4.50, SD � 4.57, t847 � 0.61, p � .55) and bythe father (mean retained in study � 4.34, SD � 4.29;mean dropped out of study � 3.93, SD � 4.29, t568 �1.15, p � .25). Attrition was not associated with geneticrelatedness to the child (�2
1 � 0.94, p � .33). The effectsof potential biases caused by sample attrition wereinvestigated by running T1 analyses on the subgroupretained across waves; the same pattern of results wasfound (available on request).
Comparisons with U.K. national norms have shownthat this sample does not differ from the generalpopulation in psychological adjustment, with minimaldifferences found between the conception groups.13
The present study used data from families in which themother had responded (n � 852, 431 boys, 421 girls atT1; n � 459, 231 boys, 228 girls at T2). At T1 thenumbers in each conception group were 436 homolo-gous, 208 sperm donation, 173 egg donation, and 35embryo donation, and at T2 the numbers were 254homologous, 99 sperm donation, 91 egg donation, and15 embryo donation. The genetically unrelated groupconsisted of 208 mother–child pairs (egg, embryodonation) and the genetically related group consistedof 644 mother–child pairs (homologous, sperm dona-tion). Children were 4 to 10 years old (mean � 6.3years) at T1 and 7 to 13 years old (mean � 9.9 years) atT2. Mothers were 27 to 61 years old (mean � 41.44years) and fathers were 28 to 76 years old (mean � 44.3years) at T1. Most children (91%) resided with both
parents.JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011
MeasurementsMaternal Depression Symptoms. Maternal depressionsymptoms were assessed using the seven-item self-report depression subscale of the Hospital Anxiety andDepression Scale.14 This subscale showed good inter-nal consistency in this sample (� � 0.75 at T1 and � �0.70 at T2) and is well validated.15 Scores on thesubscale range from 0 through 21, with higher scoresrepresenting greater depression symptoms. A recom-mended clinical cutpoint higher than 8 has been vali-dated in clinical and community samples.15
Child Anxiety and Depression Symptoms. Child de-pression symptoms were assessed using parent ratings(mothers and fathers separately) on the Short Moodand Feelings Questionnaire (SMFQ). Child self-reportswere not obtained because of the children’s young ageand for ethical reasons (children might not be aware ofparental IVF treatment). The SMFQ is a 13-item self-report measurement of the presence and severity ofDSM-IV depression symptoms, which showed goodinternal consistency in this sample (� � 0.73 for
others and 0.79 for fathers at T1 and � � 0.75 forothers at T2), and is a well-validated measurement in
linical and community samples.16 Total scores rangerom 0 through 26, with higher scores representingreater depression symptoms and the recommendedlinical cutpoint is higher than 8.16 Child anxietyymptoms were assessed using parent reports on sixSM-IV items for generalized anxiety disorder over
he previous 3 months (worries, restless, easily tired,rritable, difficulty concentrating, problems sleeping).he anxiety scale showed good internal consistency in
his sample (� � 0.73 for mothers and 0.67 for fathersat T1 and � � 0.76 for mothers at T2). Anxiety scoresanged from 0 through 12, with higher scores repre-enting greater anxiety symptoms. A combined de-ression/anxiety scale was created by summingMFQ and DSM-IV anxiety items and showed goodnternal consistency (� � 0.83 for mothers and 0.85 for
fathers at T1 and � � 0.87 for mothers at T2). Scores onhe composite measurement ranged from 0 through 38,
ith higher scores representing more depression/nxiety symptoms.
Negative Life Events. A 35-item Life Events Check-list17 completed by mothers measured the occurrence
f a range of significant events in the child’s life duringhe previous year such as “death of a parent, grand-arent or sibling.” Fourteen independent negative lifevents likely to affect mother and child were used.
Family Income. Mothers and fathers were each askedto rate the approximate gross family income on asix-point Likert scale ranging from �10,000 to �60,000a year.Family Socio-occupational Class. Families were clas-sified according to the occupation of the main earner
(Office for National Statistics, 2000).453www.jaacap.org

pa(af
.ig4mrep
dlmnu10du10rsPsdsm3Sp
LEWIS et al.
Statistical AnalysesThe sample was divided into two groups: geneticallyunrelated mother–child pairs (egg and embryo dona-tion) and genetically related mother–child pairs (ho-mologous IVF and sperm donation). Association be-tween maternal depression symptoms and childdepression/anxiety symptoms was calculated sepa-rately in each group. The principle of the IVF design isconsistent with the classic behavioral genetic adoptiondesign: The presence of an association in unrelatedmother–child pairs would provide evidence of envi-ronmental transmission because inherited links areremoved, therefore indicating the role of a sharedenvironment (C). If an association is seen only inrelated mother–child pairs, then this indicates inher-ited transmission suggesting that parent–child linksare due to genetic factors (G). When an association isseen in both groups but is stronger in the relatedgroup, this indicates genetic and environmental links(G � C). Associations were calculated using the Pear-son product-moment correlation coefficient (r) since vari-ables were continuous and normally distributed aftertransformation. The difference in the magnitude of cor-relation coefficients across groups was tested using theFisher R to Z transformation. This test converts Pearson rto the normally distributed variable Z, enabling a com-parison of the strength of associations. Associations werethen retested in each group controlling for differences inmaternal age, child age, and family structure (two-parentor single-parent family).
To test whether associations differed according tochild age, analyses were conducted separately at T1(mean child age � 6.3 years) and T2 (mean child age �9.9 years). The sample was then split at T2 intochildren (�11 years old) and adolescents (�11 yearsold). All analyses were conducted using mother andfather ratings of child symptoms to control for sharedrater effects; however, father ratings were availableonly at T1 because of low paternal response at T2.Associations between maternal depression symptomsand child depression/anxiety symptoms (mother andfather rated) were then tested adjusting for threemeasurements of shared adversity: independentstressful life events, family income, and family socialoccupational class. The role of shared adversity wasexamined at T1 because of the larger available sample.
The role of child gender was tested next. Mother–child associations were examined separately for boysand girls at both time points (using mother and fatherratings at T1 and mother ratings only at T2) to testwhether the effects of gender varied by child age.
The role of paternal depression symptoms was nextexamined. First, associations between maternal de-pression symptoms and child depression/anxietywere tested controlling for paternal depressionsymptoms to rule out the possibility that fatherpsychopathology could have been driving mother–
child associations. Second, the association betweenJOURN
454 www.jaacap.org
aternal depression symptoms and child depression/nxiety was tested separately in genetically relatedhomologous IVF, egg donation) and unrelated (spermnd embryo donation) father–child pairs controllingor shared adversity.
RESULTSDemographic Characteristicsand Parent and Child SymptomsChildren were significantly younger in themother unrelated group (egg and embryo dona-tion; mean age T1 unrelated group � 6.00 years;mean age T1 related group � 6.35 years, t850 �3.5, p � .001). A larger percentage of childrenlived with their mothers only in the unrelated(10%) versus related (5%) group and this differ-ence was statistically significant (�2
1 � 5.1, p �05). Mothers in the unrelated group were signif-cantly older; mean maternal age in the unrelatedroup was 44.91 years and in the related group,0.31 years (t849 � 12.79, p � .001). There wereore multiple births in the unrelated versus the
elated group (24% versus 21%) but this differ-nce was not statistically significant (�2
1 � 0.76,� .05).Mean maternal depression symptoms did not
iffer according to relatedness at T1 (mean unre-ated � 4.63, SD � 3.06, range � 0–15, n � 208;
ean related � 4.24, SD � 3.06, range � 0–18,� 642; t848 � 1.59, p � .11) or T2 (mean
nrelated � 4.58, SD � 3.49, range � 0–18, n �06; mean related � 4.04, SD � 3.19, range �–21, n � 353; t457 � 1.48, p � .14). Mean paternalepression symptoms did not differ at T1 (meannrelated � 3.86, SD � 2.70, range � 0–14, n �67; mean related � 3.87, SD � 3.12, range �–21, n � 410; t575 � 0.4, p � .97). Motherseported significantly higher mean depressionymptoms than fathers (t576 � 5.64, p � .01).arent depression symptoms were positivelykewed so were square root transformed. Childepression/anxiety symptoms also showed noignificant differences across groups according toother ratings (mean unrelated � 4.04, SD �
.54, range � 0–19, n � 208; mean related � 4.78,D � 4.44. range � 0–19, n � 641; t847 � 2.18,� .06, at T1; mean unrelated � 5.18, SD � 4.21,
range � 0–21, n � 105; mean related � 4.91,SD � 4.82, range � 0–30, n � 352; t455 � 0.522,p � .60, at T2) and father ratings (mean unrelated �3.66, SD � 3.79, range � 0–20, n � 133; meanrelated � 4.32, SD � 4.37, range � 0–32, n � 437;
t568 � 1.58, p � .12). Fifteen percent of mothersAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011

auaCccsaraWpra
ENVIRONMENTAL TRANSMISSION OF DEPRESSION SYMPTOMS
and 9% of fathers scored above the clinical cut-point on the Hospital Anxiety and DepressionScale at T1 and 14% of mothers at T2. Fivepercent of children scored above the clinicalcutpoint on the SMFQ at T1 according to motherand father ratings and 7% at T2 according tomother ratings.Testing for Inherited and Environmental Links Be-tween Maternal Depression Symptoms and ChildDepression/Anxiety. The association between ma-ternal depression symptoms and child depression/anxiety was significant in both groups for mother-rated (unrelated: n � 207, r � 0.32, p � .001; related:n � 639, r � 0.31, p � .001) and father-rated(unrelated: n � 132, r � 0.26, p � .01; related: n �436, r � 0.22, p � .001) child symptoms at T1.Correlation coefficients did not differ across relatedand unrelated groups according to Fisher R to Z formother ratings (Z � 0.28, p � .39) or father ratings(Z � 0.31, p � .38) of child symptoms. Correlationcoefficients did not differ across raters in unrelated(Z � 0.66, p � .25) and related (Z � 1.56, p � .06)groups. To control for known group differences,maternal age, child age, and family structure werethen entered as covariates at T1. Associations re-mained significant for mother (unrelated: n � 207,r � 0.33, p � .001; related: n � 638, r � 0.31, p �.001) and father (unrelated: n � 132, r � 0.26, p �.01; related: n � 436, r � 0.22, p � .001) ratings ofchild symptoms. The pattern of results was thesame when child depression and anxiety symp-toms were examined separately (Table S1, available
TABLE 1 Testing Environmental Transmission Controlling
Geneticall
Partial CorrelatioCoefficient
Independent negative life eventsMother-rated child symptoms 0.30***Father-rated child symptoms 0.23***
Family incomeMother-rated child symptoms 0.29***Father-rated child symptoms 0.21***
Family socio-occupational classMother-rated child symptoms 0.31***Father-rated child symptoms 0.23***
Multiple partial correlationMother-rated child symptoms 0.30***Father-rated child symptoms 0.22***
Note: **p � .01, ***p � .001.
online). F
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011
Testing Contribution of Shared Adversity. The asso-ciation at T1 was examined controlling for nega-tive life events likely to affect mother and child,family income, and family social occupationalclass (Table 1). Associations remained significantand unattenuated after controlling for each ad-versity separately across groups for mother- andfather-rated child symptoms. When all threevariables were entered into a multiple partialcorrelation analysis with maternal depressionsymptoms, associations for mother- and father-rated child symptoms remained significant in thetwo groups.Age Effects. The analyses at T2 when childrenwere 7 to 13 years old showed the same patternof effects as T1 (Table 2). Correlation coefficientsdid not differ according to Fisher R to Z (Z �1.04, p � .15). Maternal depression symptomslso predicted child depression/anxiety in thenrelated and related groups in children youngernd older than 11 years.hild Gender. Associations tested separately forhild gender are presented in Table 3. A signifi-ant association between maternal depressionymptoms and mother-rated child depression/nxiety was found for girls in unrelated andelated groups at T1. Correlations did not differccording to Fisher R to Z (Z � 0.31, p � .38).hen father-rated data were used, the same
attern was evidenced for girls in unrelated andelated groups and correlations did not differccording to Fisher R to Z (Z � 0.1.21, p � .11).
Shared Adversity
ated Genetically Unrelated
nPartial Correlation
Coefficient n
637 0.30*** 206434 0.26** 131
614 0.33*** 202431 0.23** 131
622 0.31*** 197431 0.25** 131
596 0.30*** 191416 0.22** 129
for
y Rel
n
or girls at T2 the association remained signifi-
455www.jaacap.org
LEWIS et al.
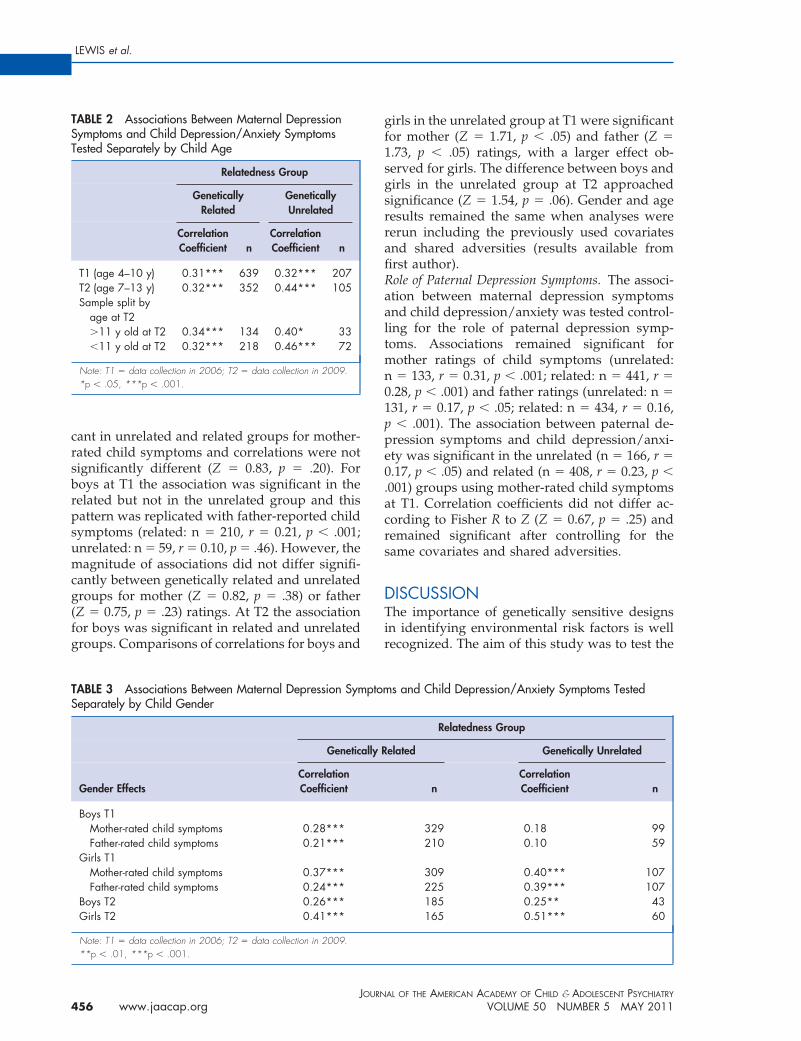
cant in unrelated and related groups for mother-rated child symptoms and correlations were notsignificantly different (Z � 0.83, p � .20). Forboys at T1 the association was significant in therelated but not in the unrelated group and thispattern was replicated with father-reported childsymptoms (related: n � 210, r � 0.21, p � .001;unrelated: n � 59, r � 0.10, p � .46). However, themagnitude of associations did not differ signifi-cantly between genetically related and unrelatedgroups for mother (Z � 0.82, p � .38) or father(Z � 0.75, p � .23) ratings. At T2 the associationfor boys was significant in related and unrelatedgroups. Comparisons of correlations for boys and
TABLE 2 Associations Between Maternal DepressionSymptoms and Child Depression/Anxiety SymptomsTested Separately by Child Age
Relatedness Group
GeneticallyRelated
GeneticallyUnrelated
CorrelationCoefficient n
CorrelationCoefficient n
T1 (age 4–10 y) 0.31*** 639 0.32*** 207T2 (age 7–13 y) 0.32*** 352 0.44*** 105Sample split by
age at T2�11 y old at T2 0.34*** 134 0.40* 33�11 y old at T2 0.32*** 218 0.46*** 72
Note: T1 � data collection in 2006; T2 � data collection in 2009.*p � .05, ***p � .001.
TABLE 3 Associations Between Maternal Depression SymSeparately by Child Gender
Genetic
Gender EffectsCorrelationCoefficient
Boys T1Mother-rated child symptoms 0.28***Father-rated child symptoms 0.21***
Girls T1Mother-rated child symptoms 0.37***Father-rated child symptoms 0.24***
Boys T2 0.26***Girls T2 0.41***
Note: T1 � data collection in 2006; T2 � data collection in 2009.
**p � .01, ***p � .001.JOURN
456 www.jaacap.org
girls in the unrelated group at T1 were significantfor mother (Z � 1.71, p � .05) and father (Z �1.73, p � .05) ratings, with a larger effect ob-served for girls. The difference between boys andgirls in the unrelated group at T2 approachedsignificance (Z � 1.54, p � .06). Gender and ageresults remained the same when analyses werererun including the previously used covariatesand shared adversities (results available fromfirst author).Role of Paternal Depression Symptoms. The associ-ation between maternal depression symptomsand child depression/anxiety was tested control-ling for the role of paternal depression symp-toms. Associations remained significant formother ratings of child symptoms (unrelated:n � 133, r � 0.31, p � .001; related: n � 441, r �0.28, p � .001) and father ratings (unrelated: n �131, r � 0.17, p � .05; related: n � 434, r � 0.16,p � .001). The association between paternal de-pression symptoms and child depression/anxi-ety was significant in the unrelated (n � 166, r �0.17, p � .05) and related (n � 408, r � 0.23, p �.001) groups using mother-rated child symptomsat T1. Correlation coefficients did not differ ac-cording to Fisher R to Z (Z � 0.67, p � .25) andremained significant after controlling for thesame covariates and shared adversities.
DISCUSSIONThe importance of genetically sensitive designsin identifying environmental risk factors is wellrecognized. The aim of this study was to test the
s and Child Depression/Anxiety Symptoms Tested
Relatedness Group
elated Genetically Unrelated
nCorrelationCoefficient n
329 0.18 99210 0.10 59
309 0.40*** 107225 0.39*** 107185 0.25** 43165 0.51*** 60
ptom
ally R
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011

wtepm
dimdtfasf
ENVIRONMENTAL TRANSMISSION OF DEPRESSION SYMPTOMS
extent to which environmental links betweenmaternal depression symptoms and child symp-toms demonstrated in previous reports wereexplained by measurements of shared adversityand by child age and gender.
Results are consistent with an environmentallink between maternal depression symptoms andchild depression/anxiety. Associations were ob-served regardless of whether mothers and chil-dren were genetically related. There are nowconverging findings across different geneticallysensitive designs of environmental links betweenmaternal and offspring depression.2,3,12 The pres-ent findings therefore consolidate evidence thatintergenerational transmission of depressionsymptoms is due at least in part to environmentalmechanisms and does not arise entirely fromshared genetic liability. The presence of an asso-ciation in the unrelated group also rules outpassive gene-environment correlation, which isabsent in genetically unrelated mother–childpairs. The present study accounted for threemeasurements of shared adversity: negative lifeevents, family income and family socioeconomicstatus, and depression in fathers. Adjusted asso-ciations remained significant in genetically unre-lated and related parent–child pairs. This favorsthe suggestion that noninherited links betweenmother and child depression may arise fromdirect environmental effects and are not attribut-able to the extraneous variables measured in thisstudy. This is consistent with findings thatshared stressful life events and social supportnetworks do not contribute to links betweenmaternal and child depression.4 Although thecovariates, family income, family social occu-pational class, and life events, may be geneti-cally influenced and meaningful genetic vari-ance may therefore be unsystematicallyremoved, the pattern of genetic and environ-mental transmission was the same whether thecovariates were included.
Child age is an important factor to considerbecause depression etiology has been found todiffer developmentally, with greater genetic in-fluences in adolescence.18 Significant environ-mental links were found when children were 4 to10 and 7 to 13 years old. At T2 significantenvironmental transmission effects were foundin younger children (7 to 11 years) and those inearly adolescence (11 to 13 years). Significantenvironmental transmission effects were found
in both age groups, suggesting that associationsJOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011
ere not due to the young age of the sample andhat environmental links also operate in childrenntering early adolescence. This concurs withrevious genetically sensitive studies on trans-ission effects that looked at older samples.2,3
Tully et al.2 found some indication for the roleof genetic factors. Although genetic influencescannot be ruled out in the present study, no clearsupport was found for a genetic contributionto transmission apart from in boys (see later);maternal–child associations were not stronger inthe genetically related group. Interestingly, thestudy by Silberg et al.3 also reported no signifi-cant genetic influence. However, in contrast tothe study by Tully et al.,2 our findings and thoseof Silberg et al.3 relied on symptoms rather than
iagnoses of depression so it is possible thatnherited transmission is more pronounced for
ore severe maternal depression symptoms. In-eed, a study of adolescent female twins found
hat the contribution of shared environmentalactors differed according to the phenotype ex-mined, with shared environmental effects ob-erved for a broad depressive phenotype but notor major depressive disorder.19 Alternatively, it
may be that the heritable phenotype manifests ina different way, for example, as overall levels ofpsychopathology in children rather than as de-pression symptoms per se. In contrast to theseprevious studies, the present study examined acomposite of depression/anxiety scores. How-ever, the pattern of maternal–child associationswas found to be the same for child depressionscores alone. Another consideration is that noneof the designs (adoption, children of twins, IVF)are able to account for genetic heterogeneitybetween depression in childhood and depressionin adulthood. If different genes are responsiblefor depression in childhood versus adulthood,11
then this may have the effect of decreasing thegenetic transmission estimate. This is an impor-tant direction for future research.
Based on a range of studies suggesting thatmaternal depression may have stronger adverseeffects for girls, the present study examinedwhether patterns of intergenerational transmis-sion differed by gender. The significant associa-tion in genetically unrelated mother–daughterpairs indicated an environmental effect. Formother–son pairs, the association was significantonly in the genetically related group, suggestingthat environmental transmission was less strong
for boys. These findings are in agreement with457www.jaacap.org

siTmppdc
dtdtttomeegsdaia
LEWIS et al.
numerous nongenetic studies that have reportedstronger associations between maternal depres-sion and child depression in girls7,8 and suggestthat for girls this effect may occur through envi-ronmental pathways because the association wasof a similar magnitude in the genetically unre-lated and related groups. This concurs with re-search suggesting that girls are more sensitive tostressful life events in general, especially those ofan interpersonal nature. The significant associa-tion between maternal depression symptoms andchild depression/anxiety in related but not inunrelated groups for boys does not conclusivelyrule out environmental transmission for boysbecause the difference in the magnitude of corre-lations was not large. Indeed, environmentaltransmission was seen for boys in analyses con-ducted at T2. Prior nongenetic studies of theassociation between maternal and child depres-sion have reported stronger associations for girlsonly at puberty, which coincides with the emer-gence of the gender difference in depressionprevalence.8 However the present study suggeststhat from a younger age, girls may already pos-sess an increased vulnerability to maternal de-pression exposure. A recent study attests to thisview.20
The results of this study must be interpreted inlight of certain limitations. Other unmeasuredshared adversities may have contributed to theintergenerational link. The association betweenmaternal depression symptoms and child moodcannot be assumed to be unidirectional. A lack ofpower in the longitudinal analyses when thesample is split by conception group and genderprecluded an investigation of reverse causation.Despite evidence that the association is likely tobe bidirectional, research suggests that it is un-likely to be accounted for by child effects onparent symptoms alone. A recent prospectivelongitudinal study of parental depressive symp-toms and child temperament found significantparent-to-child effects but little support for child-to-parent effects.21 Like other longitudinal stud-ies, attrition affected sample retention especiallyfor father participation. There was no evidencethat this biased the results (those who droppedout of the study did not differ from those whowere retained in maternal and child depressionsymptom scores), but it did limit the scope andpower available for some T2 analyses. Significantenvironmental transmission but a lack of differ-
ences between the related and unrelated groupsJOURN
458 www.jaacap.org
suggesting no genetic transmission could also beaccounted for by the use of self-report question-naire measurements, which are subject to greatererror than interview measurements. The presentstudy focused on symptom ratings and furtherstudies focusing on clinical diagnoses of parentdepression and on clinical outcomes in childrenwould be of value. However, focus on symptomsis still useful to an understanding of clinicaldiagnoses because symptoms and disordershow similar correlates (e.g., increased rates inpostpubertal girls) and similar patterns of as-sociation with risk factors (e.g., life events,family adversity).
Another issue is the use of an age-based cutoff toapproximate the effects of pre- and postpubertybecause this is not an exact measurement of puber-tal development. However, pubertal data were notcollected so this was the best available approxima-tion. IVF may result in epigenetic modificationsthat lead to offspring born with imprinting disor-ders.22 In practice, however, this sample has beenhown to be comparable to the normal populationn terms of emotional and behavioral adjustment.his does not rule out the possibility that epigeneticodifications have occurred, although this would
resumably have the effect of introducing greaterhenotypic differences between parents and chil-ren in this sample compared with naturally con-eived offspring and parents.
The findings have clinical implications for theesign of preventive interventions: concluding
hat a putative causal risk factor such as parentalepression symptom exposure confers its effect
hrough an environmental mechanism suggestshat this factor can be targeted to prevent andreat child and adolescent depression. In supportf this, evidence suggests that changes in currentaternal depression status have corresponding
ffects on child outcome.23 The environmentalffect of maternal depression appears to be stron-er in girls than in boys, suggesting that depres-ion in mothers carries a particular risk effect foraughters, implying that interventions targetedt treating parental depression may have a largermpact on girls as supported by a recent meta-nalysis of preventive interventions.24 In addi-
tion, parent depression was found to have anenvironmental link with anxiety/depressionsymptoms from childhood through to early ado-lescence. Little support was found for the role ofgenetic factors on the transmission of depression
symptoms apart from for boys, and this concursAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011

ENVIRONMENTAL TRANSMISSION OF DEPRESSION SYMPTOMS
with a prior genetically sensitive study using achildren-of-twins model.3 This does not negatethe role of child- and adult-specific genetic fac-tors in the etiology of depression symptoms,which is a well-established and consistent find-ing. It is likely that the etiology and transmissionof depression are caused by a complex interplaybetween genetic and environmental factors.
Accepted January 19, 2011.
Ms. Lewis and Drs. Collishaw and Thapar are with the Child andAdolescent Psychiatry Section and the Medical Research CouncilCentre for Neuropsychiatric Genetics and Genomics, Cardiff Univer-sity. Dr. Rice is with the Division of Psychology and LanguageSciences, University College London. Dr. Harold is with the College of
Biological Sciences, University of Leicester.[published online ahead of print September 22, 2010]. PsycholMed. doi: 10.1017/S0033291710001753.
JOURNAL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011
This study was supported by a Wellcome Trust showcase award and aWellcome Trust Project grant.
We thank the families who participated in this study and our fertilitycenter collaborators. We thank Professors Dale Hay and Jacky Boivinof Cardiff University for assistance in the study design and AllysonLewis and Val Russell, also of Cardiff University, for antenatal datacollection and administrative support.
Disclosure: Ms. Lewis has received funding from the Economic andSocial Research Council and the Nuffield Foundation. Drs. Rice,Harold, Collishaw, and Thapar report no biomedical financial inter-ests or potential conflicts of interest.
Correspondence to Gemma Lewis, B.Sc., MRC Centre forNeuropsychiatric Genetics and Genomics, Department ofPsychological Medicine and Neurology, Cardiff University, HeathPark, Cardiff, CF14 4 XN, UK; e-mail: [email protected]
0890-8567/$36.00/©2011 American Academy of Child andAdolescent Psychiatry
DOI: 10.1016/j.jaac.2011.01.015
REFERENCES1. Weissman M, Wickramaratne P, Nomura Y, Warner V, Pilowsky
D, Verdeli H. Offspring of depressed parents: 20 years later. AmJ Psychiatry. 2006;163(6):1001-1008.
2. Tully EC, Iacono WG, McGue M. An adoption study of parentaldepression as an environmental liability for adolescent depres-sion and childhood disruptive disorders. Am J Psychiatry. 2008;165(9):1148-1154.
3. Silberg J, Maes H, Eaves L. Genetic and environmental influenceson the transmission of parental depression to children’s depres-sion and conduct disturbance: an extended Children of Twinsstudy. J Child Psychol Psychiatry. 2010;51:734-744.
4. Rice F, Harold GT, Thapar A. The link between depression inmothers and offspring: An extended twin analysis. Behav Genet.2005;35(5):565-577.
5. Eley T, Deater-Deckard K, Fombonne E, Fulker DW, Plomin R.An adoption study of depressive symptoms in middle childhood.J Child Psychol Psychiatry. 1998;39(3):337-345.
6. Silberg J, Pickles A, Rutter M, et al. The influence of genetic factorsand life stress on depression among adolescent girls. Arch GenPsychiatry. 1999;56:225-232.
7. Fergusson DM, Horwood LJ, Lynskey MT. Maternal depressivesymptoms and depressive symptoms in adolescents. J ChildPsychol Psychiatry. 1995;36(7):1161-1178.
8. Cortes RC, Fleming CB, Catalano RF, Brown EC. Gender differ-ences in the association between maternal depressed mood andchild depressive phenomena from grade 3 through grade 10. JYouth Adolesc. 2006;35:815-826.
9. Bureau JF, Easterbrooks MA, Lyons-Ruth K. Maternal depressivesymptoms in infancy: Unique contributions to children’s depres-sive symptoms in childhood and adolescence. Dev Psychopathol.2009;21:519-537.
10. Thapar A, McGuffin P. A twin study of depressive symptoms inchildhood. Br J Psychiatry. 1994;165:259-265.
11. Kendler KS, Gardner CO, Lichtenstein P. A developmental twinstudy of symptoms of anxiety and depression: evidence forgenetic innovation and attenuation. Psychol Med. 2008;38:1567-1575.
12. Harold GT, Rice F, Hay DF, Boivin J, Van den Bree M, Thapar A.Familial transmission of depression and antisocial behavioursymptoms: disentangling the contribution of inherited and envi-ronmental factors and testing the mediating role of parenting
13. Shelton KH, Boivin J, Hay D, et al. Examining differences inpsychological adjustment problems among children conceived byassisted reproductive technologies. Int J Behav Dev. 2009;33(5):385-392.
14. Zigmond AS, Snaith RP. The hospital anxiety and depressionscale. Acta Psychiatr Scand. 1983;67(6):361-370.
15. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of theHospital Anxiety and Depression Scale. An updated literaturereview. J Psychosom Res. 2002;52(2):69-77.
16. Thapar A, McGuffin P. Validity of the shortened Mood andFeelings Questionnaire in a community sample of children andadolescents: a preliminary research note. Psychiatry Res. 1998;81(2):259-268.
17. Johnson JH, McCutcheon S. Assessing life stress in older childrenand adolescents: preliminary findings with the life events check-list. In: Sarason IE, Spielberger CD, eds. Stress and Anxiety. NewYork: Hemisphere; 1980:111-125.
18. Rice F, Harold G, Thapar A. Assessing the effects of age, sex andshared environment on the genetic aetiology of depression inchildhood and adolescence. J Child Psychol Psychiatry. 2002;43(8):1039-1051.
19. Glowinski AL, Madden PA, Bucholz KK, Lynskey MT, Heath AC.Genetic epidemiology of self-reported lifetime DSM-IV majordepressive disorder in a population-based twin sample of femaleadolescents J Child Psychol Psychiatry. 2003;44:988-996.
20. Silk JS, Shaw DS, Skuban EM, Oland AA, Kovacs M. Emotionregulation strategies in offspring of childhood-onset depressedmothers. J Child Psychol Psychiatry. 2006;47(1):69-78.
21. Hanington L, Ramchandani P, Stein A. Parental depression andchild temperament: assessing child to parent effects in a longitu-dinal population study. Infant Behav Dev. 2010;33:88-95.
22. DeBaun MR, Niemitz EL, Feinberg AP. Association of in vitrofertilization with Beckwith-Wiedemann syndrome and epigeneticalterations of LIT1 and H19. Am J Hum Genet. 2003;72(1):156-160.
23. Weissman M, Pilowsky D, Wickramaratne P, et al. Remissions inmaternal depression and child psychopathology. JAMA. 2006;295(12):1389-1398.
24. Stice E, Shaw H, Bohon C, Marti CN, Rohde P. A meta-analyticreview of depression prevention programs for children andadolescents: factors that predict magnitude of intervention effects.
J Consult Clin Psychol. 2009;77(3):486-503.459www.jaacap.org

Note: T1 � data collection in 2006; T2 � data collection in 2009.
LEWIS et al.
JOURN
459.e1 www.jaacap.org
TABLE S1 Correlations Presented Separately for ChildDepression and Anxiety Symptoms
GeneticallyRelated
GeneticallyUnrelated
CorrelationCoefficient n
CorrelationCoefficient n
Child depressionsymptoms T1
Mother-rated childsymptoms
0.25 639 0.29 207
Father-rated childsymptoms
0.18 439 0.32 133
Child anxietysymptoms T1
Mother-rated childsymptoms
0.31 638 0.31 207
Father-rated childsymptoms
0.23 439 0.16 133
Child depressionsymptoms T2
0.29 340 0.40 99
Child anxietysymptoms T2
0.27 347 0.40 100
AL OF THE AMERICAN ACADEMY OF CHILD & ADOLESCENT PSYCHIATRY
VOLUME 50 NUMBER 5 MAY 2011