Depression Symptoms and Treatment Among HIV Infected and Uninfected Veterans
Upload
independentCategory
view
4download
0
Invasive bacterial and fungal infections among hospitalized HIV-infected and HIV-uninfected children and infants in northernTanzania
John A. Crump1,2,3,4, Habib O. Ramadhani3,4, Anne B. Morrissey1, Levina J. Msuya3,4, Lan-Yan Yang5,6, Shein-Chung Chow6, Susan C. Morpeth1, Hugh Reyburn7, Boniface N. Njau3,Andrea V. Shaw1, Helmut C. Diefenthal3,4, John A. Bartlett1,2,3,4, John F. Shao3,4, WernerSchimana3, Coleen K. Cunningham8, and Grace D. Kinabo3,4
1Division of Infectious Diseases and International Health, Department of Medicine, andDepartment of Pathology, Duke University Medical Center, Durham, NC, USA2Duke Global Health Institute, Duke University, Durham, NC, USA3Kilimanjaro Christian Medical Centre, Moshi, Tanzania4Kilimanjaro Christian Medical College, Tumaini University, Moshi, Tanzania5Department of Biostatistics and Bioinformatics, Duke University School of Medicine, Durham,NC, USA6National Cheng Kung University, Tainan, Taiwan7London School of Hygiene and Tropical Medicine, UK8Division of Pediatric Infectious Diseases, Department of Pediatrics, Duke University MedicalCenter, Durham, NC, USA
SummaryOBJECTIVE—To describe the contribution of paediatric HIV and of HIV co-infections toadmissions to a hospital in Moshi, Tanzania, using contemporary laboratory methods.
METHODS—During 1 year, we enrolled consecutively admitted patients aged ≥2 months and<13 years with current or recent fever. All patients underwent standardized clinical history taking,a physical examination and HIV antibody testing; standard aerobic blood cultures and malaria filmwere also done, and hospital outcome was recorded. Early infant HIV diagnosis by HIV-1 RNAPCR was performed on those aged <18 months. HIV-infected patients also received serumcryptococcal antigen testing and had their CD4-positive T-lymphocyte count and percentdetermined.
RESULTS—A total of 467 patients were enrolled whose median age was 2 years (range 2months–13 years); Of those patients, 57.2% were female and 12.2% were HIV-infected.Admission clinical diagnosis of HIV disease was made in 10.7% and of malaria in 60.4%. Ofblood cultures, 5.8% grew pathogens; of these 25.9% were Salmonella enterica (including 6
© 2011 Blackwell Publishing Ltd
Corresponding Author: John A. Crump, Division of Infectious Diseases and International Health, Department of Medicine, DukeUniversity Medical Center, Box 102359, Durham, NC 27710, USA. Tel.: +1 919 684 2660; Fax: +1 919 684 8902;[email protected].
This paper was presented in part at the 58th American Society of Tropical Medicine and Hygiene annual meeting, Washington, DC,18–22 November 2009, abstract 472. Its content is solely the responsibility of the authors and does not necessarily represent theofficial views of the NIH, which largely funded the work.
NIH Public AccessAuthor ManuscriptTrop Med Int Health. Author manuscript; available in PMC 2012 July 24.
Published in final edited form as:Trop Med Int Health. 2011 July ; 16(7): 830–837. doi:10.1111/j.1365-3156.2011.02774.x.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
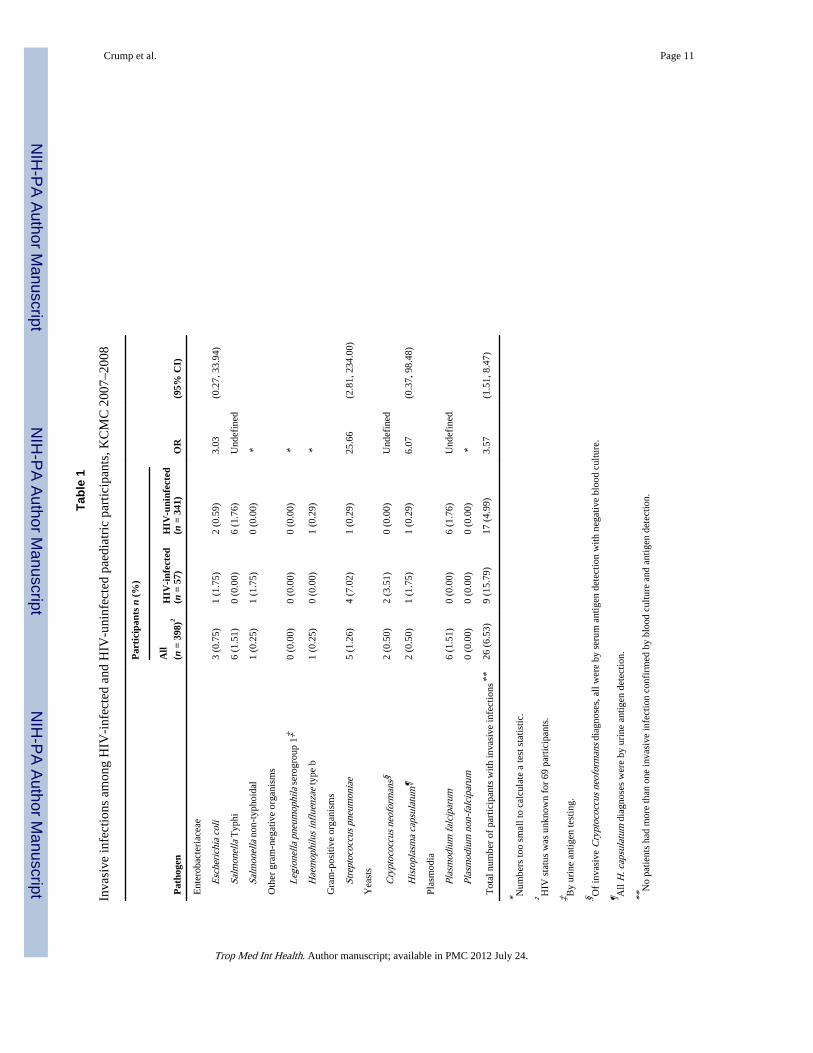
Salmonella Typhi) and 22.2% Streptococcus pneumoniae. Plasmodium falciparum was identifiedon blood film of 1.3%. HIV infection was associated with S. pneumoniae (odds ratio 25.7, 95% CI2.8, 234.0) bloodstream infection (BSI), but there was no evidence of an association withEscherichia coli or P. falciparum; Salmonella Typhi BSI occurred only among HIV-uninfectedparticipants. The sensitivity and specificity of an admission clinical diagnosis of malaria were100% and 40.3%; and for an admission diagnosis of bloodstream infection, they were 9.1% and86.4%, respectively.
CONCLUSION—Streptococcus pneumoniae is a leading cause of bloodstream infection amongpaediatric admissions in Tanzania and is closely associated with HIV infection. Malaria was over-diagnosed clinically, whereas invasive bacterial disease was underestimated. HIV and HIV co-infections contribute to a substantial proportion of paediatric febrile admissions, underscoring thevalue of routine HIV testing.
KeywordsAfrica; bacteremia; HIV; paediatrics; Salmonella enterica; Streptococcus pneumoniae
IntroductionFever is a common presenting feature among children and infants admitted to hospital insub-Saharan Africa (Petit & van Ginneken 1995). Malaria, bacteremia, or other infectiousconditions presenting as a febrile illness account for a large proportion of deaths in sub-Saharan Africa (Bryce et al. 2005), yet the laboratory capacity to make aetiologic diagnosisis often lacking (Archibald & Reller 2001; Petti et al. 2006). Consequently, clinicians oftenrely on syndromic approaches to patient management (WHO 2000, 2005) and whileapplication of such algorithms improves patient care, a proportion of patients inevitably donot receive specific therapy for potentially life threatening infections (Reyburn et al. 2004).Although malaria is often considered to be the leading life threatening cause of febrileillness in sub-Saharan Africa, malaria transmission intensity varies considerably by location(Hay et al. 2009). Furthermore, recent efforts to expand coverage with insecticide-treatedbed nets and switch to more effective malaria treatment regimens have been associated withsubstantial declines in malaria parasite rates in the community and in the proportion ofoutpatient visits and hospital admissions because of malaria in a number of countries (WHO2009; O’Meara et al. 2010).
While routine use of blood cultures is uncommon in sub-Saharan Africa, expanded use ofblood culture at a few sentinel sites has highlighted the importance of invasive bacterialdisease as a cause of illness and death among children both within and outside the hospital(Campbell et al. 2004; Berkley et al. 2005; Brent et al. 2006; Gordon et al. 2008; Sigauqueet al. 2009; Nadjm et al. 2010; Reddy et al. 2010). Patients with invasive bacterial diseasefrequently are treated empirically with antimalarial drugs without antibacterial therapy,resulting in adverse outcomes (Reyburn et al. 2004). To investigate the aetiology,management and outcomes of febrile illness in an area of low malaria transmission intensity(Hay et al. 2009), we studied paediatric inpatients at a consultant referral hospital innorthern Tanzania. The results of a similar study among adults and adolescents are describedelsewhere (Crump et al. 2011).
Methods and materialsSetting
Moshi (population >144 000) is the administrative centre of Kilimanjaro Region (population>1.4 million) in northern Tanzania, situated at 890 m above sea level. The climate is
Crump et al. Page 2
Trop Med Int Health. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
characterized by a long rainy period (March–May) and a short rainy period (October–December; National Bureau of Statistics & ORC Macro 2005). Kilimanjaro ChristianMedical Centre (KCMC), a consultant referral hospital with 458 inpatient beds servingseveral regions in northern Tanzania, is an important provider of hospital care to residents ofMoshi. In 2008, KCMC admitted 22 099 patients. Neither Haemophilus influenzae type Bnor pneumococcal conjugate vaccine was available through the Tanzania expandedprogramme on immunizations during the study period. The HIV seropre-valence inTanzania from population-based surveys of adults in 2003–2004 was 7.0% (Mishra et al.2006).
ParticipantsParticipants were prospectively identified from among paediatric inpatients at KCMC inMoshi, Tanzania, from 17 September 2007 through 25 August 2008. Admitted patients agedfrom ≥2 months to <13 years, with a history of fever in the past 48 h or an axillarytemperature ≥37.5 °C or a rectal temperature of ≥38.0 °C, were eligible to participate in thestudy. Patients admitted with known malignancy, renal failure, hepatic failure, bone marrowaplasia, trauma or surgery were excluded. A standardized clinical history and a physicalexamination were performed by a trained clinical officer who was a member of the studyteam. Provisional admission diagnoses of the usual hospital clinical team were recorded andcoded using the International Statistical Classification of Diseases and Related HealthProblems 10th Revision (ICD-10) codes. After cleansing of the skin with isopropyl alcoholand povidone iodine, blood was drawn for a single aerobic blood culture (4 ml) as well asfor complete blood count, examination for blood parasites and HIV antibody testing. Thecase definition for attribution of febrile illness to malaria for children aged <5 years was≥1000 asexual parasites/µl and ≥500 parasites/µl for children aged ≥5 years (Chandler et al.2006). Acute serum, plasma and whole blood were archived on all participants. For patientsfound to be HIV seropositive, CD4-positive T-lymphocyte count and per cent and serumcryptococcal antigen were also measured. Early infant diagnosis for those aged <18 monthswas performed by HIV-1 RNA PCR. Urine was collected as soon as possible afteradmission for detection of urine antimicrobial activity and for antigen detection ofHistoplasma capsulatum and Legionella pneumophila serogroup 1. When requested by thehospital clinical team, a chest radiograph was ordered and reported using a standardizedform by a radiologist (HCD). A discharge form was completed at the time of discharge fromhospital that captured in-hospital management, whether the patient died in hospital, and thedischarge diagnoses coded using ICD-10 codes. The results of all study investigations wereprovided immediately to the hospital clinical team to inform patient management.
Laboratory methodsComplete blood count and differential were performed using the CellDyn 3500 automatedhaematology analyzer (Abbott Laboratories. Abbott Park, IL, USA) and interpreted usinglocally established reference ranges (Buchanan et al. 2010). Thick and thin blood filmsstained with Giemsa were examined for blood parasites by oil immersion microscopy.Parasite density was determined by standard methods (Greenwood & Armstrong 1991).
Blood culture bottles were assessed for volume adequacy by comparing the weight beforeand after inoculation with blood. Adequate volume was defined as recommended volume of4 ml ± 20%. BacT/ALERT® paediatric fan (PF) bottles were loaded into the BacT/ALERT®
3D Microbial Detection System (BioMérieux Inc., Durham, NC, USA) where they wereincubated for 5 days. Standard methods were used for identifying bloodstream isolates. S.pneumoniae were serotyped by latex agglutination and the Quellung reaction using antiserafrom Statens Serum Institut, Denmark. Non-typhoidal Salmonella (NTS) were serotypedaccording to the Kauffmann–White scheme (Grimont & Weill 2007). Antimicrobial
Crump et al. Page 3
Trop Med Int Health. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
susceptibility testing was performed according to the methods of the Clinical LaboratoryStandards Institute (CLSI, Wayne, PA, USA), M100-S18, January 2008 (ClinicalLaboratories Standards Institute 2008).
HIV-1 antibody testing was performed on whole blood using both the Capillus™ HIV-1/HIV-2 (Trinity Biotech PLC, Bray, Ireland) and Determine™ HIV-1/2 (AbbottLaboratories) rapid HIV antibody tests. The Capillus test was replaced with the SD BiolineHIV-1/2 3.0 (Standard Diagnostics Inc., Kyonggi-do, Korea) on 4 March 2008 after achange in Tanzania Ministry of Health HIV testing guidelines. If rapid tests were discordant,the sample was tested with an ELISA (Vironostika® Uni-Form II plus O Ab; BioMérieux).If the ELISA was negative, no further testing was performed. If the ELISA was positive, aWestern blot (Genetic Systems HIV-1 Western Blot kit; Bio-Rad, Hercules, CA, USA) wasperformed to confirm the result (Mayhood et al. 2008). HIV-1 RNA PCR was performedusing the Abbott m2000 system RealTime™ HIV-1 assay (Abbott Laboratories; Crump etal. 2009; Scott et al. 2011). The CD4-positive T-lymphocyte count or per cent was measuredusing the FACSCalibur™ system (Becton Dickinson, Franklin Lakes, NJ, USA).Cryptococcal antigen was measured using the Latex Cryptococcal Antigen DetectionSystem assay (Immuno-Mycologics, Norman, OK, USA), and cryptococcal antigen titre wasdetermined by twofold dilution until endpoint was achieved.
Urine was tested for Legionella pneumophila serogroup 1 antigen using the LegionellaUrinary Antigen Test (Binax Inc., Scarborough, ME, USA). Urine was tested forHistoplasma capsulatum antigen using the MVista™ Histoplasma capsulatum QuantitativeAntigen EIA (Miravista Diagnostics, Indianapolis, IN, USA; Connolly et al. 2007).Antimicrobial activity in urine was measured using a modification of the method describedby Liu et al. (1999) where Bacillus subtilis ATCC 6633 was substituted for Bacillusstearothermophilus ATCC 7953.
During the study, the laboratory participated successfully in relevant external qualityassurance programmes of the College of American Pathologists, the Viral Quality Assuranceprogramme of the AIDS Clinical Trials Group, and the United Kingdom National ExternalQuality Assessment Service.
Statistical analysisData were entered using the Cardiff Teleform system (Cardiff Inc., Vista, CA, USA) into anAccess database (Microsoft Corp). For continuous responses, analysis of variance was usedto assess treatment difference between groups. For categorical data and binary responses,Cochran-Mantel-Haenszel test was performed. Descriptive statistics were used forcomparisons of baseline demographics and patient characteristics. Weight for age z-scores(WAZ) were calculated using WHO (WHO) AnthroPlus software (WHO, Geneva,Switzerland) and WHO growth standards. The performance of clinical diagnosis atadmission, the WHO manual ‘Management of the child with severe infection or severemalnutrition: guidelines for care at first-referral level in developing countries’ (WHOmanual; WHO 2000) for septicaemia, typhoid fever, and suspicion of HIV (WHO 2000),and WHO Integrated Management of Childhood Illness (IMCI) guidelines for malaria wereassessed against laboratory findings. For the septicaemia analysis, the following signs wereused: fever with no obvious focus of infection; blood film for malaria is negative; no stiffneck or other specific signs of meningitis or a lumbar puncture for meningitis is negative;and signs of systemic upset (e.g., inability to drink or breastfeed, convulsions, lethargy orvomiting everything). For the typhoid fever analysis, the following signs were used: fever(particularly ≥7 days), plus any of the following: diarrhoea or constipation, vomiting,abdominal pain, headache or cough; fever with no obvious focus of infection; no stiff neckor other specific signs of meningitis, or a lumbar puncture for meningitis is negative; signs
Crump et al. Page 4
Trop Med Int Health. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
of systemic upset; and blood smear for malaria is negative. All statistical tests wereperformed at the 5% level of significance (two-sided) with SPSS 12.0 software (SPSS Inc,Chicago, IL, USA).
Research ethicsThis study was approved by the KCMC Research Ethics Committee, the Tanzania NationalInstitute for Medical Research National Research Ethics Coordinating Committee and anInstitutional Review Board of Duke University Medical Center.
ResultsOver the study period, 1154 patients admitted to the paediatric services of KCMC werescreened for eligibility. Of these, 644 (55.8%) met eligibility criteria. Ultimately, 467(72.5%) could be enrolled into the study. The median age (range) of study participants was 2years (2 months, 13 years) and 267 (57.2%) were female. The median (range) volume ofblood inoculated into PF bottles was 2.9 ml (0.15, 9.35 ml), and 139 (29.8%) were classifiedas adequately filled. Of enrolled patients, 27 (5.8%) had a clinically important organismisolated from blood culture and 16 (3.4%) had an organism classified as a contaminantisolated. Fifty-seven (12.2%) participants were HIV infected. Of HIV-infected patients, themedian (range) CD4-positive T-lymphocyte value was 11% (6–21%) for those aged <12months, 16% (3–34%) for those aged ≥12 months to <5 years and 205 cells/mm3 (2– 1631cells/mm3) for those aged ≥5 years of age. Of 425 participants aged ≤10 years, the median(range) WAZ was −0.93 (5.00–6.00); 106 (24.9%) had WAZ <−2 and 49 (11.5%) had WAZ<−3.
Relationship between HIV and invasive infectionsThe relationship between invasive disease and HIV infection is shown in Table 1. Of 26invasive infections diagnosed, Plasmodium falciparum, Salmonella Typhi and Streptococcuspneumoniae accounted for 6 (22.2%) each; 2 (7.4%) were because of Cryptococcusneoformans. Of three children aged <5 years with positive malaria films, 2 (66.7%) had≥1000 asexual parasites/µl. Of three children aged ≥5 years, none had ≥500 parasites/µl. Ofsix S. pneumoniae bloodstream isolates, one (16.7%) belonged to serotype 1; one (16.7%) toserotype 4; one (16.7%) to serotype 5; one (16.7%) to serotype 6B; and two (33.3%) toserotype 14. The non-typhoidal Salmonella bloodstream isolate was serotype Typhimurium.Of six S. pneumoniae isolates, six (100%) were susceptible to chloramphenicol; six (100%)were susceptible to erythromycin; four (66.7%) were susceptible to penicillin by meningitisbreakpoints and two showed intermediate susceptibility; one (16.7%) was susceptible totrimethoprim-sulfamethoxazole (SXT) and the remainder were resistant. Of sevenSalmonella enterica, two (28.6%) were susceptible to ampicillin and the remainder wereresistant; seven (100%) were susceptible to ceftriaxone and none produced extended-spectrum β-lactamases; three (42.9%) were susceptible to chloramphenicol and theremainder were resistant; two (28.6%) were susceptible to SXT and the remainder wereresistant; and seven (100%) were susceptible to ciprofloxacin and none showed decreasedciprofloxacin susceptibility (Crump et al. 2003).
Antimicrobial use prior to admissionA total of 220 (47.1%) patients reported taking antibacterial drugs during their illness priorto admission to hospital. Of these, 47 (21.4%) reported taking SXT, 53 (24.1%) reportedtaking amoxicillin and 120 (54.5%) reported taking another antibacterial drug. In addition,143 (30.6%) patients reported taking antimalarial drugs during their illness and prior toadmission to hospital. However, among those whose urine was tested, 154 (33.0%)demonstrated urine antimicrobial activity. Of 105 blood cultures drawn from patients with
Crump et al. Page 5
Trop Med Int Health. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
urine antimicrobial activity, 4 (3.8%) were positive whereas 12 (5.1%) of 236 blood culturesdrawn from patients without urine antimicrobial activity were positive (OR = 0.74; 95% CI,0.23–2.35; P = 0.610).
In-hospital case fatalityOf 464 (99.4%) patients whose hospital outcome was known, 34 (7.3%) died, 2 (0.4%) withinvasive infection and 32 (6.8%) without documented invasive infection (P = 0.840). One(0.2%) child with S. pneumoniae BSI died. However, there were no deaths among thosewith typhoid fever, cryptococcal disease, or malaria. Of HIV-infected participants, 5 (8.8%)died in hospital, against 18 (5.3%) of HIV-uninfected participants (P = 0.460).
Reliability of clinical diagnosesThe sensitivity, specificity, positive predictive value (PPV) and negative predictive value(NPV) of an admission clinical diagnosis of malaria for the presence of malaria parasites onblood smear was 100%, 40.3%, 3.9% and 100%. The sensitivity, specificity, PPV and NPVof an admission diagnosis of bloodstream infection were 9.1%, 86.4%, 3.2% and 95.0%,respectively. The sensitivity, specificity, PPV, and NPV of an admission diagnosis of HIVinfection was 66.7%, 98.8%, 90.0% and 94.6%, respectively.
Diagnostic performance of first-referral level guidelineThe sensitivity, specificity, PPV and NPV of the WHO manual for septicaemia (bloodculture positive for bacterial pathogen) were 94.1%, 2.5%, 4.4% and 90.0%, respectively,and were 60%, 44.4%, 11.4% and 1.2% for typhoid fever (blood culture positive forSalmonella Typhi). For suspicion of HIV infection, the sensitivity, specificity, PPV andNPV of the guidelines were 86.4%, 44.1% 20.9% and 95%, respectively. The sensitivity,specificity, PPV and NPV of the IMCI guidelines for the diagnosis of malaria (blood filmpositive for Plasmodium spp) were 70%, 16.1%, 1.9% and 95.8%, respectively.
Appropriateness of WHO manual for antimicrobial management of septicaemiaThe WHO manual (WHO 2000) for antimicrobial management of septicaemia recommendsthe combination of benzylpenicillin and chloramphenicol switching to chloramphenicol andampicillin if there has been a poor response after 48 h. In settings where antimicrobialresistance is common among Gram-negative bacteria, the use of a third generationcephalosporin is suggested to be appropriate (WHO 2000). Among all bacterial pathogensisolated from the bloodstream, 12 (48%) were resistant to ampicillin, 5 (20%) were resistantto chloramphenicol and 4 (16%) were resistant to both. No resistance to ceftriaxone orciprofloxacin was identified.
DiscussionWe demonstrate that febrile illness is a common presenting feature among paediatricpatients admitted to a tertiary hospital in northern Tanzania in an area of low malariatransmission intensity. Evaluation for malaria, HIV, and invasive bacterial and fungaldisease confirmed that malaria was uncommon and that a substantial minority of patientswere HIV-infected. Pneumococcal disease, often HIV-associated, and Salmonella entericaaccounted for a substantial proportion of invasive bacterial disease. The diagnostic tests usedin this study failed to identify a laboratory diagnosis for a large majority of patients. Malariawas over-diagnosed and invasive bacterial disease was under-diagnosed clinically. Bacterialpathogens were often resistant to commonly used antimicrobial agents. Despite this, clinicaloutcomes for those with laboratory-confirmed infections were good. However, a largerproportion of those without a laboratory diagnosis using the tests available in this study died
Crump et al. Page 6
Trop Med Int Health. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
prior to hospital discharge. The high case-fatality rate in the group without a laboratorydiagnosis underscores the need for further investigation for both infectious andnoninfectious conditions.
As anticipated in a low malaria transmission area, malaria was relatively uncommon amongfebrile patients enrolled in this study (Hay et al. 2009) and no malaria-associated deathsoccurred. Although most participants did not have laboratory evidence of malaria, malariawas a common clinical diagnosis on admission presumably associated with initial over useof antimalarial medications and under treatment of other conditions. This finding supportsthe recent WHO recommendation to use malaria diagnostic testing in all cases of suspectedmalaria before treatment (WHO 2010).
Invasive bacterial disease was predominantly caused by S. pneumoniae and Salmonellaenterica; cryptococcal disease and histoplasmosis were also indentified. Haemophilusinfluenzae bloodstream infection was uncommon despite the use of laboratory techniquesthat would optimize its isolation. Non-malaria bloodstream infection was under-diagnosedclinically, suggesting that antibacterial therapy was under-utilized on admission. Whilemalaria may be excluded using diagnostic tests that are available or could be made widelyavailable in sub-Saharan Africa (WHO 2010), diagnostic tests for invasive bacterial andfungal disease are not widely available at healthcare facilities in sub-Saharan Africa(Archibald & Reller 2001; Petti et al. 2006). In a tertiary hospital setting such as KCMC,treatment of febrile patients without malaria following current guidelines (WHO 2000)would result in substantial over use of antibacterial therapy, illustrating the limitations ofempiric treatment strategies. Consistent with many other studies from sub-Saharan Africa,bacterial bloodstream isolates were frequently resistant to the commonly used antimicrobialagents ampicillin, chloramphenicol and SXT (Mandomando et al. 2010; Nadjm et al. 2010;Reddy et al. 2010). Taken together, this evidence suggests that consideration should begiven to the reevaluation of recommendations for first-line antimicrobial management ofpaediatric bacterial sepsis in sub-Saharan Africa (WHO 2000).
Of Salmonella enterica bloodstream isolates, serotype Typhi was much more common thannon-typhoidal Salmonella. This pattern of invasive salmonellosis differs from that reportedin most other studies in sub-Saharan Africa including studies performed elsewhere inTanzania (Nadjm et al. 2010), where non-typhoidal Salmonella predominates (Crump et al.2004; Mweu & English 2008; Morpeth et al. 2009; Reddy et al. 2010). The apparentprotective effect of HIV against typhoid fever is consistent with the results of a recent meta-analysis and of a study among adults and adolescents in the same area of Tanzania (Reddy etal. 2010; Crump et al. 2011). This finding raises interesting questions about theepidemiology of invasive salmonellosis in sub-Saharan Africa, including the role of HIVand malaria, that warrant further research (Morpeth et al. 2009; MacKenzie et al. 2010;Levine & Farag 2011).
HIV infection, documented in 12.2% of febrile patients, was often immunologicallyadvanced. HIV was not always identified based on clinical suspicion nor would HIV alwayshave been detected by following clinical guidelines (WHO 2000). Pneumococcal diseaseand cryptococcal disease were associated with HIV infection, and HIV-infected patientswere less likely to be discharged alive from the hospital than those without HIV infection.These findings underscore the benefit of routinely offering HIV testing to hospitalizedpaediatric patients through provider-initiated testing (WHO/UNAIDS 2007).
More than 90% of enrolled patients had no laboratory diagnosis confirmed by the expandedlaboratory evaluations provided by the study. Furthermore, while deaths in hospital wereuncommon among those patients with laboratory-confirmed malaria and invasive bacterial
Crump et al. Page 7
Trop Med Int Health. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

and fungal disease, almost 7% of those patients without a laboratory diagnosis died.Although the range and consistent application of laboratory tests performed through thisstudy was greater than that available for routine care, we were not able to make otherlaboratory evaluations that could have explained some of the deaths. For example, we didnot have access to cerebrospinal fluid samples; we did not study respiratory tract samples tosupport the aetiologic diagnosis of pneumonia; nor did we examine stool in patients withdiarrhoea. Furthermore, the sensitivity of a single blood culture is <100% and may befurther diminished by the prior antimicrobial exposure common among patients at a tertiaryhospital. However, it is also possible that infections beyond those identified by examinationof such specimens could have played a role. Evaluation of this patient group for otherinfectious aetiologies is warranted.
This study had a number of limitations. Bias may have been introduced because of failure toenroll all eligible patients. Because the study was designed before the availability of theWHO pocket book of hospital care of children (WHO 2005), the performance of thoseguidelines could not be assessed. Furthermore, the study duration of only 1 year did notallow us to assess changes across longer time periods.
In summary, the hospital management of febrile illness in sub-Saharan Africa poses manychallenges. Recent recommendations to use malaria diagnostic tests to guide the use ofantimalarial medications, if adopted, should lead to reductions in the over-diagnosis ofmalaria particularly in low transmission intensity areas, such as Moshi. Full implementationof routine provider-initiated HIV testing should contribute to ensuring that infants andchildren with HIV and associated co-infections receive appropriate care. However, targetingantibacterial treatment to those with the highest risk of invasive bacterial disease ischallenging. Whereas current practice in many settings underutilizes antibacterial therapy(Reyburn et al. 2004), following existing guidelines may result in overuse of antibacterialtherapy. Expansion of clinical microbiology services and focused research would provideuseful evidence to guide policy on targeted and empiric management. Furthermore, a largeproportion of paediatric patients without laboratory evidence of malaria or invasive bacterialdisease died in hospital. Further research on this group using an expanded range ofdiagnostic evaluations may contribute to reducing mortality in these children.
AcknowledgmentsThe authors thank Ahaz T. Kulanga, MBA, for providing administrative support to this study and Pilli M. Chambo,Beata V. Kyara, Beatus A. Massawe, Anna D. Mtei, Godfrey S. Mushi, Lillian E. Ngowi, Flora M. Nkya andWinfrida H. Shirima for reviewing and enrolling study participants. We are grateful to the leadership, clinicians andpatients of KCMC for their contributions to this research. We thank Angela Karani, KEMRI-Wellcome TrustResearch Programme, Kilifi, Kenya, for serotyping S. pneumoniae strains, and Gino R. Micalizzi and John R.Bates, Queensland Health Forensic and Scientific Services, Brisbane, Australia, for assistance with serotyping non-typhoidal Salmonella strains. We thank Inverness Medical for donating Binax® NOW Legionella Urinary AntigenTest kits for the study. We thank Miravista Diagnostics, Indianapolis, Indiana, USA, for performing Histoplasmacapsulatum Quantitative Antigen EIA on patient samples. We acknowledge the Hubert-Yeargan Center for GlobalHealth at Duke University for critical infrastructure support for the Kilimanjaro Christian Medical Centre-DukeUniversity Collaboration.
ReferencesArchibald LK, Reller LB. Clinical microbiology in developing countries. Emerging Infectious
Diseases. 2001; 7:302–305. [PubMed: 11294729]
Berkley JA, Lowe BS, Mwangi I, et al. Bacteremia among children admitted to a rural hospital inKenya. New England Journal of Medicine. 2005; 352:39–47. [PubMed: 15635111]
Brent AJ, Ahmed I, Ndiritu M, et al. Incidence of clinically significant bacteraemia in children whopresent to hospital in Kenya: community-based observational study. Lancet. 2006; 367:482–488.[PubMed: 16473125]
Crump et al. Page 8
Trop Med Int Health. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Bryce J, Boschi-Pinto C, Shibuya K, Black RE. the WHO Child Health Epidemiology ReferenceGroup. WHO estimates of the causes of death in children. Lancet. 2005; 365:1147–1152. [PubMed:15794969]
Buchanan AM, Muro FJ, Gratz J, et al. Establishment of haematological and immunological referencevalues for healthy Tanzania children in the Kilimanjaro Region. Tropical Medicine andInternational Health. 2010; 15:1011–1021. [PubMed: 20636301]
Campbell JD, Kotloff KL, Sow SO, et al. Invasive pneumococcal infections among hospitalizedchildren in Bamako, Mali. The Pediatric Infectious Disease Journal. 2004; 23:642–649. [PubMed:15247603]
Chandler CIR, Drakeley CJ, Reyburn H, Carneiro I. The effect of altitude on parasite density casedefinitions for malaria in northeastern Tanzania. Tropical Medicine and International Health. 2006;11:1178–1184. [PubMed: 16903881]
Clinical Laboratories Standards Institute. CLSI document M100-S18. Wayne, PA: ClinicalLaboratories Standards Institute; 2008. Performance Standards for Antimicrobial SusceptibilityTesting: 18th Informational Supplement.
Connolly PA, Durkin MM, LeMonte AM, Hackett EJ, Wheat JL. Detection of Histoplasma antigen bya quantitative enzyme immunoassay. Clinical and Vaccine Immunology. 2007; 14:1587–1591.[PubMed: 17913863]
Crump JA, Barrett TJ, Nelson JT, Angulo FJ. Reevaluating fluoroquinolone breakpoints forSalmonella enterica serotype Typhi and for non-Typhi salmonellae. Clinical Infectious Diseases.2003; 37:75–81. [PubMed: 12830411]
Crump JA, Luby SP, Mintz ED. The global burden of typhoid fever. Bulletin of the World HealthOrganization. 2004; 82:346–353. [PubMed: 15298225]
Crump JA, Scott LE, Msuya E, et al. Evaluation of the Abbott m2000rt RealTime HIV-1 assay withmanual sample preparation compared with the ROCHE COBAS AmpliPrep/AMPLICOR HIV-1MONITOR 1.5 using specimens from East Africa. Journal of Virological Methods. 2009;162:218–222. [PubMed: 19729037]
Crump JA, Ramadhani HO, Morrissey AB, et al. Invasive bacterial and fungal infections amonghospitalized HIV-infected and HIV-uninfected adults and adolescents in northern Tanzania.Clinical Infectious Diseases. 2011; 52:341–348. [PubMed: 21217181]
Gordon MA, Graham SM, Walsh AL, et al. Epidemics of invasive Salmonella enterica serovarEnteritidis and S. enterica serovar Typhimurium infection associated with multidrug resistanceamong adults and children in Malawi. Clinical Infectious Diseases. 2008; 46:963–969. [PubMed:18444810]
Greenwood BM, Armstrong JRM. Comparison of two simple methods for determining malariaparasite density. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1991;85:186–188. [PubMed: 1887466]
Grimont, PAD.; Weill, F-X. Antigenic Formulae of the Salmonella Serovars. 9th edn. WHOCollaborating Centre for Reference and Research on Salmonella. , editor. Paris, France: InstitutPasteur; 2007.
Hay SI, Guerra CA, Gething PW, et al. A world malaria map: Plasmodium falciparum endemicity in2007. PLoS Medicine. 2009; 6 e1000048.
Levine MM, Farag TH. Invasive Salmonella infections and HIV in northern Tanzania. ClinicalInfectious Diseases. 2011; 52:349–351. [PubMed: 21217182]
Liu Y-C, Huang WK, Huang TS, Kunin CM. Detection of antimicrobial activity in urine forepidemiologic studies of antibiotic use. Journal of Clinical Epidemiology. 1999; 52:539–545.[PubMed: 10408993]
MacKenzie G, Ceesay SJ, Hill PC, et al. A decline in the incidence of invasive non-typhoidalSalmonella infection in the Gambia temporally associated with a decline in malaria infection.PLoS One. 2010; 5 e10568.
Mandomando I, Sigauque B, Morais L, et al. Antimicrobial drug resistance trends in bacteremiaisolates in a rural hospital in southern Mozambique. American Journal of Tropical Medicine andHygiene. 2010; 83:152–157. [PubMed: 20595494]
Crump et al. Page 9
Trop Med Int Health. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mayhood MK, Afwamba IA, Odhiambo CO, et al. Validation, performance under field conditions, andcost-effectiveness of Capillus HIV-1/HIV-2 and Determine HIV-1/2 rapid humanimmunodeficiency virus antibody assays using sequential and parallel testing algorithms inTanzania. Journal of Clinical Microbiology. 2008; 46:3946–3951. [PubMed: 18923015]
Mishra V, Vaessen M, Boerma JT, et al. HIV testing in national population-based surveys: experiencefrom the Demographic and Health Surveys. Bulletin of the World Health Organization. 2006;84:537–545. [PubMed: 16878227]
Morpeth SC, Ramadhani HO, Crump JA. Invasive non-Typhi Salmonella disease in Africa. ClinicalInfectious Diseases. 2009; 49:606–611. [PubMed: 19591599]
Mweu E, English M. Typhoid fever in children in Africa. Tropical Medicine and International Health.2008; 13:1–9. [PubMed: 18578806]
Nadjm B, Amos B, Mtove G, et al. WHO guidelines for antimicrobial treatment in children admitted tohospital in an area of intense Plasmodium falciparum transmission: prospective study. BMJ. 2010;340 c1350.
National Bureau of Statistics & ORC Macro. Tanzania Demographic and Health Survey 2004–05. In:National Bureau of Statistics & ORC Macro. , editor. Dar es Salaam: National Bureau of Statistics& ORC Macro; 2005.
O’Meara WP, Mangeni JN, Steketee R, Greenwood B. Changes in the burden of malaria in sub-Saharan Africa. The Lancet Infectious Diseases. 2010; 10:545–555. [PubMed: 20637696]
Petit PL, van Ginneken JK. Analysis of hospital records in four African countries 1975–1990, withemphasis on infectious diseases. The Journal of Tropical Medicine and Hygiene. 1995; 98:217–227. [PubMed: 7636917]
Petti CA, Polage CR, Quinn TC, et al. Laboratory medicine in Africa: a barrier to effective health care.Clinical Infectious Diseases. 2006; 42:377–382. [PubMed: 16392084]
Reddy EA, Shaw AV, Crump JA. Community acquired bloodstream infections in Africa: a systematicreview and meta-analysis. The Lancet Infectious Diseases. 2010; 10:417–432. [PubMed:20510282]
Reyburn H, Mbatia R, Drakeley C, et al. Overdiagnosis of malaria in patients with severe febrileillness in Tanzania: a prospective study. BMJ. 2004; 329:1212–1215. [PubMed: 15542534]
Scott LE, Crump JA, Msuya E, et al. Abbott RealTime HIV-1 m2000rt viral load testing: manualextraction versus the automated m2000sp extraction. Journal of Virological Methods. 2011;172:78–80. [PubMed: 21172389]
Sigauque B, Roca A, Mandomando I, et al. Community-acquired bacteremia among children admittedto a rural hospital in Mozambique. The Pediatric Infectious Disease Journal. 2009; 28:108–113.[PubMed: 19131902]
WHO. Geneva: WHO; 2000. Management of the Child with a Serious Infection or SevereMalnutrition: Guidelines for Care at the First-Referral Level in Developing Countries.
WHO. Geneva: WHO; 2005. Pocket Book of Hospital Care for Children: Guidelines for theManagement of Common Illnesses with Limited Resources.
WHO. Geneva: WHO; 2009. World Malaria Report 2009.
WHO. 2nd edn. Geneva: WHO; 2010. Guidelines for the Treatment of Malaria.
WHO/UNAIDS. Geneva: WHO; 2007. Guidance on Provider-Initiated HIV Testing and Counseling inHealthcare Facilities.
Crump et al. Page 10
Trop Med Int Health. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Crump et al. Page 11
Tabl
e 1
Inva
sive
infe
ctio
ns a
mon
g H
IV-i
nfec
ted
and
HIV
-uni
nfec
ted
paed
iatr
ic p
artic
ipan
ts, K
CM
C 2
007–
2008
Par
tici
pant
s n
(%)
Pat
hoge
nA
ll(n
= 3
98)†
HIV
-inf
ecte
d(n
= 5
7)H
IV-u
ninf
ecte
d(n
= 3
41)
OR
(95%
CI)
Ent
erob
acte
riac
eae
E
sche
rich
ia c
oli
3 (0
.75)
1 (1
.75)
2 (0
.59)
3.03
(0.2
7, 3
3.94
)
S
alm
onel
la T
yphi
6 (1
.51)
0 (0
.00)
6 (1
.76)
Und
efin
ed
S
alm
onel
la n
on-t
ypho
idal
1 (0
.25)
1 (1
.75)
0 (0
.00)
*
Oth
er g
ram
-neg
ativ
e or
gani
sms
L
egio
nella
pne
umop
hila
ser
ogro
up 1
‡0
(0.0
0)0
(0.0
0)0
(0.0
0)*
H
aem
ophi
lus
infl
uenz
ae ty
pe b
1 (0
.25)
0 (0
.00)
1 (0
.29)
*
Gra
m-p
ositi
ve o
rgan
ism
s
S
trep
toco
ccus
pne
umon
iae
5 (1
.26)
4 (7
.02)
1 (0
.29)
25.6
6(2
.81,
234
.00)
Yea
sts
C
rypt
ococ
cus
neof
orm
ans§
2 (0
.50)
2 (3
.51)
0 (0
.00)
Und
efin
ed
H
isto
plas
ma
caps
ulat
um¶
2 (0
.50)
1 (1
.75)
1 (0
.29)
6.07
(0.3
7, 9
8.48
)
Plas
mod
ia
P
lasm
odiu
m fa
lcip
arum
6 (1
.51)
0 (0
.00)
6 (1
.76)
Und
efin
ed
P
lasm
odiu
m n
on-f
alci
paru
m0
(0.0
0)0
(0.0
0)0
(0.0
0)*
Tot
al n
umbe
r of
par
ticip
ants
with
inva
sive
infe
ctio
ns**
26 (
6.53
)9
(15.
79)
17 (
4.99
)3.
57(1
.51,
8.4
7)
* Num
bers
too
smal
l to
calc
ulat
e a
test
sta
tistic
.
† HIV
sta
tus
was
unk
now
n fo
r 69
par
ticip
ants
.
‡ By
urin
e an
tigen
test
ing.
§ Of
inva
sive
Cry
ptoc
occu
s ne
ofor
man
s di
agno
ses,
all
wer
e by
ser
um a
ntig
en d
etec
tion
with
neg
ativ
e bl
ood
cultu
re.
¶ All
H. c
apsu
latu
m d
iagn
oses
wer
e by
uri
ne a
ntig
en d
etec
tion.
**N
o pa
tient
s ha
d m
ore
than
one
inva
sive
infe
ctio
n co
nfir
med
by
bloo
d cu
lture
and
ant
igen
det
ectio
n.
Trop Med Int Health. Author manuscript; available in PMC 2012 July 24.
Copyright © 2022 FDOKUMEN