Intraoperative sentinel lymph node mapping in stage I non-small cell lung cancer: detection of...
6
Intraoperative sentinel lymph node mapping in stage I non-small cell lung cancer: detection of micrometastases by polymerase chain reaction § Franca M.A. Melfi a, * , Marco Lucchi a , Federico Davini a , Andrea Viti a , Gabriella Fontanini b , Laura Boldrini b , Giuseppe Boni c , Alfredo Mussi a a Division of Thoracic Surgery, Cardiac and Thoracic Department, University of Pisa, Italy b Department of Surgery, University of Pisa, Italy c Division of Nuclear Medicine, Department of Oncology, University of Pisa, Italy Received 21 September 2007; received in revised form 18 February 2008; accepted 4 March 2008; Available online 27 May 2008 Abstract Objective: We previously reported the results achieved in detecting sentinel lymph nodes (SLN). We applied the molecular techniques (RT-PCR) to improve the detection of micrometastasis in order to evaluate an improvement of staging in early non-small cell lung cancer (NSCLC) patients (pts). Methods: This study was carried out on 22 consecutive NSCLC pts with stage I disease. A dose of 37 MBq (1 ml 99m Tc-nanocolloid W suspension) was administered. The intralesional injection was performed underCT-guidance (7 pts), by using bronchoscopy (5 pts), VATS (2 pts) and at time of the thoracotomy (8 pts). RT-PCR analysis for cytokeratin 7 and 19 (CK7—CK19) was used to identify tumour-derived material in lymph nodes (LN). Each SLN was bisected: half was used for conventional examination (H&E staining/by immunohistochemistry (IHC), half was snap-frozen to 80 8C for RNA-detection of CK7 and CK19. Results: SLN was detected in 16 out of 19 pts. In three pts SLN was not identified (due to an incorrect technique). Conventional pathologic examination showed stage I disease in 13 pts, T3N0 disease in 1 pt, N2 in 5 pts. The IHC analysis identified micrometastasis in seven pts (two evaluated N0 according to H&E staining). RT-PCR analysis, performed in 10/16 pts, identified micrometastasis in 6 pts (3 pts evaluated N0 disease by H&E; 1 of these evaluated N0 even by IHC). All N2 patients relapsed. One patient (N0 pts after H&E and IHC analysis) with positive CK7 and CK19 expression by RT-PCR analysis relapsed (systemic relapse) 3 months after surgery. Conclusions: SLN technique could provide a subgroup of patients in which the use of RT-PCR could be applied on a well-focused target. This approach may be useful for stratifying histologically N0 patients into higher risk and lower risk groups. # 2008 European Association for Cardio-Thoracic Surgery. Published by Elsevier B.V. All rights reserved. Keywords: Lung cancer; Sentinel lymph node; Molecular staging; Cytokeratin 7 and 19 1. Introduction The prognosis of patients with non-small cell lung cancer (NSCLC) is closely related to the pathologic stage of the disease, with the pattern of regional lymph node (LN) involvement as a major determinant [1]. Although surgical treatment represents the best chance in 30% of patients with early stage cancer, a high relapse rate (40%) is recorded within 24 months after complete resection (surgery and complete lymph-adenectomy) [2—4]. Undetected metastatic disease is the cause of these recurrences, which may remain undetected for three reasons: (1) an inadequacy of the lymph-adenectomy (the lymph nodes draining the tumour are either not or incompletely removed), (2) inadequacy of pathologic examinations (methods used to detect tumour-derived material in LNs are insensitive) and finally, (3) the lymphatic drainage does not always follow the predicted pattern. Previous studies sought to improve LN micrometastases identification during surgery through sentinel lymph node (SLN) mapping, or to improve the sensitivity of detecting tumour cells within the resection. Experience with mela- noma [5] and breast cancer [6] demonstrated that SLNs were diagnostically accurate, in predicting the status of more distant lymph node stations. In NSCLC, a few studies identified SLN in >80% of patients and the SLN status was predictive in 80—100% of patients [7—9]. We previously reported the positive results achieved in detecting SLN with a 99m Tc-nanocolloid suspension and micrometastasis by immunohistochemistry (IHC) in NSCLC-stage I patients [9]. However, standard detection methods have a low sensitivity, reverse tran- scriptase-polymerase chain reaction (RT-PCR), which was developed to detect transcripts of genes expressed by tumour cells, is a tool for detecting LN-micrometastasis that is more sensitive than IHC [10—12]. Micrometastasis detected by RT-PCR has been associated with a worse www.elsevier.com/locate/ejcts European Journal of Cardio-thoracic Surgery 34 (2008) 181—186 § Presented at the 21st Annual Meeting of the European Association for Cardio-thoracic Surgery, Geneva, Switzerland, September 16—19, 2007. * Corresponding author. Tel.: +39 050 995211; fax: +39 050 9957239. E-mail address: f.melfi@med.unipi.it (F.M.A. Melfi). 1010-7940/$ — see front matter # 2008 European Association for Cardio-Thoracic Surgery. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.ejcts.2008.03.059
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Intraoperative sentinel lymph node mapping in stage I non-small cell lung cancer: detection of...

Intraoperative sentinel lymph node mapping in stage I non-small cell lungcancer: detection of micrometastases by polymerase chain reaction§
Franca M.A. Melfi a,*, Marco Lucchi a, Federico Davini a, Andrea Viti a, Gabriella Fontanini b,Laura Boldrini b, Giuseppe Boni c, Alfredo Mussi a
aDivision of Thoracic Surgery, Cardiac and Thoracic Department, University of Pisa, ItalybDepartment of Surgery, University of Pisa, Italy
cDivision of Nuclear Medicine, Department of Oncology, University of Pisa, Italy
Received 21 September 2007; received in revised form 18 February 2008; accepted 4 March 2008; Available online 27 May 2008
www.elsevier.com/locate/ejctsEuropean Journal of Cardio-thoracic Surgery 34 (2008) 181—186
Abstract
Objective:We previously reported the results achieved in detecting sentinel lymph nodes (SLN). We applied themolecular techniques (RT-PCR)to improve the detection of micrometastasis in order to evaluate an improvement of staging in early non-small cell lung cancer (NSCLC) patients(pts). Methods: This study was carried out on 22 consecutive NSCLC pts with stage I disease. A dose of 37 MBq (1 ml 99mTc-nanocolloidW
suspension) was administered. The intralesional injection was performed under CT-guidance (7 pts), by using bronchoscopy (5 pts), VATS (2 pts)and at time of the thoracotomy (8 pts). RT-PCR analysis for cytokeratin 7 and 19 (CK7—CK19) was used to identify tumour-derived material inlymph nodes (LN). Each SLN was bisected: half was used for conventional examination (H&E staining/by immunohistochemistry (IHC), half wassnap-frozen to�80 8C for RNA-detection of CK7 and CK19. Results: SLNwas detected in 16 out of 19 pts. In three pts SLNwas not identified (due toan incorrect technique). Conventional pathologic examination showed stage I disease in 13 pts, T3N0 disease in 1 pt, N2 in 5 pts. The IHC analysisidentified micrometastasis in seven pts (two evaluated N0 according to H&E staining). RT-PCR analysis, performed in 10/16 pts, identifiedmicrometastasis in 6 pts (3 pts evaluated N0 disease by H&E; 1 of these evaluated N0 even by IHC). All N2 patients relapsed. One patient (N0 ptsafter H&E and IHC analysis) with positive CK7 and CK19 expression by RT-PCR analysis relapsed (systemic relapse) 3 months after surgery.Conclusions: SLN technique could provide a subgroup of patients in which the use of RT-PCR could be applied on a well-focused target. Thisapproach may be useful for stratifying histologically N0 patients into higher risk and lower risk groups.# 2008 European Association for Cardio-Thoracic Surgery. Published by Elsevier B.V. All rights reserved.
Keywords: Lung cancer; Sentinel lymph node; Molecular staging; Cytokeratin 7 and 19
1. Introduction
The prognosis of patients with non-small cell lung cancer(NSCLC) is closely related to the pathologic stage of thedisease, with the pattern of regional lymph node (LN)involvement as a major determinant [1]. Although surgicaltreatment represents the best chance in 30% of patients withearly stage cancer, a high relapse rate (40%) is recordedwithin 24 months after complete resection (surgery andcomplete lymph-adenectomy) [2—4].
Undetected metastatic disease is the cause of theserecurrences, which may remain undetected for threereasons: (1) an inadequacy of the lymph-adenectomy (thelymph nodes draining the tumour are either not orincompletely removed), (2) inadequacy of pathologicexaminations (methods used to detect tumour-derived
§ Presented at the 21st Annual Meeting of the European Association forCardio-thoracic Surgery, Geneva, Switzerland, September 16—19, 2007.* Corresponding author. Tel.: +39 050 995211; fax: +39 050 9957239.E-mail address: [email protected] (F.M.A. Melfi).
1010-7940/$ — see front matter # 2008 European Association for Cardio-Thoracicdoi:10.1016/j.ejcts.2008.03.059
material in LNs are insensitive) and finally, (3) the lymphaticdrainage does not always follow the predicted pattern.
Previous studies sought to improve LN micrometastasesidentification during surgery through sentinel lymph node(SLN) mapping, or to improve the sensitivity of detectingtumour cells within the resection. Experience with mela-noma [5] and breast cancer [6] demonstrated that SLNs werediagnostically accurate, in predicting the status of moredistant lymph node stations.
In NSCLC, a few studies identified SLN in >80% ofpatients and the SLN status was predictive in 80—100% ofpatients [7—9]. We previously reported the positive resultsachieved in detecting SLN with a 99mTc-nanocolloidsuspension and micrometastasis by immunohistochemistry(IHC) in NSCLC-stage I patients [9]. However, standarddetection methods have a low sensitivity, reverse tran-scriptase-polymerase chain reaction (RT-PCR), which wasdeveloped to detect transcripts of genes expressed bytumour cells, is a tool for detecting LN-micrometastasisthat is more sensitive than IHC [10—12]. Micrometastasisdetected by RT-PCR has been associated with a worse
Surgery. Published by Elsevier B.V. All rights reserved.

F.M.A. Melfi et al. / European Journal of Cardio-thoracic Surgery 34 (2008) 181—186182
prognosis in patients with melanoma and prostate carci-noma [13—15]. In lung cancer few reports exist in this field[16,17]. Our previous study on intraoperative SLN mappingestablished the feasibility of this technique and formed thebasis of this progress report on the evolving utility of thistechnique in lung cancer [9]. Thus, since January 2005, wecombined the SLN mapping technique with molecularstaging using cytokeratin 7 and 19 (CK7-CK19), which aremarkers of epithelial cells. We hypothesised that the RT-PCR for RNA-detection of CK7 and CK19 would accuratelydetect micrometastases and define an improvement ofstaging in patients with early lung cancer (stage I disease).The preliminary results show that this technique couldprovide a sub-group of patients in which the use of RT-PCRcould be applied on a well-focused target. This approachmay be useful for stratifying histologically N0 patients intohigher risk and lower risk groups.
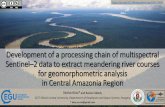
Fig. 1. Peripheral tumours: radio injection (99mTc-nanocolloidW) underCT-guidance/thoracoscopy.
2. Materials and methods
From May 2001 to June 2006, 51 consecutive patients withNSCLC (stage IA—IB) were enrolled. The first 29 pts wereincluded in the first step of our study (validation phase). Allresected lymph nodes were analysed by conventionalpathologic methods (haematoxylin and eosin staining(H&E) and immunohistochemistry (IHC). Since January2005, 22 consecutive pts (11 female; median age 69 years,range: 56—78) were selected for SNL mapping by using a newprotocol. SLNs were analysed in 16 out of 19 pts by usingconventional pathologic examination (H&E/IHC), and mole-cular analysis by RNA transcriptase-polymerase chain reac-tion (RT-PCR).
The study was approved by the local ethics committee andinformed consent was obtained from each patient.
2.1. Eligibility
Only patients able to tolerate anatomic resection andcomplete mediastinal node dissection were included in thisstudy. Routine preoperative staging was performed includ-ing: clinical examination, blood chemistry analysis, chest X-ray, thoracic computed tomography (CT) scanning andpositron emission tomography (PET) scanning, abdominalultrasonography and bronchoscopy. Furthermore, bonescintigraphy and brain CT scan were performed in patientswith suspected distant metastases. The tumour stage wasclassified according to the Revisions in the InternationalSystem for Staging Lung Cancer [18].
Selection criteria were: (a) over 18 years of age (legalmajority), (b) clinical stage I NSCLC (stage IA—IB), (c)absence of intra-thoracic adenopathy with normal broncho-scopic appearance. Patients with pulmonary metastasis,previous thoracic surgery/adjuvant therapy, enlarged med-iastinal lymph nodes more than 1.0 cm in short axis diameteron CT/PET scan or with primary tumour larger than 3 cm insize were excluded. In accordance with our then normalpractice for small lesions without mediastinal lymphadeno-pathy (on the CT/PET scan), mediastinoscopy was notundertaken. These patients were judged to have clinicalstage I (NSCLC).
Standard lobectomy combined with systematic lymphnode dissection was performed to achieve anatomic resec-tion of the tumour.
2.2. Technique
The SLN technique previously described in our paper wassimilar to that of other authors [7—9].
99mTc-nanocolloids of human albumin (particle size: over95% <80 nm) was used. A total dose of 37 MBq in a maximumvolume of 1 ml was administered in 2—4 divided aliquots(depending on the size of the tumour), injected at theperiphery of the tumour. Readings were taken with thegamma ray detector (Scinti Probe MR100-Pol.hi.tech.,Aquila, Italy).
The radiotracer was administered on the basis of thetumour’s location: the medium-parenchyma tumours wereinjected by bronchoscopy or at the time of thoracotomy;those located at periphery were injected under CT-guidanceor by thoracoscopy. The molecular analysis (RT-PCR) wasadded at conventional pathologic SNL examination (H&Eand IHC).
2.3. Peripheral tumours
The tumours were localised by means of 5 mm thick highresolution axial computed tomographic sections or by 7 mmendoscopic camera usually at sixth/seventh intercostal spacealong the midaxillary line. A 22G needle was introduced atthe peripheral margins of the tumour through which wasinjected the radiotracer (Fig. 1).
2.4. Medium-parenchyma tumours
The radioisotope suspension was administered by a fibre-optic bronchoscope or directly during thoracotomy if thetechnique using bronchoscope was not applicable. Thisprocedure was performed under fluoroscopic guidance byusing an endoscopic-needle inserted at the carina of the

F.M.A. Melfi et al. / European Journal of Cardio-thoracic Surgery 34 (2008) 181—186 183
Fig. 2. Medium-parenchyma tumours. Radio injection (99mTc-nanocolloidW) bybronchoscopy.
most distal pulmonary sub-segment closed to the tumour(Fig. 2).
The intraoperative radioactivity counting at the nodalstations started an average of 1 h (range 50—70 min) afterthe injection. The radiolabelled tumour and lymph nodestations were examined in vivo and ex vivo. The migration ofthe 99mTc-nanocolloid suspension was considered successfulif a specific nodal station measured greater than three timesthe background. The sentinel node was classified as thenode(s) with the highest count rate.
At the end of the operation (after lobectomy and excisionof the sentinel lymph node) the mediastinal stations werealso examined before performing a complete lymph nodedissection. On completion of the procedure a repeatedexamination with gamma probe was performed to check theresidual activity. If indicated by the gamma counter, wecompleted the re-resections of the nodal stations.
Mediastinal nodal dissection was performed in all eligiblepatients. Mediastinal metastasis was considered skipping ifany one of the mediastinal lymph nodes was involved by thetumour, without hilar or intrapulmonary node metastases.Reassessment of the mediastinum with gamma probe afterdissection was routinely performed.
The locations of the lymph nodes were defined accordingto Naruke’s map.
2.5. Pathologic evaluation
The pathological analysis was not employed intraopera-tively. One-half of the SNL was fixed in formalin and wasembedded in paraffin for histological analysis and immuno-histochemical staining. The other half of the resected nodewas snap-frozen in liquid nitrogen and stored at �80 8C untilthe time of RNA isolation for the analysis of cytokeratin 7(CK7) and cytokeratin 19 (CK19), as markers of epithelialdifferentiation.
After formalin fixation and embedding in paraffin,sections (2 or 3) were cut and stained with haematoxylinand eosin. Sentinel and non-sentinel nodes were subse-quently examined by IHC for pankeratin CK, CK7 and CK19(Ventana Medical System).
Molecular analysis (RT-PCR) was applied in our secondseries (our present study). The presence of mRNA forcytokeratin (CK7 and CK19) within the sentinel lymph
nodes was accepted as evidence of micrometastatic tumourcells.
2.5.1. Technical detailsThe RNAwas extracted by a standard method, assessed by
electrophoresis on a 0.8% agarose gel to determine itsintegrity and was quantified spectrophotometrically.
Using two rounds of amplifications (RT-PCR) and serialdilutions of RNA it was possible to detect down to onetumoural cell in 106. The primer sequences for CK7 wereas follows: A: 50-TGAAATTAACCGCCGCACAG-30 and B: 50-TGCATTTGGCCATCTCCTCA-30 for the first PCR, and C: 50-GGATGCTGCCTACATGAGC-30 and D: 50-CCAGGGAGCGAC-TGTTGT-30 for the second PCR. First round amplificationstarted with a ‘hot start’ of 100 8C for 10 min. Thirty-fivecycles were performed consisting of 1 min denaturation at94 8C, annealing at 65 8C for 1 min, and extension for 2 min at72 8C. The PCR reaction was terminated with a 10 minextension. This set of primers produced, after the two roundsof amplification, three bands: 163, 220, and 277 bp. Theprimer sequences for CK19 were as follows: A: 50-AAGC-TAACCATGCAGAACCTCAACGACCGC-30 and B: 50-TTATTGG-CAGGTCAGGAGAAGAGCC-30 for the first PCR, and C:50-AGGTGGATTCCGCTCCGGGCA-30 and D: 50-CGCGACTT-GATGTCCATGAGCCGCTGGTAC-30 for the second PCR. Thecycling conditions were as follows: 94 8C for 1 min, 68 8C for2 min for 20 cycles for the first PCR and 20 cycles for thesecond PCR. All PCR reactions were preceded by adenaturation step at 94 8C for 3 min, and terminated by a10 min extension at 72 8C. The expected size for CK19amplification band was 409 bp.
All frozen specimens were held until the final pathologyreport was issued in case the tissue was needed for routineanalysis.
3. Results
Positive results in detecting micrometastasis (by IHC) onthe first series (29 pts) were previously published [Eur. J.Cardiothorac. Surg., Feb 2003;23:214—20]. Briefly, SLNswere identified in 96.1% of patients, with a total of 31 SLNsdetected. Seven out of 31 SLNs (22.5%) were positive formetastatic involvement after full histo-pathologic evaluation(including IHC). In 2/7 of these positive SLNs (positive SLN inlevel 10) IHC revealed an additional positive N2 station. Twopositive SLN (28.5%) were skipping metastases (levels 9 and7). Step sections and IHC examination revealed microme-tastases in 5 (20%) out of 25 patients without metastasis inthe routine haematoxylin and eosin-stained sections. OverallKaplan—Meier survival at 3 years was 78.1 � 11 months for p-stage I pts vs 50 � 12.3 months for overstaged pts (with IHC).No significant difference ( p = 0.1) was observed.
In the present series, 22 patients were selected for SLNmapping. Three patients with benign lesions were excludedfrom further analysis. All patients underwent major lungresections (lobectomy was the only procedure performed)and complete lymph-adenectomy. The mean tumour size was2.5 � 0.7 cm (range 0.8—3.5 cm).
SLNs were detected in 16/19 patients. In 3 out of the 19patients (#17, #18, #19) SLN was not identified due to

F.M.A. Melfi et al. / European Journal of Cardio-thoracic Surgery 34 (2008) 181—186184
Table 1Patient data
Sex Age Histology pTNM SLN IHC PCR
M 78 Adenocarcinoma T4N2 7 Positive PositiveF 56 Adenocarcinoma T2N2 12 Positive Not appliedF 73 Adenocarcinoma T1N0 10 Negative Not appliedM 74 Adenocarcinoma T1N2 7 Positive PositiveM 76 Squamous cell carcinoma T3N0 12 Negative NegativeM 71 Adenocarcinoma T1N0 8 Negative Not appliedM 67 Large cell carcinoma T2N0 11 Not applied Not appliedM 63 Adenocarcinoma T2N2 10 Positive PositiveF 67 Adenocarcinoma T2N0 11 Positive Positivea
F 75 Adenocarcinoma T2N0 4 Negative NegativeF 78 Squamous cell carcinoma T1N0 10 Negative NegativeM 74 Bronchoalveolar carcinoma T1N0 4 Negative Not appliedM 73 Adenocarcinoma T1N0 10 Negative NegativeM 72 Adenocarcinoma T1N0 10 Negative Positivea
F 57 Adenocarcinoma T2N0 11 Positive Positivea
F 71 Adenocarcinoma T2N2 11 Positive Not appliedF 58 Adenocarcinoma T1N0 No Not applied Not appliedF 66 Adenocarcinoma T1N0 No Not applied Not appliedM 76 Adenocarcinoma T1N0 No Not applied Not applied
a Upstaged pts.
Fig. 3. Results differences in detecting micrometastases by H&E/IHC/RT-PCR.
incorrect technique in which the radiotracer injected intothe tumour had a poor migration, due to the fact that thetracer was not administered at periphery. Patient’s data aresummarised in Table 1.
A single SLN was identified in each patient (total numberof SLNs were 16). Among the 16 SLNs, 5 were noted to bemediastinal LN (25%), of which 2 were level 7 and 2were level4; 1 was level 8. Five SLNs were found at level 10, 4 at level11, and 2 at level 12.
H&E revealed 15 adenocarcinomas, 2 squamous cellcarcinomas, 1 large cell carcinoma, and 1 bronchoalveolarcarcinoma. According to TNM classification, pathologicstaging identified: 10 patients with stage I disease; 1 patientswith stage IIB; 4 patients with stage IIIA disease; and 1 patientwith stage IIIB disease (Table 1).
IHC examination revealed micrometastases in 7 out of 16(43.75%) patients; 2 of them evaluated N0 by H&E staining.
RT-PCR analysis was applied in 10 out of 16 pts (in theremaining six samples, the frozen half of each SLN wasinsufficient). Micrometastases were detected in six patients;four of these evaluated N0 according to conventionalexamination (three N0 by H&E, one N0 by IHC).
3.1. Upstaging by conventional and molecular analysis(Table 2, Fig. 3)
All SLNs tested by RT-PCR, were analysed also by H&E andIHC. In 9 out of 10 patients, RT-PCR confirmed the IHC stagingin all SNLs that could be evaluated. Three patients (#9, #14,#15) who had stage I disease according to routine patholo-gical examination, were upstaged from stage I to stage II(from N0 to N1). Two of them (#9, #15) with positive IHC forpankeratin were evaluated stage II also by RT-PCR. In the 3rdpatient (#14) with negative IHC, micrometastasis wereidentified only by RT-PCR analysis. The presence ofcytokeratin 19 (CK19) as markers of epithelial differentiationwas accepted as evidence of micrometastatis (Fig. 4). Thispatient had a systemic relapse 3 months after surgery anddied 4 months later. Any patients with N0 or N1 disease by RT-
PCR staging had recurrences. Of the five patients with N2disease according to the RT-PCR analysis, three (#1, #4, #8)patients developed recurrent disease 3, 13, and 14 monthafter surgery, respectively.
During the follow-up of 9—24 months, three patients died(#1, #8, #14) due to recurrent disease. Of the patients whoremained alive, one pt with N2 disease (#4) has recurrence.
Summarizing our data: No complications were observedduring the sentinel lymph node mapping procedure. Success-ful radio nuclide migration was 84.21% (with 0 out of 16 falsenegative patients). Regarding the pathologic methods, onefalse negative was noticed by IHC technique, and none by RT-PCR analysis. In this series no skipping was observed.
4. Comment
Lymph node metastasis is the most important prognosticfactor in localised and resectable NSCLC. Patients with N0

F.M.A. Melfi et al. / European Journal of Cardio-thoracic Surgery 34 (2008) 181—186 185
Fig. 4. Patient (#14): pathologic profile.
disease have favourable survival rates. However, up to 40% ofthese patients have a recurrence of the tumour andsubsequently die, despite complete surgical resection [18].This suggests that occult micrometastasis tumour cells,undetected by clinical staging examinations and routinehisto-pathological methods, have already spread to theregional nodes at the time of surgery [1—4]. Therefore, aplausible explanation could be an inadequate nodal dissec-tion or inadequate pathological analysis [19,20].
SLN is commonly defined as first lymph node that receivesafferent lymphatic drainage from a primary tumour [5—11];therefore, this node is the first site of lymphatic involvementif metastasis has occurred. If this concept is correct, whenmetastasis is not found in a SLN, it most likely will not bepresent in themore distal nodes. As shown, for early stages inmalignant melanoma and breast cancer, the SLN allowedselective sensitive pathologic analysis to assess micrometas-tases [5,6]. In NSCLC a few studies identified SLN in >80% ofpatients, and found that the SLN status was predictive of thestatus of all other LNs in 80—100% of patients [7—9,21].However, standard detection methods have a low sensitivity.Better methods for detecting SLN involvement wouldimprove the ability to determine the risk of recurrence,which may affect patient treatment. The staining of serialsections of SLNs by IHC has been themost reported method ofidentifying micrometastases.
However, themolecular analysis of cytokeratin 7 and 19 byRT-PCR offers a sensitive tool for the detection of micro-metastasis [10—12]; this takes advantage of the developmentof a variety of probes for genes that may be over-expressed incertain tumours. For melanoma, this includes tyrosinase-related proteins (TRP-1, TRP-2), microphthalmia-associatedtranscription factor (MITF), MAGE-3, gp100, and MART-1; forbreast cancer, cytokeratin 19, 12 MUC-1, 13 mammaglobin B,
Table 2Upstaging
Micrometastases in SLN
PCR Stage IA (T1N0)� stage IIA (T1N1) 1 patientIHC Stage IB (T2N0)� stage IIB (T2N1) 2 patient
14 and MAGE-A3 15 have been identified as potentialmarkers, among others. Carcinoembryonic antigen (CEA)and MAGE-A are the most frequently used in colon cancer[22].
In lung cancer few studies exist in this field [16]. Wepreviously reported the positive results achieved in detectingSLN by IHC in early stage patients [9]. Our present protocolincludes the application of molecular analysis (RT-PCR forCK7-CK19) in addition to conventional methods (H&E/IHC).Moreover, radiotracer injection has been performed byvarious procedures (bronchoscopy, thoracotomy, CT-gui-dance or thoracoscopy) in order to avoid prolongedanaesthesia, and to obtain a tracer migration-time compa-tible with the course of the nodal dissection. Our preliminarydata found RT-PCR evidence of micrometastasis in 6 out of 10SLNs that could be evaluated. An interesting result was thepresence of cytokeratin 19 (CK19) as a marker of epithelialdifferentiation in one patient (#14) who was evaluated N0 byIHC, and who was upstaged from SI (T1N0) to SII (T1N1) onlyby molecular analysis. In this case the presence ofcytokeratin was accepted as evidence of micrometastasis.However, because the prognostic significance of molecularupstaging in NSCLC is not yet known, this patient wasconsidered as a stage IA, and thus no adjuvant chemotherapywas administered. On the other hand, although adjuvantchemotherapy is becoming the standard of care for mostNSCLC patients, and recent studies have demonstrated itsbenefits in early staging [23], the real advantage in lungcancer patients remains unclear. Intraoperative SLN map-ping, in this field could be useful for stratifying histologicallyN0 patients into higher risk groups.
Regarding the role of radical lymph-adenectomy in lungcancer stage I patients (especially those who have undergoneSLN mapping), it is still considered a critical point. Somerandomised trials (Izbicki and colleagues) showed no survivalbenefit [4]; others stressed the therapeutic value of radicalsystematic lymph-adenectomy [1,24,25].
Sentinel lymph node biopsy was initially developed as aminimally invasive surgical alternative to routine (elective)complete lymph-adenectomy. However, lymph-adenectomyfor staging and therapeutic benefit in lung cancer stillremains the gold standard for lung cancer staging. Further-more, trials such as ACOSOG Z0030l will likely define the bestprocedure in the near future. Taking all of this intoconsideration, we hypothesised that SLN mapping in lungcancer should be used to improve staging in patients withstage I disease. Therefore, in contrast to other solid tumours,in which this technique has been applied to minimise lymph-adenectomy, in lung cancer this method should be consideredas a new technique for stratifying N0 patients. This approachcould be a useful way to enable pathologists to identify withhigher sensitivity, micrometastasis. Despite the smallnumber of patients in our series, our preliminary data areencouraging and show a sensitivity up to 84.21%, which wassimilar to other studies [7—9] (the undetected SLNs in thepresent series (due to a technical error) explain the lowdetection rate compared to the higher detection rate (96%)found in our first study.) In any cases, it is noteworthy thatnone of the patients with N0 disease according to the RT-PCRanalysis developed recurrent disease by the time of lastfollow-up.

F.M.A. Melfi et al. / European Journal of Cardio-thoracic Surgery 34 (2008) 181—186186
In conclusion, the current study confirmed the feasibilityof SLN mapping in NSCLC, and demonstrated that SLNmolecular studies could improve greatly the detection ofmicro-metastases in patients with N0 disease. Thus, withincreased experience this technique may become a standardpractice in the management of early stage NSCLC. Just asmicrometastases are codified as N0 sub-stages in breast andcolon cancers (American Joint Committee on Cancer (AJCC)staging systems) [24], a similar sub-stage could be applied inlung cancer stage I patients.
However, the actual clinical impact of SLNmapping in lungcancer remains to be elucidated through further studies;moreover, molecular analysis needs to be performed largelyin research settings (since the prognostic significance ofpositive RT-PCR is still unclear). Nevertheless, in the nearfuture, this technique may be useful in selecting a subset ofNSCLC N0 patients who are most likely to be cured by surgeryalone, as well as those patients who aremore likely to benefitfrom adjuvant therapy.
References
[1] Graham ANJ, Chan KJ, Pastorino U, Goldstraw P. Systematic nodal dis-section in the intrathoracic staging of patients with non-small cell lungcancer. J Thorac Cardiovasc Surg 1999;117:246—51.
[2] Naruke T, Goya T, Tsuchiya R, Suemasu K. Prognosis and survival inresected lung cancer based on the new international staging system. JThorac Cardiovasc Surg 1988;96:440—7.
[3] Chen Z-L, Perez S, Holmes EC, Wang HJ, Coulson WF, Wen D-R. Frequencyand distribution of occult micrometastases in lymph nodes of patientswith non-small cell lung carcinoma. J Natl Cancer Ins 1993;85:4493—8.
[4] Izbicki JR, Passlick B, Hosch SB, Kuuschock B, Schneider C, Busch C. Modeof spread in the early phase of lymphatic metastases in non-small cell lungcancer: significance of nodal micrometastases. J Thorac Cardiovasc Surg1996;112:623—30.
[5] Morton DL, Duan-Ren W, Wong SG. Technical details of intraoperativelymphatic mapping for early stage melanoma. Arch Surg 1992;127:392—9.
[6] Giuliano AE, Kirgan DM, Guentha JM, Morton DL. Lymphatic mapping andsentinel lymphadenectomy for breast cancer. Ann Surg 1994;220:391—401.
[7] Liptay MJ, Grodin SC, Winchester DJ, Edelman BL, Garrido BJ, HirschtrittTR, Perlman RM, Fry WA. Intraoperative radioisotope sentinel lymph nodemapping in non-small cell lung cancer. Ann Thorac Surg 2000;70:384—9.
[8] Nomori H, Horio H, Naruke T, Orikasa H, Yamazaki K, Suemasu K. Use ofthecnetium-99 m tin colloid for sentinel lymph node identification inNSCLC. J Thorac Cardiovasc Surg 2002;124:486—92.
[9] Melfi FM, Chella A, Menconi GF, Givigliano F, Boni G, Mariani G, Sragia P,Angeletti CA. Intraoperative radioguided sentinel lymph node biopsy innon-small cell lung cancer. Eur J Cardiothorac Surg 2003;23:214—20.
[10] Blaheta HJ, Shittek B, Breuningen H. Detection of melanoma microme-tastasis in sentinel nodes by reverse transcription polymerase chainreaction correlates with tumor thickness and is predictive of micrometa-static disease in the lymph node basin. Am J Surg Pathol 1999;23:822—8.
[11] Deghuci T, Doi T, Ehara H, Ito S, Takahashi Y, Nishino Y, Kawamura T,Komeda H. Detection of micrometastatic prostate cancer cells in lymphnodes by reverse transcriptase polymerase chain reaction. Cancer Res1993;53:5320—54.
[12] Sanchez-Cespedes M, Esteller M, Hibi K, Cope FO, Westra WH, PiantadosiS, Herman JG, Jen J, Sidransky D. Molecular detection of neoplastic cellsin lymph nodes of metastatic colorectal cancer patients predicts recur-rence. Clin Cancer Res 1999;5:2450—4.
[13] Shariat SF, Roudier MP, Wilcox GE, Kattan MW, Scardino PT, Vessella RL,Erdamar S, Nguyen C, Wheeler TM, Slawin KM. Comparison of immuno-histochemistry with reverse transcription PCR for the detection of micro-metastatic prostate cancer in lymph nodes. Cancer Res 2003;63:4662—70.
[14] Blaheta HJ, Ellwanger U, Schittek B, Sotlar K, MacZey E, Breuninger H,Thelen MH, Bueltmann B, Rassner G, Garbe C. Examination of regionallymph nodes by sentinel node biopsy and molecular analysis provides newstaging facilities in primary cutaneous melanoma. J Invest Dermatol2000;114:637—42.
[15] Okegawa T, Nutahara K, Higashihara E. Detection of micrometastaticprostate cancer cells in the lymph nodes by reverse transcriptase poly-merase chain reaction is predictive of biochemical recurrence in patho-logical stage T2 prostate cancer. J Urol 2000;163(4):1183—8.
[16] Pulte D, Li E, Crawford BK, Newman E, Alexander A, Mustalish DC,Jacobson DR. Sentinel lymph node mapping and molecular staging inNSCLC. Cancer 2005;104:1453—61.
[17] Strauss GM, Kwiatkawski DJ, Harpole DH, Lynch TJ, Skarin AT, SugarbakerDJ. Molecular and pathologic markers in stage I non-small cell carcinomaof the lung. J Clin Oncol 1995;13(5):1265—79.
[18] Mountain CF. Revisions in International System for Staging Lung Cancer.Chest 1997;11:1710—7.
[19] Naruke T, Tsuchia R, Kondo H, Asamura H, Nakayama H. Implications ofstaging in lung cancer. Chest 1997;112:242S—8S.
[20] Naruke T, Tsuchia R, Kondo H, Asamura H. Prognosis and survival afterresection for bronchogenic carcinoma based on the 1997 TNM stagingclassification: the Japanese experience. Ann Thorac Surg 2001;71:1759—64.
[21] Keller SM, Adak S, Wagner H, Johnson DH. Mediastinal lymph nodedissection improves survival in patients with stages II and IIIa non-smallcell lung cancer. Eastern Cooperative Oncology Group. Ann Thorac Surg2000;70(2):358—65. Aug discussion 365—6.
[22] Greenson JK, Isenhart CE, Rice R, Mojzisik C, Houchens D, Martin Jr EW.Identification of occult micro metastases in pericolic lymph nodes ofDuke’s B colorectal cancer patients using monoclonal antibodies againstcytokeratin and CC49. Correlation with long-term survival. Cancer1994;73:563—9.
[23] Strauss GM, Herndon J, Maddaus MA. Randomized clinical trial of adju-vant chemotherapy with paclitaxel and carboplatin following resection instage IB NSCLC: report of Cancer and Leukemia Group B (CALGB) Protocol9633 [abstract]. J Clin Oncol 2004;22(14S):A7019.
[24] Izbicki JR, Passlick B, Pantel K, Pichlmeiner U, Hosch SB, Karg O, ThetterO. Effectiveness of radical systematic mediastinal lymphadenectomy inpatients with resectable non-small cell lung cancer: results of a pro-spective randomized trial. Ann Surg 1998;227:138—44.
[25] Martini N, Flehinger BJ, Zaman MB, Beattie Jr EJ. Results of resection innon-oat cell carcinoma of the lung with mediastinal lymph node metas-tases. Ann Surg 1983;198:386—97.
Appendix A. Conference discussion
Dr F. Venuta (Rome, Italy): What is the minimum time you need betweenthe injection and the intraoperative control?
Dr Melfi: The injection is just before the operation. So the most we canwait is 1 h before detecting sentinel nodes.