Interleukin1-producing plasma cells in close contact with hepatocytes in patients with chronic...
12
Journal of Hepatology 1991; 21: 6-11 Printed in Denmark ~ 411 rights reserved Munksgaard Copenhagen Journal of Hepatology ISSN 0168-X278 Interleukin-l-producing plasma cells in close contact with hepatocytes in patients with chronic active hepatitis Giorgio Hassan ‘, Sandra Moreno2, Mara Massimi2, Paola Di Biagio’ and Stefania Stefanini2 ‘Centro Studi Malattie de1 Fegato, Ospedale S. ,Giacomo, ‘Dipartimento di Biologia Cellularr r dello Sviluppo, Universitd di Rorna “Lu Sapienza “, Rome, Ital\. BackgvoundAims: In chronic active liver diseases (CALD) with viral aetiology, a population of plasma cells localised in the piecemeal necrosis areas was pre- viously detected by means of autoradiography after in vitro3H-proline incorporation, a method which proved much more sensitive than conventional immunohisto- chemical procedures. These plasma cells, character- istically located in niches among hepatocytes, in close contact with collagen fibrils, have been hypothesised to exert a role in fibrogenesis stimulation, and particu- larly in collagen synthesis, possibly through secretion of lymphokines. Specifically, we investigated the pres- ence of interleukin-1, well known to play a crucial role in inflammation and production of collagen by epithelial cells, and to be present in activated plasma cells of myeloma. Met/z&: The immunohistochemical localisatiou of interleukin-l/? in biopsies of patients suffering from chronic active hepatitis was studied, using an affinity- purified rabbit polyclonal antibody. F IBROSIS is a common feature of chronic active liver diseases (CALD) (1,2). In chemically induced hepatitis, perisinusoidal (Ito) cells have been demonstrated to be responsible for col- lagen synthesis (3-10) and a schematic model for the progression of this disease has been formulated (for review, see 11). According to this model, chemically in- jured hepatocytes release factors that attract Kupffer cells and additional mononuclear phagocytes recruited from blood and bone marrow precursors; once local- ised in the liver, the macrophages become activated by Received 25 July 1996: revised 7 Januur)-; accepted I8 Fehrwry 1997 Correspondence: Dr. Stefania Stefanini, Dipartimento di Biologia Cellulare e dello Sviluppo, Universita di Roma “La Sapienza”, Piazzale Aldo Moro, 5, 00185 Rome, Italy. Tel: 0039-6-49912878. Fax: 0039-6-49912351. Results: The strongest interleukin-l/i immunostaining was observed in the above-described plasma cell popu- lation, identified by anti-immunoglobulin antibodies, and 3H-proline incorporation. Conclusions: The ability of plasma cells to produce interleukin-1 during viral CALD suggests that in these pathologies plasma cells play a major role, mainly of paracrine nature. Interleukiu-1, possibly to- gether with other mediators, might in turn stimulate the production of collagen. Hepatocytes of the piece- meal necrosis area appear to be possible candidates for this synthesis, as they show a significant labelling after 3H-proline incorporation, which is absent from hepatocytes far from necrotic areas. Key words: B cell; Cytokine; Fibrosis; Immunohisto- chemistry; Ultrastructure. hepatocyte-derived factors, or directly by fibrogenic agents (for example, carbon tetrachloride or excess vit- amin A), and release cytokines such as interleukin-1 (IL-l), which induce proliferation and activation of en- dothelial cells. Cytokines, together with other me- diators (e.g. oxygen radicals, basic fibroblast growth factor), besides acting on damaged hepatocytes leading to their death, are supposed to affect principally fat- storing cells, which proliferate, differentiate into myo- fibroblasts and actively produce extracellular proteins. In contrast to chemically induced hepatitis. in chronic active liver diseases (CALD) with either auto- immune or viral aetiology, the cell type responsible for fibrous collagen synthesis has not been positively iden- tified. Moreover, the data concerning cytokine profile alterations during the progression of CALD (12--l 7), although demonstrating their involvement in these 6
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Interleukin1-producing plasma cells in close contact with hepatocytes in patients with chronic...
Journal of Hepatology 1991; 21: 6-11 Printed in Denmark ~ 411 rights reserved Munksgaard Copenhagen Journal of Hepatology
ISSN 0168-X278
Interleukin-l-producing plasma cells in close contact with hepatocytes in patients with chronic active hepatitis
Giorgio Hassan ‘, Sandra Moreno2, Mara Massimi2, Paola Di Biagio’ and Stefania Stefanini2
‘Centro Studi Malattie de1 Fegato, Ospedale S. ,Giacomo, ‘Dipartimento di Biologia Cellularr r dello Sviluppo, Universitd di Rorna “Lu Sapienza “,
Rome, Ital\.
BackgvoundAims: In chronic active liver diseases (CALD) with viral aetiology, a population of plasma cells localised in the piecemeal necrosis areas was pre- viously detected by means of autoradiography after in vitro3H-proline incorporation, a method which proved much more sensitive than conventional immunohisto- chemical procedures. These plasma cells, character- istically located in niches among hepatocytes, in close contact with collagen fibrils, have been hypothesised to exert a role in fibrogenesis stimulation, and particu- larly in collagen synthesis, possibly through secretion of lymphokines. Specifically, we investigated the pres- ence of interleukin-1, well known to play a crucial role in inflammation and production of collagen by epithelial cells, and to be present in activated plasma cells of myeloma. Met/z&: The immunohistochemical localisatiou of interleukin-l/? in biopsies of patients suffering from chronic active hepatitis was studied, using an affinity- purified rabbit polyclonal antibody.
F IBROSIS is a common feature of chronic active liver diseases (CALD) (1,2).
In chemically induced hepatitis, perisinusoidal (Ito) cells have been demonstrated to be responsible for col- lagen synthesis (3-10) and a schematic model for the progression of this disease has been formulated (for review, see 11). According to this model, chemically in- jured hepatocytes release factors that attract Kupffer cells and additional mononuclear phagocytes recruited from blood and bone marrow precursors; once local- ised in the liver, the macrophages become activated by
Received 25 July 1996: revised 7 Januur)-; accepted I8 Fehrwry 1997
Correspondence: Dr. Stefania Stefanini, Dipartimento di Biologia Cellulare e dello Sviluppo, Universita di Roma “La Sapienza”, Piazzale Aldo Moro, 5, 00185 Rome, Italy. Tel: 0039-6-49912878. Fax: 0039-6-49912351.
Results: The strongest interleukin-l/i immunostaining was observed in the above-described plasma cell popu- lation, identified by anti-immunoglobulin antibodies, and 3H-proline incorporation. Conclusions: The ability of plasma cells to produce interleukin-1 during viral CALD suggests that in these pathologies plasma cells play a major role, mainly of paracrine nature. Interleukiu-1, possibly to- gether with other mediators, might in turn stimulate the production of collagen. Hepatocytes of the piece- meal necrosis area appear to be possible candidates for this synthesis, as they show a significant labelling after 3H-proline incorporation, which is absent from hepatocytes far from necrotic areas.
Key words: B cell; Cytokine; Fibrosis; Immunohisto- chemistry; Ultrastructure.
hepatocyte-derived factors, or directly by fibrogenic agents (for example, carbon tetrachloride or excess vit- amin A), and release cytokines such as interleukin-1 (IL-l), which induce proliferation and activation of en- dothelial cells. Cytokines, together with other me- diators (e.g. oxygen radicals, basic fibroblast growth factor), besides acting on damaged hepatocytes leading to their death, are supposed to affect principally fat- storing cells, which proliferate, differentiate into myo- fibroblasts and actively produce extracellular proteins.
In contrast to chemically induced hepatitis. in chronic active liver diseases (CALD) with either auto- immune or viral aetiology, the cell type responsible for fibrous collagen synthesis has not been positively iden- tified. Moreover, the data concerning cytokine profile alterations during the progression of CALD (12--l 7), although demonstrating their involvement in these
6
IL-l-producing plasma cells in CAH
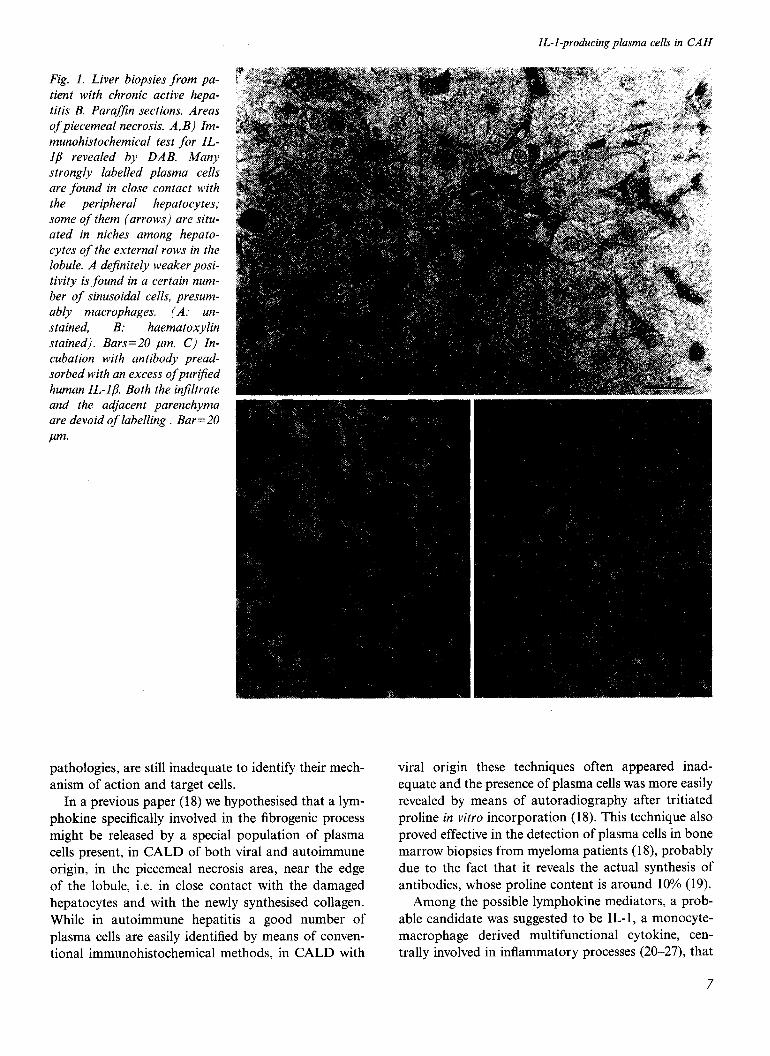
Fig. 1. Liver biopsies from pa- tient with chronic active hepa- titis B. Parafjn sections. Areas of piecemeal necrosis. A,B) Im- munohistochemical test for IL- Ip revealed by DAB. Many strongly labelled plasma cells are found in close contact with the peripheral hepatocytes; some of them (arrows) are situ- ated in niches among hepato- cytes of the external rows in the lobule. A dejinitely weaker posi- tivity is found in a certain num- ber of sinusoidal cells, presum- ably macrophages. (A: un-
stained, B. haematoxylin stained). Bars=20 pm. C) In- cubation with antibody pread- sorbed with an excess of purt$ed human IL-l/X Both the in$ltrate and the adjacent parenchyma are devoid of labelling . Bar=20
pm.
pathologies, are still inadequate to identify their mech- anism of action and target cells.
In a previous paper (18) we hypothesised that a lym- phokine specifically involved in the fibrogenic process might be released by a special population of plasma cells present, in CALD of both viral and autoimmune origin, in the piecemeal necrosis area, near the edge of the lobule, i.e. in close contact with the damaged hepatocytes and with the newly synthesised collagen. While in autoimmune hepatitis a good number of plasma cells are easily identified by means of conven- tional immunohistochemical methods, in CALD with
viral origin these techniques often appeared inad- equate and the presence of plasma cells was more easily revealed by means of autoradiography after tritiated proline in vitro incorporation (18). This technique also proved effective in the detection of plasma cells in bone marrow biopsies from myeloma patients (18), probably due to the fact that it reveals the actual synthesis of antibodies, whose proline content is around 10% (19).
Among the possible lymphokine mediators, a prob- able candidate was suggested to be IL-l, a monocyte- macrophage derived multifunctional cytokine, cen- trally involved in inflammatory processes (20-27), that
7

G. Hussan et al.
has been found to be produced by activated plasma
cells in myeloma (28). When human liver diseases are
considered, in vitro studies showed that IL-l is released
by primary-cultured hepatic macrophages from pa-
tients with cirrhosis (17) while in situ detectable
amounts of this cytokine have been reported only in
bile duct epithelial cells, and to a lesser extent, in
Kupffer cells and hepatocytes, of patients with al-
coholic hepatitis (29).
In order to investigate the role/s played by IL-1 in
regulating fibrogenesis in viral CALD, we chose to in-
vestigate the distribution of this cytokine in situ, i.e. on
liver biopsies from patients affected by chronic active
hepatitis or active cirrhosis with viral aetiology and,
for comparison, acute hepatitis, rather than in pa-
tients’ sera or in cultured purified cell populations.
Only in situ studies, in fact, can give insight into cell-
cell and cell-environment interactions, which might be
different depending on the various areas of inflam-
mation and fibrosis (30). Moreover, this approach
could reveal, for example, different cell types as well as
different modalities possibly involved in the collagen
synthesis during CALD progression.
In this study, immunolocalisation of IL-l was per-
formed using a polyclonal, affinity-purified rabbit anti-
body to human IL-lb. Plasma cells were unequivocally
identified by means of both the widely used immuno-
cytochemical method employing antibodies to im-
Fig. 2. Liver biopq~,fiom patient u,ith chronic active hepatitis B. Area of‘ piecemeal necrosis. Bars=20 pm. A) Paraj$n sec- tion incubated with anti-Ig light drains. The plasrnc~ cells are dis- tributed at the boundary bc- tu’een i~flrnnmutor~-! il?Jjltrate tmd liver lobule. Bl Contiguous .section inc~ubrrtrd IlYth mti-IL- l/l. Positive cells sliol~’ N distri- bution quite siniilw to that
.fi~Ld ,fi)l the Ig-contuining wlls. A \\,eah-er. staining can be seen on .smw .sinLr.soirk~irl cells.

IL-l-producing plasma cells in CAH
Fig. 3. Liver biopsy from patient with chronic active hepatitis B, incubated with 3H-proline. Area of piecemeal necrosis. Bars= 100 pm. A) ParafJin section submitted to autoradiography and developed after 7-day-ex- posure. The plasma cells are strongly labelled; a weaker but signiJicant positivity can be seen on the peripheral hepatocytes and on the biliary duct (arrow). B) Contiguous section incu- bated with anti-IL-l/?. The posi- tive cells, present at the bound- ary between inflammatory injil- trate and liver lobule, show a closely similar distribution to JH-proline positive plasma cells.
munoglobulin light chains and by autoradiography after 3H-proline incorporation, previously proved to be highly sensitive in detecting plasma cells (18).
As a further positive control, bone marrow biopsies from patients with myeloma, whose plasma cells have been reported to contain IL-l (28), were submitted to the same methods.
Materials and Methods Patients and serological tests
For the present investigation we examined liver biop- sies from 23 patients affected with chronic active hepa- titis (18 with hepatitis B, and five with hepatitis C) and from four patients affected with acute viral hepatitis
(two with hepatitis B, and two with hepatitis C). Pa- tients were of either sex, aged between 20 and 58 years, and were classified on the basis of histological examin- ation of their liver biopsies and serological tests, per- formed by commercial immunoassay techniques (Ab- bott Laboratories, North Chicago, IL, USA), as fol- lows: of the 18 chronic hepatitis B, two were HBsAg positive, HBeAg positive; three HBsAg positive, HBeAg negative, anti-HBe positive, anti-HBc positive; 13 HBsAg negative, HBeAg negative, anti-HBs nega- tive, anti-HBe positive, anti-HBc positive. The five pa- tients with chronic hepatitis C were all HCV-RNA positive. Of the four patients with acute hepatitis, two were HBV-DNA positive, and two were HCV-RNA positive.
9

G. Hassan et al.
We also examined three bone marrow biopsies: two were from patients affected with IC myeloma and one from a patient with cirrhosis and monoclonal hyper- gammaglobulinaemia, but not myeloma.
All patients gave informed consent; study protocols were approved by the Italian Ethical Committee of Hu- man Experimentation and conformed to the ethical guidelines of the 1975 Declaration of Helsinki.
Incorporation studies
Liver bioptic or bone marrow bioptic specimens were suspended in 2 ml of Hank’s Balanced Salt Solution (HBSS) supplemented with 50 mM HEPES and 12 mM glucose, pH 7.4. 100 ,nCi per ml (final concen- tration) of L-(2,3,4,5-[3]H)-proline (specific activity: 126 Ci per mmol; New England Nuclear, Boston, MA, USA) was added and the specimens were incubated at 37°C for 1 h, under continuous bubbling with oxygen. After incubation, the tissue samples were extensively rinsed with HBSS.
Tissue processing Some tissue blocks were fixed in Bouin’s solution, em- bedded in paraffin and cut into sections 10 ,um thick.
Other blocks were fixed by immersion in 2.5% glutaraldehyde in 0.1 M cacodylate buffer, pH 7.5, containing 5% sucrose, at 4°C for 1 h, rinsed three times in the same buffer and postfixed in 1% osmium tetroxide in the same buffer at 4°C for 1 h. After dehy-
dration in ethanol, specimens were embedded in Epon 812 and cut on an Ultrotome III LKB.
Ultrastructural morphology
Ultrathin sections were contrasted with uranyl acetate and lead citrate, and observed in a Philips 400T elec- tron microscope.
AutoradiographJ
Paraffin sections and semi-thin sections from Epon- embedded specimens were processed for autoradiogra- phy according to Boyd (31). using Ilford L4 emulsion. Paraffin sections were developed after 7-15 days of ex- posure in a dark-room and routinely stained with haematoxylin and eosin; semi-thin sections were de- veloped after 20-30 days and stained with toluidine blue.
Ultrathin sections were processed for autoradiogra- phy according to Moses (32), as described by Bos- man & Feldman (33). and were developed after 40-90 days of exposure.
Iinmzmohistoclzemistrl, Immunohistochemical procedures were carried out on paraffin sections contiguous to those analysed by auto- radiography.
The presence and localisation of IL-1 were analysed by means of a polyclonal. affinity-purified rabbit anti- human IL-lp antibody (Collaborative Biomedical
Fig. 4 A,B. Liver biopsy from put&t with chronic uctive heptr- titis B, incubated with -‘H-pro- line. Electron microscopic uuto- radiogruphs developed afier 90 days. Silver grtrirls are restricted to the rough endoplasmic retic- ulum of’ the two plusrr~a cells. Large aiwoui~ts of‘ collagen ji- hrils (asterisks) are present in close contact to plasma cel1.r. Bars=2 ,wn.

IL-l-producing plasma cells in CAH
Fig. 5. Liver biopsies from pa- tients with chronic active hepa- titis B. Paraf$n sections incu- bated with anti-human CD68. A) The positivity is localised on a certain number of sinusoidal macrophages and on some mononuclear cells (monocytes), scattered in the inflammatory infiltrate. Bar=50 pm. B) Higher magntfication showing the immunoreactive monocytes randomly distributed in the in- flammatory infiltrate. Bar=50
pm.
Products, Bedford, USA), diluted 1500 in PBS con- taining 0.1% BSA, with incubation for either 30 min at room temperature, or overnight at 4°C.
Control sections were either incubated with normal rabbit serum (Vector Laboratories, Burlingame, CA, USA), diluted l:lOO, or with PBS alone. In some sec- tions, contiguous to those immunoreacted with anti- human IL- lp antibody, anti-human IL- lp diluted 1:500 and preadsorbed (60 min at room temperature) with an excess (150) of purified human IL-l/I (Boehringer, Mannheim, Germany) was used as control.
The presence of immunoglobulin light chains was as-
sessed by immunoreaction with a 1:l mixture of poly- clonal, affinity-purified rabbit anti-human immuno- globulin kappa and anti-human immunoglobulin lambda light chain antibodies (Dako, Glostrup, Denmark), with a final dilution of each antibody at 1:20000 in the above medium, with incubation for 30 min at room temperature.
The above immunoreactions were revealed by the avi- din-biotin-peroxidase complex method (ABC Elite Vect- astain, Vector Laboratories, Burlingame, CA, USA).
Some sections were incubated with a monoclonal mouse anti-human CD68, clone KPl (Dako, Glostrup,
11

G. H~rssan et al.
Fig. 6. Liver biopsyfrompatient with chronic active hepatitis B. Ultrathin section. Area of piecemeal necrosis, showing many plasma cells (arrows), located in niches formed b_v the hepatoc_vtes. Perisinusoidal cells show normal morphological features, with no sign qf activation. Bar=5 pm.
Denmark), diluted 1:50 in PBS containing 0.1% BSA, for 60 min at room temperature. The immunoreaction
was revealed by the alkaline phosphatase method (Supersensitive Multilink Alk Phos, Bio Genex, San Ra- mon, CA, USA), using new fucsin (Bio Genex) as chromogen.
Finally, sections from biopsies of patients classified as hepatitis B on the basis of serological tests were in- cubated with anti-HBs rabbit polyclonal antibody (Dako, Milan, Italy), diluted 1: 1000, or with anti-HBc rabbit polyclonal antibody (Dako). diluted 1:500; the immunoreaction was revealed by the peroxidase method (LSAB, Dako).
All the immunoreacted sections were examined un- stained, or mildly counterstained with haematoxylin.
Results Liver biopsies jiom patients with chronic active
hepatitis B and C
In sections incubated for the immunolocalisation of IL- lb a specific and intense positivity was found on cells morphologically identifiable as plasma cells, character- istically localised at the lobular edges, in the area of piecemeal necrosis (Fig. 1 A.B): concerning the speci- ficity of IL-1 immunolocalisation, a slight background was found in control sections treated with normal rabbit serum, while no staining at all was found after incuba- tion with PBS alone or with anti-IL-l/I antibody pre- viously adsorbed with an excess of IL- l/J (Fig. 1 C).
In sections contiguous to those submitted to the im- munocytochemical detection of IL- 1. plasma cells were
Fig. 7. Liver biopqJ,from patient with chronic active hepatitis B. Ultrathin section showing a
plasma cell [viny in a niche
among peripheral hepatoq~tes.
Along the ,rhole extent of’ con- tact IzGth the plasma cell, the I1epatoq.te.s show 0 smooth sur-
,face; arro~vs point to numerol4s
rollagen,fibrils that arcJ.fountr’ in
tight contact between plrsmu
cells and hepatocvte surfaces.
Bar= I pm. _
IL-l-producing plasma cells in CAH
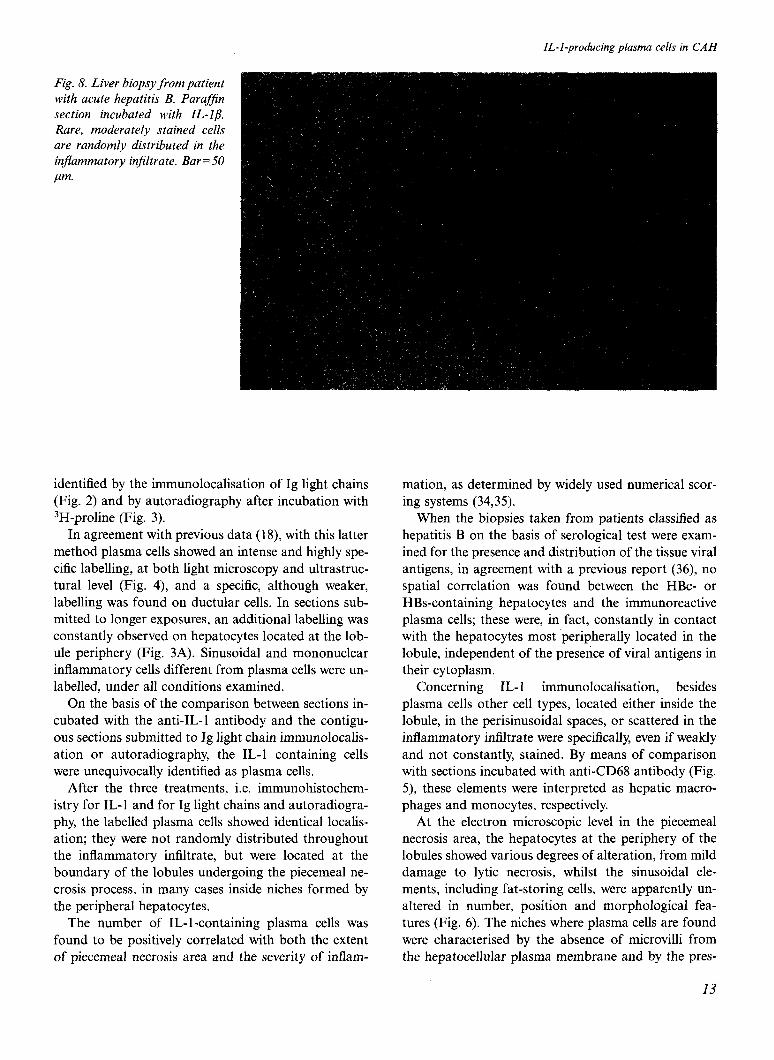
Fig. 8. Liver biopsy from patient with acute hepatitis B. ParafJin section incubated with IL-ID. Rare, moderately stained cells are randomly distributed in the inflammatory injiltrate. Bar=50
lum.
identified by the immunolocalisation of Ig light chains (Fig. 2) and by autoradiography after incubation with 3H-proline (Fig. 3).
In agreement with previous data (18), with this latter method plasma cells showed an intense and highly spe- cific labelling, at both light microscopy and ultrastruc- tural level (Fig. 4), and a specific, although weaker, labelling was found on ductular cells. In sections sub- mitted to longer exposures, an additional labelling was constantly observed on hepatocytes located at the lob- ule periphery (Fig. 3A). Sinusoidal and mononuclear inflammatory cells different from plasma cells were un- labelled, under all conditions examined.
On the basis of the comparison between sections in- cubated with the anti-IL-l antibody and the contigu- ous sections submitted to Ig light chain immunolocalis- ation or autoradiography, the IL-l containing cells were unequivocally identified as plasma cells.
After the three treatments, i.e. immunohistochem- istry for IL-l and for Ig light chains and autoradiogra- phy, the labelled plasma cells showed identical localis- ation; they were not randomly distributed throughout the inflammatory infiltrate, but were located at the boundary of the lobules undergoing the piecemeal ne- crosis process, in many cases inside niches formed by the peripheral hepatocytes.
The number of IL-l-containing plasma cells was found to be positively correlated with both the extent of piecemeal necrosis area and the severity of inflam-
mation, as determined by widely used numerical scor- ing systems (34,359.
When the biopsies taken from patients classified as hepatitis B on the basis of serological test were exam- ined for the presence and distribution of the tissue viral antigens, in agreement with a previous report (36), no spatial correlation was found between the HBc- or HBs-containing hepatocytes and the immunoreactive plasma cells; these were, in fact, constantly in contact with the hepatocytes most peripherally located in the lobule, independent of the presence of viral antigens in their cytoplasm.
Concerning IL- 1 immunolocalisation, besides plasma cells other cell types, located either inside the lobule, in the perisinusoidal spaces, or scattered in the inflammatory infiltrate were specifically, even if weakly and not constantly, stained. By means of comparison with sections incubated with anti-CD68 antibody (Fig. 5) these elements were interpreted as hepatic macro- phages and monocytes, respectively.
At the electron microscopic level in the piecemeal necrosis area, the hepatocytes at the periphery of the lobules showed various degrees of alteration, from mild damage to lytic necrosis, whilst the sinusoidal ele- ments, including fat-storing cells, were apparently un- altered in number, position and morphological fea- tures (Fig. 6). The niches where plasma cells are found were characterised by the absence of microvilli from the hepatocellular plasma membrane and by the pres-
13

G. Hassan et al.
ence of collagen fibrils in the space between plasma cells and hepatocytes (Fig. 6 and 7).
Liver biopsies from patients with acute hepatitis
At both light and electron microscopic level, hepato- cytes and sinusoidal cells showed the morphological features typical for this pathology. The immunocytoch- emistry with anti-kappa and anti-lambda immuno- globulin light chain antibodies showed only a few plasma cells, randomly distributed in the inflammatory infiltrate. Incubation with anti-IL- 1 antibody, carried out under the same experimental conditions applied to biopsies from patients with chronic active hepatitis, showed a faint but specific staining on a few mono- nuclear cells, presumably monocytes, scattered in the inflammatory infiltrate (Fig. 8).
Bone marrow biopsies
In biopsies from patients with k myeloma, the numer- ous Ig-containing plasma cells were found to incorpor-
ate proline with a label intensity closely comparable with that seen under the same experimental conditions by plasma cells of CALD. The comparison of consecu- tive sections showed that a fraction of the IgG-produc- ing cells were also IL-1 immunoreactive; traces of IL-l immunostaining were found in other bone marrow cells (Fig. 9A, B, C).
In the normal bone marrow, in contrast, after IL- 1 immunolocalisation, no specific immunostaining was found on plasma cells (Fig. 9D).
Discussion The liver biopsies that we examined from patients with chronic hepatitis B and C showed a conspicuous num- ber of plasma cells. This result is in agreement with our previous data (1 S), but in disagreement with other studies concerning CALD with viral aetiology, in which plasma cells were described as scanty in the in- flammatory infiltrate and their role in the progression of disease received very little attention (3641).
Fig. 9. A,B, C) Bone marrow hiopsies,from patient with h- my- elomu. Bars=20 ,um. A) Purclf- fin section incubated with unti-Ig light chains. Plusmm cells shoM. u strong immwzoreu~tivit~. B) Contiguous section processed,jiw IL-I/3 iir~mztnolo~ali,scition. Im- munorcuctiw plusmu cells ure evident, although smuller in number u,itli respect to Ig-posi- tive cells; a weuker label is ulso detected on mononuclear ele- ments. C) Purqffin section sub- mitted to uutorudioradiogruphy qfter in vitro proline incorpor- ution und developed ufter 7 days. Plusmu cells .show N high degree of luhelling. D) Normut bone murrobt’ biopsy. Puruj$n section processed for IL-lg immunoio- culisution. A +tleuk lube1 is onl? .found on monocytes and pol.v- morphonucleur elements; the,fiw identifiable plusmu cells ure practically unlubelled. Bur = 20
,W?l.

An intense IL-l immunostaining was found on nu- merous plasma cells, identified by both Ig light chain immunocytochemistry and autoradiography; because of proline incorporation into newly synthesised anti- bodies, this latter method was found to be especially effective in revealing plasma cells in liver of CALD pa- tients, as well as in myelomatous bone marrow (18). Other cells already known to produce IL- 1, as mono- cytes and macrophages, show a weaker and inconstant staining, but in any case their distribution is quite dif- ferent from that of plasma cells (as shown by the CD68 immunocytochemistry).
The ability of B elements (4247) and, more specifi- cally, of plasma cells (28) to release IL-l has been re- ported earlier. At the same time, IL-l immunoreactiv- ity found in plasma cells of myeloma, previously dem- onstrated to contain this cytokine (28), strengthens the immunohistochemical data obtained in CALD.
In contrast to liver biopsies of patients with acute hepatitis, where plasma cells are scanty and scattered in the inflammatory infiltrate, in biopsies from viral CALD the IL-l-positive plasma cells are conspicuous in number and preferentially localised at the boundary of the lobules, in niches situated among the hepato- cytes directly involved in piecemeal necrosis; this par- ticular contact is highly suggestive of a paracrine and/ or autocrine role, rather than a humoral role.
Our immunohistochemical data suggest that in chronic active hepatitis with viral aetiology, plasma cells can produce both immunoglobulins (41) and IL- 1, the latter probably acting in a paracrine manner.
This supposed paracrine action seems not to affect fat-storing cells. Indeed in our specimens these cells showed unchanged morphological features and failed to incorporate 3H-proline, in contrast to the myo- fibroblastoid features and 3H-proline incorporation that they showed in CC4induced experimental fi- brosis, even when comparable rates and times of incor- poration and exposure were employed (9).
A weaker but specific proline incorporation was found in the hepatocytes located at the lobule periph- ery, in close proximity with the IL-l-producing plasma cells; collagen fibrils were also constantly seen in exact- ly this contact area.
Proline is known to be incorporated into neosyn- thesised collagen and hepatocytes were reported to ex- press specific receptors and to respond specifically to this cytokine (48-53). Furthermore, they were reported to synthesise collagen in fibrotic liver, in rat experimen- tal cirrhosis (54,55), as well as in alcoholic human liver
(56). On the basis of our data, the following hypothesis
can be tentatively formulated: at least in the early
IL-l-producing plasma cells in CAH
phases of progressive collagen deposition, in CALD, plasma cell-derived IL-l may induce the adjacent hepatocytes to synthesise collagen, thus forming the fibrils found at the boundary between the lobules and the inflammatory infiltrate (57,58).
Later, during the progression of disease, changes in the physicochemical properties and in the distribution of collagen types are encountered (59,60) and different pathways of synthesis and/or deposition may occur, the histological appearance of dense, paucicellular fibrosis (61,62) being, for example, possibly due to typical fibroblasts, which are constantly found, in CALD- affected patients, in portal spaces far from the piece- meal necrosis areas (18).
Finally, the role hypothesised above of plasma cell- derived IL-l in inducing collagen synthesis by adjacent hepatocytes does not disagree with data suggesting that the same cytokine, produced by macrophages scat- tered in the lobule, stimulates the collagen deposition found in virtually all the perisinusoidal spaces.
Further investigation is needed to clarify whether, during the progression of chronic liver diseases, IL-l can act as a fibrogenic factor on different cell targets, possibly located in different lobular zones.
References 1. Rojkind M. Fibrogenesis in cirrhosis. Potential for thera-
peutic intervention. Pharmacol Ther 1992; 53: 81-104. 2. Andus T, Bauer J. Gerok W. Effects of cytokines on the liver.
Hepatology 1991; 13: 36475. 3. McGee JO’D, Patrick R. The role of perisinusoidal cells in
hepatic fibrogenesis. Lab Invest 1972; 26: 42940. 4. Kent G, Gay S, Inouye T, Bahu R, Minick OT, Popper H.
Vitamin A-containing lipocytes and formation of type III collagen in liver injury. Proc Nat1 Acad Sci USA 1976; 73: 3719-22.
5. Ballardini G, Degli Esposti S, Bianchi FB, Badiali De Giorgi L, Faccani A, Biolchini L, et al. Correlation between Ito cells and fibrogenesis in an experimental model of hepatic fibrosis. A sequential stereological study. Liver 1983; 3: 58-63.
6. Mak K, Leo MA, Lieber CS. Alcoholic liver injury in ba- boons: transformation of lipocytes to transitional cells. Gas- troenterology 1984; 87: 188-200.
7. Callea F, Desmet VJ. Transformation of fat storing cells (Ito cells) to myofibroblasts. J Hepatol 1985; 2: S206.
8. Tanikawa K, Ueno T. Fine structural features and roles of fat-storing cells and basement membrane in hepatic fibrosis. In: Hirayama C, Kivirikko KI, eds. Pathobiology of Hepatic Fibrosis. Amsterdam: Excerpta Medica, 1985; 3-l 1.
9. Enzan H, Hara II. Ito cells (fat storing cells) and collagen
10.
formation in carbon tetrachloride-induced liver fibrosis. A light and electron microscopic autoradiographic study using 3H-proline as a tracer. In: Kirn A, Knook DL, Wisse E, eds. Cells of the Hepatic Sinusoid. Vol I. Rijswijk: The Kupffer Cell Foundation, 1986; 233-8. Milani S, Herbst H, Schuppan D, Hahn EG, Stain H. In situ hybridization for procollagen types I, III and IV mRNA in normal and fibrotic rat liver: evidence for predominant ex-
I.5

G. Hassan et ul.
pression in nonparenchymal liver cells. Hepatology 1989; 10: 84-92.
1 I, Laskin DL. Nonparenchymal cells and hepatotoxicity. Semin Liver Dis 1990; 10: 293-304.
12. Alexander GJ. Nom-i-Aria KT. Neuberger J, Bakhtiar M, Vo- gel W. Anderson MG, et al. In vitro effects of lymphoblastoid interferon on lymphocyte activation and cell-mediated cy- tolysis in patients with chronic hepatitis B virus infection. J Hepatol 1986; 3 (suppl 2): S269977.
13. Anastassakos Ch, Alexander GJM. Wolstencroft RA, Avery JA, Portmann BC, Panayi GS, et al. lnterleukin I
1 activity
16

IL-I-producing plasma cells in CAH
fects, and biochemical properties. Cell Immunol 1985; 94: 41 S-26.
45. Pistoia V, Cozzolino F, Rubartelli A, Torcia M, Roncella S, Ferrarini M. In vitro production of interleukin 1 by normal and malignant human B lymphocytes. J Immunol 1986; 136: 1688-92.
46. Bersani L, Colotta F, Peri G, Mantovani A. Cytotoxic effector function of B lymphoblasts. J Immunol 1987; 139: 645-8.
47. Scala G, Morrone G, Tamburrini M, Alfinito F, Pastore CI, D’Alessio G, et al. Autocrine growth function of human in- terleukin 1 molecules on ROHA-9, an EBV-transformed hu- man B cell line. J Immunol 1987; 138: 2527-34.
48. Rupp RG, Fuller GM. The effects of leucocytic and serum factors on fibrinogen biosynthesis in cultured hepatocytes. Exp Cell Res 1978; 118: 23-30.
49. Sztein MB, Vogel SN, Sipe JD, Murphy PA, Mizel SB, Op- penheim JJ, et al. The role of macrophages in the acute-phase response: SAA inducer is closely related to lymphocyte activ- ating factor and endogenous pyrogen. Cell Immunol 1981; 63: 164-76.
50. Le PT, Mortensen RF Induction and regulation by mono- kines of hepatic synthesis of the mouse serum amyloid P- component (SAP). J Immunol 1986; 136: 252&33.
51. Sipe JD, Vogel SN, Douches S, Neta R. Tumor necrosis fac- tor/cachectin is a less potent inducer of serum amyloid A synthesis than interleukin 1. Lymphokine Res 1987; 6: 93- 101.
52. Hagiwara T, Suzuki H, Kono I, Kashiwagi H, Akiyama Y, Onozaki K. Regulation of fibronectin synthesis by interleu- kin-l and interleukin-6 in rat hepatocytes. Am J Path01 1990; 136: 3947.
53. Kohira T, Matsumoto K, Ichihara A, Nakamura T. Identifi- cation of a biologically functional novel IL-l&specific recep- tor on adult rat hepatocytes. J Biochem 1993; 114: 658-62.
54. Martinez-Hernandez A. The hepatic extracellular matrix. II. Electron immunohistochemical studies in rats with CC14-in- duced cirrhosis. Lab Invest 1985; 53: 16686.
55. Chojkier M, Lyche KD, Filip M. Increased production of collagen in vivo by hepatocytes and nonparenchymal cells in rats with carbon tetrachloride-induced hepatic fibrosis. Hepatology 1988; 8: 808-14.
56. Clement B, Grimalds JA, Campion JP Deugnier Y, Guillou- zo A. Cell types involved in collagen and fibronectin produc- tion in normal and fibrotic human liver. Hepatology 1986; 6: 225-34.
57. Cenacchi G, Ballardini G, Badiali De Giorgi L, Busachi CA, Del Rosso M, Bianchi FB, et al. Relationship between con- nective tissue cells and fibronectin in a sequential model of experimental hepatic fibrosis. Virchows Arch B Cell Path01 1983; 43: 75-84.
58. De Groote J, Desmet VJ, Gedigk P Korb G, Popper H, Poulsen H, et al. A classification of chronic hepatitis. Lancet 1968; ii: 6268.
59. Voss B, Rauterberg J, Allam S, Pott G. Distribution of colla- gen type I and type III and of collagenous components of basement membrane in the human liver. Path01 Res Pratt 1980; 170: 50-60.
60. Murata K, Kudo M, Onuma F, Motoyama T. Changes of collagen types at various stages of human liver cirrhosis. Hepatogastroenterology 1984; 3 1: 158-61.
61. Popper H, Martin GR. Fibrosis of the liver: the role of the ektoskeleton. In: Popper H, Schaffner F, eds. Progress in Liver Disease, Vol. VII. New York: Grune and Stratton, 1982: 133-56.
62. Hutterer F, Eisenstadt M, Rubin E. Turnover of hepatic col- lagen in reversible and irreversible fibrosis. Experientia 1970; 26: 2445.
17