Interferon Alpha2a Reduces Early Erythema After Full-Thickness Skin Graft in the Pig
11
Interferon Alpha-2a Reduces Early Erythema After Full-Thickness Skin Graft in the Pig JUN SIK KIM, MD, PHD, DAEGU SON, MD, PHD, y TAE HYUN CHOI, MD, PHD, z KIHWAN HAN, MD, PHD, y JUN HYUNG KIM, MD, PHD, y HYUN MI CHO, MSC, y WON HEE KIM, MSC, y SANG-HYON KIM, MD, y NAM GYUN KIM, MD, KYUNG SUK LEE, MD, O. HYUN HWANG, MD, z GU SEOB ROH, MD, PHD, J AND JUNGBIN PARK BACKGROUND Skin grafting is a commonly performed procedure, but studies of changes in the levels of cytokines after skin grafting have not been reported. OBJECTIVE We examined changes in cytokines and the degree of erythema after skin grafting in pigs in the control group. Interferon alpha (IFN-a) was injected to reduce erythema, and subsequent changes in cytokines and the degree of erythema were examined in the experimental group. METHODS Vascular endothelial growth factor (VEGF), thrombospondin-1 (TSP1), and CD31 were ex- amined using Western blot analysis and immunohistochemistry. The degree of erythema was measured at 2, 4, and 8 weeks using a chromometer. RESULTS In the control group, VEGF increased at 2 weeks and decreased at 4 and 8 weeks. TSP1 increased over time. CD31 increased to 4 weeks and decreased at 8 weeks. In the experimental group, VEGF was lower at 2 weeks and higher at 8 weeks than in the control group, TSP1 was higher at 2 weeks and lower at 8 weeks, and CD31 was lower at 4 and 8 weeks. Erythema in the experimental group was lower than that in the control group at 2 and 8 weeks. CONCLUSION IFN-a may be one of the agents that reduces erythema by suppressing excessive re- vascularization. The authors have indicated no significant interest with commercial supporters. S kin grafting is one of the procedures that is per- formed most commonly in the field of surgery. Survival mechanisms of skin graft are known to be serum imbibition and revascularization. 1 Vascular endothelial growth factor (VEGF) has been discovered to be a mitogen for vascular endothelial cells, and its importance as a potent regulator of angiogenesis has been shown. 2 In the last decade, improvements in wound healing and the viability of skin grafts and skin flaps have been demonstrated after application of VEGF. 3,4 Thrombospondin-1 (TSP1) was the first endogenous inhibitor of angio- genesis to be identified. TSP1 inhibits angiogenesis by modulating the proliferation and migration of endothelial and vascular smooth muscle cells. Isen- berg and colleagues found that blocking TSP1 binding or suppressing CD47 expression dramati- cally increased skin graft survival. 5 Nonetheless, to the authors’ knowledge, studies of alterations in VEGF or TSP1 during the revascularization of skin grafts have not been reported. & 2009 by the American Society for Dermatologic Surgery, Inc. Published by Wiley Periodicals, Inc. ISSN: 1076-0512 Dermatol Surg 2009;35:1514–1524 DOI: 10.1111/j.1524-4725.2009.01267.x 1514 Jun Sik Kim and O. Hyun Hwang contributed equally to this paper as first authors. Department of Plastic and Reconstructive Surgery and J Department of Anatomy, Institute of Health Sciences, College of Medicine and Hospital, Gyeongsang National University, Jinju, Republic of Korea; y Department of Plastic and Reconstructive Surgery and y Department of Internal Medicine, Keimyung University Dongsan Medical Center, Daegu, Republic of Korea; z Department of Reconstructive Plastic Surgery, Seoul National University Hospital, Seoul, Republic of Korea; z Department of Plastic and Reconstructive Surgery, Changwon Fatima Hospital, Changwon, Republic of Korea; Daegu Science High School, Daegu, Republic of Korea.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Interferon Alpha2a Reduces Early Erythema After Full-Thickness Skin Graft in the Pig

Interferon Alpha-2a Reduces Early Erythema AfterFull-Thickness Skin Graft in the Pig
JUN SIK KIM, MD, PHD,� DAEGU SON, MD, PHD,y TAE HYUN CHOI, MD, PHD,z
KIHWAN HAN, MD, PHD,y JUN HYUNG KIM, MD, PHD,y HYUN MI CHO, MSC,y WON HEE KIM, MSC,y
SANG-HYON KIM, MD,y NAM GYUN KIM, MD,� KYUNG SUK LEE, MD,� O. HYUN HWANG, MD,z
GU SEOB ROH, MD, PHD,J AND JUNGBIN PARK��
BACKGROUND Skin grafting is a commonly performed procedure, but studies of changes in the levelsof cytokines after skin grafting have not been reported.
OBJECTIVE We examined changes in cytokines and the degree of erythema after skin grafting in pigs inthe control group. Interferon alpha (IFN-a) was injected to reduce erythema, and subsequent changes incytokines and the degree of erythema were examined in the experimental group.
METHODS Vascular endothelial growth factor (VEGF), thrombospondin-1 (TSP1), and CD31 were ex-amined using Western blot analysis and immunohistochemistry. The degree of erythema was measuredat 2, 4, and 8 weeks using a chromometer.
RESULTS In the control group, VEGF increased at 2 weeks and decreased at 4 and 8 weeks. TSP1increased over time. CD31 increased to 4 weeks and decreased at 8 weeks. In the experimental group,VEGF was lower at 2 weeks and higher at 8 weeks than in the control group, TSP1 was higher at 2 weeksand lower at 8 weeks, and CD31 was lower at 4 and 8 weeks. Erythema in the experimental group waslower than that in the control group at 2 and 8 weeks.
CONCLUSION IFN-a may be one of the agents that reduces erythema by suppressing excessive re-vascularization.
The authors have indicated no significant interest with commercial supporters.
Skin grafting is one of the procedures that is per-
formed most commonly in the field of surgery.
Survival mechanisms of skin graft are known to be
serum imbibition and revascularization.1
Vascular endothelial growth factor (VEGF) has been
discovered to be a mitogen for vascular endothelial
cells, and its importance as a potent regulator of
angiogenesis has been shown.2 In the last decade,
improvements in wound healing and the viability of
skin grafts and skin flaps have been demonstrated
after application of VEGF.3,4 Thrombospondin-1
(TSP1) was the first endogenous inhibitor of angio-
genesis to be identified. TSP1 inhibits angiogenesis
by modulating the proliferation and migration of
endothelial and vascular smooth muscle cells. Isen-
berg and colleagues found that blocking TSP1
binding or suppressing CD47 expression dramati-
cally increased skin graft survival.5 Nonetheless, to
the authors’ knowledge, studies of alterations in
VEGF or TSP1 during the revascularization of skin
grafts have not been reported.
& 2009 by the American Society for Dermatologic Surgery, Inc. � Published by Wiley Periodicals, Inc. �ISSN: 1076-0512 � Dermatol Surg 2009;35:1514–1524 � DOI: 10.1111/j.1524-4725.2009.01267.x
1 5 1 4
Jun Sik Kim and O. Hyun Hwang contributed equally to this paper as first authors.
�Department of Plastic and Reconstructive Surgery and JDepartment of Anatomy, Institute of Health Sciences, Collegeof Medicine and Hospital, Gyeongsang National University, Jinju, Republic of Korea; yDepartment of Plastic andReconstructive Surgery and yDepartment of Internal Medicine, Keimyung University Dongsan Medical Center, Daegu,Republic of Korea; zDepartment of Reconstructive Plastic Surgery, Seoul National University Hospital, Seoul, Republicof Korea; zDepartment of Plastic and Reconstructive Surgery, Changwon Fatima Hospital, Changwon, Republic ofKorea; ��Daegu Science High School, Daegu, Republic of Korea.

Erythema develops in grafted skin during the early
period after surgery and is attributable to revas-
cularization. Because of the erythema, the grafted
skin appears distinctly different from the surround-
ing skin, and patients are often dissatisfied with the
aesthetic results.6
Interferon alpha (IFN-a) is a cytokine with pleio-
tropic cellular functions that include antiviral,
antiproliferative, immunomodulatory, and anti-
angiogenic activities. Clinical studies have demon-
strated that IFN-a treatment can induce impressive
responses in angioproliferative diseases, such as
Kaposi’s sarcoma and hemangiomas.7 Our hypoth-
esis was that the application of IFN-a, which has
antiangiogenic activities, would suppress the ery-
thema that develops after skin grafting and thus
improve patient satisfaction.
To examine the changes in VEGF, TSP1, and CD31
occurring during skin graft surgery in pigs, we per-
formed Western blot and immunohistochemistry
analyses. In an attempt to reduce the erythema de-
veloping in the early period after grafting, recombi-
nant IFN-a-2a was injected. After injection, changes
in the cytokines were examined, and to assess the
level of reduction in erythema, skin color was mea-
sured objectively using a chromometer.
Materials and Methods
Materials and Full-Thickness Skin
Graft Procedure
The experimental animals were Yorkshire pigs, aged
2 to 3 months old, weighing 20 to 30 kg, and with-
out dermatological diseases. They were fed with
standard pig feed and allowed to consume water
freely. The environment was maintained at one
atmosphere pressure, 201C to 231C, and 65%
humidity, with a 12-hour light–dark cycle.
Sedation was performed using an intramuscular injec-
tion of 2.2 mg/kg azaperone (Stresnil, Janssen, Beerse,
Belgium), and 37 mg/kg propofol (Diprivan-PFS,
AstraZeneca Korea, Seoul, Korea) was injected into
the external ear vein to induce anesthesia. Two iden-
tical experiments per pig were performed on the right
and left side. The hairs on the dorsum (recipient site)
were removed, and a 5� 5 cm wound was created
using a dermatome (Acculan, Aesculap Inc., Center
Valley, PA) with the depth adjusted to 0.8 mm. From
the inguinal area (donor site), full-thickness skin
5� 5 cm in size was harvested, and the defect area was
primarily closed with 2-0 nylon suture (Blue Nylon,
Ailee, Busan, Korea). The harvested skin was grafted
to the recipient site and immobilized using 3-0 chromic
catgut (Catgut chrom, B. Braun, Penang, Malaysia)
and a skin stapler (Reflex One and Reflex TL, Con-
med, Utica, NY). After surgery, a bolster dressing was
applied in the skin graft area to prevent injury. To
prevent infection, antibiotics were injected intramus-
cularly for 3 days. The Keimyung University School of
Medicine Institutional Animal Care and Use Commit-
tee approved the study.
Control Group: Four pigs received skin grafts using
the method described above.
Experimental Group: Three pigs received skin grafts
using the method described above. From 1 day after
surgery, recombinant human IFN-a-2a (Intermax
alpha, LG Life Sciences, Seoul, Korea) at a concen-
tration of 2,000,000 units/m2 was injected intra-
muscularly three times per week for 3 weeks.
Negative Control (Normal Skin): The negative con-
trol was a 5-� 5-cm area of skin harvested from
both sides of the back of the pigs that had not been
grafted.
Western Blot Analysis
Procedure: At 2, 4, and 8 weeks after surgery, an area
of the dorsal skin graft approximately 0.5� 1 cm in
size was harvested from control and experimental
pigs, and the following experiments were performed.
A sample of normal skin (negative control) was also
harvested, and identical experiments were performed.
Briefly, the tissues were transferred into five volumes
of RIPA buffer and homogenized in an ice bath with
3 5 : 1 0 : O C T O B E R 2 0 0 9 1 5 1 5
K I M E T A L

a tissue homogenizer. Five bursts of 15 seconds at
maximum speed with 45-second intervals of cooling
between each burst were applied. The homogenate
was then centrifuged at 2,000 g for 15 minutes at 41C.
The supernatant was recovered, and an aliquot was
used to evaluate the amount of protein. Fifty micro-
grams of protein were separated using 6% and 10%
sodium dodecyl sulfate polyacrylamide gel electro-
phoresis and then electrophoretically transferred to a
polyvinylidene fluoride membrane (Bio-Rad, Hercules,
CA) for immunoblot analysis according to standard
protocols. For protein detection, the membranes were
incubated with the primary antibodies (Abcam, Cam-
bridge, UK). Peroxidase-conjugated anti-mouse
immunoglobulins (KPL, Guelph, Ontario, Canada)
were used as secondary antibodies. The signals were
detected using the enhanced chemiluminescence West-
ern blot analysis system (Amersham Pharmacia,
Piscataway, NJ).
Quantitative data were determined as the mean ratio
of the optical density of the specific bands normal-
ized to that of b-actin. The densitometric analysis
was carried out using a Scion Image Data Analyzer
(SCION Corporation, Frederick, MD).
Analysis of Data: In each group, the change in ex-
pression of proteins with time was analyzed, and at
each (specific) time point, the difference in the ex-
pression of proteins between the control and exper-
imental groups was analyzed. In analysis of the
Western blot results, it was assumed that, as the
measurements were repeated, the measured values
followed a normal distribution, and the parametric
one-way analysis of variance (ANOVA) test was used.
Immunohistochemistry
The harvesting methods were as described for the
Western blot analysis. The harvested samples were
embedded in Optimal Cutting Temperature Com-
pound (Sakura, Tokyo, Japan) for frozen tissue
specimens and sectioned using a Cryocut Microtome
(Shandon, England) at 8mm thickness.
Cryosections were washed three times with phosphate
buffered saline (PBS) and fixed in methanol for 10
minutes at �201C. After being washed with PBS, sec-
tions were treated with 3% hydrogen peroxide for 20
minutes at room temperature and with antibody
diluent (Golden Bridge International Inc., Mukilteo,
WA) to block nonspecific reactions. The following
antibodies were used: VEGF (dilution 1/80; Abcam),
TSP1 (dilution 1/25; Abcam), and CD31 (dilution 1/
100; Chemicon, CA). After 1.5 hours incubation with
primary antibodies in a humidity chamber, a
DakoCytomation EnVision 1 System-horseradish
peroxidase–labelled polymer (DakoCytomation,
Glostrup, Denmark) was used for 30 minutes in
conjunction with all of the primary antibodies. A
DakoCytomation Liquid DAB Substrate Chromogen
System was used to label the antibodies. The slides
were counterstained with Mayer’s hematoxylin for
1 minute.
Chromometer Measurement and Analysis
of Results
Using a chromometer (Chromometer CR-300,
Minolta Co., Osaka, Japan), the redness of the re-
cipient site or skin graft was measured before surgery
and 2, 4, and 8 weeks after surgery in the control and
experimental groups. The area from which the skin
graft was taken was measured three times, and the
final value was defined as the average of the values
obtained.
In each group, change in redness of the skin graft
with time was analyzed, and at each (specific) time
point, the difference in redness between the control
and experimental groups was analyzed.
The Rate of Viability
The viability rate of the skin grafts was assessed 2
weeks after surgery. The viability rate was calculated as
the area of the skin graft that had taken as a percentage
of the original size (25 cm2). The viability rates of
the control and experimental groups were compared.
D E R M AT O L O G I C S U R G E RY1 5 1 6
I N T E R F E R O N -a - 2 A R E D U C E S E A R LY E RY T H E M A A F T E R S K I N G R A F T

Results
Changes in Levels of Cytokines According to
Western Blot Analysis
Changes in VEGF, TSP1, and CD31 in the Control
Group: The level of VEGF in the normal skin was
0.43; 2 weeks after surgery, it increased to 1.02, and
then 4 and 8 weeks after surgery decreased to 0.55
and 0.56, respectively. The values were significantly
different with time according to the one-way
ANOVA (po.001). Using the Tukey test, the value
was significantly higher than that of the normal skin
at 2 weeks (po.001), but at 4 and 8 weeks it was not
different from that of the normal skin (p = .08, .06).
The level of TSP1 in the normal skin was 0.34. At 2,
4, and 8 weeks after surgery, it increased to 0.49,
0.50, and 1.10, respectively. Using ANOVA, the
values were significantly different with times (po.001). Using the Tukey test, at 2, 4, and 8 weeks,
the levels were significantly higher than those in
normal skin (p = .008, .006, o.001).
The level of CD31 in the normal skin was 0.21. It
increased to 0.35 at 2 weeks and to 0.95 at 4 weeks
after surgery and then decreased slightly to 0.63 at 8
weeks. The values varied significantly with time
(ANOVA; po.001) and were significantly different
from those in normal skin at 2, 8, and 4 weeks
(Tukey; p = .01, o.001, o.001). In summary, the
level of CD31 increased continuously up to 4 weeks
and then decreased slightly at 8 weeks (Figure 1).
Changes in VEGF, TSP1, and CD31 in the Exper-
imental Group: The level of VEGF in the normal
skin was 0.43, and values at 2, 4, and 8 weeks after
surgery were 0.90, 0.53, and 0.68, respectively. Us-
ing one-way ANOVA, the values were significantly
different with time (po.001). The Tukey test showed
a significantly higher value at 2 weeks (po.001), and
at 8 weeks, the level was higher than in normal skin
(po.001). The level of VEGF therefore increased
maximally at 2 weeks, decreased at 4 weeks to the
normal skin level, and then increased again at 8
weeks.
The level of TSP1 in the normal skin was 0.34, and
the values at 2, 4, and 8 weeks after surgery were
1.07, 0.61, and 0.41, respectively. ANOVA showed
that the values differed significantly with time (po.001). At 2 and 4 weeks, the level was significantly
higher than in normal skin (Tukey; po.001,
p = .007). The level increased maximally at 2 weeks;
at 4 weeks, it decreased slightly but remained
higher than in normal skin, and by 8 weeks it had
decreased to the normal skin level.
The level of CD31 in the normal skin was 0.21, and
the values at 2, 4, and 8 weeks after surgery were
0.32, 0.86, and 0.37, respectively. According to
ANOVA, the values varied significantly with time (p
o.001). The Tukey test showed that, at 4 weeks, the
level of CD31 was significantly higher than in nor-
mal skin (po.001), but at 8 weeks it had decreased
to the normal skin level (Figure 1).
Comparison of the Control and Experimental
Groups: The control and experimental groups were
compared using an independent t-test. The level of
VEGF in the experimental group was lower than that
in the control group at 2 weeks (p = .03) but was not
different at 4 weeks (p = .74) and was higher at 8
weeks (p = .03). The level of TSP1 in the experimental
group was higher than that in the control group at 2
weeks (po.001), was not different at 4 weeks
(p = .16), and lower at 8 weeks (po.001). The level of
CD31 in the experimental group was not different
from the control group at 2 weeks (p = .56), but was
lower at 4 and 8 weeks (p = .04, .009) (Figure 1).
Expression of Cytokines According
to Immunohistochemistry
Vascular Endothelial Growth Factor: The dermis
and epidermis showed immunohistochemical stain-
ing, indicating VEGF protein expression. In the epi-
dermis, VEGF was expressed abundantly in
keratinocytes primarily, and in the dermis VEGF was
expressed abundantly in the endothelial cells of
blood vessels (Figure 2).
3 5 : 1 0 : O C T O B E R 2 0 0 9 1 5 1 7
K I M E T A L

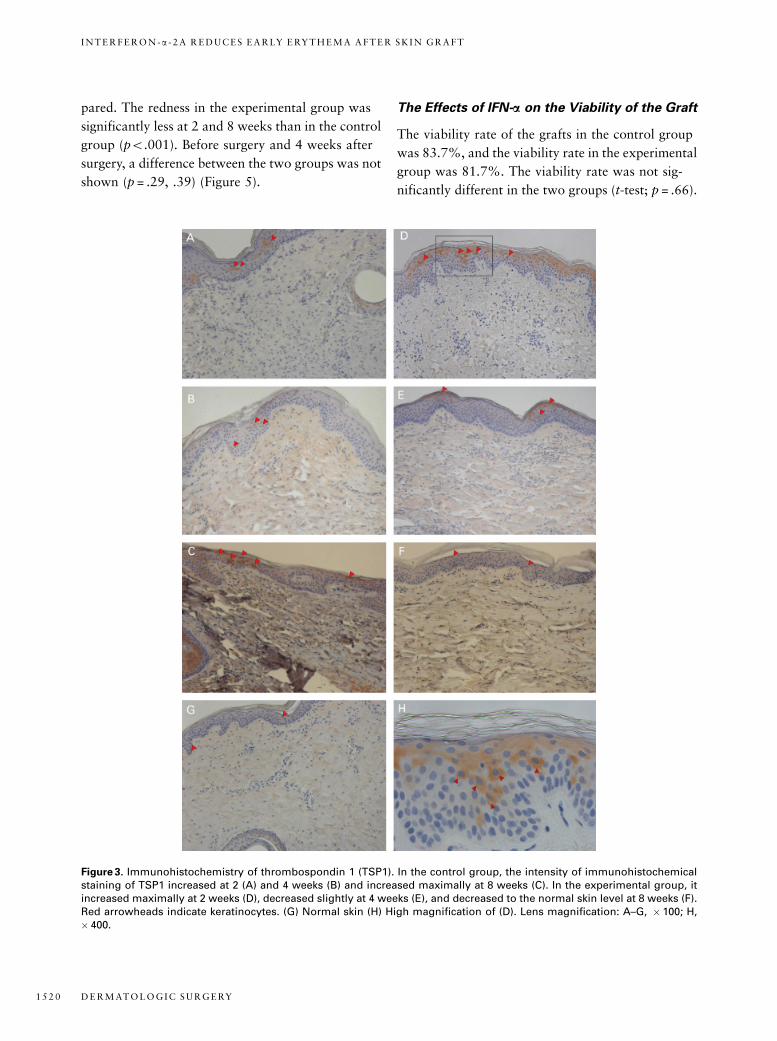
Thrombospondin 1: Expression of TSP1 was mainly
observed in keratinocytes in the epidermis (Figure 3).
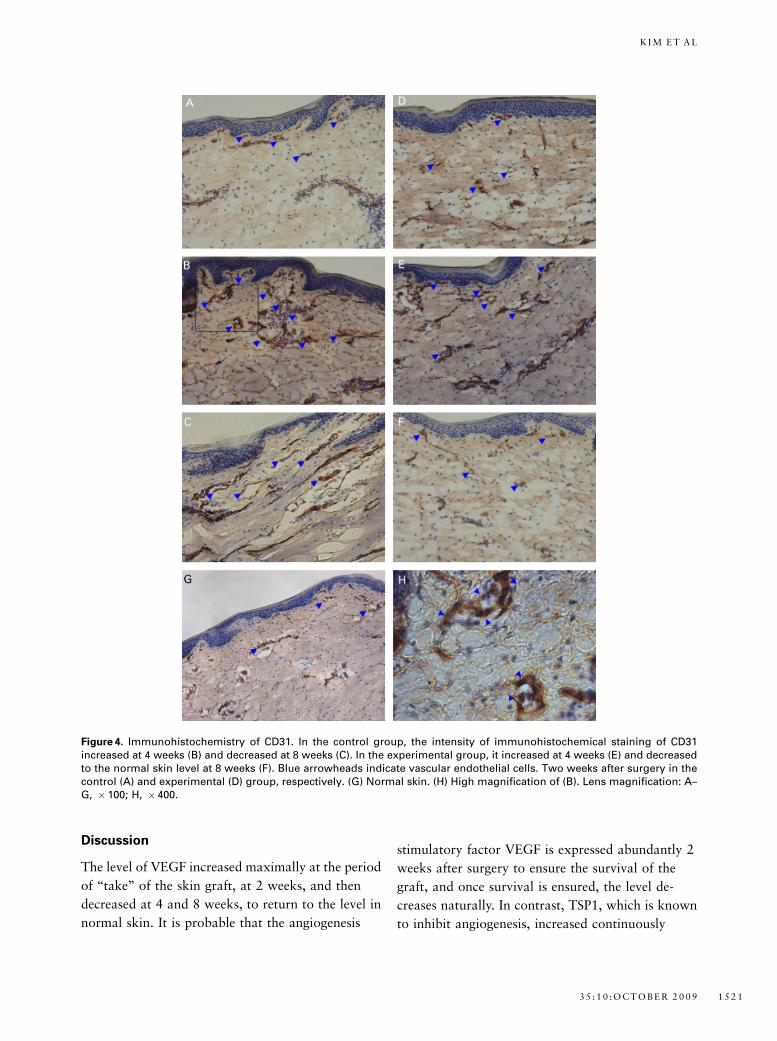
CD31: Because blood vessels are mainly present in
the dermis, CD31, which is expressed in the endo-
thelial cells of the vessels, was mainly observed in the
dermis (Figure 4).
The Effects of IFN-a on the Redness of
Grafted Skin
In the control group, the redness of the recipient
site was 6.85. At 2, 4, and 8 weeks after the skin
graft, the redness of the grafted skin was 18.95,
11.31, and 11.17, respectively. A significant differ-
ence between the four groups was shown according
to ANOVA (po.001). Using the Scheffe test, a sig-
nificant difference was shown between the redness of
the recipient site and the redness at 2, 4, and 8 weeks
(po.001 for all), although a significant difference
was not shown between the values at 4 and 8 weeks,
(p = 1.00). In summary, the redness was greatest at 2
weeks and decreased at 4 and 8 weeks; nonetheless,
the redness at 8 weeks remained different from that
at the recipient site (Figure 5).
In the experimental group, the redness of the recip-
ient site was 7.59. The redness of the grafted skin at
2, 4, and 8 weeks was 9.12, 10.70, and 9.36,
Figure 1. Expression of vascular endothelial growth factor (VEGF), thrombospondin 1 (TSP1), and CD31 according to West-ern blot analysis (above, left). The relative protein levels of VEGF (above, right), TSP1 (below, left), and CD31 (below, right)are shown. One-way analysis of variance was used to compare the multiple group means, followed by the Tukey test. AoBoCoD or A’oB’oC’, results of the Tukey test (compared with normal skin) in the control and experimental groups,respectively. Both groups were compared using an independent t-test (significance compared with control group, ypo.05).NS, normal skin; C, control group; E, experimental group; wk, weeks after skin graft.
D E R M AT O L O G I C S U R G E RY1 5 1 8
I N T E R F E R O N -a - 2 A R E D U C E S E A R LY E RY T H E M A A F T E R S K I N G R A F T

respectively. A significant difference between the four
groups was shown using ANOVA (p= .006). Using the
Scheffe test, a significant difference was found between
the recipient site and the graft at 4 weeks (p= .007),
although there was no significant difference between the
recipient site and the graft at 2 or 8 weeks (p= .29, .19).
In summary, at 4 weeks, the redness had significantly
increased, but it had decreased at 8 weeks and was then
not different from that at the recipient site (Figure 5).
Using the independent t-test, the redness of the skin
in the control and experimental groups was com-
Figure 2. Immunohistochemistry of vascular endothelial growth factor (VEGF). In the control group, the intensity ofimmunohistochemical staining of VEGF increased at 2 weeks (A) and returned to the normal skin level at 4 (B) and 8 (C)weeks. In the experimental group, it increased maximally at 2 weeks (D), decreased at 4 weeks (E), and increased again at 8weeks (F). Red and blue arrowheads indicate positive immunohistochemical staining in keratinocytes and vascular endo-thelial cells, respectively. (G) Normal skin. (H) High magnification of (D). Lens magnification: A–G, � 100; H, � 400.
3 5 : 1 0 : O C T O B E R 2 0 0 9 1 5 1 9
K I M E T A L
pared. The redness in the experimental group was
significantly less at 2 and 8 weeks than in the control
group (po.001). Before surgery and 4 weeks after
surgery, a difference between the two groups was not
shown (p = .29, .39) (Figure 5).
The Effects of IFN-a on the Viability of the Graft
The viability rate of the grafts in the control group
was 83.7%, and the viability rate in the experimental
group was 81.7%. The viability rate was not sig-
nificantly different in the two groups (t-test; p = .66).
Figure 3. Immunohistochemistry of thrombospondin 1 (TSP1). In the control group, the intensity of immunohistochemicalstaining of TSP1 increased at 2 (A) and 4 weeks (B) and increased maximally at 8 weeks (C). In the experimental group, itincreased maximally at 2 weeks (D), decreased slightly at 4 weeks (E), and decreased to the normal skin level at 8 weeks (F).Red arrowheads indicate keratinocytes. (G) Normal skin (H) High magnification of (D). Lens magnification: A–G, � 100; H,� 400.
D E R M AT O L O G I C S U R G E RY1 5 2 0
I N T E R F E R O N -a - 2 A R E D U C E S E A R LY E RY T H E M A A F T E R S K I N G R A F T
Discussion
The level of VEGF increased maximally at the period
of ‘‘take’’ of the skin graft, at 2 weeks, and then
decreased at 4 and 8 weeks, to return to the level in
normal skin. It is probable that the angiogenesis
stimulatory factor VEGF is expressed abundantly 2
weeks after surgery to ensure the survival of the
graft, and once survival is ensured, the level de-
creases naturally. In contrast, TSP1, which is known
to inhibit angiogenesis, increased continuously
Figure 4. Immunohistochemistry of CD31. In the control group, the intensity of immunohistochemical staining of CD31increased at 4 weeks (B) and decreased at 8 weeks (C). In the experimental group, it increased at 4 weeks (E) and decreasedto the normal skin level at 8 weeks (F). Blue arrowheads indicate vascular endothelial cells. Two weeks after surgery in thecontrol (A) and experimental (D) group, respectively. (G) Normal skin. (H) High magnification of (B). Lens magnification: A–G, �100; H, �400.
3 5 : 1 0 : O C T O B E R 2 0 0 9 1 5 2 1
K I M E T A L

after skin grafting and was expressed maximally at 8
weeks. In other words, it is probable that, during the
early period after skin grafting, VEGF increases and
thus stimulates revascularization for survival. At 4 to
8 weeks, after survival is ensured, VEGF decreases,
and the angiogenesis inhibitor factor TSP1 increases,
resulting in reduced revascularization, and thus ho-
meostasis is maintained. Thus, VEGF and TSP1 are
speculated to maintain a balance during revas-
cularization of the skin graft. Our results are similar
to those of the study reported by Yano and
colleagues on the effects of ultraviolet B (UVB) ir-
radiation. According to Yano and colleagues, skin
vascularity in the upper dermis increased greatly af-
ter a single dose of UVB irradiation until day 8 and
was associated with upregulation of VEGF messen-
ger ribonucleic acid (mRNA) expression and down-
regulation of TSP1 mRNA. After 13 days, skin
vascularity was normalized, with downregulation of
VEGF mRNA expression and upregulation of TSP1
mRNA expression.8 One point of difference is that,
in our study, the expression of TSP1 was not
downregulated during the early period after surgery.
To evaluate the revascularization of the skin graft
objectively, we measured CD31, which has been
used as a vascular endothelial cell marker. We also
measured the redness of the skin graft objectively
using a chromometer. The redness of the skin color is
mainly affected by the degree of vascularization.9
Consistent with the changes in VEGF and TSP1 de-
scribed above, CD31 increased up to 4 weeks after
surgery and then decreased gradually to 8 weeks.
The redness increased maximally at 2 weeks and
decreased gradually to 4 and 8 weeks. This result is
almost in full agreement with the report of Kim
and colleagues, which described the color changes in
skin grafts with time in human patients.10 One factor
to be considered here is that the level of CD31 was
decreased at 4 weeks after surgery, whereas the
redness decreased after 2 weeks. It could be that
blood flow in vessels generated during revas-
cularization decreases slowly, owing to unknown
factors from 2 weeks after skin grafting. This spec-
ulation is in agreement with the claim of Omori and
Kurata that, after the 10th day after a skin graft,
circulation increased to a level greater than that seen
in normal skin. Circulation in the skin graft nor-
malized on the 20th day.11
As mentioned earlier, because IFN-a is a cytokine
with antiangiogenic activities,7 it could be expected
that IFN-a would inhibit the expression of VEGF
and increase that of TSP1. Review of the literature
shows that IFN-a can downregulate VEGF expres-
sion, represented by mRNA and protein levels, in
MHCC97 cells,12 and that IFN-a dose-dependently
inhibits VEGF release in peripheral blood mononu-
clear cells.13 The above reports are in agreement
with our research. At 2 weeks after surgery, the ex-
pression of VEGF in the experimental group injected
with IFN-a was lower than in the control group. At 8
weeks, the level of VEGF had increased more than in
the control group, which may be due to a rebound
phenomenon after the withdrawal of IFN-a.
Reports on the relationship between IFN-a and TSP1
are rare. It has been reported that the increased level
of platelet surface-associated TSP in essential
thrombocythemia tended to be normalized during
IFN-a treatment.14 In contrast, in our research, the
Figure 5. Redness value of the grafted skin. One-way anal-ysis of variance was used to compare the multiple groupmeans, followed by the Scheffe test. AoBoC or A’oB’, re-sults of the Scheffe test (compared with recipient site) in thecontrol and experimental groups, respectively. Both groupswere compared using the independent t-test (significancecompared with control group, ypo.05). C, control group; E,experimental group; RS, recipient site; wk, weeks after skingraft.
D E R M AT O L O G I C S U R G E RY1 5 2 2
I N T E R F E R O N -a - 2 A R E D U C E S E A R LY E RY T H E M A A F T E R S K I N G R A F T

expression of TSP1 increased in the experimental
group at 2 weeks and decreased at 8 weeks as a result
of the rebound phenomenon. More studies are re-
quired on the relationship between IFN-a and TSP1.
Consistent with the changes in cytokines described
above, CD31 decreased at 4 and 8 weeks in the
grafted skin of the experimental group, and the
redness was less at 2 and 8 weeks than in the control
group.
One potential cause for concern is that, because of
the action of IFN-a in suppressing revascularization,
the graft survival rate could be reduced, but the
survival rate in the experimental group was not sig-
nificantly different from that in the control group. In
other words, without a difference in survival rate,
administration of IFN-a reduced erythema in the
skin graft.
There have been a few studies of drugs that decrease
erythema by suppressing excessive revascularization
during the early phase of skin grafting, but IFN-ais thought to be a candidate for use in clinics.
Although more studies on human patients are re-
quired, if IFN-a can ameliorate erythema after skin
grafting, it is anticipated that the aesthetic satisfac-
tion of patients would be much greater.
One of the advantages of our study is that pigs were
used as experimental animals. Because pig skin is
similar to human skin anatomically and physiolog-
ically, the pig makes an excellent animal model for
studies of human wound healing.15 In addition, to
evaluate the redness of the skin graft objectively, a
chromometer was used. Because redness is shown
numerically on this instrument, changes in redness
and treatment effectiveness could be evaluated ac-
curately and objectively.
The shortcomings of our study are that the studies
were performed only in vivo. In the future, it may be
necessary to investigate the relationship between
cells that are present in the skin, such as keratin-
ocytes, fibroblasts, and endothelial cells, and IFN-a
in vitro. In addition, as mentioned earlier, more
studies on the relationship between IFN-a and TSP1
are required.
Acknowledgments This work was supported by
the Korea Research Foundation Grant, funded by the
Korean Government (MOEHRD) (KRF-2006-331-
E00225) and a special clinical fund of Gyeongsang
National University Hospital.
References
1. Paletta CE, Pokorny JJ, Rumbolo PM. Skin grafts. In: Mathes SJ,
editor. Plastic Surgery. 2nd ed. Philadelphia: Saunders Elsevier;
2006. p. 293–316.
2. Celik-Ozenci C, Akkoyunlu G, Korgun ET, et al. Expressions of
VEGF and its receptors in rat corpus luteum during interferon
alpha administration in early and pseudopregnancy. Mol Reprod
Dev 2004;67:414–23.
3. Zhang F, Oswald TM, Lin L, et al. Improvement of full-thickness
skin graft survival by application of vascular endothelial growth
factor in rats. Ann Plast Surg 2008;60:589–93.
4. Richter GT, Fan CY, Ozgursoy O, et al. Effect of vascular endo-
thelial growth factor on skin graft survival in Sprague-Dawley
rats. Arch Otolaryngol Head Neck Surg 2006;132:637–41.
5. Isenberg JS, Pappan LK, Romeo MJ, et al. Blockade of
thrombospondin-1-CD47 interactions prevents necrosis of full
thickness skin grafts. Ann Surg 2008;247:180–90.
6. Cho SH, Yoo SI, Noh BK, et al. Color analysis of forehead flap
and full thickness skin graft in facial reconstruction. J Kor Soc
Plast Reconstr Surg 2008;35:35–40.
7. Marschall ZV, Scholz A, Cramer T, et al. Effects of interferon
alpha on vascular endothelial growth factor gene transcription
and tumor angiogenesis. J Natl Cancer Inst 2003;95:437–48.
8. Yano K, Kajiya K, Ishiwata M, et al. Ultraviolet B-induced skin
angiogenesis is associated with a switch in the balance of vascular
endothelial growth factor and thrombospondin-1 expression. J
Invest Dermatol 2004;122:201–8.
9. Han K, Choi T, Son D. Skin color of Koreans: statistical evalu-
ation of affecting factors. Skin Res Technol 2006;12:170–7.
10. Kim JS, Park SW, Choi TH, et al. The evaluation of relevant
factors influencing skin graft changes in color over time. Dermatol
Surg 2008;34:32–9.
11. Omori S, Kurata K. Experimental studies on the blood supply to
various types of skin grafts in rabbits using isotope P32. Plast
Reconstr Surg 1960;25:547–55.
12. Wu WZ, Sun HC, Shen YF, et al. Interferon alpha 2a downreg-
ulates VEGF expression through PI3 kinase and MAP kinase
signaling pathways. J Cancer Res Clin Oncol 2005;131:169–78.
13. Salven P, Anttonen K, Repo H, et al. Endotoxins induce and in-
terferon-a suppresses vascular endothelial growth factor (VEGF)
3 5 : 1 0 : O C T O B E R 2 0 0 9 1 5 2 3
K I M E T A L

production in human peripheral blood mononuclear cells. FASEB
J 2001;15:1318–20.
14. Legrand C, Bellucci S, Disdier M, et al. Platelet thrombospondin
and glycoprotein IV abnormalities in patients with essential
thrombocythemia: effect of a-interferon treatment. Am J Hematol
1991;38:307–13.
15. Sullivan TP, Eaglstein WH, Davis SC, Mertz P. The pig as a model
for human wound healing. Wound Rep Reg 2001;9:66–76.
Address correspondence and reprint requests to: Tae HyunChoi, MD, PhD, Department of Plastic and ReconstructiveSurgery, Seoul National University College of Medicine,Seoul National University Hospital, 101 Daehang-roJongno-gu, Seoul 110-744 Republic of Korea, ore-mail: [email protected]
D E R M AT O L O G I C S U R G E RY1 5 2 4
I N T E R F E R O N -a - 2 A R E D U C E S E A R LY E RY T H E M A A F T E R S K I N G R A F T