Integrating the cognitive and physiological aspects of craving
8
Journal of Psychopharmacology 12(1) (1998) 31-38 ©1998 British Association for Psychopharmacology (ISSN 0269-8811) SAGE Publications, London, Thousand Oaks, CA and New Delhi 0269-8811 [199803]12:1; 31-38; 003053 Integrating the cognitive and physiological aspects of craving AvivWeinstein, Barbara Feldtkeller, Andrea Malizia, Sue Wilson, Jayne Bailey and David J. Nutt The Psychopharmacology Unit, School of Medical Sciences, University of Bristol, University Walk, Bristol BSB lTD, UK. 'Craving is generally considered a significant factor in opiate addiction that is associated with drug-dependence and in relapse to drug use after treatment'-ARC expert consensus (Pickens and Johanson, Drug and Alcohol Dependence 30: 127-131). There are however difficulties in defining craving and urges to use drugs and in associating craving with drug use and relapse. Tiffany [Psychological Review 97(2): 147-168] has reviewed a considerable number of studies that associated reports of craving with consumption measures of drugs and revealed only an overall modest correlation of 0.4.These findings call into question the general assumption that subjective cravings are invariably associated with drug use. Furthermore, it led to Tiffany's provocative argument that cravings are not necessary for drug use. We have addressed these issues by using a range of complementary techniques derived from research in related fields such as the cognitive psychology of anxiety and depression, physiological response measurements and positron emission tomography (PET) neuro-imaging. Initially we developed computerized assessments to probe cognitive dysfunction in addiction that related to biased processing of automatic thoughts and beliefs about craving and drug use in opiate-dependent subjects and alcoholics. Subsequently in an attempt to develop a reliable method of inducing craving we explored an imagery-based technique that relied on the memory of craving experiences, These experiments were conducted both in opiate addicts who had achieved abstinence and in those undergoing detoxification. Finally, we have begun a study to understand the neural mechanisms of craving using imagery-based procedures at the same time as performing PET studies of regional blood flow using the 0 15 -labelled water technique. Key words: alcoholism; craving; cue-exposure; imagery; opiate addiction The processing of automatic thoughts and beliefs about craving and drug use There is good evidence that cognitive biases are associated with emotional disorders such as depression and anxiety (Williams et al., 1988). These seem to reflect an altered cognitive function and may have aetiological, diagnostic and treatment implications. Cognitive studies over the past 20 years have investigated the role of priming to a relevant context in emotional disorders such as anxiety. Contextual priming techniques have been previously applied to the study of processing of anxiety-related information by anxious patients. Clark et at. (1988) have shown that in panic patients performing a contextual priming task, sentence completions with negative words were significantly faster than sentence completions with neutral words, whereas in normal control subjects completion times for the two word types were comparable. However, contextual priming investigations in anxious patients by Weinstein and Nutt (1995) and traumatized patients by Weinstein et at. (1996b) have shown an overall slowness of responses to anxiety-related words following congruent anxiety-related sentences. Despite the extensive knowledge of and research into this area in other psychiatric disorders there has been little extension of this approach to addiction, the following series of studies were therefore conducted. In our first set of studies (Weinstein et al., 1996c) we investigated the processing of sentences describing automatic thoughts and beliefs associated with drug craving in opiate- dependent subjects who attended a methadone-maintenance clinic after a weekend of abstinence, half an hour prior to receiving methadone. Twenty opiate-dependent patients meet- ing DSM-IV (American Psychiatric Association, 1994) criteria for opiate dependence and 20 control subjects who were not opiate dependent with normal or corrected-to-normal vision participated in the experiment. Control subjects were clinical and administrative staff at the clinic. It was decided to use staff from the methadone-maintenance clinic as control subjects since, although they did not use opiates, they were familiar with the automatic thoughts, beliefs and language that opiate- dependent subjects use to describe their drug use. The mean age of patients was 30 (SD=7.05 years) and mean age of control subjects was 36 (SD = 6.57 years). In the addiction group there was one female and 19 males and in the control group there were 13 females and seven males. Subjects were tested on a computerized contextual priming task. In our study, the contextual priming task required responding to craving (positive expectancies and avoidance of withdrawal)
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Integrating the cognitive and physiological aspects of craving

Journal of Psychopharmacology 12(1) (1998) 31-38©1998 British Association for Psychopharmacology (ISSN 0269-8811)SAGE Publications, London, Thousand Oaks, CA and New Delhi0269-8811 [199803]12:1; 31-38; 003053
Integrating the cognitive and physiological aspects of cravingAvivWeinstein, Barbara Feldtkeller, Andrea Malizia, Sue Wilson, Jayne Baileyand David J. NuttThe Psychopharmacology Unit, School of Medical Sciences, University of Bristol, University Walk, Bristol BSB lTD, UK.
'Craving is generally considered a significant factor in opiate addiction that is associated with drug-dependenceand in relapse to drug use after treatment'-ARC expert consensus (Pickens and Johanson, Drug and AlcoholDependence 30: 127-131). There are however difficulties in defining craving and urges to use drugs and inassociating craving with drug use and relapse. Tiffany [Psychological Review 97(2): 147-168] has reviewed aconsiderable number of studies that associated reports of craving with consumption measures of drugs andrevealed only an overall modest correlation of 0.4.These findings call into question the general assumptionthat subjective cravings are invariably associated with drug use. Furthermore, it led to Tiffany's provocativeargument that cravings are not necessary for drug use. We have addressed these issues by using a range ofcomplementary techniques derived from research in related fields such as the cognitive psychology of anxietyand depression, physiological response measurements and positron emission tomography (PET) neuro-imaging.Initially we developed computerized assessments to probe cognitive dysfunction in addiction that related tobiased processing of automatic thoughts and beliefs about craving and drug use in opiate-dependent subjectsand alcoholics. Subsequently in an attempt to develop a reliable method of inducing craving we explored animagery-based technique that relied on the memory of craving experiences, These experiments were conductedboth in opiate addicts who had achieved abstinence and in those undergoing detoxification. Finally, we havebegun a study to understand the neural mechanisms of craving using imagery-based procedures at the sametime as performing PET studies of regional blood flow using the 015 -labelled water technique.
Key words: alcoholism; craving; cue-exposure; imagery; opiate addiction
The processing of automatic thoughts andbeliefs about craving and drug useThere is good evidence that cognitive biases are associatedwith emotional disorders such as depression and anxiety(Williams et al., 1988). These seem to reflect an alteredcognitive function and may have aetiological, diagnostic andtreatment implications. Cognitive studies over the past 20years have investigated the role of priming to a relevantcontext in emotional disorders such as anxiety. Contextualpriming techniques have been previously applied to the studyof processing of anxiety-related information by anxiouspatients. Clark et at. (1988) have shown that in panic patientsperforming a contextual priming task, sentence completionswith negative words were significantly faster than sentencecompletions with neutral words, whereas in normal controlsubjects completion times for the two word types werecomparable. However, contextual priming investigations inanxious patients by Weinstein and Nutt (1995) andtraumatized patients by Weinstein et at. (1996b) have shownan overall slowness of responses to anxiety-related wordsfollowing congruent anxiety-related sentences. Despite theextensive knowledge of and research into this area in otherpsychiatric disorders there has been little extension of this
approach to addiction, the following series of studies weretherefore conducted.
In our first set of studies (Weinstein et al., 1996c) weinvestigated the processing of sentences describing automaticthoughts and beliefs associated with drug craving in opiate-dependent subjects who attended a methadone-maintenanceclinic after a weekend of abstinence, half an hour prior toreceiving methadone. Twenty opiate-dependent patients meet-ing DSM-IV (American Psychiatric Association, 1994) criteriafor opiate dependence and 20 control subjects who were notopiate dependent with normal or corrected-to-normal visionparticipated in the experiment. Control subjects were clinicaland administrative staff at the clinic. It was decided to use stafffrom the methadone-maintenance clinic as control subjectssince, although they did not use opiates, they were familiarwith the automatic thoughts, beliefs and language that opiate-dependent subjects use to describe their drug use. The meanage of patients was 30 (SD=7.05 years) and mean age ofcontrol subjects was 36 (SD = 6.57 years). In the addictiongroup there was one female and 19 males and in the controlgroup there were 13 females and seven males. Subjects weretested on a computerized contextual priming task. In ourstudy, the contextual priming task required responding tocraving (positive expectancies and avoidance of withdrawal)
32
and general physical symptoms (control) sentences. Thesentences were followed by either drug-related neutral wordsor non-words (targets). Subjects had to decide whether thetargets were proper words or non-words, e.g.:
SentenceI would certainly enjoy a shot of drugs
Word/non-word'Fixing''Fexing''Touch''Tooch'
I feel a need for medical treatment
Subjects were seated 100 ern in front of the display screen.Their heads were directly in front of and level with the positionof the fixation point. Subjects were instructed to pay attentionto sentences which were followed by words. The words wereeither semantically proper English words or strings of letters(non-words). Subjects were instructed to press the right keywith their right index finger for proper words and the left keywith their left index finger for non-words. Several practicetrials were done to ensure a proper understanding of the task.The reaction time and response rates from all subjects for allconditions were subjected to factorial analysis of variance. In acontextual priming task, subjects typically make faster word-naming responses if the target word is one they would expectfrom the priming sentence than if it is a word that they wouldnot expect given the priming sentence. If opiate-dependentsubjects were facilitated by automatic thoughts of craving wewould, therefore, expect that they would be relatively quicker('primed') at responding to addiction-related words whichfollow congruent craving sentences than to neutral wordswhich follow congruent non-addiction sentences.In order to test this hypothesis, a three-way repeated
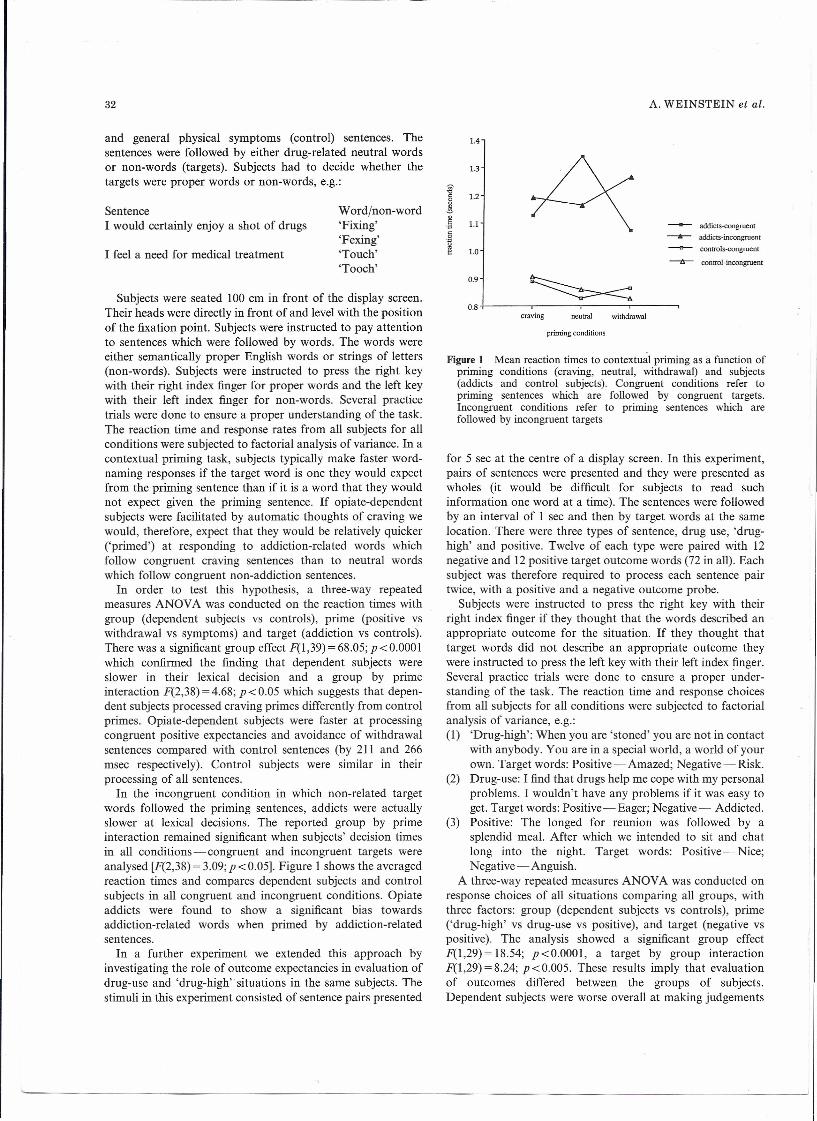
measures ANOVA was conducted on the reaction times withgroup (dependent subjects vs controls), prime (positive vswithdrawal vs symptoms) and target (addiction vs controls).There was a significant group effect F(I,39) = 68.05; p <0.0001which confirmed the finding that dependent subjects wereslower in their lexical decision and a group by primeinteraction F(2,38) =4.68; P <0.05 which suggests that depen-dent subjects processed craving primes differently from controlprimes. Opiate-dependent subjects were faster at processingcongruent positive expectancies and avoidance of withdrawalsentences compared with control sentences (by 211 and 266msec respectively). Control subjects were similar in theirprocessing of all sentences.In the incongruent condition in which non-related target
words followed the priming sentences, addicts were actuallyslower at lexical decisions. The reported group by primeinteraction remained significant when subjects' decision timesin all conditions-congruent and incongruent targets wereanalysed [F(2,38) =3.09;p <0.05]. Figure I shows the averagedreaction times and compares dependent subjects and controlsubjects in all congruent and incongruent conditions. Opiateaddicts were found to show a significant bias towardsaddiction-related words when primed by addiction-relatedsentences.In a further experiment we extended this approach by
investigating the role of outcome expectancies in evaluation ofdrug-use and 'drug-high' situations in the same subjects. Thestimuli in this experiment consisted of sentence pairs presented
A. WEINSTEIN et al.
1.4
1.3
-;;,"0
1.2s!.~ 1.1
§.~
1.0
0.9
0.8
addicts-congruent
--..- addicts-incongruent
controls-congruent
~ control-incongruent
craving neutral withdrawal
priming conditions
Figure 1 Mean reaction times to contextual priming as a function ofpriming conditions (craving, neutral, withdrawal) and subjects(addicts and control subjects). Congruent conditions refer topriming sentences which are followed by congruent targets.Incongruent conditions refer to priming sentences which arefollowed by incongruent targets
for 5 see at the centre of a display screen. In this experiment,pairs of sentences were presented and they were presented aswholes (it would be difficult for subjects to read suchinformation one word at a time). The sentences were followedby an interval of 1 sec and then by target words at the samelocation. There were three types of sentence, drug use, 'drug-high' and positive. Twelve of each type were paired with 12negative and 12 positive target outcome words (72 in all). Eachsubject was therefore required to process each sentence pairtwice, with a positive and a negative outcome probe.Subjects were instructed to press the right key with their
right index finger if they thought that the words described anappropriate outcome for the situation. If they thought thattarget words did not describe an appropriate outcome theywere instructed to press the left key with their left index finger.Several practice trials were done to ensure a proper under-standing of the task. The reaction time and response choicesfrom all subjects for all conditions were subjected to factorialanalysis of variance, e.g.:(I) 'Drug-high': When you are 'stoned' you are not in contact
with anybody. You are in a special world, a world of yourown. Target words: Positive-Amazed; Negative-Risk.
(2) Drug-use: I find that drugs help me cope with my personalproblems. I wouldn't have any problems if it was easy toget. Target words: Positive-Eager; Negative- Addicted.
(3) Positive: The longed for reunion was followed by asplendid meal. After which we intended to sit and chatlong into the night. Target words: Positive-Nice;Negative - Anguish.
A three-way repeated measures ANOVA was conducted onresponse choices of all situations comparing all groups, withthree factors: group (dependent subjects vs controls), prime('drug-high' vs drug-use vs positive), and target (negative vspositive). The analysis showed a significant group effectF(I,29)= 18.54; p<O.OOOI, a target by group interactionF(I,29) = 8.24; p<0.005. These results imply that evaluationof outcomes differed between the groups of subjects.Dependent subjects were worse overall at making judgements

COGNITIVE AND PHYSIOLOGICAL ASPECTS OF CRAVING
compared with control subjects (the group effect). This effectwas moderated by a specific interaction between target-outcome and group. In order to clarify this finding, a posthoc comparison of response choices by using one-wayANOVAs confirmed the prediction that dependent subjectsmade more responses in favour of positive outcomes to 'drug-high' situations (in the 'drug-high' incongruous condition)F(l,29) =8.54; p<O.OI and in favour of positive outcomes todrug-use situations (in the drug-use incongruous condition)F(l ,29)=8.69;p <0.001 compared with controls. Furthermore,they showed the opposite pattern for positive situations andendorsed less positive outcomes.Figure 2 shows that compared with control subjects,
dependent subjects endorsed more positive outcomes to'drug-high' and drug-use situations. Taken together thesetwo sets of experiments imply that thoughts and beliefs aboutdrug use may play an active role in drug craving in opiate-dependent individuals. In order to explore how generalizablethese cognitive factors might be in the addictions wesubsequently used the contextual priming task with alcoholicswho were in an abstinence programme in a local alcohol clinic(Feldtkeller et al., 1997). Subjects were 28 alcohol-dependentpatients who met DSM-IV (American Psychiatric Association,1994) criteria for alcohol dependence recruited from arehabilitation unit (day centre) and 28 matching controlswho were not alcohol dependent recruited by displayingposters in local shops and job centres. The level of alcoholdependence was assessed with the Severity of AlcoholDependence Questionnaire (SADQ; Stockwell et al., 1979).The patient group (n =28) had been dry for 3 weeks to 6months (mean age 42±8.68 years; mean age at first drink17.04±2.33 years; mean SADQ 35.91±7.09) and controlsubjects (n =20; mean age 40.08 ± 9.96 years; mean age at firstdrink 16.8± 1.68 years). All subjects were matched for age andsocio-economic status, as well as spelling ability using anadapted version of the Mill Hill Vocabulary spelling test. Thetask and the procedure were exactly the same as the firstexperiment, however, the priming sentences and target wordswere different. Participants were primed to positive sentencesof craving (e.g. 'I want to drink so bad I almost can taste it')which were followed by an alcohol congruent or incongruenttarget word/non-word (e.g. addict/meter or addoct/mitor).The results of this experiment revealed a selective bias in
processing craving-related sentences in the alcohol-dependentgroup but in a different direction to that found in the opiateaddicts. A three-way repeated measures ANOVA over thefactors 'group' (alcoholics vs control subjects), 'prime' (neutralvs craving) and target (congruent vs incongruent) wasperformed. It revealed a group by prime interactionF(2,38) =4.03; p <0.05 which implied that alcoholicsresponded to craving priming sentences differently fromneutral priming sentences. A consequent analysis has showna significant interference, i.e. slower response times, inalcoholics responding to alcohol words following cravingsentences compared with their responses to neutral wordsfollowing neutral sentences (by 140 msec) whereas the controlgroup performed equally fast in all conditions. Since it isdifficult to induce craving in alcoholics by external cues, it isplausible that the observed interference is due to delay inmaking lexical decisions of alcohol words (rather than
33
7.--------------------------------,w6..cEE5<1>
~4o0-(/l
~3
2(A) negative positive
outcome words
8 .-------~----------------------_,
3(8)
w7..cE~ 6 + ~C!.J
~5o0-
~4•....
negative positiveoutcome words
12
w 10..cE 8:::JC<1> 6 ~ ·······································rc~············ ...........................................•......... I(/lc~ 4 + ,~ .(/l
~ 2
(e)
o~------~--------------~----~negative positive
outcome words
I- addicts • controls IFigure 2 Response numbers in the opiate study for situations as afunction of type of situation (A) 'drug-high', (B) drug-use and (C)positive-outcome words (negative, positive) and subjects (addictsand control subjects)
contextual pnnung of sentences). See Fig. 3 for contextualpriming in alcoholics and control subjects. Craving was clearlyindicated by the subjective rating questionnaires that wereadministered immediately after the task was completed. Inthese, the patients rated themselves as having high levels ofautomatic thoughts referring to substance use as well asdysfunctional beliefs of craving and substance use.Taken together these studies demonstrated a different
cognitive profile of responses to craving-related informationin opiate-dependent individuals and alcoholics. In the opiateaddicts, addiction-related sentences resulted in accelerated

34
0.9
~~-0
"0o~o.§ 0.8
"0"fles1:!
alcoholicscontrols
0.7+----r------,-----,.---~craving neutral withdrawal
Figure 3 Mean reaction times to contextual priming as a function ofpriming conditions (craving, neutral, withdrawal) and subjects(alcoholics and control subjects)
response to addiction-related words whereas in the alcoholicsexposure to craving-related sentences slowed response times.
One explanation of these findings is that opiate-dependentpersons tend to react impulsively to drug-related information,whether this information relates to their craving state or to theevaluation of the positive aspects of being high on drugs orusing drugs. However, alcoholics who are currently attemptingto abstain from drinking seem to be interfered with in theirprocessing of alcohol-related information. This may be due totheir current concern over their drinking problems andattempted abstinence. Another possible explanation may bedue to the manifestation of a reactive emotional state such asanxiety; similar findings are well established in the field ofanxiety research where a range of tests have shown delayedprocessing of anxiety-related automatic thoughts (Weinsteinand Nutt, 1995). Indeed, many of our patients with late onsetdrinking problems tended to drink in order to deal with theiranxiety and attempting abstinence may increase anxiety. Apsychological test which primes or activates thoughts aboutcraving may enhance anxiety and pre-occupation with suchissues.
Finally, there may be a link between cognitive processingand personality. In polydrug users there is evidence thatimpulsivity was significantly correlated with craving and thepotentially rewarding consequences of opiate use (powell et al.,1992). In alcohol, there is growing evidence for subtypes ofalcoholism with the best established nosology being that ofCloninger (1987) who suggests two distinct group, Type 1being late onset alcoholics who start having problems withdependence after the age of 25 years and who often drink toreduce stress or anxiety. Type 2 alcoholics in contrast, showearly onset of use with associated criminal behaviour andimpulsive personality traits.
It is possible that the interference (rather than facilitation) inthe processing of alcohol-related words was associated withpersonality factors as well as cognitive mechanisms. However,since we have not assessed personality and family variablesdirectly, this suggestion is a tentative one. Figure 4 illustratesideas for the possible mechanisms underlying opiate andalcohol dependence.
A. WEINSTEIN et al,
Compulsive Impulsive
Antisocial PO
/Type Ialcoholism/
~11alcoholismOpiate addicts?
teuphoria• anxiety
Figure 4 Possible paths linking personality Type 1 and Type 2alcoholics, anxiety and drug use
These studies have implications for cogmtrve models ofinformation processing of emotional disorders in general andin the addictions in particular. Our studies describe theprocessing of automatic thoughts and beliefs but we do notargue that our findings support the argument that craving inthe addict is an automatic process. Though we used typicalautomatic thoughts of craving in our patient sample, they hadample time to process this information above the threshold ofawareness. In this way, such processing would not be regardedas 'subliminal' or 'automatic'. Our studies therefore do notrefute Tiffany's (1990) hypothesis which suggested that cravingis a non-automatic cognitive process. Future studies may testthis hypothesis by using 'subliminal' 'automatic' cognitivetasks. Furthermore, there are inherent limitations in cognitivetasks that measure facilitation or interference in processing ofcondition-related information in patients. Investigating prim-ing to threat has yielded conflicting and confusing results overthe past few years (MacLeod and Mathews, (991). There isalready absence of clear evidence of either facilitation orinhibition of lexical priming to panic-related or social phobicwords (Cloitre et al., 1992). There is a need for further studieson cognitive processing in addictions in order to clarify theseissues. In the meantime, any findings of contextual priming orinterference should be interpreted with caution.
The imagery of craving experiencesIn addition to studies of cognitive processing of thoughts andbeliefs in addicted individuals we have also begun to explorethe deeper 'layer' of the experience of craving as such using theapproach of Bradley and Moorey (1988). They showed in aseries of single case studies that cue-exposure craving can beassociated with vivid imagery of drug-taking. One of theirsubjects imagined herself preparing for drug-taking andshooting-up. The image appeared to act as a trigger forimagery of drug-taking and she would visualize it being used inthe preparation or ingestion of heroin. Another subject had animage of the kitchen in his house where he habitually usedheroin, an image which would be sufficient to provoke craving.Recently, Tiffany and Drobes (1990) have shown that it ispossible to elicit strong urges to smoke cigarettes in smokers by

COGNITIVE AND PHYSIOLOGICAL ASPECTS OF CRAVING 35
of control over using heroin. We used this measure since itovercomes the major limitations of previous craving assess-ments which were based on a single-item VAS. As pointed outby Tiffany (1992), the use of only one or two items for the VASmay result in low reliability and validity. A variety of itemsmay allow the identification of the various aspects of drugaddiction such as desire, intention, positive and negativeexpectancies and control over drug use. We did not use thisquestionnaire prior to the imagery exercise in order to preventany priming effects. Our observations in the laboratory in aprevious study have suggested that the HCQ affected subjects'mood (unpublished data).
Figure 5 shows ratings on VASs for all scripts in drug-freesubjects, the first experiment after the drug-related, neutraltalking and imagery. The analysis of ratings using theWilcoxon test demonstrated an increase in ratings of craving(W= 16; p<0.05) and urges (W=21; p<0.05) for the cravingscripts compared with the neutral scripts in alf subjects. Thisincrease was followed by a significant increase in ratings forsadness for the craving scripts compared with neutral scripts(W=21; p<0.05) in all subjects.
using imagery scripts containing descriptions of smokingurges. This was indicated by ratings of self-reported urges. Ina further study, Elash et al. (1995) used a brief imageryprocedure which included sentences with varying affectivecontent with or without smoking urges in smokers. They haveshown that smoking-cue sentences produced augmented urgesand startle responding in their subjects. Particularly, in thepositive affect manipulation, heart rate was higher in thesmoking-cue condition than in the no-smoking-cue condition,indicating a link between positive affect autonomic arousaland urges to smoke.
In the following series of studies, we investigated the effectsof imagery in drug-taking experience on ratings of craving inopiate addicts, but with the addition of physiological measures(heart rate and the new technique of continuous bloodpressure recording) in an attempt to produce a more objectivemeasure of craving. There is substantial evidence for changesin autonomic responses (such as heart rate, blood pressure andskin conductance) as a result of exposure to drug-relatedstimuli (see review by Niaura et al., 1988 on reactivity toalcohol and cigarettes and Childress et al., 1986 a,b, 1987, 1988on reactivity to opiates). However, in opiate dependence thereis no evidence of an association between craving, imagery andsuch arousal. The physiological measures were performedusing the Finapres apparatus which uses a small cuff on onefinger and gives a continuous measure of both systolic anddiastolic blood pressure plus heart rate and can also be used tomeasure the variability of each of these parameters (Couplandet al., 1995). Our prediction was that imagery of craving wouldbe associated with an increase in arousal, shown by greaterheart rate and possibly blood pressure to these imagescompared with imagery of neutral scenes. In the first study,we explored the basic paradigm of imagery together withautonomic measures. Since this is a paradigm which subse-quently led to our further studies of imagery and craving wewill describe it in detail. Our first group of subjects had beenaddicted to heroin for the past 1-3 years and had been drug-free for at least a year. There were five males and one female inthis sample and their mean age was 36.75 (SD=7 years). Aninitial Finapres recording of baseline during 5 min of rest wastaken. Subjects were then requested to describe an ordinarypleasurable leisure activity for 2 min after which they wereinstructed to close their eyes and continue to imaginethemselves in this situation for a further 2 min. Theexperimenter requested them to stop then and after 2 minrest they were requested to describe a situation in which theyexperienced a strong craving for opiates. Again, they wererequired to describe their experiences for a further 2 min andthen to close their eyes and continue to imagine themselves inthis situation for a further 2 min. They were then requested torest and the recording equipment was removed.
Subjects then rated their scripts (ratings 0-100) on a visualanalogue scale (VAS) for measures of vividness, craving, urges,sadness, anxiety and happiness. Immediately after imagery ofcraving subjects completed the Heroin Craving Questionnaire(HCQ; S. T. Tiffany, in preparation). This seven-point ques-tionnaire was validated in a sample of 230 heroin users whowere not attempting to cease using heroin. The questionnaireassessed desire to use heroin, intention to use heroin, positive-outcome expectancies, relief of withdrawal symptoms and lack
80
70~0 600-,-'-'"'eo 50c::
'"~40
30
20
10
o1 2 3 4 5 6
vividness craving urges sadness anxiety happiness
Conditions
Figure 5 Ratings of imagery scripts (neutral and craving) of all visualanalogue scale items by opiate-abstinent subjects who werepreviously dependent. Error bars show standard deviations. *,Significant and 5 percent level
Figure 6 shows mean scores on all subscales of Tiffany'sHCQ in all subjects. The HCQ was not used before theimagery exercise in order to prevent possible priming effects,hence the ratings are not compared to baseline. However, it isinteresting to note ratings of lack of control over drug use andavoidance of withdrawal on the scale and to compare these

36
7
• Desire
6 III Intention
I!I Positive
[] Relief....•
S 0 Controli=?~ 4C/)OJC
Cii 3a:
2
0-+-----Factors of the HCQ
Figure 6 Ratings on all factors of the Heroin Craving Questionnaire(HCQ) by opiate abstinent subjects who were previously dependent.Error bars show standard deviations
norms to those of opiate addicts undergoing detoxification(Weinstein et al., 1997).
Subjects showed a significant increase in mean arterialpressure during drug-related talking (128.8 mmHg) comparedwith neutral talking (123.3 mmHg) when individual beat-by-beat pressure values over 2 min were compared by means of apaired Wilcoxon test [W(I,6)=21;p<0.05].
The results of this study provided preliminary evidence thatimagery is powerful in induction of craving for opiates asindicated by subjective ratings and by autonomic arousal.Though some of the reported increase in mean arterial pressureis probably due to the breathing changes experienced intalking, some of the observed effect was probably due tospecific arousal while describing personal craving experiences.However, the observed effects were demonstrated in compar-ison with neutral talks and were also seen in the case ofimagery per se (without talking). It is interesting in this contextthat cocaine administration itself raises blood pressure by onlyabout 15 mmHg (Foltin et al., 1988), therefore the effect onblood pressure of imagery is quite high compared with the 'realthing'.
Our findings supports previous studies reviewed byChildress et aI., (1986 a,b) which suggested that opioid-relatedstimuli (such as drug 'works') are powerful in elicitingautonomic conditioned responses. Our imagery techniqueused a different source of stimuli which consisted of thesubjects' own images (interoceptive cues) as a source foreliciting such responses. In fact our subjects reported that theywere more emotionally affected by their own previousexperiences compared to videotapes we had used in earlierexperiments to induce craving, these showed other peopleinjecting or smoking heroin. Our procedure could possibly beused as cue exposure for the extinction of craving.
There are some limitations of this study, the main ones beingthe fixed order of presentation of the stimuli and the reliabilityof heart rate as a measure of cue reactivity. Only one order of
A. WEINSTEIN et al.
presentation was used in this experiment. The order wastalking and imagery of neutral experiences first, followed bytalking and imagery of craving. This was done in order toprevent any effect of craving imagery over neutral imagery (ifthe order was reversed). It is therefore difficult to assess thedifferent contribution of each component of the neutral scripte.g. talking and imagining to craving imagery reactivity. Thereare further limitations in predicting increases in heart rate forcue-related scripts in addiction. In smoking urges research,Tiffany and Hakenewerth (1991) originally reported increasedheart rate in their smokers during urge imagery scriptscompared with neutral imagery scripts. However, in ourstudy, unlike systolic blood pressure, heart rate effects weremodest.
In the second study, Weinstein et al. (1997) repeated thisprocedure with opiate addicts undergoing detoxification.Thirteen opiate addicts in detoxification went through thesame procedure of active imagery whilst connected to theFinapres. As before, subjects displayed a significant increase insystolic blood pressure and heart rate while describing drugcraving compared with neutral descriptions. Furthermore, anincrease in systolic blood pressure during imagery of cravingdescriptions compared with neutral descriptions was observed.These results supported the evidence of the first study thatimagery is powerful in eliciting craving for opiates as indicatedby subjective ratings and autonomic measures. All the HCQsubscales were rated higher than those of abstinent ex-opiateaddicts reported in the first study. This is because this grouphad been abstinent for a very short time (less than 2 weeks)compared to the first group (up to a year). There were otherinteresting associations between cognitive and physiologicalfactors in the second study. We found evidence to supportcognitive models of 'self efficacy' and 'outcome-expectancies'of addiction. We discovered a significant positive correlation(Spearman 1'=0.758; p<O.OI) between urge and crave ratingson the VAS after the imagery exercise and the scores on lowself-efficacy (the lack of control sub scale on the HCQ).Furthermore, the objective measure of craving; increase insystolic blood pressure during the craving talk, was associatedpositively with ratings on the positive outcome expectanciessub scale on the HCQ (Spearman r =0.558; P <0.05).
Imagery and positron emission tomography(PET) imaging of craving experiencesOne reason for developing a method of craving induction wasto use it to identify the brain circuits which subserve this stateusing PET imaging. We have utilized the well-established 015_
labelled water technique to measure regional cerebral bloodflow during craving and control periods. Subjects are scannedwhilst they listen to their own scripts of craving and neutraldescriptions. The radiotracer is injected just after the start ofthe script and the brain is scanned for the next 90 sec. Eachscript is repeated six times in randomized order which gives apowerful statistical design. The VAS (vividness, craving, urges,anxiety, sadness and happiness) were rated after each script sochanges in these can be covaried with changes in rCBF, thusallowing the circuits subserving each component to beidentified. So far six patients have been successfully studied,

COGNITIVE AND PHYSIOLOGICAL ASPECTS OF CRAVING 37
a tendency to habituate and a progressive slowing of heart ratethroughout the experiment.
Our preliminary results from the PET imaging study(Weinstein et al., 1996a) in subjects who were previouslyopiate-dependent and responsive to the induction of urges touse heroin showed activation of several regions of interest suchas the basal ganglia, cerebellum and the hippocampus (see Fig .8). Of particular interest is the urge-related activation in thebasal ganglia, a region that shows similar metabolic increaseswith urges such as those seen in obsessive-compulsive disorder(Baxter et aI., 1992). Another important region of interestactivated was the left hippocampal gyrus, an area which isknown to be sensitive to contextual cues. Although these arepreliminary findings and should be interpreted with caution,we hope that further studies will illuminate the circuits ofmemory that are associated with the activation of craving foropiates and other drugs.
100
*9S
-----S 90
2-..•...•II)•... 8S<1:S...•......<1:SII) 80..c=
75
70
craving tape *
*neutral tape -
6
session no.iO 11 12
Figure 7 Habituation of heart rate responses to craving scripts duringpositron emission tomography scanning in a typical subject. In thescanner responses were presented at random whereas here they arepresented in ascending order Conclusion
Craving is a complex psychological and motivational statewhich has physiological manifestations. We have attempted tounderstand craving by using cognitive techniques and physio-logical measurements. Our findings in the laboratory help toilluminate the complexity of the craving state. There seem to bevarious cognitive levels of processing of addiction-relatedinformation. These include addiction-related words (superficial
of whom four showed a significant degree of craving in thescanner, thus allowing the brain circuits activated during thisstate to be identified. Figure 7 shows a single subject scannerrecording immediately after detoxification. The data demon-strates a consistent elevation of heart rate during the cravingscans compared with the neutral scans although these showed
VPC'lACcorono!
-104 68 trons· ...'ersEpositive correlation craving(A)
VPC vP.CsaqlHol coronol
-104 68 transverSEurge
positive covariates(8)
Figure 8 Scanning proton microscope maps of regions which show positive correlations between (A) rCBF increases and (B) craving/urges to use drugs

38
encoding), thoughts and beliefs about drug craving and druguse and elaborate images of drug craving experiences. We havealready generated some data which suggest that opiate addictsprocess craving-related information differently from alco-holics. This evidence lends support to the idea thataddictions are not homogenous constructs and may be theconsequence of, or at least related to, different cognitiveresponse mechanisms. Further work is required to substantiatethis early observation. We are aware of the limitations inlinking the concept of craving to actual addictive behaviour,drug use and relapse. We hope that future research will help usto understand the concept of craving and its association withdrug use behaviour.
AcknowledgementsCombining these various aspects of craving has only been possible
because of the multi-disciplinary collaboration of psychologists,psychopharmacologists and clinicians. We are grateful to ourclinical colleagues, Judy Miles, Fergus Law and Helen Cotteefrom the Avon Drug Problem Team, Simon Britten and SteveBarnes from the Weston Area Health Authority and ColinBrewer from the Stapleford Centre who provided access topatients and to the Medical Research Council and South WestRegional Health Authority who funded this research.
Address for correspondenceA.WeinsteinThe Psychopharmacology UnitSchool of Medical SciencesUniversity WalkUniversity of BristolBristol BS81TD, UKEmail: [email protected]. uk
ReferencesAmerican Psychiatric Association (1994)Diagnostic and statistical
manual of mental disorders, 4th edn. American Psychiatric Asso-ciation, Washington, DC
Baxter L R, Schwartz J M, Bergman K, Szuba M P, Guze B H,Mazziota, J C (1992)Caudate glucose metabolic rate change withboth drug and behaviour therapy for obsessive compulsivedisorder. Archs Gen Psychiat 49: 681-689
Bradley P B, Moorey S (1988)Extinction of craving during exposureto drug-related cues: three single case reports. Behav Psychother16:45-56
Childress A R, McLellan AT, O'Brien CP (1986a).Abstinent opiateabusers exhibit conditioned craving, conditioned withdrawal andreductions in both through extinction. Br J Addict 81:655-660
Childress AR, McLellan AT, O'Brien CP (1986b) Conditionedresponses in methadone population-a comparison of labora-tory, clinic and natural settings. J Substance Abuse Treat 3: 173-179
Childress A R, McLellan AT, Ehrman R, O'Brien C P (1987)Extinc-tion of conditioned responses in abstinent cocaine or opioidusers. In Problems of drug dependence, NIDA Research Mono-graph 76. US Government Printing Office, Washington, DC,pp.189-195
Childress A R, McLellan AT, O'Brien C P (1988)Classically condi-tioned responses in cocaine and opiate dependence: a role inrelapse? In Ray B (ed.), Learning factors in drug dependence,
A. WEINSTEIN et al.
NIDA Research Monograph 84. Government Printing Office,Washington, DC, pp. 25-43
Clark D M, Salkovskis PM, Gelder M, Koehler C, Martin M,Anastasiades P, Hackman A, Middleton H, Jeavons A (1988)Tests of a cognitive theory of panic. In Hand I, Wittchen H U(eds), Panic and phobias, Vol.2. Springer-Verlag, Berlin
Cloitre M, Heimberg RG, Holt CS, Leibowitz MR (1992)Reactiontime to threat stimuli in panic disorder and social phobia. Beha-viour Res Ther 30: 609-617
Cloninger CR (1987)Neurogenetic adaptive mechanisms in alco-holism. Science 236: 410-416
Coupland N J, Bailey J E,Wilson S J, Horvath R, Nutt D J (1995)Theeffects of clonidine on cardiovascular responses to standing inhealthy volunteers. Clin Autonom Res 5: 171-177
Elash CA, Tiffany ST, Vrana SR (1995)Manipulation of smokingurges and affect through a brief-imagery procedure: self-report,psychophysiological and startle probe responses. Exp ClinPsychopharmac 3: 156-162
Feldtkeller B, Weinstein A, Jones B, McMahon J, Nutt D J (1997)Contextual priming to craving in alcohol dependent patients. JPsychopharmac 11(Suppl.): A15, 59
Foltin R W, McEntee M A, Capriotti R M, Pedroso J J, FischmanM W (1988) Effects of cocaine, alone and in combination withtask performance, on heart rate and blood pressure. PharmacBiochem Behav 31:387-391
MacLeod C, Mathews A (1991) Biased cognitive operations inanxiety: accessibility of information or assignment of processingpriorities. Behav Res Ther 29: 599-610
Niaura SR, Rohsenow DJ, Binkoff JA, Monti PM, Pedraza M,Abrams DB (1988)Relevance of cue reactivity to understandingalcohol and smoking relapse. J Abnorm Psychol 97:133-152
Powell J, Bradley B, Gray J A (1992) Classical conditioning andcognitive determinants of subjective craving for opiates: an inves-tigation of their relative contributions. Br J Addict 87:1133-1144
Stockwell T, Hodgson R, Edwards G,Taylor C, Rankin H (1979)Thedevelopment of a questionnaire to measure severity of alcoholdependence. Br J Addict 74:79-87
Tiffany ST (1990) A cognitive model of drug urges and drug-usebehaviour: role of automatic and non-automatic processes.Psychol Rev 97:147-168
Tiffany S T (1992) A critique of contemporary urge and cravingresearch: methodological, psychometric, and theoretical issues.Adv Behav Res Ther 14:123-139
Tiffany S T, Drobes D J (1990) Imagery and smoking urges: themanipulation of affective content. Addict Behav 15:531-539
Tiffany S T, Hakenwerth D M (1991) The production of smokingurges through an imagery manipulation: psychophysical andverbal manifestations. Addict Behav 16: 389-400
Weinstein A M, Nutt D J (1995)Do anti-depressants (SSRIs) amelio-rate cognitive dysfunction in anxiety? J Psychopharmac 9: 83-89
Weinstein A M, Malizia A,Wilson S, Bailey J E, Britten S, Brewer C,Nutt D J (1996a)Imagery and PET imaging of craving experiencesin abstinent opiate addicts, NIDA Research Monographs 85, USGovernment Printing Office,Washington DC
Weinstein A M, Neal L, Lillywhite A, Potokar J and Nutt D J (1996b)Cognitive processing in PTSD. Anxiety 2: 130-139
Weinstein A M, Myles J, Wilson S, Bailey J, Nutt D J (1996c) Theprocessing of automatic thoughts, outcome-expectancies andpersonal experiences in craving of opiate addicts. Presented atthe Addiction 96 Symposium, Hilton Head Island
Weinstein A M, Wilson S, Bailey J E, Myles J, Nutt D J (1997)Imagery of craving in opiate addicts undergoing detoxification.Drug Alcohol Depend 48: 25-31
Williams J M G,Watts F N, MacLeod C, Mathews A (1988)Cognitivepsychology and emotional disorders. Wiley,NewYork