Integrating Genetics and Genomics in Primary Aldosteronism
10
Brief Reviews Integrating Genetics and Genomics in Primary Aldosteronism Maria-Christina Zennaro, Xavier Jeunemaitre, Sheerazed Boulkroun P rimary aldosteronism (PA) is the most common form of secondary hypertension, with an estimated prevalence of 10% in referred patients and 4% in primary care 1,2 but as high as 20% in patients with resistant hypertension. 3,4 It is characterized by hypertension with low plasma renin and elevated aldosterone that is often seen with hypokalemia. PA occurs as a result of a dysregulation of the normal mechanisms controlling adrenal aldosterone production. The 2 major causes are aldosterone-producing adenomas (APAs) and bilateral adre- nal hyperplasia (BAH), also called idiopathic hyperaldoste- ronism. The early detection of PA has an enormous impact on clinical outcome and survival, given the major cardiovascular adverse effects of aldosterone excess, which are independent of blood pressure, 5,6 and predict outcome after surgical treatment. 7,8 Patients with PA have a significantly higher risk of nonfatal myocardial infarction, atrial fibrillation, and stroke compared with age-, sex-, and blood pressure–matched essential hypertensives. 5 Furthermore, changes in cardiac structure and function 9 and partially reversible renal dysfunc- tion 10 have been described, whereas the increased occurrence of metabolic abnormalities in patients with PA is still a matter of debate. 11,12 Although the 2008 guidelines for the management of PA have been pivotal for homogenizing screening procedures and treatment among specialized centers, 13 there remain a few critical issues related to diagnosis, subtype differentia- tion, and treatment of nonsurgically correctable forms. Reli- able diagnostic and prognostic biomarkers are lacking for more sensitive and specific screening, as well as new thera- peutic avenues, because medical and/or surgical treatment of PA leads to normotension in only a minority of patients. This may come from a better understanding of the pathogenic mechanisms of the disease, in particular, identification of the genetic and molecular determinants leading to the develop- ment of APA and BAH. Over the last few years, considerable efforts have been made to this end by different groups, taking advantage of developments in high-throughput “omics” tech- nologies, in particular transcriptomics, and more recently new generation exome sequencing, together with genetically mod- ified mouse models. This review summarizes our current knowledge on the genetics (genes and their roles in inheri- tance) and genomics (genome-wide studies addressing vari- ations in gene structure and expression) of PA, in both familial and sporadic forms of the disease, trying to integrate genetic abnormalities and gene dosage effects into a patho- physiological perspective related to aldosterone production and cell proliferation. Genetic Forms of PA Although the majority of PA is apparently sporadic, 3 familial forms displaying mendelian inheritance have been described. Familial hyperaldosteronism (FH) 1, also called glucocorticoid- suppressible aldosteronism, was first described 50 years ago. 14 The disorder is characterized by early and severe hyperten- sion, most often before the age of 20 years, in subjects with biochemical abnormalities of PA of variable intensity and in some cases adrenal nodules. 15 FH-1 is inherited as an autosomal dominant trait and is characterized by significant production of hybrid steroids (18-hydroxycortisol and 18- oxocortisol) and normalization of aldosterone levels and blood pressure with low doses of dexamethasone. 16 The condition reflects the presence of a hybrid gene resulting from unequal crossing over between the adjacent highly homologous genes CYP11B2 and CYP11B1 on chromosome 8q21-q22, coding for aldosterone synthase and steroid 11- hydroxylase. 17,18 Fusion of the promoter region of CYP11B1 to the coding region of CYP11B2 produces a chimeric gene, with activity of aldosterone synthase, but tissue specificity and regulation that of 11-hydroxylase, so that the synthesis of aldosterone is under control of adrenocorticotropic hor- mone rather than plasma potassium concentrations and the renin-angiotensin system. Although the prevalence of FH-1 in patients with PA has been reported previously to be 0.36%, 19 more recent studies, including large cohorts of patients with PA, set the prevalence of FH-1 between 0.66% and 1.00%. 20,21 Prevalence as high as 3.1% has been reported recently in a hypertensive pediatric population. 22 FH-2 also reflects autosomal dominant transmission, but not associated with a hybrid gene and with hyperaldosteron- ism not suppressible by dexamethasone. 23 The phenotype is variable from APA to BAH, with a variable response of Received April 13, 2012; first decision April 28, 2012; revision accepted June 20, 2012. From the Institut National de la Santé et de la Recherche Médicale (M.-C.Z., X.J., S.B.), UMRS 970, Paris Cardiovascular Research Center, Paris, France; Université Paris Descartes (M.-C.Z., X.J., S.B.), Sorbonne Paris Cité, Paris, France; Assistance Publique-Hôpitaux de Paris (M.-C.Z., X.J.), Hôpital Européen Georges Pompidou, Paris, France. Correspondence to Maria-Christina Zennaro, Institut National de la Santé et de la Recherche Médicale, U970, Paris Cardiovascular Research Center-PARCC, 56 rue Leblanc, 75015 Paris, France. E-mail [email protected] (Hypertension. 2012;60:580-588.) © 2012 American Heart Association, Inc. Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.111.188250 580 by guest on April 18, 2016 http://hyper.ahajournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Integrating Genetics and Genomics in Primary Aldosteronism

Brief Reviews
Integrating Genetics and Genomics inPrimary Aldosteronism
Maria-Christina Zennaro, Xavier Jeunemaitre, Sheerazed Boulkroun
Primary aldosteronism (PA) is the most common form ofsecondary hypertension, with an estimated prevalence of
�10% in referred patients and 4% in primary care1,2 but ashigh as 20% in patients with resistant hypertension.3,4 It ischaracterized by hypertension with low plasma renin andelevated aldosterone that is often seen with hypokalemia. PAoccurs as a result of a dysregulation of the normal mechanismscontrolling adrenal aldosterone production. The 2 major causesare aldosterone-producing adenomas (APAs) and bilateral adre-nal hyperplasia (BAH), also called idiopathic hyperaldoste-ronism. The early detection of PA has an enormous impact onclinical outcome and survival, given the major cardiovascularadverse effects of aldosterone excess, which are independentof blood pressure,5,6 and predict outcome after surgicaltreatment.7,8 Patients with PA have a significantly higher riskof nonfatal myocardial infarction, atrial fibrillation, andstroke compared with age-, sex-, and blood pressure–matchedessential hypertensives.5 Furthermore, changes in cardiacstructure and function9 and partially reversible renal dysfunc-tion10 have been described, whereas the increased occurrenceof metabolic abnormalities in patients with PA is still a matterof debate.11,12
Although the 2008 guidelines for the management of PAhave been pivotal for homogenizing screening proceduresand treatment among specialized centers,13 there remain afew critical issues related to diagnosis, subtype differentia-tion, and treatment of nonsurgically correctable forms. Reli-able diagnostic and prognostic biomarkers are lacking formore sensitive and specific screening, as well as new thera-peutic avenues, because medical and/or surgical treatment ofPA leads to normotension in only a minority of patients. Thismay come from a better understanding of the pathogenicmechanisms of the disease, in particular, identification of thegenetic and molecular determinants leading to the develop-ment of APA and BAH. Over the last few years, considerableefforts have been made to this end by different groups, takingadvantage of developments in high-throughput “omics” tech-nologies, in particular transcriptomics, and more recently newgeneration exome sequencing, together with genetically mod-ified mouse models. This review summarizes our current
knowledge on the genetics (genes and their roles in inheri-tance) and genomics (genome-wide studies addressing vari-ations in gene structure and expression) of PA, in bothfamilial and sporadic forms of the disease, trying to integrategenetic abnormalities and gene dosage effects into a patho-physiological perspective related to aldosterone productionand cell proliferation.
Genetic Forms of PAAlthough the majority of PA is apparently sporadic, 3 familialforms displaying mendelian inheritance have been described.Familial hyperaldosteronism (FH) 1, also called glucocorticoid-suppressible aldosteronism, was first described �50 years ago.14
The disorder is characterized by early and severe hyperten-sion, most often before the age of 20 years, in subjects withbiochemical abnormalities of PA of variable intensity and insome cases adrenal nodules.15 FH-1 is inherited as anautosomal dominant trait and is characterized by significantproduction of hybrid steroids (18-hydroxycortisol and 18-oxocortisol) and normalization of aldosterone levels andblood pressure with low doses of dexamethasone.16 Thecondition reflects the presence of a hybrid gene resultingfrom unequal crossing over between the adjacent highlyhomologous genes CYP11B2 and CYP11B1 on chromosome8q21-q22, coding for aldosterone synthase and steroid 11�-hydroxylase.17,18 Fusion of the promoter region of CYP11B1to the coding region of CYP11B2 produces a chimeric gene,with activity of aldosterone synthase, but tissue specificityand regulation that of 11�-hydroxylase, so that the synthesisof aldosterone is under control of adrenocorticotropic hor-mone rather than plasma potassium concentrations and therenin-angiotensin system. Although the prevalence of FH-1 inpatients with PA has been reported previously to be�0.36%,19 more recent studies, including large cohorts ofpatients with PA, set the prevalence of FH-1 between 0.66%and 1.00%.20,21 Prevalence as high as 3.1% has been reportedrecently in a hypertensive pediatric population.22
FH-2 also reflects autosomal dominant transmission, butnot associated with a hybrid gene and with hyperaldosteron-ism not suppressible by dexamethasone.23 The phenotype isvariable from APA to BAH, with a variable response of
Received April 13, 2012; first decision April 28, 2012; revision accepted June 20, 2012.From the Institut National de la Santé et de la Recherche Médicale (M.-C.Z., X.J., S.B.), UMRS 970, Paris Cardiovascular Research Center, Paris,
France; Université Paris Descartes (M.-C.Z., X.J., S.B.), Sorbonne Paris Cité, Paris, France; Assistance Publique-Hôpitaux de Paris (M.-C.Z., X.J.),Hôpital Européen Georges Pompidou, Paris, France.
Correspondence to Maria-Christina Zennaro, Institut National de la Santé et de la Recherche Médicale, U970, Paris Cardiovascular ResearchCenter-PARCC, 56 rue Leblanc, 75015 Paris, France. E-mail [email protected]
(Hypertension. 2012;60:580-588.)© 2012 American Heart Association, Inc.
Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.111.188250
580 by guest on April 18, 2016http://hyper.ahajournals.org/Downloaded from

aldosterone to angiotensin II (Ang II). Clinical and biologicalfeatures of FH-2 are indistinguishable from sporadic PA, andFH-2 is diagnosed on the basis of �2 affected members in afamily, however, with phenotypic variability within affectedfamilies typical for the disease.20,21 The prevalence of FH-2 isestimated to be between 2.8% and 6.0% in adult populationswith PA.20,21,23 In a large family with FH-2, a locus associ-ated with the disease has been mapped to chromosome7p22,24 although no causal mutations have been identified inany of the genes located in the linkage area thus far. We haveexplored in depth the family history of 350 index cases in ourPA database.20 In this study, 12 families (4%) had criteriasuggestive of FH-2, with �2 affected first-degree relatives.The distribution of the affected subjects within the familieswas compatible with an autosomal dominant trait, with a highnumber of hypertensives in additional family members, suggest-ing the possibility of other unrecognized cases. Analysis ofpositional candidates located at chromosome 7p22 showed nomutations on the genes coding for fascin 1 (FSCN1) and thecAMP-dependent protein kinase type I-� regulatory subunit(PRKAR1B).20
Candidate gene approaches to study the genetic basis ofFH-2 and sporadic PA have included genes involved insteroidogenesis or in familial cancer syndromes.25 In sometumors, loss of heterozygosity was found at chromosome11q13 harboring the MEN1 locus, which is a tumor suppres-sor gene responsible for multiple endocrine neoplasia type 1,characterized by adenomas of the adrenal cortex in 30% ofcases.26,27 In patients experiencing FH-2, as well as inpatients with sporadic APA, no genetic abnormality has beenidentified in genes coding for aldosterone synthase (CYP11B2),the Ang II type 1 receptor (AT1R), or the tumor suppressor genep53 (Reference 28 and references therein). However, a higherpercentage of a particular allele of the CYP11B2 gene (�344T)was found in hypertensive patients with elevated aldosterone torenin ratio, which is compatible with PA.27
More recently, a third form of familial hyperaldosteronism,referred to as FH-3, was reported in a family with severe,early-onset hypertension resistant to treatment.29 Affectedfamily members showed hyporeninemia, hyperaldosteronism,and very high levels of the hybrid steroids 18-oxocortisol and18-hydroxycortisol but no suppression of aldosterone produc-tion by dexamethasone. Early bilateral adrenalectomy wasrequired to correct blood pressure, showing dramatic enlarge-ment of the adrenals with massive hyperplasia of the cortex.The genetic basis of FH-3 has been elucidated recently (seebelow).
From Physiological to PathologicalAldosterone ProductionIn the adrenal cortex, cortisol and aldosterone are synthesizedby the isozymes steroid 11�-hydroxylase (encoded byCYP11B1) and aldosterone synthase (encoded by CYP11B2),respectively. 11�-Hydroxylase catalyzes the 11�-hydroxylationof 11-deoxycortisol to cortisol and of 11-deoxycorticosterone tocorticosterone. Aldosterone synthase catalyzes the 11�-hydroxylation of 11-deoxycorticosterone to corticosterone, 18-hydroxylation of corticosterone to 18-hydroxycorticosterone,and 18-oxidation of 18-hydroxycorticosterone to aldosterone in
the zona glomerulosa (ZG). Aldosterone production is tightlycontrolled to maintain electrolyte and fluid homeostasis by thekidney. Thus, the 2 most important physiological stimuli ofaldosterone secretion are Ang II and serum potassium. The keyplayer in regulating aldosterone biosynthesis is calcium (Ca2�)signaling. Stimulation of glomerulosa cells by Ang II or potas-sium results in depolarization of the ZG cell membrane andopening of voltage-dependent Ca2�-channels, leading to anincreased intracellular Ca2� concentration. Ang II also signalsthrough the Ang II type 1 receptors to stimulate inositoltrisphosphate–dependent Ca2� release from the endoplasmicreticulum.30 Activation of the calcium signaling pathway trig-gers a phosphorylation cascade, involving calmodulin andcalmodulin-dependent kinase I/IV, ultimately leading to theactivation of transcription factors (ie, Nurr1 and NGF1B) thatpositively regulate the transcription of CYP11B2.
Different studies have explored gene expression changes inAPA, investigating relevant candidate genes and more re-cently using pangenomic approaches. Among the candidategenes, those coding for steroidogenic enzymes in the adrenalgland have been intensively investigated (Table 1). Usingvarious techniques, several studies have thus reported in-creased expression of CYP11B2 in APA compared withnormal adrenals or peritumoral adjacent cortex31–36 (through-out this review, “adjacent cortex” refers to the entire cortexof an adrenal gland harboring an APA). In addition toCYP11B2, expression of CYP21A2 (coding for steroid21-hydroxylase, responsible for the conversion of proges-terone into 11-deoxycorticosterone) has been found to beconsistently increased in APA,37,38 whereas mRNA levelsof CYP11B1 were decreased,32,38 and there were no changesin CYP11A1 expression.36
Remarkably enough, these studies also revealed a relativeheterogeneity in terms of gene expression. In particular,HSD3B2 (encoding 3�-hydroxysteroid dehydrogenase re-sponsible for the conversion of pregnenolone into progester-
Table 1. Changes in Steroidogenesis Pathway in APA
Gene Name (Protein)Expression
in APA References
Steroidogenic enzymes
CYP11B2 (aldosterone synthase) 1, ¡, 2 31–33, 36–39
CYP11B1 (steroid 11�-hydroxylase) 2 32, 38
CYP17A1 (cytochrome P450 17A1) 2or ¡ 32, 36, 38, 39
HSD3B2 (3�-HSD II) 1 or ¡ 37, 38
CYP21A2 (steroid 21-hydroxylase) 1 37, 38
CYP11A1 (cytochrome P450[scc]) ¡ 36
Cholesterol and electron supply
SCARB1 (SR-B1) 1 38
ADXR (adrenodoxin reductase) 1 38
POR (NADPH-cytochrome P450 reductase) 1 38
1 indicates increased expression; ¡, unchanged expression; 2, de-creased expression; cytochrome P450(scc), cholesterol side-chain cleavageenzyme, mitochondrial; 3�-HSD II, 3�-hydroxysteroid dehydrogenase/delta5-�4-isomerase type 2; cytochrome P450 17A1, steroid 17�-hydroxylase/17,20 lyase; SR-B1, scavenger receptor class B member 1; APA, aldosterone-producing adenoma.
Zennaro et al Genetics and Genomics of Primary Aldosteronism 581
by guest on April 18, 2016http://hyper.ahajournals.org/Downloaded from

one) has been found to be either increased37 or unchanged inAPA,38 whereas expression of CYP17A1 (coding for thesteroid 17�-hydroxylase/17,20 lyase responsible for the con-version of pregnenolone and progesterone to the respective17�-hydroxylated precursors of glucocorticoids and adrenalandrogens) was either decreased36,38 or unchanged.32 Mostunexpectedly, however, different authors found subsets oftumors with highly heterogeneous expression of CYP11B2either increased, unchanged, or decreased compared withcontrol adrenal tissue.34,36 A very recent transcriptome studyfurther demonstrated the tumor heterogeneity of CYP11B2expression and the correlation of high versus low CYP17A1expression in APA with morphological features, that is,adenomas composed of zona fasciculata–like cells versustumors composed of ZG-like cells, respectively.39
One possible reason for different studies reporting varyingresults in terms of the heterogeneity of CYP11B2 expressionin APA samples may relate to the small number of samplesinvestigated, the different technical approaches used, and/orthe different screening procedures for selecting patients forsurgery. In addition, in some studies APAs were comparedwith adrenal cortices obtained from nephroadrenalectomiesfor renal cancer, whereas others used adjacent adrenal cortexas a control, with both tissues having their own pitfalls (seebelow). An additional reason, however, is most probablyrelated to the real heterogeneity of the molecular phenotypeof APA, reflecting the possibility that modifications indifferent pathways may converge to increase aldosteroneproduction and cell proliferation. This is supported by 2subsequent transcriptome analyses performed in our labora-tory on 123 APA samples and 11 control adrenals, whichshowed a subgroup structure that could reflect distinct patho-genic mechanisms and which was confirmed by functionalpathological investigations.40,41 Nevertheless, CYP11B2 ex-pression appears to be consistently increased, although tovariable extent, among APA samples, with low expression ofCYP11B2 in APA being a rare finding.42
Intracellular Signaling andTranscriptional RegulationIn response to the intracellular increase in Ca2� concentrationinduced by Ang II and K�, the mitochondria rapidly take upCa2�, and a slower activation of calcium/calmodulin depen-dent kinase is observed. The mitochondria play a prominentrole in Ca2� homeostasis by capturing Ca2� when its con-centration rises in the cytosol. The rate-limiting step in steroidbiosynthesis is the conversion of cholesterol to pregnenolone,which occurs in the mitochondria and requires the transfer ofthe substrate from the cytosol across the double membrane.The rise in intracellular Ca2� stimulates both intramitochon-drial cholesterol transfer and the expression of the steroido-genic acute regulatory protein StAR, which promotes thetransport of cholesterol from the outer to the inner mitochon-drial membrane and constitutes the rate-limiting step insteroid hormone biosynthesis.43 Despite its critical role, theexpression of StAR shows only small variations among thedifferent types of adrenal tumors, including APA, cortisol-producing adenomas, and nonfunctional adenomas, comparedwith normal adrenal.37,44 Overexpression of the high-density
lipoprotein scavenger receptor B1 suggests that cholesterolsupply to the cell is increased through the high-density lipopro-tein pathway; increases in adrenodoxin and P450 oxidoreductaseindicate that additional electrons are provided via these 2pathways to both mitochondrial P450 enzymes and enzymeslocated in the endoplasmic reticulum38 (Table 1).
Assié et al38 showed that several genes involved in calciumsignaling were differently expressed between control adrenaland APA, particularly the calcium effector calmodulin andgenes encoding proteins involved in calcium storage, that is,the endoplasmic reticulum calreticulin and the calciumATPase SERCA3. These results indicate an increase incalcium signaling and in intracellular calcium tone. Oneexplanation for the activation of calcium signaling in APAmay be an abnormal expression of G-protein coupled recep-tors triggering chronic calcium activation as one of the initialand critical events responsible for the development of PA.Indeed, in adrenal Cushing syndrome, ectopic peptide hor-mone receptor expression has been demonstrated as the basisfor the excessive glucocorticoid secretion in a subset ofpatients.45 Several analyses demonstrate ectopic expressionof G-protein coupled receptors in some APAs (Table 2),including the 5-HT receptor 4,46,47 the adrenocorticotropic
Table 2. Calcium Signaling and Transcriptional Regulationin APA
Gene Name (Protein)Expression
in APA References
Calcium signaling
CALM2 (calmodulin) 1 38
ATP2A3 (SERCA3) 1 38
G protein–coupled receptors
HTR4 (5-HT4) 1 46, 47
MC2R (ACTH-R) 1 47, 48
LHCGR (LHR) 1 47, 49
HTR7 (5-HT7) 1 47, 50
AGTR1 (AT1R) 1 52, 53
DRD2 (D[2] dopamine receptor) 2 54
GNRHR (GnRH-R) 1 47
GPR37 (endothelin B receptor-like protein 1) 1 47
GRM3 (metabotropic glutamate receptor 3) 1 47
Nuclear receptors and transcription factors
NR4A1 (NGFIB) ¡ 36, 37
NR4A2 (NURR1) 1 or ¡ 36, 37
NR5A1 (SF-1) 1 or ¡ 36, 37, 81
NR0B1 (DAX-1) 1 or ¡ 36, 37
GATA4 (transcription factor GATA-4) 1 37
GATA6 (transcription factor GATA-6) 1 37
NGF1B indicates nerve growth factor 1B; SF-1, steroidogenic factor 1;DAX-1, dosage-sensitive sex reversal-adrenal hypoplasia congenita criticalregion on the X chromosome, gene 1; 5-HT4, 5-hydroxytryptamine receptor 4;ACTH-R, adrenocorticotropic hormone receptor; LHR, luteinizing hormonereceptor; 5-HT7, 5-hydroxytryptamine receptor 7; AT1R, type 1 angiotensin IIreceptor; GnRH-R, gonadotropin releasing hormone receptor; SERCA3, sarco-plasmic/endoplasmic reticulum calcium ATPase 3; 1, increased expression;¡, unchanged expression; 2, decreased expression; APA, aldosterone-producing adenoma.
582 Hypertension September 2012
by guest on April 18, 2016http://hyper.ahajournals.org/Downloaded from

hormone receptor (MC2-R),47,48 the luteinizing hormonereceptor (LHR),47,49 or the 5-HT7 receptor.47,50 It is interest-ing to note that, in vitro, serotonin (5-HT) is able to stimulatealdosterone production through the activation of the 5-HTreceptor 4.51 Overexpression of the Ang II type 1 receptor52,53
and downregulation of the dopamine D2 receptor have also beendescribed.54 In a subset of APAs, overexpression of the putativeendothelin receptor type-like protein (GPR37), the glutamatereceptor metabotropic 3 (GRM3), and the gonadotropin-releasing hormone receptor (GNRHR) has also been described.47
All of these receptors are coupled to different G proteins (Gs,Gq/G11, Gq/Gi, or G12/G13), potentially leading to activation ofdifferent signaling pathways in APAs.
The regulation of steroid biosynthetic enzymes is under thecontrol of several orphan nuclear receptors and transcriptionfactors. The presence of specific response elements has beenreported on the human CYP11B2 promoter, in particular, acAMP response element, also called adrenal 1, a nervegrowth factor-induced clone B (NGFIB) response element(NBRE-1), and Ad4 and Ad5 elements.55 Interestingly,NBRE-1 and Ad5 were found in the 5=-flanking region ofCYP11B2 but not of CYP11B1. The NBRE-1 site is a nuclearreceptor half-site that binds NGFIB family members, whichincludes NGFIB (NR4A1) and NURR1 (NR4A2). The Ad5element represents a direct repeat of 2 nuclear receptorhalf-sites in tandem, which can bind NGFIB family membersSF-1 (NR5A1) and COUP-TF (chicken ovalbumin upstreampromoter-transcription factor), whereas the Ad4 sequence isbound specifically by SF-1, the main transcription factorinvolved in steroidogenesis. SF-1 and DAX-1 (NR0B1) are 2orphan nuclear receptors known to regulate StAR, CYP11A,and CYP17A1. Given that DAX-1 is a known repressor ofSF-1, it has been suggested that, in addition to the level ofexpression of these receptors, it is the SF-1/DAX-1 ratio thatcould be important in regulating adrenal steroid hormoneproduction.55 Although the expression of genes coding forNURR1, SF-1, and DAX-1 has been reported to be increasedor unchanged in APA, investigations into the expression ofGATA4 and GATA6, coding for transcription factors involvedin adrenal cortisol and androgen production through theregulation of CYP17A1 and/or steroid sulfotransferase 2A1(SULT2A1), show increased expression of both37 (Table 2). Itmight well be that, more than modification of expression ofthese transcription factors, the nonappropriate activation of Gprotein–coupled receptors could modulate their phosphory-lation state through different signaling pathways, thus leadingto binding to specific target sequences and activation of genetranscription.
Potassium Channels and the New Era of PAAmong other potassium channels, TWIK-related acid sensi-tive potassium (TASK) channels are highly expressed in theadrenal cortex and are central to the maintenance of themembrane resting potential of ZG cells.56 The functionalrelevance of TASK channels has been highlighted by 2different mouse models both developing hyperaldosteronism,albeit with important pathophysiological differences. Geneticdeletion of Task1 led to depolarization of adrenocortical cellsand to a remarkable ectopic expression of aldosterone syn-
thase in the zona fasciculata of female mice. As a result,female Task1�/� mice display a diet-independent, low renin,and glucocorticoid-remediable form of hyperaldosteronism.57
Neonatal male mice show the same features as females but atpuberty become normal in terms of zonation and steroidsecretion. In Task1/Task3 double knockout male mice, glo-merulosa cells showed no acid-sensitive K� current and werestrongly depolarized. The mice showed low renin hyperaldo-steronism partly responsive to sodium diet, with a phenotypereminiscent of patients with idiopathic primary hyperaldoste-ronism.58 Although these models suggest that hypomorphicalleles of the KCNK3 and KCNK9 genes, coding for TASK1and TASK3, respectively, may play a role in the developmentof PA in humans, sequencing of these genes in 22 patientswith APA,59 as well as in both germinal and somatic DNAfrom a large cohort of patients with PA in our laboratory,60
has not led to the identification of causative mutations.A major advance in our understanding of the pathogen-
esis of PA has recently come from the identification ofrecurrent somatic mutations of the KCNJ5 gene in APA, aswell as germline mutations of the same gene in familieswith FH-3.40,59,61–63 KCNJ5 encodes the G protein–activatedinward rectifier potassium channel Kir3.4. The differentmutations identified in APA (p.G151R and p.L168R) andFH-3 (p.T158A) are all located near or within the selectivityfilter of Kir3.4 and affect the ion selectivity of the channel,with increased sodium conductance leading to chronic mem-brane depolarization. These changes are presumed to beresponsible for the constitutive secretion of aldosterone andfor cell proliferation attributed to the continued opening ofmembrane voltage-dependent calcium channels and activa-tion of the calcium signaling pathway.59 The causal link toaldosterone production has been formally established by Okiet al,64 who demonstrated that expression of channels harbor-ing the inherited p.T158A mutation in adrenal cortical carci-noma cells potentiated aldosterone production both in basalconditions and after stimulation by Ang II. The increase inaldosterone biosynthesis was dependent on membrane depo-larization followed by calcium influx leading to increasedexpression of CYP11B2. In contrast, it remains unclearwhether or how KCNJ5 mutations affect cell proliferation,because expression of mutated channels in 2 different celllines resulted in either reduced cell proliferation64 or rapidsodium-dependent cell lethality.65
Analysis of a large number of patients (380 APA and174 BAH), recruited through referral centers from theEuropean Network for the Study of Adrenal Tumors(ENS@T, www.ensat.org), has shown that somatic KCNJ5mutations are present in a large proportion of APAs, with anestimated prevalence in unselected patients of 34%.40 Evenhigher frequencies have been described, depending on samplesize, screening procedures for selecting patients for adrenal-ectomy, and genetic background.62,63 In contrast, germlinemutations of the KCNJ5 gene are not similarly responsible forsporadic BAH, the most common form of PA in Westerncountries.40 KCNJ5 mutations in APAs appear to be moreprevalent in females than males and in younger patients andare associated with higher preoperative aldosterone levels butnot with therapeutic outcomes after surgery.40 Although an
Zennaro et al Genetics and Genomics of Primary Aldosteronism 583
by guest on April 18, 2016http://hyper.ahajournals.org/Downloaded from

association of KCNJ5 mutations with tumor size has beendescribed in 1 study investigating 73 patients with APA,62
this result has not been replicated in our large cohort ofunselected patients40 or in a recent study from Japan.63
Interestingly, a significant association of genotype with thealdosterone response to upright posture (corresponding to therise in plasma aldosterone from the recumbent to the uprightposition) has been reported in 10 patients.62
Following the first description of a p.T158A KCNJ5mutation in a severe form of FH3, additional mutations andphenotypic variability of FH3 have been reported. In partic-ular, the same p.G151R mutation occurring as a somaticevent in APA was found as an inherited mutation in 2 familieswith early and severe hyperaldosteronism. These patients hadbilateral adrenal cortical hyperplasia and required bilateraladrenalectomy during childhood to control blood pressure.59
Conversely, a second inherited mutation affecting the sameamino acid, p.G151E, was described recently in 3 familieswith a diagnosis of nonglucocorticoid remediable familialhyperaldosteronism.61,65 Remarkably, although this mutationhad similar consequences on channel function as the previ-ously described mutations, it was associated with a much lesssevere phenotype, resembling that of FH-2, with bloodpressure and hypokalemia easily controlled by medicationand no evidence of adrenal hyperplasia.
New Signaling Pathways Contributing toAPA FormationUsing once again a transcriptomic approach, Williams et al66
identified 53 genes differentially expressed between normaladrenals (n�3) and APAs (n�8). Among them, teratocarcinoma-derived growth factor 1 (TDGF-1) was identified as an upregu-lated gene in APA. TDGF-1, also known as Cripto-1, belongsto the epidermal growth factor-Cripto-FRL1-cryptic proteinfamily and plays a key role in early vertebrate developmentand carcinogenesis.67,68 TDGF-1 expression is restricted toZG in normal adrenals, whereas its expression is found in theentire peritumoral adjacent cortex in adrenals with APA.Interestingly, TDGF-1 is localized to nuclei in APAs,whereas it is cytoplasmic in normal adrenal and peritumoraltissue. The possible role of TDGF-1 in APA developmentwas investigated in vitro in the human adrenocortical cell lineNCI H295R. In this model, TDGF-1 activates the Aktsignaling pathway, mediating increased aldosterone secretionand protecting cells from apoptosis. These results suggest adual function of TDGF-1 in APA through deregulation of theAkt signaling pathway.66
In their microarray analysis, the same authors also showedthat visinin-like 1 (VSNL1) was upregulated in APAs.69
VSNL1 belongs to the visinin-like (VSNL) protein subfamilyof neuronal calcium sensor proteins.70 VSNLs play a role inthe transduction of calcium signals and act as modulators ofmultiple intracellular targets, similar to calmodulin. Interest-ingly, a recent study identified VSNL1 as a positivelyregulated target of SF-1, raising the possibility that VSNL1could be involved in the regulation of adrenal developmentand steroidogenesis.71 In H295R cells, VSNL1 appears tomodulate CYP11B2 gene expression and aldosterone secre-tion and to protect cells from calcium-induced apoptosis.
Interestingly, the expression of VSNL1 was significantlyincreased in APAs harboring KCNJ5 mutations comparedwith those without, indicating that VSNL1 may play a keyrole in the development of KCNJ5 mutant APAs via itsantiapoptotic effect in response to calcium cytotoxicity andits role in the regulation of aldosterone production.69
The involvement of the Wnt/�-catenin pathway in thedevelopment of adrenocortical carcinomas is now well estab-lished.72–74 The presence of activating mutations in exons 3and 5 of the CTNNB1 gene, which encodes �-catenin, hasbeen described in a wide variety of human cancers, includingadrenocortical tumors.72,75–77 These mutations prevent�-catenin phosphorylation and induce nucleocytoplasmic ac-cumulation of the protein, resulting in constitutive activationof �-catenin target genes. Recently, Berthon et al74 showedthat mice expressing a constitutively active �-catenin in theadrenal cortex present with adrenal hyperplasia and dysplasiaand develop hyperaldosteronism at 10 months, with subse-quent evolution toward malignant tumors after 17 months ofage. Similarly, mice carrying a mutation in the APC gene, acomponent of the Wnt/�-catenin degradation complex, de-velop multiple intestinal tumors but also present with aphenotype of hyperaldosteronism.78 These data demonstratethat constitutively active �-catenin is an adrenal oncogene,which can trigger aberrant differentiation of aldosterone-secreting cells and promote malignancy. Recently, we haveshown that activation of �-catenin occurs in approximatelytwo thirds of APAs.41 However, �-catenin activation statuswas not associated with any biological or clinical parameters.Moreover, the sequencing of exons 3 and 5 of the CTNNB1gene in tumor DNA from 41 patients did not show mutationsthat could account for �-catenin activation. The transcriptomeprofiles of the Wnt/�-catenin pathway genes were also investi-gated in 12 APA samples. Interestingly, we observed separateclustering of control adrenals and APA samples supportingchanges in the Wnt/�-catenin pathway gene expression betweenthese 2 groups. Moreover, in APAs, those characterized bynonactive �-catenin were distinct from those showing nuclearlocalization. Surprisingly, APAs with an accumulation of�-catenin in the cytoplasm, which is considered to be the activeform, clustered with tumors showing membrane localization,possibly indicating activation of distinct pathways depending onintracellular �-catenin localization.41
Similar to �-catenin, Sonic hedgehog (Shh) plays a keyrole in adrenocortical development in the mouse. Conditionalinactivation of Shh in the adrenal cortex produces severehypoplasia and histological disorganization.79 Moreover,mice null for Shh specifically in SF-1–positive cells showreduced proliferation of capsular cells and a significantreduction of both adrenocortical thickness and adrenal sizebut no modification of adrenal zonation, indicating that Shh isessential for expansion of the adrenal cortex but not forzonation and differentiation.80 In normal human adrenals,Shh expression is restricted to a small number of cells locatednear the capsule, where stem/precursor cells are assumed tobe localized.41 Interestingly, we have shown that Shh isexpressed in APA; transcriptome analysis of the Shh signal-ing pathway separated normal adrenals from APA, and APAwith homogeneous expression of Shh from those with heter-
584 Hypertension September 2012
by guest on April 18, 2016http://hyper.ahajournals.org/Downloaded from

ogeneous expression. Remarkably, we observed a dramaticincrease of Shh expression in peritumoral hyperplastic ZG,similar to what we observed previously for CYP11B2 anddisabled-2.41
Indeed, adrenals from patients with APA show intenseadrenal cortex remodeling and functional ZG hyperplasia,suggesting a potential link with APA formation.33 Takentogether these results suggest that both APA and the adjacentZG may have acquired some characteristics of stem/precursorcells or that re-expression of fetal markers from the definitivezone in the adrenal cortex may underlie excessive prolifera-tion and APA formation.41 Interestingly, however, KCNJ5
mutations appear to be isolated events in the progressiontoward APA, because they are not found in the adjacentadrenal cortex of an APA carrying a mutation.40 This sug-gests that KCNJ5 mutations may occur within a proliferatingand hyperplastic cortex, leading to growth advantage, clonalexpansion, and APA formation in a considerable number ofcases. Alternatively, they may represent the primary eventleading to APA formation, with adrenal cortex hyperplasiabeing secondary to reduced vascularization and/or tissuehypoxia. Remarkably, however, KCNJ5 mutations do notinduce a unique molecular phenotype of APA, as could havebeen expected from mutations acting on key signaling path-
AT1R
Ang II
TASK1,TASK3
Kir3.4 wt
Kir3.4 mut
Ca2+
L & T-Type Channels
PLCαq/11
TASK3K+
K+PIP2
DAG + IP3
Ca2+
PKC
PKD
TDGF-1
PI3K
β-cateninaccumula�on
Frizzled
LRP
Wnt4
Depolariza�on
Depolariza�on
L & T-Type Channels
Ca2+
NURR1-PNGF1B-P
NBRE-1 Ad4 Ad5 CRE
CYP11B2
Scavenger receptor B1
Cholesterol
CYP11A1
SF-1
[Ca2+]Calmodulin 2
CaMK I/IVAldosterone
HDLHSL
ACATFree cholesterol
Lipiddroplet
PI3K
AktAkt-P
β-catenin
StAR
NURR1-P
CREB-P
NGF1B-PCREB-P
NURR1-PNGF1B-P
ATP cAMPLDL receptor
receptor B1(SR-B1)
Pregnenolone
PKA
CREB-P
3 β -HSD2
CYP11B2
LDL
Endosome
β catenin
α
MC2-R, LHR, 5-HT4
3 β -HSD2CYP21A
αs
K+
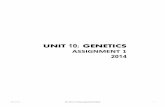
Figure. Mechanisms converging toward increased aldosterone production in aldosterone-producing adenoma. The key player in regu-lating aldosterone biosynthesis is calcium (Ca2�) signaling. Stimulation by angiotensin II (Ang II) or potassium results in depolarizationof the zona glomerulosa cell membrane and opening of voltage-dependent Ca2�-channels, leading to an increased intracellular Ca2�
concentration. Ang II also signals through the Ang II type 1 receptors (AT1R) to stimulate inositol trisphosphate–dependent Ca2�
release from the endoplasmic reticulum. Activation of the calcium signaling pathway triggers a phosphorylation cascade, involving cal-modulin and calmodulin-dependent kinase I/IV, leading to the activation of transcription factors (NURR1 and NGF1B, CREB) that bindto the promoter region and positively regulate the transcription of CYP11B2. Gain of function mutations in Kir3.4, as well as inactivationof TASK1 and TASK3 potassium channels, lead to cell membrane depolarization and increased intracellular calcium through the open-ing of L- and T-type calcium channels. Increased expression of AT1R, as well as ectopic expression of G protein–coupled receptorscoupled with G�q/11, result in activation of phospholipase C (PLC) and hydrolysis of phosphatidylinositol-4,5-bisphosphate (PIP2) todiacylglycerol (DAG) and inositol 1,4,5-trisphosphate (IP3). DAG increases the activity of protein kinase C (PKC) and protein kinase D(PKD), increasing CREB phosphorylation. The ectopic expression of G protein–coupled receptors coupled to �s such as the adrenocor-ticotropic hormone (ACTH) receptor (MC2-R), the luteinizing hormone receptor (LH-R), or the serotonin receptor type 4 (5HTR4) mayresult in an increase of intracellular cAMP concentration and, thus, of CREB phosphorylation. Increased expression of teratocarcinoma-derived growth factor 1 (TDGF-1) results in Akt phosphorylation and indirectly in increased aldosterone production. Activation of Wnt/�-catenin signaling may contribute to increased proliferation and aldosterone production. Finally, increased expression of the scavengerreceptor B1 promoting increased capture of high-density lipoprotein (HDL) and increased free cholesterol in the cell, together withincreased expression of the steroidogenic acute regulatory protein (StAR), and steroid biosynthetic enzymes (3�-HSD2) may contributeto aldosterone overproduction.
Zennaro et al Genetics and Genomics of Primary Aldosteronism 585
by guest on April 18, 2016http://hyper.ahajournals.org/Downloaded from

ways or master transcriptional regulators.40 Rather, they mayrepresent one of several possible mechanisms triggering, viaincreased Ca2� signaling and/or other pathways, increasedcell proliferation and aldosterone production (Figure).
ConclusionsUnderstanding the mechanisms involved in the developmentof PA is crucial to the development of more powerfuldiagnostic procedures and possibly innovative therapeuticoptions, which could benefit �10% of hypertensives. Al-though KCNJ5 mutations play a prominent role in thepathogenesis of both APA and FH3, the genetic determinantsand/or the genomic changes occurring in the most commonforms of familial and sporadic PA, namely FH2 and BAH,remain to be identified. This will be an exciting challenge forthe next decade and may also open new therapeutic perspec-tives for the management of hypertension in the generalpopulation.
AcknowledgmentsWe thank Dr Amanda J. Rickard for careful reading of the article.
Sources of FundingThis work was funded through institutional support from InstitutNational de la Santé et de la Recherche Médicale and by the AgenceNationale pour la Recherche (ANR Physio 2007, No. 013-01;Genopat 2008, No. 08-GENO-021), the Fondation pour la Recherchesur l’Hypertension Artérielle (AO 2007), the Fondation Pour laRecherche Médicale (ING20101221177), the Programme Hospital-ier de Recherche Clinique (PHRC grant AOM 06179), and by grantsfrom Institut National de la Santé et de la Recherche Médicale andMinistère Délégué a la Recherche et des Nouvelles Technologies.
DisclosuresNone.
References1. Hannemann A, Wallaschofski H. Prevalence of primary aldosteronism in
patient’s cohorts and in population-based studies: a review of the currentliterature. Horm Metab Res. 2012;44:157–162.
2. Plouin PF, Amar L, Chatellier G. Trends in the prevalence of primaryaldosteronism, aldosterone-producing adenomas, and surgically cor-rectable aldosterone-dependent hypertension. Nephrol Dial Transplant.2004;19:774–777.
3. Douma S, Petidis K, Doumas M, Papaefthimiou P, Triantafyllou A,Kartali N, Papadopoulos N, Vogiatzis K, Zamboulis C. Prevalence ofprimary hyperaldosteronism in resistant hypertension: a retrospectiveobservational study. Lancet. 2008;371:1921–1926.
4. Calhoun DA, Nishizaka MK, Zaman MA, Thakkar RB, Weissmann P.Hyperaldosteronism among black and white subjects with resistant hyper-tension. Hypertension. 2002;40:892–896.
5. Milliez P, Girerd X, Plouin PF, Blacher J, Safar ME, Mourad JJ. Evidencefor an increased rate of cardiovascular events in patients with primaryaldosteronism. J Am Coll Cardiol. 2005;45:1243–1248.
6. Rossi GP, Sechi LA, Giacchetti G, Ronconi V, Strazzullo P, Funder JW.Primary aldosteronism: cardiovascular, renal and metabolic implications.Trends Endocrinol Metab. 2008;19:88–90.
7. Rossi GP, Bolognesi M, Rizzoni D, Seccia TM, Piva A, Porteri E, TiberioGA, Giulini SM, Agabiti-Rosei E, Pessina AC. Vascular remodeling andduration of hypertension predict outcome of adrenalectomy in primaryaldosteronism patients. Hypertension. 2008;51:1366–1371.
8. Letavernier E, Peyrard S, Amar L, Zinzindohoue F, Fiquet B, Plouin PF.Blood pressure outcome of adrenalectomy in patients with primary hyper-aldosteronism with or without unilateral adenoma. J Hypertens. 2008;26:1816–1823.
9. Catena C, Lapenna R, Baroselli S, Nadalini E, Colussi G, Novello M,Favret G, Melis A, Cavarape A, Sechi LA. Insulin sensitivity in patients
with primary aldosteronism: a follow-up study. J Clin Endocrinol Metab.2006;91:3457–3463.
10. Sechi LA, Novello M, Lapenna R, Baroselli S, Nadalini E, Colussi GL,Catena C. Long-term renal outcomes in patients with primary aldoste-ronism. JAMA. 2006;295:2638–2645.
11. Zennaro MC, Caprio M, Feve B. Mineralocorticoid receptors in themetabolic syndrome. Trends Endocrinol Metab. 2009;20:444–451.
12. Reincke M, Meisinger C, Holle R, Quinkler M, Hahner S, Beuschlein F,Bidlingmaier M, Seissler J, Endres S. Is primary aldosteronism associatedwith diabetes mellitus? Results of the German Conn’s Registry. HormMetab Res. 2010;42:435–439.
13. Funder JW, Carey RM, Fardella C, Gomez-Sanchez CE, Mantero F,Stowasser M, Young WF Jr, Montori VM. Case detection, diagnosis, andtreatment of patients with primary aldosteronism: an endocrine societyclinical practice guideline. J Clin Endocrinol Metab. 2008;93:3266–3281.
14. Sutherland DJ, Ruse JL, Laidlaw JC. Hypertension, increased aldosteronesecretion and low plasma renin activity relieved by dexamethasone. CanMed Assoc J. 1966;95:1109–1119.
15. Pascoe L, Jeunemaitre X, Lebrethon MC, Curnow KM, Gomez-SanchezCE, Gasc JM, Saez JM, Corvol P. Glucocorticoid-suppressible hyperal-dosteronism and adrenal tumors occurring in a single French pedigree.J Clin Invest. 1995;96:2236–2246.
16. Stowasser M, Gordon RD. Familial hyperaldosteronism. J SteroidBiochem Mol Biol. 2001;78:215–229.
17. Lifton RP, Dluhy RG, Powers M, Rich GM, Cook S, Ulick S, Lalouel JM.A chimaeric 11�-hydroxylase aldosterone synthase gene causesglucocorticoid-remediable aldosteronism and human hypertension.Nature. 1992;355:262–265.
18. Pascoe L, Curnow KM, Slutsker L, Connell JM, Speiser PW, New MI,White PC. Glucocorticoid-suppressible hyperaldosteronism results fromhybrid genes created by unequal crossovers between CYP11B1 andCYP11B2. Proc Natl Acad Sci U S A. 1992;89:8327–8331.
19. Gordon RD, Stowasser M, Tunny TJ, Klemm SA, Finn WL, Krek AL.Clinical and pathological diversity of primary aldosteronism, including anew familial variety. Clin Exp Pharmacol Physiol. 1991;18:283–286.
20. Medeau V, Assie G, Zennaro MC, Clauser E, Plouin PF, Jeunemaitre X.Familial aspect of primary hyperaldosteronism: analysis of families com-patible with primary hyperaldosteronism type 2 [in French]. Ann Endo-crinol (Paris). 2005;66:240–246.
21. Mulatero P, Tizzani D, Viola A, Bertello C, Monticone S, Mengozzi G,Schiavone D, Williams TA, Einaudi S, La Grotta A, Rabbia F, Veglio F.Prevalence and characteristics of familial hyperaldosteronism: thePATOGEN Study (Primary Aldosteronism in Torino-Genetic Forms).Hypertension. 2011;58:797–803.
22. Aglony M, Martinez-Aguayo A, Carvajal CA, Campino C, Garcia H,Bancalari R, Bolte L, Avalos C, Loureiro C, Trejo P, Brinkmann K,Giadrosich V, Mericq V, Rocha A, Avila A, Perez V, Inostroza A,Fardella CE. Frequency of familial hyperaldosteronism type 1 in a hyper-tensive pediatric population: clinical and biochemical presentation.Hypertension. 2011;57:1117–1121.
23. Stowasser M, Gunasekera TG, Gordon RD. Familial varieties of primaryaldosteronism. Clin Exp Pharmacol Physiol. 2001;28:1087–1090.
24. Lafferty AR, Torpy DJ, Stowasser M, Taymans SE, Lin JP, Huggard P,Gordon RD, Stratakis CA. A novel genetic locus for low renin hyper-tension: familial hyperaldosteronism type II maps to chromosome 7(7p22). J Med Genet. 2000;37:831–835.
25. Stowasser M, Gordon RD. Primary aldosteronism. Best Pract Res ClinEndocrinol Metab. 2003;17:591–605.
26. Iida A, Blake K, Tunny T, Klemm S, Stowasser M, Hayward N, GordonR, Nakamura Y, Imai T. Allelic losses on chromosome band 11q13 inaldosterone-producing adrenal tumors. Genes Chromosomes Cancer.1995;12:73–75.
27. Lim PO, Macdonald TM, Holloway C, Friel E, Anderson NH, Dow E,Jung RT, Davies E, Fraser R, Connell JM. Variation at the aldosteronesynthase (CYP11B2) locus contributes to hypertension in subjects with araised aldosterone-to-renin ratio. J Clin Endocrinol Metab. 2002;87:4398–4402.
28. Stowasser M, Gordon RD. Primary aldosteronism: from genesis togenetics. Trends Endocrinol Metab. 2003;14:310–317.
29. Geller DS, Zhang J, Wisgerhof MV, Shackleton C, Kashgarian M, LiftonRP. A novel form of human mendelian hypertension featuringnonglucocorticoid-remediable aldosteronism. J Clin Endocrinol Metab.2008;93:3117–3123.
586 Hypertension September 2012
by guest on April 18, 2016http://hyper.ahajournals.org/Downloaded from

30. Hattangady NG, Olala LO, Bollag WB, Rainey WE. Acute and chronicregulation of aldosterone production. Mol Cell Endocrinol. 2012;350:151–162.
31. Enberg U, Farnebo LO, Wedell A, Grondal S, Thoren M, Grimelius L,Kjellman M, Backdahl M, Hamberger B. In vitro release of aldosteroneand cortisol in human adrenal adenomas correlates to mRNA expressionof steroidogenic enzymes for genes CYP11B2 and CYP17. World J Surg.2001;25:957–966.
32. Fallo F, Pezzi V, Barzon L, Mulatero P, Veglio F, Sonino N, Mathis JM.Quantitative assessment of CYP11B1 and CYP11B2 expression inaldosterone-producing adenomas. Eur J Endocrinol. 2002;147:795–802.
33. Boulkroun S, Samson-Couterie B, Dzib JF, Lefebvre H, Louiset E, AmarL, Plouin PF, Lalli E, Jeunemaitre X, Benecke A, Meatchi T, ZennaroMC. Adrenal cortex remodeling and functional zona glomerulosa hyper-plasia in primary aldosteronism. Hypertension. 2010;56:885–892.
34. Enberg U, Volpe C, Hoog A, Wedell A, Farnebo LO, Thoren M, Ham-berger B. Postoperative differentiation between unilateral adrenaladenoma and bilateral adrenal hyperplasia in primary aldosteronism bymRNA expression of the gene CYP11B2. Eur J Endocrinol. 2004;151:73–85.
35. Nishimoto K, Nakagawa K, Li D, Kosaka T, Oya M, Mikami S, ShibataH, Itoh H, Mitani F, Yamazaki T, Ogishima T, Suematsu M, Mukai K.Adrenocortical zonation in humans under normal and pathological con-ditions. J Clin Endocrinol Metab. 2010;95:2296–2305.
36. Lenzini L, Seccia TM, Aldighieri E, Belloni AS, Bernante P, Giuliani L,Nussdorfer GG, Pessina AC, Rossi GP. Heterogeneity of aldosterone-producing adenomas revealed by a whole transcriptome analysis. Hyper-tension. 2007;50:1106–1113.
37. Bassett MH, Mayhew B, Rehman K, White PC, Mantero F, Arnaldi G,Stewart PM, Bujalska I, Rainey WE. Expression profiles for steroid-ogenic enzymes in adrenocortical disease. J Clin Endocrinol Metab.2005;90:5446–5455.
38. Assié G, Auzan C, Gasc JM, Baviera E, Balaton A, Elalouf JM, Jeun-emaitre X, Plouin PF, Corvol P, Clauser E. Steroidogenesis inaldosterone-producing adenoma revisited by transcriptome analysis.J Clin Endocrinol Metab. 2005;90:6638–6649.
39. Azizan EA, Lam BY, Newhouse SJ, Zhou J, Kuc RE, Clarke J, Hap-perfield L, Marker A, Hoffman GJ, Brown MJ. Microarray, qPCR, andKCNJ5 sequencing of aldosterone-producing adenomas reveal dif-ferences in genotype and phenotype between zona glomerulosa- and zonafasciculata-like tumors. J Clin Endocrinol Metab. 2012;97:E819–E829.
40. Boulkroun S, Beuschlein F, Rossi GP, Golib-Dzib JF, Fischer E, Amar L,Mulatero P, Samson-Couterie B, Hahner S, Quinkler M, Fallo F, LetiziaC, Allolio B, Ceolotto G, Cicala MV, Lang K, Lefebvre H, Lenzini L,Maniero C, Monticone S, Perrocheau M, Pilon C, Plouin PF, Rayes N,Seccia TM, Veglio F, Williams TA, Zinnamosca L, Mantero F, BeneckeA, Jeunemaitre X, Reincke M, Zennaro MC. Prevalence, clinical, andmolecular correlates of KCNJ5 mutations in primary aldosteronism.Hypertension. 2012;59:592–598.
41. Boulkroun S, Samson-Couterie B, Golib-Dzib JF, Amar L, Plouin PF,Sibony M, Lefebvre H, Louiset E, Jeunemaitre X, Meatchi T, Benecke A,Lalli E, Zennaro MC. Aldosterone-producing adenoma formation in theadrenal cortex involves expression of stem/progenitor cell markers.Endocrinology. 2011;152:4753–4763.
42. Boulkroun S, Samson-Couterie B, Golib Dzib JF, Meatchi T, Claes A,Tareen SK, Plouin PF, Jeunemaitre X, Benecke A, Zennaro MC. Tran-scriptional and pathological analysis of aldosterone producing tumors andhyperplasias. Paper presented at: ENDO 2009: The 93rd Annual Meeting,June 10–13, 2009; Washington DC.
43. Spat A, Hunyady L. Control of aldosterone secretion: a model for con-vergence in cellular signaling pathways. Physiol Rev. 2004;84:489–539.
44. Zenkert S, Schubert B, Fassnacht M, Beuschlein F, Allolio B, Reincke M.Steroidogenic acute regulatory protein mRNA expression in adrenaltumours. Eur J Endocrinol. 2000;142:294–299.
45. Lacroix A, Ndiaye N, Tremblay J, Hamet P. Ectopic and abnormalhormone receptors in adrenal Cushing’s syndrome. Endocr Rev. 2001;22:75–110.
46. Lefebvre H, Cartier D, Duparc C, Lihrmann I, Contesse V, Delarue C,Godin M, Fischmeister R, Vaudry H, Kuhn JM. Characterization ofserotonin(4) receptors in adrenocortical aldosterone-producing adenomas:in vivo and in vitro studies. J Clin Endocrinol Metab. 2002;87:1211–1216.
47. Ye P, Mariniello B, Mantero F, Shibata H, Rainey WE. G-protein-coupled receptors in aldosterone-producing adenomas: a potential causeof hyperaldosteronism. J Endocrinol. 2007;195:39–48.
48. Beuschlein F, Fassnacht M, Klink A, Allolio B, Reincke M. ACTH-receptor expression, regulation and role in adrenocortial tumor formation.Eur J Endocrinol. 2001;144:199–206.
49. Saner-Amigh K, Mayhew BA, Mantero F, Schiavi F, White PC, Rao CV,Rainey WE. Elevated expression of luteinizing hormone receptor inaldosterone-producing adenomas. J Clin Endocrinol Metab. 2006;91:1136–1142.
50. Contesse V, Lenglet S, Grumolato L, Anouar Y, Lihrmann I, Lefebvre H,Delarue C, Vaudry H. Pharmacological and molecular characterization of5-hydroxytryptamine(7) receptors in the rat adrenal gland. MolPharmacol. 1999;56:552–561.
51. Lefebvre H, Compagnon P, Contesse V, Delarue C, Thuillez C, VaudryH, Kuhn JM. Production and metabolism of serotonin (5-HT) by thehuman adrenal cortex: paracrine stimulation of aldosterone secretion by5-HT. J Clin Endocrinol Metab. 2001;86:5001–5007.
52. Cook MD, Phillips MI, Cook VI, Kimura B, Wilcox CS. Angiotensin IIreceptor subtypes on adrenal adenoma in primary hyperaldosteronism.J Am Soc Nephrol. 1993;4:111–116.
53. Schubert B, Fassnacht M, Beuschlein F, Zenkert S, Allolio B, Reincke M.Angiotensin II type 1 receptor and ACTH receptor expression in humanadrenocortical neoplasms. Clin Endocrinol (Oxf). 2001;54:627–632.
54. Chang HW, Chu TS, Huang HY, Chueh SC, Wu VC, Chen YM, HsiehBS, Wu KD. Down-regulation of D2 dopamine receptor and increasedprotein kinase Cmu phosphorylation in aldosterone-producing adenomaplay roles in aldosterone overproduction. J Clin Endocrinol Metab. 2007;92:1863–1870.
55. Bassett MH, Suzuki T, Sasano H, White PC, Rainey WE. The orphannuclear receptors NURR1 and NGFIB regulate adrenal aldosterone pro-duction. Mol Endocrinol. 2004;18:279–290.
56. Bandulik S, Penton D, Barhanin J, Warth R. TASK1 and TASK3potassium channels: determinants of aldosterone secretion and adreno-cortical zonation. Horm Metab Res. 2010;42:450–457.
57. Heitzmann D, Derand R, Jungbauer S, Bandulik S, Sterner C, Schweda F,El Wakil A, Lalli E, Guy N, Mengual R, Reichold M, Tegtmeier I,Bendahhou S, Gomez-Sanchez CE, Aller MI, Wisden W, Weber A,Lesage F, Warth R, Barhanin J. Invalidation of TASK1 potassiumchannels disrupts adrenal gland zonation and mineralocorticoid homeo-stasis. EMBO J. 2008;27:179–187.
58. Davies LA, Hu C, Guagliardo NA, Sen N, Chen X, Talley EM, CareyRM, Bayliss DA, Barrett PQ. TASK channel deletion in mice causesprimary hyperaldosteronism. Proc Natl Acad Sci U S A. 2008;105:2203–2208.
59. Choi M, Scholl UI, Yue P, Bjorklund P, Zhao B, Nelson-Williams C, JiW, Cho Y, Patel A, Men CJ, Lolis E, Wisgerhof MV, Geller DS, ManeS, Hellman P, Westin G, Akerstrom G, Wang W, Carling T, Lifton RP.K� channel mutations in adrenal aldosterone-producing adenomas andhereditary hypertension. Science. 2011;331:768–772.
60. Boulkroun S, Tareen SK, Perdry H, Golib Dzib JF, Karam O, Samson-Couterie B, Simian C, Bendahhou S, Benecke A, Barhanin J, JeunemaitreX, Zennaro MC. Study of the Role of KCNK3 and KCNK9 in thepathogenesis of primary aldosteronism. Paper presented at: ENDO 2011:The 93rd Annual Meeting, June 4–7, 2011; Boston, MA.
61. Mulatero P, Tauber P, Zennaro MC, Monticone S, Lang K, Beuschlein F,Fischer E, Tizzani D, Pallauf A, Viola A, Amar L, Williams TA, StromTM, Graf E, Bandulik S, Penton D, Plouin PF, Warth R, Allolio B,Jeunemaitre X, Veglio F, Reincke M. KCNJ5 mutations in Europeanfamilies with nonglucocorticoid remediable familial hyperaldosteronism.Hypertension. 2012;59:235–240.
62. Azizan EA, Murthy M, Stowasser M, Gordon R, Kowalski B, Xu S,Brown MJ, O’Shaughnessy KM. Somatic mutations affecting the selec-tivity filter of KCNJ5 are frequent in 2 large unselected collections ofadrenal aldosteronomas. Hypertension. 2012;59:587–591.
63. Taguchi R, Yamada M, Nakajima Y, Satoh T, Hashimoto K, ShibusawaN, Ozawa A, Okada S, Rokutanda N, Takata D, Koibuchi Y, HoriguchiJ, Oyama T, Takeyoshi I, Mori M. Expression and mutations of KCNJ5mRNA in Japanese patients with aldosterone-producing adenomas. J ClinEndocrinol Metab. 2012;97:1311–1319.
64. Oki K, Plonczynski MW, Luis Lam M, Gomez-Sanchez EP, Gomez-Sanchez CE. Potassium channel mutant KCNJ5 T158A expression inHAC-15 cells increases aldosterone synthesis. Endocrinology. 2012;153:1774–1782.
65. Scholl UI, Nelson-Williams C, Yue P, Grekin R, Wyatt RJ, Dillon MJ,Couch R, Hammer LK, Harley FL, Farhi A, Wang WH, Lifton RP.Hypertension with or without adrenal hyperplasia due to different
Zennaro et al Genetics and Genomics of Primary Aldosteronism 587
by guest on April 18, 2016http://hyper.ahajournals.org/Downloaded from

inherited mutations in the potassium channel KCNJ5. Proc Natl Acad SciU S A. 2012;109:2533–2538.
66. Williams TA, Monticone S, Morello F, Liew CC, Mengozzi G, Pilon C,Asioli S, Sapino A, Veglio F, Mulatero P. Teratocarcinoma-derivedgrowth factor-1 is upregulated in aldosterone-producing adenomas andincreases aldosterone secretion and inhibits apoptosis in vitro.Hypertension. 2010;55:1468–1475.
67. Adamson ED, Minchiotti G, Salomon DS. Cripto: a tumor growth factorand more. J Cell Physiol. 2002;190:267–278.
68. Sun Y, Strizzi L, Raafat A, Hirota M, Bianco C, Feigenbaum L, Kenney N,Wechselberger C, Callahan R, Salomon DS. Overexpression of humanCripto-1 in transgenic mice delays mammary gland development and differ-entiation and induces mammary tumorigenesis. Am J Pathol. 2005;167:585–597.
69. Williams TA, Monticone S, Crudo V, Warth R, Veglio F, Mulatero P.Visinin-like 1 is upregulated in aldosterone-producing adenomas withKCNJ5 mutations and protects from calcium-induced apoptosis.Hypertension. 2012;59:833–839.
70. Braunewell KH, Klein-Szanto AJ. Visinin-like proteins (VSNLs): inter-action partners and emerging functions in signal transduction of a sub-family of neuronal Ca2� -sensor proteins. Cell Tissue Res. 2009;335:301–316.
71. Ferraz-de-Souza B, Hudson-Davies RE, Lin L, Parnaik R, Hubank M,Dattani MT, Achermann JC. Sterol O-acyltransferase 1 (SOAT1, ACAT)is a novel target of steroidogenic factor-1 (SF-1, NR5A1, Ad4BP) in thehuman adrenal. J Clin Endocrinol Metab. 2011;96:E663–E668.
72. Tissier F, Cavard C, Groussin L, Perlemoine K, Fumey G, Hagnere AM,Rene-Corail F, Jullian E, Gicquel C, Bertagna X, Vacher-Lavenu MC,Perret C, Bertherat J. Mutations of �-catenin in adrenocortical tumors:activation of the Wnt signaling pathway is a frequent event in both benignand malignant adrenocortical tumors. Cancer Res. 2005;65:7622–7627.
73. El Wakil A, Lalli E. The Wnt/� -catenin pathway in adrenocorticaldevelopment and cancer. Mol Cell Endocrinol. 2011;332:32–37.
74. Berthon A, Martinez A, Bertherat J, Val P. Wnt/� -catenin signalling inadrenal physiology and tumour development. Mol Cell Endocrinol. 2012;351:87–95.
75. Gaujoux S, Grabar S, Fassnacht M, Ragazzon B, Launay P, Libe R,Chokri I, Audebourg A, Royer B, Sbiera S, Vacher-Lavenu MC, DoussetB, Bertagna X, Allolio B, Bertherat J, Tissier F. �-Catenin activation isassociated with specific clinical and pathologic characteristics and a pooroutcome in adrenocortical carcinoma. Clin Cancer Res. 2011;17:328–336.
76. Bonnet S, Gaujoux S, Launay P, Baudry C, Chokri I, Ragazzon B, LibeR, Rene-Corail F, Audebourg A, Vacher-Lavenu MC, Groussin L,Bertagna X, Dousset B, Bertherat J, Tissier F. Wnt/� -catenin pathwayactivation in adrenocortical adenomas is frequently due to somaticCTNNB1-activating mutations, which are associated with larger andnonsecreting tumors: a study in cortisol-secreting and -nonsecretingtumors. J Clin Endocrinol Metab. 2011;96:E419–E426.
77. Tadjine M, Lampron A, Ouadi L, Bourdeau I. Frequent mutations of�-catenin gene in sporadic secreting adrenocortical adenomas. Clin Endo-crinol (Oxf). 2008;68:264–270.
78. Bhandaru M, Kempe DS, Rotte A, Rexhepaj R, Kuhl D, Lang F. Hyper-aldosteronism, hypervolemia, and increased blood pressure in miceexpressing defective APC. Am J Physiol Regul Integr Comp Physiol.2009;297:R571–R575.
79. Ching S, Vilain E. Targeted disruption of Sonic Hedgehog in themouse adrenal leads to adrenocortical hypoplasia. Genesis. 2009;47:628–637.
80. Huang CC, Miyagawa S, Matsumaru D, Parker KL, Yao HH. Progenitorcell expansion and organ size of mouse adrenal is regulated by sonichedgehog. Endocrinology. 2010;151:1119–1128.
81. Sasano H, Shizawa S, Suzuki T, Takayama K, Fukaya T, Morohashi K,Nagura H. Ad4BP in the human adrenal cortex and its disorders. J ClinEndocrinol Metab. 1995;80:2378–2380.
588 Hypertension September 2012
by guest on April 18, 2016http://hyper.ahajournals.org/Downloaded from

Maria-Christina Zennaro, Xavier Jeunemaitre and Sheerazed BoulkrounIntegrating Genetics and Genomics in Primary Aldosteronism
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 2012 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/HYPERTENSIONAHA.111.188250
2012;60:580-588; originally published online July 16, 2012;Hypertension.
http://hyper.ahajournals.org/content/60/3/580World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertensionin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on April 18, 2016http://hyper.ahajournals.org/Downloaded from