
Innovations in the Management of Displaced Proximal ...
15
Innovations in the Management of Displaced Proximal Humerus Fractures Abstract The management of displaced proximal humerus fractures has evolved toward humeral head preservation, with treatment decisions based on careful assessment of vascular status, bone quality, fracture pattern, degree of displacement, and patient age and activity level. The AO/ASIF fracture classification is helpful in guiding treatment and in stratifying the risk for associated disruption of the humeral head blood supply. Nonsurgical treatment consists of sling immobilization. For patients requiring surgery, options include closed reduction and percutaneous fixation; transosseous suture fixation; open reduction and internal fixation, with either conventional or locking plate fixation; bone graft; and hemiarthroplasty. Proximal humerus fractures must be evaluated on an individual basis, with treatment tailored according to patient and fracture characteristics. P roximal humerus fractures are increasingly common in socie- ties with maturing populations. 1 These fractures are not simple to treat. A variety of options exists; however, outcomes are less than ide- al in many patients. 2,3 Most proxi- mal humerus fractures are either nondisplaced or minimally displaced and can be treated nonsurgically. 4 Nonsurgical options focus on early functional exercises with the goal of achieving a functionally acceptable range of motion (ROM). For the 15% to 20% of displaced proximal hu- merus fractures that may benefit from surgery, no single approach is considered to be the standard of care. Surgeons should be familiar with the different treatment options avail- able, including recent advances in the management of complex periar- ticular fractures 5-11 and in locking plate technology, 8,12 which are par- ticularly relevant to the care of these fractures. 7,13-15 Locking plate tech- nology and the use of osteobiologics may become increasingly important in the management of displaced proximal humerus fractures, facili- tating humeral head preservation in appropriately selected patients. Epidemiology Proximal humerus fracture is the second most common fracture of the upper extremity, following distal forearm fracture. 1 In people older than age 65 years, fracture of the proximal humerus is the third most common fracture, after hip fracture and Colles’ fracture. 1 Proximal hu- merus fracture is associated with Shane J. Nho, MD Robert H. Brophy, MD Joseph U. Barker, MD Charles N. Cornell, MD John D. MacGillivray, MD Dr. Nho is Resident, Department of Orthopaedic Surgery, Hospital for Special Surgery, New York, NY. Dr. Brophy is Resident, Department of Orthopaedic Surgery, Hospital for Special Surgery. Dr. Barker is Resident, Department of Orthopaedic Surgery, Hospital for Special Surgery. Dr. Cornell is Attending Orthopaedic Surgeon, Department of Orthopaedic Surgery, Hospital for Special Surgery. Dr. MacGillivray is Assistant Attending Orthopaedic Surgeon, Department of Orthopaedic Surgery, Hospital for Special Surgery. None of the following authors or the departments with which they are affiliated has received anything of value from or owns stock in a commercial company or institution related directly or indirectly to the subject of this article: Dr. Nho, Dr. Brophy, Dr. Barker, Dr. Cornell, and Dr. MacGillivray. Reprint requests: Dr. MacGillivray, Department of Orthopaedic Surgery, Hospital for Special Surgery, 535 East 70th Street, New York, NY 10021. J Am Acad Orthop Surg 2007;15:12-26 Copyright 2007 by the American Academy of Orthopaedic Surgeons. 12 Journal of the American Academy of Orthopaedic Surgeons
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Innovations in the Management of Displaced Proximal ...

Innovations in theManagement ofDisplaced ProximalHumerus Fractures
AbstractThe management of displaced proximal humerus fractures hasevolved toward humeral head preservation, with treatmentdecisions based on careful assessment of vascular status, bonequality, fracture pattern, degree of displacement, and patient ageand activity level. The AO/ASIF fracture classification is helpful inguiding treatment and in stratifying the risk for associateddisruption of the humeral head blood supply. Nonsurgicaltreatment consists of sling immobilization. For patients requiringsurgery, options include closed reduction and percutaneousfixation; transosseous suture fixation; open reduction and internalfixation, with either conventional or locking plate fixation; bonegraft; and hemiarthroplasty. Proximal humerus fractures must beevaluated on an individual basis, with treatment tailored accordingto patient and fracture characteristics.
Proximal humerus fractures areincreasingly common in socie-
ties with maturing populations.1These fractures are not simple totreat. A variety of options exists;however, outcomes are less than ide-al in many patients.2,3 Most proxi-mal humerus fractures are eithernondisplaced or minimally displacedand can be treated nonsurgically.4Nonsurgical options focus on earlyfunctional exercises with the goal ofachieving a functionally acceptablerange of motion (ROM). For the 15%to 20% of displaced proximal hu-merus fractures that may benefitfrom surgery, no single approach isconsidered to be the standard of care.Surgeons should be familiar with thedifferent treatment options avail-able, including recent advances inthe management of complex periar-
ticular fractures5-11 and in lockingplate technology,8,12 which are par-ticularly relevant to the care of thesefractures.7,13-15 Locking plate tech-nology and the use of osteobiologicsmay become increasingly importantin the management of displacedproximal humerus fractures, facili-tating humeral head preservation inappropriately selected patients.
Epidemiology
Proximal humerus fracture is thesecond most common fracture of theupper extremity, following distalforearm fracture.1 In people olderthan age 65 years, fracture of theproximal humerus is the third mostcommon fracture, after hip fractureand Colles’ fracture.1 Proximal hu-merus fracture is associated with
Shane J. Nho, MD
Robert H. Brophy, MD
Joseph U. Barker, MD
Charles N. Cornell, MD
John D. MacGillivray, MD
Dr. Nho is Resident, Department ofOrthopaedic Surgery, Hospital forSpecial Surgery, New York, NY. Dr.Brophy is Resident, Department ofOrthopaedic Surgery, Hospital forSpecial Surgery. Dr. Barker is Resident,Department of Orthopaedic Surgery,Hospital for Special Surgery. Dr. Cornellis Attending Orthopaedic Surgeon,Department of Orthopaedic Surgery,Hospital for Special Surgery. Dr.MacGillivray is Assistant AttendingOrthopaedic Surgeon, Department ofOrthopaedic Surgery, Hospital forSpecial Surgery.
None of the following authors or thedepartments with which they areaffiliated has received anything of valuefrom or owns stock in a commercialcompany or institution related directly orindirectly to the subject of this article:Dr. Nho, Dr. Brophy, Dr. Barker, Dr.Cornell, and Dr. MacGillivray.
Reprint requests: Dr. MacGillivray,Department of Orthopaedic Surgery,Hospital for Special Surgery, 535 East70th Street, New York, NY 10021.
J Am Acad Orthop Surg 2007;15:12-26
Copyright 2007 by the AmericanAcademy of Orthopaedic Surgeons.
12 Journal of the American Academy of Orthopaedic Surgeons

significant morbidity, leading tofunctional impairment lasting atleast 3 months.16 Displaced proxi-mal humerus fractures generally re-sult in long-term functional disabil-ity. This type of injury usually issustained after a moderate-energyfall in an individual with low bonedensity.16
Anatomy
The proximal humerus is dividedinto the shaft, surgical neck, ana-tomic neck, lesser tuberosity, andgreater tuberosity. Classification ofproximal humerus fractures basedon these anatomic divisions predi-cates treatment and predicts out-come. The humeral head has aspherically shaped articular surface;the anatomic neck demarcates thejunction of the head and metaphy-sis. The neck-shaft angle is 130°, andthe head is retroverted 19° to 22° rel-ative to the shaft.17 The greater andlesser tuberosities are located adja-cent to the articular margin of thehead; they are separated by the bicip-ital groove. The surgical neck servesas the junction between the metaph-ysis and the humeral diaphysis.
Tendinous insertions contributeto the pattern of fracture displace-ment around the proximal humerusby transmitting deforming muscularforces to the bony fragments. The in-sertions of the supraspinatus, in-fraspinatus, and teres minor tendonsonto the greater tuberosity contrib-ute to the typical posterior and supe-rior retraction of this fragment. Therotator interval functions as a check-rein on the humeral head fragmentand limits displacement of two-partfractures and most three-part frac-tures. Functionally significant tearsof the rotator interval are uncom-mon. The pull of the subscapularismuscle tends to retract lesser tuber-osity fragments medially. When thelesser tuberosity remains attached tothe head fragment, the head frag-ment is rotated internally. Althoughthe bone at the tendinous insertion
tends to be very dense and strong,thus providing a potential site forfracture fixation, it is importantwhen using suture fixation to re-member that the tendons are evenstronger than the bone.18
The anterior circumflex humeralartery and the arcuate artery are con-sidered to be the major sources ofhumeral head perfusion,19 but stud-ies characterizing the vascular anat-omy were performed in the intactproximal humerus.20,21 Even in sim-ple fracture patterns, the anteriorcircumflex humeral artery is often
disrupted, implying, in the fracturedproximal humerus that perfusionfrom the posterior circumflex hu-meral artery alone may be sufficientfor humeral head survival. Hertel etal22 conducted perfusion studies inproximal humerus fractures to deter-mine factors predictive of humeralhead ischemia. They demonstratedthe significance of metaphyseal headextension (ie, the amount of me-taphysis, typically posteromedial)that remains attached to the humer-al head determines the amount ofhead extension22 (Figure 1, A). Meta-
Figure 1
Hertel radiographic criteria. A and B, Metaphyseal head extension is a radiographicmeasurement of the articular fragment from the head-neck junction to the inferiorextent of the medial cortex. A, Metaphyseal head extension >8 mm. B, Metaphysealhead extension <8 mm. C and D, Medial hinge integrity is determined by thecontinuity of the medial calcar. C, Undisplaced medial hinge. D, Medial hingedisplaced >2 mm. (Adapted with permission from Hertel R, Hempfing A, StiehlerM, Leunig M: Predictors of the humeral head ischemia after intracapsular fracture ofthe proximal humerus. J Shoulder Elbow Surg 2004;13:427-433.)
Shane J. Nho, MD, et al
Volume 15, Number 1, January 2007 13

physeal head extension <8 mm wasfound to be a good predictor of is-chemia (accuracy, 0.84).22 Anotherpredictor of ischemia was medialhinge disruption >2 mm (accuracy,0.79)22 (Figure 1, B). In this series, thecombination of metaphyseal headextension <8 mm with medial hingedisruption >2 mm as well as an ana-tomic neck fracture pattern had apositive predictive value of 97% for
humeral head ischemia.22
Classification
The Neer classification4 and the AO/ASIF classification23 are the mostwidely used systems to evaluate anddetermine treatment of proximalhumeral fractures. The Neer classi-fication is based on the number offracture parts (displacement >1 cm,
angulation >45°), direction of dislo-cation, and involvement of the artic-ular surface.4 The AO/ASIF classifi-cation system for proximal humerusfractures broadly groups fracturesbased on the degree of articular in-volvement and likelihood of vascu-lar injury23 (Figure 2). Observer reli-ability and reproducibility for boththe Neer and the AO/ASIF classifica-tion is fair to poor; it is unlikely thatone orthopaedic surgeon will assignthe same classification to a proximalhumerus fracture at two separatetimes, just as it is unlikely that twoorthopaedic surgeons will agree on aclassification. Given these limita-tions, the AO/ASIF classification forthe three basic types of humerusfracture is more user-friendly thanthe Neer classification,24 althoughstill complex.
Treatment Algorithm
Although the management of dis-placed proximal humerus fractureshas evolved toward humeral headpreservation, treatment should beguided by careful assessment of vas-cular status, bone quality, fracturepattern, and degree of comminution,as well as patient factors, such as ageand activity level. Patients who areeither medically unstable or inactiveare poor candidates for surgery andinstead may be treated with slingimmobilization until the fractureheals. The ultimate goal is maxi-mum shoulder function and mini-mal shoulder pain. A proposed treat-ment algorithm (Figure 3) provides aworking guideline for the manage-ment of proximal humerus fractures,but treatment, whether nonsurgicalor surgical, must be individualizedaccording to patient and fracturecharacteristics.
The likelihood of humeral headosteonecrosis is implicit in theAO/ASIF classification; thus, deter-mining the AO/ASIF fracture type isthe initial step in determining theprobability of humeral head preser-vation (Figure 3). Type A is a unifo-
Figure 2
AO/ASIF classification for proximal humerus fractures. Top, A, Unifocal, extra-articular two-part fracture with intact vascular supply. Middle, B, Bifocal extra-articular fracture with possible injury to the vascular supply. Bottom, C, Articularfracture involving the anatomic neck, with high likelihood of necrosis. (Adapted withpermission from Müller ME: Appendix A: The comprehensive classification offractures of long bones, in Müller ME, Allgöwer M, Schneider R, Willenegger H[eds]: Manual of Internal Fixation: Techniques Recommended by the AO-ASIFGroup. Berlin, Germany: Springer-Verlag, 1991, pp 118-125.)
Innovations in the Management of Displaced Proximal Humerus Fractures
14 Journal of the American Academy of Orthopaedic Surgeons
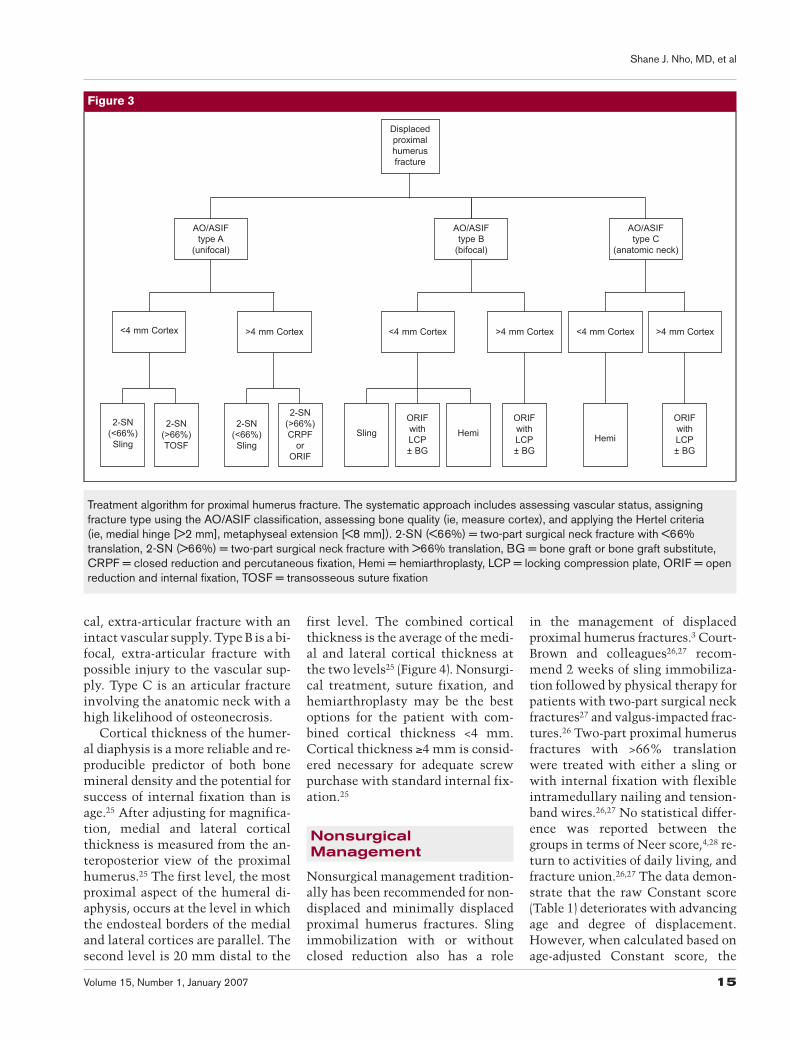
cal, extra-articular fracture with anintact vascular supply. Type B is a bi-focal, extra-articular fracture withpossible injury to the vascular sup-ply. Type C is an articular fractureinvolving the anatomic neck with ahigh likelihood of osteonecrosis.
Cortical thickness of the humer-al diaphysis is a more reliable and re-producible predictor of both bonemineral density and the potential forsuccess of internal fixation than isage.25 After adjusting for magnifica-tion, medial and lateral corticalthickness is measured from the an-teroposterior view of the proximalhumerus.25 The first level, the mostproximal aspect of the humeral di-aphysis, occurs at the level in whichthe endosteal borders of the medialand lateral cortices are parallel. Thesecond level is 20 mm distal to the
first level. The combined corticalthickness is the average of the medi-al and lateral cortical thickness atthe two levels25 (Figure 4). Nonsurgi-cal treatment, suture fixation, andhemiarthroplasty may be the bestoptions for the patient with com-bined cortical thickness <4 mm.Cortical thickness ≥4 mm is consid-ered necessary for adequate screwpurchase with standard internal fix-ation.25
NonsurgicalManagement
Nonsurgical management tradition-ally has been recommended for non-displaced and minimally displacedproximal humerus fractures. Slingimmobilization with or withoutclosed reduction also has a role
in the management of displacedproximal humerus fractures.3 Court-Brown and colleagues26,27 recom-mend 2 weeks of sling immobiliza-tion followed by physical therapy forpatients with two-part surgical neckfractures27 and valgus-impacted frac-tures.26 Two-part proximal humerusfractures with >66% translationwere treated with either a sling orwith internal fixation with flexibleintramedullary nailing and tension-band wires.26,27 No statistical differ-ence was reported between thegroups in terms of Neer score,4,28 re-turn to activities of daily living, andfracture union.26,27 The data demon-strate that the raw Constant score(Table 1) deteriorates with advancingage and degree of displacement.However, when calculated based onage-adjusted Constant score, the
Figure 3
2-SN(<66%)Sling
2-SN(>66%)TOSF
2-SN(<66%)Sling
2-SN(>66%)CRPF
orORIF
SlingORIFwithLCP± BG
HemiORIFwithLCP± BG
Hemi
ORIFwithLCP± BG
<4 mm Cortex >4 mm Cortex <4 mm Cortex >4 mm Cortex <4 mm Cortex >4 mm Cortex
AO/ASIFtype A
(unifocal)
AO/ASIFtype B
(bifocal)
AO/ASIFtype C
(anatomic neck)
Displacedproximalhumerusfracture
Treatment algorithm for proximal humerus fracture. The systematic approach includes assessing vascular status, assigningfracture type using the AO/ASIF classification, assessing bone quality (ie, measure cortex), and applying the Hertel criteria(ie, medial hinge [>2 mm], metaphyseal extension [<8 mm]). 2-SN (<66%) = two-part surgical neck fracture with <66%translation, 2-SN (>66%) = two-part surgical neck fracture with >66% translation, BG = bone graft or bone graft substitute,CRPF = closed reduction and percutaneous fixation, Hemi = hemiarthroplasty, LCP = locking compression plate, ORIF = openreduction and internal fixation, TOSF = transosseous suture fixation
Shane J. Nho, MD, et al
Volume 15, Number 1, January 2007 15

older patients actually had betterscores than did the younger pa-tients.26,27,29,30 Therefore, sling immo-bilization is an appropriate treat-ment option for patients older thanage 60 years with valgus-impacted,two-part surgical neck or two-parttuberosity fractures.
Surgical Management
Transosseous SutureFixation
AO/ASIF type A fractures with>66% translation and combined cor-tical thickness <4 mm are appropri-ate candidates for suture fixationwith tension band constructs. Ten-sion band fixation takes advantage ofthe soft-tissue anchorage of the rota-tor cuff tendon, which provides
stronger fixation than does the softbone of the humeral head.18 Tensionband, figure-of-8 constructs incorpo-rating the rotator cuff tendons haveproved to be an excellent method offixation for tuberosity fractures.18,31
For isolated greater tuberosity frac-tures with >5 mm of displacement,Flatow et al32 describe a transosseoussuture fixation technique using a lat-eral approach to the shoulder. Fouror five no. 2 nonabsorbable suturesare passed through the supraspinatustendon, and drill holes are created inthe humerus to secure anatomic re-duction of the greater tuberosityfragment.
Transosseous suture fixation alsocan be done on two-part surgicalneck fractures and three-part proxi-mal humerus fractures.32-34 Three
no. 2 or no. 5 nonabsorbable suturesare inserted into the supraspinatusand subscapularis tendons to obtaincontrol of the head fragment. Thehead is reduced over the humeralshaft, and drill holes are made on ei-ther side of the bicipital groove to re-approximate the head to the shaft(Figure 5). With a three-part fracture,in order to stabilize the greater tu-berosity fragment, the sutures in thefragment are passed through transos-seous humeral shaft drill holes afterthe head is reduced to the shaft andthe rotator interval is closed. Sever-al studies report similarly good clin-ical results in two-part, three-part,and valgus-impacted proximal hu-merus fractures, as well as a low rateof complications, including osteone-crosis.19,32,34
Closed Reduction andPercutaneous Fixation
Closed reduction and percutane-ous fixation with either threadedpins or screws is a reasonable optionin AO/ASIF type A (unifocal) frac-tures with translation >66% andcombined cortical thickness >4 mm.The advantage of closed reductionwith percutaneous fixation is that itrequires minimal surgical dissectionwith less disruption of the remain-ing vascular supply. Adequate corti-cal purchase is required; thus, os-teoporotic bone with extensivecomminution is a relative contrain-dication.
Using fluoroscopy, an indirectclosed reduction is performed. Ifnecessary, a pointed hook retractorcan be introduced into the subacro-mial space to assist in the reduction.Two to three threaded Kirschnerpins (0.045 to 0.0625 in) engage thelateral cortex distal to the deltoid in-sertion and then are advanced intothe subchondral bone of the hu-meral head without penetrating thearticular surface. For greater tuber-osity fractures in isolation or in con-junction with surgical neck frac-ture, two pins should purchase themedial cortex >20 mm distal to the
FIgure 4
Anteroposterior radiographs of the proximal humerus demonstrating the two levelsused to measure the combined medial and lateral cortical thickness of the humeraldiaphysis. Level one, the most proximal aspect of the humeral diaphysis, occursat the level in which the endosteal borders of the medial and lateral cortices areparallel. Level two is 20 mm distal to the first level. Examples of patients with lowbone mineral density (A) and high bone mineral density (B). (Reproduced withpermission from Tingart MS, Apprelexa M, von Stechow D, et al: The corticalthickness of the proximal humeral diaphysis predicts bone mineral density of theproximal humerus. J Bone Joint Surg Br 2003;85:611-617.)
Innovations in the Management of Displaced Proximal Humerus Fractures
16 Journal of the American Academy of Orthopaedic Surgeons

inferior border of the head. How-ever, if anatomic reduction cannotbe obtained with indirect reductionmaneuvers, the surgeon should havea low threshold for converting toopen reduction techniques.
Pendulum exercises may be initi-ated after surgery, and serial radio-
graphs should be taken weekly toensure that the pins have not migrat-ed. The pins may be removed 6 to 8weeks later once fracture union ispresent, at which time active andactive-assisted ROM exercises arebegun. Good clinical results and lowrates of osteonecrosis have been
achieved with closed reduction andpercutaneous fixation in three- andfour-part fractures, even thoughthese fractures are technicallymore demanding than two-part frac-tures11 (Table 2).
Open Reduction andInternal FixationConventional Plate Fixation
Proximal humerus fractures typi-cally occur in elderly patients withosteoporotic bone; thus, successfulimplant fixation in these fracturesmust account for the mechanicaland biologic aspects of osteoporoticbone. Poor bone mineral density cor-relates with reduced ability to se-curely hold conventional plates andscrews,31 making it difficult toachieve sufficient screw torque to
Table 1
Constant Score29
Subjective Shoulder Assessment (35 total points)
Criteria Points
Pain (15 points)NoneMildModerateSevere
151050
Activities of daily living (10 points)Ability to workAbility to engage in recreational activitiesAbility to sleep
0-40-40-2
Ability to work at a specific level (10 points)WaistChestNeckHeadAbove head
2468
10
Objective Shoulder Assessment (65 points)
Criteria Points
Flexion and abduction (scored separately)>150°121°-150°91°-120°61°-90°31°-60°0°-30°
1086420
Combined active external rotation (10 points)Hand behind head, elbow forwardHand behind head, elbow backHand on top of head, elbow forwardHand on top of head, elbow backFull elevation from top of head
22222
Combined active internal rotation (10 points)Interscapular regionInferior tip of scapulaTwelfth ribLumbosacral junctionButtockLateral thigh
1086420
Strength (25 points) 1/lb
Figure 5
Transosseous suture fixation forAO/ASIF type A extra-articular, proximalhumerus fracture with <4 mmcombined cortical thickness. Thetension-band construct withtransosseous suture fixation can beused for type A fractures involving thesurgical neck, greater tuberosity, andlesser tuberosity. (Reproduced withpermission from Flatow EL, Cuomo F,Macky MG, et al: Open reduction andinternal fixation of two-part displacedfractures of the greater tuberosity ofthe proximal part of the humerus.J Bone Joint Surg Am 1991;73:1213-1218.)
Shane J. Nho, MD, et al
Volume 15, Number 1, January 2007 17

prevent plate and fracture motion.37
Screw loosening and pull-out, notimplant breakage, is the reason forconstruct failure and related poorclinical outcomes.5,33 Furthermore,with extensive comminution, par-ticularly in valgus-impacted frac-tures, using conventional screws tolag the fracture fragments to theplate typically results in malreduc-tion. Conventional plate-and-screwfixation of displaced proximal hu-merus fractures has historically beenassociated with osteonecrosis, non-union, malunion, screw cutout, andscrew loosening.7
In young patients, open reduction
and internal fixation with buttressplate fixation is appropriate for mul-tifragmentary fractures (ie, AO/ASIFtype B). The goal of buttress plate fix-ation is anatomic reduction, whichtypically can be accomplished infractures with an adequate diaphy-seal cortex (>3.5 mm) and no meta-physeal comminution.7 Disruptionof the medial hinge is a relative con-traindication to the use of buttressplate fixation.22 Buttress plate appli-cation requires extensive soft-tissuedissection, resulting in an increasedrisk of disruption of the intraosseousblood supply, which predisposes thepatient to osteonecrosis. In older, os-
teoporotic patients, reported rates ofosteonecrosis may be as high as 35%with open reduction and internal fix-ation with plate fixation.7,35 Al-though patients treated with conven-tional plate fixation may havesatisfactory clinical results evenwhen osteonecrosis develops,7,35 pa-tients without humeral head necro-sis have significantly (P < 0.0005)better clinical outcomes than do pa-tients in whom necrosis develops.7
Plates should not be used tobridge gaps in osteoporotic bone;however, double-plating on the op-posite cortex may be a reasonable al-ternative for stabilizing such gaps.5
Table 2
Recent Studies on the Treatment of Proximal Humerus Fractures
StudyNo. of
ShouldersFracture Pattern
(No.) Treatment Outcome ScoreComplications
(No.)
Court-Brownet al26
125 Minimal (57), greatertuberosity (19), surgicalneck (18), greatertuberosity and surgicalneck (31)
Sling Mean Constant, 71.8Mean Neer, 80.6% good to
excellent
NR
Chenet al33
19 Two-part (13),three-part (6)
CRPF Neer, 84% good toexcellent
Painfulhardware(1 [6%]),osteonecrosis(0)
Reschet al11
27 Three-part (9), four-part(18)
CRPF Average Constant,three-part: 85.4 (91%)
Average Constant,four-part: 82.5 (87%)
Osteonecrosis infour-part(2 [11%])
Parket al34
28 Greater tuberosity (13),surgical neck (9), greatertuberosity and surgicalneck (6)
TOSF Average ASES, 87.1Average Neer, 78%
excellent, 11% satisfactory,11% unsatisfactory
Second surgery(2 [7%]: 1irrigation anddébridement, 1capsulotomy),osteonecrosis(0)
Gerberet al7
34 Two-part (2), three-part(16), four-part (16)
Internalfixation(CRPF,TOSF,ORIF) ±bone graft
Mean Constant for allshoulders, 78 (89%)
Constant withoutosteonecrosis, 83 (96%)
Constant withosteonecrosis, 66 (76%)(P < 0.0005)
Osteonecrosis(12 [35%]),malunion (4[12%]),arthroplasty (2[6%],second surgery(6 [18%]: 4SAD, 1hematomaevacuation, 1capsulotomy)
ASES = American Shoulder and Elbow Surgeons, CRPF = closed reduction and percutaneous fixation, NR = not reported,ORIF = open reduction and internal fixation, SAD = subacromial decompression, TOSF = transosseous suture fixation
Innovations in the Management of Displaced Proximal Humerus Fractures
18 Journal of the American Academy of Orthopaedic Surgeons

Wanner et al10 managed 60 shoulderswith one-third tubular plates fixedorthogonally on the anterior and lat-eral cortices (Figure 6). Sixty-threepercent of patients had good or verygood results. Seven patients (12%)experienced complications, includ-ing fracture displacement, osteone-crosis, adhesive capsulitis, subacro-mial impingement, and hardwareloosening.10
Locking Plate FixationLocking plate technology has
been developed as a potential solu-tion to the difficulties encounteredusing conventional plating to treat
fractures in osteoporotic bone, par-ticularly with metaphyseal commi-nution. The key to this technology isthe fixed-angle relationship betweenthe screws and plate. The threadedscrew heads are locked into thethreaded plate holes to prevent screwtoggle, slide, and pull-out, thus di-minishing the possibility of primaryor secondary loss of reduction.38 Theload is transmitted from the bone tothe plate via the screw-platethreaded connection. Because theplate and screws form a single stablesystem, the stability of the fracturedepends on the stiffness of the entireconstruct.38 Analogous to multiple,
small blade plates,8 several longmetaphyseal screws locked to theplate perpendicular to the limb axisare better able to resist cantileverbending forces and torsional forces.8Precontoured, fixed-angle plate de-signs likely provide a mechanical ad-vantage in fractures with metaphy-seal comminution that lack bonycontact opposite the plate.8
For AO/ASIF type B (bifocal) andtype C (anatomic neck) proximal hu-merus fractures, humeral head pres-ervation may be accomplished withthe contoured proximal humeruslocking compression plate6,12 and,when necessary, bone graft or bone
Table 2 (continued)
StudyNo. of
ShouldersFracture Pattern
(No.) Treatment Outcome ScoreComplications
(No.)
Wijgmanet al35
60 Three- andfour-part
ORIF withcerclage wiresor T-plate
Constant, 87% good orexcellent, 13% poor
Osteonecrosis (22 [37%]:17 [77%] had good orexcellent Constantscore)
Hessmannet al36
98 Two-part (50),three-part (37),four-part (6)
ORIF withT-plate ± bonecement orbone graft
Constant, 69% good toexcellent
Neer, 59% good toexcellent
Malunion (20 [20%]),osteonecrosis (3 [4%]),nonunion (1 [1%])
Wanneret al10
71 (60available
forfollow-up)
Two-part (10),three-part (41),four-part (20)
ORIF withdoubleone-thirdtubular plate
Mean Constant, 61 (78%) Complications (7 [12%]):fracture displacement,osteonecrosis, frozenshoulder, SAD,loosening
Age and pattern had noeffect on outcome
RobinsonandPage9
25 Valgusimpacted
Screws withNorianSkeletalRepairSystem, orbuttress platewith NorianSkeletalRepair System
Constant (median), 80Dash (median), 22
Impingement (3 [12%]),wound infection(2 [8%]), adhesivecapsulitis (1 [4%]),osteonecrosis (0)
Fankhauseret al6
29 AO type A (4),type B (15),type C (9)
ORIF withlocking plate
Mean Constant (allshoulders), 74.6
Type A, 82.6Type B, 78.3Type C, 64.6
Redislocation (4 [14%]),varus malunion(1 screw cutout; 2impingement) (3 [10%]),partial osteonecrosis(2 [7%]), plate breakage(1 [3%]), deep infection(1 [3%])
ASES = American Shoulder and Elbow Surgeons, CRPF = closed reduction and percutaneous fixation, NR = not reported,ORIF = open reduction and internal fixation, SAD = subacromial decompression, TOSF = transosseous suture fixation
Shane J. Nho, MD, et al
Volume 15, Number 1, January 2007 19

graft substitute.7,9,39 Open reductionand locked plate fixation is contrain-dicated in some fracture-dislocationpatterns, head-splitting fractures, andimpression fractures involving >40%to 50% of the articular surface.15,40,41
Surgical TechniqueThe patient may be positioned in
the lateral decubitus position, su-pine on a radiolucent table, or in thebeach chair position. We prefer toplace the patient in the beach chairposition and to use a standard del-topectoral approach. The anteriorone third of the deltoid is dissectedoff its insertion into the deltoid tu-bercle. When necessary, the greaterand lesser tuberosity fragments aretagged with 5-0 braided, nonabsorb-able suture. For three- and four-partfractures, the tuberosity fragmentsare reduced to the lateral cortex ofthe shaft. Reduction of the tuberos-ities may indirectly reduce the headfragment; alternatively, to restorethe medial calcar of the proximal hu-merus, an elevator can be inserted to
disimpact the head fragment. Thefracture must be reduced and provi-sionally fixed into position beforepermanent fixation with the con-toured proximal humerus lockingplate.
The tagged sutures are passedthrough the proximal humerusplate, and the plate is positioned di-rectly in the middle of the lateralcortex (Figure 7, A). On the antero-posterior view, the plate should bepositioned roughly 8 mm distal tothe superior tip of the greater tuber-osity; from the lateral view, the plateshould be centered against the later-al aspect of the greater tuberosity(Figure 7, B). An adequate gap shouldbe left between the plate and the bi-ceps tendon to prevent disruption ofthe anterior humeral circumflex ar-tery. The initial screw is placed inthe elongated hole in the humeralshaft so that the height of the platecan be adjusted. Once appropriatefracture reduction and plate positionhave been achieved, the lockedscrews are inserted into the humer-
al head using the insertion guide andsleeve assembly. At least three distalshaft screws are inserted. The finalfluoroscopic images should demon-strate anatomic reduction of theproximal humerus fracture (Figure 7,C and D).
ResultsFankhauser et al6 reported the
first series of patients treated withproximal humerus locking plates.Twenty-nine shoulders with proxi-mal humerus fractures (5 AO/ASIFtype A, 15 type B, 9 type C) were eval-uated at minimum 1-year follow-upusing Constant scores and plain ra-diographs. Mean Constant score forall patients at 1 year was 74.6 (typeA, 82.6; type B, 78.3; type C, 64.6).Four patients had redislocation; onefracture was associated with a deepinfection. Three patients had varusmalunion in which the screws cutthrough the humeral head; in twoof these patients, subacromial im-pingement developed because theplate was positioned too proximal.
Figure 6
Open reduction and internal fixation of four-part (AO/ASIF type B) proximal humerus fracture with double, one-third tubularplates. A, Anteroposterior (left) and scapular-Y (right) injury radiographs demonstrating four-part proximal humerus fracture.B, Postoperative anteroposterior (left) and scapular-Y (right) radiographs following placement of one-third tubular plates on thelateral and anterior cortices of the proximal humerus. (Reproduced with permission from Wanner GA, Wanner-Schmid E,Romero J, et al: Internal fixation of displaced proximal humeral fractures with two one-third tubular plates. J Trauma2003;54:536-544.)
Innovations in the Management of Displaced Proximal Humerus Fractures
20 Journal of the American Academy of Orthopaedic Surgeons

Only 2 of the 29 patients in thestudy had partial osteonecrosis ofthe humeral head. In one patient,the plate fractured before fracturehealing, necessitating revision sur-gery.6
Strohm et al12 reported 64% goodand very good results in 35 patientstreated with the proximal humeruslocking plate. Partial humeral headnecrosis was noted in 16% of pa-tients. The authors reported thatsome patients have a high risk ofproximal screw perforation of thehumeral head. Although prelimi-nary results are promising withlocking plates, additional studieswith larger cohorts and longer fol-low-up are necessary to better definethe appropriate indications for andexpected outcomes with this tech-nology.
OsteobiologicsDisplaced proximal humerus
fractures may have significantmetaphyseal comminution, whichoften is more apparent after ana-tomic reduction of fracture frag-ments. Bone graft or bone graft sub-stitute may be used as a localadjuvant to fracture healing. The in-dications have not yet been clearlydefined, but improved rates of frac-ture healing and decreased rates ofmalunion have been reported.7,36
Autogenous bone graft, which hasbeen shown to have osteoinductive,osteoconductive, and osteogenic31
properties, can stimulate new boneformation in metaphyseal defectsassociated with complex proximalhumerus fractures. Elderly, os-teoporotic patients have limitedquantity and quality of available il-iac crest graft, necessitating largerexposure, thus placing them at riskof increased complications associ-ated with a second surgical site.5
Bone graft substitutes are an at-tractive alternative, particularly inosteoporotic patients. Substitutes in-clude synthetic osteoconductive ma-terials, allograft bone, and deminer-alized allograft bone matrix.5,7,36
Calcium phosphate cements (eg, No-rian Skeletal Repair System, Syn-thes, West Chester, PA; Alpha BSM,Etex, Cambridge, MA) can be in-jected or molded into small bone de-fects; they provide structural supportwith good compressive strengths.42
Using the Skeletal Repair System,Robinson and Page9,39 achieved os-
seous union without evidence of os-teonecrosis in all fractures, and theaverage head-neck inclination re-mained within previously publishednormal values9 (Figure 8).
The disadvantages of calciumphosphate cements are poor shearstrength, slow resorption, and com-plete lack of osteoinductivity.42 For
Figure 7
Treatment of AO/ASIF type B proximal humerus fracture with locked plate fixation.A, Tagged sutures are passed through the proximal humerus locking plate. B,Locked plate on the lateral cortex with suture fixation to the plate. Anteroposterior(C) and internal rotation (D) radiographs demonstrating anatomic reduction afteropen reduction and internal fixation with a proximal humerus locking plate.
Shane J. Nho, MD, et al
Volume 15, Number 1, January 2007 21

larger metaphyseal defects (>20 mLvolume), structural allograft, morcel-lized allograft, or autograft may beused to fill the void.39 Demineralizedhuman bone matrix can enhancestructural integrity and has variableosteoinductive properties; however,
as with other allografts, there arerisks, including unpredictable qual-ity and the possibility (howeverslight) of disease transmission.42 Bonegraft substitute in conjunction withlocked plate fixation has not yet beenstudied, and its effect on fracture
union and malunion is unknown.
HemiarthroplastyTraditionally, the indications for
hemiarthroplasty in the manage-ment of proximal humerus fracturesare four-part fractures, three-part
Figure 8
Use of the Norian Skeletal Repair System (Synthes) to repair metaphyseal defects in the humeral head. A, After provisionalfixation of the fracture and tagged tuberosity sutures, the metaphyseal defect is evident between the articular fragment and thetuberosity fragments. B, Fluoroscopic image demonstrating the area of radiolucency after anatomic reduction. C, Themetaphyseal cavity is closed by suturing together the tuberosity fragments. Anteroposterior (D) and modified axial (E)radiographs demonstrating anatomic reduction after open reduction and internal fixation and use of the Norian Skeletal RepairSystem (the radiodense area behind the humeral head). GT = greater tuberosity, LT = lesser tuberosity. (Reproduced withpermission from Robinson CM, Page RS: Severely impacted valgus proximal humeral fractures. J Bone Joint Surg Am 2004;86[suppl 1 pt 2]:143-155.)
Innovations in the Management of Displaced Proximal Humerus Fractures
22 Journal of the American Academy of Orthopaedic Surgeons

fractures in older patients withosteoporotic bone, fracture-disloca-tions, head-splitting fractures, andimpression fractures involving>40% to 50% of the articular sur-face.15,40,41 The tenuous fixation offracture fragments in osteoporoticbone15 and the high rates of osteone-crosis in the humeral head afterthree- or four-part fracture suggestthat hemiarthroplasty is a bettertreatment alternative for these frac-ture patterns. Although hemiarthro-plasty has been shown to providegood pain relief, achieving excellentROM has been less predictable.Rehabilitation, particularly earlypassive ROM43,44 and long-term ac-tive ROM and strengthening, is con-sidered essential to achieve optimaloutcome after shoulder hemiarthro-plasty.43,45 In recent studies, theresults of hemiarthroplasty forproximal humerus fractures havebeen reasonable, although not quiteas good as the results in earlierstudies.15,41,43-48
Surgical TechniqueShoulder hemiarthroplasty tech-
nique is well-described in the lit-erature. Typically, a standard del-topectoral approach is used. Deepsoft-tissue dissection may be mini-mal, depending on the fracture pat-tern and soft-tissue injury. It is essen-tial to identify and tag the tuberosityfragments. The humeral head andshaft fragments are exposed; the gle-noid should be carefully inspected todetermine whether a glenoid compo-nent is warranted. After adequatelyexposing and cleaning the joint, prep-aration of the humeral shaft begins.It is critical to place the humeralcomponent in the correct retrover-sion (typically 30° to 40°) and height.Different modular heads can be tri-aled to identify the optimal configu-ration. With most fractures, the stemshould be cemented to ensure rota-tional control of the prosthesis. Oncethe humeral component is secure,the proximal anatomy is restored,with particular emphasis on correct,
secure positioning of the tuberositiesthrough a variety of suturing tech-niques. Bone graft may be necessary.The shoulder should be takenthrough a ROM before closing.
ResultsRecent studies have focused on
maximizing tuberosity healing in ananatomic position and optimizingthe degree of component retrover-sion.43,49 Most authors recommend30° to 40° of retroversion, typicallyusing the bicipital groove as thelandmark for prosthesis orienta-tion.49 However, an individualizedapproach has been proposed, inwhich the contralateral humerus isused to estimate the proper retrover-sion for each patient.43 A recentstudy found no difference in terms ofmean Constant score when compar-ing patients treated with these dif-ferent techniques for achieving prop-er version, although the sample size(26 patients) and resulting statisticalsignificance were limited.43
Complications after hemiarthro-plasty include tuberosity malunionor nonunion, heterotopic ossifica-tion, degenerative changes in theglenoid, prosthetic loosening, andnerve injury. Malunion or nonunionof tuberosity osteosynthesis occursin 4% to 50% of shoulders and is themost significant complication afterhemiarthroplasty for displaced prox-imal humerus fractures.40,45,47 In onestudy, the factors that led to tuberos-ity malunion were poor intraopera-tive positioning of the prosthesis (ex-cessive height and/or retroversion),age and sex (women older than age75 years), and initial malposition ofthe greater tuberosity.47
Boileau et al47 reported an 11%rate of heterotopic ossification, sim-ilar to the rate reported by Prakash etal45 (9%), but lower than that report-ed by Mighell et al41 (27%) and Beck-er et al46 (56%). Mighell et al41 re-ported an 8% rate of degenerativechanges in the glenoid at 36-monthaverage follow-up. A recent quanti-tative radiographic analysis of gle-
noid wear after shoulder hemiarthro-plasty found a decrease in averagejoint space from 2.9 to 1 mm over amean 43-month period in eight pa-tients.50 The data suggest that func-tional outcome, as measured byConstant score, negatively correlat-ed with joint space narrowing.50
Prosthetic loosening occurs lessoften, with reported rates of 3% to6%,43,45 although higher rates of ra-diolucencies (30%) have been report-ed.47 Infection usually occurs at aneven lower rate, typically 1% to2%,41,48 although one study reporteda 7.7% rate of infection.43 Althoughup to 15% of patients may presentpreoperatively with nerve injuryfrom the original trauma,41,43,48 thereported rate of intra- or postopera-tive nerve injury typically is close tozero.41,43,45,48 However, one study re-ported a rate of 4.5%.47
Both surgeon and patient musthave realistic postoperative expecta-tions for proximal humerus fractureafter hemiarthroplasty. Typical endROM achieves shoulder-level func-tion. Although the mean reportedROM for forward flexion is oftenabove 100°,41,43,47 only 42% of pa-tients could flex above 90° in the se-ries reported by Kralinger et al.44
Most studies suggest mean internalrotation to approximately L2/L3,41,44,45 with mean external rota-tion typically varying between 20°and 40°.41,43,44,46,47 Functional resultsare usually satisfactory, with recentstudies showing a mean Constantscore between 55 and 70.43,44,47
The importance of anatomic res-toration of the tuberosities withsecure fixation and restoration ofhumeral length and retroversioncannot be overemphasized (Figure 9).One recent cadaveric study evaluat-ed a design in which the bone-tendon interface of the rotator cuff isfixed to holes in the articular rim ofthe prosthesis.51 The fixation wasstrong enough to resist fracture frag-ment displacement under the forcesassociated with activities of dailyliving, suggesting that this design
Shane J. Nho, MD, et al
Volume 15, Number 1, January 2007 23

might allow earlier rehabilitationeven in the presence of poor bonequality. Biomechanical studies haveshown that incorporation of medialcircumferential cerclage around thetuberosities decreases interfragmen-tary motion and strain, maximizesfracture stability, and facilitatespostoperative rehabilitation.52
Postoperative outcomes dependon several variables, chief amongthem displacement of the tuberosi-ties. Robinson et al48 retrospectivelyreviewed the results of shoulderhemiarthroplasty for proximal hu-merus fractures at a single center.They found consistent improvementin the Constant score from 6 weeksto 6 months postoperatively but lit-tle change thereafter. At 1 year, pa-tients reported reasonable pain reliefbut poorer scores for function, ROM,and strength. The factors assessed 6weeks postoperatively that predicted1-year Constant score included pa-tient age, persistent neurologic defi-cit, need for early revision, as well asthe degree of displacement of theprosthetic head from the central axisof the glenoid and the degree of dis-placement of the tuberosities (seenradiographically).
In their retrospective multicenterreview, Kralinger et al44 (P = 0.0001)found that patients with healed,nondisplaced tuberosities had signif-icantly higher Constant scores andsubjective patient satisfaction scores(P = 0.031) than did patients whosetuberosities did not heal or healed indisplacement >0.5 cm. However,pain did not correlate with displace-ment of the tuberosity. AlthoughColeman and Craig53 also reportedno difference in overall pain scorebetween patients with a healedgreater tuberosity and those with-out, their retrospective review didfind greater forward flexion and ex-ternal rotation in patients with ahealed greater tuberosity. In a retro-spective review of the results of asingle surgeon, Mighell et al41 foundsignificantly lower ASES (P < 0.01)and Simple Shoulder Test (P < 0.001)scores as well as decreased forwardflexion in patients with superior mi-gration of the greater tuberosity.
The optimal timing of hemiar-throplasty is important—specifical-ly, acute versus late reconstruction.Because it is technically easier, acutetreatment is generally preferable tolater hemiarthroplasty. Most recent
reports tend to show better resultsafter early treatment,41,46 althoughone study found no difference be-tween early (≤30 days postinjury)and late (>30 days postinjury) treat-ment.45 A series of 27 displaced four-fragment fractures of the proximalhumerus treated with hemiarthro-plasty showed better shoulder mo-tion (measured by video motionanalysis) and better clinical out-comes (Neer and Constant scores)when treated within 2 weeks of inju-ry, compared with those treated lat-er.46 Mighell et al41 found significant-ly (P < 0.01) greater ASES scores inpatients treated within 2 weeks ofinitial injury. Prakash et al45 did notfind any difference in final ROM be-tween patients who underwent sur-gery within 30 days of initial injuryand patients who underwent surgerymore than 30 days after injury, eventhough the mean time from injury tosurgery among the latter group was13 months.
Summary
Proximal humerus fracture manage-ment is constantly evolving, partic-ularly in light of improved under-
Figure 9
Anteroposterior (A), scapular-Y (B), and axillary (C) radiographs following shoulder hemiarthroplasty.
Innovations in the Management of Displaced Proximal Humerus Fractures
24 Journal of the American Academy of Orthopaedic Surgeons

standing of proximal humerusfracture characteristics and innova-tions in surgical technique and tech-nology. The orthopaedic surgeonshould approach proximal humerusfractures on a case-by-case basis andtailor treatment according to pa-tient and fracture characteristics.Treatment decision-making shouldinclude assessing the vascular sta-tus of the humeral head, determin-ing the optimal fixation constructs,and implementing local adjuvantsas needed to enhance anatomic frac-ture healing. The likelihood of hu-meral head ischemia is establishedusing the AO/ASIF classificationand Hertel’s radiographic criteria.Fractures with AO/ASIF type C pat-tern, metaphyseal extension <8mm, or medial hinge displacement>2 mm are associated with highprobability of osteonecrosis andprobably are best treated with hemi-arthroplasty.
When fixation is required, frac-ture pattern and cortical thicknessshould guide the treatment approachand fixation technique. AO/ASIFtype A fractures are typically treatedwith sling immobilization. Proximalhumerus fractures with surgicalneck translation >66% or tuberositydisplacement >5 mm may be treatedwith transosseous suture fixation(cortex <4 mm) or closed reductionand percutaneous fixation (cortex >4mm). For multifragment fractures,locked compression plating creates astable construct with preservation ofthe periosteal blood supply. Calciumphosphate cement, demineralizedbone matrix, and allografts are im-portant local adjuvants that may im-prove rates of osseous union andminimize malunion. Given recentdevelopments in locking plate andosteobiologics technology, the mostrelevant question may be whetheropen reduction and internal fixationwill in future produce better resultsthan hemiarthroplasty and, if so, inwhich patients.
References
Evidence-based Medicine: There areno level I or II randomized prospec-tive studies referenced. The majori-ty of references are observational co-hort or case control studies (level III/IV) or expert opinion (level V).
Citation numbers printed in boldtype indicate references publishedwithin the past 5 years.
1. Baron JA, Barrett JA, Karagas MR: Theepidemiology of peripheral fractures.Bone 1996;18(3 suppl):209S-213S.
2. Naranja RJ Jr, Iannotti JP: Displacedthree- and four-part proximal humer-us fractures: Evaluation and manage-ment. J Am Acad Orthop Surg 2000;8:373-382.
3. Schlegel TF, Hawkins RJ: Displacedproximal humerus fractures: Evalua-tion and treatment. J Am AcadOrthop Surg 1994;2:54-66.
4. Neer CS II: Displaced proximal hu-meral fractures: I. Classification andevaluation. J Bone Joint Surg Am1970;52:1077-1089.
5. Cornell CN: Internal fracture fixationin patients with osteoporosis. J AmAcad Orthop Surg 2003;11:109-119.
6. Fankhauser F, Boldin C, SchippingerG, Haunschmid C, Szyszkowitz R: Anew locking plate for unstable frac-tures of the proximal humerus. ClinOrthop Relat Res 2005;430:176-181.
7. Gerber C, Werner CM, Vienne P: In-ternal fixation of complex fractures ofthe proximal humerus. J Bone JointSurg Br 2004;86:848-855.
8. Haidukewych GJ: Innovations inlocking plate technology. J Am AcadOrthop Surg 2004;12:205-212.
9. Robinson CM, Page RS: Severely im-pacted valgus proximal humeral frac-tures: Results of operative treatment.J Bone Joint Surg Am 2003;85:1647-1655.
10. Wanner GA, Wanner-Schmid E,Romero J, et al: Internal fixation ofdisplaced proximal humeral fractureswith two one-third tubular plates.J Trauma 2003;54:536-544.
11. Resch H, Povacz P, Frohlich R,Wambacher M: Percutaneous fixationof three- and four-part fractures of theproximal humerus. J Bone Joint SurgBr 1997;79:295-300.
12. Strohm PC, Kostler W, Sudkamp NP:Locking plate fixation of proximalhumerus fractures. Techniques inShoulder & Elbow Surgery 2005;6:8-13.
13. Resch H, Beck E, Bayley I: Recon-struction of the valgus-impacted hu-meral head fracture. J ShoulderElbow Surg 1995;4:73-80.
14. Zyto K, Ahrengart L, Sperber A,Tornkvist H: Treatment of displacedproximal humeral fractures in elderlypatients. J Bone Joint Surg Br 1997;79:412-417.
15. Zyto K, Wallace WA, Frostick SP, Pre-ston BJ: Outcome after hemiarthro-plasty for three- and four-part frac-tures of the proximal humerus.J Shoulder Elbow Surg 1998;7:85-89.
16. Lee SH, Dargent-Molina P, Breart G,EPIDOS Group. Epidemiologie del’Osteoporose Study: Risk factors forfractures of the proximal humerus:Results from the EPIDOS prospectivestudy. J Bone Miner Res 2002;17:817-825.
17. Robertson DD, Yuan J, Bigliani LU,Flatow EL, Yamaguchi K: Three-dimensional analysis of the proximalpart of the humerus: Relevance to ar-throplasty. J Bone Joint Surg Am2000;82:1594-1602.
18. Hawkins RJ, Bell RH, Gurr K: Thethree-part fracture of the proximalpart of the humerus: Operative treat-ment. J Bone Joint Surg Am 1986;68:1410-1414.
19. Panagopoulos AM, Dimakopoulos P,Tyllianakis M, et al: Valgus impactedproximal humeral fractures and theirblood supply after transosseous sutur-ing. Int Orthop 2004;28:333-337.
20. Gerber C, Schneeberger AG, Vinh TS:The arterial vascularization of the hu-meral head: An anatomical study.J Bone Joint Surg Am 1990;72:1486-1494.
21. Brooks CH, Revell WJ, Heatley FW:Vascularity of the humeral head afterproximal humeral fractures: An ana-tomical cadaver study. J Bone JointSurg Br 1993;75:132-136.
22. Hertel R, Hempfing A, Stiehler M,Leunig M: Predictors of humeral headischemia after intracapsular fractureof the proximal humerus. J ShoulderElbow Surg 2004;13:427-433.
23. Müller ME: Appendix A: The compre-hensive classification of fractures oflong bones, in Müller ME, AllgöwerM, Schneider R, Willenegger H (eds):Manual of Internal Fixation: Tech-niques Recommended by the AO-ASIF Group. Berlin, Germany:Springer-Verlag, 1991, pp 118-125.
24. Siebenrock KA, Gerber C: The repro-ducibility of classification of fracturesof the proximal end of the humerus.J Bone Joint Surg Am 1993;75:1751-1755.
Shane J. Nho, MD, et al
Volume 15, Number 1, January 2007 25

25. Tingart MJ, Apreleva M, von StechowD, Zurakowski D, Warner JJ: The cor-tical thickness of the proximal hu-meral diaphysis predicts bone mineraldensity of the proximal humerus.J Bone Joint Surg Br 2003;85:611-617.
26. Court-Brown CM, Cattermole H, Mc-Queen MM: Impacted valgus frac-tures (B1.1) of the proximal humerus:The results of non-operative treat-ment. J Bone Joint Surg Br 2002;84:504-508.
27. Court-Brown CM, Garg A, McQueenMM: The translated two-part fractureof the proximal humerus: Epidemiol-ogy and outcome in the older patient.J Bone Joint Surg Br 2001;83:799-804.
28. Neer CS II, Watson KC, Stanton FJ:Recent experience in total shoulderreplacement. J Bone Joint Surg Am1982;64:319-337.
29. Constant CR, Murley AH: A clinicalmethod of functional assessment ofthe shoulder. Clin Orthop Relat Res1987;214:160-164.
30. Katolik LI, Romeo AA, Cole BJ,Verma NN, Hayden JK, Bach BR: Nor-malization of the Constant score.J Shoulder Elbow Surg 2005;14:279-285.
31. Cornell CN, Levine D, Pagnani MJ:Internal fixation of proximal humerusfractures using the screw-tensionband technique. J Orthop Trauma1994;8:23-27.
32. Flatow EL, Cuomo F, Maday MG,Miller SR, McIlveen SJ, Bigliani LU:Open reduction and internal fixationof two-part displaced fractures of thegreater tuberosity of the proximal partof the humerus. J Bone Joint Surg Am1991;73:1213-1218.
33. Chen CY, Chao EK, Tu YK, Ueng SW,Shih CH: Closed management and per-cutaneous fixation of unstable proxi-mal humerus fractures. J Trauma1998;45:1039-1045.
34. Park MC, Murthi AM, Roth NS,Blaine TA, Levine WN, Bigliani LU:Two-part and three-part fractures ofthe proximal humerus treated withsuture fixation. J Orthop Trauma2003;17:319-325.
35. Wijgman AJ, Roolker W, Patt TW,Raaymakers EL, Marti RK: Open re-duction and internal fixation of threeand four-part fractures of the proximalpart of the humerus. J Bone JointSurg Am 2002;84:1919-1925.
36. Hessmann M, Baumgaertel F, GehlingH, Klingelhoeffer I, Gotzen L: Platefixation of proximal humeral frac-tures with indirect reduction: Surgi-cal technique and results utilizingthree shoulder scores. Injury 1999;30:453-462.
37. Egol KA, Kubiak EN, Fulkerson E,Kummer FJ, Koval KJ: Biomechanicsof locked plates and screws. J OrthopTrauma 2004;18:488-493.
38. Wagner M: General principles for theclinical use of the LCP. Injury2003;34(suppl 2):B31-42.
39. Robinson CM, Page RS: Severely im-pacted valgus proximal humeral frac-tures: Surgical techniques. J BoneJoint Surg Am 2004;86(suppl 1 pt 2):143-155.
40. Bosch U, Skutek M, Fremerey RW,Tscherne H: Outcome after primaryand secondary hemiarthroplasty inelderly patients with fractures of theproximal humerus. J Shoulder ElbowSurg 1998;7:479-484.
41. Mighell MA, Kolm GP, Collinge CA,Frankle MA: Outcomes of hemiar-throplasty for fractures of the proxi-mal humerus. J Shoulder Elbow Surg2003;12:569-577.
42. Ladd AL, Pliam NB: Use of bone-graftsubstitutes in distal radius fractures.J Am Acad Orthop Surg 1999;7:279-290.
43. Christoforakis JJ, Kontakis GM, Kato-nis PG, Stergiopoulos K, HadjipavlouAG: Shoulder hemiarthroplasty in themanagement of humeral head frac-tures. Acta Orthop Belg 2004;70:214-218.
44. Kralinger F, Schwaiger R, WambacherM, et al: Outcome after primary hemi-arthroplasty for fracture of the head ofthe humerus: A retrospective multi-centre study of 167 patients. J BoneJoint Surg Br 2004;86:217-219.
45. Prakash U, McGurty DW, Dent JA:
Hemiarthroplasty for severe fracturesof the proximal humerus. J ShoulderElbow Surg 2002;11:428-430.
46. Becker R, Pap G, Machner A, Neu-mann WH: Strength and motion afterhemiarthroplasty in displaced four-fragment fracture of the proximal hu-merus: 27 patients followed for 1-6years. Acta Orthop Scand 2002;73:44-49.
47. Boileau P, Krishnan SG, Tinsi L,Walch G, Coste JS, Mole D: Tuberos-ity malposition and migration: Rea-sons for poor outcomes after hemiar-throplasty for displaced fractures ofthe proximal humerus. J ShoulderElbow Surg 2002;11:401-412.
48. Robinson CM, Page RS, Hill RM,Sanders DL, Court-Brown CM, Wake-field AE: Primary hemiarthroplastyfor treatment of proximal humeralfractures. J Bone Joint Surg Am 2003;85:1215-1223.
49. Kontakis GM, Damilakis J, Christo-forakis J, Papadakis A, Katonis P, Pras-sopoulos P: The bicipital groove as alandmark for orientation of the hu-meral prosthesis in cases of fracture.J Shoulder Elbow Surg 2001;10:136-139.
50. Parsons IM IV, Millet PJ, Warner JJP:Glenoid wear after shoulder hemiar-throplasty: Quantitative radiographicanalysis. Clin Orthop Relat Res2004;421:120-125.
51. De Wilde LF, Berghs BM, Beutler T,Ferguson SJ, Verdonk RC: A new pros-thetic design for proximal humeralfractures: Reconstructing the gleno-humeral unit. J Shoulder Elbow Surg2004;13:373-380.
52. Frankle MA, Ondrovic LE, Markee BA,Harris ML, Lee WE III: Stability of tu-berosity reattachment in proximal hu-meral hemiarthroplasty. J ShoulderElbow Surg 2002;11:413-420.
53. Coleman SH, Craig EV: Hemiarthro-plasty for complex fractures of theproximal humerus: Surgical tech-nique and results with the Atlas tri-modular prosthesis. Am J Orthop2002;31(1 suppl):11-17.
Innovations in the Management of Displaced Proximal Humerus Fractures
26 Journal of the American Academy of Orthopaedic Surgeons




















