
Influence of heart rate in the selection of the optimal reconstruction window in routine clinical...
14
Abstract Purpose. The aim of our study was to assess the influence of heart rate on the selection of the optimal reconstruction window with 40-slice multidetector-row computed tomography (40-MDCT) coronary angiography. Materials and methods. We studied 170 patients (114 men, age 60±11.3 years) with suspected or known coronary artery disease with 40-MDCT coronary angiography. Patients [mean heart rate (HR) 62.9±9.3 bpm, range 42–94 bpm] were clustered in two groups (group A: HR ≤65 bpm; group B: HR >65 bpm). Multiphase reconstruction data sets were obtained with a retrospective electrocardiogram (ECG)-gated 40-MDCT coronary angiography scan from 0% to 95% every 5% of the R-R interval. Two radiologists in consensus evaluated the best data sets for diagnostic purposes. Results. In group A, the optimal reconstruction windows were at 70% (55/110, 71/110 and 69/110 for the right coronary artery, left anterior descending and the left circumflex, respectively) and 75% (26/110, 28/110 and 28/110, respectively) of the R-R interval. In group B, a wide range of reconstruction windows were employed, both in the end-systolic phase at 40% (32/60, 18/60 and 17/60, for the right coronary artery, left anterior descending and circumflex, respectively) and diastolic phases at 70% (12/60, 22/60 and 19/60, respectively). Six scans were excluded due to severe respiratory artefacts. Conclusions. Optimal position of the image reconstruction Riassunto Obiettivo. Scopo del nostro studio è valutare l’influenza della frequenza cardiaca (FC) nella scelta della migliore fase di ricostruzione in angiografia coronarica mediante TC a 40 strati (AC-TCMS). Materiali e metodi. Centosettanta pazienti (114 uomini, età 60±11,3 anni) con sospetta o nota malattia coronarica sono stati sottoposti ad AC-TCMS. I pazienti (frequenza media 62,9±9,3 bpm, range 42–94 bpm) sono stati suddivisi in due gruppi (gruppo A: FC≤65 bpm; gruppo B: FC>65 bpm). I dataset multifasici dell’AC-TCMS sono stati ricostruiti ogni 5% da 0% a 95% dell’intero intervallo R-R. Due radiologi hanno valutato in accordo i dataset utilizzabili clinicamente per la refertazione. Risultati. Nel gruppo A le fasi di ricostruzione ritenute ottimali sono state il 70% (55/110, 71/110 e 69/110, rispettivamente, per la coronaria destra – CDx – per l’interventricolare anteriore – IVA – e per la circonflessa – CX) ed il 75% (26/110, 28/110 e 28/110, rispettivamente). Nel gruppo B è stata utilizzata un ampia gamma di ricostruzioni, in particolare al 40% (32/60, 18/60 e 17/60, rispettivamente per la CDx, per l’IVA e per la CX) ed al 70% (12/60, 22/60 e 19/60, rispettivamente). Sei esami sono stati esclusi dallo studio per la presenza di artefatti da movimento respiratorio. Conclusioni. La scelta della finestra temporale di ricostruzione è significativamente dipendente dalla FC media durante la scansione. Le ricostruzioni in fase CARDIAC RADIOLOGY CARDIORADIOLOGIA Radiol med (2008) 113:644–657 DOI 10.1007/s11547-008-0303-4 Influence of heart rate in the selection of the optimal reconstruction window in routine clinical multislice coronary angiography Influenza della frequenza cardiaca sulla scelta della finestra temporale di ricostruzione ottimale nella coronaro-TC utilizzata nella routine clinica G. Runza 1 • L. La Grutta 1 • V. Alaimo 1 • L. Damiani 1 • A. La Fata 1 • F. Alberghina 1 • M. Galia 1 G. Lo Re 1 • G. Luccichenti 2 • T. Bartolotta 1 • F. Cademartiri 3,4 • M. Midiri 1 • M. De Maria 1 R. Lagalla 1 1 Department of Radiology, University Hospital “P. Giaccone”, Via del Vespro 127, 90127 Palermo, Italy 2 Department of Radiology, IRCCS – Fondazione Santa Lucia, Rome, Italy 3 Department of Radiology and Cardiology, University Hospital, Parma, Italy 4 Department of Radiology and Cardiology, Erasmus Medical Center, Rotterdam, The Netherlands Correspondence to: G. Runza, Tel.: +39-091-6552349, Fax: +39-091-6552324, e-mail: [email protected] Received: 28 May 2007 / Accepted: 31 October 2007 / Published online: 1 July 2008 © Springer-Verlag 2008
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Influence of heart rate in the selection of the optimal reconstruction window in routine clinical...

AbstractPurpose. The aim of our study was to assess the influenceof heart rate on the selection of the optimal reconstructionwindow with 40-slice multidetector-row computedtomography (40-MDCT) coronary angiography.Materials and methods. We studied 170 patients (114men, age 60±11.3 years) with suspected or knowncoronary artery disease with 40-MDCT coronaryangiography. Patients [mean heart rate (HR) 62.9±9.3 bpm,range 42–94 bpm] were clustered in two groups (group A:HR ≤65 bpm; group B: HR >65 bpm). Multiphasereconstruction data sets were obtained with a retrospectiveelectrocardiogram (ECG)-gated 40-MDCT coronaryangiography scan from 0% to 95% every 5% of the R-Rinterval. Two radiologists in consensus evaluated the bestdata sets for diagnostic purposes.Results. In group A, the optimal reconstruction windowswere at 70% (55/110, 71/110 and 69/110 for the rightcoronary artery, left anterior descending and the leftcircumflex, respectively) and 75% (26/110, 28/110 and28/110, respectively) of the R-R interval. In group B, awide range of reconstruction windows were employed,both in the end-systolic phase at 40% (32/60, 18/60 and17/60, for the right coronary artery, left anteriordescending and circumflex, respectively) and diastolicphases at 70% (12/60, 22/60 and 19/60, respectively). Sixscans were excluded due to severe respiratory artefacts.Conclusions. Optimal position of the image reconstruction
RiassuntoObiettivo. Scopo del nostro studio è valutare l’influenzadella frequenza cardiaca (FC) nella scelta della migliorefase di ricostruzione in angiografia coronarica medianteTC a 40 strati (AC-TCMS).Materiali e metodi. Centosettanta pazienti (114 uomini,età 60±11,3 anni) con sospetta o nota malattia coronaricasono stati sottoposti ad AC-TCMS. I pazienti (frequenzamedia 62,9±9,3 bpm, range 42–94 bpm) sono statisuddivisi in due gruppi (gruppo A: FC≤65 bpm; gruppo B:FC>65 bpm). I dataset multifasici dell’AC-TCMS sonostati ricostruiti ogni 5% da 0% a 95% dell’interointervallo R-R. Due radiologi hanno valutato in accordo idataset utilizzabili clinicamente per la refertazione.Risultati. Nel gruppo A le fasi di ricostruzione ritenuteottimali sono state il 70% (55/110, 71/110 e 69/110,rispettivamente, per la coronaria destra – CDx – perl’interventricolare anteriore – IVA – e per la circonflessa –CX) ed il 75% (26/110, 28/110 e 28/110, rispettivamente).Nel gruppo B è stata utilizzata un ampia gamma diricostruzioni, in particolare al 40% (32/60, 18/60 e 17/60,rispettivamente per la CDx, per l’IVA e per la CX) ed al70% (12/60, 22/60 e 19/60, rispettivamente). Sei esamisono stati esclusi dallo studio per la presenza di artefattida movimento respiratorio.Conclusioni. La scelta della finestra temporale diricostruzione è significativamente dipendente dalla FCmedia durante la scansione. Le ricostruzioni in fase
CARDIAC RADIOLOGYCARDIORADIOLOGIA
Radiol med (2008) 113:644–657DOI 10.1007/s11547-008-0303-4
Influence of heart rate in the selection of the optimal reconstructionwindow in routine clinical multislice coronary angiography
Influenza della frequenza cardiaca sulla scelta della finestra temporale diricostruzione ottimale nella coronaro-TC utilizzata nella routine clinica
G. Runza1 • L. La Grutta1 • V. Alaimo1 • L. Damiani1 • A. La Fata1 • F. Alberghina1 • M. Galia1
G. Lo Re1 • G. Luccichenti2 • T. Bartolotta1 • F. Cademartiri3,4 • M. Midiri1 • M. De Maria1
R. Lagalla1
1Department of Radiology, University Hospital “P. Giaccone”, Via del Vespro 127, 90127 Palermo, Italy2Department of Radiology, IRCCS – Fondazione Santa Lucia, Rome, Italy3Department of Radiology and Cardiology, University Hospital, Parma, Italy4Department of Radiology and Cardiology, Erasmus Medical Center, Rotterdam, The NetherlandsCorrespondence to: G. Runza, Tel.: +39-091-6552349, Fax: +39-091-6552324, e-mail: [email protected]
Received: 28 May 2007 / Accepted: 31 October 2007 / Published online: 1 July 2008 © Springer-Verlag 2008

window relative to the cardiac cycle is significantlyinfluenced by the heart rate during scanning. Diastolicreconstruction phases often allowed an optimal assessmentin group A. Reconstruction phases from 30% to 45% areadvisable for higher heart rates.
Keywords Multislice computed tomography · Coronaryangiography · Retrospective ECG gating · Heart rate
Introduction
Coronary angiography with multidetector-row computed to-mography (MDCT) is finding increasing use in routine clin-ical practice as a noninvasive diagnostic tool for evaluatingcoronary arteries. Scanners with increasing spatial and tem-poral resolution have been developed over the years [1–6].However, regardless of their diagnostic performance, arte-facts caused by heart motion are still the greatest obstacle inclinical practice, given their negative influence on the diag-nostic accuracy of the technique.
Image quality is highly dependent on heart rate (HR) andthe reconstruction window selected using retrospective elec-trocardiogram (ECG) gating. Various studies have evaluat-ed the optimal reconstruction window with 4-slice [7–9],16-slice [10–12] and recently 64-slice CT [13]. Increasingtemporal resolution could lead to use of a single reconstruc-tion window, thus limiting the amount of data to be recon-structed and therefore the amount of data to be archived, aswell as minimising the dose of ionising radiation deliveredto the patient [14].
The aim of our study was to evaluate the influence of HRon the choice of the optimal reconstruction window for re-porting an examination performed with 40-slice MDCTcoronary angiography.
Materials and methods
Study population
Between February and May 2006, 170 consecutive patients(114 men, 56 women; mean age 60±11.3 years, range 19–80years) underwent 40-MDCT coronary angiography (Bril-liance 40, Philips Medical Systems, Cleveland, OH, USA).Indications for examination were stable angina (61), atypicalchest pain (37), unstable angina (5), follow-up of proximalstents (20), follow-up of bypass grafts (30), elevated cardio-vascular risk (patients with metabolic syndrome – 11), sus-pected coronary anomalies (2), suspected cardiac masses (2)and preoperative planning for valve replacement (2).
diastolica consentono spesso una valutazione ottimale conFC≤65 bpm. La scelta delle fasi sistoliche (30%–45%) èconsigliabile, invece, per FC più elevate.
Parole chiave Tomografia computerizzata multistrato ·Angiografia coronarica · Sincronizzazione retrospettivaall’ECG · Frequenza cardiaca
Introduzione
L’angiografia coronarica mediante tomografia computeriz-zata multistrato (AC-TCMS) viene sempre più spesso utiliz-zata nella routine clinica come strumento diagnostico noninvasivo per la valutazione delle arterie coronarie. Le ap-parecchiature con una sempre migliore risoluzione spazialee temporale si sono alternate negli ultimi anni [1–6]. Tutta-via, a prescindere dal miglioramento della performancediagnostica, gli artefatti da movimento cardiaco continuanoa costituire la più grossa difficoltà della routine clinica de-terminando un peggioramento dell’accuratezza diagnosticadella metodica.
La qualità dell’immagine è fortemente dipendente dallafrequenza cardiaca (FC) e dalla finestra temporale di rico-struzione selezionata utilizzando il gating retrospettivoall’ECG. Numerosi studi hanno valutato l’intervallo otti-male di ricostruzione con la TC a 4 strati [7–9], con la TCa 16 strati [10–12] e recentemente con la TC a 64 strati[13]. L’aumento della risoluzione temporale potrebbe con-durre in futuro all’impiego di un singolo intervallo di rico-struzione, ridimensionando l’ammontare dei dati ricostruitie, quindi, gli spazi di archiviazione, e minimizzando la dosedi radiazioni ionizzanti assorbita dal paziente [14].
Scopo del presente lavoro è valutare l’influenza della FCnella scelta della fase di ricostruzione ottimale per la refer-tazione di un esame di AC-TCMS a 40 strati.
Materiali e metodi
Popolazione studiata
Nel periodo compreso tra febbraio e maggio 2006, 170 pa-zienti (114 uomini, 56 donne; età media 60±11,3 anni, ran-ge 19–80 anni) consecutivi sono stati sottoposti ad angio-grafia coronarica TC a 40 strati (Brilliance 40, Philips Me-dical Systems, Cleveland, Ohio, USA). I pazienti hanno ese-guito l’indagine per angina stabile (n=61), dolore toracicoatipico (n=37), angina instabile (n=5), follow-up di stentprossimali (n=20), follow-up di by-pass (n=30), rischio
Radiol med (2008) 113:644–657 645

The normally recognised inclusion criteria for MDCTcoronary angiography are sinus cardiac rhythm with <70beats per minute (bpm) and ability to maintain breath-holdfor at least 15 s. For clinical reasons, our study also includedpatients with a mean HR ≥70 bpm. Unless contraindicated,patients with an initial HR ≥70 bpm (98; 57.6%) received a20-mg oral dose of propranolol (Inderal®, AstraZenecaReim, Reims, Cedex, France) 30 min prior to the examina-tion, and the entire population received a 2.5-mg dose of di-azepam (Tranquirit®, Aventis Pharma, Waterford, Ireland).Patients with demonstrated refractoriness to a single dose ofbeta-blockers received an additional dose of the same agent(73; 43%). Exclusion criteria were failure to provide in-formed consent, severe renal insufficiency (creatininaemia>120 μmol/l), known allergy to iodinated contrast material,possible pregnancy, presence of wall-motion arrhythmias(e.g. atrial fibrillation, extrasystoles, etc.), compromised res-piratory function, thyroid disorders, unstable clinical condi-tions or marked heart failure. All patients received an expla-nation of the different phases of the procedure as well as in-structions on how to correctly maintain a breath-hold.
Despite administration of 20–40 mg of beta-blockers,mean HR in 20 patients recorded during the scan was >70bpm. The patient population (mean HR 62.9±9.3 bpm,range 42–94) was divided into two groups, with a thresholdof 65 bpm (group A: HR ≤65 bpm; group B HR>65 bpm).
Scan and reconstruction parameters
All scans were performed with a 40-slice CT scanner (Bril-liance 40, Philips Medical Systems, Cleveland, Ohio, USA).A quantification of coronary calcium was performed withprospective triggering at 70% of the R-R interval with thefollowing scan parameters: FOV 150–200 mm, kV 120,mAs 70, slice thickness 2.5 and 50% overlap.
The angiographic scans were performed with the follow-ing parameters: retrospective ECG gating, number of detec-tors/collimation 40×0.625, voxel 0.34 mm3 (isotropic reso-lution), gantry rotation time 420 ms (effective temporal res-olution, with linear reconstruction algorithm at 180°, 210ms), feed/rotation 11.9 mm/s (pitch 0.2), voltage 120 kV,tube current 1,035 mAs, scan direction craniocaudal. Tubecurrent modulation was not selected by the operator.
A bolus of 120 ml of nonionic iodinated contrast material(Iomeprol, Iomeron® 400, Bracco, Milan, Italy) was injectedat a flow rate of 5 ml/s with an automatic power injector (Stel-lant, MedRAD, Pittsburgh, PA, USA) connected to an 18-gauge needle cannula with right antecubital access. To opti-mise intraluminal enhancement of the coronary arteries, thebeginning of the scan was synchronised by using the bolus-tracking technique (Philips Medical Systems, Cleveland,Ohio, USA) with a region of interest (ROI) at the level of theascending aorta. The scan began automatically with a delay of
cardiovascolare elevato (pazienti affetti da sindrome meta-bolica, n=11), sospette anomalie coronariche (n=2), so-spette masse cardiache (n=2), in previsione di un interven-to di sostituzione valvolare (n=2).
I criteri di inclusione normalmente riconosciuti per laAC-TCMS sono: ritmo cardiaco sinusale e <70 battiti perminuto (bpm), e capacità di mantenere un’apnea inspirato-ria per almeno 15 secondi. Per ragioni cliniche nel nostrostudio sono stati inclusi anche pazienti con frequenza car-diaca (FC) media ≥70 bpm. Nei pazienti che presentavanouna FC media inizialmente ≥70 bpm (n=98 pazienti,57,6%), a meno di controindicazioni, sono state sommini-strate 30 minuti prima della scansione, una dose orale di 20mg propanololo cloridrato (Inderal®, AstraZeneca Reims,Reims, Cedex, Francia), ed all’intera popolazione studiatauna dose di 2,5 mg di diazepam (Tranquirit, Aventis Phar-ma, Waterford, Irlanda). Ai pazienti con dimostrata refrat-tarietà alla singola dose di β-bloccante è stata sommini-strata una dose aggiuntiva dello stesso farmaco (n=73,43%). I criteri di esclusione sono stati: rifiuto di fornire ilconsenso informato, grave compromissione renale (creati-ninemia>120 μmol/l), allergia nota ai mezzi di contrastoiodati, possibile gravidanza, presenza di aritmie ipercineti-che (ad esempio fibrillazione atriale, extrasistolia, ecc.),compromissione della funzione respiratoria, disordini tiroi-dei, stato clinico instabile o marcata insufficienza cardiaca.A tutti i pazienti sono state spiegate le diverse fasi della pro-cedura d’esame e la corretta modalità di esecuzionedell’apnea inspiratoria.
Nonostante la somministrazione di 20–40 mg di β-bloc-cante, in 20 pazienti la FC media registrata durante lascansione si è mantenuta >70 bpm. I pazienti (frequenzacardiaca media 62,9±9,3 bpm, range 42–94 bpm) sono sta-ti suddivisi in due gruppi, impiegando un valore soglia di 65bpm (gruppo A: FC≤65 bpm; gruppo B: FC>65 bpm).
Parametri di scansione e di ricostruzione
Tutte le scansioni sono state effettuate con una TC a 40strati (Brilliance 40, Philips Medical Systems, Cleveland,Ohio, USA). È stata eseguita una quantificazione del calciocoronarico mediante gating prospettico al 70% dell’inter-vallo R-R, con i seguenti parametri di scansione: FOV150–200 mm, kV 120, mAs 70, spessore 2,5 mm e sovrappo-sizione del 50%.
Le scansioni angiografiche sono state effettuate con i se-guenti parametri: modalità di sincronizzazione retrospettivaal tracciato ECG, numero di detettori/collimazione40×0,625 mm, voxel 0,34 mm3 (risoluzione isotropica), tem-po di rotazione 420 ms (risoluzione temporale effettiva, conalgoritmo di ricostruzione lineare a 180°, 210 ms), avanza-mento/rotazione 11,9 mm/s (pitch 0,2), voltaggio del tuboradiogeno 120 kV, tensione del tubo radiogeno 1035 mAs,
646 Radiol med (2008) 113:644–657

8 s after the threshold of 120 HU was reached within the ROI.A retrospective reconstruction was performed for each
coronary artery (right coronary artery – RCA; left anteriordescending coronary artery – LAD: left circumflex coronaryartery – LCX) in the various phases of the cardiac cycle, each5% of the R-R interval from 0% to 95%, for a total of 20 da-ta sets. The reconstructions were performed with the follow-ing parameters: slice thickness 0.8 mm, reconstruction incre-ment 0.4 mm, medium (CB) and sharp (CC) convolution ker-nels. The data sets were transferred to a dedicated worksta-tion (Extended BrillianceTM Workspace, Version 3.0.1.3200,Philips Medical Systems, Cleveland, Ohio, USA).
Data analysis
Data analysis was performed on all segments of the coro-nary arteries with a diameter ≥1.5 mm. All reconstructedimages were evaluated by two radiologists with level-3 ex-perience in MDCT coronary angiography by using multi-planar reconstructions (MIP) and maximum intensity pro-jections (MIP) [15].
The data sets retrospectively reconstructed every 5% ofthe R-R interval were compared, and the data set with thebest image quality per individual vessel was identified. Foreach MDCT coronary angiography examination, a global as-sessment was made of image quality in relation to a single re-constructed data set or the integration of several data sets. Afour-point scale was used to evaluate the coronary arterieswith a diameter ≥1.5 mm: absence of motion artefacts andclear outline of the vessel (grade 1); minor artefacts with min-imal blurring (grade 2); blurring artefacts without interruptionin the course of the vessel (grade 3); artefacts with severedoubling/interruption of the course of the vessel (grade 4)[16]. A diagnostic assessment within grade 3 was consideredacceptable in terms of image quality for routine clinical prac-tice. The operators performed all evaluations by consensus.
Statistical analysis
Statistical analysis was performed with a dedicated softwarepackage (Statistica, version 5.0, StatSoft Italia, Vigonza, PD,Italy). An estimation was made of the statistical differencebetween the two groups in terms of age (t test), Agatston cal-cium score (t test), gender and administration of beta-block-ers (Fisher’s exact test). The chi-squared test was used toevaluate the difference in distribution in the systolic and di-astolic phases in the two groups for each coronary artery.
Results
No significant difference was found with regard to age(group A: 60.7±10.7 years; group B: 59.0±12.3 years;
direzione della scansione cranio-caudale. Dall’operatorenon è stata scelta la modalità di modulazione dell’ampe-raggio del tubo radiogeno.
Un bolo di 120 ml di mezzo di contrasto iodato non-ioni-co (Iomeprol, Iomeron® 400, Bracco, Milano, Italia) è sta-to iniettato con un flusso di 5 ml/s mediante iniettore auto-matico (Stellant, MedRAD, Pittsburgh, PA, USA) collegatoad un’agocannula da 18 gauge, posizionata in una vena an-tecubitale destra. Allo scopo di ottimizzare l’enhancementintraluminale dei vasi arteriosi coronarici la sincronizza-zione dell’inizio della scansione con il passaggio del bolo dimezzo di contrasto è stata eseguita mediante tecnica del Bo-lus Tracking (Philips Medical Systems, Cleveland, Ohio,USA), con una ROI (region of interest) posizionata al livel-lo dell’aorta ascendente. La scansione è partita automati-camente con un ritardo di 8 secondi dopo il raggiungimen-to all’interno della ROI di una soglia di 120 UH.
Per ogni coronaria (arteria coronaria destra, CDx; ar-teria interventricolare anteriore, IVA; arteria circonflessa,CX) è stata effettuata una ricostruzione retrospettiva nellevarie fasi del ciclo cardiaco ogni 5% dell’intervallo R-Rdallo 0% al 95% per un totale di 19 dataset. Le ricostru-zioni sono state effettuate con i seguenti parametri: spesso-re 0,8 mm, incremento 0,4 mm, filtri di convoluzione medio(CB) e sharp (CC). I dataset sono stati trasferiti su unaworkstation dedicata (Extended BrillianceTM Workspace,Versione 3.0.1.3200, Philips Medical Systems, Cleveland,Ohio, USA).
Analisi dei dati
L’analisi è stata effettuata in tutti i segmenti di arterie co-ronarie con diametro ≥1,5 mm. Tutte le immagini ricostrui-te sono state indipendentemente valutate da due radiologicon esperienza di livello 3 in AC-TCMS mediante riformat-tazioni multiplanari (MPR) e proiezioni di massima inten-sità (MIP) [15].
Tra i dataset ricostruiti retrospettivamente ogni 5%dell’intervallo R-R, è stato identificato quello con la mi-gliore qualità di immagine per singolo vaso coronarico edin grado di consentire l’ottimale espressione di un giudiziodiagnostico. Ad ogni AC-TCMS ottenuta è stato anche at-tribuito un giudizio sulla qualità d’immagine globale otte-nuta mediante un singolo dataset di ricostruzione o l’inte-grazione di più dataset. È stata utilizzata una scala in gra-di per la valutazione delle arterie coronarie con diametro≥1,5 mm: assenza di artefatti di movimento con chiara de-lineazione del vaso (grado 1); artefatti minori con minimoblurring (grado 2); artefatti da blurring senza disconti-nuità di decorso dei vasi (grado 3); artefatti severi consdoppiamento/discontinuità dei vasi (grado 4) [16]. Ungiudizio diagnostico entro il grado 3 è stato consideratoaccettabile in termini di qualità di immagine per la routine
Radiol med (2008) 113:644–657 647

p=0.29), Agatston calcium score (group A: 185±278; groupB: 205±352; p=0.68) and administration of beta-blockers(61 patients in group A; 37 patients in group B; p=0.51). Asignificantly higher number of women were found in groupB (30 patients; p < 0.05).
The number of examinations assessed as having diagnos-tic quality for routine clinical practice (absence of motionartefacts with clear outline of the vessel; minor artefactswith minimal blurring; blurring artefacts without interrup-tion in the course of the vessel) was 164. Acceptable imagequality (grades 1–3) was found in 96.5% of our population(Fig. 1; Table 1). Only six patients (3.5%) with a mean HR >65 bpm during the scan were considered grade 4, asnone of the available data sets allowed an acceptable diag-
clinica. Tutte le valutazioni sono state svolte in accordodagli operatori.
Analisi statistica
L’analisi statistica è stata eseguita con un software dedica-to (Statistica, versione 5.0, StatSoft Italia, Vigonza, PD, Ita-lia). È stata stimata la differenza statistica tra i due gruppiper età (test t di Student), calcium score calcolato secondo ilsistema di Agatston (test t di Student), sesso e somministra-zione di β-bloccanti (test esatto di Fisher). Il test del χ2 èstato utilizzato per valutare la differente distribuzione dellefasi sistoliche e diastoliche nei due differenti gruppi per cia-scuna arteria coronarica.
648 Radiol med (2008) 113:644–657
Fig. 1 Distribution of artefacts in thestudy population examined with 40-row multidetector computed tomogra-phy coronary angiography.
Fig. 1 Distribuzione degli artefattinelle indagini AC-TCMS della popo-lazione analizzata.
Table 1 Image quality of the 40-row multidetector computed tomography coronary angiography examination in the study population by vessel in the twogroups
Grade Artefacts Group A (HR ≤65 bpm) Group B (HR >65 bpm) RCA LAD LCX RCA LAD LCX
1 Absent 80 (72.7%) 102 (92.7%) 94 (85.5%) 22 (36.7%) 28 (46.7%) 24 (40%)2 Minor 24 (21.8%) 8 (7.3%) 12 (10.9%) 21 (35%) 23 (38.3%) 19 (31.7%)3 Moderate 6 (5.5%) 0 4 (3.6%) 11 (18.3%) 5 (8.3%) 12 (20%)4 Severe 0 0 0 6 (10%) 4 (6.7%) 5 (8.3%)
HR, heart rate; RCA, right coronary artery; LAD, left anterior descending coronary artery; LCX, left circumflex coronary artery
Tabella 1 Qualità delle immagini delle indagini AC-TCMS nella popolazione analizzata per singolo vaso nei due gruppi
Grado Artefatti Gruppo A (FC≤65 bpm) Gruppo B (FC>65 bpm) CDx IVA CX CDx IVA CX
1 Assenti 80 (72,7%) 102 (92,7%) 94 (85,5%) 22 (36,7%) 28 (46,7%) 24 (40%)2 Minori 24 (21,8%) 8 (7,3%) 12 (10,9%) 21 (35%) 23 (38,3%) 19 (31,7%)3 Moderati 6 (5,5%) 0 4 (3,6%) 11 (18,3%) 5 (8,3%) 12 (20%)4 Severi 0 0 0 6 (10%) 4 (6,7%) 5 (8,3%)
FC, frequenza cardiaca; CDx, arteria coronaria destra; IVA, arteria coronaria interventricolare anteriore; CX, arteria coronaria circonflessa
ARTEFACTS
nostic evaluation due to the presence of excessive motionartefacts (doubling/interruption of the vessel).
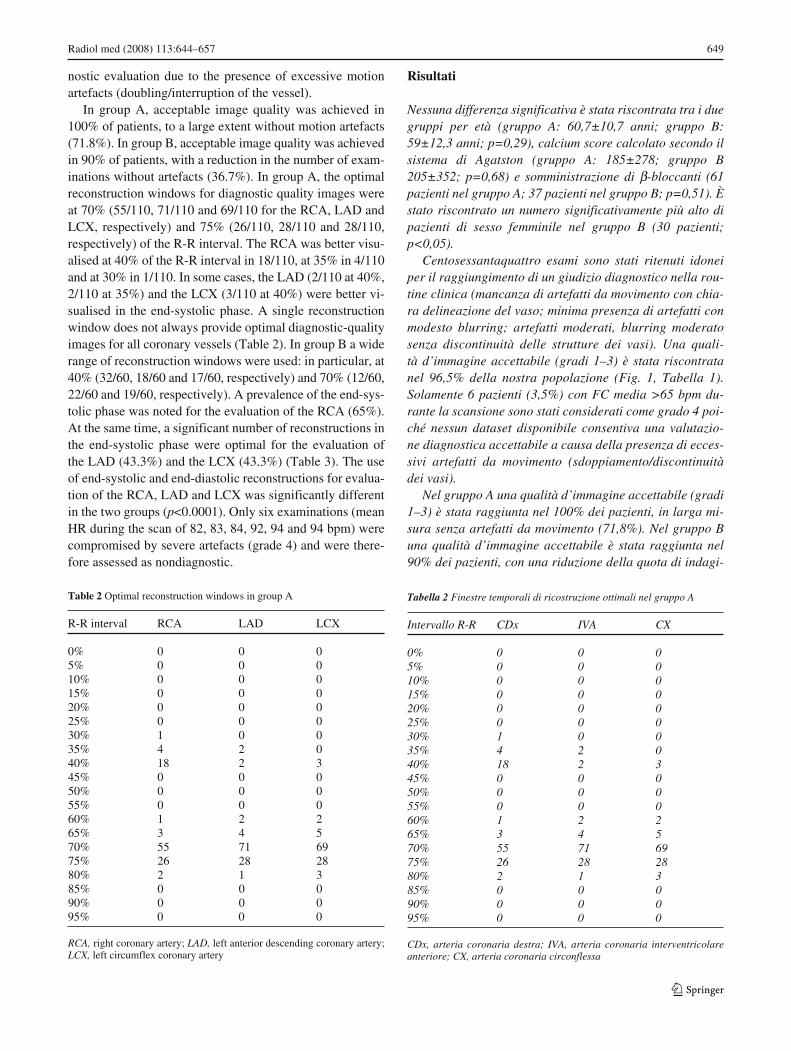
In group A, acceptable image quality was achieved in100% of patients, to a large extent without motion artefacts(71.8%). In group B, acceptable image quality was achievedin 90% of patients, with a reduction in the number of exam-inations without artefacts (36.7%). In group A, the optimalreconstruction windows for diagnostic quality images wereat 70% (55/110, 71/110 and 69/110 for the RCA, LAD andLCX, respectively) and 75% (26/110, 28/110 and 28/110,respectively) of the R-R interval. The RCA was better visu-alised at 40% of the R-R interval in 18/110, at 35% in 4/110and at 30% in 1/110. In some cases, the LAD (2/110 at 40%,2/110 at 35%) and the LCX (3/110 at 40%) were better vi-sualised in the end-systolic phase. A single reconstructionwindow does not always provide optimal diagnostic-qualityimages for all coronary vessels (Table 2). In group B a widerange of reconstruction windows were used: in particular, at40% (32/60, 18/60 and 17/60, respectively) and 70% (12/60,22/60 and 19/60, respectively). A prevalence of the end-sys-tolic phase was noted for the evaluation of the RCA (65%).At the same time, a significant number of reconstructions inthe end-systolic phase were optimal for the evaluation ofthe LAD (43.3%) and the LCX (43.3%) (Table 3). The useof end-systolic and end-diastolic reconstructions for evalua-tion of the RCA, LAD and LCX was significantly differentin the two groups (p<0.0001). Only six examinations (meanHR during the scan of 82, 83, 84, 92, 94 and 94 bpm) werecompromised by severe artefacts (grade 4) and were there-fore assessed as nondiagnostic.
Risultati
Nessuna differenza significativa è stata riscontrata tra i duegruppi per età (gruppo A: 60,7±10,7 anni; gruppo B:59±12,3 anni; p=0,29), calcium score calcolato secondo ilsistema di Agatston (gruppo A: 185±278; gruppo B205±352; p=0,68) e somministrazione di β-bloccanti (61pazienti nel gruppo A; 37 pazienti nel gruppo B; p=0,51). Èstato riscontrato un numero significativamente più alto dipazienti di sesso femminile nel gruppo B (30 pazienti;p<0,05).
Centosessantaquattro esami sono stati ritenuti idoneiper il raggiungimento di un giudizio diagnostico nella rou-tine clinica (mancanza di artefatti da movimento con chia-ra delineazione del vaso; minima presenza di artefatti conmodesto blurring; artefatti moderati, blurring moderatosenza discontinuità delle strutture dei vasi). Una quali-tà d’immagine accettabile (gradi 1–3) è stata riscontratanel 96,5% della nostra popolazione (Fig. 1, Tabella 1). Solamente 6 pazienti (3,5%) con FC media >65 bpm du-rante la scansione sono stati considerati come grado 4 poi-ché nessun dataset disponibile consentiva una valutazio-ne diagnostica accettabile a causa della presenza di ecces-sivi artefatti da movimento (sdoppiamento/discontinuitàdei vasi).
Nel gruppo A una qualità d’immagine accettabile (gradi1–3) è stata raggiunta nel 100% dei pazienti, in larga mi-sura senza artefatti da movimento (71,8%). Nel gruppo Buna qualità d’immagine accettabile è stata raggiunta nel90% dei pazienti, con una riduzione della quota di indagi-
Radiol med (2008) 113:644–657 649
Table 2 Optimal reconstruction windows in group A
R-R interval RCA LAD LCX
0% 0 0 05% 0 0 010% 0 0 015% 0 0 020% 0 0 025% 0 0 030% 1 0 035% 4 2 040% 18 2 345% 0 0 050% 0 0 055% 0 0 060% 1 2 265% 3 4 570% 55 71 6975% 26 28 2880% 2 1 385% 0 0 090% 0 0 095% 0 0 0
RCA, right coronary artery; LAD, left anterior descending coronary artery;LCX, left circumflex coronary artery
Tabella 2 Finestre temporali di ricostruzione ottimali nel gruppo A
Intervallo R-R CDx IVA CX
0% 0 0 05% 0 0 010% 0 0 015% 0 0 020% 0 0 025% 0 0 030% 1 0 035% 4 2 040% 18 2 345% 0 0 050% 0 0 055% 0 0 060% 1 2 265% 3 4 570% 55 71 6975% 26 28 2880% 2 1 385% 0 0 090% 0 0 095% 0 0 0
CDx, arteria coronaria destra; IVA, arteria coronaria interventricolareanteriore; CX, arteria coronaria circonflessa

Discussion
The acquisition of image data in MDCT coronary angiogra-phy is continuous during the cardiac cycle if retrospectivecardiac gating is used. For this reason, data corresponding tothe phase in which heart motion is at a minimum needs to be
ni AC-TCMS prive di artefatti (36,7%). Nel gruppo A le fa-si ottimali di ricostruzione per esprimere un giudizio dia-gnostico risultano al 70% (55/110, 71/110 e 69/110 per laCDx, la IVA e la CX) ed al 75% (26/110, 28/110 e 28/110,rispettivamente). La CDx è stata meglio visualizzata al40% in 18/110, al 35% in 4/110 ed al 30% in 1/110. In al-cuni casi anche la IVA (2/110 al 40%, 2/110 al 35%) e laCX (3/110 al 40%) sono state visualizzate in fase telesisto-lica. Non sempre una sola finestra temporale consente unalettura ottimale dell’esame per tutti i vasi coronarici (Ta-bella 2). Nel gruppo B è stata utilizzata un’ampia gammadi fasi di ricostruzioni: in particolare al 40% (32/60, 18/60e 17/60, rispettivamente) ed al 70% (12/60, 22/60 e 19/60,rispettivamente). È stata registrata una prevalenza dellefasi telesistoliche per la valutazione della CDx (65%). Allostesso tempo, un consistente numero di ricostruzioni in fa-se telesistolica è stato riscontrato per la valutazione di IVA(43,3%) e CX (43,3%) (Tabella 3). L’impiego delle rico-struzioni telesistoliche e telediastoliche per la valutazionedi CDx, IVA e CX è risultato significativamente differentenei due gruppi (p<0,0001). Solamente 6 indagini di AC-TCMS (FC media durante la scansione di 82, 83, 84, 92 e94, quest’ultima in due casi) sono state considerate infi-ciate da artefatti severi (grado 4) e quindi reputate nondiagnostiche.
Discussione
L’acquisizione dei dati dell’immagine in AC-TCMS è conti-nua all’interno del ciclo cardiaco se si utilizza un gatingcardiaco di tipo retrospettivo, per tale motivo i dati corri-spondenti alla fase in cui il movimento cardiaco è minimodevono essere estratti, spostando il punto d’inizio della ri-costruzione delle immagini relativamente all’onda R con ilfine di ridurre al minimo gli artefatti da blurring e da movi-mento [17].
Numerosi approcci possono essere utilizzati quando sieseguono le ricostruzioni. Possono essere elencate almenoquattro differenti tecniche: 1) percentuale di ritardo sullabase dell’onda R; 2) ritardo assoluto prospettico sulla basedell’onda R; 3) intervallo assoluto inverso sulla basedell’onda R; 4) fine della finestra temporale posizionata alvertice dell’onda P [18]. Una reale ottimizzazione della tec-nica di gating retrospettivo deve ancora essere raggiunta.Le quattro tecniche possono essere utilizzate indiscrimina-tamente, ma questo dipende dal grado di esperienzadell’operatore, dalle capacità del software/hardware e daltempo disponibile per le ricostruzioni. La fase del ciclo car-diaco che fornisce la maggior parte delle informazioni èquella compresa tra meso- e telediastole; in questa fase ilcuore è in riempimento isovolumetrico e il movimento è ri-
650 Radiol med (2008) 113:644–657
Table 3 Optimal reconstruction windows in group B
R-R interval RCA LAD LCX
0% 0 0 05% 0 0 010% 0 0 015% 0 0 020% 0 0 025% 0 0 030% 3 3 135% 2 4 640% 32 18 1745% 2 1 250% 0 0 055% 0 0 060% 1 2 265% 2 1 170% 12 22 1975% 3 6 980% 3 3 385% 0 0 090% 0 0 095% 0 0 0
RCA, right coronary artery; LAD, left anterior descending coronary artery;LCX, left circumflex coronary artery
Tabella 3 Finestre temporali di ricostruzione ottimali nel gruppo B
Intervallo R-R CDx IVA CX
0% 0 0 05% 0 0 010% 0 0 015% 0 0 020% 0 0 025% 0 0 030% 3 3 135% 2 4 640% 32 18 1745% 2 1 250% 0 0 055% 0 0 060% 1 2 265% 2 1 170% 12 22 1975% 3 6 980% 3 3 385% 0 0 090% 0 0 095% 0 0 0
CDx, arteria coronaria destra; IVA, arteria coronaria interventricolareanteriore; CX, arteria coronaria circonflessa

extracted by shifting the beginning of image reconstructionwith regard to the R wave, with the aim of reducing motionand blurring artefacts to a minimum [17].
A number of approaches can be used when performingthe reconstructions. These include: (1) relative delay strate-gy, whereby the delay time is a percentage of the R-R inter-val; (2) absolute delay strategy, whereby the delay time isconstant after the previous R wave; (3) absolute reverse de-lay strategy, whereby the delay time is constant prior to thenext R wave; (4) end of the time window positioned at thepeak of the P wave [18]. A real optimisation of retrospectivegating is yet to be achieved. The four techniques describedcan be used indiscriminately, but this depends on the degreeof experience of the operator, the software/hardware capa-bilities and the time available for reconstruction. The car-diac cycle phase that provides the most information extendsfrom mid to end diastole. In this phase, the heart is in iso-volumetric filling, and motion is at a minimum. In manycases, the end-systolic phase can provide relevant informa-tion, as the motion of the coronary arteries is also at a mini-mum at the end of myocardial contraction [8].
Multiple reconstructions are usually performed in differ-ent reconstruction windows, and later the operator selectsthe data set where motion artefacts are at a minimum, possi-bly using different reconstruction windows in the same pa-tient for visualisation of the RCA, LAD and LCX [1–5]. Ofcourse, routine clinical practice in this case is conditionedby two factors: (1) the time required by the operator to per-form the reconstructions and any consequent increase inarchiving space, and (2) the radiation dose used for retro-spective gating, which poses important questions for justifi-cation of the examination.
Various studies have investigated the relationship be-tween image quality and the optimal reconstruction windowwith 4-, 16- and 64-slice scanners [7–13, 19]. With 4-MD-CT, the LAD is best visualised at 50%–70%, the LCX at50%–60% and the RCA at 40%–50% of the R-R interval[7–9], thus indicating the need for separate reconstructionsfor the different vessels. With 16-MDCT, optimal imagequality is usually obtained in mid diastole (350 ms, –400 msor –450 ms, corresponding approximately to 60%–70%)[10], with additional reconstructions in the end-systolicphase for higher HR where required [10–12]. The study byLeschka et al. with 64-MDCT showed that additional recon-structions during systole were no longer necessary, even athigher HR, as even at HR >65 bpm, the 4% of segmentswith better image quality during systole were also of diag-nostic quality during diastole [13]. As MDCT coronary an-giography is characterised by the use of high doses of ionis-ing radiation, particularly with 64-MDCT, the results of thisstudy could pave the way for the widespread use of ECGpulsing, that is, an acquisition targeted exclusively at themid- to end-diastolic reconstruction windows, thus reducing
dotto al minimo. In numerosi casi la fase telesistolica puòfornire informazioni rilevanti; infatti, anche al termine del-la contrazione miocardica il movimento delle arterie coro-narie risulta minimo [8].
Di solito, vengono eseguite multiple ricostruzioni in dif-ferenti finestre temporali e l’operatore, successivamente,sceglie il dataset dove gli artefatti da movimento sono ri-dotti al minimo, eventualmente utilizzando nello stesso pa-ziente differenti finestre temporali per la rappresentazionedella CDx, dell’IVA e della CX [1–5]. Indubbiamente, laroutine clinica è condizionata, in questo caso, da due fatto-ri: il tempo necessario per le operazioni di ricostruzione daparte dell’operatore cui consegue certamente un aumentodegli spazi di archiviazione; la dose di radiazioni impiega-ta nell’utilizzo del gating retrospettivo che pone in partenzaseri interrogativi sulla giustificazione dell’esame.
Vari studi hanno indagato sul rapporto tra qualità d’im-magine ed intervallo temporale ottimale di ricostruzionecon differenti TC a 4, 16 e 64 detettori [7–13, 19]. Con laTC a 4 strati, l’IVA era meglio visualizzata al 50%–70%, laCX al 50%–60%, la CDx al 40%–50% dell’intervallo R-R[7–9], indicando il bisogno di ricostruzioni separate per ivari vasi. Con la TC a 16 strati la migliore qualità di imma-gine veniva solitamente raggiunta nella diastole media (–350 ms, –400 ms o –450 ms, corrispondenti approssimati-vamente al 60%–70%) [10], con eventuali ricostruzioni ad-dizionali telesistoliche per frequenze elevate [10–12]. Lostudio di Leschka et al. [13] con la TC a 64 strati ha messoin evidenza che ricostruzioni addizionali durante la sistolenon sono più necessarie, anche a frequenze elevate, dal mo-mento che anche con frequenze >65 bpm, il 4% dei segmen-ti con miglior qualità d’immagine in sistole raggiungevauna qualità d’immagine diagnostica anche in diastole [13].Dal momento che la AC-TCMS con gating retrospettivo ècaratterizzata dall’utilizzo di un’elevata dose di radiazioniionizzanti specialmente con la TC a 64 strati, i risultati diquesto studio potrebbero autorizzare in futuro all’utilizzoindiscriminato dell’ECG-pulsing, cioè ad un’acquisizionemirata esclusivamente nelle finestre temporali meso-tele-diastoliche, con riduzione di dose del 48% negli uomini edel 45% nelle donne [4, 14]. Nonostante ciò tutti gli studicon TC a 64 strati per la valutazione dell’accuratezza dia-gnostica nell’individuazione delle stenosi emodinamica-mente significative su popolazioni selezionate non applica-no questa tecnica ed utilizzano più finestre temporali di ri-costruzione del ciclo cardiaco [1–5].
La recente introduzione di TC a 64 strati con doppio tu-bo radiogeno-sistema rilevatore (dual source-CT), graziead una migliore risoluzione temporale (82,5 ms), offre lapossibilità di ottenere una qualità d’immagine indipenden-te dalla FC e rende, pertanto, superfluo l’utilizzo dei ‚-bloccanti per ridurla [20, 21]. L’utilizzo di questa nuovatecnologia di TCMS con la possibilità di modulare la cor-
Radiol med (2008) 113:644–657 651

the radiation dose by 48% in men and 45% in women [4, 14]. Despite this, most studies with 64-MDCT for the eval-uation of diagnostic accuracy in the identification of haemo-dynamically significant stenoses in selected populations donot apply this technique and, instead, use reconstruction win-dows from different phases of the cardiac cycle [1–5].
With its significant improvement in temporal resolution(82.5 ms), the recently introduced 64-slice dual-source CToffers the possibility of obtaining image quality indepen-dent of HR and therefore eliminates the need for beta-block-ers to reduce HR [20, 21]. The use of this new MDCT tech-nology could optimise tube current modulation and reducethe radiation dose delivered to the patient [20, 21]. A furtherdevelopment could be 256-MDCT with its real-time scan-ning and ECG gating, which would eliminate the need forreconstructions in different time windows of the cardiac cy-cle, although at present, the only study reported in the liter-ature is a work in progress limited to two patients [22].
In routine clinical practice, however, despite the admin-istration of beta-blockers to reduce HR or where their ad-ministration is contraindicated, the HR may unexpectedlyrise above 65 bpm (due to anxiety and reaction to high flowrates of contrast material, particularly in women). More-over, the numerous clinical applications of MDCT coronaryangiography and the variability in patient characteristics donot always allow an optimal HR to be achieved [23].
Our study, therefore, aimed to evaluate the influence ofHR on the choice of reconstruction window, independentlyof a threshold (≤65 bpm), while recognising a reduction, al-though modest, of the diagnostic value directly proportionalto the increase in HR (six group B patients were excludedwith nondiagnostic quality images due to severe motionartefacts).
In group A (HR ≤65 bpm, Figs. 1, 2), the optimal recon-struction windows were at 70% (55/110, 71/110 and 69/110for the RCA, LAD and LCX, respectively) and 75%(26/110, 28/110 and 28/110, respectively). In group B (HR>65 bpm – Figs. 3–5), in contrast, a broad range of recon-structions were used, particularly in the end-systolic phase,at 40% (32/60, 18/60 and 17/60, respectively). In this group,six examinations were judged nondiagnostic due to exces-sive motion artefacts.
Whereas the most used reconstruction windows in groupA (Fig. 7) were at 70%–75% with some exceptions (40%;18/110 for RCA, 2/110 for LAD and 3/110 for LCX), withhigh HR (group B, Fig. 8), the number of reconstructions required to achieve diagnostic quality images at MDCTcoronary angiography significantly increased, suggestingthat the use of the end-systolic phase is indispensable. Withthe temporal resolution achieved by our 40-MDCT scanner,the use of ECG pulsing appears impracticable. The bettertemporal resolution of a 64-slice scanner could allow for itsuse. Nonetheless, the current ECG-pulsing model does not
rente del tubo radiogeno potrebbe consentire l’ottimizza-zione dei meccanismi di ECG-pulsing con una riduzionedella dose di radiazioni al paziente [20, 21]. Un ulterioreavanzamento potrebbe essere rappresentato dalla TC a256 strati con scansioni real-time prive di ECG-gating, cheeliminerebbero la necessità della valutazione di ricostru-zioni in differenti finestre temporali del ciclo cardiaco, maal momento l’unica esperienza clinica riportata in Lettera-tura è un work-in-progress limitato a due soli pazienti[22].
Nella routine clinica, tuttavia, nonostante la sommini-strazione di β-bloccanti per ridurre la FC o nell’impossibi-lità di poterli somministrare per l’esistenza di controindica-zioni, ci si può confrontare, a volte inaspettatamente (ansiae reazione agli elevati flussi di infusione del mezzo di con-trasto, specialmente, nel sesso femminile), con FC media>65 bpm. Peraltro, la moltitudine di applicazioni clinichedella AC-TCMS e le variabili caratteristiche del pazienteche ne conseguono non sempre permettono di raggiungereuna FC ottimale [23].
Il nostro studio intende, quindi, valutare, utilizzando unaTC a 40 strati, l’influenza della FC media sulla scelta dellafinestra temporale di ricostruzione del ciclo cardiaco, indi-pendentemente da un valore soglia (≤65 bpm) e riconoscen-done una riduzione, anche se modesta, del valore diagnosti-co direttamente proporzionale all’aumento della FC media(6 pazienti del gruppo B esclusi dalla valutazione diagno-stica per gli eccessivi artefatti da movimento).
Nel gruppo A (FC≤65 bpm) (Figg. 1, 2) le finestre tem-porali di ricostruzione risultano ottimali al 70% (55/110,71/110 e 69/110 per la CDx, l’IVA e la CX, rispettivamente)ed al 75% (26/110, 28/110 e 28/110 per la CDx, l’IVA e laCX, rispettivamente). Nel Gruppo B (FC>65 bpm) (Figg.3–5) è stata utilizzata, invece, un’ampia gamma di ricostru-zioni, con rilievo particolare di quelle telesistoliche al 40%(32/60, 18/60 e 17/60, rispettivamente). In questo gruppo 6indagini sono state considerate non diagnostici per gli ec-cessivi artefatti da movimento.
Mentre nel gruppo A (Fig. 7) le finestre temporali di ri-costruzione più utilizzate sono quelle al 70%–75% con al-cune eccezioni (40%: 18/110 per la CDx, 2/110 per l’IVA e3/110 per la CX; 35%: 4/110 per la CDX, 2/110 per l’IVA;30%: 1/110 per la CDX), con frequenze elevate (gruppo B)(Fig. 8) il numero delle ricostruzioni per una AC-TCMSdiagnostica aumenta significativamente ed appare impre-scindibile l’utilizzo delle fasi telesistoliche. Con la risolu-zione temporale raggiunta dalla nostra apparecchiaturaTC, l’utilizzo dell’ECG-pulsing risulta prematuro. La riso-luzione temporale migliore di scanner a 64 strati potrebbeconsentirne l’utilizzo. Tuttavia il modello attuale di ECG-pulsing non appare ancora consigliabile per le valutazionicliniche dal momento che tutti gli studi di accuratezza dia-gnostica della AC-TCMS riportati in letteratura si servono,
652 Radiol med (2008) 113:644–657

Radiol med (2008) 113:644–657 653
Fig. 3 Volume-rendered reconstruc-tions performed every 5% of the R-R interval from 0% to 95% of thecardiac cycle for a total of 20 datasets in the same group A patient asFig. 2, with a mean heart rate of 49bpm. The left coronary artery tree(left main, left anterior descending,left circumflex and intermediatebranch) can also be evaluated withthe reconstruction windows in theend-systolic (40%) and mid- to end-diastolic (from 60% to 80%) cardiacphases in precisely the same way asthe right coronary artery.
Fig. 3 Riformattazioni Volume Ren-dering effettuate ogni 5% dell’inter-vallo R-R dallo 0% al 95% del ciclocardiaco per un totale di 20 dataset,nello stesso paziente del gruppo Ariportato in Fig. 2, con frequenzacardiaca media di 49 bpm. Ancheper l’albero coronarico sinistro(tronco comune, arteria coronariainterventricolare anteriore, arteriacirconflessa e ramo intermedio) èpossibile utilizzare a scopo valutati-vo diagnostico le finestre temporalidi ricostruzione sia in fase telesisto-lica (40%) che in meso-telediastoli-ca (dal 60% all’80%), in manieradel tutto sovrapponibile a quelle perl’arteria coronaria destra.
Fig. 2 Volume-rendered reconstructions performed every 5% of the R-R interval from 0% to 95% of the cardiac cycle for a total of 20 data sets in a groupA patient with a mean heart rate of 49 bpm. The images clearly show that both the end-systolic (40%) and the mid- to end-diastolic (from 60% to 80%) re-construction windows are of diagnostic quality in the evaluation of the right coronary artery.
Fig. 2 Riformattazioni Volume Rendering effettuate ogni 5% dell’intervallo R-R dallo 0% al 95% del ciclo cardiaco per un totale di 20 dataset, in un pa-ziente del gruppo A, con frequenza cardiaca media di 49 bpm. È ben dimostrata la possibilità di utilizzo a scopo valutativo diagnostico delle finestre tem-porali di ricostruzione sia in fase telesistolica (40%) che in meso-telediastolica (dal 60% all’80%), per la valutazione dell’arteria coronaria destra.

654 Radiol med (2008) 113:644–657
Fig. 4 Volume-rendered reconstruc-tions performed every 5% of the R-Rinterval from 0% to 95% of the car-diac cycle for a total of 20 data sets ina group B patient with a mean heartrate of 84 bpm. The reconstructionwindows useful for diagnostic pur-poses are those in systole (from 30%to 45%), although image quality isreduced and diagnosis is limited tothe proximal and mid segments of thecoronary artery tree.
Fig. 4 Riformattazioni Volume Ren-dering effettuate ogni 5% dell’inter-vallo R-R dallo 0% al 95% del ciclocardiaco per un totale di 20 dataset,in un paziente del gruppo B, con fre-quenza cardiaca media di 84 bpm. Lefinestre temporali di ricostruzioneutilizzabili a scopo diagnostico, an-che se con una ridotta qualitàdell’immagine e limitatamente aisegmenti prossimali e medi dell’albe-ro coronarico, sono quelle che com-prendono la sistole (dal 30% al45%).
Fig. 5 Volume-rendered reconstructions performed every 5% of the R-R interval from 0% to 95% of the cardiac cycle for a total of 20 data sets in a groupB patient with a mean heart rate of 81 bpm. The reconstruction windows useful for diagnostic purposes of the right coronary artery are those in systole (from30% to 45%).
Fig. 5 Riformattazioni Volume Rendering effettuate ogni 5% dell’intervallo R-R dallo 0% al 95% del ciclo cardiaco per un totale di 20 dataset, in un pa-ziente del gruppo B, con frequenza cardiaca media di 81 bpm. Le finestre temporali di ricostruzione utilizzabili a scopo diagnostico per l’arteria corona-ria destra sono quelle che comprendono la sistole (dal 30% al 45%).
appear advisable for clinical evaluation, as all of the pub-lished studies of diagnostic accuracy of MDCT coronary an-giography perform the evaluation with a number of differentreconstruction windows of the cardiac cycle.
Conclusions
On the basis of our clinical experience with MDCT coronaryangiography, the choice of the reconstruction window of the
comunque, per la valutazione di più ricostruzioni in diffe-renti finestre temporali del ciclo cardiaco.
Conclusioni
Sulla base della nostra esperienza clinica con AC-TCMS lascelta della finestra temporale di ricostruzione del ciclocardiaco appare influenzata dalla frequenza cardiaca me-dia registrata durante la scansione. L’utilizzo di protocollidi ricostruzione preimpostati in base alla frequenza cardia-
Radiol med (2008) 113:644–657 655
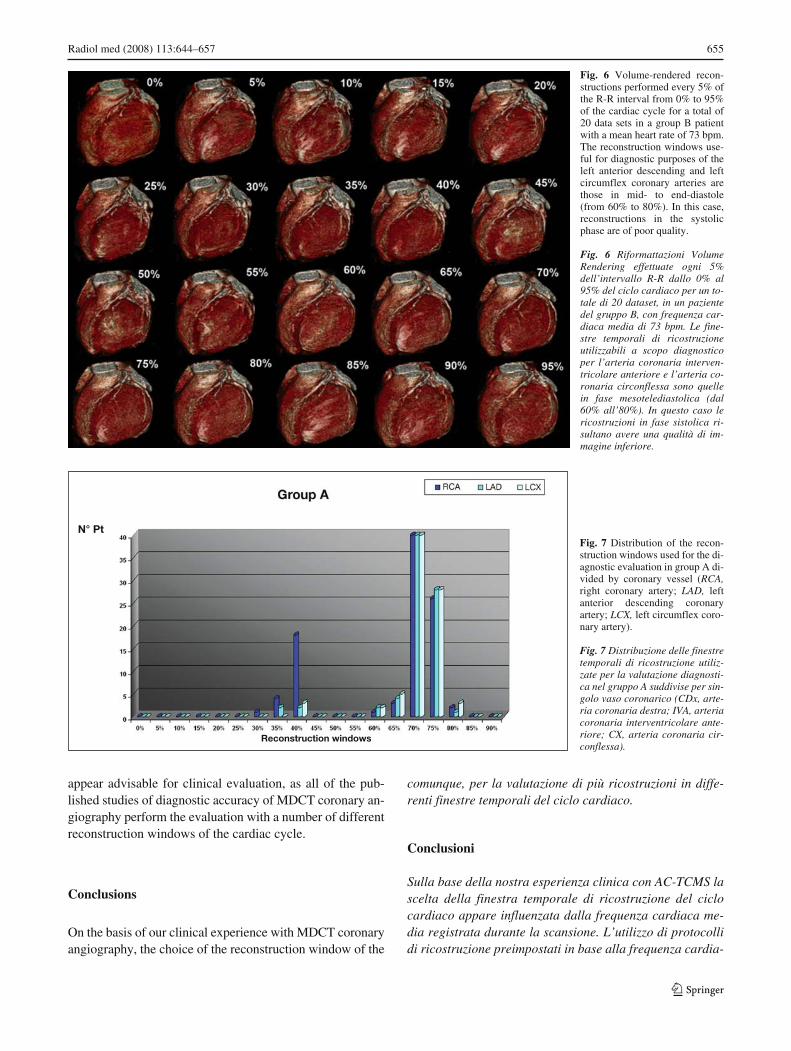
Fig. 7 Distribution of the recon-struction windows used for the di-agnostic evaluation in group A di-vided by coronary vessel (RCA,right coronary artery; LAD, leftanterior descending coronaryartery; LCX, left circumflex coro-nary artery).
Fig. 7 Distribuzione delle finestretemporali di ricostruzione utiliz-zate per la valutazione diagnosti-ca nel gruppo A suddivise per sin-golo vaso coronarico (CDx, arte-ria coronaria destra; IVA, arteriacoronaria interventricolare ante-riore; CX, arteria coronaria cir-conflessa).
Fig. 6 Volume-rendered recon-structions performed every 5% ofthe R-R interval from 0% to 95%of the cardiac cycle for a total of20 data sets in a group B patientwith a mean heart rate of 73 bpm.The reconstruction windows use-ful for diagnostic purposes of theleft anterior descending and leftcircumflex coronary arteries arethose in mid- to end-diastole(from 60% to 80%). In this case,reconstructions in the systolicphase are of poor quality.
Fig. 6 Riformattazioni VolumeRendering effettuate ogni 5%dell’intervallo R-R dallo 0% al95% del ciclo cardiaco per un to-tale di 20 dataset, in un pazientedel gruppo B, con frequenza car-diaca media di 73 bpm. Le fine-stre temporali di ricostruzioneutilizzabili a scopo diagnosticoper l’arteria coronaria interven-tricolare anteriore e l’arteria co-ronaria circonflessa sono quellein fase mesotelediastolica (dal60% all’80%). In questo caso lericostruzioni in fase sistolica ri-sultano avere una qualità di im-magine inferiore.
N° Pt
Reconstruction windows

cardiac cycle appears to be influenced by the mean HRrecorded during the scan. The use of preset reconstructionprotocols based on mean HR during the scan could enablethe reduction in reconstruction time for the operator and thequantity of space occupied in image archiving systems.
Reconstructions in the diastolic phase in most cases en-able an optimal diagnostic evaluation with mean HR ≤65bpm. With HR >65 bpm, reconstructions from 30% to 45%are advisable to obtain acceptable image quality for diag-nostic purposes.
ca media durante la scansione potrebbe consentire una ri-duzione dei tempi di ricostruzione per l’operatore e dellaquantità di spazio occupato sui sistemi di archiviazione del-le immagini.
Le ricostruzioni in fase diastolica consentono nella mag-gior parte dei casi un’ottimale valutazione per frequenzecardiache medie ≤65 bpm. Per frequenze >65 bpm, rico-struzioni dal 30% al 45% sono consigliabili per ottenereuna qualità d’immagine accettabile, necessaria a fornire ungiudizio diagnostico.
656 Radiol med (2008) 113:644–657
Fig. 8 Distribution of the reconstruc-tion windows used for the diagnosticevaluation in group B divided bycoronary vessel (RCA, right coronaryartery; LAD, left anterior descendingcoronary artery; LCX, left circumflexcoronary artery).
Fig. 8 Distribuzione delle finestretemporali di ricostruzione utilizzateper la valutazione diagnostica nelgruppo B suddivise per singolo vasocoronarico (CDx, arteria coronariadestra; IVA, arteria coronaria inter-ventricolare anteriore; CX, arteriacoronaria circonflessa).
References/Bibliografia
1. Leber AW, Knez A, von Ziegler F et al(2005) Quantification of obstructiveand nonobstructive coronary lesions by64-slice computed tomography: acomparative study with quantitativecoronary angiography and intravascularultrasound. J Am Coll Cardiol46:147–154
2. Leschka S, Alkadhi H, Plass A et al(2005) Accuracy of MSCT coronaryangiography with 64-slice technology:first experience. Eur Heart J26:1482–1487
3. Raff GL, Gallagher MJ, O’Neill WW,Goldstein JA (2005) Diagnosticaccuracy of noninvasive coronaryangiography using 64-slice spiralcomputed tomography. J Am CollCardiol 46:552–557
4. Mollet NR, Cademartiri F, vanMieghem CA et al (2005) High-resolution spiral computed tomographycoronary angiography in patientsreferred for diagnostic conventionalcoronary angiography. Circulation112:2318–2323
5. Pugliese F, Mollet NR, Runza G et al(2006) Diagnostic accuracy of non-invasive 64-slice CT coronaryangiography in patients with stableangina pectoris. Eur Radiol 16:575–582
6. Flohr TG, Stierstorfer K, Ulzheimer Set al (2005) Image reconstruction andimage quality evaluation for a 64-sliceCT scanner with z-flying focal spot.Med Phys 32:2536–2547
7. Giesler T, Baum U, Ropers D et al(2002) Noninvasive visualization ofcoronary arteries using contrast-enhanced multidetector CT: influenceof heart rate on image quality andstenosis detection. AJR Am JRoentgenol 179:911–916
8. Hong C, Becker CR, Huber A et al(2001) ECG-gated reconstructed multi-detector row CT coronary angiography:effect of varying trigger delay on imagequality. Radiology 220:712–717
9. Kopp AF, Schroeder S, Kuettner A et al(2001) Coronary arteries:retrospectively ECG-gated multi-detector row CT angiography withselective optimization of the imagereconstruction window. Radiology221:683–688
10. Hamoir XL, Flohr T, Hamoir V et al(2004) Coronary arteries: assessment ofimage quality and optimalreconstruction window in retrospectiveECG-gated multislice CT at 375-msgantry rotation time. Eur Radiol15:296–304
N° Pt
Reconstruction windows

Radiol med (2008) 113:644–657 657
11. Bley TA, Ghanem NA, Foell D et al(2005) Computed tomography coronaryangiography with 370-millisecondgantry rotation time: evaluation of thebest image reconstruction interval. J Comput Assist Tomogr 29:1–5
12. Sanz J, Rius T, Kuschnir P et al (2005)The importance of end-systole foroptimal reconstruction protocol ofcoronary angiography with 16-slicemultidetector computed tomography.Invest Radiol 40:155–163
13. Leschka S, Husmann L, Desbiolles LMet al (2006) Optimal imagereconstruction intervals for non-invasive coronary angiography with 64-slice CT. Eur Radiol 16:1964–1972
14. Jakobs TF, Becker CR, Ohnesorge B etal (2002) Multislice helical CT of theheart with retrospective ECG gating:reduction of radiation exposure byECG-controlled tube currentmodulation. Eur Radiol 12:1081–1086
15. Budoff MJ, Achenbach S, Fayad Z et al(2006) Task Force 12: training inadvanced cardiovascular imaging(computed tomography): endorsed bythe American Society of NuclearCardiology, Society for CardiovascularAngiography and Interventions, Societyof Atherosclerosis Imaging andPrevention, and Society ofCardiovascular ComputedTomography. J Am Coll Cardiol47:915–920
16. Shim SS, Kim Y and Lim SM (2005)Improvement of image quality withbeta-blocker premedication on ECG-gated 16-MDCT coronary angiography.AJR Am J Roentgenol 184:649–654
17. Ohnesorge B, Flohr T, Becker C et al(2000) Cardiac imaging by means ofelectrocardiographically gatedmultisection spiral CT: initialexperience. Radiology 217:564–571
18. Cademartiri F, Luccichenti G, MaranoR et al (2003) Non-invasiveangiography of the coronary arterieswith multislice computed tomography:state of the art and future prospects.Radiol Med 106:284–296
19. Hoffmann MH, Shi H, Manzke R et al(2005) Noninvasive coronaryangiography with 16-detector row CT:effect of heart rate. Radiology234:86–97
20. Flohr TG, McCollough CH, Bruder Het al (2006) First performanceevaluation of a dual-source CT (DSCT)system. Eur Radiol 16:256–268
21. Johnson TR, Nikolaou K,Wintersperger BJ et al (2006) Dual-source CT cardiac imaging: initialexperience. Eur Radiol 16:1409–1415
22. Kondo C, Mori S, Endo M et al (2005)Real-time volumetric imaging ofhuman heart withoutelectrocardiographic gating by 256-detector row computed tomography:initial experience. J Comput AssistTomogr 29:694–698
23. Hendel RC, Patel MR, Kramer CM etal (2006)ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriatenesscriteria for cardiac computedtomography and cardiac magneticresonance imaging: a report of theAmerican College of CardiologyFoundation Quality Strategic DirectionsCommittee Appropriateness CriteriaWorking Group, American College ofRadiology, Society of CardiovascularComputed Tomography, Society forCardiovascular Magnetic Resonance,American Society of NuclearCardiology, North American Societyfor Cardiac Imaging, Society forCardiovascular Angiography andInterventions, and Society ofInterventional Radiology. J Am CollCardiol 48:1475–1497




















