
Influence of dipyridamole and its combination with NO donor or NO synthase inhibitor on adjuvant...
9
Influence of dipyridamole and its combination with NO donor or NO synthase inhibitor on adjuvant arthritis Adel Gomaa a, ⁎, Mohsen Elshenawy b , Noha Afifi c , Eman Mohammed d , Romany Thabit b a Dept. of Pharmacology & Toxicology, College of Pharmacy, Taibah University, Al-madinah Almunawwarah, KSA b Dept. of Pharmacology, Faculty of Medicine, Assiut University, Assiut, Egypt c Dept. of Microbiology and Immunity, Faculty of Medicine, Assiut University, Assiut, Egypt d Dept. of Pathology, Faculty of Medicine, Assiut University, Assiut, Egypt abstract article info Article history: Received 15 May 2010 Received in revised form 9 August 2010 Accepted 9 August 2010 Keywords: Phosphodiesterase inhibitor Adjuvant arthritis NO synthase inhibitor NO donor Synergism The anti-arthritic and anti-inflammatory effects of dipyridamole and the possible involvement of NO in the dipyridamole action are not yet clear. The aim of this study was to evaluate the effects of dipyridamole alone and in combination with either the nitric oxide donor, sodium nitroprusside (SNP) or the non-selective nitric oxide synthase inhibitor, L-NG- monomethyl arginine (L-NMMA), on pathogenesis of adjuvant-induced arthritis model in rats. The results of the present work showed that prophylactic administration of dipyridamole alone and dipyridamole administration in combination with either low dose of SNP or L- NMMA significantly ameliorated pathogenesis of adjuvant arthritis in rats as evidenced by significant decrease in arthritis index, hind paws volume, loss of body weight, hyperalgesia compared with control vehicle (1% DMSO) treated adjuvant arthritic rats. Inflammatory cellular infiltrate in synovium of ankle joint and pannus formation were also markedly inhibited. Interleukin-10(IL-10) levels were significantly increased in these groups of animals. In contrast, a high dose of SNP counteracted the anti-inflammatory and anti-arthritic effects of dipyridamole. The inhibitory effect of therapeutic administration of dipyridamole alone on adjuvant arthritis syndrome was not significantly different from that of vehicle administration. In conclusion, dipyridamole has prophylactic but not therapeutic anti-arthritic and anti-inflammatory effects that appear to be dependent on inhibition of NO synthase. A synergistic combination between dipyridamole and NO synthase inhibitor or low dose of NO donor may have prophylactic and therapeutic values in autoimmune diseases like RA. © 2010 Elsevier B.V. All rights reserved. 1. Introduction Dipyridamole is a widely established drug for treatment of angina pectoris and cerebrovascular diseases. Its main mechanism of action is to inhibit the cellular uptake and metabolism of adenosine with resulting vasodilatory and anti-aggregatory effects. Through the combination of its antiplatelet and vasodilator function, dipyridamole probably improves tissue perfusion [1]. Dipyridamole is also a non- selective phosphodiesterase (PDE) inhibitor which inhibits degrada- tion of cAMP and cGMP. The rank order of the inhibition of phosphodiesterase by dipyridamole is PDE5 N PDE4 N PDE2 N PDE1 and 3 [2]. Increasing evidence has indicated that many phosphodiesterase inhibitors possess anti-inflammatory effects. Dipyridamole has been shown to have selective anti-inflammatory properties that may contribute to its action in the secondary prevention of stroke. Weyrich et al. found that dipyridamole differentially inhibited the expression of several gene products in human models of cellular inflammation [3]. In addition, it has shown that dipyridamole exerts its anti- inflammatory effect via activation of MKP-1, which dephosphorylates and inactivates p38 MARK. Inactivation of p38 MARK in turn inhibits 1KK-β activation and subsequently the NF-κβ signaling pathway that mediates lipopolysaccharide-induced cyclooxygenase-2 expression in RAW 264.7 cells [4]. It has also been reported that dipyridamole possesses antioxidant properties and attenuates the reactive oxygen species (ROS) forma- tion in platelets and endothelial cells [5]. The antioxidant effects of dipyridamole in endothelial cells are at least partially mediated via suppression of inflammatory NF-κβ signaling [6]. Furthermore, it has shown that dipyridamole has another beneficial effect; it inhibits NO production by adenosine-independent processes [7]. Therefore, it is possible that inhibition of NO production by dipyridamole contributes to evoke the anti-inflammatory and antioxidant effects of dipyridamole. Recently, it has been investigated that combination of a very low dose of prednisolone and dipyridamole has exhibited statistically significant synergistic effects in human clinical trials [8]. The synergistic effect of prednisolone with dipyridamole was also International Immunopharmacology 10 (2010) 1406–1414 ⁎ Corresponding author. E-mail address: [email protected] (A. Gomaa). 1567-5769/$ – see front matter © 2010 Elsevier B.V. All rights reserved. doi:10.1016/j.intimp.2010.08.006 Contents lists available at ScienceDirect International Immunopharmacology journal homepage: www.elsevier.com/locate/intimp
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Influence of dipyridamole and its combination with NO donor or NO synthase inhibitor on adjuvant...

International Immunopharmacology 10 (2010) 1406–1414
Contents lists available at ScienceDirect
International Immunopharmacology
j ourna l homepage: www.e lsev ie r.com/ locate / in t imp
Influence of dipyridamole and its combination with NO donor or NO synthaseinhibitor on adjuvant arthritis
Adel Gomaa a,⁎, Mohsen Elshenawy b, Noha Afifi c, Eman Mohammed d, Romany Thabit b
a Dept. of Pharmacology & Toxicology, College of Pharmacy, Taibah University, Al-madinah Almunawwarah, KSAb Dept. of Pharmacology, Faculty of Medicine, Assiut University, Assiut, Egyptc Dept. of Microbiology and Immunity, Faculty of Medicine, Assiut University, Assiut, Egyptd Dept. of Pathology, Faculty of Medicine, Assiut University, Assiut, Egypt
⁎ Corresponding author.E-mail address: [email protected] (A. Gomaa).
1567-5769/$ – see front matter © 2010 Elsevier B.V. Adoi:10.1016/j.intimp.2010.08.006
a b s t r a c t
a r t i c l e i n f oArticle history:Received 15 May 2010Received in revised form 9 August 2010Accepted 9 August 2010
Keywords:Phosphodiesterase inhibitorAdjuvant arthritisNO synthase inhibitorNO donorSynergism
The anti-arthritic and anti-inflammatory effects of dipyridamole and the possible involvement of NO in thedipyridamole action are not yet clear. The aim of this study was to evaluate the effects of dipyridamole aloneand in combination with either the nitric oxide donor, sodium nitroprusside (SNP) or the non-selective nitricoxide synthase inhibitor, L-NG- monomethyl arginine (L-NMMA), on pathogenesis of adjuvant-inducedarthritis model in rats. The results of the present work showed that prophylactic administrationof dipyridamole alone and dipyridamole administration in combination with either low dose of SNP or L-NMMA significantly ameliorated pathogenesis of adjuvant arthritis in rats as evidenced by significantdecrease in arthritis index, hind paws volume, loss of body weight, hyperalgesia compared with controlvehicle (1% DMSO) treated adjuvant arthritic rats. Inflammatory cellular infiltrate in synovium of ankle jointand pannus formation were also markedly inhibited. Interleukin-10(IL-10) levels were significantlyincreased in these groups of animals. In contrast, a high dose of SNP counteracted the anti-inflammatoryand anti-arthritic effects of dipyridamole. The inhibitory effect of therapeutic administration of dipyridamolealone on adjuvant arthritis syndrome was not significantly different from that of vehicle administration. Inconclusion, dipyridamole has prophylactic but not therapeutic anti-arthritic and anti-inflammatory effectsthat appear to be dependent on inhibition of NO synthase. A synergistic combination between dipyridamoleand NO synthase inhibitor or low dose of NO donor may have prophylactic and therapeutic values inautoimmune diseases like RA.
ll rights reserved.
© 2010 Elsevier B.V. All rights reserved.
1. Introduction
Dipyridamole is a widely established drug for treatment of anginapectoris and cerebrovascular diseases. Its mainmechanism of action isto inhibit the cellular uptake and metabolism of adenosine withresulting vasodilatory and anti-aggregatory effects. Through thecombination of its antiplatelet and vasodilator function, dipyridamoleprobably improves tissue perfusion [1]. Dipyridamole is also a non-selective phosphodiesterase (PDE) inhibitor which inhibits degrada-tion of cAMP and cGMP. The rank order of the inhibition ofphosphodiesterase by dipyridamole is PDE5NPDE4NPDE2NPDE1and 3 [2].
Increasing evidence has indicated that many phosphodiesteraseinhibitors possess anti-inflammatory effects. Dipyridamole has beenshown to have selective anti-inflammatory properties that maycontribute to its action in the secondary prevention of stroke.Weyrichet al. found that dipyridamole differentially inhibited the expression
of several gene products in human models of cellular inflammation[3]. In addition, it has shown that dipyridamole exerts its anti-inflammatory effect via activation of MKP-1, which dephosphorylatesand inactivates p38 MARK. Inactivation of p38 MARK in turn inhibits1KK-β activation and subsequently the NF-κ β signaling pathway thatmediates lipopolysaccharide-induced cyclooxygenase-2 expression inRAW 264.7 cells [4].
It has also been reported that dipyridamole possesses antioxidantproperties and attenuates the reactive oxygen species (ROS) forma-tion in platelets and endothelial cells [5]. The antioxidant effects ofdipyridamole in endothelial cells are at least partially mediated viasuppression of inflammatory NF-κ β signaling [6]. Furthermore, it hasshown that dipyridamole has another beneficial effect; it inhibits NOproduction by adenosine-independent processes [7]. Therefore, it ispossible that inhibition of NO production by dipyridamole contributesto evoke the anti-inflammatory and antioxidant effects ofdipyridamole.
Recently, it has been investigated that combination of a very lowdose of prednisolone and dipyridamole has exhibited statisticallysignificant synergistic effects in human clinical trials [8]. Thesynergistic effect of prednisolone with dipyridamole was also

1407A. Gomaa et al. / International Immunopharmacology 10 (2010) 1406–1414
observed in collagen and adjuvant arthritic animal based on inhibitionof additional inflammatory chemokine [9]. On the contrary, dipyr-idamole did notmodify the symptoms of rheumatoid arthritis in otherclinical trial described by Forrest et al. [10]. However, in animalmodels of rheumatoid, it is not clear whether or not dipyridamole hasanti-inflammatory and immunomodulating effects and the roleplayed by NO in dipyridamole actions remains to be determined.Therefore, in the present study, we examine whether dipyridamolepossesses anti-inflammatory and anti-arthritic effects in adjuvantarthritic rats and whether the suppression of NO production oraddition of exogenous NO can modify the dipyridamole action. Wealso examined the change in serum cytokines and histopathologyafter administration of dipyridamole alone or in combination witheither NO synthase inhibitor, LNMMA or NO donor, sodium nitroprus-side using prophylactic and therapeutic protocol.
2. Materials and methods
2.1. Animals
Adult female albino rats of the Sprague–Dawely strain weighingbetween 160 and 200 g were used. The animals were acclimatized in alight-and temperature-controlled room with a 12–12 h dark-lightcycle. The rats were fed with commercial pelleted rat feed and waterwas given ad libitum. Food was placed on the floor of the cage tofacilitate access, as the pain that accompanies adjuvant-inducedarthritis renders the rats immobile and unable to use their hind limbsto obtain food from the cover mesh of the cage. The experimentalprotocol was approved by the local ethical committee of Faculty ofMedicine, Assiut University.
2.2. Reagents and drugs
Complete Freund's adjuvant (CFA) was purchased from Difcolaboratories, (Detroit, Michigan, USA). Squalene was purchased fromMP Biomedicals, Inc. Dipyridamole was obtained from BoehringerIngelheim Pharmaceuticals, Inc. NG monomethyl-L-arginine (L-NMMA)and sodium nitroprusside (SNP) were purchased from Sigma chemical,(St.Louis, USA). Dipyridamole was dissolved in 1% DMSO in distilledwater.SNP and L-NMMA were freely dissolved in water.
2.3. Experimental induction of arthritis and drug treatment
In this study, adjuvant arthritis was induced in rats according tothe previously described methods for evaluation of rheumatoidarthritis. Based on preliminary experiments, to increase the sensitivityof rats used to CFA, the method of Trentham et al. [11] was modifiedby intradermally injecting 0.1 ml of squalene before inoculation ofCFA into a different site in the subplantar surface of right hind paw.Each animal in all groups, except those in the control non-adjuvantgroup, was injected with 0.1 ml squalene and 0.1 ml CFA.
Ninety six rats were used in this study. Two groups (I & II) of sixanimals each served as controls; these non-adjuvant and untreatedadjuvant arthritic rats received saline orally. Other animals wererandomly allocated to two treatment protocols (prophylactic ortherapeutic). Each treatment protocol contains seven groups of sixanimals. Drug or vehicle treatment was started on day 5 till day 14 inprophylactic protocol and on day 16 till day 25 for the therapeuticprotocol. The first four groups (III, IV, V and VI) in each protocolreceived oral dipyridamole alone in doses of 0, 270, 180 and 90 mg/kg/day respectively. Group III served as vehicle (1% DMSO) treatedgroup. The other three groups (VII, VIII and IX) were treated with180 mg/kg/day dipyridamole orally combined with 1 mg/kg/day SNP,0.01 mg/kg/d SNP or 30 mg/kg/d L-NMMA respectively.
The day of inoculation was regarded as day 0 whereas day 16was the day in which oedema in the contralateral, non-injected,
hind paw was observed. This prophylactic schedule of treatmentwas selected to evaluate the inhibitory effect of dipyridamole onthe development of arthritis in contralateral hind paws. Thisprotocol demonstrates the immunomodulator effect of dipyrida-mole. However, a therapeutic protocol was used to assess the anti-inflammatory effect of dipyridamole on the development ofarthritis
Arthritis index, volume of oedema in paws, body weight, rectaltemperature and pain threshold to pressure on hind paws, weremeasured daily from day 0 until day 30 after adjuvant inoculation. Atthe end of the study, the animals were killed and the blood wascollected. Blood samples were immediately centrifuged at 3000 rpmfor 10 min and serum samples were stored at−80 °C until assayed forTNF-alpha and IL-10. Specimens of ankle joint tissues were alsoexamined for histopathology.
2.4. Arthritis index
Rats were evaluated daily for arthritis. The physical symptomsof arthritis were judged by the following grading system [12]:0=normal paws; 1=erythema of toes; 2=erythema and swell-ing of paws; 3=swelling of ankles; and 4=complete swelling ofthe whole leg and inability to bend it. The maximum achievablescore is thus 16. Arthritis index for each rat was calculated byadding the four scores of individual paws. A sensitized animal wasconsidered to have arthritis when at least one non-injected pawwas inflamed [13].
2.5. Measurement of body weight and temperature in arthritic rats
The body weight for each rat was recorded before and daily afteradjuvant inoculation to assess food intake and weight gain through-out the period of arthritis. The difference between body weight on agiven day and that on day 0was calculated to determine the change inbody weight in arthritic rats.
The body temperature, as an index of inflammation, wasmonitored for rats, before and daily after disease induction between9:00 AM and 11:00 AM, using a rectal thermometer.
2.6. Measurement of paw volume changes
Volumes of both ipsilateral (injected) and contralateral (non-injected) hind paws were measured before and daily after adjuvantinoculation by using water displacement plethysmometry [14]. Thechanges in volumes of hind paws compared with those on day 0 werecalculated.
2.7. Analgesimetry
Using a Ugo basile analgesimeter (Ugo Basile Biological ResearchApparatus, Italy), a crescent pressure (in grams) was appliedseparately to the posterior paws until the animal displayed a reactionthat consisted of withdrawing the paw and/or vocalizing [15]. Theslide of the device moved at the speed of 16 mm per second. The forceon the paw was at rate of 16 g per second, so a distance of 11.5 mm isequivalent 115 g. The pain threshold to pressure on hind paws of ratswas measured. The following formula was used to calculate thepercentage change in pressure to the hind paws needed to elicitresponse on day x for each animal:
Pressure on day x−pressure before adjuvant injectiononday 0ð Þ × 100Pressure before adjuvant injection on day 0

Fig. 1. Effect of prophylactic (A), and therapeutic (B) administration of dipyridamole on thearthritis index of adjuvant arthritic rats. Saline-treated non-adjuvant rats. Adjuvantnon-treated arthritic rats; Vehicle-treated adjuvant arthritic rats; dipyridamole-treated (270 mg/kg/d) arthritic rats; dipyridamole-treated (180 mg/kg/d)arthritic; dipyridamole (90 mg/kg/d) arthritic rats; dipyridamole (180 mg/kg/d) in combination with in combination with SNP (1 mg/kg/d); dipyridamole(180 mg/kg/d) in combination with SNP (0.01 mg/kg/d); dipyridamole (180 mg/kg/d) in combination with L-NMMA(30 mg/kg/d). *pb0.05 versus group II, opb0.05versus group III, +pb0.05 versus group V.
1408 A. Gomaa et al. / International Immunopharmacology 10 (2010) 1406–1414
2.8. TNF-alpha and IL-10 assays
Animals were killed on day 30 after disease induction and samplesof blood were taken to separate sera from all animals. Serum levels ofTNF-alpha and IL-10 were determined using enzyme-linked immu-nosorbent assay kits from (Bender Medsystems, Vienna, Austria).Antibodies specific for rat TNF-alpha and IL-10 were coated onto thewells of the microtiter strips and the samples including standards ofknown rat TNF-alpha and IL-10 were pipetted into the wells,incubated and washed. Intensity of the color was determined at450 nm with a correction wave length of 630 nm.
2.9. Histopathological examination
Ankle joint tissues from all animals were excised and fixed in 10%buffered formalin, decalcified in 10% ethylenediaminetetraacetic acid,embedded in paraffin, sectioned and stained with hematoxylin andeosin and then evaluated under light microscope. The evaluationparameters were mononuclear inflammation, vascular proliferation,oedema, synovial hyperplasia and vasculitis causing fibrinoid necrosison the vessel wall in periarticular and subcutaneous adipose tissue[16]. The pathological evaluation was performed randomly by apathologist, blind to the specimens.
2.10. Statistical analysis
The results are presented as the mean±standard error of themean. Changes in arthritis index, body weight, temperature, pawsvolumes, pain threshold to paw pressure and serum levels ofcytokines measured in different treatment groups were comparedwith vehicle-treated group (group III), adjuvant untreated controlgroup (group II) and non-adjuvant control group (group I) by one-way analysis of variance and Student's t-tests for significance. Also,significance tests were calculated to determine the differencesbetween the effects of different doses of dipyridamole anddipyridamole alone compared dipyridamole in combination withSNP or L-NMMA.
3. Results
3.1. Arthritis index
Arthritis was successfully created in rats by the administration ofCFA and squalene. After induction of arthritis in the control untreatedgroup (group II), the injected hind paw (right one) showed, on day 1,obvious swelling of the ankle and small joints of the foot with markedredness of the inflamed joints whereas the left non-injected hind pawshowed swelling and redness on day 15 after adjuvant inoculation. Onday 5 after adjuvant inoculation, arthritis indexwas 3.3±0.3. Arthritisindex peaked on day 15 (6.3±0.3) and slightly decreased on thesubsequent days until the end of experiments on day 30 (5.3±0.3).
Prophylactically administration of dipyridamole significantly de-creased (Pb0.05) the arthritic scores of arthritic rats compared withvehicle treated group. The arthritic scores of arthritic rates treatedwith 270,180, 90 and 0 mg/kg/day (groups IV, V, VI and III) on day 30were 1.25±0.1, 1.33±0.2, 1.5±0.2 and 4.3±0.3 respectively. On theother hand, therapeutic administration of dipyridamole at all dosesused 270, 180, 90 mg/kg/day did not decrease significantly (PN0.05)the arthritic scores on day 30 (2.9±0.1, 3.2±0.2, and 3.5±0.2respectively) compared with that of adjuvant arthritic rats treatedwith vehicle (group III, 3.5±0.3) (Fig. 1).
In prophylactic or therapeutic groups, the combination of 30 mg/kg/day .L-NMMA or 0.01 mg/kg/day SNP with 180 mg/kg/day dipyr-idamole significantly decreased the arthritic scores compared witharthritic scores of vehicle treated group and significantly enhanced theinhibitory effect of dipyridamole comparedwith the arthritic scores of
group treatedwith dipyridamole alone. Arthritic scores of prophylacticadministration of dipyridamole (180 mg/kg/day) alone, with a lowdose of SNP (0.01 mg/kg/day) or with L-NMMA (30 mg/kg/day) were1.33±0.2, 0.5±0.1 or 0.25±.1 respectively. Similarly, the therapeuticco-administration of SNP (0.01 mg/kg/day) or L-NMMA (30 mg/kg/day)with dipyridamole decreased the arthritic scores from3.2±0.2 to0.5±0.2 or 0.67±0.1 respectively. In contrast, SNP at a dose of 1 mg/kg/day significantly reduced (PN0.05) the inhibitory effect ofdipyridamole and the arthritic score was increased from 1.33±0.2to 5.2±0.4 in prophylactic group and from 3.2±0.2 to 6.2±0.5 intherapeutic group (Fig. 1).
3.2. Body weight changes
The body weight of adjuvant untreated control rats (group II)was markedly decreased starting from day 5 and the maximum loss(21.7±1.2 g) was observed on day 30.
Prophylactic and therapeutic treatment of arthritic rats withdipyridamole alone (groups IV, V and VI) and in combination witheither low dose of SNP (0.01 mg/kg/day, group VIII) or 30 mg/kg/dayL-NMMA (group IX) significantly prevented the loss in the bodyweight of arthritic rats. However, there was non-significantdifferences only between the effect of therapeutic administrationof dipyridamole alone at all doses levels (270, 180 and 90 mg/kg/day) and the effect of vehicle (1% DMSO). Prophylactic administra-tion of dipyridamole significantly increased (PN0.05) the body
1409A. Gomaa et al. / International Immunopharmacology 10 (2010) 1406–1414
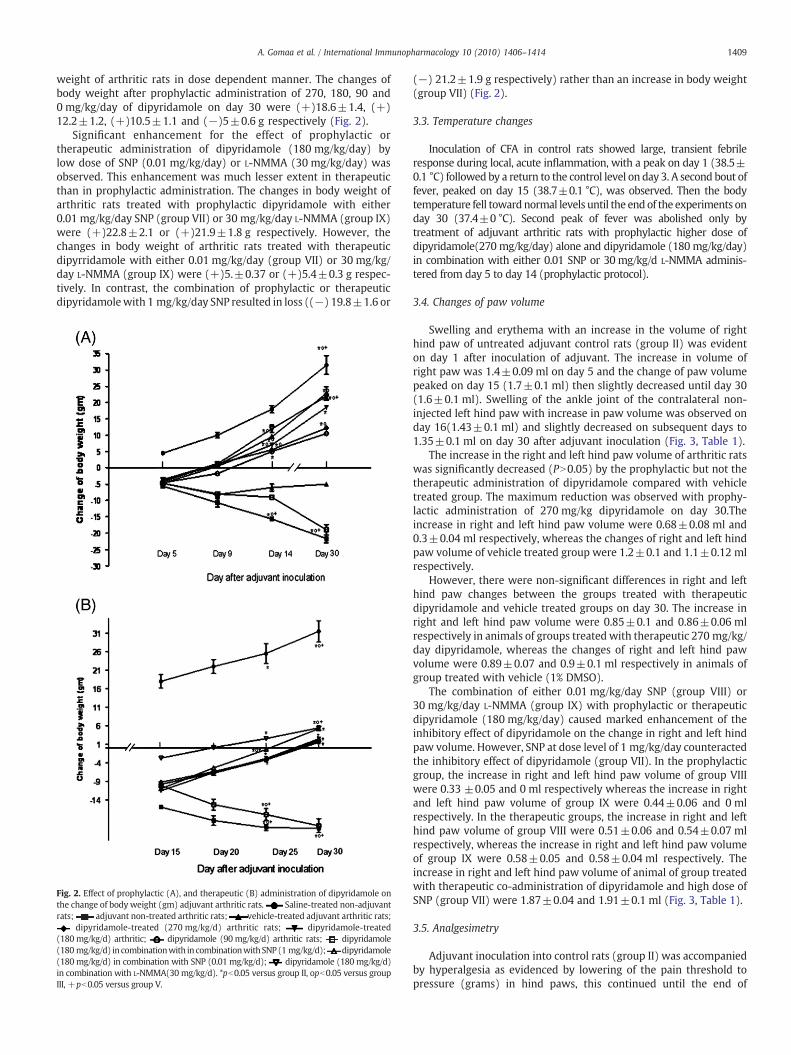
weight of arthritic rats in dose dependent manner. The changes ofbody weight after prophylactic administration of 270, 180, 90 and0 mg/kg/day of dipyridamole on day 30 were (+)18.6±1.4, (+)12.2±1.2, (+)10.5±1.1 and (−)5±0.6 g respectively (Fig. 2).
Significant enhancement for the effect of prophylactic ortherapeutic administration of dipyridamole (180 mg/kg/day) bylow dose of SNP (0.01 mg/kg/day) or L-NMMA (30 mg/kg/day) wasobserved. This enhancement was much lesser extent in therapeuticthan in prophylactic administration. The changes in body weight ofarthritic rats treated with prophylactic dipyridamole with either0.01 mg/kg/day SNP (group VII) or 30 mg/kg/day L-NMMA (group IX)were (+)22.8±2.1 or (+)21.9±1.8 g respectively. However, thechanges in body weight of arthritic rats treated with therapeuticdipyrridamole with either 0.01 mg/kg/day (group VII) or 30 mg/kg/day L-NMMA (group IX) were (+)5.±0.37 or (+)5.4±0.3 g respec-tively. In contrast, the combination of prophylactic or therapeuticdipyridamolewith 1 mg/kg/day SNP resulted in loss ((−) 19.8±1.6 or
Fig. 2. Effect of prophylactic (A), and therapeutic (B) administration of dipyridamole onthe change of body weight (gm) adjuvant arthritic rats. Saline-treated non-adjuvantrats; adjuvant non-treated arthritic rats; vehicle-treated adjuvant arthritic rats;
dipyridamole-treated (270 mg/kg/d) arthritic rats; dipyridamole-treated(180mg/kg/d) arthritic; dipyridamole (90 mg/kg/d) arthritic rats; dipyridamole(180mg/kg/d) incombinationwith in combinationwithSNP(1 mg/kg/d); dipyridamole(180mg/kg/d) in combination with SNP (0.01 mg/kg/d); dipyridamole (180 mg/kg/d)in combination with L-NMMA(30 mg/kg/d). *pb0.05 versus group II, opb0.05 versus groupIII, +pb0.05 versus group V.
(−) 21.2±1.9 g respectively) rather than an increase in body weight(group VII) (Fig. 2).
3.3. Temperature changes
Inoculation of CFA in control rats showed large, transient febrileresponse during local, acute inflammation, with a peak on day 1 (38.5±0.1 °C) followed by a return to the control level on day 3. A second bout offever, peaked on day 15 (38.7±0.1 °C), was observed. Then the bodytemperature fell towardnormal levels until the end of the experiments onday 30 (37.4±0 °C). Second peak of fever was abolished only bytreatment of adjuvant arthritic rats with prophylactic higher dose ofdipyridamole(270 mg/kg/day) alone and dipyridamole (180 mg/kg/day)in combination with either 0.01 SNP or 30 mg/kg/d L-NMMA adminis-tered from day 5 to day 14 (prophylactic protocol).
3.4. Changes of paw volume
Swelling and erythema with an increase in the volume of righthind paw of untreated adjuvant control rats (group II) was evidenton day 1 after inoculation of adjuvant. The increase in volume ofright paw was 1.4±0.09 ml on day 5 and the change of paw volumepeaked on day 15 (1.7±0.1 ml) then slightly decreased until day 30(1.6±0.1 ml). Swelling of the ankle joint of the contralateral non-injected left hind paw with increase in paw volume was observed onday 16(1.43±0.1 ml) and slightly decreased on subsequent days to1.35±0.1 ml on day 30 after adjuvant inoculation (Fig. 3, Table 1).
The increase in the right and left hind paw volume of arthritic ratswas significantly decreased (PN0.05) by the prophylactic but not thetherapeutic administration of dipyridamole compared with vehicletreated group. The maximum reduction was observed with prophy-lactic administration of 270 mg/kg dipyridamole on day 30.Theincrease in right and left hind paw volume were 0.68±0.08 ml and0.3±0.04 ml respectively, whereas the changes of right and left hindpaw volume of vehicle treated group were 1.2±0.1 and 1.1±0.12 mlrespectively.
However, there were non-significant differences in right and lefthind paw changes between the groups treated with therapeuticdipyridamole and vehicle treated groups on day 30. The increase inright and left hind paw volume were 0.85±0.1 and 0.86±0.06 mlrespectively in animals of groups treated with therapeutic 270 mg/kg/day dipyridamole, whereas the changes of right and left hind pawvolume were 0.89±0.07 and 0.9±0.1 ml respectively in animals ofgroup treated with vehicle (1% DMSO).
The combination of either 0.01 mg/kg/day SNP (group VIII) or30 mg/kg/day L-NMMA (group IX) with prophylactic or therapeuticdipyridamole (180 mg/kg/day) caused marked enhancement of theinhibitory effect of dipyridamole on the change in right and left hindpaw volume. However, SNP at dose level of 1 mg/kg/day counteractedthe inhibitory effect of dipyridamole (group VII). In the prophylacticgroup, the increase in right and left hind paw volume of group VIIIwere 0.33 ±0.05 and 0 ml respectively whereas the increase in rightand left hind paw volume of group IX were 0.44±0.06 and 0 mlrespectively. In the therapeutic groups, the increase in right and lefthind paw volume of group VIII were 0.51±0.06 and 0.54±0.07 mlrespectively, whereas the increase in right and left hind paw volumeof group IX were 0.58±0.05 and 0.58±0.04 ml respectively. Theincrease in right and left hind paw volume of animal of group treatedwith therapeutic co-administration of dipyridamole and high dose ofSNP (group VII) were 1.87±0.04 and 1.91±0.1 ml (Fig. 3, Table 1).
3.5. Analgesimetry
Adjuvant inoculation into control rats (group II) was accompaniedby hyperalgesia as evidenced by lowering of the pain threshold topressure (grams) in hind paws, this continued until the end of
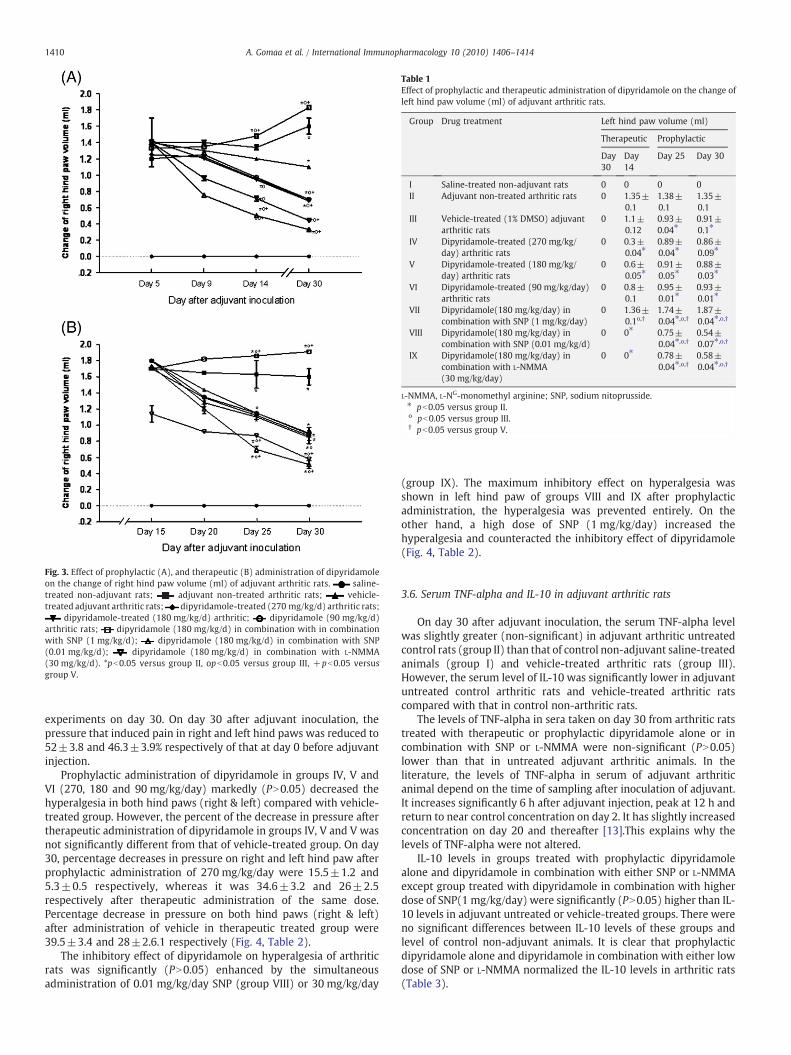
Table 1Effect of prophylactic and therapeutic administration of dipyridamole on the change ofleft hind paw volume (ml) of adjuvant arthritic rats.
Group Drug treatment Left hind paw volume (ml)
Therapeutic Prophylactic
Day30
Day14
Day 25 Day 30
I Saline-treated non-adjuvant rats 0 0 0 0II Adjuvant non-treated arthritic rats 0 1.35±
0.11.38±0.1
1.35±0.1
III Vehicle-treated (1% DMSO) adjuvantarthritic rats
0 1.1±0.12
0.93±0.04⁎
0.91±0.1⁎
IV Dipyridamole-treated (270 mg/kg/day) arthritic rats
0 0.3±0.04⁎
0.89±0.04⁎
0.86±0.09⁎
V Dipyridamole-treated (180 mg/kg/day) arthritic rats
0 0.6±0.05⁎
0.91±0.05⁎
0.88±0.03⁎
VI Dipyridamole-treated (90 mg/kg/day)arthritic rats
0 0.8±0.1
0.95±0.01⁎
0.93±0.01⁎
VII Dipyridamole(180 mg/kg/day) incombination with SNP (1 mg/kg/day)
0 1.36±0.1o,†
1.74±0.04⁎,o,†
1.87±0.04⁎,o,†
VIII Dipyridamole(180 mg/kg/day) incombination with SNP (0.01 mg/kg/d)
0 0⁎ 0.75±0.04⁎,o,†
0.54±0.07⁎,o,†
IX Dipyridamole(180 mg/kg/day) incombination with L-NMMA(30 mg/kg/day)
0 0⁎ 0.78±0.04⁎,o,†
0.58±0.04⁎,o,†
L-NMMA, L-NG-monomethyl arginine; SNP, sodium nitoprusside.⁎ pb0.05 versus group II.o pb0.05 versus group III.† pb0.05 versus group V.
Fig. 3. Effect of prophylactic (A), and therapeutic (B) administration of dipyridamoleon the change of right hind paw volume (ml) of adjuvant arthritic rats. saline-treated non-adjuvant rats; adjuvant non-treated arthritic rats; vehicle-treated adjuvant arthritic rats; dipyridamole-treated (270 mg/kg/d) arthritic rats;
dipyridamole-treated (180 mg/kg/d) arthritic; dipyridamole (90 mg/kg/d)arthritic rats; dipyridamole (180 mg/kg/d) in combination with in combinationwith SNP (1 mg/kg/d); dipyridamole (180 mg/kg/d) in combination with SNP(0.01 mg/kg/d); dipyridamole (180 mg/kg/d) in combination with L-NMMA(30 mg/kg/d). *pb0.05 versus group II, opb0.05 versus group III, +pb0.05 versusgroup V.
1410 A. Gomaa et al. / International Immunopharmacology 10 (2010) 1406–1414
experiments on day 30. On day 30 after adjuvant inoculation, thepressure that induced pain in right and left hind paws was reduced to52±3.8 and 46.3±3.9% respectively of that at day 0 before adjuvantinjection.
Prophylactic administration of dipyridamole in groups IV, V andVI (270, 180 and 90 mg/kg/day) markedly (PN0.05) decreased thehyperalgesia in both hind paws (right & left) compared with vehicle-treated group. However, the percent of the decrease in pressure aftertherapeutic administration of dipyridamole in groups IV, V and V wasnot significantly different from that of vehicle-treated group. On day30, percentage decreases in pressure on right and left hind paw afterprophylactic administration of 270 mg/kg/day were 15.5±1.2 and5.3±0.5 respectively, whereas it was 34.6±3.2 and 26±2.5respectively after therapeutic administration of the same dose.Percentage decrease in pressure on both hind paws (right & left)after administration of vehicle in therapeutic treated group were39.5±3.4 and 28±2.6.1 respectively (Fig. 4, Table 2).
The inhibitory effect of dipyridamole on hyperalgesia of arthriticrats was significantly (PN0.05) enhanced by the simultaneousadministration of 0.01 mg/kg/day SNP (group VIII) or 30 mg/kg/day
(group IX). The maximum inhibitory effect on hyperalgesia wasshown in left hind paw of groups VIII and IX after prophylacticadministration, the hyperalgesia was prevented entirely. On theother hand, a high dose of SNP (1 mg/kg/day) increased thehyperalgesia and counteracted the inhibitory effect of dipyridamole(Fig. 4, Table 2).
3.6. Serum TNF-alpha and IL-10 in adjuvant arthritic rats
On day 30 after adjuvant inoculation, the serum TNF-alpha levelwas slightly greater (non-significant) in adjuvant arthritic untreatedcontrol rats (group II) than that of control non-adjuvant saline-treatedanimals (group I) and vehicle-treated arthritic rats (group III).However, the serum level of IL-10 was significantly lower in adjuvantuntreated control arthritic rats and vehicle-treated arthritic ratscompared with that in control non-arthritic rats.
The levels of TNF-alpha in sera taken on day 30 from arthritic ratstreated with therapeutic or prophylactic dipyridamole alone or incombination with SNP or L-NMMA were non-significant (PN0.05)lower than that in untreated adjuvant arthritic animals. In theliterature, the levels of TNF-alpha in serum of adjuvant arthriticanimal depend on the time of sampling after inoculation of adjuvant.It increases significantly 6 h after adjuvant injection, peak at 12 h andreturn to near control concentration on day 2. It has slightly increasedconcentration on day 20 and thereafter [13].This explains why thelevels of TNF-alpha were not altered.
IL-10 levels in groups treated with prophylactic dipyridamolealone and dipyridamole in combination with either SNP or L-NMMAexcept group treated with dipyridamole in combination with higherdose of SNP(1 mg/kg/day) were significantly (PN0.05) higher than IL-10 levels in adjuvant untreated or vehicle-treated groups. There wereno significant differences between IL-10 levels of these groups andlevel of control non-adjuvant animals. It is clear that prophylacticdipyridamole alone and dipyridamole in combination with either lowdose of SNP or L-NMMA normalized the IL-10 levels in arthritic rats(Table 3).
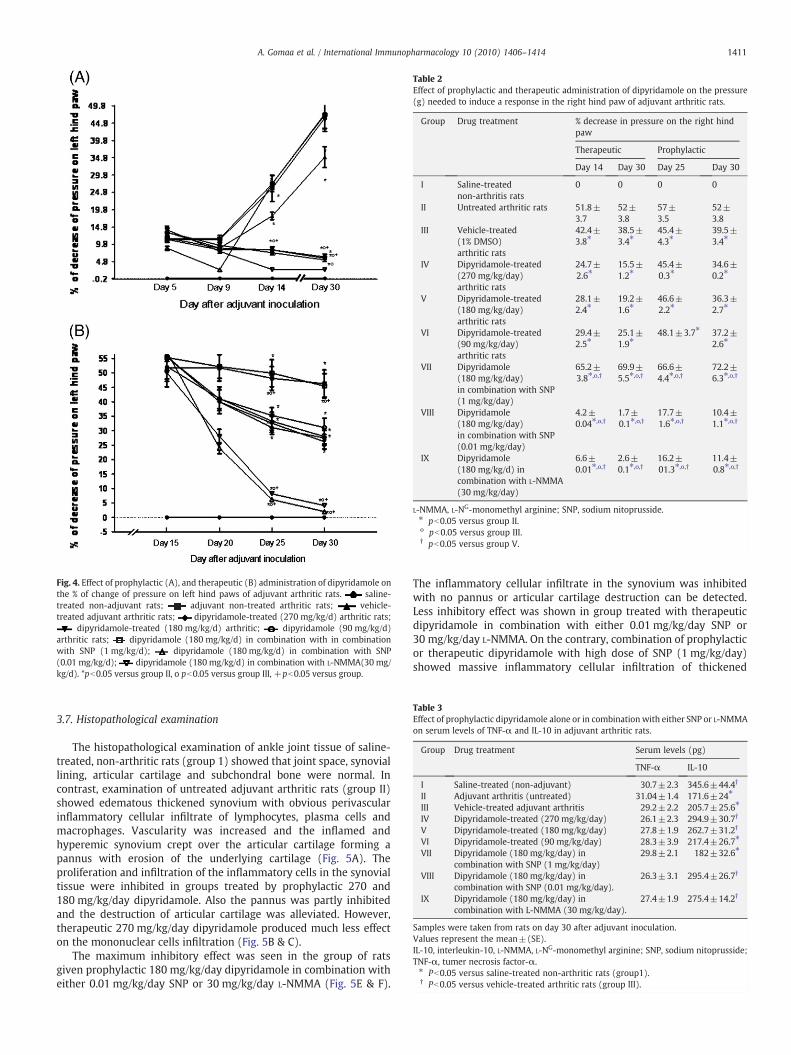
Table 2Effect of prophylactic and therapeutic administration of dipyridamole on the pressure(g) needed to induce a response in the right hind paw of adjuvant arthritic rats.
Group Drug treatment % decrease in pressure on the right hindpaw
Therapeutic Prophylactic
Day 14 Day 30 Day 25 Day 30
I Saline-treatednon-arthritis rats
0 0 0 0
II Untreated arthritic rats 51.8±3.7
52±3.8
57±3.5
52±3.8
III Vehicle-treated(1% DMSO)arthritic rats
42.4±3.8⁎
38.5±3.4⁎
45.4±4.3⁎
39.5±3.4⁎
IV Dipyridamole-treated(270 mg/kg/day)arthritic rats
24.7±2.6⁎
15.5±1.2⁎
45.4±0.3⁎
34.6±0.2⁎
V Dipyridamole-treated(180 mg/kg/day)arthritic rats
28.1±2.4⁎
19.2±1.6⁎
46.6±2.2⁎
36.3±2.7⁎
VI Dipyridamole-treated(90 mg/kg/day)arthritic rats
29.4±2.5⁎
25.1±1.9⁎
48.1±3.7⁎ 37.2±2.6⁎
VII Dipyridamole(180 mg/kg/day)in combination with SNP(1 mg/kg/day)
65.2±3.8⁎,o,†
69.9±5.5⁎,o,†
66.6±4.4⁎,o,†
72.2±6.3⁎,o,†
VIII Dipyridamole(180 mg/kg/day)in combination with SNP(0.01 mg/kg/day)
4.2±0.04⁎,o,†
1.7±0.1⁎,o,†
17.7±1.6⁎,o,†
10.4±1.1⁎,o,†
IX Dipyridamole(180 mg/kg/d) incombination with L-NMMA(30 mg/kg/day)
6.6±0.01⁎,o,†
2.6±0.1⁎,o,†
16.2±01.3⁎,o,†
11.4±0.8⁎,o,†
L-NMMA, L-NG-monomethyl arginine; SNP, sodium nitoprusside.⁎ pb0.05 versus group II.o pb0.05 versus group III.† pb0.05 versus group V.
Table 3Effect of prophylactic dipyridamole alone or in combination with either SNP or L-NMMAon serum levels of TNF-α and IL-10 in adjuvant arthritic rats.
Group Drug treatment Serum levels (pg)
TNF-α IL-10
I Saline-treated (non-adjuvant) 30.7±2.3 345.6±44.4†
II Adjuvant arthritis (untreated) 31.04±1.4 171.6±24⁎
III Vehicle-treated adjuvant arthritis 29.2±2.2 205.7±25.6⁎
IV Dipyridamole-treated (270 mg/kg/day) 26.1±2.3 294.9±30.7†
V Dipyridamole-treated (180 mg/kg/day) 27.8±1.9 262.7±31.2†
VI Dipyridamole-treated (90 mg/kg/day) 28.3±3.9 217.4±26.7⁎
VII Dipyridamole (180 mg/kg/day) incombination with SNP (1 mg/kg/day)
29.8±2.1 182±32.6⁎
VIII Dipyridamole (180 mg/kg/day) incombination with SNP (0.01 mg/kg/day).
26.3±3.1 295.4±26.7†
IX Dipyridamole (180 mg/kg/day) incombination with L-NMMA (30 mg/kg/day).
27.4±1.9 275.4±14.2†
Samples were taken from rats on day 30 after adjuvant inoculation.Values represent the mean±(SE).IL-10, interleukin-10, L-NMMA, L-NG-monomethyl arginine; SNP, sodium nitoprusside;TNF-α, tumer necrosis factor-α.⁎ Pb0.05 versus saline-treated non-arthritic rats (group1).† Pb0.05 versus vehicle-treated arthritic rats (group III).
Fig. 4. Effect of prophylactic (A), and therapeutic (B) administration of dipyridamole onthe % of change of pressure on left hind paws of adjuvant arthritic rats. saline-treated non-adjuvant rats; adjuvant non-treated arthritic rats; vehicle-treated adjuvant arthritic rats; dipyridamole-treated (270 mg/kg/d) arthritic rats;
dipyridamole-treated (180 mg/kg/d) arthritic; dipyridamole (90 mg/kg/d)arthritic rats; dipyridamole (180 mg/kg/d) in combination with in combinationwith SNP (1 mg/kg/d); dipyridamole (180 mg/kg/d) in combination with SNP(0.01 mg/kg/d); dipyridamole (180 mg/kg/d) in combination with L-NMMA(30 mg/kg/d). *pb0.05 versus group II, o pb0.05 versus group III, +pb0.05 versus group.
1411A. Gomaa et al. / International Immunopharmacology 10 (2010) 1406–1414
3.7. Histopathological examination
The histopathological examination of ankle joint tissue of saline-treated, non-arthritic rats (group 1) showed that joint space, synoviallining, articular cartilage and subchondral bone were normal. Incontrast, examination of untreated adjuvant arthritic rats (group II)showed edematous thickened synovium with obvious perivascularinflammatory cellular infiltrate of lymphocytes, plasma cells andmacrophages. Vascularity was increased and the inflamed andhyperemic synovium crept over the articular cartilage forming apannus with erosion of the underlying cartilage (Fig. 5A). Theproliferation and infiltration of the inflammatory cells in the synovialtissue were inhibited in groups treated by prophylactic 270 and180 mg/kg/day dipyridamole. Also the pannus was partly inhibitedand the destruction of articular cartilage was alleviated. However,therapeutic 270 mg/kg/day dipyridamole produced much less effecton the mononuclear cells infiltration (Fig. 5B & C).
The maximum inhibitory effect was seen in the group of ratsgiven prophylactic 180 mg/kg/day dipyridamole in combination witheither 0.01 mg/kg/day SNP or 30 mg/kg/day L-NMMA (Fig. 5E & F).
The inflammatory cellular infiltrate in the synovium was inhibitedwith no pannus or articular cartilage destruction can be detected.Less inhibitory effect was shown in group treated with therapeuticdipyridamole in combination with either 0.01 mg/kg/day SNP or30 mg/kg/day L-NMMA. On the contrary, combination of prophylacticor therapeutic dipyridamole with high dose of SNP (1 mg/kg/day)showed massive inflammatory cellular infiltration of thickened

(A) (B)
(C)
(F)(E)
(D)
Fig. 5. Representative histopathology of left ankle joints of (A) Adjuvant arthritic rats non-treated rats. (B) arthritic rats treated with prophylactic 270 mg/kg/day. (C) Adjuvantarthritic rats treated with prophylactic 180 mg/kg/d dipyridamole. (D) Adjuvant arthritic rats treated with 180 mg/kg/d dipyridamole in combination with 1 mg/kg/day SNP.(E) Arthritic rats treated with prophylactic 180 mg/kg/d dipyridamole in combination with 0.01 mg/kg/d SNP and (F) arthritic rats treated with prophylactic 180 mg/kg/ddipyridamole in combination with 30 mg/kg/d L-NMMA. Note the dramatic protective effect observed with prophylactic dipyridamole in combination with low dose of SNP orL-NMMA and less effect was shown with prophylactic 270 dipyridamole alone, as evident by minimal inflammatory cellular infiltrate of synovium and inhibited articularcartilage erosion. On the contrary, note the massive cellular infiltration, eroded articular cartilage and destructed subchondral bone produced by dipyridamole in combinationwith high dose of SNP (1 mg/kg/day).
1412 A. Gomaa et al. / International Immunopharmacology 10 (2010) 1406–1414
edematous synovium blood vessels are obstructed by endarteritisobliterans and fibrocellular pannus was observed eroding thearticular cartilage causing its destruction with penetration into thesubchondral bone (Fig. 5D).
4. Discussion
Inhibition of several functions of different types of cells involved inimmune responses is usually associated with an increase of

1413A. Gomaa et al. / International Immunopharmacology 10 (2010) 1406–1414
intracellular cAMP or cGMP [17–19]. Increased levels of cAMP orcGMP have been reported to decrease activity of proinflammatoryTH1 cells, attenuate experimental autoimmune encephalmyelitus andexperimental arthritis [20]. Therefore, drugs that increase cAMP orcGMP as PDE inhibitors have been employed for treatment of severalautoimmune disorders as rheumatoid arthritis. They are known tohave immunosuppressive properties and to prevent or attenuateinflammatory cell response [17,21].
Interestingly, recent studies suggested that level of phosphodi-esterase may be used as marker for autoimmune disease severity[22–24]. They supported the immunomodulatory action of PDEinhibitors in autoimmune disease and confirmed the possibleinvolvement of phosphodiesterases in the pathogenesis of autoim-mune diseases.
A few studies that were designed to test the effect ofdipyridamole, a non-specific phosphodiesterase inhibitor, on thepathogenesis of autoimmune diseases [8–10]. In the present study,we carefully evaluated the prophylactic and therapeutic potential ofdipyridamole, for the treatment of adjuvant-induced arthritis in rats.Our findings show that dipyridamole has prophylactic but nottherapeutic anti-inflammatory and arthritic actions. It was observedthat dipyridamole after prophylactic administration markedly sup-pressed the adjuvant arthritis syndrome in rats. It reducedsignificantly the arthritis index, loss in body weight, second peak offever, increased in hind paw volume, hyperalgesia, inflammatorycellular infiltrate in the synovium of the ankle joints and pannusformation. The maximum protective effect of dipyridamole alonewas seen with the highest dose (270 mg/kg/day). However, therewere insignificant differences between the effects of therapeuticadministration of dipyridamole and effects of vehicle (1% DMSO) onthe arthritic syndrome.
The anti-inflammatory and anti-arthritic activity of dipyridamolehas been mainly studied at cellular or clinical levels. Chen et al. [4]suggested that dipyridamole exerts anti-inflammatory effect viaactivation of MKP-1 which dephosphorylates and inactivates p38MAPK. Inactivation of p38MARK in turn inhibits 1KK-β activation andsubsequently the NF-κ β signaling pathway that mediates LPS-induced cyclooxgenase-2 expression in RAW 264.7 cells. AlsoChakrabarti et al. [6] demonstrated that dipyridamole's antioxidanteffects in vascular cells are at least partially mediated via suppressionof inflammatory NF-κ β signaling. Other investigators found thatdipyridamole differentially inhibited the expression of several geneproducts in humanmodels of cellular inflammation [3] and suggestedthat the anti-inflammatory and antioxidant actions of dipyridamoleactions of dipyridamole may contribute to some or its therapeuticbenefits [25].
In the clinical studies, there is only one study has evaluated theeffect of dipyridamole alone in rheumatoid patients [10].Theyreported that rheumatoid patients showed no clinical improvementfollowing treatment with dipyridamole for 6 months. However, morerecent articles demonstrated synergistic interaction of dipyridamoleas potential adjuvant therapy to low dose of glucocorticoid in thetreatment of osteoarthritis [8,26,27] and periodontitis [28].
In our study, we observed that dipyridamole has immunomodu-lator effect as evidence by its ability to protect the animal fromadjuvant arthritic syndrome when it was used as prophylactic agentand failed to inhibit the adjuvant arthritis when it was used astherapeutic agent. Dipyridamole also prevents the decrease of IL-10level in arthritic rats and destruction of the articular cartilage.Therefore, our results are in agreement with the only one publishedarticles that demonstrated the effect of dipyridamole in combinationwith glucocorticoid in animal models of rheumatoid [9]. Theyreported that therapeutic administration of dipyridamole has weakimmunomodulator effect but it can selectively amplifies prednisolo-ne's anti-inflammatory and immunomodulatory effects withoutreplicating steroid side effects.
However, in the present work, the synergistic interaction wasobserved between dipyridamole and low dose of nitric oxide donor(SNP) or nitric oxide synthase inhibitor. In our experiment, the anti-inflammatory and anti-arthritic actions of dipyridamole were ampli-fied markedly by L-NMMA, a non-specific NOs inhibitor. These resultsare in markedly good agreement with those studies that provideevidence of the involvement of inhibition of NO production in theanti-inflammatory and anti-arthritic effects of PDE inhibitors [29–31].Our present results support the studies suggested that inhibition ofNO synthase are potentially beneficial in treatment of conditionassociated with an overproduction of NO as neurodegenerativedisorders and inflammation [32,33]. Moreover, dipyridamole wasshown to have powerful inhibitory effect on the production of NO[34]. Therefore, added NO synthase inhibitor (L-NMMA) will causemore or prolonging inhibition of production of NO that contributes toamplification of dipyridamole actions against adjuvant arthritis.
Another interesting finding in our study was the amplification ofprotective effect of dipyridamole against adjuvant arthritic syndromeby a low dose of NO donor, SNP and the counteract of this effect by ahigh dose of NO donor, SNP. The reversing of the protective effect ofdipyridamole by a high dose of NO donor is relevant to our suggestionthat dipyridamole protected the animal from adjuvant arthriticsyndrome, at least in part through an inhibition of NO productiondependent mechanism. Therefore, an increase of NO levels by highdose of NO donor will antagonize the action of dipyridamole.However, the effect of low dose of NO donor, was unexpected, it hassimilar effect to action of NO synthase inhibitor, may due to itsnegative feedback regulation action on iNOS activities [35,36].Consistently, Mackenzie et al. [37] investigated that NSAID linkedwith low dose of NO donating moiety are more effective in treatmentof osteoarthritis than NSAID alone.
In conclusion, the results presented in this study reveal thatdipyridamole has prophylactic anti-inflammatory and anti-arthriticactions but weak insignificant therapeutic effects in adjuvant arthriticrats. It appears that dipyridamole's effects are mediated via inhibitionof nitric oxide synthase. These effects were markedly amplified by thenon-specific NOs inhibitor, L-NMMA, and a low dose of NO donor, SNP.These findings suggest that dipyridamole in combination with a non-specific NOs inhibitor or a low dose of NO donor have potentialprophylactic and therapeutic value for various chronic inflammatorydiseases such as rheumatoid arthritis.
References
[1] Stafford NP, Pink AE, White AE, Glenn JR, Heptinstall S. Mechanisms involved inadenosine triphosphate-induced platelet aggregation in whole blood. ArteriosclerThromb Vasc Biol 2003;23:1928–33.
[2] Beavo JA. Cyclic nucleotide phosphodiesterases: functional implications ofmultiple isoforms. Physiol Rev 1995;75:725–48.
[3] Weyrich AS, Denis MM, Kuhlmann-Eyre JR, Spencer ED, Dixon DA, Marathe GK,et al. Dipyridamole selectively inhibits inflammatory gene expression in platelet-monocyte aggregates. Circulation 2005;111:633–42.
[4] Chen TH, Kao YC, Chen BC, Chen CH, Chan P, Lee HM. Dipyridamole activation ofmitogen-activated protein kinase phosphatase-1 mediates inhibition of lipopoly-saccharide-induced cyclooxygenase-2 expression in RAW 264.7 cells. Eur JPharmacol 2006;541:138–46.
[5] Chakrabarti S, Vitseva O, Iyu D, Varghese S, Freedman JE. The effect ofdipyridamole on vascular cell-derived reactive oxygen species. J Pharmacol ExpTher 2005;315:494–500.
[6] Chakrabarti S, Blair P, Wu C, Freedman JE. Redox state of dipyridamole is a criticaldeterminant for its beneficial antioxidant and anti-inflammatory effects. JCardiovasc Pharmacol 2007;50:449–57.
[7] Wykretowicz A, Filipiak A, Szczepanik A, Wysocki H. Dipyridamole inhibitshydroxylamine augmented nitric oxide (NO) production by activated polymor-phonuclear neutrophils through an adenosine-independent mechanism. PhysiolRes 2004;53:645–52.
[8] Kvien TK, Fjeld E, Slatkowsky-Christensen B, Nichols M, Zhang Y, Prøven A, et al.Efficacy and safety of a novel synergistic drug candidate, CRx-102, in handosteoarthritis. Ann Rheum Dis 2008;67:942–8.
[9] Zimmermann GR, Avery W, Finelli AL, Farwell M, Fraser CC, Borisy AA. Selectiveamplification of glucocorticoid anti-inflammatory activity through synergisticmulti-target action of a combination drug. Arthritis Res Ther 2009;11:105.

1414 A. Gomaa et al. / International Immunopharmacology 10 (2010) 1406–1414
[10] Forrest CM, Stone TW, Mackay GM, Oxford L, Stoy N, Harman G, et al. Purinemetabolism and clinical status of patients with rheumatoid arthritis treated withdipyridamole. Nucleosides Nucleotides Nucleic Acids 2006;25:1287–90.
[11] Trentham DE, Townes AS, Kang AH. Autoimmunity to type II collagen: anexperimental model of arthritis. J Exp Med 1977;146:857–68.
[12] Wooley PH, Luthra HS, Stuart JM, David CS. Type II collagen-induced arthritis inmice. Major histocompatibility complex (I region) linkage and antibody response.J Exp Med 1981;154:688–700.
[13] Philippe L, Gegout-Pottie P, Guinamp C, Bordji K, Terlain B, Netter P, et al. Relationsbetween functional, inflammatory, and degenerative parameters during adjuvantarthritis in rats. Am J Physiol 1997;273:R 1550–6.
[14] David IB, Elizabeth AK, Michael FJ, Chih-Hung L, Shripad SB, Michael W, et al. Anti-inflammatory effects of ABT-702, a novel non-nucleoside adenosine kinaseinhibitor in rat adjuvant arthritis. J Pharmacol Exp Ther 2001;296:495–500.
[15] Andersen ML, Tufik S. Altered sleep and behavioral patterns of arthritic rats. SleepRes Online 2000;3:161–7.
[16] McCartney-Francis NL, Chan J, Wahl SM. Inflammatory joint disease: clinical,histological, and molecular parameters of acute and chronic inflammation andtissue destruction. In: Winyard PG, Willoughby DA, editors. InflammationProtocols. New Jersey: Humana Press; 2003. p. 147–59.
[17] Silva JC, Rocha MF, Limaa AA, Brito AG, deMenezes DB, Ria VS. Effect ofpentoxifylline and nabumetone on the serum of IL-1beta and TNFalpha in ratswith adjuvant arthritis. Inflamm Res 2000;49:14–9.
[18] Skapenko A, Leipe J, Lipsky PE, Schuiz-Koops H. The role of the T cell in autoimmuneinflammation. Arthritis Res Ther 2005;7:s4–s14.
[19] Weiner HL. The challenge of multiple sclerosis:how do we cure a chronicheterogenous disease? Ann. Neurol 2009;65:239–48.
[20] Shenoy P, Agarwal V. Phosphodiesterase inhibitors in the management ofautoimmunedisease. Autoimmun Rev 2010;9:511–5.
[21] Folicik VA, Smith T, O'Bryant S, Kawczak JA, Zhu B, Sakurai H, et al. Treatmentwith BBB022A or rolipram stabilizes the blood–brain barrier in experimentalautoimmune encephalomyelitis: an additional mechanism for the therapeuticeffect of type IV phosphodiesterase inhibitors. J Neuroimmunol 1999;97:119128.
[22] Mizrachi K, Aricha R, Feferman T, Kela-Madar N, Mandel I, Paperna T, et al.Involvement of phosphodiesterase in autoimmune diseases. J Neuroimmunol2010;220:43–51.
[23] Menon RT, Feferman T, Aricha R, Souroujon MC, Fuchs S. Suppression ofexperimental autoimmune myasthenia gravis by combination therapy; pentox-ifylline as a steroid-sparing agent. J Neuroimmunol 2008;201:128–35.
[24] Aricha R, Feferman T, Souroujon MC, Fuchs S. Overexpression of phosphodiester-ase in experimental autoimmune myasthenia gravis: suppression of disease by aphosphodiesterase inhibitor. FASEB J 2006;20:374–6.
[25] Kim H, Liao JK. Translational therapeutics of dipyridamole. Arterioscler Throm VasBiol 2008;28:s39–42.
[26] Huttner K., shergy W.J., Romney C., Randle J.C. CRx-1002 (Preednisolone/Dipyridamole combination) enhances glucorticoid (GC) efficacy and reducesadverse effects in OA therapy: 3–12 month results. Presentation: ACR/ARHP;Annual Scientific Meeting october20,2009. http://acr.confex.com/acr/2009/ebprogram/paper/12928.html.
[27] Haugen Ik, Slatkowsky-Christensen B, Lessem J, Kvien TK. The responsiveness ofjoint counts, patient-reported measures and proposed composite scores in handosteoarthritis: analyses from a placebo-controlled trial. Ann Rheum Dis 2010;69:1436–40.
[28] Renvert S, Lindahi C, Roos-Jansaker AM, Lessem J. Short-term effects of an anti-inflammatory treatment on clinical parameters and serum levels of C-reactiveprotein and proinflammatory cytokines in subjects with periodontitis. J Period-ontol 2009;80:892–900.
[29] Markovic M, Miljkovic D, Trajkovic V. Regulation of inducible nitric oxide synthaseby cAMP-elevating phosphodiesterase inhibitors. Curr Drug Targets InflammAllergy 2003;2:63–79.
[30] Yoshikawa M, Suzumura A, ITO A, Tumaru T, Takayanagi T. Effect of phosphodi-esterase inhibitors on nitric oxide production by glial cells. Tohoku J Exp Med2002;196:167–77.
[31] Beshay E, Croze F, Prud'homme GJ. The phosphodiesterase inhibitors pentoxifyl-line and rolipram suppress macrophage activation and nitric oxide production invitro and in vivo. Clin Immunology 2001;98:272–9.
[32] Hobbs AJ, Higgs A, Moncada S. Inhbition of nitric oxide synthase as a potentialtherapeutic. Ann Rev Pharm Tox 1999;39:191–220.
[33] Conner JR, Manning PT, Settle S, Moore WM, Jerome G, Webber RK, et al.Suppression of adjuvant-induced arthritis by selective inhibition of nitric oxidesynthase. Eur J Pharm 1995;273:15–24.
[34] Wykretowicz A, Filipia KA, Szczepanik A, Wysocki H. Dipyridamole inhibithydroxylamine augmented nitric oxide(NO) production by activated polymor-phonuclear neutrophils through an adenosine-independent mechanism. PhysiolRes 2004;53:645–52.
[35] Gomaa A, Elshenawy M, Afifi N, Mohammed E, Thabit R. Dual effect of nitric oxidedonor on adjuvant arthritis. Int Immunopharmacol 2009;9:439–47.
[36] Kim HA, Lee KB, Bae SC. The mechanism of low-concentration sodium nitroprus-side — mediated protection of chondrocyte death. Arthritis Res Ther 2005;7:R526–35.
[37] Mackenzie IS, Rutherford D, MacDonald TM. Nitric oxide and cardiovasculareffects: new insights in the role of nitric oxide for the management ofosteoarthritis. Arthritis Res Ther 2008;10:1s–12s.




















