
The Addition of High Doses of Hyaluronic Acid to a Biphasic ...

© Masson, Paris, 2006. Gastroenterol Clin Biol 2006;30:763-768
763
ORIGINAL ARTICLE
Influence of acetaminophen at therapeutic doses on surrogate markers of severity of acute viral hepatitis
César YAGHI, Khalil HONEIN, Joseph BOUJAOUDE, Rita SLIM, Rami MOUCARI, Raymond SAYEGH
Division of Gastroenterology, Hôtel-Dieu de France University Hospital, Beirut, Lebanon.
SUMMARYObjectives — Data on the influence of acetaminophen intake onacute viral hepatitis is scarce, but it could play a role in the worsen-ing of this disease. The aim of this study was to determine whetherthe intake of acetaminophen at therapeutic doses affects the severityof acute viral hepatitis.
Methods — This was a prospective study concerning 37 consecutivepatients hospitalized for acute viral hepatitis. Acetaminophen con-sumption and time since last intake were assessed by a question-naire. Parameters of severity were studied in comparison to timerelated serum concentrations of acetaminophen.
Results — Patients hospitalized for acute viral hepatitis (18 male,19 female patients) had a mean age of 29.2 ± 11.5 years. Thecausal virus was HAV (n = 23), HBV (n = 7) and other viruses(n = 8). The mean cumulated dose of acetaminophen was7.7 ± 5.65 g. The daily dose did not exceed the therapeutic dosageand the mean was 1.95 ± 0.81 g (1-3 g). Patients who received7.5 g of acetaminophen or more had a lower prothrombin index52.4 ± 30.3% vs 74.2 ± 17.2% (P = 0.039), and a lower factor V54.7 ± 33.2% vs 83.3 ± 19.6% (P = 0.033). Prothrombin index andbilirubinemia were negatively correlated with time related plasmaacetaminophen concentrations.
Conclusions — The use of acetaminophen at therapeutic doses wasassociated with greater alterations of surrogate markers of theseverity of acute viral hepatitis especially hepatitis A. This wasrelated to cumulated dosages and correlated to the time relatedacetaminophen plasma concentrations. Acetaminophen use shouldbe interrupted when acute hepatitis is suspected.
RÉSUMÉ
César YAGHI, Khalil HONEIN, Joseph BOUJAOUDE, Rita SLIM, Rami MOUCARI, Raymond SAYEGH
Objectifs — Les données concernant l’influence de la prise d’acéta-minophène sur les hépatites virales sont rares, mais cette prise pour-rait avoir un rôle dans leur aggravation. Notre objectif était d’établirsi la prise d’acétaminophène avait une influence sur la sévérité deshépatites aiguës virales.
Malades et méthodes — Il s’agit d’une étude prospective concernant37 malades consécutifs hospitalisés pour hépatite virale aiguë. Laquantité d’acétaminophène et l’intervalle de temps depuis la dernièreprise étaient évalués par un questionnaire. Les paramètres de sévéritéde l’hépatite étaient étudiés par la concentration plasmatique d’acé-taminophène en fonction du temps écoulé depuis la dernière prise.
Résultats — Les malades hospitalisés pour hépatite aiguë virale(18 hommes, 19 femmes) d’âge moyen 29,2 ° 11,5 ans présen-taient une hépatite aiguë A, B, ou autre chez respectivement 23, 7,et 8 malades. La dose cumulée moyenne d’acétaminophène parmalade était de 7,7 ° 5,65 g. La posologie quotidienne moyenneétait de 1,95 ° 0,81 g (1-3 g). Les malades qui avaient reçu unedose cumulée d’acétaminophène ² 7,5 g avaient un taux deprothrombine plus bas (52,4 ° 30,3 % vs 74,2 ° 17,2 %)(P = 0,039), ainsi qu’un taux plus faible du facteur V (54,7 ° 33,2 %vs 83,3 ° 19,6 %) (P = 0,033). Le taux de prothrombine et la biliru-binémie étaient corrélés négativement avec la concentration plasma-tique d’acétaminophène.
Conclusion — L’utilisation d’acétaminophène à posologie thérapeu-tique était associée par une altération des marqueurs biologiques desévérité des hépatites virales en particulier les hépatites A. Cettealtération était liée à la prise cumulée d’acétaminophène, et corréléeavec la concentration plasmatique d’acétaminophène en fonction dutemps écoulé depuis la dernière prise. La prise d’acétaminophènedevrait être arrêtée quand le diagnostic d’hépatite aiguë est posé.
Introduction
Acetaminophen is used to treat symptoms such as pain andfever. Therapeutic plasma levels range from 10 to 30 µg/mL.Peak levels after therapeutic doses do not exceed 20 µg/mL andthey do not accumulate with multiple daily dosing [1]. However,patients who develop severe liver injury and continue to ingestmultiple doses of acetaminophen may accumulate the drug dueto prolongation of the half life of acetaminophen [2]. In the clini-
cal setting, therapeutic dosages should take into account severalfactors, including history of ethanol abuse as well as the underly-ing hepatic illness. Several cases of severe liver toxicity havebeen reported even when the drug was taken at normal doses inalcoholic patients [3-6]. Furthermore, acetaminophen overdose,either intentional or unintentional, plays a major role in the etiol-ogy of acute liver failure.
During the prodromal period of viral infections, there is adown regulation of the gene expression of major cytochromeP-450 enzymes through proinflammatory cytokines, such as
Influence de la prise d’acétaminophène à doses thérapeutiques sur les marqueurs de sévérité des hépatites virales aiguës
(Gastroenterol Clin Biol 2006;30:763-768)
Reprints: C. YAGHI, Division of Gastroenterology, Hôtel-Dieu de France Adib Ishac Street, Achrafieh, Beirut, Lebanon.E-mail : cesar.yaghi @usj.edu.lb
Part of the content of this paper was presented at the “JournéesFrancophones de Pathologie Digestive” on Paris in March 2004 andat the poster session of the UEGW 2004 held in Prague onSeptember 2004.

C. Yaghi et al.
764
interleukins, transforming growth factor beta1, human hepato-cyte growth factor, and lymphocytotoxin. The resulting effect var-ies according to the involved cytokines and the specificcytochrome P-450, eventually leading to either metabolite-medi-ated adverse drug reactions or alteration of the metabolism ofthe drug [7]. Thus, acetaminophen metabolism is altered duringacute viral hepatitis, and this alteration persists during the conva-lescence phase and disappears only after complete recoveryfrom hepatitis. The elimination phase of acetaminophen is pro-tracted, whereas the peak plasmatic concentration following asingle dose is not affected [8]. The evolution of plasma acetami-nophen concentrations after multiple dosages has not been stud-ied in this setting. In patients with liver failure and portalhypertension, the absorption of acetaminophen is faster espe-cially in the presence of esophageal varices [9]. Patients with cir-rhosis have a higher area under curve and lower clearance ofacetaminophen [9]. Increased absorption may be related to por-tal hypertension whereas protracted elimination is mainly due toliver failure [9]. Data on the role of acetaminophen in the courseof acute viral hepatitis is scarce, but it seems to contribute to liverinjury. Many questions remain unanswered [2]. In a recent paperit was shownthat fulminant hepatitis A was associated with femalegender, the rapid elimination of HAV detected by PCR, genotypeother than genotype 1A, and acetaminophen intake [10]. How-ever, in multivariate analysis, the only two independent prognosticvariables were increased bilirubin levels and low or undetectableviremia. Acetaminophen is currently used for fever especially dur-ing the prodromal period before acute viral hepatitis is suspected.Data from the Acute Liver Failure Study Group showed that aceta-minophen was detected in the serum of 20% of patients with acuteviral hepatitis. In these patients median alanine aminotransferaselevels were higher than in patients who did not take acetami-nophen [11]. In a recent review, it was suggested that the 24 hourintake of acetaminophen in patients with acute or chronic liverdisease should be restricted to around 2 g/day, which is half thesuggested maximal dose of 4 g/day [12].
The aim of our study was to assess whether the intake ofacetaminophen at usual therapeutic levels is associated withincreased severity in the course of acute viral hepatitis.
Patients and methods
Study populationThis was a prospective study of 37 consecutive patients hospitalized
for acute viral hepatitis of various etiologies between December 2002and February 2004. The causes for hospitalization were either acuteliver failure or oral intolerance. A standardized questionnaire evaluatingthe quantity of ingested acetaminophen since the beginning of the symp-toms, the interval since the last intake, as well as the search for factorsassociated with increased acetaminophen toxicity, (alcohol use, pro-longed fasting, and underlying liver disease).
Prolonged fasting was defined as the absence of food intake formore than 24 hours. An underlying liver disease was ruled out by takinginto account clinical, biological and serology parameters particularly inpatients with hepatitis B.
Acetaminophen concentrations were assessed upon admission. Aquantitative colorimetric method in the serum at 430 nm was used, witha precision ranging from 1 to 1.07 (Sigma Diagnostics, Acetamino-phen). Acute hepatitis was diagnosed by Anti HAV IgM for acute hepati-tis A, Anti HBc IgM along with the absence of Anti HBc IgG, for acutehepatitis B, IgM Anti viral capsid antibodies (Anti VCA) for EBV associa-ted hepatitis, and IgM Anti CMV and pp65 antigen for CMV associated
hepatitis. All patients had an abdominal ultrasound rule out chronic liverdisease. All patients had liver enzyme tests as well as bilirubin,prothrombin index and factor V dosages. The severity of hepatitis andfulminant liver failure were defined in accordance with the Beaujon crite-ria [13]. Alcohol consumption was classified into 4 groups: (0) no alco-hol, (1) less than 20 g per week, (3) 20 to 60 g per week, and (4) morethan 60 g per week.
Statistical analysisNumeric data are expressed as mean ± standard deviation. Compa-
risons were made using the Chi square test and Fisher exact test for cate-gorical data. Comparison of continuous variables was performed usingthe Student’s unpaired t-test and non parametric tests, as indicated. Atwo tailed probability P value of less than 0.05 was considered signifi-cant. Linear regression was used to assess the influence of acetamino-phen concentrations on the prothrombin index while taking into accountthe interval since the last intake of acetaminophen.
Results
Clinical characteristics
Thirty seven consecutive patients (18 males and 19 females)were included in our study. Mean age was 29.3 ± 11.5 yearsand age ranged from 15 to 69 years. Fever was found in 33(89.2%) patients. None of our patients had a chronic liver dis-ease. Prolonged fasting was found in only one patient and wasrelated to repeated vomiting and oral intolerance. Alcohol con-sumption was less than 60 g/week (n = 19, 51.4%) or absent(n = 18, 48.6%) in all our patients. None of our patients hadchronic alcohol abuse or recurrent binges.
Etiology
Twenty two patients had an acute hepatitis A, 7 an acutehepatitis B, and among 8, hepatitis was related to either EBV orCMV. Out of the patients presenting with hepatitis B, 4 weresevere, of whom, 3 had a fulminant liver failure, with 2 deathsrelated to liver disease (table I). Eight patients had a severe hep-atitis in the HAV group. With respect to EBV related hepatitis asingle patient had an increased prothrombin index (table I).
Acetaminophen intake in patients with acute viral hepatitis
Thirty two patients (86.5%) had taken acetaminophen. Thequantity of acetaminophen and the interval since the last Intakecould be precisely established in 25 patients. Total consumption,the mean number of days of acetaminophen intake and the dailydose of acetaminophen was equivalent in all groups. Intervalsince the last intake was longest in patients with acute hepatitis B(table I). All patients received acetaminophen prior to hospitaliza-tion and/or to the diagnosis of acute hepatitis and did not receiveany further dose once the diagnosis was established. The meancumulated dose of acetaminophen was 7.7 ± 5.7 g ranging from1.5 g to 28 g taken over a mean period of 4.2 ± 3.2 days rang-ing from 1 to 14 days. The mean daily dose was 1.9 ± 0.8 g andextreme doses ranged from 1 g/day to 3 g/day. There werenovoluntary or involuntary acetaminophen overdoses in ourpopulation. Mean plasma acetaminophen concentrations were32.3 ± 15.7 mg/L. Mean interval since the last intake was33.5 ± 23.7 hours. When the interval was ≥ 24 hours, the meanplasma acetaminophen concentration was 34.8 mg/L, whereaswhen the delay was < 24 hours, the mean plasma concentrationwas 27.9 mg/L. This difference was not statistically significant.On the other hand, all patients (11/25) with a prothrombinindex < 60% had acetaminophen detectable in plasma after adelay ≥ 24 hours. None of the patients with severe acute hepati-tis had an interval of < 24 hours since” the last intake. For
ABBREVIATIONS :HAV : Hepatitis A virusHBV : Hepatitis B virusCMV : CytomegalovirusEBV : Epstein-Barr virus
Acetaminophen and acute viral hepatitis
765
patients with prothrombin index ≥ 60%, 9 patients were detectedwithin 24 hours, and 5 after 24 hours. When the intervalwas ≥ 24 hours, 68.7% had severe hepatitis whereas 31.3%had non severe hepatitis (P < 0.001).
Prothrombin index in relation to acetaminophen concentrations
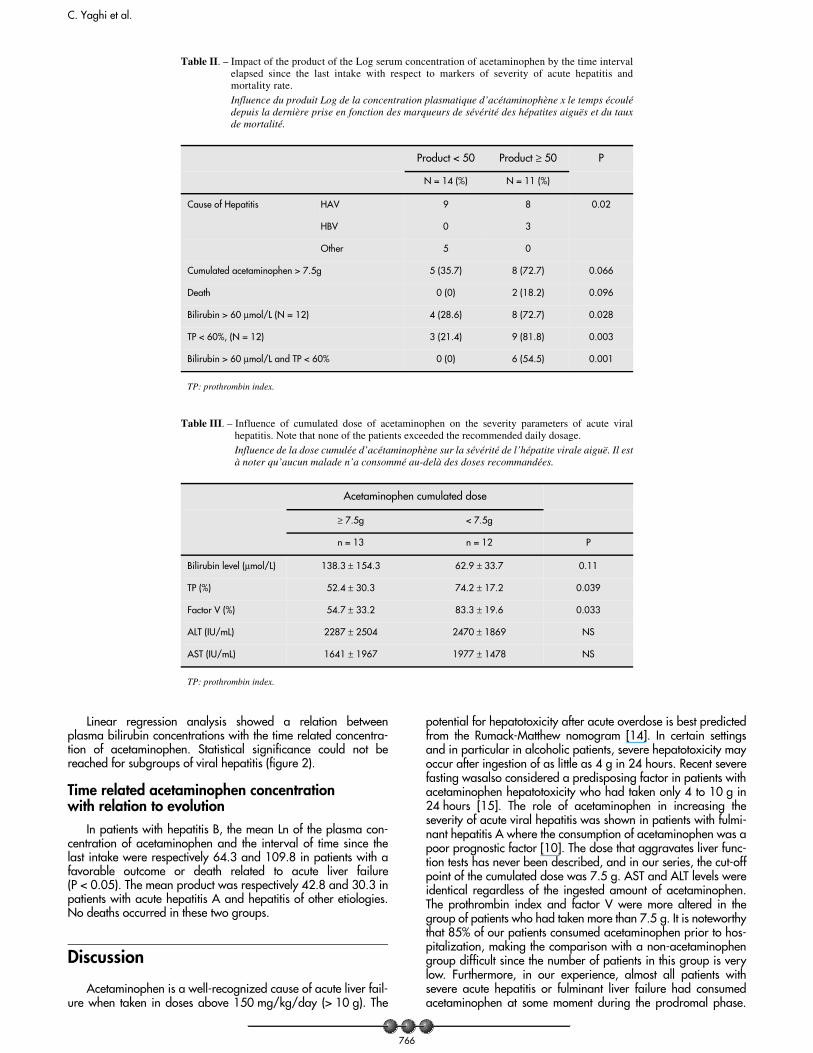
The Log (Ln) of the plasma concentration of acetaminophenand the time interval since the last intake were negatively corre-lated with the prothrombin index. This correlation was found inpatients with acute hepatitis A. There was no statistically signifi-cant correlation in either of the groups of patients with acute hep-atitis B nor EBV or CMV related hepatitis (figure 2).
On the other hand, the product of the mean serum concen-tration of acetaminophen times the time interval since the lastintake was 66.8 when the prothrombin index was less than 60%versus 30.9 when the prothrombin index was above 60%(P = 0.001) (table II). This difference was found in the acute hep-atitis A group and could not be analyzed in the hepatitis B groupsince all the patients had a prothrombin index < 60% in this sub-group. There was no significant difference in patients with CMVor EBV related hepatitis.
The cumulated dose of acetaminophen in our population was7.7 ± 5.7 g. Patients who received 7.5 g of acetaminophen ormore had a lower prothrombin index, and a lower factor Vactivity. It should be noted that none of the patients exceeded therecommended dose of acetaminophen. There was no difference
in aminotransferase levels, AST or ALT for the cumulated dose ofacetaminophen (table III).
Two patients died from fulminant liver failure related to HBVinfection. Both had a cumulated acetaminophen consumption ofmore than 7.5 g, and these patients had the highestproduct of theserum concentration of acetaminophen times the interval elapsedsince the last intake in our studied population, with respectively90.0 and 129.7. This product was respectively 41.0 ± 21.2 and109.9 ± 28.1 for spontaneous recovery and for death (table II).
Bilirubin relation to acetaminophen concentrations
Patients who received 7.5 g of acetaminophen or more, hada tendency to have higher bilirubin levels but this was not statisti-cally significance. The product of the mean serum concentrationsofacetaminophen times the interval since the last intake was 61.2when the bilirubin level was above 60 µmol/L versus 33.3 whenthe bilirubin level was below 60 µmol/L (P = 0.01). This differ-ence was also significant in the group with acute hepatitis A(54.0 vs 29.1, P = 0.02), but not in patients with acute hepatitisB in whom the difference was not statistically significant (109.9vs. 64.3, P > 0.05). Patients who had bilirubin above 60 µmol/Land a prothrombin index below 60% had the highest product(81.7 ± 26.5), whereas the lowest product was found in patientswith neither (23.5 ± 10.8). In patients with a bilirubin> 60 µmol/L or prothrombin activity < 60%, the value was inter-mediate (39.9 ± 22.3 and 49 ± 13.3 respectively for bilirubinand prothrombin index) (figure 1) (table II).
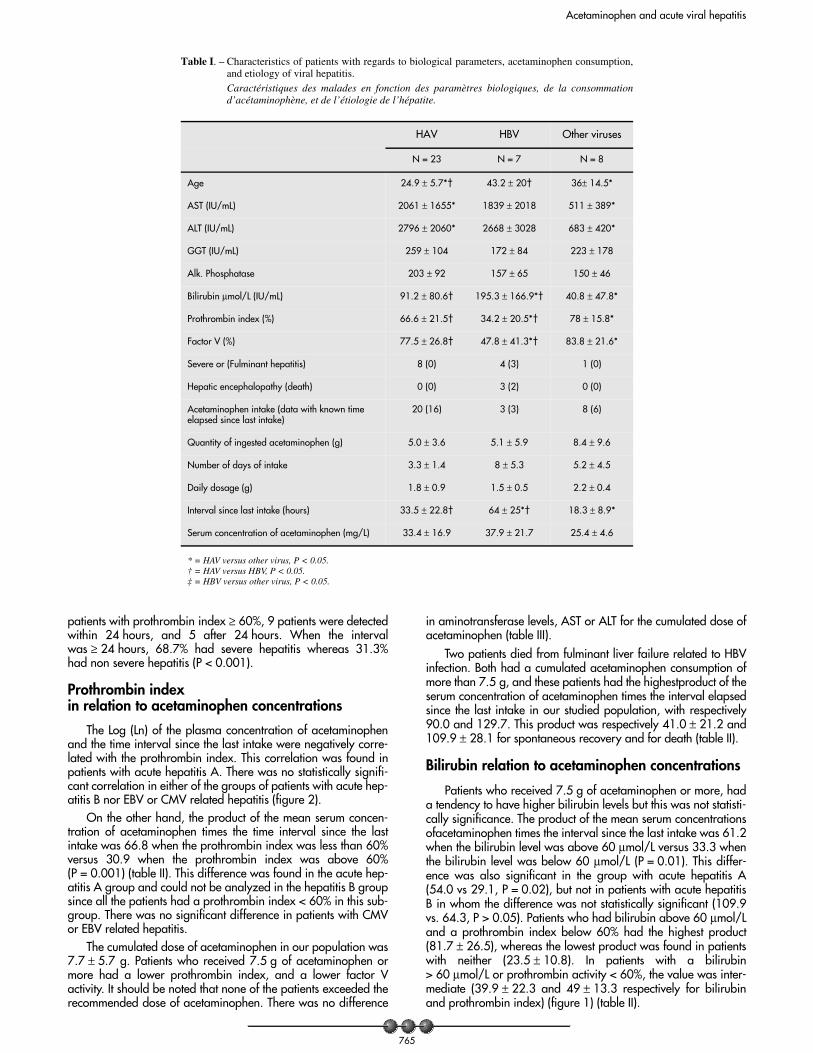
Table I. – Characteristics of patients with regards to biological parameters, acetaminophen consumption,and etiology of viral hepatitis.Caractéristiques des malades en fonction des paramètres biologiques, de la consommationd’acétaminophène, et de l’étiologie de l’hépatite.
HAV HBV Other viruses
N = 23 N = 7 N = 8
Age 24.9 ± 5.7*† 43.2 ± 20† 36± 14.5*
AST (IU/mL) 2061 ± 1655* 1839 ± 2018 511 ± 389*
ALT (IU/mL) 2796 ± 2060* 2668 ± 3028 683 ± 420*
GGT (IU/mL) 259 ± 104 172 ± 84 223 ± 178
Alk. Phosphatase 203 ± 92 157 ± 65 150 ± 46
Bilirubin µmol/L (IU/mL) 91.2 ± 80.6† 195.3 ± 166.9*† 40.8 ± 47.8*
Prothrombin index (%) 66.6 ± 21.5† 34.2 ± 20.5*† 78 ± 15.8*
Factor V (%) 77.5 ± 26.8† 47.8 ± 41.3*† 83.8 ± 21.6*
Severe or (Fulminant hepatitis) 8 (0) 4 (3) 1 (0)
Hepatic encephalopathy (death) 0 (0) 3 (2) 0 (0)
Acetaminophen intake (data with known time elapsed since last intake)
20 (16) 3 (3) 8 (6)
Quantity of ingested acetaminophen (g) 5.0 ± 3.6 5.1 ± 5.9 8.4 ± 9.6
Number of days of intake 3.3 ± 1.4 8 ± 5.3 5.2 ± 4.5
Daily dosage (g) 1.8 ± 0.9 1.5 ± 0.5 2.2 ± 0.4
Interval since last intake (hours) 33.5 ± 22.8† 64 ± 25*† 18.3 ± 8.9*
Serum concentration of acetaminophen (mg/L) 33.4 ± 16.9 37.9 ± 21.7 25.4 ± 4.6
* = HAV versus other virus, P < 0.05. † = HAV versus HBV, P < 0.05. ‡ = HBV versus other virus, P < 0.05.
C. Yaghi et al.
766
Linear regression analysis showed a relation betweenplasma bilirubin concentrations with the time related concentra-tion of acetaminophen. Statistical significance could not bereached for subgroups of viral hepatitis (figure 2).
Time related acetaminophen concentration with relation to evolution
In patients with hepatitis B, the mean Ln of the plasma con-centration of acetaminophen and the interval of time since thelast intake were respectively 64.3 and 109.8 in patients with afavorable outcome or death related to acute liver failure(P < 0.05). The mean product was respectively 42.8 and 30.3 inpatients with acute hepatitis A and hepatitis of other etiologies.No deaths occurred in these two groups.
Discussion
Acetaminophen is a well-recognized cause of acute liver fail-ure when taken in doses above 150 mg/kg/day (> 10 g). The
potential for hepatotoxicity after acute overdose is best predictedfrom the Rumack-Matthew nomogram [14]. In certain settingsand in particular in alcoholic patients, severe hepatotoxicity mayoccur after ingestion of as little as 4 g in 24 hours. Recent severefasting wasalso considered a predisposing factor in patients withacetaminophen hepatotoxicity who had taken only 4 to 10 g in24 hours [15]. The role of acetaminophen in increasing theseverity of acute viral hepatitis was shown in patients with fulmi-nant hepatitis A where the consumption of acetaminophen was apoor prognostic factor [10]. The dose that aggravates liver func-tion tests has never been described, and in our series, the cut-offpoint of the cumulated dose was 7.5 g. AST and ALT levels wereidentical regardless of the ingested amount of acetaminophen.The prothrombin index and factor V were more altered in thegroup of patients who had taken more than 7.5 g. It is noteworthythat 85% of our patients consumed acetaminophen prior to hos-pitalization, making the comparison with a non-acetaminophengroup difficult since the number of patients in this group is verylow. Furthermore, in our experience, almost all patients withsevere acute hepatitis or fulminant liver failure had consumedacetaminophen at some moment during the prodromal phase.
Table II. – Impact of the product of the Log serum concentration of acetaminophen by the time intervalelapsed since the last intake with respect to markers of severity of acute hepatitis andmortality rate.Influence du produit Log de la concentration plasmatique d’acétaminophène x le temps écoulédepuis la dernière prise en fonction des marqueurs de sévérité des hépatites aiguës et du tauxde mortalité.
Product < 50 Product ≥ 50 P
N = 14 (%) N = 11 (%)
Cause of Hepatitis HAV 9 8 0.02
HBV 0 3
Other 5 0
Cumulated acetaminophen > 7.5g 5 (35.7) 8 (72.7) 0.066
Death 0 (0) 2 (18.2) 0.096
Bilirubin > 60 µmol/L (N = 12) 4 (28.6) 8 (72.7) 0.028
TP < 60%, (N = 12) 3 (21.4) 9 (81.8) 0.003
Bilirubin > 60 µmol/L and TP < 60% 0 (0) 6 (54.5) 0.001
TP: prothrombin index.
Table III. – Influence of cumulated dose of acetaminophen on the severity parameters of acute viralhepatitis. Note that none of the patients exceeded the recommended daily dosage.Influence de la dose cumulée d’acétaminophène sur la sévérité de l’hépatite virale aiguë. Il està noter qu’aucun malade n’a consommé au-delà des doses recommandées.
Acetaminophen cumulated dose
≥ 7.5g < 7.5g
n = 13 n = 12 P
Bilirubin level (µmol/L) 138.3 ± 154.3 62.9 ± 33.7 0.11
TP (%) 52.4 ± 30.3 74.2 ± 17.2 0.039
Factor V (%) 54.7 ± 33.2 83.3 ± 19.6 0.033
ALT (IU/mL) 2287 ± 2504 2470 ± 1869 NS
AST (IU/mL) 1641 ± 1967 1977 ± 1478 NS
TP: prothrombin index.

Acetaminophen and acute viral hepatitis
767
There is controversial evidence on the efficiency of acetylcysteinetreatment for non-acetaminophen-induced acute liver failure[16]. Some of the controversy might be explained by a suscepti-bility to low dose acetaminophen in some patients, and its role inaggravating liver failure. Acetylcysteine could be beneficial inthis subset of patients.
Criteria for the severity of acute viral hepatitis include INRor prothrombin ratio, serum bilirubin and prothrombin index.The prothrombin index INR may be affected by multiple fac-tors including liver failure, chronic cholestasis, acetaminophen,N-acetyl-cysteine [17-19]. Acetaminophen may decrease theprothrombin index in patients with acetaminophen poisoningwithout hepatic injury. This effect is proportional to the ingesteddose and to the nomogram-based risk [18]. It is due to adecrease in the function of factor VII but not to the amount ofantigenic factor VII in exposed patients [18]. In our patients, theingested amount of acetaminophen was within therapeutic rangeand the mean cumulated dose was 7.7 g, which is low in com-parison to described doses affecting the prothrombin index. Fur-thermore, the plasma concentration of acetaminophen was lowerthan concentrations seen in acetaminophen intoxications, and itis not known if such concentrations affect the prothrombin index.Finally, the drop in the prothrombin index was correlated with adecrease in factor V suggesting that the latter was probablymainly related to the severity of hepatitis. N-acetylcysteine treat-ment was reported to decrease the prothrombin index in allpatients [17]. In our patients, all plasma acetaminophen dosageswere performed prior to the start of N-acetylcysteine perfusion. Ina recent study, the detection of plasmatic acetaminophen-contain-ing protein adducts showed that unrecognized acetaminophen
R2 = 0.523, P< 0.001
Overall population
0 20 40 60 80 100 120 140
Time X Ln plasma acetaminophen
25
50
75
100
Prot
hrom
bin
inde
x
R2= 0.30, P= 0.024
HAV
0 20 40 60 80 100 120 140
Time X Ln plasma acetaminophen
25
50
75
100
Prot
hrom
bin
inde
x
R2 = 0.404, P= 0.001
Overall population
0 20 40 60 80 100 120 140
Time X Ln plasma acetaminophen
0
100
200
300
400
500
Bili
rubi
n
HAV
R2= 0.124, P= 0.166
0 20 40 60 80 100 120 140
Time X Ln plasma acetaminophen
0
100
200
300
400
500
Bili
rubi
n
Fig. 2 – Graphic representation of the regression curves of Log (Ln) plasma acetaminophen concentration with respect to severity parameters of acute hepatitisshowing overall population and HAV patients with respect to prothrombin index and bilirubin.Représentation graphique des courbes de régression du produit du Log de la concentration plasmatique d’acétaminophène x le temps écoulé depuis ladernière prise en fonction du taux de prothrombine et de la bilirubine dans la population globale et chez les malades atteints d’hépatite aiguë A.
1020
3040
5060
7080
90100
110120
Mea
n Ln
ace
tam
inop
hen
× tim
e
<60, < 60%<60, >=60% >=60, < 60% >=60,
A B C D
Fig. 1 – Line Chart representing mean Log acetaminophen plasma concen-tration x time interval since the last intake in relation to Prothrom-bin index and bilirubin in all patients. A = bilirubin < 60 µmol/Land prothrombin index > 60%, B = bilirubin ≥ 60 µmol/L andprothrombin index ≥ 60%, C = bilirubin < 60 µmol/L and pro-thrombin index < 60%, D = bilirubin ≥ 60 µmol/L and prothrom-bin activity < 60%. Differences were statistically significant(P < 0.05) excepted for B versus C (P = 0.09).Représentation graphique du Log de la concentration plasmatiqued’acétaminophène x le temps écoulé depuis la dernière prise enfonction du taux de prothrombine et de la bilirubine plasmatique.A = bilirubine < 60 mmol/L et TP > 60 %, B = bilirubine ² 60mmol/L et TP ² 60 %, C = bilirubine < 60 mmol/L et TP < 60 %,D = bilirubine ² 60 mmol/L et TP < 60 %. Les différences étaientstatistiquement significatives sauf pour B versus C (P = 0,09).

C. Yaghi et al.
768
poisoning might account for 20% of acute liver failure of unknownetiologies [19, 20]. This technique might be interesting for detect-ing the influence of acetaminophen in acute viral hepatitis.
The increase in serum bilirubin observed in viral hepatitis isalso a marker of severity. However, increased serum bilirubincan interfere with the enzymatic and chromogenic reactionsinvolved in the acetaminophen dosing methods. Acetaminophenwas detected in specimens from hyperbilirubinemic patients with-out a history of recent acetaminophen exposure. Dilution ofhyperbilirubinemic specimens produces a correction of apparentacetaminophen concentrations. The threshold for interference ofbilirubin with acetaminophen dosage is < 85 µmol/L [21].
In conclusion, Acetaminophen might be toxic even whenused at therapeutic dosages in the patients with acute viral hepa-titis, in particular acute hepatitis A. In our patients, time relatedplasma concentrations of acetaminophen was correlated tobilirubin levels and the prothrombin index which are surrogatemarkers for the severity of acute viral hepatitis. Acetaminophenshould be discontinued and avoided once the diagnosis of acutehepatitis is established.
REFERENCES
1. Rumack BH. Acetaminophen misconceptions. Hepatology 2004;40:10-5.
2. Kaplowitz N. Acetaminophen Hepatoxicity: What Do We Know, WhatDon’t We Know, and What Do We Do Next? Hepatology 2004;40:23-6.
3. Mofredj A, Cadranel JF, Darchy B, Barbare JC, Cazier A, Pras V,et al. Hepatotoxicity caused by therapeutic doses of paracetamol in al-coholics. Report of 2 cases of fatal hepatitis in cirrhosis. Ann MedInterne, Paris 1999;150:507-11.
4. Andreu V, Gomez-Angelats E, Bruguera M, Rodes J. Severe hepatitisfrom therapeutic doses of paracetamol in an alcoholic patient.Gastroenterol Hepatol 1999;22:235-7.
5. Seeff LB, Cuccherini BA, Zimmerman HJ, Adler E, Benjamin SB.Acetaminophen hepatotoxicity in alcoholics: a therapeutic misadven-ture. Ann Intern Med 1986;104:399-404.
6. Schmidt LE, Dalhoff K, Poulsen HE. Acute versus chronic alcoholconsumption in acetaminophen-induced hepatotoxicity. Hepatology2002;35:876-82.
7. Prandota J Important role of prodromal viral infections responsible forinhibition of xenobiotic metabolizing enzymes in the pathomecha-nism of idiopathic Reye’s syndrome, Stevens-Johnson syndrome, au-toimmune hepatitis, and hepatotoxicity of the therapeutic doses of
acetaminophen used in genetically predisposed persons. Am J Ther2002;9:149-56.
8. Jorup-Ronstrom C, Beermann B, Wahlin-Boll E, Melander A,Britton S. Reduction of acetaminophen and aspirin metabolism duringviral hepatitis. Clin Pharmacokinet 1986;11:250-6.
9. Zapater P, Lasso De La Vega MC, Horga JF, Such J, Frances R,Esteban A, et al. Pharmacokinetic variations of acetaminophen accor-ding to liver dysfunction and portal hypertension status. AlimentPharmacol Ther 2004;20:29-36.
10. Rezende G, Roque-Afonso AM, Samuel D, Gigou M, Nicand E,Ferre V, et al. Viral and clinical factors associated with the fulminantcourse of hepatitis A infection. Hepatology 2003;38:613-18.
11. Polson J, Ocama P, Larson AM, Hynan L, Lalani E, Harrison M, et al.Role of acetaminophen in acute liver failure due to viral hepatitis (abs-tract). Hepatology 2003;34:544A.
12. Lee W. Acetaminophen and the U.S. Acute Liver Failure Study Group:lowering the Risks of Hepatic Failure. Hepatology 2004;40:6-9.
13. Bernuau J, Rueff B, Benhamou JP. Fulminant and subfulminant liverfailure: definitions and causes. Semin Liver Dis 1986;6:97-106.
14. Rumack BH. Acetaminophen hepatotoxicity: the first 35 years.J Toxicol Clin Toxicol 2002;40:3-20.
15. Whitcomb DC, Block GD. Association of acetaminophen hepatotoxi-city with fasting and ethanol use. JAMA 1994;272:1845-50.
16. Sklar GE, Subramaniam M. Acetylcysteine treatment for non-acetaminophen-induced acute liver failure. Ann Pharmacother 2004;38:498-500.
17. Schmidt LE, Knudsen TT, Dalhoff K, Bendtsen F. Effect of acetylcys-teine on prothrombin index in paracetamol poisoning without hepato-cellular injury. Lancet 2002;360:1151-2.
18. Whyte IM, Buckley NA, Reith DM, Goodhew I, Seldon M,Dawson AH. Acetaminophen causes an increased InternationalNormalized Ratio by reducing functional factor VII. Ther Drug Monit2000;22:742-8.
19. Muldrew KL, James LP, Coop L, McCullough SS, Hendrickson HP,Hinson JA, et al. Determination of acetaminophen-protein adducts inmouse liver and serum and human serum after hepatotoxic doses ofacetaminophen using high-performance liquid chromatography withelectrochemical detection. Drug Metab Dispos 2002;30:446-51.
20. Davern TJ, James L, Larson A, Fontana R, Polson J, Lalani E, et al.Serum acetaminophen adducts identify patients with severe acetami-nophen toxicity (abstract). Hepatology 2003;34:539A.
21. Bertholf RL, Johannsen LM, Bazooband A, Mansouri V. False-positiveacetaminophen results in a hyperbilirubinemic patient. Clin Chem2003;49:695-8.
Copyright © 2022 FDOKUMEN




















