
Indian Journal of Practical Pediatrics, Chennai
98
2008; 10(3) : 191 1 IJPP INDIAN JOURNAL OF PRACTICAL PEDIATRICS • IJPP is a quarterly subscription journal of the Indian Academy of Pediatrics committed to presenting practical pediatric issues and management updates in a simple and clear manner • Indexed in Excerpta Medica, CABI Publishing. Vol.10 No.3 JULY.-SEP.2008 Dr. K.Nedunchelian Dr. S. Thangavelu Editor-in-Chief Executive Editor CONTENTS FROM THE EDITOR'S DESK 193 TOPICS FROM “IAP-IJPP CME 2008” Intractable epilepsies in children 196 - Kumaresan G Constipation in Children 201 - Bhaskar Raju B, Sumathi B How do I manage atopic dermatitis? 208 - Jayakar Thomas Surfactant therapy 213 - Lakshmi V Approach to neonatal sepsis 221 - Karthikeyan G Allergic rhinitis 227 - Shivbalan So, Gowrishankar NC Long term control of childhood asthma 235 - Balachandran A Urinary tract infection - When and how to evaluate? 242 - Vijayakumar M, Prahlad N Journal Office and address for communications: Dr. K.Nedunchelian, Editor-in-Chief, Indian Journal of Practical Pediatrics, 1A, Block II, Krsna Apartments, 50, Halls Road, Egmore, Chennai - 600 008. Tamil Nadu, India. Tel.No. : 044-28190032 E.mail : [email protected]
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of Indian Journal of Practical Pediatrics, Chennai
2008; 10(3) : 191
1
IJPPINDIAN JOURNAL OFPRACTICAL PEDIATRICS
••••• IJPP is a quarterly subscription journal of the Indian Academy of Pediatricscommitted to presenting practical pediatric issues and managementupdates in a simple and clear manner
••••• Indexed in Excerpta Medica, CABI Publishing.
Vol.10 No.3 JULY.-SEP.2008
Dr. K.Nedunchelian Dr. S. ThangaveluEditor-in-Chief Executive Editor
CONTENTS
FROM THE EDITOR'S DESK 193
TOPICS FROM “IAP-IJPP CME 2008”
Intractable epilepsies in children 196
- Kumaresan G
Constipation in Children 201
- Bhaskar Raju B, Sumathi B
How do I manage atopic dermatitis? 208
- Jayakar Thomas
Surfactant therapy 213
- Lakshmi V
Approach to neonatal sepsis 221
- Karthikeyan G
Allergic rhinitis 227
- Shivbalan So, Gowrishankar NC
Long term control of childhood asthma 235
- Balachandran A
Urinary tract infection - When and how to evaluate? 242
- Vijayakumar M, Prahlad N
Journal Office and address for communications: Dr. K.Nedunchelian, Editor-in-Chief, Indian Journal ofPractical Pediatrics, 1A, Block II, Krsna Apartments, 50, Halls Road, Egmore, Chennai - 600 008. Tamil Nadu,India. Tel.No. : 044-28190032 E.mail : [email protected]

Indian Journal of Practical Pediatrics 2008; 10(3) : 192
Published on behalf of the Indian Academy of Pediatrics by Dr.K.Nedunchelian, Editor-in-Chief,Indian Journal of Practical Pediatrics from 1A, Block II, Krsna Apartments, 50, Halls Road, Egmore,Chennai - 600 008. Tamil Nadu, India and printed by Mr. D. Ramanathan, at Alamu Printing Works,9, Iyyah Street, Royapettah, Chennai - 600 014.
2
FOR YOUR KIND ATTENTION
* The views expressed by the authors do not necessarily reflect those of the sponsor orpublisher. Although every care has been taken to ensure technical accuracy, no responsibility isaccepted for errors or omissions.
* The claims of the manufacturers and efficacy of the products advertised in the journal are theresponsibility of the advertiser. The journal does not own any responsibility for the guarantee of theproducts advertised.
* Part or whole of the material published in this issue may be reproduced withthe note "Acknowledgement" to "Indian Journal of Practical Pediatrics" without prior permission.
- Editorial Board
Antimicrobials in acute encephalitis 250
- Vishwanathan V
GENERAL ARTICLES
Cyclic vomiting syndrome 254
- Neelam Mohan
Genetic counseling for preventable disorders 263
- Madhulika Kabra
RADIOLOGIST TALKS TO YOU
Intracranial hemorrhage and hypoxic ischemic encephalopathyin the neonate 279
- Vijayalakshmi G, Elavarasu E, Vijayalakshmi M, Venkatesan MD
PICTURE QUIZ 283
DERMATOLOGY
Alopecia areata in children 284
- Madhu.R
BOOK REVIEW 220
NEWS AND NOTES 207,212,226,234,241,262,282,288

2008; 10(3) : 193
3
FROM THE EDITOR’S DESK
In this issue we have included few topicscovered in the “IAP - IJPP CME 2008” organisedby “Indian Academy of Pediatrics” and “IndianJournal of Practical Pediatrics”, conducted atChennai on 15th June 2008. It was uniformly feltthat topics covered were practical and mostuseful in the present context. With the requestfor the proceedings of CME from all over thecountry, this issue is dedicated to bring out someof the articles from CME for the benefit of ourreaders.
The static infant mortality rate (IMR) in ourcountry for the past few decades is contributedmostly by the persistently high neonatal mortality.Among the neonatal morbidity, birth weight andgestational age related complications includingimmature lungs contribute to increased mortalityin these groups. Surfactant therapy seems to bea promising solution to this problem. Descriptionon surfactant, preparations available, indications,etc are given in the article “Surfactant therapy”.Sepsis is one of the common causes of neonatalmorbitity and mortality. “Approach to manage-ment of neonatal sepsis” is also covered in thisissue.
Constipation in children would lead tosignificant discomfort physical as well aspsychological, to the child and mental stress tothe parents. Conditions leading to constipationand management are brought out very well in thearticle “Constipation in children”.
Rhinitis is the another condition, which ifpersists or recurs causes significant morbidity.Allergy as a cause of rhintis is most often notappreciated by pediatrician. When to suspect thisand how to approach and manage this conditionare narrated in the article “Allergic rhinitis”.
Increasing awareness about “asthma”, betterunderstanding of its pathogenesis, etc have
revolutionalised the management of thiscondition, especially the long term managmentand an article in this issue deals with this aspect.Certain proportion of epilepsies even with regularcompliance of antiepileptic drugs becomeintractable. Intractable epilepsy is a nightmareto both parents and pediatrician or neurologist.An article on “intractable epilepsies in children”covers modalities of treatment for the same.Urinary tract infection is a condition, oncediagnosed, has to be evaluated thoroughly forunderlying urological abnormalities. If undertreated, urinary tract infection in young childrencan lead on to end stage renal disease.
Atopic dermatitis runs a protracted coursewith its associated significant morbidity.Theclinical presentation and its management arecovered in the article “Atopic dermatitis inchildren”. Acute encephalitis is dreaded for itsmorbidity in the form of sequelae and highmortality. Mainstay of treatment is supportivewith antiedema measures and in a few conditionsantimicrobials have definite role, which arediscussed in the article on “Antimicrobials inencephalitis”.
Apart from articles selected from “IAP-IJPPCME 2008”, there are two more interestingarticles, “Cyclic vomiting syndrome” and“Genetic counseling”. These are important topicsbecause the practicing pediatrician should knowhow to manage and when to refer for expertopinion. This prompted us to cover these twoconditions. Under “Radiologist talks to you”column “Radiological evaluation of intracranialhemorrhage and HIE in the neonate” is coveredand “Alopecia areata” is included underDermatology Series, which deals with varioustypes and management strategies of the condition.
Dr. K.Nedunchelian,Editor-in-Chief.

Indian Journal of Practical Pediatrics 2008; 10(3) : 194
GeneralPrint the manuscript on one side of standard size A4, white bond paper, with margins of at least 2.5 cm (1”)in double space typescript on each side. Use American English using Times New Roman font 12 size.Submit four complete sets of the manuscript.They are considered for publication on the understanding that they are contributed to this journal solely.All pages are numbered at the top of the right corner, beginning with the title page.All manuscripts should be sent to: The Editor-in-Chief, Indian Journal of Practical Pediatrics
Manuscript1st Page –
TitleName of the author and affiliationInstitutionAddress for correspondence (Email, Phone, Fax if any)Word countNo. of figures (colour / black and white)No. of referencesAuthors contribution
2nd Page –Abstract (unstructured, not exceeding 100 words) with key words (not exceeding 4)
3rd Page -AcknowledgementPoints to remember (not more than 5 points)TextReferencesTablesFigures – should be good quality, 4 copies black & white / colour, (4 x 6 inches – Maxi size) G l o s s yprint. (Each colour image will be charged Rs.1,000/- separately)Legends
TextOnly generic names should be usedMeasurements must be in metric units with System International (SI) Equivalents given in parentheses.
ReferencesRecent and relevant references onlyStrictly adhere to Vancouver styleShould be identified in the text by Arabic numerals in parentheses.Type double-space on separate sheets and number consecutively as they appear in the text.Defective references will entail rejection of article
TablesNumbered with Roman numerals and typed on separate sheets.Title should be centered above the table and explanatory notes below the table.
Figures and legendsUnmounted and with figure number, first author’s name and top location indicated on the back of eachfigure.Legends typed double-space on separate sheet. No title on figure.
INSTRUCTIONS TO AUTHORS
4

2008; 10(3) : 195
Article Categories
Review article
Article should be informative covering the recent and practical aspects in that field. Main articles can be in1500 – 2000 words with 12 – 15 recent references and abstract not exceeding 100 words.
Case report (covering practical importance)
250 – 600 words, 8 – 10 recent references
Clinical spotters section
100 – 150 words write up
With 1 or 2 images of clinically recognizable condition
(of which one could be in the form of clinical photograph / specimen photograph / investigation)
Letters to the Editor
200 – 250 words pertaining to the articles published in the journal or practical viewpoints with scientificbacking and appropriate references in Vancouver style.
Selection procedures
All articles including invited articles will be peer reviewed by two masked reviewers. The decision of theEditorial Board based on the reviewers’ comments is final.
Check List
Covering letter by corresponding author
Declaration (as enclosed) signed by all authors **
Manuscript (4 copies)
Accompanied by a copy in CD / or submit as an email attachment in addition to hard copy.
Failing to comply with the requirement at the time of submission would lead to the rejection of the article.
Author’s contribution / Authorship Criteria
All persons designated as authors should qualify for the authorship. Authorship credit should be based onsubstantial contributions to i) concept and design, or collection of data, and interpretation of data;ii) drafting the article or revising it critically for important intellectual content; and iii) final approval of theversion to be published. All conditions i), ii) and iii) must be met.
**Declaration by authors
I/We certify that the manuscript titled ‘……………………………….’ represents valid work and that neitherthis manuscript nor one with substantially similar content under my/our authorship has been published or isbeing considered for publication elsewhere. The author(s) undersigned hereby transfer(s), assign(s), or otherwiseconvey(s) all copyright ownership, including any and all rights incidental thereto, exclusively to the IndianJournal of Practical Pediatrics, in the event that such work is published in Indian Journal of Practical Pediatrics.I / we assume full responsibility for any infringement of copyright or plagiarism.
Authors’ name(s) in order of appearance in the manuscript
Signatures (date)
All manuscripts, which are rejected will not be returned to author. Those submitting articles shouldtherefore ensure that they retain at least one copy and the illustrations, if any.
5

Indian Journal of Practical Pediatrics 2008; 10(3) : 196
INTRACTABLE EPILEPSIES IN
CHILDREN
* Kumaresan G
Abstract : Despite effective newer drugs andother treatment modalities, 20 - 25% epilepsiesremain intractable. It is essential that realintractability should be established. Treatmentoptions available are anti epileptic drugs,surgery, ketogenic diet and vagal nervestimulation. The indications and advantages ofeach of these modalities are discussed.
Keywords : Intractable epilepsy, Drugs, Surgery,Non pharmacological methods.
Refractory epilepsies,difficult to treatepilepsies or intractable epilepsies refer to ourinability to control seizures effectively.With theintroduction of sodium valproate in 1993 therewas a hope that an ideal anti-convulsant has beendiscovered. However despite the introduction ofmore than ten new drugs, the problem ofintractability exists. 20-25% of epilepsies remainintractable, not responding to standard drugswith significant impairment in quality of life andunacceptable side effects of drugs and risksassociated with every episode of seizure.
The definition of intractable epilepsy is notclearly established.The three importantcomponents include medical intractability,subjective handicap and social disability.
Medical intractability: Is defined as failure torespond to two primary drugs in correct dosage
(checked by drug assay) for atleast six monthsfor each drug. The earlier definition of minimumof two years of drug trial is not acceptable as incatastrophic seizures where denying the benefitsof early surgical therapy leads to loss of valuabletime with permanent impact on quality of life.With many drugs now available no clear cutguidelines are established for order of selectionof drugs
Social disability: This will vary with patient’slife style. While occasional mild complex partialseizures is acceptable to a person doing routinesemiskilled job, even a brief absence attack willbe unacceptable to a person appearing frequentlyin media. Hence the definition of social disabilityis individualised.
Subjective handicap : Refers to how much theseizures interfere with the person’s quality oflife.This is particularly important in children asearly control of seizures will give them betteropportunities for good education,social life andemployment.
The evaluation of intractable epilepsy beginswith a comprehensive re-evaluation of diagnosisand past medical history. The diagnosis ofepilepsy has to be clearly established, as manynon-epileptic conditions may masquarade asintractable epilepsy (as high as 20% in manyepileptic clinics). The drugs tried earlier have tobe checked as to their appropriateness to the typeof epilepsy or syndrome, the dose, the duration,and possibilities of drug interactions due to wrongcombinations.The possibilities of precipitatingfactors including psycho-social factorscontributing to intractability has to be excluded.
IAP-IJPP CME 2008
* Former Professor of Pediatric Neurology,Institute of Child Health and Hospital forChildren, Egmore, Chennai - 8.
6

2008; 10(3) : 197
If these factors are present then the condition isrecognised as pseudo-intractability.
Once real intractability is establised theoptions available include
1. New anti–epileptic drugs
2. Epileptic surgery
3. Vagal nerve stimulation
4. Ketogenic diet
5. Other non-pharmacological methods.
New drugs
Since 1990 there has been a vigorousresearch for a new ideal anti-epileptic drug andin the last 10 years more than 10 new drugs havebeen introduced. Of these, four drugs have beenfound to have broad spectrum action, effectiveagainst many types of seizures. This includeslevitiracetam, topiramate, lamotrigene andzonisamide.
Levitiracetam: This drug is very close to idealantiepileptic drug.It is highly effective againstmany types of seizures,with less adverse effectsand has no drug interaction.It can be titratedrapidly and needs no monitoring of laboratorytests.The dose is 5-10mg/kg/day up to amaximum of 60mg/kg/day.
Topiramate: This drug is highly effectiveagainst many types of seizures including variouschildhood epileptic encephalopathies. But it hasa long list of side effects including effects oncognition and behaviour which restricts its useto intractable epilepsies not responding to otherdrugs.The dose is 0.5mg/kg/day to 5-9mg/kg/day.
Lamotrigine: This drug has broad spectrum ofaction in all types except myoclonicseizures.However it needs slow titration needinga long time to build effective dose.It can causeserious skin lesions like Stevens-Johnsonsyndrome especially when started on highdoses.There is significant drug interaction withsodium valproate and carbamazepine. When
given with valproate the starting dose will be0.15 to 0.6mg/kg/day and over two weeksincreased to1-5mg/kg/day. If given alone thedose will be 0.6mg/kg/day to start with, followedby 1-2mg/kg/day to 5-15 mg/kg/day. Whenintroduced it was claimed as the ideal drug forwomen inview of least toratogenicity but the doseneeds to be monitored during pregnancy andlactation.
Zonisamide: This drug has action againstgeneralised seizures, focal seizures and epilepticencephalopathies. However side effect profileincludes anhydrosis, Stevens-Johnson syndrome,nephrolithiasis and effects on cognition. Dosestarts from 1-2mg/kg/day and increased upto4-8mg/kg/day.
Other new drugs, but with narrow spectruminclude ox-carbazepine, tigabin, felbamate,sulthiam, vigabatrin and gabapentine.
Ox-Carbazepine is the first among new drugsto be approved as first choice drug for focalseizures and approved by FDA for use inchildren. However it does not have a high profilein combination therapy due to drug interaction.It has less incidence of skin reactions comparedto its pro drug carbamazepine.
Sulthiam is reemerging as a drug of choice forbenign childhood focal seizures. Its mode ofaction is similar to acetazolamide and its sideeffects are hence similar to acetazolamide-paresthesia, acidosis and hyperventilation.
Felbamate was withdrawn soon afterintroduction due to occurence of aplastic anemiaand liver toxicity. Its present use is cautiouslylimited to severe cases of Lennox-Gastautsyndrome and should be withdrawn after twomonths if there is no response.
Vigabatrine is another drug with limited use dueto unfavourable side effects profile. It causesvisual field defects which may be difficult torecognise in mentally retarded children.Its use is
7

Indian Journal of Practical Pediatrics 2008; 10(3) : 198
restricted to infantile spasms and intractable focalseizures not responding to other drugs.
Tigabine has a narrow spectrum againstintractable focal seizures and spasms of epilepticencephalopathies. It may aggravate absenceseizures.
Gabapentine and pregabaline were found tobe useful in focal seizures but are not promisingand are used more often for relief of neuropathicpain.
Other drugs awaiting completion of clinical trialsinclude ganaxolone and caraberset inphase 3 and valroceramide and telampanel inphase 2 trial stage.
In general, newer drugs are believed to havelesser side effects but long term clinical trialsare needed . The various trials published aremainly aimed at satisfying drug regulatoryauthorities and do not provide useful guidelinesto the clinician. There has been no head to headcomparison among the various new drugs. Theyare expensive. However ox-carbazepine,lamotrigine, topiramate and levitiracetam haveestablished their places as first-line drugs.
However the availability of many drugs hasraised issues like (1) What is the initial drug ofchoice for various types of seizures to choosefrom the long list of drugs available for the sametype of seizures? (2) What is the proper orderof drugs to be tried? (3) How long to try medicaltherapy in focal lesions before surgery?
Epileptic surgery
The advances in neuro-imaging has usheredin a new era of epileptic surgery. Epilepsy surgeryis no longer considered a treatment of last resortand has now become a realistic therapeuticoption. Recent text books on therapy of epilepsydevote almost one third of their books to surgery.It is found to be useful in 5-10% of intractableepilepsies. With increasing experience in adults
it is found to be useful and safe in children.Theearly resort to surgery is indicated in catostrophicepilepsies to achieve early seizure control andimprove quality of life and prevent aggravationof epilepsy through secondary epileptogenesisor the extension of epileptogenic areas.
The evaluation of a child for epilepticsurgery is done in stages. The first step is acomprehensive review of diagnosis and pasttherapy to exclude pseudo-refractoriness assuitable modifications of these can lead to controlof seizures and surgery will not be needed. Thesecond step will be to evaluate for congruenceof data from various tests to see whether there isclinico-electrical correlation and whether thereis a resectable focus in a non-eloquent regionpredicting a possible successful outcome withoutresidual deficits. The recognition of focal originof seizures is made possible by advances in EEGtechniques, advances in neuro-imagingtechniques and the EEG recordings from corticalsurface.
MR spectroscopy, PET studies, SPECTstudies and funtional MRI mapping help torecognise epileptogenic zone on physiologicalbasis even in the absence of anatomical evidenceof structural damage.
These studies have helped to recognise therole of surgery in some refractory forms ofchildhood epilepsies like West syndrome withfocal cortical malformations amenable to surgery.The possible local pathology is suspected inchildren presenting with focal infantile spasms,asymmetrical spasms, presence of partialseizures, hemihypsarrythmia on EEG andpresence of hemiplegia.
Indications for surgery
1.Drug resistant epilepsy: The limitations aredue to variable definitions. There are noguidelines on order of drugs or combinations todefine this entity.
8

2008; 10(3) : 199
2. Surgically resectable epileptic syndromes:These are well defined pathological substrateswith excellent prognosis after surgery. Eg: mesialtemporal sclerosis, structural lesions and corticaldevelopmental abnormalities.
3. Catastrophic epilepsies: These are conditionswith well defined pathological substratesassociated with poor response to medicaltherapy and delay in seizure control leading topoor outcome in relation to quality of life.Examples include Sturge-Weber syndrome,hemimegalencephaly and tuberous sclerosis.
Contra-indications
(1) Primary generalised epilepsies (someforms) and idiopathic focal epilepsies ofchildhood. (2) Epilepsy caused by underlyingprogressive brain disease. (3) Psychiatricdisorders and (4) Severely dysfunctional family.
Types of surgery
(1) Lesionectomy includes removal of focallessions like cortical dysplasias,benign tumoursor focal atrophic lesions. (2.) Resective surgerieslike anterior temporal lobe resection andhemispherectomy. (3) Palliative surgicalprocedures like callosal resections and sub-pialresections for conditions with no focal resectablelesions.
The disadvantages include (a) Too long awaiting period, (b) Lengthy evaluation; at the endof evaluation only 50% may be suitable forsurgery. In one series out of 120 patients referred,only 83 were ultimately found to be suitable forsurgery. (c) There is yet no uniformly acceptedguidelines on order of selection of drugs orduration of medical therapy before consideringsurgical options. (d) Surgery is expensive andonly very few centers perform surgery. In India,Sri Chitra Tirunal Institute at Trivandrum andNIMHANS at Bangalore have done large series.
The overall prognosis depends on thepathology. In general, low grade gliomas have100% relief, followed by 62% relief in corticaldysplasia. “Poor results are seen in patients withfrontal epilepsy, poorly congruent pre operativedata and no definite pathology”.
Recent advances include use of gamma-knife radiosurgery for cavernous angiomas anddeep brain stimulation.
Ketogenic diet
This mode of therapy was introduced75 years ago and despite the availability of manynew drugs still holds a place in treatment ofepilepsy. It is a useful therapeutic alternative tobe considered in difficult cases. This method oftherapy needs an organised set up involving adedicated team and is worthy of trial more widely.The basic principle is to give 80% of calorierequirements through fat and create ketosis. Thebrain utilises the keto-acids thus formed in theKrebs cycle instead of pyruvate derived fromcarbohydrates and the exact mode of action isnot clearly established. The classical ketogenicdiet introduced earlier with 4 to1 ratio of fatswas unpalatable. Modified diets with mediumchain triglycerides and subsequent modifiedMCT diet have been tried of late. Atkin diet withless restrictions has been tried in a pilot study.The main draw back is the inability by the parentsto maintain this schedule due to unpalatibilityand only 35-47% could remain on the diet formore than one year. The response was noted tobe more than 90% reduction in 32% of childrenand about 50% reduction in about in 56% ofchildren. 16% of cases are reported to have fullseizure control. This form of therapy is indicatedin all forms of intractable epilepsy and certainmetabolic disorders like glucose transportdisorders and pyruvate de–carboxylasedeficiency. The results are better in myoclonicseizures and atonic seizures. It is contraindicatedin mitochondrial disorders and fatty oxidation
9

Indian Journal of Practical Pediatrics 2008; 10(3) : 200
disorders. Concomitant use of sodium valproateand carbonic acid inhibitors like sulthiam,topiramate, acetazolamide and zonisamide needsto be avoided. The complications includeconstipation, gastro-esophageal reflux, growthretardation, hyperlipidemia and bonedemineralisation. The exact duration of therapyis not clearly established.
Vagal nerve stimulation
This form of therapy may be tried in patientswho are unfit for surgical procedures. Theprocedure consists of an implanted stimulatorwhich the patient switches on at the onset ofsymptoms with variable frequency. The successrate is reported to be more than 80% reductionin one third, 30-50% reduction in another onethird, and no response in rest of the one third ofpatients. The procedure is very expensive andmay be unsuitable for developing countries. Thecomplications include change in voice, throatpain and cough.
The role of various forms of psycho-therapies are not well establised. They need anorganised set up and may be effective in a veryfew in whom known precipitating factors existor have warning premonitory symtoms. Theseinclude bio-feed back therapy and various formsof relaxation therapy. These help to increase themorale of patients as methods of “self control”.
Thus in summary, about 20-25% of childrenmay have chronic epilepsy causing concern tothe physician and the parents. Early recognitionof this difficult group is important for counselingthe family. The warning signs for intractabilityinclude the following. (a) onset of seizures ininfancy, (b) seizure type - tonic, myoclonic,absence and multiple seizure pattern, (c) organicbrain damage - sequelae of infections, cerebralpalsy and mental retardation, (d) long durationof seizures, (e) bad epileptic syndromes - Westsyndrome, Rasmussen Syndrome, Lennox-Gastaut syndrome.
Points to remember
• 20-25% epilepsies remain intractable notresponding to standard drugs.
• Levitiracetam, topiramate, lamotrigine andzonisamide are the four drugs found tohave broad spectrum anti-epileptic action.
• Surgery for epilepsy is becoming a realistictherapeutic option.
• Ketogenic diet still seems to be a usefultherapeutic alternative for difficult cases.
• Vagal nerve stimulation may be tried inpatients unfit for surgery.
Bibliography
1. Conway JM, Kriel RL, Birnbaum AK.Antiepileptic Drug Therapy in Children.In: Pediatric Neurology: Principles &Practice,Eds, Kenneth F. Swainman, Stephen Ashwal,Donna M. Ferriero, 4
th Edn, Mosby Elsevier,
Oxford, UK, 2006; pp 1105-1130.2. Shinnar S, Dell CO. Treatment Decisions in
childhood Seizures. In: Pediatric Epilepsy-Diagnosis and Therapy, 2
nd Edn, Eds, Pellock
JM, Dodson WE, Bourgeois BFD. Demos,2001; pp 291-300.
3. Medical Treatment. In: Epilepsy in Children,3
rd Edn, Eds, Alexis Arzimanoglou Renzo,
Guerrini Jean Aicardi, Lipincott Williams&Wilkins, Philadelphia, USA 2004; pp 387-396.
4. Patasalos PN, Sander JWAS. Anti epilepticDrugs in Clinical Trials. In: The Treatment ofEpilepsy, 2
nd Edn, Blackwell, UK 2004; pp 568-
576.5. Wheless JW. The Ketogenic Diet. In: Pediatric
Neurology: Principles & Practice, 4th Edn,
Eds, Kenneth F. Swainman, Stephen Ashwal,Donna M. Ferriero, Mosby Elsevier, Oxford,UK 2006;pp. 1131-1150.
6. Panayiotopoulos CP. Principles of therapy inepilepsies: Vagus nerve stimulation. In: TheEpilepsies: Seizures, Syndromes and Manage-ment. Ed, Panayiotopoulos CP, Bladon MedicalPublishing; Oxford, UK 2005; pp 80-86.
10

2008; 10(3) : 201
CONSTIPATION IN CHILDREN
* Bhaskar Raju B** Sumathi B
Abstract: Constipation in children is a commonproblem encountered by the practicingpediatrician and the primary care physicianstaking care of children. Functional constipationis the most common cause of inadequateevacuation. History, clinical examination and arectal examination are adequate for diagnosisof functional constipation. However, organiccauses will have to be sought for and ruled out ifthe presentation is atypical or therapy fails toelicit the desired response. Treatment offunctional constipation consists of laxatives,dietary modification and bowel training.
Key words: Functional habitual constipationchildren management.
Introduction
Constipation is a common problem intoddlers and preschool children. Constipationseen in childhood is usually functional in97% of children, with equal frequency in boysand girls.1 In older children, situations that makedefecation uncomfortable or inconvenient suchas unpleasant toilet facilities at school or perianalpain results in infrequent bowel emptying. Thepresence of red flag signs may indicateuncommon but serious organic causes of
constipation, such as Hirschsprung’s disease,pseudo-obstruction, spinal cord abnormality,hypothyroidism, congenital anorectal malforma-tions, and rare conditions like diabetes insipidus,cystic fibrosis, gluten enteropathy.2 A changefrom human milk to cow’s milk or cow’s milk orsoya based formula may lead to firmer stools andhence painful defecation in an infant.
Definition
Constipation has been defined as “delay ordifficulty in defecation, present for two or moreweeks, sufficient to cause significant distress tothe patient”.3 It is also defined by the occurrenceof any of the following characteristics,independent of stool frequency: passage of hard,scybalous, pebble like, or cylindrical crackedstools; straining or painful defecation; passageof large stools that may clog the toilet; or stoolfrequency less than 3 per week except in breastfed infants.4
Epidemiology
Worldwide 0.3% to 28% of children areconstipated.5 Van den Berg gives 0.7% to 29.6%as values for prevalence of constipation inchildren.6 Up to a third of children aged six to12 years report constipation during any givenyear.7 25% of the pediatric gastroenterologyconsultations are constipation referred for furtherevaluation.8
Causes of constipation
Functional constipation is the most commoncause of constipation. However one has to lookfor congenital anorectal malformations,
IAP-IJPP CME 2008
* Professor,
** Asst. Professor,
Pediatric Gastro Enterology,Institute of Child Health and Hospital forChildren, Chennai, Tamil Nadu.
11

Indian Journal of Practical Pediatrics 2008; 10(3) : 202
underlying neurological, endocrine and metaboliccauses besides some miscellaneous ones(Table 1).
Pathogenesis of functionalconstipation
Several mechanisms have been associatedwith constipation. Idiopathic / functionalconstipation often starts as a painful bowelmovement due to any reason which makes thechild withhold stools in fear of pain next time itmoves its bowels. This becomes a vicious cyclesince withholding stools makes the stool evenharder and more painful to push out next time.This results in incomplete evacuation and chronicconstipation. Other factors like genetic, dietaryhabits especially low intake of fibre in the dietand disturbances of intestinal motility may playa role in causation and perpetuation of functionalconstipation.9, 10 The presence of methane inbreath would suggest disturbed motility andconsequent prolonged colonic transit time inchildren with chronic constipation.11 In functionalconstipation the child responds to the urge todefecate by voluntarily contracting the external
anal sphincter and gluteal muscles to withholdstool and avoid pain of defecation. Child oftenadopts various postures including standing withlegs crossed, and straining to hold stool-referredto as ‘fecal withholding’, or ‘functional fecalretention’.12 In due course this will lead toinhibition of reflex defecation and reduced rectalmovement and the rectum will be filled with hardstool and fecal soiling follows (Fig. 1). One thirdof children with functional constipation willpresent with encopresis. This leads to frustration,decreased self-esteem, depression, loss of copingskills, anxiety and other affective disturbances.13
History and clinical examination
Each child should undergo a detailed history,a thorough physical examination including digitalrectal examination to identify presence of stoolat anal verge, assess rectal tone and determinethe presence of rectal distention or impaction.7
Delayed passage of meconium may suggesthypothyroid or Hirschsprung’s disease. Fever,abdominal distension, anorexia, nausea,vomiting, weight loss or poor weight gain couldbe signs of an organic disorder (Red flag signs).
Table 1. Causes of constipation
S. No. Causes Conditions
1. Idiopathic Functional (95%-97%)
2. Anal lesions and congenital Anal fissure, anteriorly placed anus, anal stenosisanorectal malformations
3. Neurological disorders Hirschsprung’s disease, spinal cord abnormalities:myelomeningocele, spina bifida, cerebral palsy, tetheredcord
4. Endocrine/metabolic Hypothyroidism, hypercalcemia, hypokalemia, diabetesinsipidus, diabetes mellitus
5. Drugs Anticonvulsants, heavy-metal (lead) poisoning, anti-diarrhoeals, antipsychotic agents.
6. Miscellaneous Prune Belly syndrome, Down’s, Cystic fibrosis, Cow milkprotein allergy, connective tissue disorders, tumors
12

2008; 10(3) : 203
Fig.1. Mechanism of encopresis
Table 2. Comparison of functional fecal retention and Hirschsprung’s disease
Symptom Functional fecal retention Hirschsprung disease
Delayed meconium passage Rarely 60%
Constipation as newborn Rarely Almost always
Failure to thrive Uncommon Possible
Enterocolitis None Possible
Onset after age 2 years Common Sometimes
Abdominal distension Rare Common
Fecal incontinence Common Almost never
Difficult bowel training Common Rare
Avoidance of toilet Common Rare
Withholding behavior Common Rare
Stool in rectal ampulla Common Rare
Fissure Common Rare
Obstructive symptoms Rare Common
Transition zone in barium enema Absent Present
Aganglionosis on biopsy Absent Present
13

Indian Journal of Practical Pediatrics 2008; 10(3) : 204
Bloody diarrhea in an infant with a history ofconstipation could be an indication ofenterocolitis complicating Hirschsprung’sdisease. Presence of stool in the rectum onPerrectal examination confirms the diagnosis offunctional constipation and generally needs nofurther confirmatory imaging studies. Thepresence of anal fissures is suggestive offunctional constipation. Table 2 gives theessential differences between functionalconstipation and constipation due toHirschsprung’s disease. Physical examinationshould include neurological examination andassessment of abdominal, cremasteric and lowerextremity deep tendon reflexes, as well as thepresence of anal wink (the contraction of the anuswhen stroked). Abnormal physical findingssuggesting organic causes like failure to thrive,lack of lumbo-sacral curve, sacral agenesis,anteriorly placed anus and features ofhypothyroidism should be looked for.
Classic presentation
Children who have functional constipationoften present from pre-school to elementaryschool age with a history of infrequent stool,prolonged defecation, abnormal posturing,painful act of defecation and withholding of stool.Children who are older than 3 years of age mostfrequently present with soiling, impaction, andwithholding.14
Laboratory tests
Since functional constipation is the mostcommon cause and only 5% of children haveorganic etiology, special diagnostic tests arerarely needed.15 If a rectal examination is notpossible, plain x-ray abdomen may be considered.Loaded rectum in a plain radiograph of abdomenis highly predictive of fecal impaction on digitalrectal examination. A barium enema in anunprepared colon will demonstrate a transition
zone in a case of Hirschsprung’s disease and alsouseful when other anatomic abnormalities suchas a colonic or rectal stricture is suspected.15
In the child with infrequent bowel movementsand no other signs of constipation, colonic transittime can be evaluated with radio-opaque markers.Presence of the markers throughout the colonindicate pancolonic delay.16 Assessment ofsegmental colonic transit time using radio opaquemarkers may be indicated for children withneurologic disorders, such as myelomeningoceleor cerebral palsy.17 Anal manometry is useful inHirschsprung’s disease. 30% of childhoodconstipation is associated with urinary infectionand a urine culture may be useful when indicated.
Management
Constipation due to functional etiology (alsoreferred to as habitual constipation) is the mostcommon type seen in clinical practice. Treatmentconsist of stool disimpaction, prevention offurther stool retention, promotion of regularbowel habit, dietary advice, psychosocial supportand close follow up.18
Disimpaction
Whenever child has palpable fecal mass inthe abdomen, loaded rectum identified by thedigital examination or rarely on plain x-rayabdomen, disimpaction is indicated. This can bedone by oral or by rectal route. Usually oraladministration of medication (oral enema!) isbetter than the rectal route as this is non-invasiveand is not associated with discomfort or pain.Rectal administration of drug usually causesdiscomfort to children, making stool retentionworse. Polyethelene glycol (PEG) orally is idealfor oral disimpaction.19 The dose is 20ml/kg/hourfor four hours and can be repeated the next dayif necessary. Such lavaging can be done orally orby nasogastric tube (25ml/kg/hour). Single doseof prokinetic agent namely 5 to 10 mg ofmetaclopramide may be given half an hour
14

2008; 10(3) : 205
before lavaging. Phosphate enema, glycerinesuppositories may be used rectally.
Maintenance therapy
Once the impacted feces is dislodged andevacuated, treatment of constipation should aimto prevent fecal re-impaction by maintenancetherapy with laxatives (Table 3), dietarymodifications, bowel training and close follow-up. In general the dosage of drugs used would
depend on the response seen and will need to bemodified constantly based upon the nature of thestool it results in.
Dietary modification
Children with functional constipationshould be encouraged to consume diet rich infibre. The recommended amount of daily dietaryfibre for all children is equal to 5 g plus the child’sage in years.20 Fruits like apple, pear and prune
Table 3. Laxatives
S. No Drug Dosage Side effects
1 Lactulose 1-3ml/kg/day, 1-2 doses. Abdominal cramps, flatulanceAdjust dosage to response seen
2 Milk of magnesia 1-3ml/kg/day,1-2 doses Over dose-hypermagnesemia,Adjust dose to response seen hypophosphatemia,
hypocalcemia
3 Sorbitol 1-3ml/kg/day,1-2 doses Abdominal cramps, flatulance
4 Mineral oil Disimpaction 15-30ml/year Lipoid pneumonia(Liquid Paraffin) of age.(max 240ml)
Maintenance- 1-3 ml/kg/day
5 PEG (Poly Disimpaction-25ml/kg/hour Nausea, bloating, cramps,Ethylene Glycol) Maintenance-5-10ml/kg/day vomiting, anal irritation.
or 0.5-1g/kg/day
6 Senna syrup: 8.8 g sennoside/ 5 ml Idiosyncratic hepatitis,2–5 years: 2.5–7.5 ml/day melanosis coli, hypertrophicin two divided dosages. osteoarthropathy, analgesic6–12 years 5–15 ml/day nephropathy, abdominalin two divided dosages cramping. Melanosis coli(Tablets and granules available) improves after medication
stopped
7 Bisacodyl 5 mg tablets, 1–3 tablets/dosage Abdominal cramping,1–2 times daily. diarrhea, hypokalemia10 mg suppositories,0.5–1 suppository, 1–2 times daily
15

Indian Journal of Practical Pediatrics 2008; 10(3) : 206
juices that contain nonabsorbable carbohydrateslike sorbitol are helpful. Fluid intake should beencouraged. The diet should contain wholegrains, fresh fruits and vegetables rich in fiber.
Toilet training
This is possible after 2 to 3 years of age.Child should be encouraged to sit in the toiletfor 5 to 10 minutes, 3 to 4 times per dayimmediately after meals for initial few months,regularly. The gastrocolic reflex that occurs aftermeals can be made use of, to ease the bowelmovement. Child should be rewarded wheneverthere is no fecal soiling. This will act as a positivereinforcement and provide psychological supportto these children. Re-education is an importantpart of bowel training. Child should be advisednot to strain excessively and never to ignore/suppress the urge to defecate.
Outcome: In studies on functional constipation,recovery is defined as greater than three stoolsper week with no soiling. However the responsedepends on age of onset and associatedencopresis. Approximately two third of cases offunctional constipation need laxative therapy formonths to years and the rest require even longerterm treatment. Significant number may continueto have constipation into adulthood. In one study,52 percent of children with constipation andencopresis, the symptoms persisted even afterfive years of treatment.21 Clayden has shown that22% of children required laxatives for less than6 months, 44%for less than 12months, and therest for more than 12 months.22
Follow up
The successful management of functionalconstipation in childhood depends on closefollow-up, till normal bowel movement isachieved, followed by review every two to threemonths for the next 2 years and then yearlythereafter.
Points to Remember
• Functional constipation is the mostcommon cause of constipation in children.
• Good history and thorough physicalexamination including per rectal (PR) areall that is needed for a diagnosis offunctional constipation.
• Laxative therapy is usually needed forseveral months.
• Early withdrawal of therapy leads torelapse.
• Effective treatment depends on (a) childand family education, (b) adequatedisimpaction (c) maintenance phase whichincludes behavioral therapy, medicationand dietary modification.
References
1. Baucke VL. Prevalence, symptoms andoutcome of constipation in infants and Toddlers,J Pediatr 2005;146:359-363.
2. Wendy S, Biggs, Dery WH. Evaluation andTreatment of Constipation in Infants andChildren, Am Fam Physician 2006;73:469-477.
3. Baker SS, Liptak GS, Colletti RB, et al.Constipation in infants and children: evaluationand treatment. A medical position statement ofthe North American Society for PediatricGastroenterology and Nutrition. [erratumappears in J Pediatr Gastroenterol Nutr 2000Jan;30(1):109]. J Pediatr Gastroenterol Nutr1999; 29 : 612-626.
4. Hyams J, Colletti RB, Faure C, et al. Functionalgastrointestinal disorders, J Pediatr Gastro-enterol Nutr 2002;35 (suppl):110-117.
5. Benninga MA, Voskuijl WP, Taminiau JA.Childhood constipation: is there new light inthe tunnel? J Pediatr Gastroenterol Nutr 2004;39 : 448-464.
16

2008; 10(3) : 207
6. Van den Berg, Maartje M, Benninga, et al.Epidemiology of Childhood Constipation:A Systematic Review. Am J Gastroenterol.October 2006, 101(10): 2401-2409.
7. Felt B, Brown P, Coran A, et al. Functionalconstipation and soiling in children. Universityof Michigan Health System guidelines forclini-cal care 2003. Accessed online February2, 2005
8. Taitz LS, Wales JK, Urwin OM, et al. Factorsassociated with outcome in management ofdefecation disorders, Arch Dis Child1986;61(5):472-477.
9. Morais MB, Vitolo MR, Aguirre ANC, et al.Measurement of low dietary fibre intake as arisk factor for chronic constipation in children,J Pediatr Gastroenterol Nutr. 1999;29: 132-135.
10. Di Lorenzo C, Pediatric anorectal disorders,Gastroenterol Clin North Am.2001;30:269-287.
11. Ana Christina FS, Henrique ML, Ulysses FN,et al. Breath methane associated with slowcolonic transit time in children with chronicconstipation, J Clin Gastroenterol.volume 2,Oct-Dec 2005; 241-244.
12. D.C. A.Candy, D. Edwards. The managementof chronic constipation, Current Paediatrics,2003; 13,101-106.
13. Childhood constipation: Finally some hard dataabout hard stool. J Pediatr 2000; 136:4-7.
14. Partin JC, Hamill SK, Fischel JE, et al. Painfuldefecation and fecal soiling in children.Pediatrics 1992;89(6 Pt 1):1007-1009.
15. Joseph M. Croffie Constipation In Children,Indian J Pediatr 2006;73:697-701.
16. Padopoulou A, Clayden G S, Booth I W. Theclinical value of solid marker transit studies inchildhood constipation and soiling. Eur J Pediatr1994; 153: 560–564.
17. Youssef NN, Di Lorenzo C. Childhoodconstipation: evaluation and treatment. J ClinGastroenterol 2001;33(3):199-205.
18. Clinical Practice Guideline, Evaluation andTreatment of Constipation in Infants andChildren: Recommendations of the NorthAmerican Society for PediatricGastroenterology, Hepatology and Nutrition, JPediatr Gastroenterol Nutr 2006;43: e1-e3.
19. Vincent R, Candy DCA. Movicol for thetreatment of faecal impaction in children – anaudit of the first thirty patients.Gastroenterology Today 2001; 11: 50–52.
20. Position of the American Dietetic Association.Health implications of dietary fiber. J Am DietAssoc 1997;97(10):1157-1159.
21. Staiano A, Andreotti MR, Greco L, et al. Long-term follow-up of children with chronicidiopathic constipation. Dig Dis Sci 1994;39:561-564.
22. Clayden GS. Management of chronicconstipation. Arch Dis Child 1992;67:340-344.
17
JHARKHAND PEDICON 2008, DHANBAD
November 22-23, 2008
Contact
Dr.B.B.Sahni
President, IAP Jharkhand State and
Sr.Specialist, Department of Pediatrics,
Tata Central Hospital,Dhanbad-828 301, India.
Res:0326-2320769, 6612229, Office:03266612285, Mobile:09334015806
Email:[email protected]
NEWS AND NOTES

Indian Journal of Practical Pediatrics 2008; 10(3) : 208
HOW DO I MANAGE ATOPIC
DERMATITIS?
* Jayakar Thomas
Abstract: Management of atopic dermatitis(AD) should always commence with a globalassessment of the disease in terms of severity,psychological well-being and checkingadherence to optimal therapy. Counseling andeducation should include stepwise approachto management and demonstration on how touse medications, how to recognise a flare andexplanation of benefits and harms oftreatment. Emollients are applied all the timeand with all treatments. One must offer choiceof products, prescribe large quantities (morethan 250g per week), to be applied liberallyand frequently and after bathing. Topicalcorticosteroids (TCS) of lowest potencycapable of controlling symptoms are to beused. They are to be applied to areas of activeAD only. One uses mild TCS to prevent flares.Mild potency only is used on face and neckand thin skin, once or twice daily. One canconsider short course (7-10days) of potentTCS to control symptoms. Never use a)Potenton children under 12 months b)Very potent onchildren under 12 years c)On face, axilla orgroin.
Topical calcineurin inhibitors (TCI) are not firstline therapy on the body (limbs and trunk).Tacrolimus is used for moderate/ severe eczemain children more than 2 years if uncontrolled by
TCS. Pimecrolimus is reserved for moderateeczema in children more than 2 years ifuncontrolled by TCS. Never use TCIs: a)Underocclusion b)For eczema requiring long term use.Systemic treatment and phototherapy are forspecialist only as last resort.
Key words: Atopic Dermatitis, Management,TCSs, TCIs.
Atopic dermatitis (AD) is a commoncondition that affects more than one in tenchildren and the incidence is increasing. Thereare probably several reasons for this, includinghigher exposure to air pollution, smaller familieswith less exposure to infections, more pets, highermaternal age, a wider range of foods and thepractice of evidence-based medicine. There isclearly also an important hereditary componentto atopic eczema. This is complex because notall affected children are atopic, though the genesimplicated in atopy are likely to be involved,together with others as yet unknown. AD usuallypresents during the first year of life and when itis severe it is extremely disabling. It may alsocause major psychological problems.
Diagnosis
There is no gold standard laboratory test fordiagnosis of AD. Several criteria have beensuggested, as follows:
• Hanifin and Rajka
• Schultz-Larsen
• Danish Allergy Research Centre(DARC)
• Jan Bos’ millennium
• Doctor-based clinical diagnosis
* Senior Consultant Dermatologist,Kanchi Kamakoti CHILDS Trust Hospital,Chennai, INDIA
IAP-IJPP CME 2008
18

2008; 10(3) : 209
Clinical diagnosis only is reliable andconsists of.
• Severe pruritus
• Classical morphology
• Typical distribution
• Positive family history
It is also observed that the first eczema,during the first year, in the first born, is usuallyatopic dermatitis.
Management1,2,3
Explanation and counseling are a vital partof the successful management of atopicdermatitis. Parents would have received a barrageof advice from a range of medical, paramedicaland non-medical “experts” and require a clearunderstanding of the nature of the condition, along term management plan and a realisticexpectation of the results of treatment.Terminology is often confusing; the terms atopiceczema and atopic dermatitis are often usedsynonymously. It is essential to talk in terms ofcontrol rather than cure, otherwise parents willsearch for an end point after which care will nolonger be required and this is an unrealisticexpectation. The condition should be explainedas a multifactorial disorder and it must beappreciated that just as there is no “cure” thereis no single “cause.” Often no explanation canbe found for a particular flare up of the condition,and many factors are probably working incombination at all times.
Dealing with xerosis
Bath oils and products containing oatmealare useful and prevent the drying of the skin thatbathing can induce. Bath oils that containantiseptic may have added benefit in certain casesbut have a tendency to over-dry and sometimesactually irritate the skin. The child should haveeither a bath with additive or a short shower. It is
essential to find a suitable moisturizer that canbe applied all over twice a day whether or notthere is active eczema. Creams containingmoisturizing agents, emulsifying ointment andcreams or ointments with lanolin can be used.If a product stings the skin it must be abandoned.The most likely irritant in emollient creams is thestabilizer propylene glycol. Products that containurea almost always sting broken skin and areunsuitable in these children.
Use of wet dressings
Wet dressings are useful in children withsevere widespread eczema. This is essentially aninpatient procedure but can be used for shortperiods at home. A water based emollient isapplied all over; a corticosteroid cream (ratherthan ointment in this case because cream is morewater miscible) is applied to the areas of activeeczema. The creams are covered with a doublelayer of wrapping, the innermost of which iswetted with tepid water. The material may becotton sheeting covered with a crepe bandage,though an easier alternative is the use of adouble layer of tubular elasticized bandage.The procedure is repeated three times a day.This treatment is usually effective in clearing theeczema in three or four days.
Avoidance of allergens
House dust mite is the most importantallergen. Avoidance measures have to be carriedout assiduously and must include encasing themattress and pillows as well as dealing with thetop covers, either by encasement or by hot (morethan 60°C) washing. If food allergy is suspected,the child should be referred to a pediatricdietician. In general, it is children with severeatopic eczema who have food allergy or foodintolerance. Children with flexural eczema areunlikely to have food allergy, unless the historysuggests otherwise.
19

Indian Journal of Practical Pediatrics 2008; 10(3) : 210
Topical corticosteroids
It is often necessary to spend some timecounseling the parents that topical steroidpreparations used appropriately are safe. Thestrength chosen depends on the severity of theeczema and the site affected. The frequency ofapplication depends on the individual product.
Class I1.Clobetasol diproprionate 0.05%,2.Halbetasol proprionate 0.05%,3.Diflorasone diacetate 0.05%
Class II1. Fluocinonide 0.05%,2. Halcinonide 0.05%,3.Amcinonide 0.05%
Class III1. Mometasone furoate 0.1%,2.Betamethasone diproprionate 0.05%
Class IV1. Fluocinolone acetonide 0.01-0.2%,2. Hydrocortisone valerate 0.2%3. Hydrocortisone butyrate 0.1%
Class V1. Triamcinalone acetonide 0.1%,2. Fluticasone propionate 0.05%,3. Desonide 0.05%
Class VI1. Prednicarbate 0.05%,2. Triamcinalone acetonide 0.025%
Class VII1. Hydrocortisone 2.5%,2.Hydrocortisone 1%
Topical antibacterials
Staphylococcus aureus is commonlycultured from eczematous skin and there may beobvious signs of infection. For localizedinfections, mupirocin, sisomycin and fusidic acid
ointment may be effective. To prevent infectionsit is useful to bathe the child in preparationscontaining triclosan or benzalkonium chloride.
Topical immunosuppressant
Tacrolimus is a potent immunosuppressivedrug used in organ transplantation. A topicalformulation has been shown to be effective intrials in patients with moderate to severe atopicdermatitis. Studies specifically related tochildhood eczema have confirmed its efficacy.The main side effect is a sensation of burning.A concern has been raised as to whetherapplication to skin exposed to sun could increasethe long term risk of skin cancer. Pimecrolimus(an ascomycin derivative) is a newer immuno-suppressive agent, similar to tacrolimus. Studiesin children are very encouraging. The approvalof topical calcineurin inhibitors for the treatmentof AD represents a significant advance inour management options for this disease.The distinction between pimecrolimus andtacrolimus is that the former is a cream while thelatter is an ointment. Tacrolimus is currentlymarketed as an ointment that is more potent butalso more irritating. Importantly, there aresituations in which topical calcineurin inhibitorsmay be advantageous over topical corticosteroidsand may be useful as first-line therapy. Thesewould include treatment of patients who arepoorly responsive to topical steroids or havesteroid phobia and treatment of face and neckdermatitis where ineffective, low-potency topicalcorticosteroids are usually used due to fears ofsteroid-induced skin atrophy. The potential useof topical calcineurin inhibitors as maintenancetherapy is also intriguing for prevention of ADflares and progression of the atopic march.However, although systemic absorption of thesecompounds is low, there is a need for carefulsurveillance to rule out the possibility that skincancers and increased viral skin infections willappear when such agents are used long-term.
20

2008; 10(3) : 211
Never use TCIs:
• Under occlusion
• For eczema requiring long term use
Oral medications
Immunosuppressive drugs : Severe atopiceczema is a serious condition, with huge loss ofquality of life for the child on par with juvenilerheumatoid arthritis. It is therefore essential thatsuch children are treated adequately. The use oforal steroids should be avoided because of severerebound of the eczema on withdrawal, the eczemabecoming unstable after several courses and thelong term side effects. There are generally twoalternatives for severe eczema, cyclosporin andazathioprine.
Cyclosporin: Recent studies have confirmed theefficacy of cyclosporin in childhood atopiceczema. Regrettably the improvement is often notmaintained after withdrawal of the drug.Continuous treatment is rarely justified in viewof the long term risks (such as hypertension andrenal dysfunction). However, it has a place as aneffective, safe and well tolerated short term optionfor the management of severe refractory diseasein children.
Azathioprine is a safer drug for long termuse, though it does have several side effects,including nausea, fatigue, myalgia and liverdysfunction. It is essential to assay for thiopurinemethyl transferase before treatment starts aschildren deficient in this enzyme will experiencemarked bone marrow suppression. In mostchildren it is effective at low dosage. The mainlong term side effect that could theoretically occur(as with cyclosporin) is the development oflymphoma. The advantage of this drug is that itcan be used continuously. Other possibilitiesinclude the leukotriene inhibitors zafirlukast andmontelukast given orally. Chinese herbalmedicines have also been used successfully butare not without danger.
Antihistamines : Sedating antihistamines suchas promethazine given at bedtime are useful.The sedation is an important feature of theirantipruritic action. It is still debatable whethernon-sedating antihistamines such as cetirizine andloratadine are useful because generally the roleof histamine in eczema is somewhat limited.However, a large study of the use of cetirizine inadults with atopic eczema showed a significantreduction of clinical manifestations in thosetreated.
21
Treatment may be summarized as follows :
MILD MODERATE SEVERE
1. Bathing and moisturization 1. Bathing and moisturization 1. Bathing and moisturization
2. Avoidance of trigger factors 2. Avoidance of trigger factors 2. Avoidance of trigger factors
3. Treat superinfection 3. Treat superinfection 3. Treat superinfection
4. Intermittent short-term use 4. Intermittent short-term use 4. Intermittent short-term useof Class VI to VII topical of Class IV to V topical of Class II to III topicalsteroids + TCI steroids + TCI steroids + TCI
5. Oral antihistaminics 5. Oral antihistaminics
6. Consider oral rescuemedication / UVB therapy

Indian Journal of Practical Pediatrics 2008; 10(3) : 212
NEWS AND NOTES
IAP Drug Formulary
IAP Drug Formulary Web-Update 2008 (1) - Edition 10
The ninth web update of the IAP Drug Formulary, the first for 2008, is now available fordownload. These updates are being made available, free of cost, to all our esteemed users as IAPExecutive Board considers this as a service to pediatric care in our country. This quarterly webpublication of the IAP is possibly the first drug formulary in the world that provides such afacility. Users should to regularly update their formulary through the formulary installed in theircomputers as and when they receive the newsletter announcing the availability of an update
The Formulary contains information, which, to the best of our knowledge, is accurate andup-to-date. But every practitioner must, as we have always insisted, take individual responsibilityfor taking all precautions when dispensing and administering drugs to children. We are lookingforward to comments and criticism regarding the update. Useful and meaningful quarterly updateswill continue to be made available so that this ongoing publication of IAP meets internationalstandards and continues to be sought after by all those caring for children and adolescents.
Those who have not yet bought the formulary could do so by sending a DD in favour of‘IAP, Mumbai’ for Rs 350 (three hundred and fifty only) to the IAP office.
Dr Jeeson C Unni MD, DCH, FIAP
Editor-in-Chief, IAP Drug Formulary
Consultant pediatrician, Dr Kunhalu’s Nursing Home, T D Road, Cochin – 682011
Points to Remember
• Atopic dermatitis in children is a complexcondition .
• Four in five children with atopic eczemahave IgE mediated allergy to inhalants orfoods.
• House dust mite and mosquitoesexacerbates atopic dermatitis .
• Food allergy exacerbates eczema in lessthan one in ten children.
• To reduce the need for admission to hospitalchildren with severe eczema can be treatedwith topical or oral immuno-suppression.
Bibliography
1. Thomas Jayakar. Understanding Atopicdermatitis and its management in Children.Pediatric Oncall [serial online] 2008;5.Available from: http://www.pediatriconcall.com/fordoctor /d iseasesandcondi t ion/pediatric_dermatology/atopicdermatitis.asp
2. Thomas Jayakar. Common DermatologicalProblems in Adolescents. In: Bhave SY. Editor.Textbook of Adolescent Medicine. 1
st Edn.
New Delhi: Jaypee Brothers; 2006. pp.554-576.
3. Thomas Jayakar. Atopic Dermatitis. In: ThomasJ. edit. Pediatric Dermatology Ward Rounds.1
st Edn. New Delhi: Jaypee Brothers, 2007;
pp.17-19.
22

2008; 10(3) : 213
IAP-IJPP CME 2008
SURFACTANT THERAPY
* Lakshmi V
Abstract: The incidence of respiratory distresssyndrome increases with lower gestational ageand surfactant is the standard of care in themanagement of Respiratory distress syndrome(RDS).
Large number of trials have come in surfactanttherapy and many of them are still ongoing.Surfactant acts by lowering the alveolar surfacetension thus preventing their end expiratorycollapse and establishing functional residualvolume (FRV). Prophylactic surfactants arebeing given for <30 weeks gestation and theyare quickly extubated to Nasal CPAP. Naturalsurfactants in adequate dose has improved themorbidity and mortality. Babies requiringsurfactant and ventilation are monitored andweaned rapidly once the complianceimproves.Surfactant also has proved to beeffective in meconium aspiration babies whohave secondary surfactant deficiency.
Key words: Preterm, RDS, Surfactant.
Respiratory distress syndrome (RDS) is themajor cause of morbidity and mortality in pretermbabies.1 The incidence of RDS is inverselyproportional to the gestational age occurring in15-30% of babies between 32-36 weeks, 50% ofthe babies born before 30 weeks of gestation and60-80% of babies of less than 28 weeks ofgestation.2 Surfactant therapy has become thestandard of care in the management of RDS in
preterm babies. Surfactant is also used in themanagement of secondary surfactant deficiencystates like meconium aspiration, pulmonaryedema, congenital pneumonia and ARDS.
Avery and Mead in the year 1959 were thefirst to demonstrate that surfactant was deficientin the lungs of babies dying due to Hyalinemembrane disease (HMD). AerosolizedDipalmitoyl Phosphatidyl Choline (DPPC) triedin 1964 by Robillard and 1967 by Chuetal wereunsuccessful. Fujiwara reported the first clinicalstudy of intratracheal surfactant in1980. In 1989commercial surfactant preparations wereapproved by FDA in USA.
Composition of surfactant
The mammalian surfactant contains80% phospholipids, 8% neutral lipids and12% proteins.
The phospholipid pool consists ofdipalmitoyl phosphatidyl choline 60%,unsaturated phosphatidyl choline (PC) 25%,phosphatidyl glycerol(PG) 15% along with traceamounts of phosphatidyl inositol, phosphatidylethanolamine, phosphatidyl serine, sphingo-myelins and neutral lipids like cholesterol. DPPCalone is primarily responsible for the functionbut is poorly adsorbable through the air liquidinterface and is facilitated by the surfactantproteins and other lipids like phosphatidylglycerol.
About half of the protein content is thecontaminating plasma and lung tissue and the restare surfactant associated apopoteins Sp A, B, Cand D (Table 1).
* Consultant Neonatologist,Mehta Children’s Hospital, Chennai.
23

Indian Journal of Practical Pediatrics 2008; 10(3) : 214
Table 1. Surfactant apo proteins
SPA 36000kDa, water soluble Regulates surfactant metabolism, formation of tubular Chromosome6 myelin, participate in host defense and phagocytosis
SPB 8000kDa, hydrophobic Surface lowering property helps in absorptionChromosome2
SPC 3800kDa, hydrophobic Lines the airway in developing lung. helps in absorption
SPD 43000kDa, hydrophilic Host defense
Synthesis and secretion
Surfactant is identified as early as 16 weeksin the fetal lung though its proper secretion beginsafter 24 weeks of gestation and more abundantlyafter the 35th week of gestation. Surfactants arephospolipids synthesized and recycled by type IIpneumocytes which form the air liquid interface.Proteins are synthesized on the roughendoplasmic reticulum and lipids in theendoplasmic reticulum and golgi bodies.The lipidcontent is stored in the membrane boundorganelles called the lamellar bodies.The contents are secreted through the apices ofthe type II cells into the extracellular aqueouslining of the alveoli by exocytosis .Here theyunravel into tubular myelin which is a lipidbilayer membrane and also is the extracellularreservoir for DPPC monolayer at the air liquidinterphase (Fig.1).
The surfactant pool size varies with thegestational age. In a term baby the amniotic fluidcontains 100mg/kg of surfactant.3 The pool sizein a preterm baby is low and in a preterm babywith RDS have 2-10mg/kg. Half-life of surfactantis 30 hours. Exogenous surfactant increasesalveolar and tissue pools. In babies with RDSthere is a steady increase in phospatidyl cholinelevels to normal by 4-5 days.
Ninety percent of the DPPC is taken backby type II cells and recycled. 10% is degradedby alveolar macrophages.
Fig.1. Surfactant production from typeII pneumocytes and secretion intoalveolar surface
24
Surfactant synthesis is reduced in thefollowing conditions: Birth asphyxia, hypoxia,caesarian section, acidosis, diabetic mothers,hypotension, cold stress .
Accelerated production is observed withhormones like, catecholamines, glucocorticoids,thyroid hormone and fetal stress like intra uterinegrowth retardation, preterm, prelabour rupture ofmembranes.
Surfactant is released into the alveoli as soonas the lungs are distended with the first fewbreaths and surfactant synthesis and the releaseis enhanced by antenatal steroids.4

2008; 10(3) : 215
Reduced release and function are seen whenthere is meconium, blood, fluid in the alveoli.
Surfactant functions
Surfactant molecules once released spreadto line the alveolar surface. These molecules arepushed together during expiration and lower thesurface tension, which prevents alveolar collapsethus maintaining the residual volume andimproving the lung compliance. As a result thelung can expand and oxygenate well and the workof breathing is less.It also plays a role in hostdefence mechanisms against infections.
Deficiency of surfactant results in collapseof alveoli during expiration leading to difficultyin re-expansion with the next breath. Thus theinspiratory pressure to open the alveoli arefurther increased and FRC is not established orlow.The compliance decreases. As a result, thework of breathing is more with chest wallretractions and grunt where endogenous PEEPis produced to keep the alveoli open.V/Q mismatch ensues and eventually respiratoryfailure sets in.
Timing
Instillation of surfactant prior to the firstbreath has the better outcome5,6 as the spread ishomogenous in fluid filled lungs.
1. Prophylactic treatment when started forbabies more than 30 weeks, it was found to bebeneficial and hence preferred over rescue7,8. Butit also leads to unnecessry treatment in 30% ofbabies who maynot require it9,10.
2. Early rescue given to preterm babies withrespiratory distress within 2 hours of age.
3. Late rescue in those with established RDSafter 2 hours of life.
Early rescue has better outcome in terms ofmortality and airleaks and CLD than latetreatment.11
Instillation and procedure
Surfactant is instilled directly into the lungsthrough the endotracheal tube under strict asepticconditions.Once intubated a smaller size (5 Fr)nasogastric tube cut short to the length of ETTis introduced through the ETT after disconnectingthe ventilator or through a side port adaptor or adual lumen ETT (Fig.2). The desired dose isloaded into a sterile syringe given as a bolus over15 mts in 2-4 aliquots.Changing the position ofthe baby than given in supine position had noeffect on the outcome and the spread is moreuniform in supine position.12 The baby may beconnected back to the ventilator or hand baggedfor a few minutes. Precautions to be taken are tokeep the endotracheal tube in position and patentprior to instillation. Adverse events reported werereflux of solution in the tube, apnoea,bradycardia, hypotension and desaturation whichimproves with positive pressure ventilation.Hence it is imperative to monitor these
25
Fig. 2. Surfactant being instilledthrough a NG tube into the endotra-cheal tube

Indian Journal of Practical Pediatrics 2008; 10(3) : 216
parameters during the procedure (Table 2). AvoidETT suctioning for atleast 2-4 hours unlessdeemed necessary.
Following surfactant there is a rapidimprovement in oxygenation and followed byslow improvement in compliance. Hence FiO
2,
PIP and ventilator rate should be appropriatelyweaned. Chest expansion, Blood gases, Chestx-ray and pulmonary graphics are useful guideto improvement in oxygenation and compliance.If ventilation is not adjusted appropriatelyalveolar over distention and hyperventilation leadto air leaks.
Types of surfactant
Natural surfactants: Animal derived by eitherlung mince extract or by lung lavage extract.It has phospolipids and surfactant proteins.
Synthetic surfactant: Onlyphospolipids.
Newer surfactant: Synthetic surfactants withsynthetic peptides modeled on surfactantproteins. Aerosolized Surfactant.
Natural vs synthetic surfactant
Both natural and synthetic surfactants arebeneficial for prevention and treatment of RDS.But natural surfactant leads to lower mortality,airleaks and faster weaning from the ventilator13.
Dose
Surfactant dose is 50-200mg/kg and is yetto be standardized. Further exogenous surfactantdoes not inhibit endogenous production and isthought to be reutilized in the lungs, hence it isvery difficult to study the pharmaco dynamics.Different manufacturers recommend differentdoses as shown in the Table 3.
Fujiwara showed FiO2 requirement was
higher with lower dose (51-58mg/kg). Higherdose (120mg/ kg) has maximal beneficial effectregarding lesser duration of ventilation, intracranial hemorrhage and bronchopulmonarydysplasia.14
Number of doses
Some times repeat second or third dosingmay be necessary especially when given as laterescue. The need for repeat dosage was lowerwith a higher initial dose and when usedprophylactically.
The criteria for repeat dosing may be lowthreshold (FiO
2>0.3 and still intubated) or high
threshold (FiO2>0.4 and MAP>7cm H
2O).But
both regimen were found to be equally effective.15
Again the timing of the second dose varieswith the manufacturer’s recommendation asSurvanta recommends 6 hours or earlier andCurosurf recommends 12 hours gap between twodoses. Neosurf recommends upto 3 doses in first5 days of age.
Table 2. Monitoring
During the procedure Post surfactant Weaning
Colour Chest rise FiO2
Heart rate SpO2
Ventilator rate
Respirations Blood gas PIP
Blood pressure Chest x-ray
Pulmonary graphics
26

2008; 10(3) : 217
Ventilation strategies
Not all babies receiving surfactant therapyneed to be ventilated. Especially when givenprophylactically or in early rescue where theycan be extubated to nasal CPAP. As endotrachealtube ventilation is an important risk factor forBPD, CPAP especially when given early supportventilation with minimal damage to the lungs.16
INSURE (Intubate, surfactant and extubate toCPAP) therapy has reduced the need formechanical ventilation.17
Indication for mechanical ventilation iswhen the respiratory distress is severe with shockor apnoea and when the baby has respiratorydistress on CPAP.
Blood gas criteria for ventilation : pH is <7.2and hypoxemia PO
2<50-60mmHg despite
FiO2>0.6-0.7 and CPAP of 8cm H
2O. Target to
achieve by ventilation should be a PO2 of 50-
70mmHg and PCO2 35-45mmHg. This should
be achieved with rapid rates, adequate PEEP,short IT, low tidal volumes of 4-6ml/kg withminimal PIP.
Weaning problems
Inability to wean: Repeat dosage
Weaned but requires increase in setting by24 hours: PDA
Sudden deterioration: Pulmonary hemorrhage /air leak
Surfactant Trade name Preparation Protein PL Dosefamily concentration
Natural Survanta (bovine) DPPC,PG SPB,SPC 25mg/ml 4ml/kg
Curosurf (porcine) DPPC,PG SPB.SPC 80mg/ml 2.5ml/kg1.25ml/kg
Neosurf (BLES) DPPC,PG SPB,SPC 27mg/ml 5ml/kg
Infasurf (bovine) DPPC,PG SPB,SPC 35mg/ml 3ml/kg
Alveofact(bovine) DPPC,PG SPB,SPC 4Omg/ml 1.2ml/kg
Synthetic Surfact DPPC No 13.5mg/ml 5ml/kg
Pumactant DPPC,PG No 40mg/ml 1.2ml/kg
Exosurf DPPC No 13.5mg/ml 5ml/kg9% Hexadecanol6% Tyloxapol
NewerSurfactants Surfaxin DPPC,POPG KL4 pepide 30mg/ml 5.8mg/ml
as SPB
Venticute DPPC,DOPG r-SPC 50mg/mlAerosolizedsurfactant
Table 3. Types of surfactant
27

Indian Journal of Practical Pediatrics 2008; 10(3) : 218
Secondary or acquired surfactantdeficiency or dysfunction
Quantitative deficiency of alveolarsurfactant pool may develop secondary to lunginjury and inflammation resulting in loss oftype II cells or impairment in their ability toproduce surfactant.
Surfactant metabolism may be affectedresulting in a change in the phospolipid panellike decrease in the surface active PC/PG thanless surface-active compounds without alteringthe phospholipid pool.
Change in the more surface-active largeaggregates to small aggregates, which impairs thefunction of surfactant.
Damage to the alveolar capillary membrane
Inactivation of surfactant by disease or drugslike hypothermia and acidosis
Mechanism of surfactantdysfunction in mature lungs
• Quantitative deficiency : Decreasedsynthesis / type II cell injury, increasedclearance.
• Altered metabolism of surfactant :Phospolipid composition, composition ofaggregate forms.
• Biophysical alteration of surface activefilms: Altered phospolipid configuration,adsorption of less surface-active agents.
• Biochemical degradation of surface activecompounds : Lytic enzymes and oxygen freeradicals.
Agents inhibiting surfactantfunction
Plasma/serum, hemoglobin, fibrin monomers,RBC membrane lipids, fibrinogen, cholesterol,
albumin, bilirubin, immunoglobulin, amnioticfluid,elastin and meconium.
Meconium aspiration syndrome(MAS)
In a dose dependent manner meconiuminhibits the function of surfactant bycompetitively displacing surfactant from thealveolar monolayer in vitro.
This inhibition is seen with hydrophobic andhydrophilic extracts of meconium and can beovercome by surfactant supplementation.Treatment with natural surfactant had improvedoxygenation in full term babies with MAS.18,19
Earlier administration within 6 hours and higherdoses of 150mg/kg and repeated doses upto fourwere shown to reduce airleaks, ventilationduration and hospital stay.20There was stepwisenature of response to serial doses. There was alsosignificant reduction in the need for ECMO interm infants with MAS after treatment withsurfactant.21
Congenital diaphragmatic hernia(CDH)
There are conflicting data about whetherpatients with CDH actually are surfactantdeficient. Studies have demonstrated normallecithin sphingomyelin ratios and PC, PG inbronchoalveolar lavage fluid in babies with CDH.Wilcox, et al showed improvement in lunginflation, compliance and blood gases and Glick,et al reported reduction in mortality when givenonly prophylactically. However controlledclinical trial is still ongoing.
Other condition where in surfactant is beingadministered is for Group B streptococcalpneumonia as it also plays a role in antibacterialdefense system of the lung. Bulk of the functionis provided by surfactant A and D which areremoved by processing of commercial
28

2008; 10(3) : 219
preparation, B and C which are retained alsocontribute to function. However there are noprospective trials.
Points to Remember
• Surfactant therapy is the standard of carefor neonatal respiratory distress syndrome.
• Intense monitoring during instillation andrapid weaning from ventilator reduces thecomplications.
• Prophylactic surfactant in <30 weekspreterms is beneficial.
• Treatment with natural surfactant andearly rescue therapy has better outcome.
• INSURE therapy has reduced the need formechanical ventilation.
• Early surfactant therapy has reduced theneed for ECMO in meconium aspirationsyndrome.
References
1. Lemons JA, Bauer CR, Oh W, et al. Very lowbirth weight infants outcome of NICHDNeonatal Research Network. Jan 1995-Dec1996.Pediatrics 2001; 107: el-8.
2. Greenough A, Milner A.D, Roberton NRC.Surfactant replacement therapy in NeonatalRespiratory distress syndrome. Comparison ofhigh vs low does of surfactant TA. Euro J Pediatr1998;147(1):20-25.
3. Jobe AH, Ikegami M, Biology ofSurfactant.Clin Perinatol 2001;28:655-669.
4. Crowley PA. Antenatal corticosteroid Therapy-A meta analysis of the Randomized trials 1972-1994.Am Jl Obst Gynec 1995;173:322-335.
5. Jobe A, Ikegami M, Jacobs H, Jones S,ConawayD. Permeability of premature lamb lungs toprotein and the effect of surfactant on thatpermeability. J Appl Physiol 1983 55:169-176.
6. Jobe A, Ikegami M, Jacobs H, Jones S.Surfactant and pulmonary blood flowdistributions following treatment of premature
lambs with natural surfactant. J Clin Invest1984;73:848-856.
7.. Sweet D, Bevilaqua G, Carnielli V, et al.European consensus Guidelines in themanagement of Neonatal Respiratory distresssyndrome. J Perinat Med 2007;35:175-186.
8. Soll RF, Moley CJ. Prophylactic vs selectiveuse of surfactant in preventing morbidity andmortality in preterm infants.Cochrane databaseSyst Rev .2001;2:CD000510.
9. Enhorning G, Shennon A, Possmayer F, et al.Prevention of Neonatal respiratory distresssyndrome by Tracheal instillation of Surfactant:A randomized clinical trial. Pediatrics1985;76:145-153.
10. Kwong MS, Egan EA, Notter RH, et al. Doubleblind clinical trial of calf lung surfactant extractfor the prevention of Hyaline membrane diseasein extremely premature infants. Pediatrics 1985;76:585-592.
11. Yost CC,Soll RF. Early vs delayed selectivesurfactant treatment for neonatal respiratorydistress syndrome.Cochrane Database SystRev.2000;2:CD001456.
12. Broadbent R, Fok TF, Dolovich M,et al. Chestposition and pulmonary deposition of surfactantin surfactant deleted rabbits.Arch Dis ChildFetal and Neonatal Ed 1995;72:F84-89.
13. Soll RF,Blanco F. Natural vs Syntheticsurfactant for neonatal RDS. Cochrane databaseSyst Rev 2001;2:CD00014.
14. Konishi M, Fujiwara T, Naito T, et al. Surfactantreplacement therapy in neonatal respiratorydistress syndrome.Comparison of High vs lowdose of surfactant. Euro J Pediatr 1988;147(1):20-25.
15. Kattwinkel J, Bloom BT, Delmore P, et al. Highvs low threshold retreatment for neonatalrespiratory distress syndrome. Pediatrics2000;106:282-288.
16. Ho JJ, Henderson Smart DJ, Davis PG. Earlyvs delayed initiation of continuous distendingpressure for respiratory distress syndrome inpreterm infants. Cochrane database Syst Rev2002; 2:CD002975.
29

Indian Journal of Practical Pediatrics 2008; 10(3) : 220
17. Bohlin K, GudmundsdottirT,Katz-Salamon M,Jonsson B, Blennow M. Implementation ofsurfactant treatment during continuous positiveairway pressure. J Perinatol 2007;27:422-427.
18. Auten RL, Notter RH, Kendig JW, et al.Surfactant treatment of fullterm newbornswith Respiratory failure. Pediatrics 1991;87:101-107.
19. Khammash H, Perlman M, Wojulewicz J, et al.Surfactant therapy in full term neonates with
severe respiratory failure. Pediatrics 1993;92:135-139.
20. Findlay RD, Taeusch HW, Walther FJ.Surfactant replacement therapy for meconiumaspiration syndrome.Pediatrics1996;97:48-52.
21. Soll RF, Dargaville P. Surfactant for meconiumaspiration syndrome in full term infants.Cochrane database of Syst Rev 2000;2:CD002054.
Name : Radiologist talks to you
Editor : Dr.Elizabeth John
Review : The most popular articles published under the column of “Radiologist talksto you” serially in IJPP is now brought out as the “IJPP Series - I”.Interpretation of X-ray has almost become a part of extended clinicalexamination. For clinicians having a vast knowledge in radiology is notsensible and a simple. It would be of immense help if salient andcomprehensive practical guidelines to interpret skiagrams is given for dayto day practice. This is a long felt need among pediatricians, which is beingfulfilled by the “Radiologist Talks to you” as “IJPP series - I”. NormalX-rays and others that are likely to be missed in clinical practice are coveredin this series. The X-ray picture quality is good. This book apart fromimparting radiological interpretation skill to the reader, will definitely serveas an important desk top reference for the busy pediatric practioner and willbe a must have book for every pediatrician.
Publishers : Indian Journal of Practical Pediatrics1A, Block-II, KRSNA Apartments,No.50, Halls Road, Egmore, Chennai-600 008.Tamil Nadu. India.Phone : 044 - 28190032
Price : Rs.200/-
BOOK REVIEW
30

2008; 10(3) : 221
APPROACH TO NEONATAL
SEPSIS
* Karthikeyan G
Abstract: Antibiotic treatment and aggressivesupportive care are the cornerstones in themanagement of neonatal sepsis. Earlyrecognition is very important but notoriouslydifficult as there are no specific clinical signs ofneonatal sepsis. Sepsis screen is useful to confirmthe clinical suspicion of sepsis but search is stillon for an ideal screening test that has 100%sensitivity and 100% negative predictive value.Intravenous immunoglobulin therapy is not costeffective in treating neonatal sepsis. Colonystimulating factors are useful only in the selectsubset of septic neonates with neutropenia.Exchange transfusion may be helpful in sepsiscomplicated by disseminated intravascularcoagulation, sclerema or neutropenia.
Key words: Neonatal sepsis, Antibiotic therapy,Sepsis screen, Intravenous immunoglobulin,Colony stimulating factor, Exchange transfusion.
Neonatal sepsis is a major neonatal problemaccounting for 1.6 million deaths annually indeveloping countries1. Early recognition is veryimportant as delay can inevitably lead to deathbut this is notoriously difficult as there is nosingle specific clinical symptom or sign that isunique to neonatal sepsis and no laboratory testcan identify a baby with neonatal sepsis with100% sensitivity and 100% negative predictive
value. Neonatal sepsis is a great mimic, itsprotean symptoms mimicking problems in almostevery other organ system. This article will presentan evidence based approach to neonatal sepsis,its diagnosis, antibiotic treatment and otheradjunctive therapies like IV immunoglobulin,colony stimulating factors and exchangetransfusion.
Early versus late onset neonatalsepsis
Sepsis onset within 48 – 72 hours after birthis termed as early onset sepsis and is presumablyacquired vertically from the flora of maternalgenital tract. The risk factors for early onsetsepsis are prematurity, prolonged rupture ofmembranes, intra partum maternal pyrexiamore than 38oC, asphyxia, maternal urinary tractinfection or diarrhea 48-72 hours before deliveryand positive high vaginal swabs. Sepsis onsetafter the first 48 – 72 hours is termed as late onsetsepsis and is acquired horizontally from theenvironment. The risk factors for late onset sepsisare lack of hand washing, low birth weight,mechanical ventilation, indwelling intravenouscatheters and cannulae, superficial infections etc.In a study on neonatal sepsis from Chennai50% of the cases of neonatal sepsis were of earlyonset2.
Pathogens causing neonatal sepsis
Klebsiella pneumoniae, Staphylococcusaureus and E. coli are the predominant pathogenscausing neonatal sepsis in India3. This is incontrast to western countries where Group Bstreptococcus (GBS) and coagulase negativestaphylococci are the predominant pathogens.
* Consultant Neonatologist,G.K Baby Hospital,Coimbatore.
IAP-IJPP CME 2008
31

Indian Journal of Practical Pediatrics 2008; 10(3) : 222
Antibiotic resistance is very common withsensitivity to commonly used antibiotics likeampicillin, gentamicin and cefotaxime being verylow2,3. In the Chennai study 66% of theStaphylococcus aureus isolates were resistant tomethicillin (MRSA).
Diagnostic challenge
Blood culture considered the gold standardfor diagnosis is positive in only about 50% of allneonates with a clinical diagnosis of sepsis2,3.Moreover test results with antibiotic sensitivitytakes about 48–72 hours and hence the initialchoice of antibiotics has to be empirical or basedon sepsis screening.
Sepsis screening
Various hematological and nonhematological parameters have been evaluatedfor rapid evaluation of neonatal sepsis termed assepsis screening4,5. An ideal sepsis screen has tohave 100% sensitivity and 100% negativepredictive value; that is, it should not miss anycase of neonatal sepsis while some overtreatmentcan be accepted. Further it should have a rapidturn over time, be cost effective and results haveto be consistent across different test centres. Nosingle test fulfils these criteria and hence a batteryof tests is employed constituting a sepsis screenpanel. The National Neonatology Forum (NNF)has recommended the following 5 tests asneonatal sepsis screen6.
1. Leucopenia (total leucocyte count less than5000)
2. Neutropenia (total neutrophil count less than1800)
3. Immature : Total neutrophil count ratio morethan 0.2
4. C- Reactive Protein (CRP) more than6mg/L
5. Micro- ESR more than 15 mm in first hour
Two or more positive tests is taken aspositive sepsis screen.
Apart from CRP, other acute phase reactantslike fibrinogen, orosomucoid and procalcitoninhave also been evaluated in some studies but CRPis the one commonly used in sepsis screen panels.Polymerase chain reaction (PCR) has beenevaluated in an Indian study7 and it was found tohave a sensitivity of 100% and specificity of95.6%. Cytokines like Interleukin 6 (IL 6) andTumour Necrosis Factor (TNF) have beenevaluated in experimental studies8. Interleukin 6was raised very early in the course of the diseaseand levels reached normal values by the end of24 hours. Hence it is an early and sensitivemarker. Future sepsis screens are predicted tocomprise of interleukin 6 and CRP.
Antibiotic use and laboratory sepsisscreen
1. In the symptomatic newborn, antibioticsshould not be withheld on the face of a negativesepsis screen as none of the available screen has100% negative predictive value. A completesepsis work up including blood culture, lumbarpuncture (LP) and a chest X-ray needs to be donebefore starting antibiotics. Antibiotics can bestopped in such a situation once the cultures(blood and CSF) are negative.
2. In the symptomatic newborn with apositive sepsis screen whose cultures are negativeantibiotics should be continued for 24 – 48 hoursafter the repeat screen is negative.
3. In the asymptomatic newborn with anegative sepsis screen in whom antibiotics arestarted because of the presence of major ormultiple perinatal risk factors for sepsis,antibiotics can be safely stopped once culturesare negative and a repeat screen is also negative.
4. In the asymptomatic newborn with anegative sepsis screen in the presence of only
32

2008; 10(3) : 223
minor risk factors for sepsis, antibiotics can bewithheld and the neonate should be observed forthe next 24 hours for symptoms and signs ofsepsis.
5. In the asymptomatic newborn with apositive sepsis screen antibiotics should beadministered and continued until the cultures arereported negative or for 24 -48 hours after therepeat screen is negative whichever is later.
6. For blood culture positive casesantibiotics are continued for 10 – 14 days andfor meningitis cases intravenous antibiotics arecontinued for 14 – 21 days or more dependingon repeat CSF culture reports.
Clinical sepsis screening
Who is a symptomatic newborn? Lethargy,feed intolerance, temperature instability and thegut feeling that the baby is just not alright areoften the early presenting features of neonatalsepsis. Never ignore the concerns expressed byexperienced nurses. Bleeding diathesis, purpura,shock and sclerema are more overt but late signsof neonatal sepsis. Recent studies have attemptedto validate different clinical signs and symptomsof neonatal sepsis. A WHO multicentric studyhas identified the following nine clinical featuresthat can be recognized by community healthworkers as being predictive of a serious bacterialillness in young infants9.
1. Feeding ability reduced
2. No spontaneous movement
3. Temperature more than 38oC
4. Prolonged capillary refill time
5. Lower chest wall retractions
6. Respiratory rate more than 60 / min
7. Grunting
8. Cyanosis
9. H/O convulsions
Singh et al have recommended the use offollowing seven clinical signs as having highpredictive ability of neonatal sepsis in a NICUsetting10.
1. Abdominal distension
2. Increased prefeed aspirates
3. Hyperthermia (present on at least2 occasions 1 hour apart)
4. Tachycardia (present on at least2 occasions 1 hour apart)
5. Chest retractions
6. Grunting
7. Lethargy
A cut off score of 1 had the highest negativepredictive value and negative likelihood ratio(85% and 0.44) whereas cut off score of 2 or morehad the best positive predictive value and positivelikelihood ratio (52 % and 2.65) in diagnosis oflate onset sepsis. In a subsequent study to validatethis clinical score in a cohort of VLBW babies,the authors report that the clinical score whencoupled with a laboratory sepsis screen (2 or morepositive of abnormal absolute neutrophil count,immature: total neutrophil count, micro ESR andCRP) had a sensitivity of 95 % and negativepredictive value of 90.6 %11.
Role of lumbar puncture in theevaluation of neonatal sepsis
Meningitis is an important complication oflate onset neonatal sepsis and at least 15% ofculture proven meningitis cases have negativeblood cultures. Hence a recent review hasrecommended that LP has to be part of routineinvestigation in late onset neonatal sepsis (morethan 48 hours)12. A recent review has concludedthat meningitis is very uncommon inasymptomatic neonates with only risk factors forearly onset sepsis and LP can be safely omitted
33
Indian Journal of Practical Pediatrics 2008; 10(3) : 224
in this group of neonates13. LP still has to beundertaken in babies who are symptomatic withearly onset sepsis or those with strong suspicionof meningitis13.
Guidelines for antibiotic therapy
Antibiotic therapy has to be startedwhenever there is a doubt of neonatal sepsis buthas to be stopped once it is reasonably certainthat the baby is not infected. Choice of antibioticsdepends on local sensitivity pattern of bacterialisolates. Wherever possible, narrow spectrumantibiotics to which the isolates are sensitive haveto be preferred to more broad spectrum antibioticsto minimize chances of antibiotic resistance14.But on the face of a seriously ill neonate, thereshould not be a hesitation to embark on broadspectrum antibiotics like meropenam,fluroquinolones etc. Antibiotic rotation policieshelp to keep emergence of antibiotic resistancein check.
Supportive therapy in neonatalsepsis
High level intensive supportive care is thecornerstone in the management of neonatal sepsisespecially those cases with shock syndrome andmulti organ dysfunction syndrome. Respiratorysupport strategies, hemodynamic support usingblood products, fluids and inotropes andnutritional support using total parenteral nutritionfor those cases with necrotizing enterocolitis arecrucial in the resuscitation and management ofseptic shocked neonate with multiorgandysfunction.
Novel adjunctive therapy inneonatal sepsis
Intravenous immunoglobulin in neonatalsepsis: Intravenous immunoglobulin (IVIG)despite its theoretical benefits has failed to liveup to the expectations in the clinical trials so far.
A cochrane review on IVIG for prevention ofnosocomial sepsis in preterm or low birth weightneonates reports a meager 3% decrease in theincidence of sepsis in the treated group with nodecline in mortality or morbidity15. AnotherCochrane review on IVIG for suspected orsubsequently proven infection in neonates foundborderline significant decrease in mortality andconcludes that there is need for further adequatelypowered trials16. The results of InternationalNeonatal Immunotherapy Study (INIS) thatenrolled 3500 neonates with sepsis to IVIGtherapy in addition to antibiotics are expected in2009 – 2010. Given the cost of IVIG and thenumber needed to treat because of the smallbeneficial effect, it is not cost effective toadminister IVIG for prevention or treatment ofneonatal sepsis in India and its use has to berestricted to individual circumstances. Thepolyclonal non specific nature of the IVIGpreparations used in these trials could have beenresponsible for the not so bright results achievedand specific immunoglobulin therapy like antistaphylococcal immunoglobulin is being tried insome clinical trials.
Colony stimulating factors (CSFs) in neonatalsepsis: The granulocyte colony stimulating factor(G- CSF) and granulocyte- monocyte colonystimulating factor (GM- CSF) are naturallyoccurring cytokines that stimulate the productionand antibacterial function of granulocytes andmonocytes. Neonates whose chemotaxis andphagocytic abilities are reduced when comparedto adults especially when complicated byneutropenia may benefit from the administrationof CSFs. A cochrane review has suggested thatG- CSF and GM- CSF decrease the mortality atday 14 in a sub group of 97 neonates withsystemic infection complicated by neutropenia(< 1.7 x 109/l) but there is no evidence of anybeneficial role in the prevention of sepsis in highrisk neonates as well as reducing mortality in
34

2008; 10(3) : 225
those with systemic infection uncomplicated byneutropenia17. The dose of G- CSF and GM- CSFused in the studies range from 5–10 mcg/kg/daygiven subcutaneously or intravenously for3–21 days.
Exchange transfusion in neonatalsepsis
Fresh blood exchange transfusion canreplenish the clotting factors, correct anemia,remove circulating bacterial toxins and provideopsonins and immunoglobulins. But there is nolarge well conducted randomized controlled trialto validate its efficacy in treating neonatal sepsis.Limited review of available studies18 hassuggested that exchange transfusion may beconsidered in severe neonatal sepsis complicatedby a) disseminated intravascular coagulationb) sclerema c) neutropenia.
Conclusions
Apart from antibiotic therapy and supportivecare no further definite therapeutic choices areavailable to treat neonatal sepsis. Given the riskof increased mortality despite therapy andsequelae like periventricular leukomalacia andthe cost of treatment, it is wiser to emphasize onpreventive strategies of neonatal sepsis. Goodhand hygiene and exclusive breastfeeding are themajor time tested preventive strategies and tryto avoid the ‘give sepsis, treat sepsis’ cycle inneonatal intensive care.
Points to Remember
• Antibiotics should not be withheld in asymptomatic neonate even in the presenceof a negative sepsis screen as none of theavailable tests has 100% negative predictivevalue.
• Lumbar puncture is mandated in allneonates with late onset sepsis and insymptomatic babies with early onset sepsis.
• Existing evidence does not support routineuse of intravenous immunoglobulin inneonatal sepsis.
• Colony stimulating factors are beneficialin the select subset of septic babies withneutropenia.
• Exchange transfusion may be helpful inneonatal sepsis complicated bydisseminated intravascular coagulation,sclerema or neutropenia.
References
1. Vergnanao S, Sharland M, Kazambe P,Mwansambo C, Heath PT. Neonatal sepsis: aninternational perspective. Arch Dis Child FetalNeonatal Ed 2005; 90: 220 – 224.
2. Karthikeyan G, Premkumar K. Neonatal sepsis:Staphylococcus aureus as the predominantpathogen. Indian J Pediatr 2001; 68: 715 – 717.
3. Neonatal morbidity and mortality: Report of theNational Neonatal – Perinatal Database. IndianPediatr 1997; 34 :1039–1042.
4. Chiesa C, Panero A, Osborn JF, Simonetti AF,Pacifico L. Diagnosis of neonatal sepsis:A clinical and laboratory challenge. ClinicalChemistry 2004 ; 50 : 279 – 287. Availablefrom http://www.clinchem.org/cgi/content/full/50/2/279
5. Rodwell RL, Leslie AL, Tudehope DI. Earlydiagnosis of neonatal sepsis using ahaematological scoring system. J Pediatr1988; 112 : 761 – 767.
6. Neonatal sepsis. NNF teaching aids availablefrom http://www.gujhealth.gov.in/family-wel/pdf/Newborn%20Care/neonatalsepsis.pdfaccessed on 29.4.2008
7. Yadav AK, Wilson CG,Prasad PL, Menon PK.Polymerase chain reaction in rapid diagnosisof neonatal sepsis. Indian Pediatr 2005; 42 :681–685.
8. Mishra UK, Jacobs SE, Doyle LW, Garland SM.Newer approaches to the diagnosis of earlyonset neonatal sepsis. Arch Dis Child FetalNeonatal Ed 2006 ; 91 : F208 – 212.
35

Indian Journal of Practical Pediatrics 2008; 10(3) : 226
9. The WHO Young Infants Study Group. Clinicalprediction of serious bacterial infections inyoung infants in developing countries. PediatricInfect Dis J 1999;18:S23 -31.
10. Singh AS, Dutta S, Narang A. Predictive clinicalscores for diagnosis of late onset neonatalsepticemia. J Trop Pediatr 2003;49:235–239.
11. Kudawala M, Dutta S, Narang A. Validation ofa clinical score for the diagnosis of late onsetneonatal septicemia in babies weighing 1000 –2500 g. J Trop Pediatrics Advance accesspublished August 14, 2007.
12. Malbon K, Mohan R, Nicholl R. Should aneonate with possible late onset infectionalways have a lumbar puncture? Arch Dis Child2006; 91: 75 – 76.
13. Ray B, Mangalore J, Harikumar C, Tuladhar A.Is lumbar puncture necessary for evaluation ofearly neonatal sepsis? Arch Dis Child 2006; 91:1033 – 1035.
14. Isaacs D. Unnatural selection: reducingantibiotic resistance in neonatal units.
Arch Dis Child Fetal Neonatal Ed 2006; 91:F72 – F74.
15. Ohlsson A, Lacy JB. Intravenous immuno-globulin for preventing infection in preterm and/or low birth weight infants. Cochrane Databaseof Systematic Reviews 2004, Issue 1. Art. No.:CD000361. DOI: 10.1002/14651858.CD000361.pub2.
16. Ohlsson A, Lacy JB. Intravenous immuno-globulin for suspected or subsequently proveninfection in neonates. Cochrane Database ofSystematic Reviews 2004, Issue 1. Art. No.:CD001239. DOI:10.1002/14651858.CD001239. pub2.
17. Carr R, Modi N, Doré C. G-CSF and GM-CSFfor treating or preventing neonatal infections.Cochrane Database of Systematic Reviews2003, Issue 3. Art. No.: CD003066. DOI:10.1002/14651858.CD003066.
18. Nangia S, Saili A. Exchange transfusion inneonatal sepsis - Does it help? J Neonatol2006; 20: 333 – 337.
36
BAI JERBAI WADIA HOSPITAL FOR CHILDREN
PAREL, MUMBAI 400 012
Department of Pediatric Hematology & Oncology
• 2 yrs Fellowship course in Pediatric Hematology and Oncology(PHO) is conducted under
the auspices of National Board of Examination (NBE), Delhi
• Four centres recognised / accredited by NBE are: B.J. Wadia Hospital for Children, Mumbai,
Gangaram Hospital, Delhi, Rajiv Gandhi Cancer Centre, Delhi, Kasturba Medical College,
Mangalore.
• All the Head of Departments pediatric departments are requested to encourage their
postgraduates to avail of this attractive Fellowship programme and appear for the entrance
test conducted by NBE at various cities in November / December 2008. Please keep track of
the details on their website (www.natboard.nic.in).
Dr. Bharat AgarwalHead of Department,
Paediatric Hematology & Oncology.
NEWS AND NOTES

2008; 10(3) : 227
37
ALLERGIC RHINITIS
* Shivbalan So** Gowrishankar NC
Abstract : Allergic rhinitis (AR) is a symptomcomplex characterised by paroxysmal sneezing,rhinorrhea, nasal obstruction and itching of eyes,nose, palate on exposure to allergen. ARis not uncommon and about a third of childrenwith AR have asthma. AR interferes with feedingand sleep in very young children while it causespersistent nasal obstruction and chronic mouthbreathing in older children. Diagnosis is byhistory and physical examination while skinprick tests are rarely needed. Managementincludes avoidance of allergens, intranasalcorticosteroids and/or antihistamines.
Keywords : Allergic rhinitis, Clinical features,Intranasal cortico steroids.
An allergy is our body’s immune systemresponse to a substance that is usually harmless.Rhinitis is defined as an inflammation of themucus membrane lining the nose resulting in theoccurrence of annoying nasal symptomsincluding discharge, itching, sneezing,congestion, and pressure. Allergic reactions inthe nose are frequent as inhaled allergens aretrapped by the nasal filtration system.
Allergic rhinitis (AR) is defined as one ofthe rhinitis syndromes, associated with a
symptom rhinorrhea, nasal obstruction anditching of the eyes, nose and palate, occurringupon inhalation of allergens among individualspreviously exposed to such allergens and againstwhich they have IgE antibodies.
Pathogenesis
Allergic rhinitis (AR) occurs in a geneticallyhypersensitivity response. There is an increasein circulating IgE levels with release ofinflammatory mediators like, histamine,prostaglandins and leukotrienes resulting insymptoms within a few minutes of exposure(early-phase response). In about half of patients,symptoms recur two to eight hours after exposureto allergen and without further exposure,resulting from infiltration of inflammatory cells(late-phase response).
Clinical features
Characteristic features of allergic rhinitisinclude sneezing, watery rhinorrhea, and nasalcongestion. This may be accompanied by itchywatery eyes and intense itching of the nose andsoft palate. A family history of allergy is thesingle-most important factor predisposingchildren to the development of allergic diseases.AR generally begins in childhood or adolescenceand continues into adulthood. In fact, more thantwo-thirds of people with AR are diagnosed atyounger than 20 years of age. Most cases ofallergic rhinitis begin in the teens or early adultlife.
Symptoms are less common in infants orvery young children. When they do occur,obstruction may interfere with feeding and
IAP-IJPP CME 2008
* Consultant Pediatrician and Pulmonologist,Sundaram Medical Foundation, Chennai.
** Asst. Professor of Pediatrics,Dept. of Pulmonology,Institute of Child Health and Hospital forChildren, Chennai - 8.

Indian Journal of Practical Pediatrics 2008; 10(3) : 228
contribute to irritability. Children are particularlyaffected by the consequences of this illnessespecially because nasal obstruction often leadsto disturbed sleep patterns, poor quality sleep,fatigue, daytime sleepiness, poor concentration,hearing difficulty, poor appetite and poor growth.Persistent nasal obstruction predisposes tochronic mouth breathing, which in turn in agrowing child causes abnormal development ofthe mouth and teeth associated with changes infacial features. About one-third of people withAR have asthma. Treating AR with systemic orlocal agents can alleviate the symptoms ofasthma. AR may be associated with allergicconjunctivitis, chronic sinusitis or rhinosinusitisdue to blockage of the osteomeatal unit andrepeated bouts of otitis media with or withouteffusion due to eustachian tube inflammation.
Allergic rhinitis can also be associated withuncontrolled asthma, halitosis, husky voice, sorethroat and recurrent eye infections. Allergicrhinitis should be considered in children withcontinuous or recurrent upper respiratoryinfections, frequent sore throat, mouth breathingand snoring, recurrent infective sinusitis,headaches, recurrent upper respiratory tract ormiddle ear infections.
Physical examination
Focus the physical examination on thepatient’s nose, eyes, throat, ears, lungs andskin. Observe the patient for “allergic salute”(ie., repeated nose wiggling, wiping, pushing,etc., usually with an open, upward-facing palm)and mouth breathing (chronic). Transverse nasalcrease and Dennie-Morgan infra orbital creaseoccurs secondary to allergic salute. Nasalexamination usually reveals clear nasalsecretions, edematous, boggy nasal mucousmembranes with little or no erythema andswollen, purple turbinates that may block thenasal airway. Thick nasal secretions may indicateinfection. AR often reveals conjunctival,
periorbital edema, periorbital “shiners” or darkcircles under the eyes attributed to venous stasisresulting from interference with blood flowcaused by edematous nasal mucous membrane.
Pattern of AR
Traditionally AR has been described asbeing either seasonal (hay fever) or perennial,although both types often coexist. Seasonal ARoccurs at defined yearly intervals in response towind borne outdoor allergens such as tree, grassand weed pollens. Plants that rely on insectpollination rarely cause AR. Perennial AR aretriggered by exposure to allergen present all yearround like house dust mite, animal dander ormoulds.
The World Health Organization in itsguidelines, “Allergic Rhinitis and Its Impact onAsthma,” proposed that AR no longer beclassified as seasonal or perennial (occupational)but rather be categorized as either persistent orintermittent, and that symptoms be gradedrelative to severity. This is in relation to theconcept of one airway and one disease that thechronic inflammatory reactions in the nose, eyes,and upper airways of people with AR areidentical to those that occur in the lower airwaysof people with asthma, and that the twoconditions are inextricably linked. IntermittentAR is defined as symptoms less than 4 days perweek or less than 4 weeks at a time. PersistentAR is defined as symptoms more than 4 days perweek or more than 4 weeks at a time. Mild tosevere AR is categorized based on anyimpairment of sleep and daily activities (Fig.1).
Differential diagnosis
• Nonallergic perennial rhinitis (vasomotorrhinitis)
• Non-allergic rhinitis with eosinophiliasyndrome (NARES)
• Rhinitis medicamentosa.
38

2008; 10(3) : 229
• Gustatory rhinitis
• Anatomic nasal obstruction (eg, polyps,deviated septum, enlarged turbinates,adenoid hypertrophy, tumor)
• Nasal foreign bodies (particularly in youngchildren)
• Infectious rhinitis, atrophic rhinitis,rhinosinusitis.
• Environmental/ Occupational rhinitis(eg. animal exposure, woods dusts, industrialenzymes, food processing, latex).
• Rarely: Malignancy, vasculitis(eg. Wegeners granulomatosis), sarcoidosis,hypothyroidism.
Diagnosis
History and physical examination areusually sufficient to diagnosis and manage AR.In select situations skin prick tests or serumassays for allergen- specific IgE may be required
to differentiate allergic and nonallergic rhinitiswhen they are not adequately controlled bymedication and trigger avoidance. Presence ofeosinophils in nasal smear is usually in favor ofallergic origin but does not conclusivelydifferentiate AR from nonallergic eosinophilicrhinitis.
Allergy testing
Allergy testing is performed in order toconfirm the diagnosis in difficult cases and toidentify the allergens that could be avoided or beincluded in immunotherapy regimens. Culpableallergens can be identified by skin prick test orin vitro tests to test the presence of allergen-specific IgE antibodies.
In vitro tests for serum IgE antibody toallergens by radioallergosorbent test (RAST) andenzyme-linked immunosorbent assay (ELISA),estimate the amount of allergen-specific IgEantibody in a patient’s serum.
39
Intermittent (Symptoms)
• < 4days/ Wk
• or < 4 Wks
Pers(Symp
• > 4 days
• and > 4
Mild (All of the following)
• Normal sleep • No impairment of daily activities, sport, leisure • No impairment of work & school • No troublesome symptoms
Modera(One or m
• Abnormal s• Impairment activities, s• Impaired w school • Troublesom
Fig.1. Classification of AR
Indian Journal of Practical Pediatrics 2008; 10(3) : 230
Management
Five general approaches can be used in themanagement of allergic diseases: identificationof allergens, patient education, avoiding orminimizing exposure to allergens, pharmaco-therapy and allergen immunotherapy.
Allergen avoidance
Allergen identification and avoidance arecritical first steps in treatment, particularly inpatients with perennial symptoms. Neithermedications nor immunotherapy should be usedas substitutes for, but rather as adjuncts to,reducing exposure to allergic triggers.
The common allergens are: (a) Pollen,(b) Molds/Fungi, (c) Dust Mites: Air cleanerswith high-energy particulate air (HEPA) filtersmay reduce particulate air matter. (d) AnimalDander: The root of the problem is the proteinsecreted primarily by sebaceous glands which isalso found in urine and saliva. Dander becomeseasily airborne and accumulates in upholsteredfurniture and carpets. For patients allergic to petdander, the only way to completely eliminatesymptoms is to remove the pet from the home.(e) Cockroaches, (f) Viral upper respiratoryinfections can aggravate allergies. They shouldavoid contact with people who have viral upperrespiratory illnesses, if possible, wash handsfrequently, and refrain from sharing food, drink,etc.
Pharmacotherapy
The therapeutic options in AR managementare shown in Table 1 and topical medications aregiven in Table 2.
Inhaled nasal glucocorticosteroids (INGCs)have been shown to be effective in themanagement of allergic rhinitis. They relievenasal blockage, discharge, sneezing, nasal itch,post-nasal drip and eye symptoms. Corticosteroidnasal sprays act as prophylactic agents and are
not intended to relieve acute symptoms, hencethey need to be used on a regular basis. TheUnited States Food and Drug Administration(FDA) has approved six intranasal steroids foruse in AR: beclomethasone, budesonide,flunisolide, fluticasone, mometasone, andtriamcinolone. All work by down-regulatingnumerous steps in the inflammatory process.When used prophylactically, they attenuate bothearly- and late-phase reactions. Most agents inthis drug class are administered once or twicedaily and have an onset of action of 12 to24 hours. Maximum benefit can take days orweeks to manifest. Once control of symptomshas been achieved the dosage should be reducedprogressively to the minimum dose to controlsymptoms. Daily use is required in most patients.
In clinical practice for children, INGCs canbe started with the maximal dose for age. Oncesymptoms are adequately controlled, “step down”the dose at one week intervals to the lowesteffective dose. Patients with severe symptomswill require daily use on a chronic basis.
Step on how to use INGCs;
• Shake the bottle.
• Blow your nose so that your nostrils areclear.
• Wash your hands.
• Take the lid off the bottle.
• Tilt your head slightly forward.
• Close one nostril by gently pressingagainst the side of your nose with yourfinger.
• Insert the tip of the nasal spray awayfrom the septum into the other nostril andstart to breathe in slowly through yournose. While you are still breathing insquirt one spray into the nostril keepingthe bottle upright.
40

2008; 10(3) : 231
Table 1. Therapies for allergic rhinitis
Agent Action Indication Example Side effects
Second- Blocks H1
Reduces sneezing, Fexofenadine; Mild sedation, drygeneration receptors ocular and Cetrizine, mouth inantihistamine and inhibits- nasopharyngeal- Loratadine minorityof
autacoid release itching, rhinorrhea Azelastine* patients
Intra nasal Inhibits influx Reduces sneezing, Beclomethasone Nosebleed,corticosteroid* of inflammatory ocular and Budesonide nasal septal
cells nasopharyngeal- Fluticasone perforationitching, rhinorrhea, Mometasonemucosal congestion
Leukotriene- Blocks Reduces mucosal Montelukast Elevated levels ofreceptor leukotriene inflammation AST, ALT,antagonist receptors Bilirubin
Anticholinergic Blocks Reduces copious Ipratropium* Headache,agent acetylcholine rhinorrhea nosebleed
receptors
α adrenergic Vasoconstrictor Relieves nasal Pseudoephedrine, Arrhythmias,agonist congestion Phenylephrine hypertension,(decongestant) nervousness,
insomnia
* Intranasal application
Table 2. Dosage of nasal topical medication
Azelastine 5-11 yrs, 1 spray each nostril BD≥12 yrs, 2 spray each nostril BD
Beclomethasone ≥6 yrs, 1-2 spray each nostril BD
Budesonide ≥6 yrs, 1-2 spray each nostril OD(≥12 yrs max of 4 spray each nostril OD)
Fluticasone ≥4 yrs, 1-2 spray each nostril OD
Mometasone 2-11 yrs, 1 spray each nostril OD≥12 yrs, 1-2 spray each nostril BD
Ipratropium ≥5 yrs, 2 spray each nostril 2-3 times/ day.
41

Indian Journal of Practical Pediatrics 2008; 10(3) : 232
• Remove the spray from the nostril andbreathe out through your mouth.
• Repeat the same for the other nostril.
• Replace the lid on the bottle.
• Once daily preparations may be moreeffective if administered in the evening,as nasal inflammation is greater at nightthan during the day
Antihistamine nasal sprays or eye drops(azelastine) act rapidly (within minutes) to relievesneezing or itching and are generally welltolerated. In general, they are less effective atrelieving severe nasal congestion.
Decongestant nasal sprays or drops provide quickrelief, but should only be used in the short-term(up to a maximum of 5 days) to clear excessivenasal blockage. In patients with severe nasalobstruction, they may be used for a few days toopen the air passages to allow access to the nasalmucosa by corticosteroid nasal sprays. Repeatedor long term use of this can lead to rhinitismedicamentosa. Intranasal decongestants(eg.phenylephrine, oxymetolazine, xylometola-zine, and naphazoline), which act more rapidlyand have fewer systemic side effects than oralcounterparts, continue to be used widely bypatients with AR, but use for more than seven toeight days causes rebound congestion upon drugwithdrawal.
Anticholinergic sprays (Ipratropium) are veryeffective in reducing watery rhinorrhoea.
Mast cell stabilising nasal sprays or eye dropscromolyn sodium reduce inflammation withregular use.
Oral medication
Systemic corticosteroids are indicated for allergicrhinitis only in exceptional circumstances.
Leukotriene antagonists (montelukast), whiletopical nasal steroids appear to provide superiorsymptoms control, these drugs may provideadditional relief in selected patients.
Non medicated treatment with steam and saltwater (saline) sprays when used on a regular basiscan help to relieve nasal blockage and thicksecretions.
Diet has only a minor influence onsymptoms in most people. The results from strict“elimination diets” are usually disappointing andmay affect nutrition.
The stepwise algorithm for management ofAR is depicted in Fig.2.
Immunotherapy
Immunotherapy (desensitisation) is theclosest thing to a cure for allergic rhinitis and aneffective adjunct to drug therapy in selectedpatients. Immunotherapy, or the repeated,controlled administration of specific allergens topatients with IgE-mediated conditions and isusually given to patients as weekly or biweeklyinjection over a period of years.
Immunotherapy decreases early and latephase response to nasal allergen challenge. Themajor risk with the use of immunotherapy isanaphylaxis, and serum sickness too can occurrarely.
Allergy prevention in children
Allergies are often life-long and althoughtreatable, they are not curable. To preventallergies in children with a strong family historyof allergies it is suggested to exclusively breastfeed infants till 6 months, starting complimentaryfeeding after 6 months with hypoallergenic diet,avoid exposure to environmental tobacco smoke,delay introduction of allergenic foods andminimise exposure to dust mites.
42

2008; 10(3) : 233
Fig.2. Management of AR
43

Indian Journal of Practical Pediatrics 2008; 10(3) : 234
Points to Remember
• Allergic rhinitis is not uncommon inchildren
• Allergies are often life-long and althoughtreatable, they are not curable
• AR is most often a clinical diagnosis andinvestigations are rarely required
• Allergen avoidance is the first step in ARmanagement.
• INGCs and 2nd generation antihistaminicsare the main stay of pharmacotherapy
• Skin testing and immunotherapy is used asa last resort in difficult cases
44
Bibliography
1. Greiner AN. Allergic rhinitis: impact of thedisease and considerations for management.Med Clin North Am, 2006;90:17-38.
2. Lai L, Casale TB, Stokes J. Pediatric allergicrhinitis: treatment. Immunol Allergy Clin NorthAm, 2005;25:283-299.
3. Plaut M, Valentine MD. Clinical practice.Allergic rhinitis. N Engl J Med 2005;353:1934-1944.
4. ARIA, At-A-Glance Pocket Reference 2007.New aria update based on the allergic rhinitisand its impact on asthma workshop report Incollaboration with the World HealthOrganisation, GA
2LEN, and allergen.
NEWS AND NOTES
“THILLAI NEOCON 2008”VI Annual Convention of National Neonatology Forum
TamilNadu Chapter
Venue: Rajah Muthiah Medical CollegeAnnamalai UniversityAnnamalai Nagar – 608 002
Date : 4th & 5th October 2008.
Organised by : Rajah Muthiah Medical College and Indian Academy of Pediatrics – Cuddalore District
For details contact:
Dr.S.RameshProfessor & H.O.D of PediatricsRajah Muthiah Medical College & HospitalAnnamalai UniversityAnnamalai Nagar – 608 002E.mail: doc_ramesh [email protected]@gmail.comFax : 04144 - 237333Phone No: 04144 – 237333Mobile No: 9443271734, 9486223289

2008; 10(3) : 235
LONG TERM CONTROL OF
CHILDHOOD ASTHMA
* Balachandran A
Abstract : Asthma, an inflammatory disorder ofairway is known for its episodic presentation.Clincial evaluation is based on history, clinicalexamination and laboratory investigations. Longterm management comprises of allergen control,aerosol therapy and follow up.
Keywords : Asthma, Clinical evaluation,Chronic managment, Children.
Asthma is defined as a chronic inflammatorydisorder of the tracheobronchial treecharacterized by reversible recurrent airwayobstruction either spontaneously or with therapy.Asthma is characteristically episodic hence theremay not be signs and symptoms of airwayobstruction at the time of evaluation. Thesepatients have airway hypersensitivity to a varietyof stimuli.
The pathologic changes include anatomicnarrowing of the tracheobronchial airway causingincreased resistance to air flow, over inflation ofthe lung, uneven distribution of ventilation withregional hypoventilation in relation to pulmonaryblood flow (reduced V/Q) causing hypoxemiaand increased ventilation drive. This is secondaryto airway inflammation, mucus plugging andepithelial injury. In uncontrolled persistentasthma, over a period of time these changes leadto airway remodeling.
Clinical evaluation
The diagnosis of asthma is basedpredominantly on history, clinical examinationand laboratory investigations.
History
1. A complete description of the symptoms:
a. Symptoms such as recurrent cough orwheeze or breathlessness, chest discomfort,post tussive vomiting
b. Pattern of symptoms with regards to onset,severity, duration, character, diurnalvariation, sleep disturbance and child’sactivity.
c. Precipitating factors such as allergens,infections, nonspecific exposure to irritants,weather changes, emotional factors andphysical stress (exercise) which may inducecough and wheeze.
2. History of associated illness, rhinitis, sinusitis,atopic dermatitis and nasal polyps.
3. Details of previous episodes and medicationsand the response to bronchodilators or steroids.
4. Environment of the child at home, school, playarea, presence of pets or pollutants.
5. Impact of the disease on the child and family,both at home and around in consideration ofsocioeconomic and emotional factors.
6. Family history of allergy, asthma or othersignificant medical problems.
Also look for evidence of atopy like eczema,bilateral pale hypertrophied inferior turbinate and
IAP-IJPP CME 2008
* Consultant Pediatric Pulmonologist,Mehta Children’s Hospital,Chennai
45

Indian Journal of Practical Pediatrics 2008; 10(3) : 236
insect bite allergy. Look for the shape of chest inpersistent asthma, there may be an increase inanteroposterior diameter.
It is important to remember that asthma ischaracteristically episodic and children may nothave signs or symptoms at the time ofexamination. Diagnosis of asthma is based ondetailed history and clinical examination andabsence of wheeze during examination does notexclude a diagnosis of asthma. Hence it isnecessary to know the symptoms and signs ofairway obstruction and to assess them inevaluation to make a diagnosis of asthma.
Symptoms suggestive of airway obstructionare: recurrent wheeze, recurrent isolated cough,recurrent breathlessness, nocturnal cough,tightness of chest and/ or exercise induced cough/wheeze. Asthma symptoms tend to cluster in laterpart of the night. Hormonal changes are attributedto play a role in night time symptoms of asthma.The serum cortisol and epinephrine levels are attheir nadir in early morning causing increasedairway resistance and nocturnal symptoms.
Signs suggestive of airway obstruction are:generalised rhonchi, prolonged expiration and/or chest hyperinflation (increased anteroposteriordiameter of the chest).
It is important to remember that allasthmatics need not have wheeze. Coughresponding to bronchodilators may be anevidence of reversible bronchospasm. Asthmacan manifest either as acute exacerbations orchronic asthma.
Diagnosis
No definitive diagnostic test for asthmaexists and the diagnosis of asthma is based on aclinical constellation of symptoms, the patient’spersonal and family history, physical examinationfindings (which are often absent when acute
symptoms are not present), and supportivelaboratory tests like spirometry.
Grading of asthma severity
History of inability to eat due to symptoms,sleep disturbance, restriction of play and activity,frequency of school absenteeism along with thenumber of emergency room visits andhospitalization need to be taken into account forassessing the severity of asthma. Based onsymptoms, severity of chronic asthma can beclassified (Table 1).
However, for practical purposes gradingseverity of asthma is done by assessing symptoms(day and night) with or without peak expiratoryflow (PEF) over a period of time (eg. last3 months).
Aerosol therapy is the cornerstone in asthmamanagement. There are number of deliverysystems available that are suitable for differentages. The advantages of aerosol therapy aresmaller dose, target delivery, quick action, safetyand fewer side-effects. The delivery systems thatare commonly utilized are: metered dose inhalers(MDI), dry powder inhalers (DPI) and nebulisers(Table 2).
Successful pharmacologic management ofasthma should incorporate two major strategies:reversal of acute and chronic airway obstruction,long-term attenuation and prophylaxis of theintrabronchial sequelae due to inflammatory cellsand their mediators. The current treatment ofasthma involves two major classes of drugs:
a) Relievers, i.e. bronchodilators used forimmediate relief of symptoms. e.g. salbutamol,terbutaline.
b) Controllers, i.e. anti-inflammatory drugs thathelp in stopping bronchial wall remodelling andin prevention of excacerbations. They can beeither inhaled or oral medications.
46

2008; 10(3) : 237
Table 1. Severity of asthma
Grade of severity Day time Night time Peak expiratorysymptoms symptoms flow(PEF)*
Intermittent · < twice a week · < twice a month · > 80% of personal best· Brief exacerbation · <20% diurnal variation**
Mild persistent · > twice a week but · > twice a month · >80% of personal best< twice a day · 20-30% diurnal variation
· Exacerbation mayaffect sleep andactivity
Moderate persistent · Daily · > once a week · > 60%-<80% of personal· Exacerbation may best or
affect sleep and · > 30% diurnal variation**activity
Severe persistent · Daily · Frequent · < 60% of personal best· Limited physical · > 30% diurnal variation**
activity· Frequent
exacerbation
* Not essential
** A diurnal variation of < 10% in PEF values is normal. Lowest PEF levels are seen on wakingand highest levels about 12 hours later.
Table 2. Age appropriate devices
Device Suitable age % of drugdelivery
MDI + <4 years 10-15%Spacer + (preschool)Face mask
MDI + >4 –6 years 10-15%Spacer (early school age)
DPI >7-8 years 5-10%(late childhood)
MDI adolescence 5-10%
Home all ages 1-5%nebuliser*
* Not recommended routinely except in acutesevere exacerbations or where other modalitiesof drug delivery had failed especially in infants.
Inhaled drugs are inhaled corticosteroids(ICS) like beclomethasone, budesonide,fluticasone and ciclesonide, long acting betaagonists (LABA) like salmeterol and formoteroland mast cell stabilizer like cromolyn sodium.
Oral medications are leukotriene antogonists(LTRA) like montelukast, sustained release(SR) theophylline and oral steroids. Controllersonly control but do not cure asthma and there isno role for controller therapy in intermittentasthma.
Long term management of asthma consistsof environmental control of dust and pollution,management of chronic asthma with aerosoltherapy and treatment of acute episodes ofasthma, regular follow up and effective parent/patient education.
47

Indian Journal of Practical Pediatrics 2008; 10(3) : 238
Specific goals of asthma management are:
• Control of symptoms
• No emergency room visits orhospitalizations
• No school absenteeism
• No exercise limitations
• No sleep disturbance
• Optimal lung function
• Limited side effects due to drugs
• Normal day to day life like their peers.
Normal growth
Once a diagnosis of asthma has been madeappropriate management should be instituted.Assessment of severity of asthma should be madebased on duration, frequency and severity ofsymptoms. Peak flow rate is not always requiredand is an additional objective measurement forgrading and diagnosis. The latest trend in themanagement of asthma is aerosol therapyi.e. inhaled drugs are better than systemic drugsbecause of target delivery, smaller dose, rapidaction and fewer side effects. For the inhaled drugto be effective it should reach the lungs insufficient amount. The penetration and depositionof aerosol depends upon the particle size,velocity, type of device and ventilatory pattern.
Initiation of aerosol therapy: Once diagnosishas been reached appropriate management shouldbe instituted. Assess severity of asthma. Thereare two methods in practice: one is “step down”method, where control is achieved by startingthe regime suitable to higher severity and titrateddown. Other method is step up method in whichthe regime appropriate to the grade assessed isstarted and titrated upwards if control is notachieved. The drug and dosage for asthmamanagement are given in Table 3 and 4.Medication plans must accommodate the fact thatasthma is both a chronic and a dynamic condition
and severity has to be reassessed on every followup visit.
On follow up
Follow up is basically to reassess the childfor symptom control or exacerbations, checkingreinforcing drug compliance and technique.
Therapy is initiated based on the degree ofsymptoms, airflow limitation, and lung functionvariability which have allowed asthma to beclassified by severity as intermittent, mildpersistent, moderate persistent, or severepersistent asthma. However, it is important torecognize that asthma severity involves both theseverity of the underlying disease and itsresponsiveness to treatment. The severity ofasthma may change over months or years.Therefore, for subsequent ongoing managementof asthma, the more relevant and usefulclassification of asthma would be by the level ofcontrol.
The goal of asthma care is to achieve andmaintain control of the clinical manifestationsof the disease for prolonged periods. Whenasthma is controlled, patients can prevent mostattacks, avoid troublesome symptoms at day andnight, and be physically active.
To reach this goal, four interrelatedcomponents of therapy are required: (1) Developpatient/ family and doctor partnership,(2) Identify and reduce exposure to risk factors,(3) Assess, treat, and monitor asthma,(4) Manage acute episodes of asthma.
Assess, treat and monitor asthma
The ultimate goal of asthma management isto achieve and maintain clinical control. This canbe achieved during regular follow-up byassessing asthma control, accordingly treating toachieve control and monitoring further tomaintain control
48

2008; 10(3) : 239
Table 4. Equipotent daily dose ICS and LABA in children
Relievers Low dose Medium dose High dose(μg / day) (μg / day) (μg / day)
Budesonide/ Beclomethasone 100-200 >200-400 >400
Fluticasone 100- 200 >200-500 >500
Ciclesonide 80-160 >160-320 >320
Salmetrerol Max 150 μg / day
Formoterol Max 24 μg / day
Table 3. Drugs used in asthma management
Grade* First choice Alternate choice
Intermittent Short acting β2 agonist when requiredNo controllers
Mild Persistent Low dose ICS LTRA/ SR theophylline
Moderate Persistent Low dose ICS + LABA or Low dose ICS+ LTRA/Medium dose ICS SR theophylline (SRT)
Severe persistent Medium dose ICS + LABA High dose ICS + LABAThen add LTRA/ SRTIf needed add oral steroid Anti-IgE (Omalizumab)
• At every grade of severity, avoid allergens / irritants and acute episodes should be managedwith reliever drugs as appropriate.
For children 5 years and younger, the besttreatment to control asthma is inhaledglucocorticosteroids.
Exacerbations of asthma (asthma attacks oracute asthma) are episodes of progressiveincrease in shortness of breath, cough, wheezing,or chest tightness, or some combination of thesesymptoms. Respiratory distress is common butneed not be always present.
In children above 5 years, after initiation oftreatment as discussed before, further dosing hasto be titrated depending on the level of control.
Monitoring is essential to maintain control andestablish the lowest step and dose of treatmentto minimize cost and maximize safety. Typically,patients should be seen one to three months afterthe initial visit, and every three months thereafter.After an exacerbation, follow-up should beoffered within two weeks to one month(Table 5).
a) If asthma is not controlled on the currenttreatment regimen, step up treatment. Generally,improvement should be seen within 1 month.If the control is not good, reassess and reconfirm
49

Indian Journal of Practical Pediatrics 2008; 10(3) : 240
the diagnosis, check compliance, eliminatetriggers, treat concurrent medical conditions, treatexacerbation and if required seek a secondopinion.
b) If asthma is partly controlled, considerstepping up treatment, depending on safety, costand patient’s satisfaction with the level of controlachieved. If nothing is contributory, increase thedose of steroids by 50% to a maximum dose thenadd on inhaled long acting β
2 agonist/ Oral
sustained release theophylline/ Oral steroid. Thenimmunotherapy/ immunomodulators agents likemethotrexate or anti IgE therapy (Omalizumab)can be tried.
c) If control is maintained for at least3 months, step down with a gradual, stepwisereduction to minimum dose possible in treatment,with the principle of tapering by 25-50%
reduction in dose of ICS and stopping medicationon the principle of last in first out basis. The goalis to decrease treatment to the minimummedication necessary to maintain control.
In most patients, the increase from a mediumto a high-dose of inhaled cocorticosteroid (ICS)provides relatively little additional benefit.Controller treatment can be stopped if thepatient’s asthma remains controlled on the lowestdose of controller and no recurrence of symptomsoccurs for one year.
In asthma, control is equated to cure and itis considered to be in control (remission) if thepatient is free from symptoms or not on any formof reliever or controller therapy for the last12 months. Monitoring is still necessary evenafter control is achieved, as asthma is a dynamicdisease and relapse or recurrence can happen.
Table 5. Assessment of levels of asthma control
Controlled Partly controlled Uncontrolled(All of the following) (Any measure present
in any week)
Daytime symptoms None More than twice/ week(twice or less/ week)
Limitation of activities None Any
Nocturnal symptoms/awakening None Any
Need for reliever None More than twice/ weekmedications (twice or less/ week)
Lung function Normal <80% predicted or(PEF/FEV
1) personal best
Exacerbations None One or more/ year†† One in any week**
Management options Continue the same/ Look up# or Step upStep down
#Check on compliance, trigger avoidance, diagnosis and co-morbid conditions††Any exacerbation should prompt review of maintenance treatment to ensure that it is adequate.
**An exacerbation in any week makes that an uncontrolled asthma week.
Three or morefeatures of partlycontrolled asthmapresent in any week
50

2008; 10(3) : 241
Points to Remember
• As asthma is characteristically episodicthere may not be any symptom or sign ofasthma.
• Proper clinical evaluation andcategorisation of cases is important formanagement.
• The ultimate goal of asthma managementis to achieve and maintain clinicl control.
• Successful pharmacologic managementaims at reversal and prevention of(a) acute and chronic airway obstruction,(b) avoidence of intra bronchial sequelae.
Bibliography
1. Mathur SK, Busse WW. Asthma: diagnosis andmanagement. Med Clin North Am 2006; 90:39-60.
2. Carroll W, Lenney W. Drug therapy in themanagement of acute asthma. Arch Dis ChildEduc Pract Ed. 2007; 92:82-86.
3. British Thoracic Society, National AsthmaCampaign, Royal College of Physicians ofLondon in association with the GeneralPractitioners in Asthma Group, BritishAssociation of Accident and EmergencyMedicine, British Paediatric Society, Royal
51
College of Paediatrics and Child Health. TheBritish guidelines on asthma management1995 review and position statement. Thorax1997; 52(suppl 1): s1-21.
4. Global strategy for Asthma Management andPrevention — revised 2006 (inwww.ginasthma.org
5. National Institutes of Health, National Health,Lung, and Blood Institute, National AsthmaEducation and Prevention Program, ExpertPanel Report 2. Guidelines for the Diagnosisand Management of Asthma. Washington, DC:U.S. Government Printing Office; 1997. NIHPublication No. 97-4051.
6. National Institutes of Health, National Health,Lung, and Blood Institute, NAEPP Expert PanelReport. Guidelines for the Diagnosis andManagement of Asthma: Update on SelectedTopics 2003. Washington, DC: U.S.Government Printing Office; 2002. NIHPublication No. 02-5075.
7. C Lemière, T Bai, M Balter, et al. On behalf ofthe Canadian Adult Consensus Group of theCanadian Thoracic Society. Adult AsthmaConsensus Guidelines Update 2003. Can RespirJ 2004; 11(Suppl A):9A-18A.
8. Indian Academy of Pediatrics- Nationalguideline. Asthma by Consensus. Consensusstatement on the diagnosis and management ofasthma in children- Update 2007.
NEWS AND NOTES
1ST CENTRAL ZONE CONFERENCE AND XXIX AP STATE CONFERENCE,
ANDHRA PRADESH
November 14-16, 2008
Contact
Dr.P.Venugopal
Organizing Secretary, Department of Pediatrics,
KGH, Maharanipeta, Visakhapatnam-530 002.
Andhra Pradesh, India.
Tel: 09848027203
Email: [email protected]

Indian Journal of Practical Pediatrics 2008; 10(3) : 242
URINARY TRACT INFECTION –
WHEN AND HOW TO EVALUATE?
* Vijayakumar M* Prahlad N
Abstract: Urinary tract infection in a growingchild can result in parenchymal damage and leadon to renal scars with resultant hypertension andend stage renal disease. Upper tract UTI andcomplicated UTI needs early and aggressivemanagement to reduce morbidity and mortality.Essential evaluation with ultrasonography,voiding cystourethrography and radionuclideimaging is the need of the day. Follow-upimaging to assess the progression of the diseaseand to document the efficacy of therapeuticintervention should be remembered. Correctusage of intravenous urogram and directradionuclide cystogram is needed. Voidingdysfunction needing urodynamic studies anduroflow EMG should not be forgotten in recurrentand complicated UTI. Asymptomatic bacteriuriain adolescent girls needs at least a goodultrasound to document anatomical anomaliesas renal scars are being documented in few ofthem.
Keywords: Urinary tract infection,ultrasonogram, radionuclide imaging, voidingcystourethrogram
Introduction
Urinary tract infection (UTI) and respiratorytract infections are common bacterial infections
in children. UTI in children is peculiar with itsvariable symptomatology. Acute presentation assepticemia is commonly seen with UTI in theneonatal period. Both acute and chronicpresentations of UTI are seen in infants and olderchildren. It is characterized by recurrences ininfants and young children and various urinaryanomalies and voiding dysfunctions, which aidin chronicity are commonly seen in childhoodUTI. High morbidity is usual with renal scarring,hypertension and chronic renal failure in chronicUTI1,2. Early diagnosis, most of the times onsuspicion, is mandatory for better managementso as to prevent the resultant mortality andmorbidity. Management of UTI in children isnot treatment alone and it involves steps toidentify the severity of acute damage and todocument associated anatomical or functionalanomalies. Steps includes investigations at theinitial stage for treating acute UTI followed bysubsequent evaluation to prevent scarring of thegrowing kidney in infants and young children.Investigations like ultrasonography, voidingcystourethrography and radio isotope imaginghave become useful and mandatory for a propermanagement of UTI in children3. Consensusstatement on management of UTI from IndianPediatric Nephrology Group has given clearguidelines to aim at correct management of UTIin children4. Individual unit’s experience is addedto the existing knowledge on evaluation ofchildhood UTI so that every child gets the priorityof adequate and aggressive initial managementfollowed by essential evaluation to make kidneysof children grow normally into adult kidneys.UTI in a child up to 2 years of age and if feasibleeven up to 5 years of age should be treated and
* Consultant Pediatric Nephrologist,Mehta Children’s Hospital,Chennai 600 031.
IAP-IJPP CME 2008
52

2008; 10(3) : 243
evaluated completely so as to reduce theparenchymal damage to the growing kidney.
Why should we evaluate UTI?
Delay in diagnosis results in delayedtreatment which causes extensive morbidity.Most of the times, this is due to vaguesymptomatology of UTI in infants and youngchildren. Young age, delay in initiatingantibacterial therapy, wrong choice of antibiotics,short duration of therapy, recurrences andassociated disorders like vesicoureteric reflux areessential risk factors for renal scarring1,5. About50% of the children with symptomatic UTI haverecurrences5. It was also documented that 10-25%of children with asymptomatic bacteriuriaacquire focal renal scars and a proportion developrenal stones, hypertension, chronic renal failureor complications of pregnancy1. Hospitalacquired infection should be always kept in mindespecially with indwelling urinary catheter.
UTI with lower tract symptoms like urgency,dysuria and pollakiuria due to inflammation ofbladder mucosa is called lower tract UTI orcystitis and is being described as dysuria-frequency syndrome. Usually fever is not therule. On the contrary features of upper tractinfection include fever, flank pain and systemicsymptoms. Upper tract infection is bacterialinfection of renal parenchyma and is termed acutepyelonephritis. Lower tract infection is commonin females and can be benign with less chance ofassociated anomalies. But upper tract infectionshould always be considered as malignantinfection and is usually associated with urinarytract anomalies. Asymptomatic bacteriuria issignificant bacteriuria without classicalsymptoms and diagnosed on routine screening.This is commonly seen in school going andadolescent girls. Upper tract infections, UTIassociated with anomalies and recurrent UTIconstitute complicated UTI. Second attack of UTIis usually termed as recurrent UTI. It is the
recurrence of symptoms and significant bacteriuria in a child who had previously recoveredclinically with appropriate treatment. The secondepisode (recurrence) may be early (relapse:within 2 weeks) or late (re-infection)6.
Unless the child with UTI is evaluatedcompletely treatment will not be adequate. Forexample, radio nuclide scan using Dimercaptosuccinic acid (DMSA) to document nucleopenicareas will be needed to document acute pyelonephritis in a child. This investigation is the goldstandard for evidence of pyelonephritis. But forthis investigation the child will not be treatedadequately for sufficient duration with thepresumption that it is a simple UTI. This isespecially so when the child becomes afebrileand asymptomatic within 3 or 4 days ofappropriate antibiotic therapy only to make thechild develop parenchymal damage and theresultant scars. DMSA scans are found usefuleven in culture negative UTI to document acutepyelonephritis7. A prospective study was doneby us to assess the frequency of acutepyelonephritis (APN) documented by Tc99mDMSA scintigraphy (DMSA) and the frequencyof vesicoureteric reflux (VUR) in febrile childrenwith positive urine culture.We also determinedthe frequency of APN, in febrile children withsupportive evidence for UTI but with negativeurine culture, as documented by DMSA andfrequency of VUR in them. This study stressedthe utility of DMSA to diagnose APN in urineculture negative febrile children and suggestedDMSA as a clinical tool in evaluation of fever ofunknown origin (FUO). This study included42 children with positive urine culture and26 children with negative urine culture who hadclinico-biological features of UTI as determinedby the predetermined criteria and diagnosed tohave APN by DMSA. The clinico-biologicalfeatures included febrile illness, renal angletenderness, toxic child, positive acute phasereactants, elevated total counts of WBC and
53

Indian Journal of Practical Pediatrics 2008; 10(3) : 244
polymorphonuclear leucocytosis. All of them hadultrasonogram (USG), DMSA and micturatingcystourethro-gram (MCU). They were followedup for a minimum period of 6 months. Out of the42 children with positive urine culture 92.9% hadfeatures of APN in the DMSA of whom 82.1%had vesicoureteric relux (VUR). The DMSA wasabnormal in 26 children with negative urineculture, of whom 65.4% had VUR. Ultrasoundsuggestive of parenchymal change was observedin 47.6% in the culture positive group and65.4% in the culture negative group.In conclusion, it was suggested, that DMSA isa useful investigation for the diagnosis of APNin febrile UTI. DMSA is indicated in febrilechildren with negative urine culture but withsupportive evidence of UTI and in FUO.An abnormal DMSA is a strong indicationfor work up for VUR7. Others investigationslike ultrasonogram done with the help ofa knowledgeable sonologist, voidingcystourethrogram, direct radionuclide cystogram,intravenous urogram, MRI urograms, etc are veryuseful to document associated anomalies and toprevent morbidity in the form of renal scars,hypertension and end stage renal disease.Appropriate usage of these imaging modalitiesshould be done for a better treatment of childhoodUTI.
Investigations
Collection of urine sample: Ideally clean catchmidstream urine specimen is useful andcontamination from periurethral flora should beavoided. If it cannot reach laboratoryimmediately, it should be stored at a temperatureof 4-80 C. In infants and young children whencollection of midstream urine sample is difficultor when contamination of culture is noted,suprapubic aspiration is ideal. Due to high falsepositive rates bag samples are not useful1. Morethan the positive culture the negative culture froma bag specimen is found useful in ruling out UTI.
Repeat cultures are indicated when contami-nation is suspected with mixed growth as wellas with growth of organisms normallyconstituting the periurethral flora likelactobacillus in healthy girls and enterococci ininfants and toddlers4.
Urinalysis: Mild proteinuria, leukocyturia (morethan 5 WBC/HPF in centrifuged urine and morethan 10 WBC/mm3 in uncentrifuged urine) andbacteria on Gram stain can indicate UTI4.Enhanced urinalysis using uncentrifuged urineand Neubauer counting chamber along withGram staining of urine sediment is found usefulto get at the suspicion of UTI early. More than10 WBCs/mm3 with a positive gram staining willindicate the possibility of UTI to a veryreasonable extent.
Rapid tests: The popular rapid tests like nitriteor Greiss test and leucocyte esterase tests haveproblems of false positivity and negativity.Bacterial enzyme nitrate reductase can convertthe urinary nitrate to nitrite, which can bedetected. If sufficient time is not allowed forincubation of bacteria with urine, the testsbecome negative as in children with increasedfrequency. If UTI is caused by a bacterium thatdoes not contain nitrate reductase as instreptococcal species, false negative results areseen. Similarly leucocyte esterase test detectsleucocytes in urine, which can be present in UTIas well as in other conditions like interstitialnephritis or glomerulonephritis. A better methodof utilizing these rapid tests is by getting acombined positive test for leucocyte esterase andnitrite in a child with clinico-biological featuresof upper tract UTI. A positive enhanced urinalysiswith positive rapid test will definitely indicateUTI with certainty.
Initial evaluation: This evaluation becomesmandatory even at the stage of initial diagnosisof UTI as this will give clues towards underlyinganomalies and seriousness of the UTI1,4.
54

2008; 10(3) : 245
Estimation of total and differential counts ofWBC, peripheral smear study, ESR andC-reactive protein (CRP) as acute phasereactants, are done for pointers for infection.Blood culture is done if acute pyelonephritis isconsidered. Renal dysfunction is assessed byblood urea and serum creatinine estimation.Ultrasound (USG) examination can be done atthis stage itself to rule out underlying anatomicaldefects to a reasonable extent in the beginningitself, which will help us to plan furthermanagement (Fig. 1-3). Good sonologist can giveideas on acute pyelonephritis by differentialnephromegaly or with increased echotexture ofone or both the kidneys which will guide us forearly suspicion on acute pyelonephritis. Presenceof VUR and scars can be documented byultrasound but a normal ultrasound will not ruleout them as USG is a poor test to indicate VURand renal scarring8.
Child gets adequate treatment for UTI as perdocumentation of it as acute pyenlonephritis ornot and as per age and symptomatology. Extendedspectrum beta lactamases (ESBL) producing
organisms grown in culture is increasingly beingdocumented and it needs adequate and aggressivetherapy. After making urine sterile there is a rolefor chemoprophylaxis in recurrent UTI,complicated UTI, UTI with VUR and/or DMSAshowing nucleopenic areas. The duration ofchemoprophylaxis is at least for 6 months to2 years or for up to the age of 5 years dependingon the background illness1,2.
Subsequent evaluation : In the recent past,diagnostic radiology has revolutionized theevaluation of childhood UTI dramatically. Moreimportance is given to children less than 5 yearswith UTI to reduce the renal damage in growingkidney. One should note that evaluation after thefirst episode and with recurrent episodes differs.Diagnostic radiology is aimed at identifying theunderlying anatomical defect predisposing torecurrent attacks of UTI and hence decides futurefollow-up strategy.
First episode: Ultrasound is needed in everychild with first attack of UTI1,3. MCU and DMSAare mandatory in children less than 2 years of
First UTI
Ultrasound
Normal Abnormal
< 2 yrs 2-5 yrs > 5 yrs > 5 yrs
MCU and DMSA scan No further MCU and DMSA scan MCU if scar on DMSA evaluation DMSA scan
or if DMSA not available
Fig 1. Investigation plan for UTI4
55

Indian Journal of Practical Pediatrics 2008; 10(3) : 246
age even if USG is normal for the first attack offebrile UTI1,3. We also feel that this principle canbe used even up to 5 years of age in whom theunderlying defects are being increasinglydetected which made us believe that in 2-5 yearsage group even if USG is normal one has to doDMSA scan. MCU is indicated if there is scaron DMSA scan or if DMSA scan facilities arenot available. In more than 5 years age groupwith first UTI with normal USG, no furtherevaluation is usually needed. If USG is abnormalin this group of more than 5 years of age, MCUand DMSA scan should be done4 (Fig.1).
The advantage of USG is that it can be usedat any stage of illness and can be done evenduring acute UTI and forms part of initialevaluation. Posterior urethral valve, post voidresidual urine, bladder hypertrophy, dilatation ofureters, ureterocele, hydronephrosis as well aspelvicalyceal anomalies can be detected. VURalso can be detected by an experiencedultrasonologist.
MCU is useful in detecting VUR, posteriorurethral valve (Fig.4&5), ureterocele and bladderor urethral diverticuli. For the fear of introducingsepsis, it is better avoided during acute UTI. Aftermaking urine sterile child is started onchemoprophylaxis and after 1-2 weeks MCU canbedonesafely. A single dose of 1 mg/kg/dose ofgentamicin given 60 minutes before doing MCUis found to be useful in our experience.
Renal scintigraphy using 99mTc- radio labeleddimercapto succinic acid (DMSA scan) shouldbe performed in every child below 2 years oras indicated.(Fig. 6-8). It can be done even duringacute phase and even with renal failure. It isbecoming a gold standard test for detecting acutepyelonephritis with documentation of cold areas.DMSA scan is an excellent method for detectingrenal cortical scars1.
If DMSA is showing cold areas/corticalscars but VUR is absent in MCU, direct
radionuclide cystogram (DRNC) is usually doneto pick up VUR as it is more sensitive than MCUin documenting VUR (Fig 9). It is always saferand wiser to do classical initially and only as perneed DRNC should be done in the initialevaluation. Unfortunately the grading of VURcannot be done precisely and posterior urethralanomalies cannot be detected by DRNC.
Recurrent UTI: It is very clear to every one thatchildren with recurrent UTI should have USG,DMSA and MCU irrespective of age to detectunderlying anatomical anomalies withoutambiguity. In hydronephrosis, DTPA (diureticrenography using 99mTc-labelled diethylenetriamine penta acetic acid) scan to assess thefunction of individual kidney and drainage of thedilated collecting system will be useful.Intravenous urogram (IVU) is being replaced byDTPA for this purpose.
Other investigations: Spinal dysraphism andradio opaque calculi are detected by X-ray of theKUB region. Need for IVU in UTI is very muchless with the availability of DMSA and DTPAscans. It is useful in double collecting systemevaluation and for delineating the level ofobstruction in obstructive uropathy associatedwith UTI (Fig 10). Areas of loss of renalparenchyma and clubbing and distortion ofcalyces as pointers for renal cortical scars can beidentified by IVU. Voiding dysfunction shouldbe remembered with recurrent and complicatedUTI and will need uroflow EMG and urodynamicstudies.
Follow-up: Urine culture negativity indicates asuccessful treatment. Urine culture every monthfor 3 months and then every 3 months for thefirst year is found useful. Urine culture is alwaysmandatory when child gets fever without focusand presenting with urinary symptoms with orwithout fever1. Children kept on long-termchemoprophylaxis need periodic follow-up.Repeat DMSA is done after 6 months to
56

2008; 10(3) : 247
Fig 2. USG showing dilated posteriorurethra, distended bladder with thickand trabeculated urinary bladder wall
Fig 4. MCU showing posteriorurethral valve and secondaryvesicoureteric reflux
Fig 5. MCU showing bilateral grade5VUR
Fig 7. Repeat DMSA after 6monthsshowing healing of acute pyelone-phritis shown in Fig.6
Fig 6. DMSA showing bilateral pyelo-nephritis with nucleopenic areas
57
Fig 3. USG showing left ureterocele

Indian Journal of Practical Pediatrics 2008; 10(3) : 248
Fig 8. DMSA showing small rightkidney with scars
Fig 10. Right megaureter in IVU
Fig 9. DRNC showing bilateralmassive VUR even in prevoid films
document resolution of inflammation and fordelineating scars if any. Follow-up DMSAs areneeded as and when indicated and followinginfection suggesting acute pyelonephritis. RepeatMCU or DRNC is needed after 1 year of follow-up to see for down grading of reflux and laterrepeated as per need. Repeat ultrasonogram toassess the growth of the kidneys is done atperiodic intervals of at least once a year for up to5-7 years of age, if child had renal scars in DMSAand/or VUR in MCU or DRNC in initialevaluation.
Conclusion
UTI in children is not uncommon. Think ofUTI in children with fever without focus or withfailure to thrive. Urine culture is still the goldstandard to diagnose UTI. USG in the initialevaluation of UTI is very much needed but is nota good tool for ruling out VUR and renal scars.DMSA radionuclide scan is the gold standard testfor acute pyelonephritis. We evaluate childrenwith first attack of febrile UTI with USG, DMSAand MCU as per indication. Consider DRNC
58

2008; 10(3) : 249
for follow-up of VUR children and in girls if theparents refuse MCU at the initial stage afterexplaining the inadequacies of DRNC indocumenting bladder and urethral anatomy.Voiding dysfunction is a problem to beconsidered in recurrent UTI and needs adequateevaluation.
Acknowledgement
We are thankful to Dr.BR Nammalwar,Pediatric Nephrologist, Mehta Children’sHospital, Chennai and Dr.V.Sripathi, PediatricUrologist, Mehta Children’s Hospital, Chennaifor their kind contribution in providing materialfor various figures quoted in the article.
Points to remember
• Every child less than two years with firstattack of UTI should have USG, MCU andDMSA to detect parenchymal damage andto document associated anatomicalanomalies. This strategy can be followedup to 5 years of age as increasing numbersof associated anomalies are being identifiedeven with fist attack of UTI in 2-5 years ofage group also.
• Children above five years of age with firstattack of UTI should have MCU andDMSA scan if ultrasound evaluation isabnormal.
• Children with recurrent UTI irrespectiveof age should have USG, MCU and DMSAas a policy.
• Direct radio nuclide cystogram (DRNC)can be used for follow-up of VUR childrenand not as the initial screening test as it isnot going to delineate urethral anatomy.
• Children with positive DMSA with negativeVUR by MCU should have DRNC todocument VUR in them.
References
1. Vijayakumar M, Prahlad N, Sharma NL,Nammalwar BR. Urinary tract infection (UTI).In: Suraj Gupte Ed, Recent advances inPediatrics-17 - Hot topics. 1
st Edn, Ed. Jaypee
Brothers Medical Publishers, New Delhi, 2007;pp 240-260.
2. Vijayakumar M, Prahlad N. Urinary tractinfection in children. In: Nammalwar BR,Vijayakumar M, (eds) Principles and Practiceof Pediatric Nephrology, 1
st Edn. Jaypee
Brothers, New Delhi, 2004; pp 348-356.
3. Kher KK, Leichter HE, Urinary tract infection.In: Kher KK, Makker SP (eds). ClinicalPediatric Nephrology. International edn, McGraw Hill, Inc Health Professions Division,New York, 1992; pp 277-321.
4. Indian Pediatric Nephrology Group: IndianAcademy of Pediatrics, Consensus statement onmanagement of urinary tract infection. IndianPediatr 2001; 38:1106-1115.
5. Bagga A, Sharma J. Urinary tract infection:Clinical features, evaluation and treatment.Pediatr Today 2000; 6:395-401.
6. Vijayakumar M, Bagga A. Reader’s Forum:Definition of recurrent UTI. Indian Pediatr2006; 43: 148-149.
7. Nammalwar BR, Vijayakumar M, Sankar J,Ramnath B, Prahlad N. Evaluation of the useof DMSA in culture positive UTI and culturenegative acute pyelonephritis. Indian Pediatr2005; 42: 691-696.
8. Veyrac C, Kotzki PO, Lopez C, etal.Comparison of ultrasound and dimercapto-succinic acid scintigraphy changes in acutepyelonephritis. Pediatr Nephrol 1999;13:219-222.
59

Indian Journal of Practical Pediatrics 2008; 10(3) : 250
ANTIMICROBIALS IN ACUTE
ENCEPHALTIS
* Viswanathan V
Abstract:Encephalitis in children is a commoncause for admissions to hospitals in India andthey present usually with fever, altered sensorium,seizures and other neurological signs. The mostcommon causes are usually viral like Herpes,Japanese B, mumps, varicella etc. More recentlyit has been recognized that Mycoplasmapnenumonia can present with encephalitis andthese children respond to treatment withAzithromycin. Management of these children ismainly supportive apart from acyclovir inchildren with suspected herpes encephalitis.
Keywords: Antimicrobials, Encephalitis,Mycoplasma infection
Encephalitis and meningitis are commoncauses of admission to hospitals in India. Theetiology for encephalitis and the differentialdiagnosis for these in our country differs slightlyfrom the western world although he overallclinical picture is very similar.
The word encephalitis is used when there isinvolvement of the brain parenchyma, cerebellumor the brain stem, where as in meningitis there isinflammation of the meninges only. Quite ofteninvolvement of both occurs and the termmeningoencephalitis is used.
Pathophysiology
Spread of infection can be through the bloodstream or through the endoneurium or theperineurium of the neuron as in the case of HSV,rabies or poliomyelitis.
Etiology
Acute encephalitis can occur in epidemics(Japanese B encephalitis, Chandipuraencephalitis) or sporadic of which Herpessimplex virus type I and II, cytomegalovirus,mumps, measles, varicella zoster, Epstein BarrVirus are most common.1 Mycoplasma
* Consultant Pediatric NeurologistKanchi Kamakoti Childs Trust Hospital,Chennai - 600 034.
IAP-IJPP CME 2008
Table 1. Encephalitis - Etiology andprodrome
• Japanese encephalitis (Epidemics) -high fever, headache
• HSV I and II - Fronto-temporal regions -olfactory, gustatory, bizzare behaviour,personality and memory alterations
• Enterovirus - cold, diarrhea, rash,abdominal pain
• Enterovirus 70 - preceding conjunctivitis,rash
• Adenovirus - respiratory symptoms, rash
• Measles - rash, conjunctivitis
• Mumps, EBV - parotitis
• CMV, Varicella - hepatitis, pneumonia,varicella inf.
• HIV - parotitis, lymphadenopathy
60

2008; 10(3) : 251
pneumoniae was reported as a probable orpossible etiologic agent in 70% of the childrenwho presented with acute encephalitis fromwhom an etiologic agent was identified in a studyfrom Canada2.
Clinical features
Fever, altered sensorium, focal findings likeaphasia, ataxia, hemiparesis, involuntarymovements, cranial nerve palsies, seizures, etc.are the usual findings. The prodromal featuresduring the illness may give a clue to the etiologyin these children as outlined in Table 1. Thesechildren may develop temperature dysregulation,SIADH or diabetes insipidus.
Seizures are usually in the form of recurrentpartial seizures or status epileptics with orwithout secondary generalization and associatedaltered mental status requiring hospitalization.The seizures are seen mostly during the acutephase of the illness but can be difficult to controlin some cases.
Studies suggest that most children whodevelop M.pneumoniae infection were older than5 years of age, where as children who werediagnosed to have HSV encephalitis wereyounger than 2.8 years of age.2
Investigations
CSF examination: Shows lymphocyticpleocytosis3,4 raised protein, normal sugar. RBC’sin the CSF may be seen in children with HSVencephalitis. The timing of the lumbar puncture(LP) is the difficult decision in these children asit may not be possible to consider the LP whenthe child presents with altered sensorium andfeatures of raised intra-cranial pressure.
CSF PCR for HSV, CMV, Varicella Zoster, EBVand entero-viruses is most helpful forconfirmation of diagnosis.
Serology : Paired samples of blood or CSF arerequired for a clear diagnosis and many a timeshave limited value, useful only for retrospectivediagnosis.
Neuro-imaging : CT brain may be easier to getfor practical reasons. Studies reveal that initialCT brain scans may be abnormal in 44% of thecases but subsequent scans increased theproportion of abnormalities to 69% during theperiod of hospitalization.5 MRI brain scans areparticularly helpful for differentiating acutedisseminated encephalomyelitis.6 Temporal lobewas commonly affected in children with HSVencephalitis although there were multifocalinvolvement in many as compared to adults whoshowed typical localization to temporal lobes.7
EEG : Very sensitive tool for diagnosing childrenwith encephalitis; showed abnormalities in morethan 87% of patients initially and in 96% duringthe course of their illness.2 Diffuse slowingtypically bilateral, was the most commonfinding.8 Periodic lateralized epileptiformdischarges (PLEDs) and Frontal or occipitalrhythmic delta activity (FIRDA or OIRDA) oftenoccur with HSV encephalitis.5
Differential diagnosis
Two main conditions that are treatable andmimic viral encephalitis are mycoplasmapneumoniae encephalitis and cerebral malaria.
Mycoplasma pneumoniaeencephalitis
Mycoplasma pneumoniae, a commonrespiratory pathogen has been implicated as anetiology of encephalitis. Clinically they aresimilar to enterovirus encephalitis, although theyfrequently require intensive care with prolongedhospitalization.9 Studies suggest that 1% - 10%of cases of acute childhood encephalitis arecaused by this organism.10
61

Indian Journal of Practical Pediatrics 2008; 10(3) : 252
Fever, lethargy, altered sensorium withassociated respiratory infection are the usualpresentation. The criteria for diagnosis ofprobable M.pneumoniae encephalitis includedthe detection of M.pneumoniae by culture or PCRof specimens from the throat, the CSF, or both toeliminate the potential impact of false-positiveserologic test results. The clinical manifestations,CSF abnormalities, EEG and neuroimagingfindings associated with M.pneumoniaeencephalitis are indistinguishable from those ofother viral encephalitis2, Antibiotic therapy hasbeen shown to suggest earlier recovery in thesechildren although conclusive evidence is stilllacking due to the small number of cases in thestudies so far.10 Macrolide antibiotics such aserythromycin and azithromycin, doxycycline orchloramphenicol have all been used for treatment.Neurologic sequelae have been reported in up to64% of the survivors in some studies followingmycoplasma encephalitis.10
Cerebral malaria
Common problem in our country, nearly40% of all the malaria is caused by plasmodiumfalciparum which is resistant to chloroquine.11
Mortality occurs mainly in children less than 5years. Fever altered sensorium, seizures,encephalopathy, retinal hemorrhages andinvolvement of other systems are the usualpresenting features. The detection of the parasitesin the thick blood smear is the gold standard fordiagnosis. Hypoglycemia is seen in close to 25%of these children and so needs to be watched forand corrected if it occurs. Apart from supportivetreatment quinine and artemesinin derivatives areeffective in treating this condition.
Management
Any child with suspected encephalitisrequires admission and close monitoring in anintensive care unit preferably, where frequent
monitoring of the level of consciousness can bedone along with anticipatory care for potentialcomplications. Supportive management is themost important treatment in acute encephalitis.
Seizures are common in these children andbenzodiazepines, phenytoin or phenobarbitoneare the anticonvulsants of choice as needed.These are given as a loading dose followed bymaintenance doses.
Increased intra cranial pressure contributessubstantially to the mortality and morbidity inencephalitis. Mechanical ventilation andintravenous Mannitol 1g/kg initially followed by0.25g/kg 4 to 6 hourly are very useful measuresin reducing ICP. close monitoring of the CVP,BP, fluid and electrolyte balance are importantin these children.
Patients with suspected or confirmed HSVencephalitis should receive IV Acycolovir 10mg/kg for 10 to 14 days at the earliest. varicellaencephalitis an uncommon complication of AIDsor immuno-compromised children should betreated with IV acyclovir in the same way for 10to 14 days. Gancyclovir is used if a child issuspected to have CMV encephalitis.
Points to Remember
• Viral encephalitis is a common problem inour country.
• CSF PCR for specific viruses is valuabletool in diagnosis.
• MRI brain scans may show multiple patchychanges in children with HSV encephalitisunlike adults.
• EEG is a very useful tool for diagnosis ofencephalitis.
• Mycoplasma pneumoniae encephalitis andcerebral malaria are important to considerin the differential diagnosis.
62

2008; 10(3) : 253
References
1. Rao PN, Kumar PA, Rao TA, et al. Role ofchandipura virus in an epidemic brain attack inAndhra Pradesh. Indian J Paediatr Neurol2004; 2: 131-143.
2. KolskiH Ford Jones, Richardson S, Prteic S,Nelson F, et al. Etiology of acute childhoodencephalitis at the hospital for Sick Children,Toronto, 1994-1995. Clin Infect Dis J1998;26:398-409.
3. Cizman M, Jazbec J. Etiology of acuteencephalitis in childhood in Slovenia. PaediatrInfect Dis J 1993;12:903-908.
4. Rantala H, Uhari M. Occurrence of childhoodencephalitis: a population based study. PaediatrInfect Dis J 1989;8:426-430.
5. Miller JD, Ross CA. Encephalitis: f afour yearsurvey. Lancet 1968;1:1121-1126.
6. Caldemeyer KS, Simth RR, harris TM, EdwardsMK. MRI in acute disseminated encephalo-myelitis. Neuro-radiology 1994;36:216-220.
7. Whitley RJ, Lakeman F. Herpes simplex virusinfections of the central nervous system:therapeutic and diagnostic considerations. ClinInfect Dis J 1995; 20:414-420.
8. Kennard C, SwashM. Acute viral encephalitis;its diagnosis and outcome. Brain 1981;104:129-148.
9. laura JC, Honarmand S, deborah F, et al.Pediatric Encephalitis: What is the role ofmycoplasma pneumoniae? Pediatrics2007;120:305-333.
10. Bitnun A, Lee E, Petric M, et al. Acutechildhood encephalitis and mycoplasmapneumoniae. Clin Infect Dis J 2001;32:1674-1684.
11. Kalra V. Practical paediatric neurology. AryaPublications.2002;pp97-99.
63
APLS: THE PEDIATRIC EMERGENCY MEDICINE COURSE
6th-7th December 2008
Organizer: IAP, Delhi and Center for Child Health, Sir Ganga Ram Hospital, Delhi
Venue: Auditorium, Working Women Hostel, Sir Ganga Ram Hospital, Delhi
Registration: Limited to 40 delegates,
Registration Fee: Rs 2000/- in favor of “Ambulatory Pediatrics”.
Course Director and Mailing Address
Dr Suresh Gupta,
Consultant,
Pediatric Emergency Medicine,
Centre for Child Health,
Sir Ganga Ram Hospital,
Rajender Nagar, Delhi 110060
Email: [email protected],
Phone: 9811426628, 28312591, 42251156
NEWS AND NOTES

Indian Journal of Practical Pediatrics 2008; 10(3) : 254
CYCLIC VOMITING SYNDROME
* Neelam Mohan** Bhat NK
*** Amit Gupta
Abstract : Cyclic vomiting is a syndromecharecterised by recurrent episodes of vomitinginterspersed with well intervals. It is consideredas a migraine variant with no clear etiology.Among various causes, altered intestinal motilityand mitochondrial DNA mutations are thoughtto play a role. Median age of onset is between5-7 years with slight female preponderance.Associated symptoms are abdominal pain,headache and autonomic symptoms. Infection,psychological stress and food products are someidentifiable precipitating factors. There is a longlist of differential diagnosis including surgicaland non-surgical causes of acute abdomen, CNSdisorders like brain tumor, ICP and porphyria.It is a diagnosis of exclusion by history, physicialexamination and laboratory studies.Management includes rehydration andantiemetics such as ondansetran. Majority ofthem improve as they grow into adolescence andone third of patients tranform themselves tomigraine headaches.
Key words : Cyclic vomiting, Migraine, Acuteabdomen, Ondansetron.
GENERAL ARTICLE
Cyclic vomiting syndrome (CVS) is aparoxysmal, severe, recurrent vomiting disorderof unknown etiology. It was first described in the19th century with earliest references being thatof Dr W Heberden in 1806 (French literature)and Dr Simuel Gee in 1882 (English literature).1,2
Li in 1995, described CVS as a unique temporalpattern of recurrent, discrete, and stereotypicalepisodes of explosive vomiting that punctuateperiods of completely normal health.3
Definition
Consensus diagnostic criteria wereestablished in 1994 at the First Internationalsymposium on CVS.4
Essential criteria : (a) Recurrent, severe,discrete episodes of vomiting, (b) Varyingintervals of normal health between episodes,(c) Vomiting episodes lasting from hours to daysand (d) No apparent cause of vomiting withnegative laboratory, radiographic, andendoscopic evaluation.
Supportive criteria : (a) Vomiting pattern isstereotypical, and each episode is similar in termsof time of onset, intensity, duration, frequency,associated symptoms, and signs within anindividual, (b) Vomiting pattern is self-limitedand episodes resolve spontaneously if leftuntreated, (c) Associated symptoms includenausea, abdominal pain, headache, motionsickness, photophobia and lethargy and(d) Associated signs include fever, pallor,diarrhea, dehydration, excess salivation, andsocial withdrawal.
* Consultant Pediatric Gastroenterologist,** Associate Consultant
Pediatric Gastroenterology, Hepatology,Nutrition and Liver transplantation unit,Center for Child Health,Sir Ganga Ram Hospital
*** Senior Resident, GTB Hospital, NewDelhi
64

2008; 10(3) : 255
Associations between CVS,abdominal migraine and migraine
CVS, abdominal migraine and migraineheadache all seem to be manifestations of thespectrum of migraine diathesis.5 Each is afunctional, episodic disorder with attacksseperated by symptom-free intervals. A patientwith any of these disorders may experienceheadache, abdominal pain, nausea and vomitingduring their attack. However, the distinction ofthese three syndromes is based on theirpredominant symptoms: headache predominatesin migraine; intense, sustained, midlineabdominal pain predominates in abdominalmigraine; and nausea and vomiting predominatein CVS.
Etio-pathophysiology
The etiology, pathophysiology, and targetorgan in CVS remain unknown. Renewed interestin CVS since 1990 has led to a flurry of researchover the last decade. Existing pathophysiologicalevidence points to CVS as a brain-gut disorderinvolving neuroendocrine pathways ingenetically predisposed individual.6,7,8 Supportexists for migraine-related mechanisms, aspatients with CVS have a significantly higherprevalence of family members with migraineheadaches epidodes5. Furthermore, one third ofpatients with CVS whose vomiting resolved,subsequently developed migraine headaches.Also 80% of CVS patients with positive familyhistory of migraine respond to antimigrainetherapy.
Proposed mechanisms by which CVS occursare based primarily on clinical observations ofCVS and related conditions.9 The commonlyproposed etiologies for CVS include hormonaldysfunction, gastrointestinal dysrhythmias,autonomic dysfunction, food allergy, mitochon-drial DNA mutation and ion channelopathies.
Endocrine factors
Infectious, psychological and physical stressare known triggers of episodes of CVS.4,9,10.It has been shown that ACTH, cortisol, andcatecholamine levels are elevated just prior tovomiting episodes in patients with CVS.8,9,11
According to Tache’s corticotropin-releasing-factor hypothesis, physical or psychologicalstress releases corticotropin releasing factor(CRF) from the hypothalamus which inducesgastric stasis, nausea and vomiting.6 CRF alsostimulates the anterior pituitary to secrete ACTH,thereby activating the hypophyseal-pituitary-adrenal axis (HPA) and the stress response. Basalsecretion of CRF has a diurnal rhythm withincreasing secretion beginning at 1 am, reachingits peak at 6am. This may account for thepredominance of night and morning times ofonset of CVS episodes. The CRF may bepotential brain-gut mediator of CVS and CRFreceptor antagonists (currently under develop-ment) can theoretically ablate an attack of CVS.6
Gastrointestinal motility disorders
Gastrointestinal motility dysfunction ispostulated as a possible etiology in CVS. It hasbeen shown that gastrointestinal dysmotility(hypermotility, hypomotility, or dysrhythmia)involving either the stomach or the small bowelis present even during asymptomatic periods inCVS patients.10 Also, the number of emeses inchildren with CVS has been reported to decreaseby administration of prokinetic agents.12
Autonomic nervous system
Autonomic dysfunction has been observedin patients with CVS and migraine.13,14 Many ofthe associated symptoms, such as pallor, flushing,fever, lethargy, salivation and diarrhea aremediated by the autonomic nervous system.However, it is unclear whether primary ANSabnormality results in CVS and migraine or if
65

Indian Journal of Practical Pediatrics 2008; 10(3) : 256
another disorder leads to an ANS abnormality incombination with either CVS or migraine.
Genetic associations
Mitochondrial DNA mutations may beinvolved in the pathogenesis of CVS.Boles et al have demonstrated that, amongchildren with CVS and neuromuscular disease,80% have maternal-side migraines.15,16 Mostcases of CVS have been described as sporadic,but family history may be an important factor.Several families, have been described withmultiple members involved.17-19 In these familialcases of CVS, the mode of inheritance ispredominantly matrilineal. This supports theBoles’ hypothesis that defects in mitochondrialenergy production due to mutations maypredispose to onset of episodes of vomitingduring periods of heightened demands for energy;for example, stress or excitement, in patients whomay be well compensated for usual dailydemands.8,15-20 Because the functional integrityof the gastrointestinal tract involves a great dealof interplay between smooth muscle and nervoustissues, gastrointestinal symptoms are oftenprominent in mitochondrial DNA disorders.16,20
Although universal genetic associations ofCVS are yet to be identified, case studies ofpatients and/or families have shown an A3243Gmitochondrial DNA mutation along with severalother less well-characterized mitochondrial DNAmutations exhibiting vomiting as a commonfeature.15,19
Allergy
Food allergy has been suggested as apossible etiology of CVS. Lucarelli, et al.evaluated eight children with CVS but nosymptoms of food allergy.21 Most of thesechildren had a positive skin prick test and thespecific IgE present for various foods, includingcow’s milk proteins, soy, and egg white.Elimination of the offending foods from diet led
to significant clinical improvement in their CVSsymptoms.
Mitochondrial enzymopathies
Renewed interest in mitochondrialenzymopathies and CVS, suggested that energysupply and demand might not be met undercertain circumstances in predisposedindividuals.15-19,22,23 This energy deficit can altervoltage-gated membrane channels for calcium,magnesium, and other ions. Some patients mayhave genetic mutations of various ion channels.Perturbations in delicate cellular electrochemicalgradients can result in depolarization andhyperexcitability of neurons that in turn couldlead to any of the above-mentionedneuroendocrine phenomena.
Demographics and epidemiology
CVS has been described in all races andethnicities, although whites appear to be affectedto a greater degree than other races.24 Theprevalence of CVS is not well studied . It isestimated to be 0.04% to 1.9% in children.24,25
CVS occurs in all age groups. Children as youngas 6 months and adults as old as 73 years havebeen described as having CVS.10,24 The medianage at onset of symptoms ranges from 5.2 to6.9 years.9,26 There is a slight femalepredominance (M:F 45:55).9
Symptoms
Each attack of CVS can be divided into fourphases. Recognition of this phasic pattern helpsin making the diagnosis and in management.
1. Prodrome phase: The patient senses theapproach of an episode during the prodromalphase, but is still able to take and retain oralmedications. Prodromal symptoms consist ofnausea, lethargy, anorexia, and pallor. This phase,which is often marked by abdominal pain, canlast from few minutes to several hours.
66

2008; 10(3) : 257
2. Vomiting phase: This consists of nauseaand vomiting; inability to eat, drink or takemedicines without vomiting; paleness;drowsiness and exhaustion.
3. Recovery phase: The recovery phasebegins as soon as nausea remits and ends whenthe patient has recovered appetite,color, strengthand body weight lost during the vomiting phase.
4. Interepisodic symptom-free phase.
The frequency of CVS episodes ranges from1 to 70 episodes per year with an average of12 episodes a year.26,27 The severity of CVS ismild if the illness doesn’t interfere with work orschool, moderate if attendance at work or schoolis in jeopardy, and severe if the patient isfrequently disabled and sick.
The symptoms which occur during theattack of CVS are as follows:9,26-30
a. Vomiting: It is present in all cases. Thevomiting in CVS typically is severe andintermittent with a peak rate of 12.6 emeses perhour. The median peak rate of emeses is 6 timesper hour during the attack. Only Bacillus cereusfood poisoning matches this high intensity ofemesis. The emesis is often projectile andfrequently contains bile, mucus, and blood.Vomiting peaks in the first hour and then beginsto decline over the ensuing 4-8 hours, lasting amean of 24 hours. Episodes commonly occur inthe early morning (2-4 am) or upon awakening(6-8 am). Forceful vomiting and retching oftencause hematemesis due to prolapse gastropathyor Mallory-Weiss tears. Peptic esophagitis andhemorrhagic lesions of the gastric mucosa aretypical endoscopic findings that result from,rather than cause, vomiting episodes.
b. Abdominal pain is present in 5%-80%of children and may initially be severe enoughto mimic acute abdomen.
c. Retching and nausea are frequentaccompaniments.
d. Signs and symptoms of an intense stressresponse are common, including increased heartrate and blood pressure, drenching diaphoresis,minor loose stooling, low-grade fever andneutrophilia.
e. Autonomic symptoms are also common,particularly lethargy, pallor, anorexia, increasedsalivation and social withdrawal. Lethargy maybe profound, and patients may be unable to walk,talk or may appear comatose.
f. Many patients with CVS haveneurologic symptoms, which supports therelationship between migraine and CVS.Symptoms include headache, photophobia,phonophobia and vertigo.
Precipitating events4,9,10,24,26,27,31
Most children (68-80%) can identify aspecific condition or event that triggered anepisode.The most common precipitating event isinfection, particularly chronic sinusitis.Psychological stresses and food products,including chocolate, cheese, and monosodiumglutamate (MSG), rank close behind chronicsinusitis. Others recognize physical exhaustionor lack of sleep, atopic events, motion sicknessand menses as triggers.
Differential diagnosis32-41
1. Gastrointestinal disorders (nonsurgical):Peptic ulcer disease, hepatitis, pancreatitis withor without pseudocyst, motility disorders,inflammatory bowel disease, infections(giardiasis, entamoeba, pinworms).
2. Gastrointestinal disorders (surgical):Pancreatic pseudocyst, recurrent subacuteappendicitis, bowel obstruction, intermittentduodenal intussusception, duodenal web/atresia/
67

Indian Journal of Practical Pediatrics 2008; 10(3) : 258
diverticulum, adhesions, choledochal cyst,cholelithiasis/gallbladder dyskinesia.
3. Urologic/renal/gynecologic disorders:Urolithiasis, reteropelvic junction obstruction,ovarian cyst, pregnancy, premenstrual syndrome.
4. Neurological disorders: Hydrocephalus,brain tumors, Arnold Chiari malformations,epilepsy, subdural hematomas or effusions,familial dysautonomia.
5. Endocrine disorders: Diabetes mellitus,adrenal insufficiency, pheochromocytoma.
6. Miscellaneous disorders: Abdominal,migraine/abdominal epilepsy, hypothalamicsurge, paroxysmal asthma, chronic sinusitis,benign positional vertigo, anxiety, depression,secondary gain, Munchasen-by-proxy.
A common diagnostic dilemma is todifferentiate CVS from chronic vomiting. Mostpatients with the chronic vomiting do not have acyclic pattern, usually vomit less then four timesan hour, are less likely to have autonomicsymptoms and often have no family history ofmigraine headaches.26,29,30
Diagnostic evaluation
CVS is a diagnosis of exclusion andrequires that other known and treatable causesof vomiting be excluded. When a patient presentswith acute vomiting, severe disorders can usuallybe excluded by history, physical examination, andbasic laboratory studies (such as a complete bloodcount and a complete metabolic panel includingliver function tests,renal function tests, amylase,and lipase, urinalysis, pregnancy test and anupper GI series/small bowel follow through).
Abdominal ultrasound of the liver, gallbladder, pancreas, kidneys, and adrenals may helpin evaluation of possible gallstones, pancreatitis,and ureteropelvic junction obstruction. An
endoscopic gastro duodenoscopy (EGD) needsto be performed in patients with acute vomiting,often for hematemesis or on clinical suspicionof peptic ulcer disease.
If the above tests are negative, structurallesions need to be excluded with imaging studiessuch as head and abdominal/pelvis CT. An EEGmay be obtained depending upon the clinicalsuspicion of seizure disorder.
In the case of patients presenting with cyclicsymptoms of vomiting, metabolic disordersincluding pituitary-adrenal disorders, organicacid and amino acid disorders need to be screenedfor.
Complications
Possible complications include dehydration,hypovolemic shock, electrolyte depletion, pepticesophagitis, hematemesis, Mallory-Weiss tear,tooth decay and secretion of inappropriateantidiuretic hormone.
Treatment
In the absence of known pathophysiology,treatment of CVS remains empiric. Treatment isusually individualized and often is a trial anderror process.9,26,27 Treatment is applied accordingto the phase the patient is in at the time ofpresentation. The goal during the prodromalphase is to abort the oncoming vomiting phase.The goal during the vomiting phase is to preventdehydration and terminate the nausea andvomiting. The goal of the recovery phase is torefeed the patient without causing a relapse ofnausea.42 The therapeutic goal during theinterepisodic phase is prophylaxis of furtherepisodes.
Prophylactic therapy to prevent CVS
Daily prophylactic pharmacotherapy maybe used to prevent episodes that occur more than
68
2008; 10(3) : 259
once per month or if they are extremely severeand disabling, (eg, lasting >3 days).42,43 Alongwith medical therapy, predisposing factors shouldbe identified and prevented. Prophylacticantimigraine medication should be considered,especially if patient has a family history ofmigraine headaches or if the episode is associatedwith symptoms of photophobia, phonophobia,scotomas, headache, or diplopia.9,44 Themainstays of prophylactic therapy includecyproheptadine, amitriptyline, propranolol,phenobarbital, and erythromycin.13,45-50 The NorthAmerican Society for Pediatric Gastroenterology,Hepatology, and Nutrition guidelines recommendcyproheptadine as first-line therapy in childrenyounger than 5 years. However, cyproheptadinecan cause substantial weight gain because of anincrease in appetite. Amitriptyline is the first-linechoice in children older than 5 years andadolescents.26
In sleep-deprived patients, restoration of anormal sleep pattern aids in preventing attacks.
If a CVS patient has an abnormal EEG,antiepileptic drugs such as phenobarbital,carbamazapine, and pizotifen have been shownto be effective.49,50
Abortive therapy for CVS
Abortive therapy is used during theprodromal phase when the patient begins to senseearly nausea signaling the approach of vomiting,but is still able to take and retain oralmedications.9,44,51
Patients should be kept in a dark, quietnonstimulating environment.29 Many antiemeticagents have been proven to be clinicallybeneficial; specifically ondansetron andpromethazine. Benzodiazepines may be used tohelp induce sleep and terminate the episode.9,45
Symptomatic treatment for pain, hypertension,diarrhea, headache, and heartburn may also benecessary.
Treatment during the vomiting phase
Dehydration requires correction withappropriate intravenous fluids. Serotoninantagonists, e.g., ondansetron, may beadministered as soon as restoration ofintravascular volume is well under way. Whenthe patient is normovolemic, attempt to terminatethe vomiting phase with intravenous lorazepamand ondansetron. If these measures abolish thesymptoms of the vomiting phase, and if relief issustained, the episode will have been terminated.
If the episode cannot be terminated, thepatient must then be relieved by giving sedatives.(e.g., chlorpromazine combined withdiphenhydramine).41 Try not to interrupt sleep forroutine vital signs and other procedures.
Psychiatric aspects of care
Help of a mental health professionalexperienced with CVS should be sought for thepatient and entire family.52
Prognosis27,31,52,53
Shared observations suggest that two-thirdof patients cease to have emetic episodes andremain asymptomatic whereas one-third patientsappear to transform emeses to migraineheadaches. Some patients progress through allthe three disorders: from CVS to abdominalmigraine to migraine headaches.
Most published series indicate that CVSlasts an average of 2.5-5.5 years, resolving in latechildhood or early adolescence. However,younger age at onset of CVS is likely correlatedwith a longer duration of illness. For age at CVSonset less than 3 year, 3-8 year, and greater that8 year reported lengths of illness are 5.8 year,4.9 year, and 2.9 year respectively and about 75%of patients eventually cease to vomit and havemigraines by 18 year of age.
69

Indian Journal of Practical Pediatrics 2008; 10(3) : 260
78% parents felt that the provision of apositive diagnosis and information made asignificant impact on the severity of vomiting.
Summary
CVS is an intermittent functional vomitingdisorder that affects individuals of all ages andis punctuated by variable duration ofasymptomatic periods. Etiology is yet to beidentified but present evidence points to maternalinheritance and mitochondrial DNA mutationsin some. A large number of CVS patients and/orfamily members are affected by other similarepisodic disorders of unknown etiology.Advanced CVS symptoms are more difficult totreat; therefore, clinicians should startsymptomatic treatment as soon as possible afterruling out other potential life-threatening causesof vomiting. Some CVS patients live relativelynormal lives and are free of symptoms in theiradulthood while others develop either abdominalmigraine or migraine headaches. Renewedinterest and research shall lead to moreknowledge and insight into CVS symptoms aswell as better options for prevention andtreatment in the future.
Points to Remember
• Consider cyclic vomiting in any childpresenting with recurrent vomiting.
• It is a diagnosis of exclusion after rulingout serious causes of acute abdomen andICP.
• Usual onset of symptoms is between 5-7years of age.
• Between the episodes child will enjoynormal health.
• In majority of them symptoms resolve byadolescence. One third of them developmigraine headace.
References
1. Heberden W. Commentaries on the history andcauses of diseases, 3rd Edn. London: Payne andFoss, 1806.
2. Gee S. On fitful or recurrent vomiting. St BartHosp Rep 1882;18:1-6.
3. Li BUK. Cyclic vomiting: the pattern andsyndrome paradigm. J Pediatr GastroenterolNutr 1995; 21 Suppl 1: S6-10
4. Li BUK (Ed). Cyclic vomiting syndrome.Proceedings of the 1st international scientificsymposium on cyclic vomiting syndrome heldat St. Bartholomen’s Hospital, London,England, July 1994. J Ped Gastro Nutr 1995;SZI and Li BUK, Sarna S, Issenman R (Ed).Proceedings of the 2nd International ScientificSymposium on CVS. Held at the MedicalCollege of Wisconsin, April 1998. Dig Dis Sci1999;44:S1-120.
5. Li BUK, Murray RD. Is cyclic vomiting relatedto migraine? J Pediatr 1999;134:567-572.
6. Tache Y. Cyclic vomiting syndrome: Thecorticotrophin-releasing-factor hypothesis. DigDis Sci 1999;44:S79-86.
7. Sato T, Igarashi N, Minami S, et al. Recurrentattacks of vomiting, hypertension and psychoticdepression: A syndrome of periodiccatecholamine and prostaglandin discharge.Acta Endocrinol (Copenh) 1988;117:189-197.
8. Boles RG, Adams K, Li BU. Maternalinheritance in cyclic vomiting syndrome. Am JMed Genetics 2005;133A:71-77.
9. Fleisher DR, Gornowicz B, Adams K, et al.Cyclic vomiting syndrome in 41 adults: Theillness, the patients and problems ofmanagement. BMC Med 2005;3:20.
10. Prakash C, Staiano A, Rothbaum RJ, et al.Similarities in cyclic vomiting syndrome acrossage groups. Am J Gastroenterol 2001;96:684-688.
11. Pasricha PJ, Schuster MM, Saudek CD, et al.Cyclic vomiting: Association with multiplehomeostatic abnormalities and response toketorolac. Am J Gastroenterol 1996;91:2228-2232.
70

2008; 10(3) : 261
12. Vanderhoof JA, Young R, Kaufman SS, et al.Treatment of cyclic vomiting in childhood witherythromycin. J Pediatr Gastroenterol Nutr1993;17:387-391.
13. Rashed R, Familioni BO, Abell TL, et al.Autonomic function in cyclic vomitingsyndrome and classic migraine. Dig Dis Sci1999;44:S74-78.
14. To J, Issenman RM, Kamath MV. Evaluationof neurocardiac signals in pediatric patients withcyclic vomiting syndrome through powerspectral analysis of heart rate variability. JPediatr 1999;135:363-366.
15. Boles RG, Williams JC. Mitochondrial diseaseand cyclic vomiting syndrome. Dig Dis Sci1999;44:S103-107.
16. Boles RG, Adams K, Ito M, et al. Maternalinheritance in cyclic vomiting syndrome withneuromuscular disease. Am J Med Geneti2003;120A:4744-4782.
17. Haan J, Kores EE, Ferrari MD. Familial cyclicvomiting syndrome. Cephalagia 2002;22:552-554.
18. Boles RG, Chun N, Senadheera D, et al. Cyclicvomiting syndrome and mitochondrial DNAmutations. Lancet 1997;350:1299-1300.
19. Salpietro CD, Briuglia S, Merlino MV, et al. Amitochondrial DNA mutation (A3243GmtDNA) in a family with cyclic vomiting. AmJ Pediatr 2003;162:727-728.
20. Wang Q, Ito M, Adams K, et al. MitochondrialDNA control region sequence variation inmigraine headache and cyclic vomitingsyndrome. Am J Med Genet A 2004;131:50-58.
21. Lucarelli S, Corrado G, Pelliccia A, et al. Cyclicvomiting syndrome and food allergy/intolerancein seven children: A possible association. Eur JPediatr 2000;159:360-363.
22. Goto Y, Nonaka I, Horai S. A mutation in thetRNA Leu gene associated with the MELASsubgroup of mitochondrial encephalomyo-pathies. Nature 1990;348:651-653.
23. Hirano M, Pavlakis SG. Mitochondrialmyopathy, encephalopathy, lactic acidosis and
stroke like episodes (MELAS): Currentconcepts. J Child Neurol 1993;9:4-15.
24. Li BUK, Misiewicz L. Cyclic vomiting: A brain-gut disorder. Gastroenterol Clin N Am2003;32:997-1019.
25. Abu-Arafeh I, Russel G. Cyclical vomitingsyndrome in children: A population based study.J Pediatr Gastroenterol Nutr 1995;21:454-458.
26. Li BUK, Balint JP. Cyclic vomiting syndrome:Evolution in our understanding of a brain-gutdisorder. Adv Pediatr 2000;47:1-44.
27. Fleisher DR, Matar M. The cyclic vomitingsyndrome: A report of 71 cases and literaturereview. J Pediatr Gastroenterol Nutr1993;17:361-369.
28. Stickler GB. Relationship between cyclicvomiting syndrome and migraine. Clin Pediatr2005;44:505-508.
29. Pfau BT, Li BU, Murray RD, et al.Differentiating cyclic from chronic vomitingpatterns in children: Quantitative criteria anddiagnostic implications. Pediatr 1996;97:364-369.
30. Li BUK, Fleisher DR. Cyclic vomitingsyndrome. Dig Dis Sci 1999;44:S13-18.
31. Li BUK, Hayes JR. Unpublished data, 1999.Cited by Li, BUK and Misiewicz, L. Cyclicvomiting: A brain-gut disorder. GastroenterolClin N Am 2003;32:997-1019.
32. Selimoglu MA. Myopathic cyclic vomitingsyndrome associated with gastroesophagealreflux and chronic sinusitis. J Pediatr2003;143:545.
33. Rasquin-Weber A, Hyman PE, Cucchiara S, etal. Childhood functional gastrointestinaldisorders. Gut 1999;45:SII60-1168.
34. Coker SB. Cyclic vomiting and the slit ventriclesyndrome. Pediatr Neurol 1987;187:297-299.
35. Jhonston JM, Harnsberger JK. Episodicvomiting due to intermittent duodenalintussusception. J Pediatr Gastroenterol Nutr1990;10:405-408.
36. Mira E, Piacentino G, Lanzi G, et al. Benignparoxysmal vertigo in childhood. ActaOtolaryngol 1984;406:S271-274.
71

Indian Journal of Practical Pediatrics 2008; 10(3) : 262
37. Meyers FA, Dempsy D, Caroline D, et al.Duodenal diverticulum as cause of cyclicvomiting. Dig Dis Sci 1989;34:1148-1149.
38. Schulte-Bockholt A, Kuqathasan S MesrobianHG, et al. Ureteropelvic junction obstruction:An overlooked cause of cyclic vomiting. Am JGastroenterol 2002;97:1043-1045.
39. Vinograd I, Lernau OZ, Frand M, et al.Fundoplication and pyloroplasty - a surgicaltreatment for intractable “cyclic vomiting” infamilial dysautonomia. J Pediatr Surg1982;17:80-81.
40. Li BUK, Murray RD, Heitlinger LA, et al.Heterogeneity of diagnoses presenting as cyclicvomiting. Pediatrie 1998;103:583-587.
41. Fleisher DR. Empiric guidelines for themanagement of cyclic vomiting syndrome.Available at: http://www.ch.missouri.edu/fleisher.
42. Li BU. Cyclic vomiting syndrome: a pediatricRorschach test. J Pediatr Gastroenterol Nutr1993 Nov; 17(4): 351-353
43. Li BU. Cyclic vomiting: new understanding ofan old disorder. Contemp Pediatr 1996; 13: 48-62.
44. Fleisher DR. Cyclic vomiting syndrome andmigraine. J Pediatr 1999;134:533-535.
45. Anderson J. Effective prophylactic therapy forcyclic vomiting syndrome in children usingamitriptyline or cyproheptadine. Pediatrie
1997;100:977-981.
46. Weitz R. Prophylaxis of cyclic vomiting withpropranolol. Drug Intellig Clin Pharmacol1982;16:161-162.
47. Forbes D, Withers G. Prophylactic therapy incyclic vomiting syndrome. J PediatrGastroenterol Nutr 1995;21:S57-59.
48. Prakash C, Clause RE. Cyclic vomitingsyndrome in adults: Clinical features andresponse to tricyclic antidepressants. Am JGastroenterol 1999;94:2857-2860.
49. Gokhale R, Huttenlocher PR, Brady L, et al.Use of barbiturates in the treatment of cyclicvomiting during childhood. J PediatrGastroenterol Nutr 1997;25:64-67.
50. Symon DN, Russell G. Double blind placebocontrolled trial of pizotifen syrup in thetreatment of abdominal migraine. Arch DisChildhood 1995;72:48-50.
51. Forbes D, Withers G, Silburn S, et al.Psychological and social characteristics andprecipitants of vomiting in children with cyclicvomiting syndrome. Dig Dis Sci 1999;44:S19-22.
52. Hoyt CS, Stickler GB. A study of 44 childrenwith the syndrome of recurrent (cyclic)vomiting. Pediatr 1960;25:775-780.
53. Hammond J. The late sequelae of recurrentvomiting of childhood. Develop Med ChildNeurol 1974;16:15-22.
72
5TH NATIONAL CONFERENCE OF CHILDHOOD DISABILITY GROUP,
MEERUT, UP
October 11-12, 2008
Contact
Dr.Priyanka Jain
(Developmental Pediatrician),
Organising Chairperson,
Jain Medical Center,
166, Civil Lines, Meerut (UP), India.
Mobile: 09927008961,
Web: http://www.iapcdg2008.com E-mail: [email protected]
NEWS AND NOTES

2008; 10(3) : 263
GENERAL ARTICLE
GENETIC COUNSELING FOR
PREVENTABLE DISORDERS
*Neerja Gupta* *Madhulika Kabra
Abstract: Rapid advances in the field of medicinehas led to recognition of more and more geneticdisorders. Most of the genetic disorders presentin childhood and the pediatricians are theprimary physicians involved in the diagnosis andmanagement. Hence, there is a strong need tounderstand the principles of genetic counselingwhich incorporates the knowledge about thegenetic basis of these disorders, chances ofrecurrence for individual disorders , the variousgenetic tests available and also the preventivestrategies.
Key words : Genetic counseling, Preventabledisorders
Advances in molecular genetics have led tothe completion of human genome project in2000-2003. New inventions are affectingmedical understanding of common as well as rarediseases. A major contribution of these advanceshas been in diagnosis, management and prenataldiagnosis of genetic disorders as treatment inmost cases is multidisciplinary, difficult, orimpossible and where available beyond the
means of most families. Genetic services are anexcellent example of preventive medicine. Thegenetic facilities are widespread in developedcountries. But in most of the developing countriesgenetic services are still unavailable or underdeveloped.The prevention of genetic disorderscould be effective at two levels, (a) Generalpopulation and (b) Families and individuals atrisk.
Prevention of genetic disorders may beachieved by
A. Identification of risk factors
1. Consanguinity
Since relatives share some of their genes bycommon descent, consanguineous matinginfluences the incidence of some inheriteddisease. The frequency of children with recessiveand multifactorial diseases in consanguineousmatings is high compared with nonconsan-guineous matings.
Consanguinity rate remains high in non-industrial countries which may be over 50% witha high inbreeding coefficient.
2. Advanced maternal age
Relation between advanced maternal ageand the occurrence of chromosomalabnormalities is present in all ethnic groups.
3. Previous affected family members
In these situations it may be easier toconvince relatives for genetic counseling.
* Senior Research Officer,Genetics Division,Department of Pediatrics
** Additional Professor,Department of Pediatrics,
All India Institute of Medical Sciences,New Delhi.-110029, India.
73

Indian Journal of Practical Pediatrics 2008; 10(3) : 264
B. Screening Programmes
Population screening
This is defined as the presumptiveidentification of the unrecognized diseases ordefects by certain tests, examination or otherprocedure that can be applied to sort outapparently well persons who probably have thedisease, from those who probably do not havethe disease. With better understanding of variousgenetic diseases public health applications havebeen developed. It is reasoned that all membersof a population at risk should be screened for agiven defect if treatment or preventive measuresare possible. Screening of certain genetic carrierstates has been recommended to allow geneticcounseling. These programmes are distinct fromthe usual retrospective genetic counseling. Asconsanguinity is important, a number of recessivediseases attain high frequencies in specialpopulation groups; hemoglobinopathies arefrequent in most South-Mediterranean , Arab andAfrican countries (Table 1).
Newborn screening
The objective is to screen all newborns fordisorders in which symptoms are not clinicallyevident until irreversible damage results andearly treatment can prevent or atleast amelioratethe consequences. For disorders likephenylketonuria, congenital hypothyroidism,hemoglobinopathies and congenital adrenalhyperplasia, newborn screening is universallyadapted by most developed countries. Suchprograms are going on in a few non industrialisedcountries, and remain limited to regions or tosmall size populations in developing countries.
Carrier/Heterozygote screening
Aim of the screeing is to identify all theindividuals who themselves are healthy but areat risk of having children with a severe autosomalrecessive or X linked illness. A heterozygote
screening programme should be implemented inpopulation with high frequency of carriers of aparticular disorder.
Following screening, carriers should becounseled regarding the genetic and medical risksof the disease and provided with informationregarding the various reproductive alternatives.Carrier couple should have access to appropriategenetic counseling and prenatal diagnosis. In ourcountry most couples come to know about theircarrier status after having an affected child.Unless an active carrier screening program is inplace it is unusual for a couple to learn that theyare at risk of having affected children. Premaritalknowledge of carrier status also is not free ofchallenges as the carrier state may be taken as ataboo and decision of a carrier not marrying acarrier, avoid having children or using alternativereproductive options is too personal an issue. Theonly viable option remains that if a carrier marriesanother carrier the couple should voluntarily optfor prenatal testing and selective termination ofaffected pregnancies. Couple should getcounseling before conception or early inpregnancy.
Prenatal screening
Various screening tests either invasive ornoninvasive can be done in any couple dependingupon the indication
Indications
1. Advanced maternal age
2. Previous child with any chromosomalabnormality
3. Previous child with a common singlegene disorder like thalassemia, CysticFibrosis(CF), duchenne muscular dystrophy(DMD), spinal muscular atrophy (SMA) ormultifactorial disorder like neural tube defects(NTD), cleft lip/palate
4. Abnormal USG in pregnancy
74
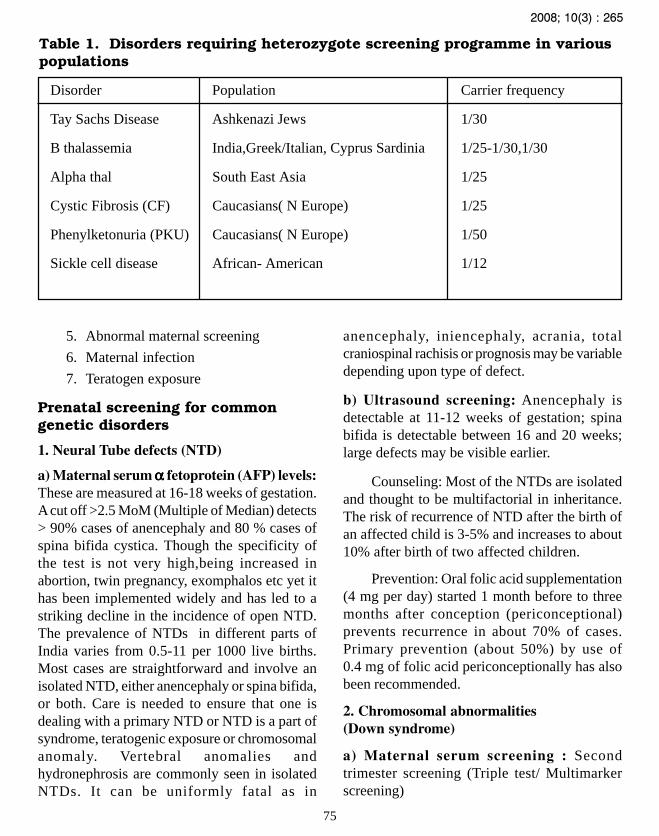
2008; 10(3) : 265
5. Abnormal maternal screening
6. Maternal infection
7. Teratogen exposure
Prenatal screening for commongenetic disorders
1. Neural Tube defects (NTD)
a) Maternal serum α α α α α fetoprotein (AFP) levels:These are measured at 16-18 weeks of gestation.A cut off >2.5 MoM (Multiple of Median) detects> 90% cases of anencephaly and 80 % cases ofspina bifida cystica. Though the specificity ofthe test is not very high,being increased inabortion, twin pregnancy, exomphalos etc yet ithas been implemented widely and has led to astriking decline in the incidence of open NTD.The prevalence of NTDs in different parts ofIndia varies from 0.5-11 per 1000 live births.Most cases are straightforward and involve anisolated NTD, either anencephaly or spina bifida,or both. Care is needed to ensure that one isdealing with a primary NTD or NTD is a part ofsyndrome, teratogenic exposure or chromosomalanomaly. Vertebral anomalies andhydronephrosis are commonly seen in isolatedNTDs. It can be uniformly fatal as in
anencephaly, iniencephaly, acrania, totalcraniospinal rachisis or prognosis may be variabledepending upon type of defect.
b) Ultrasound screening: Anencephaly isdetectable at 11-12 weeks of gestation; spinabifida is detectable between 16 and 20 weeks;large defects may be visible earlier.
Counseling: Most of the NTDs are isolatedand thought to be multifactorial in inheritance.The risk of recurrence of NTD after the birth ofan affected child is 3-5% and increases to about10% after birth of two affected children.
Prevention: Oral folic acid supplementation(4 mg per day) started 1 month before to threemonths after conception (periconceptional)prevents recurrence in about 70% of cases.Primary prevention (about 50%) by use of0.4 mg of folic acid periconceptionally has alsobeen recommended.
2. Chromosomal abnormalities(Down syndrome)
a) Maternal serum screening : Secondtrimester screening (Triple test/ Multimarkerscreening)
75
Table 1. Disorders requiring heterozygote screening programme in variouspopulations
Disorder Population Carrier frequency
Tay Sachs Disease Ashkenazi Jews 1/30
B thalassemia India,Greek/Italian, Cyprus Sardinia 1/25-1/30,1/30
Alpha thal South East Asia 1/25
Cystic Fibrosis (CF) Caucasians( N Europe) 1/25
Phenylketonuria (PKU) Caucasians( N Europe) 1/50
Sickle cell disease African- American 1/12

Indian Journal of Practical Pediatrics 2008; 10(3) : 266
It includes alpha fetoprotein (AFP), humanchorionic gonadotropin(hCG) and unconjugatedestriol(uE3)estimation in maternal serum.Expressed in multiple of median (MoM) values,maternal serum AFP and uE3 are reduced by 25%whereas hCG levels are doubled in pregnancieswith Down syndrome. None of these parametersalone gives absolute discrimination but takentogether they provide a means of modifying awoman’s prior age related risk to give an overallprobability that the unborn is unaffected.Whenthis probability exceeds 1 in 250, invasive testingin the form of amniocentesis or placental biopsyor cordocentesis is offered. Disadvantages ofsecond trimester screening is that it creates moreanxiety and late intervention if fetus is affectedposing risk to mother. First trimester screeningusing β hCG and pregnancy associated plasmaprotein A (PAPP-A) has been advocated recentlywith similar sensitivity and advantage of earlydetection.
Now a days the concept of one stop clinicfor assessment of risk for fetal anomaly (OSCAR)is prevalent in western countries. It means thatin one hour single visit both the biochemical(βhCG, Pregnancy associated plasne protein APAPP-A) and USG (Nuchal translucency (NT)+ crown rump length (CRL) + anomaly scan) iscarried out between 11-14 weeks. It has apredictive value of 86%.b) Ultrasound screening: Routine fetal anomalyscan is done at 16-18 weeks to look at the majormalformations. Significant sonographic findingsare seen in nearly all fetuses with trisomy 13,77-100% of trisomy 18 and 33-50% of fetus withDown syndrome. Presence of multipleabnormalities raises the risk of chromosomalabnormality to 35%.3. Single gene disorders (Thalassemia,Cystic fibrosis,spinal muscular atrophy, etc)
Most important in this group is thalassemiaespecially in North India.Screening protocol is shown in Fig. 1
Pre-test and post test counseling
Preliminary genetic counseling ofcandidates who desire prenatal diagnosis usuallydeals with the following: a) The risk that the fetusis affected, (b) The nature and probableconsequences of the specific problem, (c) Therisks and limitations of the procedures to be used,(d) The time required before a report can beissued, (e) The possible need for a repeatprocedure in the event of a failed attempt and(f) The limitation of a test (in view of lab error).
Definition and aims of geneticcounseling
The American Society of Human Genetics(ASHG)1 defined genetic counseling as acommunication process that deals with the humanproblems associated with the occurrence or therisk of recurrence of a genetic disorder in afamily. The process involves an attempt by oneor more appropriately trained persons to help theindividual or family to understand the problem,choose a course of action and adjust to thesituation.
Understand
a) The diagnosis, prognosis and availablemanagement
b) The genetic basis and chance of recurrence
c) The options available (including genetictesting) for dealing with the risk ofrecurrence
Choose
The course of action appropriate to theirpersonal and family situation and their ethicaland religious standards and act in accordancewith the decision
Adjust
To the psychosocial impact of the geneticcondition in the family.
76

2008; 10(3) : 267
Non pregnant woman Pregnant womanMCV & MCH
MCV<80fland/or MCH<27pg
HbA2 Estimation and Hb
No Yes electrophoresis
HbA2 > 3.5% and/or abnormal Hb
No Yes
HbA2 and Hb electrophoresis
of spouse
Spouse if β thalassemia carrier orabnormal Hb carrier
Reassurance No YesNo risk of child with Thalassemia major
Counsel for risk of β thalassemia+ prenatal diagnosis
Fig.1. Screening protocol for thalassemia.
77

Indian Journal of Practical Pediatrics 2008; 10(3) : 268
While genetic counseling is a compre-hensive activity, the particular focus willdepend upon the family situation. A pregnantcouple at high genetic risk may need to makeurgent decisions concerning prenataldiagnosis; parents of a newly diagnosed childwith a rare genetic disorder may be desperatefor further prognostic information, while stillcoming to terms with the diagnosis; a youngadult at risk of a late onset degenerativedisorder may be well informed about thecondition, but require ongoing discussionsabout whether to go ahead with a presympto-matic test; and a teenage girl, whose brotherhas been affected with an X linked disorder,may be apprehensive to learn about theimplication for her future children. Being ableto establish the individual’s and the family’sparticular agenda, to present information ina clear manner, and to address psychosocialissues are all crucial skills required in geneticcounseling. Indications for genetic counselingare given in Table 2.
When to suspect a genetic disorder
Genetics in Primary Care (GPC) FacultyDevelopment Initiative have endorsed theconcept of developing a simple set of red flagsthat could alert clinicians to the possibility ofgenetic condition. The working group definedthe red flag as any clinical finding discoveredin history, physical examination, or laboratorystudies that suggests the presence of agenetically influenced disease and that mayrequire further action such as intervention,counseling, referral, screening or follow-up.These are not 100% sensitive or specific, butshould raise a clinician’s sensitivity to geneticinfluences on their patients. One can memorizethese genetic red flags by a mnemonic-”FamilyGENES”.
‘F’Family history to look for any otheraffected member in single or multiple generation
Table 2. Indications of geneticcounseling
• History of a previous child or family historyof unexplained mental retardation/dysmorphism/multiple malformations
• History of a previous child or family historyof degenerative brain disease-regression ofmile stones
• Acutely sick neonate or infant, failure tothrive, recurrent vomiting, acidosis,convulsions
• Neuromuscular disorders
• Childhood deafness
• Down syndrome and other chromosomaldisorders
• Relatives of a person with chromosomaltranslocation
• Exposure to teratogens
• Unexplained still birth/s with or withoutcongenital malformation
• Skeletal dysplasia (Proportionate/disproportionate short stature)
• Ambiguous genitalia, primary amennorhea,infertility
• Familial cancers and cancer prone disease
• Single gene disorder like thalassemia, Spinalmuscular atrophy, hemophilia or familypedigree suggestive of a typical pattern ofinheritance(AR, AD, X linked)
• Multifactorial/polygenic-Hypertension,diabetes, obesity, psychotic disorders
• Consanguineous marriage
• Advanced maternal age
• Positive maternal serum screen
• Patient or family member with a knownmendelian disorder
• Previous child with a chromosomal disorder
• Abnormal USG findings
• Recurrent pregnancy loss/still births
78

2008; 10(3) : 269
to establish a particular pattern of inheritance likeAR, AD, etc. However, lack of family historydoes not rule out genetic cause.
‘G’ Group of congenital anomalies.A patient with three or more minor congenitalanomalies warrants additional evaluation to lookfor a major anomaly like structural heart, kidneyor cerebral defect. Single minor anomalies occurin approximately 15% all newborns. Presenceof 3 or more anomalies is unusual and present in1% of all newborns.
‘E’ Extreme or exceptional presentation ofcommon conditions. Early onset of disease orunusual severe reaction to infective or metabolicdisease.
‘N’ Neuro-developmental delay orregression in children, or early onset neurologicdeterioration in adults. Increasing severity ofneurologic disease, association with otherunusual findings like facial dysmorphism andearly onset increase the likelihood of anunderlying genetic cause for any given neurologicabnormality. Recent evidence suggests that atleast 15-20% of mental retardation (MR) iscaused by identifiable genetic problem.Chromosomal abnormalities are seen in 4-28%of children with MR. However, manyneurogenetic conditions are associated with fewor no non-neurologic findings like spinalmuscular atrophy and spinocerebellar ataxias.
‘E’ Extreme and unusual pathologicfindings. Bilaterality of pathologic findings inpaired organs or structure is considered anextreme presentation and is suggestive of a strongrole for genetic factors e.g. bilateral breast cancercorrelate strongly with autosomal dominantmutations in BRCAI and BRCA2 genes.Likewise the appearance of multiple primaryneoplasms in the same person is a red flag.Physician in practice and training shouldrecognize these unusual findings for pursuing
a genetic diagnosis especially because earlydiagnosis may enable effective surveillance andprevent complications.
‘S’Surprising lab values in healthy patientsmay precede the onset of clinical symptoms of adisorder. Two important examples are highcholesterol in familial hypercholesterolemia andhigh serum transferrin saturation or ferritin levelin hereditary hemochromatosis. In such casesearly diagnosis of a hereditary condition can leadto prevention of the serious, irreversibleconsequences of untreated disease.
Steps in evaluation of a child withgenetic disorder
1. History with particular emphasis onpedigree construction and analysis (see Box 1&2)
2. Detailed clinical examination
3. Diagnosis
4. Management with strong emphasis ongenetic counseling regarding recurrence risk andprenatal diagnosis if possible.
1. History and pedigree analysis
• Draw at least 3 generation pedigree usingstandard set of symbols (Box 1&2 )
• Male lines are placed on left
• All the members of same generation areplaced on same horizontal levels
• Roman numerals indicate generations andArabic numerals indicate each individualwithin a generation
• Write name and age of each member ofpedigree
• History suggestive of maternal infections orantenatal drug exposure
• Developmental milestones
79

Indian Journal of Practical Pediatrics 2008; 10(3) : 270
• Identify consanguineous marriages,miscarriages, infertility, congenitalmalformations, and similarly affectedindividuals in a family
• Identify pattern of inheritance dependingupon the detailed history
2. Clinical examination
• Complete anthropometric measurementsalong with percentile depending upon thesuspected disorder
• Head to toe examination for facialdysmorphism, any skin abnormalities, anymalformation or deformities
• Any dysmorphic facial features with relevantfacial measurements
• Presence of any minor or majormalformation or neurocutaneous stigmata
• Complete general and systemic examination
• Clinical photograph of the patient
• Examination of parents
3. Diagnosis
A) Clinical
i. Syndromic diagnosis is based on identificationof known syndromes based on the clinicalphenotype. There are excellent texts available forunderstanding this interesting field of clinicalgenetics. In addition, there are computerdatabases available for syndrome search such asLondon Dysmorphology Database and Picturesof Standard Syndromes and UndiagnosedMalformations (POSSUM). Referring to thebooks giving detailed descriptions of syndromesand diagnostic approaches is also of greathelp4-8.
ii. Chromosomal (to be confirmed bycytogenetic analysis)- Important indicators of achromosomal abnormality are failure to thrive,
presence of dysmorphism, confirmation orexclusion of the diagnosis of knownchromosomal syndromes, for example DownSyndrome, unexplained mental retardation withor without dysmorphism, multiple malformationsyndrome, X-linked recessive syndromemanifesting in a female, two or more than twomonogenic disorders in a patient, pregnancy at arisk of aneuploidy because of previouschromosomally abnormal child, abnormalmaternal serum screening, advanced maternalage, or abnormality detected on fetal ultrasoundscanning, abnormalities of sexual differentiationand development, infertility, recurrentmiscarriages or still births.
iii. Single gene disorder(Thalassemia, SMA,DMD, Neurometabolic disorder, etc)
B) Laboratory
a. Cytogenetic (Conventional/High Resolutionbanding HRB) and /or fluorescence insituhybridization (FISH) if a specific microdeletionsyndrome is suspected. 2 ml blood in heparin isrequired and should be sent to lab within 24hours.
b. Molecular studies for a specific suspectedsingle gene disorders DNA diagnostic tests areextremely important for prenatal diagnosis andcarrier detection. Presently DNA diagnosis forthalassemia, hemoglobinopathies, hemophilia,Duchenne muscular dystrophy, fragile-X-mentalretardation, cystic fibrosis, megalencephalicleucodystrophy and spinal muscular atrophy areavailable in India. For providing prenataldiagnosis, the DNA diagnosis of the affectedchild in the family needs to be done beforehand.Sample for molecular tests should be saved inEDTA vials. Unless the type of mutations in theproband or carrier parents is identified, prenataldiagnosis is not feasible. It is limited by high cost,genetic heterogeneity, and ethnic difference ofdisease prevalence.
80

2008; 10(3) : 271
c. Enzyme studies for lysosomal storagedisorders like Gaucher disease, mucopoly-saccharidosis
Nondirectiveness in geneticcounseling
The main principle of genetic counseling isnondirectiveness which is the art of presentingfacts without influencing decision. It promotesthe autonomy or self determination and personalcontrol for the client. To maintain the sense ofpsychological well being amongst the clients,genetic counseling has also been defined as adynamic psycho educational process centered ongenetic information. With a therapeuticrelationship established between providers andclients, clients are helped to personalize technicaland probabilistic genetic information, to promoteself determination and to enhance their ability toadapt over time. The goal is to facilitate client’sability to use genetic information in a personallymeaningful way that minimizes psychologicaldistress and increases personal control. Itpromotes understanding, decision making,personal control, adaptation to stress inducingevents and reduces psychological distress.
As it is evident genetic counseling is acomplex process and ideally requires thefollowing: (a) Correct diagnosis, (b) Trainedcounselor with good knowledge of geneticsand excellent communication skills and(c) Psychosocial support to the family in copingup with the disorder and making decision withnon directive counseling.
The person who seeks genetic counselingis called the consultand or counselee and the onewho gives it is the counselor. In addition tomedical specialists, trained persons with variousbackgrounds like nursing, social work educationand psychology can function as geneticcounselors.
Psychosocial issues
The psychosocial impact of a geneticdiagnosis for affected individuals and theirfamilies cannot be over emphasized. Thediagnosis of any significant medical conditionin a child or adult may have psychological,financial and social implications, but if thecondition has a genetic basis a number ofadditional issues arise. These include guilt andblame, the impact on future reproductivedecisions and the genetic implications to theextended family.
Guilt and blame: Feelings of guilt arise inrelation to a genetic diagnosis in the family inmany different situations. Parents very oftenexpress guilt at having transmitted a geneticdisorder to their children, even when they hadno previous knowledge of the risk. On the otherhand, parents may also feel guilty for havingtaken the decision to terminate an affectedpregnancy. Healthy members of a family may feelguilty that they have been more fortunate thantheir affected relatives and at-risk individualsmay feel guilty about imposing a burden ontotheir partner and partner’s family. Although inmost situations the person expressing guilt willhave played no objective causal role, it isimportant to allow him or her to express theseconcerns and for the counselor to reinforce thatthis is a normal human reaction to thepredicament. Blame can sometimes occur infamilies where only one member carries thegenetic risk (“It wasn’t our side”), but again thisis less likely to occur when the genetic situationhas been explained and is understood.
Reproductive decision making: Couples awareof an increased genetic risk to their offspring mustdecide whether this knowledge will affect theirplans for a family. Some couples may be facedwith a perplexing range of options includingdifferent methods of prenatal diagnosis and the
81

Indian Journal of Practical Pediatrics 2008; 10(3) : 272
use of assisted reproductive technologies. Forothers the only available option will be to choosebetween taking the risk of having an affectedchild or remaining childless. Couples may needto reconsider these choices on repeated occasionsduring their reproductive years. Decision makingmay be more difficult in particular circumstances,including marital disagreement, religious orcultural conflict, and situations where theprognosis for an affected child is uncertain. Formany genetic disorders with variable severity,although prenatal diagnosis can be offered, theclinical prognosis for the fetus cannot bepredicted. When considering reproductivedecisions, it can also be difficult for a couple toreconcile their love for an affected child or familymember, with a desire to prevent the birth of afurther affected child.
Impact on the extended family: Theimplications of a genetic diagnosis usuallyreverberate well beyond the affected individualand his or her nuclear family. For example, theparents of a boy just diagnosed with Duchennemuscular dystrophy will not only be coming toterms with his anticipated physical deterioration,but may have concerns that a younger son couldbe affected and that daughters could be carriers.They also face the need to discuss the possiblefamily implications with the mother’s sisters andfemale cousins who may already be having theirown children.
Bereavement: Bereavement issues arisefrequently in genetic counseling sessions. Thesemay pertain to losses that have occurred recentlyor in the past. A genetic disorder may lead toreproductive loss or death of a close familymember. The grief experienced after terminationof pregnancy following diagnosis of abnormalityis like that of other bereavement reactions andmay be made more intense by parents’ feelingsof guilt. After the birth of a baby with congenitalmalformations, parents mourn the loss of the
imagined healthy child in addition to theirsadness about their child’s disabilities, and thischronic sorrow may be ongoing throughout theaffected child’s life.
Long-term support and follow up: Mostfamilies will require ongoing information andsupport following the initial genetic counselingsession, whether for coping with an actualdiagnosis or the continued risk of a geneticdisorder.Follow up sessions may be needed toreinforce the informations (usually forgotten orwrongly remembered by the consultands), toanswer new queries, to provide latest informationand to provide psychological support to thefamily during the process of coping up, till theacceptance and adjustments take place.
Counseling before genetic testing
Genetic counseling is an integral part of thegenetic testing process and is required becauseof the potential impact of a test result on anindividual and family, as well as to ensureinformed choice about undergoing genetictesting. The extent of the counseling and theissues to be addressed will depend upon the typeof test being offered, which may be diagnostic,presymptomatic, carrier or prenatal testing.
Though many genetic disorders can besuspected and finally diagnosed by molecular/cytogenetic or enzyme estimation tests, most ofthem are without any treatment or the treatmentis expensive. As a result carrier detection,antenatal screening, prenatal diagnosis followedby termination of pregnancy in case of affectedchild remains the only option. Management andcounseling depending upon the type of geneticdisorders is given below.
1) Mendelian disorders: For most of thecommon genetic single gene disorders eitherenzyme based or molecular diagnosis is availablethough facilities for diagnosis of all disorders arenot available in our country.
82

2008; 10(3) : 273
a) Neurogenetic disorders (Single gene):
There are a multitude of neurogeneticdisorders (NGD) and the number is increasingdue to identification of new genes. Counselingis easier if the inheritance is known but becomescomplex if the etiology is multifactorial/polygenic. In the latter situation most of the timesone has to resort to empiric risk figures forcounseling.
There are some well known neurogeneticdisorders with classical Mendelian inheritance.If a confirmed diagnosis of any of these disordersis possible then counseling and prenatal diagnosisis straight forward. Problems arise due to aphenotypic overlap of many of these disorders,non availability of diagnostic modalities andgenetic heterogeneity. Hereditary ataxias areimportant example : more than 50 syndromeshave been described with almost all types ofinheritance patterns. Following are somecommon single gene neurogenetic disorders.
i) Autosomal recessive: Majority ofneurometabolic disorders (eg. phenyl ketonuria,maple syrup urine disease, biotinidase deficiency,methyl melonic aciduria, etc), lysosomal storagedisorders (MPS other than Hunter syndrome,Gaucher’s type2&3, Niemann Picks disease, etc),neuromuscular disorders like SMA etc.
ii) Autosomal dominant disorders :Huntingtons disease, Myotonic dystrophy,Tuberous sclerosis, Neurofobromatosis, etc.
iii) X-linked disorders: Duchenne musculardystrophy, Fragile X syndrome, Menke’s Kinkyhair disease, Pelizaeus Merzbacher disease ,Ornithine transcarbamylase deficiency, Rettsyndrome, etc.
iv) Mitochondrial Disorders: MERRF,MELAS, KSS, etc.
In single gene disorders, the risk ofrecurrence will depend on the type of inheritance.
In an autosomal recessive disorder risk ofrecurrence is 25% for the sibling. In autosomaldominant disorder the risk of recurrence for thesib is 50% if one of the parents is affected. If itis a sporadic case (new mutation) risk ofrecurrence in sib is very low but gonadalmosaicism cannot be ruled out. In X-linkedrecessive disorders, risk of recurrence for boysis 50% where as females usually do not manifest.
b) Hemoglobinopathies
In most of the common haemoglobinopathies likealpha, beta thalassemias and sickle cell anemiathe mode of inheritance is autosomal recessive.Autosomal recessive disorders manifest if boththe parents are carrier of the mutant gene. Thedisease usually occurs in one generation only.The risk of occurrence and recurrence is 25% insuch cases (Fig.2). Identification of mutation insuch couples or proband is a prerequisite forprenatal diagnosis. So, to have an affected childboth parents need to be carriers and prenataldiagnosis is also indicated in this situation.
There is no risk of having an affected childif only one partner is a carrier or is affected(Figs.3 and 4). If only one partner is a carrierthere is a 50% chance of the baby being a carrierand all babies will be carriers if one partner isaffected with an autosomal recessivehemoglobinopathy. Identification of carrierstatus is easy and is possible by measurement ofHbA
2 which is almost always high in carriers
except in a rare situation of silent carrier statuswhen HbA
2 may be normal and carrier status can
only be confirmed by molecular studies.
In X-linked recessive disorders, risk ofrecurrence for boys is 50% where as femalesusually do not manifest. Majority of geneticdiseases exhibit genetic heterogeneity wheredifferent gene mutations lead to identicalphenotype.
83

Indian Journal of Practical Pediatrics 2008; 10(3) : 274
Fig.2. 25% Risk of affected child if both parents are carrier
Fig.3. No risk of affected child if only one parent is carrier
Fig.4. No risk of affected child if one parent is affected
Affected
Carrier
Normal
84

2008; 10(3) : 275
Table 3. Empiric risk of recurrence of isolated malformation
Malformation Frequency per Recurrence for normal1000 births parents of one affected child
Anencephaly/Spina bifida 4 – 5 5 %
Cardiac malformation 6 – 8 3 – 4 %
Cleft lip and cleft palate 2 4 – 5 %
Cleft palate alone 0.5 2 – 6 %
Pyloric stenosis 2 – 3 3 %
Talipes equinovarus 3 – 4 2 – 8 %
Dislocation of hip 3 – 4 3 – 4 %
Hischsprung disease 0.1 6 %
For most of the common single genedisorders either enzyme based or moleculardiagnosis is available though facilities fordiagnosis of all disorders are not available in ourcountry. Prenatal diagnosis is possible by usingthe same techniques on fetal tissues – Chorionicvillus biopsy or amniotic fluid.
2. Chromosomal disorders: Majority ofchromosomal disorders have associated mentalretardation. eg Down Syndrome, Edwardsyndrome (Trisomy18), Patau Syndrome(Trisomy 13). All de novo numerical andstructural chromosomal abnormalities have a lowrisk of recurrence (< 1%). Risk is higher if eitherof the parents is carrying a balanced translocation.Prenatal screening for common chromosomaldisorders has good sensitivity using maternalserum biochemical markers and ultrasonography.Definitive diagnosis can be provided bychromosomal studies on amniotic fluid, chorionicvillus biopsy or cord blood sample.
3. Multifactorial disorders: Counselingand risk of recurrence in these disorders is based
on empiric risk figures available in literature.Prenatal diagnosis is possible in some defectsusing fetal ultrasonography. Table 3 shows riskof recurrence of some common malformations.
Points to Remember
• Genetic counseling has an integral role inthe management of genetic disorders.Counseling should be nondirective, psychoeducational and involves goodcommunication with latest information,confidentiality, and truthfulness. Besidestreating the patients, physicians shouldmake the parents or couple aware of thegenetic disorder, risk of recurrence,prognosis and prenatal diagnosis.
• Because of the increased requirement forgenetic counseling an expansion ofgenetics training for residents andclinicians and the development ofcomputer-based interactive video programsfor genetic counseling is recommended.
85

Indian Journal of Practical Pediatrics 2008; 10(3) : 276
Instructions• Key should contain all information relevant to interpretation of pedigree (e.g. define shading)• For clinical (non-published) pedigrees include:
a) family names/initials, when appropriate b) name and title of person recording pedigreec) historian (person relaying family history information) d) date of intake/update
• Recommended order of information placed below symbol (below to lower right, ifnecessary):a) age/date of birth or age at death b) evaluation c) pedigree number (e.g. I-1, I-2, I-3)
Male Female Sex Commentsunknown
Individual Assign gender by phenotype. Squarerepresents male; circle represents afemale; a diamond represents whose sex
b. 1925 30 y 4 mo in not known. Age/date of birth can begiven at the bottom right hand corner.
Affected Fillings can be shading, hatches,Individual dots, lines, etc
Multiple For ≥ 2 conditions the symbols aretraits in an partitioned correspondingly, eachindividual quadrant with different fillings/patterns
representing different features.
Multiple Number of the siblings is writtenindividuals; inside the symbols; affectednumber individuals should not be grouped.known
Multiple “n” is used in the place of “?”individuals;numberunknown
Deceased If known, write “d” with age at deathindividual below symbol.
d. 35 y d.4 mo
Stillbirth Birth of a dead child with gestational(SB) age noted.
SB28 wk SB30 wk SB34 wk
6 66
n n n
Box 1. Common pedigree symbols, definitions and abbreviations
86
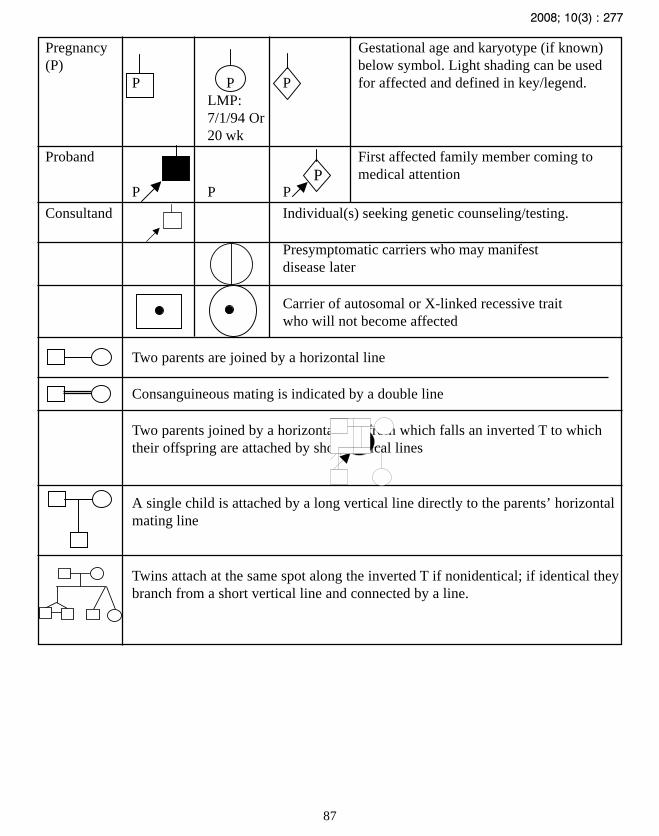
2008; 10(3) : 277
Pregnancy Gestational age and karyotype (if known)(P) below symbol. Light shading can be used
P P P for affected and defined in key/legend.LMP:7/1/94 Or20 wk
Proband First affected family member coming tomedical attention
P P P
Consultand Individual(s) seeking genetic counseling/testing.
Presymptomatic carriers who may manifestdisease later
Carrier of autosomal or X-linked recessive traitwho will not become affected
Two parents are joined by a horizontal line
Consanguineous mating is indicated by a double line
Two parents joined by a horizontal line from which falls an inverted T to whichtheir offspring are attached by short vertical lines
A single child is attached by a long vertical line directly to the parents’ horizontalmating line
Twins attach at the same spot along the inverted T if nonidentical; if identical theybranch from a short vertical line and connected by a line.
P
87

Indian Journal of Practical Pediatrics 2008; 10(3) : 278
Instructions
• Symbols are smaller than standard ones and individual’s line is shorter (even if sex is known,triangles are preferred to a small square / circle; symbols may be mistaken for the ones givenin the previous table box 1, especially in hand drawn pedigrees)
• If gender and gestational age known, write below symbol in that order.
• Parents who are unaffected and unrelated may be omitted from the pedigree.
• To save space, huge pedigrees are sometimes drawn in circular or spiral form rather than in arectangular form.
Box-2. Pedigree symbols and abbrevations for pregnancies not carried to term
Male Female Sex Commentsunknown
Spontaneous If ectopic pregnancy, writeabortion (SAB) ECT below symbol
male female ECT
Affected SAB If gestational age known, writebelow symbol. Key / legend
male female 16 week used to define shading
Termination Other abbreviations (eg. TAB,of pregnancy VTOP, Ab) not used for sake(TOP) of consistency
male female
Affected Key/legend used to defineTOP shading
male female
Bibliography
1. Fraser FC. Genetic Counseling. Am J HumanGenet 1974:26; 636-661.
2. Harper PS. Practical Genetic Counseling, 5thedn. USA Butterworth Heinemann. OxfordUniversity Press, 2004.
3. Biesecker BB. Goals of Genetic Counseling.Clinical Genet 2001; 60:323-330.
4. Aase JM. Diagnostic Dysmorphology. NewYork, Plenum Medical Book Company, 1990.
5. Jones KL, Smith WS. Smith’s RecognizablePatterns Of Human Malformation Sixth Edition.
6. Gardner RJM, Day TC, Sutherland GR.Chromosomal Abnormality and GeneticCounseling. 3
rd edition Oxford University
Press,USA 2003.
7. Shprintzen RJ. Robin sequence. In: Cassidy SB,Allanson JE. Management of geneticsyndromes. 1
st edn. Wiley-Liss, New York,
2001;pp323-336.
88

2008; 10(3) : 279
RADIOLOGIST TALKS TO YOU
INTRACRANIAL HEMORRHAGE
AND HYPOXIC ISCHEMIC
ENCEPHALOPATHY IN THE
NEONATE
* Vijayalakshmi G** Elavarasu E
*** Vijayalakshmi M*** Venkatesan MD
Intracranial bleed is a common event in thefragile neonatal brain. It can occur in thegerminal matrix, choroid plexus, brainparenchyma and in the subdural andsubarachnoid compartments. In the preterm,germinal matrix hemorrhage (GMH) is common.The germinal matrix consists of thin walledvessels that are likely to rupture easily withsudden changes in pressure. This delicatevasculature is found in the area between thecaudate nucleus and the thalamus on both sides.It is prominent between 24 and 34 weeks andalmost completely regresses by term. In thenewborn period autoregulation of cerebral bloodflow is easily upset leaving the brain open tosudden rushes of blood and rupture of bloodvessels. Therefore there is a high risk ofintracranial hemorrhage.
For all preterm babies less than 34 weeks orwhen there is a suspicion of bleed, ultrasound of
the brain should immediately be carried out. Mostof the germinal matrix hemorrhage occurs within24 to 72 hours of birth. The second scan is doneat the end of a week. Subsequently, scans maybe repeated at various times to study progress ofthe lesion. Fig.1 is a parasagittal view. Thenormal choroid plexus is a regular, white, C-shaped structure. In the figure there is a bulbousthickening of the choroid plexus in the floor ofthe lateral ventricle. This is GMH orsubependymal hemorrhage. It is sometimesdifficult to decide whether GMH is localized tothe subependymal area or has extended into theventricle as intraventricular hemorrhage (IVH).This has led to it being referred to as GMH-IVH.The focus of hemorrhage undergoes liquefactionin 2 to 4 weeks leaving behind a cyst (Fig.2).These cysts can be of varying sizes. If large, theycan cause obstructive hydrocephalus.
Sometimes large hemorrhages extend intoand distend the ventricle.
In Fig.3 you can see blood distending theleft lateral ventricle and spreading into anddistending the third ventricle. The black rightlateral ventricle is dilated due to obstruction ofthe foramen of Munroe with blood and thepressure of the hematoma. Dilatation of ventriclesdoes not indicate a good prognosis.
As we try to localize hemorrhage let usidentify some helpful landmarks on certainstandard sections of the cranium. Fig.4 is amidcoronal section. The choroid plexus in thefloor of the lateral ventricles and the roof of thethird ventricle are seen as three white dots (V).“S” is the Sylvian fissure. So normal ventricles
* Associate Professor** Asst. Professor
*** ProfessorDepartment of Radiology,Chenglepet Medical College Hospital,Chenglepet, Tamilnadu.
89

Indian Journal of Practical Pediatrics 2008; 10(3) : 280
Fig.1. Subependymal or GMH. Thebulbous thickening is seen anteriorly.
Fig.2 GMH which has evolved into acyst. Note the dilated ventricles.
Fig.4 Normal midcoronal section.
Fig.6. Normal posterior coronalsection.
Fig.3. Intraventricular hemorrhage(IVH). Hypoechoic clot in LLV and 3V.
Fig.5. Intraparenchymal hemorrhage.
90

2008; 10(3) : 281
are hardly seen. It is the white choroid plexusthat indicates their location in the midcoronalsection.The curved white lines are the sulci andin between them are the gyri. Posteriorly, thetriangular part is the posterior fossa with thetentorium and the cerebellum. Fig.5 shows around white area corresponding to a largeparenchymal hemorrhage in a term neonate.Note that there are no sulci and gyri in that area.The opposite lateral ventricle is dilated becauseof obstruction due to pressure from the hematomawhile the ipsilateral ventricle is compressed.
Hemorrhage can also occur within thechoroid plexus especially in the term infant. Fig.6is a posterior coronal section. The normal choroidplexus is seen as thin, symmetrical whitedivergent lines. In Fig.7. hemorrhage has madethe choroid on the right appear thicker. So watchfor asymmetries between the two sides.
Hypoxia and ischemia in the newborn causeinjury to the brain. In 24 to 48 hours there isswelling of brain tissue. This manifests ascompressed slit –like ventricles and a diffuse lossof sulcal-gyral echodistinction in ultrasound.After 48 hours, signs of ischemic injury in theterm infant are bright areas in the basal ganglia,thalami and the parasagittal, subcortical
watershed area between the vascular territoriesof the middle cerebral, anterior and posteriorcerebral arteries. MRI also shows changes inthe same areas. One important abnormality inMRI which is a very good predictor of a pooroutcome is abnormal signals in the posterior limbof the internal capsule. Later, delayedmyelination and cortical atrophy are seen.
In the preterm, the immature neurons oroligodendrocytes which are metabolically veryactive between the 23 and 32 weeks are moresusceptible to ischemic injury. This tissue isaround the ventricles which is the location ofperiventricular leukomalacia (PVL). It is anischemia-reperfusion brain injury that occurs inthe periventricular region. This is seen asunilateral or bilateral white areas around thelateral ventricles (Fig.8). They assume a wedgeshape with the apex towards the lateral ventricle.Most of these babies develop cerebral palsy andtherefore this is an indicator of poor prognosis.In 2 to 3 weeks the infarcted area will evolveinto small cysts. The cystic lesions mayeventually disappear leaving behind dilatedventricles with scalloped edges. Mildperiventicular halos can disappear without signsof ischemic neuronal loss. Follow-up scans willdetermine if damage is permanent.
Fig.7. Choroid plexus hemorrhage. Fig.8. Periventricular leukomalacia.
91

Indian Journal of Practical Pediatrics 2008; 10(3) : 282
Hydrocephalus is a complication of GMHand IVH. The cause is either an obliterativearachnoiditis that causes a communicativehydrocephalus or obstruction of interventricularCSF pathways due to clot. Post hemorrhagicventricular dilatation can be transient till CSFpathways clear. Sometimes it may persist orprogress. Serial scans are necessary to evaluatefor the need for surgical intervention.
Atrophy of the brain due to ischemia is alsoseen as passive dilatation of ventricles. ThereforePVL has to be followed with repeat scans.
Cranial ultrasound is a valuable tool in thestudy of the newborn brain. It is reliable andportable and can be used repeatedly to study theevolution of lesions.It can easily identifygerminal matrix and parenchymal hemorrhageand can be used in follow-up that will enable thepediatrician to predict long term outcome.
CT is more effective for parenchymallesions but the ease of obtaining ultrasound is itsadvantage. MRI is superior to ultrasound butimpractical for repeated usage.
92
NATIONAL CONFERENCE ON CEREBRAL PALSY(IIIrd NATIONAL CONFERENCE OF IACP)
21st – 23rd November 2008-08Organised by
NKP Salve Institute of Medical Sciences and Lata Mangeshkar Hospital, Nagpur.
Organising Secretariat
Dr.Vithalrao DandgeProf. and Head, Dept. of PaediatricsV-42, Narendra Nagar, Nagpur-440015Tel:0712-2744951, Fax: 0712-2747937, Mob.9422106774E-mail: [email protected]
NEWS AND NOTES
NATIONAL WORKSHOP ON MOLECULAR CYTOGENETICS:
RAPID PRENATAL DIAGNOSIS BY FISH
New Delhi.
November 3-8, 2008
Contact
Dr.Ashutosh Halder
Associate Professor, Department of Reproductive Biology,
All India Institute of Medical Sciences, New Delhi-110 029.India
Tel: 011-26593304 ext 4211 (O) or 3694® Mobile: 09313309579
Email: [email protected]

2008; 10(3) : 283
A term neonate with facial asymmetry (mouth deviated to right on crying) with no evidence offacial palsy had deformed pinna, and preauricular tags. Echo cardiogram revealed atrial septal defect.Can you spot the diagnosis?
Compiled by
Dr.Ramesh Bhat Y.
Associate Professor, Department of Pediatrics
Kasturba Medical College, Manipal,
Udupi District, Karnataka – 576 104.
Answer on Page: 288
PICTURE QUIZ
93

Indian Journal of Practical Pediatrics 2008; 10(3) : 284
DERMATOLOGY
ALOPECIA AREATA IN CHILDREN
* Madhu R
Abstract : Alopecia areata is an autoimmunenon-scarring disorder of hair growth affectinggenetically predisposed individuals. It ischaracterised by the sudden appearance of oneor more round or oval well circumscribed patchesof hair loss. Different patterns such as oophiasis,alopecia totalis, alopecia universalis may occur.It is associated with autoimmune disorders suchas Hashimoto’s thyroiditis and vitiligo. Increasedincidence is seen in patients with Down’ssyndrome. Its severity, course and prognosis areunpredictable. Prognosis is good in children withlimited involvement. Treatment only controls thecondition, but does not cure or prevent furtherspread.
Key Words: Alopecia areata, Children, Hair loss,Autoimmune.
Alopecia areata (AA), is characterised bythe sudden appearance of one or more round oroval well circumscribed patches of hair loss. Itis a non scarring, non inflammatory type ofalopecia, that occurs in 0.1% to 0.2% of thepopulation.1 Though this disorder occurs in allages, 24- 50% present in childhood with the firstepisode before 16 years of age.2 It has beendescribed in neonates and infants.3 Alopeciaareata can cause tremendous emotional andpsychosocial stress in affected patients and theirfamilies.
Aetiology
Cause of alopecia areata is unknown, but itis believed to be a T cell mediated autoimmunedisorder occurring in genetically predisposedindividuals. Emotional stress has been consideredas a precipitating factor.
Genetic : Familial occurrence is reported in10% to 20% of affected persons.4,5 Mode ofinheritance is thought to be autosomal dominantwith variable penetrance. Simultaneousoccurrence in identical twins has been reported.3
Presence of HLADR5 and DR4 has been shownto correlate with the disease severity. Chronicform of alopecia areata is associated with DQ3.Long standing alopecia totalis or universalis haveadditional associations with DR4, DR5, DR11and DQ7.4,6 IL 1 receptor antagonist gene is saidto correlate with disease severity.4
An increased incidence has been noted inpatients with Down’s syndrome,7,8,9,10 This highfrequency suggests that a genetic linkage for AAmay exist on chromosome 21. The Downsyndrome region of chromosome 21 has theMX1 gene that encodes interferon-induced p78protein MXA. This protein is strongly expressedin lesional anagen hair bulbs from patients withalopecia areata. In a case-control study, theMX1 (+9959) polymorphism was significantlyassociated with alopecia areata, with an increasedrisk for early onset disease.6 Atopy is found in10% to 22% of patients.11
Autoimmunity: Hypothesis that alopecia areatais an autoimmune disease is well supported bythe statistically significant association with otherautoimmune disorders such as vitiligo,
* Asst Professor,Dept of Dermatology & Leprosy,Govt. Stanley Hospital, Chennai.
94

2008; 10(3) : 285
Hashimoto’s thyroiditis, Addison’s disease,myasthenia gravis, pernicious anemia,rheumatoid arthritis and Candida endocrinopathysyndrome where candidal infections tends tobegin by 5 years of age, but endocrinologicaldysfunction may not be apparent untiladolescence or even adult years.4,5,12,13 Increasedincidence of organ specific antibodies againstthyroid, gastric parietal cells, etc has beenreported. High titres of antibodies to hairfollicular components have been observed inaffected patients.4
With regard to cell mediated immunity, ithas been found that there is altered T-cellregulation of the immune response. Lymphocyticinfiltration around the hair follicles support theautoimmune theory. Neuropeptides such asCalcitonin gene-related peptide (CGRP) andsubstance-P play a significant role. CGRP whichhas potent anti-inflammatory action is found tobe decreased in alopecia areata. There is adecreased expression of substance-P , which iscapable of inducing hair growth, in the scalp ofpatients with alopecia areata.11
Psychological : Role of stress has beenfrequently cited.4,14
Pathogenesis
Studies have shown that the injury is mostsevere in the centre of the patch leading topremature and sudden precipitation of a groupof follicles into telogen, the resting phase, withresultant hair shedding. In the periphery,impaired keratinisation and shaft breakage occursin anagen follicles, followed by precipitation intotelogen which results in the formation of thecharacteristic “Exclamation Point” hairs.3 Short,loose hairs, in the margins of the patch thatgradually thin towards the scalp are called“Exclamation Point” hairs, which arepathognomic of alopecia areata. The hairbulbrepresents the dot of the exclamation point. Whenseen under a low-power microscope , free endsare splayed giving a “frayed rope” appearance.
Clinical features
Alopecia areata, usually occurs over thescalp, but may involve eyebrows and beard area.The classical picture is that of a suddenappearance of one or more oval or round wellcircumscribed smooth patches of hair loss that isasymptomatic. Skin is smooth and soft. Rarelyerythema or mild edema may be present in early
95
Fig.1. Single patch of alopecia Fig.2. Multiple patches of hair loss

Indian Journal of Practical Pediatrics 2008; 10(3) : 286
stages. Increased hair shedding has been reported.Thin depigmented hair shafts may be seen beforehair loss or with early hair regrowth. These greyhairs may repigment later. Exclamation markhairs may be found in the margins. Positive pulltest at the periphery of a plaque usually indicatesthat the disease is active, and further hair losscan be expected. In alopecia areata, when a tuftof hair is forced inward or bent, hairs kink at5-10 mm above the surface. Shuster describedthis as the “ Coudability sign”.15
Various clinical patterns are as follows:
Single or multiple patches.
Ophiasis (Gk–serpent) pattern - Hair loss beginsas a bald spot on the posterior occiput andextends anteriorly and bilaterally in a 1 to 2 inchwide band, above the ears, occasionally extendingto the anterior aspect of the scalp. This patternmostly seen in children, occurs in less than 5%of the patients and often progresses to alopeciatotalis or universalis.
Sisaipho (Converse-ophiasis spelled backwards)pattern occurs when hair loss spares the sidesand the occiput.
Alopecia totalis: 100% hair loss on the scalp
Alopecia universalis: Complete loss of hair onall hair-bearing areas.
Reticular or the diffuse pattern occurs when hairloss is more extensive and the patches coalesce.
Nail involvement : Nail changes are seen in10-44% of patients, with severe involvementbeing observed in alopecia totalis or universalis.The most characteristic pattern is the presenceof superficial, uniform , minute pits arrangedregularly in horizontal and or vertical rows.Trachyonychia (rough sandpaper nails), proximalshedding, opacity, punctate leukonychia mayoccur.16,17
Differential Diagnosis
Diagnosis is mainly clinical. However, thefollowing conditions should run through one’smind :
1. Naevus sebaceous, present since birth ,presents as a patch of congenital alopecia
2. Physiological hair cycle changes in earlyinfancy.
3. Frictional alopecia due to tight braidedhairstyle.
4. Trichotillomania – patches of alopeciawith twisted and broken hairs of different lengthsseen
5. Tinea capitis – signs of inflammation,scaling and lymphadenopathy
6. Scarring alopecia, post inflammatoryatrophy - absence of follicular ostia or somedegree of atrophy.
7. Rarely lichen planopilaris, morphea,.
8. Diffuse alopecia areata resemblingtelogen effluvium may be difficult to diagnose,wherein a punch biopsy will help confirmdiagnosis. Characteristic histopathologic featureis the presence of a peribulbar lymphocyticinfiltrate (swarm of bees).
Prognosis
The course of alopecia areata is variable andunpredictable. Spontaneous regrowth occurswithin a few months, with or without treatment.When there is limited involvement of fewpatches, prognosis is good , with completeregrowth occurring within one year in 95% ofchildren. The severe, chronic form is seen inabout 7% to 10% of patients.1
96

2008; 10(3) : 287
Poor prognostic signs3, 18
Early age of onset, ( less than 10 years at firstepisode), family history
Multiple patches with rapid progression
Oophiasis, Sisaiphoo
Alopecia totalis, alopecia universalis
Associations – atopy, autoimmune conditions,nail dystrophy, Down’s syndrome
Poor response to previous treatment.
Treatment1,11,19
Therapy of alopecia areata,at best controlsrather than cure or prevent the further spread ofthe disease. First and foremost step is to offerpsychological support and counseling to the childand the parents.
1. Topical corticosteroid – Mid to highpotent, applied twice daily
2. 5% topical minoxidil solution appliedtwice daily. Efficacy is enhanced when used incombination with anthralin or betamethasonedipropionate. Anthralin is applied two hours afterthe second minoxidil application, whereasbetamethasone is applied twice daily 30 minutesafter use of minoxidil.
3. Short contact anthralin- 0.2 to 1% for30 minutes.
4. Topical tacrolimus 0.1% twice daily.20,21
5. Intralesional triamcinolone acetonide inchildren over 10 years.
6. Systemic corticosteroids in severeand rapid progression- oral prednisolone0.5-1mg/kg/d for 4 wks and then tapered toalternate day therapy for few months, duringwhich period the child should be monitored forside effects of steroids.
7. Topical immunotherapy in chronic, severealopecia areata - Dinitrochlorobenzene (DNCB)SADBE (Squaric acid dibutyl ester),diphenylcyclopropenone.
8. Cryotherapy, oral cyclosporin,phototherapy, aromatherapy.
Points to Remember
• Alopecia areata is a clinical diagnosis.Various modalities of therapy that areavailable, only control and not cure orprevent further progression of the disease.
• Psychological support and counseling ismandatory.
• Any mode of treatment is considered tohave failed only after a minimum periodof 3-6 months because of the long periodfor regrowth of hair.
• Thyroid screening should be routinelyperformed in all children withlongstanding AA.
References
1. Paller AS, Mancini AJ, eds. Hurwitz ClinicalPediatric dermatology. 3
rd ed. Elsevier Saunders,
2006;pp157- 160.2. Sharma VK, Dawn G, Kumar B. Profile of
alopecia areata in Northern India. Int J Dermatol1996;35:22-27.
3. Wadhwa SL, Khopkar U, Mhaske V. Hair andScalp disorders, Alopecia areata. In: Valia RGand Valia AR. Eds, IADVL Textbook and atlasof dermatology.Vol I, 2
nd Edn, Bhalani, Mumbai
2001;pp733-738.4. Dawber RPR, Berker D,Wojnarowska F.
Disorders of hair, Alopecia areata. In:Champion RH, Burton JL, Burns DA,Breathnach SM, Eds. Textbook of dermatology.6
th Edn., Blackwell Science publications, 1998;
pp2919- 2927.
5. Ahmed I,Nasreen S, Bhatti R. Alopecia areatain children. J Coll Physicians Surg Pak2007;17:587-590.
97

Indian Journal of Practical Pediatrics 2008; 10(3) : 288
6. McDonagh AJ, Tazi-Ahnini R. Epidemiologyand genetics of alopecia areata. Clin ExpDermatol 2002;27:405-409.
7. Du Vivier A, Munro DD. Alopecia areata,autoimmunity and Down syndrome. Br Med J1975;1:191-192.
8. Tan E, Tay YK, Giam YC. A clinical study ofchildhood alopecia areata in Singapore. PediatrDermatol 2002;19:298-301.
9. Tan E, Tay YK, Goh CL, Giam YC. The patternand profile of alopecia areata in Singapore: Astudy of 219 Asians. Int J Dermatol2002;41:748-753.
10. Sharma VK, Kumar B, Dawn G. A clinical studyof childhood alopecia areata in Chandigarh,India. Pediatr Dermatol 1996;13:372-377.
11. Rogers M, Tay YK. Hair disorders, Alopeciaareata. In : Schachner LA , Hansen RC, Eds.Pediatric dermatology. 3
rd Edn . Mosby, London
2003; pp546- 549.
12. Kurtev A, Iliev E. Thyroid autoimmunity inchildren and adolescents with alopeciaareata.Int J Dermatol.2005;44:457-461.
13. Nanda A, Alsaleh QA, Al-Hasawi F, Al-Muzairai I. Thyroid function, autoantibodies,and HLA tissue typing in children with alopeciaareata. Pediatr Dermatol.2002;19:486-491
14. Kakourou T,Karachristou K, Chrousos G.A case series of alopecia areata in children:
impact of personal and family history of stressand autoimmunity. J Eur Acad DermatolVenereol. 2007;21:356-359.
15. Shelley WB, Shelley ED. Alopecia areata. In:Advanced dermatologic diagnosis.W.B.Saunders, Philadelphia 1992;pp224- 227.
16. Tosti A, Morelli R, Bardazzi F, et al. Prevalenceof nail abnormalities in children with alopeciaareata. Pediatr Dermatol 1994; 112-115.
17. Tosti A, Fanti PA, Morelli R, et al.Trachyonychia associated with alopecia areata:A clinical and pathological study. J Am AceadDermatol 1991;25:266-270.
18. Sinclair R, Scarff CE. Alopecia areata. In:Williams H, Bigby M et al, Eds. Evidence-based Dermatology. Prism books pvt ltd, 2003;pp577- 588.
19. Shelley WB, Shelley ED. Alopecia areata.Eds. Advanced dermatologic therapy II.WB Saunders, Philadelphia 2001; pp68- 79.
20. Rallies E, Korfitis C, Gregoriou S, RigopoulosD. Assigning new roles to topical tacrolimus.Expert Opin Investig Drugs. 2007;16:1267-1276.
21. Yamamoto S, Kato R. Hair growth- stimulatingeffects of cyclosporine A and FK506, potentimmunosuppressants. J Dermatol Sci. 1994;7 suppl: S47- 54.
98
Picture Quiz Answer: Cayler cardio-facial syndrome (Characterised by underdevelopment or absenceof depressor anguli oris muscle on one side associated with major congenital anomalies, mostcommonly in cardiovascular system).
XINCPID – 2008
XI NATIONAL CONFERENCE OF PEDIATRIC INFECTIOUS DISEASES
Organized by: Indian Academy of Pediatrics, Varanasi
Date: 22nd & 23rd November 2008 Venue: Hotel Ramada, Varanasi
Registration Fee: Rs.2000/- till 31st July 2008
Address of correspondence
Dr.Ashok Rai, Organizing Secretary, XI NCPID-2008
C-29/61-A, KH-1, Raghubir, Maldahiya, Varanasi-221 002.
Mobile: 94152-01567 / 98390-56960, Email: [email protected]
NEWS AND NOTES




















