Increases in correct administration of chloroquine in the home and referral of sick children to...
10
TRANSACTIONSOF THE ROYAL SOCIETY OF TROPICALMEDICINEAND HYGIENE (2003) 97, 481-490 Increases in correct administration of chloroquine in the home and referral of sick children to health facilities through a community-based intervention in Bougouni District, Mali P. J. Winch 1, A. Bagayoko 2, A. Diawara 3, M. Kan6 4, F. Thi6ro 2, K. Gilroy 1, Z. Daou 2, Z. Berth6 2 and E. Swedberg s 1Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA; 2Save the Children~USA, Bougouni, Mali; 3Facultk de Mkdecine, de Pharmaeie et d'Odontostomatologie, Universit~ du Mali, Bamako, Mali; 4Secretary General, Ministry of Health, Bamako, Mali; 5Save the Children~USA, Westport, CT, USA Abstract Save the Children/USA in collaboration with the Ministry of Health of Mali has established over 300 village drug kits in southern Mali since 1996. A cluster-randomized trial was conducted between November 2001 and February 2002 in 10 health zones of Bougouni District to evaluate an intervention to (i) improve the skills of the village drug kit managers to counsel parents on correct home administra- tion of chloroquine (CQ), and (ii) increase the referral of sick children to community health centres (CHC). Children's carers were interviewed 5 d after the sale of CQ about knowledge of danger signs requiring referral, quality of counselling, administration of CQ, and referral. The intervention was associated with significant increases in knowledge of danger signs requiring referral, reported quality of counselling by the manger of the drug kit, and correct administration of CQ in the home. Parents reported that 42.1% of children in the intervention group were referred to the CHC by the drug kit manager compared with 11.2% in the comparison group (odds ratio = 7.12, 95 % CI 2.62-19.38). CHC registers indicated that 87.0% of referrals recorded in drug kit referral notebooks arrived at the health centre. Further research is needed to increase the effectiveness of the counselling and the community referral mechanism tested in this study. Keywords: malaria, chloroquine, compliance, Integrated Management of Childhood Illness, cluster-randomized trials, Mali Introduction In areas where malaria is endemic, episodes of fever are commonly managed in the home using antimalarial and antipyretic medications obtained from pharmacies, shops or ambulatory drug vendors, or with herbal remedies. Reasons that self-medication prevails over care seeking from health facilities include convenience, user fees and other costs associated with facility-based care, and decreased economic access to health facilities during the rainy season (Sauerbom et al., 1996a, 1996b). Inappropriate use of antimalarial drugs asso- ciated with self-medication limits therapeutic efficacy and favours the emergence and spread of drug-resistant parasites. Promotion of early and appropriate treatment of those febrile episodes that do not reach health facilities is an essential part of both the community component of the Integrated Management of Childhood Illness (IMCI) and Roll Back Malaria initiatives. Approaches to promote early and appropriate treatment include training of shopkeepers and ambulatory drug vendors on appropriate treatment practices (Oshiname & Brie- ger, 1992; Marsh et al., 1999), training community health workers (CHW) and other cadres of volunteer worker on presumptive diagnosis and treatment of malaria (Ruebush & Godoy, 1992; Okanurak & Rue- bush, 1996; Ghebreyesus et al., 1996), establishment of village pharmacies (Krause et al., 1998), sale of pre- packaged complete courses of antimalarial treatment (Gomes et al., 1998; Ansah et al., 2001; Agyepong et al., 2002; Brieger et al., 2002), training of mother coordinators who train other mothers to maintain a stock of CQ in the home and provide age-appropriate treatments (Kidane & Morrow, 2000), and training mothers to access a central stock of prepackaged anti- malarials maintained by CHWs (Pagnoni et al., 1997; Sirima et al., 2003). Address for correspondence: Peter Winch, Department of International Health, Room E5030, Social and Behavioral Interventions Program, Johns Hopkins Bloomberg School of Public Health, 615 North Wolfe Street, Baltimore, MD 21205, USA; phone +1 410 955 9854, fax +1 410 502 6733, e-fax +1 413 556 4112, e-mail [email protected] These and other similar interventions have several important limitations. First, providers often focus on dispensing the right amount of medicine and account- ing for the money received, and may neglect to provide sufficient information to patients or parents of young children about how to correctly administer the drug in the home, and the importance of seeking care if the symptoms fail to resolve. Second, CHWs, shopkeepers, and other classes of provider trained through these interventions typically are not an integral part of the formal health system. One consequence may be that, when cases of treatment failure occur or patients with signs of severe illness present, appropriate referral of the patient to a health facility is not made (Font et al., 2002), and people seek other forms of treatment in the informal sector or from traditional providers (Makem- ba et al., 1996). Malaria is a major public health problem in Sikasso Region, Mali. A study on malaria treatment was con- ducted in the District of Yanfolila on the western side of Sikasso Region at the end of the rainy season in 1998 (Th6ra et al., 2000). Of 399 mothers interviewed, 131 had sick children, of whom 58 had a febrile illness, and 57 were parasitaemic with parasite densities of 80-213 600 parasites/pL (Thfira et al., 2000). Significant CQ resistance is present in Mali (Djimde et al., 1998; Delley et al., 2000; Plowe et al., 2001) and, at the time of the current study, the Ministry of Health felt that it was elevated enough to justify switching to an alterna- tive first-line drug. The Ministry of Health is now considering changing the first-line drug to either arte- mether-lumefantrine or sulfadoxine-pyrimethamine/ artesunate. Plowe et al. (2001) reported 13-17% para- sitological resistance rates and 10-15% treatment fail- ure rates in a recent study. Save the Children/USA, working in collaboration with the Ministry of Health of Mali, has established over 300 village drug kits (caisses pharmaceutiques) in Bougouni, Yanfolila, and Kolondieba Districts of Sikasso Region in villages with individual populations of about 1 000 between 1997 and 2003. Stocked with only 7 items (Aureomycin 1% eye ointment, paraceta- mol, oral rehydration solution sachets, alcohol, ban- dages, CQ tablets, and CQ syrup), these drug kits enable people to have immediate access to treat many
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Increases in correct administration of chloroquine in the home and referral of sick children to...

TRANSACTIONS OF THE ROYAL SOCIETY OF TROPICAL MEDICINE AND HYGIENE (2003) 97, 481-490
Increases in correct administration of chloroquine in the home and referral of sick children to health facilities through a community-based intervention in Bougouni District, Mali
P. J. Winch 1, A. B a g a y o k o 2, A. D i a w a r a 3, M. Kan6 4, F. Thi6ro 2, K. Gi lroy 1, Z. D a o u 2, Z. Berth6 2 and E. S w e d b e r g s 1Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA; 2Save the Children~USA, Bougouni, Mali; 3Facultk de Mkdecine, de Pharmaeie et d'Odontostomatologie, Universit~ du Mali, Bamako, Mali; 4Secretary General, Ministry of Health, Bamako, Mali; 5Save the Children~USA, Westport, CT, USA
Abstract Save the Children/USA in collaboration with the Ministry of Health of Mali has established over 300 village drug kits in southern Mali since 1996. A cluster-randomized trial was conducted between November 2001 and February 2002 in 10 health zones of Bougouni District to evaluate an intervention to (i) improve the skills of the village drug kit managers to counsel parents on correct home administra- tion of chloroquine (CQ), and (ii) increase the referral of sick children to community health centres (CHC). Children's carers were interviewed 5 d after the sale of CQ about knowledge of danger signs requiring referral, quality of counselling, administration of CQ, and referral. The intervention was associated with significant increases in knowledge of danger signs requiring referral, reported quality of counselling by the manger of the drug kit, and correct administration of CQ in the home. Parents reported that 42.1% of children in the intervention group were referred to the CHC by the drug kit manager compared with 11.2% in the comparison group (odds ratio = 7.12, 95 % CI 2.62-19.38). CHC registers indicated that 87.0% of referrals recorded in drug kit referral notebooks arrived at the health centre. Further research is needed to increase the effectiveness of the counselling and the community referral mechanism tested in this study.
Keywords: malaria, chloroquine, compliance, Integrated Management of Childhood Illness, cluster-randomized trials, Mali
Introduct ion In areas where malaria is endemic, episodes of fever
are commonly managed in the home using antimalarial and antipyretic medications obtained from pharmacies, shops or ambulatory drug vendors, or with herbal remedies. Reasons that self-medication prevails over care seeking from health facilities include convenience, user fees and other costs associated with facility-based care, and decreased economic access to health facilities during the rainy season (Sauerbom et al., 1996a, 1996b). Inappropriate use of antimalarial drugs asso- ciated with self-medication limits therapeutic efficacy and favours the emergence and spread of drug-resistant parasites.
Promotion of early and appropriate treatment of those febrile episodes that do not reach health facilities is an essential part of both the community component of the Integrated Management of Childhood Illness (IMCI) and Roll Back Malaria initiatives. Approaches to promote early and appropriate treatment include training of shopkeepers and ambulatory drug vendors on appropriate treatment practices (Oshiname & Brie- ger, 1992; Marsh et al., 1999), training community health workers (CHW) and other cadres of volunteer worker on presumptive diagnosis and treatment of malaria (Ruebush & Godoy, 1992; Okanurak & Rue- bush, 1996; Ghebreyesus et al., 1996), establishment of village pharmacies (Krause et al., 1998), sale of pre- packaged complete courses of antimalarial treatment (Gomes et al., 1998; Ansah et al., 2001; Agyepong et al., 2002; Brieger et al., 2002), training of mother coordinators who train other mothers to maintain a stock of CQ in the home and provide age-appropriate treatments (Kidane & Morrow, 2000), and training mothers to access a central stock of prepackaged anti- malarials maintained by CHWs (Pagnoni et al., 1997; Sirima et al., 2003).
Address for correspondence: Peter Winch, Department of International Health, Room E5030, Social and Behavioral Interventions Program, Johns Hopkins Bloomberg School of Public Health, 615 North Wolfe Street, Baltimore, MD 21205, USA; phone +1 410 955 9854, fax +1 410 502 6733, e-fax +1 413 556 4112, e-mail [email protected]
These and other similar interventions have several important limitations. First, providers often focus on dispensing the right amount of medicine and account- ing for the money received, and may neglect to provide sufficient information to patients or parents of young children about how to correctly administer the drug in the home, and the importance of seeking care if the symptoms fail to resolve. Second, CHWs, shopkeepers, and other classes of provider trained through these interventions typically are not an integral part of the formal health system. One consequence may be that, when cases of treatment failure occur or patients with signs of severe illness present, appropriate referral of the patient to a health facility is not made (Font et al., 2002), and people seek other forms of treatment in the informal sector or from traditional providers (Makem- ba et al., 1996).
Malaria is a major public health problem in Sikasso Region, Mali. A study on malaria treatment was con- ducted in the District of Yanfolila on the western side of Sikasso Region at the end of the rainy season in 1998 (Th6ra et al., 2000). Of 399 mothers interviewed, 131 had sick children, of whom 58 had a febrile illness, and 57 were parasitaemic with parasite densities of 80-213 600 parasites/pL (Thfira et al., 2000). Significant CQ resistance is present in Mali (Djimde et al., 1998; Delley et al., 2000; Plowe et al., 2001) and, at the time of the current study, the Ministry of Health felt that it was elevated enough to justify switching to an alterna- tive first-line drug. The Ministry of Health is now considering changing the first-line drug to either arte- mether-lumefantrine or sulfadoxine-pyrimethamine/ artesunate. Plowe et al. (2001) reported 13-17% para- sitological resistance rates and 10-15% treatment fail- ure rates in a recent study.
Save the Children/USA, working in collaboration with the Ministry of Health of Mali, has established over 300 village drug kits (caisses pharmaceutiques) in Bougouni, Yanfolila, and Kolondieba Districts of Sikasso Region in villages with individual populations of about 1 000 between 1997 and 2003. Stocked with only 7 items (Aureomycin 1% eye ointment, paraceta- mol, oral rehydration solution sachets, alcohol, ban- dages, CQ tablets, and CQ syrup), these drug kits enable people to have immediate access to treat many

482 P.J. WINCH ETAL.
common health problems, including malaria. The kits are operated by a manager (gdrant) recruited from the community, and with training and responsibilities simi- lar to depot holders and community-based distributors in other health and family planning programmes. Drug kits were initially successful in increasing the availability of CQ at the village level, but problems remained. In 1999 during the final evaluation of a child survival project implemented in Bougouni District, it was noted that incomplete courses of treatment were often sold, and minimal counselling was provided by the managers of these village drug kits to people coming for treatment of febrile illnesses. There were no print materials avail- able to help the manager of the village drug kit to explain to mothers in detail when and how the medica- tion is to be given to the child, materials which might increase compliance with treatment regimens (Ngoh & Shepherd, 1997). Furthermore, there was concern that children with lower respiratory tract infection, severe malaria, or other conditions that could not be managed at the village level were not being referred to health facilities.
These observations lead to the development of the current study. The study aimed to define an interven- tion to address these deficiencies in the village drug kit intervention, and more specifically (i) assess whether the intervention could increase the proportion of chil- dren who were treated with a full course of CQ in the home, and (ii) increase the proportion of children with indications for referral to a health facility who were referred to and subsequently reached the facility.
Materials and Methods Coordination with concurrent study on Integrated Management of Childhood Illness training
The district (Cercle) of Bougouni contains 25 health zones (aires de santd) each one consisting of 1 commun- ity health centre (CHC) and the villages in its catch- ment area. In a concurrent study described elsewhere, head nurses in intervention group health centres re- ceived the standard WHO training course in IMCI at the regional hospital in Sikasso in June 2001, and the impact of the training on quality of counselling on drug administration given by the head nurses to parents of sick children, and compliance with a full course of antimicrobial therapy in the home was evaluated (Gil- roy et al., in press; P. J. Winch et al., unpublished data). During their training, head nurses were told about the training that the drug kit managers were to receive and the new referral system. The same randomization scheme was used for both studies.
Assignment of health zones to intervention and comparison groups
In the 14 health zones in Bougouni District where drug kits had been established by 2001, 10 were eligible for the study based on having a flmctional, fully staffed CHC. This corresponded to the number of zones needed according to the sample size calculation (see next section), although this did not allow for the possi- bility that it might not prove possible to complete the study in some zones. The 10 zones were grouped into 5 pairs (Torakoro/Keleya, Sido/Garalo, Kologo/Zantie- bougou, Bougouni West/Bougouni East, and Fara- gouaran/Bougouni South), and 1 health zone from each pair was randomly assigned to receive the inter- vention. Pairing was based on when drug kits had first been established in the zone (during first health project 1996-99 or more recent project 1999-2002) and de- gree of urban or rural character of the zone.
The referral system was set up in March 2001. The visual aids and training for the drug kit managers (described below) were pilot tested between August and November 2001 in the health zones not included in the study. In the 5 intervention health zones, the managers for all the drug kits located in the zone were
trained for 5 days in mid-November 2001. Evaluation of the impact of the intervention took place between December 2001 and February 2002.
There are 2 managers for each village drug kit, one is the main person responsible and the other is his/her replacement. When a new village drug kit is estab- lished, all managers go through standard training which consists of a 35-d literacy course in which they are taught to read and write the national language, Bam- bara, using a phonetic alphabet, followed by a 1-week course on how to manage the drug kit including the correct doses to recommend and sell for each product in the kit. All of the drug kit managers in both the intervention and comparison groups had had this stan- dard training prior to the study reported here. In the intervention areas, the following 5 activities were car- ried out in addition to the routine training, the first 4 at the level of the village drug kit, and the fifth at the community level.
Interventions at the level of the village drug kits
(i) Visual aids have been found to be a key compo- nent of other interventions to improve compliance (Ngoh & Shepherd, 1997; Okonkwo et al., 2001). Visual aids were provided to the managers of the drug kits for explaining to carers of young children how to administer CQ to children in various age groups (2-12 months, 1-3 years, 3 -5 years, 6-10 years, 10-14 years, and adult). CQ is given once per day for 3 d at a dosage of 10 mg/kg on days 1 and 2, and 5 mg/kg on day 3 in Mali. The aids were developed by the National Centre for Information, Education and Communica- tion for Health (CNIECS) of Mali.
(ii) Visual aids, also developed by CNIECS, were provided to the managers for explaining to carers of young children the symptoms such as convulsions and difficulty breathing which require immediate referral to a government health facility.
(iii) A referral mechanism from the community to first-level facility was put in place. Each manager had a referral notebook and a referral bag. If, based on the assessment of the manager, a child was seen that required referral to a health facility, the manager was to write the child's name, the date, and the reason for the referral in the referral notebook, place the book in the referral bag, and instruct the cater of the sick child to take the child and the referral bag to the nearest CHC. The health workers in the CHCs were instructed to write the diagnosis, treatment given, and instructions for follow-up in the referral notebook before dischar- ging the child so that the drug kit manager subse- quently could monitor the condition of the child. Some programmes refer to this feedback as counter-referral.
(iv) Managers of the drug kits attended a 5-d addi- tional training course conducted in a local elementary school that covered: (i) doses of CQ for different age groups (also covered in the standard course), (ii) how to counsel carers of young children regarding the cor- rect administration of CQ in the home and the impor- tance of going to the CHC when referred, (iii) indications for referral including danger signs and fail- ure of the child's symptoms to respond to treatment, (iv) basic evaluation of a sick child for danger signs such as dehydration requiring referral, and (v) how to use the referral notebook and the visual aids. Counsel- ling guidelines were adapted from the IMCI guidelines for facility-based health workers.
Intervention at the village level In the intervention zone, a meeting was held in each
of the villages with a drug kit to explain to community members the improvements that had been made to the village drug kits and to encourage people to seek treat- ment from the managers of the kits.

HOME TREATMENT AND REFERRAL INTERVENTION IN MALI 483
Measurement of study outcomes Fifteen field interviewers were recruited. In 6 of the
10 health zones there was 1 interviewer only, while the other 4 health zones had 2 or 3 interviewers due to their large size. Each interviewer was assigned a set of village drug kits and their clients to study. At least twice a week the interviewer visited the manager of the village drug kit, talked to him/her and examined the register of sales maintained by him/her, noting down the cases where CQ had been sold to treat a child aged <6 years. On the fifth day after the sale, the field interviewer went to the child's house and interviewed the person who had administered the treatment to the child. The ques- tionnaire that was administered to the child's carer included questions on (i) knowledge of danger signs that require referral to a CHC, (ii) the quality and content of the counselling received from the manager of the village drug kit, (iii) the treatments given to the child on each day of his/her illness, (iv) knowledge of treatments for convulsions (known by the local term kono), (v) referral of the child by the manager of the drug kit, and (vi) compliance with referral. In addition, the interviewer counted the number of CQ pills or the volume of syrup remaining. The entire questionnaire was reviewed by the study coordinator, and the degree of adherence to the IMCI standards for treatment of children with fever was assessed. Although the health worker's interaction with the child's cater was directly observed in the companion intervention at the CHCs (Gilroy et al., in press; P. J. Winch et al., unpublished data), direct observation was not possible in the current study due to the low and irregular numbers of people who visit the village drug kit manager on any given day.
Sample size calculation Based on a survey administered at the time of the
final project evaluation in 1999, it was estimated that the proportion of caters correctly administering a full course of CQ to their children would be low (20%). The study aimed to raise the level of correct adminis- tration to at least 50%. The standard formula for the detection of the difference between 2 proportions in a study where randomization is conducted at the indivi- dual level yields a sample size of 45 in each of the intervention and comparison groups. However, rando- mization was carried out at the level of the health zone, so a formula for the comparison of proportions appro- priate for a cluster-randomized trial, which corrects for the design effect (or variance inflation factor) was used. Assuming that follow-up at the household level could be completed on 30 children per health zone over a 3 month period (m = 30 per cluster) and an intra-cluster correlation coefficient (ICC or p) of 0.10 (at the health zone level) yields a sample size (n) of 139 and a mini- mum of 4.64 clusters for each of the intervention and comparison groups. It was found in the analysis that the intra-cluster correlation at the village level was a more important source of variation, which will be addressed below.
Methods of analysis Analysis was carried out using Stata Statistical Soft-
ware, version 7.0 (Stata Corp., College Station, TX, USA) and SPSS, version 10 (SPSS Inc., Chicago, IL, USA). Intra-cluster correlation coefficients were calcu- lated using a one-way analysis of variance for both the health zone and village levels. Analysis of the effect of the intervention on the major outcome variables took into account that significant ICCs were likely to be present at the village level. Random effects regression was used to examine the fixed effects of the intervention while accounting for the random effects of the 51 villages in the study area. Sales of CQ and specific components of compliance in the home were compared using )~2 tests corrected using variance inflation factors to account for correlation in the outcomes present at
the village level This paper will present the results of the random effects regression for the village level, because (i) this analysis in general yielded more con- servative estimates of the effect of the intervention, and (ii) large differences in performance were observed between the managers of village drug kits.
Analysis of referral system through examination of records kept at drug kits and in health centres
The referral notebooks maintained at all village drug kits in the intervention group were examined at the conclusion of the study for all children referred from the inception of the monitoring system for referrals in March 2001 to the end of the study in June 2002, and the registers in the health centres were examined to ascertain the outcome of referral. Only intervention group drug kits were included due to the low numbers of children referred in the comparison group. The out- come of referral was assessed by examining the registers maintained in the CHCs, as well as comments for the drug kit manager written by the health worker in the drug kit referral notebook when he/she discharged the child back to the village. Variables assessed included the proportion of children who reached the health centre, final diagnosis children received, and treatment provided to each child at the health centre.
Results Description of the sample
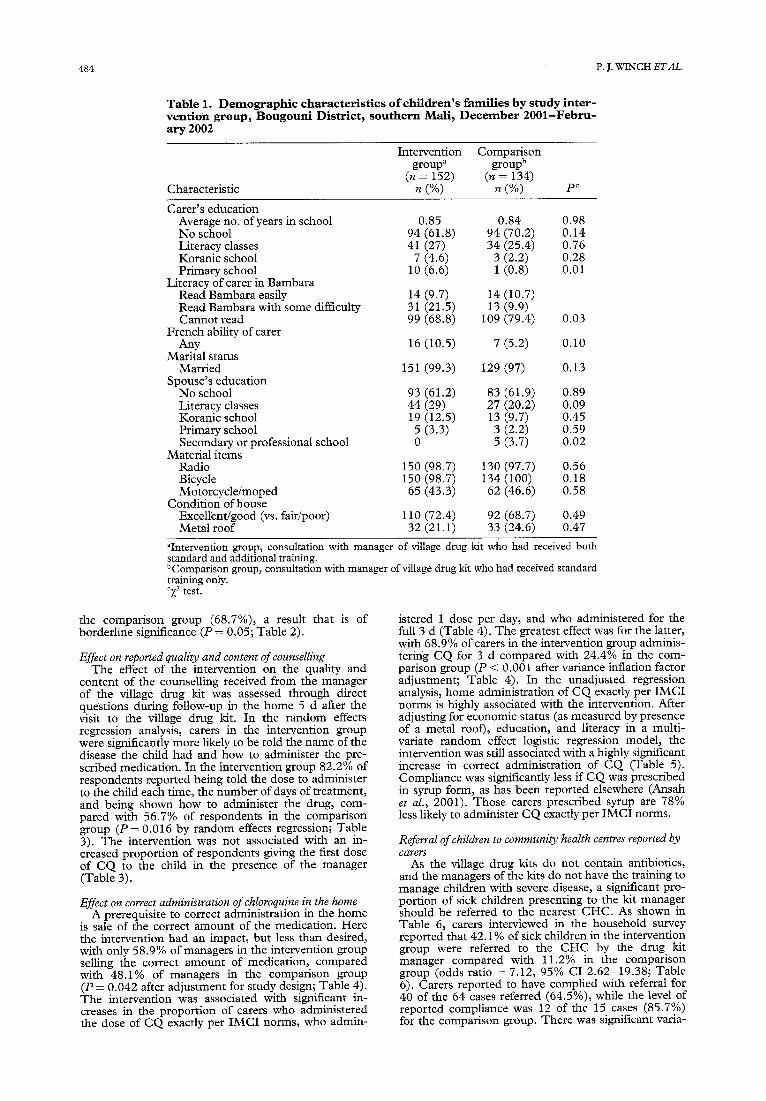
Follow-up was conducted on a total of 286 children coming from 51 villages who had presented with fever to a village drug kit manager and whose cater had been sold CQ as a treatment. The average age of the children treated was 22.4 months, with a standard deviation of 15.9 months and range of I month to 72 months. The 15 field interviewers conducted a mean of 19.1 inter- views each, ranging from 4 to 39. Caters of children in the intervention and comparison groups were compar- able on most measures of education and socio-econom- ic status as shown in Table 1. Caters in the intervention group had slightly higher levels of primary education and ability to read Bambara, the most widely spoken local language in Mali. Significant intra-cluster correla- tions were found at the village level, while correlation at the health zone level was negligible after accounting for intra-village correlations.
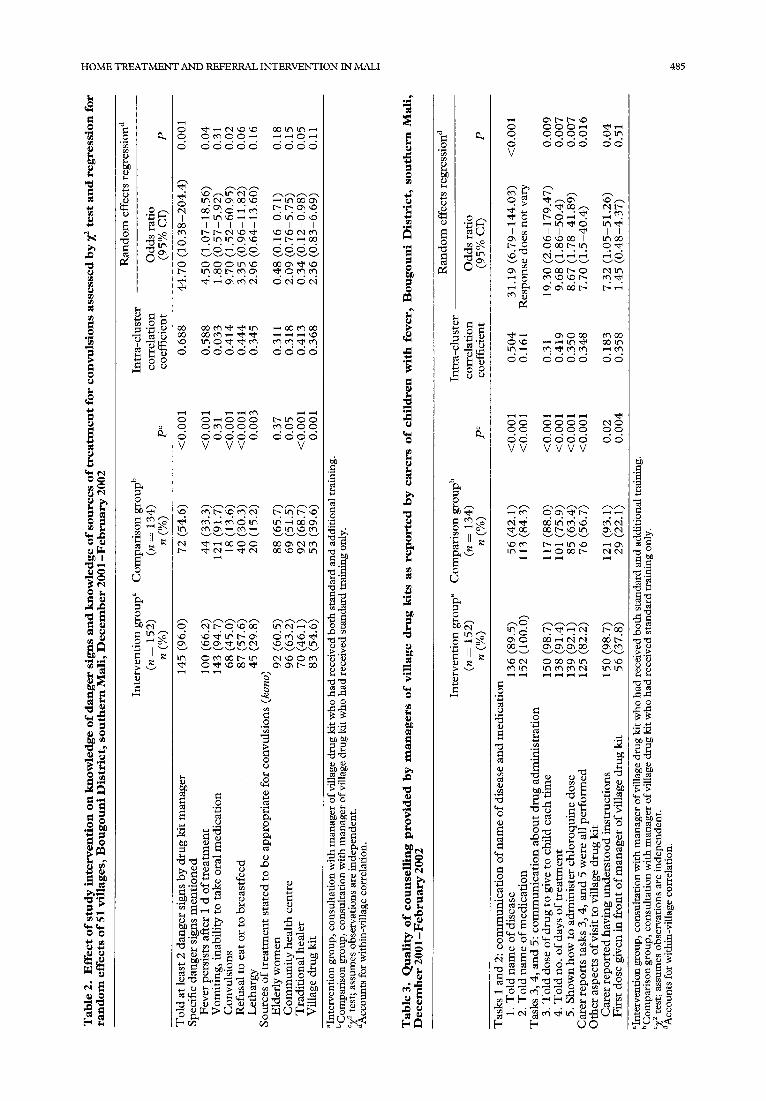
Effect on knowledge of danger signs Managers of the village drug kits were to tell the
child's carer to look out for 5 danger signs. As shown in Table 2, carers in the intervention group were signifi- cantly more likely to report having been told about at least 2 danger signs by the manager of the drug kit ( P = 0.001). The 5 danger signs stressed in the inter- vention were all mentioned with greater frequency by carets in the intervention group, however, only fever lasting more than 1 d and convulsions were signifi- cantly more likely to be mentioned by intervention group respondents (Table 2).
Effect on reported sources of treatments for convulsions There is a term in the Bambara language, kono,
which refers to both convulsions as a symptom, and a locally recognized illness (also with convulsions as a symptom) that is caused by a malevolent bird and traditionally treated by incantations performed by el- derly women and/or traditional healers. Respondents were most likely to state in a closed-ended question that elderly women were a source of treatment for this condition, and the proportion stating so was nearly identical in the intervention (60.5%) and the compari- son (65.7%) groups (Table 2). The intervention is, however, associated with a much lower proportion of respondents stating that traditional healers are a source of treatment for this condition (46.1%) in relation to
484 P.J. WINCH E T A L .
Table 1. Demographic characteristics of children's families by study inter- vention group, Bougouni District, southern Marl, December 2001-Febru- ary 2O02
Intervention Comparison group a group b
(n = 152) (n = 134) Characteristic n (%) n (%) P°
Carer's education Average no. of years in school 0.85 0.84 0.98 No school 94 (61.8) 94 (70.2) 0.14 Literacy classes 41 (27) 34 (25.4) 0.76 Koranic school 7 (4.6) 3 (2.2) 0.28 Primary school 10 (6.6) 1 (0.8) 0.01
Literacy of caret in Bambara Read Bambara easily 14 (9.7) 14 (10.7) Read Bambara with some difficulty 31 (21.5) 13 (9.9) Cannot read 99 (68.8) 109 (79.4) 0.03
French ability of carer Any 16 (10.5) 7 (5.2) 0.10
Marital status Married 151 (99.3) 129 (97) 0.13
Spouse's education No school 93 (61.2) 83 (61.9) 0.89 Literacy classes 44 (29) 27 (20.2) 0.09 Koranic school 19 (12.5) 13 (9.7) 0.45 Primary school 5 (3.3) 3 (2.2) 0.59 Secondary or professional school 0 5 (3.7) 0.02
Material items Radio 150 (98.7) 130 (97.7) 0.56 Bicycle 150 (98.7) 134 (100) 0.18 Motorcycle/moped 65 (43.3) 62 (46.6) 0.58
Condition of house Excellent/good (vs. fair/poor) 110 (72.4) 92 (68.7) 0.49 Metal roof 32 (21.1) 33 (24.6) 0.47
aIntervention group, consultation with manager of village drug kit who had received both standard and additional training. bComparison group, consultation with manager of viUage drug kit who had received standard training only. °X 2 test.
the comparison group (68.7%), a result that is of borderline significance (P = 0.05; Table 2).
Effect on reported quality and content of counselling The effect of the intervention on the quality and
content of the counselling received from the manager of the village drug kit was assessed through direct questions during follow-up in the home 5 d after the visit to the village drug kit. In the random effects regression analysis, caters in the intervention group were significantly more likely to be told the name of the disease the child had and how to administer the pre- scribed medication. In the intervention group 82.2% of respondents reported being told the dose to administer to the child each time, the number of days of treatment, and being shown how to administer the drug, com- pared with 56.7% of respondents in the comparison group ( P = 0.016 by random effects regression; Table 3). The intervention was not associated with an in- creased proportion of respondents giving the first dose of CQ to the child in the presence of the manager (Table 3).
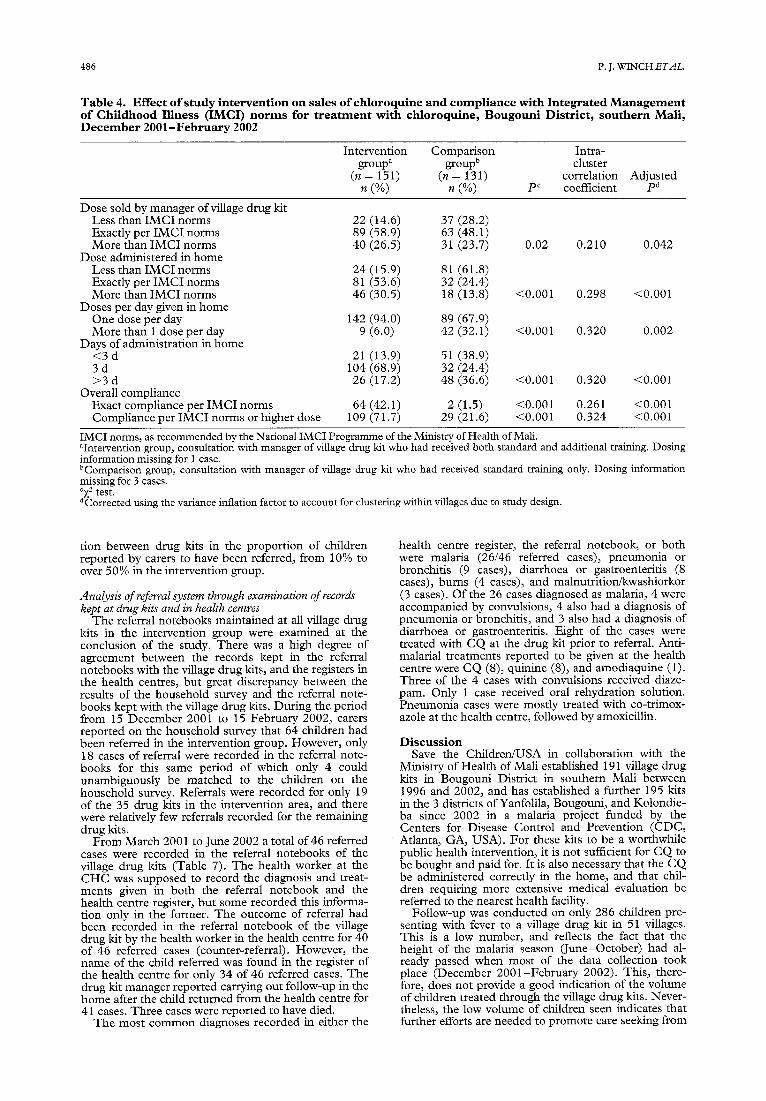
Effect on correct administration of chloroquine in the home A prerequisite to correct administration in the home
is sale of the correct amount of the medication. Here the intervention had an impact, but less than desired, with only 58.9% of managers in the intervention group selling the correct amount of medication, compared with 48.1% of managers in the comparison group (P = 0.042 after adjustment for study design; Table 4). The intervention was associated with significant in- creases in the proportion of caters who administered the dose of CQ exactly per IMCI norms, who admin-
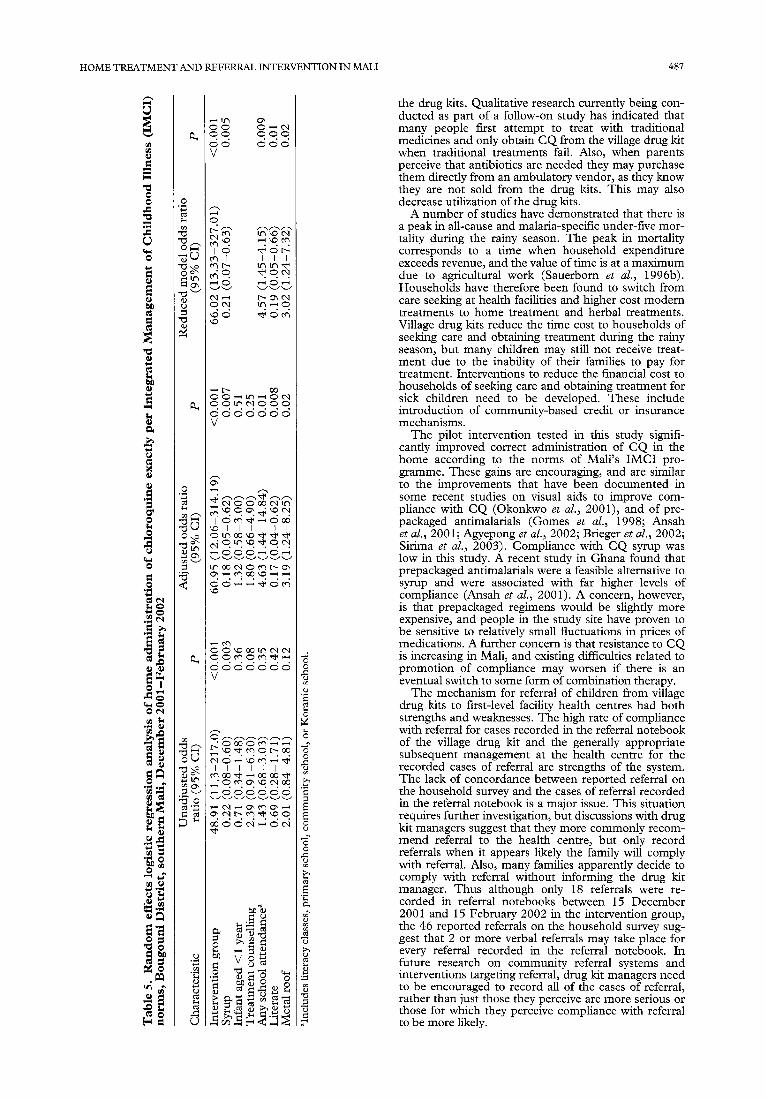
istered 1 dose per day, and who administered for the full 3 d (Table 4). The greatest effect was for the latter, with 68.9% of carers in the intervention group adminis- tering CQ for 3 d compared with 24.4% in the com- parison group (P < 0.001 after variance inflation factor adjustment; Table 4). In the unadjusted regression analysis, home administration of CQ exactly per IMCI norms is highly associated with the intervention. After adjusting for economic status (as measured by presence of a metal roof), education, and literacy in a multi- variate random effect logistic regression model, the intervention was still associated with a highly significant increase in correct administration of CQ (Table 5). Compliance was significantly less if CQ was prescribed in syrup form, as has been reported elsewhere (Ansah et al., 2001). Those carers prescribed syrup are 78% less likely to administer CQ exactly per IMCI norms.
Referral of children to community health centres reported by c a ~
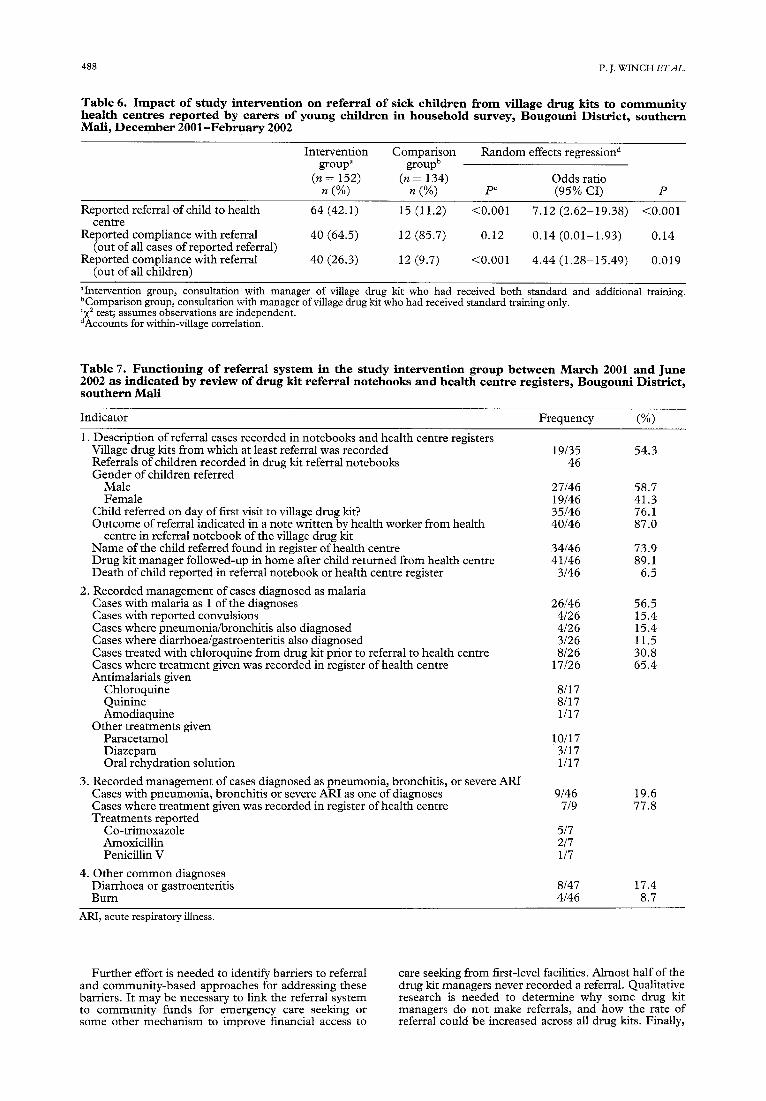
As the village drug kits do not contain antibiotics, and the managers of the kits do not have the training to manage children with severe disease, a significant pro- portion of sick children presenting to the kit manager should be referred to the nearest CHC. As shown in Table 6, carets interviewed in the household survey reported that 42.1% of sick children in the intervention group were referred to the CHC by the drug kit manager compared with 11.2% in the comparison group (odds ratio = 7.12, 95% CI 2.62-19.38; Table 6). Carers reported to have complied with referral for 40 of the 64 cases referred (64.5%), while the level of reported compliance was 12 of the 15 cases (85.7%) for the comparison group. There was significant varia-
HOME TREATMENT AND REFERRAL INTERVENTION IN MALl 485
° ~ ~
0
0
0
% 0
0 r~
0
~s
d d d d d d d d d d
~ d ~ d £ d b b e ~
I I I I I I [ 1 1
£ d £ d d d d d d
4 ~ d d d d M
d d d d d d d d d d
0 ~ 0 0 0 0 0 ~ 0 0 0 d d d d d d V V V V
d d d d V
N
m o m m b m ~ o m
m
0
0 ~
.~ o
,
, ~
~.~,~ = o ~ ~ . ~ ~
O ~ o N
~.8
o 0
o 0
~,~
s ~.~
0 r n . ~
.~N~,
o ' - u 72~<
,,I
~a
..~
0
a 0 "a
01
0
0 0
0
bl~ (xl
~ u'g ~ s
V
• ' 4~ r - ,
, ~ o d,.4'~. ,4 ~. ,,~ - ¢ 4 ~ ' , ,
Oa ~ t r i o 0
d 'a d 4 4 4 4 8
d d d d d d d d
V V V V V V
N~ ~Md% dN
c~o ~c4d
O
i:i O,-~ O
~ ~ " ~ ~ 0 0
• . , - . M . , .
06~4
~,~
O
(no
0
0 0
.o .o ~
e ~,~ e'~ ,..~ . ~
0 m - ~
0 m
486 P.J. WINCH ETAL.
Table 4. Effect o f s tudy intervent ion on sales o f ch loroquine and c o m p l i a n c e with Integrated M a n a g e m e n t o f Chi ldhood I l lness (IMCI) n o r m s for t r e a t m e n t with chloroquine , Bougoun i Distr ic t , southern Mall, D e c e m b e r 2 0 0 1 - F e b r u a r y 2002
Intervention Comparison Intra- group a group b cluster
(n = 151) (n = 131) correlation Adjusted n (%) n (%) pc coefficient pd
Dose sold by manager ofviUage drug kit Less than IMCI norms Exactly per IMCI norms More than IMCI norms
Dose administered in home Less than IMCI norms Exactly per IMCI norms More than IMCI norms
Doses per day given in home One dose per day More than 1 dose per day
Days of administration in home <3 d 3 d > 3 d
Overall compliance Exact compliance per IMCI norms Compliance per IMCI norms or higher dose
22 (14.6) 37 (28.2) 89 (58.9) 63 (48.1) 40 (26.5) 31 (23.7)
24 (15.9) 81 (61.8) 81 (53.6) 32 (24.4) 46 (30.5) 18 (13.8)
0.02 0.210 0.042
<0.001 0.298 <0.001
142 (94.0) 89 (67.9) 9 (6.0) 42 (32.1) <0.001 0.320 0.002
21 (13.9) 51 (38.9) 104 (68.9) 32 (24.4)
26 (17.2) 48 (36.6) <0.001 0.320 <0.001
64 (42.1) 2 (1.5) <0.001 0.261 <0.001 109 (71.7) 29 (21.6) <0.001 0.324 <0.001
IMCI norms, as recommended by the National IMCI Programme of the Ministry of Health of Mall aIntervention group, consultation with manager of village drug kit who had received both standard and additional training. Dosing information missing for 1 case. UComparison group, consultation with manager of village drug kit who had received standard training only. Dosing information missing for 3 cases. c){2 test. aCorrected using the variance inflation factor to account for clustering within villages due to study design.
tion between drug kits in the proportion of children reported by carers to have been referred, from 10% to over 50% in the intervention group.
Analysis of referral system through examination of records kept at drug kits and in health cemres
The referral notebooks maintained at all village drug kits in the intervention group were examined at the conclusion of the study. There was a high degree of agreement between the records kept in the referral notebooks with the village drug kits, and the registers in the health centres, but great discrepancy between the results of the household survey and the referral note- books kept with the village drug kits. During the period from 15 December 2001 to 15 February 2002, carers reported on the household survey that 64 children had been referred in the intervention group. However, only 18 cases of referral were recorded in the referral note- books for this same period of which only 4 could unambiguously be matched to the children on the household survey. Referrals were recorded for only 19 of the 35 drug kits in the intervention area, and there were relatively few referrals recorded for the remaining drug kits.
From March 2001 to June 2002 a total of 46 referred cases were recorded in the referral notebooks of the village drug kits (Table 7). The health worker at the CHC was supposed to record the diagnosis and treat- ments given in both the referral notebook and the health centre register, but some recorded this informa- tion only in the former. The outcome of referral had been recorded in the referral notebook of the village drug kit by the health worker in the health centre for 40 of 46 referred cases (counter-referral). However, the name of the child referred was found in the register of the health centre for only 34 of 46 referred cases. The drug kit manager reported carrying out follow-up in the home after the child returned from the health centre for 41 cases. Three cases were reported to have died.
The most common diagnoses recorded in either the
health centre register, the referral notebook, or both were malaria (26/46 referred cases), pneumonia or bronchitis (9 cases), diarrhoea or gastroenteritis (8 cases), burns (4 cases), and malnutrition/kwashiorkor (3 cases). Of the 26 cases diagnosed as malaria, 4 were accompanied by convulsions, 4 also had a diagnosis of pneumonia or bronchitis, and 3 also had a diagnosis of diarrhoea or gastroenteritis. Eight of the cases were treated with CQ at the drug kit prior to referral. Anti- malarial treatments reported to be given at the health centre were CQ (8), quinine (8), and amodiaquine (1). Three of the 4 cases with convulsions received diaze- pam. Only 1 case received oral rehydration solution. Pneumonia cases were mostly treated with co-trimox- azole at the health centre, followed by amoxicillin.
D i s c u s s i o n Save the Children/USA in collaboration with the
Ministry of Health of Mali established 191 village drug kits in Bougouni District in southern Mall between 1996 and 2002, and has established a further 195 kits in the 3 districts of Yanfolila, Bougouni, and Kolondie- ba since 2002 in a malaria project funded by the Centers for Disease Control and Prevention (CDC, Atlanta, GA, USA). For these kits to be a worthwhile public health intervention, it is not sufficient for CQ to be bought and paid for. It is also necessary that the CQ be administered correctly in the home, and that chil- dren requiring more extensive medical evaluation be referred to the nearest health facility.
Follow-up was conducted on only 286 children pre- senting with fever to a village drug kit in 51 villages. This is a low number, and reflects the fact that the height of the malaria season (June-October) had al- ready passed when most of the data collection took place (December 2001-February 2002). This, there- fore, does not provide a good indication of the volume of children treated through the village drug kits. Never- theless, the low volume of children seen indicates that further efforts are needed to promote care seeking from
H O M E T R E A T M E N T A N D R E F E R R A L I N T E R V E N T I O N I N M A L I 487
0
v
0
0
0
0
o
0 0
o
0
~g
° ~,.,~ . ~
.~°
o
O O O O O V
O
~ 1 I l l
0 0 0 0 0 0 0 V
~ l l l l l l
d e d e d e d V
I I I l I I I ~
d d d N ~ d N ~
i
o ~ .~ ~ V O ~
O "4
O o
Z
<
the drug kits. Qualitative research currently being con- ducted as part of a follow-on study has indicated that many people first attempt to treat with traditional medicines and only obtain CQ from the village drug kit when traditional treatments fail. Also, when parents perceive that antibiotics are needed they may purchase them directly from an ambulatory vendor, as they know they are not sold from the drug kits. This may also decrease utilization of the drug kits.
A number of studies have demonstrated that there is a peak in all-cause and malaria-specific under-five mor- tality during the rainy season. The peak in mortality corresponds to a time when household expenditure exceeds revenue, and the value of time is at a maximum due to agricultural work (Sauerborn et al., 1996b). Households have therefore been found to switch from care seeking at health facilities and higher cost modern treatments to home treatment and herbal treatments. Village drug kits reduce the time cost to households of seeking care and obtaining treatment during the rainy season, but many children may still not receive treat- ment due to the inability of their families to pay for treatment. Interventions to reduce the financial cost to households of seeking care and obtaining treatment for sick children need to be developed• These include introduction of community-based credit or insurance mechanisms.
The pilot intervention tested in this study signifi- cantly improved correct administration of CQ in the home according to the norms of Mali's IMCI pro- gramme. These gains are encouraging, and are similar to the improvements that have been documented in some recent studies on visual aids to improve com- pliance with CQ (Okonkwo et al., 2001), and of pre- packaged antimalarials (Gomes et al., 1998; Ansah et al., 2001; Agyepong et al., 2002; Brieger et al., 2002; Sirima et al., 2003). Compliance with CQ syrup was low in this study. A recent study in Ghana found that prepackaged antimalarials were a feasible alternative to syrup and were associated with far higher levels of compliance (Ansah et al., 2001). A concern, however, is that prepackaged regimens would be slightly more expensive, and people in the study site have proven to be sensitive to relatively small fluctuations in prices of medications. A further concern is that resistance to CQ is increasing in Mali, and existing difficulties related to promotion of compliance may worsen if there is an eventual switch to some form of combination therapy.
The mechanism for referral of children from village drug kits to first-level facility health centres had both strengths and weaknesses. The high rate of compliance with referral for cases recorded in the referral notebook of the village drug kit and the generally appropriate subsequent management at the health centre for the recorded cases of referral are strengths of the system. The lack of concordance between reported referral on the household survey and the cases of referral recorded in the referral notebook is a major issue. This situation requires further investigation, but discussions with drug kit managers suggest that they more commonly recom- mend referral to the health centre, but only record referrals when it appears likely the family will comply with referral. Also, many families apparently decide to comply with referral without informing the drug kit manager. Thus although only 18 referrals were re- corded in referral notebooks between 15 December 2001 and 15 February 2002 in the intervention group, the 46 reported referrals on the household survey sug- gest that 2 or more verbal referrals may take place for every referral recorded in the referral notebook. In future research on community referral systems and interventions targeting referral, drug kit managers need to be encouraged to record all of the cases of referral, rather than just those they perceive are more serious or those for which they perceive compliance with referral to be more likely.
488 P.J. WINCH ETAL.
Table 6. I m p a c t o f s tudy intervent ion on referral o f s ick chi ldren f r o m village d rug kits to c o m m u n i t y heal th centres reported by care t s o f young chi ldren in househo ld survey, B o u g o u n i Dis tr ic t , southern Mali , D e c e m b e r 2001 -February 2002
Intervention Comparison Random effects regression d group a group b
(n = 152) (n = 134) Odds ratio n (%) n (%) pc (95% CI) P
Reported referral of child to health centre
Reported compliance with referral (out of all cases of reported referral)
Reported compliance with referral (out of all children)
64 (42.1) 15 (11.2) <0.001 7.12 (2.62-19.38) <0.001
40 (64.5) 12 (85.7) 0.12 0.14 (0.01-1.93) 0.14
40 (26.3) 12 (9.7) <0.001 4.44 (1.28-15.49) 0.019
alntervention group, consultation with manager of village drug kit who had received both standard and additional training. bComparison group, consultation with manager of village drug kit who had received standard training only. cX2 test; assumes observations are independent. dAccounts for within-village correlation.
Table 7. Funct ion ing o f referral s y s t e m in the study intervent ion group be tween March 2001 and June 2002 as indicated by rev iew o f drug kit referral notebooks and health centre regis ters , Bougouni Dis tr ic t , southern Mali
Indicator Frequency (%)
1. Description of referral cases recorded in notebooks and health centre registers Village drug kits from which at least referral was recorded 19/35 54.3 Referrals of children recorded in drug kit referral notebooks 46 Gender of children referred
Male 27/46 58.7 Female 19/46 41.3
Child referred on day of first visit to village drug kit? 35/46 76.1 Outcome of referral indicated in a note written by health worker from health 40/46 87.0
centre in referral notebook of the village drug kit Name of the child referred found in register of health centre 34/46 73.9 Drug kit manager followed-up in home after child returned from health centre 41/46 89.1 Death of child reported in referral notebook or health centre register 3/46 6.5
2. Recorded management of cases diagnosed as malaria Cases with malaria as 1 of the diagnoses 26/46 56.5 Cases with reported convulsions 4/26 15.4 Cases where pneumonia/bronchitis also diagnosed 4/26 15.4 Cases where diarrhoea/gastroenteritis also diagnosed 3/26 11.5 Cases treated with chloroquine from drug kit prior to referral to health centre 8/26 30.8 Cases where treatment given was recorded in register of health centre 17/26 65.4 Antimalarials given
Chloroquine 8/17 Quinine 8/17 Amodiaquine 1/17
Other treatments given Paracetamol 10/17 Diazepam 3/17 Oral rehydration solution 1/17
3. Recorded management of cases diagnosed as pneumonia, bronchitis, or severe ARI Cases with pneumonia, bronchitis or severe ARI as one of diagnoses 9/46 19.6 Cases where treatment given was recorded in register of health centre 7/9 77.8 Treatments reported
Co-trimoxazole 5/7 Amoxicillin 2/7 Penicillin V 1/7
4. Other common diagnoses Diarrhoea or gastroenteritis 8/47 17.4 Burn 4/46 8.7
ARI, acute respiratory illness.
Further effort is needed to identify barriers to referral and community-based approaches for addressing these barriers. It may be necessary to link the referral system to community funds for emergency care seeking or some other mechanism to improve financial access to
care seeking from first-level facilities. Almost half of the drug kit managers never recorded a referral. Qualitative research is needed to determine why some drug kit managers do not make referrals, and how the rate of referral could be increased across all drug kits. Finally,
HOME TREATMENT AND REFERRAL INTERVENTION IN MALI 489
of the recorded referrals with a diagnosis of malaria, only 31% were treated with C Q prior to referral. Referral may therefore be contributing to a delay in the initiation of therapy, and consideration should be given to having all drug kit managers give an initial t reatment with C Q prior to referral if the child is able to take oral medication.
Analysis methods were used that are appropriate for cluster-randomized trials. Intra-cluster correlation co- efficients were negligible for the health zone level and usually found to be within 0.3 and 0.5 for the village levels. This indicates that respondents from the same village have reported knowledge and behaviours more similar to others in the same village than to those in other villages. Reasons for this phenomenon include (i) everyone in each village visits and is counselled by the same drug kit manager, (ii) people in each village may interact with each other and share information they heard during their visit to the drug kit manager , and (iii) more than 1 child from same extended family was sometimes treated during the period of the study.
E t h i c a l s t a t e m e n t Ethical clearance was granted by the Commi t t ee on
H u m a n Research at the Johns Hopkins School of Pub- lic Health, M D , U S A and by the Ethical Commi t t ee of the Universi ty of Mall School of Medicine, Pharmacy, and Dentistry.
Acknowledgements We thank the Director General of Health for Sikasso Region
Dr Brahima Konr, the District Medical Officer for Bougouni District Dr Drissa Ouattara, and Maureen Cunningham, Patrick Connors and Lynn Lederer and the field staff of Save the Children/USA for their partnership and facilitation of all aspects of data collection during this study. We also wish to thank the other district level authorities, community leaders, and health workers who granted us permission to enter their communities and collect data. Finally, we acknowledge the contribution of Robert Black, Ruth Frischer, and Neal Brandes for their continued support and encouragement. This work was supported financially by the United States Agency for Interna- tional Development through the Family Health and Child Survival Cooperative Agreement (HRN-A-00-96-90006-00) with Johns Hopkins Bloomberg School of Public Health.
References Agyepong, I. A., Ansah, E., Gyapong, M., Adjei, S., Barnish,
G. & Evans, D. (2002). Strategies to improve adherence to recommended chloroquine treatment regimes: a quasi- experiment in the context of integrated primary health care delivery in Ghana. Social Science and Medicine, 55, 2215-2226.
Ansah, E. K., Gyapong, J. O., Agyepong, I. A. & Evans, D. B. (2001). Improving adherence to malaria treatment for chil- dren: the use of pre-packed chloroquine tablets vs. chloro- quine syrup. Tropical Medicine and International Health, 6, 496-504.
Brieger, W. R., Salako, L. A., Umeh, R. E., Agomo, P. U., Afolabi, B. M. & Adeneye, A. K. (2002). Promoting pre- packaged drugs for prompt and appropriate treatment of febrile illnesses in rural Nigerian communities. International Quarterly of Community Health Education, 21, 19-40.
Delley, V., Bouvier, P., Breslow, N., Doumbo, O., Sagara, I., Diakite, M., Mauris, A., Dolo, A. & Rougemont, A. (2000). What does a single determination of malaria parasite density mean? A longitudinal survey in Mall Tropical Medicine and International Health, 5, 404-412.
Djimde, A., Howe, C. V., Diop, S., Dicko, A., Wellems, T. E. & Doumbo, O. (1998). Use of antimalarial drugs in Mall: policy versus reality. American Journal of Tropical Medicine and Hygiene, 59, 376-379.
Donner, A. & Klar, N. (2000). Design and Analysis of Cluster Randomization Trials in Health Research. London: Arnold Publishers.
Font, F., Quinto, L., Masanja, H., Nathan, R., Ascaso, C., Menendez, C., Tanner, M., Schellenberg, J. & Alonso, P. (2002). Paediatric referrals in rural Tanzania: the Kilo- mbero District Smdy--a case series. BMC International Health and Human Rights, 2, 4.
Ghebreyesus, T. A., Alemayehu, T., Bosman, A., Witten, K. H. & Te!dehaimanot, A. (1996). Community participation in malaria control in Tigray region Ethiopia. Acta Tropica, 61, 145-156.
Gilroy, K., Winch, P. J., Diawara, A., Swedberg, E., Thi6ro, E., Kan6, M., Daou, Z., Berth6, Z. & Bagayoko, A. (in press). Impact of IMCI training and language used by provider on quality of counseling provided to parents of sick children in Bougouni District, Mall Patient Education and Counseling.
Gomes, M., Wayling, S. & Pang, L. (1998). Interventions to improve the use of antimalarials in south-east Asia: an over- view. Bulletin of the World Health Organization, 76, supple- ment 1, 9-19.
Katz, K. R., West, C. G., Doumbia, F. & Kane, F. (1998). Increased access tO family planning services in rural Mall through community-based distribution. International Family Planning Perspectives, 24, 104-110.
Kidane, G. & Morrow, R. H. (2000). Teaching mothers to provide home treatment of malaria in Tigray, Ethiopia: a randomised trial. Lancet, 356, 550-555.
Krause, G., Benzler, J., Heinmuller, R., Borchert, M., Ko0b, E., Ouattara, K. & Diesfeld, H. J. (1998). Performance of village pharmacies and patient compliance after implemen- tation of essential drug programme in rural Burkina Faso. Health Policy and Planning, 13, 159-166.
Kreft, I. & De Leeuw, J. (1998). Introducing Multilevel Model- ing. Thousand Oaks, California: Sage Publications.
Makemba, A. M., Winch, P. J., Makame, V. M., Mehl, G. L., Premji, Z., Minjas, J. N. & Shift, C. J. (1996). Treatment practices for degedege, a locally recognized febrile illness, and implications for strategies to decrease mortality from severe malaria in Bagamoyo District, Tanzania. Tropical Medicine and International Health, 1, 305 -313.
Marsh, V. M., Mutemi, W. M., Muturi, J., Haaland, A., Watkins, W. M., Otieno, G. & Marsh, K. (1999). Changing home treatment of childhood fevers by training shop keepers in rural Kenya. Tropical Medicine and International Health, 4, 383-389.
McCombie, S. C. (1996). Treatment seeking for malaria: a review of recent research. Social Science and Medicine, 43, 933-945.
Ngoh, L. N. & Shepherd, M. D. (1997). Design, develop- ment, and evaluation of visual aids for communicating prescription drug instructions to nonliterate patients in rural Cameroon. Patient Education and Counseling, 31,245-261.
Okanurak, K. & Ruebush, T. K. 2nd (1996). Village-based diagnosis and treatment of malaria. Acta Tropica, 61, 157-167.
Okonkwo, P. O., Akpala, C. O., Okafor, H. U., Mbah, A. U. & Nwaiwu, O. (2001). Compliance to correct dose of chloroquine in uncomplicated malaria correlates with im- provement in the condition of rural Nigerian children. Transactions of the Royal Society of Tropical Medicine and Hygiene, 95, 320-324.
Oshiname, F. O. & Bricger, W. R. (1992). Primary care training for patent medicine vendors in rural Nigeria. Social Science and Medicine, 35, 1477 - 1484.
Pagnoni, F., Convelbo, N., Tiendrebeogo, J., Cousens, S. & Esposito, F. (1997). A community-based programme to provide prompt and adequate treatment of presumptive malaria in children. Transactions of the Royal Society of Tropical Medicine and Hygiene, 91, 512- 517.
Howe, C. V., Doumbo, O. K., Djimde, A., Kayentao, K., Diourte, Y., Doumbo, S. N., Coulibaly, D., Thera, M., Wellems, T. E. & Diallo, D. A. (2001). Chloroquine treat- ment of uncomplicated Plasmodium falciparum malaria in Mall: parasitologic resistance versus therapeutic efficacy. American Journal of Tropical Medicine and Hygiene, 64, 242-246.
Ruebush, T. K. 2nd & Godoy, H. A. (1992). Community participation in malaria surveillance and treatment. I. The Volunteer Collaborator Network of Guatemala. American ffournal of Tropical Medicine and Hygiene, 46, 248-260.
Sauerborn, R., Adams, A. & Hien, M. (1996a). Household strategies to cope with the economic costs of illness. Social Science and Medicine, 43, 291-301.
Sauerborn, R., Nougtara, A., Hien, M. & Diesfeld, H. J. (1996b). Seasonal variations of household costs of illness in Burkina Faso. Social Science and Medicine, 43, 281-290.
Sirima, S. B., Konate, A., Tiono, A. B., Convelbo, N., Cousens, S. & Pagnoni, F. (2003). Early treatment of child- hood fevers with pre-packaged antimalarial drugs in the home reduces severe malaria morbidity in Burkina Faso. Tropical Medicine and lnternational Health, 8, 133-139.

490 P.J. WINCH ETAL.
Smith, P. & Morrow, R. (editors) (1996). Field Trials of Health Intewentions in Developing Countries. London: Macmillan Education.
Th6ra, M. A., D'Alessandro, U., Thiero, M., Ouedraogo, A., Packou, J., Souleymane, O. A., Fane, M., Ade, G., Alvez, F. & Doumbo, O. (2000). Child malaria treatment practices among mothers in the district of Yanfolila, Sikasso region, Mali. Tropical Medicine and International Health, 5, 876-881.
Tomkins, A. (1993). Environment, season and infection. In: Seasonali~y and Human Ecology. Ulijaszek, S. J. & Stricldand, S. S. (editors). Cambridge UK: Cambridge University Press, pp. 123-134.
Wears, R. L. (2002). Advanced statistics: statistical methods for analyzing cluster and cluster-randomized data. Academic Emergency Medicine, 9, 330-341.
Winch, P. J., LeBan, K., Casazza, L., Walker, L. & Pearcy, K. (2002). An implementation framework for household and community integrated management of childhood illness. Health Policy and Planning, 17, 345-353.
Received 18 December 2002; revised 23 April 2003; accepted for publication 25 April 2003
Book Review
Antibiot ic and C h e m o t h e r a p y . Ant i - infect ive Agents and their use in Therapy, 8th edition. Roger G. Finch, David Greenwood, S. Ragnar Norrby & Richard J. Whitley (editors). Edinburgh, London, New York, Philadelphia, St Louis, Sydney, Toronto: Churchill Livingstone, 2003. xii + 964 pp. Price £115.00. ISBN 0443071292.
This book is a manual of antibiotic and chemo- therapy therapy. It is now in its eighth edition in 30 years and the rapid growth of information on these subjects is such that the volume has to be updated at intervals of less than 4 years. The original was a manual in a real sense in that it was small enough to carry around. There were only a few groups of antibiotics in 1963. Mary Barber and Lawrence Garrod performed a great job of compression and summarized the informa- tion with such characteristic lucidity that its value to laboratory workers and clinicians alike was immediately recognized. This work was carried on with Harold Lambert and Francis O'Grady for many subsequent editions.
As the editors point out, along with other contribu- tors to the book, the second gold rush of antibiotics/ chemotherapy starting in the late 1960s has enormously increased the range of agents which now have to be discussed. The editors and authors have won one battle; they maintain the book as a concise summary of the state of knowledge of the agents available for treat- ing infections (bacterial, viral, fungal, and parasitic) and provide advice on how to use these agents. There is not a lot of superfluity. They have not won the unwin- nable battle against the inexorable increase in size and weight. The rapid expansion in the number of effective agents and the widening range of infections amenable to antimicrobial agents means that the size of successive editions has continually increased. The number of pub- lications dealing with antibiotics is now at a level that the useful knowledge--essential knowledge much of i t -- that needs distilling into an antibiotic manual is enormous. So the distillate gets bigger. But it is still a distillate~a source of valuable information but no longer easy to carry around.
In some instances the distillate of information could have been larger. The general chapters cover 13 major subjects such as antibiotic resistance, pharmacody- namics, laboratory testing and assays, and effects on the immune system. It is difficult to shoehorn the essential information on these subjects into a few pages. The authors have had to be very selective in what they are able to include and sometimes too little space has been available. Similarly, the authors writing the 27 chapters on specific antimicrobial agents have also had
to be sparing on the information. Each of the com- pounds mentioned has a standardized entry with anti- microbial activity, resistance, pharmacokinetics (not pharmacodynamics), and clinical uses. The essentials are in, but only essentials are possible with so many compounds to be included. The major, frequently used, classes (such as beta-lactams, quinolones, and macrolides) quite rightly get the major share of the space. Is there sufficient information to satisfy all the readers of this book? Maybe some need more and the further reading section becomes very important in this section of the book.
The third section relating to the use of antibiotics is fully referenced, as are the chapters in the general section. Despite the similarities of the chapter headings to those in the seventh edition the text shows many changes with many new experts contributing to the book and with much of the text presenting new data. A different system of referencing has been used in the eighth edition so it is not easy to see how much still remains. In general, there is more detailed information on management of a wide variety of infections making this the most updated part of the book. There is, how- ever, much non-antibiotic-related material on patho- genesis, epidemiology, clinical and microbiological diagnosis, prevention of infection, and hospital infec- tion control. The difference in emphasis comes in the first of these chapters where 'Septicaemia' becomes 'Sepsis'. The material in this and in subsequent chap- ters is interesting, well written, and accurate but some is not essential to the use of antibiotics. Do we really need 40 pages on implanted medical devices with 549 references? Pharmacodynamics has only 10 pages and 25 references and laboratory control of antibiotic ther- apy 7 pages and 6 references. Some authors appear to have stuck closely to the aim of being a user's guide to antimicrobial therapy and have dealt predominantly with the antimicrobial treatment of infection.
This is an edition worthy of its illustrious predeces- sors. Some other infection 'Classics' have gone down the road of splitting the contents into 2 or more separate volumes. There is certainly a need for a refer- ence bible containing the data previously available in Antibiotika Fibel. The second section of this book could well form the basis for a modern Fibel. A volume 2 with some of the general chapters and those on clinical uses would become portable and more easily available where most needed--at the patient's bedside.
J. D . Wi l l i ams Editor-in-chief International Journal of Antimicrobial Agents FESCI/ECC Office 31 St Olav's Court 25 Lower Road London ES16 2XB, UK