
Camel Brucellosis: Evaluation of field sera by conventional serological tests and ELISA.
Upload
independentCategory
view
1download
0
1160
INCREASED LEVELS OF SOLUBLE TUMOR NECROSIS FACTOR RECEPTORS
IN THE SERA AND SYNOVIAL FLUID OF PATIENTS WITH RHEUMATIC DISEASES
ANDREW P. COPE, DAN ADERKA, MICHAEL DOHERTY, HARTMUT ENGELMANN, DEENA GIBBONS, ADRIAN C. JONES, FIONULA M. BRENNAN, RAVINDER N. MAINI,
DAVID WALLACH, and MARC FELDMANN
Objective. Recently, 2 classes of cytokine inhibi- tors have been defined at the molecular level. The largest group comprises the extracellular domains of cell surface cytokine receptors, and includes both tumor necrosis factor receptors (TNF-R). The present study was conducted to investigate the role of TNF inhibitors in arthritis.
Methods. We measured p55 and p75 soluble TNF-R (sTNF-R) in serum and synovial fluid (SF)
From The Mathilda and Terence Kennedy Institute of Rheumatology, Bute Gardens and Sunley Research Centre, Lon- don, the Rheumatology Unit, City Hospital, Nottingham, United Kingdom, the Department of Medicine T, Souraski-Tel-Aviv Med- ical Centre, Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, and the Department of Molecular Genetics and Virology, Weizmann Institute of Science, Rehovot, Israel.
Supported by the Arthritis and Rheumatism Council of Britain, by The Wellcome Trust, and by the Medical Research Council of Britain.
Andrew P. Cope, MD: The Mathilda and Terence Kennedy Institute of Rheumatology, Sunley Research Centre; Dan Aderka, MD: Department of Medicine T, Souraski-Tel-Aviv Medical Centre, Sackler Faculty of Medicine, Tel-Aviv University; Michael Doherty, MD: Rheumatology Unit, City Hospital, Nottingham; Hartmut Engelmann, MD, PhD: Department of Molecular Genetics and Virology, Weizmann Institute of Science; Deena Gibbons, BSc: The Mathilda and Terence Kennedy Institute of Rheumatology, Sunley Research Centre; Adrian C. Jones, MD: Rheumatology Unit, City Hospital, Nottingham; Fionula M. Brennan, PhD: The Mathilda and Terence Kennedy Institute of Rheumatology, Sunley Research Centre; Ravinder N. Maini, MD: The Mathilda and Terence Kennedy Institute of Rheumatology, Bute Gardens; David Wallach, PhD: Department of Molecular Genetics and Virology, Weizmann Institute of Science; Marc Feldmann, MD, PhD: The Mathilda and Terence Kennedy Institute of Rheumatology, Sunley Research Centre.
Address reprint requests to Marc Feldmann, MD, PhD, The Mathilda and Terence Kennedy Institute of Rheumatology, Sunley Research Centre, 1 Lurgan Avenue, Hammersmith, London W6 8LW, UK.
Submitted for publication January 15, 1992; accepted in revised form March 24, 1992.
samples from patients with rheumatic diseases and compared their levels with levels of soluble interleukin-2 receptors (sIL-2R). Sensitive enzyme-linked immuno- sorbent assays (ELISA), specific for p55 and p75 sTNF-R and for sIL-~R, were used.
Results. Serum levels of p75 sTNF-R were 3-4- fold higher than levels of p55 sTNF-R, and both were significantly elevated in patients with osteoarthritis (OA) and rheumatoid arthritis (RA) compared with healthy controls. RA SF levels of sTNF-R were 4-5-fold higher than levels in serum, suggesting local production in the joint, and were significantly higher than levels in the SF of patients with seronegative arthropathy or OA. Fur- thermore, levels of p55 and p75 sTNF-R, but not sIL-2R or TNFa measured by ELISA, were increased in the SF of patients with clinically active RA. The soluble TNF-R in RA and OA SF were functional since they inhibited TNF activity in a cytotoxicity assay in proportion to the levels of inhibitor present. Evaluation of serially ob- tained serum samples suggested that sTNF-R may be a useful parameter for monitoring RA disease activity.
Conclusion. Biologically active soluble TNF-R are up-regulated in patients with rheumatic disease and are produced locally in the joints. Measurement of serum levels of TNF-R may be useful for monitoring of disease, and determination of SF levels could be of diagnostic value.
Tumor necrosis factor a (TNFa) is an inducible cytokine produced primarily by monocytes and macrophages. Many biologic activities of TNFa ap- pear to be involved in the pathogenesis of chronic inflammation and arthritis. Thus, TNFa can induce resorption of cartilage and bone (1,2), endothelial adherence and activation of granulocytes (3,4), class I
Arthritis and Rheumatism, Vol. 35, No. 10 (October 1992)

SOLUBLE TNF RECEPTORS IN RHEUMATIC DISEASE 1161
major histocompatibility complex expression (3, stim- ulation of fibroblast growth via platelet-derived growth factor (6), and stimulation of synovial cell prostaglan- din E, and collagenase production (7). Experiments demonstrating the neutralizing effects of anti-TNFa antibody on interleukin- 1 (IL-1) (8) and granulocyte- macrophage colony-stimulating factor (GM-CSF) pro- duction (9) in rheumatoid synovial joint cell cultures confirmed the notion that T N F a has a significant role in arthritis. The in vivo protective effects of anti-TNFa in the collagen-induced arthritis model in DBA/1 mice (10) have provided further support for our hypothesis that T N F a is pivotal in the pathogenesis of rheumatoid arthritis (RA) (8,9,11).
TNFa and T N F p bind to 2 high-affinity cell surface receptors (TNF-R) of MW 55 kd and 75 kd, respectively, which have been recently cloned and expressed (12-17). One or more of these receptors are present on virtually all cell types, including T cells, macrophages, and neutrophils, and they mediate the biologic effects of TNF. Cytokine inhibitors have been found in biologic fluids (18); in particular, inhibitors of TNFa bioactivity have been detected in the blood and urine of healthy subjects and patients with fever (19-21). Recent serologic and sequencing studies have shown that these inhibitors represent shed cell surface receptors, which may function as natural regulators of TNF activity (17,19,21).
Two proteins of -30 kd, termed TNF binding proteins I and 11, have been isolated and purified to homogeneity from the urine of healthy individuals (19). These binding proteins represent the naturally occurring shed receptors for the 55-kd and 75-kd surface proteins, respectively, and have been shown to retain the ability to bind T N F a and, to a lesser extent, TNFP. In in vitro assays, they inhibit the effects of T N F (19,21,22). Specific monoclonal anti- bodies (MAb) have been raised against these proteins and used to develop highly sensitive enzyme-linked immunosorbent assays (ELISAs) for both TNF-R (23), which are hereinafter referred to as p55 sTNF-R and
We have recently shown that both membrane forms of TNF-R are up-regulated on synovial mono- nuclear cells, at both the protein and messenger RNA (mRNA) levels (24), and have confirmed these findings in synovial tissue by immunohistochemical studies (25). We were therefore interested to study the pro- duction of TNF-R in synovial joints at sites of en- hanced T N F a and TNF-R production, in order to gain a clearer understanding of the interactions between
p75 sTNF-R.
these molecules in RA. Using ELISAs for p55 sTNF-R and p75 sTNF-R, we investigated whether levels of TNF-R were increased in the sera and synovial fluids (SF) of patients with rheumatic disease. In addition, we used a commercially available ELISA to compare soluble IL-2 receptor (sIL-2R) levels with those of both sTNF-R, since elevated levels of sIL-2R in serum and S F have also been described in patients with rheumatic disease (26).
PATIENTS AND METHODS Patient selection. One hundred forty patients with
rheumatic diseases, seen in the Departments of Rheumatol- ogy at Charing Cross Hospital and the Nottingham City Hospital, were studied. An age-matched control group com- prised 38 healthy volunteers with a median age of 69 years (range 25-82 years).
Among the study patients, 74 (median age 66 years, range 25-82) had classic or definite RA according to the American College of Rheumatology (formerly, the American Rheumatism Association) criteria (27) and 41 (median age 69, range 45-8 1 ) had clinically and radiologically diagnosed osteoarthritis (OA), predominantly involving the knee. Twenty-five patients (median age 44, range 22-68) had seronegative polyarthropathy, including 4 with psoriatic arthritis, 2 with ankylosing spondylitis, 2 with Reiter’s syndrome, and 17 with chronic polyarthropathy of undefined origin. The majority of patients with OA, RA, and seroneg- ative arthritis were being treated with nonsteroidal anti- inflammatory drugs (NSAIDs). In addition, several of the patients with RA and seronegative arthritis were receiving a disease-modifying antirheumatic drug (DMARD), i.e., sul- fasalazine (n = 18), methotrexate (n = 8), gold salts (n = 8), D-penicillamine (n = 2), azathioprine (n = l), or hydroxy- chloroquine (n = l ) , either alone, or in combination with low-dose prednisolone (n = 11).
Clinical evaluation. To evaluate the relationship be- tween SF sTNF-R levels and clinical disease activity of the affected joint, knees were examined and assessed by a single observer (MD) for clinical parameters of inflammation as previously described (28). Using a summed score based on 6 features (duration of early morning and inactivity stiffness, warmth, joint tenderness, effusion, and synovial thickening), the joint was globally defined as having “high inflammatory activity” if 4-6 parameters were present, and “low inflam- matory activity” if 1 2 were present. Intermediate scores of 3 were not included.
Sample preparation. A total of 88 serum and 149 SF samples were collected consecutively and coded. Sera were stored at -20°C until assayed. All SF samples were aspi- rated from knee joints. Samples were treated with bovine testicular hyaluronidase (1,500 unitdml; Sigma, St. Louis, MO) for 30 minutes at 37°C prior to centrifugation at 2,200 revolutions per minute for 12 minutes, and stored at -20°C. This pretreatment had no effect on the functions studied in this investigation. Included in the above samples were paired sera and SF from patients with RA (n = 30) and seronegative arthritis (n = 19). Laboratory parameters recorded for the patients included Westergren erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and hemoglobin levels.
1162 COPE ET AL
6 40-
2 . Y
2 30- z k . $ 20- P
10 -
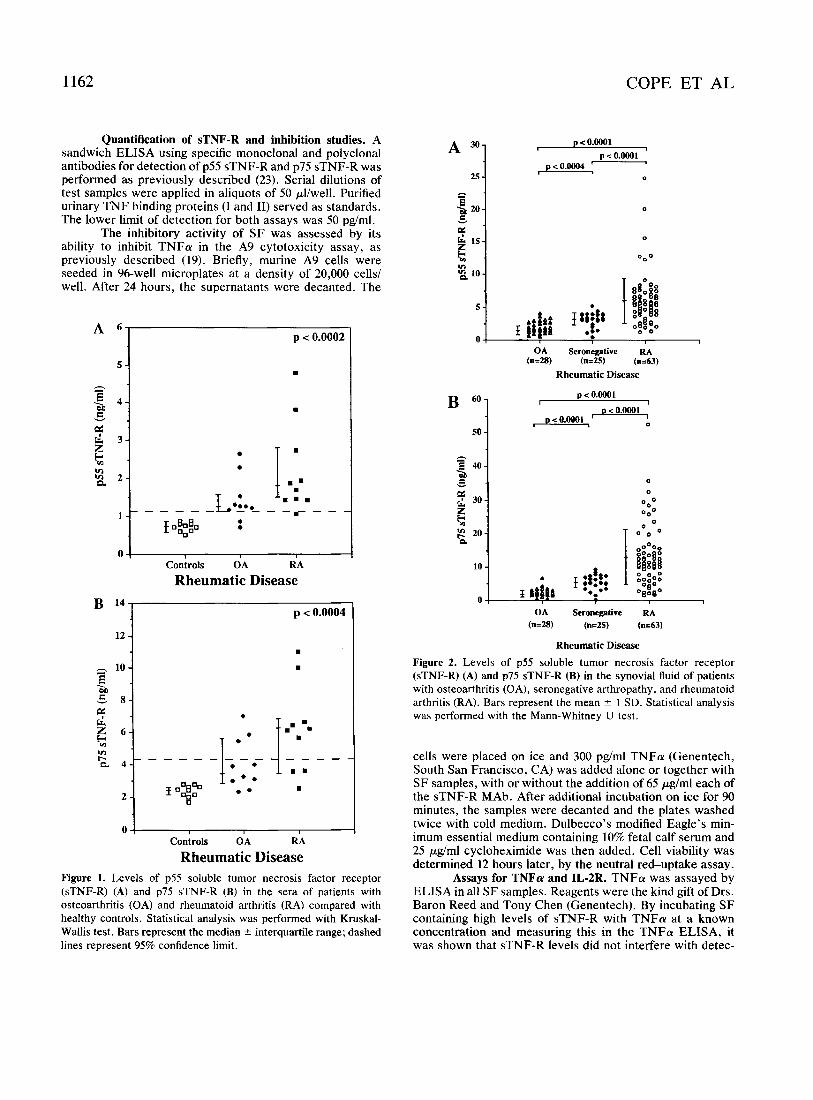
Quantification of sTNF-R and inhibition studies. A sandwich ELISA using specific monoclonal and polyclonal antibodies for detection of p55 sTNF-R and p75 sTNF-R was performed as previously described (23). Serial dilutions of test samples were applied in aliquots of 50 pl/well. Purified urinary TNF binding proteins (I and 11) served as standards. The lower limit of detection for both assays was 50 pg/ml.
The inhibitory activity of SF was assessed by its ability to inhibit TNFa in the A9 cytotoxicity assay, as previously described (19). Briefly, murine A9 cells were seeded in 96-well microplates at a density of 20,000 cells/ well. After 24 hours, the supernatants were decanted. The
p c 0.0002 A 6
1 - -€A-
*
I .=. =:= - - r - -
Controls OA RA Rheumatic Disease
p c 0.0004 B 14
O ! I I I I
Rheumatic Disease Controls OA RA
Figure 1. Levels of p55 soluble tumor necrosis factor receptor (sTNF-R) (A) and p75 sTNF-R (B) in the sera of patients with osteoarthritis (OA) and rheumatoid arthritis (RA) compared with healthy controls. Statistical analysis was performed with Kruskal- Wallis test. Bars represent the median -C interquartile range; dashed lines represent 95% confidence limit.
< o.oO01 1
p c o.oO01 "'1 25 'L pco.oO04 - 0
0
OA Seronegative RA (n=28) (n=25) (n=63)
Rheumatic Disease
p c o.oO01
pco.oO01 50
0 L
0
0
0 O 0
0 O 0
OA Seronegative RA (n=28) (n=25) (n=63)
Rheumatic Disease
Figure 2. Levels of p55 soluble tumor necrosis factor receptor (sTNF-R) (A) and p75 sTNF-R (B) in the synovial fluid of patients with osteoarthritis (OA), seronegative arthropathy, and rheumatoid arthritis (RA). Bars represent the mean ? 1 SD. Statistical analysis was performed with the Mann-Whitney U test.
cells were placed on ice and 300 pg/ml TNFa (Genentech, South San Francisco, CA) was added alone or together with S F samples, with or without the addition of 65 pg/ml each of the sTNF-R MAb. After additional incubation on ice for 90 minutes, the samples were decanted and the plates washed twice with cold medium. Dulbecco's modified Eagle's rnin- irnum essential medium containing 10% fetal calf serum and 25 pg/ml cycloheximide was then added. Cell viability was determined 12 hours later, by the neutral red-uptake assay.
Assays for TNFa and IL3R. TNFa was assayed by ELISA in all SF samples. Reagents were the kind gift of Drs. Baron Reed and Tony Chen (Genentech). By incubating SF containing high levels of sTNF-R with TNFa at a known concentration and measuring this in the TNFa ELISA, it was shown that sTNF-R levels did not interfere with detec-
SOLUBLE TNF RECEPTORS IN RHEUMATIC DISEASE 1163
A l o -
9 -
8 -
I -
- - 6 -
v
2 5 - z k 2 4 - n
3 -
2 -
1 -
B 35-
30-
25 - h - E 2 2 0 - v
2 z + n
; 1 5 - I-
10 -
5 -
0 -
p c 0.0001
I I
0 - Serum synovial fluid
R A sample
p c 0.0001
I
Serum synovial fluid
RA sample
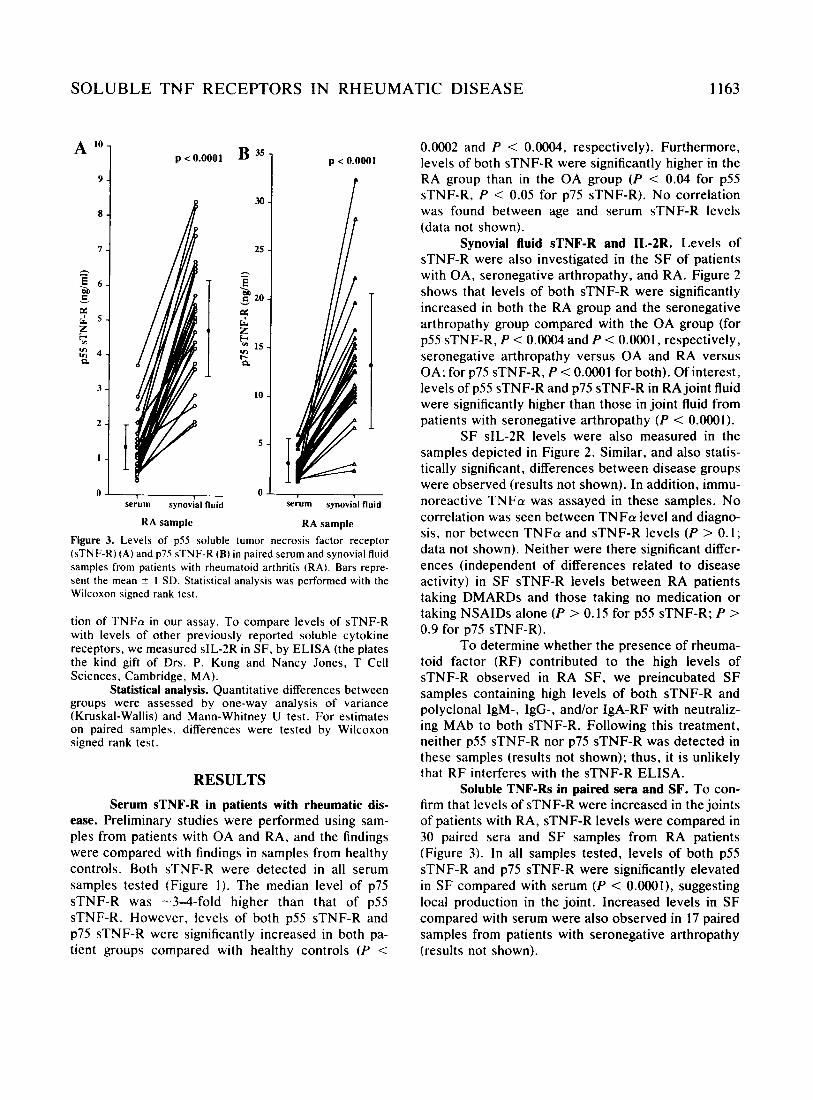
Figure 3. Levels of p5S soluble tumor necrosis factor receptor (sTNF-R) (A) and p75 sTNF-R (B) in paired serum and synovial fluid samples from patients with rheumatoid arthritis (RA). Bars repre- sent the mean ? I SD. Statistical analysis was performed with the Wilcoxon signed rank test.
tion of TNFa in our assay. To compare levels of sTNF-R with levels of other previously reported soluble cytokine receptors, we measured sIL-2R in SF, by ELISA (the plates the kind gift of Drs. P. Kung and Nancy Jones, T Cell Sciences, Cambridge, MA).
Statistical analysis. Quantitative differences between groups were assessed by one-way analysis of variance (Kruskal-Wallis) and Mann-Whitney U test. For estimates on paired samples, differences were tested by Wilcoxon signed rank test.
RESULTS Serum sTNF-R in patients with rheumatic dis-
ease. Preliminary studies were performed using sam- ples from patients with OA and RA, and the findings were compared with findings in samples from healthy controls. Both sTNF-R were detected in all serum samples tested (Figure I ) . The median level of p75 sTNF-R was -3-4-fold higher than that of p55 sTNF-R. However, levels of both p55 sTNF-R and p75 sTNF-R were significantly increased in both pa- tient groups compared with healthy controls ( P <
0.0002 and P < 0.0004, respectively). Furthermore, levels of both sTNF-R were significantly higher in the RA group than in the OA group ( P < 0.04 for p55 sTNF-R, P < 0.05 for p75 sTNF-R). No correlation was found between age and serum sTNF-R levels (data not shown).
Synovial fluid sTNF-R and IL-2R. Levels of sTNF-R were also investigated in the SF of patients with OA, seronegative arthropathy, and RA. Figure 2 shows that levels of both sTNF-R were significantly increased in both the RA group and the seronegative arthropathy group compared with the OA group (for p55 sTNF-R, P < 0.O004 and P < O.OOO1, respectively, seronegative arthropathy versus OA and RA versus OA; for p75 sTNF-R, P < O.OOO1 for both). Of interest, levels of p55 sTNF-R and p75 sTNF-R in RA joint fluid were significantly higher than those in joint fluid from patients with seronegative arthropathy ( P < 0.OOOl).
SF sIL-2R levels were also measured in the samples depicted in Figure 2. Similar, and also statis- tically significant, differences between disease groups were observed (results not shown). In addition, immu- noreactive T N F a was assayed in these samples. No correlation was seen between T N F a level and diagno- sis, nor between T N F a and sTNF-R levels (P > 0.1; data not shown). Neither were there significant differ- ences (independent of differences related to disease activity) in SF sTNF-R levels between RA patients taking DMARDs and those taking no medication or taking NSAIDs alone (P > 0.15 for p55 sTNF-R; P > 0.9 for p75 sTNF-R).
To determine whether the presence of rheuma- toid factor (RF) contributed to the high levels of sTNF-R observed in RA SF, we preincubated SF samples containing high levels of both sTNF-R and polyclonal IgM-, IgG-, and/or IgA-RF with neutraliz- ing MAb to both sTNF-R. Following this treatment, neither p55 sTNF-R nor p75 sTNF-R was detected in these samples (results not shown); thus, it is unlikely that RF interferes with the sTNF-R ELISA.
Soluble TNF-Rs in paired sera and SF. To con- firm that levels of sTNF-R were increased in the joints of patients with RA, sTNF-R levels were compared in 30 paired sera and SF samples from RA patients (Figure 3). In all samples tested, levels of both p55 sTNF-R and p75 sTNF-R were significantly elevated in SF compared with serum (P < O.OOOl), suggesting local production in the joint. Increased levels in SF compared with serum were also observed in 17 paired samples from patients with seronegative arthropathy (results not shown).
1164
- B p 20- v
E IS- z c,
COPE ET AL
D 400-
350 - 12000 - 300 - - Ioooo- B 250-
cz
c 14000-
- a 2 200-
sr 0 150-
100-
2 8OOo-
6Ooo-
4Ooo- z =!
v)
2000- 0 I @ @ @ f I*:* so 0 -
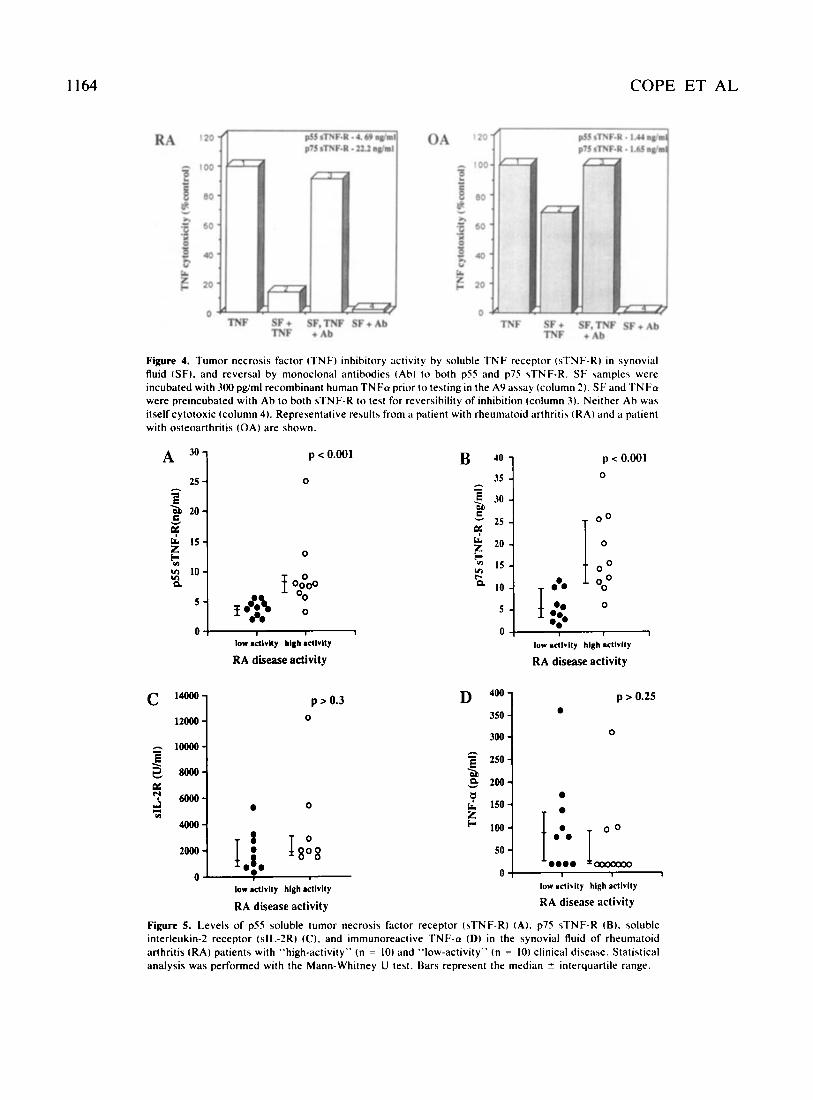
Figure 4. Tumor necrosis factor (TNF) inhibitory activity by soluble TNF receptor (sTNF-R) in synovial fluid (SF). and reversal by monoclonal antibodies (Ah) t o both p55 and p75 sTNF-R. SF samples were incubated with 300 pg/ml recombinant human TNFa prior to testing in the A9 assay (column 2) . SF and TNFa were preincubated with Ab to both sTNF-R to test for reversibility of inhibition (column 3 ) . Neither Ab was itself cytotoxic (column 4). Representative results from a patient with rheumatoid arthritis ( R A ) and a patient with osteoarthritis (OA) are shown.
0 0 I;;@ I, ,
A 301 p c 0.001 p < 0.001
25 4 0
0
low actlvlty hlgh actlvlty
RA disease activity
IS In I- n 10
5
0
0 1
low acllvlly hlgh actlvlty
RA disease activity
p > 0.25
0
p > 0.3 0

SOLUBLE TNF RECEPTORS IN RHEUMATIC DISEASE
- 12.0
- 11.5
- 11.0
- I05
. 10.0
- 95
- 9.0
1165
- 40
. 3s -30
. 2s
. 20
. IS ’ 10
.s
. 0
2 1.0 n
0 5
0.0
- 1M)
- 9 0
- 8 0
- 70
-60 . so . 40
-30
. 20
. 10
- 0
Hb ESR
p75 sTNF-R (ng/ml) --A- Hb(&) + ESR + CRP
Hb ESR CRP
time (weeks)
Figure 6. Longitudinal evaluation of serum levels of p55 soluble tumor necrosis factor receptor (sTNF-R) (upper panel) and p75 sTNF-R (lower panel). relative to hemoglobin (Hb) levels, erythrocyte sedimentation rate (ESR). and C-reactive protein (CRP) levels, in rheumatoid arthritis patient PB, over a 6-week period following treatment with prednisolone and sulfasalazine.
Reversal of sTNF-R inhibition of TNF cytotoxic- ity after treatment with MAb to p55 and p75 sTNF-R. Using the A9 cytotoxicity assay, we measured TNFa bioactivity of SF samples incubated with TNFa, in order to demonstrate that the sTNF-R present in the SF are functional and can effectively inhibit TNF activity. In addition, to assess the specificity of the sTNF-R and whether this inhibition could be reversed, we preincubated samples with neutralizing concentra- tions of MAb to both sTNF-R. Representative results are illustrated in Figure 4. The degree of TNF cyto- toxicity was inhibited by -80% and -26% in the presence of SF from patients with RA and with OA,
respectively; this reflected the total amount of both sTNF-R present (-27 ng/ml and -3 ng/ml, respective- ly). Moreover, this inhibition could be reversed by preincubation with MAb to the 2 sTNF-R. No cyto- toxicity to A9 cells was observed upon treatment with SF and MAb alone.
Correlating between SF sTNF-R levels and dis- ease activity. SF levels of sTNF-R were compared in RA patients whose knee joints (from which the SF was obtained) had been designated as having “high” clin- ical disease activity and those designated as having “low” clinical disease activity, as described in Pa- tients and Methods. Figures 5A and B summarize the
1166 COPE ET AL
findings for p55 sTNF-R and p75 sTNF-R, respec- tively. A significant increase in both sTNF-R was found in joints with active disease ( P < 0.001 for both sTNF-R). In contrast, no difference was observed between the disease activity groups with regard to sIL-2R or TNFa levels (Figures 5C and D). Likewise, differences in bioactive TNFa levels between the groups were not significant (results not shown).
Correlation between serial measurements of sTNF-R and laboratory parameters of disease activity. Figure 6 shows the results of longitudinal evaluation of serum sTNF-R levels in a representative patient with RA; altogether, 6 patients were studied, with similar results. Following treatment with prednisolone (15 mg daily) and sulfasalazine (500 mg daily, increasing over 4 weeks to 2 gm daily), we observed distinct variation in serum sTNF-R levels measured over a 6-week period, associated with concurrent changes in hemo- globin levels, ESR, and CRP levels measured in the same samples. Of note, levels of p55 sTNF-R seemed to reflect ESR levels, and to a lesser extent CRP levels, better than did those of p75 sTNF-R. In con- trast, levels of p55 and p75 sTNF-R assayed over a 6-8-week period in 7 healthy controls were consis- tently within the normal range (data not shown).
DISCUSSION In the last two years, 2 types of cytokine
inhibitors have been reported. There is an IL-1 recep- tor antagonist protein (IL-lra), which is related to IL-Ip and functions as a competitive inhibitor of IL-la and IL-lp, by binding to IL-I receptors (29). The second, and much larger group of cytokine inhibitors, consists of cytokine-binding proteins derived from the extracellular domain of the cytokine receptors. These have been described for a number of different recep- tors, including both TNF receptors (19-22), interfer- on-yR (18), IL-2R (30), IL-4R (31), IL-5R (32), IL-6R (18), IL-7R (33), and CSF-R (34). There is consider- able interest in cytokine inhibitors because they may have therapeutic potential in diseases in which cyto- kines are overexpressed (35). Furthermore, their dis- covery has allowed a more detailed investigation into the role and regulation of cytokines in health and disease, since it is now possible to study the expres- sion of ligands such as TNFa, in conjunction with both their surface receptors and their inhibitors.
We have developed the concept that TNFa is of pivotal importance in the pathogenesis of RA, and is thus a suitable therapeutic target. This is based on the
observations that TNFa is up-regulated in RA joints and induces destruction of cartilage and bone resorp- tion (1,2,36). Furthermore, inhibition of TNFa in RA joint cell cultures with anti-TNFa antibodies resulted in down-regulation of other proinflammatory cytokines such as IL-I (8) and GM-CSF (9). Using the collagen-induced arthritis model in DBA/I mice, we have tested this concept in vivo and found that neu- tralizing hamster anti-TNFa MAb reduces synovial cell infiltration (10). This protective effect was also demonstrable if anti-TNFa was added after the onset of arthritis.
In recent studies we have also shown that both surface TNF-R are up-regulated in RA synovial mono- nuclear cell cultures (24) and are found in abundance in synovial membrane tissue sections, as demon- strated using immunohistochemical techniques (25). Of particular importance was the increased expression of TNF-R at sites of cartilage destruction, such as the cartilage-pannus junction. It was therefore of interest to study levels of both p55 and p75 sTNF-R at sites of enhanced TNFa and surface TNF-R production, since soluble receptors may be important for regulating TNFa in vivo.
Herein we report the results of studies of serum and SF p55 and p75 sTNF-R levels. These revealed a number of interesting features. All patients with arthri- tis had elevated levels of sTNF-R, although the degree of elevation varied between diseases and with degree of disease activity. Soluble p75 TNF-R were more abundant than p55 sTNF-R in all groups, including normal subjects. We have also observed increased levels in patients with Sjogren’s syndrome (Cope et al: unpublished data) and very high levels in patients with active systemic lupus erythematosus (SLE) (37). SF sTNF-R levels were highest in patients with RA, and levels of SF were increased compared with levels in serum, suggesting local production in the joint. Fi- nally, when we compared serum sTNF-R levels with several laboratory parameters, and S F levels with a clinical index, there appeared to be a correlation between sTNF-R levels and disease activity in RA. This was also found in SLE, as described elsewhere (37).
Little is known about the cellular source of sTNF-R, or of the mechanism(s) through which solu- ble receptors are produced. Since there is no evidence for a truncated mRNA encoding a soluble receptor, it is likely that proteolytic cleavage is the mechanism by which sTNF-R are derived from surface TNF-R, an- alogous to the mechanisms described for IL-2R (38). T cells are a likely source of p75 sTNF-R, since elevated

SOLUBLE T N F RECEPTORS IN RHEUMATIC DISEASE 1167
levels of p75 cell surface receptors have been detected on these cells (24,39), and T cells are abundant in RA joints. B cells, which also preferentially express p75 TNF-R may also contribute. Likewise, the increased levels of pSS sTNF-R may be derived from macro- phages, fibroblasts, and epithelial cells, which express surface pS5 TNF-R (40). Neutrophils, found in abun- dance in SF, have been shown to shed their surface TNF-R in response to potent physiologic stimuli such as FMLP, C5a, and GM-CSF (41). Moreover, a recent study has demonstrated that cleavage of surface TNF-R by neutral serine proteases, such as elastase, may be an alternative mechanism by which these cells produce p75 sTNF-R (42). It is therefore likely that these cells are also responsible, at least in part, for the elevated levels of sTNF-R found in SF.
There is evidence that serum sIL-2R are up- regulated in patients with RA but not in patients with OA (26), a finding which is in keeping with the lack of T cells in OA, as well as its non-autoimmune patho- genesis. In our study, we compared sIL-2R and sTNF-R levels and made 2 interesting observations. First, serum sTNF-R levels were elevated in patients with OA. Second, while SF sIL-2R and sTNF-R levels distinguished equally well between different disease groups, only sTNF-R correlated with disease activity in this series. This is in contrast to previous studies in which sIL-2R levels correlated with disease activity (43); the reasons for the discordant results are not known.
While sTNF-R were discovered as serum and urine T N F binding proteins (19-23), it was conceivable that SF sTNF-R, measured in this study by ELISA, may not be capable of inhibiting TNFa. Thus, the capacity of sTNF-R to inhibit TNFa was evaluated. We showed that both RA and OA SF were capable of protecting A9 cells from T N F a cytotoxicity to a degree commensurate with their titer, verifying the potential of sTNF-R to compete for TNFa with sur- face receptors. Thus, it appears that sTNF-R are the natural homeostatic regulators of T N F a action, and that the degree of TNFa-driven inflammatory activity depends on the balance of TNFa and TNF inhibitor
Taken together, these findings suggest that measuring serum sTNF-R levels may be useful for monitoring disease activity, while measuring S F levels could be of potential diagnostic value, in that it can distinguish between different inflammatory arthropa- thies. We have evidence that, despite the presence of high levels of T N F inhibitors in RA joints, levels are
(sTNF-R).
insufficient to neutralize T N F a activity, particularly in sites where surface TNF-R expression is also mark- edly increased. Thus, we have found that all RA joint cell cultures produce T N F a and sTNF-R, and that despite the presence of T N F inhibitors, there is bio- active TNFa, indicating that not all the T N F a is neutralized. In contrast, in some OA joint cell cul- tures, all the bioactive T N F a is neutralized (Brennan FM et al: manuscript in preparation). These results suggest that if T N F a bioactivity could be inhibited further, the destructive process may be halted; thus, clinical trials of anti-TNFa therapy would be of interest.
I .
2.
3.
4.
5 .
6.
7.
8.
9.
REFERENCES Saklatvala J: Tumour necrosis factor a stimulates re- sorption and inhibits synthesis of proteoglycan in carti- lage. Nature 322547-549, 1986 Bertolini DR, Nedwin GE, Bringman TS, Smith DE. Mundy GR: Stimulation of bone resorption and inhibi- tion of bone formation in vitro by human tumour necro- sis factor. Nature 319:516518, 1986 Gamble JR, Harlan JM, Klebanoff SJ, Vadas MA: Stimulation of the adherence of neutrophils to umbilical endothelium by human recombinant tumor necrosis fac- tor. Proc Natl Acad Sci U S A 82:8667-8671, 1985 Shalaby MR, Aggarwal BB, Rinderknecht E, Svedersky LP, Finkle BS, Palladino MA: Activation of human polymorphonuclear neutrophil function by interferon gamma and tumor necrosis factor. J Immunol 135:2069- 2073, 1985 Collins T, Lapierre LA, Fiers W, Strominger JL, Pober JS: Recombinant human tumor necrosis factor increases mRNA levels and surface expression of HLA-A, B antigens in vascular endothelial cells and dermal fibro- blasts in vitro. Proc Natl Acad Sci U S A 83:446450, I986 VilCek J , Palombella VJ, Henriksen-DeStefano D, Swenson C, Feinman R, Hirai M, Tsujimoto M: Fibro- blast growth enhancing activity of tumor necrosis factor and its relationship to other polypeptide growth factors. J Exp Med 163:632-643, 1986 Dayer J-M, Beutler B, Cerami A: Cachectin/tumor ne- crosis factor stimulates collagenase and prostaglandin E2 production by human synovial cells and dermal fibroblasts. J Exp Med 162:2163-2168, 1985 Brennan FM, Chantry D, Jackson A, Maini RN, Feld- mann M: Inhibitory effect of TNFa antibodies on syn- ovial cell interleukin-I production in rheumatoid arthri- tis. Lancet I1:244-247, 1989 Haworth C, Brennan FM, Chantry D, Turner M. Maini RN, Feldmann M: Expression of granulocyte-macro- phage colony stimulating factor (GM-CSF) in rheuma-
1168 COPE ET AL
toid arthritis: regulation by tumour necrosis factor a. Eur J Immunol 21:2575-2579, 1991
isation of a tumour necrosis factor binding protein from urine. Eur J Haematol 42:270-275, 1989
10. Williams RO, Feldmann M, Maini RF: Anti-tumour 22. Seckinger P, Isaaz S, Dayer J-M: Purification and bio-
I I
necrosis factor treatment inhibits the progression of established collagen-induced arthritis (abstract). Arthri- tis Rheum 34 (suppl 9):S67, 1991 Feldmann M, Brennan FM, Chantry D, Haworth C, Turner M, Katsikis P, Londei M, Abney E, Buchan G, Barrett K, Corcoran A, Kissonerghis M , Zheng R, Grubeck-Loebenstein B, Barkley D, Chu CQ. Field M, Maini RN: Cytokine assays: role in evaluation of the pathogenesis of autoimmunity. Immunol Rev 119: 105- 123. 1991
12. Gray PW, Barrett K, Chantry D, Turner M , Feldmann M: Cloning of human tumor necrosis factor (TNF) receptor cDNA and expression of recombinant soluble TNF-binding protein. Proc Natl Acad Sci U S A 87: 7380-7384, 1990
13. Schall TJ, Lewis M, Koller KJ, Lee A, Rice GC, Wong GHW, Gatanaga T , Granger GA, Lentz R, Raab H, Kohr WJ, Goeddel DV: Molecular cloning and expres- sion of a receptor for human tumor necrosis factor. Cell
14. Nophar Y, Kemper 0, Brakebusch C, Engelmann H, Zwang R, Aderka D, Holtmann H, Wallach D: Soluble forms of tumour necrosis factor receptors (TNF-Rs): the cDNA for the type I TNF-R, cloned using amino acid sequence data of its soluble form, encodes both the cell surface and a soluble form of the receptor. EMBO J 9:3269-3278, 1990
15. Smith CA, Davis T, Anderson D, Solam L, Beckmann MP, Jerzy R, Dower SK, Cosman D, Goodwin RG: A receptor for tumor necrosis factor defines an unusual family of cellular and viral proteins. Science 248: 1019- 1023, 1990
16. Heller RA, Song K, Onasch MA, Fischer WH, Chang D, Ringold GM: Complementary DNA cloning of a recep- tor for tumor necrosis factor and demonstration of a shed form of the receptor. Proc Natl Acad Sci U S A 87:6151-6155, 1990
17. Kohno T, Brewer MT, Baker SL, Schwartz PE, King MW, Hale KK, Squires CH, Thompson RC, Vannice JL: A second tumor necrosis factor receptor gene prod- uct can shed a naturally occurring tumor necrosis factor inhibitor. Proc Natl Acad Sci U S A 87:8331-8335, 1990
18. Novick D, Engelmann H, Wallach D, Rubenstein M: Soluble cytokine receptors are present in normal urine. J Exp Med 170:1409-1414, 1989
19. Engelmann H, Novick D, Wallach D: Two tumor necro- sis factor-binding proteins purified from human urine. J Biol Chem 265:1531-1536, 1990
20. Seckinger P, Isaaz S, Dayer J-M: A human inhibitor of TNFa. J Exp Med 167:1511-1516, 1988
21. Olsson I, Lantz M, Nilsson E: Isolation and character-
61:361-370, 1990
logic characterization of a specific tumor necrosis factor inhibitor. J Biol Chem 264: 11966-1 1973, 1989
23. Aderka D, Engelmann H, Hornik V, Skornick Y, Lev0 Y, Wallach D, Kushtai G: Increased serum levels of soluble receptors for tumor necrosis factor in cancer patients. Cancer Res 51:5602-5607. 1991
24. Brennan FM, Gibbons DL, Mitchell T , Cope AP, Maini RN, Feldmann M: Enhanced expression of TNF recep- tor mRNA and protein in mononuclear cells isolated from rheumatoid arthritis synovial joints. Eur J Immunol
25. Deleuran BD, Chu C-Q, Field M, Brennan FM, Mitchell T , Feldmann M, Maini RN: Localization of tumor necrosis factor receptors in the synovial tissue and cartilage-pannus junction in patients with rheumatoid arthritis: implications for local actions of tumor necrosis factor a. Arthritis Rheum 35: 1170-1178, 1992
26. Keystone EC, Snow KM, Bombardier C, Chang C-H, Nelson DL, Rubin LA: Elevated soluble interleukin-2 receptor levels in the sera and synovial fluids of patients with rheumatoid arthritis. Arthritis Rheum 31 :844-849, I988
27. Ropes MW, Bennett GA, Cobb S, Jacox R, Jessar RA: 1958 revision of diagnostic criteria for rheumatoid arthri- tis. Bull Rheum Dis 9: 175-176, 1958
28. Doherty M, Richards N, Hornby J , Powell R: Relation between synovial fluid C3 degradation products and local joint inflammation in rheumatoid arthritis, osteo- arthritis, and crystal associated arthropathy. Ann Rheum Dis 47: 190-197, 1988
29. Hannum CH, Wilcox CJ, Arend WP, J o s h FG, Dripps DJ, Heimdal PL, Armes LG, Sommer A, Eisenberg SP, Thompson RC: Interleukin- 1 receptor antagonist activ- ity of a human interleukin-1 inhibitor. Nature 343:33& 340, 1990
30. Rubin LA, Kurman CC, Fritz ME, Biddison WE, Bou- tin B, Yarchoan R, Nelson DL: Soluble interleukin-2 receptors are released from activated human lymphoid cells in vitro. J Immunol 135:3172-3177, 1985
31. Fernandez-Botran R, Vitetta ES: A soluble, high affinity interleukin-4 binding protein is present in the biological fluids of mice. Proc Natl Acad Sci U S A 87:4202-4206, 1990
32. Tavernier J , Devos R, Cornelis S, Tuypens T , van der Heyden J, Fiers W, Plaetinck G: A human high affinity interleukin-5 receptor (ILSR) is composed of an IL5- specific a chain and a p chain shared with the receptor for GM-CSF. Cell 66: 1175-1 184, 1991
33. Goodwin RG, Friend D, Ziegler SF, Jerzy R, Falk BA, Gimpel S, Cosman D, Dower SK, March CJ, Namen AE, Park LS: Cloning of the human and murine inter- leukin-7 receptors: demonstration of a soluble form and
22:1907-1912, 1992

SOLUBLE TNF RECEPTORS IN RHEUMATIC DISEASE 1169
homology to a new receptor superfamily. Cell 60:941- 951, 1990
34. Downing JR, Roussel MF, Sherr CJ: Protein kinase C “transrnodulates” the colony stimulating factor-I recep- tor by activating a membrane-associated protease that specifically releases the receptor ligand-binding domain from the cell. Clin Res 37:544A, 1989
35. Feldmann M: Review: cytokine networks; do we under- stand them well enough to facilitate clinincal benefits? Eur Cytokine Net 2:5-9, 1991
36. Buchan G, Barrett K, Turner M, Chantry D, Maini RN, Feldmann M: Interleukin- I and tumour necrosis factor mRNA expression in rheumatoid arthritis: prolonged production of IL-la. Clin Exp Immunol 73:449-455, 1988
37. Aderka D, Engelmann H, Wyssenbeek, Cope AP. Mo- lad Y, Feldmann M, Hornick V , Maini RN, Alpert G. Lev0 Y, Wallach D: Increased serum soluble receptors for tumour necrosis factor in systemic lupus erythema- tows correlate with disease activity. Submitted for publication
38. Robb RJ, Kutny RM: Structure-function relationships for the IL-2 receptor system IV analysis of the sequence
and ligand binding properties of soluble Tac protein. J Immunol 139:855-862, 1987
39. Andrews JS, Berger AE, Ware CF: Characterization of the receptor for tumor necrosis factor (TNF) and lym- photoxin (LT) on human T lymphocytes. J Immunol
40. Brockhaus M, Schoenfeld HJ, Schlaeger E-J, Hunziker W, Lesslauer W, Loetscher H: Identification of two types of tumor necrosis factor receptors on human cell lines by monoclonal antibodies. Proc Natl Acad Sci U S
41. Porteu F, Nathan C: Shedding of tumor necrosis factor receptors by activated human neutrophils. J Exp Med 172:599-607, 1990
42. Porteu F, Brockhaus M, Wallach D, Engelrnann H, Nathan C: Human neutrophil elastase releases a ligand- binding fragment from the 75-kDa tumor necrosis factor (TNF) receptor. J Biol Chem 266:1884&18853, 1991
43. Symons JA, Wood NC, DiGiovane FS, Duff GW: Solu- ble IL-2 receptor in rheumatoid arthritis: correlation with disease activity, IL-I, and IL-2 inhibition. J Imrnu- no1 141:2612-2618, 1988
144:2582-2591, 1990
A 87~3127-3131, 1990
Copyright © 2022 FDOKUMEN




















